Report edited
30
of 1 30 Non-medical Related, Supportive Information Needs for Parents with Newly Diagnosed Sick Children Ryerson University Submitted to: Dr. James Tiessen December 12th, 2013 Submitted by: Peter (Yi Nan) Zhang 500597806
-
Upload
peter-zhang -
Category
Documents
-
view
37 -
download
0
Transcript of Report edited

! of !1 30
!!!!!
Non-medical Related, Supportive Information Needs for Parents
with Newly Diagnosed Sick Children
!Ryerson University
Submitted to:
Dr. James Tiessen
December 12th, 2013
!Submitted by:
Peter (Yi Nan) Zhang
500597806
!!

! of !2 30
Abstract
! Quality, timeliness, and relevancy of non-medical related supportive information are
critical for parents with newly diagnosed sick children.
Objectives: This project had two broad objectives. The first is to identify the supportive
information parents are unaware of, and the best timing to disseminate such information. The
second was to investigate links between parent characteristics and satisfaction with information
provided.
Methods: A quantitative methodology is adopted in order to find out descriptive statistics
on the informational gap existing in parental groups. Two paper-based surveys were developed
and reviewed by members of the Family Advisory Console from The Hospital for Sick Children
(SickKids). These surveys contain close ended demographic questions, and checklists of existing
informational knowledge and gaps (see Appendix). Open ended questions are also provided to
find out additional information needs in the two cohorts (see Appendix). Parents are asked to rate
their overall satisfaction with the amount of information they received. The surveys were
distributed by SickKids’ clinical staff at in-patient settings, in the oncology and haematology
units and clinics. Over the time period of 5 days, 34 responses were collected from the oncology
cohort, while 20 were collected from the haematology cohort.
Conclusions: The length of exposure to the management of the child’s condition, the
timing of information given, and availability of financial and supportive information are the
central factors that effect the quality, timeliness, and relevancy of non-medical related supportive
information.

! of !3 30
Table of Content
!Abstract 2
Table of Content 3
Introduction 4
Literature Review 5
Retrieval Methods 5
Parental Involvement in Paediatric Care 6
Challenges Faced by Parental Caregivers 7
Analysis of Stressors 8
Informational Needs 9
Informational Barriers 10
Literacy barriers 10
Information overload 10
Accessibility of information 11
Methodology 12
Data Collection 12
Analysis 12
Data Analysis: Oncology Cohort 13
Data Analysis: Haematology Cohort 19
Conclusion 25
Reference 26
Appendix A— Synopsis of Verbatim Responses 29
! of !4 30
Introduction
Canada has a tradition of patient-oriented medicine practice, and such practice involves
keeping a close partnership between the patients and the health care professionals (Ygge &
Arnetz, 2001). This was advocated both in the US and England as a means of improving quality
of healthcare and treatment outcomes (Hummelinck & Pollock, 2006). The availability of
accurate and comprehensive medical related information are regarded as integral parts of
patients’ rights, and a precondition for a successful partnership between patients and healthcare
professionals (Hummelinck & Pollock, 2006). Despite efforts to disseminate information
formally and informally through the healthcare system, dissatisfaction regarding the direct
communication of information in clinical encounters has been widespread (Minaya et al., 2012).
Hummelinck & Pollock (2006) suggested that patients are dissatisfied with the “amount, quality
and consistency of information about their condition and treatment provided to them by the
professionals”. The complexity of communication between patients and healthcare professionals
are further escalated in the paediatric setting, where parents often act as the intermediary
between the child and the healthcare team.
Other than the amount, quality and consistency of medical information, healthcare
professionals should be aware of the source of stress and categories of challenges faced by
parents in the paediatrics setting. For example, a hostile response by parents during therapeutic
communication could have multiple causes, and only by identifying and providing the right
guidance and support, can the real causes of stress and barriers of communication be resolved.
Evidences had accumulated in three categories of informational barriers: literacy barrier,
informational overload, and the accessibility of information. These factors must be sensitively
! of !5 30
considered when constructing educational materials for parents in the paediatric setting.
However, the creation of such material which encompasses a variety of parental needs is
difficult, since parental responses under difference stressors are highly unpredictable
(Hummelinck & Pollock, 2006). Moreover, several studies have reported that “health
professionals often remain unaware of patients’ treatment preferences and consistently
underestimate bother their information needs and desire for involvement in medical consolation.”
(Hummelinck & Pollock, 2006, p. 229). This leads to an even greater demands for needs-
assessment on the part of healthcare facilities.
This paper pinpoints few theoretical approaches of defining and identifying parental
involvement in paediatric healthcare setting, and challenges faced by parents. Analysis of
stressors and parental informational needs are also highlighted in the literature review. Lastly,
this paper presents the findings from surveys conducted in two paediatric settings (oncology &
haematology units) regarding ancillary (non-medical related) informational gaps.
Literature Review
!!Retrieval Methods
! A search of research literature in the Google Scholar, OVID, PubMED and CINAHL
databases produced 35 articles . The combination of search terms used were: “information
needs”, “caregivers”, “paediatrics”, “oncology”, “quality of care” “meta-analysis” & “literature
review”. 17 articles were excluded due to irrelevancy and non-matching demographics.
! of !6 30
Parental Involvement in Paediatric Care
! Conventional patient care involves direct communication and collaboration between
healthcare professionals and patients, and patient autonomy is treated with special respect.
However, in the case with paediatric care where the patients might be deemed incompetent to
make medical treatment choices, parents become important intermediaries between the patients,
the medical staff, and the final decision makers (Ygge & Arnetz, 2001). In addition, parental
caregivers are often ladened with emotional, physical, social and financial burdens involved in
the patients’ care, and they contribute to patients’ adherence to the treatments (Minaya et al.,
2012).
The Platt Report (1959) had identified that children’s separation from parents could stunt
their character and mental development. Given the sensitive and stressful circumstance when a
child is placed in a hospital environment, parental guidance and presence are ever more essential
in the successful care of the child. Other researchers such as Callery (1997) also emphasize the
importance of parental involvement in the quality and outcome of care for children. Furthermore,
from a moral and legal perspective, parents have the responsibility for the welfare of their
children, and therefore should be actively involved in the care process (Ygge & Arnetz, 2001).
Parental involvement also leads to the parents being more satisfied about the quality of care and
the hospital experience, leading to a positive feedback loop (Ygge & Arnetz, 2001).
!
! of !7 30
Challenges Faced by Parental Caregivers
! During a hospital stay, many stressors such as uncertainty of treatment, guilt, and
burnout, that can challenge parental caregivers’ emotional and physical ability in managing their
children’s care. These stressors can lead to deleterious mental and physical health problems for
the caregivers (Goode, Haley, Roth, & Ford, 1998), and subsequently undermine the caregivers
role in the care of paediatric patients. Depression, emotional distress, and general anxiety are
some common complaints among parental caregivers, and they can sometimes lead to an
increased risk of caregiver mortality in the extreme cases (Minaya et al., 2012). Generally,
quality of life would be severely affected (Minaya et al., 2012).
Two demographic factors are shown to affect the level of stress and health sequalae
experienced by paternal caregivers: age and gender. Age is “negatively related to subjective
burden, impact on schedule, role overload, depression, and mood disturbance” (Minaya et al.,
2012). This can been explained either by the caregivers’ adaptability as their children’s condition
persist through the years, or by the caregivers’ improving cognitive and multitasking abilities.
Meanwhile, gender is well supported by research as a defining factor for the degree of negative
impacts a caregiver encounters. Women are disproportionally afflicted with anxiety, role
captivity, emotional distress, depression and impact on health (Minaya et al. 2012), and Minaya
et al. (2012) also found significant differences between men and women in their quality of life
scores, with women bing more negatively affected. This discrepancy seems paradoxical given
that 39% of caregivers are males (the percentage is higher in the case of cancer caregiving)
(Minaya et al. 2012). Several explanations are given, one involving gender-role socialization,

! of !8 30
and the other states that male caregivers are likely to perceive their experience in caregiving
beneficial to the family unit, thus reporting a higher level of quality of life (Kim, Baker &
Spillers, 2007).
Analysis of Stressors
! There are many theoretic models to understand some of the difficulties experienced by
parental caregivers. Atwood (1989) identified three stressors faced by caregivers: a)
Intrapersonal stressors related to psychological factors such as uncertainty and ineffective
coping; b) Interpersonal stressors, which arise when dealing with multiple staff members or
other caregivers; c) Extrapersonal stressors such as financial distress, and transportation
problems. Another classification is between objective caregiver strain, and subjective
caregiver burden, the first category of stress relates to tasks and functionality (Archbold,
Stewart, Greenlick, & Harvath, 1990), while the latter relates to emotional reaction towards the
caregiving role (Pinquart & Sorenson, 2003).
Despite of the usefulness in categorization of stressors provided by the aforementioned
frameworks, they are very linear and one-dimensional in providing medical practitioners
guidelines in helping parental caregivers. An interactionist approach to role theory was proposed
by Schumacher et al. (2008), as an alternative view to caregiver stressors. This approach views
caregivers as fulfilling certain roles, and three components determine whether a role transition
from parents to caregivers will be successful: caregiving demand (goal-oriented pattern of
behaviour) , mutuality (interpersonal aspects and support network) , and preparedness
(resource obtained, and adaptive behaviours). Mary & Scherbring (2002) reported a significant
! of !9 30
inverse relationship between preparedness and burden score; as preparedness increase by one-
unit, burden decrease by 17%. Moreover, meta-analysis by Sorenson et al. (2004) suggests that
supportive interventions that increase preparedness (e.g. timely information), foster mutuality
(e.g. effective communication), and solve caregiving demand (e.g. home-care training), were
effective in reducing caregiver burden among caregivers from heterogeneous chronic illness
populations.
Informational Needs
! In a systematic literature review of caregiver informational needs, Adams, Boulton &
Watson (2009) point out that, in order of importance, caregivers identified four kinds of
information they viewed as crucial: treatment-related information, prognosis-related information,
coping information, and information on home-care. In addition to medical related information,
paediatric oncology caregivers want to know about resources both in the community and the
hospital, and they identified financial assistance information as valuable (James & Johnson,
1997). Adams, Boulton & Watson (2009) corroborated this last view by stating: “family
members have a wide range of information needs…oncology practice may need to pay greater
attention to proving information on non-medical supportive care topics (to caregivers)”.
!!!
! of !10 30
Informational Barriers
!Literacy barriers
Since parents are often the intermediaries between the children and healthcare
professionals, information package should be tailored towards the parents’ literacy level and
understanding. However, paediatricians in the United States rarely screen the parental caregivers
for reading abilities (Davis, Mayeaux, Fredrickson & Bocchini, 1994), and Davis et al. (1994)
found that two-thirds of parents they studied could not read at a level more than ninth grade, but
the reading materials provided by the hospital are not written at that level. Moreover, many
parents are discouraged by their experience of talking to physicians about diagnosis, due to the
extensive use of medical jargons (Hummelinck & Pollock, 2006). Information needs are shaped
by caregivers level of confidence in dealing with their children’s condition (Hummelinck &
Pollock, 2006), and if caregivers cannot understand and process information given to them, their
ability, competency, and confidence would be severely hampered.
Information overload
When dealing with multidisciplinary teams, parents reported being overwhelmed by the
amount of information they receive, particularly at the time of diagnosis (Hummelinck &
Pollock, 2006). This contributed to caregivers’ finding it difficult to process the information
given and express their information needs, and this situation is further exacerbated because
parents are reluctant to interrupt “busy nurses and doctors” when they did formulate any
questions (Schubart, Kinzie & Farace, 2007). Distraught by the lack of information or the fear of
insufficient information, some parents resort to the media and Internet as a alternative route for
! of !11 30
information (Hummelinck & Pollock, 2006; Schubart, Kinzie & Farace, 2007). This behaviour is
understandable but worrisome, since the quality and trustworthiness of such sources could
further “overload” the caregivers or create unnecessary stress.
Accessibility of information
With “information overload” in mind, it is not hard to imagine caregivers forgetting
information explained to them. Bailey & Caldwell (1997) found that “parents do not always
remember what has been explained to them, particularly in the stressful hospital environment”.
Parents also expressed the need for access to a personal advisor who knew their child and can
spend time with them to answer questions, in addition to written or verbal information (Smith &
Daughtrey, 2000). Therefore, multimedia information packages should be given to parents in
order to facilitate retention of knowledge, thus reducing caregiver stress and anxiety.
! In conclusion, parental involvement in paediatric care is vital to the health outcomes of
the patients, since parents act as advocates and intermediaries during the care process. Parents
are placed under immense stresses, and they often suffer negative physical and emotional
consequences from these stressors. Such stressors can be categorized into: intrapersonal,
interpersonal, and extrapersonal, and effective dealings of these stressors can reduce caregiver
burdens. Lastly, by providing appropriate and timely information, the overall stress of parents
can be greatly reduced. However, literacy barriers, information overload, and accessibility of
information are identified as informational barriers.
! of !12 30
Methodology
!Data Collection
A quantitative methodology is adopted in order to find out descriptive statistics on the
informational gap existing in parental groups. The purpose of the surveys is to identify parents’
familiarity to supportive services provided, and recognize the method of delivery parents prefer
and opportune timing of this non-medical related supportive information. Two paper-based
surveys were developed and reviewed by members of the Family Advisory Console from The
Hospital for Sick Children (SickKids). These surveys contain close ended demographic
questions, and checklists of existing informational knowledge and gaps (see Appendix). Open
ended questions were also provided to find out additional information needs in the two cohorts
(see Appendix). Parents are also asked to rate their overall satisfaction with the amount of
information they received.
The surveys were distributed by SickKids’ clinical staff at in-patient settings, in the
oncology and haematology units and clinics. Over the time period of 5 days, 34 responses were
collected from the oncology cohort, while 20 were collected from the haematology cohort.
Analysis
! Survey data were entered into SPSS Version 21, and close ended questions were coded
and labeled, while open ended questions are collected into verbatim report that is not included in
the SPSS analysis. Descriptive statistics of the demographic information are charted, and
checklists responses are measured and ranked in order of informational awareness (i.e. the least
! of !13 30
known information topic is placed on the top of charts). Finally, correlation and regression
analysis are conducted in order to find out possible relationships between demographical
characteristics/specific informational gaps and parental satisfaction with amount of supportive
information provided.
Data Analysis: Oncology Cohort
The survey yielded 35 responses, 1 was discarded due to incomplete information.
Frequency distribution of each survey questions will be discussed first, following synopsis of
verbatim qualitative data (see Appendix).
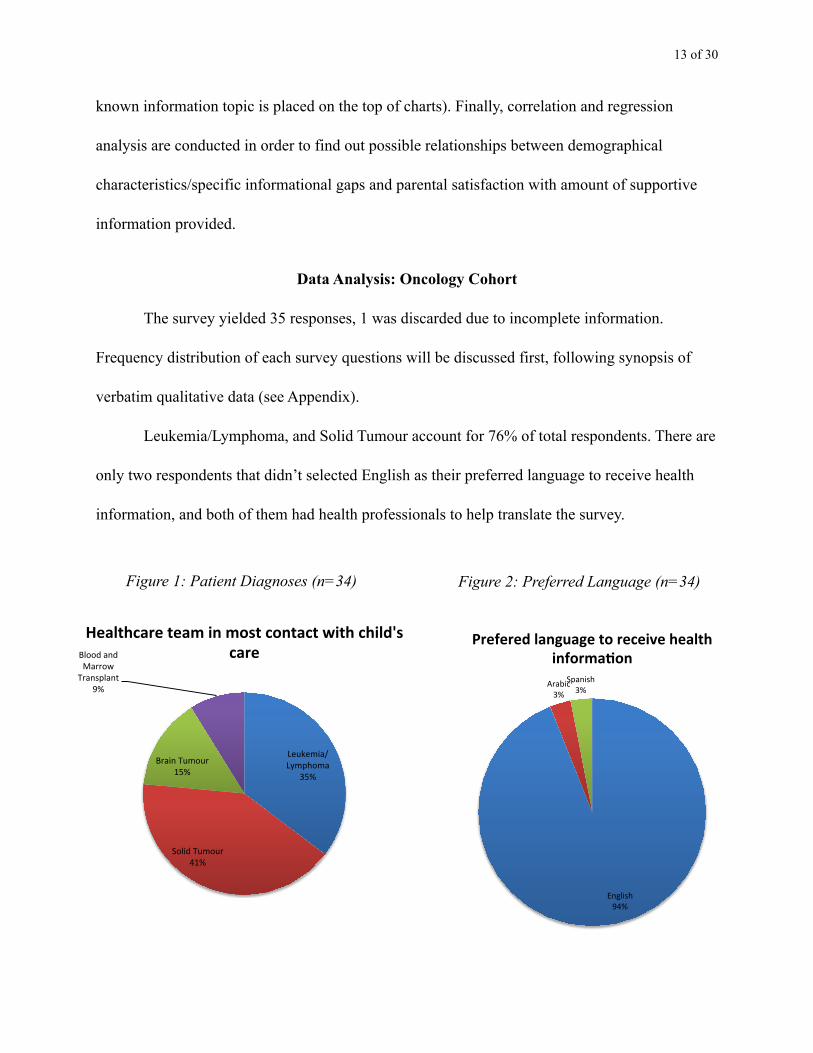
Leukemia/Lymphoma, and Solid Tumour account for 76% of total respondents. There are
only two respondents that didn’t selected English as their preferred language to receive health
information, and both of them had health professionals to help translate the survey.
!
!!!!!
!
Leukemia/Lymphoma-
35%-
Solid-Tumour-41%-
Brain-Tumour-15%-
Blood-and-Marrow-
Transplant-9%-
Healthcare)team)in)most)contact)with)child's)care)
English(94%(
Arabic(3%(
Spanish(3%(
Prefered&language&to&receive&health&informa3on&
Figure 1: Patient Diagnoses (n=34) Figure 2: Preferred Language (n=34)

! of !14 30
79% of Oncology patients were newly diagnosed (between 2010 to 2013), and they
visited most frequent weekly (41%) and every 3 months (38%). “Year of diagnoses” is connected
with general satisfaction with the amount of information received. The more recent the diagnosis,
the better rating for satisfaction level. This correlation might be brought about by the freshness of
information given.
! Most parents come from more than 10 km away from SickKids, and this does not effect
the satisfaction with the amount of information given. However, traveling and parking
arrangement information should be distributed to parents, as 45% (adjusted figure) of them do
not know about parent multi-use/long stay parking passes.
!
!
!!
41%$
15%$
38%$
6%$0%$
5%$
10%$
15%$
20%$
25%$
30%$
35%$
40%$
45%$
Weekly$ Monthly$ Every$3$months$ Every$year$
Freqency(of(visit(to(SickKids(
0%#
10%#
20%#
30%#
40%#
50%#
60%#
70%#
80%#
90%#
2005-2010# 2010-2013#
Year%of%diagnoses%
Figure 3: Patients’ Year of Diagnoses (n=34) Figure 4: Patients’ Frequency of Visits (n=34)
! of !15 30
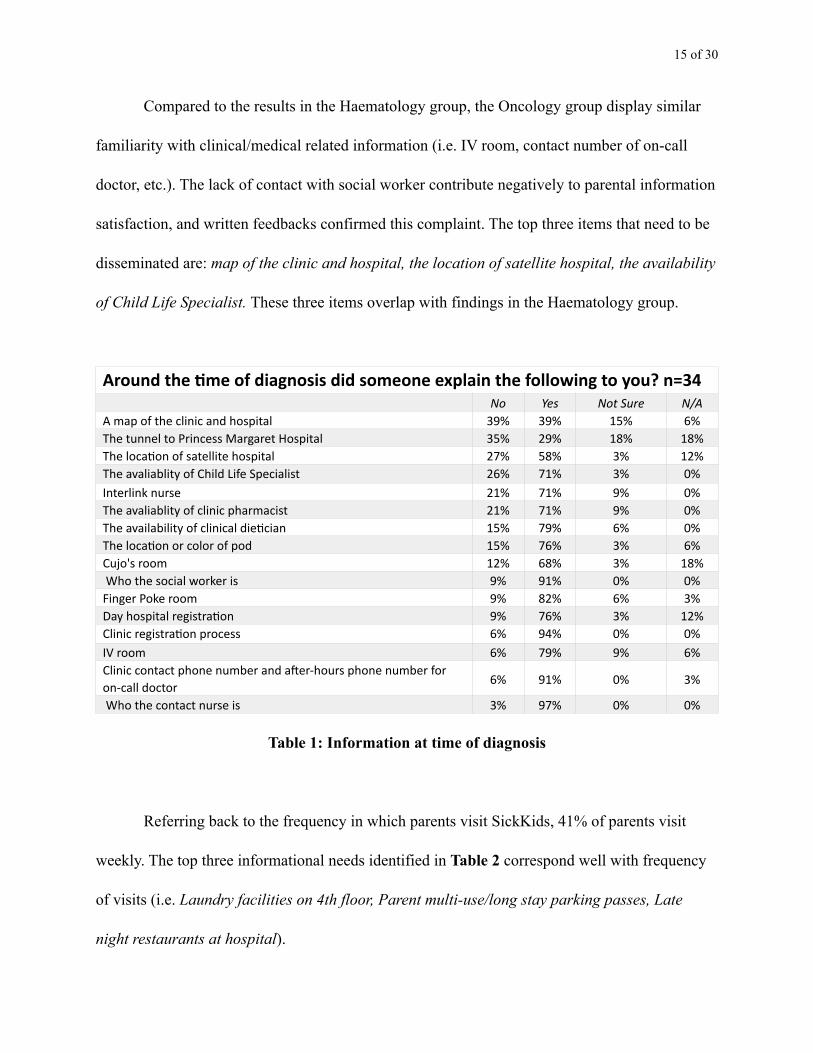
! Compared to the results in the Haematology group, the Oncology group display similar
familiarity with clinical/medical related information (i.e. IV room, contact number of on-call
doctor, etc.). The lack of contact with social worker contribute negatively to parental information
satisfaction, and written feedbacks confirmed this complaint. The top three items that need to be
disseminated are: map of the clinic and hospital, the location of satellite hospital, the availability
of Child Life Specialist. These three items overlap with findings in the Haematology group.
!
Table 1: Information at time of diagnosis
Referring back to the frequency in which parents visit SickKids, 41% of parents visit
weekly. The top three informational needs identified in Table 2 correspond well with frequency
of visits (i.e. Laundry facilities on 4th floor, Parent multi-use/long stay parking passes, Late
night restaurants at hospital).
Around the +me of diagnosis did someone explain the following to you? n=34No Yes Not Sure N/A
A map of the clinic and hospital 39% 39% 15% 6%The tunnel to Princess Margaret Hospital 35% 29% 18% 18%The loca@on of satellite hospital 27% 58% 3% 12%The avaliablity of Child Life Specialist 26% 71% 3% 0%Interlink nurse 21% 71% 9% 0%The avaliablity of clinic pharmacist 21% 71% 9% 0%The availability of clinical die@cian 15% 79% 6% 0%The loca@on or color of pod 15% 76% 3% 6%Cujo's room 12% 68% 3% 18% Who the social worker is 9% 91% 0% 0%Finger Poke room 9% 82% 6% 3%Day hospital registra@on 9% 76% 3% 12%Clinic registra@on process 6% 94% 0% 0%IV room 6% 79% 9% 6%Clinic contact phone number and aSer-‐hours phone number for on-‐call doctor 6% 91% 0% 3%
Who the contact nurse is 3% 97% 0% 0%

! of !16 30
!
Table 2: Information familiarity around the time of diagnosis
Satisfaction level is high (36% “very good”,
52% “excellent”), and this might be due to frequent
visits resulting in more contacts with medical/support
staff. High cure rates of paediatric cancer (75%) can
also reduce stress level of parents, leading to better
absorption of information.
!!
Top items are: YMCA on Shutter Street-free use for parents, Northern Health Travel
Grant, Carepages or Caringbridge, website/blogs, SickKids Theatre, Kids Health website (Table
3). These can further be categorized as “transportation resource needs” and “multimedia resource
Around the +me of diagnosis, did someone tell you about the following services? n=34
No Yes Not Sure N/A
Laundry facili@es on 4th floor 52% 35% 10% 3%
Parent mul@-‐use/long stay parking passes 40% 43% 7% 10%
Late night restaurants at hospital 39% 48% 6% 6%
Meal train purchase for parents 29% 61% 6% 3%
Free Wi Fi 19% 74% 0% 6%
In-‐pa@ent procedures/registra@on 7% 83% 7% 3%
Parent fridge and microwave 0% 97% 0% 3%
52%$
36%$
6%$
6%$
0%$ 10%$ 20%$ 30%$ 40%$ 50%$ 60%$
Excellent$
Very$good$
Good$
Fair$
Overall'sa)sfac)on'with'the'amount'of'informa)on'about'people,places'and/or'services'received'at'diagnosis'
Figure 5: Overall satisfaction level (n=34)

! of !17 30
needs”. Research indicates that multimedia enhances information retention, therefore should be
developed and distributed.
Table 3: Familiarity with supportive service & preferred timing of information
Did someone explain the following suppor+ve services to you? When is the best +me to get this informa+on? n=34
No YesNot Sure N/A
At Diagnosis
1st month 3 months
YMCA on ShuYer Street-‐free use for parents 74% 9% 6% 12% 23% 65% 12%
Carepages or Caringbridge website/blogs 65% 18% 12% 6% 30% 57% 13%
SickKids Theatre 53% 35% 6% 6% 22% 67% 11% Kids Health website 50% 35% 12% 3% 41% 48% 10%
Northern Health Travel Grant 44% 6% 6% 44% 57% 39% 4%
Parent support programs in your community
41% 44% 9% 6% 42% 42% 15%
Nearby hotels with special rates 35% 21% 3% 41% 70% 30% 0%
EI Caregiver Benefit 35% 47% 6% 12% 74% 22% 4% OPACC & Parent Liaison 32% 44% 18% 6% 41% 59% 0% Marnie' Place (4th floor) 30% 52% 9% 9% 25% 71% 4% Employment benefits 30% 45% 9% 15% 69% 27% 4%
Ronald McDonald House 24% 29% 3% 44% 82% 18% 0%
Starlight Room (9th floor) 21% 74% 3% 3% 13% 80% 7%
Camp Ooch at SickKids 21% 76% 0% 3% 36% 57% 7% Access to translators 21% 15% 0% 65% 88% 12% 0%
Canadian Cancer Society Transporta@on program
21% 59% 3% 18% 65% 35% 0%
Canadian Cancer Society Family Transporta@on Reimbursment
18% 65% 9% 9% 61% 36% 4%
Interlink Nurse visit to child's school 6% 65% 9% 21% 33% 56% 11%
POFAP Financial Assistance through POGO 3% 91% 3% 3% 64% 32% 4%
! of !18 30
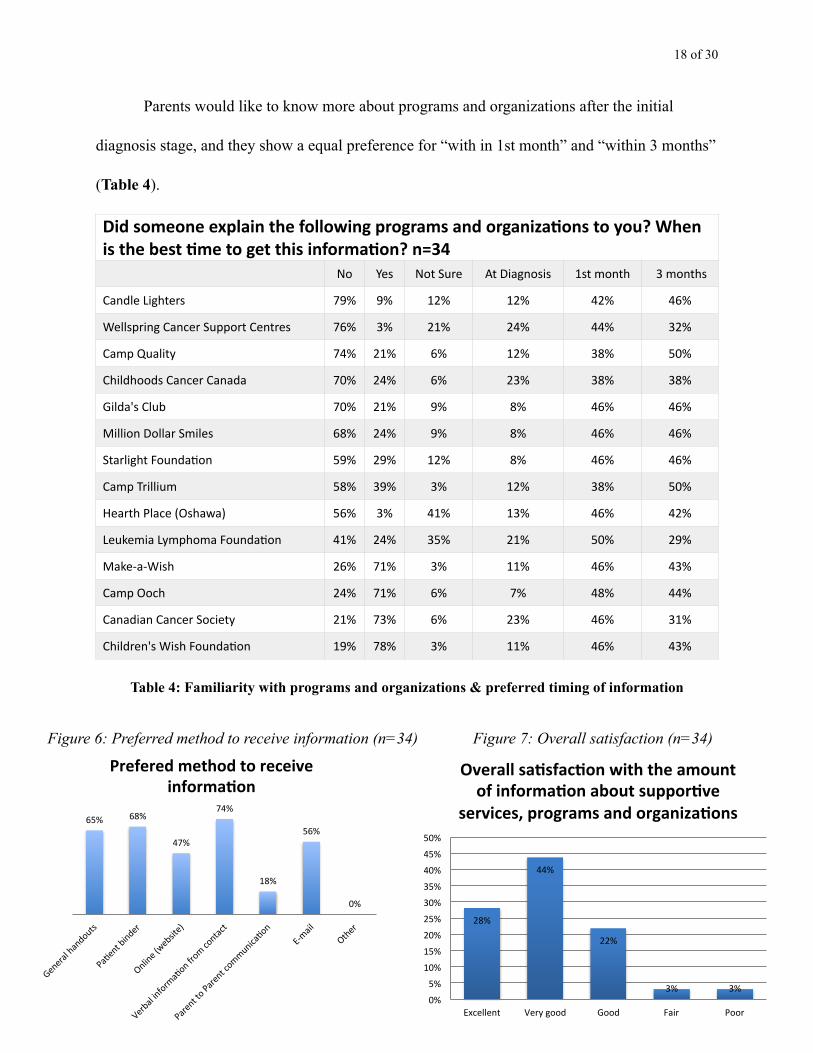
Parents would like to know more about programs and organizations after the initial
diagnosis stage, and they show a equal preference for “with in 1st month” and “within 3 months”
(Table 4).
Table 4: Familiarity with programs and organizations & preferred timing of information
Did someone explain the following programs and organiza+ons to you? When is the best +me to get this informa+on? n=34
No Yes Not Sure At Diagnosis 1st month 3 months
Candle Lighters 79% 9% 12% 12% 42% 46%
Wellspring Cancer Support Centres 76% 3% 21% 24% 44% 32%
Camp Quality 74% 21% 6% 12% 38% 50%
Childhoods Cancer Canada 70% 24% 6% 23% 38% 38%
Gilda's Club 70% 21% 9% 8% 46% 46%
Million Dollar Smiles 68% 24% 9% 8% 46% 46%
Starlight Founda@on 59% 29% 12% 8% 46% 46%
Camp Trillium 58% 39% 3% 12% 38% 50%
Hearth Place (Oshawa) 56% 3% 41% 13% 46% 42%
Leukemia Lymphoma Founda@on 41% 24% 35% 21% 50% 29%
Make-‐a-‐Wish 26% 71% 3% 11% 46% 43%
Camp Ooch 24% 71% 6% 7% 48% 44%
Canadian Cancer Society 21% 73% 6% 23% 46% 31%
Children's Wish Founda@on 19% 78% 3% 11% 46% 43%
65%$ 68%$
47%$
74%$
18%$
56%$
0%$
General$handouts$
Pa7ent$binder$
Online$(website)$
Verbal$informa7on$from
$contact$
Parent$to$Parent$communica7on$
ECmail$
Other$
Prefered&method&to&receive&informa0on&
28%$
44%$
22%$
3%$ 3%$0%$
5%$
10%$
15%$
20%$
25%$
30%$
35%$
40%$
45%$
50%$
Excellent$ Very$good$ Good$ Fair$ Poor$
Overall'sa)sfac)on'with'the'amount'of'informa)on'about'suppor)ve'
services,'programs'and'organiza)ons'
Figure 6: Preferred method to receive information (n=34) Figure 7: Overall satisfaction (n=34)
! of !19 30
Data Analysis: Haematology Cohort
The survey yielded 20 responses, and frequency distribution of each survey questions
will be discussed first, following synopsis of verbatim qualitative data.
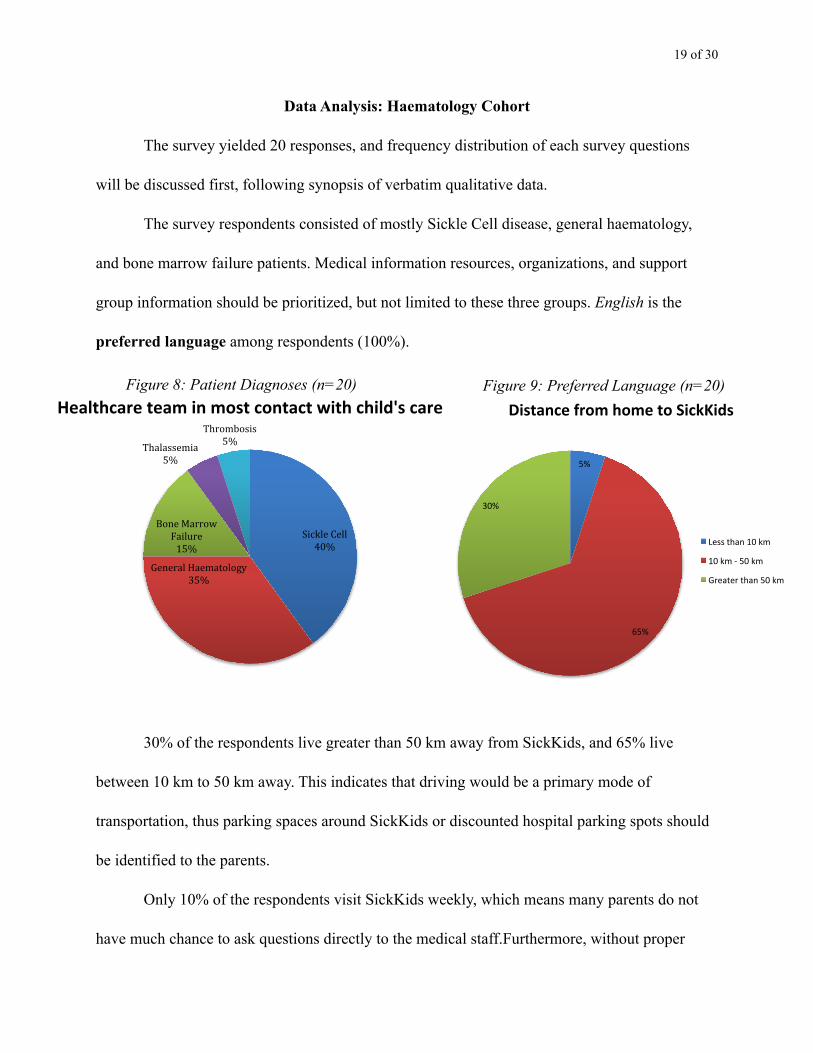
The survey respondents consisted of mostly Sickle Cell disease, general haematology,
and bone marrow failure patients. Medical information resources, organizations, and support
group information should be prioritized, but not limited to these three groups. English is the
preferred language among respondents (100%).
! 30% of the respondents live greater than 50 km away from SickKids, and 65% live
between 10 km to 50 km away. This indicates that driving would be a primary mode of
transportation, thus parking spaces around SickKids or discounted hospital parking spots should
be identified to the parents.
Only 10% of the respondents visit SickKids weekly, which means many parents do not
have much chance to ask questions directly to the medical staff.Furthermore, without proper
Sickle'Cell'40%'
General'Haematology'35%'
Bone'Marrow'Failure'15%'
Thalassemia'5%'
Thrombosis'5%'
Healthcare)team)in)most)contact)with)child's)care)
5%#
65%#
30%#
Distance)from)home)to)SickKids)
Less#than#10#km#
10#km#1#50#km#
Greater#than#50#km#
Figure 8: Patient Diagnoses (n=20) Figure 9: Preferred Language (n=20)

! of !20 30
educational/reference materials, it is likely for parents to forget the information given to them,
leading to greater extent of anxiety in subsequent visits. Since medical information handouts
already exist for parents to take home, a resource-based checklist would most benefit the parents.
SickKids serves patients up to the age of
18, and the data collected span from 1995 to
2013. Therefore the frequency of “year of
diagnoses” can be seen as demographic
information. The age group then is separated
into quartiles: 0-5 year-olds (11%); 5-10
year-olds (22%); 10-15 year-olds (39%), and
15-18 year-olds (28%). Depending on the age
group, there should be resources that reflects
the patient demographic (data here might not reflect the actual demographic due to small sample
size).
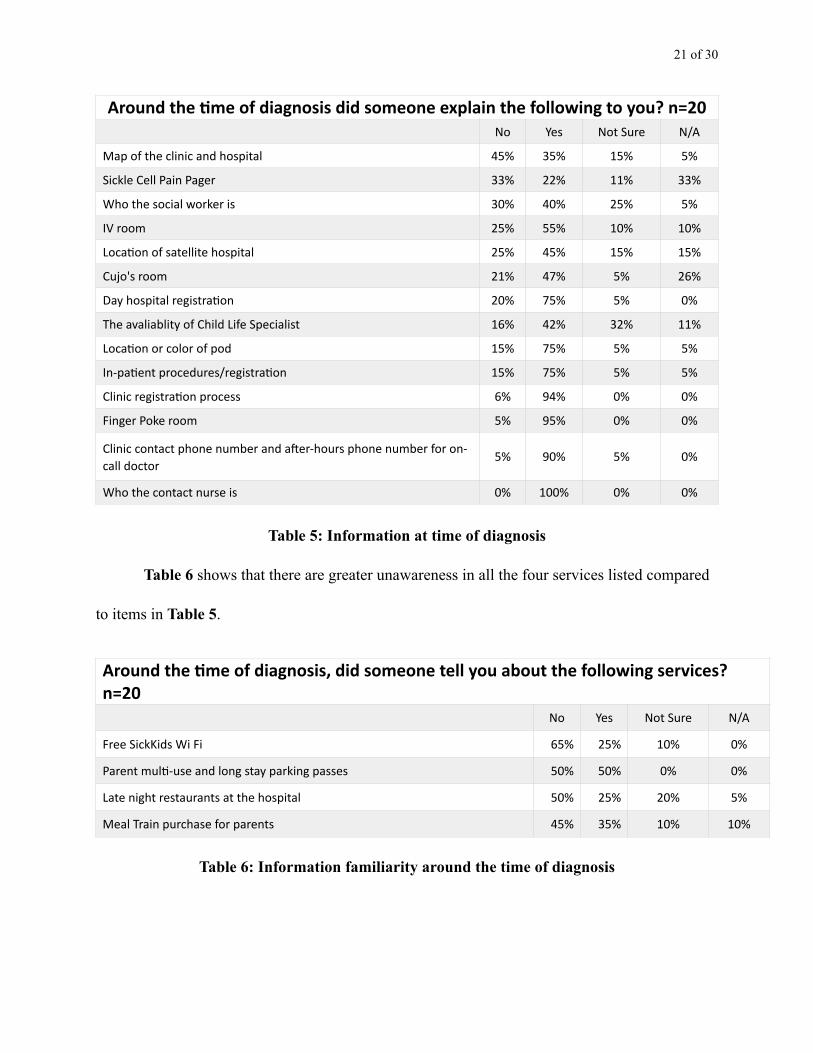
! Table 5 and all other further tables are arranged in descending order interns of how many
people were unaware of the resources offered at SickKids. This process identifies knowledge
gaps that could be filled with proposed Patient Orientation Checklist. The top five information
needs are: Map of the clinic and hospital, Who the social worker is, IV room, Location of satellite
hospital, and Availability of Child Life Specialist. (ranking has been adjusted due to N/A
answers).
!
11%#
22%#
39%#
28%#
0%#
5%#
10%#
15%#
20%#
25%#
30%#
35%#
40%#
45%#
1995+2000# 2000+2005# 2005+2010# 2010+2013#
Year%of%diagnoses%
Figure 10: Patients’ Year of Diagnoses (n=20)
! of !21 30
Table 5: Information at time of diagnosis
Table 6 shows that there are greater unawareness in all the four services listed compared
to items in Table 5.
Table 6: Information familiarity around the time of diagnosis
!
Around the +me of diagnosis did someone explain the following to you? n=20No Yes Not Sure N/A
Map of the clinic and hospital 45% 35% 15% 5%
Sickle Cell Pain Pager 33% 22% 11% 33%
Who the social worker is 30% 40% 25% 5%
IV room 25% 55% 10% 10%
Loca@on of satellite hospital 25% 45% 15% 15%
Cujo's room 21% 47% 5% 26%
Day hospital registra@on 20% 75% 5% 0%
The avaliablity of Child Life Specialist 16% 42% 32% 11%
Loca@on or color of pod 15% 75% 5% 5%
In-‐pa@ent procedures/registra@on 15% 75% 5% 5%
Clinic registra@on process 6% 94% 0% 0%
Finger Poke room 5% 95% 0% 0%
Clinic contact phone number and aSer-‐hours phone number for on-‐call doctor
5% 90% 5% 0%
Who the contact nurse is 0% 100% 0% 0%
Around the +me of diagnosis, did someone tell you about the following services? n=20
No Yes Not Sure N/A
Free SickKids Wi Fi 65% 25% 10% 0%
Parent mul@-‐use and long stay parking passes 50% 50% 0% 0%
Late night restaurants at the hospital 50% 25% 20% 5%
Meal Train purchase for parents 45% 35% 10% 10%
! of !22 30
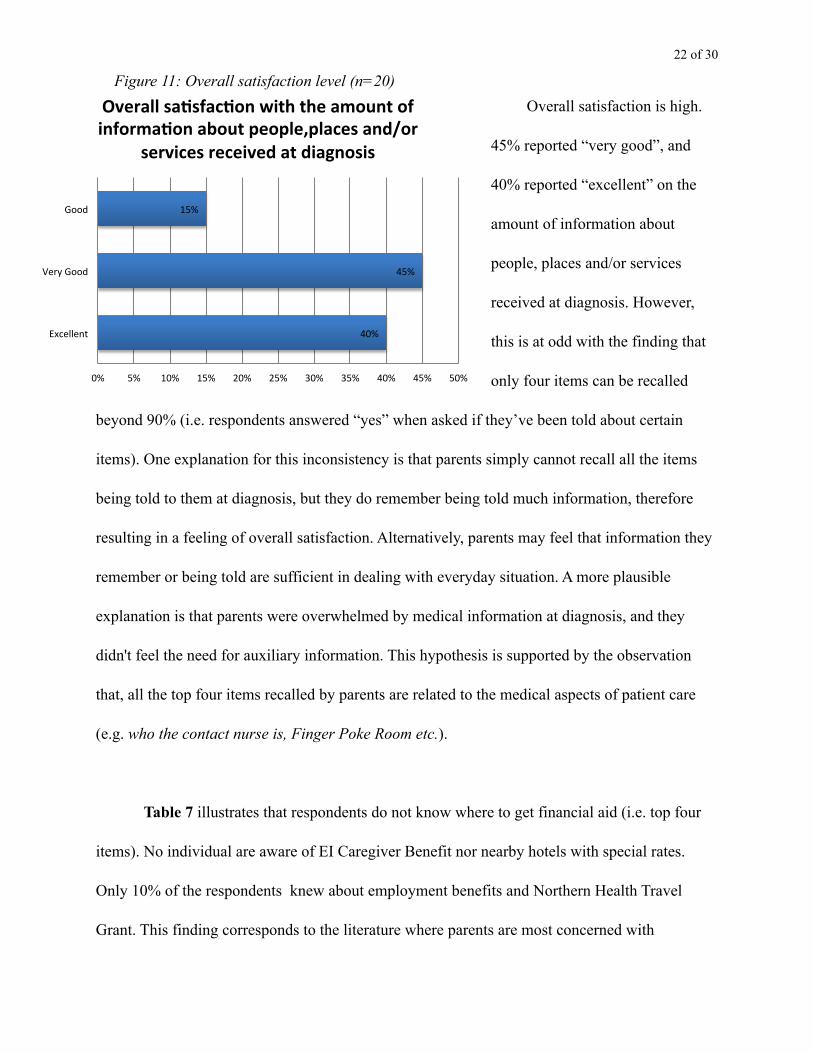
Overall satisfaction is high.
45% reported “very good”, and
40% reported “excellent” on the
amount of information about
people, places and/or services
received at diagnosis. However,
this is at odd with the finding that
only four items can be recalled
beyond 90% (i.e. respondents answered “yes” when asked if they’ve been told about certain
items). One explanation for this inconsistency is that parents simply cannot recall all the items
being told to them at diagnosis, but they do remember being told much information, therefore
resulting in a feeling of overall satisfaction. Alternatively, parents may feel that information they
remember or being told are sufficient in dealing with everyday situation. A more plausible
explanation is that parents were overwhelmed by medical information at diagnosis, and they
didn't feel the need for auxiliary information. This hypothesis is supported by the observation
that, all the top four items recalled by parents are related to the medical aspects of patient care
(e.g. who the contact nurse is, Finger Poke Room etc.).
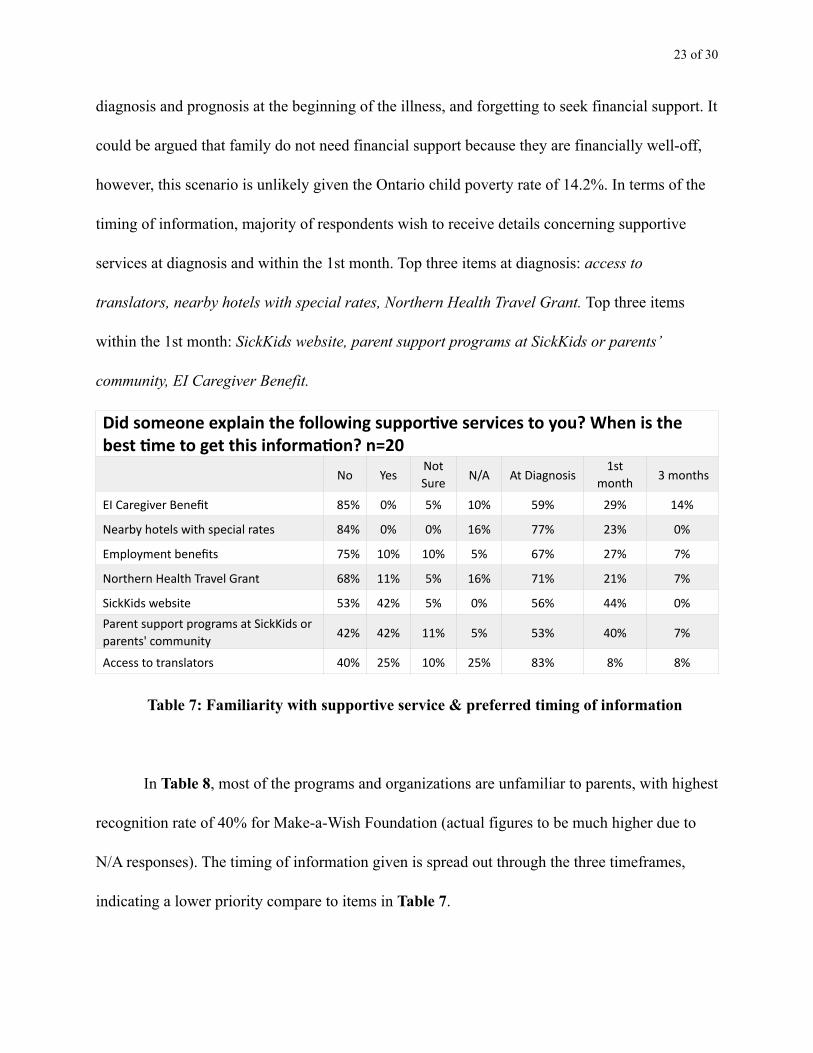
! Table 7 illustrates that respondents do not know where to get financial aid (i.e. top four
items). No individual are aware of EI Caregiver Benefit nor nearby hotels with special rates.
Only 10% of the respondents knew about employment benefits and Northern Health Travel
Grant. This finding corresponds to the literature where parents are most concerned with
40%$
45%$
15%$
0%$ 5%$ 10%$ 15%$ 20%$ 25%$ 30%$ 35%$ 40%$ 45%$ 50%$
Excellent$
Very$Good$
Good$
Overall'sa)sfac)on'with'the'amount'of'informa)on'about'people,places'and/or'
services'received'at'diagnosis'
Figure 11: Overall satisfaction level (n=20)
! of !23 30
diagnosis and prognosis at the beginning of the illness, and forgetting to seek financial support. It
could be argued that family do not need financial support because they are financially well-off,
however, this scenario is unlikely given the Ontario child poverty rate of 14.2%. In terms of the
timing of information, majority of respondents wish to receive details concerning supportive
services at diagnosis and within the 1st month. Top three items at diagnosis: access to
translators, nearby hotels with special rates, Northern Health Travel Grant. Top three items
within the 1st month: SickKids website, parent support programs at SickKids or parents’
community, EI Caregiver Benefit.
Table 7: Familiarity with supportive service & preferred timing of information
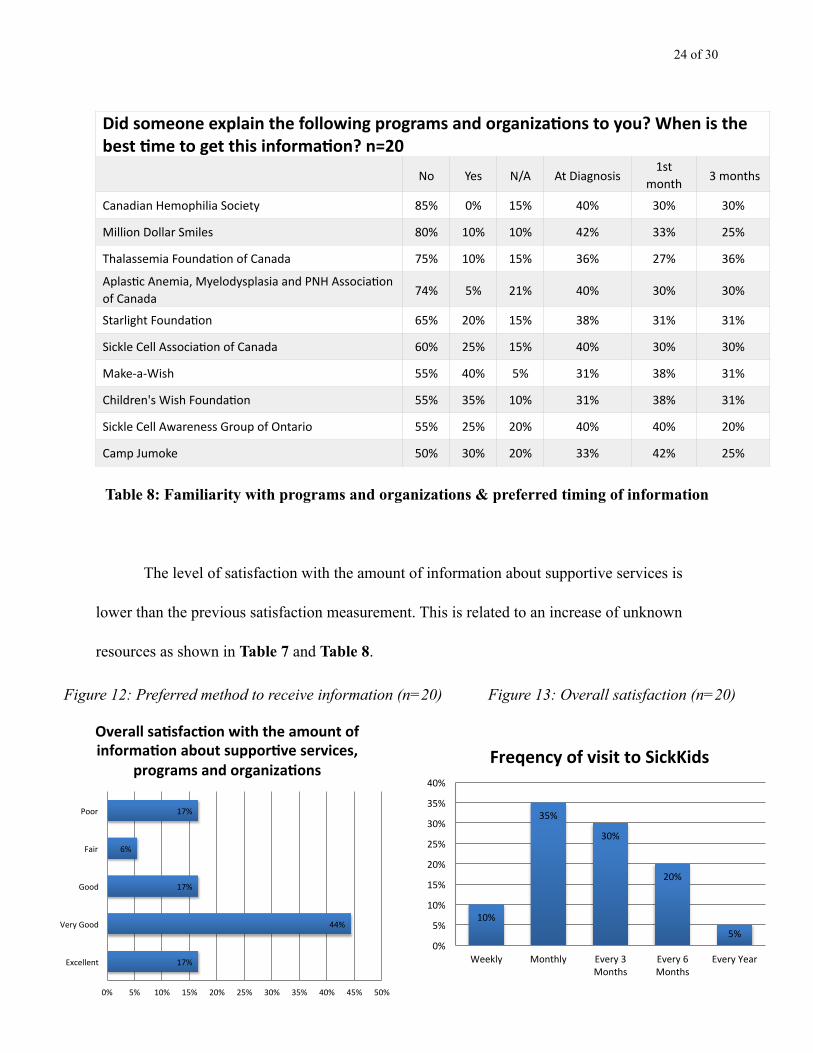
! In Table 8, most of the programs and organizations are unfamiliar to parents, with highest
recognition rate of 40% for Make-a-Wish Foundation (actual figures to be much higher due to
N/A responses). The timing of information given is spread out through the three timeframes,
indicating a lower priority compare to items in Table 7.
Did someone explain the following suppor+ve services to you? When is the best +me to get this informa+on? n=20
No YesNot Sure N/A At Diagnosis
1st month 3 months
EI Caregiver Benefit 85% 0% 5% 10% 59% 29% 14%
Nearby hotels with special rates 84% 0% 0% 16% 77% 23% 0%
Employment benefits 75% 10% 10% 5% 67% 27% 7%
Northern Health Travel Grant 68% 11% 5% 16% 71% 21% 7%
SickKids website 53% 42% 5% 0% 56% 44% 0%Parent support programs at SickKids or parents' community 42% 42% 11% 5% 53% 40% 7%
Access to translators 40% 25% 10% 25% 83% 8% 8%
! of !24 30
Table 8: Familiarity with programs and organizations & preferred timing of information
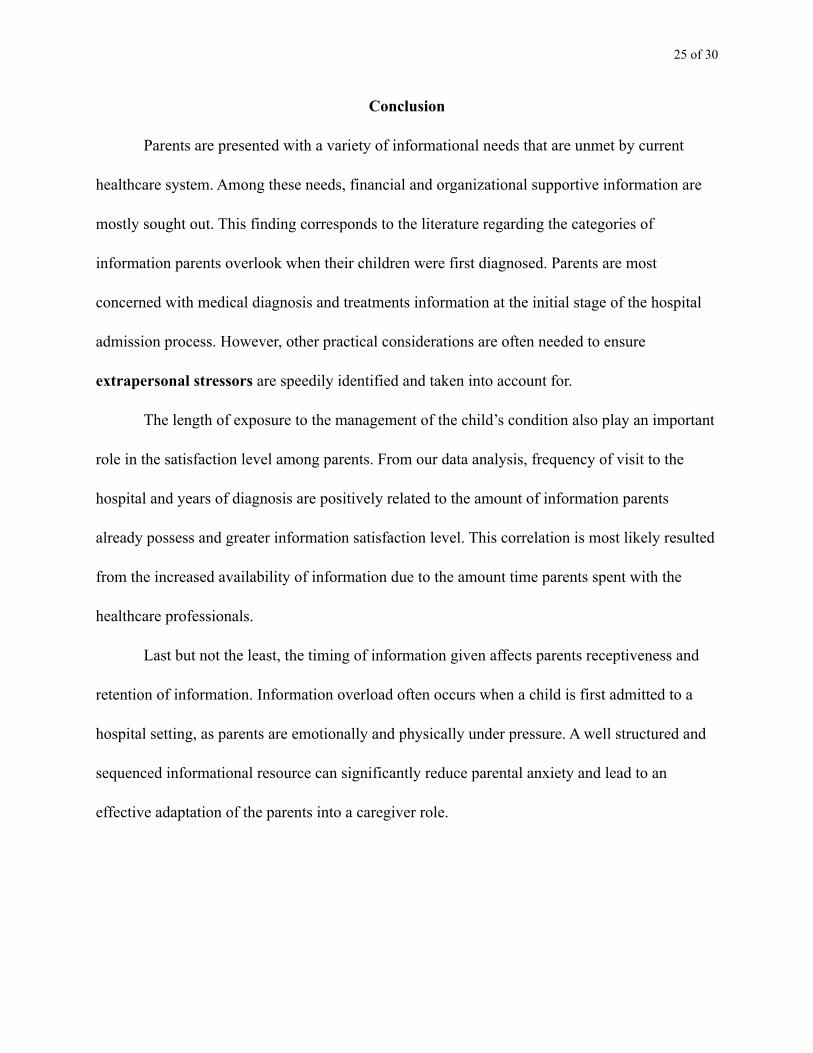
! The level of satisfaction with the amount of information about supportive services is
lower than the previous satisfaction measurement. This is related to an increase of unknown
resources as shown in Table 7 and Table 8.
!
17%$
44%$
17%$
6%$
17%$
0%$ 5%$ 10%$ 15%$ 20%$ 25%$ 30%$ 35%$ 40%$ 45%$ 50%$
Excellent$
Very$Good$
Good$
Fair$
Poor$
Overall'sa)sfac)on'with'the'amount'of'informa)on'about'suppor)ve'services,'
programs'and'organiza)ons'
10%$
35%$
30%$
20%$
5%$0%$
5%$
10%$
15%$
20%$
25%$
30%$
35%$
40%$
Weekly$ Monthly$ Every$3$Months$
Every$6$Months$
Every$Year$
Freqency(of(visit(to(SickKids(
Figure 12: Preferred method to receive information (n=20) Figure 13: Overall satisfaction (n=20)
Did someone explain the following programs and organiza+ons to you? When is the best +me to get this informa+on? n=20
No Yes N/A At Diagnosis1st
month 3 months
Canadian Hemophilia Society 85% 0% 15% 40% 30% 30%
Million Dollar Smiles 80% 10% 10% 42% 33% 25%
Thalassemia Founda@on of Canada 75% 10% 15% 36% 27% 36%
Aplas@c Anemia, Myelodysplasia and PNH Associa@on of Canada 74% 5% 21% 40% 30% 30%
Starlight Founda@on 65% 20% 15% 38% 31% 31%
Sickle Cell Associa@on of Canada 60% 25% 15% 40% 30% 30%
Make-‐a-‐Wish 55% 40% 5% 31% 38% 31%
Children's Wish Founda@on 55% 35% 10% 31% 38% 31%
Sickle Cell Awareness Group of Ontario 55% 25% 20% 40% 40% 20%
Camp Jumoke 50% 30% 20% 33% 42% 25%
! of !25 30
Conclusion
Parents are presented with a variety of informational needs that are unmet by current
healthcare system. Among these needs, financial and organizational supportive information are
mostly sought out. This finding corresponds to the literature regarding the categories of
information parents overlook when their children were first diagnosed. Parents are most
concerned with medical diagnosis and treatments information at the initial stage of the hospital
admission process. However, other practical considerations are often needed to ensure
extrapersonal stressors are speedily identified and taken into account for.
The length of exposure to the management of the child’s condition also play an important
role in the satisfaction level among parents. From our data analysis, frequency of visit to the
hospital and years of diagnosis are positively related to the amount of information parents
already possess and greater information satisfaction level. This correlation is most likely resulted
from the increased availability of information due to the amount time parents spent with the
healthcare professionals.
Last but not the least, the timing of information given affects parents receptiveness and
retention of information. Information overload often occurs when a child is first admitted to a
hospital setting, as parents are emotionally and physically under pressure. A well structured and
sequenced informational resource can significantly reduce parental anxiety and lead to an
effective adaptation of the parents into a caregiver role.
!!!
! of !26 30
Reference
!Agrawal, S., Archbold, P. G., Caparro, M., Multale, F., Schumacher, K.L. & Stewart, B. J.
(2008). Effects of caregiving demand, mutuality, and preparedness on family caregiver
outcomes during cancer treatment. Oncology Nursing Forum, 55, 49-65.
Adams, E., Boulton, M. & Watson, E. (2009). The information needs of partners and family
members of cancer patients: A systematic literature review. Patient Education and
Counseling, 77, 179-186.
Contro, N., Larson, J., Scofield, S., Sourkes, B. & Cohen, H. (2002). Family Perspectives on the
quality of paediatric palliative care. Arch Pediatr Adolesc Med, 156, 14-19.
Davis, T. C., Mayeaux, E. J., Fredrickson, D., Bocchini J. A., Jackson, R. H. & Murphy, P. W.
(1994). Reading ability of parents compared with reading level of paediatric patient
education materials. Pediatrics, 93, 460-468.
Honea, N. J., Brintnall, R., Given, B., Sherwood, P., Colao, D. B., Somers, S. C.& Northouse, L.
I. (2008). Putting evidence into practice: Nursing assessment and interventions to reduce
family caregiver strain and burden. Clinical Journal of Oncology Nursing, 12, 507-516.
Hummelinch, A. & Pollock, K. (2005). Parents’ information needs about the treatment of their
chronically ill child: A qualitative study. Patient Education and Counseling, 62, 228-234.
Hardwick, C. & Lawson. N. (1995). The information and learning needs of the caregiving family
of the adult patient with cancer. European Journal of Cancer Care, 4, 118-121.

! of !27 30
James, L. & Johnson, B. (1997). The needs of parents of paediatric oncology patient during the
palliative care phase. Journal of Pediatric Oncology Nursing, 14, 83-95.
Minaya, P., Baumstarck, K., Berbis, J., Goncalve, A., Barlesi, F., Michel, G., Salas, S., Chinot,
O., Grob, J., Seitz, J. F., Bladou, F., Clement, A., Mancini, J. Simeoni, M. & Auquier, P.
(2012). The Caregiver Oncology Quality of Life Questionnaire (CarGOQoL):
Development and validation of an insturment to measure the quality of life of the
caregivers of patients with cancer. European Journal of Cancer, 48, 904-911.
Meyer. E. C., Ritholz, M. D., Burns, J. P. & Truog, R. D. (2005). Improving the quality of end-
of-life care in the paediatric intensive are unit: Parents’ priorities and recommendations.
Pediatrics, 117, 649-657.
Noyes, J. (1998). A critique of studies exploring the experiences and needs of parents of children
admitted to paediatric intensive care units. Journal of Advanced Nursing, 28, 134-141.
Scherbring, M. (2002). Effect of caregiver perception of preparedness on burden in an oncology
population. ONF, 29, 70-76.
Schubart, J. R., Kinzie, M. B. & Farace, E. (2007). Caring for the brain timor patient: Family
caregiver burden and unmet needs. Society for Nero-Oncology, 61-72.
Smith, L. & Daughtrey, H. (1999). Weaving the seamless web of care: an analysis of parents’
perceptions of their needs following discharge of their child from hospital. Issues and
Innovations in Nursing Practice, 31, 812-820.
! of !28 30
Yim, Y. Baker, F. & Spillers, R. L. (2007). Cancer caregivers’ quality of life: effects of gender,
relationship, and appraisal. Journal of Pain and Symptom Management, 34, 294-304.
Ygge, B. & Arnetz, J. E. (2001). Quality of paediatric care: application and validation of an
instrument for measuring parent satisfaction with hospital care. International Journal for
Quality in Health Care, 13, 33-43.
Ygge, B. M., Lindholm, C. & Arnetz, J. (2005). Hospital staff perceptions of parental
involvement in paediatric hospital care. Issues and Innovations in Nursing Practice, 76,
534-542.
Ygge. B. M. & Arnetz, J. E. (2004). A study of parental involvement in paediatric hospital care:
Implementations for clinical practice. Journal of Pediatric Nursing, 19, 217-223.
!!!!!!!!
! of !29 30
Appendix A— Synopsis of Verbatim Responses
Oncology Group !Q8. People, places and/or services you wish you knew about at diagnosis in SickKids oncology experience: !• Parental parking discounts and weekly passes • Should be services that allow parents to question hospital policies and procedures • Restaurants/food places around hospital, laundry • Resources(personnel/services) for use during new therapies (i.e. CBC draw, transaction). • Never offered assistance from a social worker • Child Life Specialist, restaurants outside of hospital • Marnies lunge assistance services through social worker , special benefits for parents !Q11. Any other supportive services that you wish you knew about during your SickKids oncology experience: !• NOFCC Child Life • Unclear who to talk to when have questions requiring staff or procedure (maybe introduce
duties in the hospital and procedures, and why they are done). • In terms of parenteral nutrition (GI feed, etc.), Ensure/Boost, trail (sampling) of different
products with kids to see which one works the best with individual kids since there are so many products on the market.
• Out-patient chemo nurses were scarce, wants a list of all the out-patient (visiting nurses). !Q13. Any other programs and/or organizations that you wish you knew about during your SickKids oncology experience: • Many services offered were not used by this couple • Nutritional !Q16. Add. feedback: • After first few days after diagnosis, parents should be taken on a guided tour of 8D & Sears
Day Clinic to get an idea of the layout and procedures. • Overwhelming information and understanding the treatments and side effects are most
important that should be distributed • One parent on EI and are distressed about his/her inability to afford message therapy for the
child. • Nutrition mentioned again here • Personal connections are where one parent got most of his/her information about support
services & resources. Only through serious treatment did the parents receive more information from social workers.
• Wants to know more more about prognosis.
! of !30 30
• Lot of information, but too scared and sad to remember. !!!Haematology Group !
Q8. People, Places and/or Service that parents wish they had known: !● ATM machines ● Parking passes ● Map/direction of clinic ● Cross matching for MBT ● Use of Hydroxyurea !!Q11. Supportive services that you wish you knew about during your visit to SickKids: !● Request refresher/reminder at 1 month and 3 month as there are too much to understand for their child’s diagnosis. ● ACOR list for parents with children with cancer (great support and resource for sharing/requesting info). ● Educational program while children are away from their school. ● The parking ● Process of treatment to be more effective interns of time, for frequent visitors to SickKids (waiting 2-3 hours for 45 mins procedure) ● Nearby hotels with special rate ● EI Caregiver Benefit ● Northern Health Travel Grant ● Employment Benefit ● Help in buying Medication ● Talk to other parents with similar circumstances to get a feeling of what lays ahead !!Q13. Programs and/or organizations that you wish you knew: !● Sickle Cell Association of Canada ● Medical information related to Thalassemia ● Add. info concerning Camp Ooch, Camp Trillium etc. at 3 months ● Internet access & Wi-Fi !Q16. Add. Comments: !● One binder with tabs for all the services etc. would be helpful as a reference at latter date. ● Important to put parents in contact with other parents whom have gone through the same route, this makes the experience more friendly.