Reperfusion Strategies for ST elevation MI. Tom P Stys, FACC, MD Medical Director Sanford...
40
Reperfusion Strategies for ST elevation MI. Tom P Stys, FACC, MD Medical Director Sanford Cardiology
-
Upload
noah-eagleton -
Category
Documents
-
view
214 -
download
0
Transcript of Reperfusion Strategies for ST elevation MI. Tom P Stys, FACC, MD Medical Director Sanford...

Reperfusion Strategies for ST elevation MI.
Tom P Stys, FACC, MDMedical Director
Sanford Cardiology

ACS and Rural Hospitals• 4897 community hospitals in the United States1
– 2900 are located in urban areas1
– 1997 are located in rural areas1
• Although primary PCI is often the preferred strategy for STEMI, only about 25% of US hospitals are capable of performing PCI2
• Non–PCI-capable institutions are often located in rural areas and face challenges related to their distance from PCI centers
• Almost 60% of US adults live in an area where a non–PCI-capable institution is their closest hospital2 – Guideline-based multidisciplinary care and coordinated transfer protocols are
important for best outcomes
1. American Hospital Association Statistics. Available at: www.aha.org/aha/resource-center/Statistics-and-Studies/fast-facts.html. Accessed May 23, 2010.
2. Nallamothu BK, et al. Circulation. 2006;113(9):1189-1195.

STEMI Chain of Survival

Time to Treatment Is Critical in STEMI
Onset of symptoms of
STEMI
9-1-1EMS
dispatch
EMS on-scene• Encourage 12-lead ECGs• Consider prehospital fibrinolytic if
capable and EMS-to-needle within 30 min
Total ischemic time: within 120 min
EMS Transport
GOALSPCI
capable
Not PCIcapable
Golden hr = 1st 60 min
Patient Prehospital fibrinolysisEMS-to-needlewithin 30 min
EMS transportEMS-to-balloon within 90 minPatient self-transport Hospital door-to-balloon within 90 min
Dispatch1 min
5 min
8 min
0.4 million discharges per year for STEMI in US
● Time to reperfusion is a critical determinant of the extent of myocardial damage and clinical outcomes in patients with STEMI
● Key factors in STEMI care are rapid, accurate diagnosis and keeping the encounter time to reperfusion as short as possible

The Thrombus in STEMISTEMI is generally caused by a completely occlusive fibrin-rich thrombus in a coronary artery
Results from stabilization by fibrin mesh of a platelet aggregate at site
of plaque rupture
*RBC = red blood cell.GP IIb-IIIa inhibitors are not indicated for STEMI.Van de Werf F. Thromb Haemost. 1997;78(1):210-213; White HD. Am J Cardiol. 1997;80(4A):2B-10B; Davies MJ. Heart. 2000;83(3):361-366.

Achieve Coronary Patency
• Initial Reperfusion Therapy - Defined as the initial strategy employed to restore blood flow to the occluded coronary artery
• 3 Major Options:• Pharmacological Reperfusion • PCI • Acute Surgical Reperfusion
Class I All patients should undergo rapid evaluation for reperfusion therapy & have a reperfusion strategy implemented promptly after contact with the medical system
Antman et al. JACC 2004;44:680.

Goals When Considering a Reperfusion Strategy
• Decrease amount of myocardial necrosis• Preserve LV function• Prevent major adverse cardiac events • Treat life threatening complications

Importance of EarlyReperfusion Therapy in STEMI
Outcomes Dependent Upon:• Time to treatment-TIME IS STILL MUSCLE• Early and full restoration in coronary blood flow• Sustained restoration of flow

Reperfusion Recommendations
- STEMI patients presenting to a hospital with PCI capability should be treated with primary PCI within 90 minutes of first medical contact.
I IIIIIa IIb
A
•STEMI patients presenting to a hospital without PCI capability and who cannot be transferred to a PCI center for intervention within 90 minutes of first medical contact should be treated with fibrinolytic therapy within 30 minutes of hospital presentation, unless contraindicated.
I IIIIIa IIb
B
ACC/AHA 2007 STEMI Focused UpdateCirculation 2007; on line, December 10.

Risk StratificationBased on initial
Evaluation, ECG, andCardiac markersSTEMI
Patient?YES NO
- Assess for reperfusion- Select & implement
reperfusion therapy- Directed medical
therapy
UA or NSTEMI- Evaluate for Invasive vs. conservative treatment- Directed medical therapy

Choices:Reperfusion Strategies for STEMI
Plan A: percutaneous coronary intervention (primary PCI)
-Mechanical means of restoring blood flow• Balloon angioplasty• Stents
- More effective- Lower bleeding risk- Available at only 25% of U.S. hospitals
• Treatment delaysPlan B: thrombolytics (fibrinolytics)
- Pharmacologic means of restoring blood flow •“Clot-busting” drugs
- Less effective- Greater bleeding risk- Widely available at U.S. hospitals

STEMI cardiac care• Determine preferred reperfusion strategy
Fibrinolysis preferred if: <3 hours from onset PCI not available/delayed
door to balloon > 90min door to balloon minus door
to needle > 1hr Door to needle goal <30min No contraindications
PCI preferred if: PCI available Door to balloon < 90min Door to balloon minus door to
needle < 1hr Fibrinolysis contraindications Late Presentation > 3 hr High risk STEMI
Killup 3 or higher STEMI dx in doubt

STEMI cardiac care
• Assessment- Time since onset of symptoms
90 min for PCI / 12 hours for fibrinolysis- Is this high risk STEMI?
- KILLIP classification- If higher risk may manage with more invasive rx
- Determine if fibrinolysis candidate- Meets criteria with no contraindications
- Determine if PCI candidate- Based on availability and time to balloon rx

Acute Phase Risk Stratification:Importance of LV dysfunction
Killip Classification % patients Mortality (%)
I No CHF 30-50 5
II Rales, S3, Pulmonary venous hypertension 33 15-20
III Pulmonary edema 15 40
IV Cardiogenic shock 10 80-100
Continuing Medical Implementation ….. .bridging the care gap

Fibrinolysis indications
• ST segment elevation >1mm in two contiguous leads• New LBBB• Symptoms consistent with ischemia• Symptom onset less than 12 hrs prior to presentation

Absolute contraindications for fibrinolysis therapy in patients with acute STEMI
• Any prior ICH• Known structural cerebral vascular lesion (e.g., AVM) • Known malignant intracranial neoplasm (primary or metastatic)• Ischemic stroke within 3 months EXCEPT acute ischemic stroke within 3 hours• Suspected aortic dissection• Active bleeding or bleeding diathesis (excluding menses)• Significant closed-head or facial trauma within 3 months

CONTRAINDICATIONS
It is estimated that 20-30% of patients ineligible for
thrombolytic therapy…

Which Lytic Agent?EFFICACY
• Benefit first demonstrated w/ streptokinase (GISSI-2 and ISIS-2 trials). ISIS-2 showed combination of ASA and streptokinase reduced mortality from 10.2% (placebo) to 7.2%.
• GUSTO-I: alteplase superior to streptokinase (although more expensive)• ASSENT-2 and GUSTO-III: newer agents like tenecteplase, reteplase, lanoteplase as effective as
alteplase but have significantly lower incidence of noncerebral bleeding complications and need for
transfusion.

Comparison of Approved Fibrinolytic Agents
Streptokinase Alteplase Reteplase Tenecteplase
• Dose 1.5 MU over Up to 100mg in 10U x 2 30-50mg
30-60 min 90 min (wt-based) each over 2 min based on weight• Bolus Admin. No No Yes
Yes• Antigenic Yes No
No No• Allergic React Yes No No
No• Systemic Marked Mild Moderate
Minimal Fibrinogen Depletion• ~90-min patency 50 75 75? 75 rates (%)• TIMI grade 3 flow, % 32 54 60 63
Adapted from Table 15, pg 53.Accessed on August 6, 2004http://www.acc.org/clinical/guidelines/stemi/index.pdf.

Assessment of response …
• Relief of symptoms• Maintenance or restoration of hemodynamic
and/or electrical stability• Reduction of at least 50% of initial ST segment
injury pattern on a follow-up EKG 60-90 min after initiation of therapy• Serial measurements of cardiac biomarkers

Long-term survival…
• Long-term benefit primarily seen in patients who achieved TIMI 3 flow w/ lytic administration. Vessel opening (TIMI 2 or 3) reported in 60-87% of patients receiving lytics,
but normalization (TIMI 3) in only 50-60% of arteries. Only TIMI 3 flow associated with
improved LV function and survival.***Note: TIMI 3 flow is achieved in ~90% of patients treated with primary PCI.

Time from Symptom Onset to TreatmentPredicts 1-year Mortality after Primary PCI
The relative risk of 1-year mortality increases by7.5% for each 30-minute delay
De Luca et al, Circulation 2004;109:1223-1225De Luca et al, Circulation 2004;109:1223-1225

2009 ACC/AHA STEMI/PCI Guidelines Focused Updates
Triage and Transfer for PCI (for STEMI)New Recommendation
B • It is reasonable to transfer high- risk patients who receive
fibrinolytic therapy as primary reperfusion therapy at a non–PCI-capable facility to a PCI-capable facility as soon as possible where PCI can be performed either when needed or as a pharmacoinvasive strategy

EFFECT OF DOOR-TO-BALLOON TIME ON MORTALITY IN PATIENTS WITH STEMI
8
7
6
5
4
3
2
1
0≤90 >90 - 120 >120 - 150 >150
In-h
ospi
tal M
orta
lity,
%
≤90 >90 - 120 >120 - 150 >150
Door-to-Balloon Time (min)
In-hospital mortality and door-to-balloon time; P for trend <.001.
Reproduced with permission from McNamara RL, et al. J Am Coll Cardiol. 2006;47(11):2180-2186.
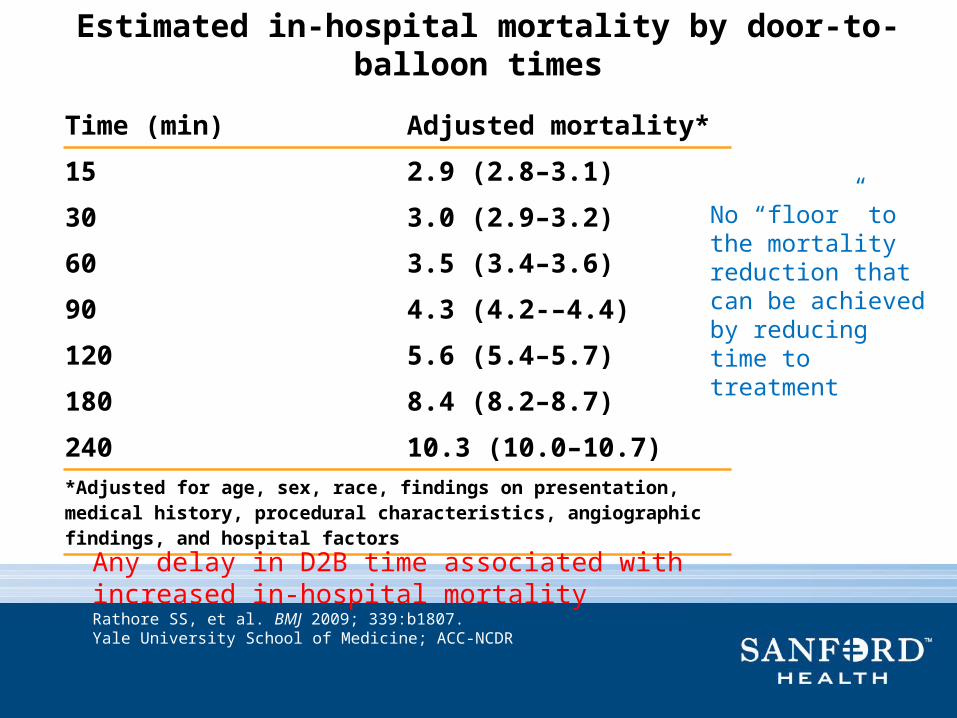
Estimated in-hospital mortality by door-to-balloon times
Time (min) Adjusted mortality*
15 2.9 (2.8–3.1)
30 3.0 (2.9–3.2)
60 3.5 (3.4–3.6)
90 4.3 (4.2-–4.4)
120 5.6 (5.4–5.7)
180 8.4 (8.2–8.7)
240 10.3 (10.0–10.7)*Adjusted for age, sex, race, findings on presentation, medical history, procedural characteristics, angiographic findings, and hospital factors
No “floor” to the mortality reduction that can be achieved by reducing time to treatment
Any delay in D2B time associated with increased in-hospital mortalityRathore SS, et al. BMJ 2009; 339:b1807.Yale University School of Medicine; ACC-NCDR

D2B: PCI Engineering
1. ED physician activates cath laba. Via Field Interpretationb. Via Referral Interpretationc. Via ED Interpretation
2. One call activates the cath lab3. Cath lab team ready in 20-30 minutes4. Prompt data feedback5. Senior management commitment6. Team-based approach

PCI after thrombolytics???
This issue remains unresolved…3 possible scenarios…*Facilitated PCI—lytic drug given prior to planned PCI in
attempt to achieve an open infarct-related artery before arrival of cath lab
*Adjunctive PCI—PCI performed within hours after thrombolysis
*Early elective PCI—PCI performed within a few days after thrombolysis

Comparing outcomes: PCI vs Lytics

The Golden Rule: Once a STEMI is Identified it Must Trigger a Clear Response
Downstream!
Rapid Recognition of STEMI on ECG will only improve the process IF Recognition leads to a concrete action occurring downstream
Recognition allows early Reperfusion… but does not guarantee it!

STEMI – Door-to-Balloon and Door-to-Needle Times
Cumulative 12-Month Data from ACTION Registry
ACTION DATA: January 1, 2007 – December 31. 2007 (n=19,523)DTB = 1st door to balloon for primary PCIDTN = Door to needle for lytics

ACTION Median Door-to-Balloon TimesFor Transfer In & Non-Transfer In Patients
123
236
62
103
Q1 07
120
223
60
102
Q2 07
116
215
57
Q3 07
113
212
57
95
Q4 07
Tim
e (
min
)
50
220210
60708090
110100
120130140150160170
200
180190
240230
96
403020
250
100
7979 7878 7575 7474
169
169 15
8158
151
151
156
156
Transfer in DTB Times Non-Transfer in DTB Times

Today: The 5 Essential Elements of STEMI System Optimization
R1 RelationshipsR2 RecognitionR3 ReperfusionR4 Real-time data collectionR5 Reassessment & refinement
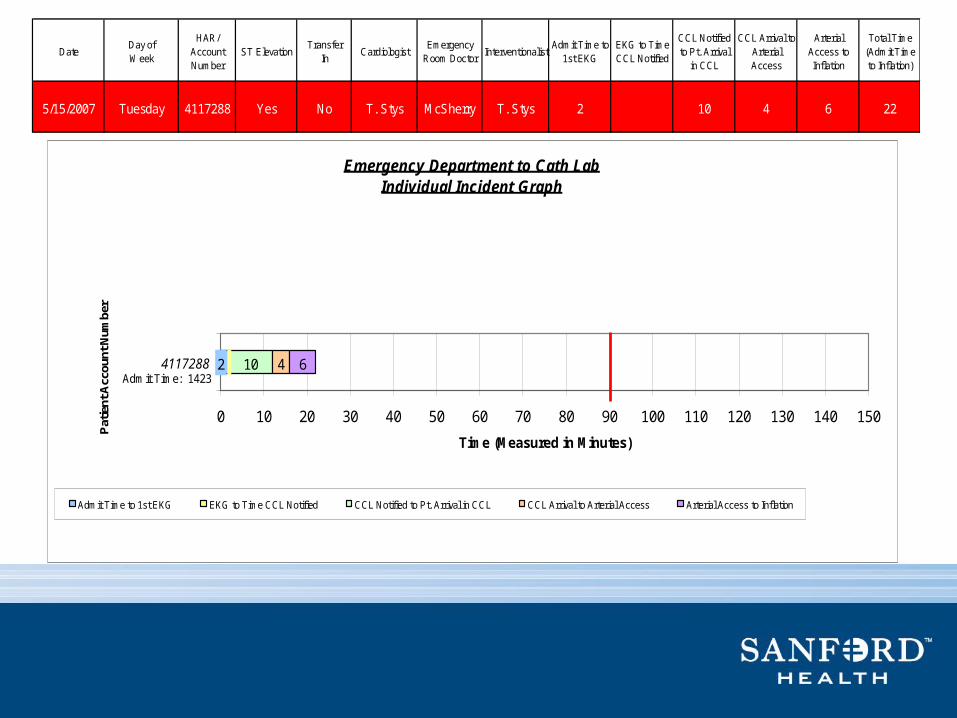
DateDay of Week
HAR/ Account Number
ST ElevationTransfer
InCardiologist
Emergency Room Doctor
InterventionalistAdmit Time to
1st EKGEKG to Time CCL Notified
CCL Notified to Pt. Arrival
in CCL
CCL Arrival to Arterial Access
Arterial Access to Inflation
Total Time (Admit Time to Inflation)
5/15/2007 Tuesday 4117288 Yes No T. Stys McSherry T. Stys 2 10 4 6 22
Emergency Department to Cath LabIndividual Incident Graph
10 4 62
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150
4117288
Pat
ient
Acc
ount
Num
ber
Time (Measured in Minutes)
Admit Time to 1st EKG EKG to Time CCL Notified CCL Notified to Pt. Arrival in CCL CCL Arrival to Arterial Access Arterial Access to Inflation
*Cardiologist Examined Patient
Admit Time: 1423
*

What we should do about STEMI Cardiogenic Shock• Emergency angiography and revascularisation: Primary PCI preferably
- All patients <75 years
- Selected patients ≥75 years
• On-table echo to rule out mechanical defects
• Stabilise the patient in the lab before revascularisation
- IABP
- Pressors if required (Norepinephrine/dopamine)
- Anaesthetic support
• Consider calling the surgeon for true surgical disease
• PCI culprit artery. Other vessels if shock persists
• Use abciximab for PCI
• Consider percutaneous LVAD if shock persists with IABP + multi-vessel revascularisation

Motor
Blood outlet
Blood Inlet
Cardiogenic Shock: Impella• Axial flow pump• Much simpler to use• Increases cardiac output & unloads LV• LP 2.5
- 12 F percutaneous approach; Maximum 2.5 L flow• LP 5.0
- 21 F surgical cut down; Maximum 5L flow• Cost: 3-5K
Pressure Lumen

STEMI 2012: “60 is the New 90”
• <30 Minutes : First Medical Contact (Recognition) to Thrombolytic administration
• <90 Minutes : First Medical Contact to on-site PCI (AHA/ACC recs) ?????
• <90 Minutes : First Medical Contact followed by inter-facility transfer to a PCI-capable facility
• ***BUT realistically <60 Minutes should be the goal for Contact/Recognition to Reperfusion @ a STEMI Receiving Facility (PCI Center)!

CARESS-in-AMI: Primary Outcome

Barriers to Timely Reperfusion• The patient
- Failure to promptly recognize symptoms
- Hesitation to seek medical attention
• Time to transport- Mandated delivery to the closest
hospital, regardless of PCI capabilities
- Long transport in rural areas• Decision process on arrival
- Clot-busting drugs vs. PCI- Off hours- Transfer to PCI facility
• Time to implement treatment strategy
- Procedural factors- Team assembly

1970 Cardiology invented EMS
Emergency!Gage & DeSoto
2010 EMS transforming Cardiology

Thank You!