Prosthetic Treatment For Difficult Cases Of Completely Edentulous Cl II And Cl III Patients
55
Prosthetic Treatment For Difficult Cases Of Completely Edentulous Cl II And Cl III Patients Done By: Mohammed AbdulAziz Supervised by: Dr Faeza M Hussain
-
Upload
mohammed-aziz -
Category
Health & Medicine
-
view
39 -
download
1
Transcript of Prosthetic Treatment For Difficult Cases Of Completely Edentulous Cl II And Cl III Patients

Prosthetic Treatment For Difficult Cases Of Completely
Edentulous Cl II And Cl III Patients
Done By: Mohammed AbdulAzizSupervised by: Dr Faeza M Hussain

Introduction When talking in general about steps of complete denture
fabrication and occlusal scheme of complete denture, we discuss mainly a class I jaw relation and how to set teeth in class I incisal and molar relation.
But applying these concepts to all patients, will lead definitely to failure in a huge number of cases.
Consideration now needs to be given to those situations where a considerable discrepancy in the horizontal jaw relationship exists. This seminar will deal with the retrognathic situation and with the prognathic situation to see what possible solutions we can do to deal with them.

Content Introduction. Ridge Relation. Development of the natural occlusion. The prosthetic problem. Retrognathic jaw relation.
The prosthodontic problem in retrognathic jaw relation. Possible solutions.
Prognathic Jaw relation. The prosthodontic problem in prognathic Jaw relation. Possible solutions.
Lingualised Occlusion In retrognathic jaw relation In prognathic jaw relation
Surgical Correction Case Reports Conclusion References

Ridge Relation
We have two types of classes that we consider in our study here Dental Classification Skeletal Classification Both are equally important to our complete denture being
fabricated since the skeletal relation affects mainly the final occlusion of the denure.
And previous teeth position greatly affects forces on teeth from facial muscles and determine aesthetics and position of neutral zone.
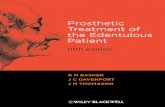
Angles ClassificationFor Incisors-Canines-Molars

Ridge Relation According to GPT “the positional relation of the mandibular ridge to the
maxillary ridge” maxilla resorbs upward and inward while the mandible resorbs downward and
outward

Normal ridge relation normal ridge relationship: The maxillary and mandibular ridges are
considered to be in normal relation when, in centric relation, the upper ridge in the anterior region is slightly labial to the lower ridge.
When, in the posterior region, the interalveolar crest line between two ridges forms an 80 degree angle to a horizontal plane, i.e., the crest of the lower ridge is slightly buccal to that of the upper ridge.(B.K. Goyal, 1974)

Normal Vs Abnormal
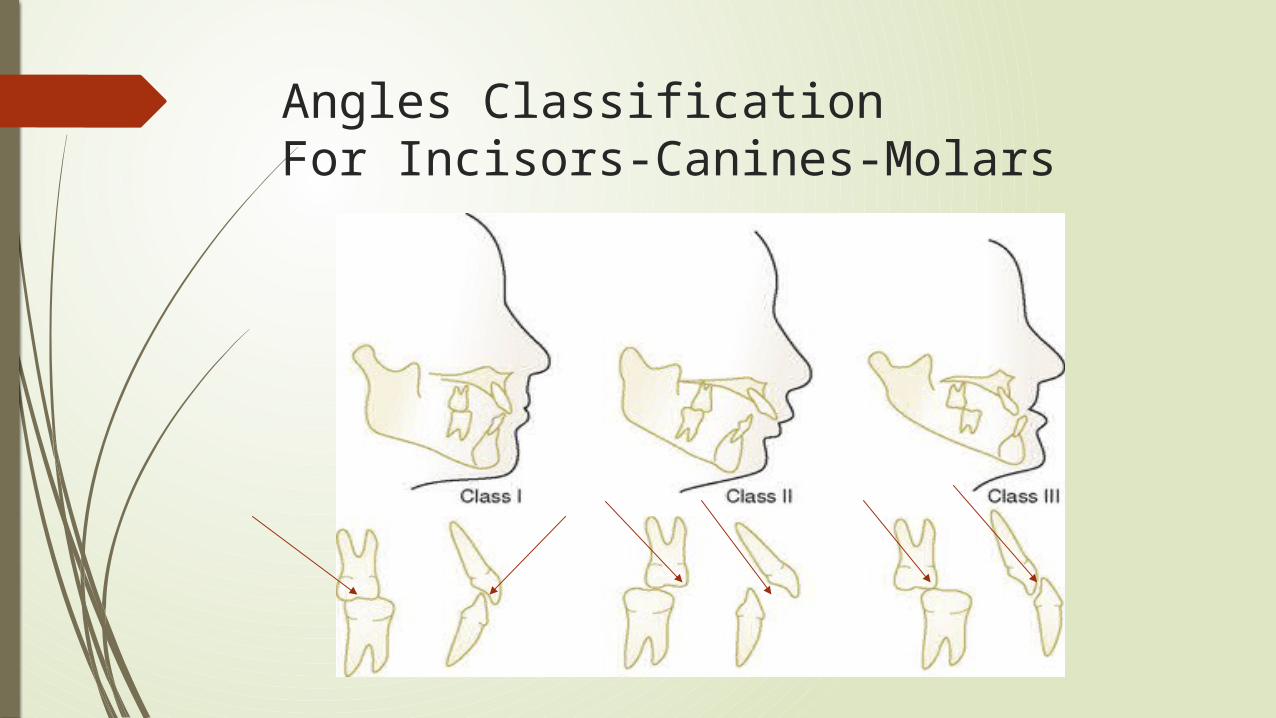
Development of the natural occlusion As teeth erupt into the oral environment, their position is
influenced by the activity and posture of the surrounding muscles, the size, shape and relationship of the jaws, and the occlusal forces produced by tooth contact.
The position of natural teeth is influenced more by the long-term forces associated with muscle posture than by the short-term forces occurring during function.
Complete dentures displaced both by the short-term functional forces and also perhaps by the long-term postural forces.
The design of complete dentures particularly that of the lower prosthesis, therefore has to take muscular displacement into account if stability is to be achieved.
Short-term
Long-term
Long-term
Short-term
Natural Complete denture

The prosthetic problem
When both clinician and dental technician are first taught to set up artificial teeth for complete dentures, it is traditional to position them in a Class I incisal relationship with a horizontal overlap of 2 mm and a vertical overlap of 2 mm.
But for how many edentulous patients does this ‘normal’ incisal relationship resemble the previous natural dentition?

Foster & Walpole Day 1974
44% !!!

Foster & Walpole Day 1974
41% !!!

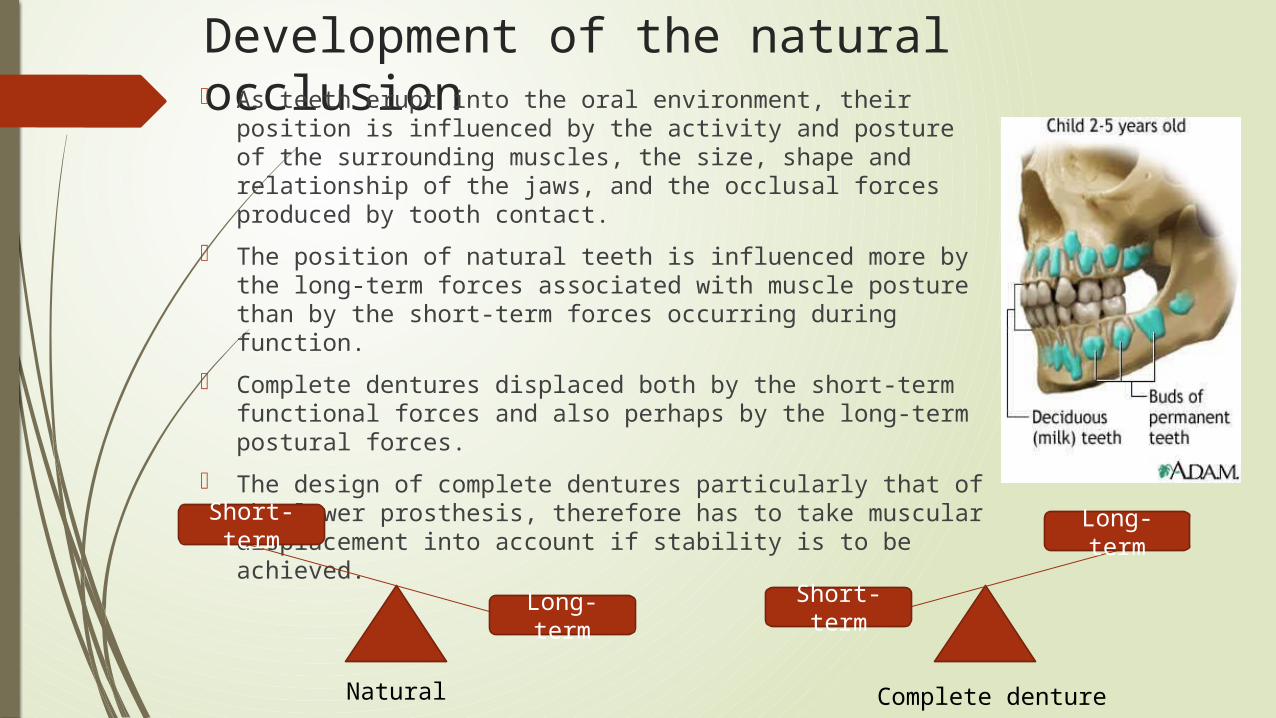
Surveying of Local Factors in Edentulous Iraqi PopulationDr Abbas F. Al-Rahmani
Ridge relationship:There are centric and eccentric jaw relationships. This study was concerned only with centric jaw – relationship. This relation can be classified into three classes as fallow:-
a.Class I:- in which the most anterior point of the upper jaw is located on the same alignment with the most anterior point of the lower jaw or slightly anterior to it, about(2)mm.
b.Class II:- in which the most anterior point of the mandible is retruded more than (2)mm from that of the maxilla.
c.Class III:-in which the most anterior point of the mandible is protruded. In other wards the mandible is anterior to the maxilla.

Retrognathic jaw relation
OrthodontistsClass II Div 1
Class II Div 2

Retrognathic jaw relation
ProsthodontistsHigh FMA
Low FMA

High FMA OR Class II Div 1 Problems:
Condylar guidance steeper in the high FMA group. In the high FMA group the ridges diverge
considerably, it is possible to reduce the occlusal vertical dimension to improve this divergence but it has adverse effects.
Skeletal Class II individuals have an extensive range of motion of the mandible
Post: different sizes of the arches means that a narrowing of the arch in the premolar region, because a narrow segment of the lower arch must articulate with a wider part of the upper

Anterior teeth setting In this case we have two solutions: Either to set the upper anterior teeth
more palataly, just like class I relationship.
but this will cause aesthetic problems by “collapsing” the upper lip and, more importantly, functional problems by limiting the forward movement of the mandible.

Or the final solution will be to reduce the overbite by setting the upper anteriors a little higher.
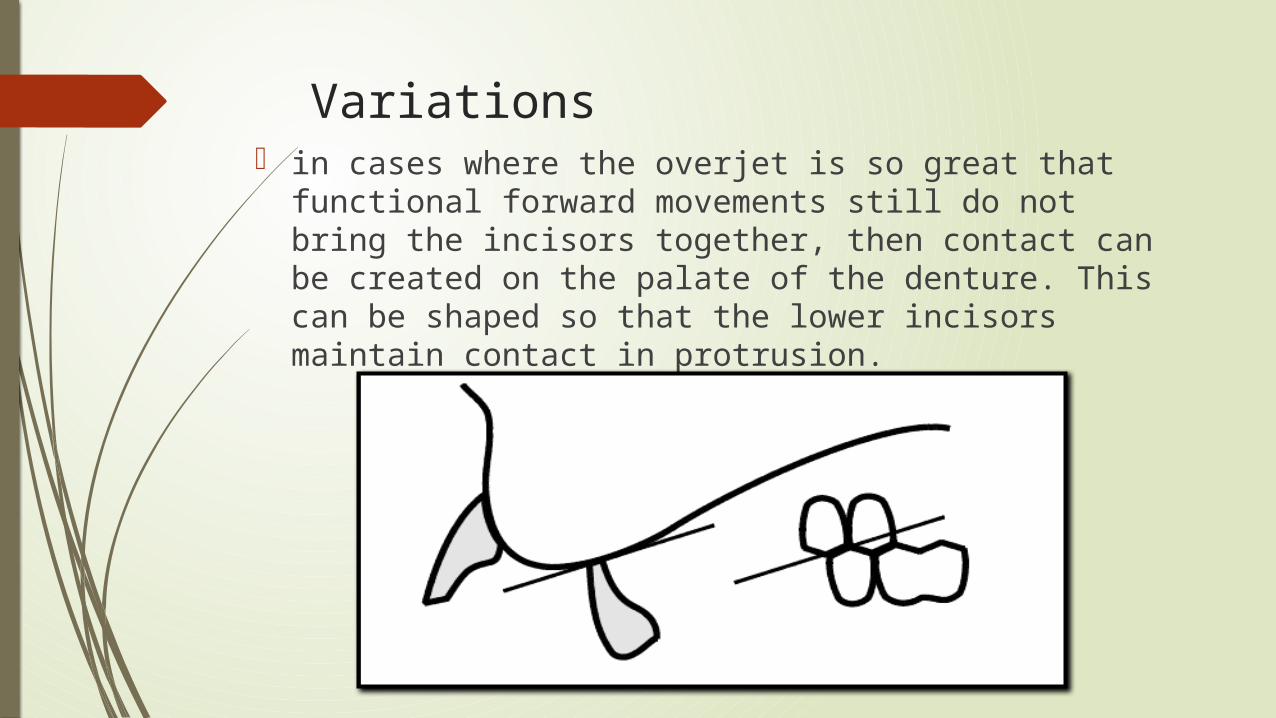
Variations in cases where the overjet is so great that functional
forward movements still do not bring the incisors together, then contact can be created on the palate of the denture. This can be shaped so that the lower incisors maintain contact in protrusion.

Low FMA Or Class II Div 2
The ridge relationships differ between the high FMA group and the low FMA group. In the low FMA group the edentulous ridges will nearly always be parallel.
Skeletal Class II individuals have an extensive range of motion of the mandible.
Low FMA cases often have deep overbites with minimal overjet, and the mandible rotates considerably to clear the overbite before it can translate forwards.

Anterior teeth setting Clearly if the overbite and minimal overjet of these
cases is reproduced in an artificial tooth set-up, the patient could be locked into an impossible situation. So there needs to be some re-positioning of the teeth to reduce the overbite as much as possible without overly compromising aesthetics.

Posterior teeth Setting
skeletal Class II cases have, as stated, discrepancies in both the antero-posterior and medio-lateral size and position of the arches.
The antero-posterior discrepancy can normally be solved by leaving out either a premolar or the second molar from the lower arch.
In addition, an extra premolar can be placed distal to the upper second molar.
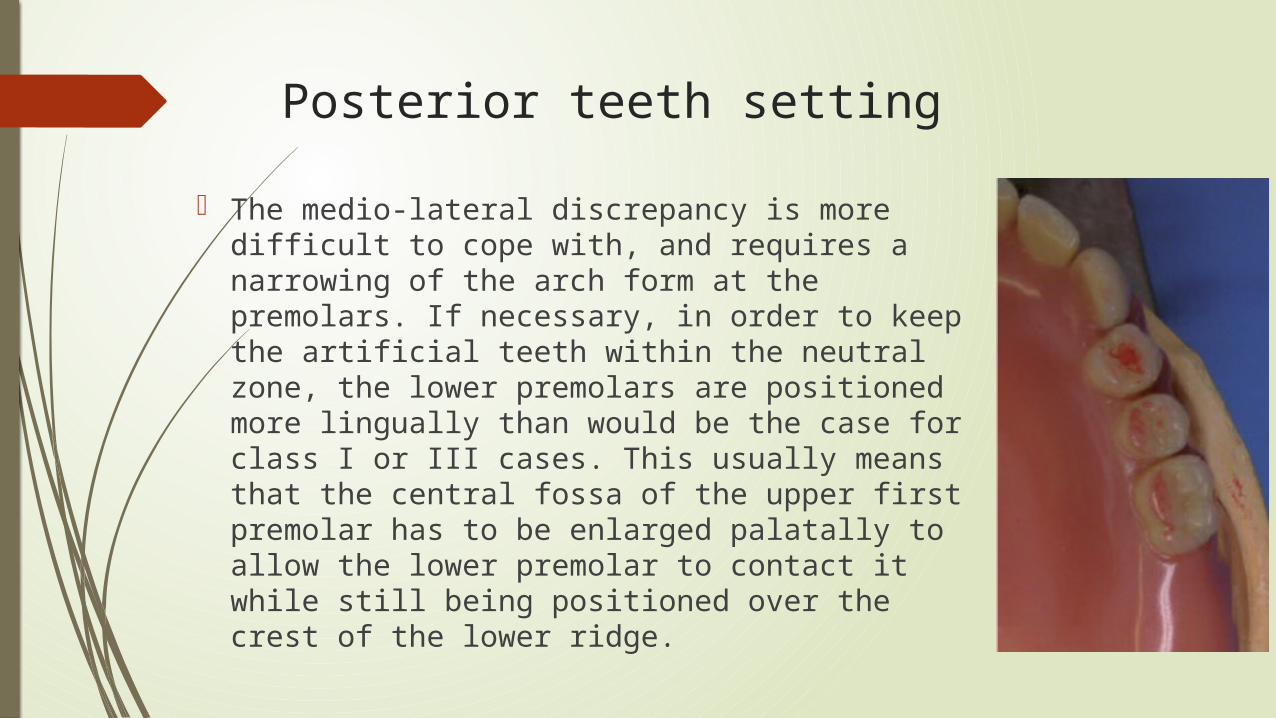
Posterior teeth setting The medio-lateral discrepancy is more difficult
to cope with, and requires a narrowing of the arch form at the premolars. If necessary, in order to keep the artificial teeth within the neutral zone, the lower premolars are positioned more lingually than would be the case for class I or III cases. This usually means that the central fossa of the upper first premolar has to be enlarged palatally to allow the lower premolar to contact it while still being positioned over the crest of the lower ridge.

A further complication arises in those cases where the upper arch is much wider than the lower. In these cases, the lower teeth are first set in their most appropriate positions relative to the lower arch. The uppers are then set in their most appropriate positions for aesthetics. If then it is found that the uppers and lowers don’t meet, a further line of teeth can be placed palatal to the uppers, or the base can be waxed to the lowers and replaced with tooth-colored resin.

Lingualised Occlusion As has been stated, the problem is that the patient functions in a
variety of positions anterior to centric relation position, and providing for protrusive balance is very difficult with cusped teeth. With a lingualised concept, however, the occlusal tables of each tooth can be successively recruited to maintain contact during protrusion, and a long anteroposterior area of contact can be obtained. This is done by placing the lower teeth on an appropriate compensating curve and then adjusting the occlusal tables for all protrusive movements.

Prognathic jaw relation The Angle classification related to this situation is that
of the Class III, where the mandible is now in advance of the maxillae. Characteristically the incisor relations in the natural teeth are either in edge-to-edge relationship or display a reverse overjet (where the lower anteriors are in advance of the upper anteriors).

The prosthodontic problem in prognathic jaw relation Anteriorly placeing the artificial teeth in the positions occupied
by the natural teeth seems a logical solution; but if this means reproducing a reverse overjet, this is often unacceptable to the patient.
Posteriorly, the main problem is the discrepancy in arch size, whereby the lower arch is considerably narrower than the upper.
Determining the most appropriate occlusal vertical dimension is very important in these cases.

Anterior teeth placement If the ridges are edge to edge or mandible is slightly
advanced anteriorly then edge to edge incisal relation can be easily made usually by slight proclination of upper incisors.
Normal class I arrangement shouldn’t be considered at all for class III patients.
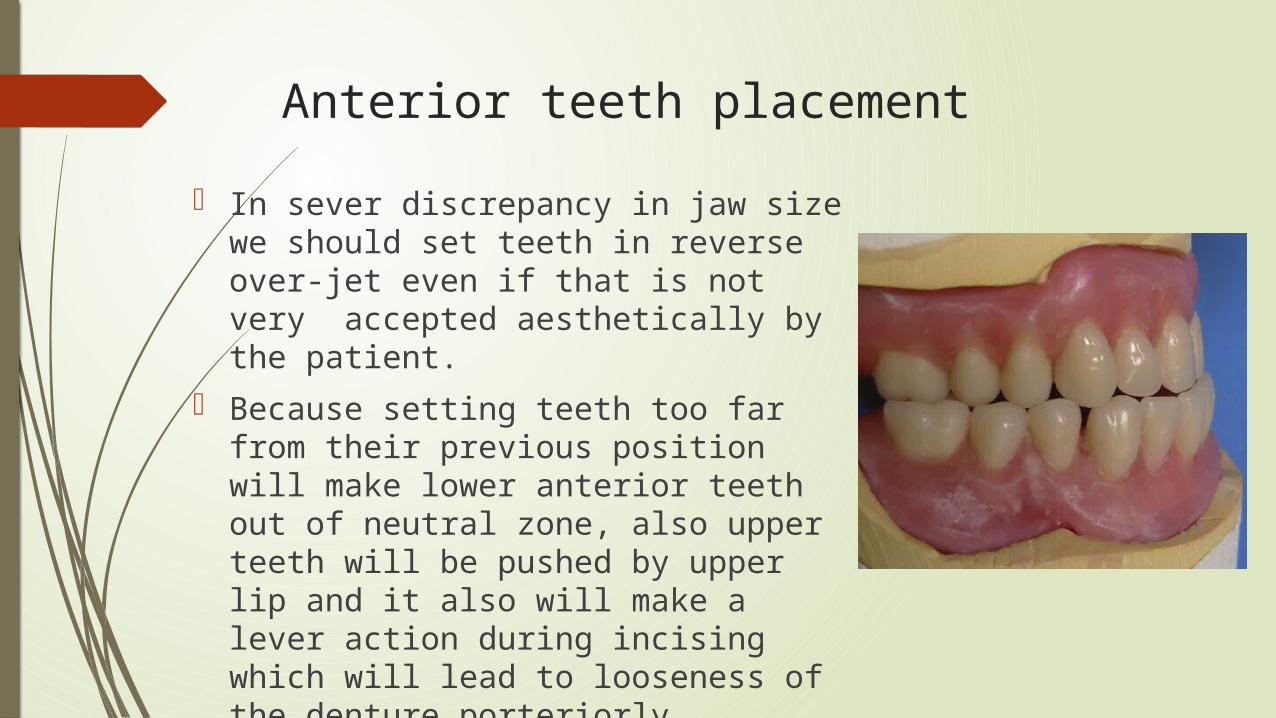
Anterior teeth placement In sever discrepancy in jaw size we
should set teeth in reverse over-jet even if that is not very accepted aesthetically by the patient.
Because setting teeth too far from their previous position will make lower anterior teeth out of neutral zone, also upper teeth will be pushed by upper lip and it also will make a lever action during incising which will lead to looseness of the denture porteriorly.

Posterior teeth placement Multiple ways could be used in class III
patients depending on severity of the case and dentist experience: If the difference in size is slight and the upper ridge
is well formed, the upper posterior teeth can be set slightly buccal to the crest of the upper.
Non-anatomic teeth may be used. These teeth allow more freedom in their buccolingual placement.
The mandibular teeth can be placed buccal to the maxillary teeth (Cross bite). After the arrangement of teeth, the buccal aspect of the tooth should be trimmed and polished in order to decrease the occlusal table.
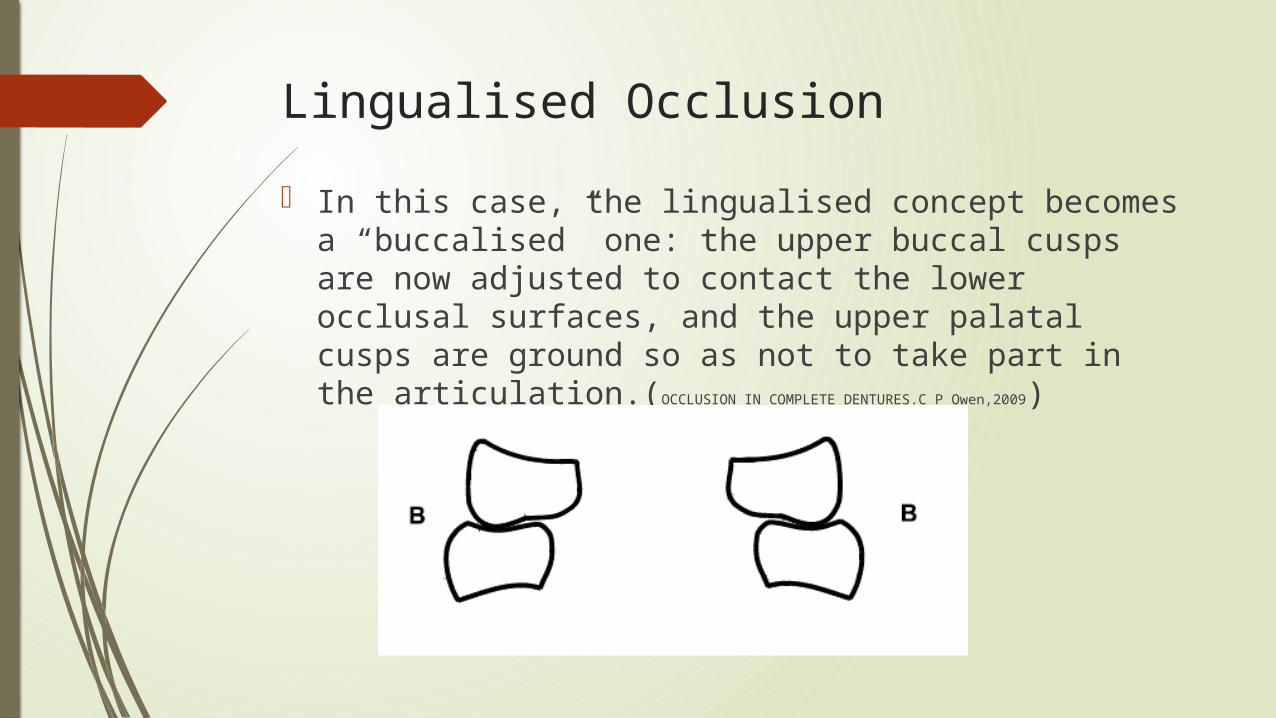
Lingualised Occlusion In this case, the lingualised concept becomes a
“buccalised” one: the upper buccal cusps are now adjusted to contact the lower occlusal surfaces, and the upper palatal cusps are ground so as not to take part in the articulation.(OCCLUSION IN COMPLETE DENTURES.C P Owen,2009)

Surgical correction of severe discrepancy In case of severe jaw size discrepancy, surgical correction may be a
successful alternative for routine prosthetic work. In many cases this choice may be refused due to systemic disease or
patient aware. Ridge osteotomy is considered a major surgery usually done under
general anesthesia so benefits must be weighted against harms.

Case Report Class II Relation Female patient 65 years old hypertensive doesn’t have any previous
denture only partials.
Principles And Practices Of Complete Dentures Creating The Mental Image Of A Denture - Quintessence Pub; 1 edition (April 1999).







Case report of jaw size discrepancySimple Method For Cross-bite Setup For Complete Dentures: A Case Report. Leonardo Marchini,2014
This case report is about a 67-year-old female patient , Severe residual ridge resorption and a large difference in size between
the mandible and maxilla. Commercially-available artificial teeth in a cross-inverted manner: The
maxillary right posterior teeth were mounted in the lower left posterior region and vice versa for the lower right posterior teeth.




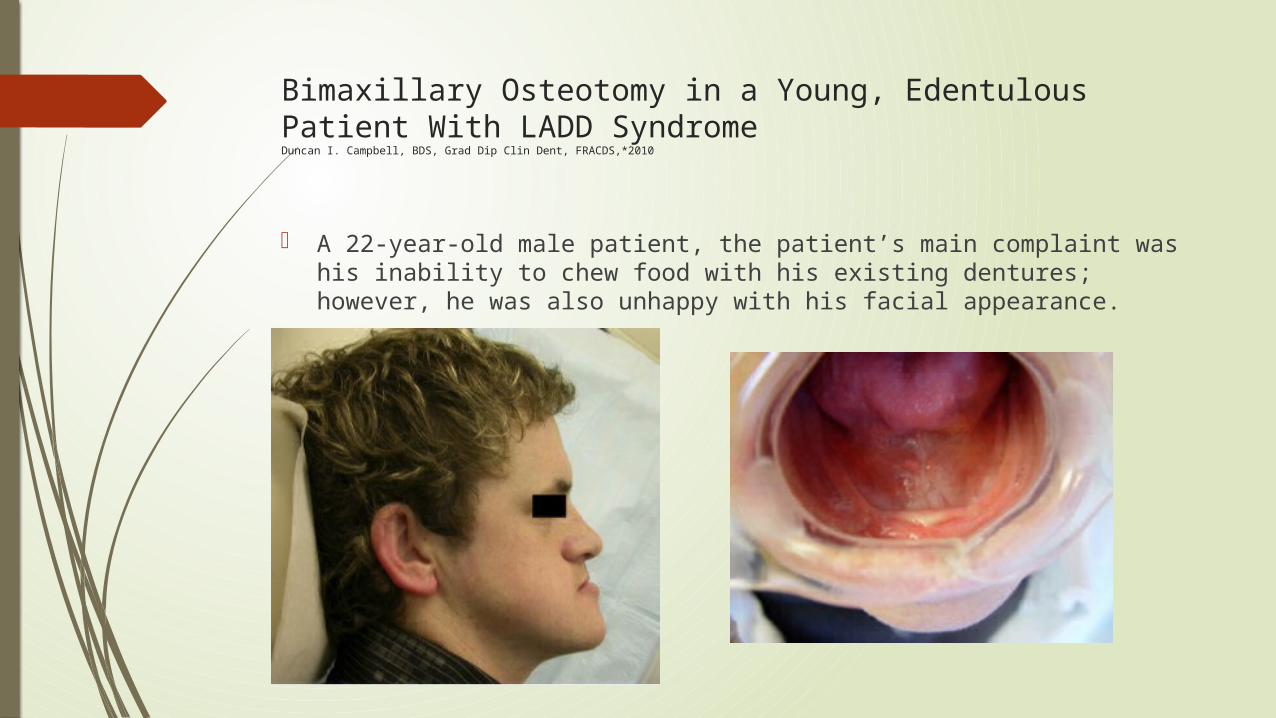
Bimaxillary Osteotomy in a Young, Edentulous Patient With LADD SyndromeDuncan I. Campbell, BDS, Grad Dip Clin Dent, FRACDS,*2010
A 22-year-old male patient, the patient’s main complaint was his inability to chew food with his existing dentures; however, he was also unhappy with his facial appearance.

Articulated models demonstrating projected A-P movement required.
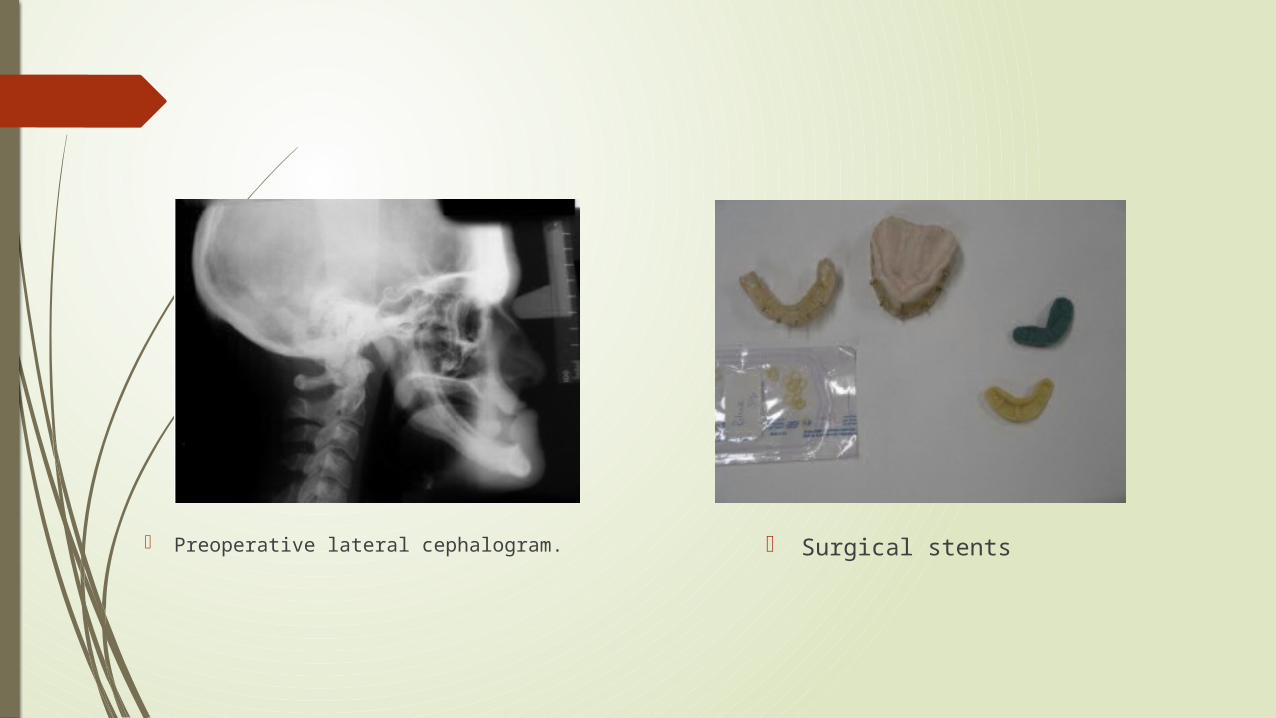
Preoperative lateral cephalogram. Surgical stents


end


Conclusion
Multiple approaches were discussed in textbooks and literature to deal with class II and class III edentulous patients, any evidence based technique when followed precisely to the right indicated patient will give successful result, but time must be taken in diagnosing patient’s condition and deciding the correct treatment plan.

References 1-Occlusal considerations for partially or completely edentulous skeletal class II patients. Part I: Background
information, Thomas A. Curtis, D.D.S. 2-Occlusal considerations for partially or completely edentulous skeletal class II patients. Part II: Treatment
concepts Thomas A. Curtis, D.D.S. 3-A contemporary review of the factors involved in complete dentures. Part II: Stability.T. E. Jacobson, D.D.S. 4-OCCLUSION IN COMPLETE DENTURES.C P Owen. 5-Principles And Practices Of Complete Dentures Creating The Mental Image Of A Denture - Quintessence
Pub; 1 edition (April 1999). 6-Prosthetic Treatment of the Edentulous Patient - Wiley-Blackwell; 5th edition (25 Mar 2011). 7-Techniques in Complete Denture Technology - Wiley-Blackwell; 1 edition (April 23, 2012). 8-Textbook of Complete Denture Prosthodontics - Jaypee Brothers Medical Pub; 1 edition (December 30,
2008). 9-Textbook of Prosthodontics - Jaypee Brothers; 1 edition (December 1, 2006). 10- Simple Method For Cross-bite Setup For Complete Dentures: A Case Report. Leonardo Marchini. 11- Arrangement of artificial teeth in abnormal jaw relations: Maxillary protrusion and wider upper arch -B.K.
Goyal, B.D.S. 12- Foster, T.D. & Walpole Day, A.J. (1974) A survey of malocclusion and the need for orthodontic treatment
in a Shropshire school population. British Journal of Orthodontics, 1, 73–8. 13- Surveying of Local Factors in Edentulous Iraqi Population Abbas F. Al-Rahmani 14- Bimaxillary Osteotomy in a Young, Edentulous Patient With LADD Syndrome
Duncan I. Campbell, BDS, Grad Dip Clin Dent, FRACDS,*2010

Eight-Year Follow-Up of a Fixed-Detachable Maxillary Prosthesis Utilizing an Attachment System: Clinical Protocol for Individuals With Skeletal Class III MalocclusionsErica Dorigatti de Avila1*