RANDOMIZED CONTROL TRIALS Kinza Waqar Assisitant Clinical Research Associate Shifa Clinical research...
26
RANDOMIZED CONTROL TRIALS Kinza Waqar Assisitant Clinical Research Associate Shifa Clinical research Center (SCRC)
-
Upload
vincent-watson -
Category
Documents
-
view
226 -
download
8
Transcript of RANDOMIZED CONTROL TRIALS Kinza Waqar Assisitant Clinical Research Associate Shifa Clinical research...

RANDOMIZED CONTROL TRIALS
Kinza WaqarAssisitant Clinical Research AssociateShifa Clinical research Center (SCRC)
CONTENTS:What are RCTs?
General Principals of RCTs
Randomization: The strength of RCTs
Allocation concealment
Bias in randomization
Blinding
Inclusion and exclusion criteria
Baseline data
Intent to treat
Types of RCTs
Ethics of RCTs
Clinical equipoise
Reporting of RCTs
PICK A SHAPE!
Choose a shape, anyone you like.
Wait till the next 6 slides to find out the purpose.
WHAT IS RCT Randomized control trial is a study in which people are allocated at random to receive one of several clinical interventions.
(Jadad AR, 1980) Intervention = Any maneuver that improves health status. Can be:a. Diagnostic testb. Treatmentc. Prevention strategyd. Intervention procedure
(DeVore GR,1994)
RANDOMIZATION:
All participants should have same chance of being assigned to a particular study group.
The allocation, therefore, is not determined by the investigators, the clinicians, or the study participants
If randomization is done properly, it reduces the risk of a serious imbalance
(Altman DG, 1991)
ALLOCATION CONCEALMENT To prevent selection bias.
Allocation concealment refers to the technique used to implement the sequence, not to generate it
Methods:
1. SNOSE sequentially numbered, opaque, sealed envelopes
2.pharmacy controlled numbered or coded containers
3. central randomization— eg, by telephone to a trials office—or other method whose description contained elements convincing of concealment—eg, a secure computer-assisted method
BIAS IN RCT
In statistics it means a tendency of an estimate to deviate in one direction from a true value.
Why does it matter: true outcomes are unknown. Bias should be eliminated in concluding research results
BIAS IN RCT
Types: Selection bias: if some potentially eligible individuals are selectively excluded from the study
Ascertainment bias: occurs when the results of a trial are distorted by knowledge of which intervention each participant is receiving.
IMPORTANT SOURCES OF BIAS Bias during the planning phase of an RCT
oChoice-of-question bias: hidden agenda
oRegulation bias: IRB bias or the Bureaucracy bias.
oWrong design bias: wrong research design can produce misleading answers.
oPopulation choice bias: gender bias, age bias, literacy bias
Bias During reporting:
oSelective reporting bias
oFraud bias
opublication bias
oTime lag bias
(Jadad AR, Rennie D., 1998)
BLINDING
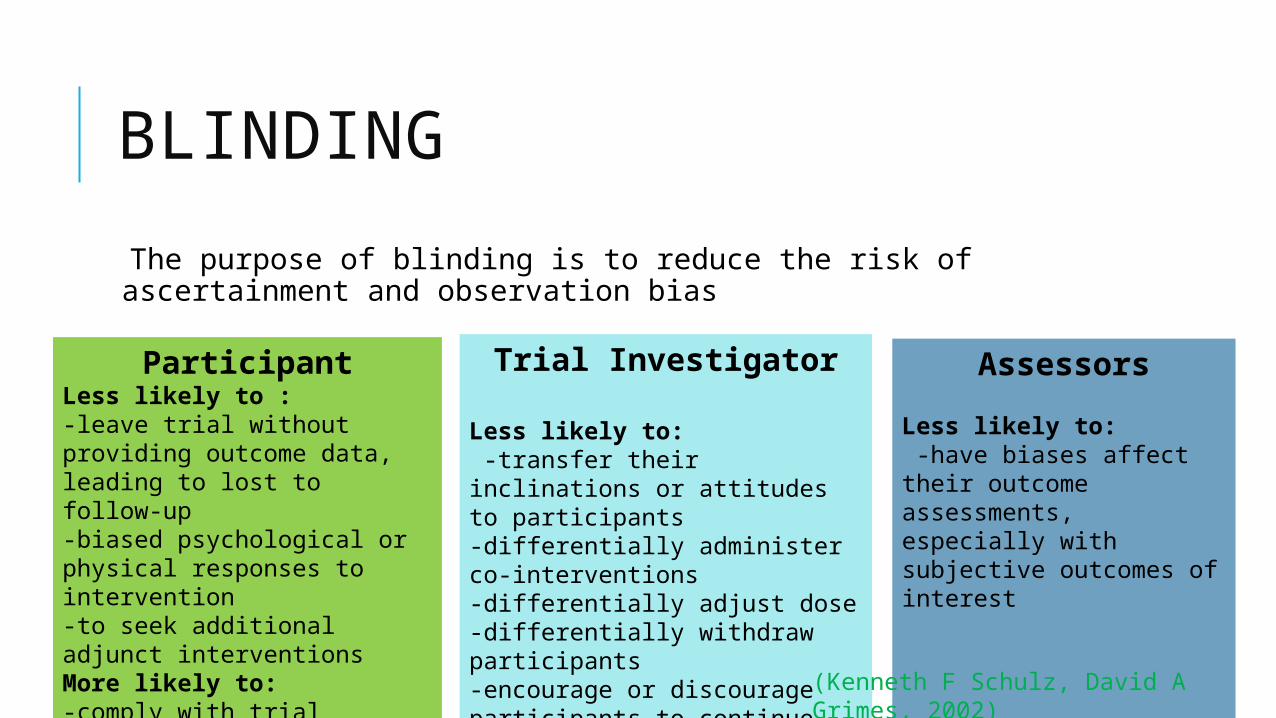
The purpose of blinding is to reduce the risk of ascertainment and observation bias
ParticipantLess likely to :-leave trial without providing outcome data, leading to lost to follow-up-biased psychological or physical responses to intervention-to seek additional adjunct interventionsMore likely to:-comply with trial regimens
Trial Investigator
Less likely to: -transfer their inclinations or attitudes to participants-differentially administer co-interventions-differentially adjust dose-differentially withdraw participants-encourage or discourage participants to continue trial
Assessors
Less likely to: -have biases affect their outcome assessments, especially with subjective outcomes of interest
(Kenneth F Schulz, David A Grimes, 2002)
WHAT SHAPE YOU CHOSE?
c Types of RCTs c Types of RCTsTreatment group
Control group
Square Triangle = Placebo
Circle
It was :RandomizedUnbiasedSingle – blinded/double blinded
TYPES OF RCT:
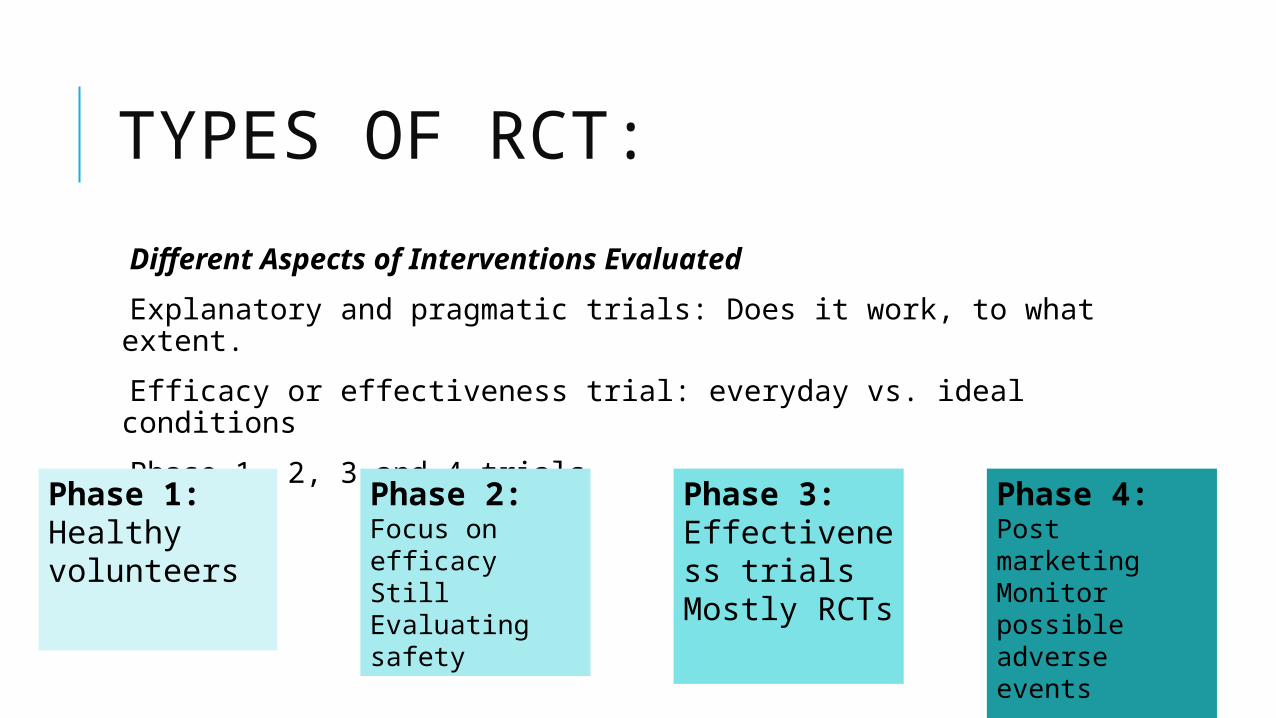
Different Aspects of Interventions Evaluated
Explanatory and pragmatic trials: Does it work, to what extent.
Efficacy or effectiveness trial: everyday vs. ideal conditions
Phase 1, 2, 3 and 4 trials
Phase 1:Healthy volunteers
Phase 2:Focus on efficacyStill Evaluating safety
Phase 3:Effectiveness trialsMostly RCTs
Phase 4:Post marketingMonitor possible adverse events
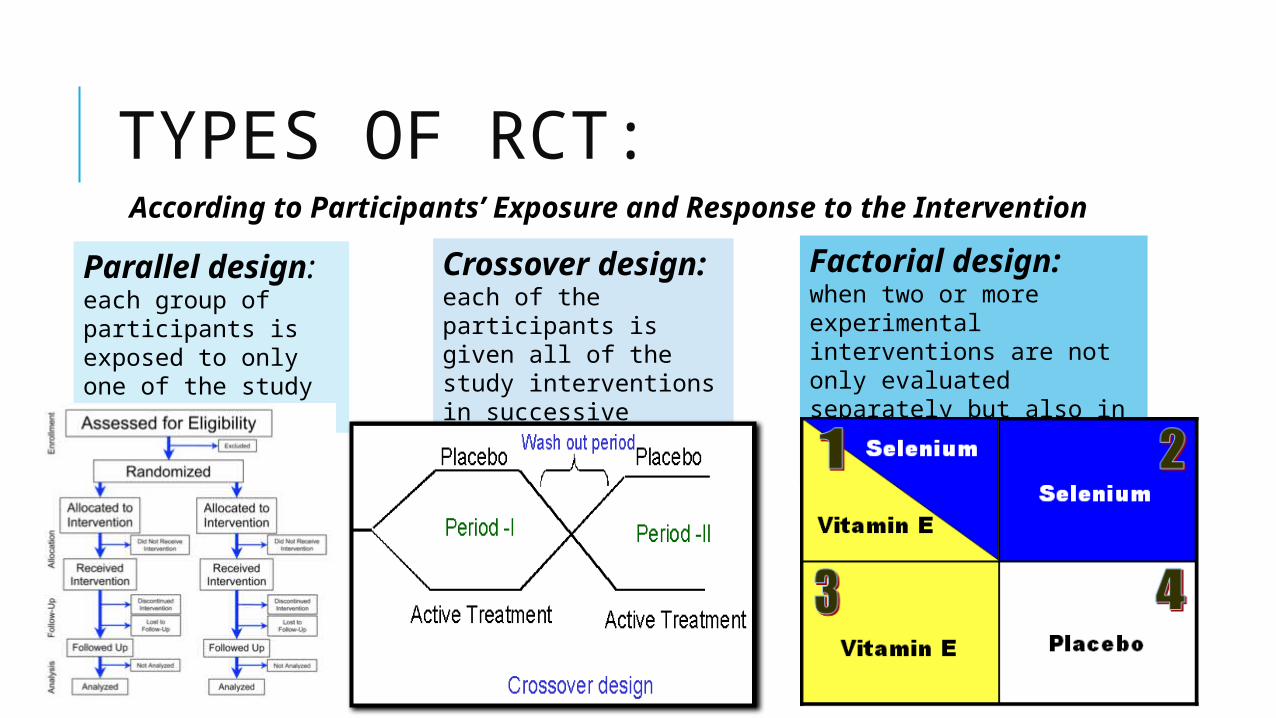
TYPES OF RCT: According to Participants’ Exposure and Response to the Intervention
Parallel design: each group of participants is exposed to only one of the study interventions
Crossover design: each of the participants is given all of the study interventions in successive periods.
Factorial design: when two or more experimental interventions are not only evaluated separately but also in combination and against a control.
TYPES OF RCT:
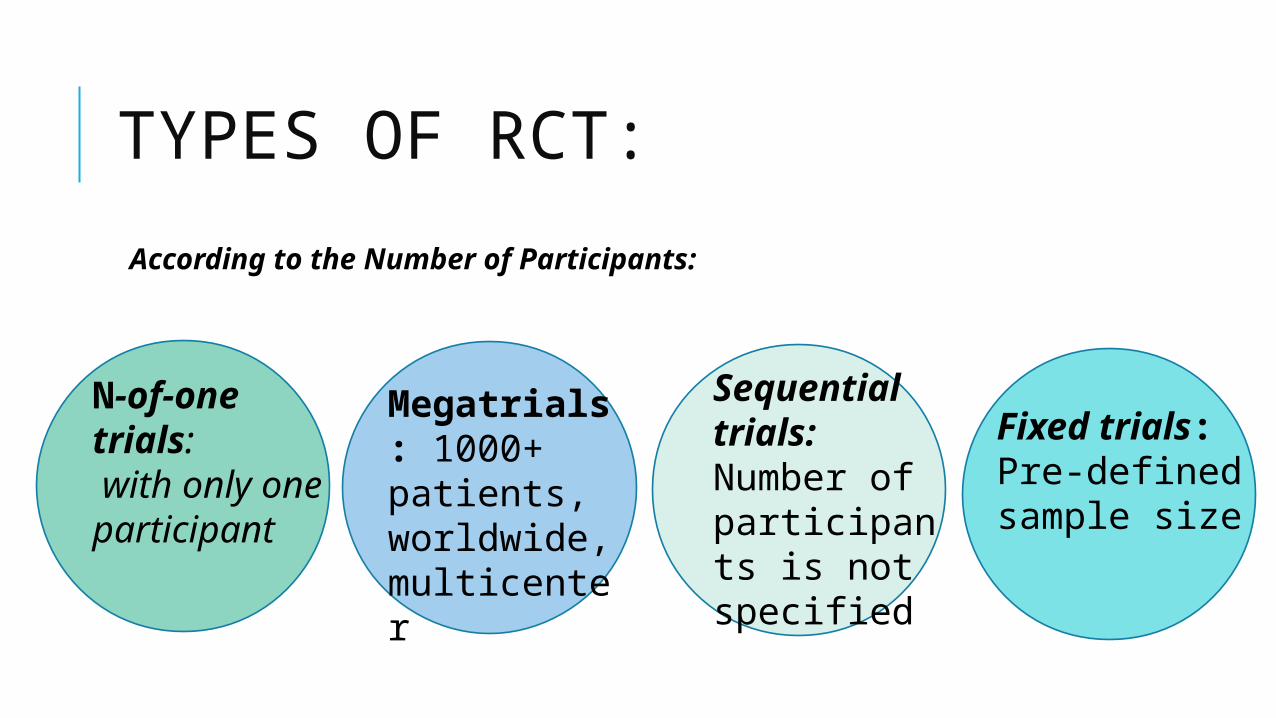
According to the Number of Participants:
N-of-one trials: with only one participant
Megatrials: 1000+ patients, worldwide, multicenter
Sequential trials: Number of participants is not specified
Fixed trials: Pre-defined sample size
TYPES OF RCT:
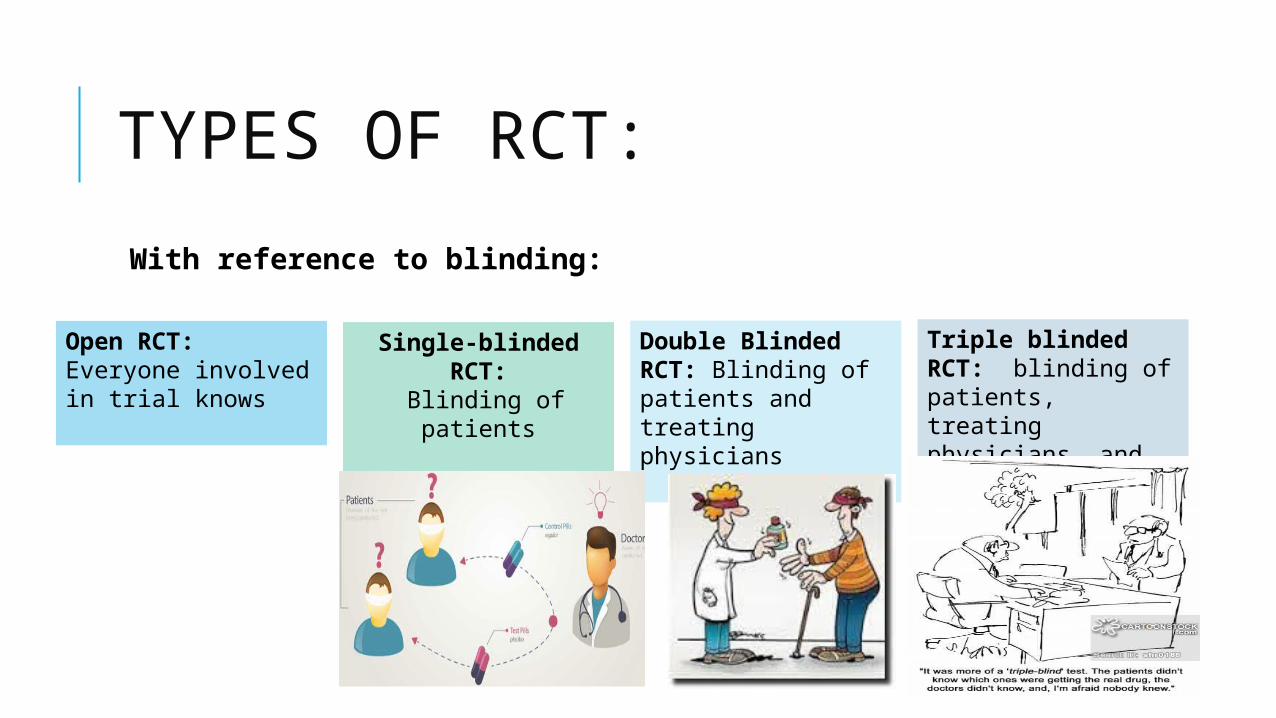
With reference to blinding:
Open RCT: Everyone involved in trial knows
Single-blinded RCT:
Blinding of patients
Double Blinded RCT: Blinding of patients and treating physicians
Triple blinded RCT: blinding of patients, treating physicians, and study investigators
TYPES OF RCT:
According to Nonrandomized Participant Preferences
Preference trials:
These are called preference trials because they include at least one group in which the participants are allowed to choose their preferred treatment from among several options offered
(Till JE, Sutherland HJ, Meslin EM., 1992)
ETHICS OF RCT:
It is not ethical to build a trial in which, before enrollment, evidence suggests that patients in one arm of the study are more likely to benefit from enrollment than patients in the other arm.
Randomized controlled trials can be planned only in areas of uncertainty and can be carried out only as long as the uncertainty remains
for example, the effect of a risk factor such as smoking cannot ethically be addressed with randomized controlled trials.
(Hellman S, Hellman DS., 1991)
CLINICAL EQUIPOISE
The principle of equipoise, provides the ethical basis for medical research that involves assigning patients to different treatment arms of a clinical trial.
i. A trial should begin with a null hypothesis
ii. here should exist no decisive evidence that the intervention or drug being tested will be superior to existing treatments or effective at all
INCLUSION CRITERIA
Specific inclusion criteria are used to optimize the following:
1. Recruitment, compliance and follow-up of patient
2. generalizability of results
3. expected efficacy of treatment
4. the rate of primary outcome
EXCLUSION CRITERIA
Some valid reason for excluding participants are:
1. When the risk of treatment (or placebo) is unacceptable
2. When the treatment is unlikely to be effective, disease is too mild or too severe or patient already failed the treatment.
3. When the patient has other conditions (co-morbidity).
4. When the patient is unable or unlikely to adhere to precool and follow ups
5. Other constraints; language, cognitive impairment, no phone at home etc.
BASELINE MEASUREMENTS
At baseline, collect information about:
1. Demographics
2. Contact details; to help in tracking subject during study.
Includes Name, email, address, tel/fax, contact info of friends or family
3. Major clinical characteristic and prognostic factors.
INTENT TO TREAT
Intent to Treat:
A method to correct for differential dropout rates between patients from one arm of the study and another is to analyze data by the intent to treat—that is, data are analyzed in the way patients were randomized, regardless of whether or not they received the intended intervention.
(Huwiler-Müntener K, Jüni P, Junker C, Egger M., 2002)
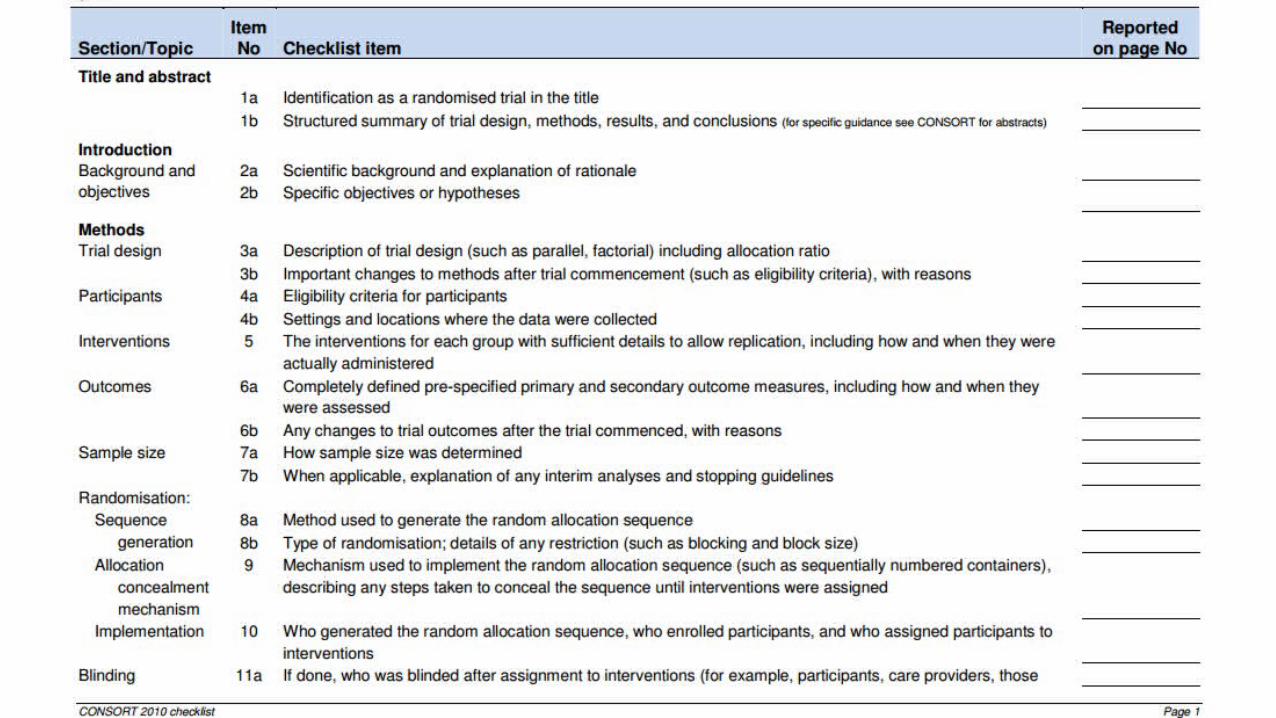
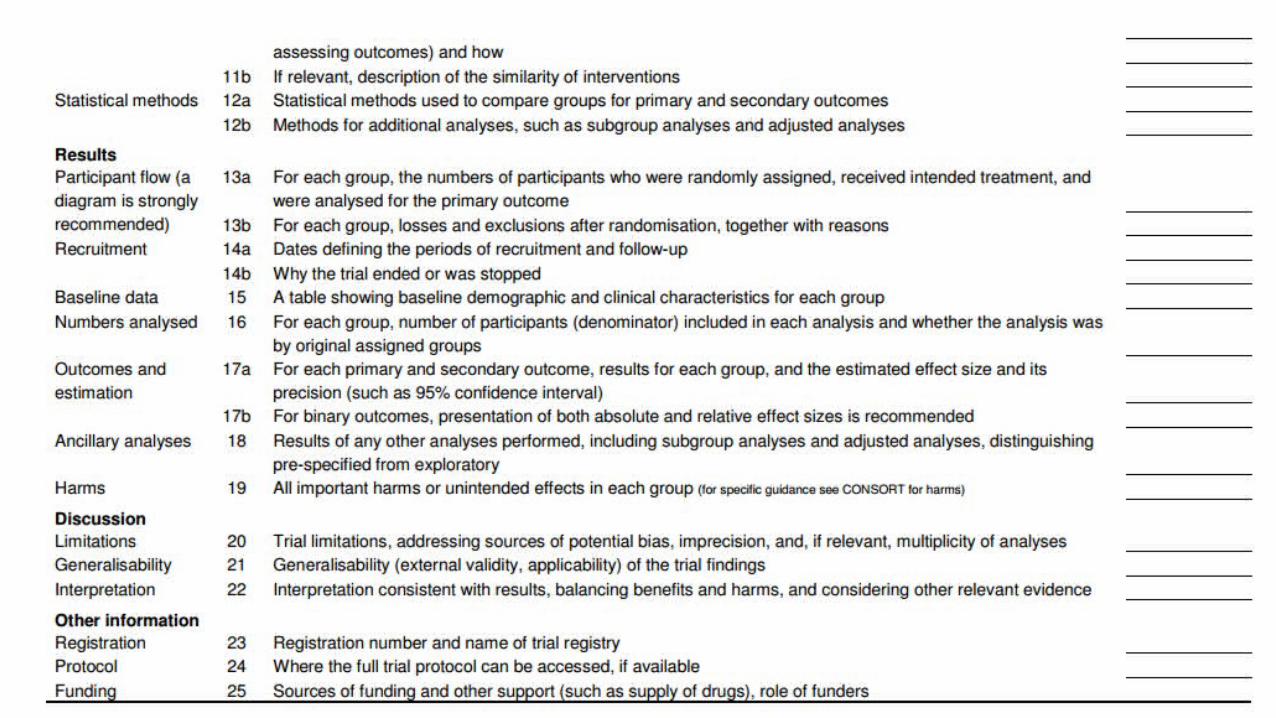
REPORTING OF RCTS
CONSORT (Consolidated Standards of Reporting Trials)
Standard format of reporting an RCT
Following slides show that CONSORT checklist
You can find the Consort Checklist on SCRC official website:
http://www.int.shifa.com.pk/video/web/scrc/article2/CONSORT%202010%20Checklist/