
RESEARCH REPORT 170 - Health and Safety Executive · such as personality and ... reporting’ of...
143
HSE Health & Safety Executive Cognitive Factors’ Influence on the Expression and Reporting of Work-Related Stress Prepared by Loughborough University, the University of Nottingham and the Institute for Employment Studies for the Health and Safety Executive 2003 RESEARCH REPORT 170
Transcript of RESEARCH REPORT 170 - Health and Safety Executive · such as personality and ... reporting’ of...
HSE Health & Safety
Executive
Cognitive Factors’ Influence on the Expression and Reporting of Work-Related Stress
Prepared by Loughborough University, the University of Nottingham and the Institute for Employment Studies for the Health and Safety Executive 2003
RESEARCH REPORT 170
HSE Health & Safety
Executive
Cognitive Factors’ Influence on the Expression and Reporting of Work-Related Stress
Kevin Daniels BSc (Hons) PhD CPsychol ILTM Loughborough University
David Jones, BSc (Hons) MSc and Eamonn Fergusson, BSc (Hons) PhD CPsychol AFBPsS FRSH
University of Nottingham
Sarah Perryman, BA (Hons) MSc MA and Jo Rick, BA (Hons) PhD CPsychol AFBPS
Institute for Employment Studies
There are questions concerning the extent to which individual differences, that is variation in factors such as personality and attitudes, are responsible for the incidence of stress-related illness and reporting of stress-related problems through questionnaires and other monitoring procedures
In the first part of this research, we conducted a meta-analysis on longitudinal studies of ill-health, work conditions and individual differences. Results indicate that both individual differences and work conditions are associated with increases in ill-health. By concentrating on the best possible longitudinal research, this meta-analysis provides some of the strongest evidence to date that both adverse work conditions and individual differences can cause stress-related illness.
In the next part of the research, we examined existing representative data-bases of the United Kingdom population. We found individual differences that influence stress-related illness to be different between genders, age groups, socio-economic groups and occupational groups, indicating differences in risk of experiencing and reporting stress-related illness amongst these groups.
In the last part of this review, we examined some of the ways in which individual differences might influence the experience and reporting of stress-related illness. Cognitive factors involved in the experience of unpleasant emotions might play a central role in both the development and reporting of stress-related illness.
This report and the work it describes were funded by the Health and Safety Executive (HSE). Its contents, including any opinions and/or conclusions expressed, are those of the authors alone and do not necessarily reflect HSE policy.
HSE BOOKS

© Crown copyright 2004
First published 2004
ISBN 0 7176 2770 5
All rights reserved. No part of this publication may bereproduced, stored in a retrieval system, or transmitted inany form or by any means (electronic, mechanical,photocopying, recording or otherwise) without the priorwritten permission of the copyright owner.
Applications for reproduction should be made in writing to: Licensing Division, Her Majesty's Stationery Office, St Clements House, 2-16 Colegate, Norwich NR3 1BQ or by e-mail to [email protected]
ii

Acknowledgements
First, we would like thank Dr Rob Briner, Prof Tom Cox CBE and Prof Philip Dewe – who formed a panel of external advisors - for their advice and encouragement during the early stages of this research. We are indebted to their knowledge of research and practice into occupational stress.
We would also like to thank others that responded to requests for material and advice on the specific questions of our review, namely: Prof Cary Cooper CBE, Dr Jan de Jonge, Prof Stanislav Kasl, Prof Roy Payne, Dr Katherine Parkes, Prof Dr Wilmar Schaufeli, Prof Paul Spector, Dr Jukka Vuori, Prof Peter Warr and Prof Jerry Wofford. Not only did these provide material invaluable as background reading for this report, but also they responded with enthusiasm for this undertaking.
Finally, from the HSE, we would like to thank our project manager Prof Colin Mackay, Dr Simon Clarke and Steve Lee for their support and help with this research.
The work reported here was undertaken while Kevin Daniels was with the University of Nottingham.
iii

iv

Contents
1 Executive Summary 1
2 Introduction 3
2.1. Aims of the project 4
2.2. Limitations of considering only hazards as an 6 explanation for occupational ill-health
2.3. Cognitive factors 7
2.3.1. What cognitive factors influence 9
2.3.1.1. Expert panel 9
2.4. Individual differences 10
2.4.1. What is an individual difference? Traits, 10 attitudes and states
2.4.2. How individual differences are linked to stress 12
2.4.3. One major orientation to stress 13
2.5. Psychosocial hazards and health 14
2.5.1. Psychosocial hazards 14
2.5.2. Health and related variables 16
2.6. Structure of report 17
3 Quantitative review: meta-analysis 18
3.1. Searching the literature. 21 3.1.1. Inclusion criteria 24
3.1.1.1. The search terms 25 3.1.2. The scale of the literature and sifting the 26
literature 3.2. Meta-analysis 30
3.2.1. A brief introduction to meta-analysis and 30 correlation coefficients
3.2.2. Coding the papers 36 3.2.3. Findings 39
3.2.3.1. Individual differences and ill-health 40 3.2.3.2. Hazards and ill-health 42
v

3.2.3.3. Stability in health measures 44
3.2.3.4. Partial correlations 45 3.3. Summary and implications of the meta-analysis 46
4 Secondary analysis of existing data-bases 51
4.1. Data-bases 51
4.1.1. Health Survey for England 2000 (HSfE) 51
4.1.2. Health and Lifestyle Survey 1991/2 (HALS2) 52
4.1.3. Procedure 52
4.2. Analysis 54
4.2.1. Analyses for HSfE2000 54
4.2.2. Analyses for HALS2 58
4.3. Summary and conclusions 64
4.3.1. Conclusion 66
5 Discussion 67
5.1. Paths from individual differences to occupational ill- 68 health
5.1.1. Affective Events Theory 69 5.1.2. Lazarus, appraisal and coping 70 5.1.3. Action-control theory and goals 71 5.1.4. CAPHEM model 74
5.2. Individual differences & self-report measures: 79 correlation inflation
5.2.1. Occasion factors 79 5.2.2. How mood and disposition interact to 80
determine how we notice psychosocial hazards 5.3. Change & stability in psychological distress 80
5.3.1. Change & stability explained in the CAPHEM 81 model
5.3.2. Small effects sizes and large changes: vicious 82 and virtuous circles
5.4. Individual differences and the experience of physical 83 symptoms
5.4.1. The role of negative orientation in the 83
vi

perception of symptoms 5.4.2. The role of negative orientation in the 84
presentation and diagnosis of symptoms 5.4.3. Negative orientation and health – is there a 86
really a link?
5.5. Individual differences and socio-cultural factors 87 6 Conclusion 90
6.1. Implications for monitoring 91 6.1.1. Are measures too insensitive? 92 6.1.2. How to assess negative orientation 93
6.2. Implications for practice 93 6.2.1. Cognitive and perceptual factors and the 93
individual6.2.2. Cognitive and perceptual factors and society 95
6.3. Implications for research 96 6.3.1. Need for detailed, time intensive studies 96 6.3.2. Researching cognitive factors in the workplace 97
6.4. Concluding remarks 99
References 100
Appendices: 107
A) Form used to sort studies 107
B) Bibliography for CAPHEM model 114
vii

viii
1. Executive Summary
There is debate over the extent to which psychosocial hazards really influence occupational ill-health, or whether findings from research really reflect individual differences, related to factors such as personality and attitudes. That is, the debate centres on whether work conditions, individual differences, or a combination of both influence stress-related illness. This debate has many implications: I) for our understanding of workrelated stress; II) for the extent to which changes in organisational practice can reasonably be expected to reduce stress-related illnesses; and III) for the means of assessing stress-related illness to gauge the success or otherwise of interventions.
In this research, we seek to examine some aspects of this debate and outline some of the implications for policy and organisational practice.
In the first part of this research, we conducted a metaanalysis on longitudinal studies of ill-health, work conditions and individual differences. Results indicate that: · In general, both individual differences and adverse
work conditions are associated with increases in illhealth.
· Adverse work conditions are associated more closely with subsequent increases in psychological symptoms than subsequent increases in physical symptoms or changes in health behaviours;
· Individual differences are associated with subsequent increases in the experience of psychological symptoms and perception of physical symptoms;
· There is a good deal of stability in psychological health.
By concentrating on the best possible longitudinal research, this meta-analysis provides the some of the strongest evidence to date that both adverse work conditions and individual differences can cause stressrelated illness.
In the next part of the research, we examined existing representative data-bases of the United Kingdom population. We found individual differences that influence stress-related illness to be different between genders, age groups, socio-economic groups and occupational groups, indicating differences in risk of
1

experiencing and reporting stress-related illness amongst these groups.
In the last part of this review, we examined some of the ways in which individual differences might influence the experience and reporting of stress-related illness. Taking into account the results of the meta-analysis, we conclude that that cognitive factors involved in the experience of unpleasant emotions might play a central role in both the development and reporting of stressrelated illness.
A number of implications arise from the findings of thisreport:· Monitoring systems assessing psychological health
are more likely to be more sensitive to changes in the work environment than those assessing physical health. However, some monitoring systems might overestimate the extent of stress-related illnesses attributable to work, especially in some demographic groups in the population.
· A greater emphasis needs to be placed on how individuals interpret the work environment in practice, for example in conducting psychosocial risk assessments, focusing interventions on how individuals pursue and attain goals, and in communication about the risks from psychosocial hazards.
· Research should place greater emphasis on the cognitive processes underpinning interpretation of the work environment and physician diagnosis of stress-related illnesses.
2
2. Introduction This research was undertaken on behalf of the HSE to provide a review of scientific evidence in relation to the cognitive processes – that is perceptual, mental and related psychological processes - involved in the expression and reporting of stress-related symptoms and ill-health.
In broad terms, we took this to mean identifying the cognitive processes not only involved in the stressresponse, but also identifying the cognitive processes that influence the expression and reporting of stressrelated psychological and physical symptoms. Indeed, it is possible to differentiate between the ‘experience’, ‘expression’ and ‘reporting’ of work-related stress and stress-related symptoms and illness. Therefore, in the context of this report:
‘experience’ refers to the cognitive experience of symptoms;
‘expression’ refers to overt displays of those symptoms, particularly to medical practitioners;
‘reporting’ refers to completion of self-report assessments in epidemiological surveys, evaluations of workplace interventions etc.
These descriptions illustrate that there are important distinctions to be made to fulfil the objectives of the research. For example, factors – like a tendency to worry – might lead some people to amplify their experience of symptoms, which might then lead to overreporting of stress-related symptoms in epidemiological surveys – thus giving a false picture of the size of any stress-related problem and, what, if anything needs to be done. Conversely, factors that might mask expression of stress-related symptoms, such an optimism, may lead to physicians to attribute symptoms to a source other than work-related stress. This then might lead to underreporting of stress-related illnesses in the population as assessed by surveillance schemes that rely on reports from physicians – again giving a false picture. Therefore, it is vital that the research distinguishes between the cognitive attributes related to different aspects of the experience, reporting and expression of symptoms.
3

In the rest of this chapter, we outline the aims of this research; define and describe cognitive processes in greater detail; explain why studies of individual differences help us identify the influence of cognitive processes; and explain our approach to the rest of the research.
2.1. Aims of the project
HSE set four objectives for this research.
1) Identify the principle factors that modify the reporting of the response to stress.
We took this to mean that the research needed to make explicit the following:
a) how the expression of work-related health outcomes is influenced by a range of psychological attributes;
b) how these psychological attributes influence various cognitive processes;
c) how these psychological attributes may influence monitoring of stress-related illnesses in the population and in relation to interventions.
Point a) is considered in the next chapter, that describes a meta-analysis of longitudinal studies. Points b) and c) are discussed in more detail in the fourth and fifth chapters. We also undertook to examine how these psychological attributes vary in the UK population (e.g. examine whether differences exist in different occupational groups). We did this by analysing existing data-bases representative of the UK population. In doing so, we were able to establish whether cognitive factors might accentuate or attenuate the experience and reporting of stress-related symptoms in different demographic groups.
2) Assess the impact of each of the psychological variables on the reporting of stress responses.
We took this to mean that the report should make clear statements about the causal processes by which principal psychological variables, for example low selfesteem, influence expression and reporting. This emphasis on causality meant that we made very strict choices about the studies that we included in the metaanalysis. We also took this to mean that we needed to establish numerical estimates of the strength of the
4

relationships between psychological attributes and the expression and reporting of stress-related symptoms and illness. By establishing such estimates – known as effect sizes - it will be possible to obtain better estimates of the influence of changes in work environments on stress-related symptoms and illness. Because the technique of meta-analysis provides a means of establishing such effect sizes, then we chose to give greatest weight in our research to meta-analysis of existing, rigorous evidence.
3) Describe how cognitive factors are implicated in the generation of the stress process.
We took this to mean that the research should attempt to explain why relationships might exist between psychological attributes and various elements of the experience, reporting and expression of stress-related symptoms, as well as establishing numerical estimates of those relationships. Therefore, the penultimate chapter of this report, informed by the results of the meta-analysis, reviews some relevant theoretical explanations of cognitive factors in the occupational stress process.
4) Give some indication of the temporal stability of the factors identified would also be useful.
We took this to mean three things:
a) whether each of the attributes that we identify are subject to change;
b) whether those attributes subject to change are subject to longer term and relatively permanent change, and/or whether they are subject to short-term fluctuations around a relatively stable average level for each person;
c) the processes by which more enduring changes may come about.
Points a) and b) are investigated in this report, by drawing on the results of our own meta-analysis and the results of other research. Point c) is considered in chapter 5, where we discuss the processes underlying change and stability in the work-related stress process and, also, the role of wider socio-cultural variables in influencing the cognitive processes underlying workrelated stress.
5

In addition to these specific objectives, the HSE also requested that we include description of any uncertainties in the evidence base and draw attention to areas where the evidence is strong or weak. In this respect, in the last chapter, we provide an indication of how research in this area might usefully proceed.
2.2. Limitations of considering only hazards as an explanation for occupational ill-health
Researchers have identified many work conditions related to health at work (Warr, 1999), yet variation in work conditions typically accounts for only small proportion of variation between people in levels of well-being (Rick, Thomson, Briner, O'Regan and Daniels, 2002). One reason for this is because individuals exhibit different reactions to seemingly similar environments (Campbell, Chew and Scratchley, 1991)
Therefore, the experience of stress-related symptoms is not always an inevitable consequence of exposure to adverse work conditions in the workplace.1 Neither does it follow that the expression of those symptoms or reporting of those symptoms follow from the experience of those symptoms, as it is also possible that there exists variation between individuals in these relationships. For example, some people might suppress how they feel when interacting with others, and others might more easily remember episodes of poor well-being or illness when reporting on absence from work over the previous year in surveys.
The issue, then, becomes what additional factors do we need to take into account to explain individual variation in these relationships. Our view is that cognitive factors – which we describe in detail in the next section – are the best candidates for explaining individual variation. We base this assertion on four main arguments.
a) Stress and related concepts such as emotions are fundamentally experiential phenomena (Lazarus, 1999) and any explanation of stress-related phenomena needs to take into account the mental or cognitive processes that shape these phenomena;
There exists variation in the terminology used to describe adverse work conditions in relation to occupational stress. Some authors prefer the term ‘stressors’ and others ‘psychosocial hazards’. HSE itself uses the term ‘psychosocial hazards’.
6
1
b) Lazarus’ appraisal theory is one of the most influential accounts of stress and emotions (Cooper, Dewe and O’Driscoll, 2001). This theory is fundamentally cognitive, and many other contemporary theories of stress and emotions build explicitly on Lazarus’ approach (see e.g. Power and Dalgleish, 1997).
c) Within the science of psychology as a whole, cognitive approaches have been dominant for a number of decades. This is an impressive feat for a young science whose institutions were established within the past 150 years. The dominance of cognitive approaches reflects their success in explaining aspects of many areas of psychological experience and informing much applied psychological practice;
d) There is a developing body of theory and evidence that indicates key aspects of the work-related stress process can be explained and new interventions formulated by drawing upon experimentally verified principles of human mental activity (Daniels, 2001; Daniels, Harris and Briner, 2002a; 2002b; 2002c; in press).
2.3. Cognitive factors
Cognition is a term that, broadly, refers to the mental processes of perception, attention, memory, learning, problem solving and decision making (Eysenck and Keane, 1990). In cognitive approaches to stress and emotions (Daniels et al, 2002b, in press; Power and Dalgleish, 1997), cognitive or mental models play a key role. To the extent that different people have different views on the world, and therefore different mental models, how mental models influence stress, emotions and health is important for understanding individual variation in response to psychosocial hazards at work. We describe and define mental models next.
At any given time, we can only pay attention to a limited amount of information. For example, when taking a decision at work, we are constrained in being able to attend only to some, not all, relevant information.
Moreover, in work situations, we often have to make sense of ambiguous, conflicting and complex information. To do this, we rely on experience and learning to help us select the most relevant information
7
to attend to and to interpret this information. Therefore, we not only use information from the environment, but also our memory when taking decisions.
To use our memory, we derive our own ‘lay’ theories of how the world works. These represent our knowledge, which is accumulated through learning and experience. These theories are simplified, generalised and abstract representations and go under many names - 'mental models' being one (after Johnson-Laird, 1989).
People develop their ‘mental models’ through a set of organising principles that group associated concepts together: Mental models can contain knowledge that provides categories or labels (e.g. ‘Unpaid overtime is an unreasonable imposition’), or about processes (e.g. ‘Talking to Susan usually makes me feel better’). When we are confronted with a situation, we simply recall the mental models that seem most appropriate to that situation at that time. Once recalled, the mental model then helps to identify which information is most important for the task at hand, how to interpret that information and so, eventually influencing our behaviour.
For instance, mental models have been shown to influence subsequent predictions about future events, decision making and communication (Daniels and Henry, 1998). Crucially for stress-related phenomena, mental models are also thought to influence our emotions by influencing how we interpret or appraise work conditions and influencing how we cope with aversive conditions and events (see e.g. Power and Dalgleish, 1997).
A mental model does not have to be in the conscious mind to influence subsequent cognition and behaviour. In some instances, recall may be entirely unconscious and we apply a mental model to a situation without being aware of it (Dutton, 1993).
Further, people synthesise mental models, rather than simply recalling them from memory – they recall several generalised and abstracted mental models and combine them in new ways to be relevant to the given context (Barsalou, 1982).
For example, in responding to heavy work demands, we may recall knowledge about how work demands influence what we want to achieve at work, synthesising this with knowledge about how work demands
8

influence our feelings and how we have coped with heavy work demands in the past. This helps us form a mental model of the likely consequences of heavy work demands and what forms of coping might be appropriate (cf. Daniels et al, in press).
2.3.1. What cognitive factors influence
As noted, it is possible to differentiate between, for example, the experience, expression and reporting of work-related stress and stress-related symptoms. It is also possible to differentiate, for example, between processes that act independently of psychosocial hazards and those that mediate or moderate the influence of psychosocial hazards (e.g. Moyle, 1995).2
After examining major organising frameworks in the literature (e.g. Schuler, 1985) it is also possible to derive a set of relationships with a range of variables related to health that are thought to be conjointly influenced by cognitive processes and psychosocial hazards.
2.3.1.1. Expert panel
At an early stage in this project, we assembled this research team with a panel of experts to discuss possible relationships.3 Taking into account direct influences, moderated and mediated relationships, and being as inclusive as possible, it was felt that cognitive factors related to work-related stress could influence:
i) Acute psychological states, such as mood;
2 In statistical terms, a mediated relationship is one where a change in one variable causes a change in another variable, which subsequently causes a change in a third variable. For example, an increase in work demands might lead to feelings of being overwhelmed and without control at work, which in turn leads to depression. A moderated relationship is one where the relationship between two variables is dependent upon another variable. For example, the relationship between discretion over how to complete work tasks and job satisfaction might be dependent upon self-esteem. Those people with low self-esteem might have less confidence in their own ability to make decisions about their job and thus will be more satisfied with work than those with high self-esteem when any discretion over how work should be performed rests with their supervisor.
3 The expert panel consisted of this report's authors, excepting Sarah Perryman and our expert advisors, namely Dr Rob Briner (University of London), Dr Simon Clarke (HSE), Prof Tom Cox CBE (University of Nottingham), Prof Philip Dewe (University of London), and Prof Colin MacKay (HSE).
9

ii) Chronic psychological states, such as depression;
iii) Acute physical symptoms such as headaches;
iv) Chronic physical conditions such as hypertension;
v) The reporting of psychological and physical states, so that self-reports of psychological and physical symptoms amplify or attenuate measurement of these symptoms by self-report;
vi) Health-related behaviours, such as smoking, drinking and sickness absence from work;
vii) Physicians’ diagnoses of symptoms as more or less stress-related.
2.4. Individual differences
Since individual differences in responses to psychosocial hazards at work gave rise to this project, it is hardly surprising that there is both a great deal of research on individual differences in the stress process (e.g. Payne and Cooper, 1991) and that individual differences can inform us of the nature of the cognitive processes related to work-related stress.
2.4.1. What is an individual difference? Traits, attitudes and states
An individual difference, in the context of this research, was defined simply as psychological variables upon which individuals may differ. Of course, we limited our consideration of individual differences to those thought to have an effect on work stress, health or related behaviour.
It is possible to differentiate three major classes of variables that reflect individual differences. These are:
a) Traits, such as the Big 5 personality factors of neuroticism, extraversion, openness to experience, agreeableness and conscientiousness (e.g. McCrae and Costa, 1997). These are thought to be relatively impervious to change after the onset of early adulthood. They are considered to have a major genetic component;
10

b) Attitudes, beliefs and related concepts, such as locus of control, Type A Behaviour Pattern, self-esteem and job satisfaction (see e.g. Payne and Cooper, 1991 for summaries of such variables in relation to work-related stress). These variables are characterised as being more fluid than traits, and, therefore, more capable of changing after early adult-hood – even if they do contain a moderate to large trait component (e.g. Dormann and Zapf, 2001).
c) State variables, such as mood and emotions.4 These variables might be influenced by traits and attitudes, but are very fluid and can change very rapidly (Parkinson, Briner, Reynolds and Totterdell, 1995).
The importance of making this differentiation with respect to individual differences is that the more trait and attitudinal individual differences can be considered indices of stable cognitive ‘structures’. These provide a backdrop to the cognitive processes underlying the experience of stress, whilst state individual differences can be considered closer to the cognitive processes as these processes unfold (cf. Lazarus, 1999).
It is obvious from our classification that some attitudes and states (e.g. job satisfaction, anger) are often studied as outcomes of the stress process rather than causes of stress. However, many theoretical models of stress indicate that many supposed outcomes can influence some causes (Edwards, 1992) and evidence indicates such outcomes influence other attitudes, the interpretation of the stressfulness of psychosocial hazards and, possibly, even the occurrence of some psychosocial hazards (Daniels and Guppy, 1997).
Demographic variables represent one form of individual difference, although we did not examine demographic variables in the review for two reasons:
a) Demographics are, at best, distal indicators of individual differences in cognitive and perceptual processes – and even then, they are more likely to represent socio-cultural factors (Lazarus, 1999), which are beyond the scope of this research. Nevertheless, the secondary analyses described later in this report give
In the psychological sciences, the term 'emotion' refers to feelings towards an event, object or person, whilst the term 'mood' refers to feelings that cannot necessarily be linked to a specific event, object or person. The term 'affect' is a more general term that subsumes both 'mood' and 'emotion' (see Parkinson, 1995).
11
4

some indication of the extent of variation in the individual differences studied here amongst demographic groups in the UK population.
b) The scale of the relevant literature. Literature searches for relevant articles with demographic variables identified over 3373 articles published in the past five years alone. Within the time limits set for this research, it was not then possible to incorporate demographic factors into the meta-analysis.
2.4.2. How individual differences are linked to stress
The cognitive processes linking individual differences to stress are based on mental models. For traits and attitudes, certain psychological characteristics, such as neuroticism, a tendency to worry and low self-esteem, are associated with a larger number of mental models about the negative consequences of work environments. These mental models are also more elaborate (Wofford and Daly, 1997).
People with negative psychological traits and attitudes are more likely to recall negative information about work environments – meaning they are more likely to notice negative aspects of the work environment and more likely to engage in further deliberation and processing of that information in a way that reflects an elaborate negative interpretation.
Consequently, it could be expected that people with certain psychological characteristics could feel worse about work, may react more strongly to psychosocial hazards – psychologically and physiologically - and might amplify their experience of physical symptoms.
Current mood or emotion is thought to interact with these psychological characteristics (Williams, Watts, MacCleod & Mathews, 1997), so that negative moods or emotional states cue the influence of mental models that reflect negative interpretations of the environment. Put another way, people in a negative mood or emotional state are more likely to recall negative information or notice negative aspects of the environment. Again, then, it could be expected that people with in a negative mood or emotional state might react more strongly to psychosocial hazards and amplify their experience of symptoms.
12

2.4.3. One major orientation to stress
To impose order on a vast literature, we decided to address individual differences on a broad continuum of positive to negative orientation, differentiating traits, attitudes and states within this broader dimension.
The reasons for doing this are threefold.
First, there is evidence that different parts of the brain are biased toward processing negative or positive emotional information (Watson, Wiese, Vaidya, and Tellegen, 1999).
Second, whilst work-related emotional or affective well-being has several distinct aspects (e.g. anxiety, depression), the major differentiation between aspects of affective well-being at work is their pleasantness or unpleasantness (Daniels 2000; Warr, 1990).
Third, a number of studies indicate that a constellation of attitudes and traits co-occur that indicate proneness to stress, negative emotional states and disease (Friedman and Booth-Kewley, 1987; Wofford and Daly, 1997).
As a result, we are able to classify the individual differences examined in this report according to their temporal stability (trait, attitude, state) and whether they represent a more negative or positive orientation toward the work or general social environment. Table 2.1. illustrates this framework.
Table 2.1. Types of individual difference in relation to occupational stress
Trait Attudinal State
+ve orientation e.g. agreeableness e.g. high self- e.g. enthusiasm esteem
-ve orientation e.g. neuroticism e.g. Type A e.g. anger (coronary prone) Behaviour Pattern NB. +ve to –ve orientation reflects a continuum. For example, high scores on a measure of neuroticism represent a negative orientation, low scores a positive orientation and scores in the mid-range represent an orientation between the two extremes.
13

2.5. Psychosocial hazards and health
Since the purpose of this report is to examine individual differences with respect with work-related stress and stress-related symptoms, it is necessary to give some consideration to characteristics of the work environment that can cause stress – so-called stressors or psychosocial hazards, and the nature of our outcome measures – namely health and related variables.
2.5.1. Psychosocial hazards
The HSE have commissioned research on psychosocial hazards to help them define minimum management standards in nine main areas (see e.g. Rick et al, 2002). These areas correspond to some of the major categories of psychologically aversive work conditions thought to cause ill-health. They have been operationalised by the research team conducting this research as:
1) Work demands - including:
1a) workload - quantity, pacing, time pressure, emotional content of work;
1b) work scheduling – total hours, breaks, travel time, shift work;
1c) work organisation and job design – task design, team working;
1d) physical environment – real and perceived danger, noise, toxins;
2) Lack of worker control or autonomy – including:
2a) Lack of skill discretion – variety, opportunity for skill use;
2b) Lack of decision authority – control and autonomy;
2c) Lack of participation in decision making.
3) Lack of support and interpersonal relationships in the working environment – including:
3a) Lack of proactive support – practical & emotional support, support from work and outside of work, feedback;
14

3b) Lack of reactive support - practical & emotional support, support from work and outside of work, feedback;
3c) Lack of team/interpersonal conflict, bullying and harassment;
We expected that most of the studies we reviewed would include psychosocial hazards that could be classified according to these three major categories: work demands; lack of work control and lack of work support. However, we also anticipated some studies would include measures of other stressful work conditions – such as job insecurity.
One issue in the literature concerns whether psychosocial hazards are assessed objectively or assessed by self-reports. One line of reasoning is that self-reports are more likely to biased by individual cognitive factors, and so do not give an accurate picture of the influence of the work environment on health. Another line of reasoning asserts that the person best able to give an accurate assessment of a person’s work environment is that person him or herself, and so selfreports might give a more accurate picture than other methods. A related concern is that psychosocial hazards such as control and support do not exist in any real, material sense, and therefore can only be assessed by subjective methods.
In the meta-analysis, then, we differentiated between studies that used subjective self-report methods and studies that used other, more objective methods to assess psychosocial hazards. The more objective methods could include the following:
a) aggregate self-reports across all workers for a given job;
b) managerial reports;
c) observations by members of the research team;
d) inferred job characteristics from analysis of job titles or job descriptions;
e) inferred job characteristics from organisational change interventions (e.g. introduction of semiautonomous work teams);
f) some combination of the above.
15

2.5.2. Health and related variables
To recap, in the context of this research, we take:
‘experience’ to refer to the cognitive experience of symptoms;
‘expression’ to refer to overt displays of those symptoms, particularly to medical practitioners;
‘reporting’ to refer to completion of self-report assessments in epidemiological surveys, evaluations of workplace interventions etc.
It is then necessary to include in our review indicators of each of these manifestations of stress-related symptoms. The approaches taken to measurement can include self-reports, physician reports or more ‘objective’ measures taken by the research team, including physiological indices and assessment by independent medical practitioners. We might expect that:
a) Self-reports tap both ‘experience’ and ‘reporting’ of symptoms;
b) Physician reports tap ‘experience’, ‘reporting’ and ‘expression’;
c) Objective measures or independent diagnosis by a research team tap ‘experience’.
In this respect, by comparing across studies that use different methods, it might be possible, to some extent, to disentangle the influence of experience of stress and related symptoms from the expression and reporting of stress and related symptoms.
Given that stress-related ill-health might encompass physical and psychological ill-health, then we must also consider studies that assess physical health, psychological health or both. It is also possible to distinguish between acute and chronic illness.
Finally, we have also included health-related behaviours for consideration (such as visits to the physician, selfreports of medication use etc). This might give us further insight into the reporting of stress-related symptoms.
Table 2.2 shows the classification of health measures used as dependent variables in this review.
16

Table 2.2. Typology of health indices.
Measurement
Health state
Self-reports Physician-reports Objective measures/research
team diagnosis Acute psychological e.g. Emotions e.g. Acute anxiety
disorder e.g. Diagnosis by
research team psychiatrist(s)
Acute physical e.g. Non-specific symptoms such as
headaches
e.g. Influenza e.g. Swabs taken for presence of flu
bugs Chronic psychological e.g. Psychiatric
screening surveys such as the Beck
depression inventory
e.g. Diagnosed depression
e.g. Diagnosis by research team psychiatrist(s)
Chronic physical e.g. Self-reports of angina
e.g. Hypertension e.g. Hypertension measured by physiological
indices Health behaviours e.g. Self-reported
drinking e.g. Visits to
physician e.g. Objective
measure of alcohol consumed
2.6. Structure of report
The rest of the report consists of four chapters:
Chapter three describes the major part of the project: a meta-analysis to identify the role of individual differences in the work-related stress process.
Chapter four is concerned with identification of variation in individual differences that influence stress in the UK population.
Chapter five is concerned with explaining the findings of the third and fourth chapters with reference to theory and other evidence.
Chapter six draws conclusions from this research with respect to implications for monitoring and measurement of work-related stress and associated symptoms; policy and practice; and research.
17

3. Quantitative review: meta-analysis Meta-analysis is a statistical technique for aggregating information across several studies to provide better estimates of relationships between two or more variables. In this way, meta-analysis is able to capitalise on larger sample sizes. It is also able to compensate for some methodological weaknesses of studies directly. As such, unlike more traditional reviews, meta-analysis allows researchers to provide quantitative estimates of relationships.
The purpose of this chapter is to outline the methodology used to identify studies to include in the meta-analysis and to convey the findings.
To recap, to identify cognitive and perceptual processes that influence the experience, expression and reporting of stress-related symptoms, it is necessary, first, to identify individual differences that provide variation in those cognitive and perceptual processes. By identifying such individual differences, it is possible to infer the differences between individuals in the cognitive processes that underpin the experience, expression and reporting of stress-related symptoms. Theoretical knowledge can be used to help these inferences.
Consequently, we have focused our review of the literature around six main questions5:
RQ1) To what extent do individual differences have an influence on subsequent health-related variables in working samples?
RQ2) Which of trait, attitudinal or state individual differences has the strongest influence on health-related variables in working samples?
RQ3) How do individual differences influence the reporting, experience and expression of health?
We were also interested in determining whether individual differences moderated the relationships between psychosocial hazards and health-related outcomes. However, only two studies that met our inclusion criteria have been published, and both these studies reported information in such a way that we could not use them for meta-analysis.
18
5

RQ4) To what extent do workplace psychosocial hazards have an influence on subsequent health-related variables?
RQ5) What are some of the influences on relationships between health-related variables and psychosocial hazards?
RQ6) How stable is psychological health?
We now explain how we addressed each research question in more detail.
RQ1) To what extent do individual differences have an influence on subsequent health-related variables in working samples?
To answer this question, we aimed simply to assess the strength of the statistical relationship between individual differences and health-related variables in working samples. We examined relations between individual differences and subsequent health so that we could be more confident that any relationship reflects the extent to which individual differences cause health (rather than changes in health changing individual differences). Therefore, we examined only longitudinal studies. We explain our reasoning in more detail in section 3.1.1.
We also assessed the strength of the statistical relationship above and beyond the influence of psychosocial hazards on health as well as above beyond the influence of initial health status, in order to rule out some alternative explanations, such as that some psychological characteristics (e.g. neuroticism) or poor health make it more difficult for job applicants to be selected for good jobs.
RQ2) Which of trait, attitudinal or state individual differences has the strongest influence on health-related variables in working samples?
To answer this question, we aimed simply to assess whether the strength of the relationship between individual differences and health variables is stronger or weaker for traits, attitudes and state individual differences.
19

RQ3) How do individual differences influence the reporting, experience and expression of health?
To answer this question, we aimed to assess whether the strength of the relationship between individual differences and health varied according to kinds of methods used to assess health and related variables. If, for example, self-reports of physical health are more strongly related to individual differences than physician reports and research team diagnosis, then we can conclude that cognitive factors influence the cognitive experience or reporting of stress-related physical illhealth, but not the expression of physical ill-health.
RQ4) To what extent do workplace psychosocial hazards have an influence on subsequent health-related variables?
Since we are interested in the role of individual differences in the work context, it seems natural to include this question. Again, since we are interested in a causal relationship, we examined the influence of psychosocial hazards on subsequent health. We also assessed the extent of the relationship between psychosocial hazards and health, above and beyond the influence of individual differences and initial health status. If a reliable statistical relationship remained after taking into account individual differences and initial health status, then we could be more confident that psychosocial hazards do cause ill-health in some way, rather than reflecting differences in how people experience the work environment.
RQ5) What are some of the influences on relationships between health-related variables and psychosocial hazards?
To answer this question, we examined whether different methods or measures of health and psychosocial hazards influenced the strength of the relationship between psychosocial hazards and health. If, for example, there is a stronger relationship between psychological health and psychosocial hazards than for physical health, then we might conclude the influence of the work environment on physical health is mediated through psychological health.
RQ6) How stable is psychological health?
Assessing the stability of psychological health does give some indication of the extent to which changes in the
20

work environment might lead to changes in psychological health, at least over the shorter term. Also, good psychological health is closely related to a positive orientation, and poor psychological health to a negative orientation – for example people nearing clinical levels of poor psychological health are more likely to rate their work demands as stressful (Daniels and Guppy, 1997). Therefore, assessing the stability of psychological health, as indexed by measures of job satisfaction or anxiety for example, would help to provide some assessment of the extent to which influential individual differences that reflect a positive to negative orientation are malleable. To do this, we aimed to assess the strength of the relationship between psychological health measured on two occasions.
In the rest of this chapter, we explain:
i) the procedures we used to search the literature for relevant studies;
ii) the procedures used in our meta-analysis;
iii) the results of the meta-analysis.
3.1. Searching the literature. To identify relevant journals, we surveyed the following data-bases for the years 1996-2001 inclusive: Web of Science, PsychInfo and MedLine. Additionally, we conducted manual trawls for relevant articles in the following journals, identified by consensus amongst the research team, HSE advisors and members of our expert panel as the top journals in this field. The journals surveyed6 were:
Academy of Management Journal Journal of Psychosomatic Research Journal of Applied Psychology Journal of Organizational Behavior Journal of Occupational Health Psychology Journal of Occupational and Organizational Psychology
Some journals were excluded from the manual review, although their quality was felt to be high. They were excluded because their focus was too general and they rarely carry material relevant to psychosocial hazards and occupational health. The journals considered, but excluded, were Epidemiology, American Journal of Epidemiology, International Journal of Epidemiology, American Journal of Public Health, Journal of Personality and Social Psychology, Journal of Epidemiology and Community Health, British Medical Journal.
21
6

Journal of Occupational and Environmental Medicine Occupational and Environmental Medicine Occupational Medicine Psychological Medicine Psychosomatic Medicine Scandinavian Journal of Work, Environment and Health Work & Stress
Articles of a theoretical nature, review articles or metaanalyses that might inform the discussion of theoretical paths linking individual differences to work-related stress were also identified from this manual search. In this respect, we extended our manual search from 19912001 inclusive for such articles. Specifically to search for theoretical and review articles, the following journals were also examined manually for the years 1991-2001 inclusive:
Academy of Management Review Psychological Bulletin Psychological Review
We restricted our search to peer-reviewed, English language journals only. We opted for English language journals since a) none of the research team has the requisite technical proficiency in other languages and b) it is widely recognised that the majority of top journals in the area are published in English, including some continental European journals.
We restricted our search to peer-reviewed journals as peer review provides an important quality control process on the literature. By considering peer-reviewed journals only, we can be confident of including only top quality studies in the review.
The researchers were aware of a wide-spread suspicion associated with publication bias in peer-reviewed journals (towards positive results). However, given the criticism of methodologies routinely employed in workrelated stress research (Kasl 1996; Zapf, Dormann and Frese, 1996), we thought it unlikely that any publication bias would make a significant impact on the rigour of the review (see below). In addition, meta-analytic procedures are capable of estimating the likely influence of publication bias in a particular area (see below).
Peer-reviewed studies were also chosen to help reduce the significant number of papers. Very little is to be gained by inclusion of non-peer-reviewed studies, since
22

there are enough peer-reviewed to provide stable estimates of correlations – especially relative to the cost that needs to be invested in finding such studies.
Although we did not include evidence from non-peer-reviewed sources, we did write to experts in the field, identified by consensus amongst the research team, HSE advisors and members of our expert panel. We asked these experts to identify any material of their own or others’ – published or unpublished – relevant to our research questions. We extend out thanks to the following who responded to our request:
Prof Cary Cooper CBE Dr Jan de Jonge Prof Stanislav Kasl Dr Katherine Parkes Prof Roy Payne Prof Dr Wilmar Schaufeli Prof Paul Spector Dr Jukka Vuori Prof Peter Warr Prof Jerry Wofford
Where experts identified peer-reviewed studies that met our inclusion criteria, they were included in the analysis. Other contributions were examined to inform the discussion of theoretical paths linking individual differences to cognitive and perceptual factors in workrelated stress.
It was the anticipated size of the literature that limited our search to the five years 1996-2001 inclusive, so that a sufficient number of studies could be reviewed within the time available. We chose these years for two reasons.
First, more recent studies are likely to have higher standards of theoretical, methodological and analytic sophistication and rigour – especially after the criticisms of stress research published in the late 1980s and early 1990s. Indeed, Zapf et al (1996) published a paper summarizing longitudinal studies of work-related stress. In their critique of this research, they outlined a number of design strategies for improving longitudinal studies to the standards where causal inference could be reasonably drawn. In their review, they noted that very few studies then published actually met these standards. Therefore, we can reasonably expect to find better and
23

more rigorous longitudinal designs published after 1996.
Second, evidence indicates the presence of societal shifts in the reporting of stress-related symptoms from the 1950s (Twenge, 2000). By limiting the review to more recent studies, we also limit the confounding due to these societal shifts and ensure the findings are more relevant to contemporary UK society.
3.1.1. Inclusion criteria In addition to peer reviewed articles published 19962001 that included measures of health, individual differences and workplace psychosocial hazards, studies were included in the review if they met the following criteria:
a) Longitudinal data collection, where the independent measures (i.e. individual differences, psychosocial hazards) were collected before the dependent measures, and lagged measures of the dependent measures were taken concurrently with the independent measures. Longitudinal data is necessary to demonstrate causation (see e.g. Rick et al, 2002) 7, since it is necessary to show that cause precedes effect at the very minimum. By including only those studies that control for initial values of the dependent variables, it is possible to relate changes in the dependent variables to individual differences and psychosocial hazards, thus strengthening our ability to say that relationships observed are causal (Cook and Campbell, 1976; Zapf et al, 1996).
b) Data collected from working samples, an obvious requirement to assess psychosocial hazards in the workplace.
c) Samples without any specific illness, either true prospective designs where participants are screened for premorbid signs of the illness under investigation or ‘slice-of-life’ designs, in which participants with non-specific illnesses might be included (Kasl, 1983). An exception to this rule
This criterion is especially important as reciprocal relationships exist amongst psychological and physical health and many individual differences (such as locus of control, e.g. Daniels and Guppy, 1997). Cross-sectional studies are therefore unsuitable for this review, since in the meta-analysis, we are trying to place a statistical estimate of an effect size on a causal relationship.
24
7

was made for studies that were investigating illness as a cause of further ill-health (where initial measures of illness were treated as an individual difference).
3.1.1.1. The search terms Consultation with the HSE advisors and our expert panel, through a formal meeting and exchange of email correspondence was used to identify the search terms for the review.
The formal meeting and subsequent email correspondence were subject to a basic Requirements Capture/Knowledge Elicitation exercise at the early stages of the research project. This exercise involved recording the initial meeting with audio equipment and the subsequent transcription of the tapes. This Requirements Capture/Knowledge Elicitation was conducted in order to serve three purposes for the review;
i) it was conducted so that it would aid the research team in more quickly and easily formalising the research questions and criteria for the review process and allow the identification of the key factors that would guide the process;
ii) this exercise also served to allow for a reference point to be established that guided subsequent discussions about the review, additions to the review process and allowed for the ‘progress’ of the review to be evaluated against a single reference point;
iii) The ‘requirements capture’ also allowed the research team to identify quickly knowledge gained from previous projects, lessons learned, skills and experience acquired, as well as methodologies and materials that could easily be re-used during the review process. This enabled the work to proceed efficiently and also ensured that the ‘wheel was not reinvented’.
The search terms for the review are shown in table 3.3. Given the inclusion criteria noted above, data-bases were scanned for studies that included measures of individual differences, psychosocial hazards, health and that met the inclusion criteria. Consequently, the search terms included ‘AND’ qualifiers for methods, sampling
25
and health. ‘OR’ qualifiers were also used to pick up several terms potentially relevant the purposes of the review or the inclusion criteria set.
The methods keywords were (longitudinal OR diary OR objective_measures OR quasi-experiment OR intervention OR experiment).
The sampling keywords were (occupational OR organisational OR organizational OR industrial OR work).
The health keywords were (stress OR well-being OR health OR illness OR emotions OR affect OR mood OR labelling).
3.1.2. The scale of the literature and sifting the literature Table 3.3. also shows the number of ‘hits’ for each search. Excluding the results of the manual search, this gave us over 4000 abstracts to sift. It was therefore decided to engage in a two-stage sifting process (cf. Rick et al, 2002). The first sift was designed to reduce the total number of abstracts to a manageable number. At this stage, the goal was to exclude papers that definitely did not meet the inclusion criteria. Abstracts were sifted according to the following criteria:
a) Abstract indicated the design was longitudinal or experimental.
b) Abstract indicated the sample was a working sample.
c) Abstract indicated the study has taken measures of individual differences AND psychosocial hazards/stressors AND some health type outcome (including absence).
26

Table 3.1. Search terms used to identify abstracts.
Individual differences keywords No. of ‘hits’ on Web of Science
No. of ‘hits’ on PsychInfo
No. of ‘hits’ on MedLine
individual differences 45 63 12
personality 143 259 49
(Big 5 OR extraversion OR neuroticism OR openess_to_experience OR conscientiousness OR agreeableness)
18 15 6
(Trait_affect OR negative_affectivity OR positive_affectivity OR pessimism OR optimism)
47 27 4
(Attitudes OR job-involvement OR work_involvement OR organizational_commitment OR organisational commitment
284 549 93
(Dysfunctional attitudes OR depression OR anxiety)
402 511 183
Hypochondria OR hypochondriasis OR self_focused_attention OR health_anxiety
500 2 0
(Type_A-Behavior_Pattern OR Type_A-Behaviour_Pattern)
1 0 0
(locus_of_control OR perceived_control OR self-efficay OR self_efficacy OR sense_of_coherence OR hardiness)
408 0 0
(coping_style OR coping_disposition) 9 0 0
(self-esteem OR self_esteem) 78 133 42
(workability OR ability_to_relax) 2 0 0
(morningness OR eveningness) 4 0 0
symptom_amplification 0 0 0
flow 324 16 61
Total 2265 1575 450
Grand total 4290
27

According to these pre-sift criteria, abstracts were sorted as follows:
a) Include;
b) Full paper required before a decision can be made;
c) Need to discuss abstract with another member of the review team;
d) Paper is potentially useful for the theoretical review;
e) Reject.
Abstracts falling into the first two categories were taken forward to the next stage of sifting. At this stage, a more rigorous sifting process was instigated, involving formal recording of information on a pro forma. This sifting pro forma is shown in Appendix A.
The pro forma was developed from templates used on previous projects by members of this research team (Rick, Briner, Daniels, Perryman and Guppy, 2001, Rick et al, 2002). The pro forma was developed through several iterations of consultation with members of the expert panel and members of the core research team. A final iteration included two of the team coding a number of abstracts together to assess the suitability of the pro forma.
The purpose of the pro forma was to ensure studies included in the final meta-analysis met, unambiguously, the criteria for inclusion. A secondary purpose was to ensure decisions made were clear and auditable.
Reviewers were asked to consider eight questions. These questions were meant to ensure that studies selected were suitable for review. The questions were:
1) Was the paper published in a peer-reviewed journal?
2) Did the paper provide evidence on relationships between an individual difference(s) and a health outcome(s)?
3) Did the paper provide evidence on an individual difference that fell into the typology of individual differences developed for the review?
4) Was the paper an empirical paper?
28

5) Did the study use any kind of longitudinal methodology?
6) Did the paper provide evidence on health outcomes that fell into the typology of health outcomes developed for the review?
7) Did the sample consist of working adults?
8) Were psychosocial hazards measured?
The paper was discarded if it failed any of the eight criteria. However, relevant theoretical papers, review papers or meta-analyses were kept in case they were useful for the theoretical phase of this project. Sifting was initially conducted on abstracts. However, if it was not possible to determine answers to the questions from the abstract, then the full paper was consulted.
To help ensure consistency of coding, an instruction set was issued to all coders (see Appendix A). Further, coders were invited to discuss, with other members of the team, problematic issues or abstracts.
Statistical reliability checks were made on the coding. A random sample of 80 abstracts coded by two of the team was second coded by another member of the team. Reliability was assessed by looking at abstracts that were rejected against those taken forward to the next stage of the review (accepted, discussed further, or in need of obtaining full paper). In both cases, there was 80% agreement between coders.
Figure 3.1. shows the number of abstracts identified and sifted at each stage of the search procedure. At the final stage, a number of papers were excluded from the metaanalysis, since they did not provide sufficient information to be included in the analysis.
29

Figure 3.1. Stages in the review process.
Initial sift
Probably suitable Possibly suitable Unsuitable N=298 N=251 N=3741
Second sift
Suitable Unsuitable N=106 N=4184
Review
Papers excluded during review N=89 Number of papers included N=17 (total 19 samples)
3.2. Meta-analysis 3.2.1. A brief introduction to meta-analysis and correlation coefficients Meta-analysis is a statistical procedure for aggregating results from several studies to provide an overall estimate of the statistical relationships between two or more variables. Its strength is its precision in aggregating results, so that, for example, stronger studies with larger samples can be given more weight in the analysis.
However, all that meta-analysis can do is provide statistical estimates. If the evidence base is not strong, for example because all studies in an area use weak cross-sectional methods, then the estimates from the meta-analysis are similarly limited. It is for this reason that we concentrated on the best available studies – i.e. longitudinal studies that meet modern standards of acceptable rigour. Indeed, as Hunter and Schmidt note ‘Substantive elimination of error of measurement is vastly superior to elimination by statistical formula after the fact’ (1990, p 122).
Also, because meta-analysis is a statistical tool, it cannot easily incorporate information from qualitative studies. Neither can the statistical analysis provide reasons that explain the nature of the relationships
30
found: more conventional review procedures are needed for this.
There are several forms of meta-analysis, each of which assesses a different form of statistical relationship. The form we use here is based on the work of Hunter and Schmidt (e.g. Hunter and Schmidt, 1990), who have developed procedures for aggregating and synthesizing correlation coefficients, as the index of statistical association. A correlation coefficient can vary between –1 and +1. –1 indicates a perfect negative relationship (i.e. as X decreases, Y always increases); 0 indicates that there is no relationship; and 1 indicates that a perfect positive relationship (i.e. as X increases, Y always increases). In reality in the social sciences, correlations approaching –1 or +1 are rare. It is more usual to encounter correlations varying between -.50 and +.50. Cohen (1977) considers that in the social sciences, a correlation over .10 (+ or –) can be considered small, a correlation over .30 can be considered medium and a correlation over .50 can be considered large.
Here, the aim of our meta-analysis, then, is to provide an overall correlation coefficient that summarises the relationships across a number of studies. To do this, we used the HLM-5 statistical programme, which includes procedures for conducting meta-analysis (Bryk and Raudenbush 1992). Since we are interested in causation, and this can be better demonstrated in longitudinal studies, the correlations we examine are those where individual differences or psychosocial hazards measured at one point in time are related to health and related variables measured at a subsequent occasion.
Initially, meta-analytic techniques were developed to estimate correlations. However, if several correlations are estimated, it is then possible estimate aggregate partial correlations. Partial correlations give an index of the strength of a relationship between two variables, after taking into account the influence of other variables. For example, if people with a generally negative orientation tend to report more psychosocial hazards at work and report more stress symptoms, any correlation observed between psychosocial hazards and stress symptoms might merely reflect the tendency of some people to perceive the world and themselves more negatively. However, using partial correlation allows us to take into account such individual variation. So, a
31

partial correlation between psychosocial hazards and health controlling for negative orientation would give us a more accurate picture of the relationship between psychosocial hazards and health. Similarly, when assessing the relationship between individual differences and subsequent health, a partial correlation controlling for the effects of prior health would give us as estimate of the relationship between individual differences and change in health status. By using partial correlation to examine changes in this way, much stronger conclusions can be drawn with respect to causality (Zapf et al, 1996).
In this research, then, we use meta-analysis to produce several aggregate correlations, which we then use to calculate a series of partial correlations:
a) Partial correlation between individual differences and subsequent health controlling for psychosocial hazards;
b) Partial correlation between individual differences and subsequent health controlling for prior health;
c) Partial correlation between individual differences and subsequent health controlling for both psychosocial hazards and prior health;
d) Partial correlation between psychosocial hazards and subsequent health controlling for individual differences;
e) Partial correlation between psychosocial hazards and subsequent health controlling for prior health;
f) Partial correlation between psychosocial hazards and subsequent health controlling for individual differences and prior health;
In this way, we used partial correlations to assess whether individual differences influenced health – above and beyond the effects of psychosocial hazards and prior health. We were also able to use partial correlations to assess the influence of psychosocial hazards on subsequent health above and beyond the effects of individual differences and prior health.
32

Clearly, the strength of relationships can vary across studies, due partly to random variation introduced by sampling, but also because of systematic factors embedded in different methods used in different studies. Meta-analysis is able to examine whether the strength of a correlation varies across studies with different features.
For example, it is possible to examine the differences in the size of a correlation between individual differences and psychological and physical health. These systematic features of studies are often referred as moderators in meta-analyses.
An examination of some moderators is included in this report. Specifically, we examined whether correlations between individual differences and health and related variables were altered:
i) when objective rather than subjective measures of health were used, since this would give us an indication whether there is a difference between the experience of health problems rather than reporting of health problems;
ii) when acute rather than chronic health problems were being assessed;
iii) when psychological health rather than physical health or health behaviours was assessed;
iv) when physical health rather than health or psychological health behaviours was assessed (NB this is a slightly different question to the one posed in iii);
v) when state and attitudinal individual differences rather than trait differences are assessed;
vi) when sample sizes increased. Larger samples are more likely to find statistically significant results. If there is a relationship between sample size and the size of correlations, this might indicate that editors are more likely to accept studies that produce statistically significant results, and that there could be a pool of studies that have not been published that show only small correlations;
vii) according to the proportion of men in the sample;
33

viii) according to the average age of the sample;
ix) according to the time lag between initial assessment of health and individual differences, since this would give an indication of the durability of any relationships uncovered;
x) the response rate of the sample;
xi) the country of origin of the sample. We conducted two analyses here. First, we compared findings from UK samples with findings from all other samples. This would give an indication of whether there is something different occurring in the UK context. Second, we examined findings from the ‘Anglo-Saxon’ cultures (e.g. UK, USA, Canada, Australia) with findings from other cultures, to examine whether there is something in the Anglo-Saxon cultural context that influences the relationships between individual differences and health and related variables.
We examined the following potential moderators of the relationships between psychosocial hazards and health and related variables:
xii) objective versus subjective measures of health;
xiii) acute versus chronic health problems assessed;
xiv) psychological health versus physical health or health behaviours assessed;
xv) physical health versus health or psychological health behaviours assessed;
xvi) self-report versus other methods used to assess psychosocial hazards;
xvii) sample size;
xviii) proportion of men in the sample;
xix) average age of the sample;
xx) time lag between initial assessment of health and psychosocial hazards;
xxi) response rate;
34
xxii) UK versus other countries, and Anglo-Saxon versus other cultures.
When assessing the stability of psychological health, we examined the following moderators:
xxiii) acute versus chronic psychological problems assessed;
xxiv) sample size;
xxv) proportion of men in the sample;
xxvi) average age of the sample;
xxvii) time lag between initial assessment of health and psychosocial hazards;
xxviii) response rate;
xxix) UK versus other countries, and Anglo-Saxon versus other cultures.
Psychosocial measurement is plagued by problems with reliability of measures. Even though we chose to include only those studies that met the highest possible methodological standards in the area of work-related stress, measurements included in the meta-analysis would contain some degree of error in their measurements.
It has been long established that random error in measurement serves to reduce the size of correlations observed in any set of data (Hunter and Schmidt, 1990). However, it is possible to estimate the degree of error in well-designed measurements and it is common practice in many journals to report estimates of the degree of error in any given measurement by providing indices of reliability. From these estimates, meta-analytic procedures are then able to produce an estimate of the size of the correlation that would be observed if all measurements were free from random error. Estimates of this nature are included in this report, based on the formula provided by Hunter and Schmidt (1990).8
Meta-analytic procedures can also provide estimates for situations where it is suspected that members of the sample vary over only a limited range of the variables under consideration. These techniques were developed for selection tools, since it is reasonable to suppose that the poorest performers would never have been selected in the first place. However, in studies of stress, there is no
35
8

Meta-analysis might produce more accurate estimates of correlations than single studies, yet they are still based on finite, even if large, aggregated samples. This means that the estimates produced might be inaccurate and could vary over a range of values.
To assess this, confidence intervals can be calculated. These provide a range of values within which the correlation is likely to fall, and where we can be, say, 95% confident that the value calculated will fall within that range.
Confidence intervals are especially useful where correlations are small. If the confidence interval includes 0, then it is possible that no relationship exists between the variables at all. Confidence intervals were calculated using the formula provided by Hunter and Schmidt (1990).
As noted above, it is possible that journal editors and reviewers are favourably biased toward studies that show positive results. We consider that this is not a problem where only very high quality studies are included in the analysis, since such high quality studies are currently rare in the work stress area, and we would expect high quality studies to be published regardless of whether findings indicate relationships or not. Nevertheless, meta-analytic techniques can provide estimates of the number of studies that would need to be conducted to bring the estimated correlation to below some pre-specified level. Again, we made these estimations using the formula by Hunter and Schmidt (1990).
3.2.2. Coding the papers To answer the research questions set and produce corrected estimates and partial correlations, we needed longitudinal papers that included:
a) An estimate of the reliability of measures used in the study;
b) Details on bivariate associations between measures of hazards, individual differences, baseline health
reason to suppose that samples would be restricted with respect to the range of ordinary human experience, and so the effect of range restriction was not assessed.
36

and subsequent health, so that partial correlations could be estimated;9
c) Details on moderators.
Upon reading the papers included in the review until this stage, it was clear that many did not provide sufficient information to be included in the metaanalysis. Some 66 papers did not include sufficient information and were therefore rejected.
A further 18 papers were rejected because close examination of the paper revealed the paper failed the initial sort criteria.
A further five papers were excluded because they used the same sample as reported in another paper.
Where more than one paper was provided from the same sample, the paper chosen for inclusion had the most extensive set of health-related variables. If this criterion could not discriminate between papers, then the paper with the most extensive set of individual differences was chosen. If this still failed to discriminate, the paper that used the largest proportion of the sample to calculate correlations was chosen.
From the 106 papers that made it through the final sift, only 17 studies provided sufficient information or were sufficiently well designed to be included in the metaanalysis. Of these 17 studies, two included separate correlation matrices for male and female participants, but did not include a combined matrix. Therefore, each of these studies was treated as if it was a separate study and the correlations entered separately into the database.
Since each study was longitudinal, we analysed correlations between health and related variables assessed at the first wave of data collection and the second wave of data collection and individual differences and psychosocial hazards assessed at the first wave of data collection.
We also analysed correlations between individual differences and psychosocial hazards assessed at the
Formulae exist for estimating Pearson correlations from other indices of association, such as odd-ratios. However, in the current review, the only papers that included sufficient information on bivariate associations between all variables of interest did so by reporting Pearson correlation coefficients.
37
9
first wave of data collection, and we analysed correlations between health and related variables assessed at the first and second waves of data collection.
To establish confidence intervals around aggregated correlations, it is necessary to have information on the sample sizes of the individual studies. Since it is common that there is incomplete information on some variables for some participants within individual studies, the number of observations used to calculate different correlations can vary within any given study. Therefore, where information was not given on the exact number of study participants used to calculate a correlation, the median number used to correlate all correlations in a study was used.
Health and related variables were coded as:
a) chronic or acute;
b) psychological, physical or a health behaviour;
c) measured objectively or subjectively.
Individual differences were coded so that high scores represented a negative orientation, and were further coded as trait, attitudinal or state.
All individual difference variables were assessed by self-report in the studies that we examined.
Psychosocial hazards were coded as:
a) measured objectively or subjectively;
b) demands, control, support or other kind of hazard.
Two of the report’s authors coded independently a random sample of 11 papers, so that 20 health and related outcomes were coded, 20 individual differences were coded and 20 psychosocial hazards were coded.
Across all ratings, a total inter-rater agreement of 88% was obtained, ranging from 75% (for whether health and related variables were chronic or acute) to 100% (for how health and related variables were measured). All of the papers were coded by one individual for the meta-analysis.
38
3.2.3. Findings The 19 studies included in the meta-analysis yielded a combined sample size of 6087.
The mean sample size was 320.4 (standard deviation = 204.6, range 87-940).
On average, men comprised 44% of each sample (standard deviation = 32%).
The average age of the samples was 36.1 years (standard deviation = 7.9).
The average lag between waves of data collection was 14.6 months (standard deviation = 17.7).
The average response rate was 58% at the first wave of data collection (standard deviation = 25%).
Two of the studies used UK samples, four used US samples and one was an Australian sample. Ten studies were conducted on mainland Europe and two were conducted in Israel (these were male and female samples reported in the same paper).
Most of the studies used self-report assessments alone (14), four used a mix of self-report methods and other objective measures and one was an intervention study. All measures of individual differences were self-report.
Eighteen out of 99 correlations between individual differences and health used objective measures of health and related variables. Eighty-one used self-report measures of health and related variables. Thirty-three involved measures of acute health problems and 66 involved measures of chronic health problems. Twentysix involved indices of physical health, 63 involved indices of psychological health and ten involved indices of health behaviours. Twenty-two of the correlations involved trait individual differences, 75 involved attitudes and just two involved psychological states.
Twenty-four out of 120 correlations between psychosocial hazards and health used objective measures of health and related variables. Ninety-six used self-report measures of health and related variables. Thirty-six correlations involved measures of acute health problems and 84 involved measures of chronic health problems. Sixteen involved indices of physical health, 88 involved indices of psychological health and 16 involved indices of health behaviours. Only four correlations out of 120 involved objective measures of psychosocial hazards, the rest using subjective methods. Forty-nine correlations involved measures of demands, 15 measures of control, 37
39
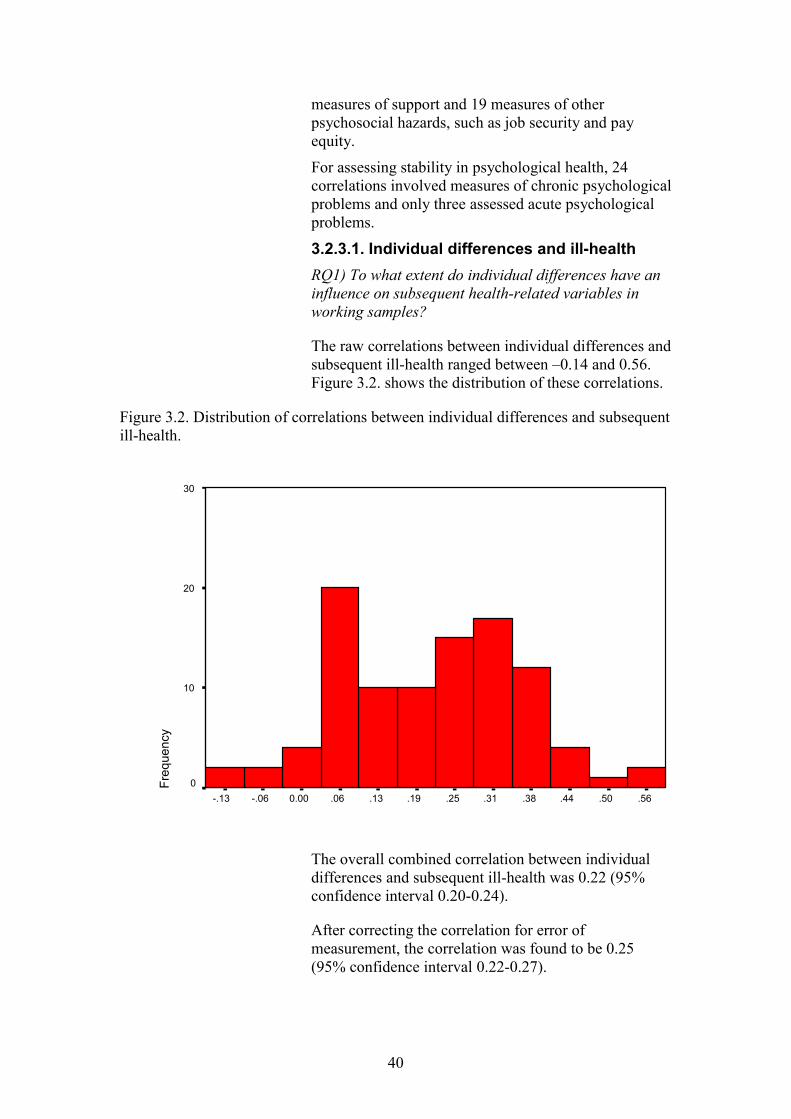
measures of support and 19 measures of other psychosocial hazards, such as job security and pay equity.
Freq
uenc
y For assessing stability in psychological health, 24 correlations involved measures of chronic psychological problems and only three assessed acute psychological problems.
3.2.3.1. Individual differences and ill-health RQ1) To what extent do individual differences have an influence on subsequent health-related variables in working samples?
The raw correlations between individual differences and subsequent ill-health ranged between –0.14 and 0.56. Figure 3.2. shows the distribution of these correlations.
Figure 3.2. Distribution of correlations between individual differences and subsequent ill-health.
30
20
10
0 -.13 -.06 0.00 .06 .13 .19 .25 .31 .38 .44 .50 .56
The overall combined correlation between individual differences and subsequent ill-health was 0.22 (95% confidence interval 0.20-0.24).
After correcting the correlation for error of measurement, the correlation was found to be 0.25 (95% confidence interval 0.22-0.27).
40

This indicates that a negative orientation is associated to a small to medium degree with measures of subsequent poor health or unhealthy behaviours.
Analysis indicates that at least another 120 longitudinal studies showing minimal effects would need to be conducted to bring this correlation down to a level that would indicate there is no statistically reliable association.10 Since Zapf et al were able to find less than 50 longitudinal studies in the review of the stress literature up to 1996, then it is unlikely that there are 120 studies showing minimal effects that have not been published in recent years. Therefore, we can be confident that our findings represent a statistically reliable association.
RQ2) Which of trait, attitudinal or state individual differences has the strongest influence on health-related variables in working samples?
Because of the small number of studies looking at state individual differences, we analysed the differences between states and attitudes on the one hand and traits on the other. However, we found that the difference between correlations was very small (difference = .02, with states and attitudes having the slightly larger correlation with health and related variables). This difference was not statistically reliable.11
RQ3) How do individual differences influence the reporting, experience and expression of health?
To answer this question, we examined a range of moderators. The majority indicated either no effects of the moderator variables or only small differences that were not statistically reliable.
However, two interesting and statistically reliable differences did emerge. First, there was a large difference between the correlation for self-reports of health and related behaviours and objective measures. This was a difference of 0.21 in the correlations. For objective measures, the correlation was a very small 0.06. For self-report measures, the correlation was
10 We judged the cut-off for an association to be statistically unreliable as 0.03, which is the maximum correlation in the 95% confidence interval around zero for the combined sample in the current meta-analysis.
The conventional statistical probability of p<.05 is used to detect a statistically reliable difference in these moderator tests.
41
11

0.27. Note however, that psychological health was only assessed by self-report in these studies.
Second, there was a statistically reliable difference of Fr
eque
ncy
0.09 in the correlations between psychological health (correlation = 0.23) and physical health and health behaviours (correlation = 0.16).
These findings indicate that individual differences might influence the experience of stress symptoms – both psychological and physical - and related emotional states. In turn, it is possible that this might then influence the expression of symptoms to physicians.
However, the results indicate that individual differences have a minimal influence on physical symptoms and health behaviours, such as absence.
3.2.3.2. Hazards and ill-health RQ4) To what extent do workplace psychosocial hazards have an influence on subsequent health-related variables?
The raw correlations between psychosocial hazards and subsequent ill-health ranged between –0.07 and 0.64. Figure 3.3. shows the distribution of these correlations.
Figure 3.3. Distribution of correlations between psychosocial hazards and subsequent ill-health.
20
10
0 -.06 0.00 .06 .13 .19 .25 .31 .38 .44 .50 .56 .63
42

The combined correlation between psychosocial hazards and subsequent ill-health was 0.18 (95% confidence interval 0.16-0.20).
After correcting the correlation for error of measurement, the correlation was found to be 0.20 (95% confidence interval 0.18-0.22).
This indicates that greater psychosocial hazards are associated to a small degree with measures of subsequent poor health or unhealthy behaviours.
Using the same criteria as for individual differences, we calculate that at least another 95 longitudinal studies showing minimal effects would be needed to reduce this association to a level that is not statistically reliable. In the context of the number of longitudinal studies in this area, then, we can be confident that there is a statistically reliable association between psychosocial hazards and subsequent health. Further, this correlation is of a similar magnitude to findings reported by Cass, Faragher and Cooper (in press) in their meta-analysis of cross-sectional associations between hazards such as low job control and indices of psychological and physical health.
RQ5) What are some of the influences on relationships between health-related variables and psychosocial hazards?
As with individual differences, many of the moderators that we examined had either no effects or effects that were so small that they were not statistically reliable. This includes examining the moderating effects of different types of hazards.
There were three effects worth noting, two of which were statistically reliable.
First, there was a statistically reliable difference between psychological health on the one hand and physical health and health related behaviours on the other (difference = .11). The correlations were .22 and .11 respectively. There was a larger statistically reliable difference between physical health on one hand and psychological health and health behaviours on the other (difference = .17). The correlations were .04 and .21 respectively. Together, these results indicate that psychosocial hazards might have the strongest effect on psychological health, a weaker influence on health
43

behaviours and the weakest influence on physical health.
Freq
uenc
y We did not find a large difference between correlations using self-report measures of hazards and those using more objective measures (difference = .04). Although not statistically reliable, self-report methods did produce higher correlations (.22). This small difference might reflect the small number of longitudinal studies that used objective measures in our sample, and so no firm conclusions can be drawn from it.
3.2.3.3. Stability in health measures RQ6) How stable is psychological health?
The raw correlations between initial and subsequent psychological health ranged between 0.19 and 0.82. Figure 3.4. shows the distribution of these correlations.
Figure 3.4. Distribution of correlations between initial and subsequent psychological health.
10
8
6
4
2
0 .19 .25 .31 .38 .44 .50 .56 .63 .69 .75 .81
The meta-analysis indicated a large combined correlation of 0.59 between indices of psychological health measured at two points in time (95% confidence interval = .57-.61).
Corrected for error in measurement, this rose to 0.72 (95% confidence interval = .69-.73).
Our analysis indicates that at least another 354 studies would be needed with null results to reduce this
44

association to a level that is not statistically reliable. Therefore, we can be confident in asserting that there is a high degree of stability in negative orientation to the work environment.
This figure of 0.59 is higher than the figure reported by Dormann and Zapf (2001) in their meta-analysis of stability in indices of job satisfaction (0.42). This might be because their analysis was focused just on satisfaction, and we included a wider range of variables. However, the time lags between measurements ranged from a few weeks to over ten years in the Dormann and Zapf study. Examining those correlations produced by Dormann and Zapf for periods of a few weeks to five years (the range of time lags in our sample) revealed more correlations in the range of 0.50 to 0.90. Also, our meta-analysis examined people that stayed in the same job. Dormann and Zapf found that the stability of job satisfaction dropped to 0.18 amongst people that change jobs. Combining both sets of analyses then, it appears that a negative orientation to the environment might be fairly stable over periods up to five years for people staying in the same job, but it can change over longer periods or if the characteristics of work change.
Examination of various moderators indicated no statistically reliable differences across the moderator variables.
3.2.3.4. Partial correlations RQ1) To what extent do individual differences have an influence on health-related variables in working samples?
The partial correlations between individual differences and health and related outcomes were found to be:
a) .20 (95% confidence interval .18-.22) when controlling for psychosocial hazards;
b) .13 (95% confidence interval .11-.15) when controlling for prior health;
c) .12 (95% confidence interval .10-.14) when controlling for psychosocial hazards and prior health.
Note - the range of the 95% confidence intervals did not include 0, and so we can be fairly confident in asserting that there is a causal relationship between a
45

psychologically negative orientation and measures of health and related outcomes.
As prior moderator analyses revealed, these analyses indicate that negative orientation is most likely to exert a causal relationship on the psychological states and the experience of symptoms, rather than the actual occurrence of physical symptoms.
RQ4) To what extent do workplace psychosocial hazards have an influence on health-related variables?
The partial correlations between psychosocial hazards and health and related outcomes were found to be:
d) .15 (95% confidence interval .13-.17) when controlling for individual differences;
e) .08 (95% confidence interval .07-.09) when controlling for prior health;
f) .06 (95% confidence interval .03-.09) when controlling for individual differences and prior health.
Again, the 95% confidence intervals did not include 0, and so, again, we can be fairly confident in asserting that there is a causal relationship between psychosocial hazards in the work place and measures of health and related outcomes. As the moderator analyses indicated, any causal effect is most likely to be noticed for psychological health, followed by health behaviours (including absence). The moderator analyses indicate any direct influence on physical health might be minimal.
3.3. Summary and implications of the meta-analysis
This meta-analysis sought answers to six questions. The analysis indicates that individual differences are associated with subsequent changes in health and related behaviours (RQ1), although the nature of the individual difference (state/attitude vs trait) did not alter the relationship between individual differences and subsequent health (RQ2).
We did find that individual differences were more likely to influence the psychological experience of stress symptoms – emotional and physical, rather than the reality of physical health (RQ3).
46

We also found that psychosocial hazards are associated with subsequent changes in health and related behaviours (RQ4), although there were no distinctions between different psychosocial hazards.
Nevertheless, we found that psychosocial hazards might exert their strongest influence on psychological health but their weakest influence on physical health (RQ5). Finally, we found a great deal of stability in psychological health (RQ6).
The main findings of the meta-analysis are summarised in table 3.2.
Table 3.2. Summary of main meta-correlations and confidence intervals.
Analysis Meta-correlation 95% confidence interval
Zero-order correlation of psychosocial hazards with subsequent ill-health.
0.18 0.16 - 0.20
Partial correlation of psychosocial hazards with subsequent ill-health, controlling for baseline health and negative orientation.
0.06 0.03 - 0.09
Zero-order correlation of negative orientation with subsequent ill-health
0.22 0.20 - 0.24
Zero-order correlation of negative orientation with subsequent ill-health, controlling for baseline health and psychosocial hazards.
0.12 0.10 - 0.14
Stability of psychological health (zero-order correlation of baseline psychological health with subsequent psychological health).
0.59 0.57 - 0.61
By focusing on the best possible longitudinal evidence and controlling for initial health status, the partial correlations derived in this meta-analysis provide some of the strongest evidence that psychosocial hazards cause changes in measurements of health and related variables. Note that whilst we can be more confident psychosocial hazards play a causal role, we can not be sure that our measures of health really do assess health accurately.
Nevertheless, even controlling for the influence of individual differences, there remained a statistically
47

reliable association between psychosocial hazards and health and related variables. Since individual differences might influence the reporting of stress symptoms, then we can be more confident of a true causal relationship between psychosocial hazards and health. In this respect, the moderator analyses are illuminating.
Individual differences have a minimal influence on physical symptoms and health behaviours, such as absence. Therefore, it may be concluded that individual differences have their strongest influence on the experience of psychological symptoms and the experience of physical symptoms. Psychological symptoms are inherently experiential, and many psychiatric disorders – especially the emotional disorders linked most closely to stress, such as anxiety and depression – are diagnosed by considering these experiential factors (Lindsay and Powell, 1994). In this case, our results suggest that self-report monitoring systems for psychological health and psychosocial hazards might be contaminated by some individuals being predisposed to experience psychological symptoms. However, this is complicated by theoretical accounts that indicate psychosocial hazards and individual differences operate in tandem to alter psychological health – not independently (see chapter 5).
For physical symptoms, the situation might be a little clearer cut. Because our results indicate that self-reports of physical symptoms are more closely related to individual differences than other measures of physical symptoms, then individual differences might influence the perception of symptoms, rather than necessarily any underlying physical problem. Therefore, our results suggest that monitoring systems reliant on individual self-reports of physical symptoms might be inaccurate and accentuated amongst those with a negative orientation to the work environment. Even so, it might be the case that the cognitive experience of symptoms leads to expression of those symptoms to practitioners. Whilst we were not able to assess the accuracy of physicians’ diagnoses in this meta-analysis, in chapter 5 we discuss how a generally negative orientation might influence how physicians diagnose and therefore report illness.
Psychosocial hazards were most strongly related to psychological health, and least strongly related to
48

physical health. The time lag in the studies was generally small (maximum of five years). This may have been insufficient to detect large variation in physical health which longer term studies might be capable of doing. However, it may be that this differentiation of relationships indicates something of the nature of any relationship between psychosocial hazards and physical health. That is, the influence of psychosocial hazards on physical health might be mediated by changes in emotions. In chapter 5, we revisit this idea.
However, these results do suggest that monitoring systems are likely to be more sensitive to changes in psychological health than physical health following psychosocial interventions. Given strong connexions between psychological health and individual differences, however, our results might suggest that monitoring systems, such as surveys, also include assessment of negative orientations.
Even if psychological health is more closely linked to psychosocial hazards, our results indicate that psychological health itself, and by extension the dynamic components of negative orientation, is quite stable. Our analysis did not include assessment of stability of trait negative orientation. It is likely that trait negative orientation is extremely stable in adults, and the trait components place limits on the extent to which negative orientation can change. However, Dormann and Zapf’s meta-analysis of job satisfaction (2001) does indicate that there can be large changes job satisfaction when the nature of work changes. In chapter 5, we consider the processes by which psychological health may change and the processes through which it remains stable.
It is worth commenting on the size of our final sample. Although we identified over 100 papers as potentially very relevant to our analysis, only 17 studies were sufficiently well reported to be included in the metaanalysis. However, our estimates are consonant with those from other meta-analytic review studies, and calculations indicate a large number of undetected studies with null findings would need to be conducted to falsify our results. Further, by concentrating on the best evidence that meets contemporary standards of rigour for longitudinal studies (cf. Zapf et al, 1996), our meta-analysis was able to afford much stronger conclusions with respect to causation than had we
49
reviewed evidence from the much larger number of studies using weaker designs.
Finally, it is worth noting that although our metaanalysis does indicate that psychosocial hazards and individual differences are both related to subsequent indices of health, the meta-analysis does not indicate how they might influence health. That is, on the basis of the statistical findings, we cannot be sure whether individual differences and psychosocial hazards influence health through two or more separate causal processes, or whether individual differences and psychosocial hazards combine to influence the causal processes underlying health. We turn to this question in chapter 5.
Nevertheless, having established the importance of negative orientation with respect to the experience and reporting of stress symptoms, in the next chapter we outline analyses to detect whether certain groups in the UK population are more likely to exhibit this orientation.
50

4. Secondary analysis of existing data- bases
The purpose of the secondary data analysis was to establish the extent to which negative orientation could be identified in certain groups in the UK population based on demographic and biographic characteristics.
4.1. Data-bases
A number of data-bases were reviewed and two offered a good range of variables in relation to the research questions and were available for use in this research.
The analyses were undertaken on these two data-bases - the Health Survey for England 2000 (HSfE) and the Health and Lifestyle Survey 1991/2 (HALS2). Sample descriptions are given here.
4.1.1. Health Survey for England 2000 (HSfE)
The Health Survey for England (HSfE) is part of a wider programme of surveys commissioned by the Department of Health, and is designed to monitor trends in the nation's health. The aims of the Health Survey series are to:
1) provide annual data about the nation's health;
2) estimate the proportion with specified health conditions;
3) estimate the prevalence of risk factors associated with these conditions;
4) examine differences between population subgroups;
5) assess the frequency with which combinations of risk factors occur;
6) monitor progress towards two Health of the Nation targets relating to blood pressure and obesity, and
7) since 1995, to measure the height of children (aged two and over) at different ages, replacing the National Study of Health and Growth.
The sample for the 2000 survey was Adults (aged 16 and over) and children (aged 2-15 Years) living in private households. There was also a separate sample of
51

older people (aged 65 and over) resident in care homes in England in the year 2000.
The 2000 HSfE consisted of two samples. The general population sample was a national cross-sectional sample. Up to two children aged 2-15 years were interviewed in each household, as well as up to 10 adults aged 16 and over. All private households in the general population sample were eligible for inclusion in the survey.
Over 5900 adults were suitable for the analyses reported here.
4.1.2. Health and Lifestyle Survey 1991/2 (HALS2)
HALS2 is a follow up to the 1984/5 Health and Lifestyle Survey. The sample is constructed of adults in Great Britain, aged 25 or over who were surveyed in 1984/5. The original participants were randomly surveyed and this is a follow up of survivors whether still living at the same address or not.
The sample is a longitudinal panel/cohort sample. Measurements included face-to-face interviews, selfcompletion questionnaires, and psychological and clinical measures.
Over 2600 adults, depending on the analyses, were suitable for the analyses reported here.
4.1.3. Procedure
The aim of the analysis was to provide evidence of relationships of state, attitudinal and trait negative individual differences to gender, age ethnicity, socioeconomic status and occupational grouping.
Both data sets were first examined for variables appropriate for the analysis. The data-bases contained self-report material on state, attitudinal and trait negative orientation as detailed in the table 4.1 below. As outlined in section 2.4.1., a trait individual difference is relatively impervious to change in adults, and traits are often taken as indicative of aspects of personality. Attitudes are more dynamic and are amenable to change, although any change is usually slow. State individual differences are very fluid and can change very quickly.
52

Table 4.1 Trait, state and attitudinal measures in the two data bases
DATA SET Self-Reports
HSfE GHQ-12
HALS2 Eysenck Personality Inventory – N scale
GHQ-12
Type A Behaviour
Of these, the Eysenck Personality Inventory N scale (EPI-N) is considered more a measure of trait negative orientation (neuroticism). Type A behaviour is here considered as attitudinal measures of negative orientation.12 Type A behaviour refers to a generalised pattern of hostility, competitiveness and impatience. Type A behaviour can change, although it is very stable.
More fluid, and hence more closely resembling state variables, is GHQ-12 score, which was designed as a measure of psychiatric morbidity. Nevertheless, like attitudinal measures, these will also reflect a large influence of trait negative orientation.
To recap, the purpose of the analysis was to look at whether self-reports of trait, attitudinal or state negative orientation were higher amongst certain subgroups of the population.13
12 HALS2 also included a measure of Locus of Control, which is also an attitudinal indicator of negative orientation. However, the scale used was specific to health, rather than work or a generalised attitude. More importantly, the scale was found to be unreliable, and therefore inaccurate (Cronbach’s a coefficient of reliability = 0.50). Therefore, we decided not to use Locus of Control in our assessments.
13 Differences between groups were examined with multi-factoral analyses of variance (ANOVAs). ANOVA examines whether there are statistically reliable differences between different groups. All demographic factors were entered simultaneously into each analysis, and the analyses were constrained to examine main effects only. In this way, the multi-factoral ANOVAs are analogous to multiple regression analyses, in which the unique effects for each demographic variable are assessed whilst controlling for the effects of all other demographic variables. Since we had made no predictions concerning the location of statistically reliable differences, post hoc tests were used to look for specific differences, if ANOVA had indicated significant variability across the different categories of a demographic factor. The specific post hoc test we used was the least significant difference (LSD) test. For both ANOVAs and LSD tests, statistical effects were
53

4.2. Analysis
4.2.1. Analyses from HSfE2000
Table 4.2. shows the means, standard deviations and ranges for each demographic variable from the HSfE for GHQ-12 scores.
Table 4.2. Descriptive statistics for GHQ-12 from HsfE2000
GHQ-12 Overall Mean 1.44 Std Dev 2.75 Range
Alpha Sample size
0-12 0.90 5955
Men Mean 1.18 Std Dev 2.49 Range Sample size
0-12 2739
Women Mean 1.66 Std Dev 2.94 Range Sample size
0-12 3216
judged to be reliable at the conventional probability level of p<.05 (two-tailed). For clarity of presentation, only statistically reliable effects are reported in the text.
54

Table 4.2. Continued
GHQ-12 Age 16-24 Mean Std Dev
1.49 2.63
Range Sample size
0-12 802
Age 25-34 Mean Std Dev
1.37 2.62
Range Sample size
0-12 1357
Age 35-44 Mean Std Dev
1.45 2.81
Range Sample size
0-12 1523
Age 45-54 Mean Std Dev
1.50 2.90
Range Sample size
0-12 1242
Age 55-64 Mean Std Dev
1.41 2.75
Range Sample size
0-12 1031
Ethnicity Mean 1.42 (White) Std Dev 2.75 Range 0-12 Sample size 5508
Ethnicity Mean 1.62 (African- Std Dev 2.70 Caribbean) Range 0-10 Sample size 105
Ethnicity Mean 1.70 (Asian) Std Dev 2.93 Range 0-12 Sample size 236
Ethnicity Mean 1.51 (Other) Std Dev 2.81 Range 0-12 Sample size 104
55

Table 4.2. Continued
GHQ-12 SES 114 Mean 1.11 (Professional) Std Dev 2.44 Range 0-12 Sample size 263
SES 2 Mean 1.32 (Managerial, Std Dev 2.53 technical) Range 0-12 Sample size 1660
SES 3 Mean 1.49 (Skilled non- Std Dev 2.83 manual) Range 012 Sample size 1485
SES 4 Mean 1.22 (Skilled Std Dev 2.60 manual) Range 0-12 Sample size 1031
SES 5 Mean 1.78 (Semi-skilled Std Dev 3.09 manual) Range 0-12 Sample size 930
SES 6 Mean 1.84 (Unskilled) Std Dev 3.04 Range 0-12 Sample size 287
14 SES is socio-economic status.
56

Table 4.2. Continued
GHQ-12 SOC115 Mean 1.16 (Managers, Std Dev 2.35 administrators)Range 0-12 Sample size 783
SOC2 Mean 1.38 (Professional) Std Dev 2.68 Range 0-12 Sample size 549
SOC3 Mean 1.34 (Associate Std Dev 2.48 professional, Range 0-12 technical) Sample size 561
SOC4 Mean 1.45 (Clerical, Std Dev 2.83 secretarial) Range 0-12 Sample size 1031
SOC5 Mean 1.31 (Craft) Std Dev 2.74 Range 0-12 Sample size 671
SOC6 Mean 1.57 (Personal & Std Dev 2.83 protective Range 0-12 service) Sample size 647
SOC7 Mean 1.64 (Sales) Std Dev 2.86
Range 0-12 Sample size 455
SOC8 Mean 1.59 (Plant & Std Dev 3.00 machine Range 0-12 operatives) Sample size 528
SOC9 Mean 1.66 (Other) Std Dev 3.00 Range 0-12 Sample size 495
15 SOC is occupational classification.
57

Analyses indicated that there were statistically reliable differences between men and women on GHQ-12 scores. There were also statistically reliable differences between socio-economic classes.
Women were found to have a more state negative orientation than men. Expressed as a percentage of the overall range of scores, there was an average difference between men and women than spanned 4% of the possible range of scores.
For socio-economic status, in general, GHQ-12 score increased amongst lower socio-economic groups, indicating state negative orientation increases amongst lower socio-economic groups. The highest scores were found amongst unskilled and semi-skilled workers compared to all other groups. Skilled non-manual workers reported higher GHQ-12 scores than skilled manual and professional groups. Expressed as a percentage of the total range of scores, the average difference between the highest and lowest scores spanned 6% of the possible range.
4.2.2. Analyses from HALS2
Table 4.3. shows the means, standard deviations and ranges for each demographic variable from the HALS2 for the EPI-N, Type A behaviour and GHQ-12 scores.
Table 4.3. Descriptive statistics for GHQ-12 from HALS2
EPI-N Type A GHQ-12 Overall Mean 9.49 0.51 1.76 Std Dev 5.34 0.20 2.68 Range
Alpha Sample size
0-24 0.86 2646
0-1 0.6586 2726
0-11 0.88 2712
Men Mean 8.26 0.53 1.63 Std Dev 5.05 0.20 2.57 Range Sample size
0-23 1218
0.04-1 1220
0-11 1226
Women Mean 10.48 0.50 1.88 Std Dev 5.36 0.19 2.76 Range Sample size
0-24 1515
0-1 1520
0-11 1523
58
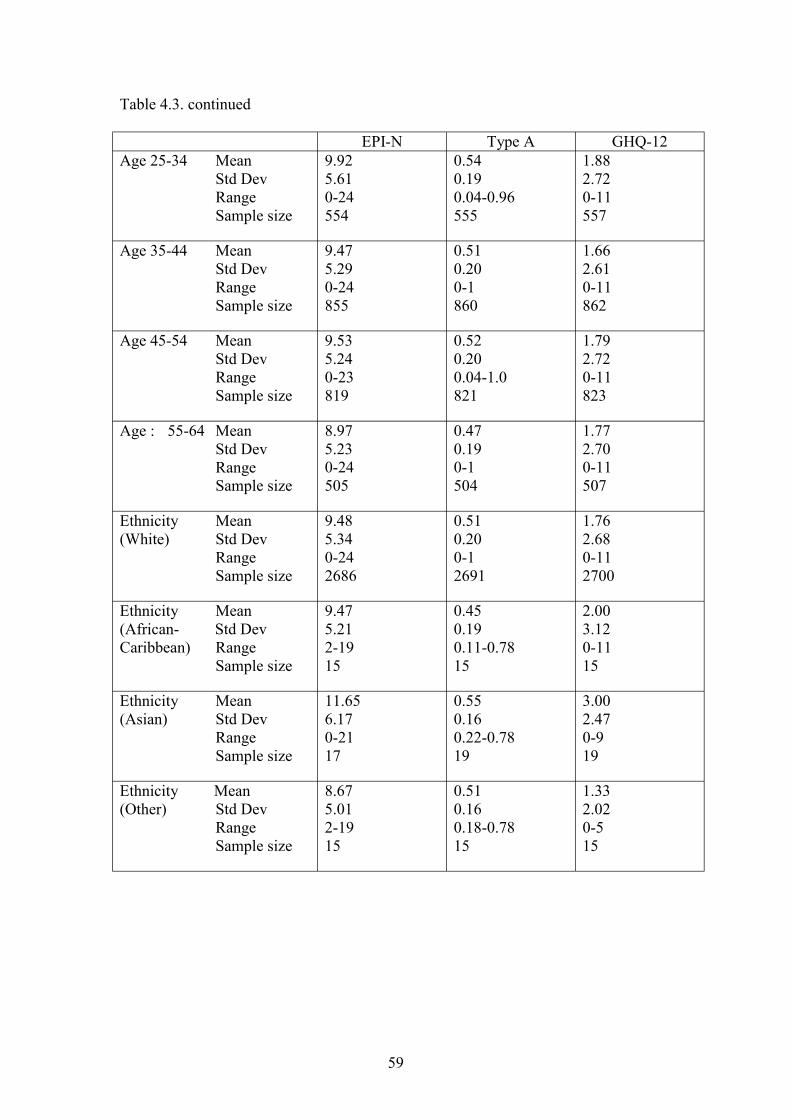
Table 4.3. continued
EPI-N Type A GHQ-12 Age 25-34 Mean Std Dev
9.92 5.61
0.54 0.19
1.88 2.72
Range Sample size
0-24 554
0.04-0.96 555
0-11 557
Age 35-44 Mean Std Dev
9.47 5.29
0.51 0.20
1.66 2.61
Range Sample size
0-24 855
0-1 860
0-11 862
Age 45-54 Mean Std Dev
9.53 5.24
0.52 0.20
1.79 2.72
Range Sample size
0-23 819
0.04-1.0 821
0-11 823
Age : 55-64 Mean Std Dev
8.97 5.23
0.47 0.19
1.77 2.70
Range Sample size
0-24 505
0-1 504
0-11 507
Ethnicity Mean 9.48 0.51 1.76 (White) Std Dev 5.34 0.20 2.68 Range 0-24 0-1 0-11 Sample size 2686 2691 2700
Ethnicity Mean 9.47 0.45 2.00 (African- Std Dev 5.21 0.19 3.12 Caribbean) Range 2-19 0.11-0.78 0-11 Sample size 15 15 15
Ethnicity Mean 11.65 0.55 3.00 (Asian) Std Dev 6.17 0.16 2.47 Range 0-21 0.22-0.78 0-9 Sample size 17 19 19
Ethnicity Mean 8.67 0.51 1.33 (Other) Std Dev 5.01 0.16 2.02 Range 2-19 0.18-0.78 0-5 Sample size 15 15 15
59

Table 4.3. continued
EPI-N Type A GHQ-12 SES 1 Mean 8.79 0.56 1.83 (Professional) Std Dev 5.23 0.18 2.71 Range 0-23 0.11-0.96 0-11 Sample size 196 196 196
SES 2 Mean 9.05 0.56 1.60 (Employers, Std Dev 5.09 0.19 2.61 managers) Range 0-23 0.04-1.00 0-11 Sample size 636 634 639
SES 3 Mean 9.44 0.53 1.81 (Other non- Std Dev 5.33 0.18 2.65 manual) Range 0-24 0.04-0.93 0-11 Sample size 524 524 526
SES 4 Mean 9.57 0.48 1.73 (Skilled Std Dev 5.35 0.19 2.64 manual) Range 0-23 0-1 0-11 Sample size 901 906 907
SES 5 Mean 10.00 0.45 2.02 (Semi-skilled, Std Dev 5.64 0.20 2.99 personal Range 0-23 0-0.93 0-11 services) Sample size 364 367 368
SES 6 Mean 10.84 0.46 1.76 (Unskilled) Std Dev 5.26 0.19 2.59 Range 0-23 0-0.89 0-10 Sample size 98 98 98
60

Table 4.3. continued
EPI-N Type A GHQ-12 SOC1 Mean 8.44 0.60 1.59 (Managers, Std Dev 4.92 0.18 2.49 administrators)Range 0-21 0-1 0-11 Sample size 306 304 306
SOC2 Mean 8.13 0.59 1.71 (Professional) Std Dev 5.14 0.17 2.59 Range 0-23 0.7-0.96 0-11 Sample size 243 242 243
SOC3 Mean 9.45 0.57 1.73 (Associate Std Dev 5.08 0.18 2.54 professional, Range 0-22 0.11-0.96 0-10 technical) Sample size 200 199 201
SOC4 Mean 9.39 0.48 1.65 (Clerical, Std Dev 5.05 0.18 2.65 secretarial) Range 0-23 0.04-0.93 0-11 Sample size 405 407 407
SOC5 Mean 8.59 0.52 1.54 (Craft) Std Dev 5.28 0.19 2.50 Range 0-21 0.04-1.00 0-11 Sample size 335 338 339
SOC6 Mean 10.20 0.51 1.73 (Personal & Std Dev 5.65 0.18 2.62 protective Range 0-23 0.04-1.00 0-11 service) Sample size 241 241 242
SOC7 Mean 10.18 0.50 1.83 (Sales) Std Dev 5.40 0.19 2.63
Range 0-24 0.04-0.89 0-11 Sample size 201 202 202
SOC8 Mean 9.71 0.47 1.85 (Plant & Std Dev 5.41 0.19 2.76 machine Range 0-23 0.07-0.96 0-11 operatives) Sample size 239 242 242
SOC9 Mean 10.24 0.45 1.59 (Other) Std Dev 5.31 0.21 2.46 Range 0-24 0-1.00 0-11 Sample size 291 292 293
61

Gender
Analyses indicated that there were statistically reliable differences between men and women on the EPI-N and GHQ-12 scores. In both cases, women were found to have a more negative orientation than men. That is, the results indicate that women have a greater state and trait negative orientation than men. These differences were more pronounced for trait negative orientation.
Expressed as a percentage of the overall range of scores, the average difference between men and women on the trait measure spanned nearly 10% of the possible range, compared to a 2% difference for the state measure on HALS2 and 4% on HSfE. It is possible that the observed differences between genders on state negative orientation, for both HALS2 and HSfE, reflect differences caused by trait negative orientation.
Type A results
There were also statistically reliable differences between age groups, socio-economic status and occupational groups on Type A scores.
Age
For age, the results indicate a general decline in Type A score for higher age groups, although there is not much change through middle age. Expressed as a percentage of the overall range of scores, the average difference between the youngest and oldest groups spanned 6% of the possible range.
There was a difference in scores between the 24-34 years age range and the 35-44 years age range. There was no difference between 35-44 years age range and 45-54 years are range, although the 45-54 year age range evidence higher scores than the 55-64 years age range.
The results indicate that the highest attitudinal negative orientation may occur amongst the youngest members of the work force, and the least negative attitudinal negative orientation amongst the oldest members of the work force. It is not clear whether this decline is a generalisable developmental effect or a peculiarity of the historical circumstances in the UK at the time of the survey.
62

Socio-economic status
For socio-economic status, the highest type A scores were found amongst the higher socio-economic groups. Expressed as a percentage of the overall range of scores, the average difference between the highest and lowest socio-economic groups was over 10% of the possible range of scores.
Professional and managerial groups scored higher than other non-manual groups. In turn, these three groups had higher scores than skilled, semi-skilled and unskilled manual groups.
Mirroring socio-economic class, the highest scores on the Type A scale were for managerial/administrative occupations and the professions. There were reliable differences too between associate professional and technical workers compared to clerical/secretarial workers, craft workers, personal and protective services workers, sales workers, plant and machine operatives and people in other occupations.
Of the remaining occupations, there were no reliable differences between craft workers, personal and protective services workers and sales workers, although craft workers scored significantly higher than clerical/secretarial workers.
Craft workers and personal and protective services workers also reported higher levels of type A behaviour than plant and machine operatives.
Other occupations reported significantly lower scores than all other groups, excepting plant and machine operatives. Expressed as a percentage of the overall range of scores, there was around a 15% average difference between the highest and lowest scoring groups over the possible range of scores on the Type A measure.
Ethnic groups
Although there were no statistically reliable differences between ethnic groups, the small numbers in the sample of non-White participants makes detecting reliable statistical differences more difficult than if there were larger numbers from different ethnic groups. Therefore, there may be differences between ethnic groups that we were unable to detect. However, there were larger sample sizes for different ethnic groups in HSfE, and no
63

reliable differences emerged between ethnic groups on GHQ-12 scores.
4.3. Summary and conclusions
The most consistent finding to emerge from the secondary analyses is that there is a greater likelihood of a more negative orientation in women than men. This finding emerged for GHQ-12 scores from the HSfE and the HALS2 data, and the EPI-N scores from the HALS2 data.
The strongest results occurred for the EPI-N scores, indicating differences in trait negative orientation between men and women. The weaker differences on the more state-like GHQ-12 that were found from data collected in the early 1990s (HALS2) and 2000 (HSfE) might reflect differences in underlying traits. This might suggest that differences in negative orientation between men and women reflect relatively immutable factors, that cannot be changed, if at all, within society over the shorter term.
The implications of this gender difference can be drawn out from the results of the meta-analysis. Since a negative orientation is associated with subsequent changes toward greater experience of psychological and physical problems, we might expect a slight tendency for there to be greater self-reports of psychological distress and self-reports of physical symptoms amongst women. In turn, this may lead to greater visits to physicians.
This tendency, which might be reflected in both selfreport and physician monitoring systems, may remain notwithstanding changes to work environments. However, any tendency is likely to be slight at best, given the relatively small differences between genders and the strength of the relationships found in the metaanalysis.
There did emerge some differences between age groups, with younger members of the adult population displaying more negative attitudes.
There was a decline in reports of negative orientation between younger groups and the middle-aged groups, and further differences emerged between the middleaged groups and the oldest groups in the adult population of working age.
64

Consequently, we might expect there to remain a tendency to experience and report more psychological and physical symptoms in younger age groups16, and a corresponding tendency to visit physicians. Again, this might manifest itself in monitoring systems based on self-reports or physician reports.
However, the age-related differences we found were attitudinal. Therefore, we might expect that such negative orientations are susceptible to slow change. Indeed, a developmental explanation of this relationship would imply change in orientation as individuals age.
Overall with respect to age, we can conclude that the tendency to experience symptoms, that are not causally attributable to the work environment, may be less evident over time as working environments change. However, any change in younger cohorts is likely to be subtle, lag far behind changes in environments, and so be observable as these groups mature. Again, any effects related to age are likely to be slight given the strength of the relationship found in the meta-analysis.
A mixed pattern of findings emerged with socioeconomic class and occupational groups. Attitudinal negative orientation was found to increase with socioeconomic status and found to be generally higher amongst professional, managerial and associate professional/technical workers and lowest amongst machine and plant operators and other workers in the HALS2 survey. In contrast, state negative orientation was found to be higher amongst lower socio-economic groups in the HSfE. There are a number of competing explanations for this finding.
One explanation centres on the time difference (8 years) between the two surveys. No differences amongst socio-economic groups were found for GHQ-12 scores in our analyses of the HALS2 survey. However, differences in GHQ-12 score emerged in the later HSfE. This might indicate that working and/or other conditions have deteriorated relative to other groups, or at least have been perceived to deteriorate, amongst lower socio-economic groups between the two surveys. Such changes are more likely to be manifest for GHQ12 scores, since they are more reactive to changes in conditions.
Although, in general, older groups might report more physical problems, since they are more likely to develop physical disorders over time.
65
16

However, this explanation gives no indication why there are differences in attitudinal negative orientation for socio-economic groups and occupational groups in the HALS2 survey. State, attitudinal and trait indicators of negative orientation are certainly highly correlated at an individual level (e.g. Wofford and Daly, 1997).
Differences between social groups might reflect socialisation of different expectations between these groups. Type A behaviour typically refers to ambition and competitiveness, amongst other things such as irritability and hostility. Ambition and competitiveness, especially in the workplace, may be attitudes that are valued by members of higher socio-economic groups and managerial, professional or associate professional occupations. Such values may be passed on in these groups, for example through career systems that reward behaviour driven by such values.
The hostility and irritability that accompany ambition and competitiveness in the Type A pattern may be reactions to expectations that exceed a person’s working and other social conditions. In support of this, the finding that Type A pattern is less prevalent amongst older people might reflect the eventual achievement of career and other life expectations (cf. Sturges, 1999).
Notwithstanding the interpretation of the pattern of results, the influence of negative orientation on reports of symptoms will dissipate more readily following improvements in job design amongst lower socioeconomic groups and less skilled workers. This is because GHQ-12 is more dynamic than Type A pattern. Once again, however, any changes are likely to be small, given the relatively small differences between socio-economic and occupational groups and the strength of the relationships found in the meta-analysis.
4.3.1. Conclusion
In conclusion, we did find differences across different demographic groups in state, attitudinal and trait negative orientation. Such differences may have implications for the accuracy of monitoring systems in different groups.
However, demographics are only weak indicators of negative orientations, and so it might be best to assess negative orientations directly in monitoring systems.
66

5. Discussion In chapter 3, on the basis of the meta-analysis, we concluded that:
a) Psychosocial hazards are associated more closely with subsequent increases in psychological symptoms;
b) A negative orientation is associated with subsequent increases in the cognitive experience of psychological and physical symptoms;
c) There is a good deal of stability in psychological health – and by implication - negative orientation (although changes in work conditions might attenuate this stability).
On the basis of these findings, we suggested that the reporting of physical symptoms might be inflated for those with a negative orientation where monitoring systems are based on self-report. We also suggested that monitoring systems are likely to be more sensitive to changes in psychological health rather than physical health, at least in the short term.
Finally, we suggested that emotions might mediate the relationships between psychosocial hazards and physical health, so that psychosocial hazards cause changes in psychological factors, which subsequently cause changes in physical factors.
We noted that the pattern of the findings do not indicate how individual differences and psychosocial hazards might cause changes in health and related variables. That is, the meta-analysis does not indicate whether psychosocial hazards and individual differences operate alone or in tandem. In reviewing explanations of the role of individual differences and psychosocial hazards, it is clear that theoretical accounts indicate that the causal paths linking work to the experience, expression and reporting of symptoms are influenced by both psychosocial hazards and individual differences. In the rest of this chapter, then, we examine theoretical models that attempt to explain:
a) how a negative orientation increases the cognitive experience of symptoms;
b) how psychosocial hazards influence emotions;
67

c) how emotions influence reporting of symptoms and psychosocial hazards;
d) the processes by which emotions change and also how they remain stable;
e) links between emotions, the experience of physical symptoms and the expression of physical symptoms to physicians;
f) how society, the person and the environment influence the development of emotions.
We place emotions17 at the centre of our analysis for three main reasons:
a) Many current and influential theoretical frameworks of the study of work-related stress accord a central role for emotions as the link between hazards and disease (e.g. Karasek and Theorell, 1990; Spector and Goh, 2001);
b) Emotional distress is central to the diagnosis of psychological disorders commonly linked to environmental stress (i.e. depression, anxiety, Lindsay and Powell, 1994);
c) It is well established that emotions influence cognitive processes (Rusting, 1998), and so emotions might influence the cognitive processes involved in the experience of psychosocial hazards and stress-related symptoms.
5.1. Paths from individual differences to occupational ill-health – theoretical overview
Spector, Zapf, Chen and Frese (2000a) have identified five ways in which a negative orientation could influence the experience and reporting emotional health at work. These are:
a) differential perception of psychosocial hazards – that is people with a negative orientation are more likely to notice psychosocial hazards, and so are more likely to report them;
Recall that ‘emotion’ refers to feelings towards an event, situation, object or person and ‘mood’ refers to feelings that can not necessarily be linked to a specific event, situation, object or person. ‘Affect’ is a term that subsumes both emotion and mood.
68
17

b) perceptual influences of mood – that is people with a negative orientation are more likely to experience negative emotions, and these negative emotions then influence the perception and impact of hazards on health;
c) greater incidence of psychosocial hazards – that is people with a negative orientation are more likely to behave in ways that encourage negative events to occur, such as getting into interpersonal conflict;
d) interaction with psychosocial hazards - that is people with a negative orientation are more reactive to psychosocial hazards, and so are more likely to experience distress when confronted with a psychosocial hazard.
e) drift into psychologically hazardous jobs – that is people with a negative orientation do not present themselves in the best possible light during selection interviews and related selection processes, and so such people are less likely to get desirable jobs and drift into jobs with more psychosocial hazards.
These five paths identified by Spector et al indicate that theoretical models need to explain; i) how psychosocial hazards influence emotions (to explain c) partly and e)); how individual differences and mood influence how we interpret emotional information (to explain a), b) and d)), and how individual differences influence the occurrence of psychosocial hazards (to explain c)).
In the following sections, we review four theoretical models of how psychosocial hazards influence emotions, namely affective events theory (AET), appraisal theory, action-control theory and a cognitive model. The last of these models illuminates each of the five paths outlined by Spector et al.
5.1.1. Affective Events Theory
Affective Events Theory (Weiss and Cropanzano, 1996) indicates:
a) work-related attitudes and behaviours are influenced by work-related emotions;
b) work events cause work-related emotions;
c) work events are caused by more stable on-going work conditions.
69
In other words, work environments and characteristics of those environments influence emotions through specific events. In a sense, this echoes suggestions made by Rick et al (2001) that assessment of psychosocial hazards should concentrate on measuring the frequency of occurrence of psychosocial hazards rather than assessing hazards using scales that indicate agreement or disagreement with a phrase describing an individual’s job.18
AET also indicates that it is not the event per se that causes affective reactions, but a person’s interpretation of that event. Indeed, the interpretation an individual gives to an event has been shown to be important in explaining stress-related reactions to that event (Dewe, 1989). AET also recognises that a negative orientation can influence that interpretation.
5.1.2. Lazarus, appraisal and coping
Appraisal based theories have considered in detail the processes by which people come to interpret events as stressful. The most influential appraisal theory, especially in relation to occupational stress (Cooper et al, 2001), is Lazarus’ theory (e.g. 1999).
Lazarus’ appraisal theory indicates that people interpret events according to whether they have an impact on a person’s ability to pursue his or her goals. According to Lazarus (1991, 1999), there are two major elements of appraisal.
a) Events are first subject to primary appraisal that determines an initial emotional reaction. During primary appraisal, an individual determines whether an event is relevant for personal goals or whether the event will enable or block pursuit of goals. These goals can come in many forms, such as performance targets. However, Lazarus suggests that we also have higher-order goals, such as establishing self-esteem, maintaining moral values and pursuing life or career goals. Events that block these more important goals,
That is, Rick et al suggest psychosocial hazard scales should ask how often something occurs (preferably in a defined time period) and ask individuals to respond on a scale that, for example, gives response options of ‘Never’, ‘Once or twice’, ‘Several times’, ‘Most of the time’ ‘All of the time’. Many current scales ask respondents to indicate their agreement with statements with response options such as ‘Strongly agree’, ‘Agree’, ‘Neither agree nor disagree’, ‘Disagree’, ‘Strongly disagree’.
70
18

or an individual’s plans to achieve them are, perhaps, more likely to arouse more intense emotional reactions.
b) Second, events are subject to secondary appraisal to determine coping. Coping can be thought of as attempts to adapt to or regulate the emotional impact of an event. It can include, for example, attempts to re-establish progress toward goals that have been disrupted, attempts to control or vent emotions, attempts to re-interpret the impact of the event on goals or attempts simply to avoid thinking about the event and its implications. If coping is successful, then emotional well-being is restored. Indeed, earlier versions of Lazarus’ appraisal theory also included a component of tertiary appraisal in the model - the evaluation of coping success (Lazarus and Folkman, 1984). However, the role of tertiary appraisal has been played down in later versions (Lazarus, 1991, 1999).
The content of these two major elements of appraisal combine to form ‘core-relational themes’ that determine the specific emotion felt. For example, the emotion of anxiety is characterised in Lazarus’ theory as related to the core-relational theme of threat.
The notion of goal-related appraisal is intuitively appealing, since it can account for individual differences as different people have different goals (not all of which accord with the formal objectives of their work). The notions of goals and coping also indicate that people are active in the work-related stress process, and attempt more or less successfully to pursue personal goals and regulate the impact of events on those goals.
Appraisal theory also indicates that paying attention to how people pursue goals (and how these can be made consonant with organisational objectives) might be an effective way of promoting well-being in the workplace.
5.1.3. Action-control theory and goals
Lazarus’ appraisal theory points to the importance of goals. Action-control theories have considered in greater detail the cognitive processes involved in relating goal progress to emotions. Action-control theories have also considered the cognitive processes involved in coping.
Carver and Scheier’s control theory (1990) proposes that it is not merely disruption to goals that causes
71

unpleasant emotions, since if we expect to be disrupted it does not influence our emotions. Rather, Carver and Scheier propose that negative emotions occur when the rate of progress toward a goal is slower than desired. Conversely, positive emotions are proposed to occur where the rate of progress is faster than desired.
This has important practical implications for managing work-related stress – since procedures have to be in place to allow individuals to pursue their goals at the rate that they desire, or organisations could aid individuals’ understanding of how fast they can expect to achieve their goals so that individuals can set their expectations accordingly.
Carver and Scheier, like Lazarus, consider goals to be arranged hierarchically, with subordinate goals representing stages in plans to achieve higher-order goals. For example, the higher-order goal of ‘SPEND MORE TIME WITH FAMILY’ might be achieved through lower-order goals such as ‘LEAVE WORK AT 5pm’ or ‘DON’T TAKE WORK HOME’. The importance of these lower-order goals is they include plans that detail behaviours to achieve a higher-order goal (Frese and Zapf, 1994).
In this sense, action-control theories link notions of cognition (e.g. how we interpret an event with respect to goal progress) with behaviour (e.g. what do we do about events that disrupt goal progress). Therefore, it is logical that people should formulate plans concerning how to prevent psychosocial hazards occurring in the first place and plans to enact coping behaviours if hazards do occur.
The practical implication of this is that if there is sufficient latitude available in the workplace to enact these plans, then there exists the possibility of individuals being able to regulate their own emotions.
In many theories of job design, the latitude to enact plans for stress-regulation is embedded in the ability to exercise discretion over work tasks, participation in decision making and availability of social support from managers and co-workers (cf. Karasek and Theorell, 1990).
However, the central place of goal-related appraisal as a cause of emotions has been criticised, in that emotional reactions to events can occur too quickly for detailed interpretation of an event’s impact on an individual’s goals
72
(Zajonc, 1980). To address this issue, Power and Dalgleish (1997) argued that emotions can occur in two ways:
a) Through interpretation of an event’s implications for goal progress, which is likely to involve detailed conscious deliberation;
b) Through learning the kinds of events that are likely to cause disruption to goal progress.
By learning that some events have disrupted progress to goals in the past, people can then infer that events of the same kind are likely to influence goal progress in the future. This learning, then, provides a cognitive short-cut through which people can infer more quickly that an event has implications for goal disruption. This inference is made on the basis of a few, key defining features of an event to enable faster processing of information.
However, whilst this learning affords a faster interpretation, and therefore faster mobilisation of coping, the process is largely unconscious, very inflexible and can involve misinterpretations of an event’s implications for goal progress. In this way, emotional responses can seem irrational.
As an example, one of the research team met a woman who became very upset when her line manager raised his voice. Although this had no implications for her work or personal goals, and the line manager didn’t raise his voice in an aggressive manner directed toward her, the woman nevertheless became upset and would often cry too.
A closer examination revealed that the woman’s father had often shouted at her when she was a child. The line manager raising his voice reminded her of this and so she associated older men raising their voices with her father being angry with her. In this way, the emotion elicited by her line manager shouting was done so automatically and with no relevance to the current work context.
For Power and Dalgleish, it is beliefs about events that influence our interpretation. If we believe an event has implications for our goals, then it is more likely to cause an emotional reaction. Power and Dalgleish suggest that we have networks of related beliefs, stored in memory as mental models (our own ‘lay’ theories of how the world works – see section 2.3), and it is these networks that influence how we respond emotionally and behaviourally to distressing events.
73

5.1.4. CAPHEM model
Building on the notion of there being two paths to generating emotion and that beliefs influence appraisal, Daniels and colleagues have been developing a cognitive model of how workplace psychosocial hazards influence emotions, and how the work environment and people’s beliefs interact to influence coping behaviour (Daniels, 2001; Daniels, Harris and Briner, 2002a; 2002b; 2002c; in press).
Daniels and colleagues have labeled their model CAPHEM,19 which stands for
CAtegorisation of
Psychosocial
Hazards and
EMotions
There are five major elements of the CAPHEM model.
1) Categorisation. Before an event can influence emotions, it needs to be noticed and then categorised as emotionally relevant. Categorisation can occur in two ways:
· First, an event can be categorised as relevant for current goals. This starts the slow process of goalrelated appraisal described by Power and Dalgleish (see element 2 below).
· Second, an event can be categorised a similar to events that have disrupted goals in the past. Here, categorisation is made on the basis of a few defining features of an event that are similar to or the same as events encountered in the past that have disrupted goal progress. This type of process starts the fast process of appraisal described by Power and Dalgleish (see element 3 below).
2) Goal-related inferences. Categorisation of an event can cue the recall of beliefs about that event. It is the interaction between what is perceived in the environment and beliefs about events of the same nature that influence how an event is appraised as influencing progress toward a person’s goals.
19 The bibliography for the CAPHEM model is shown in Appendix B.
74

For example, consider someone with the goal of writing a report for a deadline. If a colleague is being uncooperative, then this might be classified as ‘UNSUPPORTIVE COLLEAGUES’. In turn, this classification evokes the belief that ‘UNCOOPERATIVE COLLEAGUES DELAY TASKS’. In turn, the person might then conclude that lack of cooperation disrupts that person’s ability to submit the report on time and a negative emotional reaction, such as anger, anxiety or sadness results.20
Daniels et al argue that, the more important a goal, the stronger the emotional reaction produced by impediments to the desired rate of goal progress.
3) Emotional associations. Categorisation of an event through consideration of previous events of the same kind can proceed at the same time as element 2 or independently of element 2.
As categorisation is fast and made on the basis of only a few key features of the event, then minimal attention is paid to the environment, which increases the chances of a seemingly irrational emotional reaction. If we return to the example of the woman and her line manager, here the woman will have noticed the defining features of OLDER MAN and RAISED VOICE. For this woman, the combination of these features means the event is similar to that category of events where FATHER IS ANGRY WITH ME, which in turn elicits the emotional reaction the woman experienced as a child.
4) Coping. Once an event has been categorised and an initial emotional reaction has occurred, a set of plans is recalled concerning the best way of coping with an event of the same nature.
Where goal-related inferences are made and more attention is being paid to the environment, the plans are evaluated against their suitability for the specific nature of the current event and modified accordingly.
Where the faster unconscious processes cause emotion and little attention is paid to the environment, then the person tries to implement plans that might have been successful in the past but might not be suitable for the
There is differentiation between emotions in the CAPHEM model. Anger is thought to result from obstacles to goal progress; anxiety from threats to goal progress; sadness from failure of goals or the loss of the means to achieve goals; and boredom from events that have no implications for personal goals.
75
20

current situation. In this way, unconscious processes can increase the chances of ineffective coping.
Like other approaches (e.g. Karasek and Theorell, 1990), control over work tasks and support from others are thought to enable the implementation of coping plans, and so promote effective coping and well-being.
5) Feedback. There is considerable evidence that emotions influence cognition and the social processes of coping. Specifically, if coping is ineffective and a negative emotional reaction persists, this directs attention to more negative features of the environment and so increases the chances of noticing other psychosocial hazards. Also, if a negative emotion persists, there is an increased chance of having control and support withdrawn, as others perceive the person to be less competent, less capable of executing effective control and less likely to reciprocate supportive behaviours
Figure 5.1. illustrates the major elements of the CAPHEM model.
76
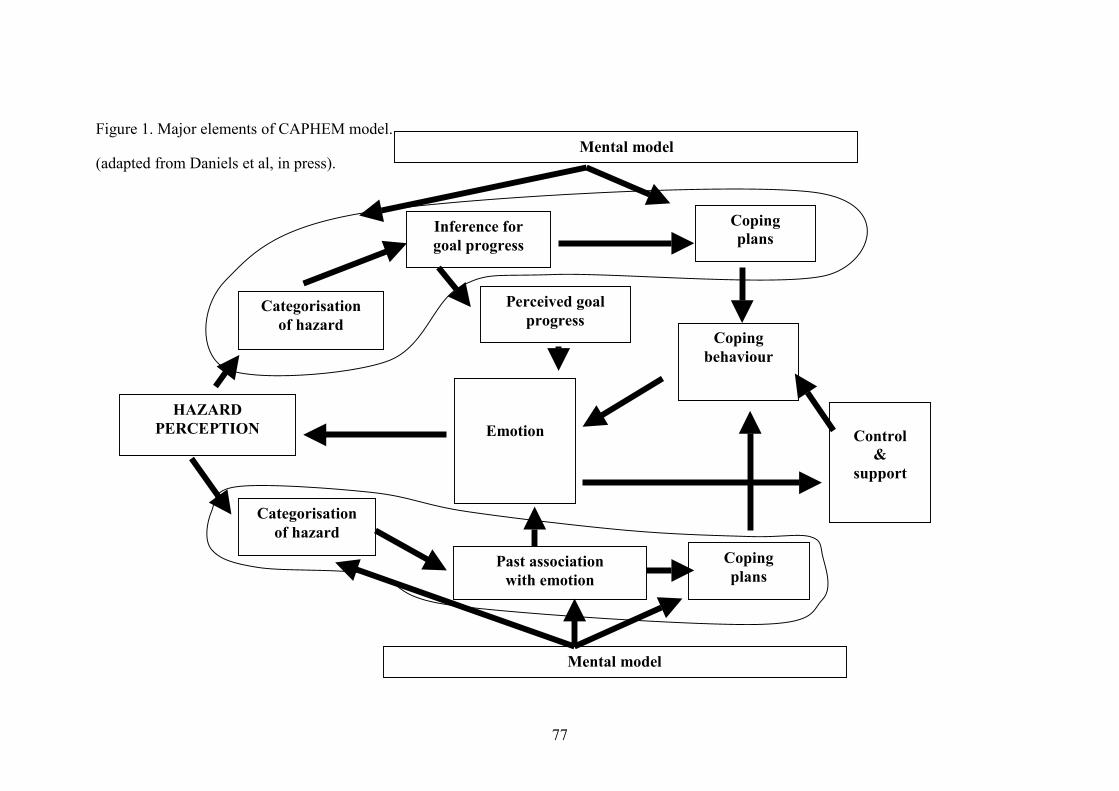
Figure 1. Major elements of CAPHEM model. Mental model
HAZARD
progress Categorisation
goal progress plans
Categorisation
plans
&
behaviour
(adapted from Daniels et al, in press).
PERCEPTION
Perceived goal of hazard
Inference for Coping
of hazard
Past association with emotion
Coping
Control
support
Emotion
Coping
Mental model
77

The CAPHEM model relates to the five paths identified by Spector et al in the following ways:
a) differential perception of psychosocial hazards: People with a negative orientation are likely to have more mental models of psychosocial hazards (Williams et al, 1997), meaning that such people are more likely to categorise events as aversive;
b) perceptual influences of mood: Because people with a negative orientation are more likely to categorise events as hazards, they are more likely to experience negative emotions. In turn then, they are more likely to notice negative aspects of the environment, leading them to categorise events as hazardous, leading to more negative emotions and so on;
c) greater incidence of psychosocial hazards: since a negative orientation is more likely to cause negative emotions, it is more likely that those with a negative orientation will receive less support and control in the work place. In turn, this makes these people less able to cope with hazards, meaning that hazards can persist for longer;
d) interaction between affectivity and psychosocial hazards: People with a negative orientation have more elaborate mental models of psychosocial hazards that indicate those hazards are somehow harmful or disruptive to personal goals. Therefore, when a hazard is noticed, people with a high negative orientation are more likely to infer that the hazard might disrupt goals or has been associated with negative emotions in the past;
e) drift into psychologically hazardous jobs: The CAPHEM model does not give an account of how people with a negative orientation might come to work in more psychologically hazardous jobs. It does, however, indicate that people who display negative emotions might be perceived as less competent – which could influence selection or promotion decisions for more desirable jobs, or redundancy decisions. The CAPHEM model does explain how hazards in less desirable jobs are linked to emotions.
The CAPHEM model also has implications for reporting of psychosocial hazards from questionnaires and for how emotions change or stay the same. These implications will be drawn out in subsequent sections. However, the CAPHEM model does not deal with the
78

expression of symptoms or the physiology of emotions – which is thought to influence physical health. Other research and models will be used to explain these processes.
5.2. Individual differences & self-report measures: correlation inflation
If individuals with a negative orientation are more prone to notice psychosocial hazards, then they could be more likely to report them. Individuals with a negative orientation are also more likely to experience and report psychological and physical symptoms.
Therefore, associations between psychosocial hazards and symptoms are likely to be inflated for people with a negative orientation – giving the impression of a false relationship between the work environment and health (but not perhaps necessarily a false impression of the relationship between perceptions of work and experience of symptoms which, as argued above, is key for the development of emotions).
Many studies have examined the influence of negative orientation on correlations between self-reports of work conditions and symptoms. In particular, much attention has been directed toward the concept of negative affectivity – or the predisposition to experience negative emotional states. It is clear from this stream of research that negative orientation does indeed inflate reports of psychosocial hazards and symptoms. Specifically, much research in this area has found that partial correlations controlling for negative orientation can be substantially lower than simple correlations between hazards and symptoms (e.g. Brief, Burke, George, Robinson and Webster, 1988).
The meta-analysis demonstrated, however, that even after controlling for negative orientation, we found that psychosocial hazards still had a significant association with changes in subsequent health status.
5.2.1. Occasion factors
Most studies of negative affectivity have been crosssectional. However, Zapf et al (1996) have noted that mood might also influence perceptions of the work environment in the same way as negative affectivity, which is also consistent with the CAPHEM model. Since mood is more variable than negative affectivity, Zapf et al argue that ‘occasion factors’ might influence
79

reports of hazards and symptoms, inflating observed associations for people in a negative emotional state at the time of measurement.
Spector, Chen and O’Connell (2000b) went someway toward testing whether occasion factors might influence associations between self-reports of hazards and symptoms. In their study, they found that associations between hazards and symptoms were usually similar in size to partial correlations controlling for negative affectivity measured some months before self-reports of hazards and symptoms.
However, there emerged significant reductions in the size of correlations between hazards and symptoms when partial correlations controlled for negative affectivity measured at the same time as hazards and symptoms. These results do suggest that occasion factors might influence self-reports of hazards and symptoms inflating observed associations between hazards and symptoms measured at the same time. Such findings underline the importance of longitudinal research for drawing inferences about whether psychosocial hazards cause symptoms.
5.2.2. How mood and disposition interact to determine how we notice psychosocial hazards
It is reasonable to suppose that occasion factors and negative affectivity interact to influence correlations amongst self-report measures (cf. Rusting, 1998). If people with a negative orientation are more likely to have more elaborate mental models of psychosocial hazards, and a negative mood directs cognitive processes to negative information, it is reasonable to suppose that a negative mood increases the chances of interpreting events as hazards disproportionately for people with a negative orientation. That is, the greatest inflation of associations between self-reports of hazards and symptoms occurs when people with a negative orientation are in a negative emotional state.
Although experimental research has indirectly assessed this proposition (see Williams et al, 1997 for a review), we know of no studies that have addressed this proposition directly in occupational samples.
5.3. Change & stability in psychological distress
Although there is stability in negative orientation and psychological health, as Spector et al (2000b) indicate,
80

even trait measures of negative orientation may be subject to some change. Therefore, it is important to consider how negative emotions in themselves, and as indicators of negative orientation, are sustained and how they change in work environments.
5.3.1. Change & stability explained in the CAPHEM model
In the CAPHEM model, emotional change can occur in several ways.
First, hazards can cause emotions through two primary processes that can be simultaneous, involving inferences concerning events’ implications for goals or learnt associations between events and past disruption of goals. The faster process might cause one emotional reaction, which is subsequently modified by the slower process. For example, you may be initially angry by being asked to work on a project with a colleague who has caused problems for you in the past. However, you may become pleased when you realise that this is an opportunity to demonstrate your managerial competence (and promotability) by getting the best out of this colleague.
Second, at least when making inferences about goal progress, a fair amount of information from the environment is used to generate inferences and decide on coping options. Therefore, as an event proceeds and the nature of the hazard changes, inferences about goals too may change. This can then produce changes in emotions.
Third, coping processes can alter emotions directly or indirectly though changing the interpretations of hazards or removing those hazards from the environment.
Fourth, psychosocial hazards can occur concurrently or sequentially and emotions influence cognitive processes. In this instance, an emotional reaction generated by one hazard might influence processing of information on another hazard.
It is the influence of emotions on cognitive processes that can explain stability in the experience of unpleasant emotions. Here, negative orientation might play a role in the maintenance of negative emotions by activating well-learnt mental models (Williams et al, 1997, cf. section 5.2.2.). Negative emotions are maintained by
81

directing information processing toward categorising events as psychosocial hazards, which then cause further negative emotions.
5.3.2. Small effects sizes and large changes: vicious and virtuous circles
Although there is a great deal of stability in psychological ill-health and negative orientation, research does indicate that psychological health can change and more negative orientations become more positive (Firth-Cozens, 1992; Firth-Cozens and Hardy, 1992).
It has been proposed that such changes follow the model of ‘vicious’ and ‘virtuous’ circles (Daniels and Guppy, 1997; Firth-Cozens, 1992), with small scale improvements in well-being leading to cognitive processes being directed to positive information, in turn leading to less attention being paid to psychosocial hazards and establishment of new mental models that replace or mutate older, more negative mental models. These new mental models allow more positive interpretations to be made, and so a negative orientation gradually becomes more positive, reinforcing further improvements in psychological health. Of course, the reverse process might occur, with worsening psychological health leading to establishment of more negative mental models, in turn reinforcing further deterioration of psychological health.
These processes are thought to be incremental and to build over a period of time. The findings from two daily diary studies reported by Harris (2002) indicate well-being before work could predict changes in mental models of work conditions over the course of a single day, although no conclusions on factors that might sustain these changes was presented. Another study two-stage longitudinal study did indicate well-being could predict subsequent improvements in some perceptions of work and a lessening of attitudes closely related to a negative orientation (Daniels and Guppy, 1997).
However, studies over periods of several months are conflicting, with one study indicating well-being can predict improvements in perceived work conditions (Wolpin, Burke and Greenglass, 1991) and another indicating no relationship between well-being and subsequent changes in perceived work conditions (de
82

Jonge, Dormann, Janssen, Dollard, Landeweerd and Nijhuis, 2001).
The factors that sustain or inhibit changes in perceptions of work environments are not widely understood. It may be that sustained changes of periods of several months are very subtle, and require measurements specific to occupations or organisations, or precise measures of appraisals or mental models, rather than more generalised measures, so that changes in perceptions of very specific work conditions can be detected (cf. Daniels & Guppy, 1997 or Harris, 2002, with de Jonge et al 2001). Moreover, some perceptions, such as those linked to personal goals, might be more readily influenced by changes in the work environment, whilst others are more closely linked to personality and/or organisational culture and therefore less amenable to change (Harris, 2002). Nevertheless, one practical implication of these suggestions is that any interventions might take some time to be noticed, perhaps as long as five years or more (Dormann and Zapf, 2001) since larger scale changes may need to build over time. Even then, a range of other factors that are not currently fully understood might need to be taken into consideration in order to determine the probability of successful intervention.
5.4. Individual differences and the experience of physical symptoms
We have suggested that emotions play a central role in the experience and reporting of physical symptoms as well as psychological symptoms. There is also some discussion of how psychosocial hazards might influence emotions, which in turn influence physiology and physical health (Schwartz, Pickering and Landsbergis, 1996).
5.4.1. The role of negative orientation in the perception of symptoms
Kirmayer, Robbins and Paris (1994) have identified five paths through which personality might influence the cognitive experience of physical symptoms, either without the presence of physical symptoms or accentuating such symptoms as are present. These are:
1) Somatic perceptions – in which some individuals are more simply more likely to notice physiological symptoms;
83

2) Somatic attention – in which some individuals are more likely to pay attention to bodily sensations, and therefore become more likely to notice symptoms that would not be noticed by others;
3) Somatic amplification – symptoms that are noticed are blown out of proportion to be experienced as worse than they really are (e.g. a tendency to experience ‘bad’ headaches).
4) Difficulty distinguishing bodily sensations from cognitive sensations – which occurs when individuals misinterpret the cognitive experience of, say, anxiety and associated physiological changes as illness;
5) Tendency to catastrophise – which occurs when common physiological symptoms are interpreted as indicating a more serious disease (e.g. indigestion interpreted as angina).
Research indicates a negative orientation is associated with paths 2), 4) and 5) (Kirmayer et al, 1994), although it is possible, of course, that a negative orientation might influence all five paths.
That negative orientation might influence the fifth path indicates that people with a negative orientation might be more inclined to visit physicians, as they interpret their symptoms as indicating serious conditions. Even so, it is clear that there is theoretical discussion to support our earlier conclusions that monitoring systems that rely on self-reports of stress-related physical symptoms might over-estimate their prevalence amongst people with a high negative orientation.
5.4.2. The role of negative orientation in the presentation and diagnosis of symptoms
If a negative orientation leads to more visits to the physician, it is also possible that physicians respond to people with a negative orientation in a way different from those with a positive orientation.
Although we were unable to find any studies on this issue amongst occupational samples, we did find one simulation study (Ellington and Wiebe, 1999) in which students were asked to role-play the symptoms of two diseases – a minor throat infection and acute appendicitis. Ellington and Wiebe’s results indicate that
84

those with a high negative orientation (specifically neuroticism) are more likely to:
1) present information on their symptoms in a more elaborate, detailed and intense manner to physicians;
2) present information on recent stressors they had experienced for the more serious disease to physicians;
3) display visible signs of anger during the consultation.
Ellington and Wiebe’s results also indicate that, during consultation, physicians perceive that people with a high negative orientation:
4) overact in the expression of their symptoms;
5) have an ulterior motive for the expression of their symptoms;
6) are less likely to have a severe illness when expressing the symptoms of a severe illness, such as acute appendicitis;
7) have psychological causes as the primary explanation of their illness, rather than physical factors.
Ellington and Wiebe’s results also indicate that, even when people present with physical symptoms, physicians are more likely to:
8) schedule follow-up appointments with people with a high negative orientation;
9) refer people with a high negative orientation to mental health professionals;
10) prescribe psychiatric medication to people with a high negative orientation.
Findings 7), 8), 9) and 10) indicate that monitoring systems that rely on physicians’ reports could overestimate the prevalence of psychological problems amongst people with a high negative orientation, and consequently diagnose conditions as being caused by work-related stress, rather than as physical diseases with no occupational cause. This conclusion should be taken with extreme caution, however. Ellington and Wiebe
85

have presented only one study, which was a simulation conducted with students with relatively inexperienced physicians (all aged under 32). It is clear that more research using occupational samples and more experienced physicians is needed before any firm conclusions can be drawn.
5.4.3. Negative orientation and health – is there a really a link?
A negative orientation might also be related to physical disease, as well as cause heightened experience of symptoms. Friedman and Booth-Kewley (1987) have outlined three ways in which this might be so:
1) Unhealthy habits: in that people with a negative orientation might be prone, for example, to eat unhealthy foods, smoke and drink more and exercise less.
2) Biological third variables: in which a negative orientation is associated with an underlying physiological susceptibility to disease. This would make it look like a negative orientation is causing a disease, although the real cause is an undetected susceptibility (see also Kirmayer et al, 1994);
3) Negative orientation as a cause of emotions: in which the physiological changes associated with negative emotions cause disease.
Those working in the field of physical illness and workrelated stress prefer an amended version of the third process. In this tripartite model (Schwartz et al, 1996), psychosocial hazards and individual differences combine to produce an emotional response (see our earlier description of the CAPHEM model for how this might occur), which in turn might influence the course of a specific disease, if the person has a physiological susceptibility to develop that disease (Schwartz et al, 1996). This susceptibility need not be genetic, but can be transient (e.g. salt in diet) or a combination of both (e.g. cholesterol levels).
There is a problem with this simple model. The cognitive and physiological components of emotion are linked, but only loosely so (Lang, 1984). Therefore, it is possible to feel anxious without showing the physiological indicators of anxiety, and it is possible to show the physiological indicators of anxiety without feeling anxious. Therefore, for the tripartite model to
86

work, the cognitive experience of negative emotions must be translated into the physiological experience.
Schwartz et al also indicate that prolonged effortful and active coping attempts might also influence disease. Where coping resources, such as control or support are in short supply, such coping might place additional demands on the body, so also leading to development of disease.
5.5. Individual differences and socio-cultural factors
It is clear from our review of different theories that both individual differences in how we process information about the environment and events that occur in that environment alter how we experience, report and express psychological and physical symptoms. Indeed, it is a combination of both individual and work characteristics that influences emotions, and emotions’ subsequent influence on health and perceptions of health.
However, it is also clear from our review that although a negative orientation is relatively stable, it can change if the work environment changes. Indeed, wider social and economic shifts (such as rising divorce rates, crime and job insecurity) indicate that as whole we might be becoming a more anxious, and hence negatively orientated, society (Twenge, 2000).
Our theoretical review suggests that it is beliefs about psychosocial hazards that, conjointly with the occurrence of psychosocial hazards, influence emotional reactions, and that changes in these beliefs might gradually change a negative orientation to a more positive orientation, or vice versa. Evidence suggests that beliefs about psychosocial hazards are influenced by three factors (Daniels et al, 2002c; Ettner and Grzywacz, 2001; Harris, 2002):
i) The person: Here, beliefs about psychosocial hazards are influenced by patterns of thinking and behaviour learnt throughout our development, as well as genetic susceptibility to think in a certain way. Indeed some researchers have indicated that around a third of the variation in job satisfaction is attributable to differences in genetic make-up (Arvey, Bouchard, Segal and Abraham, 1989). Certainly, if beliefs about hazards are influenced by patterns of thinking learnt early on in life, they will be automatic and
87
consequently very difficult to change (Power and Dalgleish, 1997).
ii) The environment: Here, the nature of psychosocial hazards experienced influence how we interpret them. For example, if we learn that some work events do prevent attainment of goals, then it is natural – not irrational – to infer that future events of the same nature will influence attainment of goals. If the environment changes so that goals can be achieved, then it is likely that beliefs about those events will change too.
The distinction between ‘hard’ and ‘soft’ environments is usefully applied to environmental influences (Frese and Zapf, 1994). A hard environment is one which many people would interpret the same way. For example, most people would recognise that redundancy announcements threaten economic and career goals, and so would cause some level of anxiety to many people. A soft environment is one that is open to more individual interpretation, where the relationship to individual goals is more idiosyncratic – such as many social situations.
Changing the nature of ‘hard’ environments is most likely to result in changes in beliefs about the work environment. However, this does not mean nothing can be done for ‘soft’ environments.
Where beliefs are shared amongst workers about a soft environment, then changing the environment too might prove an effective intervention. Indeed there is evidence that beliefs about psychosocial hazards do come to be shared, as we discuss next.
iii) Socio-cultural factors: These relate to how we learn beliefs and develop our personality orientations through interaction with our wider environment. The influence of the environment can operate on several levels. The most immediate level is that of the work group and organisation. Indeed, others in the same work group might even be able to influence our own beliefs on a daily basis (Harris, 2002). Wider levels include those that influence how society and how groups within society operate. Indeed, our secondary analysis shows differences are evident in negative orientation between demographic groups. Values, transmitted through widespread child rearing practices, the education system, the mass media, trades
88

unions and professional associations all influence the way we think about work and consequently how we respond to work (e.g. Nyambegera, Daniels and Sparrow, 2001). Such factors might influence how psychosocial hazards are appraised in a given society, perhaps making members of some societies or subgroups of society more likely to show a negative emotional response some hazards rather than others.
From this review of influences on beliefs about psychosocial hazards, it is clear that there are two main ways of changing beliefs, which are complementary:
a) Change the work environment, so that people develop new beliefs about it;
b) Change the way information about psychosocial hazards is transmitted – at the level of the work group, the organisation and within wider groups in society.
In the next chapter, we will discuss in greater detail the practical and research implications of our meta-analysis and this theoretical commentary.
89

6. Conclusion The major conclusions from this research are:
1) Psychosocial hazards are related to subsequent reports of health (r=0.18).
a. This relationship is robust, and is evident even after taking into account the influence prior health status and individual differences.
b. Psychosocial hazards are more closely related to psychological health than physical health. Any influence of psychosocial hazards on physical health is likely to be mediated through changes in health behaviours or changes in physiological reactivity, where an individual’s cognitive and physiological systems are tightly coupled and there is a physiological vulnerability.
c. It is likely that individual differences and psychosocial hazards operate jointly to determine how individuals interpret hazards and how individuals cope with hazards.
2) A negative orientation is related to subsequent reports of health (r=0.22).
a. This relationship is robust, and is evident even after taking into account the influence prior health status and psychosocial hazards.
b. The relationship is stronger for psychological health and the cognitive experience of physical symptoms, rather than physical illness itself.
c. There appears to be no difference in the magnitude of the relationship between a negative orientation that is a trait, an attitude or a state individual difference.
d. A negative orientation might inflate reporting of symptoms in epidemiological self-report surveys and monitoring systems reliant on physician reports.
e. A negative orientation is more prevalent within women and younger people of working age. There are also differences between different socioeconomic groups and occupational groups.
90

3) There is great stability in psychological health and negative orientation (r=0.59).
a. However, negative orientation can change, perhaps due to incremental changes resulting from changes in the environment or changes in socio-cultural portrayals of work-related stress. Change is likely to be slow and subtle.
In the following sections, we discuss the implications for monitoring of work-related stress, organisational practice and subsequent research arising from the findings of the meta-analysis, secondary analysis of other data-bases and our review of relevant theoretical explanations.
6.1. Implications for monitoring
Any social measurement is likely to contain some degree of error, and this also applies to systems designed to monitor work-related stress and associated ill-health. Nevertheless, our interpretation of the results of the meta-analysis, secondary analysis and review of theoretical processes indicates where monitoring systems might be more or less accurate.
a) Monitoring for stress-related symptoms is likely to be more sensitive to changes in the work environment if psychological rather than physical symptoms are assessed;
b) Monitoring systems reliant on self-reports might overestimate extent of symptoms attributable to psychosocial hazards, especially physical symptoms.
c) Monitoring systems reliant on physician reports might overestimate the extent of psychological problems attributable to work-related stress.
d) The over-estimation predicted in points b) and c) might be more prevalent in certain groups of the population where a negative orientation is more prevalent, such as women or younger people. There might also be differences that are more subtle, between different socio-economic and occupational groups. However, any differences between demographic groups are likely to be small.
Discussion of theoretical paths also indicates that changes in symptoms following improvements in work
91

conditions might take some time to be large enough to detect. Even though changes in work conditions could change health and make a negative orientation more positive, such changes could take at least five years to become apparent (cf. Dormann and Zapf, 2001).
6.1.1. Are measures too insensitive?
The high stability observed in psychological health in the meta-analysis could reflect a certain degree of insensitivity in measures of health and well-being.
In most studies, people are asked to give a generalised impression of how they have been feeling over the past few weeks, month, year, etc. Asking for such generalised impressions assumes that people are capable of recalling all relevant incidents and forming an accurate judgement on the basis of those incidents. Of course, this might be asking too much, and responses might equally reflect underlying and immutable personality factors as easily as real changes in health (cf. Barrett, 1997).
Such problems might become magnified as the period of assessment is increased. The practical implication here, then, is that measures of health might be more accurate if they ask respondents to indicate their health over a relatively recent and well-defined period (i.e. rating over the past month is better than rating over the past year, rating over the past week is better than rating over the past month). However, there is little or no research on the relative accuracy of retrospective reports of well-being or health in working samples over time frames greater than a few days or weeks. Therefore, there are currently no readily available metrics to help guide decisions on trade-offs between the accuracy of recent ratings and the wider coverage of time periods associated with retrospective reports over longer time frames.21
Parkinson et al (1995) report a study of mood ratings of 30 employed adults over two working weeks. Participants were asked to rate mood several times a day, and averaged daily mood ratings were compared to participants’ retrospective assessment of mood for that day. Average momentary ratings of mood were highly correlated with retrospective ratings of daily mood (0.66 for positive mood, 0.68 for negative mood). Parkinson et al also report a tendency for participants to overestimate their levels of positive mood at the end of a daily basis, but not their levels of negative mood.
92
21

Even so, like psychosocial hazards (Rick et al, 2001), it is possible the most sensitive measures will use frequency based scales to record symptoms, rather than asking respondents to indicate the extent of their agreement with statements about their health.
6.1.2. How to assess negative orientation
The findings of the meta-analysis indicate that a negative orientation might lead to an overestimation of some stress-related symptoms. Given that a negative orientation might change only very slowly, this might make it appear that a high frequency of stress-related illness persists, even after real improvements have been made.
It is therefore important that monitoring systems include some assessment of negative orientation so that they can take into account the level of stress-related symptoms that could be attributable to a negative orientation. Given the potential influence of occasion factors, it is important that negative orientation be measured at the same time as symptoms and hazards.
There exist short measures of negative orientation, such as the negative affectivity scale from the PANAS (Watson, Clark and Tellegen, 1988), and neuroticism scales embedded in personality questionnaires such as the Eysenck Personality Questionnaire (Eysenck and Eysenck, 1975). However, given the importance of assessing negative orientation, then a more detailed consideration of existing measures might be called for.22
6.2. Implications for practice
6.2.1. Cognitive and perceptual factors and the individual
This report has focused on individual differences and cognitive processes. It might then be tempting to conclude that the causes of stress-related ill-health reside within the individual, rather than work environment. The results of the meta-analysis show that individual differences are associated with subsequent changes in health, and that individual
22 Such a review would need not only to examine the psychometric properties of validity and reliability of measures, but also, for example, the extent they assess the whole range of negative orientation, rather than a specific facet, as well as the costs and benefits of measures that are free to use versus those that are commercially available.
93

differences are associated with how people report physical symptoms, but not more objective measures of physical ill-health. However, blaming the individual might be both erroneous and might focus attention on only a few suitable interventions (see also, Daniels et al, 2002c).
As we have argued, individual differences represent indicators of how people think. However:
a) Our meta-analysis indicates that psychosocial hazards predict subsequent health above the effects of individual differences and prior health status;
b) A range of theories we have reviewed and the evidence underpinning those theories suggest it is how individuals interpret psychosocial hazards that is important in linking hazards to health;
c) Our theoretical review indices that interpretations of psychosocial hazards might be influenced by individual experience – dating back as far as early childhood, but the work environment and the wider socio-cultural environment might also influence interpretations.
Consequently, although individually focused interventions might be appropriate for some individuals, where hazards are widely experienced and widely interpreted in much the same way, interventions focused on work groups and organisations might be more appropriate.
The finding that hazards are related to subsequent health, as well as the theoretical review, might indicate the suitability of job design interventions to prevent the occurrence of psychosocial hazards or to promote effective coping through, for example, providing discretion over work activities or social support (cf. Karasek and Theorell, 1990).
However, because the theoretical review indicates that how we categorise psychosocial hazards might influence how they affect us, there are potential implications for how psychosocial hazards are assessed to form the diagnosis for intervention. Our theoretical review might indicate that psychosocial hazards should be assessed using the categories and language used to describe those categories common to a given organisation, occupation or work group. In this way, more contextually specific assessments might provide a better basis for targetted intervention (Rick et al, 2002). This might then provide a
94

psychological basis for approaches that use assessments tailored to specific work contexts (e.g. Cox, Griffiths, Barlow, Randall, Thomson and Rial-Gonzalez, 2000).
The theoretical review also indicates that there might be benefits from work conditions that promote progress toward personal goals at a rate greater than an individual might expect (see also Frese and Zapf, 1994). Again, discretion over work or support might be important to promote this, as this might allow individuals to pursue their own goals. Additionally, performance management might be useful here. We might expect to see better psychological health in organisations where performance management systems allow line managers to i) support individuals to align their own goals with organisational goals, ii) set time-frames for achieving goals and iii) identify the means of attaining those goals.
6.2.2. Cognitive and perceptual factors and society
We have concluded that socio-cultural factors might influence how we interpret psychosocial hazards. We based this conclusion on the secondary analyses and the theoretical review.
Our theoretical review indicates that if we are led to believe that something is psychologically harmful, then it may, indeed, become so. Communicating how the socio-cultural environment shapes our beliefs about psychosocial hazards might be an important area for intervention. Using the principles of good risk communication,23 it might be necessary to inform public debate so that, for example:
a) The debate does not become polarised between those that would blame the individual and those that catastrophise the contemporary work environment;
b) The public become aware of sensible, considered scientific knowledge on the links between work, cognition and health – as well as the limits of that scientific knowledge;
c) It is clear what people, organisations and employee associations such as trades unions can do to promote well-being at work.
See, for example, Daniels (1996) and Daniels et al (2002c) for an application to psychosocial hazards.
95
23

By focusing communication on real, rather than imagined, hazards and what can sensibly be done about them, then it might be possible to engender a more positive and proactive orientation to work-related stress. However, the extent to which various institutions (such as the media, trades unions) influence our interpretations of hazards is largely unknown. Therefore, consideration of these socio-cultural factors and potential relationships to risk communication might be important.
6.3. Implications for research
6.3.1. Need for detailed, time intensive studies
The theoretical review indicates that explanations for the relationships between psychosocial hazards, health and diagnosis accord a prominent position to dynamic emotional processes that are both cognitive and social. Our theoretical review also suggests that events, rather than stable job conditions, are more proximal cause of emotions and health.
It is therefore important that research does not concentrate solely on large-scale longitudinal cohort studies or intervention studies,24 in attempts to establish causal relationships between stable job conditions and health. Although small in number relative to crosssectional studies, such studies met the stringent inclusion criteria for our meta-analysis and, therefore, dominated our meta-analytic review. Whilst useful for establishing whether there might exist generalisable, causal relationships between variables, large cohort designs have difficulty capturing the short-term dynamic, interdependent and complex processes that our theoretical review indicates underpin the relationships amongst work, more stable individual differences, health and closely related variables. For example, our meta-analysis indicated that very few longitudinal studies that met our strict inclusion criteria had examined state individual differences. Rather longitudinal studies of the kind included in our metaanalysis focus more frequently on more stable individual differences such as attitudes and personality. However, without detailed consideration of the dynamic processes underlying predictive associations found in
This is not to say such large scale longitudinal cohort or intervention studies should no longer be conducted, as they are clearly useful and vastly superior, all other things being equal, to cross-sectional designs.
96
24

longitudinal and intervention studies, it will not be possible to interpret fully associations found in large scale cohort designs. What is needed, then, to complement cohort studies, are focused studies that concentrate on the dynamic processes linking, for example:
a) stable job conditions, personal factors and social factors to the occurrence of distressing events at work;
b) events in the work place to cognitive interpretation of those events;
c) cognition to changes in emotion;
d) changes in cognition and emotion to coping choices and subsequent action.
e) changes in cognitive processes and emotion to social dynamics;
f) cognitive processes to physiological processes;
g) social processes of emotional expression to the cognitive processes underlying physician diagnosis.
Best placed to research such questions, perhaps, are well-designed studies concentrating on daily or momentary changes or specific episodes over a period of time. Whilst necessarily intensive in the time required from participants, experimental methods, diary methods and other event sampling methods might all be useful in respect of these examining these detailed processes as they occur.
The suggestion to research the social and cognitive processes underlying diagnosis is an area of importance. We were only able to find one study that examined this issue (Ellington and Wiebe, 1999). Whilst the implications of the study are worthy of detailed consideration, the study suffers from a number of design-flaws that make its findings tentative rather than definitive.
6.3.2. Researching cognitive factors in the workplace
In our meta-analysis, we used broad individual differences as an indicator of differences in cognitive processes. In our theoretical review, we indicated that cognitive processes might influence how psychosocial hazards are categorised;
97

how implications for goals are appraised; how hazards are linked to situations that have elicited emotions in the past; and how decisions about coping behaviour are made. By using broad measures of individual differences previous research may have missed some of the intricacies of the interplay between cognition and psychosocial hazards. Indeed, some studies that have examined interactions between individual differences and hazards have produced conflicting results, even when using the same individual differences and hazards (e.g. Daniels and Guppy, 1994; Parkes, 1991).
Methods that can make cognitive processes more explicit might be able to unravel more accurately the intricacies of the relationships between cognition, psychosocial hazards and emotions. One set of methods, called cognitive mapping methods, can be used to show how people understand the relations between hazards and emotions, the causes of hazards, how to cope with hazards and the likely consequences of emotions (Daniels et al, 2002c). One practical advantage of using such methods is that the methods can also help people articulate how they would change the work environment, which can then be used to feed into organisational change interventions (Harris, Daniels and Briner, 2002).
Cognitive processes are, of course, dynamic: what we think about changes from one moment to the next. Therefore, methods will need to be developed that can assess interpretations of hazards in a way to suit the special circumstances of diary and event-sampling studies. Only in this way will it be possible to capture the relationships between hazards, cognitive processes and emotions are they unfold in real contexts and in real time.
There also remains a question concerning the nature of psychosocial hazards. The meta-analysis found no difference between objective and subjective measures of hazards in the relationship between hazards and health. This might reflect the small number of studies that have used objective methods. Notwithstanding the issue of events and their relationship to stable job conditions highlighted above, it might be that it is very difficult to obtain objective measures of some, if not most, psychosocial hazards.
Many hazards are linked to the social fabric of organisations, and therefore have no reality outside of this social fabric. Unlike physical hazards, such as noise, many psychosocial hazards have no material
98
reality. This has implications for measuring psychosocial hazards, and a careful re-think might be needed of the relationship between subjective and objective measures. Different methods might be tapping qualitatively different aspects of the nature of hazards.
Given that many hazards inhabit a world defined by social rather than physical interactions, the possibility arises that different socio-cultural contexts might promote the incidence of some, rather than other, psychosocial hazards, as well the interpretation of those hazards.
6.4. Concluding remarks
In this report, we have shown that psychosocial hazards and individual differences both influence how we experience work-related health. It is clear, however, these simple relationships do not convey the underlying complexities of the interaction between a dynamic work environment, dynamic cognitive processes and the wider socio-cultural environment that influences the experience, reporting and expression of work-related stress. The complexity of these processes has implications for how work-related stress is managed and how that management is monitored.
99
7. References * indicates study was included in the meta-analysis.
Arvey, R.D., Bouchard, T.J., Segal, N.L., & Abraham, L.M. (1989). Job satisfaction: environmental and genetic components. Journal of Applied Psychology, 74, 187-192.
* Bakker, A.B., Schaufeli, W.B., Sixma, H.J., Bosveld, W., & van Dierendonck, D. (2000). Patient demands, lack of reciprocity, and burnout: a five-year longitudinal study among general practitioners. Journal of Organizational Behavior, 21, 425-441.
Barrett, L.F. (1997). The relationships among momentary emotion experiences, personality descriptions, and retrospective ratings of emotion. Personality and Social Psychology Bulletin, 23, 1100-1110.
Brief, A.P., Burke, M.J., George, J.M., Robinson, B., & Webster, J. (1988). Should negative affectivity remain an unmeasured variable in the study of job stress. Journal of Applied Psychology, 73, 193-198.
Barsalou, L.W. (1982). Context-independent and context-dependent information in concepts. Memory and Cognition, 10, 397-418.
Bryk, A.S., & Raudenbush, S.W. (1992). Hierarchical Linear Models. Newbury Park, CA: Sage.
Campbell, J.D., Chew, B., & Scratchley, L.S. (1991). Cognitive and emotional reactions to daily events: The effects of self-esteem and self-complexity. Journal of Personality, 55, 473-505.
Carver, C.S., & Scheier, M.F. (1990). Origins and functions of positive and negative affect: a control-process view. Psychological Review, 97, 19-35.
Cass, M., Farager, B., & Cooper, C.L. (in press). Health and Employment: A Review and Meta-Analysis Study. Sudbury: HSE Books.
Cook, T.D., & Campbell, D.T. (1976). The design and conduct of quasi-experiments and true experiment in field settings. In M.D.Dunnette (Ed.), Handbook of Industrial and Organizational Psychology. New York: Wiley
Cooper, C.L., Dewe, P.J., & O’Driscoll, M.P. (2001). Organizational Stress: A Review and Critique of Theory, Research, and Applications. Thousand Oaks CA: Sage.
Cox, T., Griffiths, A., Barlow, C.A., Randall, R., Thomson, L, & Rial-Gonzalez, E. (2000). Organisational Interventions for Work Stress: A Risk Management Approach. HSE Books: Sudbury.
Daniels, K (1996). Why aren’t managers concerned about occupational stress? Work & Stress, 10, 352-366.
100

Daniels, K. (2000). Measures of five aspects of affective well-being at work. Human Relations, 53, 275-294.
Daniels, K. (2001). Affect at work: cognition, categorisation and coping. British Psychological Society Centenary Conference, Glasgow.
Daniels, K., & Guppy, A. (1994). Occupational stress, social support, job control and psychological well-being. Human Relations, 47, 1523-1544.
* Daniels, K., & Guppy A. (1997). Stressors, locus of control and social support as consequences of psychological well-being. Journal of Occupational Health Psychology, 2, 156-174.
Daniels, K., Harris. C., & Briner, R. (2002a). Linking work conditions to affect: cognition, categorisation, goals and dysphoria. Paper for the Occupational Psychology Annual Conference, Blackpool.
Daniels, K., Harris, C., & Briner, R. (2002b). Negative emotions at work: the role of cognition. Paper for the British Academy of Management Conference, Hammersmith
Daniels, K., Harris, C., & Briner, R. (2002c). Understanding the Risks of Stress: A Cognitive Approach. Sudbury: HSE Books.
Daniels, K., Harris, C., & Briner, R. (in press). Linking work conditions to unpleasant affect: cognition, categorisation and goals. Journal of Occupational and Organizational Psychology.
Daniels, K., & Henry, J. (1998). Strategy: a cognitive perspective. In S.Segal-Horn (ed.), The Strategy Reader. Oxford: Blackwells.
Dewe, P. (1989). Examining the nature of work stress – individual evaluations of stressful experiences and coping. Human Relations, 42, 992-1013.
* Dierendonck van, D., Schaufeli, W.B., & Buunk, B.P. (1998). The evaluation of an individual burnout intervention program: the role of inequity and social support. Journal of Applied Psychology, 83, 392-407.
* Dormann, C., & Zapf, D. (1999). Social support, social stressors at work, and depressive symptoms: testing for main and moderating effects with structural equations in a three-wave longitudinal study. Journal of Applied Psychology, 84, 874-884.
Dormann, C., & Zapf, D. (2001). Job satisfaction: a meta-analysis of stabilities. Journal of Organizational Behavior, 22, 483-504.
Dutton, J.E. (1993). Interpretations on automatic: a different view of strategic issue diagnosis. Journal of Management Studies, 30, 339-357.
Edwards, J.R. (1992). A cybernetic theory of stress, coping, and well-being in organizations. Academy of Management Review, 17, 238-274.
101

Ellington, L., & Wiebe, D. (1999). Neuroticism, symptom presentation, and medical decision making. Health Psychology, 18, 634-643.
Ettner, S.L., & Grzywacz, J.G. (2001). Workers’ perceptions of how jobs affect health: a social ecological perspective. Journal of Occupational Health Psychology, 6, 101-113.
Eysenck, H.J., & Eynsenck S.B.G. (1975). Manual for the Eynsenck Personality Questionnaire. London: Hodder and Staughton.
Eysenck, M., & Keane, M.T. (1990). Cognitive Psychology. London: Erlbaum.
Firth-Cozens, J. (1992). Why me? a case study of the process of perceived occupational stress. Human Relations, 45, 131-141.
Firth-Cozens, J., & Hardy, G.E. (1992). Occupational stress, clinical treatment and changes in job perceptions. Journal of Occupational and Organizational Psychology, 65, 81-88.
Frese, M., & Zapf, D. (1994). Action as the core of work psychology: a German approach. In H.C. Triandis, M.D. Dunnette, L.M. Hough (Eds.), Handbook of Industrial and Organizational Psychology, 2nd ed (pp 272-340). Palo Alto, CF: Consulting Psychologists Press.
Friedman, H.S., & Booth-Kewley, S. (1987). The “disease-prone” personality: a meta-analytic view of the construct. American Psychologist, 42, 539-555.
* Frone, M.R., Russell, M., & Cooper, M.L. (1997). Relation of work-family conflict to health outcomes: a four-year longitudinal study of employed parents. Journal of Occupational and Organizational Psychology, 70, 325-355.
Harris, C. (2002). Work Stress and Mental Models. Unpublished PhD thesis, University of Nottingham.
Harris, C., Daniels, K., & Briner, R. (2002). Using cognitive mapping for psychosocial risk assessment. Risk Management: An International Journal, 4 (3), 7-22.
* Hellgren, J., Sverke, M., & Isaksson, K. (1999). A two-dimensional approach to job insecurity: consequences for employee attitudes and well-being. European Journal of Work and Organizational Psychology, 2, 179-195.
Hunter, J.E., & Schmidt, F.L. (1990). Methods of Meta-Analysis: Correcting Error and Bias in Research Findings. Sage: Newbury Park.
Johnson-Laird, P.N. (1989). Mental models. In M.I. Posner (ed.), Foundations of Cognitive Science. MIT Press, Cambridge, Massachusetts.
* Jonge de, J., Dormann, C., Janssen, P.P.M., Dollard, M.F., Landeweerd, J.A., & Nijhuis, F.J.N. (2001). Testing reciprocal relationships between job characteristics and psychological well-being: a cross-lagged structural
102

equation model. Journal of Occupational and Organizational Psychology, 74, 29-46.
Karasek, R.A., & Theorell, T. (1990). Healthy Work. New York: Basic Books.
Kasl, S.V. (1983). Pursuing the link between stressful life experiences and disease: a time for re-appraisal. In C.L.Cooper (Ed.), Stress Research: Issues for the Eighties. Chichester: Wiley.
Kasl, S. (1996). The influence of the work environment on cardiovascular health: a historical, conceptual, and methodological perspective. Journal of Occupational Health Psychology, 1, 42-56.
Kirmayer, L.J., Robbins, J.M., & Paris, J. (1994). Somatoform disorders: personality and the social matrix of somatic distress. Journal of Abnormal Psychology, 103, 125-136.
* Kivimaki, M., Vahtera, J., Thomson, L., Griffiths, A., Cox, T., & Pentti, J. (1997). Psychosocial factors predicting employee sickness absence during economic decline. Journal of Applied Psychology, 82, 858-872.
Lang, P.J. (1984). Cognition in emotion: Concept and action. In C.E.Izard, R.R. Zajonc & J. Kagan (Eds.), Emotions, Cognitions and Behaviour, (pp. 192-226). Cambridge: Cambridge University Press.
Lazarus, R.S. (1991). Emotion and Adaptation. New York: Oxford University Press.
Lazarus, R.S. (1999). Stress and Emotion: A New Synthesis. New York: Springer.
Lazarus, R.S., & Folkman, S. (1984). Stress, Appraisal and Coping. New York: Springer.
Lindsay, S.J.E., & Powell, G.E. (1994). The Handbook of Clinical Adult Psychology 2nd ed. London: Routledge.
McCrae, R., & Costa, P. (1997). Personality trait structure as a human universal. American Psychologist, 52, 509-516.
Moyle P. (1995). The role of negative affectivity in the stress process: tests of alternative models. Journal of Organizational Behavior, 16, 647-668.
* Moyle, P., & Parkes, K. (1999). The effects of transition stress: a relocation study. Journal of Organizational Behavior, 20, 625-646.
Nyamberega, S., Daniels, K., & Sparrow, P. (2001). Person-organization fit and job involvement in developing contexts. Applied Psychology: An International Review, 50, 109-140.
Parkes, K.R. (1991). Locus of control as moderator: an explanation for additive versus interactive findings in the demand-discretion model of work stress? British Journal of Psychology, 82, 291-312.
Parkinson, B. (1995). Ideas and Realities of Emotion. Routledge, London.
103

Parkinson, B., Briner, R.B., Reynolds, S., & Totterdell, P. (1995). Time frames for mood: relations between momentary and generalized ratings of affect. Personality and Social Psychology Bulletin, 21: 331-339.
Payne R., & Cooper, C.L. (1991). Personality and Stress: Individual Differences in the Stress Process. Chichester: Wiley.
Power, M., & Dalgleish, T. (1997). Cognition and emotion: From order to disorder. Hove, East Sussex: Psychology Press.
Rick, J., Briner, R., Daniels, K., Perryman, S., & Guppy, A. (2001). A Critical Review of Psychosocial Hazard Measures. Sudbury: HSE Books.
Rick, J., Thomson, L., Briner, R.B., O’Regan, S., & Daniels, K. (2002). Review of Existing Supporting Scientific Knowledge to Underpin Standards of Good Practice for Key-Work Related Stressors – Phase 1. Sudbury: HSE Books.
* Rodriguez, I., Bravo, M.J., Peiro, J.M., & Schaufeli, W. (2001). The demands-control-support model, locus of control and job dissatisfaction: a longitudinal study. Work & Stress, 15, 97-114.
Rusting, C.L. (1998). Personality, mood, and cognitive processing of emotional information: three conceptual frameworks. Psychological Bulletin, 124, 165196.
* Saks, A.M., & Ashfoth, B.E. (2000). The role of dispositions, entry stressors, and behavioral plasticity theory in predicting newcomers’ adjustment to work. Journal of Organizational Behavior, 21, 43-62.
* Sargent, L.D., & Terry, D.J. (1998). The effects of work control and job demands on employee adjustment and work performance. Journal of Occupational and Organizational Psychology, 71, 219-236.
* Schonfeld, I.S. (2001). Stress in 1st-year women teachers: the context of social support and coping. Genetic, Social, and General Psychology Monographs, 127, 133-168.
* Shaw, J.D., & Gupta, N. (2001). Pay fairness and employee outcomes: exacerbation and attenuation effects of financial need. Journal of Occupational and Organizational Psychology, 74, 299-320.
* Shirom, A., Westman, M., Shammai. O., & Carel, R.S. (1997). Effects of work overload and burnout on cholesterol and triglycerides levels: the moderating effects of emotional reactivity among male and female employees. Journal of Occupational Health Psychology, 2, 275-288.
Schwartz, J.E., Pickering, T.G., & Landsergis, P.A. (1996). Work-related stress and blood pressure: current theoretical models and considerations from a behavioral medicine perspective. Journal of Occupational Health Psychology, 1, 287-310.
104

Schuler, R.S. (1985). Integrative transactional process model of coping with stress in organizations. In T.A.Beehr & R.S. Bhagat (Eds.), Human Stress and Cognition in Organizations: An Integrated Perspective. New York: Wiley.
Spector, P.E., Chen, P.Y., & O’Connell, B.J. (2000b). A longitudinal study of relations between job stressors and job strains while controlling for prior negative affectivity and strains. Journal of Applied Psychology, 85, 211-218.
Spector, P.E., & Goh, A. (2001). The role of emotions in the occupational stress process. Exploring Theoretical Mechanisms and Perspectives, 1, 195-232.
Spector, P.E., Zapf, D., Chen, P.Y., & Frese M. (2000a). Why negative affectivity should not be controlled in job stress research: don’t throw the baby out with the bath water. Journal of Organizational Behavior, 21, 79-95.
Sturges, J. (1999). What it means to succeed: personal conceptions of career success held by male and female managers at different ages. British Journal of Management, 10, 239-252.
* Taris, R., & Feij, J.A. (2001). Longitudinal examination of the relationship between supplies-values fit and work outcomes. Applied Psychology: An International Review, 50, 52-80.
* Taris, T., Peeters, M.C.W., Le Blanc, P.M., Schreurs, P.J.G., & Schaufeli, W. (2001). From inequity to burnout: the role of job stress. Journal of Occupational Health Psychology, 6, 303-323.
Twenge, J.M. (2000). The age of anxiety? birth cohort change in anxiety and neuroticism, 1952-1993. Journal of Personality and Social Psychology, 79, 1007-1021.
Warr, P. (1990). The measurement of well-being and other aspects of mental health. Journal of Occupational Psychology, 63, 193-210.
Warr, P.B. (1999). Well-being and the workplace. In D.Kahneman, E.Diener & N.Schwarz (Eds.), Well-Being: The Foundations of Hedonic Psychology, (pp. 392-412). New York: Russell Sage Foundation.
Watson, D., Wiese, D., Vaidya, J., & Tellegen, A. (1999). The two general activation systems of affect: structural findings, evolutionary considerations, and psychobiological evidence. Journal of Personality and Social Psychology, 76: 820-838.
Weiss, H.M., & Cropanzano, R. (1996). Affective events theory: A theoretical discussion of the structure, causes, and consequences of affective experiences at work. In B.M. Staw and L.L. Cummings (Eds.), Research in Organizational Behavior (Vol. XVIII, pp. 1-74). Greenwich CT: JAI Press
Williams, J.M.G., F.N. Watts, C. MacLeod, & A. Mathews (1997). Cognitive Psychology and Emotional Disorders (2nd edn.). Wiley, Chichester.
105

Wofford, J.C., & Daly, P.S. (1997). A cognitive-affective approach to understanding individual differences in stress propensity and resultant strain. Journal of Occupational Health Psychology, 2, 134-147.
Wolpin, J., Burke, R.J., & Greenglass, E.R. (1991). Is job satisfaction an antecedent or a consequence of psychological burnout? Human Relations, 44, 193-209
Zajonc, R.B. (1980). Feeling and thinking: Preferences need no inferences. American Psychologist, 35, 151-175.
Zapf, D., Dormann, C., & Frese, M. (1996). Longitudinal studies in organizational stress research: a review of the literature with reference to methodological issues. Journal of Occupational Health Psychology, 1, 145-169.
106

8. Appendices A) Form used to sort the literature
107
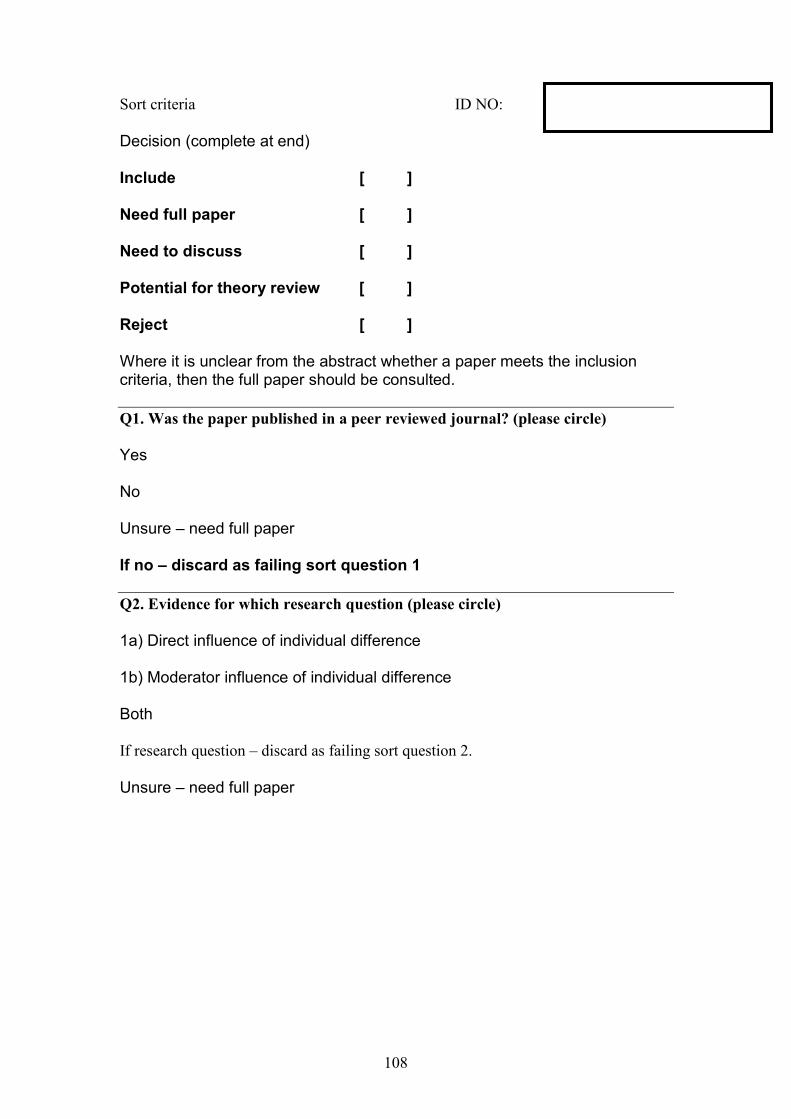
Sort criteria ID NO:
Decision (complete at end)
Include [ ]
Need full paper [ ]
Need to discuss [ ]
Potential for theory review [ ]
Reject [ ]
Where it is unclear from the abstract whether a paper meets the inclusion criteria, then the full paper should be consulted.
Q1. Was the paper published in a peer reviewed journal? (please circle)
Yes
No
Unsure – need full paper
If no – discard as failing sort question 1
Q2. Evidence for which research question (please circle)
1a) Direct influence of individual difference
1b) Moderator influence of individual difference
Both
If research question – discard as failing sort question 2.
Unsure – need full paper
108

Q3. Type of individual differences examined (please tick all that apply)
a) Trait +ve orientation (e.g. agreeableness) b) Trait –ve orientation (e.g. neuroticism) c) Attitudinal/medium term stability +ve orientation (e.g. selfesteem) d) Attitudinal/medium term stability –ve orientation (e.g. external locus of control) e) State +ve orientation (e.g. positive affect – enthusiasm, activity) f) State –ve orientation (e.g. negative affect – anxiety, anger depression)
If none of the above – discard as failing sort question 3 If unspecified in abstract, obtain full paper
Q4. Type of study (tick all that apply)
Review paper Refer to KD to include elsewhere in report Meta-analysis Refer to KD to include elsewhere in report Theory paper Refer to KD to include elsewhere in report Empirical paper Continue applying sort criteria
109
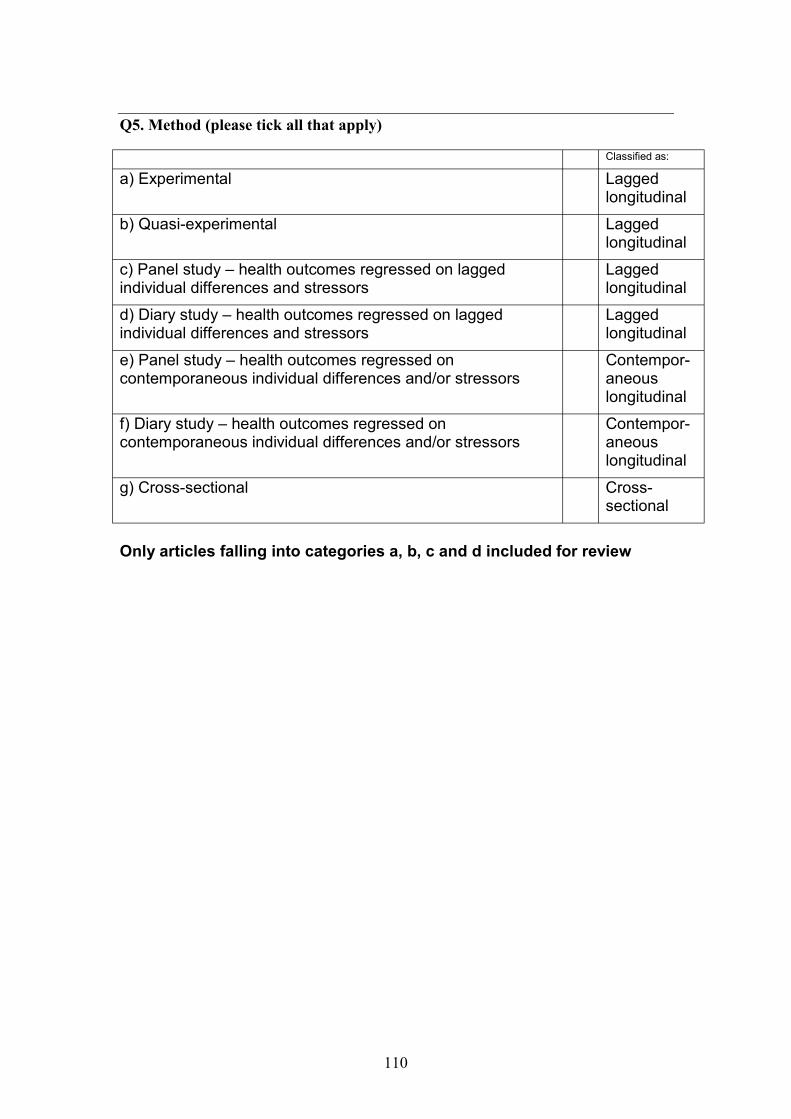
Q5. Method (please tick all that apply)
Classified as:
a) Experimental Lagged longitudinal
b) Quasi-experimental Lagged longitudinal
c) Panel study – health outcomes regressed on lagged individual differences and stressors
Lagged longitudinal
d) Diary study – health outcomes regressed on lagged individual differences and stressors
Lagged longitudinal
e) Panel study – health outcomes regressed on contemporaneous individual differences and/or stressors
Contemporaneous longitudinal
f) Diary study – health outcomes regressed on contemporaneous individual differences and/or stressors
Contemporaneous longitudinal
g) Cross-sectional Crosssectional
Only articles falling into categories a, b, c and d included for review
110

Q6. Type of health state measured (please tick all that apply)
Health state Self-report - acute psychological – e.g. mood Self-report – acute physical - e.g. non-specific symptoms such as headaches Self-report – chronic psychological - e.g. Beck depression inventory Self-report – chronic physical - e.g. self-reports of angina Self-report – health behaviours - e.g. self-reported drinking Physician report - acute psychological - e.g. acute anxiety disorder Physician report – acute physical - e.g. influenza Physician report – chronic psychological - e.g. diagnosed depression Physician report – chronic physical - e.g. hypertension Physician report – health behaviours - e.g. # visits to physician Objective measures/research team diagnosis - acute psychological -e.g. diagnosis by research team psychiatrist(s) Objective measures/research team diagnosis – acute physical - e.g. swabs taken for presence of flu bugs Objective measures/research team diagnosis – chronic psychological -e.g. diagnosis by research team psychiatrist(s) Objective measures/research team diagnosis - chronic physical - e.g. coronary heart diseased diagnosed by angiogram Objective measures/research team diagnosis - health behaviours - e.g. sickness absence from company records
If none of the above – discard as failing sort question 6
If unspecified in abstract, obtain full paper
Q7. Sample consists of working adults? (please circle)
Yes
No
If unspecified in abstract, obtain full paper
If no – discard as failing sort question 6
111

Q8. Type of psychosocial hazards examined (please tick all that apply)
1) Work demands including: 1a) workload - quantity, pacing, time pressure, emotional content
of work; 1b) work scheduling – total hours, breaks, travel time, shift work; 1c) work organisation and job design – task design, team
working; 1d) physical environment – real and perceived danger, noise,
toxins; 2) Worker control or autonomy – including:
2a) Skill discretion – variety, opportunity for skill use; 2b) Decision authority – control and autonomy; 2c) Participation in decision making.
3) Support and interpersonal relationships in the working environment – including:
3a) Proactive support – practical & emotional support, support from work and outside of work, feedback;
3b) Reactive support - practical & emotional support, support from work and outside of work, feedback;
3c) Team/intepersonal conflict, bullying and harassment;
Others - please specify
If no psychosocial hazards measured – discard as failing sort question 8
112

Final comments or discussion points
113

B) Bibliography for CAPHEM model
Aarts, H., & Dijksterhuis, A. (2000). Habits as knowledge structures: automaticity in goal-directed behavior. Journal of Personality and Social Psychology, 74, 5363.
Abelson, R.P., & Black, J.B. (1986). Introduction. In J.A.Galambos, R.P.Abelson and J.B.Black (Eds.), Knowledge Structures (pp 1-18). Hillsdale, NJ: Erlbaum.
Abrahamson, E. (1996). Management fashion. Academy of Management Review, 21, 254-285.
Adler, A. (1954). Understanding Human Nature. New York: Fawcett.
Allport, G.W. (1961). Pattern of Growth in Personality. New York: Holt, Rinehart, & Winston.
Anderson, J.R. (1983). The Architecture of Cognition. Cambridge MA: Harvard University Press.
Anderson, J.R. (1991). The Adaptive Character of Thought. Hillsdale, NJ: Erlbaum.
Andrews, F.M., & McKennell, A.C. (1980). Measures of self-reported well-being. Social Indicators Research, 25, 1-30.
Antonovsky, A. (1987). Unravelling the Mystery of Health: How People Manage Stress and Stay Well. San Francisco: Jossey Bass.
Armstrong, M. (2001). A Handbook of Human Resource Management Practice. 8th
Edition. London: Kogan Page.
Ashforth, B.E., & Humphrey, R.H. (1995). Emotion in the workplace: A reappraisal. Human Relations, 48, 97-125.
Ashkanasy, N.M., Härtel, C.E.J., & Zerbe, W.J. (2000). Emotions in the Workplace: Research, Theory and Practice. Westport: Quorum Books.
Atkinson, R.C., & Shiffrin, R.M. (1971). The control of short-term memory. Scientific American, 225, 82-90.
Austin, J.T., & Vancouver, J.B. (1996). Goal constructs in psychology: structure, process, and content. Psychological Bulletin, 120, 338-375.
Baddeley, A.D., & Hitch, G. (1974). Working memory. In G.H. Bower (Ed.), The Psychology of Learning and Motivation (Vol. VIII, pp. 647-667). New York: Academic Press.
Bandura, A. (1977). Social Learning Theory. Englewood Cliffs, NJ: Prentice Hall.
Bandura, A. (1986). Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice Hall.
114

Bandura, A. (2001). Social cognitive theory: an agentic perspective. Annual Review of Psychology, 52, 1-26.
Bandura, A., & Locke, E.A. (2003). Negative self-efficacy and goal effects revisited. Journal of Applied Psychology, 88, 87-99.
Barley, S.R., & Knight, D.B. (1992). Toward a cultural theory of stress complaints. In B.M.Staw & L.L. Cummings (Eds.), Research in Organizational Behavior (Vol. XIV, pp. 1-48).
Barsalou, L.W. (1983). Ad hoc categories. Memory and Cognition, 11, 211-27.
Barsalou, L.W. (1985). Ideals, central tendency, and frequency of instantiation as determinants of graded structure of categories. Journal of Experimental Psychology: Learning, Memory, and Cognition, 11, 629-654.
Barsalou, L.W. (1987). The instability of graded structure: Implications for the nature of concepts. In U.Neisser (Ed.), Concepts and Conceptual Development: Ecological and Intellectual Factors in Categorization. (pp. 101-140). Cambridge: Cambridge University Press.
Bartel, C.A., & Saavedra, R. (2000). The collective construction of work group moods. Administrative Science Quarterly, 45, 197-231.
Basch, J., & Fisher, C.D. (2000). Affective events-emotions matrix: a classification of work events and associated emotions. In N.M. Ashkanasy, C.E.J. Härtel & W.J. Zerbe (Eds.), Emotions in the Workplace: Research, Theory and Practice (pp 36-48). Westport: Quorum Books.
Beehr, T.A., & Newman, J.E. (1978). Job stress, employee health, and organizational effectiveness: A facet analysis, model, and literature review. Personnel Psychology, 31, 665-699.
Blaine, B., Crocker, J., & Major, B. (1995). The unintended negative consequences of sympathy for the stigmatized. Journal of Applied Social Psychology, 25, 889905.
Bless, H. (2001). Mood and the use of general knowledge structures. In L.L. Martin & G.L. Clore (Eds.), Theories of Mood and Cognition: A User’s Handbook (pp 9-26). Mahwah, NJ: Erlbaum.
Bonanno, G.A., Keltner, D., Holen, A., & Horowitz, M.J. (1995). When avoiding unpleasant emotions might not be such a bad thing: verbal-autonomic response dissociation and midlife conjugal bereavement. Journal of Personality and Social Psychology, 69, 975-989.
Bower, G.H. (1981). Mood and memory. American Psychologist, 36, 129-148.
Bowlby, J. (1988). A Secure Base. New York: Basic Books.
115

Brief, A., & George, J.M. (1991). Psychological stress and the workplace: a brief comment on Lazarus’ outlook. Journal of Social Behavior and Personality, 6, 15-20.
Brief, A.P., Butcher, A.H., & Roberson, L. (1995). Cookies, disposition, and job attitudes: The effects of positive mood-inducing events and negative affectivity on job satisfaction in a field experiment. Organizational Behavior and Human Decision Processes, 62, 55-62.
Briner R.B., & Reynolds S. (1999). The costs, benefits, and limitations of organizational level stress interventions. Journal of Organizational Behavior, 20, 647-664.
Briner, R.B. (1999). The neglect and importance of emotion at work. European Journal of Work and Organizational Psychology, 8, 323-346.
Brockner, J., & Higgins, E.T. (2001). Regulatory focus theory: implications for the study of emotions at work. Organizational Behavior and Human Decision Processes, 86, 35-66.
Brockner, J., Paruchuri, S., Idson, L.C., & Higgins, E.T. (2002). Regulatory focus and the probability estimates of conjunctive and disjunctive events. Organizational Behavior and Human Decision Processes, 87, 5-24.
Brunstein, J.C., Schultheiss, O.C., & Grässman, R. (1998). Personal goals and emotional well-being: the moderating role of motive dispositions. Journal of Personality and Social Psychology, 75, 494-508.
Butler, E.A., Egloff, B., Wilhelm, F.H., Smith. N.C., Erickson, E.A., & Gross,. J.J. (2003). The social consequences of expressive suppression. Emotion, 3, 48-67.
Buunk, B.P., & Hoorens, V. (1992). Social support and stress: The role of social comparison and social exchange processes. British Journal of Clinical Psychology, 31, 445-457.
Carayon, P. (1994). Stressful jobs and non-stressful jobs: A cluster analysis of office jobs. Ergonomics, 37, 311-323.
Carver, C.S. (1992). Cognitive processes and self-regulation: determinants of concentration and distraction. Applied Psychology: An International Review, 43, 387-391.
Carver, C.S. (2003). Pleasure as a sign you can attend to something else: placing positive feelings within a general model of affect. Cognition & Emotion, 17, 241-261.
Carver, C.S., & Scheier, M.F. (1990). Origins and functions of positive and negative affect: a control-process view. Psychological Review, 97, 19-35.
Carver, C.S., Sutton, S.K., & Scheier, M.F. (2000). Action. emotion, and personality: Emerging conceptual integration. Personality and Social Psychology Bulletin, 26, 741-751.
116

Catanzaro, S.J., Wasch, H.H., Kirsch, I., & Mearns, J. (2000). Coping-related expectancies and dispositions as prospective predictors of coping responses and symptoms. Journal of Personality, 68, 757-788.
Chaiken, S., & Trope, Y. (Eds.) (1999). Dual Process Theories in Social Psychology. New York: Guildford Press.
Choi, I., Nisbett, R.E., & Smith, E.E. (1997). Culture, category salience, and inductive reasoning. Cognition, 65, 15-32.
Clarke, M.S., & Brissette, I. (2000). Relationship beliefs and emotion: reciprocal effects. In N.H.Frijda, A.S.R. Manstead & S. Bem (Eds.), Emotions and Beliefs: How Feelings Influence Thoughts (pp 212-240). Paris: Cambridge University Press.
Clore, G.L., & Gasper, K. (2000). Feeling is believing: some affective influences on belief. In N.H.Frijda, A.S.R. Manstead & S. Bem (Eds.), Emotions and Beliefs: How Feelings Influence Thoughts (pp 10-44). Paris: Cambridge University Press.
Clore, G.L., Wyer, R.S., Dienes, B., Gasper, K., Gohm, C., & Isbell, L. (2001). Affective feelings as feedback: some cognitive consequences. In L.L. Martin & G.L. Clore (Eds.), Theories of Mood and Cognition: A User’s Handbook (pp 27-62). Mahwah, NJ: Erlbaum.
Coats, E.J., Janoff-Bulman, R., & Alpert, N. (1996). Approach versus avoidance goals: Differences in self-evaluation and well-being. Personality and Social Psychology Bulletin, 22, 1057-1067.
Cohen, S., & Wills T.A., (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98, 310-357.
Cooper, C.L., & Marshall, J. (1976). Occupational sources of stress: A review of the literature relating to coronary heart disease and mental ill health. Journal of Occupational Psychology, 49, 11-28.
Cooper, C.L., Dewe, P.J., & O’Driscoll, M.P. (2001). Organizational Stress: A Review and Critique of Theory, Research, and Applications. Thousand Oaks CA: Sage.
Cox, T., Griffiths, A., Barlow, C.A., Randall, R., Thomson, L, & Rial-Gonzalez, E. (2000). Organisational Interventions for Work Stress: A Risk Management Approach. HSE Books: Sudbury.
Coyne, J.C. (1976). Depression and the response of others. Journal of Abnormal Psychology, 85, 186-193.
Cramer, P. (2000). Defense mechanisms in psychology today: further process for adaptation. American Psychologist, 55, 637-646.
Cummings, T.G., & Cooper, C.L. (1979). A cybernetic framework for studying occupational stress. Human Relations, 32, 395-418.
117

Dalgleish, T., & Watts, F.N. (1990). Biases of attention and memory in disorders of anxiety and depression. Clinical Psychology Review, 10, 589-604.
Daniels, K (1996). Why aren’t managers concerned about occupational stress? Work & Stress, 10, 352-366.
Daniels, K. (1999). Coping and the job demands-control-support model: an exploratory study. International Journal of Stress Management, 6, 125-144.
Daniels, K. (2000). Measures of five aspects of affective well-being at work. Human Relations, 53, 275-294.
Daniels K., de Chernatony, L., & Johnson, G. (1995). Validating a method for mapping managers' mental models of competitive industry structures. Human Relations, 47, 975-991.
Daniels, K., & Guppy A. (1997). Stressors, locus of control and social support as consequences of psychological well-being. Journal of Occupational Health Psychology, 2, 156-174.
Daniels, K., & Guppy, A. (1994). Occupational stress, social support, job control and psychological well-being. Human Relations, 47, 1523-1544.
Daniels, K., Harris, C., Briner, R. (2002). Understanding the Risks of Stress: A Cognitive Approach. Sudbury: HSE Books.
Daniels, K., Harris, C., & Briner, R.B. (2003). Linking coping behaviours to coping functions. Manuscript submitted for publication.
Daniels, K., Johnson, G., & de Chernatony, L. (2002). Task and institutional influences on managers' mental models of competition. Organization Studies, 23, 31-62.
Danna, K., & Griffin, R.W. (1999). Health and well-being in the workplace: a review of the literature and synthesis of the literature. Journal of Management, 25, 357-384.
De Rijk, A.E., Le Blanc, P., Schaufeli, W., & Jonge, J. de (1998). Active coping and need for control as moderators of the job-demand-control model: effects on burnout. Journal of Occupational and Organizational Psychology, 71, 1-18
Depue, R.A., & Monroe, S.M. (1986). Conceptualization and measurement of human disorder in life stress research. Psychological Bulletin, 99, 36-51.
Diener, E. (1984). Subjective well-being. Psychological Bulletin, 95, 542-575.
Diener, E., & Fujita, F. (1995). Resources, personal strivings, and subjective wellbeing: A nomothetic and idiographic approach. Journal of Personality and Social Psychology, 68, 926-935.
118

Diener, E., & Larsen, R.J. (1993). The experience of emotional well-being. In M.Lewis & J.M. Havilland (Eds.), Handbook of Emotions. New York: Guildford Press.
Diener, E., Suh, E.M., Lucas, R.E., & Smith, H.L. (1999). Subjective well-being: three decades of progress. Psychological Bulletin, 125, 276-302.
Dubé, L., & Le Bel, J.L. (2003). The content and structure of laypeople’s concept of pleasure. Cognition & Emotion, 17, 263-295.
Dutton, J.E. (1993). Interpretations on automatic: a different view of strategic issue diagnosis. Journal of Management Studies, 30, 339-357
Edwards, J.R. (1992). A cybernetic theory of stress, coping, and well-being in organizations. Academy of Management Review, 17, 238-274.
Edwards, J.R., & Baglioni, A.J. (1993). The measurement of coping with stress: construct validity of the ways of coping checklist and the cybernetic coping scale. Work & Stress, 7, 17-31.
Elliot, A.J., & Sheldon, K.M. (1997). Avoidance achievement motivation: a person goal analysis. Journal of Personality and Social Psychology, 73, 171-185.
Elliot, A.J., Sheldon, K.M., & Church, M.A. (1997). Avoidance personal goals and subjective well-being. Personality and Social Psychology Bulletin, 23, 915927.
Emmons, R. (1986). Personal strivings: an approach to personality and subjective well-being. Journal of Personality and Social Psychology, 51, 1058-1068.
Erber, R., & Erber, M.W. (2001). Mood and processing: a view from a self-regulation perspective. In L.L. Martin & G.L. Clore (Eds.), Theories of Mood and Cognition: A User’s Handbook (pp 63-84). Mahwah, NJ: Erlbaum.
Epstein, S. (1994). Integration of the cognitive and psychodynamic unconscious. American Psychologist, 49, 709-724.
Ettner, S.L., & Grzywacz, J.G. (2001). Workers’ perceptions of how jobs affect health: a social ecological perspective. Journal of Occupational Health Psychology, 6, 101-113.
Eysenck, M.W., Keane, M.T. (1990). Cognitive Psychology: A Student’s Handbook. London: Erlbaum.
Fehr, B., & Russell, J.A. (1984). Concept of emotion viewed from a prototype perspective. Journal of Experimental Psychology: General, 113, 464-86.
Fiedler, K., & Bless, H. (2000). The formation of beliefs at the interface of affective and cognitive processes. In N.H.Frijda, A.S.R. Manstead & S. Bem (Eds.), Emotions and Beliefs: How Feelings Influence Thoughts (pp 144-170). Paris: Cambridge University Press.
119

Fisher, C.D. (1993). Boredom at work: a neglected concept. Human Relations, 46, 395-417.
Fisher, C.D. (1998). Effects of external and internal interruptions on boredom at work: two studies. Journal of Organizational Behavior, 19, 503-522.
Fisher, C.D. (2000). Mood and emotions while working: missing pieces of job satisfaction. Journal of Organizational Behavior, 21, 185-202.
Fisher, C.D. (2002). Antecedents and consequences of real-time affective reactions to work. Motivation and Emotion, 26, 3-30.
Fisher, C.D., & Ashkanasy, N.M. (2000). The emerging role of emotions in work life: an introduction. Journal of Organizational Behavior, 21, 123-129.
Fletcher, B.C., & Jones, F. (1993). A refutation of Karasek's demand-discretion model of occupational stress with a range of dependent measures. Journal of Organizational Behavior, 14, 319-330.
Folkman, S., & Moskowitz, J.T. (2000). Positive affect and the other side of coping. American Psychologist, 55, 647-654.
Forgas, J.P. (2000). Feeling is believing? the role of processing strategies in mediating affective influences on beliefs. In N.H.Frijda, A.S.R. Manstead & S. Bem (Eds.), Emotions and Beliefs: How Feelings Influence Thoughts (pp 108-143). Paris: Cambridge University Press.
Forgas, J.P. (2001). Affect, cognition, and interpersonal behavior: the mediating role of processing strategies. In J.P.Forgas (Ed.), Handbook of Affect and Social Cognition (pp 293-318). New Jersey: Erlbaum
Forgas, J.P. (2001). The affect infusion model (AIM); an integrative theory of mood effects on cognition and judgments. In L.L. Martin & G.L. Clore (Eds.), Theories of Mood and Cognition: A User’s Handbook (pp 99-134). Mahwah, NJ: Erlbaum.
Fox, M.L., Dwyer, D.J., & Ganster, D.C. (1993). Effects of stressful job demands and control on physiological and attitudinal outcomes in a hospital setting. Academy of Management Journal, 36, 289-318.
Frese, M. (1999). Social support as a moderator of the relationship between work stressors and psychological dysfunctioning: a longitudinal study with objective measures. Journal of Occupational Health Psychology, 4, 179-192.
Frese, M., & Zapf, D. (1988). Methodological issues in the study of work stress: objective vs subjective measurement work stress and the question of longitudinal studies. In C.L.Cooper & R.Payne (Eds.), Causes, Coping, and Consequences of Stress at Work (pp 375-411). Chichester: Wiley.
Frese, M., & Zapf, D. (1994). Action as the core of work psychology: a German approach. In H.C. Triandis, M.D. Dunnette, L.M. Hough (Eds.), Handbook of
120

Industrial and Organizational Psychology, 2nd ed (pp 272-340). Palo Alto, CF: Consulting Psychologists Press.
Freud, S. (1959). Beyond the Pleasure Principle. New York: Norton.
Frijda, N.H. (1986). The Emotions. Cambridge: Cambridge University Press.
Frijda, N.H., Manstead, A.S.R., & Bem, S. (Eds.) (2000). Emotions and Beliefs: How Feelings Influence Thoughts. Cambridge: Cambridge University Press.
Frijda, N.H., & Mesquita, B. (2000). Beliefs through emotions. In N.H.Frijda, A.S.R. Manstead & S. Bem (Eds.), Emotions and Beliefs: How Feelings Influence Thoughts (pp 45-77). Paris: Cambridge University Press.
Ganster, D.C., Fusilier, M.R., & Mayes, B.T. (1986). Role stress of social support in the experience of stress at work. Journal of Applied Psychology, 71, 102-110.
Goldstone, R.L. (1994). The role of similarity in categorization: Providing a groundwork. Cognition, 52, 125-157.
Gomez, P-Y., & Jones, B.C. (2000). Conventions: an interpretation of deep structure in organizations. Organization Science, 11, 969-708.
Gump, B.B., & Kulik, J.A. (1997). Stress, affiliation, and emotional contagion. Journal of Personality and Social Psychology, 72, 305-319.
Gurtman, M.B., Martin, K.M., & Hintzman. N.M. (1990). Interpersonal reactions to displays of depression and anxiety. Journal of Social and Clinical Psychology, 9, 256-267.
Hacker, W. (1982). Objective and subjective organization of work activities. In M. von Cranach & R. Harré (Eds.) The Analysis of Action (pp 81-97). Cambridge: Cambridge University Press.
Hackman, J.R., & Oldham, G.R. (1980). Work Redesign. Reading, MA: Addison Wesley.
Halberstadt, J.B., & Niedenthal, P.M. (1997). Emotional state and the use of stimulus dimensions in judgment. Journal of Personality and Social Psychology, 72, 1017-1033.
Harris, C., Daniels, K., & Briner, R. (in press). A daily diary study of goals and affective well-being at work. Journal of Occupational and Organizational Psychology.
Hartlage, S., Alloy, L.B., Vazquez, C., & Dykman, B. (1993). Automatic and effortful processing in depression. Psychological Bulletin, 113, 247-278.
Haslam, N. (1995). The discreteness of emotion concepts: categorical structure in the affective circumplex. Personality and Social Psychology Bulletin, 21, 10121019.
121

Hemenover, S.H. (2001). Self-reported processing bias and naturally occurring mood: mediators between personality and stress appraisals. Personality and Social Psychology Bulletin, 4, 387-394.
Herzberg, F. (1966). Work and the Nature of Man. London: Staples Press.
Hertel, P.T. (2002). Cognitive biases in anxiety and depression: introduction to the special issue. Cognition and Emotion, 16, 321-330.
Higgins, E.T. (1997). Beyond pleasure and pain. American Psychologist, 52, 12801300.
Hobfoll, S.E. (2001). The influence of culture, community, and the nested-self in the stress process: advancing conservation of resources theory. Applied Psychology: An International Review, 50, 337-369.
Hodgkinson, G.P. (2003). The interface of cognitive and industrial, work and organizational psychology. Journal of Occupational and Organizational Psychology, 76, 1-26.
Hodgkinson, G.P., & Sparrow, P.R. (2002). The Competent Organization. Buckingham: Open University Press.
Holman, D.J., & Wall, T.D. (2002). Work characteristics, learning-related outcomes, and strain: a test of competing direct effects, mediated, and moderated models. Journal of Occupational Health Psychology, 7, 283-301.
Horn, J.E. van, Taris, T.W., Schaufeli, W.B., & Schreurs, P.J.G. (in press). The structure of occupational well-being: a study among Dutch teachers. Journal of Occupational and Organizational Psychology.
Horowitz, M. (1979). Psychological response to serious life events. In V.Hamilton & D.M. Warburton (Eds.), Human Stress and Cognition: An Information Processing Approach, (pp. 237-265). New York: Wiley.
House, J.S. (1981). Work Stress and Social Support. Reading MA: Addison-Wesley.
Hyland, M.E. (1988). Motivational control theory: an integrative framework. Journal of Personality and Social Psychology, 55, 642-651.
Jackson, P.R., Wall, T.D., Martin, R., & Davids, K. (1993). New measures of job control, cognitive demand, and production responsibility. Journal of Applied Psychology, 78, 753-762.
Jex, S.M. (1998). Stress and Job Performance: Theory, Research, and Implications for Management Practice. Thousand Oaks CA: Sage.
Johnson, T.P. (1991). Mental health, social relations, and social selection: a longitudinal analysis. Journal of Health and Social Behavior, 32, 408-423
Johnson-Laird, P.N. (1983). Mental Models. Cambridge, UK: Cambridge University Press.
122

Johnson-Laird, P.N. (1989). Mental models. In M.I. Posner (Ed.), Foundations of Cognitive Science, (pp. 469-499). Cambridge, MA: MIT Press.
Jonge, J. de, & Dormann, C. (2002). The DISC model: demand induced strain compensation mechanisms in job stress. In M.F. Dollard, H.R. Winefield & A.H. Winefield (Eds.), Occupational Stress in the Service Professions. London: Taylor & Francis.
Jonge, J. de, Dormann, C., Janssen, P.P.M., Dollard, M.F., Landerweerd, J.A., & Nijhuis, F.J.N. (2001). Testing reciprocal relationships between job characteristics and psychological well-being: A cross-lagged structural equation model. Journal of Occupational and Organizational Psychology, 74, 1-28.
Kanfer, R. (1992). Work motivation: new directions in theory and research. In C.L.Cooper & I.T. Robertson (Eds.), International Review of Industrial and Organizational Psychology, (vol. VII, pp. 1-53). New York: Wiley.
Kanfer, R., & Ackerman, P.L. (1989). Motivation and cognitive abilities: an integrative/aptitude-treatment interaction approach to skill acquisition. Journal of Applied Psychology, 74, 657-690.
Karasek, R.A., & Theorell, T. (1990). Healthy Work. New York: Basic Books.
Kaufman, G.H., & Beehr, T.A. (1989). Occupational stressors, individual strains, and social supports among police officers. Human Relations, 42, 185-197.
Kaufman, G.M., & Beehr, T.A. (1986). Interactions between job stressors and social support – some counterintuitive results. Journal of Applied Psychology, 71, 522-526.
Kehr, H.M. (2003). Goal conflicts, attainment of new goals, and well-being among managers. Journal of Occupational Health Psychology, 8, 195-208.
Keil, F.C., Smith, W.C., Simons, D.J., & Levin, D.T. (1998). Two dogmas of conceptual empiricism: Implications for hybrid models of the structure of knowledge. Cognition, 65, 103-135.
Kelly, J.R., & Barsade, S.G. (2001). Mood and emotions in small groups and work teams. Organizational Behavior and Human Decision Processes, 86, 99-130.
Kersten, A.W., & Billman, D. (1997). Event category learning. Journal of Experimental Psychology: Learning, Memory, and Cognition, 23, 638-658.
King, L.A., Richards, J.H., & Stemmerich, E. (1998). Daily goals, life goals, and worst fears: Means, ends, and subjective well-being. Journal of Personality, 66, 713-744.
Kirmeyer, S.L., & Dougherty, T.W. (1988). Work load, tension, and coping: Moderating effects of supervisor support. Personnel Psychology, 41, 125-139.
123

Krueger, J., & Clement, R.W. (1994). Memory-based judgments about multiple categories: A revision and extension of Tajfel’s accentuation theory. Journal of Personality and Social Psychology, 67, 35-47.
Lamberts, K. (1996). Exemplar models and prototype effects in similarity based categorization. Journal of Experimental Psychology: Learning, Memory, and Cognition, 22, 1503-1507.
Lang, P.J. (1984). Cognition in emotion: Concept and action. In C.E.Izard, R.R. Zajonc & J. Kagan (Eds.), Emotions, Cognitions and Behaviour, (pp. 192226). Cambridge: Cambridge University Press.
Lang, P.J. (1985). The cognitive psychophysiology of emotion? Fear and anxiety. In A.H. Tuma & J.D. Maser (Eds.), Anxiety and the Anxiety Disorders, (pp 131170). Hillsdale NJ: Erlbaum.
Lang, P.J. (1988). What are the data of emotion. In V.Hamilton, G.H.Bower & N Frijda (Eds.), Cognitive Perspectives on Emotion and Motivation (NATO ASI Series D Vol. XXXXIV, pp. 173-191). Dordrecht: Kluwer.
Lassiter, G.D., Koenig, L.J., & Apple, K.J. (1996). Mood and behavior perception: dysphoria can increase and decrease effortful processing of information. Personality and Social Psychology Bulletin, 22, 794-810.
Latack, J.C. (1986). Coping with job stress: measures and future directions for scale development. Journal of Applied Psychology, 71, 377-385.
Latack, J.C., & Havlovic, S.J. (1992). Coping with job stress: a conceptual evaluation framework for coping measures. Journal of Organizational Behavior, 13, 479508.
Latack, J.C., Kinicki, A.J., & Prussia, G.E. (1995). An integrative process model of coping with job loss. Academy of Management Review, 20, 311-342
Lavallee, L.F., & Campbell, J.D. (1995). Impact of personal goals on self-regulation processes elicited by daily negative events. Journal of Personality and Social Psychology, 69, 341-352.
Lawrence, J.W., Carver, C.S., & Scheier, M.F. (2002). Velocity toward goal attainment in immediate experience as a determinant of affect. Journal of Applied Social Psychology, 32, 788-802.
Lazarus, R.S. (1991). Emotion and Adaptation. New York: Oxford University Press.
Lazarus, R.S. (1999). Stress and Emotion: A new synthesis. New York: Springer.
Lazarus, R.S., & Folkman, S. (1984). Stress, Appraisal, and Coping. New York: Springer.
Lingle, J.H., & Ostrom, T.M. (1980). Principles of memory and cognition in attitude formation. In R.Petty, T.Ostrom & T.Brock (Eds.), Cognitive Responses in Persuasion (pp 399-423). Hillsdale NJ: Erlbaum.
124

Locke, E.A. (1994) The emperor is naked. Applied Psychology: An International Review, 43, 367-370.
Locke, E.A., & Henne, D. (1986). Work motivation theories. In C.L.Cooper & I.T. Robertson (Eds.), International Review of Industrial and Organizational Psychology, (vol. II, pp. 1-35). New York: Wiley.
Locke, E.A., & Latham, G.P. (1990). A Theory of Goal Setting and Task Performance. Englewood Cliffs NJ: Prentice Hall.
Lord, R.G., & Levy, P.E. (1994). Moving from cognition to action: a control theory perspective. Applied Psychology: An International Review, 43, 335-367.
Lord, R.G., & Harvey, J.L. (2002). An information processing framework for emotional regulation. In R.G. Lord, R.J. Klimoski & R. Kanfer, Emotions in the Workplace: Understanding the Structure and Role of Emotions in Organizational Behavior (pp 116-146). New York: Jossey Bass
Lord, R.G., Klimoski, R.J., & Kanfer, R. (2002). Emotions in the Workplace: Understanding the Structure and Role of Emotions in Organizational Behavior. New York: Jossey Bass.
MacCleod, C. (1991). Clinical anxiety and the selective encoding of threatening information. International Review of Psychiatry, 3, 279-292.
Maddi, S.R., & Kobassa, S.C. (1984). The Hardy Executive: Health Under Stress. Pacific Grove CA: Brooks/Cole.
Maier, G. W., & Brunstein, J. C. (2001). The role of personal goals in newcomers job satisfaction and organizational commitment: A longitudinal analysis. Journal of Applied Psychology, 86, 1034-1042.
Mandler, G. (1984). Mind and Body: Psychology of Emotion and Stress. New York: Norton.
Martin, L.L. (2001). Mood as input: a configural view of mood effects. In L.L. Martin & G.L. Clore (Eds.), Theories of Mood and Cognition: A User’s Handbook (pp 135-158). Mahwah, NJ: Erlbaum.
Maslow, A.H. (1954). Motivation and Personality. New York: Harper & Row.
Matt, G.E., Vazquez, C., & Campbell, W.K. (1992). Mood-congruent recall of affectively toned stimuli: a meta-analytic review. Clinical Psychology Review, 12, 227-255.
Mayo, E. (1933). The Human Problems of Industrial Civilization. New York: MacMillan.
Medin, D.L., Goldstone, R.L., & Getner, D. (1993). Respects for similarity. Psychological Review, 100, 254-278.
125
Medin, D.L., Lynch, E.B., & Solomon, K.O., (2000). Are there kinds of concepts? Annual Review of Psychology, 51, 121-147.
Mervis, C.B., & Rosch, E. (1981). Categorization of natural objects. Annual Review of Psychology, 32, 89-115.
Moos, R.H., & Billings, A.G. (1982). Conceptualizing and measuring coping resources and processes. In L.Goldberger & S. Berznitz (Eds.), Handbook of Stress: Theoretical and Clinical Aspects, (pp. 212-230). New York: Free Press.
Morris, M.W., & Murphy, G.L. (1990). Converging operations on a basic level in event taxonomies. Memory and Cognition, 18, 407-418.
Morrison, D., Payne, R.L., & Wall, T.D. (2003). Is job a viable unit of analysis? A multilevel analysis of demand-control-support models. Journal of Occupational Health Psychology, 8, 209-219.
Moyle, P. (1995). The role of negative affectivity in the stress process: tests of alternative methods. Journal of Organizational Behavior, 16, 647-668.
Muchinsky, P.M. (2000). Emotions in the workplace: The neglect of organizational behavior. Journal of Organizational Behavior, 21, 801-805.
Mullarkey, S., Jackson, P.R., Wall, T.D., Wilson, J.R., & Grey-Taylor, S.M. (1997). The impact of technology characteristics and job control on worker mental health. Journal of Organizational Behavior, 18, 471-489.
Murphy, G.L., & Medin, D.L. (1985). The role of theories in conceptual coherence. Psychological Review, 92, 289-316.
Neumann, R., & Strack, F. (2000). “Mood contagion”: The automatic transfer of mood between persons. Journal of Personality and Social Psychology, 79, 211-223.
Nicholson, N. (1997). Evolutionary psychology: toward a new view of human nature and organizational society. Human Relations, 50, 1053-1078.
Niedenthal, P.M., Halberstadt, J.B., & Innes-Ker, Å.H. (1999). Emotional response categorization. Psychological Review, 106, 337-361.
Nosofsky, R.M., Palmeri, T.J., & McKinley, S.C. (1994). Rule-plus-exception model of classification learning. Psychological Review, 101, 53-79.
Oatley, K. (2000). The sentiments and beliefs of distributed cognition. In N.H.Frijda, A.S.R. Manstead & S. Bem (Eds.), Emotions and Beliefs: How Feelings Influence Thoughts (pp 212-240). Paris: Cambridge University Press.
Oatley, K., & Johnson-Laird, P. (1987). Towards a cognitive theory of emotions. Cognition and Emotion, 1, 29-50.
126

Ortony, A., Clore, G.L., & Collins, A. (1988). The Cognitive Structure of Emotions. Cambridge: Cambridge University Press.
Parkinson, B. (1995). Ideas and Realities of Emotion. London: Routledge.
Parkinson, B., Briner, R.B., Reynolds, S., & Totterdell, P. (1995). Time frames for mood: relations between momentary and generalized ratings of affect. Personality and Social Psychology Bulletin, 21, 331-339.
Parry, G. (1988). Mobilizing social support. In F.N.Watts (Ed.), New Developments in Clinical Psychology (Vol. II, pp. 83-104). Chichester: Wiley.
Payne, R.L., & Cooper, C.L. (2001). Emotions at Work: Theory, Research and Applications in Management. Chichester: Wiley.
Payne, R.L., & Fletcher, B.C. (1983). Job demands, supports, and constraints as predictors of psychological strain among schoolteachers. Journal of Vocational Behavior, 22, 136-147.
Payne, R.L., Wall, T.D., Borrill, C., & Carter, A. (1999). Strain as a moderator of the relationship between work characteristics and work attitudes. Journal of Occupational Health Psychology, 4, 3-14.
Pearlin L.I., & Schooler, C. (1978). The structure of coping. Journal of Health and Social Behavior, 19, 2-21.
Pekrun, R., & Frese, M. (1992). Emotions in work and achievement. In C.L.Cooper & I.T. Robertson (Eds.), International Review of Industrial and Organizational Psychology, (vol. VII, pp. 153-200). New York: Wiley.
Perrewé, P.L., & Zellars, K.L. (1999). An examination of attributions and emotions in the transactional approach to the organizational stress process. Journal of Organizational Behavior, 20, 739-7512.
Peterson, M.F. (1998). Embedded organizational events: the units of process in organization science. Organization Science, 9, 16-33.
Pillow, D.R., Zautra, A.J., & Sandler, I. (1996). Major life events and minor stressors: identifying mediational links in the stress process. Journal of Personality and Social Psychology, 70, 381-394.
Porac, J.F., & Thomas H. (1994). Cognitive categorization and subjective rivalry among retailers in a small city. Journal of Applied Psychology, 79, 54-66
Power, M., & Dalgleish, T. (1997). Cognition and Emotion: From Order to Disorder. Hove, East Sussex: Psychology Press.
Powers, W.T. (1973). Behavior: The Control of Perception. Chicago: Aldine.
Rick, J., Thomson, L., Briner, R., O’Regan, S., & Daniels, K. (2002). Review of Existing Scientific Knowledge to Underpin Standards of Good Practice for Key Work-Related Stressors – Phase 1. Sudbury: HSE Books.
127

Rifkin, A. (1985). Evidence for a basic level in event taxonomies. Memory and Cognition, 13, 538-556.
Robinson, M.D. (2000). The reactive and prospective functions of mood: its role in linking daily experiences and cognitive well-being. Cognition and Emotion, 14, 145-176.
Rogers, C.R. (1959). A theory of therapy, personality, and interpersonal relationships, as developed in the client-centered framework. In S. Koch (Ed.), Psychology: A Study of a Science (vol. III, pp. 184-256). New York: McGraw Hill.
Ronen, S. (1994). An underlying structure of motivational need taxonomies: a crosscultural confirmation. In H.C. Triandis, M.D. Dunnette, L.M. Hough (Eds.), Handbook of Industrial and Organizational Psychology, 2nd ed (pp 241-269). Palo Alto, CF: Consulting Psychologists Press.
Roney, C.J.R., Higgins, E.T., & Shah, J. (1995). Goals and framing: how outcome focus influences motivation and emotion. Personality and Social Psychology Bulletin, 21, 1151-1160.
Roth, S., & Cohen, L.J. (1986). Approach, avoidance, and coping with stress. American Psychologist, 41, 813-819.
Rumelhart, D.E. (1989). The architecture of mind: a connectionist approach. In M.Posner (Ed.), Foundations of Cognitive Science, (pp 1-47). Cambridge MA: MIT Press.
Russell, J.A. (2003). Core affect and the psychological construction of emotion. Psychological Review, 110, 145-172.
Rusting, C.L. (1998). Personality, mood, and cognitive processing of emotional information: three conceptual frameworks. Psychological Bulletin, 124, 165196.
Ryan, R.M. (1995). Psychological needs and the facilitation of integrative processes. Journal of Personality, 63, 432-444.
Ryff, C.D., & Keyes, C.L.M. (1995). The structure of psychological well-being revisited. Journal of Personality and Social Psychology, 69, 719-727.
Sargent, L.D., & Terry, D.J. (1998). The effects of work control and job demands on employee adjustment and work performance. Journal of Occupational and Organizational Psychology, 71, 219-236.
Schacter, D.L. (1989). Memory. In M.I.Posner (Ed.), Foundations of Cognitive Science (pp 683-725). Cambridge MA: MIT Press.
Schank, R.C. (1982). Dynamic Memory: A Theory of Reminding and Learning in Computers and People. Cambridge: Cambridge University Press.
Schank, R.C. (1986). Explanation Patterns. Hillsdale: NJ; Erlbaum.
128

Schaubroeck, J., & Merritt, D.E. (1997). Divergent effects of job control on coping with work stressors: the key role of self-efficacy. Academy of Management Journal, 40, 738-754.
Schein, E.HG. (1978). Career Dynamics: Molding Individual and Organizational Needs. Reading MA: Addison-Wesley.
Schneider, B.C. (1987).The people make the place. Personnel Psychology, 40, 437-53
Schneider, W., & Shiffrin, R.M. (1977). Controlled and automatic human information processing: I. detection, search, and attention. Psychological Review, 84, 1-66.
Schönpflug, W., & Battmann, W. (1988). The costs and benefits of coping. In S.Fisher & J.Reason (Eds.), Handbook of Life Stress, (pp. 699-713). Chichester: Wiley.
Schuler, R.S. (1985). Integrative transactional process model of coping with stress in organizations. In T.A.Beehr & R.S. Bhagat (Eds.), Human Stress and Cognition in Organizations: An Integrated Perspective (pp 347-374). New York: Wiley.
Schwarz, N. (2000). Emotion, cognition, and decision making. Cognition and Emotion, 14, 433-440.
Sheldon, K.M., & Elliot, A.J. (1999). Goal striving, need satisfaction, and longitudinal well-being: The self-concordance model. Journal of Personality and Social Psychology, 76, 482-497.
Sheldon, K.M., & Kasser, T. (1998). Pursuing personal goals: Skills enable progress but not all progress is beneficial. Personality and Social Psychology Bulletin, 24, 1319-1331.
Skinner, E.A., Edge, K., Altman, J., & Sherwood, H. (2003). Searching for the structure of coping: a review and critique of category systems for classifying ways of coping. Psychological Bulletin, 129, 216-269.
Sloman, S.A. (1996). The empirical case for two systems of reasoning. Psychological Bulletin, 119, 3-22.
Smith E.E., & Medin, D.L. (1981). Categories and Concepts. Cambridge MA: Harvard University Press.
Smith, C.A., & Kirby, L.D. (2001). Affect and cognitive appraisal processes. In J.P.Forgas (Ed.), Handbook of Affect and Social Cognition (pp 75-92). New Jersey: Erlbaum.
Smith, E.E., Patalano, A.L., & Jonides, J. (1998). Alternative categories of categorization. Cognition, 65, 167-196.
Smith, R.E., Leffingwell, T.R., & Ptacek, J.T. (1999). Can people remember how they coped? Factors associated with discordance between same-day and
129
retrospective reports. Journal of Personality and Social Psychology, 76, 10501061.
Sparrow, P. (2003). The future of work? In Holman, D., Wall T.D., Clegg, C.W., Sparrow, P.R, Howard (Eds.), The New Workplace: People, Technology and Organization: A Handbook and Guide to the Human Impact of Modern Working Practices (pp 371-392). Chichester: Wiley.
Spector, P.E. (1987). Interactive effects of perceived control and job stressors on affective reactions and health outcomes for clerical workers. Work & Stress, 1, 155-162.
Spector, P.E., & Goh, A. (2001). The role of emotions in the occupational stress process. Exploring Theoretical Mechanisms and Perspectives, 1, 195-232.
Spector, P.E., Jex, S.M., & Chen, P.Y. (1995). Relations of incumbent affect-related personality traits with incumbent and objectives measures of characteristics of jobs. Journal of Organizational Behavior, 16, 59-65.
Spector, P.E., Zapf, D., Chen, P.Y., & Frese M. (2000). Why negative affectivity should not be controlled in job stress research: don’t throw the baby out with the bath water. Journal of Organizational Behavior, 21, 79-95.
Staw, B.M., Sutton, R.I., & Pelled, L.H. (1994). Employee positive emotion and favorable outcomes at the workplace. Organization Science, 5, 51-71.
Suh, E., Diener, E., & Fujita, F. (1996). Events and subjective well-being: Only recent events matter. Journal of Personality and Social Psychology, 70, 1091-1102.
Suls, J. (2001). Affect, stress, and personality. In J.P.Forgas (Ed.), Handbook of Affect and Social Cognition (pp 392-409). New Jersey: Erlbaum.
Terry, D.J., & Jimmieson, N.L. (1999). Work control and employee well-being: A decade review. In C.L.Cooper & I.T. Robertson (Eds.), International Review of Industrial and Organizational Psychology (Vol. XIV, pp. 95-148). Chichester: Wiley.
Theorell, T., & Karasek, R.A. (1996). Current issues relating to psychosocial job strain and cardiovascular disease research. Journal of Occupational Health Psychology, 1, 9-26.
Totterdell, P. (2000). Catching moods and hitting runs: Mood linkage and subjective performance in professional sport teams. Journal of Applied Psychology, 85, 848-859.
Totterdell, P., Kellett, S., Teuchmann, K., & Briner, R.B. (1998). Evidence of mood linkage in work groups. Journal of Personality and Social Psychology, 74, 1504-1515.
Walsh, J.P. (1995). Managerial and organizational cognition: Notes from a trip down memory lane. Organization Science, 6, 280-321.
130

Warr, P.B. (1987). Work, Unemployment and Mental Health. Oxford: Oxford University Press.
Warr, P.B. (1990). The measurement of well-being and other aspects of mental health. Journal of Occupational Psychology, 63, 193-210.
Warr, P. (1994). A conceptual framework for the study of work and mental health. Work & Stress, 8, 84-97.
Warr, P.B. (1999). Well-being and the workplace. In D.Kahneman, E.Diener & N.Schwarz (Eds.), Well-Being: The Foundations of Hedonic Psychology, (pp. 392-412). New York: Russell Sage Foundation.
Watson, D., & Tellegen, A. (1985). Toward a consensual structure of mood. Psychological Bulletin, 98, 219-235
Watson, D., Clark, L.A., & Carey, G. (1988). Positive and negative affectivity and their relation to anxiety and depressive disorders. Journal of Abnormal Psychology, 97, 346-353.
Watson, D., Clark, L.A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: the PANAS scales. Journal of Personality and Social Psychology, 54, 1063-1070
Watson, D., Wiese, D., Vaidya, J., & Tellegen, A. (1999). The two general activation systems of affect: structural findings, evolutionary considerations, and psychobiological evidence. Journal of Personality and Social Psychology, 76, 820-838.
Watt, J.D., & Blanchard, M.J., (1994). Boredom proneness and the need for cognition. Journal of Research in Personality, 28, 44-51.
Wegener, D.T., & Petty, R.E. (2001). Understanding the effects of mood through the elaboration of likelihood and flexible correction models. In L.L. Martin & G.L. Clore (Eds.), Theories of Mood and Cognition: A User’s Handbook (pp 177-210). Mahwah, NJ: Erlbaum.
Weick, K.E. (1995). Sensemaking in Organizations. Thousand Oaks CA: Sage.
Weiner, B. (1986). An Attribution Theory of Motivation and Emotion. New York: Springer.
Weiss, H.M. (2001). Introductory comments. Organizational Behavior and Human Decision Processes, 86, 1-2.
Weiss, H.M. (2002). Introductory comments: antecedents of emotional experiences at work. Motivation and Emotion, 26, 1-2.
Weiss, H.M., & Brief, A.P. (2001). Affect at work: a historical perspective. In R.L. Payne & C.L. Cooper (Eds.). Emotions at Work: Theory, Research and Applications in Management (pp 133-170). Chichester: Wiley.
131

Weiss, H.M., & Cropanzano, R. (1996). Affective events theory: A theoretical discussion of the structure, causes, and consequences of affective experiences at work. In B.M. Staw and L.L. Cummings (Eds.), Research in Organizational Behavior, (Vol. XVIII, pp. 1-74). Greenwich CT: JAI Press.
Wenzlaff, R.M., & Bates, D.E. (1998). Unmasking a cognitive vulnerability to depression: how lapses in mental control reveal depressive thinking. Journal of Personality and Social Psychology, 75, 1559-1571.
Wicker, F.W., Lambert, F.B., Richardson, F.C., & Kahler, J. (1984). Categorical goal hierarchies and classification of human motives. Journal of Personality, 52, 285-305.
Williams, J.M.G., Watts, F.N., MacLeod, C., & Mathews, A. (1996). Cognitive Psychology and Emotional Disorders (2nd edn.). Chichester: Wiley.
Wisniewski, E.J., & Murphy, G.L. (1989). Superordinate and basic category names in discourse: a textual analysis. Discourse Processes, 12, 245-261.
Wofford, J.C., & Daly, P.S. (1997). A cognitive-affective approach to understanding stress propensity. Journal of Occupational Health Psychology, 2, 134-147.
Wofford, J.C., Goodwin, V.L., & Daly, P.S. (1999). Cognitive-affective stress propensity: a field study. Journal of Organisational Behavior, 20, 687-707.
Wright, T.A., & Cropanzano, R. (2000). The role of organisational behavior in occupational health psychology: A view as we approach the millennium. Journal of Occupational Health Psychology, 5, 5-11.
Zajonc, R.B. (1980). Feeling and thinking: Preferences need no inferences. American Psychologist, 35, 151-175.
Zellars, K.L., Perrewé, P.L., & Hochwarter, W.A. (1999). Mitigating burnout among high-NA employees in health care: what can organisations do? Journal of Applied Social Psychology, 29, 2250-2271.
132

Printed and published by the Health and Safety ExecutiveC30 1/98
Printed and published by the Health and Safety ExecutiveC1.10 03/04

9 78071 7 627707
ISBN 0-7176-2770-5
RR 170
£20.00


















