Psychosomatics lecture - web.vu.lt
30
Psychosomatics lecture 1
Transcript of Psychosomatics lecture - web.vu.lt
Psychosomaticslecture
1

HistoryofpsychosomaticsIFromtheverybeginningofthemedicineitwas
dividedbytheparadigmaticdualism:medicineoforgansvs.medicineoffunctions
Primitivemedicine:shamanicmedicine,CentralAmerica‘sLadynos;� TheideaexpressedinOldTestament,thatbodyhealthisinseparablefromthehealtofsoul(BookofJob)� Plato:“...partcannotbehealthyiftheunityisnothealthy”(Charmides)� ErasistratusfromAlexandria(IIIB.C.)diagnosed„incurable“diseaseofthesonofthekingofSyriawhichwasduetotheloveofthefathersnewwifeStratonike,andhewascured(!);
2

HistoryofpsychosomaticsIIInthemedievalIslamicworldthePersianpsychologist-physiciansAhmedibnSahlal-Balkhi(d.934)andHalyAbbas(d.994)developedanearlymodelofillnessthatemphasizedtheinteractionofthemindandthebody.Theyproposedthatapatient'sphysiologyandpsychologycaninfluenceoneanother.
3

HistoryofpsychosomaticsIII� RenéDescartes(1596–1650,France)–oneofmaintheoreticiansof„dualism“,whodividedphenomenainttwocathegories-“resextensa”and“rescogitans”(however,originallystatingitwillnotapplyformedicine)� BaruchSpinoza(1632–1677,theNetherlands)thought,thateveryeventinthepsychehasitsparalleleventinthebody–“ideoplasia”� G.W.Leibnitz(1646–1716,Germany)thought,thatthereisnointerconnectionbetweenbodyandsoul,butpredestinedcoordinationoftheeventsinbothrealms–„aharmony“
4

Historyofpsychosomatics
� J.C.Heinroth(1773–1843,Germany)–theauthoroftheterm„psychosomatics“(1818),usedtodescribethedevelopmentofinsomnia
� H.Maudsley(1835–1918,UK)–“Ifemotionsarenotexpressedbytheexternalsignsortheworkoftheorganism,theyinfluenceourorgansanddamageitsfunctions;[e.g.]sadnessisbestexpressedthroughtearsandlament...”(1876)
5

HistoryofpsychosomaticsV� S.Freud‘spsychoanalysiswasatheoreticalbackgroundforthedevelopmentofpsychoso-maticsinthe1sthalfoftheXXcentury.Mostprominentauthorsofthisperiodwere:◦ F.Dunbar(handbookin1948)◦ F.Alexander(handbookin1950)◦ F.Deutsch(handbookin1953)
� Essentialparadigmofallthesetheorieswasaconceptofintrapsychicconflictanditsinfluenceonthepathologyoftheorgansystems.
6

HistoryofpsychosomaticsAfterWWIImaincenterofthedevelopmentof
psychosomatics becameNorth America and Europe(esp. Germany). Until now in many Germanuniversities clinics of psychosomatic medicine areactive (sometimes combined with psychotherapy),andmanypsychosomaticdepartmentsorwardsareoperatinginNHCS(e.g.,inKur‘s).MaintheoreticiansoftheendofXXcentury:� Th.vonUexküll,M.vonRad(Germany)� P. Sifneos, J. C. Nemiah, M. Freedman, R.Rosenman,T.Holmes,R.Rahe(USA)� Z.Lipowsky(Canada)
7

Maintheoreticalparadigmsofpsychosomatics
1. Personality–specificparadigmofpsy-chosomatics
2. Event–specificparadigmofpsychoso-matics
3. Unspecificparadigmofpsychosomatics
8

Personality–specificparadigmofpsychosomatics
� S.Freud:“Somaticsymptomsmaybeproducedbypsychologicalcauses”
Thisgeneralstatementwasinterpretedbyseveralauthorsinaspecificways:� F.Dunbar–lookingforarelationshipbetweenspecificpersonalitytypesandrespectivediseases;� F.Alexander–connectedspecificintrapersonalconflicts(betweenaggressionandthedependencyneed)inspecialsituationswithspecificpsychosomaticreactions:
◦ DominanceoftheSympatheticnervoussystemincaseoftherepressionofaggression(hypertension)◦ DominanceoftheParasympatheticnervoussystemincaseoftherepressionofdependencyneeds(rheumatoidarthritis,ulcer)
9
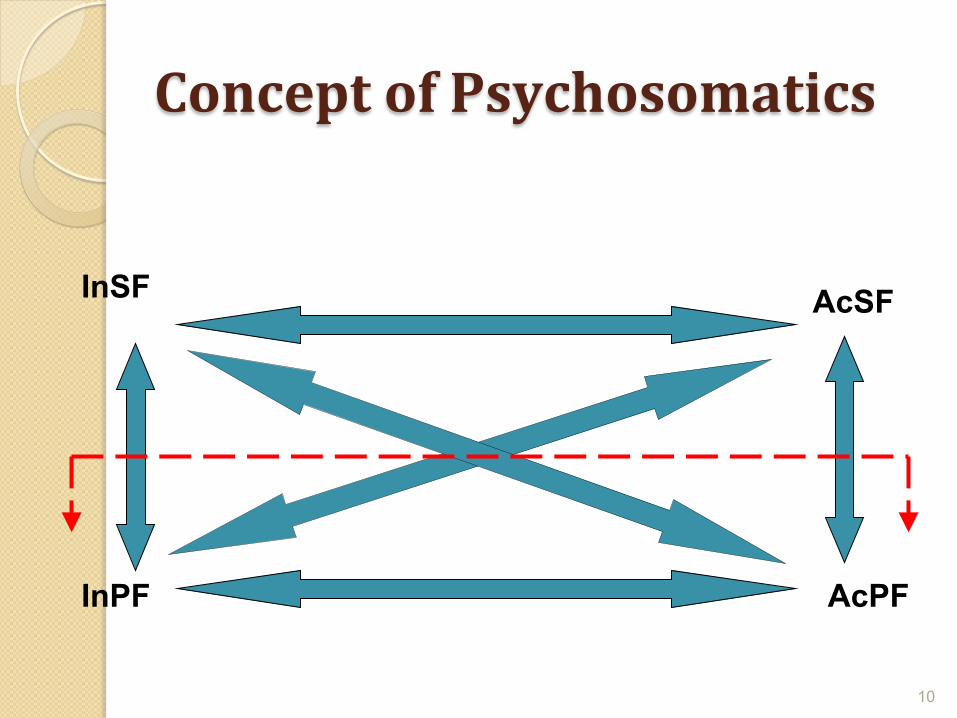
ConceptofPsychosomatics
10
InSF AcSF
AcPF InPF

Personalityspecificpsychosomatics
Aleksithymia(a-lexis-thymos)isaconceptofarelationbetweenunexpressedemotionsinlanguageofthesubjects(contentanalysis)andpsychosomaticdiseases:� Healthysubject� Neuroticpatients� PsychosomaticpatientsP.E.SifneosandJ.Nemiah(1972-1973),
11
2,5X
TypeAbehaviour(TAB)TABfoundbyM.FriedmanirR.H.Rosenmanin1959
m.ResearchprojectwascarriedintheInstituteofHeart,Lungs,andBloodofChicago,included3460healthymen49–54yearsofage.Itwasafirstprospectivestudyinafieldofpsychosomatics.TwotypesofbehaviorswerefoundconnectedwithCHDandlabeledA/B.EssentialfeaturesofTAB:
1. Constanttimerestrain1. “Steppingupon”theendofthesentence2. Inabilitytodrive„atthetail“3. Rushtomakeallpossiblejobs
12

TypeAbehaviour(TAB)2.Aggressiontowardslife:
• Loud,overpowering,anddecisivespeech• Inabilitytoloseatanysituation• Inabilitytovaluedonejobs• Attemptstodomoreandmore
3.Thisproducesaconstantstresssituation:1. PeriorbitalhyperpigmentationHypophysisACTH(+TTH) pigment
13

TypeAbehaviour(TAB)ImpactofTABoncoronaryheartdisease:
� TABdemonstratingsubjectsmaketo98,5%ofthosewithCHDandMI;� Innateformsmakeonlyabout20%ofcases,therest–conditionedTAB� TABcanbemodified,andaftermodificationtheriskofasecondMIdecreasessubstantially(intheexperimentalgroupMIhappened45%lessduring4yearsfollow-upafterfirstMI,andevenamonghealthycontrolstheincidenceofMIwassignificantlylower,thaninthepopulation)� TABmodificationispossibleonlybyPTmeans
14

TypeAbehaviour(TAB)ProblemsindiagnosticsofTAB:
� Onlyapartofsymptomscanbediagnosedusingtests(only17of35canbediagnosedbypsychologicinstruments)� Behaviouralsymptoms(18)canbediagnosedonlyafterspecializedtraining� Absolutemajority(85%)ofcardiologistsdemontrateTABthemselves(Blankenhornetal.,1981)
15

16

Event-connectedpsychosomatics� Vietnamwar(1959[1964-USA]–1975)veteransfromUSA(19–22m.)after12monthsinjunglehadscleroticchangesintheiraortas,resemblingthesameas55–60yearsoldinanordinarylifeconditions.� Thelossofaspouse–increasesarisktodieinconsecutive6months(mainlyforheartattack)2x,comparedtothesameagesubjectwhohasn’tlostthespouse.
17

Event-connectedpsychosomatics� Processofmourninganditspsychosomaticconsequences.� Stages:◦ Denialandaggression◦ Acceptanceanddepression(frequentpaindisorders):
� Vague(non-specific)� Identificatory(intheorganorsystem,wherethediseaseofthedeceasedwaslocalized
◦ ReadaptationAgriefwhichisnotcompletedincreasesthe
riskofpsychosomaticdisorderssignificantly!18

Nonspecificconceptofpsychosomatics
� Stress(generaladaptationsyndrom)conceptwasintroducedbyHansSelyein1936.� In1975hedivideditintoeustress(whichincreasesaresistanceofthesubject)andadistress(whencompensationmechanismsareexhausted,anddis-adaptationstarts).Extentofstressdependson:◦ Experienceofchange(inexternalorinternalreality)◦ Personalexpectations◦ Copingmechanisms
19

Stresscurve
20

Physiologyofthestress
21
22
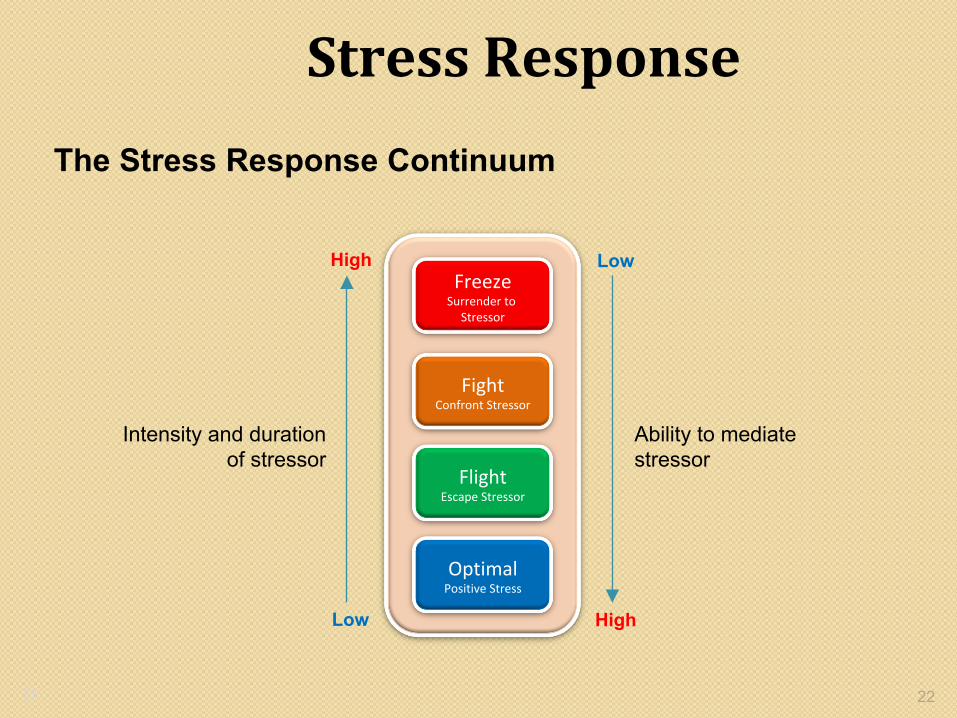
StressResponse
OptimalPositiveStress
FlightEscapeStressor
FightConfrontStressor
FreezeSurrenderto
Stressor
Intensity and duration of stressor
Ability to mediate stressor
High
High Low
Low
The Stress Response Continuum
22

Socialreadaptationscale� T.HolmesirR.Rahein1967proposedthescaleformeasuringlifechanges(LCU)aftertheevaluationoftheimpactofdifferentlifeeventsonthesomatichealthof>5000in-andout-patientscasehistories.Itwasdemonstarted,thatforbothchildrenandadults,whocollectedinapreviousyearLCU‘s:
>300–highriskofdisease299÷150–moderateriskofdisease≤149–lowriskofdisease
23

LCUscaleforadultsLIFECHANGEUNITS
EVENTIMPACT
[]DEATHOFSPOUSE100
[]DIVORCE73
[]MARITALSEPARATION65
[]JAILTERM63
[]DEATHOFCLOSEFAMILYMEMBER63
[]PERSONALINJURYORILLNESS53
[]MARRIAGE50
[]LOSSOFJOB47
[]MARITALRECONCILIATION45
[]RETIREMENT45
[]CHANGEINHEALTHOFFAMILYMEMBER44
[]PREGNANCY40
[]SEXDIFFICULTIES39
[]GAINOFNEWFAMILYMEMBER39
[]BUSINESSREADJUSTMENT39
[]CHANGEINFINANCIALSTATE38
[]DEATHOFCLOSEFRIEND37
[]CHANGETODIFFERENTLINEOFWORK36
[]CHANGEINNUMBEROFARGUMENTSWITHSPOUSE35
[]DEBTOFMORETHAN$10,00031
[]TROUBLEWITHIN-LAWS29
[]OUTSTANDINGPERSONALACHIEVEMENT28
[]SPOUSEBEGINSORSTOPSWORK26
[]BEGINORENDSCHOOL26
[]REVISIONOFPERSONALHABITS24
[]TROUBLEWITHBOSS23
[]CHANGEINWORKHOURSORCONDITIONS20
[]CHANGEINRESIDENCE20
[]CHANGEINSCHOOLS20
[]CHANGEINRECREATION19
[]CHANGEINCHURCHACTIVITIES19
[]CHANGEINSOCIALACTIVITIES19
[]DEBTOFLESSTHAN$10,00017
[]CHANGEINSLEEPINGHABITS16
[]CHANGEINNUMBEROFFAMILYGET-TOGETHERS15
[]CHANGEINEATINGHABITS15
[]VACATION13
[]CHRISTMAS12
[]MINORVIOLATIONSOFTHELAW11
24

25

26
MediatingStressThe amount of stress we experience in a given situation is mediated by our perception of how prepared we are to effectively confront it. Sapolsky (2004) has argued that the amount of stress experienced is determined by two psychological factors:
CONTROL PREDICTABILITY
26

27
MediatingStressCONTROL: The feeling that one is in control of the situation buffers the individual against stress. EX: A well-trained and well-armed police officer feels a relatively high degree of control most of the time, and thus they experience less stress than a civilian would in a similar situation. PREDICTABILITY: Being familiar with a crisis-producing situation, including the potential outcomes, also provides a buffer against stress. EX: As a result of training and experience, a police officer knows what to expect most of the time when entering a crisis situation. This high level of predictability increases control and reduces stress.
27
28
MediatingStressLOCUS OF CONTROL (Rotter, 1954, 1990) A person can have either an INTERNAL or EXTERNAL locus of control. Those with an internal orientation believe they are in control of their own destiny, regardless of the circumstances. Those with an external orientation believe their fate is determined by external forces, and that they have little control over their circumstances. Self-efficacy is the belief one has in their ability to achieve a successful outcome. High self-efficacy leads to a high level of confidence. Thus the following…
Internal locus + Self-efficacy = Control
Experience + Training = Predictability
Control + Predictability = Reduced levels of stress 28

29
MediatingStressLOCUS OF CONTROL (Rotter, 1954, 1990)
Assertive
Helpless
Confident
Cautious
Doubting
Indecisive
Low
High
Abi
lity
to m
edia
te th
e st
ress
or
High
Low
Leve
l of
stre
ss e
xper
ienc
e
29
30
MediatingStress
WHAT DOES IT ALL MEAN? 1. It is important that those agencies tasked with
crisis response focus their hiring and recruiting efforts on individuals who demonstrate an INTERNAL orientation.
2. Repetitive and realistic training is critical to increasing a sense of control and predictability in those who respond to crisis.
30