
REACH on Tour Lake County - REACH Air Medical...
39
Transcript of REACH on Tour Lake County - REACH Air Medical...


!
REACH on Tour Lake County April 16, 2015
AGENDA 12:30 PM - 1:00 PM Check-in, Registration and lunch provided
!1:00 PM - 1:05 PM Welcome and Introductions !1:05 PM - 2:05 PM Donna Stephenson, RRT, REACH Flight Respiratory Therapist Pediatric Respiratory Distress: Back to Basics !2:05 PM – 2:10 PM Break !2:10 PM - 3:25 PM JoAnne Natale, MD, PhD Medical Director, Pediatric ICU, UC Davis Medical Center Pediatric Emergency Scenarios !3:25 PM - 3:30 PM Break !3:30 PM - 4:25 PM Diana Priego, RN, REACH Flight Nurse Special Care Pediatrics, Medical Assist Devices !4:25 PM – 4:30 PM Break !4:30 PM – 5:00 PM Jeff Cress, LP, CCEMT-P, General Manager REACH Air Medical Services Tranexamic Acid: An Old Dog with New Tricks 5:00 PM Closing wrap up and evaluation forms Dessert and coffee provided
!CE certificates will be emailed to you within two weeks of the conference.
If you have any questions, please contact Annette Arnold at (707) 303-3644 or Annette_Arnold @REACHair.com

Pediatric Respiratory Distress: Back to Basics
Donna Stephenson, RRT Flight Respiratory Therapist
REACH Air Medical Services

Pediatric Respiratory Distress
Back To BasicsREACH Air Medical Services
Donna Stephenson, RRT
Objectives Review key points: !! Pediatric anatomy & physiology contributors to respiratory
distress ! Recognizing respiratory distress vs. failure ! Gas exchange ! Pearls of airway management ! Learn one thing !
!!!!!!!!
!! Majority of arrests occur <1 year of age
Data Hasn’t Changed…
1° RespiratoryShock1° Cardiac

!
PROMPT RECOGNITION !
ANTICIPATE RAPID DECOMPENSATION PREPARED TO MANAGE AIRWAY …and treat aggressively
! Smaller airways = Increased resistance ! Chest wall more compliant = Lower FRC (reserve) ! Increased metabolic and 02 demands → 02 consumption 2x adults! ! Lower FRC + increased 02 consumption = minimal safe apnea time and rapid desats ! Inadequate compensatory mechanism → Alveolar minute ventilation (VE) dependent on increased RR with little control of Vt ! Lack of muscle fiber development = fatigue easily
Factors Exacerbating Rapid Compromise
! Amount of air left in alveoli at end expiration ! Prevents airway/alveolar collapse ! Physiological PEEP ! Balloon analogy ! Intrapulmonary 02 reserve FRC = Alveolar recruitment = real estate for gas exchange = oxygenation
! Decreased in infants & young children resulting in more precipitous decline in oxygen saturation during hypoventilation and apneic periods
Elaborating on Functional Residual Capacity

!!!!!!!!! If radius is halved = resistance increases 16x
Did Someone Say Resistance?
Common Causes: Respiratory Distress
Keep cardiac and sepsis on your your radar !!!
!! Croup ! Pneumonia ! RSV /Bronchiolitis ! Asthma / RAD ! FBO !
Emergent ! Epiglottitis ! Bacterial Tracheitis ! Tension pneumothorax ! Complete upper airway obstruction

VENTILATION EtC02
PERFUSION IV?
Bolus?
OXYGENATION >94 %
! Name of the game ! Requires diffusion across alveolar membrane → Must have adequate V/Q match !
! Fi02 ! FRC = PEEP !
Can’t STRESS enough- infants will desaturate rapidly during RSI and intubation PEEP, preoxygenation VERY important
Oxygenation
! Alveolar Minute Ventilation (VE) = C02 Elimination VE = RR x Vt !! Requires PATENT pathway out→ Exhalation ! Requires TIME to escape !
! Suction → Clear obstruction ! PEEP / CPAP → prevent airway / alveolar collapse ! Meds → Bronchodilate
Ventilation

!! Tachypnea* ! Grunting ! Flaring ! Retracting ! Positioning ! Irritability, anxiety ! Airway sounds
!! LOC / mentation is KEY ! Toxic appearance ! Head bobbing ! Retractions in multiple muscle groups=
significant hypoxia ! Desats despite 02 ! WOB appears to be decreasing- tired
Distress vs. Failure
! Still OK on supportive path ! Non invasive → Initiate EARLY ! Advanced airway time
We must Decide
! Hop on it EARLY ! !
! CPAP, BiPAP, Bubble CPAP, HFNC… ! Played very successful role in avoiding advanced airways for many years !
! NCPAP standard of care infant population ! BiPAP used frequently in pedi world with great results in asthmatics
Non Invasive Support

AGE (years) WEIGHT (Kg) ETT SIZE
1 10 4.0
5 20 5.0
8 30 6.0
1- 5- 8 RULE
! Whenever possible go for the cuff ! Best of both worlds ! Sicker the lungs the more critical this decision becomes
• High PEEP and or Fi02 • Decreased pulmonary compliance • Risk of aspiration !
Cuff pressures: • Ability to measure in hospital and transport environment • Tools • Education
Cuff or No Cuff
2 Choices !! 3 x ETT size = lip line marker • Most common • Relies heavily on proper ETT size • Kids with developmental barriers may not always follow the Broslow rule
!! 12 + ½ age in years = lip line marker • More reliable formula based on studies
!
How Low Do You Go?

!5 year old What size ETT ? Depth ? !12 + 2.5 = 14.5 cm 3 x ETT =
!1 year old What size ETT ? Depth ? !!12 + 0.5 = 12.5 cm 3 x ETT =
Examples
A = AIR LEAK !
! Evaluate ENTIRE airway- not just the “D” ▪ Right size ▪ Right place ▪ Right depth ▪ LEAK ???? → Manageable or not?
“A” in DOPE ????
!!!
Do We Have Time???
Case Study

Questions….

Pediatric Emergency Scenarios
JoAnne Natale, MD, PhD Medical Director, Pediatric ICU
UC Davis Medical Center

JoAnne Natale, MD, PhD Pediatric Critical Care
Pediatric Emergency Scenarios
Objectives
▪ Using physical exam findings, differentiate between upper and lower airway obstruction in infants and children ▪ List treatments of upper and lower obstruction ▪ Practice a systematic approach to the child with
respiratory distress
Pediatric Emergency Scenarios
Systematic Approach to Child with Respiratory Distress
© American Heart Association 2011

Pediatric Emergency Scenarios
Systematic Approach to Child with Respiratory DistressEVALUATE
Clinical Assessment Brief DescriptionPrimary assessment Rapid ABCDE, includes vital signsSecondary assessment Focused history and physical
examDiagnostic tests Lab, xraysAirway
Breathing Circulation Disability Exposure
Pediatric Emergency Scenarios
Abnormal respiratory effort
Sign DefinitionNasal flaring Dilation of nostrils with each
inhalationRetractions Inward movement of chest wall,
neck, or sternum during inhalationHead bobbing Use of neck muscles to breatheSeesaw respirations
Chest retraction and abdominal expansion during inspiration
Pediatric Emergency Scenarios
Retractions

Pediatric Emergency Scenarios
Evaluate
Pediatric Emergency Scenarios
Abnormal lung and airway sounds
Sign Characteristic Significance Causes
Stridor Coarse, higher pitched, heard on inspiration
Upper airway obstruction
FBO, croup, laryngomalacia, upper airway edema, cyst
Grunting Short, low pitched, heard on expiration
Lung tissue disease
Pneumonia, ARDS
Wheezing Whistling sound, heard on expiration
Lower airway obstruction
Asthma, bronchiolitis
Crackles Sharp, heard on inspiration
Alveolar fluid Heart failure, pulmonary edema
Pediatric Emergency Scenarios
Abnormal respiratory rate
Definition Cause
Tachypnea Faster than RR for age Respiratory disease, metabolic acidosis
Bradypnea Slower than RR for age Respiratory muscle fatigue, hypothermia, medication
Apnea Cessation of breathing for > 20 sec. or < 20 sec if bradycardia, cyanosis or pallor
Extreme respiratory muscle fatigue, medication, infection (e.g. pertussis, RSV)

Pediatric Emergency Scenarios
Systematic Approach to Child with Respiratory DistressIDENTIFY
TypeUpper airway obstructionLower airway obstructionLung tissue diseaseDisordered control of breathing
Pediatric Emergency Scenarios
Systematic Approach to Child with Respiratory DistressINTERVENE
Based on respiratory problem, intervene with appropriate actionUpper airway obstruction Jaw thrust, SC epi, racemic epi,
steroidsLower airway obstruction Oxygen, Albuterol, racemic epi,
steroidsLung tissue disease Oxygen, antibiotics, fluidsDisordered control of breathing Bag valve mask ventilation,
reversal agents
Pediatric Emergency Scenarios
Case Scenario 1
▪ EMS called to home of 2 mo old infant, born full term, after 2 episodes of apnea and cyanosis. Cough, felt warm to touch, nasal congestion, poor po intake x 1-2 days. ▪ Exam: – HR 170, RR 66, SaO2 99%, Temp 37.5, 93/55
Pediatric Emergency Scenarios
Case Scenario 1
https://www.youtube.com/watch?v=lIE_UElOk3c
Start 2:04, End 3:12, + sound
Pediatric Emergency Scenarios
Case Scenario 1
Which best describes the primary ABCD assessment for this infant? !
A. A: patent. B: audible high pitched, expiratory wheeze, severe distress, tachypnea, subcostal retractions. C: pale. D: minimal interaction.
B. A: upper airway obstruction. B. stridor, tachypnea, subcostal retractions. C. pink. D. alert.
C. A. patient. B. stridor. C. cyanosis. D. alert. E. Looks well.
Pediatric Emergency Scenarios
Case Scenario 1
Based on this evaluation, what additional interventions should be given? !A. nebulized albuterol B. nebulized racemic epinephrine C. suction nose and oropharynx D. all of the above

Pediatric Emergency Scenarios
Case Scenario 1
https://www.youtube.com/watch?v=lIE_UElOk3c
Start 3:13, End 3:47, + sound
Pediatric Emergency Scenarios
Case Scenario 1: Diagnostic tests
Glucose 111 Venous blood gas pH 7.28 pCO2 57 bicarb 27 base excess -1
Pediatric Emergency Scenarios
Case Scenario 2
A 5 mo boy is brought to the ED with runny nose, cough and fever over the past 2 days. Temp 39, HR 120, RR 34, sats 94%. !
https://youtu.be/-4OhWQ8Ppko

Pediatric Emergency Scenarios
Case Scenario 2
What is the most likely cause of his stridor? A. Foreign body
B. Subglottic edema
C. Epiglottitis
D. Vascular ring
Pediatric Emergency Scenarios
Case Scenario 2
Which of the following treatments is (are) indicated?
A. humidified oxygen
B. epinephrine nebulized
C. dexamethasone
D. all of the above
Pediatric Emergency Scenarios
Case Scenario 2

Pediatric Emergency Scenarios
Case Scenario 33 yr old fully immunized boy presents to the ED with acute SOB. He had been playing with his older sister’s “lite brite” while munching on cheerios. He suddenly has a bout of coughing. He is distressed, crying and coughing intermittently. He has no stridor, RR 40, intercostal and substernal rtxs. Mild wheeze worse on the right. Sats 94% RA. CXR shown on next slide.
Pediatric Emergency Scenarios
Case Scenario 3
Pediatric Emergency Scenarios
Case Scenario 3
What is the most likely cause of his stridor? A. Foreign body
B. Subglottic edema
C. Epiglottitis
D. Vascular ring

Pediatric Emergency Scenarios
Case scenario 3True of False?
▪Most aspirated FBs will be lodged in one of the mainstem bronchi. ▪Most airway FBs in children will be visible on plain
CXR. ▪Wheezing is uncommon in children with aspirated
FBs.
Pediatric Emergency Scenarios
Case Scenario 3
▪ Steroids may be given to prevent inflammation of the airway. ▪ Bronchoscopic removal of FB is urgently indicated
in this child. ▪ If the child develops complete airway obstruction
in the ED, the child should be immediately be taken for bronch.
Pediatric Emergency Scenarios
Case Scenario 4
!https://www.youtube.com/watch?
v=EK8nzKzdnIM Start 0:14. End 0:52, mute
A 15 yo boy with previous history of asthma presents to ED with severe respiratory distress. !

Pediatric Emergency Scenarios
Case Scenario 4
Pediatric Emergency Scenarios
Case Scenario 4
▪ Given his current presentation: does this child need to be intubated and mechanically ventilated? !▪ Discuss indications for intubation/mechanical
ventilation in the child with severe status asthmaticus.
Pediatric Emergency Scenarios
Case Scenario 4
In addition to administration of continuously nebulized beta-agonist which of the following should be given next?
!A. Intravenous corticosteroid
B. Intravenous fluid bolus
C. Intravenous magnesium sulfate
D. A, B and C
E. A and C only

Pediatric Emergency Scenarios
Systematic Approach to Child with Respiratory Distress
© American Heart Association 2011
Thank you!
JoAnne Natale, MD, PhD [email protected]
1-800-UCD-4KIDs

Special Care Pediatrics: Medical Assist Devices
Diana Priego, RN Flight Nurse
REACH Air Medical Services

Special Care Pediatrics Medical Assist Devices
Outreach Education 2015
Objectives
• After this lecture the attendee will be able to: – Describe an overall approach to evaluating
children with special healthcare needs – Discuss field and nursing interventions for
children with shunts – Verbalize anatomy of a tracheostomy and methods
for delivering O2 and suctioning them. – Identify and state accessing methods for tunneled
central venous catheters. – State different types and purposes of enteral
feeding tubes.

Seeing More Special Needs?
• 30,000 annually permanently disabled
• 12 million estimated • Advances in overall
healthcare technology • Improved survivability
Interesting Information
• Many children have more than one special healthcare need.
• Children with special healthcare needs are over three times as likely as other children to require emergent ICU admission.
• Technology-dependent children are over 300 times more likely to require emergent ICU admission than other children with special health needs.
Schif, Jeff. Children with Special Health Needs in the EMS System. Minnesota Department of Health. Spring 2002
General Assessment
• Require the same priorities as other children – Clear airway – Adequate ventilation – Adequate oxygenation – Adequate cardiac output !
• Understanding of Special Needs/Equipment

Assessment should be based on the child’s own baseline vital signs and physical or mental abilities.
General Assessment
Meeting the Challenge: Improving Emergency Medical Care for Children with Special Healthcare Needs. Copyright: Arizona Emergency Research Center; 1999 Arizona Board of Regents on behalf of the University
of Arizona
General Assessment• If developmentally delayed, ascertain what the
child’s normal cognitive level is. • How does this child communicate? • Identify communication barriers. • Do not assume that a non-verbal child cannot
hear or understand your instructions.
General Assessment
• Parents or caregivers are the best resources for helping you communicate with and ascertain information about the child. !
• Additional resources – Emergency Information Form – Family Binder is common – Your notes or references
• Side brains • Palms/Blackberry/i-phone • Cheat sheets

Technology – Assisted Children• Growing sub-population of
children. • Secondary to increased
survival rates from critical injuries or disease; advances in medical technology; and more support services, decreasing hospital stay.
Technology-Assisted Children• CSF Shunts • Tracheostomy • Central Venous Catheters • Feeding Tubes • Home Ventilators • BiPAP / CPAP devices • Pacemakers • Vagus Nerve Stimulator
Hydrocephalus
Hydrocephalus is an excessive accumulation of CSF within the ventricles of the brain, resulting from interference with normal
circulation or absorption of the fluid.

CSF Shunts• A silastic tube that drains CSF
from the brain’s ventricular system into some other part of the body (peritoneum, right atrium) where it can be absorbed .
• A shunt usually remains in place for life.
• Children are at life-long risk for developing shunt failure and needing further surgery.
CSF Shunt Malfunctions
• Early Signs – Altered level of
consciousness – Headache – Nausea and vomiting – Amnesia – Changes in speech,
drowsiness, agitation, restlessness, and judgment
• Late Signs – Dilated, non-reactive, or
unequal pressures – Cushing’s reflex – Unresponsiveness – Abnormal posturing
patterns
Watch for signs of increasing intracranial pressure
Treatment• Raise the head of the bed 30 degrees • Assess and support the ABCs
– Support a patent airway – Provide 100% O2 by NRM – Provide assisted ventilation, if needed
• Establish vascular access • Anticonvulsants (if needed) • ICP management • Assess for shunt malfunction

One More Thing…Infections• Fever • May be life-threatening for the immuno-suppressed
child – Cancer, Chemotherapy, Organ Transplant,
Malnutrition, HIV infection • Bacterial Sepsis common
Tracheostomies• Placed due to upper airway
obstructions, lower airway obstructions, lung disease or neurologic conditions.
• May be used in conjunction with supplemental O2, positive pressure ventilation and suctioning.
Types of Tracheostomies
• Cuffed and uncuffed. Some require inner cannula changes daily.
• Most trach. sizes are visible printed on base of trach. • Secured around the child’s neck with ties or
commercial Velcro securement collar.

Suctioning
• Suction catheter size is chosen by multiplying size of trach x2.
eg. A 3.5 Neo Shiley would use a 6 French suction catheter.
• Depth average is 5-6cm for children, • Avoid suctioning beyond the end of the trach as this
can cause airway trauma. • Suctioning in the healthcare setting should be sterile to avoid acquired bacteria and infections.
Troubleshooting
• Use DOPE • D – Displacement O – Obstruction P – Pneumothorax E - Equipment • Unscheduled, emergency trach changes are
recommended for respiratory distress that does not respond promptly to suction, oxygen, and/or PPV.
Changing a trach
• New trachs may have a stylette in the cannula that needs to be removed after insertion.
• If you cannot put the same size tube back in, try the next size smaller.
Changing a Trach
• If you cannot replace the tube at all and the patient has a patent (open) airway, use a resuscitator bag and a face mask to ventilate the patient until the tube can be replaced. You may have to cover the tracheostomy site to prevent air leakage.
Tunneled Central Venous Catheters
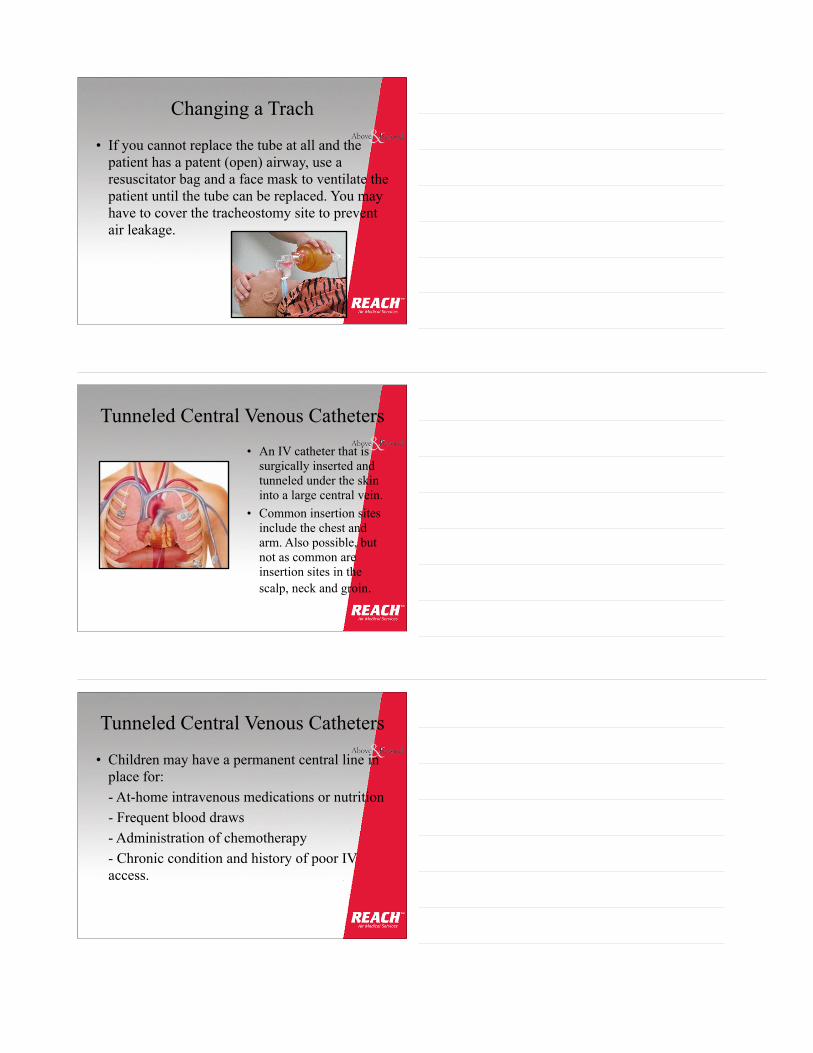
• An IV catheter that is surgically inserted and tunneled under the skin into a large central vein.
• Common insertion sites include the chest and arm. Also possible, but not as common are insertion sites in the scalp, neck and groin.
Tunneled Central Venous Catheters
• Children may have a permanent central line in place for:
- At-home intravenous medications or nutrition - Frequent blood draws - Administration of chemotherapy - Chronic condition and history of poor IV
access.

Types of Tunneled Catheters
• Broviac-Hickman catheter (also known as Groshong catheter.
• Port-a-Cath • PICC (Peripherally
Inserted Central Catheter)
• Also referred to as PVAD’s
Accessing the Catheter
• Port-a-caths require insertion of a special needle to use.
• Other catheters may be accessed by a capped or luer-lock mechanism. • Be aware of potential heparinized lines. • When drawing labs, first draw should be used for blood culture or waste and then use another syringe to draw remaining labs.
Kids and their Lines
• Always let the child know what you are going to do with the line.
eg. draw blood or infuse medication. • Some children are sensitive to the sensation
when lines are flushed quickly. • Some kids require pre-medication with
lidocaine cream to site before accessing port-a-caths.
Line Emergencies
• Line dislodgement – apply pressure to site and above insertion point.
• Save dislodged line to verify length to rule out thrombi of line tip.
• Always ensure caps are snug as hemorrhage or air emboli can occur in a short period of time from disconnected catheters.
• If you are not sure about using the line you can always place a PIV until the line has been verified.
Enteral Feeding Tubes
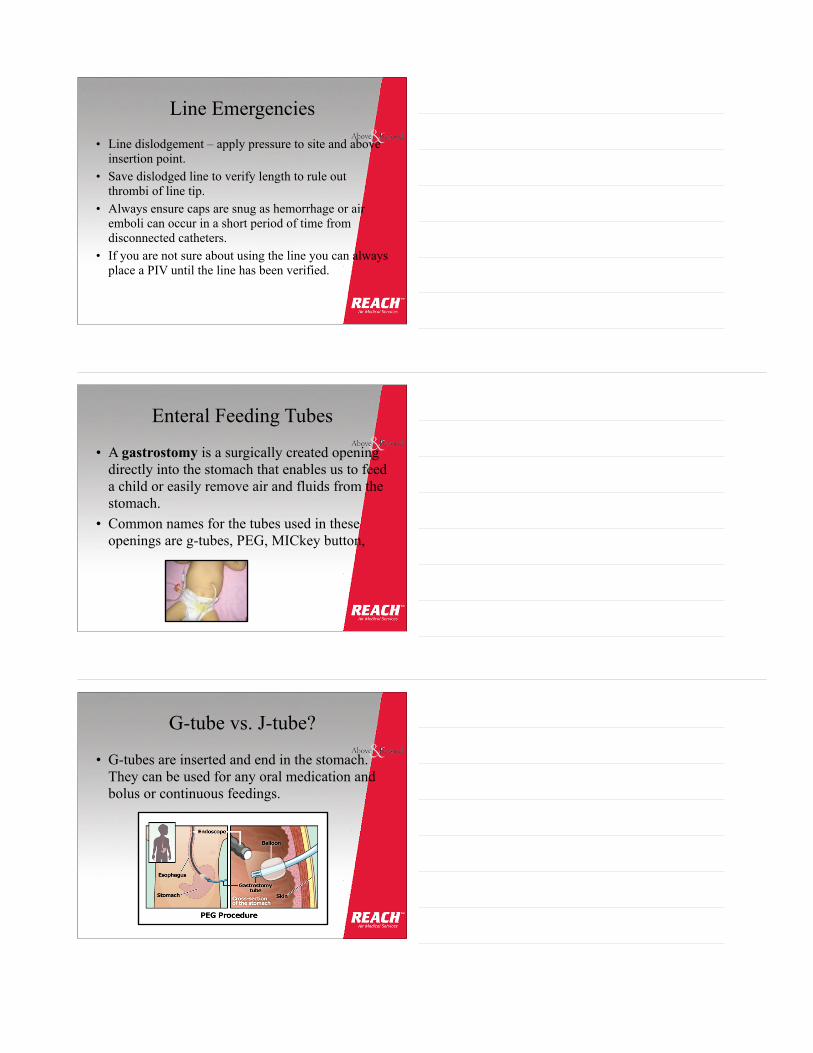
• A gastrostomy is a surgically created opening directly into the stomach that enables us to feed a child or easily remove air and fluids from the stomach.
• Common names for the tubes used in these openings are g-tubes, PEG, MICkey button,
G-tube vs. J-tube?
• G-tubes are inserted and end in the stomach. They can be used for any oral medication and bolus or continuous feedings.

G-tube vs. J-tube?• J-tubes are inserted in the
stomach wall and then have a tube that is directed into the jejunum. These tubes should only be used for continuous feedings and there may be restrictions on the types of medications that can be administered into them.
Reasons for Placement
• Babies with birth defects of the mouth, esophagus, or stomach (for example, esophageal atresia or tracheal esophageal fistula)
• Kids who cannot swallow correctly • Kids who cannot take enough food by mouth to
stay healthy • Children who are at risk for aspiration.
Accessing a G/J-tube
• Some tubes have a lumen with a plug that can be accessed by a luer tip syringe.
• Some button types may require an additional attachment that clips on, parents should have this with them at all times.
• After accessing a tube, placement can usually be verified by aspiration .

Occlusions and Air
!
• Some tubes are prone to occlusion due to small lumen size. This can also occur when certain medications mix together in the tubing and “cement” together.
• Occlusions can usually be removed by aspiration or warm water.
Occlusions and Air• G-tubes can also be vented to remove air and contents
from the stomach. This may be especially important in cases of:
- respiratory distress - procedures requiring anesthesia - intubation - after PPV with a BVM
Displaced and Dislodged Tubes
• When faced with a dislodged g-tube, cover the site with 4x4’s. Watch for skin breakdown from gastric output.
• J-tubes that have migrated into the stomach may not be tolerated for feedings and usually require interventional radiology to confirm replacement into the jejunum.

Summary
• Parents and caregivers are important sources of information
• Find out normal values/baseline for the child you are treating
• Organized approach • Knowing reason and
management for a child’s tracheostomy
Summary
• Central lines are becoming more common in the community.
• G-tubes and J-tubes come in various styles.
• Once again, in these children, your most valuable resource is the parents!
Administrative Offices: 451 Aviation Blvd., Suite 101
Santa Rosa, California 95403
707.324.2400
www.REACHair.com

Tranexamic Acid: An Old Dog with New Tricks
Jeff Cress, LP, CCEMT-P Program Manager
REACH 1 (Santa Rosa, CA)
REACH 6 (Lakeport, CA)
REACH 18 (Ukiah, CA)
REACH Air Medical Services
(Note: This presentation will be posted online after the conference.)

!!!!!THANK YOU FOR ATTENDING
!!!


















