Putting frailty into practice: perspectives from Hong Kong · perspectives from Hong Kong Jean Woo...
54
Putting frailty into practice: perspectives from Hong Kong Jean Woo Jockey Club Institute of Ageing The Chinese University of Hong Kong
Transcript of Putting frailty into practice: perspectives from Hong Kong · perspectives from Hong Kong Jean Woo...

Putting frailty into practice: perspectives from Hong Kong
Jean Woo Jockey Club Institute of Ageing
The Chinese University of Hong Kong


Background
• Frailty represents a state of diminishing reserve in the capacity to respond to various environmental challenges, as a result of the aging process.
• Frailty predicts adverse health outcomes, such as quality of life, use of hospital services, and mortality, independent of diseases and disability

Social Determinants of Frailty [Woo J et al. Gerontology 2005;51:402-408]
Multiple regression model
Socioeconomic factors
Job 0.029
Expenses 0.029
Lifestyle factors
Activities <0.001
Drink <0.001
Social support factors
Relatives 0.018
Neighbors <0.001
Help others <0.001
Factors associated with frailty among men (n = 999)

Social Determinants of Frailty [Woo J et al. Gerontology 2005;51:402-408]
Multiple regression model
Socioeconomic factors
Expenses 0.001
Lifestyle factors
Activities <0.001
Social support factors
Contact with relatives 0.038
Neighbors 0.020
Help others <0.001
Attend community/religious activities 0.010
Factors associated with frailty among women (n = 1,033)

Public health significance of the frailty index [Woo J et al. Disability and Rehabilitation 2006;28:515-521]
A total of 2032 people aged 70 years and over recruited by stratified random sampling, and information obtained regarding physical and functional health, and psychological factors. The frailty index (FI) was constructed from 62 variables. Associations between the FI, and changes in ADL score, mental score, and hospitalization days over a 10-year period were evaluated. • For the baseline to 3-year changes
0.10 increase in baseline FI is accompanied by a 0.499-point faster drop in ADL score 0.223-point faster decline in mental score 4.57-day faster increase in hospital days
• For 3-10 year changes
Frailty was a significant predictor only of changes in mental score With results indicating that, on average, each increase of 0.10 in the baseline frailty index was associated with 0.613-point drop in mental score during this period

Crude OR (95% CI)
Beijing urban Hong Kong
Female 1.50 (1.30, 1.73) 2.07 (1.74, 2.46)
Age
65-74 Ref. Ref.
75-84 1.92 (1.67, 2.19) 1.79 (1.50, 2.12)
85+ 2.44 (1.80, 3.30) 2.46 (1.69, 3.57)
Currently married 0.57 (0.50, 0.66) 0.60 (0.50, 0.71)
Education ≤ <Middle school 1.27 (1.11, 1.45) 1.98 (1.55, 2.53)
Living alone 1.53 (1.26, 1.86) 1.53 (1.22, 1.93)
Current smoking 0.74 (0.59, 0.92) 0.82 (0.58, 1.17)
Current alcohol use 0.73 (0.57, 0.93) 0.31 (0.21, 0.45)
Daily exercise < 0.5h 1.83 (1.59, 2.10) 1.73 (1.46, 2.05)
No. of diseases ≥ 3 7.72 (6.69, 8.90) 6.08 (5.09, 7.25)
Daily drugs ≥ 4 5.62 (4.89, 6.46) 2.82 (2.16, 3.68)
Crude OR of frailty in Beijing urban and Hong Kong
[Woo J et al. BMC Geriatrics 2015;15:163]

Adjusted OR (95% CI)
Beijing urban Hong Kong
Female 1.48 (1.26, 1.75) 2.15 (1.76, 2.62)
Age
65-74 Ref. Ref.
75-84 1.71 (1.47, 2.00) 1.59 (1.32, 1.93)
85+ 2.44 (1.70, 3.52) 2.48 (1.63, 3.77)
Currently married 0.70 (0.56, 0.80) /
Education ≤ <Middle school / 1.78 (1.36, 2.33)
Current alcohol use / 0.54 (0.36, 0.81)
Daily exercise < 0.5h 1.75 (1.49, 2.05) 1.71 (1.41, 2.07)
No. of diseases ≥ 3 5.20 (4.45, 6.06) 6.48 (5.38, 7.81)
Daily drugs ≥ 4 3.44 (2.95, 4.02) /
AUC 0.819 0.783
Multiple logistic regression of frailty in Beijing urban and Hong Kong
[Woo J et al. BMC Geriatrics 2015;15:163]

Attributable fraction for frailty in Beijing urban and Hong Kong
[Woo J et al. BMC Geriatrics 2015;15:163]
Attributable fraction (%)
Beijing urban Hong Kong
Female 32.43 % 53.42 %
Age
65-74 Ref. Ref.
75-84 41.52 % 37.19 %
85+ 59.02 % 59.64 %
Currently married –42.86 % /
Education ≤ <Middle school / 43.88%
Current alcohol use / –86.22%
Daily exercise < 0.5h 42.86 % 41.49 %
No. of diseases ≥ 3 80.77 % 84.58 %
Daily drugs ≥ 4 70.93 % /

Operationalizing frailty
Variables are highly specified: prototype is the frailty phenotype – Slow mobility – Weakness – Weight loss – Decreased activities – Exhaustion
• Fried et al.,. 2001;56 J Gerontol A Biol Sci Med Sci (3):M146-56.
Variables are hardly specified: prototype is the Frailty Index – Count health deficits (30-100)
• age associated but does not saturate;
• associated with adverse outcome
• <5% missing data – Divide by the number of deficits
considered. • Mitnitski et al., ScientificWorldJ
2001;1:323-326.
• Searle et al., BMC Geriatr 2008;8:24.

Consequences of frailty • Older people living with frailty are at risk of adverse outcomes such
as dramatic changes in their physical health and mental wellbeing after an apparently minor event which challenges their health
Living with frailty
• Higher risk of dramatic changes in physical and mental health
Increased risk of adverse outcomes
• Falls
• Disability
• Hospitalization
• Institutionalization
• Mortality
Increased burden
• Caregiving burden
• Healthcare expenditures

Is frailty treatable? • Frailty is not an inevitable part of ageing
• Physical frailty (sarcopenia) is reversible
Recognition of Frailty
(Screening)
Comprehensive Geriatric
Assessment
Individualized care and training /
intervention
Yu R et al. Geriatr Gerontol Int 2014;14(suppl1):15-28 Lee J et al. J Am Med Dir Assoc 2014;15(4):281-6

• Recently two sub components have been proposed: Physical frailty : sarcopenia Cognitive frailty : mild cognitive impairment or dementia
• Close link with under nutrition • Calls for incorporating frailty assessment into the primary
care setting, enabling early identification and intervention to retard decline [King’s Fund and Age UK 2014]

Tools: requirements for use in practice
• Quick, without need for special equipment and time consuming measurements, which also involve establishment of cut-off values
• Administration does not require extensive training or by professional staff
• Suitable for screening rather than detailed clinical assessment: used as the first step in a stepped care approach
• Validated against consensus definitions and clinical assessments

• No consensus regarding simple screening tools: either high sensitivity and low specificity, or the reverse
• In the primary care setting, simplicity (short questionnaire without the need for measurements), no need for trained staff/can be self-administered, and high specificity, may be a useful first step, followed by comprehensive multi domain geriatric assessment

The FRAIL Scale
5-item FRAIL scale
• Fatigue Tired all or most of the time during the past four weeks (No/Yes)
• Resistance Difficulty walking up 10 steps without resting or aids (No/Yes)
• Ambulation Difficulty walking several hundred yards alone without aids (500-600 meters) (No/Yes)
• Illnesses 5 or more illnesses (No/Yes)
• Loss of weight Weight loss > 5% within the past month (No/Yes) Robust=0; Pre-frail=1-2; Frail=3 [Morley et al J Nutr Health Ageing 2012; 16(7): 601-608]
Morley et al. J Nutr Health Aging 2012;16(7):601-8
Background

The FRAIL Scale
• Compared with the frailty phenotype and multiple deficit models, the screening tool has similar predictive properties in having high specificity but low sensitivity in predicting incident physical limitation and mortality [Woo et al J Am Geriatr Soc 2012; 60(8): 1478-1486]

Impact
• Screening in the community allows early detection and enables intervention programmes to be provided
• Retards decline from pre-frail to frail state Reverse frail to pre-frail state

Frailty Screening in the Community Using the FRAIL Scale
[Woo J et al JAMDA 2015;16:412-419]

Objective
• To explore the feasibility of using the FRAIL scale in community screening
• Comprehensive geriatric assessment of those identified as pre-frail or frail
• Doctor(s) leading a multi-disciplinary team

The Team outside a community centre in the North District
• Participants waiting for comprehensive geriatric assessment

• Over 20 talks Approximately 1500 participants
Health talks
2014 Apr – Jul
• Basic demographics
• Frailty Status
• Sarcopenia
• Mild cognitive impairment
Phase 1 assessment (Screening)
2014 Apr – Jul • Comprehensive
geriatric assessment
• Medical consultation
• Referrals
Phase 2 assessment
2014 Jul – Oct
• Bone and muscle strengthening exercises
• Brain Training
12-week comprehensive
training program for frailty prevention
Frailty screening and intervention programme

Characteristics of participants
• Aged 65+ (N = 816) • M : 119 (14.6%) • F : 697 (85.4%)
Phase 1 assessment
22%
19% 59%
Age group
65-69
70-74
75+
Phase 1 findings
Number of participants may not sum to total due to missing data
Tai Po 300
North District 240
Kowloon 16
HK Island 11
Shatin 232
Tsing Yi 1
Yuen Long 1
Tuen Mun 1
Number of participants may not sum to total due to missing data

n=274, 33.6% which include the following35 No show (4.3%)35 Couldn't be contacted (4.3%)74 Refusals (9.1%)7 Inability to participate because of cognitive or physical impairments (0.9%)1 Institutionalized (0.1%)1 Dead (0.1%)41 Community centres declined to participate (5.0%)80 Inaccessible cases in closed area (9.8%)
n = 255, 31.2%
Robust1 Pre-frail1
Pre-frail + Frail1
n = 529, 64.8%
Completed follow-upinterview
n = 286, 35.0% n = 427, 52.3% n = 102, 12.5% n = 1, 0.1%
Participants ≥ 65 yrsn = 816
Loss to follow-up
Frail1 Missing data
1Frailty score: 0 (Robust), 1-2 (Pre-frail), 3-5 (Frail)
Frailty status of participants
[Woo J et al. JAMDA 2015;16:412-419]

Tai Po 72
North District 68
Kowloon 4
HK Island 6
Shatin 100
Tsing Yi 1
Yuen Long 1
Tuen Mun 1
Characteristics of participants
• Inclusion criteria for phase 2 assessment Aged 65+, pre-frail / frail
Phase 1 assessment
• N = 255 • M : 26 (10.2%) • F : 229 (89.8%)
Phase 2 assessment
82%
18%
Frailty status
Pre-frail
Frail
Phase 2 findings
Morley et al. J Nutr Health Aging 2012;16(7):601-8
Number of participants may not sum to total due to missing data

Prevalence of frailty among those aged 65+
• About 1 in 8 (12.5 %) of community-dwelling population aged 65+ were frail
• Pre-frailty was found to be common, more than half (52.4%) of the community-dwelling population aged 65+ were pre-frail
Robust 35%
Pre-frail 52%
Frail 13%
Frailty status
Morley et al. J Nutr Health Aging 2012;16(7):601-8
Phase 1 findings

The prevalence of frailty increased with age
35.1 50 48.1
25.4
52.4
44.9 44.2
57.8
12.5 5.1 7.7 16.8
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Overall 65-69 70-74 75+
Prev
alen
ce (%
)
Age group
Robust Pre-frail Frail
Phase 1 findings

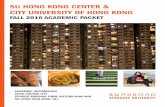
Venn diagram displaying extend of overlap of frailty with sarcopenia and mild cognitive impairment. Total represented: 396
subjects who had frailty and/or sarcopenia and/or memory impairments
Frailty 8.8%
(n=9)
Mild cognitive impairment
n=183
Sarcopenia n=32
12.8% (n=13)
63.7% (n=65)
14.7% (n=15)
[Woo J et al. JAMDA 2015;16:412-419]

Frail elderly tended to have more chronic diseases and received more medications compared with pre-frail elderly
2.23
2.94 3
4.31
0 0.5
1 1.5
2 2.5
3 3.5
4 4.5
5
Number of diseases Number of mediciations
Num
ber (
mea
n)
Pre-frail
Frail
Age- and sex-adjusted p<0.01 (no. of diseases) P<0.01 (no. of drugs)
Phase 2 findings

Elderly with a higher physical activity level showed a lower prevalence of frailty
37.8 37.8
24.4
0
5
10
15
20
25
30
35
40
< 20 min/day 20-59 min/day ≥ 1 hr/day
Prev
alen
ce o
f fra
ilty
(%)
Physical activity level
Age- and sex-adjusted p<0.05
Phase 2 findings

Frail elderly showed a higher prevalence of sarcopenia and mild cognitive impairment compared with pre-frail elderly
SARC-F questionnaire for sarcopenia (strength, assistance with walking, rise from a chair, climb stairs, and falls) Malmstrom et al. JAMDA 2013;14(8):531-2 AMIC, Abbreviated Memory Inventory for the Chinese for subjective memory problems and related complaints Lam et al. Int J Geriatr Psychiatry 2005;20(9):876-82
31.9
60.5
84.4 86.7
0
10
20
30
40
50
60
70
80
90
100
SARC-F ≥ 4 AMIC ≥ 3
Prev
alen
ce (%
)
Pre-frail
Frail
Age- and sex-adjusted p<0.01 (SARC-F) P<0.01 (AMIC)
Phase 2 findings

Falls were more common among the frail elderly compared with pre-frail elderly
19.6
35.6
0
5
10
15
20
25
30
35
40
Falls
Prev
alen
ce (%
)
Pre-frail
Frail
Age- and sex-adjusted p<0.05
Phase 2 findings

ADL and IADL disabilities were more prevalent among the frail elderly compared with pre-frail elderly
ADL, Barthel index of Activities of Daily Living. Total possible scores range from 0-20, with lower scores indicating increased disability IADL, modified Lawton Instrumental Activities of Daily Living scale . Total possible scores range from 0-12, with lower scores indicating increased disability
31.4 32.5
50
60
0
10
20
30
40
50
60
70
≥ 1 ADL disability ≥ 1 IADL disability
Prev
alen
ce (%
)
Pre-frail
Frail
Age- and sex-adjusted p<0.05 (ADL) p<0.01 (IADL)
Phase 2 findings

Depressive symptoms were more prevalent among the frail elderly compared with pre-frail elderly
GDS, Geriatric Depression Scale (15-item). Total possible scores range from 0-15, with higher scores indicating higher levels of depressive symptoms
11
28.9
0
5
10
15
20
25
30
35
Depressive symptoms (GDS≥8)
Prev
alen
ce (%
)
Pre-frail
Frail
Age- and sex-adjusted p<0.01
Phase 2 findings

Frail elderly showed a higher prevalence of poor self-rated health compared with pre-frail elderly
18.6
44.4
0
5
10
15
20
25
30
35
40
45
50
Poor self-rated health
Prev
alen
ce (%
)
Pre-frail
Frail
Age- and sex-adjusted p<0.01
Phase 2 findings

• In 2014, about 1 in 8 (12.5%) of community-dwelling population aged 65 and above had frailty
• Pre-frailty was also found to be common, more than half (52.4%) of the community-dwelling population aged 65+ were pre-frail
• The prevalence of frailty increased with age, being 5.1% for people aged 65-69 years and 16.8% for those aged 75 years and above
• Older age, number of chronic diseases, use of medication, physical activity, sarcopenia, mild cognitive impairment, falls, ADL and IADL disabilities, depressive symptoms and self-rated health were factors associated with frailty
Summary of findings

Comparison with other community studies using phenotype definitions
• Chinese populations pre-frail: 44-53% frail: 4-8%
• English Longitudinal Study of Ageing: frail : 6.5% (60-69y); 10% (70-79%)

Limitations
• Pragmatic study focusing on feasibility • No comprehensive assessment of the group who were
robust • Those who did not return for assessment tend to be older
and more were frail.

Conclusion and significance of findings
• Confirms the feasibility of this two step approach in community frailty screening
• Supports the concept that frailty has physical and cognitive components, representing cognitive and physical reserves
• Supports the need for incorporating frailty assessments into clinical practice
• Future research: community intervention programmes for modifying frailty states; use in hospital and residential care settings

Older people discharged from hospitals
• Excluding those who are from RCHEs; there is a considerable burden of frailty among this group
• Frail ranges from 30-50%; mean age 80+; Geriatric Day Hospital profile: pre-frail:frail approximately 50:50
• This group in the community require integrated medico-social care on a continuous basis. This is a current service gap

Frailty intervention : Nutrition 1872 community-dwelling people >=60 years (Leon-Munoz et al BMC Medicine 2015; 13: 11
Prospective study over 3.5 years with incident frailty as outcome
Adherence to prudent dietary pattern
Reduced risk of incident frailty between third and first tertile of adherence (OR 0.2-0.8, P-trend 0.009
5,925 men >=65 years (US Mr Os study) (Shikany et al J Gerontol A
2014;69(6):695-701)
Prospective study mean follow-up 4.6 years using incident frailty as outcome
Dietary Quality Index
High quality index inversely associated with the development of frailty (Q5 v. Q1 OR 0.18 95% CI 0.03-0.97)
690 community-dwelling people>=65 years (Talegawkar et al J Nutr 2012;142:2161-66)
Prospective study FU 6 y using frailty outcome as above
Adherence to Mediterranean diet
Score >=6 v <=3; OR 0.3 (0.14-0.66)

Frailty intervention: exercise

The Home-based older people’s exercise trial (HOPE)
• 12 week exercise intervention to improve mobility and function, compared with usual care
• Primary outcome is mobiltiy represented by the TUGT Secondary outcomes : ADL, HRQOL, depression
• 45 intervention and 39 control • Non-significant trend towards improvement in the
intervention group in primary outcome: no difference in secondary outcome [Clegg A et al Age and Ageing 2014;43:687-695]

Frailty Intervention Trial (FIT)
• RCT to prevent development of frailty in people who are pre-frail
• 230 people >=70 years who are pre-frail (Fried cirteria) • 12 month multidisciplinary intervention targetting identified
characteristics of frailty problems during geriatric assessment. www.WEBB.org.au
• Primary outcome : frailty score (Fried); SPPB Secondary outcome: mobility, mood, use of health and community services [Fairhall N et al BMJ Open 2015;5:e007091]

Results and economic evaluation
• 216 participants: at 12 months prevalence of frailty 14.7% lower in intervention group
• Cost for 1 extra person to transition out of frailty = AUD 15,955 (2011 prices) [Fairhall N et al JAMDA 2015;16:41-48]

The LIFE-P study
• 424 people (mean age 76.8) with sedentary lifestyle s and at risk of mobility disability.
• 12 m physical activity intervention versus successful aging education
• Outcome: frailty phenotype at baseline, 6m, 12 m • Significant difference of 10% noted at 12 months
[Cesari M et al J Gerontol: Med Sci 2015; 70(2):216-222]

Summary of interventions for sarcopenia
• Most exercise trials showed improved muscle strength and physical performance but only three out of seven studies showed increased muscle mass
• Nutrition: - Protein supplements - essential amino acid supplements - HMB (hydroxymethylbutyrate) - fatty acids Little effect without adding exercise. HMB showed some effect on muscle function and mass

Cognitive frailty: nutrition intervention

• Deficiencies • Mediterranean Diet • Single vitamin studies (B6, B12..) • Souvenaid

• Role of nutrition in cognitive impairment evolving topic
• Biomarker evidence for biological validity emerging • Epidemiology and RCT evidence for Med diet is
emerging • Single vitamin studies in general negative results • Multi-nutrient intervention rational and evidence for
efficacy in early stages on memory • More research needed into efficacy in relation to
biomarker evidence of deficiency

Cognitive frailty: nutrition and exercise

FINGER Finnish Geriatric Intervention Study to Prevent Cognitive
Impairment and Disability [Ngandu et al Lancet 2015]
• 1260 participants
• 69.4(60-77) years
• MMSE 26.7+2
• 2 year study
• P<.001
• INTERVENTION
Mediterranean Diet
Aerobic Exercise
Resistance Exercise
Computer based cognitive training
Social activity
• CONTROL
Intensive education

Bibliography
• Treating frailty: a practical guide Fairhall N et al BMC Medicine 2011; 9: 83

Conclusion
• Frailty: both physical and cognitive, are relatively new paradigms that are important concepts in achieving active ageing
• Nutrition and exercise have important roles in prevention and/or retarding decline