
Discharge planning – reducing admissions/re- admissions Jo Clarke, CPPE tutor 1.

Reducing emergency admissions:
are we on the right track?
Martin Roland
Professor of Health Services Research
University of Cambridge


What not to do …….. and what to do
• What not to do: five common misconceptions
about emergency admissions
• What to do

Five common misconceptions
• Overestimating the importance of frequent
fliers
• Forgetting about regression to the mean
• Assuming interventions are beneficial
• Ignoring supply induced demand
• Forgetting about random variation

What not to do …….. and what to do
1. Overestimating the importance of
‘frequent fliers’
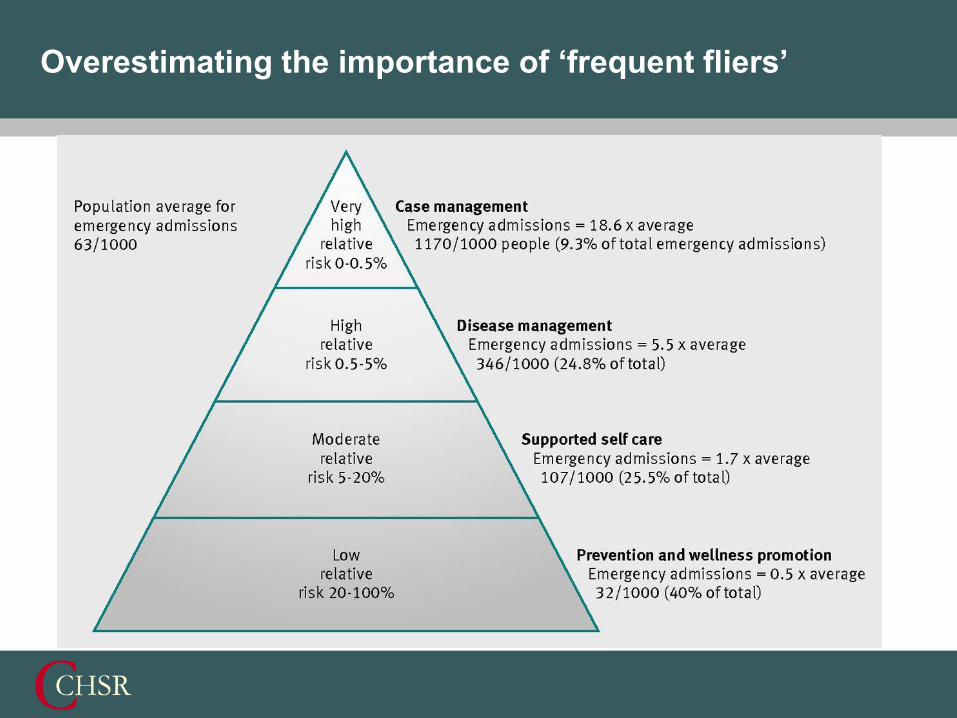
Overestimating the importance of ‘frequent fliers’

Percentage reduction in admissions in each risk group required to meet
targets for reducing emergency admissions
Target overall
reduction (%):
% reduction required in risk group
Very high risk
(0.5% of
population)
High risk (0.5-
5% of
population)
Moderate risk
(6-20% of
population)
Low risk (80%
of population)
1 10.8 4.0 3.9 2.5
2 21.5 8.1 7.8 5.0
3 32.3 12.1 11.8 7.5
4 43.0 16.2 15.7 10.0
5 53.8 20.2 19.6 12.5
10 107.5 40.4 39.2 25.0
What not to do …….. and what to do
2. Forgetting about regression to the mean

Forgetting about regression to the mean
Years 1 2 3 4 5 6
Roland et al. BMJ 2005; 330: 289

What not to do …….. and what to do
3. Assuming all interventions are beneficial
English Integrated Care Pilots (2009-2011):
Evaluation of case management interventions

English Integrated Care Pilots (2009-2011):
Evaluation of case management interventions
Aims included
• Reduced emergency admissions
• Better co-ordinated care
• Greater patient involvement of patients in decisions about their
care

English Integrated Care Pilots (2009-2011):
Evaluation of case management interventions
• Staff thought care had improved
• Patients said they were less likely to be able to see a doctor of
nurse of their choice and felt less involved in decisions about their
care
• Emergency admissions increased by 9%
• Small net reduction in costs (reduced elective admissions and
outpatient referrals)
Roland et al. International Journal of Integrated Care 2012, 12: 24 July
What not to do …….. and what to do
3. Ignoring supply induced demand
• NHS Direct
• NHS walk-in centres
• ‘New workers’ of many sorts…

It’s much easier to improve quality than reduce cost
% of studies with
a positive
outcome for
health
% of studies with
positive outcome
for patient
experience
% of studies
which showed
reduction in cost
55.4% 45.2% 17.9%
Powell Davies et al Med J Aust 2008; 188 (8): S65-S68
Systematic review of interventions to improve coordination in healthcare

“A bad day”
Forgetting about random variation due to chance

Variation due to chance (more correctly a Poisson
distribution)
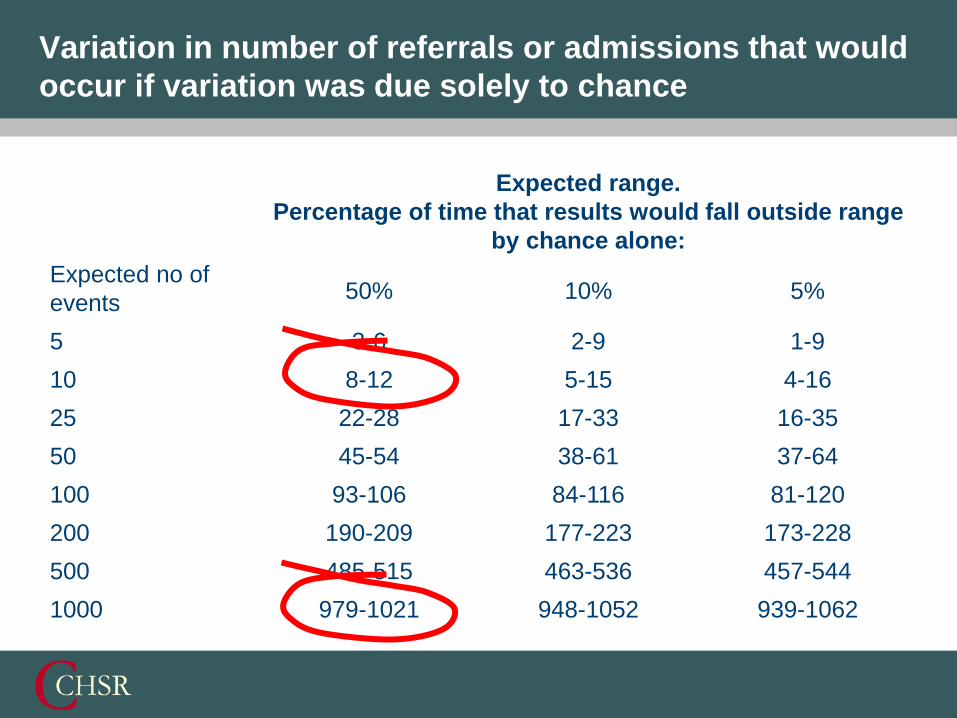
Variation in number of referrals or admissions that would
occur if variation was due solely to chance
Expected no of
events
Expected range.
Percentage of time that results would fall outside range
by chance alone:
50% 10% 5%
5 3-6 2-9 1-9
10 8-12 5-15 4-16
25 22-28 17-33 16-35
50 45-54 38-61 37-64
100 93-106 84-116 81-120
200 190-209 177-223 173-228
500 485-515 463-536 457-544
1000 979-1021 948-1052 939-1062

0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
45.00
Pete
rsfield
, C
am
bri
dge
Over
Wate
rbeach
Ma
ple
Surg
ery
, B
ar
Hill
Hea
lth
…
Tru
mp
ingto
n S
t, C
am
bri
dge
Ha
rsto
n
Ca
mbo
urn
e
Co
tten
ham
Lin
ton
Wood
lands S
urg
ery
, C
am
bri
dge
Will
ingh
am
Ca
mbo
urn
e
Que
en E
dith's
, C
am
bri
dge
Firs H
ouse, H
isto
n
Sw
avesey
East B
arn
well,
Cam
brid
ge
Ch
err
y H
into
n M
ed C
entr
e
Shelford
Le
nsfie
ld R
oa
d, C
am
bri
dge
Milt
on
Bottis
ham
Bridg
e S
t, C
am
bri
dge
Co
mbe
rton
28
1 M
ill R
oad,
Cam
brid
ge
Nu
ffie
ld R
oa
d, C
am
bri
dge
Saw
sto
n
York
St, C
am
bridg
e
Ne
wnha
m W
alk
, C
am
brid
ge
Co
rnfo
rd H
ouse,
Cherr
y H
into
n
Re
d H
ouse, C
am
bri
dge
Bourn
Hu
ntingd
on R
oad
, C
am
brid
ge
Arb
ury
Road
, C
am
bri
dge
Ca
mbri
dge
Access S
urg
ery
BA
RL
EY
SU
RG
ER
Y
RO
YS
IA S
UR
GE
RY
TH
E H
EA
LT
H C
EN
TR
E P
RA
CT
ICE
Rate
per
1,0
00 w
eig
hte
d p
op
ula
tio
n
All practices A&E rates per 1,000 weighted population compared to Greater Cambridge rate, Apr-May 11/12-12/13
All Practices 2011/2012 All Practices 2012/2013 Greater Camb 2012/2013 Series4
Off the Scale

What not to do …….. and what to do
• What not to do: five common misconceptions
about emergency admissions
• What to do

• Don’t assume that reductions in admissions in a high
risk group are due to your intervention - evaluate your
intervention against changes in overall patterns of
admission or using a control group

• Don’t assume there is a correct level of admission or
referral to hospital - clinical audit makes numbers
meaningful and should be used to identify where there
are problems in care

• Don’t assume that fewer admissions or referrals are
necessarily better - doctors with low rates of specialist
use may be a danger to their patients, just as high
referrers may be wasting resources. Use clinical audit
to bring meaning to crude rates of referral or admission
• Be cautious about using data for short time periods or
referrals to single specialties - random fluctuations may
account for much of the apparent variation in provider
performance when numbers are small. Use the table in
the BMJ paper to assess how much variation might be
due to chance
• Remind everyone who will listen that change is usually
slower than people expect (or at least hope for)

• Choose interventions that are evidence based – e.g.
from systematic reviews (Purdy et al 2012)
• However, bear in mind that context is important.
Carefully shaping the way an intervention is introduced
may increase its effectiveness, and don’t forget that
most changes can have unexpected consequences too.
Purdy et al 2012. www.bristol.ac.uk/primaryhealthcare/docs/projects/unplannedadmissions.pdf

What do systematic reviews tell us?
Intervention Effect
Case management Overall no effect except for heart failure
Specialist clinics Overall no effect except for heart failure
Care pathways and guidelines No effect, but limited evidence
Medication review No effect, but limited evidence
Education and self management Weak evidence for heart failure
Exercise and rehabilitation Effective in COPD
Telemedicine Possible effect on heart disease, diabetes,
hypertension and older people
Hospital at home Increased readmissions
Purdy et al 2012.
www.bristol.ac.uk/primaryhealthcare/docs/projects/unplannedadmissions.pdf

Patient recognises a problem
Patient arrives in A&E
GP surgery
Out of hours centre
Patient needs admission
Patient admitted
Patient doesn’t need admission
Availability of appointments
Opening hours
Continuity of care
Triage expertise
Triage expertise
Community support
Transport
‘Too late’
Patient behaviour

www.cchsr.iph.cam.ac.uk
www.cchsr.iph.cam.ac.uk/slides
twitter.com/cchsr


















