Rimodellamento Ventricolare e Conversione del Rimodellamento: soni processi confrontabili nei due...
32
Rimodellamento Ventricolare e Conversione del Rimodellamento: soni processi confrontabili nei due sessi? Marisa Di Donato IRCCS San Donato Hospital University of Florence Tenth International Symposium HEART FAILURE & Co. CARDIOLOGY SCIENCE UPDATE FEMALE DOCTORS SPEAKING ON FEMALE DISEASES Milano 9 - 10 aprile 2010
-
Upload
antony-charles -
Category
Documents
-
view
214 -
download
0
Transcript of Rimodellamento Ventricolare e Conversione del Rimodellamento: soni processi confrontabili nei due...

Rimodellamento Ventricolare e Conversione del Rimodellamento: soni processi confrontabili nei due sessi?
Marisa Di DonatoIRCCS San Donato Hospital
University of Florence
Rimodellamento Ventricolare e Conversione del Rimodellamento: soni processi confrontabili nei due sessi?
Marisa Di DonatoIRCCS San Donato Hospital
University of Florence
Tenth International Symposium
HEART FAILURE & Co.CARDIOLOGY SCIENCE UPDATE FEMALE DOCTORS SPEAKING
ON FEMALE DISEASES
Milano9 - 10 aprile 2010
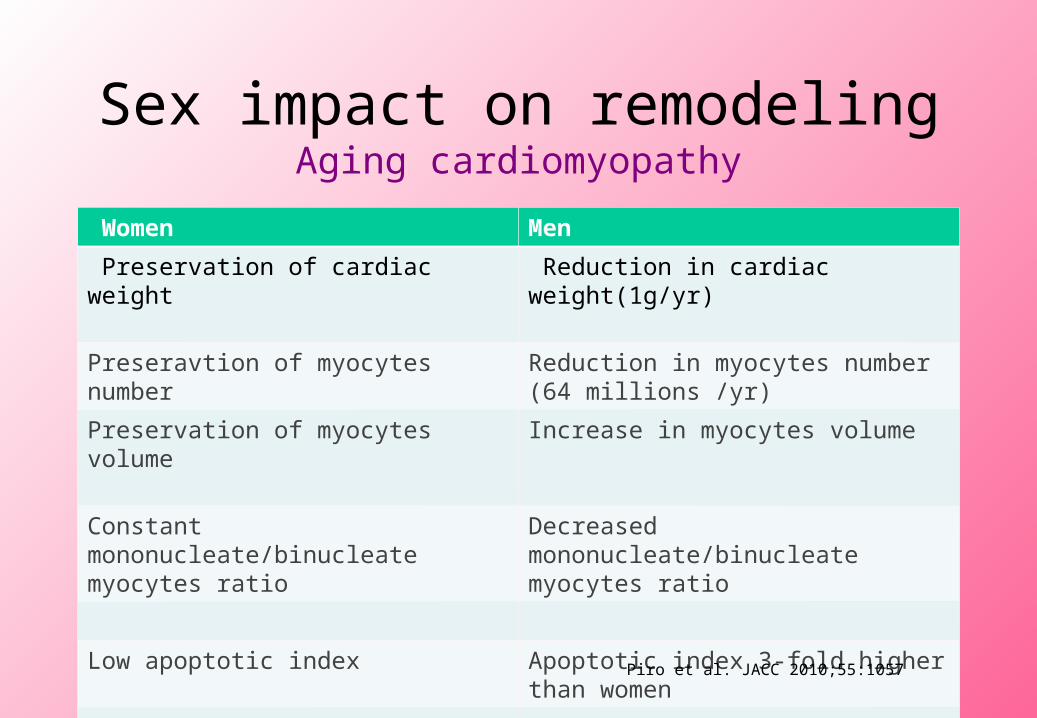
Sex impact on remodelingAging cardiomyopathy
Women Men
Preservation of cardiac weight Reduction in cardiac weight(1g/yr)
Preseravtion of myocytes number Reduction in myocytes number (64 millions /yr)
Preservation of myocytes volume Increase in myocytes volume
Constant mononucleate/binucleate myocytes ratio
Decreased mononucleate/binucleate myocytes ratio
Low apoptotic index Apoptotic index 3-fold higher than women
Decreased apoptotic rate Increased apoptotic ratePiro et al. JACC 2010;55:1057
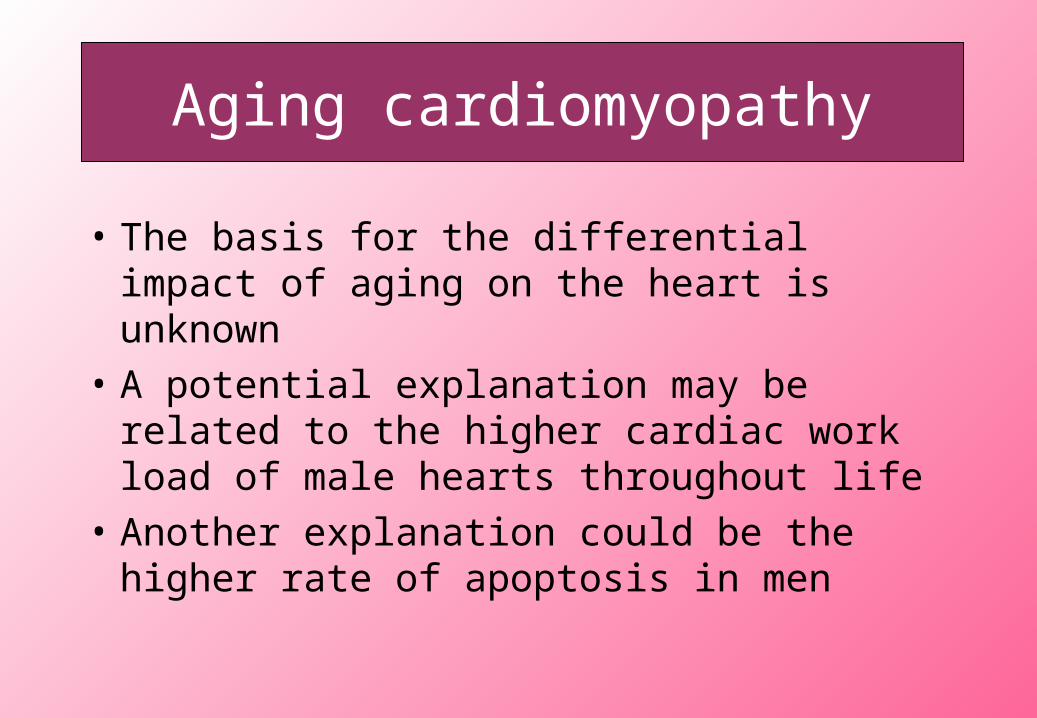
Aging cardiomyopathy
• The basis for the differential impact of aging on the heart is unknown
• A potential explanation may be related to the higher cardiac work load of male hearts throughout life
• Another explanation could be the higher rate of apoptosis in men
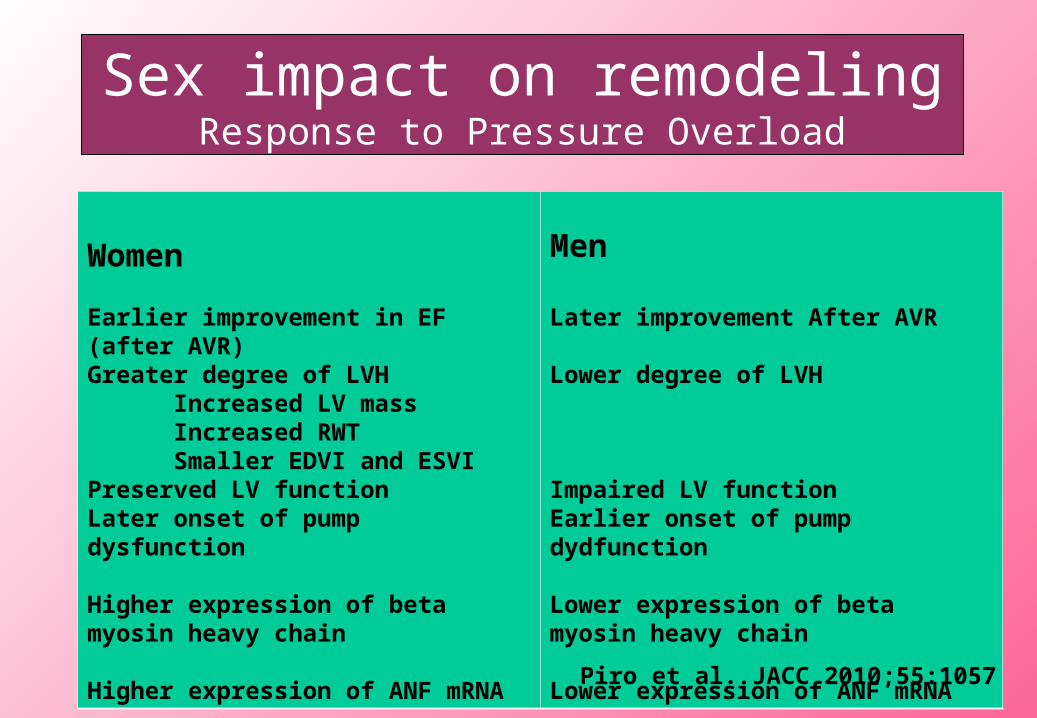
Sex impact on remodelingResponse to Pressure Overload
Women
Earlier improvement in EF (after AVR)Greater degree of LVH Increased LV mass Increased RWT Smaller EDVI and ESVIPreserved LV functionLater onset of pump dysfunction Higher expression of beta myosin heavy chain
Higher expression of ANF mRNA
Men
Later improvement After AVR
Lower degree of LVH
Impaired LV functionEarlier onset of pump dydfunction
Lower expression of beta myosin heavy chain
Lower expression of ANF mRNA
Piro et al. JACC 2010;55:1057

Sex impact on remodelingResponse to Volume Overload
Women Men
Smaller EDV and ESV Larger EDV and ESV
Greater LV mass/volume ratio Lower LV mass/volume ratio
Concentric hypertrophy No concentric hypertrophy
No impairment in cardiac function Impairment in cardiac function
Minimal ventricular dilatation
No changes in myocardial compliance
Significant ventricular dilatation
Decreased ventricular compliance
Piro et al. JACC 2010;55:1057

Sex impact on remodeling Response to acute myocardial ischemia
Women Men
Lower apoptotic rate in peri-infarct zone 10-fold higher apoptotic rate in peri-infarct zone
Longer duration of the cardiomyopathyLater onset of cardiac decompensation
Shorter duration of the cardiomyopathyEarlier onset of cardiac decompensation
Longer interval between HF and TransplantationLower infarct expansion index
Shorter interval between HF and Transplantation
Higher infarct expansion index
Three times lower mortality Worse cardiac function
Better cardiac function Maladaptive remodeling
Better remodeling Significantly greater dilatationMyocytes hypertrophyPremature exracellular matrix degradationHigher number of neutrophylisIncreased activity of metalloproteinase
Piro et al. JACC 2010;55:1057

Sex impact on remodelingHeart Failure
Women Men
Preserved LV EF Impaired LV EF
Smaller LV End diastolic volume
Smaller Stroke Volume
Higher LV end diastolic pressure
More frequent congestive symptoms
Greater LV End diastolic volume
Greater Stroke Volume
Lower LV end diastolic pressure
Less frequent congestive symptoms
Greater impairment in diastolic filling Lower impairment in diastolic filling

Sex impact on remodeling and the role of estrogens
• The mechanism by which estrogens exert their cardio-protective effects are not completely understood
• Ovarian synthesis of estrogens is subject to dramatic changes during the course of life but intramyocardial synthesis is less influenced by such variations (Grohe 1998)

Sex impact on remodeling and the role of estrogens
• Metabolic and vascular effects • Endotelium-dependent flow-mediated dilatation and aortic
compliance are greater in women
• Estrogens reduce cytopatic damage associated with myocardial injury (less apoptosis)
• Androgens adversely affect myocardial healing (Higher rate of rupture in men) and promote cardiac remodeling and dysfunction

Diastolic Heart Failure
• The reduced ventricular dilatation during remodeling in women compared with men helps explain why approximately half of women presenting with HF symptoms have preserved EF, vs one/third of men(Cleland JC, Eur Heart J 2003)
• When affected by HF women are more likely than men to present with congestive symptoms
• Both men and women with diastolic dysfunction and preserved EF show an increase in End diastolic pressure-volume ratio

THE PROCESS OF POST_INFARCTION REMODELING
Gender & Heart Failure● Myocardial Changes
Myocyte lossNecrosisApoptosis
● Alterations in extracellular matrix● Matrix degradation● Replacement fibrosis
● Alteration in LV chamber geometry● LV dilation (SIZE)● Increased LV sphericity (SHAPE)● LV wall thinning (SHAPE)● Mitral valve incompetence (SIZE AND SHAPE)
IRCCS Policlinico San Donato

Sex Differeces after MI
0
10
20
30
40
50
60
Diabetes NYHA 3-4 Inferior Site
Men
Women
0.02
0.001
0.05
496 pts (89 women) San Donato Hospital (unpublished)

0
5
10
15
20
25
30
Concentric Eccentric Dialtation
Pattern of LV Remodeling after Myocardial InfarctionIn Women
%
Concentric Eccentric Dilatation
496 pts (89 women)San Donato Hospital (unpublished)

70
72
74
76
78
80
82
84
86
88
90
Concentric Eccentric Dialtation
Pattern of LV Remodeling after Myocardial InfarctionIn Men
Concentric Eccentric Dilatation
496 pts (89 women) San Donato Hospital (unpublished)
%

95
100
105
110
115
120
F M
EDVI(ml/m2)
68
70
72
74
76
78
80
82
F M
ESVI(ml/m2)
Sex impact on LV Remodeling after Myocardial Infarction
0.0010.001
496 pts (89 women) San Donato Hospital (unpublished)

0.335
0.34
0.345
0.35
0.355
0.36
0.365
0.37
0.375
0.38
0.385
F M
Sex impact on LV Remodeling after Myocardial Infarction
P 0.04
Relative wall Thickness
496 pts (89 women) San Donato Hospital (unpublished)

Sex impact on LV Remodeling after Myocardial Infarction
150
155
160
165
170
175
180
185
F M
LV Mass Index(g.m2)
41.5
42
42.5
43
43.5
44
44.5
45
45.5
46
46.5
F M
Left Atrium Size (mm)
0.0060.003
496 pts (89 women) San Donato Hospital (unpublished)

0
0.1
0.2
0.3
0.4
0.5
0.6
SI Diast SI Diast SI Syst SI Syst
Women Men
0.007
0.001
Sex impact on LV Shape after Myocardial Infarction
(Median Values)
SPHERICITY
INDEX
Sphericity Index= Short to Long axis ratio
San Donato Hospital (unpublished)

0
0.10.2
0.3
0.40.5
0.6
0.7
0.80.9
1
1 2MI N MI N
Sex impact on LV Apical Shape (Conicity Index) after MIDiastole
00.10.20.30.40.50.60.70.80.9
11.11.2
1 2
Systole
MI N MI N
0.001
0.0010.001
0.001
0.0001
0.01
Conicity Index (CI)=Apical to Short axis ratio
San Donato Hospital (unpublished)
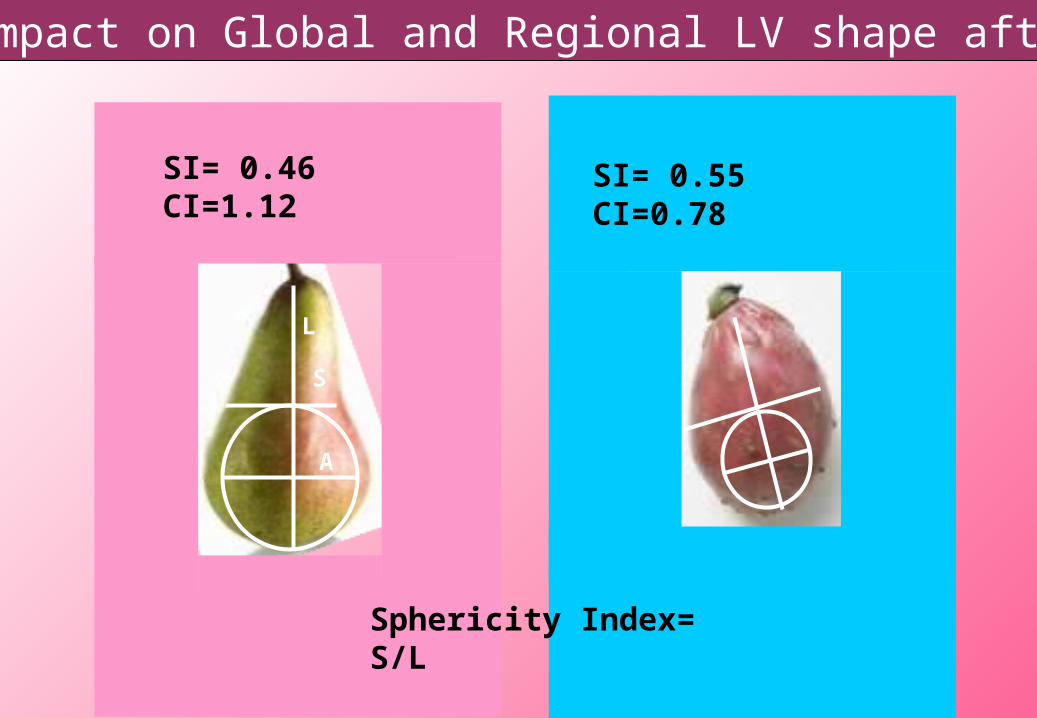
Sex impact on Global and Regional LV shape after MI
L
S
A
Sphericity Index= S/L
Conicity Index= A/S
SI= 0.46CI=1.12
SI= 0.55CI=0.78

Is it possible to revert LV remodeling?
Is there a difference in women compared to men in reverting the remodeling process ?
Non pharmachologic approaches to revert/retard LV remodeling
● Cardiomyoplasty● Volume reduction surgery (Batista operation)● Mitral valve repair +/-CABG●VAD implantation● CRT ● LV reconstruction (Dor procedure)● Mannequin guided surgical ventricular restoration
(SVR- Menicanti)● Prosthetic restraint devices
● Cells replacement

Surgical technique
• Arrested heart• Use of intraventricular mannequin to re-size and re-shape• Complete coronary revascularization• Mitral repair through ventricular approach, if needed• Cryosurgery at the border of the lesion if VA present
San Donato Hospital, Milano Italy
Menicanti 2002

San Donato Hospital SeriesPts submitted to SVR (2001-2009)
O 496 Patients with previous MI:• 89 Women (age 68+/-10 yrs)**• 407 Men (age 64+/-9 yrs)
O NYHA III-IV:• Men 166/384 (43%)• Women 50/83 (56%)**
O CABG associated in 93% of women and 94% of men
O Mitral repair in 25% of men and 27% of women
O Operative mortality:
Men 27/408 (7.6%)
Women 9/89 (10%) NS

….SURGERY for LV remodelingPre
Post
Post
Pre

-30
-25
-20
-15
-10
-5
0
5
10
EDV ESV EF+
Women
-30
-25
-20
-15
-10
-5
0
5
10
EDV ESV EF
Men
Reverse remodeling at 12 months FUP induced by SVR

-35
-30
-25
-20
-15
-10
-5
0
1 2 3
Diastole
Systole
Long Axis Short Axis Apical Axis
Reverse remodeling at 12 months FUP induced by SVR
-35
-30
-25
-20
-15
-10
-5
01 2 3
Diastole
Systole
Long Axis Short Axis Apical Axis
Women Men

0
0.1
0.2
0.3
0.4
0.5
0.6
1 2 Pre-op Post-op Pre-op Post-op
Changes in Sphericity Index following SVR
Diastole
Systole
0.010.01
0.01
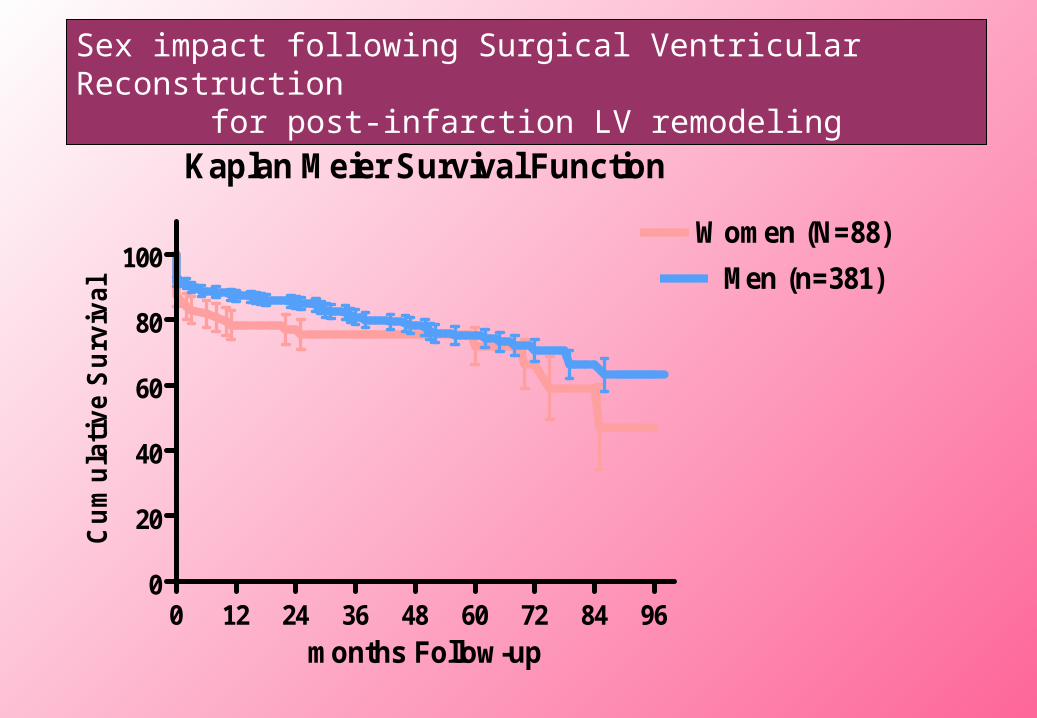
Kaplan Meier Survival Function
0 12 24 36 48 60 72 84 960
20
40
60
80
100Women (N=88)
Men (n=381)
months Follow-up
Cum
ulat
ive
Sur
viva
l
Sex impact following Surgical Ventricular Reconstruction for post-infarction LV remodeling

• LVR can revert the remodeling process both in men and women, by reducing Ventricular size and improving apical shape
• A more physiologic apex is the key to re-direct the blood flow towards the aorta and improving cardiac function
• Prognosis following LVR is not impacted by sex
Conclusions

Conclusions
• Regardless of age and menopause the remodeling process appears to be more favourable in women
• Women are more likely to present with “diastolic only” dysfunction and are at greater risk for low output syndrome acutely
• Lower awareness of heart disease in women is likely responsible for the worse outcome observed in some clinical series, and since this issue can be corrected,increased awareness of heart disease among women should still represent a number one priority
THANKS