Republic of South Sudan EARLY WARNING AND DISEASE ... · In week 15 of 2015, ARI was the top cause...
13
Early Warning and Disease Surveillance System 1 Republic of South Sudan EARLY WARNING AND DISEASE SURVEILLANCE BULLETIN (IDP CAMPS AND SETTLEMENTS) Week 15 6 – 12 April, 2015 General Overview Completeness for weekly reporting in week 15 of 2015 was 82% compared to 91% in week 14 of 2015 and 84% in week 15 of 2014. ARI, malaria, AWD, ABD and suspect measles are the top causes of morbidity among IDPs. In week 15 of 2015, ARI was the top cause of morbidity among IDPs with a proportionate morbidity of 19% and incidence of 55 cases per 10,000 population, which represents an increase in comparison to week 14 of 2015. Fifty one new suspect measles cases were reported from Bentiu (50 cases) and Lankien (1 case). A measles vaccination campaign has been conducted in Bentiu PoC following the confirmation of a measles outbreak in the PoC in week 12. A total of 182 measles cases including two deaths (CFR 1.1%) have been registered in Bentiu PoC since the beginning of 2015. In Upper Nile, measles cases have not been reported in Malakal PoC but 34 cases have been reported in Maban (24 cases), Fashoda (4 cases), and Lower Manyo (6 cases) since week 11. In week 15, two new HEV cases were reported from Bentiu while Mingkaman reported two cases. Hence the cumulative for HEV is 51 cases including one death (CFR 1.96%) and 143 cases including six deaths (CFR 4.2%) in Mingkaman. Four suspect cholera cases including one death were reported from Guit county in Unity state in week 15. Three animal bite (suspect rabies) cases were reported in PoC 1 in UN House IDP camp in week 15 of 2015. The under-5 and crude mortality rates by IDP site were below the emergency threshold in week 15of 2015. An Ebola Preparedness Support Team composed of experts from WHO-HQ and WHO-AFRO has concluded its mission to South Sudan from April 12-18, 2015. Editorial note In this bulletin, we present priority disease trends using data submitted through the Early Warning Alert and Disease Network (EWARN) by health partners providing health services to internally displaced persons (IDP) in South Sudan. Additional data from the integrated disease surveillance and response (IDSR) is also presented for select diseases like cholera, Kala-azar and AFP. All other IDSR weekly reports are published through the IDSR weekly bulletin by the EPR department, MoH-RSS. Completeness and Timeliness of Reporting Figure 1 shows the completeness for weekly reporting from week 01 of 2014 to week 15 of 2015. Figure 1 0 20 40 60 80 100 120 01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 Completeness [%] Reporting Completeness for IDP Health Facilities, 2014 - 2015 2014 2015 Target
Transcript of Republic of South Sudan EARLY WARNING AND DISEASE ... · In week 15 of 2015, ARI was the top cause...

Early Warning and Disease Surveillance System
1
Republic of South Sudan
EARLY WARNING AND DISEASE SURVEILLANCE BULLETIN (IDP CAMPS AND SETTLEMENTS)
Week 15 6 – 12 April, 2015
General Overview
Completeness for weekly reporting in week 15 of 2015 was 82% compared to 91% in week 14 of 2015 and 84% in week 15 of 2014.
ARI, malaria, AWD, ABD and suspect measles are the top causes of morbidity among IDPs. In week 15 of 2015, ARI was the top cause of morbidity among IDPs with a proportionate morbidity of 19% and
incidence of 55 cases per 10,000 population, which represents an increase in comparison to week 14 of 2015. Fifty one new suspect measles cases were reported from Bentiu (50 cases) and Lankien (1 case). A measles
vaccination campaign has been conducted in Bentiu PoC following the confirmation of a measles outbreak in the PoC in week 12. A total of 182 measles cases including two deaths (CFR 1.1%) have been registered in Bentiu PoC since the beginning of 2015. In Upper Nile, measles cases have not been reported in Malakal PoC but 34 cases have been reported in Maban (24 cases), Fashoda (4 cases), and Lower Manyo (6 cases) since week 11.
In week 15, two new HEV cases were reported from Bentiu while Mingkaman reported two cases. Hence the cumulative for HEV is 51 cases including one death (CFR 1.96%) and 143 cases including six deaths (CFR 4.2%) in Mingkaman.
Four suspect cholera cases including one death were reported from Guit county in Unity state in week 15. Three animal bite (suspect rabies) cases were reported in PoC 1 in UN House IDP camp in week 15 of 2015. The under-5 and crude mortality rates by IDP site were below the emergency threshold in week 15of 2015.
An Ebola Preparedness Support Team composed of experts from WHO-HQ and WHO-AFRO has concluded its
mission to South Sudan from April 12-18, 2015.
Editorial note In this bulletin, we present priority disease trends using data submitted through the Early Warning Alert and Disease Network (EWARN) by health partners providing health services to internally displaced persons (IDP) in South Sudan. Additional data from the integrated disease surveillance and response (IDSR) is also presented for select diseases like cholera, Kala-azar and AFP. All other IDSR weekly reports are published through the IDSR weekly bulletin by the EPR department, MoH-RSS.
Completeness and Timeliness of Reporting
Figure 1 shows the completeness for weekly reporting from week 01 of 2014 to week 15 of 2015. Figure 1
0
20
40
60
80
100
120
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Co
mp
lete
nes
s [%
]
Reporting Completeness for IDP Health Facilities, 2014 - 2015
2014 2015 Target

Early Warning and Disease Surveillance System
2
During this period, the number of health facilities expected to submit weekly reports increased from seven in week
01 of 2014 to 45 in week 15 of 2015. Timeliness for weekly reporting in week 15 of 2015 was 26 (57%), which is higher when compared to 20 (44%) in
week 14 of 2015 and 15/31 (48%) in week 15 of 2014. Completeness for weekly reporting in week 15 of 2015 was 37 (82%), which is lower when compared to 41 (91%) in
week 14 of 2015 and 26 (84%) in week 15 of 2014. In week 15 of 2015, we did not receive reports from eight facilities (Table1).
Table 1: List of silent health facilities during week 15, 2015 No. IDP site /Health Facility Reason of not reporting
1 Chuil PHCU – MedAir Inaccessibility to the area and report will be submitted monthly.
2 Yuai – MSF-OCA
3 Lul – IMA
4 Ayueldit - SMC
5 Poktap – SMC
6 Pamote – SMC
7 Mabek mobile clinic – GOAL
8 Wau Shilluk/ Malakal PoC – MSF E
Consultations (All patients seen at Outpatient and Inpatient facilities)
The total consultations in week 15 of 2015 were 15,341, which are higher when compared to 15,266 consultations in week 14 of 2015 but lower than the 16,583 consultations in week 15 of 2014. Figure 2 shows the consultations by site in week 15of 2015.
Figure 2
The cumulative consultations since week 01 of 2015 have risen to 255,785. Figure 2.1 shows the cumulative consultations by IDP site since week 01 of 2015. Figure 2.1
The annualised outpatients department (OPD) utilization for 2015 is 1.7 consultations per person per year (Figure 2.2). The IDP site-specific annualised OPD utilization rates are shown in Figure 2.2.
597
649 1479
1107 524
927
811
863
1022
161 506
488
1059
252
1255 689
633
519 387 338 402
268
234 171 0
500
1000
1500
2000
2500
3000
Aw
eria
l
Ben
tiu
Bo
r
Lan
kie
n
Mal
akal
Mel
ut
UN
HO
USE
Ak
ok
a
Ren
k
Ko
do
k
Ogo
d
Ak
ob
o
Wau
Sh
illu
k
Tw
ic E
ast
Nu
mb
er o
f co
nsu
ltat
ion
s
Consultations by IDP Camp and Partner, week 15 2015
CCM IMC IOM IRC MSF-E MSF-OCA CARE Medair HealthLink GOAL IMA SMC
34
53
4
17
30
0
17 19
4 0 7
31
7 3 5 8 8 4 2 3 0
10
20
30
40
50
60
Nu
mb
er o
f co
nsu
ltat
ion
s
Th
ou
san
ds Cumulative Consultations by IDP Site from week 01 of 2015 to week 1 of 2015

Early Warning and Disease Surveillance System
3
Figure 2.2
Overall Trends of Priority Epidemic-prone Diseases
Table 2 shows the top five causes of morbidity among IDPs with Acute Respiratory tract Infections (ARI) being at the top, followed by malaria, Acute Watery Diarrhoea (AWD), Acute Bloody Diarrhoea (ABD) and suspected measles. Also presented in Table 2 are the corresponding disease trends for week 15 of 2014 and 2015 respectively.
Table 2
No. Disease
New cases for weeks Cumulative cases since week 01 of 2015 15 of 2014 15 of 2015
1 Malaria 2,544 1,878 38,995
2 AWD 1,417 1,499 25,450
3 ARI 2,168 2,915 45,462
4 ABD 237 202 3,344
5 Measles 42 51 238
Figures 3 and 4 show the proportionate and incidence morbidity trends for ARI, malaria, AWD, suspected measles and ABD.
Figure 3
Figure 4
1.5
3.4
6.4
2.4
4.7
0.2 2.8
2.0 0.6 0.2 2.2
3.4
1.1 0.9 1.0 0.6 0.7 0.7 0.1
4.2
- - 1.7
-
1.0
2.0
3.0
4.0
5.0
6.0A
wer
ial
Ben
tiu
Bo
r
Lan
kie
n
Mal
akal
Man
-Aw
an
Mel
ut
UN
HO
USE
Yu
ai
Man-…
Ak
ok
a
Ren
k
Ko
do
k
Lu
l
Ogo
d
Ak
ob
o
Wau…
Tw
ic E
ast
Ny
iro
l
DU
K
Ayo
d
Fan
gak
Ove
rall
con
sult
atin
s p
er p
erso
n p
er
yea
r
Consultations per person per year, week 15, 2015
13.1% 19.0%
1.4% 1.3%
15.3% 12.2%
0.253% 0.332% 8.5%
9.8%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
wk 15 of 2014 wk 15 of 2015Pe
rce
nt
of
all
co
nsu
lta
tio
ns
Priority Disease Proportionate Morbidity for week 15 of 2014 and 2015
ARI Bloody Diarrhea Malaria Suspected Measles Watery Diarrhoea
61.5 54.7
7 4
72
35
1.2
1.0
40
28
-
50
100
150
200
wk 15 of 2014 wk 15 of 2015
Cas
es p
er 1
0,0
00
Incidence for Priority Diseases for week 15 of 2014 and 2015
ARI Bloody Diarrhea Malaria Suspected Measles Watery Diarrhoea

Early Warning and Disease Surveillance System
4
During week 15 of 2015, ARI was the top cause of morbidity followed by malaria, AWD, ABD, and measles. During the corresponding week of 2014, malaria was the top cause of morbidity followed by ARI, AWD, ABD, and measles. The proportionate morbidity for ARI, malaria, AWD, and measles in week 15 of 2015 represent an increase when compared to the week 14 of 2015 (Figures 3 and 4).
Specific Priority Epidemic-Prone Diseases
Acute Respiratory Infection (ARI) Figure 5
During week 15 of 2015, ARI registered the highest proportionate morbidity of 19% and incidence of 55 cases per 10,000 population (Figures 4 and 5). During the corresponding week of 2014, ARI had a proportionate morbidity of 13% and incidence of 62 cases per 10,000 population respectively. This shows that the ARI proportionate morbidity for week 15 of 2015 is higher when compared to week 15 of 2014 and week 14 of 2015. (Figure 5). Figure 5.1
During week 15 of 2015, Malakal registered the highest ARI incidence (cases per 10,000) of 246, followed by Bor (178), Bentiu (147), and Lankien (123) see Figure 5.1. During the corresponding week of 2014, the ARI incidence (cases per 10,000) was 237 in Tongping, 163 in UN House, and 162 in Malakal (Figure 5.1). Acute Watery Diarrhoea (AWD)
During week 15 of 2015, AWD registered the third highest proportionate morbidity of 9.8% and incidence of 28 cases per 10,000 population (Figures 4 and 6). During the corresponding week of 2014, AWD had the third highest proportionate morbidity of 8.5% and incidence of 40 cases per 10,000 population (Figure 6). This shows that the AWD proportionate morbidity for the current period is slightly higher when compared to week 15 of 2014 but lower when compared to week 14 of 2015. Conversely, the AWD trend has been rising slowly since the beginning of 2015.
7.7
16.5
18.7
16.2
17.9 18.4
19.4
17.5
17.2 18.9
19.3
16.3 16.1 18.4 19.0
0.0
5.0
10.0
15.0
20.0
25.0
30.0
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Per
cen
t o
f to
tal c
on
sult
atio
ns
Epidemiologic Week
ARI Proportionate Morbidity from week 51 of 2013 to week 15 of 2015
2013 2014 2015
103 97 162
98 163
237 31 147
178 123
246
13
89
52 50 44 39 23 -
100
200
300
400
500
Cas
es p
er 1
0,0
00
ARI Incidence, by IDP Site , for week 15 of 2014 and 2015
wk 15 of 2014 wk 15 of 2015
Early Warning and Disease Surveillance System
5
Figure 6
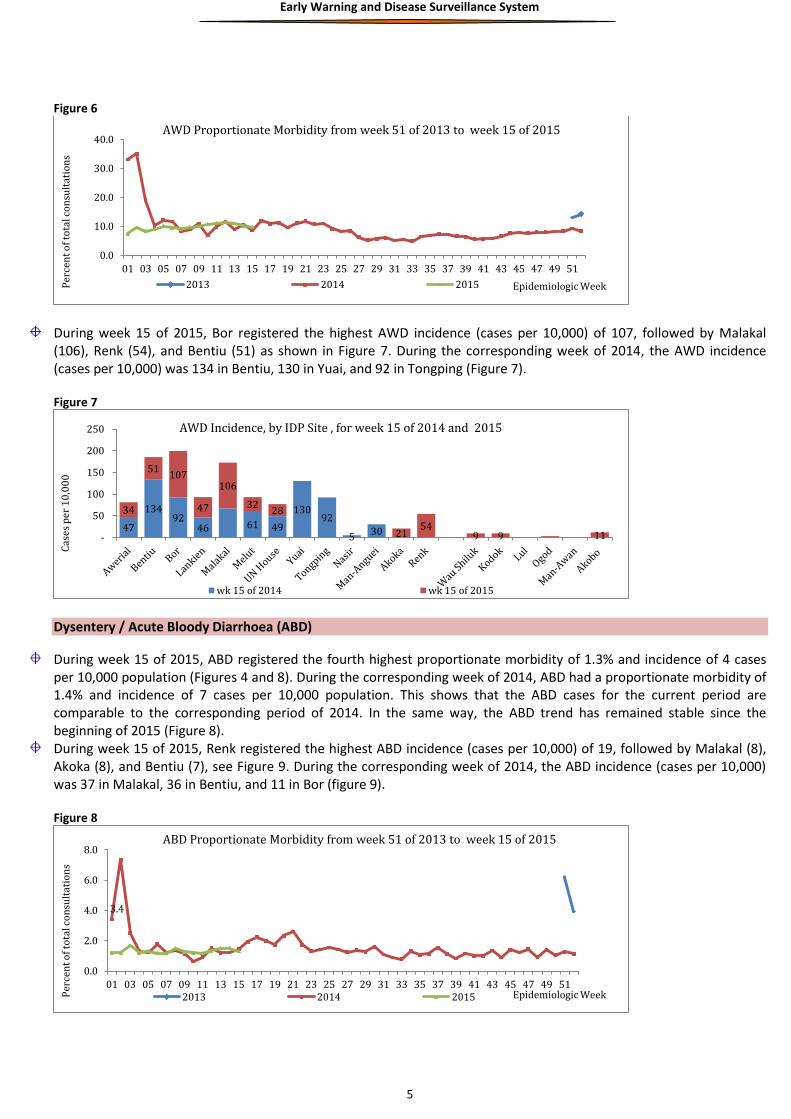
During week 15 of 2015, Bor registered the highest AWD incidence (cases per 10,000) of 107, followed by Malakal (106), Renk (54), and Bentiu (51) as shown in Figure 7. During the corresponding week of 2014, the AWD incidence (cases per 10,000) was 134 in Bentiu, 130 in Yuai, and 92 in Tongping (Figure 7). Figure 7
Dysentery / Acute Bloody Diarrhoea (ABD)
During week 15 of 2015, ABD registered the fourth highest proportionate morbidity of 1.3% and incidence of 4 cases per 10,000 population (Figures 4 and 8). During the corresponding week of 2014, ABD had a proportionate morbidity of 1.4% and incidence of 7 cases per 10,000 population. This shows that the ABD cases for the current period are comparable to the corresponding period of 2014. In the same way, the ABD trend has remained stable since the beginning of 2015 (Figure 8).
During week 15 of 2015, Renk registered the highest ABD incidence (cases per 10,000) of 19, followed by Malakal (8), Akoka (8), and Bentiu (7), see Figure 9. During the corresponding week of 2014, the ABD incidence (cases per 10,000) was 37 in Malakal, 36 in Bentiu, and 11 in Bor (figure 9). Figure 8
0.0
10.0
20.0
30.0
40.0
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Per
cen
t o
f to
tal c
on
sult
atio
ns
Epidemiologic Week
AWD Proportionate Morbidity from week 51 of 2013 to week 15 of 2015
2013 2014 2015
47
134 92
46 61 49
130 92
5 30
34
51 107
47
106
32 28
21 54
9 9 11 -
50
100
150
200
250
Cas
es p
er 1
0,0
00
AWD Incidence, by IDP Site , for week 15 of 2014 and 2015
wk 15 of 2014 wk 15 of 2015
3.4
0.0
2.0
4.0
6.0
8.0
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Per
cen
t o
f to
tal c
on
sult
atio
ns
Epidemiologic Week
ABD Proportionate Morbidity from week 51 of 2013 to week 15 of 2015
2013 2014 2015

Early Warning and Disease Surveillance System
6
Figure 9
Measles
Figure 10
During week 15 of 2015, measles registered the fifth highest proportionate morbidity of 0.33% and incidence of 1 case
per 10,000 population (Figures 4 and 10). During the corresponding week of 2014, the proportionate morbidity of suspect measles was 0.25% and incidence of 1.2 cases per 10,000 population. A sharp increase in the proportionate morbidity for measles cases was registered in week 15 of 2015 [0.33%] when compared to week 12 of 2015 [0.071%] (figure 10). Consequently, the proportionate morbidity for measles for week 15 of 2015 is higher when compared to week 15 of 2014 and week 14 of 2015. (Figure 10).
During week 15 of 2015, a total of 51 suspect measles cases were reported from Bentiu (50 cases) and Lankien (1 case).
A measles vaccination campaign has been conducted in Bentiu PoC following the confirmation of a measles outbreak in
the PoC in week 12. A total of 182 measles cases including two deaths (CFR 1.1%) have been registered in Bentiu PoC
since the beginning of 2015 (figure 10.1).
Figure 10.1
7
36
10 0
37
3 8 6
2
7
6
4
8
6 8 19
4 5 -
10
20
30
40
50
Cas
es p
er 1
0,0
00
ABD Incidence, by IDP Site , for week 15 of 2014 and 2015
wk 15 of 2014 wk 15 of 2015
0.0
1.0
2.0
3.0
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Per
cen
t o
f to
tal c
on
sult
atio
ns
Epidemiologic Week
Suspected measles Proportionate Morbidity from week 51 of 2013 to week 15 of 2015
2013 2014 2015
1 1 1 2 3 12 14
55
41 50
0
10
20
30
40
50
60
01 02 03 04 05 06 07 08 09 10 11 12 13 14 15
Nu
mb
er
of
case
s
Epidemiological week of 2015
Measles cases reported in Bentiu PoC by week 1-15, 2015
Alive Died

Early Warning and Disease Surveillance System
7
Out of the 161 line listed measles cases in Bentiu PoC since the beginning of 2015, 91 (57%) are male; and as seen from
tables 3 and 4, 66 (41%) were 0-9 months of age, while 58 (36%) were 10months to 4 years, and 22 (14%) were 5-9
years. Most of the cases have originated from PoC 5 with 45 (28%), PoC 1 with 38 (24%), PoC 6 with 36 (22%), and PoC
4 with 19 (12%) (table 3 and 4). Nearly 90% (144) of the measles cases in Bentiu were not immunised against measles.
Table 3 and 4
Age Number Percentage
0-9mths 66 41
10mths-4yrs 58 36
5-9yrs 22 14
10-14yrs 6 4
15-19yrs 1 1
20-24yrs 3 2
26-29yrs 4 2
30yrs 1 1
Grand Total 161 100
In Upper Nile state, no measles cases have been reported in Malakal PoC, Wau Shiluk, or Malakal town. However,
measles cases have continued to be reported in the host population in Maban County since week 11 of 2015 (figure
10.2). Three new measles cases were reported in week 15 bringing the cumulative in Maban to 24 cases including 2
deaths (CFR 8.3%). Additionally 10 suspect measles cases have been reported from Fahoda (4 cases) and Lower Manyo
(6 cases). Out of the 23 line listed cases in Maban County, 18 (78%) are aged 0-4 years and 20 (87%) reported being
vaccinated against measles.
Figure 10.2
Malaria
During week 15 of 2015, malaria registered the second highest proportionate morbidity of 12% and incidence of 35 cases per 10,000 population (Figures 4 and 11). Malaria had the highest proportionate morbidity of 15% and incidence of 72 cases per 10,000 population during the corresponding week of 2014. This shows that the malaria cases for the current period are slightly lower than the corresponding period of 2014. The overall malaria trend has remained relatively stable since the beginning of 2015.
- -
13
3 - 1
4 0 0
2
0 -
5
10
15
20
9 10 11 12 13 14 15
Nu
mb
er
of
case
s
Epidemiological week of onset
Measles cases in Maban County, week 11-15, 2015
Alive Died
Location in Bentiu Total Percentage
Ding Ding 2 1.2
Guit 1 0.6
PoC 1 38 23.6
PoC 2 6 3.7
PoC 4 19 11.8
PoC 5 45 28.0
PoC 6 36 22.4
PoC 3 14 8.7
Grand Total 161 100.0

Early Warning and Disease Surveillance System
8
Figure 11
During week 15 of 2015, Bor registered the highest malaria incidence (cases per 10,000) of 302, followed by Malakal (156) and Wau Shilluk (52) as seen in Figure 12. The malaria incidence (cases per 10,000) was 370 in Bor, 352 in Bentiu, 301 in Malakal, and 148 in Yuai during the corresponding week of 2014 (figure 12). Figure 12
Hepatitis E Virus (HEV)
Hepatitis E Virus remains a major public health problem among IDPs and has been confirmed in two out of eight IDP
sites where Acute Jaundice Syndrome (AJS) cases have been reported (Figure 13 and 14).
Figure 13
AJS cases were first reported in week 4 of 2014 in Juba 3 PoC and since then, HEV has been confirmed in Mingkaman
where eight cases were tested positive for HEV by ELISA/PCR and in Bentiu where two cases tested positive for HEV by
ELISA, see Figures 13 and 14. Additionally, eight AJS cases seen in Lankien during the period 1 September 2014 to 17
March 2015 tested positive for HEV on rapid testing but definitive laboratory confirmation is pending.
In week 15, two new HEV cases were reported from Bentiu PoC while Mingkaman reported two cases. Hence the
cumulative for HEV is 51 cases including one death (CFR 1.96%) in Bentiu and 143 cases including six deaths (CFR 4.2%)
in Mingkaman.
51.8
0.0
10.0
20.0
30.0
40.0
50.0
60.0
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Per
cen
t o
f to
tal c
on
sult
atio
ns
Epidemiologic Week
Malaria Proportionate Morbidity from week 51 of 2013 to week 14 of 2015
2013 2014 2015
44
352 370
43
301 74 56
148 108 9 92 39
30
302
35
156
22 36 45 23 52 29 30 -
200
400
600
800
Cas
es p
er 1
0,0
00
Malaria Incidence, by IDP Site , for week 15 of 2014 and 2015
wk 15 of 2014 wk 15 of 2015
0 0 1 2 0 0 0 0 0
3 2 5
3 6
3 5
11
2
11
5
1 3 4
7 7 7 5 6
4 4 3 6
4
0 0 1 2 1 1 4
1 1 1 1 1 1 1 1 2 1 1 2 0
2
4
6
8
10
12
14
16
3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 1 3 5 7 9 11 13 15
2014 2015
No
. cas
es
Epidemiological week
Acute Jaundice Syndrome cases by Camp from week 03, 2014 to week 15, 2015
Awerial Bor Malakal Tongping Lul Juba 3 Lankien Bentiu

Early Warning and Disease Surveillance System
9
Figure 14
Response interventions by partners include supportive case management, targeted preventive interventions during
antenatal visits, soap distribution, shock chlorination of boreholes, as well as house-to-house hygiene and sanitation
promotion.
Cholera
Four suspect cholera cases including one death were reported from Guit county in Unity state in week 15. Specimen and case management kits have been supplied by WHO to support case investigation and management. Response to the alert is being coordinated by THESO, the health implementing partner in the County.
The national cholera preparedness matrix has been disseminated to enhance readiness and support the initiation of activities for cholera prevention and control.
Acute Flaccid Paralysis (AFP) During 2015, a total of 87 AFP cases have been reported, of which five new AFP cases were reported in week 15 (Table 5). The annualized non-Polio AFP (NPAFP) rate (cases per 100,000 population children 0-14 years) is 3.67 per 100,000 population of children 0-14 years (target ≥2 per 100,000 children 0-14 years). Table 5: Summary of AFP indicators by state as of week 9, 2015
All states except Unity, Upper Nile, and Jonglei have attained the targeted NPAFP rate of ≥2 per 100,000 children 0-14 years. The non-Polio Enterovirus (NPEV) isolation rate (a measure of the quality of the specimen cold chain) is 8.2% (target ≥10%). Stool adequacy stands at 98%, a rate that is higher than the target of ≥80% .
The type 2 circulating Vaccine Derived Poliovirus (cVDPV2) cases remained two and SIAD activities are being conducted in the accessible counties of of Jonglei, Unity and Upper NileStates. Three rounds of SIAD have been conducted reaching at least 1,563,214 children in 27 counties and three PoCs. However, active surveillance stalled due to the
0 0 1 2 0 0 0 0 0
3 2
5 3
6
3 5
11
2
11
5
1 3 4
7 7 7 5 6
4 4 3
6 4
0 0 1 2 1 1
4
1 0 1 1 1 1 1 1 1 2 1 1 2
1
1
1
3 2
1
0 3
7 5 5
2 1
2 6
2 4 3 2
0
2
4
6
8
10
12
14
3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 1 3 5 7 9 11 13 15
2014 2015
No
. cas
es
Epidemiological week
Hepatitis E Virus trends in Mingkaman and Bentiu from week 10, 2014 to week 15, 2015
Awerial Bentiu
Early Warning and Disease Surveillance System
10
continued insecurity in these three states.
Other diseases of public health importance
Guinea worm (Dracunculiasis)
There was no new suspect Guinea worm disease case reported during week 15 of 2015.
Viral Haemorrhagic Fever
The Republic of South Sudan continues to enhance its readiness capacities for Ebola/Marburg virus disease. The national Ebola/Marburg taskforce is coordinating the implementation of interventions guided by a national
Ebola/Marburg contingency plan. No Ebola/Marburg cases have been confirmed in South Sudan but six alerts have been investigated in Ezo, Nzara,
Terekeka (Tali) and Juba (Hai Jalaba and Gudele) since 2014. Training of rapid response teams from seven states and 47 counties is underway with a total of 139 rapid response
team members from five states and 139 counties trained to date. The main thrust of the trainings is to enhance national capacities for preparedness and response to disease outbreaks of VHF, cholera, and epidemic meningitis.
An Ebola Preparedness Support Team composed of experts from WHO-HQ and WHO-AFRO have concluded their mission to South Sudan from April 12-18, 2015. The mission evaluated the current state of Ebola preparedness and response readiness through key informant interviews, site visits, meetings, and tabletop simulation exercise with the national Ebola taskforce. Follow up missions are planned to address the identified gaps.
Visceral Leishmaniasis (Kala-azar)
In week 15 of 2015, a total of 60 new visceral leishmaniasis cases were reported by 6 (40%) treatment centres
including Rom, Ulang, Lankien, Leer, Walgak, and Bentiu.
From week 1 to date, a total of 1428 cases, (1156 [81%] new cases; 272 [19 %] relapses/PKDL; 24 [1.7% defaulters];
and 44 [3.1%] deaths) have been reported from 16 treatment centres compared to 1374 cases (1220 new cases;
134 relapses/PKDL; 104 defaulters and; 35 deaths (CFR 2.5%) reported from 15 treatment centres by the end of
week 15 of 2014.
During 2015, Lankien has reported the highest number of cases – 756; followed by Walgak – 176; then Ulang 96;
Chuil – 76; Melut IDP - 71 and; Narus (MOH/ARC) – 70.
Males are the most affected gender with 779 cases making (54.6%) of the total cases and females with 649 (45.4%)
of the total cases.
Patients aged ≥15years constitute 596 cases (41.7%) followed by those aged 5-14years with 589 cases (41.2%) and
then the least affected are those <5years with 243 cases (17%).
Generally the number of cases reported in 2015 is higher compared to those reported in 2014.
The increase in number of cases is attributed to the displacement of non-immune population to the endemic areas,
poor nutrition or malnutrition (which is both a risk factor as well as a complication in VL) among internally displaced
persons, poor housing and in accessibility to health due to insecurity or floods. Also increase in number of
treatment centers from 15 to 16. However, the number of cases reported this week is lower compared to those
reported in the previous weeks, reasons being the low number of health facilities that reported and the beginning
of the transmission season.
WHO continues to support enhanced surveillance, case management and interventions to interrupt transmission
through the following: supporting implementing partners with case management supplies; training frontline
healthcare workers on Kala-azar case management; support supervision of treatment facilities; supporting
community sensitisation on Kala-azar; and distribution of long lasting insecticide treated nets (LLITN) in affected
and high-risk areas.

Early Warning and Disease Surveillance System
11
Meningitis
There were no new meningitis cases reported during week 15of 2015.
Animal bites (suspect rabies)
Three animal bite (suspect rabies) cases were reported in PoC 1 UN House IDP site in week 15 of 2015. All three
cases have so far received two doses of rabies vaccine as part of post exposure prophylaxis and are doing well.
All-Causes Mortality Data
During week 15 of 2015, mortality lists were received from Malakal, Bentiu, and Juba 3 PoC.
A total of 14 deaths were reported during week 15 of 2015, with 9 (64%) deaths being reported from Bentiu, see
Table 6. During the corresponding week of 2014, a total of 17 deaths were reported as seen in Table 6.
Table 6: Causes of death by IDP camp during week 15of 2014 and 2015
2014 2015
IDP site Cause of Death <5yrs >5yrs <5yrs >5yrs
Bentiu
Acute watery diarrhoea
1 Malaria
2
Not Stated 1 TB/HIV/AIDS
1 1
Hypoglycaemia
1 Cancer
1
Sepsis
1 Native herbal intoxication
1
Bor
Acute watery diarrhoea
1 Not Stated
1
Juba 3
Liver cirrhosis
1
Pneumonia 2
1 TB/HIV/AIDS
1
Malakal
Acute watery diarrhoea
1 Not Stated
4
Multiple system organ failure
1
Mingkaman Not Stated 3 2 Tongping
Not Stated
1 Perinatal death 1
Severe head ache
1 Grand Total 7 10 7 7
Under-five Mortality Rate
Figure 16
02468
1012141618
51 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 1 3 5 7 9 11 13 15
2013 2014 2015
Rat
e p
er 1
0,0
00
Epidemiologic Week
Under-5 Mortality Rate per 10,000 per day by Site - week 51 of 2013 to week 15 of 2015
Bentiu Bor Juba 3 Malakal Mingkaman Tongping Melut Threshold

Early Warning and Disease Surveillance System
12
The under-five mortality rates (U5MR) per 10,000 per day from week 51 of 2013 to week 15 of 2015 are shown in
Figure 16.
The under-five mortality rates for the three IDP sites that reported in week 15 of 2015 were lower than the
emergency threshold of 2 deaths per 10,000 per day.
Crude Mortality Rate
The crude mortality rates (CMR) from week 51 of 2013 to week 15 of 2015 are shown in Figure 17. During week 15
of 2015, the CMRs were below the emergency threshold for the three IDP sites that submitted mortality data.
Figure 17
Overall Mortality
Since the onset of the crisis, at least 1,584 deaths have been reported from the IDP sites. Children under-5 years
account for 728 (46%) of the deaths. The majority of the deaths occurred in Bentiu, Malakal, Tongping, Mingkaman
and Juba 3 PoC. The top causes of mortality during the period include AWD, severe pnuemonia, TB/HIV/AIDS and
malnutrition (Table 7).
Table 7: Overall mortality by settlement, week 51 of 2013 to week 15of 2015
IDP site Acu
te J
aun
dic
e
Syn
dro
me
acu
te w
ater
y d
iarr
ho
ea
blo
od
y
dia
rrh
oe
a
can
cer
Gu
nsh
ot
wo
un
d
He
art
dis
eas
e
hyp
erte
nsi
on
Kal
a-A
zar
mal
aria
mat
ern
al d
eat
h
me
asle
s
pe
rin
atal
de
ath
pn
eu
mo
nia
SAM
Sep
tice
mia
Stro
ke
TB/H
IV/A
IDS
trau
ma
Oth
ers
Gra
nd
To
tal
Agok 1 2 3
Bentiu 54 2 1 12 3 2 17 1 8 9 47 52 25 1 34 7 178 453
Bor 2 1 1 1 42 2 10 3 1 3 62 128
Juba 3 1 12 4 2 2 2 11 1 1 43 11 8 2 2 31 43 176
Kodok 1 0 1
Malakal 1 31 1 38 14 1 15 14 22 7 21 7 1 26 6 122 327
Melut 1 2 16 7 3 3 6 5 1 11 17 72
Mingkaman 6 30 4 2 1 1 18 1 4 8 9 4 8 1 8 2 47 154
Tomping 33 2 4 6 11 1 10 37 15 24 16 1 3 4 1 98 266
(missing) 1 1 2 4
Grand Total 8 163 8 13 58 34 9 31 78 6 92 102 115 109 46 8 117 16 571 1584
General recommendations
Conduct case-based surveillance and ongoing measles vaccination for all the new arrivals in Bentiu PoC. Cholera preparedness should be enhanced countrywide through: monitoring AWD trends and ensuring stool
samples are obtained from all suspect cholera cases; risk communication on cholera prevention and control should be intensified; sanitation and hygiene promotion should be enhanced; and stockpiles of supplies for cholera investigation and response should be prepositioned in all states.
0
1
2
3
4
5
6
51 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 41 41 43 45 47 49 51 1 3 5 7 9 11 13 15
2013 2014 2015
Rat
e p
er 1
0,0
00
Epidemiologic week
Crude Mortality Rate per 10,000 persons per day, week 51 of 2013 to week 15 of 2015
Bentiu Bor Juba 3 Malakal Mingkaman Tongping Threshold Melut

Early Warning and Disease Surveillance System
13
In response to the HEV cases in Mingkaman and Bentiu, the following interventions should be prioritized: household sanitation and hygiene promotion; improved access to safe water; and targeted interventions to prevent new infections among pregnant women.
Malaria preventive interventions including the use of LLITNs, indoor residual spraying (IRS) and prompt case management should be sustained.
Promote ARI prevention and control by sensitizing communities on respiratory hygiene, regular hand washing with soap and water, prompt recognition and treatment of pneumonia in children under-5 years and routine vaccination of children as per infant vaccination schedule.
Integrate TB/HIV/AIDS prevention and control into the routine healthcare services in all the IDP sites.
Biological samples should be obtained and shipped to Juba to allow laboratory confirmation of emerging outbreaks of measles, AJS, bloody diarrhea and cholera.
The ongoing integrated response to Kala-azar that entails enhanced surveillance, improved access to diagnosis and treatment facilities, refresher training of healthcare workers on Kala-azar case management, replenishing of drug stocks in endemic areas, as well as communication on Kala-azar prevention and control should be sustained.
Support the implementation of the Ebola preparedness and response so as to enhance capacities for case detection, investigation, response and community awareness on Ebola prevention and control.
Please send all disease surveillance information and any outbreak rumours to [email protected]. IDSR reports should be submitted by COB Monday after the close of each epidemiologic week.
For comments or questions, please contact
Department of Epidemics, Preparedness and Response, MoH-RSS E-mail: [email protected],
HF radio frequency: 8015 USP; Selcall: 7002