Sarah DuVall, M.P.H. Bureau of Immunization New York State Department of Health June, 2010.
55
Sarah DuVall, M.P.H. Bureau of Immunization New York State Department of Health June, 2010
-
Upload
rosaline-blankenship -
Category
Documents
-
view
219 -
download
1
Transcript of Sarah DuVall, M.P.H. Bureau of Immunization New York State Department of Health June, 2010.

Sarah DuVall, M.P.H.Bureau of Immunization
New York State Department of Health June, 2010

Influenza (Flu)
The flu is a viral infection that can be caused by a number of different influenza strains.
The flu affects the lungs, throat, nose, and other parts of the body.
Unlike the common cold, the flu comes on suddenly, can make people very sick for a week or longer, and can send them to the hospital.
2

How Flu is Transmitted
Easily spread from person to person via respiratory droplets when an infected person coughs or sneezes.
Also spread when someone touches a surface contaminated with the virus.
Airborne transmission of the virus is possible, when an infected person is talking.
Adults shed the infectious influenza virus 1-2 days before any symptoms appear.
3CDC Epidemiology and Prevention of Vaccine-Preventable Diseases 2009

The Flu is a Serious Illness
Flu is the 8th leading cause of death in the U.S.
Flu kills as many or more Americans than breast cancer.
Approximately 36,000 Americans will die because of the flu this year.Poland et al., Vaccine 2005;23:2251-5.
CDC/ National Center for Health Statistics. Deaths and Mortality 2006.
4

Deaths*25,000 to 72,000Hospitalizations*
117,000 to 816,000
Infections and illnesses50 to 60 million
Physician visits~25 million
Thompson WW et al. JAMA. 2003;289:179-186; Thompson WW et al. JAMA. 2004;292:1333-1340; Couch RB. Ann Intern Med. 2000;133:992-998; Patriarca PA. JAMA. 1999;282:75-77; ACIP. MMWR. 2004;53(RR06):1-40.
Influenza Disease Burden in the United States in an Average Year
* All-cause hospitalization and mortality associated with influenza virus infection.
5

Confirmed Influenza Outbreaks in NYS Hospitals and LTCFs, by Year
NYSDOH *Extended influenza season through August 2009. 6

Morbidity from Influenza Outbreaks in NYS Hospitals and LTCFs, by Year
0
2000
4000
6000
8000
10000
'00-01 '01-02 '02-03 '03-04 '04-05 '05-06 '06-07 '07-08 '08-09*Year
PatientsStaff
Nu
mb
er
Ill
NYSDOH * Extended influenza season through August 2009. 7

Impact on Health Care Facilities
Influenza is highly contagious.
Can spread rapidly through a health care facility.
Influenza is transmitted to patients by friends, family, and health care personnel (HCP).
Patients receiving home care services are at high risk of complications from influenza due to their age and medical conditions.
APIC Member Initiative Protect your patients. Protect yourself. 20048

Impact on Health Care Facilities
Up to ¼ of HCP contract influenza each season.
A CDC hospital survey conducted during flu season showed the following: 35% reported staffing shortages.
Poland et al., Vaccine 2005;23:2251-5.9

Role of HCP in Nosocomial Transmission of Influenza Many HCP work while ill with influenza like illness
(ILI).
>75% MDs and RNs surveyed reported working while ill with an ILI.
37% of residents worked while ill with ILI.
Otherwise healthy adults may experience minimal symptoms but shed, and transmit, influenza virus.
>25% who seroconverted did not recall an ILI or any respiratory tract illness. Foy, Am J Epi, 1987
10
Weingarten, AJIC, 1989

Essential Component of a Health Care Institution’s Occupational Health Program
Ensure the immunity of HCP to infections or diseases caused by relevant infectious agents.
Two fundamental legal and moral duties:
Protection of personnel from risk of the work place.
Protection of patients from risks posed by infectious HCPs.
Decker MD, et al. Hospital Epidemiology and Infection Control 3rd ed.11

Definition of HCP and Facility
Those with direct patient care: MDs, RNs, nursing assistants, therapists, technicians, emergency personnel, dental personnel, pharmacists, lab personnel, autopsy personnel, students, trainees, volunteers.
“Those not directly involved with patient care but potentially exposed to infectious agents that can be transmitted to and from HCP,” such as clerical, dietary, housekeeping, and maintenance staff.
Influenza Vaccination of Health-Care Personnel Recommendations of ACIP and HICPAC-MMWR 200612

Definition of HCP and Facility (con’t)
Facilities include “acute care hospitals, nursing homes, skilled nursing facilities, physician’s offices, urgent care centers, and outpatient clinics, and to persons who provide home health care and emergency medical services.”
Influenza Vaccination of Health-Care Personnel Recommendations of ACIP and HICPAC-MMWR 2006
13

All HCP Should Be Vaccinated
Regardless of their employment status.
Includes HCP with direct contact with patients (e.g., nurses, technicians, physical therapist, physicians, students).
Includes HCP without direct patient care responsibilities (e.g., environmental service worker, security, contract service workers, emergency medical personnel).
14Poland et al., Vaccine 2005;23:2251-5.

How to Prevent Influenza Infection1.Implement policies that motivate HCPs to stay home
when they are sick.
2.Encourage appropriate infection control techniques.
but this is not enough……
HCP can still spread the flu even when they DON’T feel sick.
50% of infected people don’t have symptoms when they are infected.
All individuals are contagious for at least 1 day before they have symptoms.
3.The best protection is VACCINATION. APIC Member Initiative Protect your patients. Protect yourself. 2004
15

Why Vaccination of HCP Works Vaccination is most effective in younger, healthier
individuals.
70%-90% effective among healthy persons <65 years of age.
Patients at highest risk, including the elderly and the immunocompromised, are least likely to develop an adequate response to the vaccine.
30-40% effective among frail elderly persons.
Therefore, vaccination of those individuals who come in contact with our vulnerable population is the most effective strategy for prevention.
CDC Epidemiology and Prevention of Vaccine-Preventable Diseases. 2009
APIC Member Initiative Protect your patients. Protect yourself. 2004
16

Benefits of Influenza Vaccination
1.Reduction in nosocomial influenza and influenza-related deaths.
Over 12 years in one hospital, vaccination coverage increased from 4% to 67%.
Laboratory-confirmed influenza cases among HCP decreased from 42% to 9%.
Nosocomial cases among hospitalized patients decreased 32% to 0 (p<0.0001). Salgado et al., Inf Cont Hosp Epi 2004;25:923-8
Two randomized controlled trials evaluated impact of HCP influenza vaccination on residents in nursing homes.
They estimated >40% decrease in overall mortality among residents in the setting of high employee vaccination levels, regardless of patient vaccination levels.
Carman et al., Lancet 2000;355(9198): 93—7
Potter, et al., J Infect Dis 1997;175:1--617

Benefits of Influenza Vaccination2.Reduction in staff illness and illness related
absenteeism.
Workers who receive influenza vaccine take approximately 50% fewer sick days.
Replacement workers can result in increased expenses caused by decreased productivity, increased medical errors, and disrupted work environments.
Staff shortages can be exacerbated by influenza outbreaks.
Double shifts increase the probability of medical errors.
The cost of promoting and delivering vaccinations to health care personnel is lower than the costs associated with influenza illness.
Burls et al., Vaccine 2006;24:4212-21.
APIC Member Initiative Protect your patients. Protect yourself. 2004
18

Reduction in the Incidence of Influenza Infection and Related Issues in HCP Receiving Vaccination
19Massachusetts Medical Society, Masspro, MDPH Employee Flu Immunization Campaign Kit 2006

Month of Peak Influenza Activity United States, 1976-2006
0
5
10
15
20
25
30
35
40
45
50
Dec Jan Feb Mar Apr May
Pe
rce
nt
13%
19%
45%
13%
3% 3%
MMWR 2007;55(RR-6):5
There is usually ample time to vaccinate HCP
before influenza occurs!
20

Vaccination Rates Need Improvement
In 2006-07, only 44% of HCP were immunized against influenza in the U.S.
Includes all HCP who have contact with patients.
Despite aggressive national efforts, rates of HCP immunized have stayed around 40%.
MMWR.2009:58(early release): 1-5221

Barriers to Vaccination Reasons HCP decline influenza vaccination:
Misconception that vaccination can cause influenza (10-45%).
Fear of adverse events (8-54%). Times/locations of vaccination were unsuitable (6-59%). Perception that they are not at risk (6-58%). Fear of injections (4-26%). Lack of vaccine efficacy (3-32%) - except physicians. Doubt that influenza is a serious disease (2-32%).
Two main barriers: Misperception of influenza, its risks, the role of HCP in its’
transmission to patients, and the importance and risks of vaccination.
Lack of (or perceived lack of) conveniently available vaccine.
22Hofman et al., Infection 2005;34:142-147

Reasons for Rejecting Vaccination Among Health Care Personnel
ReasonPhysician %
Nurse %
Technician
or Aide %
Admin. Worker %
Medical Student %
Other %
Vaccine shortage 57 40 58 53 34 48
Concern about side effects
17 34 36 25 23 28
Never get influenza 14 25 27 18 23 22
Inconvenience* 26 9 4 7 34 13
Forgot 18 8 5 2 11 8
Christini AB, et al. Infect Control Hosp Epidemiol 2007;28:171-7
*Vaccine needs to be made available during all employment shifts.
Primary Reasons >30%
Barriers to Vaccination

Reasons for Accepting Vaccination Among Health Care Personnel
ReasonPhysician %
Nurse %
Technician
or Aide %
Admin. Worker %
Medical Student %
Fear of getting influenza 77 77 60 71 75
Fear of transmission to patients
78 59 60 36 64
Vaccine is safe 77 56 42 38 63Vaccine is effective 70 55 47 36 59
Vaccine was free 44 54 49 62 76Close contact with high risk person at home
45 56 42 43 9
Convenient 28 38 44 45 53Christini AB, et al. Infect Control Hosp Epidemiol 2007;28:171-7
Motivators for VaccinationPrimary Reasons>60%

Joint Commission Quality MeasureHCP Influenza Vaccination Levels
Standards for Influenza Vaccination Programs in Accredited Institutions, 2007
1) Annual influenza vaccination program that includes at least staff and licensed independent practitioners.
2) Provide access to influenza vaccination on-site.
3) Educate staff and licensed independent practitioners about influenza vaccination; non-vaccine control measures; and diagnosis, transmission and potential impact of influenza.
4) Annually evaluate vaccination rates and reasons for nonparticipation by staff and licensed independent practitioners.
5) Implement enhancements to the program to increase participation.
This standard is an accreditation requirement as of January 1, 2007.
25

Improving Compliance
Leadership Support Education Accessibility Incentives Feedback and Follow-up Mandatory Vaccination Measure Vaccination Rates
26

Leadership Support
Leadership involvement is essential for a successful program.
Leadership is responsible for: Establishing expectation that influenza
vaccination of HCP is a patient safety issue. Making sure vaccination program has adequate
resources. Reducing or eliminating barriers. Being a role model.
CDC and The Joint Commission Improving Your Vaccination Program 200927

Education HCP need to know when and where education
and vaccinations will be offered and the importance of the vaccination.
Promoting vaccinations can take many forms in many venues, including: E-mail notice and reminders. Newsletters, with regular updates. Posters.* Screen savers. Stickers worn by health care personnel.* Messages delivered in person at meetings or health fairs.*
*NYSDOH and the CDC offer FREE materials, www.nyhealth.gov/ www.cdc.gov
CDC and The Joint Commission Improving Your Vaccination Program 2009 28

Accessibility
Provide free vaccines at work. Use leaders as supportive role models. Use vaccination clinics, mobile carts.
Link vaccinations to required activity. Mandatory tuberculin skin testing. Annual safety competency or skills days. Disaster drills.
CDC and The Joint Commission Improving Your Vaccination Program 2009
29

Incentives for HCPs
Financial incentives (discounts on benefits, impact on merit increases, consideration in granting decisions regarding time off).
HCP recognition.
Need to understand HCPs motivation.
CDC and The Joint Commission Improving Your Vaccination Program 2009
30

Feedback and Follow-up
Review list of non-vaccinated employees weekly.
Provide weekly reminders to supervisors with list of non-vaccinated employees.
Identify central authority figure to add pressure to comply. Buy-in from administration is key.
Put pressure on employee to make active decision, instead of allowing passive avoidance.
Continue until goals are met.
McCullers JA, et al., Inf Cont Hosp Epi, 2006;27:77-9.31

Mandatory VaccinationMultiple groups support mandatory vaccination:
New York State Department of Health
American College of Physicians “An ethical obligation”
Association for Professionals in Infection Control and Epidemiology “HCP have an obligation…”
Infectious Disease Society of America
“…likely to be the most effective means to protect patients against the transmission of seasonal and H1N1 influenza by HCWs.”
National Patient Safety Foundation
U.S. Department of Defense (DOD) Mandatory seasonal influenza vaccination requirement for civilian
health care personnel who provide direct patient care in DOD facilities.
32

33
U.S. Health Systems with HCP Influenza Vaccination Mandates (4/10*)
Battle Creek Health System, Battle Creek, MI Barnes Jewish Corporation (BJC) HealthCare, St.
Louis, MO Bronson Methodist Hospital, Kalamazoo, MI Capital Region Medical Center, Jefferson City, MO Children's Hospital of Orange County, CA Children’s Hospital of Philadelphia Children's Hospital of The King's Daughters Health
System, Norfolk, VA Creighton University Genesis HealthCare System, Zanesville, OH Fort Walton Beach Medical Center, Fort Walton
Beach, FL Hoag Hospital, Newport Beach, CA Hospital of the University of Pennsylvania Johns Hopkins Health System, MD Kewanee Hospital, Kewanee, IL Lakeview Medical Center, Rice Lake, WI Long Beach Memorial Medical Center, Long Beach,
CA Loyola University Health System, Chicago, IL MedStar Health, Maryland and Washington, DC
Michigan State University/Kalamazoo Center for Medical Studies
Miller Children's Hospital, Long Beach, CA New York-Presbyterian Hospital, New York Orange Coast Memorial Medical Center, Fountain
Valley, CA Pacific Hospital of Long Beach, CA Petaluma Valley Hospital, Petaluma, CA Saddleback Memorial Medical Center, Laguna Hills, CA Saint Alphonsus Regional Medical Center, Boise, Idaho Santa Rosa Memorial Hospital, Santa Rosa, CA Spectrum Health Hospitals, Grand Rapids, MI St. Joseph Health System, Orange, CA St. Jude Medical Center, Fullerton, CA Swedish Medical Center, Englewood, CO Tri-Health, Good Samaritan and Bethesda North
Hospitals, Cincinnati, OH UC ((University of California) Davis Health System,
Sacramento, CA UC (University of California) Irvine Healthcare, Orange,
CA Virginia Mason Medical Center, Seattle, WA
*http://www.immunize.org/laws/influenzahcw.asp

34MMWR Vol. 59 / No. 12 April 2, 2010

Measure HCP Vaccination Rates
Measurement is essential to your program.
Only through measurement is it possible to determine if performance is getting better, worse, or staying the same.
Capture alternative administration (for example: clinics, physician offices, pharmacies, etc.).
CDC and The Joint Commission Improving Your Vaccination Program 2009 35

Purchasing Influenza Vaccine
Pre-book vaccine in January or February.Influenza vaccines take months to produce. Vaccine manufacturers are hesitant to risk
producing products they will be unable to sell.
For more information on distributors and influenza vaccine availability, please visit the following websites: Influenza Vaccine Distributor Information http://www.flusupplynews.com/resources.cfm Influenza Vaccine Availability Tracking System (IVATS) http://www.preventinfluenza.org/ivats/ivats_healthcare.asp
36

Purchasing Influenza Vaccine
Available Vaccines 4 trivalent inactivated vaccines (TIV),
administered intramuscularly: Fluzone® - 6 mos and older FLUVIRIN® - 4 yrs and older FLUARIX™ - 18 yrs and older FluLaval™ - 18 yrs and older
1 trivalent live, attenuated vaccine (LAIV) administered as a nasal spray: FluMist® - healthy people 2 to 50 years old
37

Vaccine Information
Using Nasal Spray (LAIV )
LAIV may be used for healthy, non-pregnant HCP <50 yrs old.
At times of vaccine shortage, LAIV is “especially encouraged” unless contraindicated.
HCP who work with severely immunocompromised patients in a protected environment should NOT receive LAIV (bone marrow transplant unit staff).
LAIV can be used to vaccinate HCP who have close contact with persons with a lesser degree of immunosuppression (e.g., persons with diabetes, persons with asthma taking corticosteroids, or persons infected with HIV).
Transmission of LAIVhas NEVER been documented in a health care facility.
CDC and The Joint Commission Improving Your Vaccination Program 200938

Vaccine Information
Efficacy Intramuscular Injection (TIV): Effectiveness in adults < 65 years
80% (95% CI 56% to 91%) when vaccine matched circulating strain.
50% (95% CI 27% to 65%) when not well matched. Jefferson, et al. Cochrane Database Syst Rev. 2007 Apr 18;(2):CD001269.
Nasal Spray (LAIV): Effectiveness in healthy adults Overall efficacy of LAIV and inactivated influenza vaccine in
preventing; laboratory-documented influenza, 85% LAIV and 71% TIV.
Treanor et al., Vaccine 1999;18:899—906.
Even with suboptimal vaccine-wild virus match: 24% fewer febrile upper respiratory illness episodes (URI). 27% fewer lost work days due to febrile URI. 41%-45% fewer days of antibiotic use. Nichol et al., JAMA 1999;282:137—44.
39

Vaccine Information
Adverse Events Intramuscular Injection (TIV)
Local Reactions - 15%-20% (TIV) Fever, malaise - not common Allergic reactions - rare (<1 in 1 million, Anaphylaxis) Neurological - rare (1 in 1 million, Guillain-Barre
Syndrome) U.S. Department of Health & Human Services Influenza Vaccination of Health-care Personnel
2008
Nasal Spray (LAIV) Local Reactions:
cough 14% runny nose 45% sore throat 28% chills 9%
Belshe RB et al. Clin Infect Dis 2004;39:920--7. 40

Neither LAIV or TIV Vaccines Can Cause Influenza Disease
TIV contains only non-infectious fragments of influenza virus.
LAIV cannot replicate in the lower respiratory track.
41

Influenza Vaccination MandateSHRPC adopted an emergency regulation, 10 NYCRR,
Subpart 66-3.
Applied to HCP in certain Health Care Facilities.Direct patient contactContact with those who have direct patient contact.
ONLY medical exemptions allowed.
Began- August 13, 2009, effective immediately;Suspended-October 23, 2009Expired (no-renewal)-November 11, 2009.Vaccination or provision of documentation no later
than November 30 of each yearNew Employees- to be vaccinated November- April. NYSDOH is currently pursuing a permanenet
regulation. 42

Hospital Survey
New York State (including New York City)
211 Hospitals--------100% compliance
43

Vaccine Type
# of Hospitals
# of HCP
# of HCP Vaccinate
d
Mean # of HCP Vaccinated
Range % of HCP Vaccinated
Seasonal 08-09
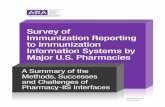
211472,806
201,118 953 0-93%
Seasonal 09-10 332,955 2,241 20-100%
H1N1 09-10 457,531 125,590 2,168 0.01-100%•66% increase in the # of HCP Vaccinated with the mandate in place.•62% less HCP were vaccinated against H1N1 influenza than seasonal influenza.
% of Health Care Personnel (HCP) Vaccinated in New York State

• The % vaccinated is the same for Seasonal influenza and lower for H1N1 influenza.
45

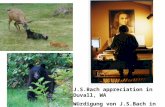
SeasonalExempt_percent
0.00
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
0.10
0.11
0.12
Seasonal_percent09
0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
% Medical Exemptions by % Vaccinated (Seasonal)
46

47

Reasons for Outliers
High Medical Exemption Rates“Local physicians opposed the mandate”Problematic medical exemptions require follow
up.
Low Vaccination RatesHCP strongly opposed the mandate. HCP concerned about vaccine safety.Limited Vaccine Supply.
48

49

Seasonal 08-09 Seasonal 09-10 H1N1 09-10
Group# of Hospitals % Range
Mean % Vaccinated % Range
Mean % Vaccinated
% Range
Mean % Vaccinated
NYC 57 9-86% 39% 20-100% 68% 0.1-40% 16%
Metro. (exc. NYC) 41 0-71% 42% 34-98% 70% 8-100% 28%
NYS (exc. NYC & Metro) 113 0-93% 51% 23-100% 74% 11-100% 46%
NYS (exc. NYC & inc. Metro)
154 0-93% 49% 23-100% 73% 8-100% 41%50

Medical Exemptions
Seasonal 09-10 H1N1 09-10
Mean Range% Mean Range%
NYC 35 20-100% 22 0-9%
Metro (exc. NYC) 19 34-98% 7 0-3%
NYS (exc. NYC and Metro) 17 23-100% 12 0-11%
NYS (exc. NYC & inc. Metro) 17 23-100% 11 0-11%51

Other Recommended Vaccinations
52

Vaccination of Health Care Personnel
HCP vaccination is an essential line of defense to prevent the spread of infections:
to and from patients to HCPs,
among HCPs, and
from HCPs to patients.
Decker MD, et al. Hospital Epidemiology and Infection Control 3rd ed.
53

Other Valuable Resources New York State Department of Health: Resources and Guidance –HCP Vaccination http://www.nyhealth.gov/prevention/immunization/health_care_personnel/
Centers for Disease Control and Prevention-Resources and Guidance-Health Care Personnel Vaccination
http://www.cdc.gov/vaccines/spec-grps/hcw.htm
U.S. Department of Health & Human Services: Toolkit-HCP Vaccination http://www.hhs.gov/ophs/programs/initiatives/vacctoolkit/index.html
Association for Professionals in Infection Control and Epidemiology: Toolkit-HCP Vaccination
http://www.apic.org/Content/NavigationMenu/PracticeGuidance/Topics/Influenza/toolkit_contents.htm
The Joint Commission: FREE-PODcasts, audio conference and additional resources-HCP Vaccination
http://www.jcrinc.com/Audio-Conferences-Web-Conferences/Flu-Vaccination-Challenge/Resources/
U.S. Food and Drug Administration: Video-HCP Vaccination http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/psn/transcript.cfm?show=81#4
54