
Research agenda for prognostication: what´s next? congresses/2014/ppt... · Formulating the...
30
Research agenda for prognostication: what´s next? Paul Glare Memorial Sloan Kettering Cancer Center New York, NY, USA June 2014
Transcript of Research agenda for prognostication: what´s next? congresses/2014/ppt... · Formulating the...

Research agenda for prognostication: what´s next?
Paul Glare Memorial Sloan Kettering Cancer Center
New York, NY, USA June 2014

Aims
• Review ‘state of the science’ of prognostication in palliative care
• Describe a broader conceptualization of prognostication in advanced disease
• What can we learn about prognostication from other academic disciplines?

I want to die at
home, Paul
Newman tells his
family as he's given
'weeks to live' By Andy Dolan Last updated at 6:43 PM on 08th August 2008
Died 27th September 2008
Frail: Paul Newman is wheeled
out of hospital

I want to die at
home, Paul
Newman tells his
family as he's given
'weeks to live' By Andy Dolan Last updated at 6:43 PM on 08th August 2008
Died 27th September 2008
Frail: Paul Newman is wheeled
out of hospital
Using prognostic information
Communicating the prognosis
Formulating the prognosis

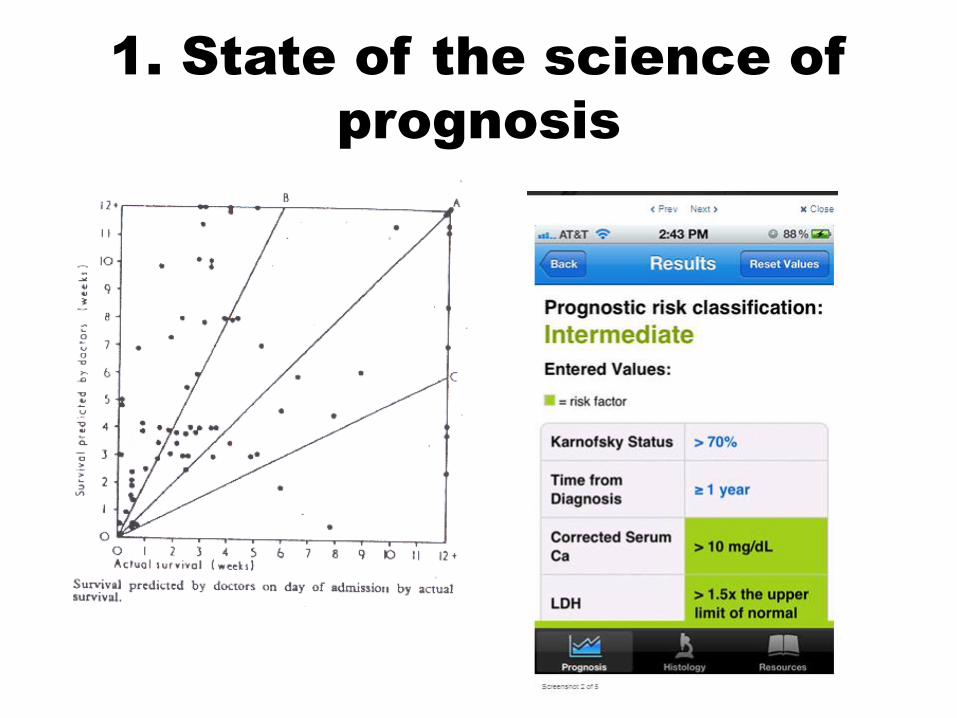
1. State of the science of
prognosis
1. State of the science of
prognosis

Hypothesis
PS and weight loss = ‘final pathway’
Translational research
Predictive factors
e.g. CRP
Clinical trials
Prognostic models
e.g. PIPS
Systematic Reviews:
Pred factors, CPS
Guidelines/
Implementation
Gold Std. Framework
The Research Cycle & Prognosis
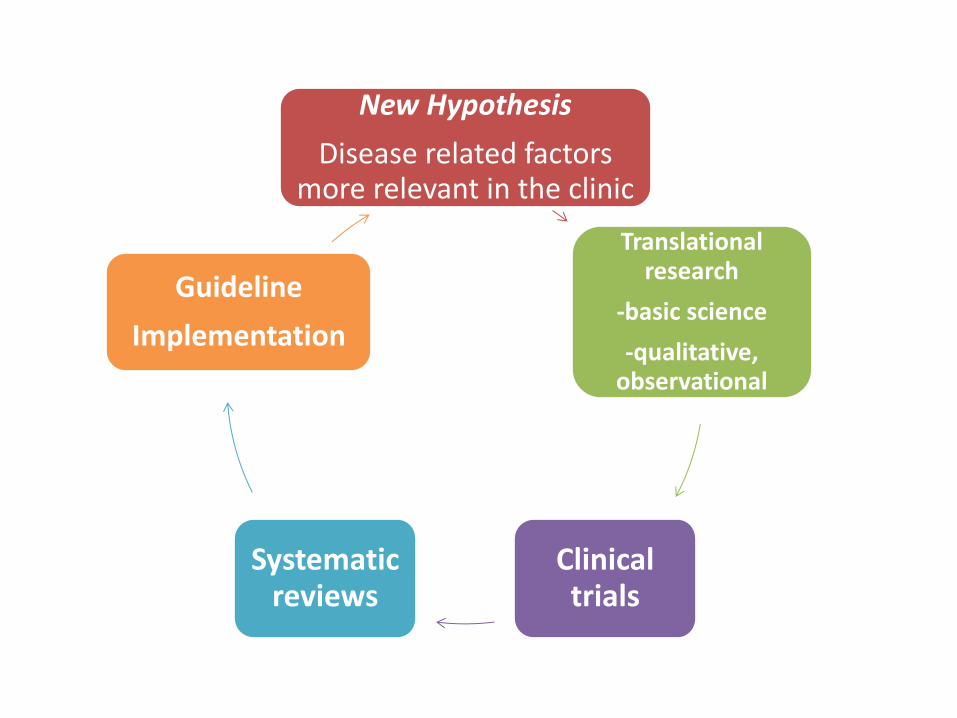
New Hypothesis
Disease related factors more relevant in the clinic
Translational research
-basic science
-qualitative, observational
Clinical trials
Systematic reviews
Guideline
Implementation

RESEARCH METHODS
& REPORTING
Prognosis and prognostic research: what, why, and how? Karel G M Moons,1 Patrick Royston,2 Yvonne Vergouwe,1 Diederick E Grobbee,1 Douglas G Altman3
Doctors have little specific research to draw on when predicting outcome. In this first article in a series Karel Moons and colleagues explain why research into prognosis is important and how to design such research Cite this as: BMJ 2009;338:b375 doi: 10.1136/bmj.b375 This article is the first in a series of four aiming to provide an accessible overview of the principles and methods of prognostic research

Setting a research agenda
on prognosis
A. Research on formulating the prognosis
B. Research on communicating the prognosis
C. Research on using prognostic information optimally
• What we already know
• Opportunities
• Challenges
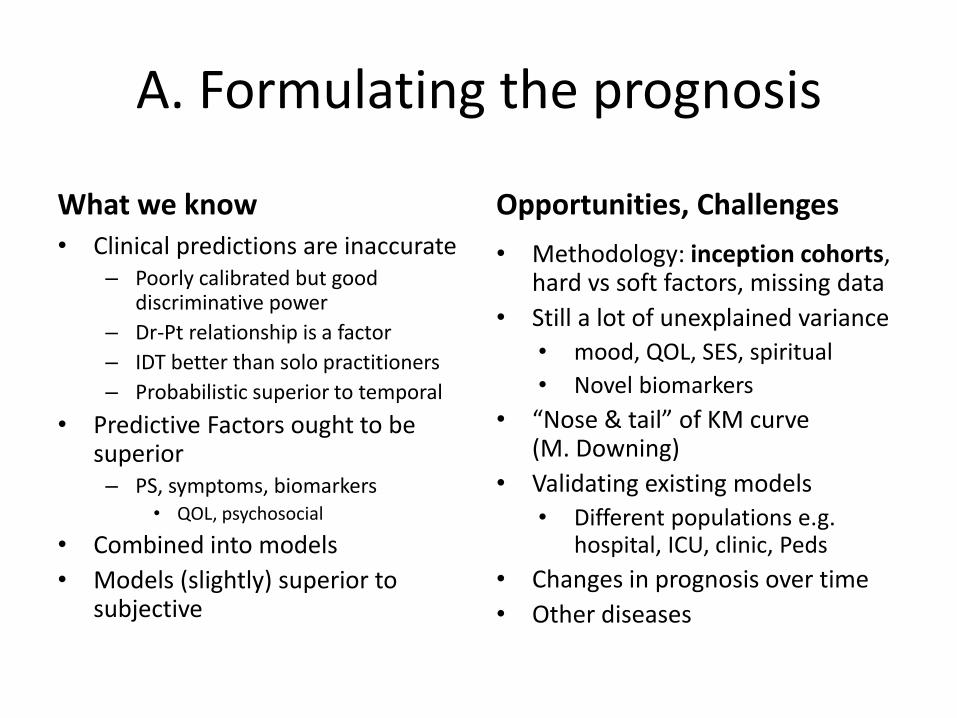
A. Formulating the prognosis
What we know • Clinical predictions are inaccurate
– Poorly calibrated but good discriminative power
– Dr-Pt relationship is a factor
– IDT better than solo practitioners
– Probabilistic superior to temporal
• Predictive Factors ought to be superior – PS, symptoms, biomarkers
• QOL, psychosocial
• Combined into models
• Models (slightly) superior to subjective
Opportunities, Challenges
• Methodology: inception cohorts, hard vs soft factors, missing data
• Still a lot of unexplained variance
• mood, QOL, SES, spiritual
• Novel biomarkers
• “Nose & tail” of KM curve (M. Downing)
• Validating existing models
• Different populations e.g. hospital, ICU, clinic, Peds
• Changes in prognosis over time
• Other diseases
Prognosisresearchstrategy(PROGRESS)1:A frameworkforresearchingclinicaloutcomes OPENACCESS Understanding and improving the prognosis of a disease or health condition is a priority in clinical research and practice. In this article, the authors introduce a framework of four interrelated themes in prognosis research, describe the importance of the first of these themes (understanding future outcomes in relation to current diagnostic and treatment practices), and introduce recommendations for the field of prognosis research HarryHemingwayprofessorofclinicalepidemiology1,PeterCroftprofessorofepidemiology2,Pablo Perelclinicalseniorlecturer3,JillAHaydenassistantprofessor4,KeithAbramsprofessorofmedical statistics5,AdamTimmisprofessorofclinicalcardiology6,AndrewBriggsLindsaychairinhealth policy&economicevaluation7,RuzanUdumyanresearchassistant1,KarelGMMoonsprofessor ofclinicalepidemiology8,EwoutWSteyerbergprofessorofmedicaldecisionmaking9,IanRoberts professorofepidemiologyandpublichealth3,SaraSchroterseniorresearcher10,DouglasGAltman professorofstatisticsinmedicine11,RichardDRileyseniorlecturerinmedicalstatistics12,forthe PROGRESSGroup
BMJ BMJ 2013; 346: e5595doi:10.1136/bmj.e5595
RESEARCH METHODS & REPORTING
Prognosis research strategy (PROGRESS) 1: A framework for researching clinical outcomes
Understanding and improving the prognosis of a disease or health condition is a priority in clinical research and practice. In this article, the authors introduce a framework of four interrelated themes in prognosis research, describe the importance of the first of these themes (understanding future outcomes in relation to current diagnostic and treatment practices), and introduce recommendations for the field of prognosis research Harry Hemingway Professor of clinical epidemiology1, Peter Croft professor of epidemiology 2, Pablo ….

B. Communicating the prognosis
What we know • most cancer patients want
prognostic information , good or bad
• Information needs vary during illness
• “Clinicians underestimate what is wanted and overestimate what was said and understood”
• Information be individualized • Probabilities better than
temporal predictions – Survival curves are exponential and
quartiles and deciles are simple multiples of the median
• Question prompt lists may help promote discussion
Opportunities and challenges
• Presenting the data to diverse patients
• Training non-specialists
• Nomograms, calculators, apps
• Impact of communication on patient/family mood, QOL, satisfaction
C. Using the prognosis
Using the prognosis
• Clinicians do it all the time (conscious & subconscious)
• SUPPORT Study – Prognostic beliefs and
utilization of aggressive EOL care
• MGH Study of palliative care and lung cancer – Discussing prognosis and
utilization data
Opportunities, Challenges
• Prognostic models as clinical prediction tools e.g. Ottawa ankle rule
• Px as a referral trigger/admission criterion
• RCT’s of Subjective vs. Actuarial: utilization, outcomes, costs, satisfaction, survival
2. Prognostication beyond survival
A typical day on rounds…
• I’ll operate if you think she’ll be alive in 3 months
• There is a 20% chance of the hypercalcemia recurring
• Unfortunately, he’ll never walk again
• No, not every one with cancer develops pain
• Call me if the nausea doesn’t wear off in a few days
• Your insurance will probably want PA for this
• Your mother is also at an increased risk of dying in the next 18 months

The 5 D’s of prognosis
a. Death b. Disease progression/recurrence c. Discomfort/disability d. Drug toxicity e. Dollars (cost)
Fries & Ehrlich
1981 • Derivatives
Glare & Christakis 1999
The 5 D’s of prognosis
a. Death b. Disease progression/recurrence c. Discomfort/disability d. Drug toxicity e. Dollars (cost)
Fries & Ehrlich
1981 f. Derivatives
Glare & Christakis 2004

Clinical epidemiology and prognosis
the relative probabilities that a patient will develop each of the alternative outcomes of the natural history of his/her disease
Sackett 1991 the probability of the specified outcome (event or
quantity) with different combinations of predictors in a well defined population
Moons 2009

Clinical epidemiology and prognosis
the relative probabilities that a patient will develop each of the alternative outcomes of the natural history of his/her disease
Sackett 1991 the probability of the specified endpoint (event or
quantity) with different combinations of predictors in a well defined population
Moons 2009

b. Disease progression/recurrence
PHASE Stable Transitional End of Life
Dead
Stable 94% 4% <1% <1%
Transitional
11% 60% 5% 24%
Dead - - -
100%
Estimated One-Month Transition Probabilities (%)
Sutradhar et al. JPSM 2013

b. Discomfort/disability
Longer time to reach stable pain control: -young age (<60), - neuropathic pain -incidental pain
Higher Final Morphine dose: -neuropathic pain, -incidental pain, -psychological distress - addiction,

d. Drug toxicity
Predictive: lung cancer (OR 2.5) Protective : males (OR 0.4), steroids (OR 0.5)

e. Dollars (cost of care)
Type of pain management Effectiveness Cost/month
Guideline based care 80% $579
Oncologist based care 55% $466
Usual care 30% $315

f. Derivatives

Use of prognostic models • Inform individuals about the future course of their illness, or their risk of
developing illness
• Guide physicians and patients in joint decisions on further treatment, if any. – Nottingham prognostic index & long term risk of cancer recurrence or death in breast cancer
patients – APACHE score & hospital mortality in critically ill patients – models for predicting postoperative nausea and vomiting. – Framingham cardiovascular risk score & cholesterol lowering and antihypertensive drugs.
• Select relevant patients for therapeutic research. – RCT of tamoxifen to prevent breast cancer. – RCT of radiotherapy after breast conserving resection in patients with a low risk of cancer
recurrence.
• Compare differences in performance between hospitals. For example, the – clinical risk index for babies (CRIB) to compare performance and mortality among neonatal
intensive care units. – model to predict the hospital standardized mortality ratio to explain differences between
English hospitals.
Moons K, BMJ 2009

3. Crosswalk with other schools
e.g. Meteorology

Decision making to evacuate or stay put
• NWS statements/evacuation orders are important
• Residents evaluate own risk and make own protective decisions – Warnings of “certain death” often
produce negative attitudes
• Quantification of uncertainty has limited impact on decisions – make them more complicated
• Decision making on a binary outcome made under a tight deadline (e.g. to evacuate or not) is complex, non-linear, non-scientific
• “when the stakes are high and the uncertainties large, ‘soft values’ dominate ‘hard facts’ ”
Morss RE et al. Weather Climate & Society
2010;2(3):174-89

Conclusions
• In past 40 years, great progress has been made to improve prognostication
• Much remains to be done to improve the accuracy of survival predictions, especially validation of existing tools & ‘upstreaming’
• Communication of prognosis and use of prognosis are also priorities
• Prediction of other outcomes is under-studied
• Other disciplines can inform our research agenda on predictions and decision making


















