Role of active observation in the management of thyroid papillary microcarcinoma Joint Hospital...
21
Role of active observation Role of active observation in the management of in the management of thyroid papillary thyroid papillary microcarcinoma microcarcinoma Joint Hospital Surgical Grand Joint Hospital Surgical Grand Round Round PYNEH, 18 PYNEH, 18 th th April 2015 April 2015 Lam Shi, RH Lam Shi, RH
-
Upload
esmond-wilkins -
Category
Documents
-
view
214 -
download
0
Transcript of Role of active observation in the management of thyroid papillary microcarcinoma Joint Hospital...
Role of active observation Role of active observation in the management of in the management of
thyroid papillary thyroid papillary microcarcinomamicrocarcinoma
Joint Hospital Surgical Grand RoundJoint Hospital Surgical Grand Round
PYNEH, 18PYNEH, 18th th April 2015April 2015
Lam Shi, RHLam Shi, RH

DefinitionDefinition
papillary thyroid microcarcinoma (PTMC)papillary thyroid microcarcinoma (PTMC)
– papillary carcinoma ≤ 1cmpapillary carcinoma ≤ 1cm
WHO monograph on histologic typing of thyroid tumorsWHO monograph on histologic typing of thyroid tumors

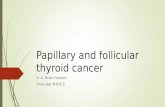
Rising incidence of Rising incidence of small papillary thyroid carcinoma (PTC)small papillary thyroid carcinoma (PTC)
North America 1980 - 2008North America 1980 - 2008
PTC
PTC follicular variantFollicular carcinoma
87% PTCs < 2cm
Pellegriti et al. J Cancer Epidemiol Pellegriti et al. J Cancer Epidemiol 20132013Davies et al. JAMA 2006Davies et al. JAMA 2006

FNAC: PTC
Risk FactorsAge > 45H&N irradiationMultifocalLocal / LN invasionAggressive histologyT3 (> 4cm)
≤ 1cm
Total or Hemithyroidectomy
1-4cm
Total thyroidectomy
No
Any
Total thyroidectomy + prophylactic Lv 6 LN dissection
therapeutic MND
Thyroid scan
+/- RAI
Current management of PTMCCurrent management of PTMC
McLeod. Lancet 2013

Excellent outcomes of Excellent outcomes of surgical treatment for PTMCsurgical treatment for PTMC
Author, yearFollow-
up (Year)
No. of patients
Recurrence Mortality
Noguchi, 2011
10 867 1% 0.2%
Baudin, 1998 7.3 281 4% 0%
Ito, 2003 10 626 5% 0%
Hay, 2008 17.2 900 6% 0.3%
Chow, 2003 10 203 7% 1%

Favorable outcome of Favorable outcome of incidentalincidental vs vs non-indicentalnon-indicental PTMC PTMC
Author N
Multicentric
(%)
Bilateral(%)
Lymph nodemet (%)
Distantmet (%)
Recurrence (%)
Mortality(%)
I NI I NI I NI I NI I NI I NI
Baudin28
13
061
13
23 22 91 0 8.62.
17.6 0 0
Pellegriti
299
25
391
522 16 45 0.7 4.7 ns ns 0 0
Roti24
31
936
11
20 4 16 0 2 ns ns 0 0
Lo18
41
232 0 39 0 2.7 0 12 0 3.6
I = incidental; NI = non-incidental

““Over-treatment” of latent PTCs?Over-treatment” of latent PTCs?
Prevalence Prevalence of PTMCof PTMC == 3 3 –– 18 % 18 % Autopsy series 1966 Autopsy series 1966 –– 1990 1990 Pacini. Pacini.
20122012
Incidence Incidence Ca thyroid =Ca thyroid = 1.6 1.6 –– 6 / 100 000 6 / 100 000 Registry data 1973 Registry data 1973 –– 1977 1977 Pre-USG era Pre-USG era Kilfoy et al. 2009Kilfoy et al. 2009
Ca thyroid relatedCa thyroid related mortality mortality = 0.5 / 100 000= 0.5 / 100 000 Epidemiology database 1973 Epidemiology database 1973 –– 2002 2002 Davies et al. Davies et al.
20062006

Can PTMCs be observed without Can PTMCs be observed without immediate surgery ? immediate surgery ?
HypothesisHypothesis A significant proportion of PTMCs are indolent and may A significant proportion of PTMCs are indolent and may
not manifest in onenot manifest in one’’s lifetimes lifetime
ProposalProposal To observe newly diagnosed incidental PTMCTo observe newly diagnosed incidental PTMC Operate only when lesion showed sign of progressionOperate only when lesion showed sign of progression
QuestionQuestion Safety of delaying surgery until lesion showed evidence Safety of delaying surgery until lesion showed evidence
of progression ? of progression ?

1993 -20011993 -2001 732 patients with 732 patients with FNAC diagnosed PTMCFNAC diagnosed PTMC exclusionexclusion (570): (570):
– RLN palsyRLN palsy– tumor close to trachea / RLNtumor close to trachea / RLN– suspicious LN in lateral compartmentssuspicious LN in lateral compartments– high grade malignancyhigh grade malignancy– patientpatient’’s choices choice
162 patients for 162 patients for observationobservation USGUSG every 6 every 6 –– 12 months 12 months surgery if tumor progresses surgery if tumor progresses ≥ 10mm≥ 10mm, new suspicious , new suspicious
LN in lateral compartmentLN in lateral compartment
Ito et al. (2003) - An observation trial for PTMCIto et al. (2003) - An observation trial for PTMC

162 patients 162 patients followed-up for followed-up for 18 – 113 months (mean 18 – 113 months (mean 47)47)
Tumor sizeTumor size no change at all time points: 70 - 83%no change at all time points: 70 - 83% increase to increase to ≥≥ 10mm: 18 (11%) 10mm: 18 (11%)
Lymph node (lateral compartment)Lymph node (lateral compartment) 2 (1.2%) newly detected by USG2 (1.2%) newly detected by USG
Operation rate Operation rate 56 patients (35%) operated56 patients (35%) operated At 19 – 56 months after observationAt 19 – 56 months after observation indications: disease progression (9), ? patientindications: disease progression (9), ? patient’’s s
choice (47)choice (47)
Ito et al. (2003) - An observation trial for PTMCIto et al. (2003) - An observation trial for PTMC

% TNM staging (AJCC 6th Ed. 2002)% TNM staging (AJCC 6th Ed. 2002)
pTpT pNpN MM
00 6363 100100
1a1a 5050 3232 00
1b1b 4141 55
22 55
33 00
4a4a 33
Clinical outcomeClinical outcome local recurrence 2.6%local recurrence 2.6% distant metastasis / mortality 0%distant metastasis / mortality 0%
Ito et al. (2003) - An observation trial for PTMCIto et al. (2003) - An observation trial for PTMC
< 1cm
1 – 4 cm
> 4 cm
Extra-cap invasion

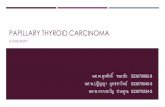
1993 -2011, 1993 -2011, n = 1235n = 1235 follow-up 1.5 – 19 years (mean 5 years)follow-up 1.5 – 19 years (mean 5 years) 58 (4.6%) with tumor enlargement; 43 (3.5%) > 12mm58 (4.6%) with tumor enlargement; 43 (3.5%) > 12mm 19 (1.5%) LN metastasis during observation19 (1.5%) LN metastasis during observation 10-year rates10-year rates
– size enlargement – 8.3% (6.8% > 12mm)size enlargement – 8.3% (6.8% > 12mm)– new LN during observation – 3.8%new LN during observation – 3.8%– Age < 40 as an independent predictorAge < 40 as an independent predictor
191 (16%) underwent operation191 (16%) underwent operation post-operative follow-up 75 monthspost-operative follow-up 75 months
– Local recurrence 0.5%Local recurrence 0.5%– Mortality 0Mortality 0
Ito et al. (2013) – Age predicts progressionIto et al. (2013) – Age predicts progression

Tumor enlargement
> 12mm
New lymph node
1993 -20011993 -2001 230 patients chose initial observation230 patients chose initial observation 300 PTMCs (multifocal in 48 pts)300 PTMCs (multifocal in 48 pts) Mean follow-up 60 monthsMean follow-up 60 months 7 patients lost to follow-up, 6 patients died of 7 patients lost to follow-up, 6 patients died of
other diseaseother disease Surgery if tumor growth towards adjacent Surgery if tumor growth towards adjacent
structures, increase in size, LN / distant structures, increase in size, LN / distant metastasis, patient’s preferencemetastasis, patient’s preference
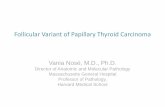
Sugitani et al. (2010) – Observation trialSugitani et al. (2010) – Observation trial

Tumor sizeTumor size no change / decrease: 93%no change / decrease: 93% increase : 7% (22 patients)increase : 7% (22 patients)
Lymph node metastasis - Lymph node metastasis - 1%1%
Operation rate Operation rate 16 patients (7%)16 patients (7%) indications: disease progression (12), patientindications: disease progression (12), patient’’s s
choice (4)choice (4) ? 6 patient with increased size not operated? 6 patient with increased size not operated
Recurrence / mortality: Recurrence / mortality: 00
Sugitani et al. (2010) – Observation trialSugitani et al. (2010) – Observation trial

SummarySummary
Natural history – 10 years (Ito)Natural history – 10 years (Ito) 8.3% increase by > 2mm8.3% increase by > 2mm 3.8% progress to > 12mm3.8% progress to > 12mm 3.8% develop new LN in lateral compartment3.8% develop new LN in lateral compartment
Operation rate: Operation rate: 7 – 16% (Ito, Sugitani)7 – 16% (Ito, Sugitani) Total thyroidectomy 13 – 50%Total thyroidectomy 13 – 50% ““limitted” thyroidectomy 50 – 87%limitted” thyroidectomy 50 – 87% Lymph node dissectionLymph node dissection
– Therapeutic lateral ND 1% - 18% Therapeutic lateral ND 1% - 18% – Prophylatic CND 6 – 100%Prophylatic CND 6 – 100%
High incidence of microscopic lymph node (38%) and High incidence of microscopic lymph node (38%) and multifocality (69%) in the operated cohortmultifocality (69%) in the operated cohort
Outcome of delayed surgeryOutcome of delayed surgery Local recurrence: 0.5 – 2.6%; Mortality: 0%Local recurrence: 0.5 – 2.6%; Mortality: 0%
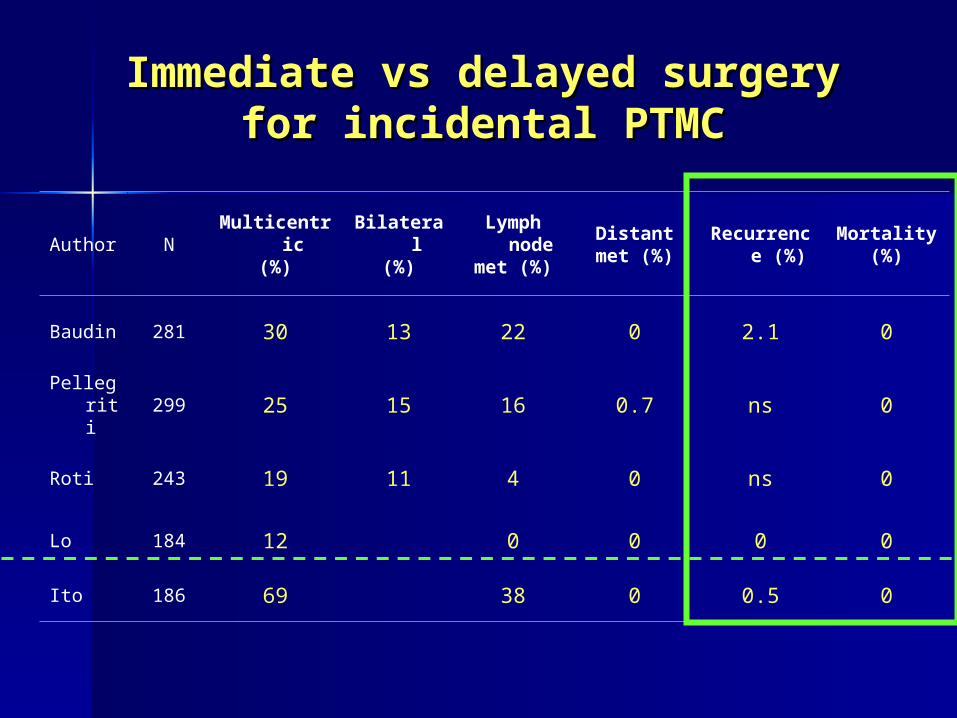
Immediate vs delayed surgery for Immediate vs delayed surgery for incidental PTMCincidental PTMC
Author NMulticentri
c(%)
Bilateral(%)
Lymph node
met (%)
Distantmet (%)
Recurrence (%)
Mortality(%)
Baudin 281 30 13 22 0 2.1 0
Pellegriti
299 25 15 16 0.7 ns 0
Roti 243 19 11 4 0 ns 0
Lo 184 12 0 0 0 0
Ito 186 69 38 0 0.5 0

LimitationLimitationStudy designStudy design Single-centered case seriesSingle-centered case series Small sample size of operated group for detection of rare Small sample size of operated group for detection of rare
eventsevents Patient’s choice to operate Patient’s choice to operate increased denominator with increased denominator with
non-progressive lesions non-progressive lesions mitigate recurrence rate mitigate recurrence rate Duration of follow-up relatively shortDuration of follow-up relatively short
Data qualityData quality Defaulted cases not explicitly describedDefaulted cases not explicitly described Some patient has tumor enlargement but not operatedSome patient has tumor enlargement but not operated
GeneralizabilityGeneralizability Dedicated USG surveillance programDedicated USG surveillance program Cultural issuesCultural issues

JSTS / JAES Guideline 2011JSTS / JAES Guideline 2011
““ observation without immediate observation without immediate surgey can be an option for surgey can be an option for patients with low-risk papillary patients with low-risk papillary microcarcinomamicrocarcinoma””

ConclusionConclusion
Role of initial observationRole of initial observation a “step” rather than “option” a “step” rather than “option” to futher risk-stratify low-risk PTMCs into to futher risk-stratify low-risk PTMCs into
progressive and non-progressive lesionsprogressive and non-progressive lesions may avoid surgery for indolent tumors in patients may avoid surgery for indolent tumors in patients
with limitted life expectancywith limitted life expectancy
Practical considerationsPractical considerations ? reliable USG surveillance programme? reliable USG surveillance programme patient anxiety / quality of lifepatient anxiety / quality of life

Thank you!Thank you!