
Research Article A Two-Tube Multiplex Reverse...
9
Hindawi Publishing Corporation BioMed Research International Volume 2013, Article ID 327620, 8 pages http://dx.doi.org/10.1155/2013/327620 Research Article A Two-Tube Multiplex Reverse Transcription PCR Assay for Simultaneous Detection of Sixteen Human Respiratory Virus Types/Subtypes Jin Li, 1,2 Shunxiang Qi, 3 Chen Zhang, 1 Xiumei Hu, 1 Hongwei Shen, 1 Mengjie Yang, 1 Ji Wang, 1 Miao Wang, 1 Wenbo Xu, 1 and Xuejun Ma 1 1 Key Laboratory for Medical Virology, Ministry of Health, National Institute for Viral Disease Control and Prevention, Chinese Center for Disease Control and Prevention, No. 155, Changbai Road, Changping District, Beijing 102206, China 2 National Institute for Nutrition and Food Safety, Chinese Center for Disease Control and Prevention, Beijing 100050, China 3 Hebei Center for Disease Control and Prevention, No. 241, Qingyuan Street, Yuhua District, Shijiazhuang 050000, China Correspondence should be addressed to Wenbo Xu; wenbo [email protected] and Xuejun Ma; [email protected] Received 7 April 2013; Accepted 25 June 2013 Academic Editor: Gregory Tannock Copyright © 2013 Jin Li et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ere is a need for the development of a rapid and sensitive diagnosis of respiratory viral pathogens. With an intended application in provincial Centers for Diseases Control and Prevention, in this study, we present a two-tube multiplex RT-PCR assay (two- tube assay) using automatic electrophoresis to simultaneously detect sixteen common respiratory viruses. e specificity and the sensitivity of the assay were tested. e assay could detect 20–200 copies per reaction when each viral type was assayed individually, 2000 copies with 9 premixed viral targets in the multiplexed assay in tube 1, and 200 copies with 8 premixed templates in tube 2. A total of 247 specimens were used to evaluate the two-tube assay, and the results were compared with those obtained from the Luminex xTAG RVP Fast assay. e discordant results were confirmed by sequencing or by the Seeplex RV15 ACE detection kit. ere were no false positives, but six false negatives occurred with the two-tube assay. In conclusion, the two-tube assay is demonstrated to have great potential for routine surveillance of respiratory virus infection in China. 1. Introduction Viral respiratory tract infections are a common cause of hospitalization and mortality in infants and young children. Influenza A, influenza B, parainfluenza, human rhinovirus, adenovirus, respiratory syncytial virus, metapneumovirus, and coronavirus are recognized as viral agents associated with respiratory tract infections [1–3]. erefore, there is a need for a rapid and sensitive differential diagnosis of respiratory viral pathogens to prevent nosocomial infections and to minimize unnecessary antibiotic usage [4–6]. Existing standard nonmolecular diagnostic methods such as viral culture and immunofluorescence (DFA) are time- consuming, labor intensive, or have low sensitivity [7, 8]. Accordingly, molecular techniques are increasingly accepted for diagnosis of viral respiratory tract infections. In the last few years, multiplex RT-PCR assays have been developed to detect respiratory viruses [9], and some have been commer- cialized, such as xTAG RVP from Luminex [10, 11], Multicode PLx RVP from EraGen Biosciences [12], and ResPlex II from Qiagen [13]. In our previous study, a multiplex PCR based on the GenomeLab Gene Expression Profiler (GeXP) analyzer had been shown to be effective for the detection of pandemic influenza A H1N1 virus [14], nine serotypes of enteroviruses associated with hand, foot, and mouth disease [15], and sixteen different respiratory virus types/subtypes in a single tube [16]. However, these methods are not likely to be widely adopted in provincial Centers for Disease Control and Prevention due to the limited availability of GeXP equip- ment. erefore, in this study, a two-tube multiplex reverse transcription PCR assay (twotube assay) to detect sixteen
Transcript of Research Article A Two-Tube Multiplex Reverse...
Hindawi Publishing CorporationBioMed Research InternationalVolume 2013 Article ID 327620 8 pageshttpdxdoiorg1011552013327620
Research ArticleA Two-Tube Multiplex Reverse Transcription PCRAssay for Simultaneous Detection of Sixteen HumanRespiratory Virus TypesSubtypes
Jin Li12 Shunxiang Qi3 Chen Zhang1 Xiumei Hu1 Hongwei Shen1 Mengjie Yang1
Ji Wang1 Miao Wang1 Wenbo Xu1 and Xuejun Ma1
1 Key Laboratory for Medical Virology Ministry of Health National Institute for Viral Disease Control and PreventionChinese Center for Disease Control and Prevention No 155 Changbai Road Changping District Beijing 102206 China
2National Institute for Nutrition and Food Safety Chinese Center for Disease Control and Prevention Beijing 100050 China3Hebei Center for Disease Control and Prevention No 241 Qingyuan Street Yuhua District Shijiazhuang 050000 China
Correspondence should be addressed to Wenbo Xu wenbo xu1yahoocomcn and Xuejun Ma maxjivdcchinacdccn
Received 7 April 2013 Accepted 25 June 2013
Academic Editor Gregory Tannock
Copyright copy 2013 Jin Li et al This is an open access article distributed under the Creative Commons Attribution License whichpermits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
There is a need for the development of a rapid and sensitive diagnosis of respiratory viral pathogens With an intended applicationin provincial Centers for Diseases Control and Prevention in this study we present a two-tube multiplex RT-PCR assay (two-tube assay) using automatic electrophoresis to simultaneously detect sixteen common respiratory viruses The specificity and thesensitivity of the assay were testedThe assay could detect 20ndash200 copies per reaction when each viral type was assayed individually2000 copies with 9 premixed viral targets in the multiplexed assay in tube 1 and 200 copies with 8 premixed templates in tube2 A total of 247 specimens were used to evaluate the two-tube assay and the results were compared with those obtained fromthe Luminex xTAG RVP Fast assay The discordant results were confirmed by sequencing or by the Seeplex RV15 ACE detectionkit There were no false positives but six false negatives occurred with the two-tube assay In conclusion the two-tube assay isdemonstrated to have great potential for routine surveillance of respiratory virus infection in China
1 Introduction
Viral respiratory tract infections are a common cause ofhospitalization and mortality in infants and young childrenInfluenza A influenza B parainfluenza human rhinovirusadenovirus respiratory syncytial virus metapneumovirusand coronavirus are recognized as viral agents associatedwithrespiratory tract infections [1ndash3]Therefore there is a need fora rapid and sensitive differential diagnosis of respiratory viralpathogens to prevent nosocomial infections and to minimizeunnecessary antibiotic usage [4ndash6]
Existing standard nonmolecular diagnosticmethods suchas viral culture and immunofluorescence (DFA) are time-consuming labor intensive or have low sensitivity [7 8]Accordingly molecular techniques are increasingly acceptedfor diagnosis of viral respiratory tract infections In the last
few years multiplex RT-PCR assays have been developed todetect respiratory viruses [9] and some have been commer-cialized such as xTAGRVP from Luminex [10 11] MulticodePLx RVP from EraGen Biosciences [12] and ResPlex II fromQiagen [13]
In our previous study a multiplex PCR based on theGenomeLab Gene Expression Profiler (GeXP) analyzer hadbeen shown to be effective for the detection of pandemicinfluenza A H1N1 virus [14] nine serotypes of enterovirusesassociated with hand foot and mouth disease [15] andsixteen different respiratory virus typessubtypes in a singletube [16] However these methods are not likely to bewidely adopted in provincial Centers for Disease Control andPrevention due to the limited availability of GeXP equip-ment Therefore in this study a two-tube multiplex reversetranscription PCR assay (twotube assay) to detect sixteen
2 BioMed Research International
respiratory viruses based on the amplicon size differencesusing automated electrophoresis system is described Onetube is used for the simultaneous detection of nine respiratoryviruses including influenza A virus (FluA) influenza B virus(FluB) seasonal influenza A virus subtypes H1N1 (sH1N1)parainfluenza virus type 1 (PIV1) human rhinovirus (HRV)coronavirus subtypes OC43 (CoV OC43) coronavirus sub-types 229E (CoV 229E) coronavirus subtypes HKU1 (CoVHKU1) and adenovirus (Adv) Another tube is used for thesimultaneous detection of seven respiratory viruses includingparainfluenza virus type 2 (PIV2) parainfluenza virus type3 (PIV3) respiratory syncytial virus A (RSVA) respiratorysyncytial virus B (RSVB) coronavirus subtypes NL63 (CoVNL63) human metapneumovirus (HMPV) and humanbocavirus (HBoV) As the two-tube assay uses the QIAxcelautomated electrophoresis systemwhich is accessible inmostof provincial Centers for Disease Control and Prevention inChina this two-tube assay may have greater potential for theroutine surveillance of respiratory virus infection in Chinaand to improve the capacity for emergency management
2 Materials and Methods
21 Specimens A total of 247 nasopharyngeal aspirates werecollected in the Childrenrsquos Hospital of Beijing China dur-ing June 2008 and March 2010 from hospitalized childrenunder two years of age presenting acute lower respiratoryinfection (ALRI) syndromes based on clinical measurementsrecommended by the World Health Organization (WHO)The patients were included in this study according to thefollowing criteria parenchymal infiltration on chest radiog-raphy dry or moist rale body temperature above 375∘C anormal or low leukocyte count or lower chest wall indrawingThe mean age of study participants was 1308 months Of247 cases 149 (6032) participants were male and 98(3968) female A total of 160 (6478) participants werefrom urban areas and 87 (3522) were from suburban orrural areas of China (Hebei Henan Shanxi Shandong andInner Mongolia) The specimens were collected within 5 to 7days after symptoms onset Patients with bacterial infectionswere excluded All aspects of the study were performed inaccordance with national ethics regulations and approved bythe Institutional Review Boards of the Center for DiseaseControl and Prevention of China Childrenrsquos parents wereapprised of the studyrsquos purpose and of their right to keepinformation confidentialWritten consent was obtained fromchildrenrsquos parents
Total RNADNA was extracted from 200120583L of clinicalsample using the QIAamp Viral RNA Mini Kit (QiagenHilden Germany) The extracts were eluted into 50 120583L ofDNase- and RNase-free water and stored at minus80∘C
22 Primers Nine pairs of chimeric primers [17] were addedto tube 1 to detect nine respiratory viruses and eight pairsof chimeric primers were added to tube 2 to detect sevenrespiratory viruses One pair of internal control primer andone pair of universal primers were added to both tubes Thesequence from human genome RNase P gene was used as an
internal control primer for the specimens [16] The primerssequences the target genes the amplicon sizes and primerworking concentrations are listed in Table 1
23 Two-Tube Assay and Detection One-Step RT-PCR Kit(Qiagen Hilden Germany) was used for the amplification Atotal of 25120583L PCRmixture containing 2 120583L of extracted RNAand varied primer concentrations (Table 1) was subjected tothe following conditions 50∘C for 30min 95∘C for 15minfollowed by 10 cycles of 95∘C for 30 s 55∘C for 30 s and 72∘C30 s 10 cycles of 95∘C for 30 s 65∘C for 30 s 72∘C for 30 s 25cycles of 95∘C for 30 s 48∘C for 30 s and 72∘C for 30 s and afinal incubation of 72∘C for 3min [15] and the reactions wereanalyzed on the QIAxcel automatic electrophoresis usingQIAxcel DNA High-Resolution kit
24 Specificity and Sensitivity of the Two-Tube Assay Thespecificity of the two-tube assay on all viral targets was testedindividually in the two multiplex reactions under the experi-mental condition as described previously Cell-cultured virusstocks contained in NATtrol Respiratory Validation Panels 2(NATRVP-2) (ZeptoMetrix Buffalo New York USA) wereused as the positive controls of FluA FluB sH1N1 PIV1-3HRV Adv RSVA RSVB HMPV CoV 229E and CoV OC43to validate the specificity Specimens genotyped previously[18 19] were used as positive controls of HBoV HKU1 andCoV NL63
To determine the analytical sensitivity of the assay serialdilutions of viral RNA transcripts of all RNA viruses andserial dilutions of the plasmids containing theAdv andHBoVtarget sequencewere analyzed by the two-tube assayThePCRproducts were cloned into a pGEM-T vector which was usedto transform DH10B cells The plasmid DNA was extractedwith an EZNA Plasmid Mini Kit I (Omega GA USA)The RNA copy number was calculated after measuring theconcentration of the RNA transcribed in vitro using a T7Large-Scale RNA Production System (Promega WisconsinUSA) For the DNA viruses Adv and HBoV the in vitrotranscription was omitted The sensitivity of the two-tubeassay was examined by using premixed quantitative viralRNA transcripts or plasmids The personnel responsible forreading these and other assays were experienced staff withbasic training in microbiology and molecular biology
25 Luminex xTAG RVP Fast Assay and Detection TheLuminex xTAG RVP Fast kit (Abbott Illinois USA) enablesusers to detect simultaneously FluA FluB RSV PIV1-4Adv HMPV CoV 229E NL63 OC43 HKU1 enterovirus(HEV)HRV and HBoV The RNADNA extracted from247 clinical specimens was tested using the Luminex xTAGRVP Fast assay in a 96-well plate format according to themanufacturerrsquos instructions [3 20] The plate was analyzedusing the Bio-Plex 200 system (Bio-Rad CA USA) and themedian fluorescence intensity (MFI) was determined
26 Resolution and Confirmation of Discordant ResultsThe additional targets detected only by the two-tube assaywere confirmed by independent PCR and sequencing
BioMed Research International 3
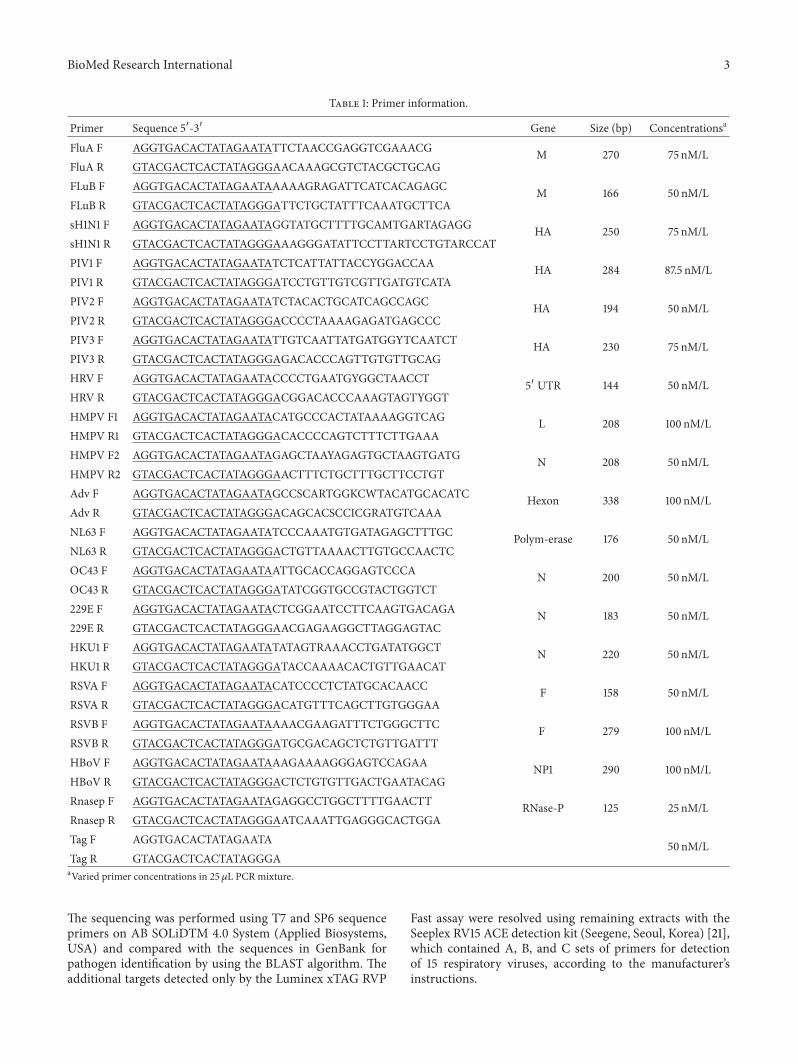
Table 1 Primer information
Primer Sequence 51015840-31015840 Gene Size (bp) Concentrationsa
FluA F AGGTGACACTATAGAATATTCTAACCGAGGTCGAAACG M 270 75 nMLFluA R GTACGACTCACTATAGGGAACAAAGCGTCTACGCTGCAGFLuB F AGGTGACACTATAGAATAAAAAGRAGATTCATCACAGAGC M 166 50 nMLFLuB R GTACGACTCACTATAGGGATTCTGCTATTTCAAATGCTTCAsH1N1 F AGGTGACACTATAGAATAGGTATGCTTTTGCAMTGARTAGAGG HA 250 75 nMLsH1N1 R GTACGACTCACTATAGGGAAAGGGATATTCCTTARTCCTGTARCCATPIV1 F AGGTGACACTATAGAATATCTCATTATTACCYGGACCAA HA 284 875 nMLPIV1 R GTACGACTCACTATAGGGATCCTGTTGTCGTTGATGTCATAPIV2 F AGGTGACACTATAGAATATCTACACTGCATCAGCCAGC HA 194 50 nMLPIV2 R GTACGACTCACTATAGGGACCCCTAAAAGAGATGAGCCCPIV3 F AGGTGACACTATAGAATATTGTCAATTATGATGGYTCAATCT HA 230 75 nMLPIV3 R GTACGACTCACTATAGGGAGACACCCAGTTGTGTTGCAGHRV F AGGTGACACTATAGAATACCCCTGAATGYGGCTAACCT
51015840 UTR 144 50 nML
HRV R GTACGACTCACTATAGGGACGGACACCCAAAGTAGTYGGTHMPV F1 AGGTGACACTATAGAATACATGCCCACTATAAAAGGTCAG L 208 100 nMLHMPV R1 GTACGACTCACTATAGGGACACCCCAGTCTTTCTTGAAAHMPV F2 AGGTGACACTATAGAATAGAGCTAAYAGAGTGCTAAGTGATG N 208 50 nMLHMPV R2 GTACGACTCACTATAGGGAACTTTCTGCTTTGCTTCCTGTAdv F AGGTGACACTATAGAATAGCCSCARTGGKCWTACATGCACATC Hexon 338 100 nMLAdv R GTACGACTCACTATAGGGACAGCACSCCICGRATGTCAAANL63 F AGGTGACACTATAGAATATCCCAAATGTGATAGAGCTTTGC Polym-erase 176 50 nMLNL63 R GTACGACTCACTATAGGGACTGTTAAAACTTGTGCCAACTCOC43 F AGGTGACACTATAGAATAATTGCACCAGGAGTCCCA N 200 50 nMLOC43 R GTACGACTCACTATAGGGATATCGGTGCCGTACTGGTCT229E F AGGTGACACTATAGAATACTCGGAATCCTTCAAGTGACAGA N 183 50 nML229E R GTACGACTCACTATAGGGAACGAGAAGGCTTAGGAGTACHKU1 F AGGTGACACTATAGAATATATAGTRAAACCTGATATGGCT N 220 50 nMLHKU1 R GTACGACTCACTATAGGGATACCAAAACACTGTTGAACATRSVA F AGGTGACACTATAGAATACATCCCCTCTATGCACAACC F 158 50 nMLRSVA R GTACGACTCACTATAGGGACATGTTTCAGCTTGTGGGAARSVB F AGGTGACACTATAGAATAAAACGAAGATTTCTGGGCTTC F 279 100 nMLRSVB R GTACGACTCACTATAGGGATGCGACAGCTCTGTTGATTTHBoV F AGGTGACACTATAGAATAAAGAAAAGGGAGTCCAGAA NP1 290 100 nMLHBoV R GTACGACTCACTATAGGGACTCTGTGTTGACTGAATACAGRnasep F AGGTGACACTATAGAATAGAGGCCTGGCTTTTGAACTT RNase-P 125 25 nMLRnasep R GTACGACTCACTATAGGGAATCAAATTGAGGGCACTGGATag F AGGTGACACTATAGAATA 50 nMLTag R GTACGACTCACTATAGGGAaVaried primer concentrations in 25120583L PCR mixture
The sequencing was performed using T7 and SP6 sequenceprimers on AB SOLiDTM 40 System (Applied BiosystemsUSA) and compared with the sequences in GenBank forpathogen identification by using the BLAST algorithm Theadditional targets detected only by the Luminex xTAG RVP
Fast assay were resolved using remaining extracts with theSeeplex RV15 ACE detection kit (Seegene Seoul Korea) [21]which contained A B and C sets of primers for detectionof 15 respiratory viruses according to the manufacturerrsquosinstructions
4 BioMed Research International
100
500400350300250200150
5015
450375
275325
2251751257525
100
500400350300250200150
5015
450375
275325
2251751257525
MM 1 2 3 4 5 6 7 8 9 10
(a)
100
500400350300250200150
5015
450375
275325
2251751257525
100
500400350300250200150
5015
450375
275325
2251751257525
MM 11 12 1413 15 16 17 18
(b)
Figure 1 Specificity analyses of the the two-tube assay based on the automatic electrophoresis All positive controls were identifiedsuccessfully and nomisprimingwas observed in either tube Lanes 1 to 9 show the results of amplification ofHRV (148 bp) FluB (171 bp) CoV229E (189 bp) CoV OC43 (208 bp) CoV HKU1 (226 bp) FluA (sH1N1) (257 bp and 276 bp) FluA (H3N2) (276 bp) PIV1 (286 bp) and Adv(342 bp) respectively Lanes 11ndash17 show the results of amplification of RSVA (163 bp) CoVNL63 (179 b) PIV2 (198 bp) HMPV (212 bp) PIV3(233 bp) RSVB (280 bp) and HBoV (298 bp) respectively For the viral targets that used clinical specimens as positive controls includingHBoV CoV HKU1 and CoV NL63 a single PCR product was detected in addition to the internal control peak (126 bp) Lanes 10 and 18 arethe negative controls (distilled water) of tube 1 and tube 2 respectively Lane MM molecular marker
100
500
400350300250200150
5015
450
375
275325
2251751257525
100
500
400350300250200150
5015
450
375
275325
2251751257525
MM 1 2 3 4 5 6 7 8 9 10 11 12
Figure 2 Sensitivity analyses of the two-tube assay based on theautomatic electrophoresis Lanes 1 to 5 contain PCR products ofpre-mixed viral targets in tube 1 of 2 times 106 to 200 copies Lanes 7to 11 contain PCR products of pre-mixed viral targets in tube 2 of2 times 105 to 20 copies Lanes 6 and 12 are the negative controls oftube 1 and tube 2 respectively Lane MM molecular marker Thedetection sensitivity in tube 1 with 9 pre-mixed viral targets was2000 copies per reaction and 200 copies per reaction in tube 2 with8 pre-mixed templates Only the amplicons of sH1N1 and CoV 229Ewere absent with dilutions of 200 copies of pre-mixed viral targets intube 1 (Lanes 5) and only the amplicons of CoV NL63 HMPV andRSVBwere absentwith dilutions of 20 copies of pre-mixed templatesin tube 2 (Lanes 11) The primer dimers which were inevitable inthe multiplex PCR are increasingly apparent with the dilution oftemplate
27 Statistical Analysis All statistical analyses were per-formed using Statistical Package for Social Sciences (SPSS)software (version 130) for Windows The 1205942-test and Fisherrsquosexact test were conducted to measure the detection agree-ment of two-tube assay with the Luminex xTAG RVP Fastassay and confirmed results
3 Results
31 Specificity and Sensitivity of the Two-Tube Assay Theexpected size of each virus typesubtype-specific ampliconwas observed and separated clearly from the other viral
targets on QIAxcel automatic electrophoresis for all of thepositive controls No mispriming (primer dimer) or otheramplification in the negative controls was observed in eithertube (Figure 1) The QIAxcel DNA High Resolution kit iscapable of resolving amplicons with as little as 5 bp sizedifference the smallest size difference in this test was 10 bpFor the viral targets that used clinical specimens as positivecontrols (HBoV CoV HKU1 and CoV NL63) a single PCRproduct was detected in addition to the internal control peak(126 bp)
The sensitivity of the assay was evaluated for each virustypesubtype individually using serial tenfold dilutions rang-ing from 10 to 105 copies of cloned PCR products in bothof the two tubes The limit of detection for HRV PIV2PIV3 RSVA HBoV and Adv was 20 copies per reaction and200 copies per reaction for the other 10 virus typesubtypesassayed in this study
The sensitivity of two-tube assay when all the viral targetswere present was also testedThe detection sensitivity in tube1 with 9 pre-mixed viral targets was 2000 copies per reactionand 200 copies per reaction in tube 2 with 7 premixedtemplates (Figure 2)
32 Evaluation of the Two-Tube Assay Using RespiratorySpecimens All the comparative detectionswere double-blindtests performed by trained staff in our laboratory All of the247 specimens assayed with the Luminex xTAG RVP Fastassay were retested by the two-tube assay The two assaysdetected presence of at least one of the 16 assayed virusesin 194 specimens and the two assays both detected virusin 181 specimens The two-tube assay detected virus in 8specimens that were negative in the Luminex xTAGRVP Fastassay (2Adv 3 RSVB 2HRV and 1 PIV3) and 5 specimenshad a positive detection of HRV only by the Luminex xTAGRVP Fast assayThe Luminex xTAGRVP Fast assay identified111 specimens to be coinfections 83 of them (7477) were
BioMed Research International 5
Table 2 Performance of the two-tube assay for individual target compared with the Luminex xTAG RVP Fast assay
VirusesNo of specimens two-tubeLuminex
xTAG RVP Fast assayPerformance of the two-tube assay compared with the Luminex xTAG RVP Fast
assay++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 22 2 0 223 100 9911 9167 100 9919 0952HRV 95 15 13 124 8796 8921 8636 9051 8866 0770HMPV 27 1 0 219 100 9955 9643 100 9960 0980Adv 24 11 1 211 9600 9505 6857 9953 9514 0773CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 7 1 0 239 100 9958 8750 100 9960 0931RSVB 86 10 0 151 100 9379 8958 100 9595 0913HBoV 28 0 5 214 8485 100 100 9772 9798 0907The numbers of positive and negative specimens detected by both testing methods are shown This table shows the sensitivity specificity positive predictivevalue (PPV) negative predictive value (NPV) and the kappa values for each target using the Luminex xTAG RVP Fast assay as the reference for comparisonAll the kappa values were above 075 indicating that the two assays were in agreement
in complete agreement between both assays and detectionof 13 viruses (in 12 specimens) was missed by the two-tubeassay Additional 14 viruses (in 14 coinfected specimens)were detected only by the two-tube assay and 2 coinfectionspecimens (no 28 and no 118) gave inconsistent resultsbetween the two assays (Table 3)
As shown in Table 2 there were 40 viral infectionsidentified only by the two-tube assay and 21 viral infectionsfound only by the Luminex xTAG RVP Fast assay Theinfection events not detected by the Luminex xTAG RVPFast assay included PIV3 (119899 = 2) HRV (119899 = 15) HMPV(119899 = 1) Adv (119899 = 11) RSVA (119899 = 1) and RSVB (119899 =10) Thirty-two of these undetected targets were found incoinfections and the remaining 8 targets (2 Adv 3 RSVB2HRV and 1 PIV3) were single-target positive specimens bythe two-tube assay The two-tube assay failed to detect thefollowing viral infections (119899 = 21) sH1N1 (119899 = 2) HRV(119899 = 13) Adv (119899 = 1) and HBoV (119899 = 5) Sixteen of the21 specimens were coinfections and the remaining 5 targetswere positive only for HRV specimens Because the HRVprimers used in the Luminex xTAG RVP Fast assay were ableto amplify both HRV and enterovirus the specimens positivefor HRV detected only by the Luminex xTAG RVP Fast assaycould be enteroviruses The sensitivity specificity negativeprediction value (NPV) positive prediction value (PPV) theaccordance rate and the kappa value of each virus for the two-tube assay when compared to the Luminex xTAG RVP Fastassay as a reference are shown in Table 2
33 Resolution and Confirmation of Discordant Results Allof the 40 additional targets detected only by the two-tubeassay were confirmed by sequencing as true positives Forthose specimens with discordant results by the two-tube andRVP assays the Seeplex RV15 ACE detection kit was used toresolve the discrepancy (Table 3)
The confirmed results were defined as the results detectedby at least two of the three PCR assays [22 23] or the resultsof sequencing The sensitivity specificity negative predictionvalue (NPV) positive prediction value (PPV) the accordancerate and the kappa value of each virus for the two-tube assaywhen compared to the confirmed results as a reference areshown in Table 4
4 Discussion
In this study a novel two-tube assay based on the QIAxcelcapillary electrophoresis to replace GeXP has been evaluatedfor the potential application in routine laboratory testingof respiratory viruses in China Under optimized workingcondition the two-tube assay revealed good specificity with-out nonspecific amplification using size detection systemthough conventional validation of specificity is usually doneby probe detection hybridization nested PCR and sequenc-ing The two-tube assay achieved a sensitivity of 20ndash200copies per reaction when assayed individually for each virustypesubtype and 2000 copies when 9 viral targets werepresent in tube 1 and 200 copies when 7 viral templates were
6 BioMed Research International
Table 3 The confirmed results for specimens with discordant results between the two-tube assay and the Luminex xTAG RVP Fast assay
Case no Two-tube Luminex xTAG RVP Fasta Seeplex Confirmed results43 HRV HEVHRVHBoV HRV HRV349 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB352 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB146 HMPV HMPVHBoV HMPV HMPV149 HMPV HMPVHEVHRVb andHBoV HRV HMPV HRV HMPV16 None HEVHRV HRV HRV125 RSVB RSVBHEVHRV HRV RSVB HRV RSVB262 RSVB PIV3 and HBoV RSVB PIV3 HBoV andHEVHRV PIV3 RSVB RSVB PIV3 and HBoV
270 PIV3 RSVB and HMPV PIV3 RSVB HMPV andHEVHRV PIV3 RSVB and HMPV PIV3 RSVB and HMPV
142 RSVB RSVBHEVHRV RSVB RSVB21 PIV3 PIV3HEVHRV PIV3 PIV366 None HEVHRV None None85 FluA sH1N1 and HBoV FluA (H1) HBoV andHEVHRV FluA FluA sH1N1 and HBoV87 None HEVHRV None None91 None HEVHRV None None114 None HEVHRV None None274 HRV RSVB HEVHRV RSVB and Adv HRV Adv HRV Adv and RSVB
28 FluA HBoV and Advc FluA (H1c) HBoV NDd FluA sH1N1 HBoV andAdv
118 FluA Adv RSVAc RSVBcand HBoV
FluA (H1c)HEVHRV Adv andHBoV
FluA RSVA Adv andHBOV
FluA sH1N1 Adv RSVARSVB and HBoV
aViruses with discordant results are shown in boldfacebThe Luminex xTAG RVP Fast assay was not able to distinguish rhinovirus from enterovirus so HRV positives are described as HEVHRVcThe Adv in no 28 specimen the RSVA RSVB in no 118 specimen and the FluA subtype H1 were confirmed by sequencingdND stands for not detected
Table 4 Performance of the two-tube assay for individual target compared with the confirmed results
Viruses No of specimens by two-tubeconfirmed results Performance of the two-tube assay compared with confirmed results++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 24 0 0 223 100 100 100 100 100 1000HRV 110 0 3 134 9735 100 100 9781 9879 0975HMPV 28 0 0 219 100 100 100 100 100 1000Adv 35 0 1 211 9722 100 100 9953 9960 0984CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 8 0 0 239 100 100 100 100 100 1000RSVB 96 0 0 151 100 100 100 100 100 1000HBoV 28 0 0 219 100 100 100 100 100 1000This table shows the sensitivity specificity positive predictive value (PPV) negative predictive value (NPV) and the kappa values for each target using theconfirmed results as the reference for comparison All the specificity and PPV were 100 all the accordance rate values were above 9879 and all the kappavalues were above 075
BioMed Research International 7
present in tube 2 These results suggest the utility of thetwo-tube assay for the detection of multiple respiratory virusinfections for laboratories not equipped to perform liquidchip-based multiplex assays
The 247 specimens from hospitalized children showeda high prevalence of infection and co-infection with thecommon respiratory viral pathogens HRV was found mostfrequently followed by RSVB The major discrepanciesbetween the two-tube assay introduced in this study and theLuminex xTAG RVP Fast assay were found for the detectionof HRV Adv HBoV RSVB and sH1N1 (kappa = 07700773 0907 0913 and 0929 resp) (Table 2) All of theHRV positive samples including 15 detected only by two-tube assay were confirmed by sequencing to be positive forHRV A The 13 HRV-positive specimens detected only bythe Luminex xTAG RVP Fast assay could be enterovirusesbecause of the Luminex RVP Fast assay detecting enterovirus(the HEV component of the HEVHRV) After resolved bythe Seeplex RV15 ACE detection kit three of them were trulydiscordant For Adv seven specimens identified as positiveonly by the two-tube assay were shown via sequencing to beAdv C and 4 were Adv B1 Only one Adv-positive specimenwas missed by two-tube assay For HBoV five specimensdetected as positive only by the Luminex xTAG RVP Fastassay were also negative by the Seeplex assay The other 14positive samples detected only by two-tube assay (10 RSVB2 PIV3 1 RSVA and 1HMPV) were confirmed by sequencingas true positives For sH1N1 all of the FluA positives weresequenced and 16 of 20 were sH1N1 the two-tube assay failedto detect 2 of the 16 sH1N1 positives The detection resultsof coronaviruses (CoV HKU1 CoV NL63 CoV 229E andCoV OC43) influenza (FluA FluB) PIV1 and PIV2 werecompletely consistent between the two assays In summaryno false positiveswere found by the two-tube assay and a totalof 6 false negatives occurred HRV (119899 = 3) sH1N1 (119899 = 2)and Adv (119899 = 1) The two-tube assay was more sensitivethan the Luminex xTAG RVP Fast assay for the detectionof HRV A RSVB Adv B1 and Adv C The overall detectionrate of the two-tube assay for each virus was comparable tothat of the Luminex xTAG RVP Fast assay (kappa gt 075)demonstrating the high sensitivity and specificity of the two-tube assay in the analysis of clinical samples
The two-tube assay as confirmed by the Luminex xTAGRVP Fast assay revealed that almost 80 of the respiratoryspecimens tested were positive for at least one viral infectionand viral coinfections were frequentThe overall co-infectionrates of the two-tube assay and the Luminex xTAG RVPFast assay were 4858 (120247) and 4494 (111247)respectively Compared with other similar reports [9 24ndash26]the extremely higher co-infection rate found by both assaysmight be due to the difference in the tested population andpossible nosocomial infections in the hospital
The routine use of extensive testing by methods suchas the two-tube assay should make large studies of theclinical relevance of single and multiple respiratory virusinfectionsmore feasibleThe clinical relevance of the outcomeof multiplex PCR tests for respiratory viruses is not yet fullydetermined In one study of children with RSV infectionhigher fever longer hospital stays and more frequent use
of antibiotics were associated with multiple infections [27]For some agents such as influenza A and B virus a positivetest may provide the basis for antiviral treatment [28] It hasbeen suggested that a rapid etiologic diagnosis of viral RTIcould reduce unnecessary prescription of antibiotics but thisremains to be shown [28]
Two distinct advantages of the two-tube assay are theshort assay time and the low costThe assay requires 5-6 hoursto complete 100 samples including a half hour to prepare PCRmixture the whole RT-PCR (3 hours) and the detection onthe QIAxcel automatic electrophoresis (12 tests15 minutes)while using other liquid chip-based assays might take anentire workday [29] The cost for two-tube assay is $10testincluding the RT-PCR kit and the consumables of detectionversus at least $120test [29] using other liquid chip-basedassays [29]
In conclusion the two-tube assay developed in thisstudy using automatic capillary electrophoresis is a rapidcost-effective method with high sensitivity and specificityfor the detection of respiratory virus infection and it isdemonstrated to have great potential for routine surveillanceof respiratory virus infection
Conflict of Interests
The authors declare that they have no conflict of interests
Authorsrsquo Contribution
Jin Li was involved in the operation of the two-tube assayand designing of primers with Qin Meng Xiumei Hu andHongwei Shen Dr Shunxiang Qi led the evaluation of thetwo-tube assay using the Seegene kit Dr Chen Zhang wasresponsible for providing the clinical samples and leadingthe evaluation of two-tube assay using the RVP methodwith Mrs Mengjie Yang Ji Wang and Mrs Miao Wang DrWenbo Xu offered great help in the supplement of differentclinical samples as well as shared previous experimentaldata Dr Xuejun Ma designed and coordinated the studyanalyzed data and drafted the paper Jin Li and ShunxiangQi contributed equally to the study
Acknowledgments
The authors are grateful to Dr Brian Ring from HuazhongUniversity of Science and Technology for critical reviewof this paper This work was supported by the ChinaMega Project for Infectious Disease (2011ZX10004-0012012ZX10004-215 and 2013ZX10004-202)
References
[1] M T Coiras J C Aguilar M L Garcıa I Casas and P Perez-Brena ldquoSimultaneous detection of fourteen respiratory virusesin clinical specimens by two multiplex reverse transcriptionnested-PCR assaysrdquo Journal of Medical Virology vol 72 no 3pp 484ndash495 2004
[2] A S Fauci N A Touchette and G K Folkers ldquoEmerginginfectious diseases a 10-year perspective from the National
8 BioMed Research International
Institute ofAllergy and InfectiousDiseasesrdquoEmerging InfectiousDiseases vol 11 no 4 pp 519ndash525 2005
[3] J Mahony S Chong F Merante et al ldquoDevelopment of a respi-ratory virus panel test for detection of twenty human respiratoryviruses by use of multiplex PCR and a fluid microbead-basedassayrdquo Journal of Clinical Microbiology vol 45 no 9 pp 2965ndash2970 2007
[4] F G Hayden A D M E Osterhaus J J Treanor et alldquoEfficacy and safety of the neuraminidase inhibitor zanamivirin the treatment of influenzavirus infectionsrdquoTheNew EnglandJournal of Medicine vol 337 no 13 pp 874ndash880 1997
[5] P C Y Woo S S Chiu W Seto and M Peiris ldquoCost-effectiveness of rapid diagnosis of viral respiratory tract infec-tions in pediatric patientsrdquo Journal of Clinical Microbiology vol35 no 6 pp 1579ndash1581 1997
[6] J Barenfanger C Drake N Leon T Mueller and T TrouttldquoClinical and financial benefits of rapid detection of respiratoryviruses an outcomes studyrdquo Journal of Clinical Microbiologyvol 38 no 8 pp 2824ndash2828 2000
[7] K J Henrickson D M E Osterhaus and J A McCullersldquoAdvances in the laboratory diagnosis of viral respiratorydiseaserdquo Pediatric Infectious Disease Journal vol 23 no 1 ppS6ndashS10 2004
[8] G A Storch ldquoDiagnostic virologyrdquo Clinical Infectious Diseasesvol 31 no 3 pp 739ndash751 2000
[9] F Raymond J Carbonneau N Boucher et al ldquoComparisonof automated microarray detection with real-time PCR assaysfor detection of respiratory viruses in specimens obtained fromchildrenrdquo Journal of Clinical Microbiology vol 47 pp 743ndash7502009
[10] N Krunic T D Yager D Himsworth F Merante SYaghoubian and R Janeczko ldquoxTAGŮ RVP assay analyticaland clinical performancerdquo Journal of Clinical Virology vol 40supplement 1 pp S39ndashS46 2007
[11] K Pabbaraju K L Tokaryk S Wong and J D Fox ldquoCompari-son of the luminex xTAG respiratory viral panel with in-housenucleic acid amplification tests for diagnosis of respiratory virusinfectionsrdquo Journal of Clinical Microbiology vol 46 no 9 pp3056ndash3062 2008
[12] F S Nolte D J Marshall C Rasberry et al ldquoMultiCode-PLx system for multiplexed detection of seventeen respiratoryvirusesrdquo Journal of ClinicalMicrobiology vol 45 no 9 pp 2779ndash2786 2007
[13] H Li M A McCormac R W Estes et al ldquoSimultaneousdetection and high-throughput identification of a panel of RNAviruses causing respiratory tract infectionsrdquo Journal of ClinicalMicrobiology vol 45 no 7 pp 2105ndash2109 2007
[14] M Qin D Wang F Huang et al ldquoDetection of pandemicinfluenza AH1N1 virus by multiplex reverse transcription-PCRwith a GeXP analyzerrdquo Journal of Virological Methods vol 168no 1-2 pp 255ndash258 2010
[15] X Hu Y Zhang X Zhou et al ldquoSimultaneously typing nineserotypes of enteroviruses associated with hand foot andmouth disease by a GeXP analyzer-based multiplex reversetranscription-PCR assayrdquo Journal of Clinical Microbiology vol50 no 2 pp 288ndash293 2012
[16] J Li N Y Mao C Zhang et al ldquoThe development of aGeXP-based multiplex reverse transcription-PCR assay forsimultaneous detection of sixteen human respiratory virustypessubtypesrdquo BMC Infectious Diseases vol 12 article 1892012
[17] T TaboneD EMather andM J Hayden ldquoTemperature SwitchPCR (TSP) robust assay design for reliable amplification andgenotyping of SNPsrdquo BMC Genomics vol 10 article 580 2009
[18] Z XuW Cheng B Li J Li B Lan and Z Duan ldquoDevelopmentof a real-time PCR assay for detecting and quantifying humanbocavirus 2rdquo Journal of Clinical Microbiology vol 49 no 4 pp1537ndash1541 2011
[19] L J Cui C Zhang T Zhang et al ldquoHuman coronavirusesHCoV-NL63 and HCoV-HKU1 in hospitalized children withacute respiratory infections in Beijing Chinardquo Adv Virol vol2011 Article ID 129134 6 pages 2011
[20] F Merante S Yaghoubian and R Janeczko ldquoPrinciples of thexTAGŮ respiratory viral panel assay (RVP Assay)rdquo Journal ofClinical Virology vol 40 supplement 1 pp S31ndashS35 2007
[21] D F Bibby I Mcelarney J Breuer and D A Clark ldquoCompara-tive evaluation of the seegene seeplex RV15 and real-time PCRfor respiratory virus detectionrdquo Journal of Medical Virology vol83 no 8 pp 1469ndash1475 2011
[22] L E S Bruijnesteijn van Coppenraet C M A Swanink AA van Zwet et al ldquoComparison of two commercial molecularassays for simultaneous detection of respiratory viruses inclinical samples using two automatic electrophoresis detectionsystemsrdquo Journal of Virological Methods vol 169 no 1 pp 188ndash192 2010
[23] H K Kim S H Oh K A Yun H Sung and M N KimldquoComparison of anyplex II RV16 with xTAG respiratory viralpanel and seeplex RV15 for the detection of respiratory virusesrdquoJournal of ClinicalMicrobiology vol 51 no 4 pp 1137ndash1141 2013
[24] L Bonzel T Tenenbaum H Schroten O Schildgen SSchweitzer-Krantz and O Adams ldquoFrequent detection of viralcoinfection in children hospitalized with acute respiratory tractinfection using a real-time polymerase chain reactionrdquoPediatricInfectious Disease Journal vol 27 no 7 pp 589ndash594 2008
[25] G Cilla E Onate E G Perez-YarzaMMontes D Vicente andE Perez-Trallero ldquoViruses in community-acquired pneumoniain children aged less than 3 years old high rate of viralcoinfectionrdquo Journal of Medical Virology vol 80 no 10 pp1843ndash1849 2008
[26] N J Gadsby A Hardie E C J Claas and K E TempletonldquoComparison of the Luminex respiratory virus panel fast assaywith in-house real-time PCR for respiratory viral infectiondiagnosisrdquo Journal of Clinical Microbiology vol 48 no 6 pp2213ndash2216 2010
[27] C Calvo M L Garcıa-Garcıa C Blanco et al ldquoMultiplesimultaneous viral infections in infants with acute respiratorytract infections in Spainrdquo Journal of Clinical Virology vol 42no 3 pp 268ndash272 2008
[28] R Brittain-Long J Westin S Olofsson M Lindh and LAndersson ldquoProspective evaluation of a novel multiplex real-time PCR assay for detection of fifteen respiratory pathogens-Duration of symptoms significantly affects detection raterdquoJournal of Clinical Virology vol 47 no 3 pp 263ndash267 2010
[29] K H Rand H Rampersaud and H J Houck ldquoComparisonof two multiplex methods for detection of respiratory virusesfilmarray RP and xTAG RVPrdquo Journal of Clinical Microbiologyvol 49 no 7 pp 2449ndash2453 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
respiratory viruses based on the amplicon size differencesusing automated electrophoresis system is described Onetube is used for the simultaneous detection of nine respiratoryviruses including influenza A virus (FluA) influenza B virus(FluB) seasonal influenza A virus subtypes H1N1 (sH1N1)parainfluenza virus type 1 (PIV1) human rhinovirus (HRV)coronavirus subtypes OC43 (CoV OC43) coronavirus sub-types 229E (CoV 229E) coronavirus subtypes HKU1 (CoVHKU1) and adenovirus (Adv) Another tube is used for thesimultaneous detection of seven respiratory viruses includingparainfluenza virus type 2 (PIV2) parainfluenza virus type3 (PIV3) respiratory syncytial virus A (RSVA) respiratorysyncytial virus B (RSVB) coronavirus subtypes NL63 (CoVNL63) human metapneumovirus (HMPV) and humanbocavirus (HBoV) As the two-tube assay uses the QIAxcelautomated electrophoresis systemwhich is accessible inmostof provincial Centers for Disease Control and Prevention inChina this two-tube assay may have greater potential for theroutine surveillance of respiratory virus infection in Chinaand to improve the capacity for emergency management
2 Materials and Methods
21 Specimens A total of 247 nasopharyngeal aspirates werecollected in the Childrenrsquos Hospital of Beijing China dur-ing June 2008 and March 2010 from hospitalized childrenunder two years of age presenting acute lower respiratoryinfection (ALRI) syndromes based on clinical measurementsrecommended by the World Health Organization (WHO)The patients were included in this study according to thefollowing criteria parenchymal infiltration on chest radiog-raphy dry or moist rale body temperature above 375∘C anormal or low leukocyte count or lower chest wall indrawingThe mean age of study participants was 1308 months Of247 cases 149 (6032) participants were male and 98(3968) female A total of 160 (6478) participants werefrom urban areas and 87 (3522) were from suburban orrural areas of China (Hebei Henan Shanxi Shandong andInner Mongolia) The specimens were collected within 5 to 7days after symptoms onset Patients with bacterial infectionswere excluded All aspects of the study were performed inaccordance with national ethics regulations and approved bythe Institutional Review Boards of the Center for DiseaseControl and Prevention of China Childrenrsquos parents wereapprised of the studyrsquos purpose and of their right to keepinformation confidentialWritten consent was obtained fromchildrenrsquos parents
Total RNADNA was extracted from 200120583L of clinicalsample using the QIAamp Viral RNA Mini Kit (QiagenHilden Germany) The extracts were eluted into 50 120583L ofDNase- and RNase-free water and stored at minus80∘C
22 Primers Nine pairs of chimeric primers [17] were addedto tube 1 to detect nine respiratory viruses and eight pairsof chimeric primers were added to tube 2 to detect sevenrespiratory viruses One pair of internal control primer andone pair of universal primers were added to both tubes Thesequence from human genome RNase P gene was used as an
internal control primer for the specimens [16] The primerssequences the target genes the amplicon sizes and primerworking concentrations are listed in Table 1
23 Two-Tube Assay and Detection One-Step RT-PCR Kit(Qiagen Hilden Germany) was used for the amplification Atotal of 25120583L PCRmixture containing 2 120583L of extracted RNAand varied primer concentrations (Table 1) was subjected tothe following conditions 50∘C for 30min 95∘C for 15minfollowed by 10 cycles of 95∘C for 30 s 55∘C for 30 s and 72∘C30 s 10 cycles of 95∘C for 30 s 65∘C for 30 s 72∘C for 30 s 25cycles of 95∘C for 30 s 48∘C for 30 s and 72∘C for 30 s and afinal incubation of 72∘C for 3min [15] and the reactions wereanalyzed on the QIAxcel automatic electrophoresis usingQIAxcel DNA High-Resolution kit
24 Specificity and Sensitivity of the Two-Tube Assay Thespecificity of the two-tube assay on all viral targets was testedindividually in the two multiplex reactions under the experi-mental condition as described previously Cell-cultured virusstocks contained in NATtrol Respiratory Validation Panels 2(NATRVP-2) (ZeptoMetrix Buffalo New York USA) wereused as the positive controls of FluA FluB sH1N1 PIV1-3HRV Adv RSVA RSVB HMPV CoV 229E and CoV OC43to validate the specificity Specimens genotyped previously[18 19] were used as positive controls of HBoV HKU1 andCoV NL63
To determine the analytical sensitivity of the assay serialdilutions of viral RNA transcripts of all RNA viruses andserial dilutions of the plasmids containing theAdv andHBoVtarget sequencewere analyzed by the two-tube assayThePCRproducts were cloned into a pGEM-T vector which was usedto transform DH10B cells The plasmid DNA was extractedwith an EZNA Plasmid Mini Kit I (Omega GA USA)The RNA copy number was calculated after measuring theconcentration of the RNA transcribed in vitro using a T7Large-Scale RNA Production System (Promega WisconsinUSA) For the DNA viruses Adv and HBoV the in vitrotranscription was omitted The sensitivity of the two-tubeassay was examined by using premixed quantitative viralRNA transcripts or plasmids The personnel responsible forreading these and other assays were experienced staff withbasic training in microbiology and molecular biology
25 Luminex xTAG RVP Fast Assay and Detection TheLuminex xTAG RVP Fast kit (Abbott Illinois USA) enablesusers to detect simultaneously FluA FluB RSV PIV1-4Adv HMPV CoV 229E NL63 OC43 HKU1 enterovirus(HEV)HRV and HBoV The RNADNA extracted from247 clinical specimens was tested using the Luminex xTAGRVP Fast assay in a 96-well plate format according to themanufacturerrsquos instructions [3 20] The plate was analyzedusing the Bio-Plex 200 system (Bio-Rad CA USA) and themedian fluorescence intensity (MFI) was determined
26 Resolution and Confirmation of Discordant ResultsThe additional targets detected only by the two-tube assaywere confirmed by independent PCR and sequencing
BioMed Research International 3
Table 1 Primer information
Primer Sequence 51015840-31015840 Gene Size (bp) Concentrationsa
FluA F AGGTGACACTATAGAATATTCTAACCGAGGTCGAAACG M 270 75 nMLFluA R GTACGACTCACTATAGGGAACAAAGCGTCTACGCTGCAGFLuB F AGGTGACACTATAGAATAAAAAGRAGATTCATCACAGAGC M 166 50 nMLFLuB R GTACGACTCACTATAGGGATTCTGCTATTTCAAATGCTTCAsH1N1 F AGGTGACACTATAGAATAGGTATGCTTTTGCAMTGARTAGAGG HA 250 75 nMLsH1N1 R GTACGACTCACTATAGGGAAAGGGATATTCCTTARTCCTGTARCCATPIV1 F AGGTGACACTATAGAATATCTCATTATTACCYGGACCAA HA 284 875 nMLPIV1 R GTACGACTCACTATAGGGATCCTGTTGTCGTTGATGTCATAPIV2 F AGGTGACACTATAGAATATCTACACTGCATCAGCCAGC HA 194 50 nMLPIV2 R GTACGACTCACTATAGGGACCCCTAAAAGAGATGAGCCCPIV3 F AGGTGACACTATAGAATATTGTCAATTATGATGGYTCAATCT HA 230 75 nMLPIV3 R GTACGACTCACTATAGGGAGACACCCAGTTGTGTTGCAGHRV F AGGTGACACTATAGAATACCCCTGAATGYGGCTAACCT
51015840 UTR 144 50 nML
HRV R GTACGACTCACTATAGGGACGGACACCCAAAGTAGTYGGTHMPV F1 AGGTGACACTATAGAATACATGCCCACTATAAAAGGTCAG L 208 100 nMLHMPV R1 GTACGACTCACTATAGGGACACCCCAGTCTTTCTTGAAAHMPV F2 AGGTGACACTATAGAATAGAGCTAAYAGAGTGCTAAGTGATG N 208 50 nMLHMPV R2 GTACGACTCACTATAGGGAACTTTCTGCTTTGCTTCCTGTAdv F AGGTGACACTATAGAATAGCCSCARTGGKCWTACATGCACATC Hexon 338 100 nMLAdv R GTACGACTCACTATAGGGACAGCACSCCICGRATGTCAAANL63 F AGGTGACACTATAGAATATCCCAAATGTGATAGAGCTTTGC Polym-erase 176 50 nMLNL63 R GTACGACTCACTATAGGGACTGTTAAAACTTGTGCCAACTCOC43 F AGGTGACACTATAGAATAATTGCACCAGGAGTCCCA N 200 50 nMLOC43 R GTACGACTCACTATAGGGATATCGGTGCCGTACTGGTCT229E F AGGTGACACTATAGAATACTCGGAATCCTTCAAGTGACAGA N 183 50 nML229E R GTACGACTCACTATAGGGAACGAGAAGGCTTAGGAGTACHKU1 F AGGTGACACTATAGAATATATAGTRAAACCTGATATGGCT N 220 50 nMLHKU1 R GTACGACTCACTATAGGGATACCAAAACACTGTTGAACATRSVA F AGGTGACACTATAGAATACATCCCCTCTATGCACAACC F 158 50 nMLRSVA R GTACGACTCACTATAGGGACATGTTTCAGCTTGTGGGAARSVB F AGGTGACACTATAGAATAAAACGAAGATTTCTGGGCTTC F 279 100 nMLRSVB R GTACGACTCACTATAGGGATGCGACAGCTCTGTTGATTTHBoV F AGGTGACACTATAGAATAAAGAAAAGGGAGTCCAGAA NP1 290 100 nMLHBoV R GTACGACTCACTATAGGGACTCTGTGTTGACTGAATACAGRnasep F AGGTGACACTATAGAATAGAGGCCTGGCTTTTGAACTT RNase-P 125 25 nMLRnasep R GTACGACTCACTATAGGGAATCAAATTGAGGGCACTGGATag F AGGTGACACTATAGAATA 50 nMLTag R GTACGACTCACTATAGGGAaVaried primer concentrations in 25120583L PCR mixture
The sequencing was performed using T7 and SP6 sequenceprimers on AB SOLiDTM 40 System (Applied BiosystemsUSA) and compared with the sequences in GenBank forpathogen identification by using the BLAST algorithm Theadditional targets detected only by the Luminex xTAG RVP
Fast assay were resolved using remaining extracts with theSeeplex RV15 ACE detection kit (Seegene Seoul Korea) [21]which contained A B and C sets of primers for detectionof 15 respiratory viruses according to the manufacturerrsquosinstructions
4 BioMed Research International
100
500400350300250200150
5015
450375
275325
2251751257525
100
500400350300250200150
5015
450375
275325
2251751257525
MM 1 2 3 4 5 6 7 8 9 10
(a)
100
500400350300250200150
5015
450375
275325
2251751257525
100
500400350300250200150
5015
450375
275325
2251751257525
MM 11 12 1413 15 16 17 18
(b)
Figure 1 Specificity analyses of the the two-tube assay based on the automatic electrophoresis All positive controls were identifiedsuccessfully and nomisprimingwas observed in either tube Lanes 1 to 9 show the results of amplification ofHRV (148 bp) FluB (171 bp) CoV229E (189 bp) CoV OC43 (208 bp) CoV HKU1 (226 bp) FluA (sH1N1) (257 bp and 276 bp) FluA (H3N2) (276 bp) PIV1 (286 bp) and Adv(342 bp) respectively Lanes 11ndash17 show the results of amplification of RSVA (163 bp) CoVNL63 (179 b) PIV2 (198 bp) HMPV (212 bp) PIV3(233 bp) RSVB (280 bp) and HBoV (298 bp) respectively For the viral targets that used clinical specimens as positive controls includingHBoV CoV HKU1 and CoV NL63 a single PCR product was detected in addition to the internal control peak (126 bp) Lanes 10 and 18 arethe negative controls (distilled water) of tube 1 and tube 2 respectively Lane MM molecular marker
100
500
400350300250200150
5015
450
375
275325
2251751257525
100
500
400350300250200150
5015
450
375
275325
2251751257525
MM 1 2 3 4 5 6 7 8 9 10 11 12
Figure 2 Sensitivity analyses of the two-tube assay based on theautomatic electrophoresis Lanes 1 to 5 contain PCR products ofpre-mixed viral targets in tube 1 of 2 times 106 to 200 copies Lanes 7to 11 contain PCR products of pre-mixed viral targets in tube 2 of2 times 105 to 20 copies Lanes 6 and 12 are the negative controls oftube 1 and tube 2 respectively Lane MM molecular marker Thedetection sensitivity in tube 1 with 9 pre-mixed viral targets was2000 copies per reaction and 200 copies per reaction in tube 2 with8 pre-mixed templates Only the amplicons of sH1N1 and CoV 229Ewere absent with dilutions of 200 copies of pre-mixed viral targets intube 1 (Lanes 5) and only the amplicons of CoV NL63 HMPV andRSVBwere absentwith dilutions of 20 copies of pre-mixed templatesin tube 2 (Lanes 11) The primer dimers which were inevitable inthe multiplex PCR are increasingly apparent with the dilution oftemplate
27 Statistical Analysis All statistical analyses were per-formed using Statistical Package for Social Sciences (SPSS)software (version 130) for Windows The 1205942-test and Fisherrsquosexact test were conducted to measure the detection agree-ment of two-tube assay with the Luminex xTAG RVP Fastassay and confirmed results
3 Results
31 Specificity and Sensitivity of the Two-Tube Assay Theexpected size of each virus typesubtype-specific ampliconwas observed and separated clearly from the other viral
targets on QIAxcel automatic electrophoresis for all of thepositive controls No mispriming (primer dimer) or otheramplification in the negative controls was observed in eithertube (Figure 1) The QIAxcel DNA High Resolution kit iscapable of resolving amplicons with as little as 5 bp sizedifference the smallest size difference in this test was 10 bpFor the viral targets that used clinical specimens as positivecontrols (HBoV CoV HKU1 and CoV NL63) a single PCRproduct was detected in addition to the internal control peak(126 bp)
The sensitivity of the assay was evaluated for each virustypesubtype individually using serial tenfold dilutions rang-ing from 10 to 105 copies of cloned PCR products in bothof the two tubes The limit of detection for HRV PIV2PIV3 RSVA HBoV and Adv was 20 copies per reaction and200 copies per reaction for the other 10 virus typesubtypesassayed in this study
The sensitivity of two-tube assay when all the viral targetswere present was also testedThe detection sensitivity in tube1 with 9 pre-mixed viral targets was 2000 copies per reactionand 200 copies per reaction in tube 2 with 7 premixedtemplates (Figure 2)
32 Evaluation of the Two-Tube Assay Using RespiratorySpecimens All the comparative detectionswere double-blindtests performed by trained staff in our laboratory All of the247 specimens assayed with the Luminex xTAG RVP Fastassay were retested by the two-tube assay The two assaysdetected presence of at least one of the 16 assayed virusesin 194 specimens and the two assays both detected virusin 181 specimens The two-tube assay detected virus in 8specimens that were negative in the Luminex xTAGRVP Fastassay (2Adv 3 RSVB 2HRV and 1 PIV3) and 5 specimenshad a positive detection of HRV only by the Luminex xTAGRVP Fast assayThe Luminex xTAGRVP Fast assay identified111 specimens to be coinfections 83 of them (7477) were
BioMed Research International 5
Table 2 Performance of the two-tube assay for individual target compared with the Luminex xTAG RVP Fast assay
VirusesNo of specimens two-tubeLuminex
xTAG RVP Fast assayPerformance of the two-tube assay compared with the Luminex xTAG RVP Fast
assay++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 22 2 0 223 100 9911 9167 100 9919 0952HRV 95 15 13 124 8796 8921 8636 9051 8866 0770HMPV 27 1 0 219 100 9955 9643 100 9960 0980Adv 24 11 1 211 9600 9505 6857 9953 9514 0773CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 7 1 0 239 100 9958 8750 100 9960 0931RSVB 86 10 0 151 100 9379 8958 100 9595 0913HBoV 28 0 5 214 8485 100 100 9772 9798 0907The numbers of positive and negative specimens detected by both testing methods are shown This table shows the sensitivity specificity positive predictivevalue (PPV) negative predictive value (NPV) and the kappa values for each target using the Luminex xTAG RVP Fast assay as the reference for comparisonAll the kappa values were above 075 indicating that the two assays were in agreement
in complete agreement between both assays and detectionof 13 viruses (in 12 specimens) was missed by the two-tubeassay Additional 14 viruses (in 14 coinfected specimens)were detected only by the two-tube assay and 2 coinfectionspecimens (no 28 and no 118) gave inconsistent resultsbetween the two assays (Table 3)
As shown in Table 2 there were 40 viral infectionsidentified only by the two-tube assay and 21 viral infectionsfound only by the Luminex xTAG RVP Fast assay Theinfection events not detected by the Luminex xTAG RVPFast assay included PIV3 (119899 = 2) HRV (119899 = 15) HMPV(119899 = 1) Adv (119899 = 11) RSVA (119899 = 1) and RSVB (119899 =10) Thirty-two of these undetected targets were found incoinfections and the remaining 8 targets (2 Adv 3 RSVB2HRV and 1 PIV3) were single-target positive specimens bythe two-tube assay The two-tube assay failed to detect thefollowing viral infections (119899 = 21) sH1N1 (119899 = 2) HRV(119899 = 13) Adv (119899 = 1) and HBoV (119899 = 5) Sixteen of the21 specimens were coinfections and the remaining 5 targetswere positive only for HRV specimens Because the HRVprimers used in the Luminex xTAG RVP Fast assay were ableto amplify both HRV and enterovirus the specimens positivefor HRV detected only by the Luminex xTAG RVP Fast assaycould be enteroviruses The sensitivity specificity negativeprediction value (NPV) positive prediction value (PPV) theaccordance rate and the kappa value of each virus for the two-tube assay when compared to the Luminex xTAG RVP Fastassay as a reference are shown in Table 2
33 Resolution and Confirmation of Discordant Results Allof the 40 additional targets detected only by the two-tubeassay were confirmed by sequencing as true positives Forthose specimens with discordant results by the two-tube andRVP assays the Seeplex RV15 ACE detection kit was used toresolve the discrepancy (Table 3)
The confirmed results were defined as the results detectedby at least two of the three PCR assays [22 23] or the resultsof sequencing The sensitivity specificity negative predictionvalue (NPV) positive prediction value (PPV) the accordancerate and the kappa value of each virus for the two-tube assaywhen compared to the confirmed results as a reference areshown in Table 4
4 Discussion
In this study a novel two-tube assay based on the QIAxcelcapillary electrophoresis to replace GeXP has been evaluatedfor the potential application in routine laboratory testingof respiratory viruses in China Under optimized workingcondition the two-tube assay revealed good specificity with-out nonspecific amplification using size detection systemthough conventional validation of specificity is usually doneby probe detection hybridization nested PCR and sequenc-ing The two-tube assay achieved a sensitivity of 20ndash200copies per reaction when assayed individually for each virustypesubtype and 2000 copies when 9 viral targets werepresent in tube 1 and 200 copies when 7 viral templates were
6 BioMed Research International
Table 3 The confirmed results for specimens with discordant results between the two-tube assay and the Luminex xTAG RVP Fast assay
Case no Two-tube Luminex xTAG RVP Fasta Seeplex Confirmed results43 HRV HEVHRVHBoV HRV HRV349 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB352 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB146 HMPV HMPVHBoV HMPV HMPV149 HMPV HMPVHEVHRVb andHBoV HRV HMPV HRV HMPV16 None HEVHRV HRV HRV125 RSVB RSVBHEVHRV HRV RSVB HRV RSVB262 RSVB PIV3 and HBoV RSVB PIV3 HBoV andHEVHRV PIV3 RSVB RSVB PIV3 and HBoV
270 PIV3 RSVB and HMPV PIV3 RSVB HMPV andHEVHRV PIV3 RSVB and HMPV PIV3 RSVB and HMPV
142 RSVB RSVBHEVHRV RSVB RSVB21 PIV3 PIV3HEVHRV PIV3 PIV366 None HEVHRV None None85 FluA sH1N1 and HBoV FluA (H1) HBoV andHEVHRV FluA FluA sH1N1 and HBoV87 None HEVHRV None None91 None HEVHRV None None114 None HEVHRV None None274 HRV RSVB HEVHRV RSVB and Adv HRV Adv HRV Adv and RSVB
28 FluA HBoV and Advc FluA (H1c) HBoV NDd FluA sH1N1 HBoV andAdv
118 FluA Adv RSVAc RSVBcand HBoV
FluA (H1c)HEVHRV Adv andHBoV
FluA RSVA Adv andHBOV
FluA sH1N1 Adv RSVARSVB and HBoV
aViruses with discordant results are shown in boldfacebThe Luminex xTAG RVP Fast assay was not able to distinguish rhinovirus from enterovirus so HRV positives are described as HEVHRVcThe Adv in no 28 specimen the RSVA RSVB in no 118 specimen and the FluA subtype H1 were confirmed by sequencingdND stands for not detected
Table 4 Performance of the two-tube assay for individual target compared with the confirmed results
Viruses No of specimens by two-tubeconfirmed results Performance of the two-tube assay compared with confirmed results++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 24 0 0 223 100 100 100 100 100 1000HRV 110 0 3 134 9735 100 100 9781 9879 0975HMPV 28 0 0 219 100 100 100 100 100 1000Adv 35 0 1 211 9722 100 100 9953 9960 0984CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 8 0 0 239 100 100 100 100 100 1000RSVB 96 0 0 151 100 100 100 100 100 1000HBoV 28 0 0 219 100 100 100 100 100 1000This table shows the sensitivity specificity positive predictive value (PPV) negative predictive value (NPV) and the kappa values for each target using theconfirmed results as the reference for comparison All the specificity and PPV were 100 all the accordance rate values were above 9879 and all the kappavalues were above 075
BioMed Research International 7
present in tube 2 These results suggest the utility of thetwo-tube assay for the detection of multiple respiratory virusinfections for laboratories not equipped to perform liquidchip-based multiplex assays
The 247 specimens from hospitalized children showeda high prevalence of infection and co-infection with thecommon respiratory viral pathogens HRV was found mostfrequently followed by RSVB The major discrepanciesbetween the two-tube assay introduced in this study and theLuminex xTAG RVP Fast assay were found for the detectionof HRV Adv HBoV RSVB and sH1N1 (kappa = 07700773 0907 0913 and 0929 resp) (Table 2) All of theHRV positive samples including 15 detected only by two-tube assay were confirmed by sequencing to be positive forHRV A The 13 HRV-positive specimens detected only bythe Luminex xTAG RVP Fast assay could be enterovirusesbecause of the Luminex RVP Fast assay detecting enterovirus(the HEV component of the HEVHRV) After resolved bythe Seeplex RV15 ACE detection kit three of them were trulydiscordant For Adv seven specimens identified as positiveonly by the two-tube assay were shown via sequencing to beAdv C and 4 were Adv B1 Only one Adv-positive specimenwas missed by two-tube assay For HBoV five specimensdetected as positive only by the Luminex xTAG RVP Fastassay were also negative by the Seeplex assay The other 14positive samples detected only by two-tube assay (10 RSVB2 PIV3 1 RSVA and 1HMPV) were confirmed by sequencingas true positives For sH1N1 all of the FluA positives weresequenced and 16 of 20 were sH1N1 the two-tube assay failedto detect 2 of the 16 sH1N1 positives The detection resultsof coronaviruses (CoV HKU1 CoV NL63 CoV 229E andCoV OC43) influenza (FluA FluB) PIV1 and PIV2 werecompletely consistent between the two assays In summaryno false positiveswere found by the two-tube assay and a totalof 6 false negatives occurred HRV (119899 = 3) sH1N1 (119899 = 2)and Adv (119899 = 1) The two-tube assay was more sensitivethan the Luminex xTAG RVP Fast assay for the detectionof HRV A RSVB Adv B1 and Adv C The overall detectionrate of the two-tube assay for each virus was comparable tothat of the Luminex xTAG RVP Fast assay (kappa gt 075)demonstrating the high sensitivity and specificity of the two-tube assay in the analysis of clinical samples
The two-tube assay as confirmed by the Luminex xTAGRVP Fast assay revealed that almost 80 of the respiratoryspecimens tested were positive for at least one viral infectionand viral coinfections were frequentThe overall co-infectionrates of the two-tube assay and the Luminex xTAG RVPFast assay were 4858 (120247) and 4494 (111247)respectively Compared with other similar reports [9 24ndash26]the extremely higher co-infection rate found by both assaysmight be due to the difference in the tested population andpossible nosocomial infections in the hospital
The routine use of extensive testing by methods suchas the two-tube assay should make large studies of theclinical relevance of single and multiple respiratory virusinfectionsmore feasibleThe clinical relevance of the outcomeof multiplex PCR tests for respiratory viruses is not yet fullydetermined In one study of children with RSV infectionhigher fever longer hospital stays and more frequent use
of antibiotics were associated with multiple infections [27]For some agents such as influenza A and B virus a positivetest may provide the basis for antiviral treatment [28] It hasbeen suggested that a rapid etiologic diagnosis of viral RTIcould reduce unnecessary prescription of antibiotics but thisremains to be shown [28]
Two distinct advantages of the two-tube assay are theshort assay time and the low costThe assay requires 5-6 hoursto complete 100 samples including a half hour to prepare PCRmixture the whole RT-PCR (3 hours) and the detection onthe QIAxcel automatic electrophoresis (12 tests15 minutes)while using other liquid chip-based assays might take anentire workday [29] The cost for two-tube assay is $10testincluding the RT-PCR kit and the consumables of detectionversus at least $120test [29] using other liquid chip-basedassays [29]
In conclusion the two-tube assay developed in thisstudy using automatic capillary electrophoresis is a rapidcost-effective method with high sensitivity and specificityfor the detection of respiratory virus infection and it isdemonstrated to have great potential for routine surveillanceof respiratory virus infection
Conflict of Interests
The authors declare that they have no conflict of interests
Authorsrsquo Contribution
Jin Li was involved in the operation of the two-tube assayand designing of primers with Qin Meng Xiumei Hu andHongwei Shen Dr Shunxiang Qi led the evaluation of thetwo-tube assay using the Seegene kit Dr Chen Zhang wasresponsible for providing the clinical samples and leadingthe evaluation of two-tube assay using the RVP methodwith Mrs Mengjie Yang Ji Wang and Mrs Miao Wang DrWenbo Xu offered great help in the supplement of differentclinical samples as well as shared previous experimentaldata Dr Xuejun Ma designed and coordinated the studyanalyzed data and drafted the paper Jin Li and ShunxiangQi contributed equally to the study
Acknowledgments
The authors are grateful to Dr Brian Ring from HuazhongUniversity of Science and Technology for critical reviewof this paper This work was supported by the ChinaMega Project for Infectious Disease (2011ZX10004-0012012ZX10004-215 and 2013ZX10004-202)
References
[1] M T Coiras J C Aguilar M L Garcıa I Casas and P Perez-Brena ldquoSimultaneous detection of fourteen respiratory virusesin clinical specimens by two multiplex reverse transcriptionnested-PCR assaysrdquo Journal of Medical Virology vol 72 no 3pp 484ndash495 2004
[2] A S Fauci N A Touchette and G K Folkers ldquoEmerginginfectious diseases a 10-year perspective from the National
8 BioMed Research International
Institute ofAllergy and InfectiousDiseasesrdquoEmerging InfectiousDiseases vol 11 no 4 pp 519ndash525 2005
[3] J Mahony S Chong F Merante et al ldquoDevelopment of a respi-ratory virus panel test for detection of twenty human respiratoryviruses by use of multiplex PCR and a fluid microbead-basedassayrdquo Journal of Clinical Microbiology vol 45 no 9 pp 2965ndash2970 2007
[4] F G Hayden A D M E Osterhaus J J Treanor et alldquoEfficacy and safety of the neuraminidase inhibitor zanamivirin the treatment of influenzavirus infectionsrdquoTheNew EnglandJournal of Medicine vol 337 no 13 pp 874ndash880 1997
[5] P C Y Woo S S Chiu W Seto and M Peiris ldquoCost-effectiveness of rapid diagnosis of viral respiratory tract infec-tions in pediatric patientsrdquo Journal of Clinical Microbiology vol35 no 6 pp 1579ndash1581 1997
[6] J Barenfanger C Drake N Leon T Mueller and T TrouttldquoClinical and financial benefits of rapid detection of respiratoryviruses an outcomes studyrdquo Journal of Clinical Microbiologyvol 38 no 8 pp 2824ndash2828 2000
[7] K J Henrickson D M E Osterhaus and J A McCullersldquoAdvances in the laboratory diagnosis of viral respiratorydiseaserdquo Pediatric Infectious Disease Journal vol 23 no 1 ppS6ndashS10 2004
[8] G A Storch ldquoDiagnostic virologyrdquo Clinical Infectious Diseasesvol 31 no 3 pp 739ndash751 2000
[9] F Raymond J Carbonneau N Boucher et al ldquoComparisonof automated microarray detection with real-time PCR assaysfor detection of respiratory viruses in specimens obtained fromchildrenrdquo Journal of Clinical Microbiology vol 47 pp 743ndash7502009
[10] N Krunic T D Yager D Himsworth F Merante SYaghoubian and R Janeczko ldquoxTAGŮ RVP assay analyticaland clinical performancerdquo Journal of Clinical Virology vol 40supplement 1 pp S39ndashS46 2007
[11] K Pabbaraju K L Tokaryk S Wong and J D Fox ldquoCompari-son of the luminex xTAG respiratory viral panel with in-housenucleic acid amplification tests for diagnosis of respiratory virusinfectionsrdquo Journal of Clinical Microbiology vol 46 no 9 pp3056ndash3062 2008
[12] F S Nolte D J Marshall C Rasberry et al ldquoMultiCode-PLx system for multiplexed detection of seventeen respiratoryvirusesrdquo Journal of ClinicalMicrobiology vol 45 no 9 pp 2779ndash2786 2007
[13] H Li M A McCormac R W Estes et al ldquoSimultaneousdetection and high-throughput identification of a panel of RNAviruses causing respiratory tract infectionsrdquo Journal of ClinicalMicrobiology vol 45 no 7 pp 2105ndash2109 2007
[14] M Qin D Wang F Huang et al ldquoDetection of pandemicinfluenza AH1N1 virus by multiplex reverse transcription-PCRwith a GeXP analyzerrdquo Journal of Virological Methods vol 168no 1-2 pp 255ndash258 2010
[15] X Hu Y Zhang X Zhou et al ldquoSimultaneously typing nineserotypes of enteroviruses associated with hand foot andmouth disease by a GeXP analyzer-based multiplex reversetranscription-PCR assayrdquo Journal of Clinical Microbiology vol50 no 2 pp 288ndash293 2012
[16] J Li N Y Mao C Zhang et al ldquoThe development of aGeXP-based multiplex reverse transcription-PCR assay forsimultaneous detection of sixteen human respiratory virustypessubtypesrdquo BMC Infectious Diseases vol 12 article 1892012
[17] T TaboneD EMather andM J Hayden ldquoTemperature SwitchPCR (TSP) robust assay design for reliable amplification andgenotyping of SNPsrdquo BMC Genomics vol 10 article 580 2009
[18] Z XuW Cheng B Li J Li B Lan and Z Duan ldquoDevelopmentof a real-time PCR assay for detecting and quantifying humanbocavirus 2rdquo Journal of Clinical Microbiology vol 49 no 4 pp1537ndash1541 2011
[19] L J Cui C Zhang T Zhang et al ldquoHuman coronavirusesHCoV-NL63 and HCoV-HKU1 in hospitalized children withacute respiratory infections in Beijing Chinardquo Adv Virol vol2011 Article ID 129134 6 pages 2011
[20] F Merante S Yaghoubian and R Janeczko ldquoPrinciples of thexTAGŮ respiratory viral panel assay (RVP Assay)rdquo Journal ofClinical Virology vol 40 supplement 1 pp S31ndashS35 2007
[21] D F Bibby I Mcelarney J Breuer and D A Clark ldquoCompara-tive evaluation of the seegene seeplex RV15 and real-time PCRfor respiratory virus detectionrdquo Journal of Medical Virology vol83 no 8 pp 1469ndash1475 2011
[22] L E S Bruijnesteijn van Coppenraet C M A Swanink AA van Zwet et al ldquoComparison of two commercial molecularassays for simultaneous detection of respiratory viruses inclinical samples using two automatic electrophoresis detectionsystemsrdquo Journal of Virological Methods vol 169 no 1 pp 188ndash192 2010
[23] H K Kim S H Oh K A Yun H Sung and M N KimldquoComparison of anyplex II RV16 with xTAG respiratory viralpanel and seeplex RV15 for the detection of respiratory virusesrdquoJournal of ClinicalMicrobiology vol 51 no 4 pp 1137ndash1141 2013
[24] L Bonzel T Tenenbaum H Schroten O Schildgen SSchweitzer-Krantz and O Adams ldquoFrequent detection of viralcoinfection in children hospitalized with acute respiratory tractinfection using a real-time polymerase chain reactionrdquoPediatricInfectious Disease Journal vol 27 no 7 pp 589ndash594 2008
[25] G Cilla E Onate E G Perez-YarzaMMontes D Vicente andE Perez-Trallero ldquoViruses in community-acquired pneumoniain children aged less than 3 years old high rate of viralcoinfectionrdquo Journal of Medical Virology vol 80 no 10 pp1843ndash1849 2008
[26] N J Gadsby A Hardie E C J Claas and K E TempletonldquoComparison of the Luminex respiratory virus panel fast assaywith in-house real-time PCR for respiratory viral infectiondiagnosisrdquo Journal of Clinical Microbiology vol 48 no 6 pp2213ndash2216 2010
[27] C Calvo M L Garcıa-Garcıa C Blanco et al ldquoMultiplesimultaneous viral infections in infants with acute respiratorytract infections in Spainrdquo Journal of Clinical Virology vol 42no 3 pp 268ndash272 2008
[28] R Brittain-Long J Westin S Olofsson M Lindh and LAndersson ldquoProspective evaluation of a novel multiplex real-time PCR assay for detection of fifteen respiratory pathogens-Duration of symptoms significantly affects detection raterdquoJournal of Clinical Virology vol 47 no 3 pp 263ndash267 2010
[29] K H Rand H Rampersaud and H J Houck ldquoComparisonof two multiplex methods for detection of respiratory virusesfilmarray RP and xTAG RVPrdquo Journal of Clinical Microbiologyvol 49 no 7 pp 2449ndash2453 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
BioMed Research International 3
Table 1 Primer information
Primer Sequence 51015840-31015840 Gene Size (bp) Concentrationsa
FluA F AGGTGACACTATAGAATATTCTAACCGAGGTCGAAACG M 270 75 nMLFluA R GTACGACTCACTATAGGGAACAAAGCGTCTACGCTGCAGFLuB F AGGTGACACTATAGAATAAAAAGRAGATTCATCACAGAGC M 166 50 nMLFLuB R GTACGACTCACTATAGGGATTCTGCTATTTCAAATGCTTCAsH1N1 F AGGTGACACTATAGAATAGGTATGCTTTTGCAMTGARTAGAGG HA 250 75 nMLsH1N1 R GTACGACTCACTATAGGGAAAGGGATATTCCTTARTCCTGTARCCATPIV1 F AGGTGACACTATAGAATATCTCATTATTACCYGGACCAA HA 284 875 nMLPIV1 R GTACGACTCACTATAGGGATCCTGTTGTCGTTGATGTCATAPIV2 F AGGTGACACTATAGAATATCTACACTGCATCAGCCAGC HA 194 50 nMLPIV2 R GTACGACTCACTATAGGGACCCCTAAAAGAGATGAGCCCPIV3 F AGGTGACACTATAGAATATTGTCAATTATGATGGYTCAATCT HA 230 75 nMLPIV3 R GTACGACTCACTATAGGGAGACACCCAGTTGTGTTGCAGHRV F AGGTGACACTATAGAATACCCCTGAATGYGGCTAACCT
51015840 UTR 144 50 nML
HRV R GTACGACTCACTATAGGGACGGACACCCAAAGTAGTYGGTHMPV F1 AGGTGACACTATAGAATACATGCCCACTATAAAAGGTCAG L 208 100 nMLHMPV R1 GTACGACTCACTATAGGGACACCCCAGTCTTTCTTGAAAHMPV F2 AGGTGACACTATAGAATAGAGCTAAYAGAGTGCTAAGTGATG N 208 50 nMLHMPV R2 GTACGACTCACTATAGGGAACTTTCTGCTTTGCTTCCTGTAdv F AGGTGACACTATAGAATAGCCSCARTGGKCWTACATGCACATC Hexon 338 100 nMLAdv R GTACGACTCACTATAGGGACAGCACSCCICGRATGTCAAANL63 F AGGTGACACTATAGAATATCCCAAATGTGATAGAGCTTTGC Polym-erase 176 50 nMLNL63 R GTACGACTCACTATAGGGACTGTTAAAACTTGTGCCAACTCOC43 F AGGTGACACTATAGAATAATTGCACCAGGAGTCCCA N 200 50 nMLOC43 R GTACGACTCACTATAGGGATATCGGTGCCGTACTGGTCT229E F AGGTGACACTATAGAATACTCGGAATCCTTCAAGTGACAGA N 183 50 nML229E R GTACGACTCACTATAGGGAACGAGAAGGCTTAGGAGTACHKU1 F AGGTGACACTATAGAATATATAGTRAAACCTGATATGGCT N 220 50 nMLHKU1 R GTACGACTCACTATAGGGATACCAAAACACTGTTGAACATRSVA F AGGTGACACTATAGAATACATCCCCTCTATGCACAACC F 158 50 nMLRSVA R GTACGACTCACTATAGGGACATGTTTCAGCTTGTGGGAARSVB F AGGTGACACTATAGAATAAAACGAAGATTTCTGGGCTTC F 279 100 nMLRSVB R GTACGACTCACTATAGGGATGCGACAGCTCTGTTGATTTHBoV F AGGTGACACTATAGAATAAAGAAAAGGGAGTCCAGAA NP1 290 100 nMLHBoV R GTACGACTCACTATAGGGACTCTGTGTTGACTGAATACAGRnasep F AGGTGACACTATAGAATAGAGGCCTGGCTTTTGAACTT RNase-P 125 25 nMLRnasep R GTACGACTCACTATAGGGAATCAAATTGAGGGCACTGGATag F AGGTGACACTATAGAATA 50 nMLTag R GTACGACTCACTATAGGGAaVaried primer concentrations in 25120583L PCR mixture
The sequencing was performed using T7 and SP6 sequenceprimers on AB SOLiDTM 40 System (Applied BiosystemsUSA) and compared with the sequences in GenBank forpathogen identification by using the BLAST algorithm Theadditional targets detected only by the Luminex xTAG RVP
Fast assay were resolved using remaining extracts with theSeeplex RV15 ACE detection kit (Seegene Seoul Korea) [21]which contained A B and C sets of primers for detectionof 15 respiratory viruses according to the manufacturerrsquosinstructions
4 BioMed Research International
100
500400350300250200150
5015
450375
275325
2251751257525
100
500400350300250200150
5015
450375
275325
2251751257525
MM 1 2 3 4 5 6 7 8 9 10
(a)
100
500400350300250200150
5015
450375
275325
2251751257525
100
500400350300250200150
5015
450375
275325
2251751257525
MM 11 12 1413 15 16 17 18
(b)
Figure 1 Specificity analyses of the the two-tube assay based on the automatic electrophoresis All positive controls were identifiedsuccessfully and nomisprimingwas observed in either tube Lanes 1 to 9 show the results of amplification ofHRV (148 bp) FluB (171 bp) CoV229E (189 bp) CoV OC43 (208 bp) CoV HKU1 (226 bp) FluA (sH1N1) (257 bp and 276 bp) FluA (H3N2) (276 bp) PIV1 (286 bp) and Adv(342 bp) respectively Lanes 11ndash17 show the results of amplification of RSVA (163 bp) CoVNL63 (179 b) PIV2 (198 bp) HMPV (212 bp) PIV3(233 bp) RSVB (280 bp) and HBoV (298 bp) respectively For the viral targets that used clinical specimens as positive controls includingHBoV CoV HKU1 and CoV NL63 a single PCR product was detected in addition to the internal control peak (126 bp) Lanes 10 and 18 arethe negative controls (distilled water) of tube 1 and tube 2 respectively Lane MM molecular marker
100
500
400350300250200150
5015
450
375
275325
2251751257525
100
500
400350300250200150
5015
450
375
275325
2251751257525
MM 1 2 3 4 5 6 7 8 9 10 11 12
Figure 2 Sensitivity analyses of the two-tube assay based on theautomatic electrophoresis Lanes 1 to 5 contain PCR products ofpre-mixed viral targets in tube 1 of 2 times 106 to 200 copies Lanes 7to 11 contain PCR products of pre-mixed viral targets in tube 2 of2 times 105 to 20 copies Lanes 6 and 12 are the negative controls oftube 1 and tube 2 respectively Lane MM molecular marker Thedetection sensitivity in tube 1 with 9 pre-mixed viral targets was2000 copies per reaction and 200 copies per reaction in tube 2 with8 pre-mixed templates Only the amplicons of sH1N1 and CoV 229Ewere absent with dilutions of 200 copies of pre-mixed viral targets intube 1 (Lanes 5) and only the amplicons of CoV NL63 HMPV andRSVBwere absentwith dilutions of 20 copies of pre-mixed templatesin tube 2 (Lanes 11) The primer dimers which were inevitable inthe multiplex PCR are increasingly apparent with the dilution oftemplate
27 Statistical Analysis All statistical analyses were per-formed using Statistical Package for Social Sciences (SPSS)software (version 130) for Windows The 1205942-test and Fisherrsquosexact test were conducted to measure the detection agree-ment of two-tube assay with the Luminex xTAG RVP Fastassay and confirmed results
3 Results
31 Specificity and Sensitivity of the Two-Tube Assay Theexpected size of each virus typesubtype-specific ampliconwas observed and separated clearly from the other viral
targets on QIAxcel automatic electrophoresis for all of thepositive controls No mispriming (primer dimer) or otheramplification in the negative controls was observed in eithertube (Figure 1) The QIAxcel DNA High Resolution kit iscapable of resolving amplicons with as little as 5 bp sizedifference the smallest size difference in this test was 10 bpFor the viral targets that used clinical specimens as positivecontrols (HBoV CoV HKU1 and CoV NL63) a single PCRproduct was detected in addition to the internal control peak(126 bp)
The sensitivity of the assay was evaluated for each virustypesubtype individually using serial tenfold dilutions rang-ing from 10 to 105 copies of cloned PCR products in bothof the two tubes The limit of detection for HRV PIV2PIV3 RSVA HBoV and Adv was 20 copies per reaction and200 copies per reaction for the other 10 virus typesubtypesassayed in this study
The sensitivity of two-tube assay when all the viral targetswere present was also testedThe detection sensitivity in tube1 with 9 pre-mixed viral targets was 2000 copies per reactionand 200 copies per reaction in tube 2 with 7 premixedtemplates (Figure 2)
32 Evaluation of the Two-Tube Assay Using RespiratorySpecimens All the comparative detectionswere double-blindtests performed by trained staff in our laboratory All of the247 specimens assayed with the Luminex xTAG RVP Fastassay were retested by the two-tube assay The two assaysdetected presence of at least one of the 16 assayed virusesin 194 specimens and the two assays both detected virusin 181 specimens The two-tube assay detected virus in 8specimens that were negative in the Luminex xTAGRVP Fastassay (2Adv 3 RSVB 2HRV and 1 PIV3) and 5 specimenshad a positive detection of HRV only by the Luminex xTAGRVP Fast assayThe Luminex xTAGRVP Fast assay identified111 specimens to be coinfections 83 of them (7477) were
BioMed Research International 5
Table 2 Performance of the two-tube assay for individual target compared with the Luminex xTAG RVP Fast assay
VirusesNo of specimens two-tubeLuminex
xTAG RVP Fast assayPerformance of the two-tube assay compared with the Luminex xTAG RVP Fast
assay++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 22 2 0 223 100 9911 9167 100 9919 0952HRV 95 15 13 124 8796 8921 8636 9051 8866 0770HMPV 27 1 0 219 100 9955 9643 100 9960 0980Adv 24 11 1 211 9600 9505 6857 9953 9514 0773CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 7 1 0 239 100 9958 8750 100 9960 0931RSVB 86 10 0 151 100 9379 8958 100 9595 0913HBoV 28 0 5 214 8485 100 100 9772 9798 0907The numbers of positive and negative specimens detected by both testing methods are shown This table shows the sensitivity specificity positive predictivevalue (PPV) negative predictive value (NPV) and the kappa values for each target using the Luminex xTAG RVP Fast assay as the reference for comparisonAll the kappa values were above 075 indicating that the two assays were in agreement
in complete agreement between both assays and detectionof 13 viruses (in 12 specimens) was missed by the two-tubeassay Additional 14 viruses (in 14 coinfected specimens)were detected only by the two-tube assay and 2 coinfectionspecimens (no 28 and no 118) gave inconsistent resultsbetween the two assays (Table 3)
As shown in Table 2 there were 40 viral infectionsidentified only by the two-tube assay and 21 viral infectionsfound only by the Luminex xTAG RVP Fast assay Theinfection events not detected by the Luminex xTAG RVPFast assay included PIV3 (119899 = 2) HRV (119899 = 15) HMPV(119899 = 1) Adv (119899 = 11) RSVA (119899 = 1) and RSVB (119899 =10) Thirty-two of these undetected targets were found incoinfections and the remaining 8 targets (2 Adv 3 RSVB2HRV and 1 PIV3) were single-target positive specimens bythe two-tube assay The two-tube assay failed to detect thefollowing viral infections (119899 = 21) sH1N1 (119899 = 2) HRV(119899 = 13) Adv (119899 = 1) and HBoV (119899 = 5) Sixteen of the21 specimens were coinfections and the remaining 5 targetswere positive only for HRV specimens Because the HRVprimers used in the Luminex xTAG RVP Fast assay were ableto amplify both HRV and enterovirus the specimens positivefor HRV detected only by the Luminex xTAG RVP Fast assaycould be enteroviruses The sensitivity specificity negativeprediction value (NPV) positive prediction value (PPV) theaccordance rate and the kappa value of each virus for the two-tube assay when compared to the Luminex xTAG RVP Fastassay as a reference are shown in Table 2
33 Resolution and Confirmation of Discordant Results Allof the 40 additional targets detected only by the two-tubeassay were confirmed by sequencing as true positives Forthose specimens with discordant results by the two-tube andRVP assays the Seeplex RV15 ACE detection kit was used toresolve the discrepancy (Table 3)
The confirmed results were defined as the results detectedby at least two of the three PCR assays [22 23] or the resultsof sequencing The sensitivity specificity negative predictionvalue (NPV) positive prediction value (PPV) the accordancerate and the kappa value of each virus for the two-tube assaywhen compared to the confirmed results as a reference areshown in Table 4
4 Discussion
In this study a novel two-tube assay based on the QIAxcelcapillary electrophoresis to replace GeXP has been evaluatedfor the potential application in routine laboratory testingof respiratory viruses in China Under optimized workingcondition the two-tube assay revealed good specificity with-out nonspecific amplification using size detection systemthough conventional validation of specificity is usually doneby probe detection hybridization nested PCR and sequenc-ing The two-tube assay achieved a sensitivity of 20ndash200copies per reaction when assayed individually for each virustypesubtype and 2000 copies when 9 viral targets werepresent in tube 1 and 200 copies when 7 viral templates were
6 BioMed Research International
Table 3 The confirmed results for specimens with discordant results between the two-tube assay and the Luminex xTAG RVP Fast assay
Case no Two-tube Luminex xTAG RVP Fasta Seeplex Confirmed results43 HRV HEVHRVHBoV HRV HRV349 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB352 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB146 HMPV HMPVHBoV HMPV HMPV149 HMPV HMPVHEVHRVb andHBoV HRV HMPV HRV HMPV16 None HEVHRV HRV HRV125 RSVB RSVBHEVHRV HRV RSVB HRV RSVB262 RSVB PIV3 and HBoV RSVB PIV3 HBoV andHEVHRV PIV3 RSVB RSVB PIV3 and HBoV
270 PIV3 RSVB and HMPV PIV3 RSVB HMPV andHEVHRV PIV3 RSVB and HMPV PIV3 RSVB and HMPV
142 RSVB RSVBHEVHRV RSVB RSVB21 PIV3 PIV3HEVHRV PIV3 PIV366 None HEVHRV None None85 FluA sH1N1 and HBoV FluA (H1) HBoV andHEVHRV FluA FluA sH1N1 and HBoV87 None HEVHRV None None91 None HEVHRV None None114 None HEVHRV None None274 HRV RSVB HEVHRV RSVB and Adv HRV Adv HRV Adv and RSVB
28 FluA HBoV and Advc FluA (H1c) HBoV NDd FluA sH1N1 HBoV andAdv
118 FluA Adv RSVAc RSVBcand HBoV
FluA (H1c)HEVHRV Adv andHBoV
FluA RSVA Adv andHBOV
FluA sH1N1 Adv RSVARSVB and HBoV
aViruses with discordant results are shown in boldfacebThe Luminex xTAG RVP Fast assay was not able to distinguish rhinovirus from enterovirus so HRV positives are described as HEVHRVcThe Adv in no 28 specimen the RSVA RSVB in no 118 specimen and the FluA subtype H1 were confirmed by sequencingdND stands for not detected
Table 4 Performance of the two-tube assay for individual target compared with the confirmed results
Viruses No of specimens by two-tubeconfirmed results Performance of the two-tube assay compared with confirmed results++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 24 0 0 223 100 100 100 100 100 1000HRV 110 0 3 134 9735 100 100 9781 9879 0975HMPV 28 0 0 219 100 100 100 100 100 1000Adv 35 0 1 211 9722 100 100 9953 9960 0984CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 8 0 0 239 100 100 100 100 100 1000RSVB 96 0 0 151 100 100 100 100 100 1000HBoV 28 0 0 219 100 100 100 100 100 1000This table shows the sensitivity specificity positive predictive value (PPV) negative predictive value (NPV) and the kappa values for each target using theconfirmed results as the reference for comparison All the specificity and PPV were 100 all the accordance rate values were above 9879 and all the kappavalues were above 075
BioMed Research International 7
present in tube 2 These results suggest the utility of thetwo-tube assay for the detection of multiple respiratory virusinfections for laboratories not equipped to perform liquidchip-based multiplex assays
The 247 specimens from hospitalized children showeda high prevalence of infection and co-infection with thecommon respiratory viral pathogens HRV was found mostfrequently followed by RSVB The major discrepanciesbetween the two-tube assay introduced in this study and theLuminex xTAG RVP Fast assay were found for the detectionof HRV Adv HBoV RSVB and sH1N1 (kappa = 07700773 0907 0913 and 0929 resp) (Table 2) All of theHRV positive samples including 15 detected only by two-tube assay were confirmed by sequencing to be positive forHRV A The 13 HRV-positive specimens detected only bythe Luminex xTAG RVP Fast assay could be enterovirusesbecause of the Luminex RVP Fast assay detecting enterovirus(the HEV component of the HEVHRV) After resolved bythe Seeplex RV15 ACE detection kit three of them were trulydiscordant For Adv seven specimens identified as positiveonly by the two-tube assay were shown via sequencing to beAdv C and 4 were Adv B1 Only one Adv-positive specimenwas missed by two-tube assay For HBoV five specimensdetected as positive only by the Luminex xTAG RVP Fastassay were also negative by the Seeplex assay The other 14positive samples detected only by two-tube assay (10 RSVB2 PIV3 1 RSVA and 1HMPV) were confirmed by sequencingas true positives For sH1N1 all of the FluA positives weresequenced and 16 of 20 were sH1N1 the two-tube assay failedto detect 2 of the 16 sH1N1 positives The detection resultsof coronaviruses (CoV HKU1 CoV NL63 CoV 229E andCoV OC43) influenza (FluA FluB) PIV1 and PIV2 werecompletely consistent between the two assays In summaryno false positiveswere found by the two-tube assay and a totalof 6 false negatives occurred HRV (119899 = 3) sH1N1 (119899 = 2)and Adv (119899 = 1) The two-tube assay was more sensitivethan the Luminex xTAG RVP Fast assay for the detectionof HRV A RSVB Adv B1 and Adv C The overall detectionrate of the two-tube assay for each virus was comparable tothat of the Luminex xTAG RVP Fast assay (kappa gt 075)demonstrating the high sensitivity and specificity of the two-tube assay in the analysis of clinical samples
The two-tube assay as confirmed by the Luminex xTAGRVP Fast assay revealed that almost 80 of the respiratoryspecimens tested were positive for at least one viral infectionand viral coinfections were frequentThe overall co-infectionrates of the two-tube assay and the Luminex xTAG RVPFast assay were 4858 (120247) and 4494 (111247)respectively Compared with other similar reports [9 24ndash26]the extremely higher co-infection rate found by both assaysmight be due to the difference in the tested population andpossible nosocomial infections in the hospital
The routine use of extensive testing by methods suchas the two-tube assay should make large studies of theclinical relevance of single and multiple respiratory virusinfectionsmore feasibleThe clinical relevance of the outcomeof multiplex PCR tests for respiratory viruses is not yet fullydetermined In one study of children with RSV infectionhigher fever longer hospital stays and more frequent use
of antibiotics were associated with multiple infections [27]For some agents such as influenza A and B virus a positivetest may provide the basis for antiviral treatment [28] It hasbeen suggested that a rapid etiologic diagnosis of viral RTIcould reduce unnecessary prescription of antibiotics but thisremains to be shown [28]
Two distinct advantages of the two-tube assay are theshort assay time and the low costThe assay requires 5-6 hoursto complete 100 samples including a half hour to prepare PCRmixture the whole RT-PCR (3 hours) and the detection onthe QIAxcel automatic electrophoresis (12 tests15 minutes)while using other liquid chip-based assays might take anentire workday [29] The cost for two-tube assay is $10testincluding the RT-PCR kit and the consumables of detectionversus at least $120test [29] using other liquid chip-basedassays [29]
In conclusion the two-tube assay developed in thisstudy using automatic capillary electrophoresis is a rapidcost-effective method with high sensitivity and specificityfor the detection of respiratory virus infection and it isdemonstrated to have great potential for routine surveillanceof respiratory virus infection
Conflict of Interests
The authors declare that they have no conflict of interests
Authorsrsquo Contribution
Jin Li was involved in the operation of the two-tube assayand designing of primers with Qin Meng Xiumei Hu andHongwei Shen Dr Shunxiang Qi led the evaluation of thetwo-tube assay using the Seegene kit Dr Chen Zhang wasresponsible for providing the clinical samples and leadingthe evaluation of two-tube assay using the RVP methodwith Mrs Mengjie Yang Ji Wang and Mrs Miao Wang DrWenbo Xu offered great help in the supplement of differentclinical samples as well as shared previous experimentaldata Dr Xuejun Ma designed and coordinated the studyanalyzed data and drafted the paper Jin Li and ShunxiangQi contributed equally to the study
Acknowledgments
The authors are grateful to Dr Brian Ring from HuazhongUniversity of Science and Technology for critical reviewof this paper This work was supported by the ChinaMega Project for Infectious Disease (2011ZX10004-0012012ZX10004-215 and 2013ZX10004-202)
References
[1] M T Coiras J C Aguilar M L Garcıa I Casas and P Perez-Brena ldquoSimultaneous detection of fourteen respiratory virusesin clinical specimens by two multiplex reverse transcriptionnested-PCR assaysrdquo Journal of Medical Virology vol 72 no 3pp 484ndash495 2004
[2] A S Fauci N A Touchette and G K Folkers ldquoEmerginginfectious diseases a 10-year perspective from the National
8 BioMed Research International
Institute ofAllergy and InfectiousDiseasesrdquoEmerging InfectiousDiseases vol 11 no 4 pp 519ndash525 2005
[3] J Mahony S Chong F Merante et al ldquoDevelopment of a respi-ratory virus panel test for detection of twenty human respiratoryviruses by use of multiplex PCR and a fluid microbead-basedassayrdquo Journal of Clinical Microbiology vol 45 no 9 pp 2965ndash2970 2007
[4] F G Hayden A D M E Osterhaus J J Treanor et alldquoEfficacy and safety of the neuraminidase inhibitor zanamivirin the treatment of influenzavirus infectionsrdquoTheNew EnglandJournal of Medicine vol 337 no 13 pp 874ndash880 1997
[5] P C Y Woo S S Chiu W Seto and M Peiris ldquoCost-effectiveness of rapid diagnosis of viral respiratory tract infec-tions in pediatric patientsrdquo Journal of Clinical Microbiology vol35 no 6 pp 1579ndash1581 1997
[6] J Barenfanger C Drake N Leon T Mueller and T TrouttldquoClinical and financial benefits of rapid detection of respiratoryviruses an outcomes studyrdquo Journal of Clinical Microbiologyvol 38 no 8 pp 2824ndash2828 2000
[7] K J Henrickson D M E Osterhaus and J A McCullersldquoAdvances in the laboratory diagnosis of viral respiratorydiseaserdquo Pediatric Infectious Disease Journal vol 23 no 1 ppS6ndashS10 2004
[8] G A Storch ldquoDiagnostic virologyrdquo Clinical Infectious Diseasesvol 31 no 3 pp 739ndash751 2000
[9] F Raymond J Carbonneau N Boucher et al ldquoComparisonof automated microarray detection with real-time PCR assaysfor detection of respiratory viruses in specimens obtained fromchildrenrdquo Journal of Clinical Microbiology vol 47 pp 743ndash7502009
[10] N Krunic T D Yager D Himsworth F Merante SYaghoubian and R Janeczko ldquoxTAGŮ RVP assay analyticaland clinical performancerdquo Journal of Clinical Virology vol 40supplement 1 pp S39ndashS46 2007
[11] K Pabbaraju K L Tokaryk S Wong and J D Fox ldquoCompari-son of the luminex xTAG respiratory viral panel with in-housenucleic acid amplification tests for diagnosis of respiratory virusinfectionsrdquo Journal of Clinical Microbiology vol 46 no 9 pp3056ndash3062 2008
[12] F S Nolte D J Marshall C Rasberry et al ldquoMultiCode-PLx system for multiplexed detection of seventeen respiratoryvirusesrdquo Journal of ClinicalMicrobiology vol 45 no 9 pp 2779ndash2786 2007
[13] H Li M A McCormac R W Estes et al ldquoSimultaneousdetection and high-throughput identification of a panel of RNAviruses causing respiratory tract infectionsrdquo Journal of ClinicalMicrobiology vol 45 no 7 pp 2105ndash2109 2007
[14] M Qin D Wang F Huang et al ldquoDetection of pandemicinfluenza AH1N1 virus by multiplex reverse transcription-PCRwith a GeXP analyzerrdquo Journal of Virological Methods vol 168no 1-2 pp 255ndash258 2010
[15] X Hu Y Zhang X Zhou et al ldquoSimultaneously typing nineserotypes of enteroviruses associated with hand foot andmouth disease by a GeXP analyzer-based multiplex reversetranscription-PCR assayrdquo Journal of Clinical Microbiology vol50 no 2 pp 288ndash293 2012
[16] J Li N Y Mao C Zhang et al ldquoThe development of aGeXP-based multiplex reverse transcription-PCR assay forsimultaneous detection of sixteen human respiratory virustypessubtypesrdquo BMC Infectious Diseases vol 12 article 1892012
[17] T TaboneD EMather andM J Hayden ldquoTemperature SwitchPCR (TSP) robust assay design for reliable amplification andgenotyping of SNPsrdquo BMC Genomics vol 10 article 580 2009
[18] Z XuW Cheng B Li J Li B Lan and Z Duan ldquoDevelopmentof a real-time PCR assay for detecting and quantifying humanbocavirus 2rdquo Journal of Clinical Microbiology vol 49 no 4 pp1537ndash1541 2011
[19] L J Cui C Zhang T Zhang et al ldquoHuman coronavirusesHCoV-NL63 and HCoV-HKU1 in hospitalized children withacute respiratory infections in Beijing Chinardquo Adv Virol vol2011 Article ID 129134 6 pages 2011
[20] F Merante S Yaghoubian and R Janeczko ldquoPrinciples of thexTAGŮ respiratory viral panel assay (RVP Assay)rdquo Journal ofClinical Virology vol 40 supplement 1 pp S31ndashS35 2007
[21] D F Bibby I Mcelarney J Breuer and D A Clark ldquoCompara-tive evaluation of the seegene seeplex RV15 and real-time PCRfor respiratory virus detectionrdquo Journal of Medical Virology vol83 no 8 pp 1469ndash1475 2011
[22] L E S Bruijnesteijn van Coppenraet C M A Swanink AA van Zwet et al ldquoComparison of two commercial molecularassays for simultaneous detection of respiratory viruses inclinical samples using two automatic electrophoresis detectionsystemsrdquo Journal of Virological Methods vol 169 no 1 pp 188ndash192 2010
[23] H K Kim S H Oh K A Yun H Sung and M N KimldquoComparison of anyplex II RV16 with xTAG respiratory viralpanel and seeplex RV15 for the detection of respiratory virusesrdquoJournal of ClinicalMicrobiology vol 51 no 4 pp 1137ndash1141 2013
[24] L Bonzel T Tenenbaum H Schroten O Schildgen SSchweitzer-Krantz and O Adams ldquoFrequent detection of viralcoinfection in children hospitalized with acute respiratory tractinfection using a real-time polymerase chain reactionrdquoPediatricInfectious Disease Journal vol 27 no 7 pp 589ndash594 2008
[25] G Cilla E Onate E G Perez-YarzaMMontes D Vicente andE Perez-Trallero ldquoViruses in community-acquired pneumoniain children aged less than 3 years old high rate of viralcoinfectionrdquo Journal of Medical Virology vol 80 no 10 pp1843ndash1849 2008
[26] N J Gadsby A Hardie E C J Claas and K E TempletonldquoComparison of the Luminex respiratory virus panel fast assaywith in-house real-time PCR for respiratory viral infectiondiagnosisrdquo Journal of Clinical Microbiology vol 48 no 6 pp2213ndash2216 2010
[27] C Calvo M L Garcıa-Garcıa C Blanco et al ldquoMultiplesimultaneous viral infections in infants with acute respiratorytract infections in Spainrdquo Journal of Clinical Virology vol 42no 3 pp 268ndash272 2008
[28] R Brittain-Long J Westin S Olofsson M Lindh and LAndersson ldquoProspective evaluation of a novel multiplex real-time PCR assay for detection of fifteen respiratory pathogens-Duration of symptoms significantly affects detection raterdquoJournal of Clinical Virology vol 47 no 3 pp 263ndash267 2010
[29] K H Rand H Rampersaud and H J Houck ldquoComparisonof two multiplex methods for detection of respiratory virusesfilmarray RP and xTAG RVPrdquo Journal of Clinical Microbiologyvol 49 no 7 pp 2449ndash2453 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
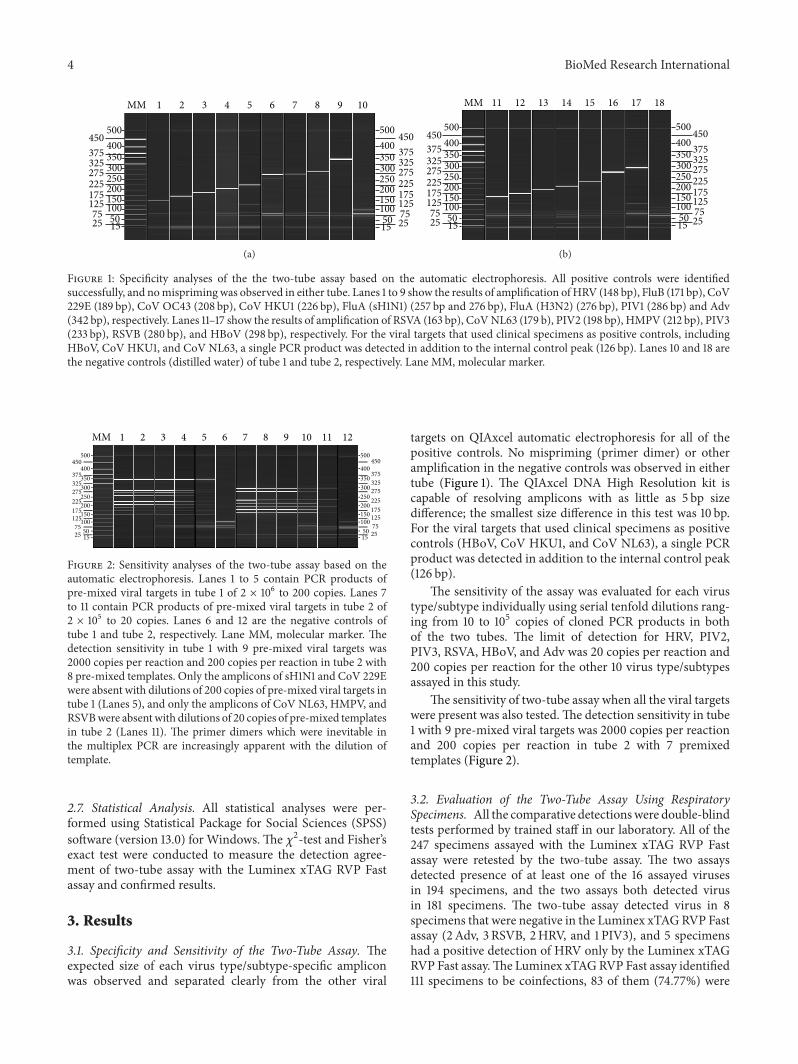
4 BioMed Research International
100
500400350300250200150
5015
450375
275325
2251751257525
100
500400350300250200150
5015
450375
275325
2251751257525
MM 1 2 3 4 5 6 7 8 9 10
(a)
100
500400350300250200150
5015
450375
275325
2251751257525
100
500400350300250200150
5015
450375
275325
2251751257525
MM 11 12 1413 15 16 17 18
(b)
Figure 1 Specificity analyses of the the two-tube assay based on the automatic electrophoresis All positive controls were identifiedsuccessfully and nomisprimingwas observed in either tube Lanes 1 to 9 show the results of amplification ofHRV (148 bp) FluB (171 bp) CoV229E (189 bp) CoV OC43 (208 bp) CoV HKU1 (226 bp) FluA (sH1N1) (257 bp and 276 bp) FluA (H3N2) (276 bp) PIV1 (286 bp) and Adv(342 bp) respectively Lanes 11ndash17 show the results of amplification of RSVA (163 bp) CoVNL63 (179 b) PIV2 (198 bp) HMPV (212 bp) PIV3(233 bp) RSVB (280 bp) and HBoV (298 bp) respectively For the viral targets that used clinical specimens as positive controls includingHBoV CoV HKU1 and CoV NL63 a single PCR product was detected in addition to the internal control peak (126 bp) Lanes 10 and 18 arethe negative controls (distilled water) of tube 1 and tube 2 respectively Lane MM molecular marker
100
500
400350300250200150
5015
450
375
275325
2251751257525
100
500
400350300250200150
5015
450
375
275325
2251751257525
MM 1 2 3 4 5 6 7 8 9 10 11 12
Figure 2 Sensitivity analyses of the two-tube assay based on theautomatic electrophoresis Lanes 1 to 5 contain PCR products ofpre-mixed viral targets in tube 1 of 2 times 106 to 200 copies Lanes 7to 11 contain PCR products of pre-mixed viral targets in tube 2 of2 times 105 to 20 copies Lanes 6 and 12 are the negative controls oftube 1 and tube 2 respectively Lane MM molecular marker Thedetection sensitivity in tube 1 with 9 pre-mixed viral targets was2000 copies per reaction and 200 copies per reaction in tube 2 with8 pre-mixed templates Only the amplicons of sH1N1 and CoV 229Ewere absent with dilutions of 200 copies of pre-mixed viral targets intube 1 (Lanes 5) and only the amplicons of CoV NL63 HMPV andRSVBwere absentwith dilutions of 20 copies of pre-mixed templatesin tube 2 (Lanes 11) The primer dimers which were inevitable inthe multiplex PCR are increasingly apparent with the dilution oftemplate
27 Statistical Analysis All statistical analyses were per-formed using Statistical Package for Social Sciences (SPSS)software (version 130) for Windows The 1205942-test and Fisherrsquosexact test were conducted to measure the detection agree-ment of two-tube assay with the Luminex xTAG RVP Fastassay and confirmed results
3 Results
31 Specificity and Sensitivity of the Two-Tube Assay Theexpected size of each virus typesubtype-specific ampliconwas observed and separated clearly from the other viral
targets on QIAxcel automatic electrophoresis for all of thepositive controls No mispriming (primer dimer) or otheramplification in the negative controls was observed in eithertube (Figure 1) The QIAxcel DNA High Resolution kit iscapable of resolving amplicons with as little as 5 bp sizedifference the smallest size difference in this test was 10 bpFor the viral targets that used clinical specimens as positivecontrols (HBoV CoV HKU1 and CoV NL63) a single PCRproduct was detected in addition to the internal control peak(126 bp)
The sensitivity of the assay was evaluated for each virustypesubtype individually using serial tenfold dilutions rang-ing from 10 to 105 copies of cloned PCR products in bothof the two tubes The limit of detection for HRV PIV2PIV3 RSVA HBoV and Adv was 20 copies per reaction and200 copies per reaction for the other 10 virus typesubtypesassayed in this study
The sensitivity of two-tube assay when all the viral targetswere present was also testedThe detection sensitivity in tube1 with 9 pre-mixed viral targets was 2000 copies per reactionand 200 copies per reaction in tube 2 with 7 premixedtemplates (Figure 2)
32 Evaluation of the Two-Tube Assay Using RespiratorySpecimens All the comparative detectionswere double-blindtests performed by trained staff in our laboratory All of the247 specimens assayed with the Luminex xTAG RVP Fastassay were retested by the two-tube assay The two assaysdetected presence of at least one of the 16 assayed virusesin 194 specimens and the two assays both detected virusin 181 specimens The two-tube assay detected virus in 8specimens that were negative in the Luminex xTAGRVP Fastassay (2Adv 3 RSVB 2HRV and 1 PIV3) and 5 specimenshad a positive detection of HRV only by the Luminex xTAGRVP Fast assayThe Luminex xTAGRVP Fast assay identified111 specimens to be coinfections 83 of them (7477) were
BioMed Research International 5
Table 2 Performance of the two-tube assay for individual target compared with the Luminex xTAG RVP Fast assay
VirusesNo of specimens two-tubeLuminex
xTAG RVP Fast assayPerformance of the two-tube assay compared with the Luminex xTAG RVP Fast
assay++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 22 2 0 223 100 9911 9167 100 9919 0952HRV 95 15 13 124 8796 8921 8636 9051 8866 0770HMPV 27 1 0 219 100 9955 9643 100 9960 0980Adv 24 11 1 211 9600 9505 6857 9953 9514 0773CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 7 1 0 239 100 9958 8750 100 9960 0931RSVB 86 10 0 151 100 9379 8958 100 9595 0913HBoV 28 0 5 214 8485 100 100 9772 9798 0907The numbers of positive and negative specimens detected by both testing methods are shown This table shows the sensitivity specificity positive predictivevalue (PPV) negative predictive value (NPV) and the kappa values for each target using the Luminex xTAG RVP Fast assay as the reference for comparisonAll the kappa values were above 075 indicating that the two assays were in agreement
in complete agreement between both assays and detectionof 13 viruses (in 12 specimens) was missed by the two-tubeassay Additional 14 viruses (in 14 coinfected specimens)were detected only by the two-tube assay and 2 coinfectionspecimens (no 28 and no 118) gave inconsistent resultsbetween the two assays (Table 3)
As shown in Table 2 there were 40 viral infectionsidentified only by the two-tube assay and 21 viral infectionsfound only by the Luminex xTAG RVP Fast assay Theinfection events not detected by the Luminex xTAG RVPFast assay included PIV3 (119899 = 2) HRV (119899 = 15) HMPV(119899 = 1) Adv (119899 = 11) RSVA (119899 = 1) and RSVB (119899 =10) Thirty-two of these undetected targets were found incoinfections and the remaining 8 targets (2 Adv 3 RSVB2HRV and 1 PIV3) were single-target positive specimens bythe two-tube assay The two-tube assay failed to detect thefollowing viral infections (119899 = 21) sH1N1 (119899 = 2) HRV(119899 = 13) Adv (119899 = 1) and HBoV (119899 = 5) Sixteen of the21 specimens were coinfections and the remaining 5 targetswere positive only for HRV specimens Because the HRVprimers used in the Luminex xTAG RVP Fast assay were ableto amplify both HRV and enterovirus the specimens positivefor HRV detected only by the Luminex xTAG RVP Fast assaycould be enteroviruses The sensitivity specificity negativeprediction value (NPV) positive prediction value (PPV) theaccordance rate and the kappa value of each virus for the two-tube assay when compared to the Luminex xTAG RVP Fastassay as a reference are shown in Table 2
33 Resolution and Confirmation of Discordant Results Allof the 40 additional targets detected only by the two-tubeassay were confirmed by sequencing as true positives Forthose specimens with discordant results by the two-tube andRVP assays the Seeplex RV15 ACE detection kit was used toresolve the discrepancy (Table 3)
The confirmed results were defined as the results detectedby at least two of the three PCR assays [22 23] or the resultsof sequencing The sensitivity specificity negative predictionvalue (NPV) positive prediction value (PPV) the accordancerate and the kappa value of each virus for the two-tube assaywhen compared to the confirmed results as a reference areshown in Table 4
4 Discussion
In this study a novel two-tube assay based on the QIAxcelcapillary electrophoresis to replace GeXP has been evaluatedfor the potential application in routine laboratory testingof respiratory viruses in China Under optimized workingcondition the two-tube assay revealed good specificity with-out nonspecific amplification using size detection systemthough conventional validation of specificity is usually doneby probe detection hybridization nested PCR and sequenc-ing The two-tube assay achieved a sensitivity of 20ndash200copies per reaction when assayed individually for each virustypesubtype and 2000 copies when 9 viral targets werepresent in tube 1 and 200 copies when 7 viral templates were
6 BioMed Research International
Table 3 The confirmed results for specimens with discordant results between the two-tube assay and the Luminex xTAG RVP Fast assay
Case no Two-tube Luminex xTAG RVP Fasta Seeplex Confirmed results43 HRV HEVHRVHBoV HRV HRV349 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB352 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB146 HMPV HMPVHBoV HMPV HMPV149 HMPV HMPVHEVHRVb andHBoV HRV HMPV HRV HMPV16 None HEVHRV HRV HRV125 RSVB RSVBHEVHRV HRV RSVB HRV RSVB262 RSVB PIV3 and HBoV RSVB PIV3 HBoV andHEVHRV PIV3 RSVB RSVB PIV3 and HBoV
270 PIV3 RSVB and HMPV PIV3 RSVB HMPV andHEVHRV PIV3 RSVB and HMPV PIV3 RSVB and HMPV
142 RSVB RSVBHEVHRV RSVB RSVB21 PIV3 PIV3HEVHRV PIV3 PIV366 None HEVHRV None None85 FluA sH1N1 and HBoV FluA (H1) HBoV andHEVHRV FluA FluA sH1N1 and HBoV87 None HEVHRV None None91 None HEVHRV None None114 None HEVHRV None None274 HRV RSVB HEVHRV RSVB and Adv HRV Adv HRV Adv and RSVB
28 FluA HBoV and Advc FluA (H1c) HBoV NDd FluA sH1N1 HBoV andAdv
118 FluA Adv RSVAc RSVBcand HBoV
FluA (H1c)HEVHRV Adv andHBoV
FluA RSVA Adv andHBOV
FluA sH1N1 Adv RSVARSVB and HBoV
aViruses with discordant results are shown in boldfacebThe Luminex xTAG RVP Fast assay was not able to distinguish rhinovirus from enterovirus so HRV positives are described as HEVHRVcThe Adv in no 28 specimen the RSVA RSVB in no 118 specimen and the FluA subtype H1 were confirmed by sequencingdND stands for not detected
Table 4 Performance of the two-tube assay for individual target compared with the confirmed results
Viruses No of specimens by two-tubeconfirmed results Performance of the two-tube assay compared with confirmed results++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 24 0 0 223 100 100 100 100 100 1000HRV 110 0 3 134 9735 100 100 9781 9879 0975HMPV 28 0 0 219 100 100 100 100 100 1000Adv 35 0 1 211 9722 100 100 9953 9960 0984CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 8 0 0 239 100 100 100 100 100 1000RSVB 96 0 0 151 100 100 100 100 100 1000HBoV 28 0 0 219 100 100 100 100 100 1000This table shows the sensitivity specificity positive predictive value (PPV) negative predictive value (NPV) and the kappa values for each target using theconfirmed results as the reference for comparison All the specificity and PPV were 100 all the accordance rate values were above 9879 and all the kappavalues were above 075
BioMed Research International 7
present in tube 2 These results suggest the utility of thetwo-tube assay for the detection of multiple respiratory virusinfections for laboratories not equipped to perform liquidchip-based multiplex assays
The 247 specimens from hospitalized children showeda high prevalence of infection and co-infection with thecommon respiratory viral pathogens HRV was found mostfrequently followed by RSVB The major discrepanciesbetween the two-tube assay introduced in this study and theLuminex xTAG RVP Fast assay were found for the detectionof HRV Adv HBoV RSVB and sH1N1 (kappa = 07700773 0907 0913 and 0929 resp) (Table 2) All of theHRV positive samples including 15 detected only by two-tube assay were confirmed by sequencing to be positive forHRV A The 13 HRV-positive specimens detected only bythe Luminex xTAG RVP Fast assay could be enterovirusesbecause of the Luminex RVP Fast assay detecting enterovirus(the HEV component of the HEVHRV) After resolved bythe Seeplex RV15 ACE detection kit three of them were trulydiscordant For Adv seven specimens identified as positiveonly by the two-tube assay were shown via sequencing to beAdv C and 4 were Adv B1 Only one Adv-positive specimenwas missed by two-tube assay For HBoV five specimensdetected as positive only by the Luminex xTAG RVP Fastassay were also negative by the Seeplex assay The other 14positive samples detected only by two-tube assay (10 RSVB2 PIV3 1 RSVA and 1HMPV) were confirmed by sequencingas true positives For sH1N1 all of the FluA positives weresequenced and 16 of 20 were sH1N1 the two-tube assay failedto detect 2 of the 16 sH1N1 positives The detection resultsof coronaviruses (CoV HKU1 CoV NL63 CoV 229E andCoV OC43) influenza (FluA FluB) PIV1 and PIV2 werecompletely consistent between the two assays In summaryno false positiveswere found by the two-tube assay and a totalof 6 false negatives occurred HRV (119899 = 3) sH1N1 (119899 = 2)and Adv (119899 = 1) The two-tube assay was more sensitivethan the Luminex xTAG RVP Fast assay for the detectionof HRV A RSVB Adv B1 and Adv C The overall detectionrate of the two-tube assay for each virus was comparable tothat of the Luminex xTAG RVP Fast assay (kappa gt 075)demonstrating the high sensitivity and specificity of the two-tube assay in the analysis of clinical samples
The two-tube assay as confirmed by the Luminex xTAGRVP Fast assay revealed that almost 80 of the respiratoryspecimens tested were positive for at least one viral infectionand viral coinfections were frequentThe overall co-infectionrates of the two-tube assay and the Luminex xTAG RVPFast assay were 4858 (120247) and 4494 (111247)respectively Compared with other similar reports [9 24ndash26]the extremely higher co-infection rate found by both assaysmight be due to the difference in the tested population andpossible nosocomial infections in the hospital
The routine use of extensive testing by methods suchas the two-tube assay should make large studies of theclinical relevance of single and multiple respiratory virusinfectionsmore feasibleThe clinical relevance of the outcomeof multiplex PCR tests for respiratory viruses is not yet fullydetermined In one study of children with RSV infectionhigher fever longer hospital stays and more frequent use
of antibiotics were associated with multiple infections [27]For some agents such as influenza A and B virus a positivetest may provide the basis for antiviral treatment [28] It hasbeen suggested that a rapid etiologic diagnosis of viral RTIcould reduce unnecessary prescription of antibiotics but thisremains to be shown [28]
Two distinct advantages of the two-tube assay are theshort assay time and the low costThe assay requires 5-6 hoursto complete 100 samples including a half hour to prepare PCRmixture the whole RT-PCR (3 hours) and the detection onthe QIAxcel automatic electrophoresis (12 tests15 minutes)while using other liquid chip-based assays might take anentire workday [29] The cost for two-tube assay is $10testincluding the RT-PCR kit and the consumables of detectionversus at least $120test [29] using other liquid chip-basedassays [29]
In conclusion the two-tube assay developed in thisstudy using automatic capillary electrophoresis is a rapidcost-effective method with high sensitivity and specificityfor the detection of respiratory virus infection and it isdemonstrated to have great potential for routine surveillanceof respiratory virus infection
Conflict of Interests
The authors declare that they have no conflict of interests
Authorsrsquo Contribution
Jin Li was involved in the operation of the two-tube assayand designing of primers with Qin Meng Xiumei Hu andHongwei Shen Dr Shunxiang Qi led the evaluation of thetwo-tube assay using the Seegene kit Dr Chen Zhang wasresponsible for providing the clinical samples and leadingthe evaluation of two-tube assay using the RVP methodwith Mrs Mengjie Yang Ji Wang and Mrs Miao Wang DrWenbo Xu offered great help in the supplement of differentclinical samples as well as shared previous experimentaldata Dr Xuejun Ma designed and coordinated the studyanalyzed data and drafted the paper Jin Li and ShunxiangQi contributed equally to the study
Acknowledgments
The authors are grateful to Dr Brian Ring from HuazhongUniversity of Science and Technology for critical reviewof this paper This work was supported by the ChinaMega Project for Infectious Disease (2011ZX10004-0012012ZX10004-215 and 2013ZX10004-202)
References
[1] M T Coiras J C Aguilar M L Garcıa I Casas and P Perez-Brena ldquoSimultaneous detection of fourteen respiratory virusesin clinical specimens by two multiplex reverse transcriptionnested-PCR assaysrdquo Journal of Medical Virology vol 72 no 3pp 484ndash495 2004
[2] A S Fauci N A Touchette and G K Folkers ldquoEmerginginfectious diseases a 10-year perspective from the National
8 BioMed Research International
Institute ofAllergy and InfectiousDiseasesrdquoEmerging InfectiousDiseases vol 11 no 4 pp 519ndash525 2005
[3] J Mahony S Chong F Merante et al ldquoDevelopment of a respi-ratory virus panel test for detection of twenty human respiratoryviruses by use of multiplex PCR and a fluid microbead-basedassayrdquo Journal of Clinical Microbiology vol 45 no 9 pp 2965ndash2970 2007
[4] F G Hayden A D M E Osterhaus J J Treanor et alldquoEfficacy and safety of the neuraminidase inhibitor zanamivirin the treatment of influenzavirus infectionsrdquoTheNew EnglandJournal of Medicine vol 337 no 13 pp 874ndash880 1997
[5] P C Y Woo S S Chiu W Seto and M Peiris ldquoCost-effectiveness of rapid diagnosis of viral respiratory tract infec-tions in pediatric patientsrdquo Journal of Clinical Microbiology vol35 no 6 pp 1579ndash1581 1997
[6] J Barenfanger C Drake N Leon T Mueller and T TrouttldquoClinical and financial benefits of rapid detection of respiratoryviruses an outcomes studyrdquo Journal of Clinical Microbiologyvol 38 no 8 pp 2824ndash2828 2000
[7] K J Henrickson D M E Osterhaus and J A McCullersldquoAdvances in the laboratory diagnosis of viral respiratorydiseaserdquo Pediatric Infectious Disease Journal vol 23 no 1 ppS6ndashS10 2004
[8] G A Storch ldquoDiagnostic virologyrdquo Clinical Infectious Diseasesvol 31 no 3 pp 739ndash751 2000
[9] F Raymond J Carbonneau N Boucher et al ldquoComparisonof automated microarray detection with real-time PCR assaysfor detection of respiratory viruses in specimens obtained fromchildrenrdquo Journal of Clinical Microbiology vol 47 pp 743ndash7502009
[10] N Krunic T D Yager D Himsworth F Merante SYaghoubian and R Janeczko ldquoxTAGŮ RVP assay analyticaland clinical performancerdquo Journal of Clinical Virology vol 40supplement 1 pp S39ndashS46 2007
[11] K Pabbaraju K L Tokaryk S Wong and J D Fox ldquoCompari-son of the luminex xTAG respiratory viral panel with in-housenucleic acid amplification tests for diagnosis of respiratory virusinfectionsrdquo Journal of Clinical Microbiology vol 46 no 9 pp3056ndash3062 2008
[12] F S Nolte D J Marshall C Rasberry et al ldquoMultiCode-PLx system for multiplexed detection of seventeen respiratoryvirusesrdquo Journal of ClinicalMicrobiology vol 45 no 9 pp 2779ndash2786 2007
[13] H Li M A McCormac R W Estes et al ldquoSimultaneousdetection and high-throughput identification of a panel of RNAviruses causing respiratory tract infectionsrdquo Journal of ClinicalMicrobiology vol 45 no 7 pp 2105ndash2109 2007
[14] M Qin D Wang F Huang et al ldquoDetection of pandemicinfluenza AH1N1 virus by multiplex reverse transcription-PCRwith a GeXP analyzerrdquo Journal of Virological Methods vol 168no 1-2 pp 255ndash258 2010
[15] X Hu Y Zhang X Zhou et al ldquoSimultaneously typing nineserotypes of enteroviruses associated with hand foot andmouth disease by a GeXP analyzer-based multiplex reversetranscription-PCR assayrdquo Journal of Clinical Microbiology vol50 no 2 pp 288ndash293 2012
[16] J Li N Y Mao C Zhang et al ldquoThe development of aGeXP-based multiplex reverse transcription-PCR assay forsimultaneous detection of sixteen human respiratory virustypessubtypesrdquo BMC Infectious Diseases vol 12 article 1892012
[17] T TaboneD EMather andM J Hayden ldquoTemperature SwitchPCR (TSP) robust assay design for reliable amplification andgenotyping of SNPsrdquo BMC Genomics vol 10 article 580 2009
[18] Z XuW Cheng B Li J Li B Lan and Z Duan ldquoDevelopmentof a real-time PCR assay for detecting and quantifying humanbocavirus 2rdquo Journal of Clinical Microbiology vol 49 no 4 pp1537ndash1541 2011
[19] L J Cui C Zhang T Zhang et al ldquoHuman coronavirusesHCoV-NL63 and HCoV-HKU1 in hospitalized children withacute respiratory infections in Beijing Chinardquo Adv Virol vol2011 Article ID 129134 6 pages 2011
[20] F Merante S Yaghoubian and R Janeczko ldquoPrinciples of thexTAGŮ respiratory viral panel assay (RVP Assay)rdquo Journal ofClinical Virology vol 40 supplement 1 pp S31ndashS35 2007
[21] D F Bibby I Mcelarney J Breuer and D A Clark ldquoCompara-tive evaluation of the seegene seeplex RV15 and real-time PCRfor respiratory virus detectionrdquo Journal of Medical Virology vol83 no 8 pp 1469ndash1475 2011
[22] L E S Bruijnesteijn van Coppenraet C M A Swanink AA van Zwet et al ldquoComparison of two commercial molecularassays for simultaneous detection of respiratory viruses inclinical samples using two automatic electrophoresis detectionsystemsrdquo Journal of Virological Methods vol 169 no 1 pp 188ndash192 2010
[23] H K Kim S H Oh K A Yun H Sung and M N KimldquoComparison of anyplex II RV16 with xTAG respiratory viralpanel and seeplex RV15 for the detection of respiratory virusesrdquoJournal of ClinicalMicrobiology vol 51 no 4 pp 1137ndash1141 2013
[24] L Bonzel T Tenenbaum H Schroten O Schildgen SSchweitzer-Krantz and O Adams ldquoFrequent detection of viralcoinfection in children hospitalized with acute respiratory tractinfection using a real-time polymerase chain reactionrdquoPediatricInfectious Disease Journal vol 27 no 7 pp 589ndash594 2008
[25] G Cilla E Onate E G Perez-YarzaMMontes D Vicente andE Perez-Trallero ldquoViruses in community-acquired pneumoniain children aged less than 3 years old high rate of viralcoinfectionrdquo Journal of Medical Virology vol 80 no 10 pp1843ndash1849 2008
[26] N J Gadsby A Hardie E C J Claas and K E TempletonldquoComparison of the Luminex respiratory virus panel fast assaywith in-house real-time PCR for respiratory viral infectiondiagnosisrdquo Journal of Clinical Microbiology vol 48 no 6 pp2213ndash2216 2010
[27] C Calvo M L Garcıa-Garcıa C Blanco et al ldquoMultiplesimultaneous viral infections in infants with acute respiratorytract infections in Spainrdquo Journal of Clinical Virology vol 42no 3 pp 268ndash272 2008
[28] R Brittain-Long J Westin S Olofsson M Lindh and LAndersson ldquoProspective evaluation of a novel multiplex real-time PCR assay for detection of fifteen respiratory pathogens-Duration of symptoms significantly affects detection raterdquoJournal of Clinical Virology vol 47 no 3 pp 263ndash267 2010
[29] K H Rand H Rampersaud and H J Houck ldquoComparisonof two multiplex methods for detection of respiratory virusesfilmarray RP and xTAG RVPrdquo Journal of Clinical Microbiologyvol 49 no 7 pp 2449ndash2453 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
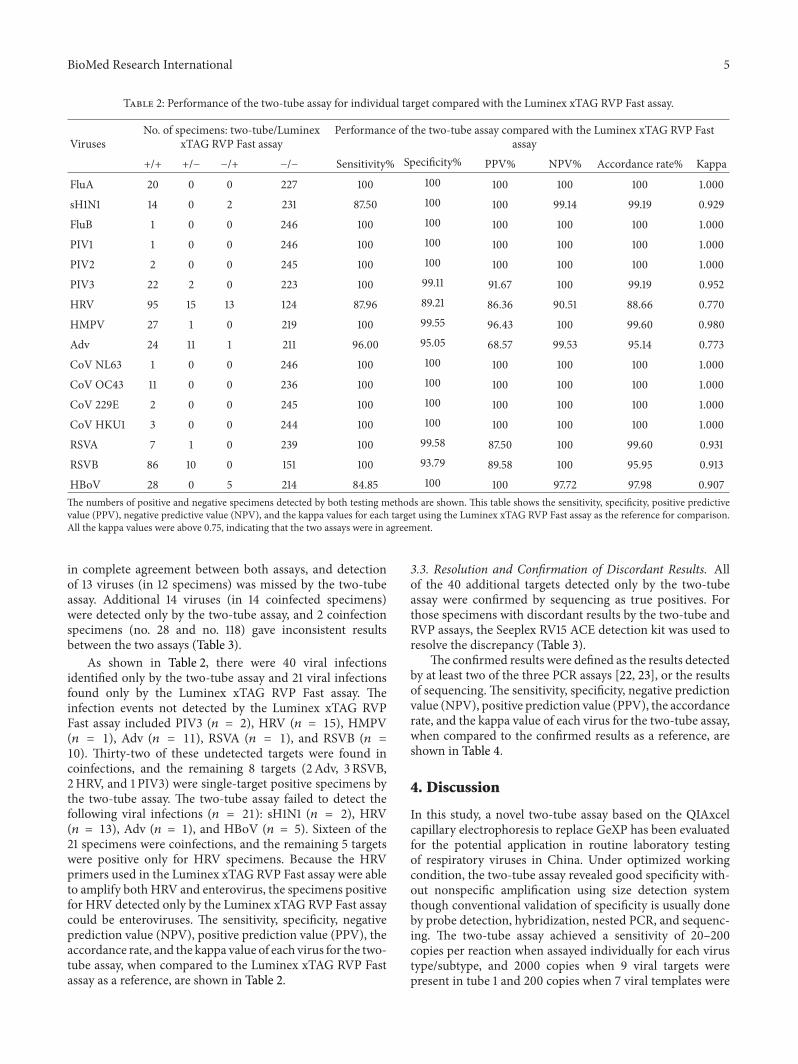
BioMed Research International 5
Table 2 Performance of the two-tube assay for individual target compared with the Luminex xTAG RVP Fast assay
VirusesNo of specimens two-tubeLuminex
xTAG RVP Fast assayPerformance of the two-tube assay compared with the Luminex xTAG RVP Fast
assay++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 22 2 0 223 100 9911 9167 100 9919 0952HRV 95 15 13 124 8796 8921 8636 9051 8866 0770HMPV 27 1 0 219 100 9955 9643 100 9960 0980Adv 24 11 1 211 9600 9505 6857 9953 9514 0773CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 7 1 0 239 100 9958 8750 100 9960 0931RSVB 86 10 0 151 100 9379 8958 100 9595 0913HBoV 28 0 5 214 8485 100 100 9772 9798 0907The numbers of positive and negative specimens detected by both testing methods are shown This table shows the sensitivity specificity positive predictivevalue (PPV) negative predictive value (NPV) and the kappa values for each target using the Luminex xTAG RVP Fast assay as the reference for comparisonAll the kappa values were above 075 indicating that the two assays were in agreement
in complete agreement between both assays and detectionof 13 viruses (in 12 specimens) was missed by the two-tubeassay Additional 14 viruses (in 14 coinfected specimens)were detected only by the two-tube assay and 2 coinfectionspecimens (no 28 and no 118) gave inconsistent resultsbetween the two assays (Table 3)
As shown in Table 2 there were 40 viral infectionsidentified only by the two-tube assay and 21 viral infectionsfound only by the Luminex xTAG RVP Fast assay Theinfection events not detected by the Luminex xTAG RVPFast assay included PIV3 (119899 = 2) HRV (119899 = 15) HMPV(119899 = 1) Adv (119899 = 11) RSVA (119899 = 1) and RSVB (119899 =10) Thirty-two of these undetected targets were found incoinfections and the remaining 8 targets (2 Adv 3 RSVB2HRV and 1 PIV3) were single-target positive specimens bythe two-tube assay The two-tube assay failed to detect thefollowing viral infections (119899 = 21) sH1N1 (119899 = 2) HRV(119899 = 13) Adv (119899 = 1) and HBoV (119899 = 5) Sixteen of the21 specimens were coinfections and the remaining 5 targetswere positive only for HRV specimens Because the HRVprimers used in the Luminex xTAG RVP Fast assay were ableto amplify both HRV and enterovirus the specimens positivefor HRV detected only by the Luminex xTAG RVP Fast assaycould be enteroviruses The sensitivity specificity negativeprediction value (NPV) positive prediction value (PPV) theaccordance rate and the kappa value of each virus for the two-tube assay when compared to the Luminex xTAG RVP Fastassay as a reference are shown in Table 2
33 Resolution and Confirmation of Discordant Results Allof the 40 additional targets detected only by the two-tubeassay were confirmed by sequencing as true positives Forthose specimens with discordant results by the two-tube andRVP assays the Seeplex RV15 ACE detection kit was used toresolve the discrepancy (Table 3)
The confirmed results were defined as the results detectedby at least two of the three PCR assays [22 23] or the resultsof sequencing The sensitivity specificity negative predictionvalue (NPV) positive prediction value (PPV) the accordancerate and the kappa value of each virus for the two-tube assaywhen compared to the confirmed results as a reference areshown in Table 4
4 Discussion
In this study a novel two-tube assay based on the QIAxcelcapillary electrophoresis to replace GeXP has been evaluatedfor the potential application in routine laboratory testingof respiratory viruses in China Under optimized workingcondition the two-tube assay revealed good specificity with-out nonspecific amplification using size detection systemthough conventional validation of specificity is usually doneby probe detection hybridization nested PCR and sequenc-ing The two-tube assay achieved a sensitivity of 20ndash200copies per reaction when assayed individually for each virustypesubtype and 2000 copies when 9 viral targets werepresent in tube 1 and 200 copies when 7 viral templates were
6 BioMed Research International
Table 3 The confirmed results for specimens with discordant results between the two-tube assay and the Luminex xTAG RVP Fast assay
Case no Two-tube Luminex xTAG RVP Fasta Seeplex Confirmed results43 HRV HEVHRVHBoV HRV HRV349 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB352 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB146 HMPV HMPVHBoV HMPV HMPV149 HMPV HMPVHEVHRVb andHBoV HRV HMPV HRV HMPV16 None HEVHRV HRV HRV125 RSVB RSVBHEVHRV HRV RSVB HRV RSVB262 RSVB PIV3 and HBoV RSVB PIV3 HBoV andHEVHRV PIV3 RSVB RSVB PIV3 and HBoV
270 PIV3 RSVB and HMPV PIV3 RSVB HMPV andHEVHRV PIV3 RSVB and HMPV PIV3 RSVB and HMPV
142 RSVB RSVBHEVHRV RSVB RSVB21 PIV3 PIV3HEVHRV PIV3 PIV366 None HEVHRV None None85 FluA sH1N1 and HBoV FluA (H1) HBoV andHEVHRV FluA FluA sH1N1 and HBoV87 None HEVHRV None None91 None HEVHRV None None114 None HEVHRV None None274 HRV RSVB HEVHRV RSVB and Adv HRV Adv HRV Adv and RSVB
28 FluA HBoV and Advc FluA (H1c) HBoV NDd FluA sH1N1 HBoV andAdv
118 FluA Adv RSVAc RSVBcand HBoV
FluA (H1c)HEVHRV Adv andHBoV
FluA RSVA Adv andHBOV
FluA sH1N1 Adv RSVARSVB and HBoV
aViruses with discordant results are shown in boldfacebThe Luminex xTAG RVP Fast assay was not able to distinguish rhinovirus from enterovirus so HRV positives are described as HEVHRVcThe Adv in no 28 specimen the RSVA RSVB in no 118 specimen and the FluA subtype H1 were confirmed by sequencingdND stands for not detected
Table 4 Performance of the two-tube assay for individual target compared with the confirmed results
Viruses No of specimens by two-tubeconfirmed results Performance of the two-tube assay compared with confirmed results++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 24 0 0 223 100 100 100 100 100 1000HRV 110 0 3 134 9735 100 100 9781 9879 0975HMPV 28 0 0 219 100 100 100 100 100 1000Adv 35 0 1 211 9722 100 100 9953 9960 0984CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 8 0 0 239 100 100 100 100 100 1000RSVB 96 0 0 151 100 100 100 100 100 1000HBoV 28 0 0 219 100 100 100 100 100 1000This table shows the sensitivity specificity positive predictive value (PPV) negative predictive value (NPV) and the kappa values for each target using theconfirmed results as the reference for comparison All the specificity and PPV were 100 all the accordance rate values were above 9879 and all the kappavalues were above 075
BioMed Research International 7
present in tube 2 These results suggest the utility of thetwo-tube assay for the detection of multiple respiratory virusinfections for laboratories not equipped to perform liquidchip-based multiplex assays
The 247 specimens from hospitalized children showeda high prevalence of infection and co-infection with thecommon respiratory viral pathogens HRV was found mostfrequently followed by RSVB The major discrepanciesbetween the two-tube assay introduced in this study and theLuminex xTAG RVP Fast assay were found for the detectionof HRV Adv HBoV RSVB and sH1N1 (kappa = 07700773 0907 0913 and 0929 resp) (Table 2) All of theHRV positive samples including 15 detected only by two-tube assay were confirmed by sequencing to be positive forHRV A The 13 HRV-positive specimens detected only bythe Luminex xTAG RVP Fast assay could be enterovirusesbecause of the Luminex RVP Fast assay detecting enterovirus(the HEV component of the HEVHRV) After resolved bythe Seeplex RV15 ACE detection kit three of them were trulydiscordant For Adv seven specimens identified as positiveonly by the two-tube assay were shown via sequencing to beAdv C and 4 were Adv B1 Only one Adv-positive specimenwas missed by two-tube assay For HBoV five specimensdetected as positive only by the Luminex xTAG RVP Fastassay were also negative by the Seeplex assay The other 14positive samples detected only by two-tube assay (10 RSVB2 PIV3 1 RSVA and 1HMPV) were confirmed by sequencingas true positives For sH1N1 all of the FluA positives weresequenced and 16 of 20 were sH1N1 the two-tube assay failedto detect 2 of the 16 sH1N1 positives The detection resultsof coronaviruses (CoV HKU1 CoV NL63 CoV 229E andCoV OC43) influenza (FluA FluB) PIV1 and PIV2 werecompletely consistent between the two assays In summaryno false positiveswere found by the two-tube assay and a totalof 6 false negatives occurred HRV (119899 = 3) sH1N1 (119899 = 2)and Adv (119899 = 1) The two-tube assay was more sensitivethan the Luminex xTAG RVP Fast assay for the detectionof HRV A RSVB Adv B1 and Adv C The overall detectionrate of the two-tube assay for each virus was comparable tothat of the Luminex xTAG RVP Fast assay (kappa gt 075)demonstrating the high sensitivity and specificity of the two-tube assay in the analysis of clinical samples
The two-tube assay as confirmed by the Luminex xTAGRVP Fast assay revealed that almost 80 of the respiratoryspecimens tested were positive for at least one viral infectionand viral coinfections were frequentThe overall co-infectionrates of the two-tube assay and the Luminex xTAG RVPFast assay were 4858 (120247) and 4494 (111247)respectively Compared with other similar reports [9 24ndash26]the extremely higher co-infection rate found by both assaysmight be due to the difference in the tested population andpossible nosocomial infections in the hospital
The routine use of extensive testing by methods suchas the two-tube assay should make large studies of theclinical relevance of single and multiple respiratory virusinfectionsmore feasibleThe clinical relevance of the outcomeof multiplex PCR tests for respiratory viruses is not yet fullydetermined In one study of children with RSV infectionhigher fever longer hospital stays and more frequent use
of antibiotics were associated with multiple infections [27]For some agents such as influenza A and B virus a positivetest may provide the basis for antiviral treatment [28] It hasbeen suggested that a rapid etiologic diagnosis of viral RTIcould reduce unnecessary prescription of antibiotics but thisremains to be shown [28]
Two distinct advantages of the two-tube assay are theshort assay time and the low costThe assay requires 5-6 hoursto complete 100 samples including a half hour to prepare PCRmixture the whole RT-PCR (3 hours) and the detection onthe QIAxcel automatic electrophoresis (12 tests15 minutes)while using other liquid chip-based assays might take anentire workday [29] The cost for two-tube assay is $10testincluding the RT-PCR kit and the consumables of detectionversus at least $120test [29] using other liquid chip-basedassays [29]
In conclusion the two-tube assay developed in thisstudy using automatic capillary electrophoresis is a rapidcost-effective method with high sensitivity and specificityfor the detection of respiratory virus infection and it isdemonstrated to have great potential for routine surveillanceof respiratory virus infection
Conflict of Interests
The authors declare that they have no conflict of interests
Authorsrsquo Contribution
Jin Li was involved in the operation of the two-tube assayand designing of primers with Qin Meng Xiumei Hu andHongwei Shen Dr Shunxiang Qi led the evaluation of thetwo-tube assay using the Seegene kit Dr Chen Zhang wasresponsible for providing the clinical samples and leadingthe evaluation of two-tube assay using the RVP methodwith Mrs Mengjie Yang Ji Wang and Mrs Miao Wang DrWenbo Xu offered great help in the supplement of differentclinical samples as well as shared previous experimentaldata Dr Xuejun Ma designed and coordinated the studyanalyzed data and drafted the paper Jin Li and ShunxiangQi contributed equally to the study
Acknowledgments
The authors are grateful to Dr Brian Ring from HuazhongUniversity of Science and Technology for critical reviewof this paper This work was supported by the ChinaMega Project for Infectious Disease (2011ZX10004-0012012ZX10004-215 and 2013ZX10004-202)
References
[1] M T Coiras J C Aguilar M L Garcıa I Casas and P Perez-Brena ldquoSimultaneous detection of fourteen respiratory virusesin clinical specimens by two multiplex reverse transcriptionnested-PCR assaysrdquo Journal of Medical Virology vol 72 no 3pp 484ndash495 2004
[2] A S Fauci N A Touchette and G K Folkers ldquoEmerginginfectious diseases a 10-year perspective from the National
8 BioMed Research International
Institute ofAllergy and InfectiousDiseasesrdquoEmerging InfectiousDiseases vol 11 no 4 pp 519ndash525 2005
[3] J Mahony S Chong F Merante et al ldquoDevelopment of a respi-ratory virus panel test for detection of twenty human respiratoryviruses by use of multiplex PCR and a fluid microbead-basedassayrdquo Journal of Clinical Microbiology vol 45 no 9 pp 2965ndash2970 2007
[4] F G Hayden A D M E Osterhaus J J Treanor et alldquoEfficacy and safety of the neuraminidase inhibitor zanamivirin the treatment of influenzavirus infectionsrdquoTheNew EnglandJournal of Medicine vol 337 no 13 pp 874ndash880 1997
[5] P C Y Woo S S Chiu W Seto and M Peiris ldquoCost-effectiveness of rapid diagnosis of viral respiratory tract infec-tions in pediatric patientsrdquo Journal of Clinical Microbiology vol35 no 6 pp 1579ndash1581 1997
[6] J Barenfanger C Drake N Leon T Mueller and T TrouttldquoClinical and financial benefits of rapid detection of respiratoryviruses an outcomes studyrdquo Journal of Clinical Microbiologyvol 38 no 8 pp 2824ndash2828 2000
[7] K J Henrickson D M E Osterhaus and J A McCullersldquoAdvances in the laboratory diagnosis of viral respiratorydiseaserdquo Pediatric Infectious Disease Journal vol 23 no 1 ppS6ndashS10 2004
[8] G A Storch ldquoDiagnostic virologyrdquo Clinical Infectious Diseasesvol 31 no 3 pp 739ndash751 2000
[9] F Raymond J Carbonneau N Boucher et al ldquoComparisonof automated microarray detection with real-time PCR assaysfor detection of respiratory viruses in specimens obtained fromchildrenrdquo Journal of Clinical Microbiology vol 47 pp 743ndash7502009
[10] N Krunic T D Yager D Himsworth F Merante SYaghoubian and R Janeczko ldquoxTAGŮ RVP assay analyticaland clinical performancerdquo Journal of Clinical Virology vol 40supplement 1 pp S39ndashS46 2007
[11] K Pabbaraju K L Tokaryk S Wong and J D Fox ldquoCompari-son of the luminex xTAG respiratory viral panel with in-housenucleic acid amplification tests for diagnosis of respiratory virusinfectionsrdquo Journal of Clinical Microbiology vol 46 no 9 pp3056ndash3062 2008
[12] F S Nolte D J Marshall C Rasberry et al ldquoMultiCode-PLx system for multiplexed detection of seventeen respiratoryvirusesrdquo Journal of ClinicalMicrobiology vol 45 no 9 pp 2779ndash2786 2007
[13] H Li M A McCormac R W Estes et al ldquoSimultaneousdetection and high-throughput identification of a panel of RNAviruses causing respiratory tract infectionsrdquo Journal of ClinicalMicrobiology vol 45 no 7 pp 2105ndash2109 2007
[14] M Qin D Wang F Huang et al ldquoDetection of pandemicinfluenza AH1N1 virus by multiplex reverse transcription-PCRwith a GeXP analyzerrdquo Journal of Virological Methods vol 168no 1-2 pp 255ndash258 2010
[15] X Hu Y Zhang X Zhou et al ldquoSimultaneously typing nineserotypes of enteroviruses associated with hand foot andmouth disease by a GeXP analyzer-based multiplex reversetranscription-PCR assayrdquo Journal of Clinical Microbiology vol50 no 2 pp 288ndash293 2012
[16] J Li N Y Mao C Zhang et al ldquoThe development of aGeXP-based multiplex reverse transcription-PCR assay forsimultaneous detection of sixteen human respiratory virustypessubtypesrdquo BMC Infectious Diseases vol 12 article 1892012
[17] T TaboneD EMather andM J Hayden ldquoTemperature SwitchPCR (TSP) robust assay design for reliable amplification andgenotyping of SNPsrdquo BMC Genomics vol 10 article 580 2009
[18] Z XuW Cheng B Li J Li B Lan and Z Duan ldquoDevelopmentof a real-time PCR assay for detecting and quantifying humanbocavirus 2rdquo Journal of Clinical Microbiology vol 49 no 4 pp1537ndash1541 2011
[19] L J Cui C Zhang T Zhang et al ldquoHuman coronavirusesHCoV-NL63 and HCoV-HKU1 in hospitalized children withacute respiratory infections in Beijing Chinardquo Adv Virol vol2011 Article ID 129134 6 pages 2011
[20] F Merante S Yaghoubian and R Janeczko ldquoPrinciples of thexTAGŮ respiratory viral panel assay (RVP Assay)rdquo Journal ofClinical Virology vol 40 supplement 1 pp S31ndashS35 2007
[21] D F Bibby I Mcelarney J Breuer and D A Clark ldquoCompara-tive evaluation of the seegene seeplex RV15 and real-time PCRfor respiratory virus detectionrdquo Journal of Medical Virology vol83 no 8 pp 1469ndash1475 2011
[22] L E S Bruijnesteijn van Coppenraet C M A Swanink AA van Zwet et al ldquoComparison of two commercial molecularassays for simultaneous detection of respiratory viruses inclinical samples using two automatic electrophoresis detectionsystemsrdquo Journal of Virological Methods vol 169 no 1 pp 188ndash192 2010
[23] H K Kim S H Oh K A Yun H Sung and M N KimldquoComparison of anyplex II RV16 with xTAG respiratory viralpanel and seeplex RV15 for the detection of respiratory virusesrdquoJournal of ClinicalMicrobiology vol 51 no 4 pp 1137ndash1141 2013
[24] L Bonzel T Tenenbaum H Schroten O Schildgen SSchweitzer-Krantz and O Adams ldquoFrequent detection of viralcoinfection in children hospitalized with acute respiratory tractinfection using a real-time polymerase chain reactionrdquoPediatricInfectious Disease Journal vol 27 no 7 pp 589ndash594 2008
[25] G Cilla E Onate E G Perez-YarzaMMontes D Vicente andE Perez-Trallero ldquoViruses in community-acquired pneumoniain children aged less than 3 years old high rate of viralcoinfectionrdquo Journal of Medical Virology vol 80 no 10 pp1843ndash1849 2008
[26] N J Gadsby A Hardie E C J Claas and K E TempletonldquoComparison of the Luminex respiratory virus panel fast assaywith in-house real-time PCR for respiratory viral infectiondiagnosisrdquo Journal of Clinical Microbiology vol 48 no 6 pp2213ndash2216 2010
[27] C Calvo M L Garcıa-Garcıa C Blanco et al ldquoMultiplesimultaneous viral infections in infants with acute respiratorytract infections in Spainrdquo Journal of Clinical Virology vol 42no 3 pp 268ndash272 2008
[28] R Brittain-Long J Westin S Olofsson M Lindh and LAndersson ldquoProspective evaluation of a novel multiplex real-time PCR assay for detection of fifteen respiratory pathogens-Duration of symptoms significantly affects detection raterdquoJournal of Clinical Virology vol 47 no 3 pp 263ndash267 2010
[29] K H Rand H Rampersaud and H J Houck ldquoComparisonof two multiplex methods for detection of respiratory virusesfilmarray RP and xTAG RVPrdquo Journal of Clinical Microbiologyvol 49 no 7 pp 2449ndash2453 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 BioMed Research International
Table 3 The confirmed results for specimens with discordant results between the two-tube assay and the Luminex xTAG RVP Fast assay
Case no Two-tube Luminex xTAG RVP Fasta Seeplex Confirmed results43 HRV HEVHRVHBoV HRV HRV349 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB352 HRV RSVB HEVHRV RSVB andHBoV HRV RSVB HRV RSVB146 HMPV HMPVHBoV HMPV HMPV149 HMPV HMPVHEVHRVb andHBoV HRV HMPV HRV HMPV16 None HEVHRV HRV HRV125 RSVB RSVBHEVHRV HRV RSVB HRV RSVB262 RSVB PIV3 and HBoV RSVB PIV3 HBoV andHEVHRV PIV3 RSVB RSVB PIV3 and HBoV
270 PIV3 RSVB and HMPV PIV3 RSVB HMPV andHEVHRV PIV3 RSVB and HMPV PIV3 RSVB and HMPV
142 RSVB RSVBHEVHRV RSVB RSVB21 PIV3 PIV3HEVHRV PIV3 PIV366 None HEVHRV None None85 FluA sH1N1 and HBoV FluA (H1) HBoV andHEVHRV FluA FluA sH1N1 and HBoV87 None HEVHRV None None91 None HEVHRV None None114 None HEVHRV None None274 HRV RSVB HEVHRV RSVB and Adv HRV Adv HRV Adv and RSVB
28 FluA HBoV and Advc FluA (H1c) HBoV NDd FluA sH1N1 HBoV andAdv
118 FluA Adv RSVAc RSVBcand HBoV
FluA (H1c)HEVHRV Adv andHBoV
FluA RSVA Adv andHBOV
FluA sH1N1 Adv RSVARSVB and HBoV
aViruses with discordant results are shown in boldfacebThe Luminex xTAG RVP Fast assay was not able to distinguish rhinovirus from enterovirus so HRV positives are described as HEVHRVcThe Adv in no 28 specimen the RSVA RSVB in no 118 specimen and the FluA subtype H1 were confirmed by sequencingdND stands for not detected
Table 4 Performance of the two-tube assay for individual target compared with the confirmed results
Viruses No of specimens by two-tubeconfirmed results Performance of the two-tube assay compared with confirmed results++ +minus minus+ minusminus Sensitivity Specificity PPV NPV Accordance rate Kappa
FluA 20 0 0 227 100 100 100 100 100 1000sH1N1 14 0 2 231 8750 100 100 9914 9919 0929FluB 1 0 0 246 100 100 100 100 100 1000PIV1 1 0 0 246 100 100 100 100 100 1000PIV2 2 0 0 245 100 100 100 100 100 1000PIV3 24 0 0 223 100 100 100 100 100 1000HRV 110 0 3 134 9735 100 100 9781 9879 0975HMPV 28 0 0 219 100 100 100 100 100 1000Adv 35 0 1 211 9722 100 100 9953 9960 0984CoV NL63 1 0 0 246 100 100 100 100 100 1000CoV OC43 11 0 0 236 100 100 100 100 100 1000CoV 229E 2 0 0 245 100 100 100 100 100 1000CoV HKU1 3 0 0 244 100 100 100 100 100 1000RSVA 8 0 0 239 100 100 100 100 100 1000RSVB 96 0 0 151 100 100 100 100 100 1000HBoV 28 0 0 219 100 100 100 100 100 1000This table shows the sensitivity specificity positive predictive value (PPV) negative predictive value (NPV) and the kappa values for each target using theconfirmed results as the reference for comparison All the specificity and PPV were 100 all the accordance rate values were above 9879 and all the kappavalues were above 075
BioMed Research International 7
present in tube 2 These results suggest the utility of thetwo-tube assay for the detection of multiple respiratory virusinfections for laboratories not equipped to perform liquidchip-based multiplex assays
The 247 specimens from hospitalized children showeda high prevalence of infection and co-infection with thecommon respiratory viral pathogens HRV was found mostfrequently followed by RSVB The major discrepanciesbetween the two-tube assay introduced in this study and theLuminex xTAG RVP Fast assay were found for the detectionof HRV Adv HBoV RSVB and sH1N1 (kappa = 07700773 0907 0913 and 0929 resp) (Table 2) All of theHRV positive samples including 15 detected only by two-tube assay were confirmed by sequencing to be positive forHRV A The 13 HRV-positive specimens detected only bythe Luminex xTAG RVP Fast assay could be enterovirusesbecause of the Luminex RVP Fast assay detecting enterovirus(the HEV component of the HEVHRV) After resolved bythe Seeplex RV15 ACE detection kit three of them were trulydiscordant For Adv seven specimens identified as positiveonly by the two-tube assay were shown via sequencing to beAdv C and 4 were Adv B1 Only one Adv-positive specimenwas missed by two-tube assay For HBoV five specimensdetected as positive only by the Luminex xTAG RVP Fastassay were also negative by the Seeplex assay The other 14positive samples detected only by two-tube assay (10 RSVB2 PIV3 1 RSVA and 1HMPV) were confirmed by sequencingas true positives For sH1N1 all of the FluA positives weresequenced and 16 of 20 were sH1N1 the two-tube assay failedto detect 2 of the 16 sH1N1 positives The detection resultsof coronaviruses (CoV HKU1 CoV NL63 CoV 229E andCoV OC43) influenza (FluA FluB) PIV1 and PIV2 werecompletely consistent between the two assays In summaryno false positiveswere found by the two-tube assay and a totalof 6 false negatives occurred HRV (119899 = 3) sH1N1 (119899 = 2)and Adv (119899 = 1) The two-tube assay was more sensitivethan the Luminex xTAG RVP Fast assay for the detectionof HRV A RSVB Adv B1 and Adv C The overall detectionrate of the two-tube assay for each virus was comparable tothat of the Luminex xTAG RVP Fast assay (kappa gt 075)demonstrating the high sensitivity and specificity of the two-tube assay in the analysis of clinical samples
The two-tube assay as confirmed by the Luminex xTAGRVP Fast assay revealed that almost 80 of the respiratoryspecimens tested were positive for at least one viral infectionand viral coinfections were frequentThe overall co-infectionrates of the two-tube assay and the Luminex xTAG RVPFast assay were 4858 (120247) and 4494 (111247)respectively Compared with other similar reports [9 24ndash26]the extremely higher co-infection rate found by both assaysmight be due to the difference in the tested population andpossible nosocomial infections in the hospital
The routine use of extensive testing by methods suchas the two-tube assay should make large studies of theclinical relevance of single and multiple respiratory virusinfectionsmore feasibleThe clinical relevance of the outcomeof multiplex PCR tests for respiratory viruses is not yet fullydetermined In one study of children with RSV infectionhigher fever longer hospital stays and more frequent use
of antibiotics were associated with multiple infections [27]For some agents such as influenza A and B virus a positivetest may provide the basis for antiviral treatment [28] It hasbeen suggested that a rapid etiologic diagnosis of viral RTIcould reduce unnecessary prescription of antibiotics but thisremains to be shown [28]
Two distinct advantages of the two-tube assay are theshort assay time and the low costThe assay requires 5-6 hoursto complete 100 samples including a half hour to prepare PCRmixture the whole RT-PCR (3 hours) and the detection onthe QIAxcel automatic electrophoresis (12 tests15 minutes)while using other liquid chip-based assays might take anentire workday [29] The cost for two-tube assay is $10testincluding the RT-PCR kit and the consumables of detectionversus at least $120test [29] using other liquid chip-basedassays [29]
In conclusion the two-tube assay developed in thisstudy using automatic capillary electrophoresis is a rapidcost-effective method with high sensitivity and specificityfor the detection of respiratory virus infection and it isdemonstrated to have great potential for routine surveillanceof respiratory virus infection
Conflict of Interests
The authors declare that they have no conflict of interests
Authorsrsquo Contribution
Jin Li was involved in the operation of the two-tube assayand designing of primers with Qin Meng Xiumei Hu andHongwei Shen Dr Shunxiang Qi led the evaluation of thetwo-tube assay using the Seegene kit Dr Chen Zhang wasresponsible for providing the clinical samples and leadingthe evaluation of two-tube assay using the RVP methodwith Mrs Mengjie Yang Ji Wang and Mrs Miao Wang DrWenbo Xu offered great help in the supplement of differentclinical samples as well as shared previous experimentaldata Dr Xuejun Ma designed and coordinated the studyanalyzed data and drafted the paper Jin Li and ShunxiangQi contributed equally to the study
Acknowledgments
The authors are grateful to Dr Brian Ring from HuazhongUniversity of Science and Technology for critical reviewof this paper This work was supported by the ChinaMega Project for Infectious Disease (2011ZX10004-0012012ZX10004-215 and 2013ZX10004-202)
References
[1] M T Coiras J C Aguilar M L Garcıa I Casas and P Perez-Brena ldquoSimultaneous detection of fourteen respiratory virusesin clinical specimens by two multiplex reverse transcriptionnested-PCR assaysrdquo Journal of Medical Virology vol 72 no 3pp 484ndash495 2004
[2] A S Fauci N A Touchette and G K Folkers ldquoEmerginginfectious diseases a 10-year perspective from the National
8 BioMed Research International
Institute ofAllergy and InfectiousDiseasesrdquoEmerging InfectiousDiseases vol 11 no 4 pp 519ndash525 2005
[3] J Mahony S Chong F Merante et al ldquoDevelopment of a respi-ratory virus panel test for detection of twenty human respiratoryviruses by use of multiplex PCR and a fluid microbead-basedassayrdquo Journal of Clinical Microbiology vol 45 no 9 pp 2965ndash2970 2007
[4] F G Hayden A D M E Osterhaus J J Treanor et alldquoEfficacy and safety of the neuraminidase inhibitor zanamivirin the treatment of influenzavirus infectionsrdquoTheNew EnglandJournal of Medicine vol 337 no 13 pp 874ndash880 1997
[5] P C Y Woo S S Chiu W Seto and M Peiris ldquoCost-effectiveness of rapid diagnosis of viral respiratory tract infec-tions in pediatric patientsrdquo Journal of Clinical Microbiology vol35 no 6 pp 1579ndash1581 1997
[6] J Barenfanger C Drake N Leon T Mueller and T TrouttldquoClinical and financial benefits of rapid detection of respiratoryviruses an outcomes studyrdquo Journal of Clinical Microbiologyvol 38 no 8 pp 2824ndash2828 2000
[7] K J Henrickson D M E Osterhaus and J A McCullersldquoAdvances in the laboratory diagnosis of viral respiratorydiseaserdquo Pediatric Infectious Disease Journal vol 23 no 1 ppS6ndashS10 2004
[8] G A Storch ldquoDiagnostic virologyrdquo Clinical Infectious Diseasesvol 31 no 3 pp 739ndash751 2000
[9] F Raymond J Carbonneau N Boucher et al ldquoComparisonof automated microarray detection with real-time PCR assaysfor detection of respiratory viruses in specimens obtained fromchildrenrdquo Journal of Clinical Microbiology vol 47 pp 743ndash7502009
[10] N Krunic T D Yager D Himsworth F Merante SYaghoubian and R Janeczko ldquoxTAGŮ RVP assay analyticaland clinical performancerdquo Journal of Clinical Virology vol 40supplement 1 pp S39ndashS46 2007
[11] K Pabbaraju K L Tokaryk S Wong and J D Fox ldquoCompari-son of the luminex xTAG respiratory viral panel with in-housenucleic acid amplification tests for diagnosis of respiratory virusinfectionsrdquo Journal of Clinical Microbiology vol 46 no 9 pp3056ndash3062 2008
[12] F S Nolte D J Marshall C Rasberry et al ldquoMultiCode-PLx system for multiplexed detection of seventeen respiratoryvirusesrdquo Journal of ClinicalMicrobiology vol 45 no 9 pp 2779ndash2786 2007
[13] H Li M A McCormac R W Estes et al ldquoSimultaneousdetection and high-throughput identification of a panel of RNAviruses causing respiratory tract infectionsrdquo Journal of ClinicalMicrobiology vol 45 no 7 pp 2105ndash2109 2007
[14] M Qin D Wang F Huang et al ldquoDetection of pandemicinfluenza AH1N1 virus by multiplex reverse transcription-PCRwith a GeXP analyzerrdquo Journal of Virological Methods vol 168no 1-2 pp 255ndash258 2010
[15] X Hu Y Zhang X Zhou et al ldquoSimultaneously typing nineserotypes of enteroviruses associated with hand foot andmouth disease by a GeXP analyzer-based multiplex reversetranscription-PCR assayrdquo Journal of Clinical Microbiology vol50 no 2 pp 288ndash293 2012
[16] J Li N Y Mao C Zhang et al ldquoThe development of aGeXP-based multiplex reverse transcription-PCR assay forsimultaneous detection of sixteen human respiratory virustypessubtypesrdquo BMC Infectious Diseases vol 12 article 1892012
[17] T TaboneD EMather andM J Hayden ldquoTemperature SwitchPCR (TSP) robust assay design for reliable amplification andgenotyping of SNPsrdquo BMC Genomics vol 10 article 580 2009
[18] Z XuW Cheng B Li J Li B Lan and Z Duan ldquoDevelopmentof a real-time PCR assay for detecting and quantifying humanbocavirus 2rdquo Journal of Clinical Microbiology vol 49 no 4 pp1537ndash1541 2011
[19] L J Cui C Zhang T Zhang et al ldquoHuman coronavirusesHCoV-NL63 and HCoV-HKU1 in hospitalized children withacute respiratory infections in Beijing Chinardquo Adv Virol vol2011 Article ID 129134 6 pages 2011
[20] F Merante S Yaghoubian and R Janeczko ldquoPrinciples of thexTAGŮ respiratory viral panel assay (RVP Assay)rdquo Journal ofClinical Virology vol 40 supplement 1 pp S31ndashS35 2007
[21] D F Bibby I Mcelarney J Breuer and D A Clark ldquoCompara-tive evaluation of the seegene seeplex RV15 and real-time PCRfor respiratory virus detectionrdquo Journal of Medical Virology vol83 no 8 pp 1469ndash1475 2011
[22] L E S Bruijnesteijn van Coppenraet C M A Swanink AA van Zwet et al ldquoComparison of two commercial molecularassays for simultaneous detection of respiratory viruses inclinical samples using two automatic electrophoresis detectionsystemsrdquo Journal of Virological Methods vol 169 no 1 pp 188ndash192 2010
[23] H K Kim S H Oh K A Yun H Sung and M N KimldquoComparison of anyplex II RV16 with xTAG respiratory viralpanel and seeplex RV15 for the detection of respiratory virusesrdquoJournal of ClinicalMicrobiology vol 51 no 4 pp 1137ndash1141 2013
[24] L Bonzel T Tenenbaum H Schroten O Schildgen SSchweitzer-Krantz and O Adams ldquoFrequent detection of viralcoinfection in children hospitalized with acute respiratory tractinfection using a real-time polymerase chain reactionrdquoPediatricInfectious Disease Journal vol 27 no 7 pp 589ndash594 2008
[25] G Cilla E Onate E G Perez-YarzaMMontes D Vicente andE Perez-Trallero ldquoViruses in community-acquired pneumoniain children aged less than 3 years old high rate of viralcoinfectionrdquo Journal of Medical Virology vol 80 no 10 pp1843ndash1849 2008
[26] N J Gadsby A Hardie E C J Claas and K E TempletonldquoComparison of the Luminex respiratory virus panel fast assaywith in-house real-time PCR for respiratory viral infectiondiagnosisrdquo Journal of Clinical Microbiology vol 48 no 6 pp2213ndash2216 2010
[27] C Calvo M L Garcıa-Garcıa C Blanco et al ldquoMultiplesimultaneous viral infections in infants with acute respiratorytract infections in Spainrdquo Journal of Clinical Virology vol 42no 3 pp 268ndash272 2008
[28] R Brittain-Long J Westin S Olofsson M Lindh and LAndersson ldquoProspective evaluation of a novel multiplex real-time PCR assay for detection of fifteen respiratory pathogens-Duration of symptoms significantly affects detection raterdquoJournal of Clinical Virology vol 47 no 3 pp 263ndash267 2010
[29] K H Rand H Rampersaud and H J Houck ldquoComparisonof two multiplex methods for detection of respiratory virusesfilmarray RP and xTAG RVPrdquo Journal of Clinical Microbiologyvol 49 no 7 pp 2449ndash2453 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 7
present in tube 2 These results suggest the utility of thetwo-tube assay for the detection of multiple respiratory virusinfections for laboratories not equipped to perform liquidchip-based multiplex assays
The 247 specimens from hospitalized children showeda high prevalence of infection and co-infection with thecommon respiratory viral pathogens HRV was found mostfrequently followed by RSVB The major discrepanciesbetween the two-tube assay introduced in this study and theLuminex xTAG RVP Fast assay were found for the detectionof HRV Adv HBoV RSVB and sH1N1 (kappa = 07700773 0907 0913 and 0929 resp) (Table 2) All of theHRV positive samples including 15 detected only by two-tube assay were confirmed by sequencing to be positive forHRV A The 13 HRV-positive specimens detected only bythe Luminex xTAG RVP Fast assay could be enterovirusesbecause of the Luminex RVP Fast assay detecting enterovirus(the HEV component of the HEVHRV) After resolved bythe Seeplex RV15 ACE detection kit three of them were trulydiscordant For Adv seven specimens identified as positiveonly by the two-tube assay were shown via sequencing to beAdv C and 4 were Adv B1 Only one Adv-positive specimenwas missed by two-tube assay For HBoV five specimensdetected as positive only by the Luminex xTAG RVP Fastassay were also negative by the Seeplex assay The other 14positive samples detected only by two-tube assay (10 RSVB2 PIV3 1 RSVA and 1HMPV) were confirmed by sequencingas true positives For sH1N1 all of the FluA positives weresequenced and 16 of 20 were sH1N1 the two-tube assay failedto detect 2 of the 16 sH1N1 positives The detection resultsof coronaviruses (CoV HKU1 CoV NL63 CoV 229E andCoV OC43) influenza (FluA FluB) PIV1 and PIV2 werecompletely consistent between the two assays In summaryno false positiveswere found by the two-tube assay and a totalof 6 false negatives occurred HRV (119899 = 3) sH1N1 (119899 = 2)and Adv (119899 = 1) The two-tube assay was more sensitivethan the Luminex xTAG RVP Fast assay for the detectionof HRV A RSVB Adv B1 and Adv C The overall detectionrate of the two-tube assay for each virus was comparable tothat of the Luminex xTAG RVP Fast assay (kappa gt 075)demonstrating the high sensitivity and specificity of the two-tube assay in the analysis of clinical samples
The two-tube assay as confirmed by the Luminex xTAGRVP Fast assay revealed that almost 80 of the respiratoryspecimens tested were positive for at least one viral infectionand viral coinfections were frequentThe overall co-infectionrates of the two-tube assay and the Luminex xTAG RVPFast assay were 4858 (120247) and 4494 (111247)respectively Compared with other similar reports [9 24ndash26]the extremely higher co-infection rate found by both assaysmight be due to the difference in the tested population andpossible nosocomial infections in the hospital
The routine use of extensive testing by methods suchas the two-tube assay should make large studies of theclinical relevance of single and multiple respiratory virusinfectionsmore feasibleThe clinical relevance of the outcomeof multiplex PCR tests for respiratory viruses is not yet fullydetermined In one study of children with RSV infectionhigher fever longer hospital stays and more frequent use
of antibiotics were associated with multiple infections [27]For some agents such as influenza A and B virus a positivetest may provide the basis for antiviral treatment [28] It hasbeen suggested that a rapid etiologic diagnosis of viral RTIcould reduce unnecessary prescription of antibiotics but thisremains to be shown [28]
Two distinct advantages of the two-tube assay are theshort assay time and the low costThe assay requires 5-6 hoursto complete 100 samples including a half hour to prepare PCRmixture the whole RT-PCR (3 hours) and the detection onthe QIAxcel automatic electrophoresis (12 tests15 minutes)while using other liquid chip-based assays might take anentire workday [29] The cost for two-tube assay is $10testincluding the RT-PCR kit and the consumables of detectionversus at least $120test [29] using other liquid chip-basedassays [29]
In conclusion the two-tube assay developed in thisstudy using automatic capillary electrophoresis is a rapidcost-effective method with high sensitivity and specificityfor the detection of respiratory virus infection and it isdemonstrated to have great potential for routine surveillanceof respiratory virus infection
Conflict of Interests
The authors declare that they have no conflict of interests
Authorsrsquo Contribution
Jin Li was involved in the operation of the two-tube assayand designing of primers with Qin Meng Xiumei Hu andHongwei Shen Dr Shunxiang Qi led the evaluation of thetwo-tube assay using the Seegene kit Dr Chen Zhang wasresponsible for providing the clinical samples and leadingthe evaluation of two-tube assay using the RVP methodwith Mrs Mengjie Yang Ji Wang and Mrs Miao Wang DrWenbo Xu offered great help in the supplement of differentclinical samples as well as shared previous experimentaldata Dr Xuejun Ma designed and coordinated the studyanalyzed data and drafted the paper Jin Li and ShunxiangQi contributed equally to the study
Acknowledgments
The authors are grateful to Dr Brian Ring from HuazhongUniversity of Science and Technology for critical reviewof this paper This work was supported by the ChinaMega Project for Infectious Disease (2011ZX10004-0012012ZX10004-215 and 2013ZX10004-202)
References
[1] M T Coiras J C Aguilar M L Garcıa I Casas and P Perez-Brena ldquoSimultaneous detection of fourteen respiratory virusesin clinical specimens by two multiplex reverse transcriptionnested-PCR assaysrdquo Journal of Medical Virology vol 72 no 3pp 484ndash495 2004
[2] A S Fauci N A Touchette and G K Folkers ldquoEmerginginfectious diseases a 10-year perspective from the National
8 BioMed Research International
Institute ofAllergy and InfectiousDiseasesrdquoEmerging InfectiousDiseases vol 11 no 4 pp 519ndash525 2005
[3] J Mahony S Chong F Merante et al ldquoDevelopment of a respi-ratory virus panel test for detection of twenty human respiratoryviruses by use of multiplex PCR and a fluid microbead-basedassayrdquo Journal of Clinical Microbiology vol 45 no 9 pp 2965ndash2970 2007
[4] F G Hayden A D M E Osterhaus J J Treanor et alldquoEfficacy and safety of the neuraminidase inhibitor zanamivirin the treatment of influenzavirus infectionsrdquoTheNew EnglandJournal of Medicine vol 337 no 13 pp 874ndash880 1997
[5] P C Y Woo S S Chiu W Seto and M Peiris ldquoCost-effectiveness of rapid diagnosis of viral respiratory tract infec-tions in pediatric patientsrdquo Journal of Clinical Microbiology vol35 no 6 pp 1579ndash1581 1997
[6] J Barenfanger C Drake N Leon T Mueller and T TrouttldquoClinical and financial benefits of rapid detection of respiratoryviruses an outcomes studyrdquo Journal of Clinical Microbiologyvol 38 no 8 pp 2824ndash2828 2000
[7] K J Henrickson D M E Osterhaus and J A McCullersldquoAdvances in the laboratory diagnosis of viral respiratorydiseaserdquo Pediatric Infectious Disease Journal vol 23 no 1 ppS6ndashS10 2004
[8] G A Storch ldquoDiagnostic virologyrdquo Clinical Infectious Diseasesvol 31 no 3 pp 739ndash751 2000
[9] F Raymond J Carbonneau N Boucher et al ldquoComparisonof automated microarray detection with real-time PCR assaysfor detection of respiratory viruses in specimens obtained fromchildrenrdquo Journal of Clinical Microbiology vol 47 pp 743ndash7502009
[10] N Krunic T D Yager D Himsworth F Merante SYaghoubian and R Janeczko ldquoxTAGŮ RVP assay analyticaland clinical performancerdquo Journal of Clinical Virology vol 40supplement 1 pp S39ndashS46 2007
[11] K Pabbaraju K L Tokaryk S Wong and J D Fox ldquoCompari-son of the luminex xTAG respiratory viral panel with in-housenucleic acid amplification tests for diagnosis of respiratory virusinfectionsrdquo Journal of Clinical Microbiology vol 46 no 9 pp3056ndash3062 2008
[12] F S Nolte D J Marshall C Rasberry et al ldquoMultiCode-PLx system for multiplexed detection of seventeen respiratoryvirusesrdquo Journal of ClinicalMicrobiology vol 45 no 9 pp 2779ndash2786 2007
[13] H Li M A McCormac R W Estes et al ldquoSimultaneousdetection and high-throughput identification of a panel of RNAviruses causing respiratory tract infectionsrdquo Journal of ClinicalMicrobiology vol 45 no 7 pp 2105ndash2109 2007
[14] M Qin D Wang F Huang et al ldquoDetection of pandemicinfluenza AH1N1 virus by multiplex reverse transcription-PCRwith a GeXP analyzerrdquo Journal of Virological Methods vol 168no 1-2 pp 255ndash258 2010
[15] X Hu Y Zhang X Zhou et al ldquoSimultaneously typing nineserotypes of enteroviruses associated with hand foot andmouth disease by a GeXP analyzer-based multiplex reversetranscription-PCR assayrdquo Journal of Clinical Microbiology vol50 no 2 pp 288ndash293 2012
[16] J Li N Y Mao C Zhang et al ldquoThe development of aGeXP-based multiplex reverse transcription-PCR assay forsimultaneous detection of sixteen human respiratory virustypessubtypesrdquo BMC Infectious Diseases vol 12 article 1892012
[17] T TaboneD EMather andM J Hayden ldquoTemperature SwitchPCR (TSP) robust assay design for reliable amplification andgenotyping of SNPsrdquo BMC Genomics vol 10 article 580 2009
[18] Z XuW Cheng B Li J Li B Lan and Z Duan ldquoDevelopmentof a real-time PCR assay for detecting and quantifying humanbocavirus 2rdquo Journal of Clinical Microbiology vol 49 no 4 pp1537ndash1541 2011
[19] L J Cui C Zhang T Zhang et al ldquoHuman coronavirusesHCoV-NL63 and HCoV-HKU1 in hospitalized children withacute respiratory infections in Beijing Chinardquo Adv Virol vol2011 Article ID 129134 6 pages 2011
[20] F Merante S Yaghoubian and R Janeczko ldquoPrinciples of thexTAGŮ respiratory viral panel assay (RVP Assay)rdquo Journal ofClinical Virology vol 40 supplement 1 pp S31ndashS35 2007
[21] D F Bibby I Mcelarney J Breuer and D A Clark ldquoCompara-tive evaluation of the seegene seeplex RV15 and real-time PCRfor respiratory virus detectionrdquo Journal of Medical Virology vol83 no 8 pp 1469ndash1475 2011
[22] L E S Bruijnesteijn van Coppenraet C M A Swanink AA van Zwet et al ldquoComparison of two commercial molecularassays for simultaneous detection of respiratory viruses inclinical samples using two automatic electrophoresis detectionsystemsrdquo Journal of Virological Methods vol 169 no 1 pp 188ndash192 2010
[23] H K Kim S H Oh K A Yun H Sung and M N KimldquoComparison of anyplex II RV16 with xTAG respiratory viralpanel and seeplex RV15 for the detection of respiratory virusesrdquoJournal of ClinicalMicrobiology vol 51 no 4 pp 1137ndash1141 2013
[24] L Bonzel T Tenenbaum H Schroten O Schildgen SSchweitzer-Krantz and O Adams ldquoFrequent detection of viralcoinfection in children hospitalized with acute respiratory tractinfection using a real-time polymerase chain reactionrdquoPediatricInfectious Disease Journal vol 27 no 7 pp 589ndash594 2008
[25] G Cilla E Onate E G Perez-YarzaMMontes D Vicente andE Perez-Trallero ldquoViruses in community-acquired pneumoniain children aged less than 3 years old high rate of viralcoinfectionrdquo Journal of Medical Virology vol 80 no 10 pp1843ndash1849 2008
[26] N J Gadsby A Hardie E C J Claas and K E TempletonldquoComparison of the Luminex respiratory virus panel fast assaywith in-house real-time PCR for respiratory viral infectiondiagnosisrdquo Journal of Clinical Microbiology vol 48 no 6 pp2213ndash2216 2010
[27] C Calvo M L Garcıa-Garcıa C Blanco et al ldquoMultiplesimultaneous viral infections in infants with acute respiratorytract infections in Spainrdquo Journal of Clinical Virology vol 42no 3 pp 268ndash272 2008
[28] R Brittain-Long J Westin S Olofsson M Lindh and LAndersson ldquoProspective evaluation of a novel multiplex real-time PCR assay for detection of fifteen respiratory pathogens-Duration of symptoms significantly affects detection raterdquoJournal of Clinical Virology vol 47 no 3 pp 263ndash267 2010
[29] K H Rand H Rampersaud and H J Houck ldquoComparisonof two multiplex methods for detection of respiratory virusesfilmarray RP and xTAG RVPrdquo Journal of Clinical Microbiologyvol 49 no 7 pp 2449ndash2453 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
8 BioMed Research International
Institute ofAllergy and InfectiousDiseasesrdquoEmerging InfectiousDiseases vol 11 no 4 pp 519ndash525 2005
[3] J Mahony S Chong F Merante et al ldquoDevelopment of a respi-ratory virus panel test for detection of twenty human respiratoryviruses by use of multiplex PCR and a fluid microbead-basedassayrdquo Journal of Clinical Microbiology vol 45 no 9 pp 2965ndash2970 2007
[4] F G Hayden A D M E Osterhaus J J Treanor et alldquoEfficacy and safety of the neuraminidase inhibitor zanamivirin the treatment of influenzavirus infectionsrdquoTheNew EnglandJournal of Medicine vol 337 no 13 pp 874ndash880 1997
[5] P C Y Woo S S Chiu W Seto and M Peiris ldquoCost-effectiveness of rapid diagnosis of viral respiratory tract infec-tions in pediatric patientsrdquo Journal of Clinical Microbiology vol35 no 6 pp 1579ndash1581 1997
[6] J Barenfanger C Drake N Leon T Mueller and T TrouttldquoClinical and financial benefits of rapid detection of respiratoryviruses an outcomes studyrdquo Journal of Clinical Microbiologyvol 38 no 8 pp 2824ndash2828 2000
[7] K J Henrickson D M E Osterhaus and J A McCullersldquoAdvances in the laboratory diagnosis of viral respiratorydiseaserdquo Pediatric Infectious Disease Journal vol 23 no 1 ppS6ndashS10 2004
[8] G A Storch ldquoDiagnostic virologyrdquo Clinical Infectious Diseasesvol 31 no 3 pp 739ndash751 2000
[9] F Raymond J Carbonneau N Boucher et al ldquoComparisonof automated microarray detection with real-time PCR assaysfor detection of respiratory viruses in specimens obtained fromchildrenrdquo Journal of Clinical Microbiology vol 47 pp 743ndash7502009
[10] N Krunic T D Yager D Himsworth F Merante SYaghoubian and R Janeczko ldquoxTAGŮ RVP assay analyticaland clinical performancerdquo Journal of Clinical Virology vol 40supplement 1 pp S39ndashS46 2007
[11] K Pabbaraju K L Tokaryk S Wong and J D Fox ldquoCompari-son of the luminex xTAG respiratory viral panel with in-housenucleic acid amplification tests for diagnosis of respiratory virusinfectionsrdquo Journal of Clinical Microbiology vol 46 no 9 pp3056ndash3062 2008
[12] F S Nolte D J Marshall C Rasberry et al ldquoMultiCode-PLx system for multiplexed detection of seventeen respiratoryvirusesrdquo Journal of ClinicalMicrobiology vol 45 no 9 pp 2779ndash2786 2007
[13] H Li M A McCormac R W Estes et al ldquoSimultaneousdetection and high-throughput identification of a panel of RNAviruses causing respiratory tract infectionsrdquo Journal of ClinicalMicrobiology vol 45 no 7 pp 2105ndash2109 2007
[14] M Qin D Wang F Huang et al ldquoDetection of pandemicinfluenza AH1N1 virus by multiplex reverse transcription-PCRwith a GeXP analyzerrdquo Journal of Virological Methods vol 168no 1-2 pp 255ndash258 2010
[15] X Hu Y Zhang X Zhou et al ldquoSimultaneously typing nineserotypes of enteroviruses associated with hand foot andmouth disease by a GeXP analyzer-based multiplex reversetranscription-PCR assayrdquo Journal of Clinical Microbiology vol50 no 2 pp 288ndash293 2012
[16] J Li N Y Mao C Zhang et al ldquoThe development of aGeXP-based multiplex reverse transcription-PCR assay forsimultaneous detection of sixteen human respiratory virustypessubtypesrdquo BMC Infectious Diseases vol 12 article 1892012
[17] T TaboneD EMather andM J Hayden ldquoTemperature SwitchPCR (TSP) robust assay design for reliable amplification andgenotyping of SNPsrdquo BMC Genomics vol 10 article 580 2009
[18] Z XuW Cheng B Li J Li B Lan and Z Duan ldquoDevelopmentof a real-time PCR assay for detecting and quantifying humanbocavirus 2rdquo Journal of Clinical Microbiology vol 49 no 4 pp1537ndash1541 2011
[19] L J Cui C Zhang T Zhang et al ldquoHuman coronavirusesHCoV-NL63 and HCoV-HKU1 in hospitalized children withacute respiratory infections in Beijing Chinardquo Adv Virol vol2011 Article ID 129134 6 pages 2011
[20] F Merante S Yaghoubian and R Janeczko ldquoPrinciples of thexTAGŮ respiratory viral panel assay (RVP Assay)rdquo Journal ofClinical Virology vol 40 supplement 1 pp S31ndashS35 2007
[21] D F Bibby I Mcelarney J Breuer and D A Clark ldquoCompara-tive evaluation of the seegene seeplex RV15 and real-time PCRfor respiratory virus detectionrdquo Journal of Medical Virology vol83 no 8 pp 1469ndash1475 2011
[22] L E S Bruijnesteijn van Coppenraet C M A Swanink AA van Zwet et al ldquoComparison of two commercial molecularassays for simultaneous detection of respiratory viruses inclinical samples using two automatic electrophoresis detectionsystemsrdquo Journal of Virological Methods vol 169 no 1 pp 188ndash192 2010
[23] H K Kim S H Oh K A Yun H Sung and M N KimldquoComparison of anyplex II RV16 with xTAG respiratory viralpanel and seeplex RV15 for the detection of respiratory virusesrdquoJournal of ClinicalMicrobiology vol 51 no 4 pp 1137ndash1141 2013
[24] L Bonzel T Tenenbaum H Schroten O Schildgen SSchweitzer-Krantz and O Adams ldquoFrequent detection of viralcoinfection in children hospitalized with acute respiratory tractinfection using a real-time polymerase chain reactionrdquoPediatricInfectious Disease Journal vol 27 no 7 pp 589ndash594 2008
[25] G Cilla E Onate E G Perez-YarzaMMontes D Vicente andE Perez-Trallero ldquoViruses in community-acquired pneumoniain children aged less than 3 years old high rate of viralcoinfectionrdquo Journal of Medical Virology vol 80 no 10 pp1843ndash1849 2008
[26] N J Gadsby A Hardie E C J Claas and K E TempletonldquoComparison of the Luminex respiratory virus panel fast assaywith in-house real-time PCR for respiratory viral infectiondiagnosisrdquo Journal of Clinical Microbiology vol 48 no 6 pp2213ndash2216 2010
[27] C Calvo M L Garcıa-Garcıa C Blanco et al ldquoMultiplesimultaneous viral infections in infants with acute respiratorytract infections in Spainrdquo Journal of Clinical Virology vol 42no 3 pp 268ndash272 2008
[28] R Brittain-Long J Westin S Olofsson M Lindh and LAndersson ldquoProspective evaluation of a novel multiplex real-time PCR assay for detection of fifteen respiratory pathogens-Duration of symptoms significantly affects detection raterdquoJournal of Clinical Virology vol 47 no 3 pp 263ndash267 2010
[29] K H Rand H Rampersaud and H J Houck ldquoComparisonof two multiplex methods for detection of respiratory virusesfilmarray RP and xTAG RVPrdquo Journal of Clinical Microbiologyvol 49 no 7 pp 2449ndash2453 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom


















