Radiotherapy in Lung Cancer Dr. Vassilis Kouloulias 1 Radiotherapy in Lung Cancer Dr. Vassilis...
54
Radiotherapy in lung cancer. Dr. V. Kouloulias 1 Radiotherapy in Lung Cancer Dr. Vassilis Kouloulias Assistant Professor of Radiation Oncologist, 2 nd Dpt. Radiology, University of Athens, Greece. Key Words Small cell lung cancer (SCLC), Non-small cell lung cancer (NSCLC), radical, palliative, radiotherapy, prophylactic cranial irradiation (PCI), radiation induced pneumonitis, cyttoprotection.
Transcript of Radiotherapy in Lung Cancer Dr. Vassilis Kouloulias 1 Radiotherapy in Lung Cancer Dr. Vassilis...
Radiotherapy in lung cancer. Dr. V. Kouloulias
1
Radiotherapy in Lung Cancer
Dr. Vassilis Kouloulias Assistant Professor of Radiation Oncologist, 2nd Dpt. Radiology, University of Athens, Greece.
Key Words
Small cell lung cancer (SCLC), Non-small cell lung cancer (NSCLC), radical, palliative,
radiotherapy, prophylactic cranial irradiation (PCI), radiation induced pneumonitis, cyttoprotection.
Radiotherapy in lung cancer. Dr. V. Kouloulias
2
Section I. Small cell lung Cancer
I.1. Introduction.
Small cell lung cancer (SCLC) accounts for 20% of all primary lung tumors. It has a high growth
fraction and at diagnosis the disease is usually extended. Bronchial obstruction is present in 30%-
40% of patients and in 14% of cases a solitary peripheral mass is found. Multiagent drug
combinations are more effective than single agents, while SCLC tumors are normally sensitive to
many chemotherapeutic drugs. Complete response to chemotherapy appears in 40-68% of patients
with limited stage disease and in 18%-40% in those with extensive disease.
I.2. Limited stage
Thoracic irradiation: doses, fractionation, target volumes, beam arrangements.
Some medical oncologists question the indication of thoracic irradiation due to the high incidence of
distant metastases. However, several trials have already shown the beneficial role of radiotherapy in
terms of tumor control and survival [1-3]. Mira et al. [4] reported 30-60% of locoregional
recurrences of patients receiving thoracic irradiation in contrast with 75-80% in patients treated with
chemotherapy alone. Perez et al. [5] in a randomized study involving 304 patients, reported an
intrathoracic failure rate of 52% in patients receiving chemotherapy alone compared with 36% in
those receiving adjuvant radiotherapy. The 2-year survival was 40% in those receiving thoracic
irradiation compared with 23% in the group receiving chemotherapy alone. Perry et al. [6] in
prospective randomized trial of 399 evaluable patients reported a significant number of complete
response in favor of radiotherapy (P=0.0013). Nevertheless, by reviewing the current literature in
reported series comparing chemotherapy alone versus chemo-radiotherapy, data concerning response
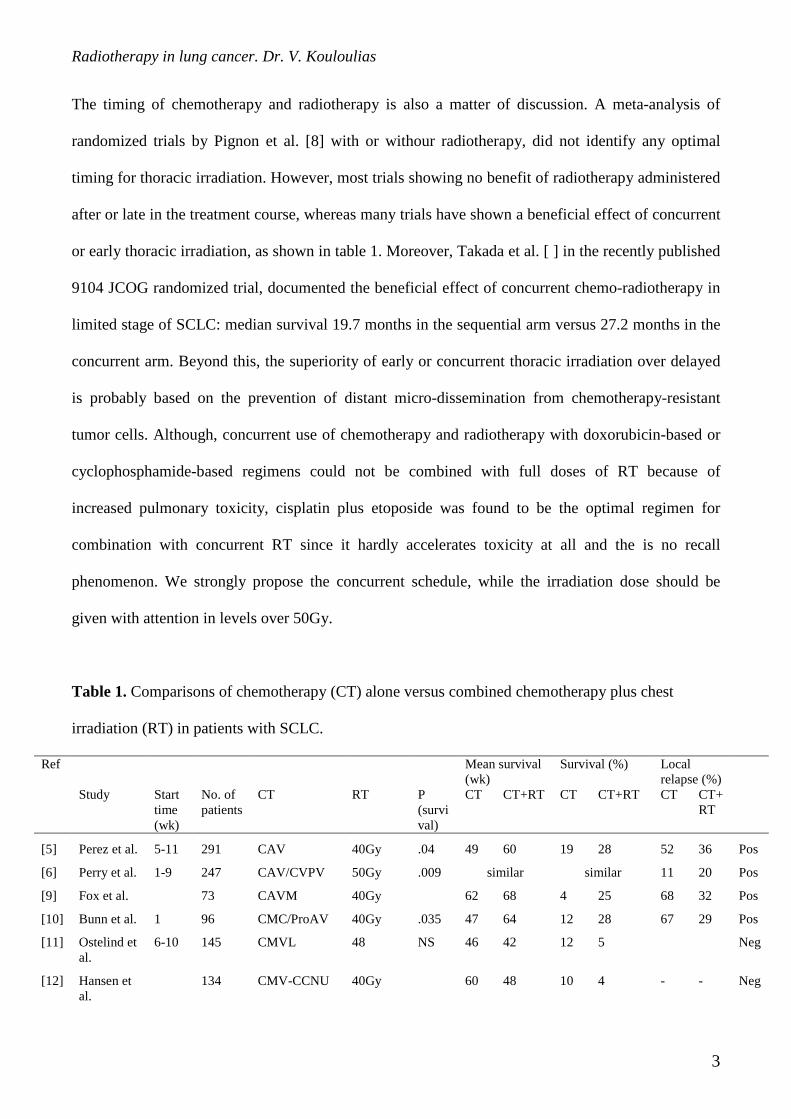
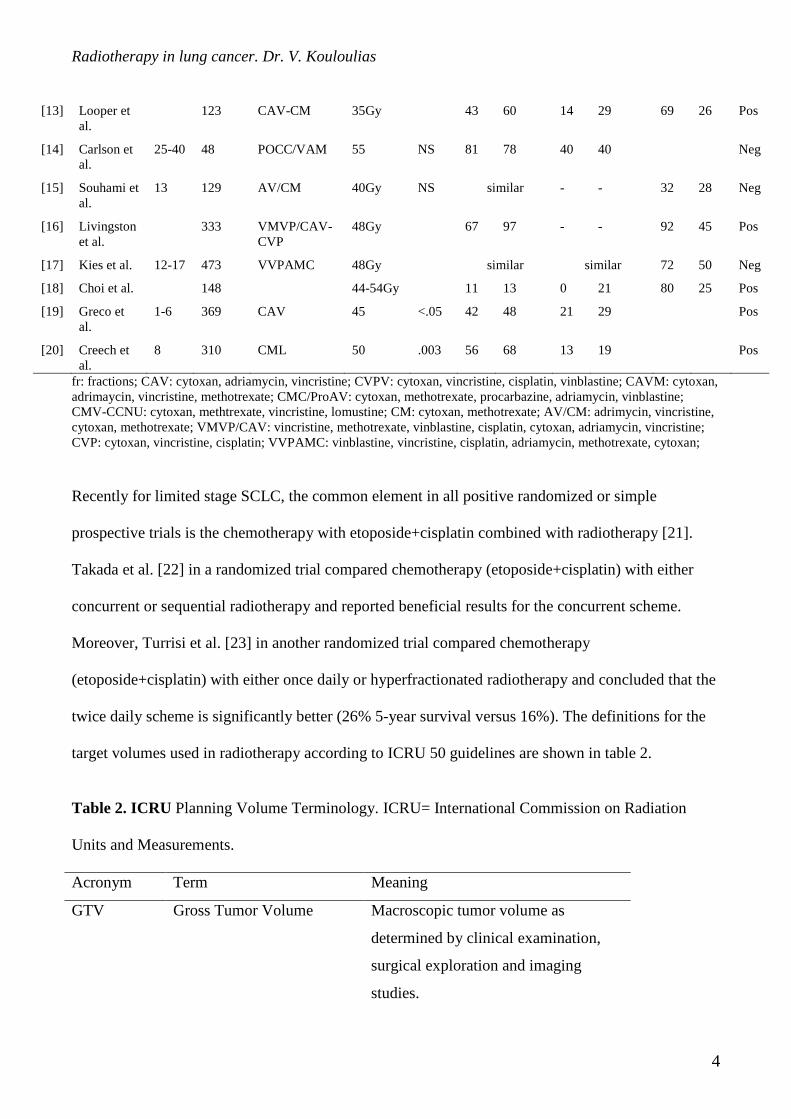
or failure rates are rather controversial [3,7]. The summary of reported series is shown in table 1. As
it is shown, most of the randomized trials are reported a positive impact of thoracic irradiation in
terms of survival and local control.
Radiotherapy in lung cancer. Dr. V. Kouloulias
3
The timing of chemotherapy and radiotherapy is also a matter of discussion. A meta-analysis of
randomized trials by Pignon et al. [8] with or withour radiotherapy, did not identify any optimal
timing for thoracic irradiation. However, most trials showing no benefit of radiotherapy administered
after or late in the treatment course, whereas many trials have shown a beneficial effect of concurrent
or early thoracic irradiation, as shown in table 1. Moreover, Takada et al. [ ] in the recently published
9104 JCOG randomized trial, documented the beneficial effect of concurrent chemo-radiotherapy in
limited stage of SCLC: median survival 19.7 months in the sequential arm versus 27.2 months in the
concurrent arm. Beyond this, the superiority of early or concurrent thoracic irradiation over delayed
is probably based on the prevention of distant micro-dissemination from chemotherapy-resistant
tumor cells. Although, concurrent use of chemotherapy and radiotherapy with doxorubicin-based or
cyclophosphamide-based regimens could not be combined with full doses of RT because of
increased pulmonary toxicity, cisplatin plus etoposide was found to be the optimal regimen for
combination with concurrent RT since it hardly accelerates toxicity at all and the is no recall
phenomenon. We strongly propose the concurrent schedule, while the irradiation dose should be
given with attention in levels over 50Gy.
Table 1. Comparisons of chemotherapy (CT) alone versus combined chemotherapy plus chest
irradiation (RT) in patients with SCLC.
Ref Mean survival (wk)
Survival (%) Local relapse (%)
Study Start time (wk)
No. of patients
CT RT P (survival)
CT CT+RT CT CT+RT CT CT+RT
[5] Perez et al. 5-11 291 CAV 40Gy .04 49 60 19 28 52 36 Pos
[6] Perry et al. 1-9 247 CAV/CVPV 50Gy .009 similar similar 11 20 Pos
[9] Fox et al. 73 CAVM 40Gy 62 68 4 25 68 32 Pos
[10] Bunn et al. 1 96 CMC/ProAV 40Gy .035 47 64 12 28 67 29 Pos
[11] Ostelind et al.
6-10 145 CMVL 48 NS 46 42 12 5 Neg
[12] Hansen et al.
134 CMV-CCNU 40Gy 60 48 10 4 - - Neg
Radiotherapy in lung cancer. Dr. V. Kouloulias
4
[13] Looper et al.
123 CAV-CM 35Gy 43 60 14 29 69 26 Pos
[14] Carlson et al.
25-40 48 POCC/VAM 55 NS 81 78 40 40 Neg
[15] Souhami et al.
13 129 AV/CM 40Gy NS similar - - 32 28 Neg
[16] Livingston et al.
333 VMVP/CAV-CVP
48Gy 67 97 - - 92 45 Pos
[17] Kies et al. 12-17 473 VVPAMC 48Gy similar similar 72 50 Neg
[18] Choi et al. 148 44-54Gy 11 13 0 21 80 25 Pos
[19] Greco et al.
1-6 369 CAV 45 <.05 42 48 21 29 Pos
[20] Creech et al.
8 310 CML 50 .003 56 68 13 19 Pos
fr: fractions; CAV: cytoxan, adriamycin, vincristine; CVPV: cytoxan, vincristine, cisplatin, vinblastine; CAVM: cytoxan, adrimaycin, vincristine, methotrexate; CMC/ProAV: cytoxan, methotrexate, procarbazine, adriamycin, vinblastine; CMV-CCNU: cytoxan, methtrexate, vincristine, lomustine; CM: cytoxan, methotrexate; AV/CM: adrimycin, vincristine, cytoxan, methotrexate; VMVP/CAV: vincristine, methotrexate, vinblastine, cisplatin, cytoxan, adriamycin, vincristine; CVP: cytoxan, vincristine, cisplatin; VVPAMC: vinblastine, vincristine, cisplatin, adriamycin, methotrexate, cytoxan;
Recently for limited stage SCLC, the common element in all positive randomized or simple
prospective trials is the chemotherapy with etoposide+cisplatin combined with radiotherapy [21].
Takada et al. [22] in a randomized trial compared chemotherapy (etoposide+cisplatin) with either
concurrent or sequential radiotherapy and reported beneficial results for the concurrent scheme.
Moreover, Turrisi et al. [23] in another randomized trial compared chemotherapy
(etoposide+cisplatin) with either once daily or hyperfractionated radiotherapy and concluded that the
twice daily scheme is significantly better (26% 5-year survival versus 16%). The definitions for the
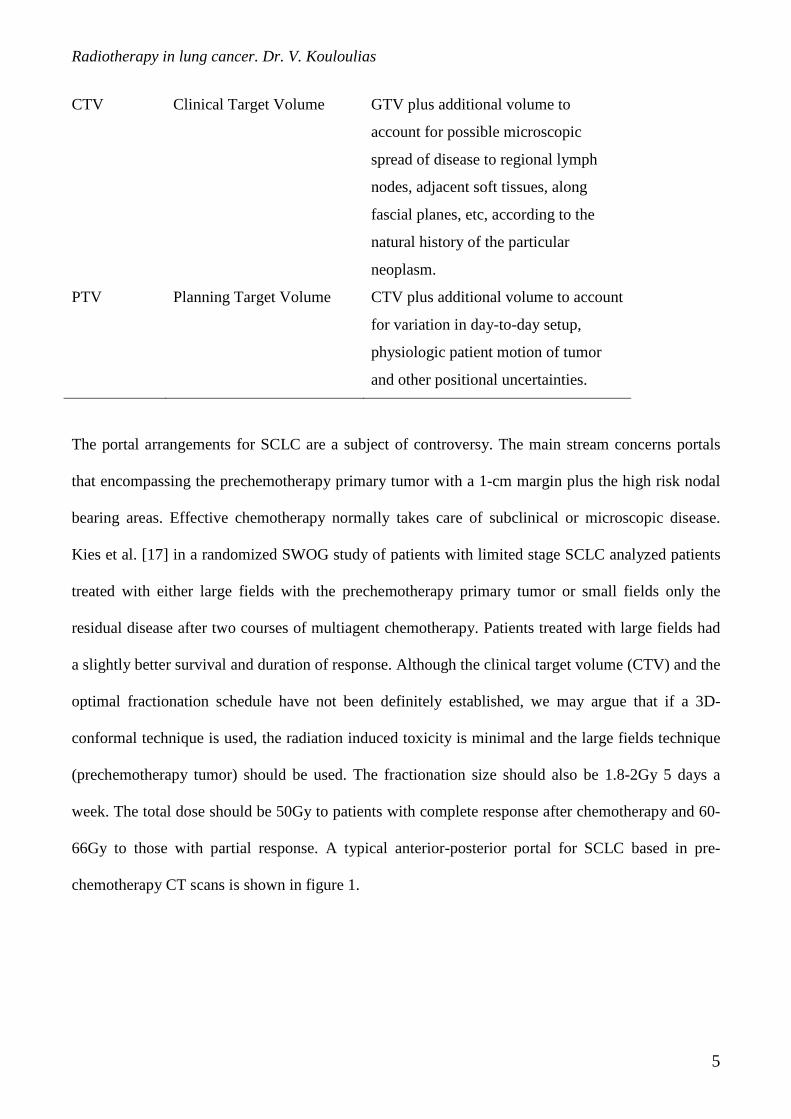
target volumes used in radiotherapy according to ICRU 50 guidelines are shown in table 2.
Table 2. ICRU Planning Volume Terminology. ICRU= International Commission on Radiation
Units and Measurements.
Acronym Term Meaning
GTV Gross Tumor Volume Macroscopic tumor volume as
determined by clinical examination,
surgical exploration and imaging
studies.
Radiotherapy in lung cancer. Dr. V. Kouloulias
5
CTV Clinical Target Volume GTV plus additional volume to
account for possible microscopic
spread of disease to regional lymph
nodes, adjacent soft tissues, along
fascial planes, etc, according to the
natural history of the particular
neoplasm.
PTV Planning Target Volume CTV plus additional volume to account
for variation in day-to-day setup,
physiologic patient motion of tumor
and other positional uncertainties.
The portal arrangements for SCLC are a subject of controversy. The main stream concerns portals
that encompassing the prechemotherapy primary tumor with a 1-cm margin plus the high risk nodal
bearing areas. Effective chemotherapy normally takes care of subclinical or microscopic disease.
Kies et al. [17] in a randomized SWOG study of patients with limited stage SCLC analyzed patients
treated with either large fields with the prechemotherapy primary tumor or small fields only the
residual disease after two courses of multiagent chemotherapy. Patients treated with large fields had
a slightly better survival and duration of response. Although the clinical target volume (CTV) and the
optimal fractionation schedule have not been definitely established, we may argue that if a 3D-
conformal technique is used, the radiation induced toxicity is minimal and the large fields technique
(prechemotherapy tumor) should be used. The fractionation size should also be 1.8-2Gy 5 days a
week. The total dose should be 50Gy to patients with complete response after chemotherapy and 60-
66Gy to those with partial response. A typical anterior-posterior portal for SCLC based in pre-
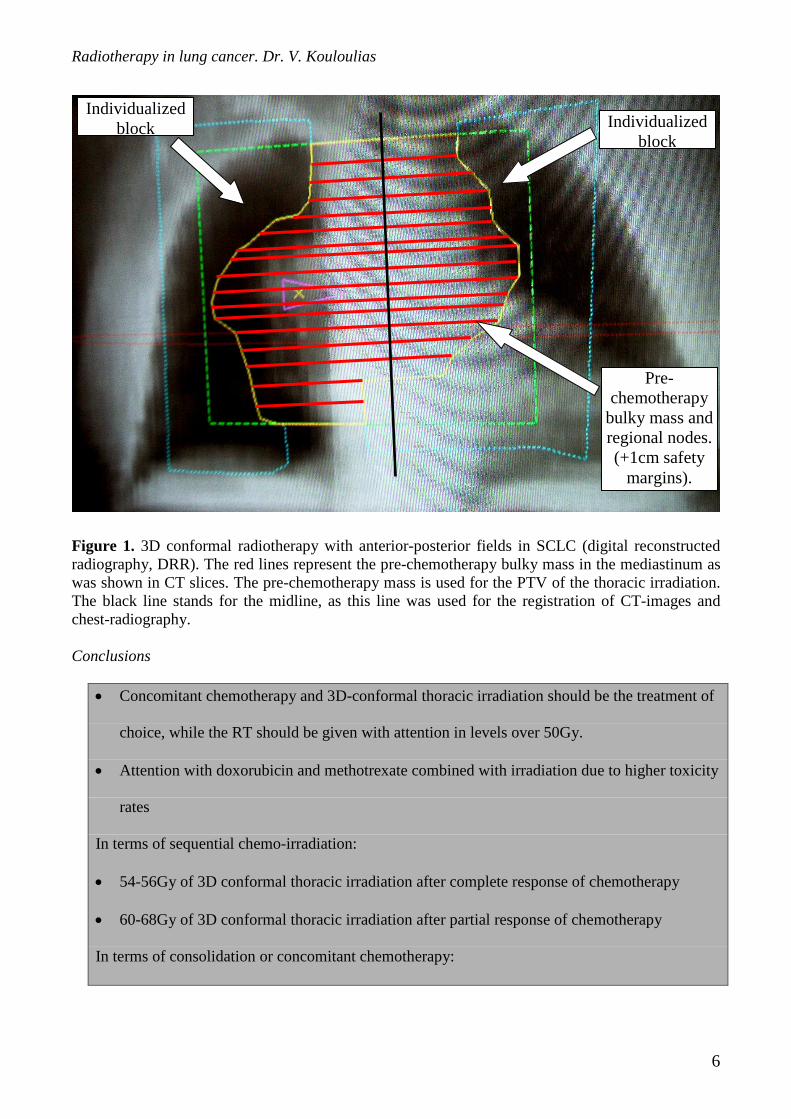
chemotherapy CT scans is shown in figure 1.
Radiotherapy in lung cancer. Dr. V. Kouloulias
6
Figure 1. 3D conformal radiotherapy with anterior-posterior fields in SCLC (digital reconstructed radiography, DRR). The red lines represent the pre-chemotherapy bulky mass in the mediastinum as was shown in CT slices. The pre-chemotherapy mass is used for the PTV of the thoracic irradiation. The black line stands for the midline, as this line was used for the registration of CT-images and chest-radiography. Conclusions
• Concomitant chemotherapy and 3D-conformal thoracic irradiation should be the treatment of
choice, while the RT should be given with attention in levels over 50Gy.
• Attention with doxorubicin and methotrexate combined with irradiation due to higher toxicity
rates
In terms of sequential chemo-irradiation:
• 54-56Gy of 3D conformal thoracic irradiation after complete response of chemotherapy
• 60-68Gy of 3D conformal thoracic irradiation after partial response of chemotherapy
In terms of consolidation or concomitant chemotherapy:
Individualized block Individualized
block
Pre-chemotherapy
bulky mass and regional nodes. (+1cm safety
margins).
Radiotherapy in lung cancer. Dr. V. Kouloulias
7
• 46-50Gy of 3D conformal thoracic irradiation should be given with precautions concerning
radiation induced pneumonitis.
• In case of bulky disease remaining after the 50 Gy, a boost schedule encompassing only the
gross tumor volume might be administered up to 60Gy.
I.3. Prophylactic cranial irradiation (PCI).
In patients with limited small-cell lung cancer, chemotherapy combined with thoracic
radiotherapy yields complete response rates of 50 to 85 percent, a median duration of survival of 12
to 20 months, and 2-year disease-free survival rates of 15 to 40 percent [23,24]. Five-year survival
rates may exceed 20 percent for patients who have complete responses [23]. With the combined
treatment, the risk of a thoracic recurrence decreases, and as a result, brain metastasis becomes one
of the main types of relapse. Although only 10 percent of patients have brain metastasis at the time of
diagnosis, the cumulative incidence at two years is more than 50 percent, [25] which is consistent
with the rate found in autopsy series [26]. Indeed, back to 1970 Mathews et al. [27] observed that
83% of patients with small-cell lung cancer (SCLC) who died one month after curative resection had
residual disease on autopsy and in 50% of them had brain metastasis. Also in the early 70s Hansen
[28] raised the question whether brain irradiation should be in conjunction with systemic
chemotherapy for the treatment of patients with SCLC. From 1977 up to 1997 eleven prospective
randomized clinical trials were published in which SCLC patients with or without limited disease
and complete response were randomized to receive or not prophylactic cranial irradiation (PCI) [29-
39]. These trials showed that PCI significantly decreased the risk of developing CNS metastases.
Most of the trials reported total irradiation dose 30 to 36 Gy [40,41].
A thorough meta-analysis by Auperine et al. [42] published by the Prophylactic Cranial
Irradiation Overview Collaborative Group evaluated prophylactic cranial irradiation in 987 patients
with small-cell lung cancer in complete remission and showed that prophylactic cranial irradiation
Radiotherapy in lung cancer. Dr. V. Kouloulias
8
leads to a small but significant absolute reduction in mortality (5.4 percent), even after adjustment for
the extent of initial disease. Additionally, irradiation not only significantly reduced the risk of brain
metastasis, as previously shown in individual trials, but also improved overall and disease-free
survival; these results confirm that prophylactic cranial irradiation prevents and does not simply
delay the emergence of brain metastases. Meert et al. [43] in another meta-analysis of twelve
randomised trials (1547 patients) revealed a decrease of brain metastases incidence (hazard ratio
(HR): 0.48; 95 % confidence interval (CI): 0.39 - 0.60) for all the studies and an improvement of
survival (HR: 0.82; 95 % CI: 0.71 - 0.96) in patients in complete response in favour of the PCI arm.
Auperine et al. also identified a trend (P=0.01) toward a decrease in the risk of brain metastasis with
earlier administration of cranial irradiation after the initiation of induction chemotherapy. Summary
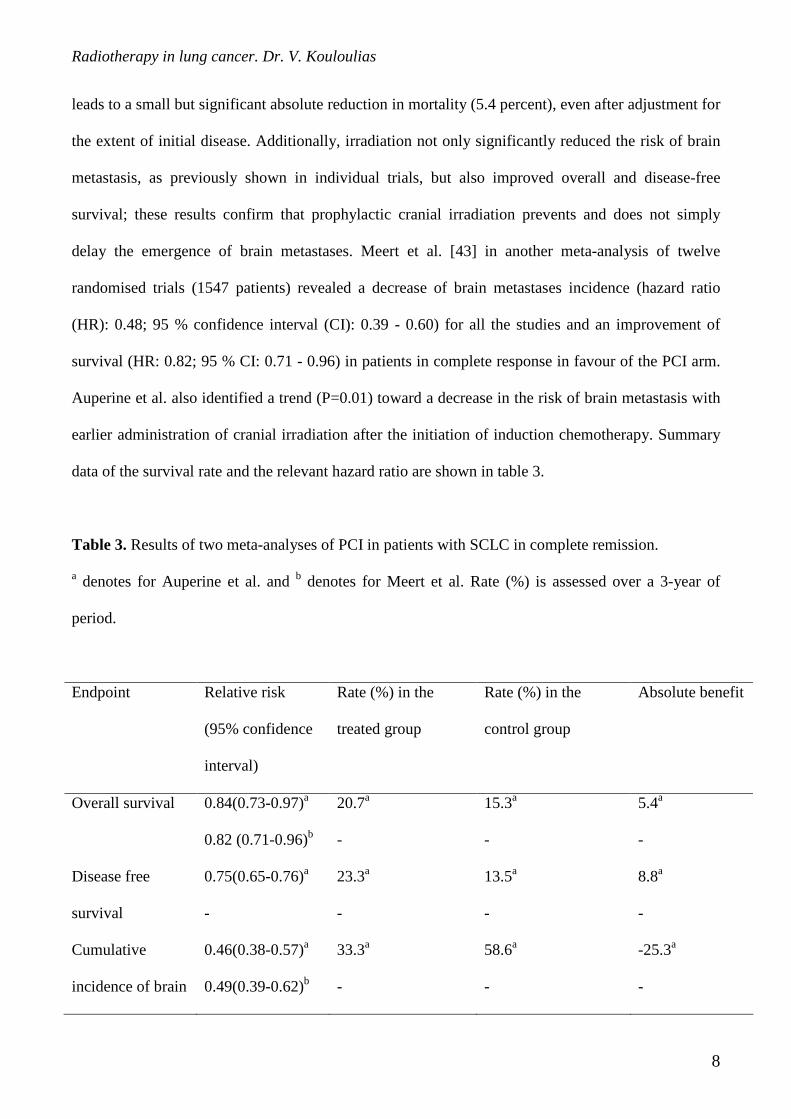
data of the survival rate and the relevant hazard ratio are shown in table 3.
Table 3. Results of two meta-analyses of PCI in patients with SCLC in complete remission.
a denotes for Auperine et al. and b denotes for Meert et al. Rate (%) is assessed over a 3-year of
period.
Endpoint Relative risk
(95% confidence
interval)
Rate (%) in the
treated group
Rate (%) in the
control group
Absolute benefit
Overall survival 0.84(0.73-0.97)a
0.82 (0.71-0.96)b
20.7a
-
15.3a
-
5.4a
-
Disease free
survival
0.75(0.65-0.76)a
-
23.3a
-
13.5a
-
8.8a
-
Cumulative
incidence of brain
0.46(0.38-0.57)a
0.49(0.39-0.62)b
33.3a
-
58.6a
-
-25.3a
-
Radiotherapy in lung cancer. Dr. V. Kouloulias
9
metastases
Radiation induced neurotoxicity comes as the main argument of the opponents of PCI [44].
From a radiobiological point of view, concerning the early injury of central nervous system, van der
Kogel [45] reported some reactions within the first 6 months after radiation. These radiation injuries
comprise demyelination (somnolence syndrome) or leukoencephalopathy. The pathogenesis is
focused on damages in oligodendrocytes and astrocytes. Some reviews of PCI studies since 1980
investigated neuropsychological effects of brain irradiation and reported cognitive disabilities,
mental abnormalities and neurological disorders [46,47]. Conflicting reports exist regarding the
cognitive effects of prophylactic brain irradiation. Retrospective analyses performed in the 1980s
reported neuropsychological modifications after PCI [48-50]. On the contrary, several randomized
trials [46,51] showed no significant evidence of neurotoxicity. All these years two major questions
are coming trough persistently: is PCI beneficial for SCLC and also is PCI neurotoxic?
Pedersen et al. [52] in a thorough review among 715 patients states that the incidence of
central nervous system relapse in those not receiving PCI was 22% versus 6% in those receiving
irradiation. However the neurological sequelae for a PCI course of 30Gy in ten fractions ranges from
0-12.5%, when chemotherapy is administered concomitant with the PCI. In table 4, the fractionation
and the neurological toxicity of several PCI courses are shown. There are articles emphasizing the
impact of radiotherapy schedule to the incidence of neurotoxicity by means of a critical value of 3
Gy per fraction and up to 30 Gy for total dose [39,41]. Moreover, the toxicity rate after PCI is rather
minimized in the first year of follow-up [41]. Additionally, previous studies suggested that the
concurrent chemotherapy in conjunction with total radiation dose more than 30 Gy in the brain might
affect higher function modifications [47,48,53,54]. Along with this, the younger the patient, the
greater the side effects of the treatment [44,55-59].
Radiotherapy in lung cancer. Dr. V. Kouloulias
10
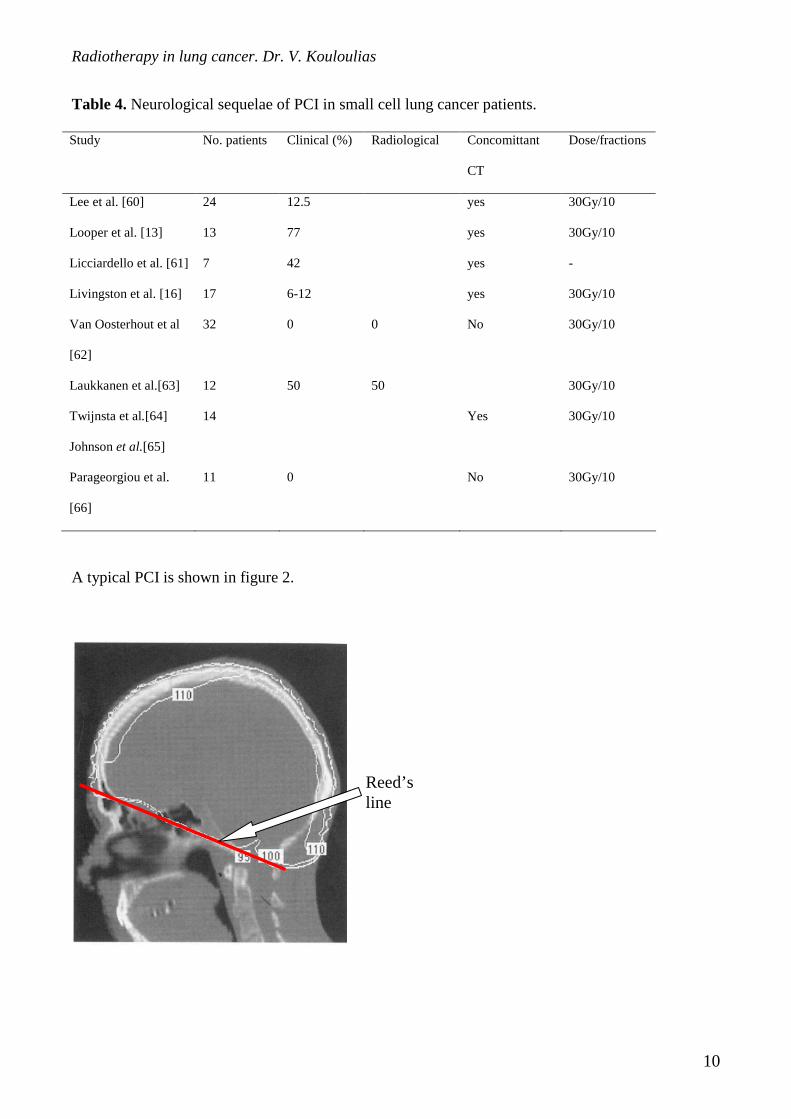
Table 4. Neurological sequelae of PCI in small cell lung cancer patients.
Study No. patients Clinical (%) Radiological Concomittant
CT
Dose/fractions
Lee et al. [60] 24 12.5 yes 30Gy/10
Looper et al. [13] 13 77 yes 30Gy/10
Licciardello et al. [61] 7 42 yes -
Livingston et al. [16] 17 6-12 yes 30Gy/10
Van Oosterhout et al
[62]
32 0 0 No 30Gy/10
Laukkanen et al.[63] 12 50 50 30Gy/10
Twijnsta et al.[64] 14 Yes 30Gy/10
Johnson et al.[65]
Parageorgiou et al.
[66]
11 0 No 30Gy/10
A typical PCI is shown in figure 2.
Reed’s line
Radiotherapy in lung cancer. Dr. V. Kouloulias
11
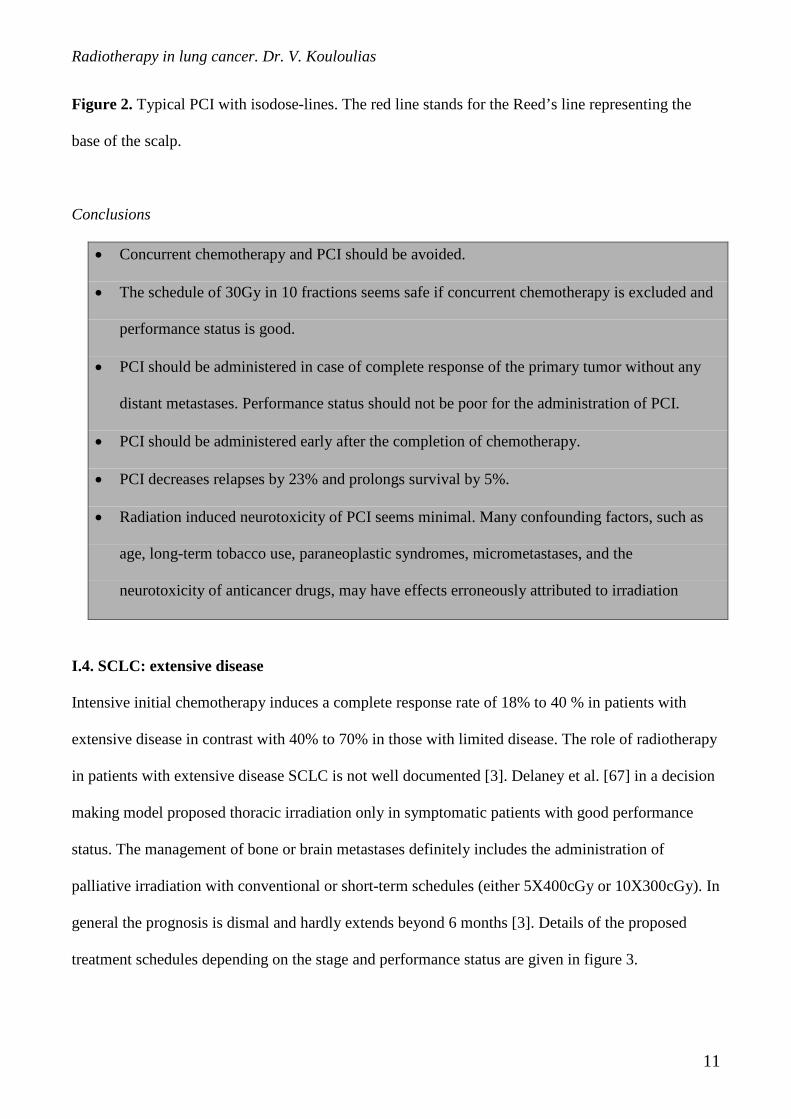
Figure 2. Typical PCI with isodose-lines. The red line stands for the Reed’s line representing the
base of the scalp.
Conclusions
• Concurrent chemotherapy and PCI should be avoided.
• The schedule of 30Gy in 10 fractions seems safe if concurrent chemotherapy is excluded and
performance status is good.
• PCI should be administered in case of complete response of the primary tumor without any
distant metastases. Performance status should not be poor for the administration of PCI.
• PCI should be administered early after the completion of chemotherapy.
• PCI decreases relapses by 23% and prolongs survival by 5%.
• Radiation induced neurotoxicity of PCI seems minimal. Many confounding factors, such as
age, long-term tobacco use, paraneoplastic syndromes, micrometastases, and the
neurotoxicity of anticancer drugs, may have effects erroneously attributed to irradiation
I.4. SCLC: extensive disease
Intensive initial chemotherapy induces a complete response rate of 18% to 40 % in patients with
extensive disease in contrast with 40% to 70% in those with limited disease. The role of radiotherapy
in patients with extensive disease SCLC is not well documented [3]. Delaney et al. [67] in a decision
making model proposed thoracic irradiation only in symptomatic patients with good performance
status. The management of bone or brain metastases definitely includes the administration of
palliative irradiation with conventional or short-term schedules (either 5X400cGy or 10X300cGy). In
general the prognosis is dismal and hardly extends beyond 6 months [3]. Details of the proposed
treatment schedules depending on the stage and performance status are given in figure 3.
Radiotherapy in lung cancer. Dr. V. Kouloulias
12
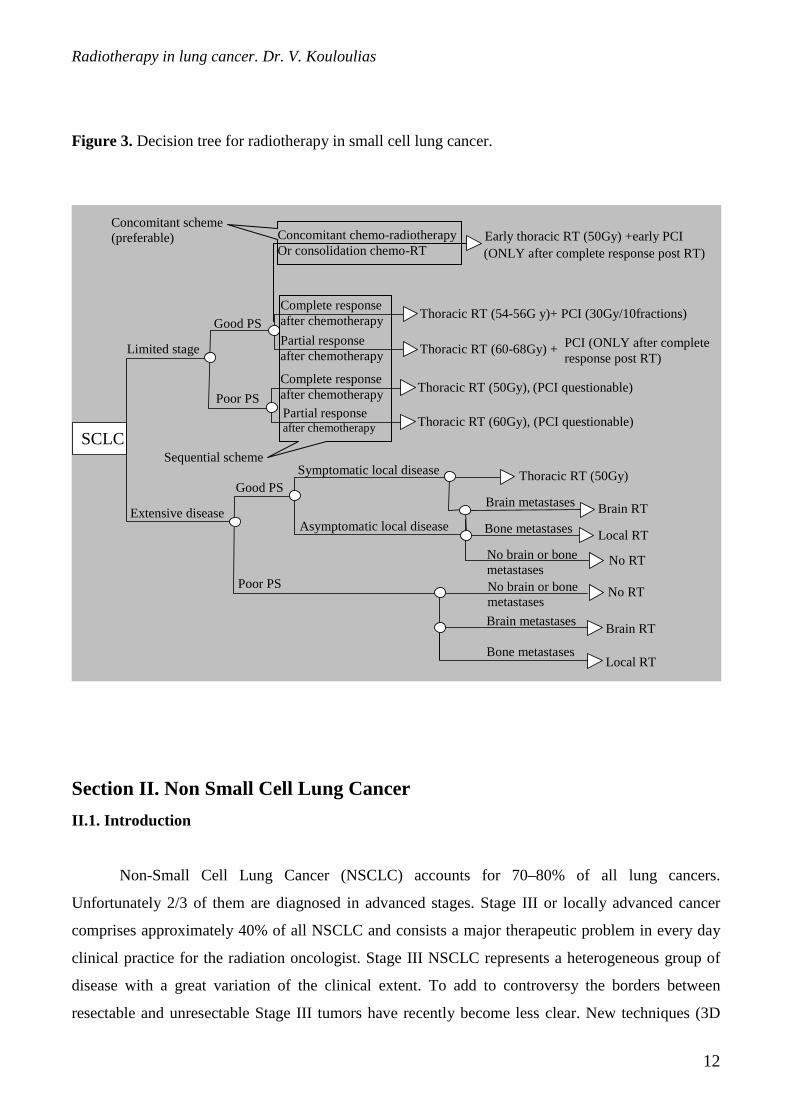
Figure 3. Decision tree for radiotherapy in small cell lung cancer.
Section II. Non Small Cell Lung Cancer
II.1. Introduction
Non-Small Cell Lung Cancer (NSCLC) accounts for 70–80% of all lung cancers.
Unfortunately 2/3 of them are diagnosed in advanced stages. Stage III or locally advanced cancer
comprises approximately 40% of all NSCLC and consists a major therapeutic problem in every day
clinical practice for the radiation oncologist. Stage III NSCLC represents a heterogeneous group of
disease with a great variation of the clinical extent. To add to controversy the borders between
resectable and unresectable Stage III tumors have recently become less clear. New techniques (3D
SCLC
Limited stage
Good PS
Poor PS
Extensive disease
Good PS
Poor PS
Symptomatic local disease
Thoracic RT (54-56G y)+ PCI (30Gy/10fractions) Complete response after chemotherapy Partial response after chemotherapy
Thoracic RT (60-68Gy) +
Thoracic RT (50Gy), (PCI questionable) Complete response after chemotherapy Partial response after chemotherapy
Thoracic RT (60Gy), (PCI questionable)
Asymptomatic local disease
Brain metastases Brain RT
No RT
No brain or bone metastases
Bone metastases
No RT
Local RT
Brain metastases
Bone metastases
Brain RT
Local RT
Thoracic RT (50Gy)
No brain or bone metastases
PCI (ONLY after complete response post RT)
Concomitant chemo-radiotherapy Or consolidation chemo-RT
Early thoracic RT (50Gy) +early PCI (ONLY after complete response post RT)
Concomitant scheme (preferable)
Sequential scheme

Radiotherapy in lung cancer. Dr. V. Kouloulias
13
conformal), fractionation schedules (hyperfractionation, CHART etc), combined Chemotherapy-
Radiotherapy (CHT-RT) have been tried with encouraging results, although long term results are not
available yet.
II.2. Postoperative adjuvant radiotherapy
Generally, postoperative radiotherapy has been advocated for positive or close surgical margins. The
definitions of positive/close or clear margins are rather arbitrary. If tumor cells are found in the
surgical margins these are called positive. If less than 0.5cm of normal tissue is present adjacent to
the tumor edge, the surgical margin is usually considered close. More than 1cm of normal tissue is
considered a clear margin. In situations of not clear margins a course of 60 to 66 Gy (2Gy/fraction) is
usually recommended. If during thoracotomy, a complete and thorough resection of mediastinal
nodes is performed and all nodes are negative, then the portal of irradiation should encompass only
the tumor bed with 1.5-2cm safety margins due to respiratory movements.
It is generally agreed that in patients after complete resection and with clear margins as well
as without nodal involvement (T1N0, T2N0), no adjuvant postoperative treatment is needed. Van
Houtte et al. [68] in a randomized trial with 222 patients (T1,2N0) with complete resection, no
beneficial effect of postoperative irradiation was noted. However, there are conflicting reports on the
beneficial effect of postoperative irradiation in patients with N1 disease. Ferguson et al. [69] reported
on 34 patients with T1,2N1 with a 10% survival for surgery alone and 40% for postoperative
radiation therapy. On the other hand Martini et al. [70] reported negative results with 45% for
surgery alone and 13% for postoperative radiotherapy. Recommendations for N2 patients are less
controversial. The Lung Cancer Study Group (LCSG) [71] reported in 1986 the results of
randomized trial in patients with stage II to III epidermoid carcinoma of the lung after complete
resection receiving either postoperative radiotherapy or no treatment. The postoperative radiotherapy
significantly reduced the rate of local recurrence but without any benefit to survival. In general the
causes of controversy for postoperative radiotherapy concerning the randomized trials are mainly due
to the following: lack of proper selection of patients, lack of uniformity in anatomic description of
nodal regions or nodal surgical resection, lack of uniformity in radiotherapeutic target volume or
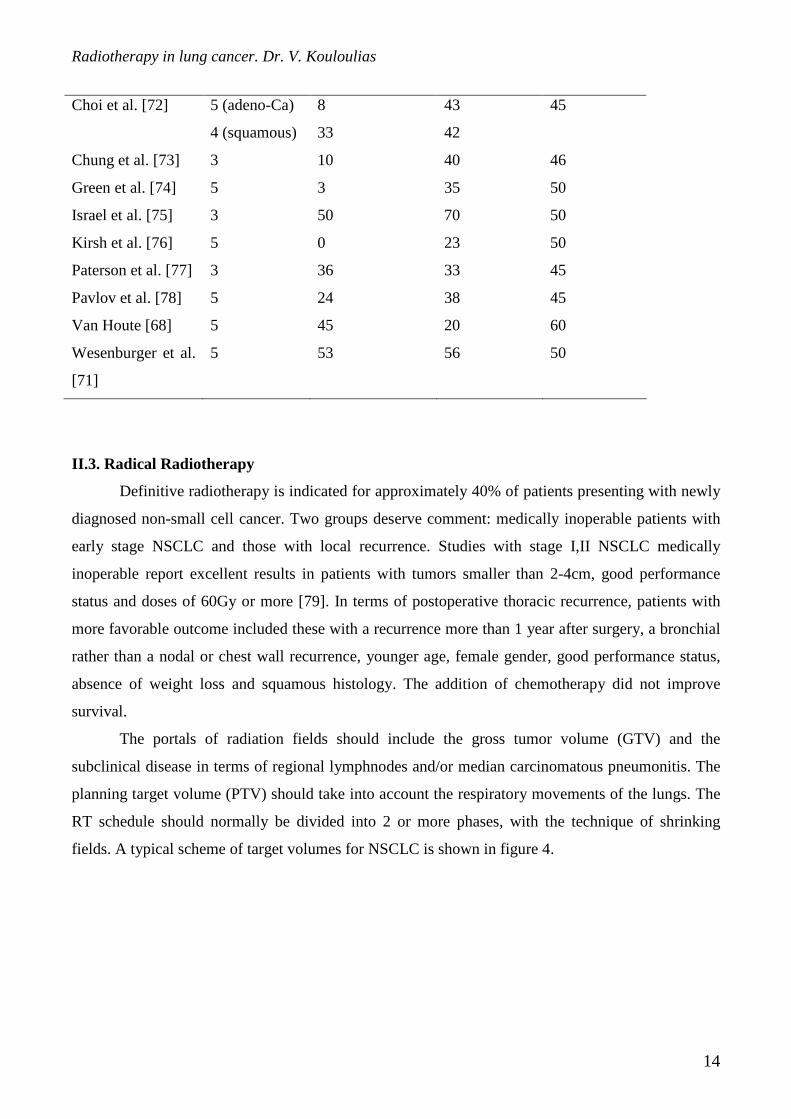
radiation dose. The survival with postoperative irradiation in NSCLC is shown in table 5.
Table 5. Survival with postoperative irradiation in NSCLC.
Survival rate (%) Median dose
Study Years Surgery alone Radiotherapy (Gy)
Radiotherapy in lung cancer. Dr. V. Kouloulias
14
Choi et al. [72] 5 (adeno-Ca)
4 (squamous)
8
33
43
42
45
Chung et al. [73] 3 10 40 46
Green et al. [74] 5 3 35 50
Israel et al. [75] 3 50 70 50
Kirsh et al. [76] 5 0 23 50
Paterson et al. [77] 3 36 33 45
Pavlov et al. [78] 5 24 38 45
Van Houte [68] 5 45 20 60
Wesenburger et al.
[71]
5 53 56 50
II.3. Radical Radiotherapy
Definitive radiotherapy is indicated for approximately 40% of patients presenting with newly
diagnosed non-small cell cancer. Two groups deserve comment: medically inoperable patients with
early stage NSCLC and those with local recurrence. Studies with stage I,II NSCLC medically
inoperable report excellent results in patients with tumors smaller than 2-4cm, good performance
status and doses of 60Gy or more [79]. In terms of postoperative thoracic recurrence, patients with
more favorable outcome included these with a recurrence more than 1 year after surgery, a bronchial
rather than a nodal or chest wall recurrence, younger age, female gender, good performance status,
absence of weight loss and squamous histology. The addition of chemotherapy did not improve
survival.
The portals of radiation fields should include the gross tumor volume (GTV) and the
subclinical disease in terms of regional lymphnodes and/or median carcinomatous pneumonitis. The
planning target volume (PTV) should take into account the respiratory movements of the lungs. The
RT schedule should normally be divided into 2 or more phases, with the technique of shrinking
fields. A typical scheme of target volumes for NSCLC is shown in figure 4.
Radiotherapy in lung cancer. Dr. V. Kouloulias
15
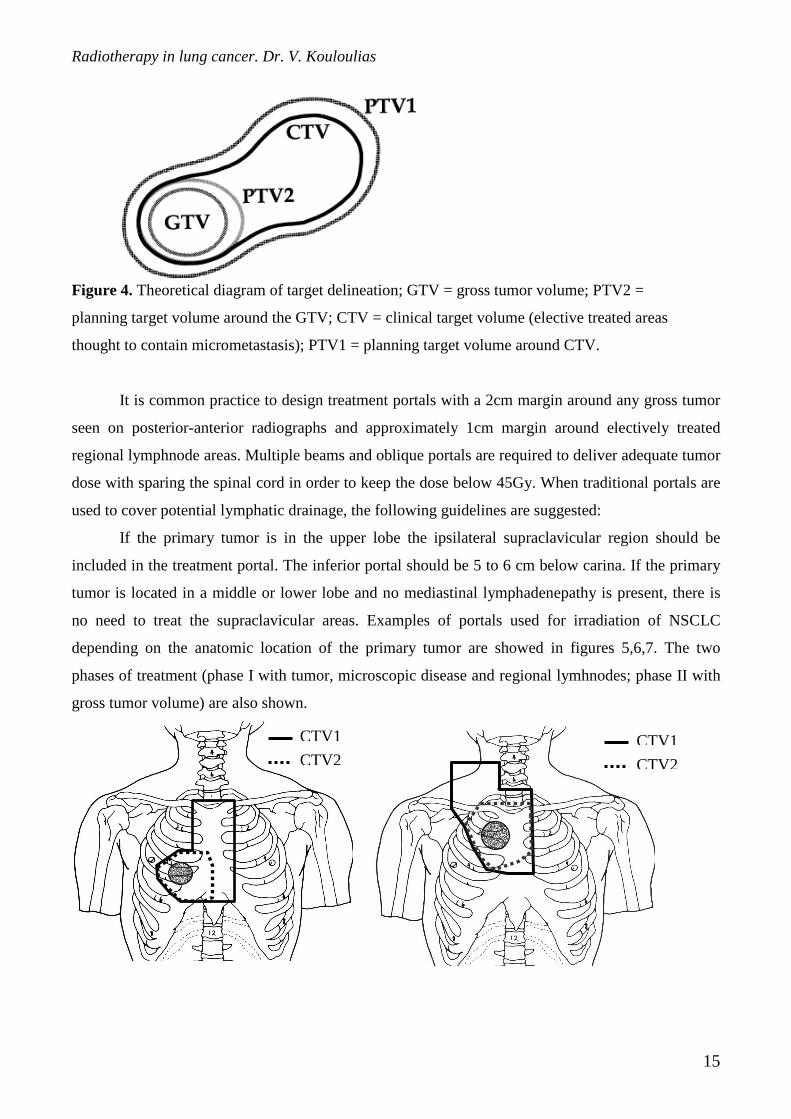
Figure 4. Theoretical diagram of target delineation; GTV = gross tumor volume; PTV2 =
planning target volume around the GTV; CTV = clinical target volume (elective treated areas
thought to contain micrometastasis); PTV1 = planning target volume around CTV.
It is common practice to design treatment portals with a 2cm margin around any gross tumor
seen on posterior-anterior radiographs and approximately 1cm margin around electively treated
regional lymphnode areas. Multiple beams and oblique portals are required to deliver adequate tumor
dose with sparing the spinal cord in order to keep the dose below 45Gy. When traditional portals are
used to cover potential lymphatic drainage, the following guidelines are suggested:
If the primary tumor is in the upper lobe the ipsilateral supraclavicular region should be
included in the treatment portal. The inferior portal should be 5 to 6 cm below carina. If the primary
tumor is located in a middle or lower lobe and no mediastinal lymphadenepathy is present, there is
no need to treat the supraclavicular areas. Examples of portals used for irradiation of NSCLC
depending on the anatomic location of the primary tumor are showed in figures 5,6,7. The two
phases of treatment (phase I with tumor, microscopic disease and regional lymhnodes; phase II with
gross tumor volume) are also shown.
CTV2
CTV1
CTV2
CTV1
Radiotherapy in lung cancer. Dr. V. Kouloulias
16
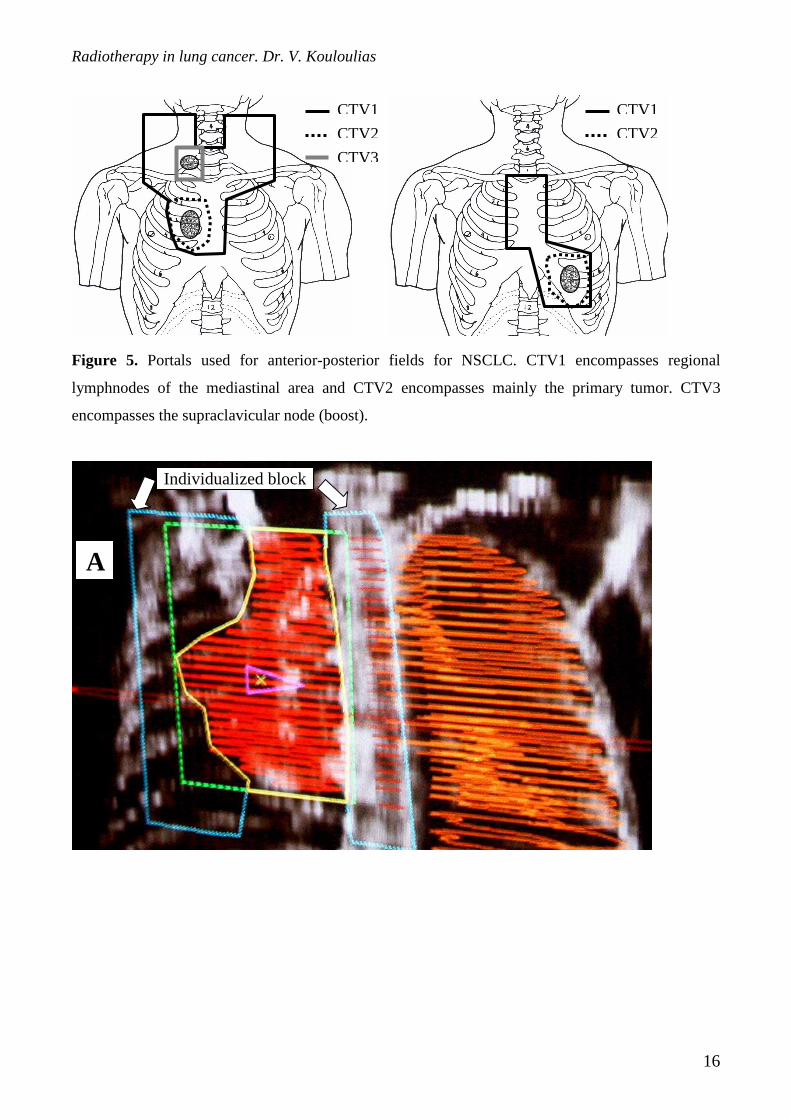
Figure 5. Portals used for anterior-posterior fields for NSCLC. CTV1 encompasses regional
lymphnodes of the mediastinal area and CTV2 encompasses mainly the primary tumor. CTV3
encompasses the supraclavicular node (boost).
CTV2
CTV1
CTV3
CTV2
CTV1
Individualized block
A
Radiotherapy in lung cancer. Dr. V. Kouloulias
17
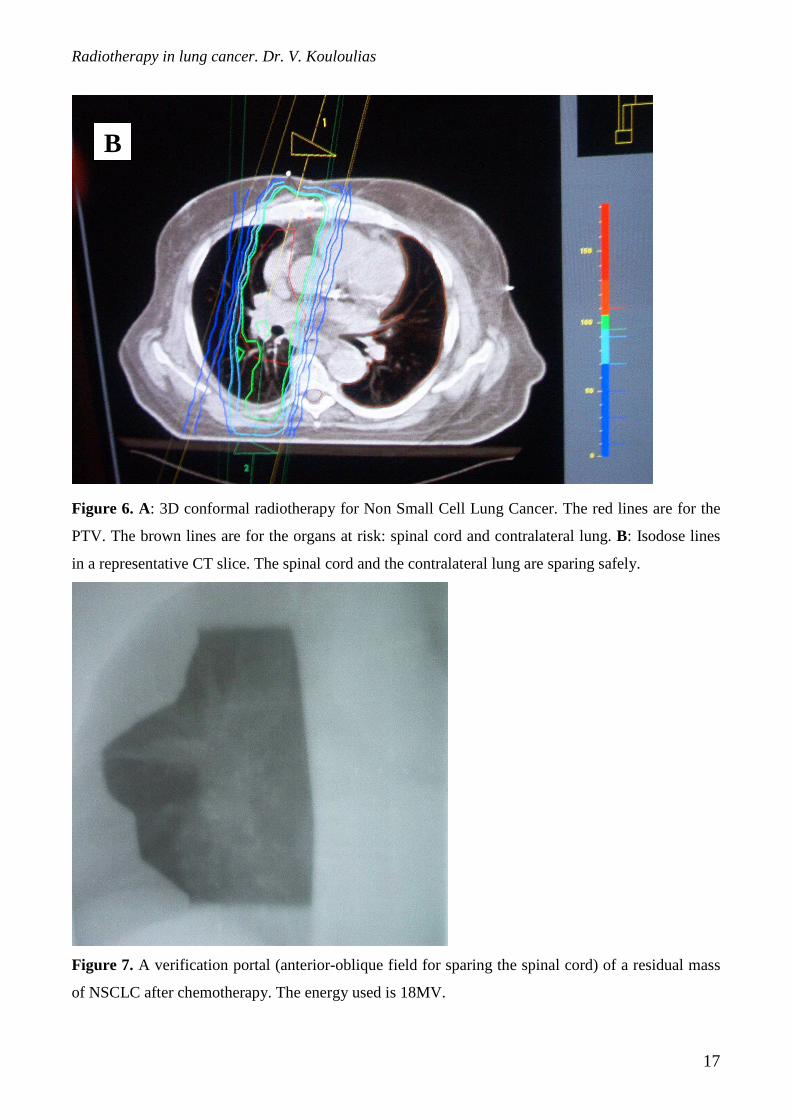
Figure 6. A: 3D conformal radiotherapy for Non Small Cell Lung Cancer. The red lines are for the
PTV. The brown lines are for the organs at risk: spinal cord and contralateral lung. B: Isodose lines
in a representative CT slice. The spinal cord and the contralateral lung are sparing safely.
Figure 7. A verification portal (anterior-oblique field for sparing the spinal cord) of a residual mass
of NSCLC after chemotherapy. The energy used is 18MV.
B
Radiotherapy in lung cancer. Dr. V. Kouloulias
18
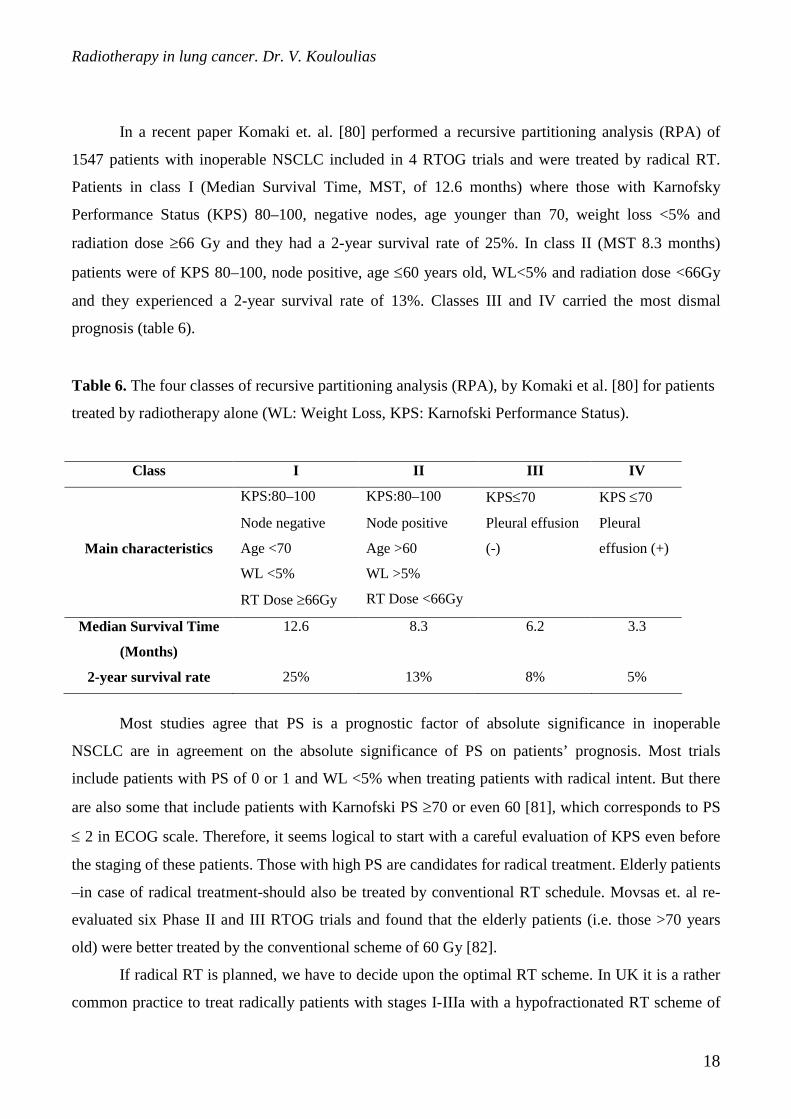
In a recent paper Komaki et. al. [80] performed a recursive partitioning analysis (RPA) of
1547 patients with inoperable NSCLC included in 4 RTOG trials and were treated by radical RT.
Patients in class I (Median Survival Time, MST, of 12.6 months) where those with Karnofsky
Performance Status (KPS) 80–100, negative nodes, age younger than 70, weight loss <5% and
radiation dose ≥66 Gy and they had a 2-year survival rate of 25%. In class II (MST 8.3 months)
patients were of KPS 80–100, node positive, age ≤60 years old, WL<5% and radiation dose <66Gy
and they experienced a 2-year survival rate of 13%. Classes III and IV carried the most dismal
prognosis (table 6).
Table 6. The four classes of recursive partitioning analysis (RPA), by Komaki et al. [80] for patients
treated by radiotherapy alone (WL: Weight Loss, KPS: Karnofski Performance Status).
Class I II III IV
KPS:80–100 KPS:80–100 KPS≤70 KPS ≤70
Main characteristics
Node negative
Age <70
WL <5%
RT Dose ≥66Gy
Node positive
Age >60
WL >5%
RT Dose <66Gy
Pleural effusion
(-)
Pleural
effusion (+)
Median Survival Time
(Months)
12.6 8.3 6.2 3.3
2-year survival rate 25% 13% 8% 5%
Most studies agree that PS is a prognostic factor of absolute significance in inoperable
NSCLC are in agreement on the absolute significance of PS on patients’ prognosis. Most trials
include patients with PS of 0 or 1 and WL <5% when treating patients with radical intent. But there
are also some that include patients with Karnofski PS ≥70 or even 60 [81], which corresponds to PS
≤ 2 in ECOG scale. Therefore, it seems logical to start with a careful evaluation of KPS even before
the staging of these patients. Those with high PS are candidates for radical treatment. Elderly patients
–in case of radical treatment-should also be treated by conventional RT schedule. Movsas et. al re-
evaluated six Phase II and III RTOG trials and found that the elderly patients (i.e. those >70 years
old) were better treated by the conventional scheme of 60 Gy [82].
If radical RT is planned, we have to decide upon the optimal RT scheme. In UK it is a rather
common practice to treat radically patients with stages I-IIIa with a hypofractionated RT scheme of
Radiotherapy in lung cancer. Dr. V. Kouloulias
19
20 fractions, while patients with ‘bulky’ stage IIIa,b are usually treated with palliative intent [83].
For this group of patients radical RT is not recommended in UK outside randomized clinical trials. In
the USA more radical treatments are usually given even for those with bulky disease. The ‘golden
standard’ of 60 Gy in 30 fractions is useful, however all authors agree that higher doses are needed to
eradicate NSCLC; on the other hand a higher incidence of morbidity is associated with a dose above
60 Gy given by conventional fractionation. In some studies dose escalation has a positive impact on
tumor control; promising results have been reported by Armstrong et al from the 3D conformal RT
for NSCLC (median dose 70.2 Gy); the authors propose that total dose increase, results in a better
outcome (MST 15.7 months and 2-year survival rate 32%) [84]. 3D conformal RT demands for high-
tec equipment, although in some centers, special techniques have been developed; Wurstbauer et al.
[85] described an interesting technique (target splitting by asymmetric collimation) which can be
easily applied by departments without available 3D planning systems.
Indication exists that some subtypes of NSCLC proliferate rapidly with a potential doubling
time of about 5 days. So there is a clear need for these tumors to be treated by a high dose in a
shorter total treatment time. Such RT schemes are termed accelerated fractionation.
RTOG 83 11 was a phase II dose escalation trial in which patients were randomized to
receive total doses of 60, 64.8, 74.4, and 79.2 Gy hyperfractionated. This trial suggested that there
was a favorable subgroup with good PS, WL<5% and received total dose of greater than 69.6 Gy
[86].
The published CHART-lung trial [87] reported 2-year survival rates of 20% for standard RT
of 60 Gy/30 fr., and 29% for the CHART arm. In the subgroup of patients with non-squamous cell
histology, the conventional RT resulted in a better 2-year survival of 27 vs. 21%, but it did not reach
statistical significance. Some authors have criticized the inclusion of stage I and II patients (30 and
7% respectively). These earlier stage patients frequently had unfavorable features such as older age,
coincidental disease, etc; all patients had to be of PS 0.1. A modified CHART scheme, the
CHARTWELL (weekend less) i.e. 60 Gy in 18 days is currently being tested [88]. The option for
CHT given with CHART is also considered [87].
II.4. Chemoirradiation
Combined chemotherapy and radiation is now considered the treatment of choice for locally
advanced inoperable non-small cell lung cancer in patients with good performance status and
absence of weight loss. The results of most randomized trials showed the superiority of sequential
chemo-radiotherapy or combined chemo-radiotherapy versus radiotherapy alone [3]. Trials that
Radiotherapy in lung cancer. Dr. V. Kouloulias
20
failed to show a difference in survival did not use cisplatin-based chemotherapy or gave low doses of
irradiation [89,90].
Despite the promising results of modified fractionation schemes both local control and distant
metastases rate are far from satisfactory. Therefore combined modality treatment is being
investigated. Chemotherapy is administered as inductive, alternating, concurrent or various
combinations with RT. A meta-analysis with updated data on individual patients, involving 52
randomized clinical trials has recently been published. Trials comparing RT with RT plus CHT gave
a 13% reduction in the risk of death (absolute benefit of 4% at 2 years) [91]. Numerous other trials
advocate the combination of RT-CHT reporting acceptable toxicities (table 6) while the few trials
reporting negative results have been criticized [92,93]. The majority of these trials include patients
with KPS of ≥70. Komaki et.al. compared the three arms of trials RTOG 88–08/ECOG 4588 and
they concluded that the addition of chemotherapy decreases the risk of distant metastases and
increases survival for non-squamous NSCLC; survival rates were similar among the treatment arms
for patients with squamous-cell carcinomas [94].
Cox et. al. in a similar study performed an evaluation of the influence of chemotherapy on
therapeutic result of the combined treatments for various histologies of stage III NSCLC [95]. They
analyzed data from 4 RTOG RT-alone studies (1415 patients) and 5 RTOG combined- treatment
studies (350 patients). The main conclusions were very important:
Conclusions
• Patients with low PS should be treated by short-term palliative RT courses
• Chemotherapy reduces distant metastases in all types of NSCLC
• Chemotherapy has different effects on the primary tumor by cell type
• Chemotherapy has no effect on the development of brain metastases
• Squamous cell carcinomas should be approached in a different manner than the other
histological types. Dose escalation studies from the radiotherapeutic point of view might be
the key point
• The high risk of brain metastases in patients with non squamous-cell NSCLC probably
justifies the use of prophylactic cranial irradiation in these patients.
Similar conclusions are drawn by Movsas et al. [83], who have re-evaluated the 979 patients
treated in 6 prospective Phase II and III clinical trials from 1982 to 1995. Treatment regimens ranged
from conventional, to hyperfractionated (69.6 Gy), induction chemotherapy plus conventional RT,
Radiotherapy in lung cancer. Dr. V. Kouloulias
21
induction+concomitant+conventional RT, etc. Patients with low KPS (50–70) had the lowest MST
(7.8 months), patients <70 years of age had improved survival with the use of aggressive therapy,
while those with >70 years of age were better treated by the conventional schedule. A dramatic
improvement was seen in patients with squamous cell histology who received induction+concomitant
chemotherapy plus conventional RT (median survival 25.7 months).
Trials RTOG 88 08 and ECOG 45 88 [96] compared in a three arm study conventional RT,
induction chemotherapy – conventional RT and hyperfractionated. The 2-year survival rates were
20%, 31% and 24% and the MST 11.4, 13.6 and 12.3 months respectively. There was a consistent
difference between radiation alone and chemo-irradiation that was statistically significant (log-rank p
= 0.05), while hyperfractionated RT was better than conventional RT at every time point but
differences were not statistically significant. Primary tumor was equally controlled with the use of
either induction chemotherapy or hyperfractionated RT. Distant metastases were less for chemo-
irradiation compared to RT alone groups. Survival rates were similar among the treatment arms for
patients with squamous cell neoplasms. Among patients with non-squamous histologies, failure
patterns did not differ by treatment group, but survival was significantly better in those treated by
induction chemotherapy (p = 0.04).
Jeremic et. al. [97] have reported a significant improvement in median survival time (MST)
and 2-year survival probability for patients treated with hyperftactionated RT plus weekly concurrent
chemotherapy (VP16, Carboplatin). The arm treated by hyperfractionated RT only gave results
similar to that given by the RTOG 83 11 trial. Toxicity of combined treatment was acceptable. None
patient died of treatment related toxicity. The same authors conducted a second trial with two arms
[98]. Hyperfractionated RT in a dose of 69.6 Gy was given in both, while chemotherapy was given to
the second arm, but it was administered in a more continuous way on each RT day and using a lower
dose per administration. The combined treatment arm experienced a MST of 22 months and a 2-year
survival of 43% vs 14 months and 26% in the RT alone arm. The problem of controlling distant
metastases remains. The additional use of intensive sequential chemotherapy should be considered.
Komaki et.al. studied two different combinations of RT and chemotherapy in a randomized trial with
two arms [99]. Patients in the first arm were treated with induction chemotherapy followed by
concurrent chemo-irradiation: Vinblastine was administered weekly and cisplatin on days
1.29.50.71.92; RT started on day 50. 63 Gy were given in 34 fractions/7 weeks. In the second arm,
patients received concurrent chemo-irradiation: RT started on day 1 and a total dose of 69.6 Gy /58
fr. was given. DDP was given in days 1 and 8 and VP16 was given during the first 10 days. Patients
had to be of PS ≥70 and WL<5%.The first arm showed greater haematologic toxicity while the

Radiotherapy in lung cancer. Dr. V. Kouloulias
22
second greater acute and late esophageal toxicity. The MST was 15.5 and 14.4 months respectively;
1-year survival 65% and 58% and 2-year survival were approximately 28% for each arm.
Therapeutic outcome was similar for both groups and similar in absolute numbers to the ‘concurrent’
arms of other trials (table 2) [100–103]. The ‘every-two-weeks’ concurrent chemo-irradiation was
tested in a trial conducted by Blanke et. el. [104]. The MST and 2-year survival rates were similar
between arms of RT, and chemo-RT (table 7). The alternating hyperfractionated RT – chemotherapy
(rather similar to the above-mentioned schedule) was tested in GOTHA I and II trials [105], giving
an MST of 13.6 months and 2-year survival of 27% with acceptable toxicity. The rates were better
than those reported by Blanke et.al., although the study included patients with KPS of 70–100.
The reported results in terms of 2-year survival rates are rather in favor of lower daily doses
of chemotherapeutic agents. In this way chemotherapeutic agents seem to behave like
radiosensitizers. Nevertheless such a regimen failed to control effectively distant metastases. To
improve overall survival further, additional use of CHT should also be considered in future
randomized clinical trials.
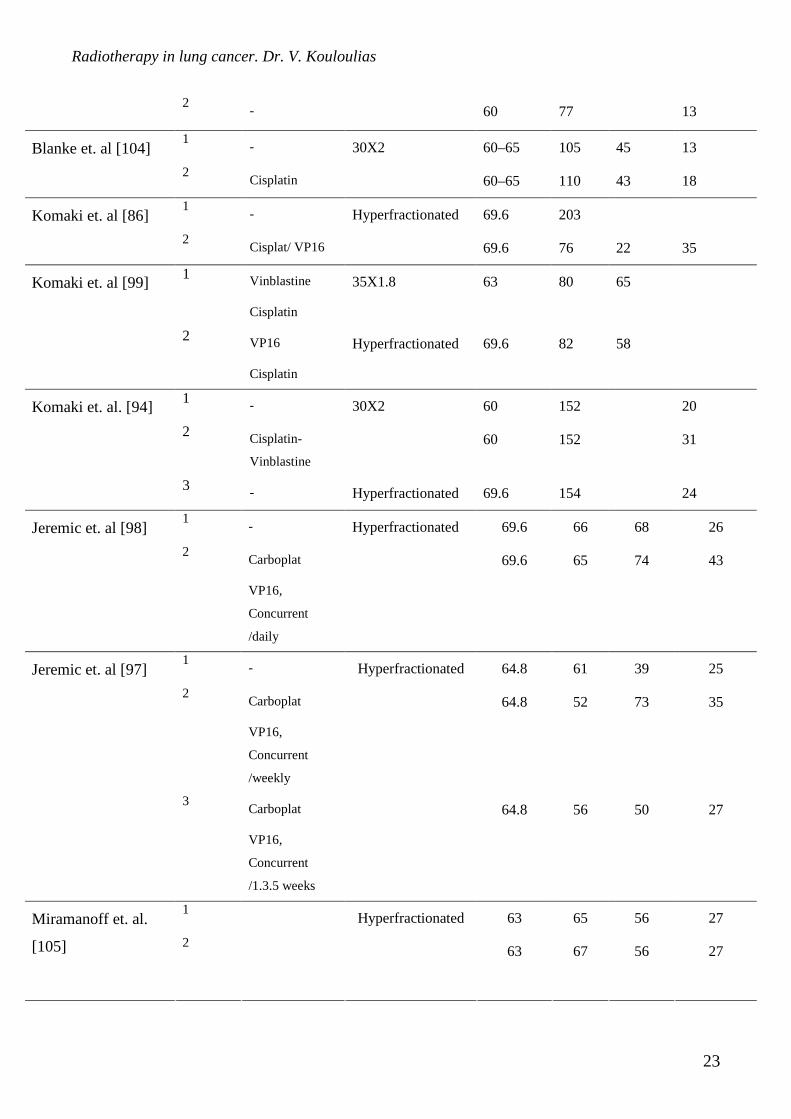
Table 7. Trials of combined chemotherapy-radiotherapy (CHT-RT).
CHT: Chemotherapy, CONC: Concurrent, IND: Induction, ALT: Alternating, STD: Standard (30x2Gy),
ACCEL: Accelerated,
AUTHORS ARMS CHT RT SCHEME RT DOSE Nm
Patient
s
1-year
survival
2-year
survival
1 - 50 48 25 Soresi et al. [106]
2 Cisplatin
25X5 50
45 73 40
1 - 55 110 46 13 Schaake-Konig et.
al. [107] 2 Cisplatin
10X3-, 3 week rest-
10x2.5 55 110 54 26
1 - 45 85 Trovo et. al. [92]
2 Cisplatin,
15x3
45 86
1 - 65 177 14 Arriagada et. al.
[100] 2 VCPC
26X2.5
65 176 21
Dillman et. al. [101] 1
Cisplatin
Vinblastine
30X2 60 78 26
Radiotherapy in lung cancer. Dr. V. Kouloulias
23
2
- 60 77 13
1 - 60–65 105 45 13 Blanke et. al [104]
2 Cisplatin
30X2
60–65 110 43 18
1 - 69.6 203 Komaki et. al [86]
2 Cisplat/ VP16
Hyperfractionated
69.6 76 22 35
1 Vinblastine
Cisplatin
35X1.8 63 80 65 Komaki et. al [99]
2 VP16
Cisplatin
Hyperfractionated 69.6 82 58
1 - 60 152 20
2 Cisplatin-
Vinblastine
30X2
60 152 31
Komaki et. al. [94]
3 - Hyperfractionated 69.6 154 24
1 - 69.6 66 68 26 Jeremic et. al [98]
2 Carboplat
VP16,
Concurrent
/daily
Hyperfractionated
69.6 65 74 43
1 - 64.8 61 39 25
2 Carboplat
VP16,
Concurrent
/weekly
64.8 52 73 35
Jeremic et. al [97]
3 Carboplat
VP16,
Concurrent
/1.3.5 weeks
Hyperfractionated
64.8 56 50 27
1 63 65 56 27 Miramanoff et. al.
[105]
2
Hyperfractionated
63 67 56 27
Radiotherapy in lung cancer. Dr. V. Kouloulias
24
1 Vinblast
+Cis-plat
60 120 54 26 Clamon et. al. [102]
2 Vinblast+Cis-
platine +carbo
30X2
60 130 56 29
1 NO 30X2 60 225 21
2 NO CHART 54 338 30
Saunders et. al. [88]
CHART 2
_ Hyperfractionated 63.9 50 60 18
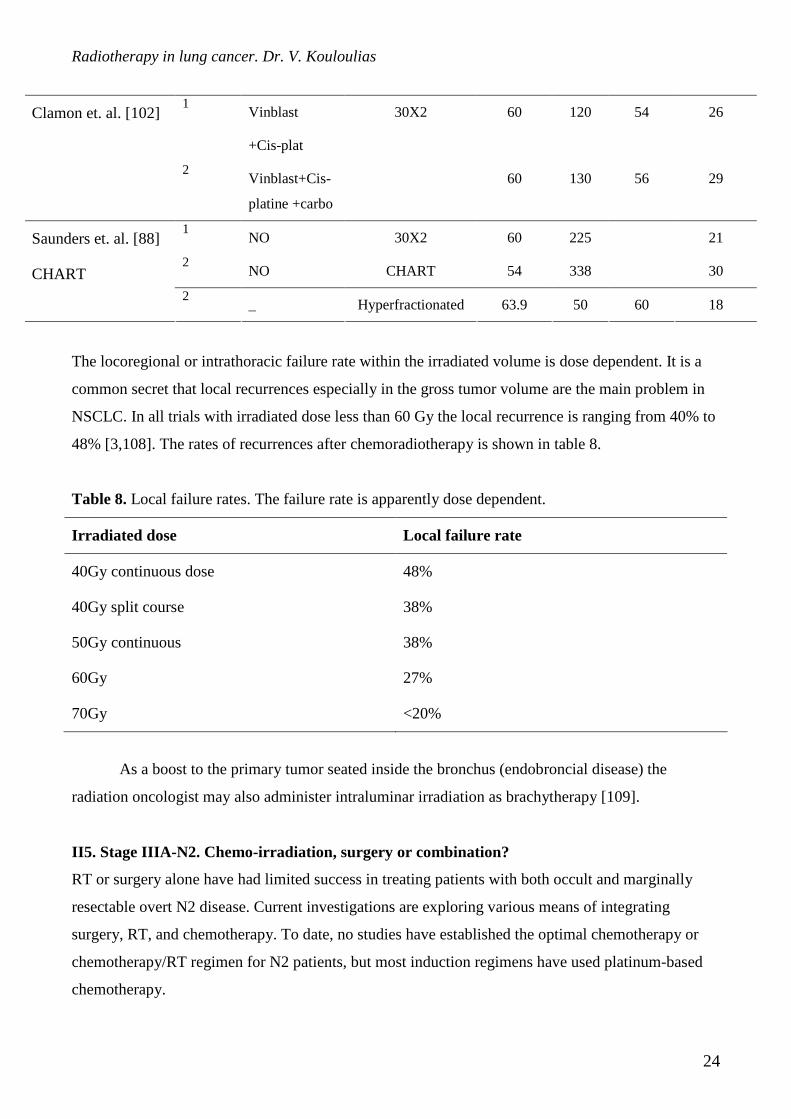
The locoregional or intrathoracic failure rate within the irradiated volume is dose dependent. It is a
common secret that local recurrences especially in the gross tumor volume are the main problem in
NSCLC. In all trials with irradiated dose less than 60 Gy the local recurrence is ranging from 40% to
48% [3,108]. The rates of recurrences after chemoradiotherapy is shown in table 8.
Table 8. Local failure rates. The failure rate is apparently dose dependent.
Irradiated dose Local failure rate
40Gy continuous dose 48%
40Gy split course 38%
50Gy continuous 38%
60Gy 27%
70Gy <20%
As a boost to the primary tumor seated inside the bronchus (endobroncial disease) the
radiation oncologist may also administer intraluminar irradiation as brachytherapy [109].
II5. Stage IIIA-N2. Chemo-irradiation, surgery or combination?
RT or surgery alone have had limited success in treating patients with both occult and marginally
resectable overt N2 disease. Current investigations are exploring various means of integrating
surgery, RT, and chemotherapy. To date, no studies have established the optimal chemotherapy or
chemotherapy/RT regimen for N2 patients, but most induction regimens have used platinum-based
chemotherapy.
Radiotherapy in lung cancer. Dr. V. Kouloulias
25
In the only other trial comparing surgical and nonsurgical treatment in this setting, Shepherd
and associates [110] have reported a randomized trial of chemotherapy plus surgery vs. RT alone for
biopsy-proven Stage IIIA NSCLC. Thirty-one patients were randomized. The median survival was
16.2 and 18.7 months for RT alone and chemotherapy plus surgery, respectively, with no
improvement in long-term survival seen with combined-modality surgical treatment.
Do any other data suggest that RT with or without chemotherapy is a reasonable alternative to
surgery with or without chemotherapy? A common conception is that RT alone is significantly
inferior to surgery alone for N2 disease. However, N2 patients referred for RT are not a comparable
group of patients to those who undergo surgery; such patients are usually rejected for surgery
because of disease bulk or medical contraindications. Accordingly, few RT data are available for a
surgically suitable group of N2 patients. The existing evidence suggests that hyperfractionated RT to
69.6 Gy in 6 weeks yields survival results surprisingly close to those for surgery. On analysis of
completed RTOG lung trials using RT alone, a group of patients was identified that had clinical N2
disease, favorable prognostic factors (Karnofsky performance score >70, and <5% weight loss), and
a T-stage distribution similar to surgical series. For standard fractionation RT, the 3-year survival
rate was only 7%, but for hyperfractionated RT it was 20% [111]. This result is similar to that in
several of the surgical series [112-113]. There will not likely ever be a direct comparison of RT and
surgery for N2 disease. [114]. Thus, even with the best locoregional treatment, one could not expect
to control the disease in more than 40% of patients. For patients with overt N2 involvement, even if
nonbulky, the risk of systemic disease is even higher, and locoregional treatment alone would fail in
90% of patients.
Some promising results have come from two small Phase III trials of chemotherapy induction
followed by surgery, with and without RT. The median survival in the first study was 26 months for
induction chemotherapy followed by surgery and RT and was 8 months without induction
chemotherapy [115]. In the second study, the median survival had not yet been reached using
induction chemotherapy followed by surgery compared with 18 months for surgery alone [116].
Moreover, Arriagada et al. [117] in a well documented meta-analysis concluded that there was no
effect of postoperative radiotherapy in patients with N2 disease, while there was no doubt for the
deleterious effect of post-RT in N0,N1 patients. These results sugest that the optimum scheme of
combined treatment for N2 patients is the following: chemo-irradiation (up to 50Gy) and in case or
respectability, then surgery. In case of unresectability, then chemotherapy in consolidation therapy.
Conclusions

Radiotherapy in lung cancer. Dr. V. Kouloulias
26
• Radiotherapy after chemotherapy and surgery for N2 patients is not recommended.
• Concomitant chemo-irradiation ±surgery might be the treatement of choice
• The dose of pre-operative radiotherapy should not exceed 50Gy.
II.6. In the context of chemoradiotherapy: sequential, concomitant, induction or consolidation
chemotherapy?
Cancer and Leukemia Group B (CALGB) study 8433 compared induction chemotherapy consisting
of cisplatin and vinblastine followed by daily radiation to daily radiation alone [101]. The induction
chemotherapy-containing arm showed improvement in median survival from 9.7 to 13.8 months. The
benefit of sequential induction chemotherapy followed by daily radiation was confirmed in an inter-
group trial (RTOG 8808, ECOG 4588, SWOG 8992) [118]. Sequential chemoradiotherapy appears
to improve survival by lowering the rate of systemic relapse and does not appear to improve local
control compared to radiotherapy alone [119]. Concomitant chemoradiotherapy also improves
survival compared to radiation alone and appears to improve survival primarily by improving local
control [120].
Sequential or concurrent chemotherapy added to daily radiation has now been compared in
phase III randomized trials. A trial by the West Japan Group compared sequential full dose
mitomycin, vindesine and cisplatin followed by daily radiation to a dose of 56 Gy to the same
chemotherapy given concurrently with a split course of daily radiation to a dose of 56 Gy [119]. The
concomitant therapy arm had a median survival of 16.5 months compared to 14.2 months in the
sequential treatment arm. Radiation Therapy Oncology Group (RTOG) trial 9410 compared
sequential versus concomitant chemotherapy as used in CALGB 8433 added to daily radiation of 2
Gy to a total dose of 60 Gy [120]. The third arm of RTOG 9410 was concomitant cisplatin and oral
etoposide with twice-daily radiation of 1.2 Gy to a total dose of 69.6 Gy. Median survival was 17
months for concomitant chemotherapy with daily radiation versus 14.6 months for sequential therapy
(P=0.038) and 15.6 months for concomitant chemotherapy and twice daily radiation. A French
randomized phase III trial compared sequential chemoradiotherapy consisting of cisplatin and
vinorelbine followed by radiation to 66 Gy to concurrent chemoradiotherapy with cisplatin and
etoposide followed by cisplatin and vinorelbine and reported a trend toward improved survival for
the concurrent therapy arm [121]. A Czech randomized phase II trial comparing sequential versus
concurrent chemoradiotherapy with cisplatin and vinorelbine showed a median survival of 396 and
619 days, respectively [122]. The results of these studies suggest that the current standard of care
should be concomitant platinum-based chemotherapy and once daily radiation for patients with good

Radiotherapy in lung cancer. Dr. V. Kouloulias
27
performance status. Patients with poor performance status, significant weight loss or pleural effusion
were excluded from RTOG 9410 and there have been no randomized trials comparing sequential to
concurrent chemoradiotherapy in that group of patients. Adding full dose chemotherapy to eradicate
occult micrometastases before or after concomitant chemoradiotherapy that improves local control
has the potential to improve survival in locally advanced NSCLC.
Giving full dose systemic chemotherapy prior to concomitant chemoradiotherapy treats
micrometastatic disease immediately before it has the opportunity to progress or become resistant to
the lower doses of chemotherapy that are typically given concomitantly with radiation. In addition
compared to consolidation therapy, induction chemotherapy is delivered at a time when the patient
will better tolerate side effects and bone marrow suppression. CALGB 9431 is a randomized phase II
trial in which all patients received two cycles cisplatin based induction doublet chemotherapy and 2
cycles of cisplatin based doublet chemotherpay concurrent with daily radiation 2 Gy per fraction to a
total dose 66 Gy [123]. Patients were randomized to receive gemcitabine, paclitaxel or navelbine as
the second chemotherapeutic agent. The median survival for all patients was 17 months and there
was no clear superiority to any of the recent generation chemotherapy agents. A phase II trial that
evaluated induction chemotherapy with paclitaxel and carboplatin followed by concomitant
chemoradiotherapy with weekly paclitaxel, carboplatin and conformal radiation therapy to a dose of
74 Gy had a median survival of 26 months with 1-, 2-, 3- and 4-year survival rates of 71, 52, 40, and
36%, respectively [124]. CALGB 30105 is an ongoing randomized phase II trial with one arm being
the above regimen and the other consisting of induction carboplatin and gemcitabine followed by
concomitant chemoradiation with twice weekly gemcitabine 35 mg/m2 also with conformal thoracic
radiation to a dose of 74 Gy.
Beginning therapy with concomitant chemoradiotherapy utilizes what appears to be the most
important component of the combination immediately before the often bulky local tumor can become
larger or become chemoradioresistant. Southwest Oncology Group (SWOG) 9019 gave concurrent
chemoradiation with cisplatin and etoposide followed by consolidation with 2 cycles of cisplatin and
etoposide. In 50 patients with stage IIIB NSCLC the median survival was 15 months [125]. SWOG
9504 used the same concomitant chemoradiotherapy as SWOG 9019 but replaced two cycles of
cisplatin and etoposide consolidation with two cycles of docetaxel. SWOG 9504 had an encouraging
median survival of 27 months, with 1- and 2-year survivals of 76 and 53%, respectively [126].
The Locally Advanced Multimodality Project or LAMP trial is a randomized phase II trial with three
arms of paclitaxel and carboplatin chemoradiation: arm 1 induction chemotherapy followed by
radiotherapy alone, arm 2 induction chemotherapy followed by concomitant chemoradiotherapy, and
arm 3 concomitant chemoradiotherapy followed by consolidation [127]. The reported median

Radiotherapy in lung cancer. Dr. V. Kouloulias
28
survivals for the three arms of the LAMP trial are arm one 13 months, arm two 12.8 months, and arm
three 16.1 months.
Conclusions
• Chemoradiotherapy is superior to radiation alone for locally advanced unresectable stage III.
NSCLC.
• Concomitant chemoradiotherapy appears to be superior to sequential chemoradiotherapy for
good performance status patients.
• Encouraging results from phase II trials suggest that induction or consolidation chemotherapy
added to concomitant chemoradiation may improve outcome
II.6. Superior vena cava syndrome
Superior vena cava syndrome is a medical emergency that requires immediate therapeutic action.
The syndrome is produced by extrinsic compression of the superior vena cava or intracaval
thrombosis which is seen in approximately 40-50% of patients with this syndrome. Although it is
generally believed that these patients have an extremely poor prognosis approximately 10% - 20%
survive longer than 2 years [128]. Therefore in the absence of distant metastases, aggressive
management and support are indicated. Radiotherapy should be initiated as soon as possible. Patients
should initially be given high dose fractions (4Gy per fraction) for 2-3 days, followed by
conventional radiotherapy [129]. The recommended total dose for patients with localized
bronchogenic carcinoma should be 60-70Gy while in patients with malignant lymphoma should be
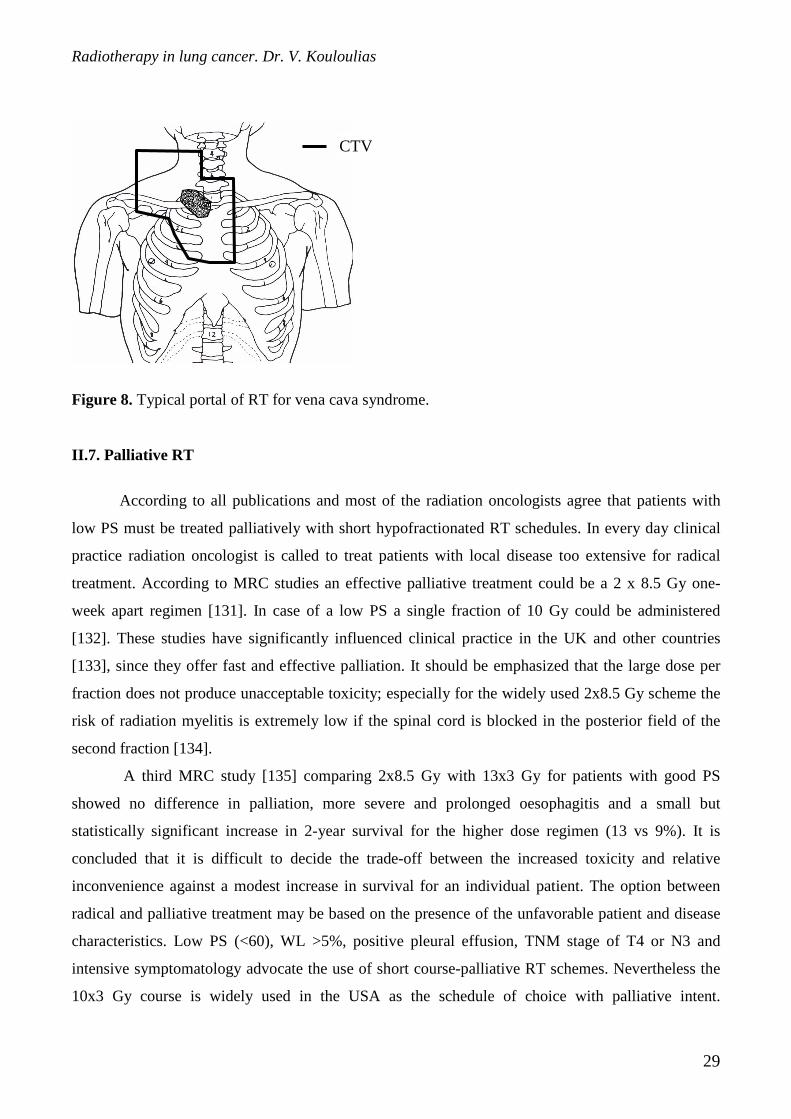
40-45Gy. Radiation therapy portals (fig. 8) should include the mediastinal, hilar, supraclavicular
nodal areas and any adjacent parenchymal pulmonary lesions.
Alternatively, superior vena cava syndrome secondary to malignant disease is preferentially
treated by endovascular stenting with highly palliative effect [130]. Adjuvantly, external beam
radiation and/or chemotherapy would also be administered for tumor mass reduction.
Radiotherapy in lung cancer. Dr. V. Kouloulias
29
Figure 8. Typical portal of RT for vena cava syndrome.
II.7. Palliative RT
According to all publications and most of the radiation oncologists agree that patients with
low PS must be treated palliatively with short hypofractionated RT schedules. In every day clinical
practice radiation oncologist is called to treat patients with local disease too extensive for radical
treatment. According to MRC studies an effective palliative treatment could be a 2 x 8.5 Gy one-
week apart regimen [131]. In case of a low PS a single fraction of 10 Gy could be administered
[132]. These studies have significantly influenced clinical practice in the UK and other countries
[133], since they offer fast and effective palliation. It should be emphasized that the large dose per
fraction does not produce unacceptable toxicity; especially for the widely used 2x8.5 Gy scheme the
risk of radiation myelitis is extremely low if the spinal cord is blocked in the posterior field of the
second fraction [134].
A third MRC study [135] comparing 2x8.5 Gy with 13x3 Gy for patients with good PS
showed no difference in palliation, more severe and prolonged oesophagitis and a small but
statistically significant increase in 2-year survival for the higher dose regimen (13 vs 9%). It is
concluded that it is difficult to decide the trade-off between the increased toxicity and relative
inconvenience against a modest increase in survival for an individual patient. The option between
radical and palliative treatment may be based on the presence of the unfavorable patient and disease
characteristics. Low PS (<60), WL >5%, positive pleural effusion, TNM stage of T4 or N3 and
intensive symptomatology advocate the use of short course-palliative RT schemes. Nevertheless the
10x3 Gy course is widely used in the USA as the schedule of choice with palliative intent.
CTV
Radiotherapy in lung cancer. Dr. V. Kouloulias
30
Particularly for patients with supraclavicular node metastases (when there is lack of other adverse
prognostic factors) Machtay et al. [136] reported that when treated with modern chemoradiotherapy
these patients appear to have similar prognosis to other stage IIIb patients. Platinum-based
chemotherapy is also recommended for patients with metastatic NSCLC and good performance
status, while short term hypofractionated radiation therapy should also be considered for symptoms
relief in these patients [137].
Conclusions
• CTV to PTV margins are 2cm around GTV and 1cm around regional lymphnodes.
• Spinal cord dose should be kept below 45Gy.
• 3D conformal should be the treatment of choice for irradiation. Traditional anterior-posterior
fields should be used only for phase I of irradiation schedule or palliative radiotherapy.
• The lung volume received dose of 20Gy (V20) should not exceed the 30% of total lung volume
in order to minimize the radiation induced pneumonitis.
• The most important unfavorable characteristics of patients with NSCLC are: low KPS, weight
loss>5%, positive pleural effusion, intensive symptomatology and distant metastases.
• For patients with unresectable stage IIIa,b and a PS of 70–100, a radical treatment should be
given in terms of combined chemo-radiotherapy.
• Results from randomized clinical trials advocate the use of intensive RT (e.g. CHART or
HFXRT).
• In case of radical RT alone the general recommendation is to administer as high dose as
possible in as short as possible overall treatment time.
• The dose of 60 Gy in 30 fractions should be the least therapeutic dose to eradicate such a bulky
disease, while it is the recommended RT schedule for patients over the age of 70 years.
• A high dose hyperfractionated RT scheme, or the CHART (in case of squamous cell
carcinoma) could be employed.
• In all randomized clinical trials it is always reproduced that combined RT+CHT gives better
therapeutic results that RT alone, and that HFX/ACCRT yields better results than STDRT
alone.
• Results from randomized trials advocate the use of combined RT-CHT as a continuous way as
possible. Platinum based chemotherapy can be combined to radiation therapy as inductive,
concurrent or in consolidation.
Radiotherapy in lung cancer. Dr. V. Kouloulias
31
• If the above-mentioned therapeutic modalities are not available a tumor dose of at least 60 Gy
in 6 weeks (or shorter) or its radiobiological equivalent could be employed.
• For patients with PS of 70 with either locally too advanced disease or positive pleural effusion,
a palliative (e.g. 2 x 8.5 Gy or 13 x 3Gy) RT regimen can be given.
• Concurrent CHT+RT and intensified RT schedules (hyperfractionated-accelerated) should be
administered for radical irradiation.
• In terms of 3D conformal, positive are regional lymphnodes with diameter more than 1.5cm
(probability 90% of having pathological involvement).
• The GTV – CTV margins are depending on the histology: 6mm for adenocarcinoma and 8mm
for squamous cell.
• The acute side effects after RT are: acute pneumonitis, acute esophagitis, cough, Lhermitte
syndrome. The management consists of bed/rest-bronchodilators-corticosteroid-O2
(pneumonitis), mucosal anesthetics-liquid antacids (esophagitis), antitusive therapy (cough),
antibiotics (secondary infection), antifungal medication (esophagitis). In severe esophagitis,
nasogastic tube or intravenous hyperalimentation. In severe acute pneumonitis, hospitalization
due to high percent of mortality.
• Spinal cord myelopathy with doses >45
• Esophagitis as a late complication (stenosis, ulceration, perforation, fistula) occurs in 5% or
more of patients with 60Gy dose delivery in esophagus. Very careful with cis-platin combined
with RT, since the previous incidence is higher.
• Doxorubicin plus RT have synergistic effect with RT for the induction of cardiotoxicity.
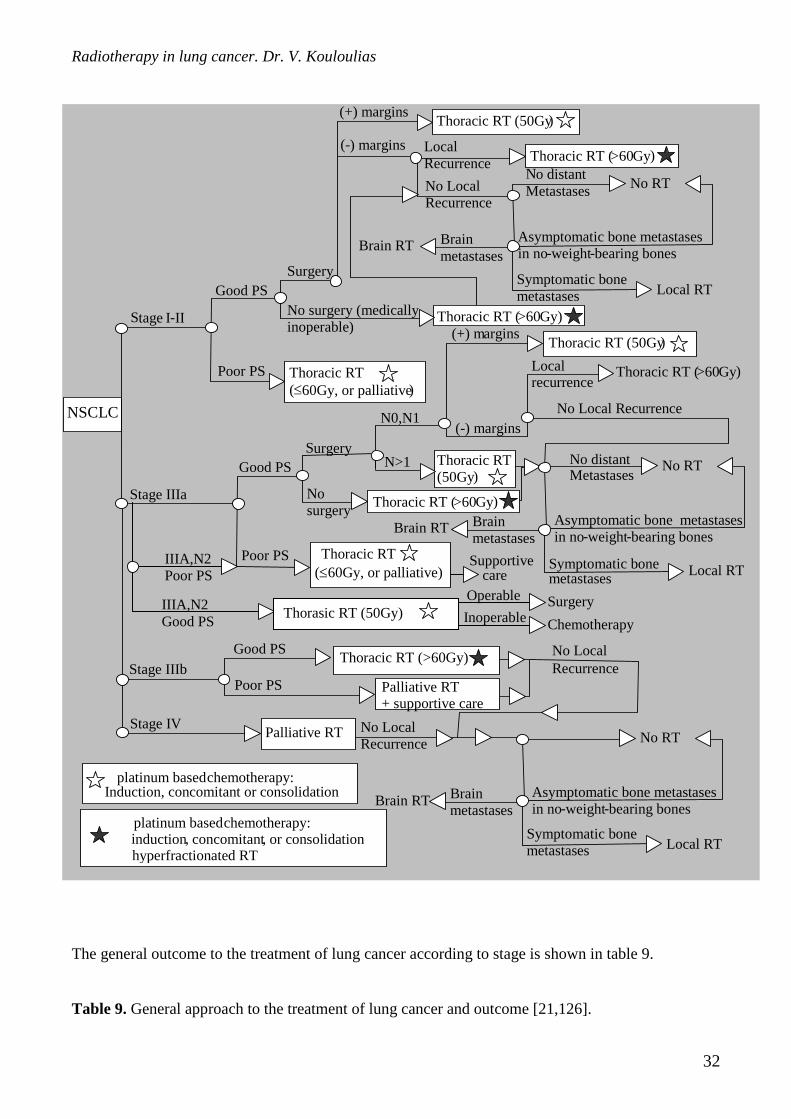
Figure 9. Decision tree for radiotherapy in non small cell lung cancer [3,125].
Radiotherapy in lung cancer. Dr. V. Kouloulias
32
The general outcome to the treatment of lung cancer according to stage is shown in table 9.
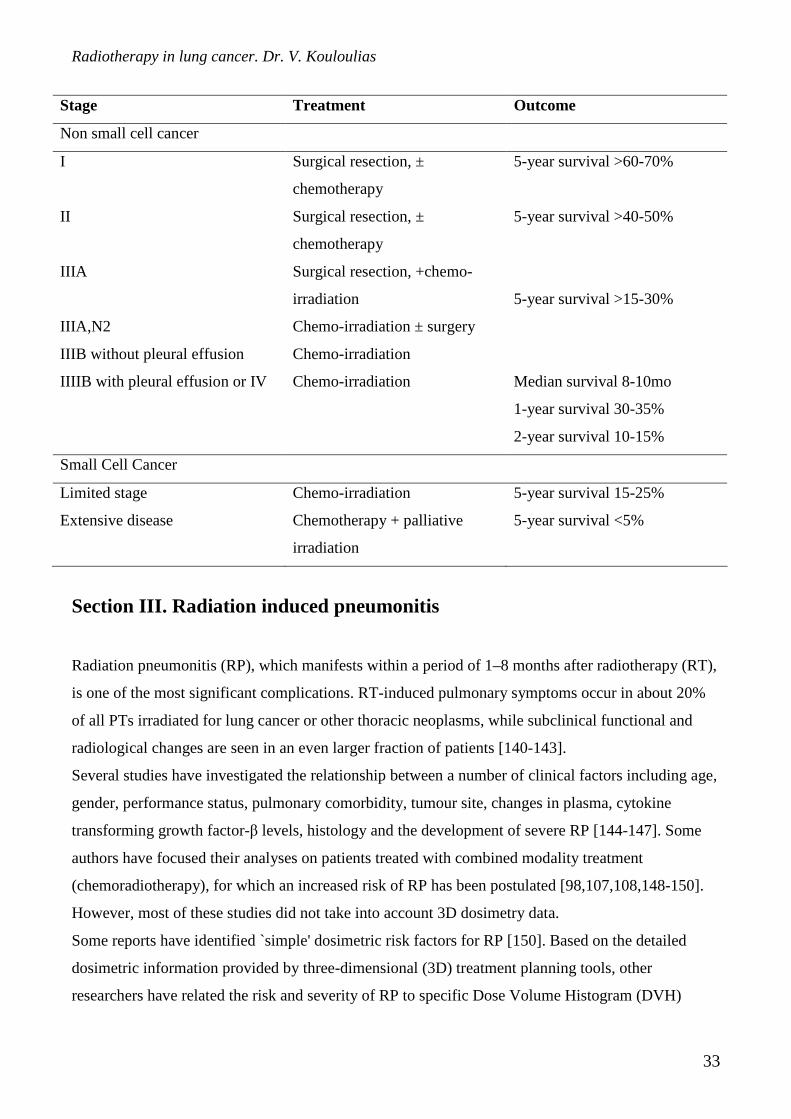
Table 9. General approach to the treatment of lung cancer and outcome [21,126].
Local recurrence
NSCLC
S tage I - II
Good PS
Poor PS
Stage IIIa
Good PS
Poor PS
S urgery
Thoracic RT (50Gy )
Surgery
No surgery (medically inoperable)
Thoracic RT ( >60 Gy)
No surgery
Good PS
Palliative RT
Stage IIIb Thoracic RT (>60Gy)
Palliative RT + supportive care
Poor PS
Stage IV
(+) margins
( - ) margins Local Recurrence Thoracic RT ( >60 Gy )
No Local Recurrence
N o distant Metastases
No RT
Asymptomatic bone metastases in no - weight - bearing bones Symptomatic bone metastases Local RT
Brain metastases
Brain RT
Thoracic RT ( ≤ 60Gy, or palliative )
N0,N1
(+) m argins Thoracic RT (50Gy )
(-) margins
Thoracic RT ( >60 Gy )
No Local Recurrence
No distant Metastases No RT
Asymptomatic bone metastases in no - weight - bearing bones
Local RT
Brain metastases
Brain RT
Thoracic RT (50Gy )
N>1
Symptomatic bone metastases
Thoracic RT ( >60 Gy )
Thoracic RT
(≤60Gy, or palliative)
No Local Recurrence
No RT
Asymptomatic bone metastases in no - weight - bearing bones
Symptomatic bone metastases Local RT
Brain metastases
Brain RT
No Local Recurrence
platinum based chemotherapy: Induction, concomitant or consolidation
platinum based chemotherapy: i nduction , concomitant , or consolidation hyperfractionated RT
Supportive care
Thorasic RT (50Gy) Surgery IIIA,N2
Good PS
IIIA,N2 Poor PS
Operable Inoperable Chemotherapy
Radiotherapy in lung cancer. Dr. V. Kouloulias
33
Stage Treatment Outcome
Non small cell cancer
I Surgical resection, ±
chemotherapy
5-year survival >60-70%
II Surgical resection, ±
chemotherapy
5-year survival >40-50%
IIIA Surgical resection, +chemo-
irradiation
IIIA,N2 Chemo-irradiation ± surgery
IIIB without pleural effusion Chemo-irradiation
5-year survival >15-30%
IIIIB with pleural effusion or IV Chemo-irradiation Median survival 8-10mo
1-year survival 30-35%
2-year survival 10-15%
Small Cell Cancer
Limited stage Chemo-irradiation 5-year survival 15-25%
Extensive disease Chemotherapy + palliative
irradiation
5-year survival <5%
Section III. Radiation induced pneumonitis
Radiation pneumonitis (RP), which manifests within a period of 1–8 months after radiotherapy (RT),
is one of the most significant complications. RT-induced pulmonary symptoms occur in about 20%
of all PTs irradiated for lung cancer or other thoracic neoplasms, while subclinical functional and
radiological changes are seen in an even larger fraction of patients [140-143].
Several studies have investigated the relationship between a number of clinical factors including age,
gender, performance status, pulmonary comorbidity, tumour site, changes in plasma, cytokine
transforming growth factor-β levels, histology and the development of severe RP [144-147]. Some
authors have focused their analyses on patients treated with combined modality treatment
(chemoradiotherapy), for which an increased risk of RP has been postulated [98,107,108,148-150].
However, most of these studies did not take into account 3D dosimetry data.
Some reports have identified `simple' dosimetric risk factors for RP [150]. Based on the detailed
dosimetric information provided by three-dimensional (3D) treatment planning tools, other
researchers have related the risk and severity of RP to specific Dose Volume Histogram (DVH)
Radiotherapy in lung cancer. Dr. V. Kouloulias
34
parameters [151-155], and a few studies have characterised the dose–response curve for RP
following RT by means of biological models [156-158].
While there is a number of differences in the published reports, there is some consensus about
the association between a few of the dosimetric factors (mainly the mean lung dose Dmean) and the
incidence of RP [152,159]. Most lung cancer patients showed poor pre-treatment pulmonary function
and among those patients, chronic obstructive pulmonary disease (COPD) was not an uncommon
clinical finding. However, the role of pre-treatment lung function and the influence of covariates
such as chemotherapy agents are still under debate. According to several publications, the incidence
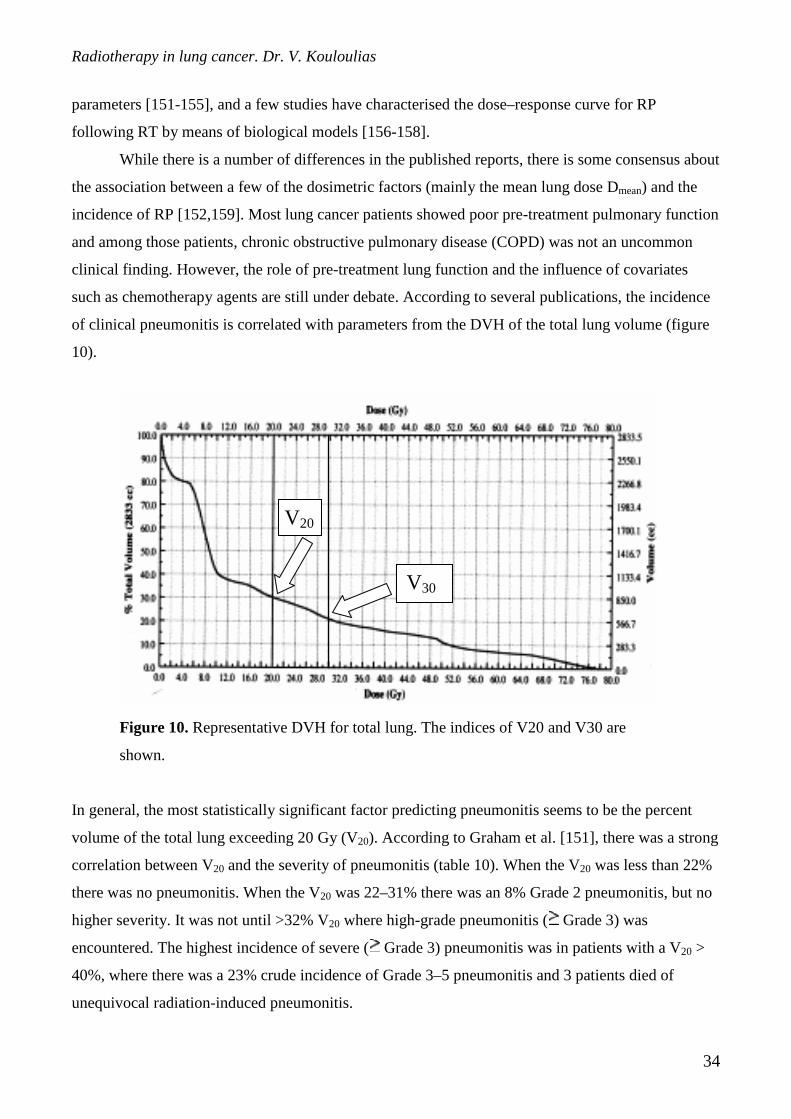
of clinical pneumonitis is correlated with parameters from the DVH of the total lung volume (figure
10).
Figure 10. Representative DVH for total lung. The indices of V20 and V30 are
shown.
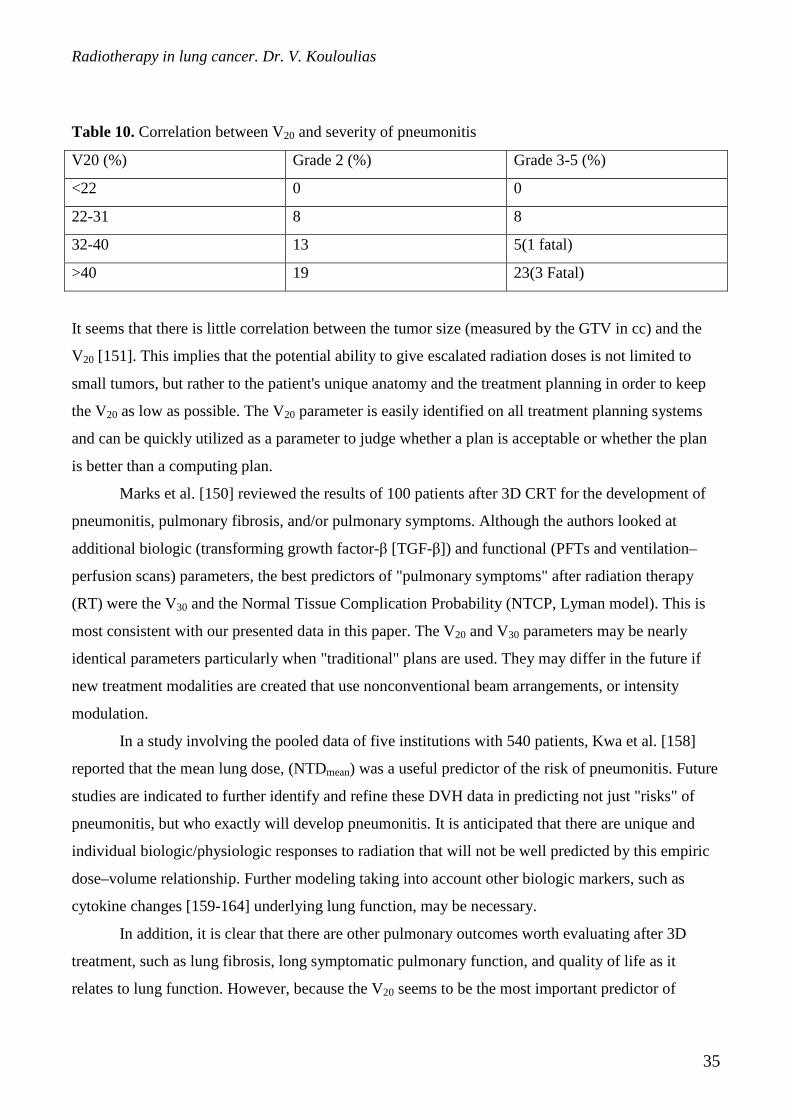
In general, the most statistically significant factor predicting pneumonitis seems to be the percent
volume of the total lung exceeding 20 Gy (V20). According to Graham et al. [151], there was a strong
correlation between V20 and the severity of pneumonitis (table 10). When the V20 was less than 22%
there was no pneumonitis. When the V20 was 22–31% there was an 8% Grade 2 pneumonitis, but no
higher severity. It was not until >32% V20 where high-grade pneumonitis ( Grade 3) was
encountered. The highest incidence of severe ( Grade 3) pneumonitis was in patients with a V20 >
40%, where there was a 23% crude incidence of Grade 3–5 pneumonitis and 3 patients died of
unequivocal radiation-induced pneumonitis.
V30
V20
Radiotherapy in lung cancer. Dr. V. Kouloulias
35
Table 10. Correlation between V20 and severity of pneumonitis
V20 (%) Grade 2 (%) Grade 3-5 (%)
<22 0 0
22-31 8 8
32-40 13 5(1 fatal)
>40 19 23(3 Fatal)
It seems that there is little correlation between the tumor size (measured by the GTV in cc) and the
V20 [151]. This implies that the potential ability to give escalated radiation doses is not limited to
small tumors, but rather to the patient's unique anatomy and the treatment planning in order to keep
the V20 as low as possible. The V20 parameter is easily identified on all treatment planning systems
and can be quickly utilized as a parameter to judge whether a plan is acceptable or whether the plan
is better than a computing plan.
Marks et al. [150] reviewed the results of 100 patients after 3D CRT for the development of
pneumonitis, pulmonary fibrosis, and/or pulmonary symptoms. Although the authors looked at
additional biologic (transforming growth factor-β [TGF-β]) and functional (PFTs and ventilation–
perfusion scans) parameters, the best predictors of "pulmonary symptoms" after radiation therapy
(RT) were the V30 and the Normal Tissue Complication Probability (NTCP, Lyman model). This is
most consistent with our presented data in this paper. The V20 and V30 parameters may be nearly
identical parameters particularly when "traditional" plans are used. They may differ in the future if
new treatment modalities are created that use nonconventional beam arrangements, or intensity
modulation.
In a study involving the pooled data of five institutions with 540 patients, Kwa et al. [158]
reported that the mean lung dose, (NTDmean) was a useful predictor of the risk of pneumonitis. Future
studies are indicated to further identify and refine these DVH data in predicting not just "risks" of
pneumonitis, but who exactly will develop pneumonitis. It is anticipated that there are unique and
individual biologic/physiologic responses to radiation that will not be well predicted by this empiric
dose–volume relationship. Further modeling taking into account other biologic markers, such as
cytokine changes [159-164] underlying lung function, may be necessary.
In addition, it is clear that there are other pulmonary outcomes worth evaluating after 3D
treatment, such as lung fibrosis, long symptomatic pulmonary function, and quality of life as it
relates to lung function. However, because the V20 seems to be the most important predictor of
Radiotherapy in lung cancer. Dr. V. Kouloulias
36
pneumonitis, this implies to us that the volume effect in the development of acute pneumonitis is a
much more important factor than the physiologic lung function and response to radiation of the
affected parts of the lung.
Until further investigations of this nature can be performed, we recommend that the total lung
volume DVH be assessed when evaluating the "goodness" of a 3D radiation plan in the treatment of
NSCLC patients. In the clinic of Carlos Perez, some practical guidelines are used for the routine lung
radiotherapy:
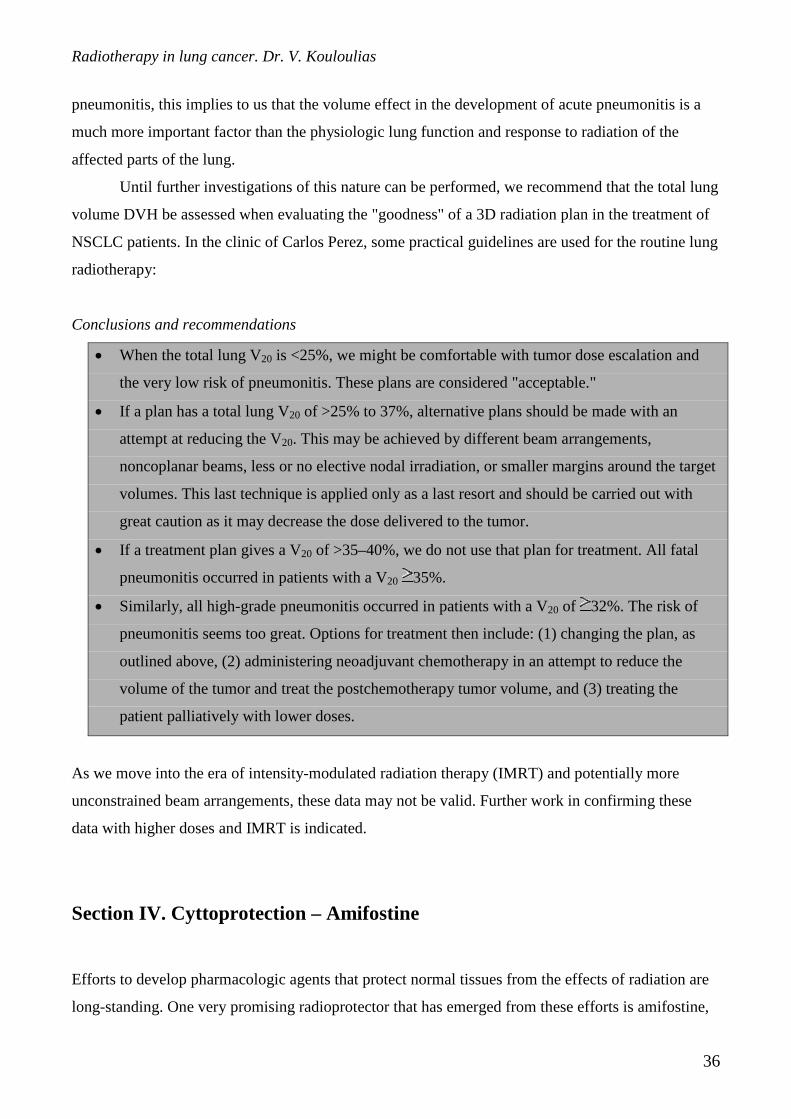
Conclusions and recommendations
• When the total lung V20 is <25%, we might be comfortable with tumor dose escalation and
the very low risk of pneumonitis. These plans are considered "acceptable."
• If a plan has a total lung V20 of >25% to 37%, alternative plans should be made with an
attempt at reducing the V20. This may be achieved by different beam arrangements,
noncoplanar beams, less or no elective nodal irradiation, or smaller margins around the target
volumes. This last technique is applied only as a last resort and should be carried out with
great caution as it may decrease the dose delivered to the tumor.
• If a treatment plan gives a V20 of >35–40%, we do not use that plan for treatment. All fatal
pneumonitis occurred in patients with a V20 35%.
• Similarly, all high-grade pneumonitis occurred in patients with a V20 of 32%. The risk of
pneumonitis seems too great. Options for treatment then include: (1) changing the plan, as
outlined above, (2) administering neoadjuvant chemotherapy in an attempt to reduce the
volume of the tumor and treat the postchemotherapy tumor volume, and (3) treating the
patient palliatively with lower doses.
As we move into the era of intensity-modulated radiation therapy (IMRT) and potentially more
unconstrained beam arrangements, these data may not be valid. Further work in confirming these
data with higher doses and IMRT is indicated.
Section IV. Cyttoprotection – Amifostine
Efforts to develop pharmacologic agents that protect normal tissues from the effects of radiation are
long-standing. One very promising radioprotector that has emerged from these efforts is amifostine,

Radiotherapy in lung cancer. Dr. V. Kouloulias
37
an organic thiophosphate developed by the United States Army (WR [Walter Reed]-2721) in the
post–World War II era to protect against the possible effects of radioactive fallout. The active
metabolite (WR-1065) is a free thiol that is thought to provide an alternative target for reactive
species from alkylating agents that would otherwise target DNA. The free thiol is also believed to
scavenge the free radicals released during the interaction of ionizing radiation and water. With regard
to its tissue selectivity, amifostine has been shown to protect both the salivary glands from the
damaging effects of RT [165] and the kidneys from the nephrotoxic effects of cisplatin [166].
Nonetheless, amifostine's ability to protect normal tissue is not well understood, and the dosage
required to reduce specific toxicities has not been established [167]. However, it appears to protect
normal tissues, including the esophagus, lung, kidney, liver, bone marrow, immune system, skin,
colon, small bowel, salivary glands, oral mucosa, and testes, from radiation damage; the brain and
spinal cord, however, were not protected. In addition, no evidence has shown that it caused tumors to
be spared the effects of RT or chemotherapy. Also in its favor, amifostine has been shown to protect
normal tissues against the toxic effects of several classes of cytotoxic agents, including the alkylating
and organo-platinum agents, anthracyclines, and taxanes [168]. All these qualities, therefore, indicate
amifostine's potentially broad applicability as a cytoprotective agent. Amifostine is already approved
for use as a radioprotector in the United States as the result of an international multi-institutional
Phase III comparative trial that showed a significant reduction in the severity of acute and late
xerostomia in patients given intravenous amifostine before each fraction of RT [165].
Several prospective randomized comparative studies of RT with and without amifostine have been
published all these years. Komaki et al. [169] in a study conducted in M. D. Anderson Cancer Center
reported a significant radioprotective effect of amifostine against radiation induced pneumonitis and
esophagitis. All the randomized studies are shown in table 11.
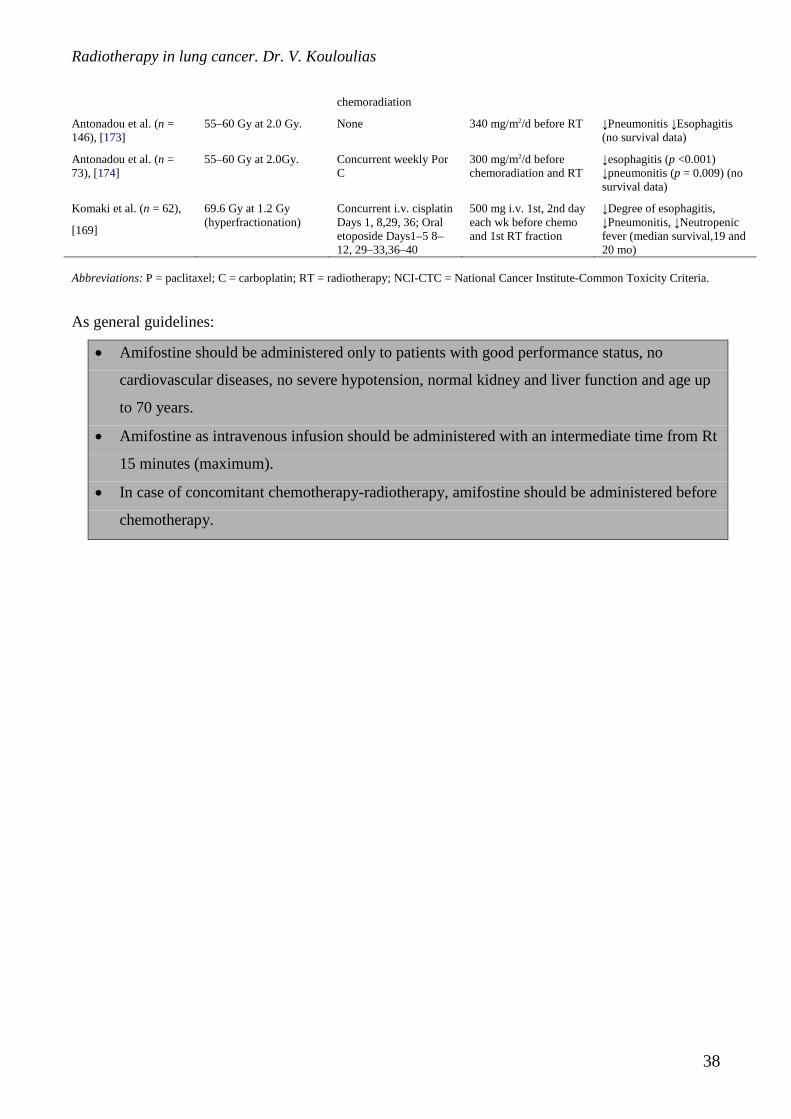
Table 11. Randomized trials with amifostine in lung cancer
Reference Radiation dose Chemotherapy Amifostine dose Comment
Movsas et al. (n = 242)
[170]
69.6 Gy at 1.2 Gy (hyperfractionation)
Induction PC 500 mg i.v. 4_/wk between RT fractions
No difference by NCI-CTC esophagitis, Swallowing diaries (p < 0.03) and weight loss (p < 0.05) favour amifostine (median survival, 15.6 and 15.8 mo)
Leong et al. (n = 60)
[171]
60–66 Gy at 2.0 Gy Induction PC 740 mg/m2 with each
chemo (Days 1, 22, 43, 50, 57,64, 71, 78)
Esophagitis Grade 2–3: 43% in amifostine, 70% in control (not significant) (median survival, 12.5 and 14.5 mo)
Senzer et al. (n = 63)
[172]
64.8 Gy at 1.8 Gy Concurrent PC, gemcitabine and cisplatin X 3 after
500 mg i.v. before weekly chemo; 200 mg i.v. daily before RT
No difference in toxicity, no survival data (ongoing trial)
Radiotherapy in lung cancer. Dr. V. Kouloulias
38
chemoradiation
Antonadou et al. (n = 146), [173]
55–60 Gy at 2.0 Gy. None 340 mg/m2/d before RT ↓Pneumonitis ↓Esophagitis (no survival data)
Antonadou et al. (n = 73), [174]
55–60 Gy at 2.0Gy. Concurrent weekly Por C
300 mg/m2/d before chemoradiation and RT
↓esophagitis (p <0.001) ↓pneumonitis (p = 0.009) (no survival data)
Komaki et al. (n = 62),
[169]
69.6 Gy at 1.2 Gy (hyperfractionation)
Concurrent i.v. cisplatin Days 1, 8,29, 36; Oral etoposide Days1–5 8–12, 29–33,36–40
500 mg i.v. 1st, 2nd day each wk before chemo and 1st RT fraction
↓Degree of esophagitis, ↓Pneumonitis, ↓Neutropenic fever (median survival,19 and 20 mo)
Abbreviations: P = paclitaxel; C = carboplatin; RT = radiotherapy; NCI-CTC = National Cancer Institute-Common Toxicity Criteria.
As general guidelines:
• Amifostine should be administered only to patients with good performance status, no
cardiovascular diseases, no severe hypotension, normal kidney and liver function and age up
to 70 years.
• Amifostine as intravenous infusion should be administered with an intermediate time from Rt
15 minutes (maximum).
• In case of concomitant chemotherapy-radiotherapy, amifostine should be administered before
chemotherapy.
Radiotherapy in lung cancer. Dr. V. Kouloulias
39
References
1. Bleehan N, Bunn P, Cox J. Role of radiation therapy in small cell anaplastic carcinoma of the lung.
Cancer Treat Rep 1983;67:11-19
2. Goodman G, Livingston R. Small cell lung cancer. Curr Probl Cancer. 1989;13:7-55
3. Emami B, Graham M. Lung In: Principles and practice of radiation oncology. Perez C, Brady L.
(eds). Lippincott-Raven Pub. Philadelphia , pp. 1181-1220, 1997
4. Mira J, Livingston R, Moore T. Influence of chest radiotherapy in frequency and patterns of chest
relapse in disseminated SCLC (SWOG study). Cancer 1982;50:1266-1272.
5. Perez C, Einhorn R, Oldham F, et al. Randomized trial of radiotherapy to the thorax in limited SC
carcinoma of the lung treated with multiagent chemotherapy and elective brain irradiation: a
preliminary report. J Clin Oncol 1984;2:1200-1208
6. Perry M, Eaton W, Propert K, Chemotherapy with or without radiation therapy in limited small cell
carcinoma of the lung. N Engl J Med 1987;316:912-918
7. Cohen M. Is thoracic radiation therapy necessary for patients with limited stage small cell lung
cancer? No. Cancer Treat Rep 1983;67:217-221
8. Pignon J, Arriagada R, Ihde D, et al. A meta-analysis of thoracic radiotherapy for small cell lung
cancer. N Engl J Med 1992;327:1618-1624
9. Fox R, Tattersall M, Woods R. Radiation therapy as an adjuvant in small cell lung cancer treated
with combination chemotherapy. A randomized study. Proc Am Soc Clin Oncol 1981;22:502.
10. Bunn P, Lichter A, Makuch R. Chemotherapy alone or chemotherapy with chest radiation therapy
in limited stage small cell lung cancer. Ann Intern Med 1987;106:655-662
11. Osterlind K, Hansen H, Hansen M, et al. Mortality and morbidity in long term surviving patients
treated with chemotherapy with or without irradiation for small cell lung cancer. J Clin Oncol
1986;4: 1044-1052
12. Hansen H, Dombernowsky P, Hansen H. Chemotherapy versus chemotherapy plus radiotherapy in
regional small cell carcinoma of the lung: a randomized trial. Proc Am Soc Clin Oncol.
1979;20:277
13. Looper J, Hornback N. The role of chest irradiation in limited cell carcinoma of the lung treated
with combination chemotherapy. Int J Radiat Oncol Biol Phys. 1984;10:1855-1860
14. Carslon R, Sikic B, Gandara D, et al. Late consolidative radiation therapy in the treatment of
limited stage small cell lung cancer. Cancer 1991;68:948-958
15. Suhami R, Geddes D, Spiro S, et al. Radiotherapy in SCLC. Br Med J 1984;288:1643-1646
Radiotherapy in lung cancer. Dr. V. Kouloulias
40
16. Livingston R, Mira J, Chen T, et al. Combined modality treatment of extensive SCLC: A SWOG
study. J Clin Oncol 1984;2:585-590
17. Kies M, Mira J, Crowely L. Multimodal therapy for limited small cell lung cancer: A randomized
study of induction combination chemotherapy with or without thoracic radiation in complete
responders and with wide-field versus reduced field radiation in partial responders. A SWOG
study. J Clin Oncol 1987;5:592-600
18. Choi N, Carey R, Kaufman D. Small cell carcinoma of the lung: A progress report of 15 years’
experience. Cancer 1987;59:6-14.
19. Greco F, Perez C, Einhorn L. Combination chemotherapy with or without concurrent thoracic
radiotherapy in limited stage SCLC. Proc Am Soc Clin Oncol 1986;5:178
20. Creech R, Richter M, Finkelstein D. Combination chemotherapy with or without consolidation
radiation therapy (RT) for regional small cell carcinoma of the lung. Proc Am Soc Clin Oncol.
1988;7:196
21. Spira A, Ettinger DS. Multidisciplinary management of lung cancer. N Engl J Med.
2004;350:379-92
22. Takada M, Fukuoka M, Kawahara M, et al. Phase II study of concurrent versus sequential thoracic
radiotherapy in combination with cisplatin and etoposide for limited stage small cell lung cancer:
results of the Japan Clinical Oncology Group Study 9104. J Clin Oncol 2002;20:3054-60.
23. Turrisi AT III, Kim K, Blum R, et al. Twice daily compared with once daily thoracic radiotherapy
in limited small cell lung cancer treated concurrently with cisplatin and etoposide. N Engl J Med
1999;340:265-71.
24. Albain KS, Crowley JJ, LeBlanc M, Livingston RB. Determinants of improved outcome in small-
cell lung cancer: an analysis of the 2,580-patient Southwest Oncology Group data base. J Clin
Oncol 1990;8:1563-1574.
25. Arriagada R, Le Chevalier T, Borie F, et al. Prophylactic cranial irradiation for patients with
small-cell lung cancer in complete remission. J Natl Cancer Inst 1995;87:183-190.
26. Hirsch FR, Paulson OB, Hansen HH, Vraa-Jensen J. Intracranial metastases in small cell
carcinoma of the lung: correlation of clinical and autopsy findings. Cancer 1982;50:2433-2437.
27. Matthews, M.J.; Kantiouwa, S.; Pickren, J.; Robinette, D. Frequency of residual and metastatic
tumor in patients undergoing curative surgical resection for lung cancer. Cancer Chemother Rep
1973;4:63-67
28. Hansen, HH. Should initial treatment of small cell carcinoma include systemic chemotherapy and
brain irradiation? Cancer Chemother Rep 1973;4:239-241
Radiotherapy in lung cancer. Dr. V. Kouloulias
41
29. Jackson, D.V.; Richards, F.; Cooper, R.; Ferree, C.; Muss, H.B.; White, D.R.; Spurr, CL.
Prophylactic cranial irradiation in small cell carcinoma of the lung. JAMA 1977;237:2730-2733
30. Beiler, D.D.; Kane, R.C.; Bernath, A.M.; Cashdollar, M.R. Low dose elective brain irradiation in
small cell carcinoma of the lung. Int J Radiat Oncol Biol Phys 1979;5:941-945
31. Maurer, L.H, Tulloh M.; Weiss, R.B.; Blom, J.; Leone, L.; Glidewell, O.; Pajak, T.F. A
randomized combined modality trial in small cell carcinoma of the lung. Cancer 1980;45:30-39
32. Eagan, R.T.; Frytac, S.; Lee, R.E.; Creacan, E.T.; Indle, J.N.; Nichols, W.C. A case for preplanned
thoracic and prophylactic whole brain radiation therapy in limited small cell lung cancer. Cancer
Clin Trials 1981;4:261-266
33. Cox, J.D.; Stanley, K.; Petrovich, Z.; Paig, C.; Yesner, R. Cranial irradiation in cancer of the lung
of all cell types. JAMA 1981;245: 469-472
34. Aroney, R.S.; Aisner, J.; Welsey, M.N.; Whitacre, M.Y.; van Echo, D.A.; Slawson, R.G.;
Wiernik, P.H. Value of prophylactic cranial irradiation given at complete remission in small cell
lung carcinoma. Cancer Treat Rep 1983;67:675-682
35. Seydel, H.G.; Creech, R.; Pagano, M.; Salazar, O.; Rubin, P.; Concannon, J.; Carbone, P.;
Mohuiddin, M.; Perez, C.; Matthews, M. Prophylactic versus no brain irradiation in region small
cell lung cancer. Am J Clin Oncol 1985;8:218-223
36. Niiramen, A.; Holsti, P.; Salmo, M. Treatment of small cell lung cancer. Acta Oncol 1989;28:501-
505
37. Ngan, S.; Ball, D.; Bull, C.; Bishop, J.; Dural, P.; Laidlaw, C.; Matthews, J. Limited small cell
lung cancer: The effects of radiotherapy on local control following response to chemotherapy Int J
Radiat Oncol Biol Phys 1991;21:459-462
38. Ohonoshi, T.; Ueoka, H.; Kawahara, S.; Kiura, K.; Kamei, H.; Hiraki, Y.; Segawaw, Y.; Hiraki,
S.; Kimura, I. Comparative study of prophylactic cranial irradiation in patients with small cell
lung cancer achieving a complete response: A long-term follow-up result. Lung cancer
1993;10:47-54
39. Arriagada, R., Le Chevalier, T.; Boire, F.; Riviere, A.; Chomy, P.; Monnet, I.; Tardivon, A.;
Viader, F.; Tarayre, M.; Benhamou, S. Prophylactic Cranial Irradiation for patients with small-cell
lung cancer in complete remission. J Nat Cancer Inst 1995;87:183-190
40. Gregor, A.; Cull, A.; Stephens, R.J.; Kirkpatrick, J.A.; Yarnold, J.R.; Girling, D.J.; Macbeth, F.R.;
Stout, R.; Machin, D. Prophylactic cranial irradiation is indicated following complete response to
induction therapy in small cell lung cancer: results of a multicentre randomized trial. Eur. J of
Cancer 1997;33:1752-1758
Radiotherapy in lung cancer. Dr. V. Kouloulias
42
41. Shaw, E.G.; Su, J.Q.; Eagan, R.T.; Jett, J.R.; Maksymiuk, A.W.; Deigert, F.A. Prophylactic
cranial irradiation in complete responders with small-cell lung cancer: analysis of the Mayo Clinic
and North Central Cancer Treatment Group Databases. J Clin. Oncol. 1994;12:2327-2332
42. Auperine A, Arriagada R, Pignon J-P, et al. ., for The Prophylactic Cranial Irradiation Overview
Collaborative Group. Prophylactic Cranial Irradiation for Patients with Small-Cell Lung Cancer in
Complete Remission. New Engl J Med 1999;341:476-484.
43. Meert A-P, Paesmans P, Berghmans T, et al. Prophylactic cranial irradiation in small cell lung
cancer: a systematic review of the literature with meta-analysis. BMC Cancer 2001;1:5
44. Fleck, J.F.; Einhorn, L.H.; Lauer, R.C.; Schultz, S.M.; Miller, M.E. Is prophylactic cranial
irradiation indicated in small-cell lung cancer? J. Clin. Oncol. 1990;8:209-214
45. Van der Kogel, A.J. Radiation response and tolerance of normal tissues. In: Basic Clinical
Radiobiology. Eds: G. Gordon Steel. 2nd ed. Arnold, London, 1997, p. 30-39.
46. Roman, D.D.; Sperduto, P.W. Neuropsychological effects of cranial radiation: current knowledge
and future directions. Int. J. Radiat. Oncol. Biol. Phys. 1995;31(4):983-998
47. Ball, D.L.; Matthews, J.P. Prophylactic cranial irradiation:More questions than answers. Sem. In
Radiat. Oncol. 1995;5:61-68
48. Catane, R.; Schwade, J.G.; Yarr, I.; Lichter, A.S.; Tepper, J.E.; Dunnick, N.R.; Brody, L.;
Brereton, H.D.; Cohen, M.; Glatstein, E. Follow-up neurological evaluation in patients with small
cell lung carcinoma treated with prophylactic cranial irradiation and chemotherapy. Int. J. Radiat.
Oncol. Biol. Phys. 1981;7:105-109
49. Johnson, B.E.; Becker, B.; Goff, W.B.; Patronas, N.; Krehbiel, M.A.; Makuch, R.W.; McKenna,
G.; Glatstein, E; Ihde, D.C. Neurological, neuropsychologic, and computed cranial tomography
scan abnormalities in 2 to 10 year survivors of small cell lung cancer. J. Clin. Oncol. 1985;3:1659-
1667
50. Frytac, S.; Shaw, J.N.; O'Neill, B.P. Leukoencephalopathy in small cell lung cancer patients
receiving prophylactic cranial irradiation. Am. J. Clin. Oncol. 1989;12:27-33
51. Stuschke, M.; Eberhardt, W.; Pottgen, C.: Stamatis, G.; Wilke, H.; Stuben, G.; Stoblen, F.:
Wilhelm, H.H.; Menker, H.; Teschler, H; Muller, R.D.; Budach, V.; Seeber, S.; Sack, H.
Prophylactic cranial irradiation in locally advanced non-small-cell lung cancer after multimodality
treatment: long-term follow-up and investigations of late neuropsychologic effects. J. Clin. Oncol.
1999;17:2700-2709
52. Pedersen AG, Kristjansen PE, Hansen HH. Prophylactic cranial irradiation and small cell lung
cancer. Cancer Treat Rev. 1988;15:85-103.
Radiotherapy in lung cancer. Dr. V. Kouloulias
43
53. Lee, J.S.; Umsawasdi, T.; Lee, Y.Y.; Barkley, H.T.Jr.; Murphy, W.K.; Welch, S.; Valdivieso, M.
Neurotoxicity in long term survivors of small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys.
1986;2:313-321
54. Van de Pol, M.; ten Velde, G.P.; Wilmink, J.T.; Volovics, A.; Twijnstra, A. Efficacy and safety of
prophylactic cranial irradiation in patients with small cell lung cancer. J. Neurooncol.
1997;35:153-160
55. Le Chevalier, T.; Arriagada, R. Small Cell Lung Cancer and Prophylactic Cranial Irradiation
(PCI): Perhaps the Question is Not who Needs PCI but who Wants PCI? Eur. J. Cancer
1997;33:1717-19
56. Einhorn, L.H. The case against prophylactic cranial irradiation in limited small cell lung cancer.
Sem. In Radiat. Oncol. 1995;5:57-60
57. Tucker, J.; Prior, P.F.; Green, C.R.; Ede, G.M.; Stevenson, J.F.; Gawler, J.; Jamal, G.A.;
Charlesworth, M.; Thakkar, C.M.; Patel, P.; Lister, T.A. Minimal neuropsychological sequelae
following prophylactic treatment of the central nervous system in adult leukaemia and lymphoma.
Br. J. Cancer 1989;60:775-780
58. Hertzberg, H.; Huk, W.J.; Uberall, M.A.; Langer, T.; Meier, W.; Dopfer, R.; Skalej, M.; Lackner,
H.; Bode, U.; Janssen, G.; Zintl, F.; Beck, J.D. CNS late effects after ALL therapy in childhood.
Part I: Neuroradiological findings in long-term survivors of childhood ALL - an evaluation of the
interferences between morphology and neuropsychological performance. The German Late
Effects Working Group. Med. Pediatr. Oncol. 1997;28:387-400.
59. Sause, W.T. Prophylactic cranial irradiation: advantages and disadvantages. Ann Oncol.
1992;3:51-55.
60. Lee J, Umsawasdi T, Lee Y. Neurotoxicity in long term survivors of small cell lung cancer. Int J
Radiat Oncol Biol Phys 1986;12:313-321.
61. Licciardello J, Cersosimo R, Karp D, et al. Disturbing central nervous system complications
following combination chemotherapy and prophylactic whole brain irradiation in patients with
small cell lung cancer. Cancer Treat Rep 1985;69:1429-1430
62. van Oosterhout A.G.M.; Ganzevles, P.G.; Wilmink, J.T.; De Geus, B.W.; Van Vonderen, R.G.;
Twijnsta, A. Sequelae in long term survivors of small cell lung cancer. Int J. Radiat. Oncol. Biol.
Phys. 1996;34:1037-1044
63. Laukkanen, E.; Klonoff, H.; Allan, B.; Graeb, D.; Muray, N. The role of prophylactic brain
irradiation in limited stage small cell lung cancer: Clinical, neuropsychologic, and CT sequelae. J.
Radiat. Oncol. Biol. Phys. 1988;14:1109-1117
Radiotherapy in lung cancer. Dr. V. Kouloulias
44
64. Twijnstra, A.; Boon, P.J.; Lormans, A.C.M.; Ten Velde, G.P.M. Neurotoxicity of prophylactic
cranial in patients with small cell carcinoma of the lung. Eur. J. Cancer Clin. Oncol. 1987;23:983-
986
65. Johnson, B.E.; Patronas, N.; Hayes, W.; Grayson, J.; Becker, B.; Gnepp, D.; Rowland, J.;
Anderson, A.; Gratstein, E.; Ihde, D.C.; Frank, J.A. Neurologic, computed cranial tomographic,
and magnetic resonance imaging abnormalities in patients with small cell lung cancer: Further
follow-up of 6- to 13-year survivors. J. Clin. Oncol. 1990;8:48-56
66. Parageorgiou C, Dardoufas C, Kouloulias V, Ventouras E, Uzunoglu N, Vlahos L, Rambavilas A,
Christodoulou G. Psychophysiological evaluation of short-term neurotoxicity after prophylactic
brain irradiation in patients with small cell lung cancer: a study of event related potentials. J
Neurooncol. 2000;50(3):275-85.
67. Delaney G, Barton M, Jacob S and Jalaludin B. A model for decision making for the use of
radiotherapy in lung cancer. The Lancet Oncol 2003;4:120-128
68. Van Houtte P, Rocmas P, Smets P, et al. Postoperative radiation therapy in lung cancer: A
controlled trial after resection of curative design. Int J Radiat Oncol Biol Phys 1980;6:983-986.
69. Ferguson M, Little A, Golomb H, et al. The role of adjuvant therapy after resection of T1N1M0
and T2N1M0 non-small cell lung cancer. J Thorac Cardiovasc Surg 1986;91:344-349.
70. Martini N, Bains M, Burt M, et al. Survival after resection of stage II non-small cell lung cancer.
Ann Thorac Surg 1992;54:460-466
71. Weiseburger T. Lung Cancer Study Group. Effects of postoperative mediastinal radiation on
completely resected stage II and stage II epidermoid cancer of the lung. N Engl J Med
1986;315:1377-1381
72. Choi N, Grillo HC, Gardiello M, et al. Basis for new strategies in postoperative radiotherapy of
bronchogenic carcinoma. Int J Radiat Oncol Biol Phys 1980;6:31-35.
73. Chung C, Stryker J, O”Neill M, et al. Evaluation of adjuvant postoperative radiotherapy for lung
cancer. Int J Radiat Oncol Biol Phys 1982;8:1877-1880
74. Green N, Melbye R. Lung cancer: retreatment of local recurrence after definitive irradiation.
Cancer 1982;49:31-34
75. Israel L, Bonadonna G, Sylvester R, et al. Controlled study with adjuvant radiotherapy,
chemotherapy, immunotherapy and chemoimmunotherapy in operable squamous carcinoma of the
lung. In Rozencweig M, Muggia F, eds: Lung Cancer: Progress in Therapeutic Research, New
York, Raven Press, 1979.
76. Kirsh M, Rotman H, Argenta L, et al. Carcinoma of the lung: results of treatment over 10 years.
Ann Thorac Surg 21:371-377.
Radiotherapy in lung cancer. Dr. V. Kouloulias
45
77. Paterson R, Russell M. Clinical trials in malignant disease: IV. Lung cancer: value of
postoperative radiotherapy. Clin Radiol 1962;13:141-144
78. Pavlov A, Pirogov A, Trachtenberg A, et al. Results of combination treatment of lung cancer
patients: surgery plus radiotherapy and surgery plus chemotherapy. Cancer Chemother Rep
1973;4:133-135.
79. Plataniotis GA, Theofanopoulou MA. Treatment of inoperable stage III and IV non-small-cell
lung cancer: the 'average' radiotherapist's point of view. Onkologie. 2001;24(4):333-9.
80. Komaki R, Scott CB, Byhardt R, Emami B, Asbell SO, Russell AH, Roach M, Parliament MB,
Gaspar LE: Failure patterns by prognostic group determined by recursive partitioning analysis
(RPA) of 1547 patients on four radiation therapy oncology group (RTOG) studies in inoperable
NSCLC. Int J Radiat Oncol Biol Phys 1998;42:263–267.
81. Karnofsky DA, Burchenal JH: The clinical evaluation of chemotherapeutic agents in cancer; in
Macleod CM (ed): Evaluation of Chemotherapeutic Agents. New York, Columbia University
Press; 1949, pp 191–205
82. Movsas B, Scott C, Sause W, Byhardt R, Komaki R, Cox J, Johnson D, Lawton C, Dar AR,
Wasserman T, Roach M, Lee JS, Andras E: The benefit of treatment intensification is age and
histology dependent in patients with locally advanced non-small cell lung cancer (NSCLC): A
quality adjusted survival analysis of radiation therapy oncology group (RTOG) chemoradiation
studies. Int Jour Radiat Oncol Biol Phys 1999;45:1143–1149.
83. Macbeth F: Radiotherapy for NSCLC: Fractionation and cost-effectiveness; in Zatlowkal P,
Petruzelka L (eds): Lung Cancer: Current topics. Prague, Scientia Medica 1996, pp 69–74
84. Armstrong J, Raben A, Zelefsky M; Burt M, Leibel S, Burman C, Kutcher G, Harrison L, Hahn
C, Ginsberg R, Rusch V, Kris M, Fuks Z: Promising survival with three dimensional conformal
radiation therapy for non-small-cell lung cancer. Radiother Oncol 1997;44: 17–22
85. Wurstbauer K, Deutschmann H, Kranziger M, Merz F, Rahim H, Sedlmayer F, Kogelnik HD:
Radiotherapy for lung cancer: Target splitting by asymmetric collimation enables reduction of
radiation doses to normal tissues and dose escalation. Int Jour Radiat Oncol Biol Phys
1999;44,333–341.
86. Komaki R, Scott CB, Lee JS, Urtasun RC, Byhardt RW, Emami B, Andras EJ, Asbell SO,
Rotman M, Cox JD: Impact of adding concurrent chemotherapy to hyperfractionated
radiotherapy for locally advanced NSCLC: Comparison of RTOG 83–11 and RTOG 91–06. Am
J Clin Oncol 1997;20:435–440.
Radiotherapy in lung cancer. Dr. V. Kouloulias
46
87. Saunders M, Dische S, Barrett A, Harvey A, Griffiths G, Palmar M: Continuous,
hyperfractionated, accelerated radiotherapy (CHART) vs conventional radiotherapy in NSCLC:
Mature data from the randomized multicentre trial. Radiother Oncol 1999;52:137–148.
88. Saunders M, Rojas A, Lyn BE, Pigott K, Powell M, Goodchild K, Hoskin PJ, Phillips H, Verma
N: Experience with dose escalation using CHARTWELL (CHART weekend Less) in NSCLC. Br
J Cancer 1998;78:1323–1328.
89. Abbatucci j, Delozier T, Quint R. Radiation myelopathy of the cervical spinal cord : time, dose
and volume factors. Int J Radiat Oncol Biol Phys 1978;4:239-248
90. Ackerby W, Choy H. Concurrent paclitaxel and thoracic radiation for advanced non-small cell
lung cancer. Lung Cancer 1995;12(suppl):S107-115.
91. Non Small Cell Lung Cancer Collaborative Group. Chemotherapy in NSCLC: A meta-analysis
using updated data on individual patients from 52 randomized clinical trials. Br Med J
1995;311:899–909.
92. Trovo MG, Minatel E, Franchin G, Boccieri MG, Nascimben O, Bolzicco G, Pizzi G, Torretta A,
Veronesi A, Gobitti C, et al.: Radiotherapy versus radiotherapy enhanced by cisplatin in stage III
NSCLC. Int J Radiat Oncol Biol Phys 1992;24:11–15
93. Komaki R: Is concomitant cisplatin and radiotherapy more efficacious treatment than
radiotherapy alone in stage III NSCLC? Int J Radiat Oncol Biol Phys 1992;24:185–186
94. Komaki R, Scott CB, Sause WT, Johnson DH, Taylor SG 4th, Lee JS, Emami B, Byhardt RW,
Curran WJ Jr, Dar AR, Cox JD: Induction cisplatin/vinblastine and irradiation vs irradiation in
unresectable squamous cell lung cancer: failure patterns by cell type in RTOG 88–08/ECOG
4588. Int J Radiat Oncol Biol Phys 1997;39:537–544.
95. Cox JD, Scott CB, Byhardt RW, Emami B, Russell AH, Fu KK, Parliament MB, Komaki R,
Gaspar LE: Addition of chemotherapy to radiation therapy alters failure patterns by cell type
within non-small cell carcinoma of the lun (NSCLC): Analysis of radiation therapy oncology
group (RTOG) trials. Int Jour Radiat Oncol Biol Phys 1999;43:505–509.
96. Sause WT, Scott C, Taylor S, Johnson D, Livingston R, Komaki R, Emami B, Curran WJ,
Byhardt RW, Turrisi AT, et al.: RTOG 88–08 and ECOG 4588: Preliminary results of a phase III
trial in regionally advanced, unresectable non-small cell lung cancer. J Natl Cancer Inst
1995;87:198–205.
97. Jeremic B, Shibamoto Y, Acimovic L, Djuric L: Randomized trial of hyperfractionated radiation
therapy with or without concurrent chemotherapy for stage III NSCLC. J Clin Oncol
1995;13:452–458.
Radiotherapy in lung cancer. Dr. V. Kouloulias
47
98. Jeremic B, Shibamoto Y, Acimovic L, Milisavjievic S: Hyperfractionated radiation therapy with
or without concurrent low-dose daily carboplatin/etoposide for stage III NSCLC: a randomized
study. J Clin Oncol 1996;14:1065–1070.
99. Komaki R, Scott S, Ettinger D, Lee JS, Fossella FV, Curran W, Evans RF, Rubin P, Byhardt
RW: Randomized study of chemotherapy/radiation therapy combinations for favorable patients
with locally advanced inoperable NSCLC: RTOG 92–04. Int J Radiat Oncol Biol Phys
1997;38:149–155.
100. Arriagada R, Le Chevalier T, Quiox E, Ruffie P, de Cremoux H, Douillard JY, Tarayre M,
Pignon JP, Laplanche A: ASTRO plenary: Effect of chemotherapy on locally advanced NSCLC:
A randomized study of 353 patients. Int J Radiat Oncol Biol Phys 1991;20:1183–1190.
101. Dillman RO, Herndon J, Seagren SL Eaton WL Jr, Green MR: Improved survival in stage III
NSCLC: Seven-year follow-up of cancer and leukemia group B (CALGB) 8433 trial. J Natl
Cancer Inst 1996;88:1210–1215.
102. Clamon G, Herndon J, Cooper, R Chang AY, Rosenman J, Green MR: Radiosensitization
with carboplatin for patients with unresectable stage III non-small cell lung cancer: A phase III
trial of the Cancer and Leukemia Group B and Eastern Cooperative Oncology Group. J Clin
Oncol 1999;17:4–11.
103. Lee JS, Scott C, Komaki R, Fossella FV, Dundas GS, McDonald S, Byhardt RW, Curran WJ
Jr: Concurrent chemoradiation therapy with oral etoposide and cisplatin for locally advanced
inoperable NSCLC: RTOG Protocol 91–06. J Clin Oncol 1996;14:1055–1064.
104. Blanke C, Ansari R, Mantravadi R, Gonin R, Tokars R, Fisher W, Pennington K, O'Connor
T, Rynard S, Miller M, et al.: Phase III trial of thoracic irradiation with or without cisplatin for
locally advanced unresectable NSCLC: A Hoosier Oncology Group protocol. J Clin Oncol
1995;13:1425–1429.
105. Mirimanoff RO, Moro D, Bolla M, Michel G, Brambilla C, Mermillod B, Miralbell: R,
Alberto P: Alternating radiotherapy and chemotherapy for inoperable stage III NSCLC: Long-
term results of two-phase II GOTHA trials. Int J Radiat Oncol Biol Phys 1998;42:487–494.
106. Soresi E, Clerici M, Grilli R. A randomized clinical trial comparing radiation therapy versus
radiation therapy radiation therapy plus cis-dichlorodiamin (platinum III) in the treatment of
locally advanced non-small cell lung cancer. Semin Oncol 1988;15:20-25
107. Schaake-Konig C, Van den Bogaert W, Dalesio O, Festen J, Hoogenhout J, van Houtte P,
Kirkpatrick A, Koolen M, Maat B, Nijs A, et al.: Effects of concomitant cisplatin and
radiotherapy on inoperable NSCLC. New Engl J Med 1992;326:524–530.
Radiotherapy in lung cancer. Dr. V. Kouloulias
48
108. Byhardt RW, Scott C, Sause WT, Emami B, Komaki R, Fisher B, Lee JS, Lawton C:
Response, toxicity, failure patterns and survival in five Radiation Therapy Oncology Group
(RTOG) trials of sequential and/or concurrent chemotherapy and radiotherapy for locally
advanced non-small-cell carcinoma of the lung. Int J Radiat Oncol Biol Phys 1998;42:469–478.
109. Spiro SG, Porter JC. Lung cancer--where are we today? Current advances in staging and
nonsurgical treatment. Am J Respir Crit Care Med. 2002;166:1166-96
110. Shepherd FA, Johnston MR, Payne D, et al., Randomized study of chemotherapy and surgery
versus radiotherapy for stage IIIA non-small cell lung cancer: A National Cancer Institute of
Canada Clinical Trials Group study. Br J Cancer 1998;78:683–685.
111. Cox JD, Azarnia N, Byhardt RW, et al. N2 (clinical) non-small cell carcinoma of the lung:
Prospective trials of radiation therapy with total doses of 60 Gy by the Radiation Therapy
Oncology Group. Int J Radiat Oncol Biol Phys 1991;20:7–12.
112. Pearson FG, Delarue NC, Ilves R, et al. Significance of positive superior mediastinal lymph
nodes identified at mediastinoscopy in patients with resectable cancer of the lung. J Thorac
Cardiovasc Surg 1982;83:1–11.
113. Sause W, Kolesar P, Taylor S, et al. Final results of phase III trial in regionally advanced
unresectable non-small cell lung cancer. Radiation Therapy Oncology Group, Eastern
Cooperative Oncology Group, and Southwest Oncology Group. Chest 2000; 117:358–364
114. Greco FA. Multidisciplinary approach to potentially curable non-small cell carcinoma of the
lung. Oncology 1997;11:27–49.
115. Roth J, Fosselle F, Komaki R, et al. A randomized trial comparing perioperative
chemotherapy and surgery with surgery alone in resectable stage III non-small cell lung cancer. J
Natl Cancer Inst 1994;86:673–680.
116. Rusch V, Albain KS, Crowley JJ, et al. Surgical resection of stage IIA and IIIB non-small
cell lung cancer after concurrent induction chemoradiotherapy: A Southwest Oncology Group
Trial. J Thor Cardiovasc Surg 1993;105:97–106.
117. Arriagada R, Le Péchoux C, Pignon J-P. Resected non-small cell lung cancer: need for
adjuvant lymph node treatment? From hope to reality Lung Cancer 2003;42:57-64
118. Arriagada R, Le Chevalier T, Rekacewicz C, et al. Cisplatin-based chemotherapy (CT) in
patients with locally advanced non-small lung cancer (NSCLC): late analysis of a French
randomized trial. Proc Am Soc Clin Oncol 1997;16:446a.
119. Furuse K, Fukuoka M, Kawahara M, et al. Phase III study of concurrent versus sequential
thoracic radiotherapy in combination with mitomycin, vindesine, and cisplatin in unresectable
stage III non-small-cell lung cancer. J Clin Oncol 1999;17:2692–2699.
Radiotherapy in lung cancer. Dr. V. Kouloulias
49
120. Curran W, Scott C, Langer C. Phase III comparison of sequential vs. concurrent chemo-
radiation for patients with unresected stage III non-small cell lung cancer (NSCLC): Report of
Radiation Therapy Oncology Group 9410, 9th World Conference on Lung Conference on Lung
Cancer. Lung Cancer 2000;29(Suppl. 1):93.
121. Pierre F, Maurice P, Gilles R, et al. A randomized phase III trial of sequential chemo-
radiotherapy versus concurrent chemo-radiotherapy in locally advanced non small cell lung
cancer (NSCLC) (GLOT-GFPC NPC 95-01 study). Proc. Am. Soc. Clin. Oncol. 2001;20:312a.
122. Zatloukal PV, Petruzelka L, Zemanova M, et al. Concurrent versus sequential radiotherapy
with vinorelbine plus cisplatin (V-P) in locally advanced non-small cell lung cancer. A
randomized phase II study. Proc Am Soc Clin Oncol 2002;21:290a.
123. Vokes E, Herndon J, Crawford J, et al. Randomized phase II study of cisplatin with
gemcitabine or paclitaxel or vinorelbine as induction chemotherapy followed by concomitant
chemoradiotherapy for stage IIIB non-small-cell lung cancer: Cancer and Leukemia Group B
Study 9431. J Clin Oncol 2002;20:4191–4198.
124. Socinski M, Roseman J, Halle J, et al. Dose-escalating conformal thoracic radiation therapy
with induction and concurrent carboplatin/paclitaxel in unresectable stage IIIA/IIIB non-small
cell lung carcinoma. A modified phase I/II trial. Cancer 2001;92:1213–1223.
125. Albain KS, Crowley JJ, Turrisi AT, et al. Concurrent cisplatin, etoposide plus radiotherapy
for pathologic stage IIIB non-small cell lung cancer: A Southwest Oncology Group phase II
study (S9019). J Clin Oncol 2002;20:3454–3460
126. Gandara Fisher MD, D'Orazio A. Concurrent chemoradiotherapy followed by consolidation
docetaxel in stage IIIB non small-cell lung cancer (SWOG 9504). Clin Lung Cancer.
2000;2(1):25-6.
127. Choy H, Curran W, Scott CB, et al. Preliminary report of locally advanced multimodality
Protocol (LAMP): ACR 427: a randomized phase II study of three chemo-radiation regimens
with paclitaxel, carboplatin, and thoracic radiation (TRT) for patients with locally advanced non
small cell lung cancer (LA-NSCLC). Proc Am Soc Clin Onc 2002;21:291a.
128. Armstrong B, Perez C, Simpson J, et al. Role of irradiation in the management of superior
vena cava syndrome. Int J Radiat Oncol Biol Phys 1987;13:531-539
129. Rubin P, Ciccio S. High daily dose for rapid decrompression. In Deeley T. (ed) Modern
radiotherapy: carcinoma of the bronchus. New York, Appleton-Century-Crofts, 1971.
130. Lanciego C, Chacon JL, Julian A, et al. Stenting as first option for endovascular treatment of
malignant superior vena cava syndrome. AJR Am J Roentgenol. 2001;177:585-93.
Radiotherapy in lung cancer. Dr. V. Kouloulias
50
131. Medical Research Council Lung Cancer Working Party. Inoperable non-small-cell lung
cancer: A MRC randomized trial with two fractions or ten fractions. Br J Cancer 1991;63:265–
270.
132. Medical Research Council Lung Cancer Working Party: A medical research council (MRC)
randomized trial of palliative radiotherapy with two fractions or a single fraction in patients with
inoperable non-small-cell lung cancer and poor performance status. Br J Cancer 1992;65:934–
941.
133. Plataniotis G., Kouvaris J, Dardoufas, Pistevou-Gobaki K, Kouloulias V, Papadopoulos LS,
Vlahos L: A short course of palliative radiotherapy for inoperable NSCLC: Biologically effective
dose to the spinal cord. Clin Oncol 2000;12:335.
134. Mcbeth FR: Radiation myelitis and thoracic radiotherapy: Evidence and anecdote. Clin Oncol
2000;12:333–334.
135. Macbeth FR, Bolger JJ, Hopwood P, Bleehen NM, Cartmell J, Girling DJ, Machin D,
Stephens RJ, Bailey AJ: Randomized trial of palliative two-fraction versus more intensive 13-
fraction radiotherapy for patients with inoperable NSCLC and good performance status. Clin
Oncol 1996;8:167–175.
136. Machtay M, Seiferheld W, Komaki R, Cox JD, Sause WT, Byhardt RW: Is prolonged
survival possible for patients with supraclavicular node metastases in non-small cell lung cancer
treated with chemoradiotherapy? Analysis of the Radiation Therapy Oncology Group experience.
Int Jour Radiat Oncol Biol Phys 1999;44:847–853.
137. Somerfield MR: Clinical practice guidelines for the treatment of unresectable non-small cell
lung cancer. J Clin Oncol 1997;15:2996–3018.
138. Pfister D, Johnson D, Azzoli C, Sause W, Smith T, Baker S Jr, Olak J, Stover D, Strawn J,
Turrisi A, Somerfield M. American Society of Clinical Oncology Treatment of Unresectable
Non–Small-Cell Lung Cancer Guideline: Update 2003 J Clin Oncol 2004;22:330-353
139. Mountain CF, Dresler CM. Regional lymph node classification for lung cancer staging. Chest
1997;111:1718-23.
140. Abratt QP and Morgan GW. Lung toxicity following chest irradiation in patients with lung
cancer. Lung Cancer 2002;35:109–203
141. Bentzen SM, Skoczylas JZ, Bernier J. Quantitative clinical radiobiology of early and late
lung reactions. Int J Radiat Biol 2000;76:453–462.
142. McDonald S, Rubin P, Phillips TL, Marks LB. Injury to the lung from cancer therapy:
clinical syndromes, measurable endpoints, and potential scoring systems. Int J Radiat Oncol Biol
Phys 1995;31:1187–1203.
Radiotherapy in lung cancer. Dr. V. Kouloulias
51
143. Monson JM, Stark P, Reilly JJ, et al. Clinical radiation pneumonitis and radiographic changes
after thoracic radiation therapy for lung carcinoma. Cancer 1988;82:842–850.
144. Quon H, Shepherd FA, Payne DG, et al. The influence of age on the delivery, tolerance, an
efficacy of thoracic irradiation in the combined modality treatment of limited stage small cell
lung cancer. Int J Radiat Oncol Biol Phys 1999;43:39–45.
145. Robnett TJ, Machtay M, Vines EF, McKenna MG, Algazy HM, McKenna WG. Factor
predicting severe radiation pneumonitis in PTs receiving definitive chemoradiation for lung
cancer. Int J Radiat Oncol Biol Phys 2000;48:89–94
146. Vujaskovic Z, Marks LB, Anscher MS. The physical parameters and molecular events
associated with radiation-induced lung toxicity. Semin Radiat Oncol 2000;10:297–307
147. Yamada M, Kudoch S, Hirata K, Nakajima T, Yoshikawa J. Risk factors of pneumonitis
following chemoradiotherapy for lung cancer. Eur J Cancer 1998;34:71–75.
148. Inoue A, Kunitoh H, Sekine I, Sumi M, Tokuuye K, Saijo N. Radiation pneumonitis in lung
cancer patients: a retrospective study of risk factors and the long-term prognosis. Int J Radiat
Oncol Biol Phys 2001;49:649–655.
149. Jensen BV, Carsen NL, Nissen NI. Influence of age and duration of follow-up on lung
function after combined chemotherapy for Hodgkin's disease. Eur Respir J 1990;3:1140–1145.
150. Roach M, Gandara DR, Yuo HS, et al. Radiation pneumonitis following combined modality
therapy for lung cancer: analysis of prognostic factors. J Clin Oncol 1995;13:2606–2612.
151. Graham MV, Purdy JA, Emami B, et al. Clinical dose-volume histogram analysis for
pneumonitis after 3D treatment for non-small cell lung cancer (NSCLC). Int J Radiat Oncol Biol
Phys 1999;45:323–329.
152. Hernando ML, Marks LB, Bentel GC, et al. Radiation-induced pulmonary toxicity: a dose-
volume histograms analysis in 201 patients with lung cancer. Int J Radiat Oncol Biol Phys
2001;51:650–659.
153. Armstrong JC, Zelefsky MJ, Leibel SA, et al. Strategy for dose escalation using 3-
dimansional conformal radiation therapy for lung cancer. Ann Oncol 1995;6:693–697.
154. Martel MK, Ten Haken RK, Hazuka MB, Turrisi AT, Fraass BA, Lichter AS. Dose-volume
histogram and 3-D treatment planning evaluation of PTs with pneumonitis. Int J Radiat Oncol
Biol Phys 1994;28:575–581.
155. Oetzel D, Schraube P, Hensley F, Sroka-Perez G, Menke M, Flentje M. Estimation of
pneumonitis risk in three-dimensional treatment planning using dose-volume histogram analysis.
Int J Radiat Oncol Biol Phys 1995;33:455–460.
Radiotherapy in lung cancer. Dr. V. Kouloulias
52
156. Burman C, Kutcher GJ, Emami, Goitein M. Fitting of normal tissue tolerance to an analytical
function. Int J Radiat Oncol Biol Phys 1991;21:125–135.
157. Gagliardi G, Bjohle J, Lax I, et al. Radiation pneumonitis after breast cancer irradiation:
analysis of the complication probability using the relative seriality model. Int J Radiat Oncol Biol
Phys 2000;46:373–381.
158. Kwa SLK, Lebesque JV, Theuws JCM, et al. Radiation pneumonitis as a function of mean
lung dose: an analysis of pooled data of 540 PTs. Int J Radiat Oncol Biol Phys 1998;28:575–581.
159. Rancati T, Ceresoli GL, Gagliardi G, Schipani S, Cattaneo GM. Factors predicting radiation
pneumonitis in lung cancer patients: a retrospective study. Radiother Oncol 2003;67:275-283.
160. Marks LB, Munley MT, Bentel GC, et al. Physical and biological predictors of changes in
whole-lung function following thoracic irradiation. Int J Radiat Oncol Biol Phys 1997;39:563–
570.
161. Anscher MS, Kong FM, Marks LB, et al. Changes in plasma transforming growth factor beta
during radiotherapy and the risk of symptomatic radiation-induced pneumonitis. Int J Radiat
Oncol Biol Phys 1997;37:253–258.
162. Anscher MS, Kong FM, Jirtle RL. The relevance of transforming growth factor beta in
pulmonary injury after radiation therapy. Lung Cancer 1998;19:109–120
163. Anscher MS, Kong FM, Andrews K, et al. Plasma transforming growth factor beta as a
predictor of radiation pneumontis. Int J Radiat Oncol Biol Phys 1998;41:1029–1035.
164. Geara FB, Komaki R, Tucker SL, et al. Factors influencing the development of lung fibrosis
after chemoradiation for small cell carcinoma of the lung: Evidence for inherent interindividual
variation. Int J Radiat Oncol Biol Phys 1998;41:279–286.
165. Brizel DM, Wasserman TH, Henke M, et al. Phase III randomized trial of amifostine as a
radioprotector in head and neck cancer. J Clin Oncol 2000;18:3339–3345
166. Kemp G, Rose P, Lurain J, et al. Amifostine pretreatment for protection against
cyclophosphamide-induced and cisplatin-induced toxicities: Results of a randomized control trial
in patients with advanced ovarian cancer. J Clin Oncol 1996;14:2101–2112.
167. Andreassen CN, Lindegaard JC. Chemical radioprotection: A critical review of amifostine as
a cytoprotector in radiotherapy. Semin Radiat Oncol 2003;13:62–72.
168. Capizzi RL. The preclinical basis for broad-spectrum selective cytoprotection of normal
tissues from cytotoxic therapies by amifostine. Semin Oncol 1999;26:3–21.
169. Komaki R, Lee JS, Milas L, et al. Effects of amifostine on acute toxicity from concurrent
chemotherapy and radiotherapy for inoperable non-small-cell lung cancer: report of a randomized
comparative trial. Int J Radiat Oncol Biol Phys. 2004;58(5):1369-77
Radiotherapy in lung cancer. Dr. V. Kouloulias
53
170. Movsas B, Scott C, Langer C, et al. Phase III study of amifostine in patients with locally
advanced non-small cell lung cancer (NSCLC) receiving chemotherapy and hyperfractionated
radiation (chemo/HFxRT): Radiation Therapy Oncology Group (RTOG) 98-01. In: S.M.
Grunberg, Editor, Proceedings of the American Society of Clinical Oncology, American Society
of Clinical Oncology, Chicago (2003), p. 636.
171. Leong SS, Tan EH, Fong K, et al. Randomized double-blind trial of combined modality
treatment with or without amifostine in unresectable stage III non-small-cell lung cancer. J Clin
Oncol 2003;21:1767–1774.
172. Senzer N. A phase III randomized evaluation of amifostine in stage IIIA/IIIB non-small cell
lung cancer patients receiving concurrent carboplatin, paclitaxel, and radiation therapy followed
by gemcitabine and cisplatin intensification: Preliminary findings. Semin Oncol 2002;29:38–41.
173. Antonadou D, Coliarakis N, Synodinou M, et al. Randomized phase III trial of radiation
treatment ± amifostine in patients with advanced-stage lung cancer. Int J Radiat Oncol Biol Phys
2000;51:915–922.
174. Antonadou D, Throuvalas N, Petridis A, et al. Effect of amifostine on toxicities associated
with radiochemotherapy in patients with locally advanced non-small-cell lung cancer. Int J
Radiat Oncol Biol Phys 2003;57:402–408.