
Pulmonary function testing (spirometry )
120
Pulmonary Function testing (Spirometry ) Dr. Emad Efat Shebin El kom Chest hospital July 2016
-
Upload
dr-emad-efat -
Category
Health & Medicine
-
view
1.500 -
download
4
Transcript of Pulmonary function testing (spirometry )

Pulmonary Function testing(Spirometry )
Dr. Emad EfatShebin El kom Chest hospital
July 2016

PFTs - Significance
1. Pulmonary Function tests (PFTs) Help in diagnosis and differentiation of many respiratory diseases (restrictive and obstructive lung disorders, diagnose exercise induced asthma, differentiate chronic bronchitis from Bronchial asthma (BA) )
2. Explain the cause of symptoms in patients who are diseased and clinically normal (as early detection of small air way disease)
3. Assessing the course of the disease and effect of therapy (as steroids with Bronchial asthma and radiotherapy with cancer)
4. Objective quantitative measurements of lung damage due to occupational injury
5. Pre-operative assessment

PFTs - Classification
1. Tests of ventilatory function:
Evaluate lung volumes and capacities:
• Spirometry (FVC, FEV1, FEF25-75, MVV)
• Body plethysmography
• Gas dilution method (functional residual capacity (FRC) and residual volume (RV) detection)
Evaluate hypersensitivity: broncho-provocative test
2. Tests for gas exchange: tests of diffusion (DLCo, ABGs) Oximetry for O2 saturation and Capnographyfor trans-cutaneous CO2

PFTs - Classification
3. Other Tests:
Tests for lung compliance
Tests for resistance and impedance: impulse oscillometry
Assessment of regional lung functions
Cardio-pulmonary stress tests (CPX) and assessment of respiratory muscle strength
Breath condensate

Spirometry
• Spirometry with flow volume loops assesses the mechanical properties of the respiratory system by measuring expiratory volumes and flow rates.
• Maximal inspiratory and expiratory effort.
• At least 3 tests of acceptable effort are performed to ensure reproducibility.

ways of representing the spirometry test
Spirometry

Acceptability and Reproducibility Criteria:
1. Acceptability criteria (within maneuver criteria):
Individual spirograms are "acceptable" if:
Lack of artifact induced by coughing, glotticclosure, or equipment problems (primarily leak).
Satisfactory start to the test without hesitation or coughing for the 1st second.
Satisfactory exhalation with 6 seconds of smooth continuous exhalation, or a reasonable duration of exhalation with a plateau of at least 1 second.
Spirometry - Acceptability criteria

Cough Variable Effort
Spirometry - Acceptability criteria
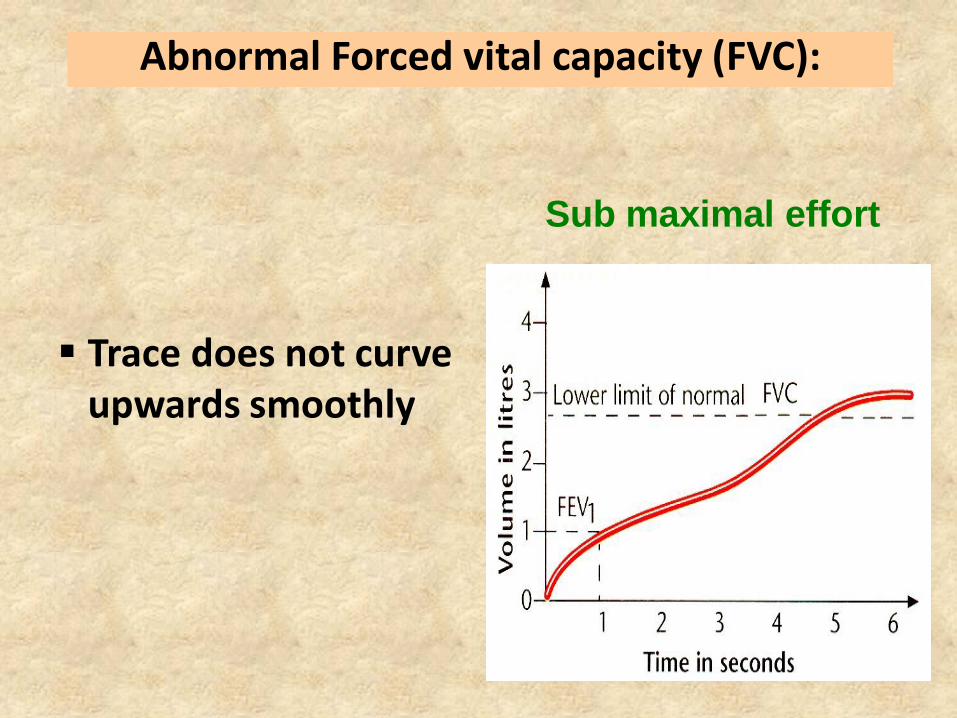
Sub maximal effort
Trace does not curve upwards smoothly
Abnormal Forced vital capacity (FVC):

Early stoppage
• Trace does not curve smoothly up to a plateau
• Affects the volume of the Forced vital capacity
Abnormal Forced vital capacity

Coughing Trace is irregular
Extra inhalation during coughing will affect volume of FVC
Coughing is a common problem with bronchial
hyper reactivity.
Abnormal Forced vital capacity

Extra breath• Trace is not smooth and upward
• Extra breath has affected the volume of the FVC
• Affect FEV1 \ FVC giving a falsely low ratio.
Abnormal Forced vital capacity

Slow start
Patient has not
made a maximum
effort from the start
of the blow
Affects the volume
FEV1 and FEV1 to
FVC
Abnormal Forced vital capacity

acceptable & unacceptable spirometric curves

Again, acceptable & unacceptable spirometric curves

2. Reproducibility criteria (Between maneuver criteria)
After 3 acceptable spirograms have been obtained, apply the following tests:
Are the two largest FVC within 0.2 L of each other?
Are the two largest FEV1 within 0.2 L of each other?
PEF values may be variable (within 15%).
If these criteria are met, the test session may be concluded.
Best two blows within 5% or 200ml of each other.
Spirometry - Reproducibility criteria

If these criteria are not met, continue testing until:
The criteria are met with analysis of additional acceptable spirograms; OR
A total of 8 tests have been performed; OR
The patient cannot or should not continue
Save at a minimum the three best maneuvers
Spirometry - Reproducibility criteria

Spirometry - Reproducibility criteria

Spirometry - Indications
• Indications:
1. Diagnostic
A. To evaluate symptoms, signs or abnormal laboratory tests Symptoms: dyspnea, wheezing, orthopnea, cough, phlegm
production, chest pain
Signs: diminished breath sounds, overinflation, expiratory slowing, cyanosis, chest deformity, unexplained crackles
Abnormal laboratory tests: hypoxemia, hypercapnia, polycythemia, abnormal chest radiographs
B. To measure the effect of disease on pulmonary function

Spirometry - Indications
C. To screen individuals at risk of having pulmonary disease:
Smokers
Individuals in occupations with exposures to injurious substances
Some routine physical examinations
D. To assess pre-operative risk
E. To assess prognosis (lung transplant ...etc.)
F. To assess health status before beginning strenuous physical activity programs

Spirometry - Indications
2. Monitoring
To assess therapeutic intervention
Bronchodilator therapy
Steroid treatment for asthma, interstitial lung disease (ILD), etc.
Management of congestive heart failure
Other (antibiotics in cystic fibrosis, etc.)
To describe the course of diseases that affect lung function
• Pulmonary diseases (Obstructive airway diseases, ILD)
• Cardiac diseases (Congestive heart failure)
• Neuromuscular diseases (Guillian-Barre Syndrome)

Spirometry - Indications
To monitor people exposed to injurious agents
To monitor for adverse reactions to drugs with known pulmonary toxicity
3. To identify flow-volume loop patterns
4. Disability/impairment evaluations To assess patients as part of a rehabilitation program (medical,
industrial, vocational)
To assess risks as part of an insurance evaluation
To assess individuals for legal reasons
5. Public healthEpidemiological surveys and Derivation of reference equations
Clinical research

Spirometry
• Contraindications to Use of SpirometryUncooperative patient and Severe dyspnoea
Infectious diseases (TB) and Hemoptysis of unknown origin
Pneumothorax
Recent myocardial infarction or unstable angina
Acute disorders (e.g., vomiting, nausea, vertigo) .
Recent abdominal or thoracic surgery
Recent eye surgery (increases in intraocular pressure during spirometry)
Thoracic aneurysms (risk of rupture because of increased thoracic pressure)
N.B Spirometry should be avoided after recent heart attack or stroke

Spirometry
• Performing Spirometry
How to do it ?? 1. Withholding Medications Before performing
spirometry, withhold:
Short acting β2-agonists for 6 hours
Ipratropium for 6 hours
Long acting β2-agonists for 12 hours
Tiotropium for 24 hours

Spirometry - Preparation
2. Preparation
Explain the purpose of the test and demonstrate the procedure
Record the patient’s age, height and gender
Note when bronchodilator was last used
The patient sits comfortably
Loosen any tight clothing
Empty the bladder
Breath in until the lungs are full

Spirometry - Preparation
Hold the breath and seal the lips tightly around a clean mouthpiece
Blast the air out as forcibly and fast as possible. Provide lots of encouragement!
Continue blowing until the lungs feel empty
Watch the patient during the blow to assure the lips are sealed around the mouthpiece
Check to determine if an adequate trace has been achieved
Repeat the procedure at least twice more until ideally 3 readings within 5% of each other are obtained.

Spirometry - Quality Control
• Most common cause of inconsistent readings is poor patient technique
• Sub-optimal inspiration
• Sub-maximal expiratory effort
• Delay in forced expiration
• Shortened expiratory time
• Air leak around the mouthpiece
• Subjects must be observed and encouraged throughout the procedure

Inadequate or incomplete blow & Lack of blast effort during exhalation
Slow start to maximal effort
Lips not sealed around mouthpiece
Coughing during the blow & Extra breath during the blow
Glottic closure or obstruction of mouth piece by tongue or teeth
Poor posture – leaning forwards
Spirometry - Common Problems

Spirometry - Lung volumes
Lung volumes that can be measured by spirometer:
1. Static Lung Volumes: Lung volumes that are notaffected by the rate of air movement in and out of the lungs (VT, IRV, ERV, IC and VC).
CAN’T MEASURE – FRC, RV, TLC. It can be measured by:
nitrogen washout technique
Helium dilution method
Body plethysmography
2. Dynamic Lung Volumes: Lung volumes that depend upon the rate at which air flows out of the lungs (FVC, MVV, FEF 25–75, MRV and FEV1)

Lung Volumes and Capacities - Static

Respiratory Volumes - Static
• Static Lung Volumes and Capacities: 4 Volumes
4 Capacities: Sum of 2 or more lung volumes
1. Tidal volume (Vt), about 500 mL, is the amount of air inspired during normal, relaxed breathing.
2. Inspiratory reserve volume (IRV), about 3,100 mL, is the additional air that can be forcibly inhaled after the inspiration of a normal tidal volume.
3. Expiratory reserve volume (ERV), about 1,200 mL, is the additional air that can be forcibly exhaled after the expiration of a normal tidal volume.
4. Residual volume (RV), about 1,200 mL, is the volume of air still remaining in the lungs after the expiratory reserve volume is exhaled.

1. Slow vital capacity (SVC): maximum amount of air that can be expired after deep inspiration by slow expiration
2. Forced (Timed) vital capacity(FVC): maximum amount of air that can be expired after deep inspiration by forced expiration
1. Vital capacity (VC), about 4,800 mL, is the total amount of air that can be expired after fully inhaling.
Vt IRV ERV VC
Respiratory Capacities - Static

Normal Slow vital capacity
• The curve is 1. Smooth
2. Has no irregularities
3. Curves upwards
4. Reaches a plateau
• FVC is read at the
top of the curve,
where it reaches a
plateau

SVC FVC
SVC FVC
SVC FVCX

2. Function residual capacity (FRC), about 2,400 mL, is the amount of air remaining in the lungs after a normal expiration.
Respiratory Capacities - Static
ERV RV FRC

3. inspiratory capacity (IC), about 3,600 mL, is the maximum amount of air that can be inspired (IC = TV + IRV).

4. Total lung capacity (TLC), about 6,000 mL, is the maximum amount of air that can fill the lungs (Vt +IRV+ ERV+ RV) { VC+RV}
TLC < 80% of predicted value = restriction.
TLC > 120% of predicted value = hyperinflation.
VC RV TLC
Vt IRV ERV RV TLC
Respiratory Capacities - Static

Relationship between VC, RV, and TLC
VCVC
VC
RV RV
RV
Normal RV\ TLC20-35%
Restrictive RV\ TLC≤20-35%
Obstructive RV\ TLC>35%


Dynamic Lung Volumes: Lung volumes that depend upon the rate at which air flows out of the lungs (FVC, FEV1, FEF 25–75, MVV, and MRV)
Minute Respiratory Volume (MRV) : quantity of air moved into and out of the lungs in one minute (TVx Respiratory rate).
Respiratory Volumes - dynamic

Forced vital capacity (FVC)
• Total volume of air that can be exhaled forcefully from TLC
• The majority of FVC can be exhaled in <3 seconds in normal people, but often is much more prolonged in obstructive diseases
• Measured in liters (L)

Forced vital capacity (FVC)
• Interpretation of % predicted:
80-120% Normal
70-79% Mild reduction
50%-69% Moderate reduction
<50% Severe reduction

Forced expiratory volume in 1 second (FEV1)
• Volume of air forcefully expired from full inflation (TLC) in the first second
• Measured in liters (L)
• Normal people can exhale more than 75-80% of their FVC in the first second; thus the FEV1/FVC can be utilized to characterize lung disease

• Interpretation of % predicted:
Normal >75%
Mild 70-75%
Moderate 50-69 %
Severe 35-49%
Very severe < 35%
Forced expiratory volume in 1 second (FEV1)

• Mean forced expiratory flow during middle half of FVC
• Measured in L/sec
• May reflect effort independent expiration and the status of the small airways
• Highly variable
• Depends heavily on FVC
Forced expiratory flow 25-75% (FEF25-75)

• Interpretation of % predicted:
>60% Normal
40-60% Mild obstruction
20-40% Moderate obstruction
<20% Severe obstruction
Forced expiratory flow 25-75% (FEF25-75)

• FEV1/FVC ratio: It indicates what percentage of the total FVC was expelled from the lungs during the first second of forced exhalation
• A ratio of <70% implies obstructive disease
• If the patient has a restrictive ventilatory defect, the FEV1 and FVC are both reduced, but in proportion, so the FEV1/FVC ratio remains normal (greater than 75%).
FEV1/FVC ratio

• It is also called the maximal breathing capacity (MBC).
• It's the maximum volume of air which can be respired in 1minute by deepest and fastest breathing (test of entire respiratory system).
• Normal value: male: 80-200 L/min, female: 60-160 L/min.
• Measured by: breathing deeply and rapidly for 15 sec.
• Significance:
Index for respiratory efficiency and physical fitness
Respiratory muscle assessment.
Pre-operative assessment.
• MVV= FEV1 X35
Maximum voluntary ventilation (MVV)

Maximum voluntary ventilation (MVV)

• It's the maximum flow rate over the first 10 milliseconds of forced expiration (first part of FEV1).
• Normal value: 10 L/s (600 L/min) in healthy adult.
• Measured by peak flow meters
• Significance:
Diagnosis of Bronchial asthma ( BA ) variability >15-20 % in PEFR in a single day or from day to day is diagnostic.
Response to treatment in BA
Diagnosis of occupational asthma , and exercise induced asthma (fall of FEV1 >15%)
Peak expiratory flow (PEF)

Peak Flow Meter
Spirometry
Tests of Ventilation


Peak flow meters

1. Normal
2. Obstructive
3. Restrictive
4. Mixed Obstructive and Restrictive
Spirogram Patterns
Criteria for Normal Post-bronchodilator Spirometry
FEV1: % predicted > 80%
FVC: % predicted > 80%
FEV1/FVC: > 0.7

Spirogram Patterns
Obstruction caused by: Restrictions caused by:
COPD
BA
Bronchiolitis
Pneumonia
Bronchiectasis
Cystic fibrosis
Acute bronchitis
Alpha1 anti-trypsin
deficiency
Obesity
Pregnancy
Ascitis
Interstitial lung disease
Kyphoscoliosis
Pleural effusion
Pleural tumors
Neuromuscular disease
Diaphragmatic abnormality
Lung resection
Congestive heart failure
Inability to breathe (pain)
Severe obstructive disorders
Cardiomegally

• Criteria: Obstructive Disease
FEV1: % predicted < 80% ( used to grade the severity )
FVC: Can be normal or reduced – usually to a lesser degree than FEV1
FEV1/FVC: < 0.7
SPIROMETRY OBSRUCTIVE DISEASE

• Criteria: Restrictive Disease
FEV1: % predicted < 80%
FVC: % predicted < 80%
FEV1/FVC: > 0.7
SPIROMETRY RESTRICTIVE DISEASE

• Criteria: Mixed Obstructive/Restrictive
FEV1: % predicted < 80%
FVC: % predicted < 80%
FEV1 /FVC: < 0.7
SPIROMETRY Mixed Obstructive/Restrictive

Measures of Assessment and Monitoring of Asthma
• Asthma diagnosis criteria:
Repeated variability in well-performed spirometic values (increase in FEV1 or FVC).
Positive bronchodilator (BD) responses (increase in FEV1 or FVC ⩾12% and 200 mL from baseline).
Positive methacholine challenge (20% fall in FEV1 at a dose ⩽8 μg/mL).
Objective lung function measurements in Asthma:
Spirometry:
Forced Expiratory Maneuvers.
Exhaled Nitric Oxide.
Peak Flows.

FEV1 Results for Asthma

Positive bronchodilator responses in asthma

GOLD 2013: Diagnosis of COPD

At Risk for COPD
Spirometric classification of airflow limitation
• Adapted from GOLD 2013
in patients with FEV1/FVC < 0.70
GOLD 1 MildFEV1 ≥80%
predicted
GOLD 2 Moderate50% ≤FEV1 <80%
predicted
GOLD 3 Severe30% ≤FEV1 <50%
predicted
GOLD 4 Very severeFEV1 <30%
predicted

Changes in Lung Volumes in Various Disease States
• Total lung capacity ( TLC ) < 80% of predicted value = restriction.
• TLC > 120% of predicted value = hyperinflation.

Volume Restrictive Air trapping Hyperinflation
TLC ↓ N ↑
VC ↓ ↓ N
FRC ↓ ↑ ↑
RV ↓ ↑ ↑
RV/TLC% N ↑ ↑
Changes in Lung Volumes in Various Disease States

Bronchodilator Reversibility Testing
Provides the best achievable FEV1 (and FVC)
Helps to differentiate COPD from asthma
Must be interpreted with clinical history - neither
asthma nor COPD are diagnosed on spirometry alone
bronchodilating agents:
Bronchodilator DoseFEV1 before and
after
Salbutamol 200 – 400 µg via large
volume spacer15 minutes
Terbutaline 500 µg via Turbohaler® 15 minutes
Ipratropium 160 µg via spacer 45 minutes

Bronchodilator Reversibility Testing
• Preparation
• Tests should be performed when patients are clinically stable and free from respiratory infection
• Patients should not have taken: Withholding Medications:

Bronchodilator Reversibility Testing - Spirometry
1. FEV1 should be measured (minimum twice, within 5%)before a bronchodilator is given.
The bronchodilator should be given by metered dose inhaler through a spacer device or by nebulizer to be certain it has been inhaled
2. FEV1 should be measured again:
10-15 minutes after a short-acting b2-agonist
30-45 minutes after the combination
The test is considered significant if there is
> 12% increase in the FEV1 and 200 ml improvement in FEV1 OR
> 12% increase in the FVC and 200 ml improvement in FVC.

• To express the degree of improvement: • Calculate the absolute changes in FEV1
• Calculate the absolute changes in FEV1 from base line
• % improvement in FEV1=
FEV1 (post BD)- FEV1 (base line) X100
FEV1 (base line)
Measuring degree of reversibility

Bronchodilator Reversibility Testing
- Spirometry

Normal flow volume loop has a rapid peak expiratory flow rate with a gradual decline in flow back to zero.
Flow Volume Loop

• As with a normal
curve, there is a
rapid peak
expiratory flow, but
the curve descends
more quickly than
normal and takes on
a concave shape
Flow Volume Loop in Obstructive lung disease
Obstruction

ObstructionNormal

Restriction
The shape of the flow volume loop:
1. Relatively unaffected in restrictive disease
2. Overall size of the curve will appear smaller when compared to normal on the same scale.
Flow Volume Loop in restrictive lung disease

Flow Volume Loop

Spirometry interpretation
1.
Assess validity
2.
Determine ventilatory pattern
3.
Grade severity
4.
Grade response to BD challenge

Interpreation of results
Take the best ofthe 3 consistent readings
of FEV1 and of FVC

Predicted Normals = Predicted Value
Depends on:
1. Age
2. Sex
3. Height
4. Race

Results classification
1. Normal
2. Obstructive
3. Restrictive
4. Combined

1. Obstructive
Pattern
2. Restrictive
Pattern
3.
Mixed Pattern
Abnormalities of lung function are categorized as:

Value (95 % function test confidence interval)
BMI 21- 25 kg/m2
FEV1 80-120%
FVC 80-120%
FEV1 /FVC > 80%
FEF 25-75% 65
TLC 80-120%
FRC 75-120%
RV 75- 120%
RV/TLC 20-35%
FRC/TLC 50%
Normal Values of Pulmonary Function Tests

Objective Measures: Spirometry
Is airflow obstruction present and is it at least partially reversible?
Use Spirometry to establish airflow
obstruction
1. FEV1/FVC <70%
2. FEV1 < 80%
Use Spirometry to establish reversibility
1. FEV1 increases >12% and at least 200 ml. after using inhaled SABA
2. A 2- to 3-week trial of oral corticosteroid therapy may be required to demonstrate reversibility

1. Patients data (age, sex, body weight, height)
BMI
2. Expiratory Time
3. Static lung volume
4. Dynamic lung volume (FEV1\ FVC, FEV1,
FVC, PEFR, PIFR, FEF25-75)
5. MVV
Interpretation of Spirometry

1). BMI= weight \ kg
(Height m)2
Interpretation of Spirometry
21-25
Normal
BMI
No effect
on PFT
< 21
Under
weight
Nutrition
suppleme
ntation
> 25
>25 < 30 >30 < 40 >40
Morbid
obesityObese
Over
weight
Restrictive pattern on
PFT

2). Expiratory Time
Interpretation of Spirometry
Expiratory Time
< 4 sec.
Poor initial effort
Restrictive
Pattern
Respiratory muscle
weakness
> 6 sec.Obstructive
Pattern
Normal
4-6 sec.

• imp NB: - Marked prolongation of exp.
Time denote either:-
Incorrect test …..or
Resp. center depression → drug overdose,
brain stem infarction, head trauma, bilat.
diaphragmatic paralysis→ all of these causes
mean marked noncompliance & incorrect test
Interpretation of Spirometry

3). SVC
Interpretation of Spirometry
SVC
< 80
Restrictive pattern
Severe obstructive
pattern
Combined pattern
80 - 120
Normal

• imp NB:-
– From TV we can calculate minute
ventilation
– MV= TV X RR (from Exp. T)
– FVC slightly less than SVC , but if there
is marked disparity → one of 2 tests is
incorrect
Interpretation of Spirometry

SVC FVC
SVC FVC
SVC FVCX

4). Dynamic lung volume:
• FEV1\ FVC
Interpretation of Spirometry
FEV1\ FVC 80-120 %
Nor. Or ↑
Normal
Restrictive
70 -80% Combined
< 70 % Obstructive

Interpretation of Spirometry
FVC
< 80%
Restrictive pattern
Severe obstructive
pattern
Combined pattern
80 – 120%
Normal
4). Dynamic lung volume:
• FVC

4). Dynamic lung volume:
• FEV1: 75 -85%
Interpretation of Spirometry
↓FEV1
Marked↓↓ Obstructive
slight↓ Restrictive
Combined

4). Dynamic lung volume:
• FEF 25 -75 % : 65 % (4-5 L\ S)
• Denote small airway diseases
• The only ventilatory parameters effort
independent
Interpretation of Spirometry

4). Dynamic lung volume:
• maximal voluntary ventilation (MVV)
MVV
Decrease
Obstructive Restrictive Resp. muscle
weakness
Neuro
muscular
Normal or↑↑
Restrictive Normal
Interpretation of Spirometry

4). Dynamic lung volume:
All parameters of obstructive lung defects are similar to that of combined defects and differentiated only by TLC
Interpretation of Spirometry
Normal or increase TLC
Obstructive pattern
Decrease TLC
Combined
Pattern

Interpreation of results of Spirometry
• Step 1. Look at the Flow-Volume loop to determine acceptability of the test, and look for upper airway obstruction pattern.
• Step 2. Look at the FEV1 to determine if it is normal (≥ 80% predicted).
• Step 3. Look at FVC to determine if it is within normal limits (≥ 80%).
• Step 4. Look at the FEV1/FVC ratio to determine if it is within normal limits (≥ 70%).
• Step 5. Look at FEF25-75% (Normal (≥ 60%)

Interpreation of results of Spirometry
• If FEV1, FEV1/FVC ratio, and FEF25-75% all are normal, the patient has a normal PFT.
• If both FEV1 and FEV1/FVC are normal, but FEF25-75% is ≤ 60% ,then think about early obstruction or small airways obstruction.
• If FEV1 ≤ 80% and FEV1/FVC ≤ 70%, there is obstructive defect, if FVC is normal, it is pure obstruction. If FVC ≤ 80% , possibility of additional restriction is there.
• If FEV1 ≤ 80% , FVC ≤ 80% and FEV1/FVC ≥ 70% , there is restrictive defect, get lung volumes to confirm.

Interpreation of results of Spirometry
• Different patterns: Mixed
A reduced FVC together with a low FEV1/FVC%
ratio is a feature of a mixed ventilatory defect,
or air trapping.
It is necessary to measure the patient's total
lung capacity to distinguish between these two
possibilities.

FEV1\FVC
> 70%
Normal or restrictive
< 70 %
Obstructive
FVC or TLC
Decrease Normal
Normal Spirometry
Restrictive
DLCO
Normal chest wall
↓ Lung diseases
FEV1 (severity)
FVC
↓↓Normal
or ↓
TLC
↓ combined ↑↑
Pseudo- restriction
Pure
Obstruction

Again , more simple

Parameter Obstructive Combined Restrictive
Expiratory time > 6 sec. <4-4 sc. < 4 sec.
FEV1 \ FVC ↓70% 70-79% Normal or ↑
FVC Normal or ↓ ↓ ↓↓
FEV1 Marked ↓↓ ↓ Normal or
slightly ↓
PEFR ↓↓ ↓ Normal or ↑with
linear ↓in flow
vs. lung volume
PEF 25-75% ↓↓ (COPD) ↓ Normal or ↓↓
MVV ↓↓ ↓↓ ↓
TLC Normal or ↑ ↓ ↓↓
Classification of Ventilatory Abnormalities by Spirometry

• Normal• SVC=FVC ≥ 80%
• FEV1 ≥ 80%
• FEV1\FVC (IVC) ≥ 80%
• FEF 25-75 ≥ 65%
• FEF50\ FIF50≤ 1
• ET= 4-6 sec
• MVV (male 80-200 L, female 60-160 L)
• Obstruction• SVC=FVC = 80% N
• FEV1
• FEV1\FVC (IVC)
• FEF 25-75 < 65%
• FEF50\ FIF50 ≤ 0.3
• ET= ≥ 6 sec
• MVV
• Restrictive • SVC=FVC
• FEV1 N
• FEV1\FVC (IVC) N \
• FEF 25-75 ≥ 65%
• FEF50\ FIF50≤ 1
• ET= 4
• MVV (male 80-200 L, female 60-160 L)


FVC NORMALFVC < 80% Pred.
80%
Normal Lungs
FEV1÷FCV is N
Obstructive Disease
FEV1÷FCV is Low
Restrictive Disease
FEV1÷FCV is High
Combined Obs+Res
FEV1÷FCV is N or L
The Four Square GameF
EV
1 N
OR
MA
LF
EV
1<
80
% o
f P
d.
80%

In normal subject: FIF 50% or MIF50% is usually greater than FEF50%
SO, FEF50% / FIF50% → <1
Upper airway obstruction

Upper airway obstruction
FEF50 %
FIF50%
(MEF 50\ MIF 50%)
1 or near 1
MEF 50= MIF 50%
Fixed large airway
obstruction
High (> 1)
FIF50%
Variable extra-thoracic airway
obstruction
Very low (0.3)
FEF50%
Variable intra –thoracic air way
obstruction

1. If FEF50% / MIF50% → Less than 1→ normal2. If FEF50% = MIF50% or FEF50% / MIF50% → 1 or near 1→
fixed large airway obstructionDD:- goiters, Neoplasm, foreign body, or stricture from previous intubationNB:- Observe FEV1 & FIV1 are nearly equal.
3. If FEF50% / MIF50% → High (usually greater than 2) →variable extra thoracic airway obstruction e.g.: vocal cord paralysis, thyromegaly, tracheomalacia, or neoplasm
NB:- Observe FEV1 is greater than FIV1 .
4. If FEF50% / MIF50% → Very low (may reach 0.3) →variable intra thoracic airway obstructione.g.: tracheomalacia or neoplasmNB:- Observe FEV1 is lower than FIV1
Upper airway obstruction

Upper Airway Obstruction
• Truncation of flow loop:
Expiratory – Intra Thoracic
Inspiratory –Extra Thoracic
Both – Fixed Obstruction

Patterns of Abnormality

Patterns of Abnormality

Patterns of Abnormality









Thank you


















