RENAL DISEASE IN END STAGE LIVER DISEASE
32
Bon Secours Liver Institute of Virginia Bon Secours Medical Group Good Help to Those in Need ® RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA
Transcript of RENAL DISEASE IN END STAGE LIVER DISEASE

Bon Secours Liver Institute of Virginia Bon Secours Medical Group Good Help to Those in Need ®
RENAL DISEASE IN END STAGE LIVER DISEASE
Mitchell L Shiffman, MD Director
Liver Institute of Virginia Bon Secours Health System
Richmond and Newport News, VA

Bon Secours Liver Institute of Virginia
Mitchell L Shiffman, MD POTENTIAL CONFLICTS OF INTEREST
Company Roles Abbvie Advisor meetings, Grant support, Speaker Bayer Speaker Bristol Myers-Squibb Advisor meetings, grant support, Speaker Conatus Grant support CymaBay Grant support Daiichi Sankyo Speaker Exalenz Grant support Galectin Grant support Genfit Grant support Gilead Advisor meetings, Grant support, Speaker Intercept Advisor meetings, Grant support, Speaker, Immuron Grant support Merck Grant support, Advisor meetings, Speaker, NGMBio Grant support Novartis Grant support Optum Rx Consulting Salix Advisor meeting Shire Grant support

Copyright © 2015 The Royal College of Physicians and Surgeons of Canada. http://rcpsc.medical.org/canmeds. Reproduced with permission.”3
X Medical Expert (as Medical Experts, physicians integrate all of the CanMEDS Roles, applying medical knowledge, clinical skills, and professional values in their provision of high-quality and safe patient-centered care. Medical Expert is the central physician Role in the CanMEDS Framework and defines the physician’s clinical scope of practice.)
Communicator (as Communicators, physicians form relationships with patients and their families that facilitate the gathering and sharing of essential information for effective health care.)
Collaborator (as Collaborators, physicians work effectively with other health care professionals to provide safe, high-quality, patient-centred care.)
X Leader (as Leaders, physicians engage with others to contribute to a vision of a high-quality health care system and take responsibility for the delivery of excellent patient care through their activities as clinicians, administrators, scholars, or teachers.)
Health Advocate (as Health Advocates, physicians contribute their expertise and influence as they work with communities or patient populations to improve health. They work with those they serve to determine and understand needs, speak on behalf of others when required, and support the mobilization of resources to effect change.)
X Scholar (as Scholars, physicians demonstrate a lifelong commitment to excellence in practice through continuous learning and by teaching others, evaluating evidence, and contributing to scholarship.)
Professional (as Professionals, physicians are committed to the health and well-being of individual patients and society through ethical practice, high personal standards of behaviour, accountability to the profession and society, physician-led regulation, and maintenance of personal health.)
CanMEDS Roles Covered

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD CATEGORIES
• Renal disease develops in 20-25% of patients with cirrhosis Systemic disorder causing renal and liver disease A renal disease which is separate from the liver disease Renal disease that is caused by ESLD
• Overall survival is poor: 50% at 1 month 20% at 6 months
TA Gonwa, HM Wadei. Am J Kidney Dis 2013;62:1198–212. P Gines, RW Schrier. N Engl J Med 2009;361:1279–90.

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD CASE 1-SYSTEMIC DISORDER
66 year old male with chronic HCV and bridging fibrosis by LBX. He had a virologic response then relapse with PEGINF and RBV in 2010 and PEGINF-BOC-RBV in 2012. He now has increasing lethargy, swelling of the abdomen and lower extremities. EXAM: Sclera anicteric, obvious ascites, 3+ lower extremity edema. LABS: Sodium 141, creatinine 3.1 mg/dL, TBILI 1.0 mg/dL, albumin 1.5 g/dL, INR 1.0 UA: 4+ protein, 1+ blood CTP 8, MELD 20, US: Echogenic liver consistent with chronic liver disease. No liver mass. Normal PV blood flow. Mild ascites.

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD SYSTEMIC DISORDERS
Liver Disease Renal Disease Viruses Chronic HCV or HBV Glomerulonephritis Metabolic syndrome NASH Diabetic nephropathy Infiltrative disorders Amyloidosis
Myeloma Amylodosis Myeloma
Hypotension Shock liver ATN Drug toxicity Acute necrosis ATN
Bon Secours Liver Institute of Virginia
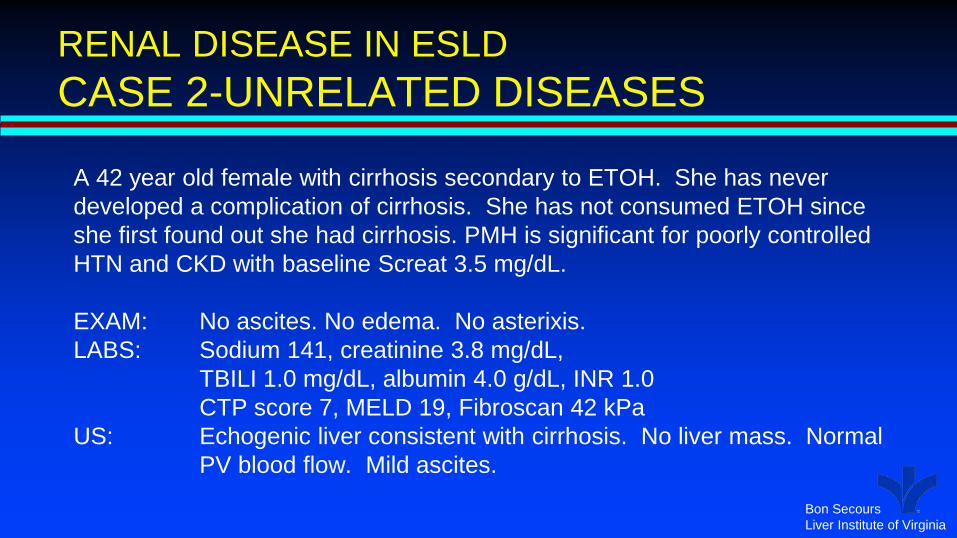
RENAL DISEASE IN ESLD CASE 2-UNRELATED DISEASES
A 42 year old female with cirrhosis secondary to ETOH. She has never developed a complication of cirrhosis. She has not consumed ETOH since she first found out she had cirrhosis. PMH is significant for poorly controlled HTN and CKD with baseline Screat 3.5 mg/dL. EXAM: No ascites. No edema. No asterixis. LABS: Sodium 141, creatinine 3.8 mg/dL, TBILI 1.0 mg/dL, albumin 4.0 g/dL, INR 1.0 CTP score 7, MELD 19, Fibroscan 42 kPa US: Echogenic liver consistent with cirrhosis. No liver mass. Normal
PV blood flow. Mild ascites.

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD BASIC PRINCIPLES
• The kidney is more susceptible to acute injury in patients with cirrhosis Dehydration Hypotension Medications
• Serum creatinine under estimates GFR in patients with cirrhosis Especially in patients with muscle wasting Screat of > 1.5 mg/dL is indicative of severe renal impairment
• Ascites precedes the development of CKD or HRS in patients with cirrhosis
• Kidney function declines with worsening liver disease and leads to excess mortality
NK Bozanich, PY Kwo Clin Liver Dis 2015: 19; 45-56.

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD IMPACT ON MELD SCORE
10
15
20
25
30
35
1.0 1.5 2.0 2.5 3.0 3.5 4.0
MEL
D S
CO
RE
Serum Creatinine (mg/dL)
140135130125
• For patients with moderate liver impairment: TBILI of 2.5 mg/dL INR 1.5
• Screatinine has the greatest impact on MELD score
• In general there is a 1 point increase in MELD for each 0.25 point increase in Screat
• Hyponatremia increases the MELD especially when this is low
Sodium

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD CASE 3-DRUG TOXICITY A 67 year old male with cirrhosis secondary to Primary HFE. A variceal bleeding 1 year ago was treated with banding. Mild ascites resolved with step 1 diuretics. Mild HE is well controlled with lactulose QD. Phlebotomy has reduced ferritin to under 50 ng/ml. He developed severe hip pain has been taking NSAIDS for the past 3 months. EXAM: No obvious ascites. 2+ lower extremity edema. LABS: Sodium 141, creatinine 2.4 mg/dL, TBILI 1.5 mg/dL, albumin 3.5 g/dL, INR 1.3 CTP 8, MELD 19 Urine NA 45 mEq US: Echogenic liver consistent with cirrhosis. No liver mass. Normal PV
blood flow. Mild ascites.

Bon Secours Liver Institute of Virginia
AKI AND CIRRHOSIS AVOID NEPHROTOXIC AGENTS
• Cirrhosis increases the susceptibility of the kidney to develop acute nephrotoxicity
• NSAIDs Inhibit renal prostaglandin production Decrease GFR
• Neomycin Portal hypertension increases intestinal mucosal permeability
• ACE inhibitors Lead to sodium retention
• IV contrast during imaging studies

Bon Secours Liver Institute of Virginia
NSAID INDUCED AKI WITH CIRRHOSIS PROGNOSIS
0
1
2
3
4
5
0 4 8 12 16 20
Seru
m C
reat
inin
e (m
g)
DAYS
Persistent
Transient
0
20
40
60
80
100
0 15 30 45 60 75 90
SUR
VIVA
L %
DAYS
C Eliara et al. J Hepatol 2015; 63:593-60.

Bon Secours Liver Institute of Virginia
CIRRHOSIS AND PORTAL HYPERTENSION IMPACT ON RENAL FUNCTION
Portal Hypertension
Decrease SVR
Increased Cardiac Output
Increase Renin-Angiotensin
Increase Vasopressin
Sodium retention
Increased epinephrine Sympathetic tone
Bacterial translocation
Inflammatory cytokines
Dilatation of splanchnic arteries
Decreased GFR
Water retention

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD ROLE OF ASCITES
0
20
40
60
80
100
0 2 4 6 8 10
% o
f Pat
ient
s
YEARS G D’Amico et al. J Hepatol 2006; 44:217-231.
• The MOST common complication of ESLD
• Leads to other complications: SBP Hyponatremia AKI CKD Hepatorenal syndrome

Bon Secours Liver Institute of Virginia
COMPLICATIONS OF ASCITES INCREASE MORTALITY
020406080
100
0 20 40 60 80 100
SUR
VIVA
L (%
)
MONTHS
NoneSBPRefractoryHypo-NaHRS
R Planas et al. Clin Gastroenerol Hepatol 2006; 1385-1394.

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD CASE 4-ACUTE AKI
• Most patients with cirrhosis and AKI do not have HRS
• Dehydration from Diuretics Bleeding
• Readily reversible: Volume expansion IV albumin to limit ascites Some normal saline Stop diuretics
0
1
2
3
4
5
0 4 8 12 16 20
Scre
atin
ine
(mg/
dL)
DAYS
IV albumin 25 gm Q6H

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD CASE 5–HYPONATREMIA
45 year female with cirrhosis secondary to NASH. She developed ascites for the first time 1 year ago. This initially resolved with step 1 diuretics. This is her 6th hospitalization in the past 3 months for ascites and AKI. During each hospitalization she is given 0.9% NS to correct hyponatremia and started back on diuretics. She has had 6 paracentesis removing 5-8 liters each. HE is treated with lactulose and rifaxamine. EXAM: 5’2”; 250 pounds, distended abdomen with obvious ascites, 4+
edema to the hips. Mild HE. No muscle wasting. LABS: Sodium 115, K 4.5, creatinine 2.1 mg/dL, TBILI 1.1 mg/dL, Albumin 1.8 g/dL, INR 1.3, CTP 10, MELD 26
Bon Secours Liver Institute of Virginia
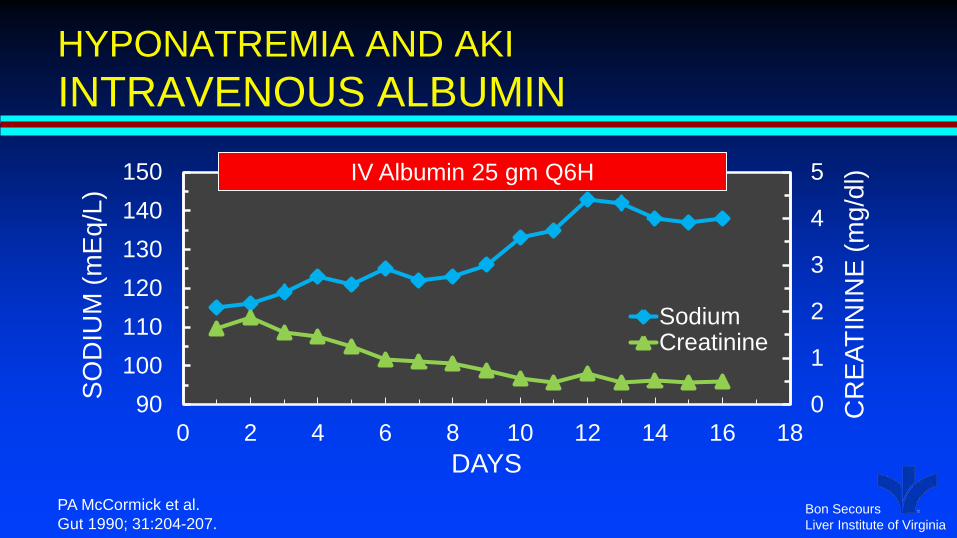
HYPONATREMIA AND AKI INTRAVENOUS ALBUMIN
0
1
2
3
4
5
90100110120130140150
0 2 4 6 8 10 12 14 16 18
CR
EATI
NIN
E (m
g/dl
)
SOD
IUM
(mEq
/L)
DAYS
SodiumCreatinine
PA McCormick et al. Gut 1990; 31:204-207.
IV Albumin 25 gm Q6H

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD ROLE OF IV ALBUMIN
• Improves vascular oncotic pressure Enhances movement of tissue fluid into vasculature Decreases edema Decreases ascites
• Expands vascular space Improves renal perfusion Enhances urine output Increases serum sodium Lowers Serum Creatinine
• Dose is 25 gm Q 6 H until Anasarca resolved Sodium back to normal Creatinine back to normal or plateaued Start diuretics once Sna > 130

Bon Secours Liver Institute of Virginia
SEVERE ASCITES AND ANASARCA IV ALBUMIN
• Start IV albumin 25 gms • Q6 hours • Large volume paracentesis on
admission • Use for several days until serum
sodium improved and creatinine is normal then add diuretics
• Continue IV albumin until serum sodium is normal
• Discharge on oral diuretics • Anasarca
0
5
10
15
20
25
30
60
70
80
90
100
110
120
A P 1 2 3 4 5 6 7
Cum
ulat
ive
UO
(L)
Wei
ght (
kg)
DAYS
Albumin 25gmQ6H Diuretics

Bon Secours Liver Institute of Virginia
IV ALBUMIN IN SBP
• Occurs in 30% with ascites • In hospital mortality 20% • Mortality and AKI reduced
significantly with IV albumin RCT, N=126 Cefotaxime + IV albumin Mean age 60 years ETOH cirrhosis 30% Mean CTP score 10 Culture positive 54% E Coli 21%
0
10
20
30
40
50
AKI In-Hospital 3 month%
of P
atie
nts
Mortality
CTMCTM+ALB
P Sort et al N Engl J Med 1999; 341:403-409.

Bon Secours Liver Institute of Virginia
IV ALBUMIN AS MAINTENANCE THERAPY
ALB SOC p Survival 77% 66% 0.028
OR Paracentesis 0.46 Refractory ascites 0.54 SBP 0.32 Non-SBP infections 0.70 AKI 0.50 HRS 0.38 HE Stage III-IV 0.48 Variceal bleeding 1.07
• Randomized controlled trial • SOC vs IV albumin • 40 mg BIW x 2 weeks then QW • N=431 • 33 Italian centers • Inclusion criteria: Ascites Spironolactone >200 mg/d Furosemide > 25 mg QD
P Caraceni et al. EASL 2017

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESLD HEPATORENAL SYNDROME
• Cirrhosis and ascites Serum creatinine > 1.5 mg/dL Urine sodium <10 mEq/L Urine output less than 500 cc/day Serum sodium < 130 mEq/L Absence of hematuria, proteinuria or intrinsic renal disease Absence of urinary tract obstruction No response to volume expansion with IV albumin
• Type 1: Cirrhosis with rapidly progressive renal failure • Type 2: Cirrhosis with subacute renal failure • HRS in the setting of ALF
F Salerno J Hepatol 2007; 47:729-731.

Bon Secours Liver Institute of Virginia
HEPATORENAL SYNDROME TYPE 1 AND TYPE 2
Type 1 Type 2 Rapid rise in Screat which doubles to >2.5 mg/dL within days - 2 weeks
Slow rise in Screat over weeks to months
Precipitating factor No precipitating factor Infection Bacterial infections
Fugal infections SIRS related to infections
Acute on chronic liver injury DILI including ETOH Acute hepatitis Shock liver
Renal hypoperfusion Sepsis with hypotension Variceal bleeding
Bon Secours Liver Institute of Virginia
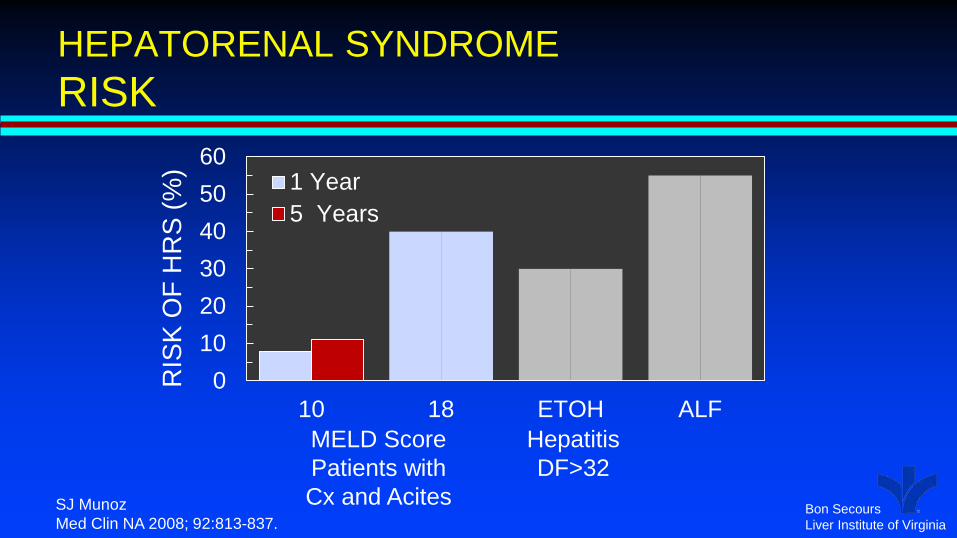
HEPATORENAL SYNDROME RISK
0102030405060
10 18 ETOH ALF
RIS
K O
F H
RS
(%) 1 Year
5 Years
MELD Score Patients with Cx and Acites
Hepatitis DF>32
SJ Munoz Med Clin NA 2008; 92:813-837.

Bon Secours Liver Institute of Virginia
HEPATORENAL SYNDROME SURVIVAL
0
20
40
60
80
100
0 100 200 300 400 500 600
SUR
VIVA
L (%
)
DAYS
Type 1Type 2No HRS
V Arroyo et al. J Hepatol. 2007; 935-946.

Bon Secours Liver Institute of Virginia
TREATMENT OF HRS MIDODRINE+OCTREOTIDE
0
50
100
0 4 8 12 0 4 8 12
C Skagen et al. J Clin Gastroenterol 2009; 43:680-685.
SUR
VIVA
L (%
)
WEEKS WEEKS
-505
1015202530
HRS1 HRS2
Cha
nge
in C
rCl M+OCT+ALB
Control
HRS Type 1 N=102
HRS Type 2 N=60

Bon Secours Liver Institute of Virginia
TREATEMENT OF HRS TERLIPRESSIN
0
50
100
0 4 8 12 0 4 8 12
M Cavallin et al. Hepatology 2015; 62:567-574.
SUR
VIVA
L (%
)
WEEKS WEEKS
020406080
100
TERLI M+OCT
Res
pons
e (%
) PartialComplete
Terlipressin+ALB N=27
M+OCT+ALB N=22
Bon Secours Liver Institute of Virginia
PORTAL HYPERTENSION BETA-BLOCKERS
• A primary treatment for patients with portal hypertension • Reduces risk of first variceal bleeding • Reduces risk of rebleeding from esophageal varices • Reduces bleeding in severe portal gastropathy • This does not mean that all patients with cirrhosis should be taking
beta-blockers Effective in patients with larger varices Does not prevent varices from appearing or growing Beta-blockers have adverse events May lead to AKI and increase mortality in patients with ascites

Bon Secours Liver Institute of Virginia
BETA-BLOCKERS IMPACT OF ASCITES
0
20
40
60
80
100
0 6 12 18 24 30 36
SUR
VIVA
L (%
)
MONTHS
NoYes
T Serste et al. Hepatology 2010; 52:1017-22.
Beta-Blockers

Bon Secours Liver Institute of Virginia
BETA-BLOCKERS IMPACT OF SBP
Use of beta-blockers significantly increased the risk of AKI and HRS in patients who developed SBP RCT, N=602 Mean age 57 years ETOH cirrhosis 55% Mean MELD 17 Child class C 50% 90 day mortality with AKI in
patients on beta-blockers and h/o SBP is 80%
0
10
20
30
40
50
AKI HRS%
of P
atie
nts
BBNo BB
M Mandorfer et al Gastroenterol 2014; 146:1680-1690.

Bon Secours Liver Institute of Virginia
RENAL DISEASE IN ESRD SUMMARY
• Not all renal dysfunction in cirrhosis is HRS • Avoid nephrotoxic agents in patients with cirrhosis • IV albumin is essential for treating the complications of renal
disease in ESLD Hyponatremia AKI Anasarca SBP to reduce risk of HRS Adjunct to treatment of HRS
• Propranolol should not be used in patients with ascites