Rib Osteomyelitis , Secondary to Actinomycosis in a Patient with Abdominal Pain
15
Rib Osteomyelitis, Secondary to Actinomycosis in a Patient with Abdominal Pain Shani Cunningham, DO Claire Bocchini, MD Texas Children’s Hospital/Baylor College of Medicine Houston, TX
-
Upload
eaton-fulton -
Category
Documents
-
view
21 -
download
2
description
Rib Osteomyelitis , Secondary to Actinomycosis in a Patient with Abdominal Pain. Shani Cunningham, DO Claire Bocchini , MD Texas Children’s Hospital/Baylor College of Medicine Houston, TX. Abstract. - PowerPoint PPT Presentation
Transcript of Rib Osteomyelitis , Secondary to Actinomycosis in a Patient with Abdominal Pain

Rib Osteomyelitis, Secondary to Actinomycosis in a Patient with
Abdominal Pain
Shani Cunningham, DOClaire Bocchini, MD
Texas Children’s Hospital/Baylor College of MedicineHouston, TX

Abstract Abdominal pain is a common childhood complaint with a broad
differential diagnosis. Osteomyelitis, an acute or chronic infection of the bone secondary to trauma or hematogenous spread of bacteria or fungus, is most common in children < 1 year and between 9 and 12 years old. Although rare, osteomyelitis of the rib may present with abdominal pain and occurs mostly in children and young adults. One study showed a mean duration of symptoms in bacterial rib osteomyelitis to be 16 weeks before a diagnosis was established. Actinomycosis, a non spore forming gram positive rod known for its ability to form sulfur granules, has a classic predilection for three areas of the body - the cervicofacial, abdominal, and pulmonary regions. Pulmonary actinomycosis can spread to involve nearby ribs or vertebrae consistent with thoracic actinomycosis disease. One fourth of thoracic actinomycosis cases are in pediatric patients. We present the case of an 11 year old male with osteomyelitis of the ribs secondary to actinomycosis infection.

Objectives
• Review differential diagnosis and work up of a chest wall mass
• Discuss etiologies of rib osteomyelitis• Review thoracic actinomycosis in children

History of Present Illness• Chief Complaint: “My stomach hurts”
• 11 year old male, with h/o Pierre Robin Sequence with tracheostomy and gastrostomy-button
• Presents initially to ER with 10 days of LUQ abdominal pain– KUB consistent with constipation, patient begins bowel regimen
• 2 days later: follows up with PCP with worsening abdominal pain and left-sided chest pain– Diagnosed with costochondritis and begins ibuprofen
• 1 day later: chest pain worsens, mom notices a “lump” over left side of chest
• Patient is taken to an outside hospital where a CXR shows a soft tissue mass of the left lateral chest
• Patient is started on clindamycin and cefotaxime and transferred to Texas Children’s Hospital for further management

Medical History• Social History
– Lives with mother, mom’s boyfriend, 2 siblings
– In 4th grade; takes regular classes and receives speech therapy
– Has 2 dogs, 1 cat– No recent travel or unusual foods– MGM visits frequently from Mexico– No additional TB risk factors
• Review of Systems– Gen: No fever, no weight loss, mild
fatigue, decreased appetite– HEENT: Tracheostomy capped– Chest: Denies cough or dyspnea– GI: G-button not in use, no N/V/D/C
• Past Medical History– Pierre-Robin Sequence
• Trach, g-button, continues to have speech impediment and swallowing difficulty (aspirates frequently)
– Hospitalized x 3 for pneumonia – Allergies: NKDA– Immunizations: UTD– Medications: Ibuprofen, Miralax
• Past Surgical History– Tracheostomy at 1 wk– G-button and fundoplication at 1 mo– Jaw reconstruction at 3 and 5 yrs
• Family History – Mother with Type 2 Diabetes– 6 siblings all healthy

Physical Exam• T: 97.7, HR: 94, BP: 98/67, RR: 24 • Wt: 19.9kg(<5th%), Ht: 124cm (<5th%)• Gen: Awake, alert, + moderate distress• HEENT: NC/AT, MMM, high arched palate,
crowded dentition, microglossia• Neck: Supple, no LAD, tracheostomy site is
clean, dry, and intact• Lungs: Mostly CTA-B, few rales LLL• Chest: Left lateral chest wall swelling
10cmx9cm, soft, non mobile, minimal erythema, warm and tender, non-fluctuant
• CV: RRR, CR brisk• Abdomen: Soft, ND, +tenderness in LUQ
near chest wall swelling upon palpation, G-button site with mild erythema and dried yellow discharge
• Skin: No rashes noted
Chest wall swelling

Differential diagnosis: Chest wall mass
• Infectious– Abscess, Osteomyelitis,
Cellulitis– Types:
• Bacterial– S. aureus, GAS, TB,
atypical mycobacteria, Bartonella, Salmonella, Actinomyces, Nocardia
• Fungal– Histoplasmosis,
coccidiomycosis, blastomycosis, cryptococcus
• Non-Infectious– Bone Tumor– Sarcoma– Lymphoma– Leukemia– Lipoma

Work-up of chest wall massLaboratory Evaluation• WBC 14.2 (56%N, 11%B, 24%L, 9%M)• H/H 10.9/33.6, Plts 685• ESR: 79, CRP: 7.5• Chemistries, LDH: WNL• Blood culture: Negative• PPD: Negative• Quantiferon test: Negative• Fungal complement fixation: Negative
Imaging Evaluation: MRI• Osteomyelitis of left lateral 8-11 ribs• Extensive inflammatory change and
suspected complex, debris-filled/ phelgmonous fluid collection
• Left lower lobe pneumonia
MRI of abdomen, post contrast

Diagnostic procedure: Biopsy
Histopathology demonstrating large sulfur granule with outer zone of granulation
with collagen fibers and fibroblasts, multinucleated giant cell
Gram stain demonstrating irregular, branching gram positive organisms,
consistent with Actinomycosis

Discussion: Rib Osteomyelitis
• Rib osteomyelitis is very rare• Review in 2000 found only 106
cases in literature: – 47 bacterial– 47 mycobacterial– 11 fungal, 1 entamoeba
• More common in children than adults
• Mean duration of sxs prior to diagnosis:– 16 wks bacterial etiology– 26 wks mycobacterial etiology– 32 wks fungal etiology
• Presenting symptoms:– Fever (73%)– Soft tissue mass (64%)– Chest pain (60%)
• Etiology with pulmonary/ pleural involvement: – 45% fungal – 25.5% bacterial – 23.4% mycobacterial
• Route of infection:– Contiguous spread (62%) – Hematogenous (38%)
Bishara, et al. Scand J Infect Dis 32: 223–227, 2000.

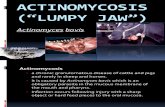
Discussion: Actinomycosis• Found in normal oral flora from infancy to adulthood• Most common infections: oral/ cervicofacial,
abdominal, pulmonary– Less common: liver, thoracic, female reproductive tract,
brain
• Irregular, non–spore-forming, non–acid-fast, nonmotile, gram-positive rods
– Grow in most rich culture media, various oxygen requirements
• Most commonly chronic infections with single or multiple indurated swellings
– Eventually soften, become fluctuant, suppurate– Walls are fibrous/ firm (“wooden”)
• Sinus tracts commonly form and extend through the overlying skin or to adjacent bones or tissues
– Overlying skin may have a bluish hue
Feigin and Cherry, http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=mmed&part=A1883.

Discussion: Thoracic actinomycosis
• 14-34% of actinomycoses infections in children • Risk factors: dental caries, trauma, debilitation, aspiration, and poorly
controlled DM• Hallmark of disease: spread that fails to respect tissue/ fascial planes• Classic radiographic triad: chronic lower lobe pulmonary consolidation,
empyema and wavy periostitis of the ribs• Review of 54 children with thoracic actinomycosis
– Male: 64%, mean age: 10 yrs– Boney involvement: 23 (42%) – Presentation: chest wall mass (49%), cough (40%), pain (36%), wt loss (35%),
fever (35%), draining sinus (15%)– Diagnosis: 58% positive culture, 38% histology with sulfur granule or ray
fungus– Outcome generally good, 1 pt (2%) died from bronchopulmonary fistula
Bartlett, et al. Pediatr Infect Dis J 2008;27: 165–169.

Discussion: Treatment of actinomycosis• Surgical debridement and prolonged antimicrobial therapy• Uniformly susceptible to penicillin
– Red Book: Most experts recommend parenteral penicillin for 4-6 weeks followed by oral therapy for 6-12 months
• Most extensive cases require drainage, resection of tissue and excision of sinus tracts in addition to antibiotics
Follow-up: Our patient• Due to his extensive disease – decision was made to treat without
surgical debridement• Pt received 6 wks high dose IV PCN and is now completing 6 months
of oral PCN • His swelling has completely resolved and he is currently pain free

Conclusion Osteomyelitis of the ribs is a rare condition that often goes undiagnosed
for several weeks. Patients typically present with fever, chest pain, and a soft tissue mass. Actinomycosis is a gram positive rod which may be found in normal oral flora that can spread throughout the body and cause disease. The most common sites for actinomycosis infections are cervicofacial, abdominal, and pulmonary. The hallmark of actinomycosis disease is spread that fails to respect tissue and fascial planes. Thoracic actinomycosis often presents with the classic radiographic triad of chronic lower lobe pulmonary consolidation, empyema and wavy periostitis of the ribs. Actinomycosis may be difficult to isolate, but is uniformly susceptible to penicillin and may be treated for up to 12 months.

References• Bishara J, Gartman-Israel D, Weinberger M, et al. Osteomyelitis of the ribs
in the antibiotic era. Scand J Infect Dis. 2000;32(3):223-7. • Fergie JE, Purcell K. Nocardiosis in South Texas children. Pediatr Infect Dis
J. 2001 Jul;20(7):711-4.• Bartlett AH, Rivera AL, Krishnamurthy R, Baker CJ. Thoracic actinomycosis
in children: case report and review of the literature. Pediatr Infect Dis J. 2008 Feb;27(2):165-9.
• Yeung VH, Wong QH, Chao NS, Leung MW, Kwok WK. Thoracic actinomycosis in an adolescent mimicking chest wall tumor or pulmonary tuberculosis. Pediatr Surg Int. 2008 Jun;24(6):751-4.
• Feigin and Cherry. Textbook of Pediatric Infectious Diseases. Philadelphia : Saunders; 2009.
• McMilan J. Oski’s Pediatrics Principles and Practice. Lippincott Williams and Wilkins; 2006.