Prosthetic Treatment of the Edentulous Patient - Wiley-Blackwell
287
Prosthetic Treatment of the Edentulous Patient Prosthetic Treatment of fifth edition R M BASKER J C DAVENPORT J M THOMASON
-
Upload
meducationdotnet -
Category
Documents
-
view
1.122 -
download
4
Transcript of Prosthetic Treatment of the Edentulous Patient - Wiley-Blackwell

Prosthetic Treatment of the Edentulous Patient
Pro
sthetic
Tre
atm
en
t of
the E
den
tulo
us P
atie
nt
The new edition of this well established and highly regarded textbook has been completely revised and updated to reflect the latest developments in the field of tooth loss and denture provision. Primarily aimed at students in the undergraduate and immediate postgraduate years, it will also be of value to all those, including clinical dental technicians, who are faced with the increasingly challenging problems of complete denture treatment in dental practice.
Starting with a thorough grounding in the background and theory of denture treatment, the book goes on to describe clinical procedures for all stages of treatment as well as devoting a chapter to the diagnosis and management of clinical problems. The clinical chapters also include sections on quality control, where topics are suggested for consideration in audit cycles.
Now in full colour throughout, this fifth edition of Prosthetic Treatment of the Edentulous Patient contains nearly 200 illustrations and also includes a brand new section on implant overdentures.
KEY FEATURES
• Stresses the importance of evidence-based treatment• Emphasises care of the elderly and the value of holistic treatment• Uses a flexible approach to accommodate patient variation• Highlights the importance of good communication between clinician and dental technician• Includes many high-quality full colour illustrations
REVIEWS OF THE PREVIOUS EDITION
“This textbook is highly recommended to undergraduate students as it is well written, clearly laid out and helpfully illustrated... The text should also be of interest to practitioners and those preparing for postgraduate exams.”Dental Update
“In summation, the authors have achieved their aims and I would recommend this textbook for undergraduates.”British Dental Journal
THE AUTHORS
R.M. Basker, OBE, DDS Birm, BDS Lond, FDSRCS Edin, MGDSRCS Eng, LDSRCS EngEmeritus Professor, University of Leeds, UK
J.C. Davenport, PhD Birm, BDS Brist, FDSRCS Eng, RBSAEmeritus Professor, University of Birmingham, UK
J.M. Thomason, PhD Ncl, BDS Ncl, FDSRCS EdProfessor of Prosthodontics and Oral Rehabilitation, Newcastle University, UK
ALSO OF INTEREST
Basics of Dental Technology: A Step by Step ApproachTony Johnson, David G. Patrick, Christopher W. Stokes, David G. Wildgoose and Duncan Wood978-1-4051-7875-4
Applied Dental MaterialsNinth EditionJohn F. McCabe and Angus W.G. Walls978-1-4051-3961-8
Removable Partial Dentures: A Clinician’s GuideJohn D. Jones and Lily T. Garcia978-0-8138-1706-4
fifth edition
fifth
ed
ition
R M BASKER
J C DAVENPORT
J M THOMASONB
AS
KE
R
DA
VE
NP
OR
T
TH
OM
AS
ON
9 781405 192613
ISBN 978-1-4051-9261-3
Cover design: Meaden CreativeCover illustration by J.C. Davenport
basker_9781405192613_pb.indd 1 11/1/11 12:11:17

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
Prosthetic Treatment of theEdentulous Patient

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
Prosthetic Treatment of theEdentulous PatientFifth Edition
R.M. BaskerOBE, DDS Birm, BDS Lond, FDSRCS Edin, MGDSRCS Eng, LDSRCS EngEmeritus Professor, University of Leeds, UKFormerly Consultant in Restorative Dentistry, Leeds Teaching Hospitals NHS TrustFormerly External Examiner in the Universities of Birmingham, Bristol, Dundee, London, MalayaManchester, Newcastle upon Tyne, Sheffield and Wales, University College Cork,Universiti Kebangsaan (Malaysia)Examiner, MGDS of the Royal College of Surgeons of England
J.C. DavenportPhD Birm, BDS Brist, FDSRCS Eng, RBSAEmeritus Professor, University of Birmingham, UKFormerly Consultant Dental Surgeon, Southern Birmingham Community Health NHS TrustFormally External Examiner in the Universities of Amman (Jordan), Dublin, Glasgow, Leeds, LondonManchester, Newcastle upon Tyne, University College Cork and Wales
J.M. ThomasonPhD Ncl, BDS Ncl, FDSRCS EdProfessor of Prosthodontics and Oral Rehabilitation, Newcastle University, UKVisiting Professor and Adjunct Professor, McGill University, Montreal, CanadaConsultant in Restorative Dentistry, Newcastle upon Tyne Hospitals NHS Foundation TrustFormally External Examiner in the Universities of Dublin, Glasgow, Manchester, King’s CollegeLondon, Hong KongExaminer in MRD and MFDS examinations of the Royal College of Surgeons of Edinburgh
A John Wiley & Sons, Ltd., Publication

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
This edition first published 2011C© 1976, 1983, 1992 by R.M. Basker, J.C. Davenport and H.R. TomlinC© 2002 by Blackwell MunksgaardC© 2011 by R.M. Basker, J.C. Davenport and J.M. Thomason
Blackwell Publishing was acquired by John Wiley & Sons in February 2007. Blackwell’s publishing program has been mergedwith Wiley’s global Scientific, Technical and Medical business to form Wiley-Blackwell.
Registered office: John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
Editorial offices: 9600 Garsington Road, Oxford, OX4 2DQ, UKThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK2121 State Avenue, Ames, Iowa 50014-8300, USA
For details of our global editorial offices, for customer services and for information about how to apply for permission toreuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell
The right of the author to be identified as the author of this work has been asserted in accordance with the UK Copyright,Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any formor by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by the UK Copyright,Designs and Patents Act 1988, without the prior permission of the publisher.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names and productnames used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. Thepublisher is not associated with any product or vendor mentioned in this book. This publication is designed to provideaccurate and authoritative information in regard to the subject matter covered. It is sold on the understanding that thepublisher is not engaged in rendering professional services. If professional advice or other expert assistance is required, theservices of a competent professional should be sought.
The contents of this work are intended to further general scientific research, understanding, and discussion only and are notintended and should not be relied upon as recommending or promoting a specific method, diagnosis, or treatment byphysicians for any particular patient. The publisher and the author make no representations or warranties with respect to theaccuracy or completeness of the contents of this work and specifically disclaim all warranties, including without limitationany implied warranties of fitness for a particular purpose. In view of ongoing research, equipment modifications, changes ingovernmental regulations, and the constant flow of information relating to the use of medicines, equipment, and devices, thereader is urged to review and evaluate the information provided in the package insert or instructions for each medicine,equipment, or device for, among other things, any changes in the instructions or indication of usage and for added warningsand precautions. Readers should consult with a specialist where appropriate. The fact that an organization or Website isreferred to in this work as a citation and/or a potential source of further information does not mean that the author or thepublisher endorses the information the organization or Website may provide or recommendations it may make. Further,readers should be aware that Internet Websites listed in this work may have changed or disappeared between when thiswork was written and when it is read. No warranty may be created or extended by any promotional statements for thiswork. Neither the publisher nor the author shall be liable for any damages arising herefrom.
Library of Congress Cataloging-in-Publication DataBasker, R.M.
Prosthetic treatment of the edentulous patient / R.M. Basker, J.C. Davenport, J.M. Thomason. – 5th ed.p. ; cm.
Includes bibliographical references and index.ISBN 978-1-4051-9261-3 (pbk. : alk. paper) 1. Complete dentures. 2. Edentulous mouth.
I. Davenport, J. C. (John Chester) II. Thomason, J. M. III. Title.[DNLM: 1. Denture, Complete. 2. Mouth, Edentulous. WU 530]RK656.B338 2011617.6′92–dc22
2010040959
A catalogue record for this book is available from the British Library.
This book is published in the following electronic formats: ePDF [978-1-4443-9324-8]; ePub [978-1-4443-9325-5]
Set in 9.5/12 pt Palatino by Aptara R© Inc., New Delhi, India
1 2011

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
To our familiesAnd to the memory of Bob Tomlin

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
Contents
Foreword to the First Edition by John Osborne ix
Foreword to the Fifth Edition by Gunnar E. Carlsson x
Preface xi
Acknowledgements xiii
1 An Appraisal of the Complete Denture Situation 1
2 Factors Influencing the Outcome of Prosthetic Treatment 20
3 Transition from the Natural to the Artificial Dentition 31
4 Stability of Dentures 55
5 Jaw Relations – Theoretical Considerations 68
6 Introductory Remarks to the Clinical Chapters 76
7 Assessment of the Patient 80
8 The Relevance of Existing Dentures 91
9 Preparation of the Mouth 111
10 Impressions 130
11 Recording Jaw Relations – Clinical Procedures 150
vii

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
viii Contents
12 Dentures and Muscles 174
13 Try-in Procedures 189
14 Fitting Complete Dentures 203
15 Recall Procedures 220
16 Some Clinical Problems and Solutions 228
Index 265

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
Foreword to the First Edition
This addition to prosthetic literature must bewidely and warmly welcomed. For a number ofyears there has been a shortage of British textsfor students concerning the edentulous patient.The authors have, correctly, stressed the seri-ous problems that more and more frequentlypresent themselves now that life expectancy ison the increase and the average age of the eden-tulous is advancing. The dental profession isbecoming aware of the particular geriatric situ-ations it now has to face and this book will un-doubtedly help in solving many prosthetic geri-atric problems.
Emphasis has been placed more upon gen-eral principles than upon the minutiae of clini-
cal or technical operative detail. Given a soundbasic understanding of the principles to be ob-served in the treatment of the edentulous, chair-side experience rapidly perfects each individ-ual’s manipulative skills.
Being not unfamiliar with the labours in-volved in producing textbooks, one is consciousof the time and effort that have gone into thepreparation of this book. It should achieve allthe success that these efforts of one’s former col-leagues deserve.
John OsborneShalfleet, Isle of Wight, 1975
ix

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
Foreword to the Fifth Edition
The breakthrough of implant-supportedand/or -retained prostheses has revolutioniseddental treatment. A great part of the pro-grammes at current prosthodontic conferencesincludes presentations based on high-techimplant treatment for partially and totallyedentulous patients. So successful have theclinical outcomes with implant treatment beenthat many clinicians have come to believe thatimplants can solve all problems related to toothloss. This is of course not true, confounded asit is not only by unfavourable oral situationsbut also by a number of non-dental factors.Of these, the greatest obstacle is undoubtedlyeconomic. Viewed in a global perspective,poverty is still extremely widespread, and itexists even in many industrialised countries.Sadly, a majority of edentulous people willnever be candidates for any type of implanttherapy and complete dentures will remaintheir sole option.
The declining prevalence of edentulismwould seem to indicate a reduction in the num-ber of people in need of complete dentures.However, when epidemiological and demo-graphic data are combined, the ongoing large
increase in the number of the elderly will coun-teract the diminishing rate of edentulism. Itis therefore likely that the need to rehabili-tate edentulous patients will remain consider-able for many more decades. Complete den-tures will continue to play a central role inthe rehabilitation of edentulism; thus, teachingand training in complete denture prosthodon-tics must continue.
This successful textbook has reached its fifthedition. It combines a straightforward descrip-tion of well-proven principles and methods forthe treatment of an edentulous patient withmodern evidence-based examples of solutionsfor problems and complicated situations. Thetext is easy to read and the illustrations giveexcellent explanations of principles and tech-niques described. The book will therefore be ofgreat value in both undergraduate and post-graduate education, and it deserves a place inthe office of any dentist who treats adult andolder patients.
Gunnar E. CarlssonGothenburg, Sweden, November 2010
x

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
Preface
Two of us have had the particular pleasureof welcoming Mark Thomason to the authors’team. His presence has ensured not only thatthe text has been brought up to date in a num-ber of important areas, but also that writing anew edition has continued to be a pleasurableand stimulating experience.
Thirty-four years ago, we commented in thepreface to the first edition that it was importantto adopt a flexible approach to the formulationof treatment plans and to the application of clin-ical techniques. This opinion was based on thefact that as there is a great deal of variation inthe condition of our patients and their mouthsa ‘one size fits all’ approach is not appropriate.We see no reason to change this view. Indeed,the recently published work of Professor Gun-nar Carlsson (Carlsson 2009) strengthens ouropinion. He has drawn the profession’s atten-tion to the lack of randomised controlled trialsin many aspects of complete denture provisionand has highlighted the fact that there is oftena poor correlation between a clinician’s assess-ment of denture quality and the level of patientsatisfaction with a prosthesis. There is surelyconsiderable scope for further research to helpto improve the reliability of clinical decisionmaking in this area. In the meantime, we hope
that the clinical approaches adopted in thisbook will play a part in clarifying that choice.
During the last 8 years, there has been anexplosion in the number of published papersdealing with implant-supported complete den-tures. This development is highly relevant tothe all-important stage when decisions have tobe made on how to manage the transition fromwhat remains of the natural dentition to the to-tally artificial one. We have expanded the chap-ters dealing with this critical period.
Another major change in the UK since thepublication of the fourth edition has been theformal registration of two further members ofthe dental team – the clinical dental technicianand the dental technician. The clinical dentaltechnician is a qualified dental technician whois able to provide complete dentures directlyto patients. Patients with natural teeth or im-plants must see a dentist before the clinical den-tal technician can begin treatment. The den-tal technician makes dentures to a prescriptionfrom a dentist or clinical dental technician. Theeducational programmes for both newly regis-tered members of the dental team are formallyrecognised.
We are strongly of the view that there mustbe good communication between dentist,
xi

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
xii Preface
clinical dental technician and dental techni-cian – the right hand must know what the left isdoing or is planning to do. Published work sug-gests that the level of communication betweensurgery and laboratory still leaves somethingto be desired (Juszczyk et al. 2009). At the endof chapters dealing with the clinical stages ofdenture construction, we have again includedshort sections on ‘communication with thedental technician’ and ‘quality control and en-hancement’. We hope that they will encouragethe development of clearer communication.
Throughout the book, the description ‘clin-ician’ refers to dentist and clinical dentaltechnician.
We have taken the opportunity of thor-oughly revising the text and, with the en-couragement of our publishers, of introducingcolour into the book.
Although there has been a major reductionin total tooth loss in many countries, the eden-
tulous population is living longer. Thus, the de-mand for prosthetic care will remain at a sig-nificant level for the foreseeable future, andthe challenges this presents to the clinician willincrease in difficulty as the patients becomeolder.
Leeds, Birmingham andNewcastle upon Tyne, 2010
RMB, JCD and JMT
ReferencesCarlsson, G.E. (2009) Critical review of some dogmas
in prosthodontics. Journal of Prosthodontic Research,53, 3–10.
Juszczyk, A.S., Clark, R.K. & Radford, D.R.(2009) UK dental laboratory technicians’views on the efficacy and teaching of clinical-laboratory communication. British Dental Journal,206, E21.

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come
Acknowledgements
We are most grateful to the many friends andcolleagues whose support over the years hasencouraged and influenced our thinking on thecare of the edentulous patient. We are also in-debted to our students and young colleaguesin training who have challenged our ideas,shaped our thinking and shared our learning.
Our grateful thanks are extended to Pro-fessor John McCabe, Professor Jim Ralph, DrChris Watson, Mr Francis Nohl and Mr StewartBarclay for the generous loan of photographs,to Dr Rachel David and Mr Simon Littlewoodfor their most helpful comments on thosesections of the book dealing with speech andorthodontics respectively, and to ProfessorDamien Walmsley for helpful discussion.
We would like to acknowledge the friendlyexpertise of the staff of the British Dental Asso-
ciation’s Information Centre in helping with theliterature searches.
We are most grateful to the members ofthe Medical and Dental Illustration Unit ofthe University of Leeds and the PhotographicDepartment of the Dental School at the Uni-versity of Birmingham for their skill over theyears.
We are most grateful to Lucy Nash and NickMorgan at Wiley-Blackwell and Amit Malik atAptara for their support, understanding andencouragement throughout the production ofthis book.
We acknowledge with thanks the permis-sion of the Editor of the British Dental Journal toreproduce figures which have appeared in thatjournal.
xiii

P1: JZP/... P2: ... Trim: 246mm X 189mmfm BLBK351-Basker January 3, 2011 13:49 Printer Name: Yet to Come

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
1An Appraisal of the CompleteDenture Situation
Total tooth lossPerhaps the most fundamental question to askin the first chapter of a book on complete den-tures is: ‘What is the demand for such treat-ment?’ Fortunately, more and more evidencehas become available to provide an increasinglyaccurate answer and one which enables futuretrends to be determined with reasonable con-fidence. Particularly notable are the series ofin-depth studies of adult dental health in theUK that have succeeded in painting a detailedpicture over a period of more than 30 years.There are also data from Sweden and Finlandand parts of Germany that allow some statisti-cal modelling of the current trends (Mojon et al.2004).
The most detailed picture comes from theUK and the information that follows is basedupon decennial surveys, the most recent oneundertaken in 1998.
The situation at the end of thetwentieth century
Whilst we await the publication of the surveyoutlining the state of adult dental health dur-
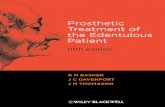
ing the first decade of the twenty-first century,let us first look at total tooth loss within adultsin the UK in 1998 (Fig. 1.1) (Steele et al. 2000).Overall, 13% of all adults were edentate, and itcan be seen that the condition was strongly cor-related with age. Total tooth loss was a rarity upto the mid-forties age group, after which therewas a steady climb to the age group 75 and overwhere the majority had lost all their teeth.
Total tooth loss is related not only to agebut also to other variables such as social classand marital status. When multivariate analy-ses were undertaken, any association betweentooth loss and gender disappeared. The differ-ences that are apparent in the UK may be illus-trated by comparing extremes. To quote fromSteele et al. (2000), women from an unskilledmanual background living in Scotland were12 times more likely to have no teeth at allthan men from a non-manual background inthe south of England. Of those who had losttheir remaining teeth in the previous 10 years,59% stated that they visited the dentist onlywhen troubled whilst 29% said that they hadattended their dentist on a regular basis. Thispattern of attendance was almost the complete
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
1

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
2 Prosthetic Treatment of the Edentulous Patient
0
10
20
30
40
50
60
70
80
90
100
16–24 25–34 35–44 45–54 55–64 65–74 75+Age group (years)
Den
tal s
tatu
s in
th
e U
K, 1
998
(%)
Edentate
Dentate
Figure 1.1 The proportion of den-tate and edentate people, by age, inthe UK in 1998 (with acknowledge-ments to Steele et al. (2000)).
opposite to that of people who still had theirown teeth. What is of particular relevance is thechange in the rate at which people lost their re-maining teeth in the last 10 years of the twen-tieth century. It has been a much more gradualprocess than previously. Whereas in 1968 two-thirds of those who were rendered edentuloushad 12 or more teeth extracted at the final stage,in 1998 the proportion had gone down to one-quarter. One possible reason for this change isthat both patient and dentist wanted to keepsome natural teeth for as long as possible. Weare fully supportive of this philosophy and en-large on the topic of transition from the naturalto the artificial dentition in Chapter 3.
As people increasingly wish to function withtheir natural teeth rather than with dentures,one would expect mental barriers to be erectedagainst the latter. This indeed appears to bethe case when we consider that, in 1998, over60% of those people who relied only on nat-ural teeth stated that they would be very up-set if they had to function with complete den-tures. This attitude seems to have strengthenedas we have moved into the twenty-first cen-tury. As the number of edentate patients falls,a ‘tipping-point’ appears to have been estab-lished, which results in a range of concerns be-ing raised, including the social acceptability of
being edentulous. Whilst edentulism was pre-viously thought to be almost inevitable, andthus an ‘acceptable’ option for patients withdental disease, this is no longer the case inmany areas of society. As the number of eden-tulous patients falls, this smaller population be-comes more manageable and allows the pos-sibility for this group of people to be offeredother treatments. For example, when there islittle chance of maintaining a functional natu-ral dentition, first-line treatment options haveincreasingly moved towards the preservationof some tooth roots and the use of overden-tures. When this is not possible, then the useof implant-supported overdentures as the ‘stan-dard of care’ has been proposed (Feine et al.2002; Thomason et al. 2009).
These changes of emphasis on how one maymanage the progression from the dentate stateto complete dentures are important, especiallyas most of the complete denture treatment inthe future will inevitably be undertaken onolder patients. It is imperative that the dentistis aware of the various treatment opportuni-ties, of the need to explore acceptable alterna-tives and to move into much longer-term treat-ment planning whilst the patients still have afunctional dentition. This longer-term planningmay be best regarded as treatment ‘mapping’ as

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
An Appraisal of the Complete Denture Situation 3
0
10
20
30
40
50
60
70
80
90
100
16–24 25–34 35–44 45–54 55–64 65–74 75+
Age group (years)
Ed
enta
te in
En
gla
nd
an
d W
ales
(%
) 1968 : 37% overall
1978 : 29% overall
1988 : 20% overall
1998 : 12% overall
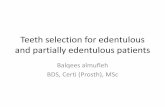
Figure 1.2 The relationship of to-tal tooth loss to age over the pe-riod 1968–1998 (with acknowl-edgements to Steele et al. (2000)).
the absolute plan may need to be more flexiblethan is commonly the case in many treatmentplans.
The past
So much for the ‘snap-shot’ of total tooth loss in1998. A fascinating picture emerges when ex-amining the trends that have developed overthe 30-year period during which there havebeen four studies of adult dental health in Eng-land and Wales – 1968, 1978, 1988 and 1998.The relationship of total tooth loss to age is pre-sented in Fig. 1.2. The first point to make isthat dental health, as measured by total toothloss, has improved dramatically. In 1968, 37%of adults in England and Wales had lost alltheir natural teeth. This figure had gone downto 12% in 1998. This improvement reflects thepoor state of oral health before and after WorldWar II when the main thrust of treatment, atthe inception of the UK’s National Health Ser-vice, had to be an attack on the high levels ofneglect, pain and sepsis existing in the com-munity. Once this battle was won, the pat-tern of extractions and dentures gave way toa desire to restore the teeth and, eventually, to
prevent further disease. We are perhaps nowseeing the next phase where alternatives andlonger-term strategies of management and re-habilitation of what remains can be realisticallyconsidered.
The very high percentage of those aged 75and over who had lost all their teeth at the timeof the earlier surveys (Fig. 1.2) is of course areflection of the high levels of dental diseasemany years earlier. For example, in 1968, 64% ofall those in the age group 55–64 were edentate.That same group of people continued to losetheir natural teeth until, 20 years later, 80% ofthem (now in the 75 and over age group) wereedentate.
Referring again to Fig. 1.2, we can see howthe huge improvement in oral health of theyounger members of the population a few yearsago is now influencing the figures as these peo-ple enter their middle years. Looking again atthe 55–64 age group the percentage that hadlost all their teeth has dropped from 64% in 1968to 18% in 1998. More dramatic still is the reduc-tion in the 45–54 age group – down from 41%to 6% in the same period. As these people growolder, it is reasonable to expect that they will,in 20–30 years time, bring down a lot further

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
4 Prosthetic Treatment of the Edentulous Patient
the current 57% of those 75 and over who areedentate.
The future
With the mass of information which has beenaccumulated over the last 30 years, it has be-come possible to predict future trends with rea-sonable confidence. If the current trends con-tinue, it is calculated that, by 2018, only 5–6%of the UK adult population will be edentate;let us not forget, though, that 5–6% equates tofour million people in the UK. We will need towait for the results of the 2008–2009 UK AdultDental Health Survey to see if the UK is stillon course for these predicted improvements.On a more salutary note, it has been suggestedthat the effect of having an ageing populationwill mitigate against the rate of reduction in theoverall prevalence of edentulism in the popu-lation. Indeed, in the US it has been predictedthat far from decreasing, the need for completedenture treatment will actually increase overthe first 2 decades of the twenty-first century(Douglass et al. 2002). The authors argue thatthe ageing ‘baby boomers’ will more than com-pensate for the falling prevalence of eden-tulism. Modelling these changes on Europeandata has suggested that in the UK there willbe a reduction in edentulism of the order of60% over the first 30 years of the century, butit will then remain stable. The mean predictionfor Finland follows a similar picture to the UKbut the spread of the data is very wide and so isinconclusive (Mojon et al. 2004).
Total tooth loss in other countries
An investigation into the oral health of adultsin the Republic of Ireland was undertaken in1989–1990 (O’Mullane & Whelton 1992). Thelevel of total tooth loss was very similar tothat in England, Wales and Northern Irelandin 1988. There had been a considerable declinein the level of edentulousness compared with10 years earlier.
Table 1.1 The percentage of people aged 35–44years and 65 years and over with no natural teeth(data from WHO (1991)).
Country35–44years
65+years
Albania 3.7 69.3Czechoslovakia 0.7 38.3Denmark 8.0 60.0Finland 9.0 46.0Ex-GDR 0.5 58.0Germany, Federal Republic 0.4 27.0Hungary 0.3 30.0Ireland 4.0 49.0Italy 0.3 18.0The Netherlands 9.4 65.4Norway 1.0 31.0Romania 15.0 55.8San Marino 1.3 40.7Sweden 1.0 20.0Turkey 2.7 75.0United Kingdom 4.0 67.0(Former) Yugoslavia 0.6 33.0
The relationship of total tooth loss to age is aworldwide phenomenon, as shown in Table 1.1,where the percentage of edentulous individualsfor two age groups in a number of countries isshown. The amount of total tooth loss recordedin or around 1990 varies considerably betweencountries (WHO 1992). Whilst most EU coun-tries do not have national survey data, in Francea recent survey in the region Rhone-Alpes re-ported that in 1995, 16% of the 65–74 age-bandwas edentulous compared with 36% for theUK and 34% for the region of Pomerania inGermany (Mojon et al. 2004).
The prospects for the future may be sum-marised as follows:
� It is unlikely that the edentulous state willdisappear, but there probably will be a fallin those requiring complete dentures so thatthere will be around 60% of the current num-ber required.

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
An Appraisal of the Complete Denture Situation 5
� More people will retain a functional naturaldentition into old age, but this dentition willnot last a lifetime in all cases.
� As the public’s expectations for oral healthcontinue to rise, a larger proportion of thosewho lose their teeth will be very upset aboutthe prospect of having to wear completedentures and this will influence their re-sponse to treatment. Therefore, it will be crit-ical to consider alternative treatment strate-gies for these patients.
� Most complete denture treatment will becentred on older people and is, therefore,likely to become more complex and de-manding. The opportunities to consider re-taining teeth as overdenture abutments orto provide osseointegrated implants as over-denture abutments for this group of patientsare likely to increase and decisions will haveto be made at an appropriate time in theplanning cycle.
� Dentists will continue to need complete den-ture skills, which will have to be of a highorder (Steele et al. 2000). Nevertheless, therewill be less opportunity for the majority ofdentists to practice these skills on a regularbasis and some parts of this treatment provi-sion are likely to move into the realm of thespecialist.
In the remainder of this book, we endeavourto deal with all these points.
The limitations of completedenturesThe limitations of complete dentures are high-lighted when one compares the difference be-tween functioning natural teeth, intimatelyconnected to and embedded in living tissues,with the removable prosthesis which replacesthem, constructed of an artificial material sim-ply resting on vital living (and often deli-cate) tissues. Between these two extremes is thecomplete overdenture. Whilst having many of
the characteristics of the conventional completedenture, it retains elements of functioning teethin the form of roots. These roots retain a vitalperiodontal organ and are, therefore, intimatelyattached to and function with the alveolar bone.Support is provided through this intimate linkwith the rest of the body and retention can beprovided through the use of attachments be-tween the root surfaces and the prosthesis. Asimilar and better researched area of clinicalpractice is the use of the dental implant whichprovides support and retention for the com-plete overdenture. Clearly, once teeth have beenextracted, the use of implants is the only waythat overdentures can be made. However, be-fore the last teeth are extracted, both treatmentoptions remain available and the use of natu-ral teeth as overdenture abutments is certainlya less expensive alternative than the implant-supported prostheses.
The resorption and prostheticreplacement of alveolar bone
It is of fundamental importance to rememberthat the extraction of teeth does not simplymean the loss of the visible crowns. With theloss of the roots, the surrounding alveolar boneresorbs. Whilst it is relatively simple to providean effective replacement for the natural crownswith a denture, it is frequently difficult, or evenimpossible, to make good all the lost alveolarbone; the more bone that is resorbed, the greateris the problem.
Atwood (1971) described the continuing re-sorption of the residual ridges as ‘a major oraldisease entity’. It occurs in all edentulous pa-tients and proceeds throughout life. Indeed,this would be a major argument in itself for re-taining tooth roots as overdenture abutments inthat their very presence will reduce the amountof alveolar resorption.
There is, though, considerable individualvariation with respect to both amount and rateof loss of bone. Much has been written on thesubject, and there has been a comprehensive

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
6 Prosthetic Treatment of the Edentulous Patient
a b
Figure 1.3 (a) This complete lower denture covers only a small proportion of the available denture-bearingtissue and (b) as a consequence there has been increased resorption of bone and the imprint of the denture canbe seen clearly.
review of the literature by Carlsson (1998). Asingle dominant factor responsible for ridge re-sorption has not yet been found. There are con-tradictory reports from investigations into thelink between bone resorption and such factorsas gender, duration of edentulousness, denture-wearing habits, quality of dentures and sys-temic influences.
What does emerge is an explanation that, inthe early stages of edentulousness, the shape ofthe residual ridge and the amount of resorp-tion is likely to be influenced particularly bylocal factors such as the inherent quality andsize of the ridge, the technique used to extractthe teeth, the healing capacity of the patientand the loads applied to the ridge (Xie et al.1997a). An example of the latter is shown inFig. 1.3a, where it can be seen that the lowerdenture covers only a small part of the areaavailable to support it and, therefore, is notspreading the load sufficiently. This design er-ror results in increased functional stress. Theconsequence is seen in Fig. 1.3b, where the im-print of the border of the denture can be seen onthe residual ridge; the bone has resorbed andthe denture has sunk into the underlying tis-sues. The ‘sinking’ denture illustrates one of thefundamental advantages of the use of an over-denture compared with a conventional com-
plete denture. Although there has been littleconclusive research in this area, it is clinicallyapparent that supporting complete dentures ontooth remnants as overdentures reduces boneresorption. This may be assumed to be by trans-ferring the usual compressive load of the den-ture through the mucosa into a tensional loadwithin the periodontium.
It is suggested that the later stages of resorp-tion in the edentulous are likely to be influ-enced more by systemic factors such as age, nu-trition, drug therapy (e.g. corticosteroids) andhormonal factors. There is also a view that se-vere resorption, particularly of the mandible, isinfluenced more by systemic factors than by lo-cal factors (Xie et al. 1997b).
In spite of the gaps in our knowledge, therewould seem to be a sensible way forward. Bear-ing in mind that a good foundation for com-plete dentures is such a valuable commodity,and that this foundation is capable of beingdamaged, it is important to take simple prac-tical steps to reduce the risk. Therefore, the firststep to be considered is maintaining some of thelast few tooth roots prior to committing a pa-tient to conventional complete dentures. Wherethis is not possible (and the use of implants asoverdenture abutments is precluded), it is wiseto encourage patients to reduce the loads on

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
An Appraisal of the Complete Denture Situation 7
Figure 1.4 This orthopantomograph shows exces-sive resorption, particularly of the mandible.
the denture-bearing tissues by leaving at leastthe lower denture out when sleeping, and toensure that there is no error in denture designwhich would promote undue resorption. Regu-lar recall and maintenance are also very impor-tant so that any developing problems are iden-tified at an early stage before serious damagehas been done. All these factors are highlightedelsewhere in this book.
The radiograph reproduced in Fig. 1.4 is anexample of extreme resorption; in simple terms,the mandible can be described as ‘pencil-thin’.With the loss of skeletal bone comes the loss ofsupport for the facial muscles resulting in theappearance seen in Fig. 1.5. It will be appreci-ated that to make good this huge volume of lostteeth and bone requires very large dentures.It can become very difficult for the patient tocontrol such substantial foreign bodies. Havinglost the opportunity to reduce the resorption byretaining some tooth roots at an early stage oftreatment planning, the practical opportunityto avoid further bone loss by the use of osseoin-tegrated implants may also have been lost, asthe amount of resorption may no longer leaveenough bone into which to place the implants.These plans need to be considered early in theplanning cycle to be of maximum benefit.
Restoration of appearance
The limitations of complete dentures in restor-ing tissue loss, and thus supporting the lips
Figure 1.5 Excessive resorption of both jaws hasresulted in a dramatic collapse of the lower portion ofthe face.
and cheeks fully, can contribute to an appear-ance of premature ageing in the edentulouspatient (Fig. 1.6). The facial muscles may losesome of their tone through the ageing pro-cess, but loss of tone may also occur becausethe muscles are unable to function as effec-tively as before. This is because the underly-ing artificial supports (the dentures) are onlysitting on the mucosa and are not attachedsecurely to the rest of the facial skeleton. Infact, one can liken the difference in oral func-tion between dentate and edentate individu-als to that of a person striding briskly alonga path rather than moving gingerly over asheet of ice. The fact that the muscles need

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
8 Prosthetic Treatment of the Edentulous Patient
Figure 1.6 This sculpture of age and youth by Gus-tav Vigeland in Frogner Park, Oslo, illustrates the agededentulous face well. Bone loss below the anteriornasal spine has occurred and is virtually impossibleto replace with a complete upper denture.
a stable surface over which to function fur-ther strengthens any arguments in favour ofthe use of overdenture abutments whether asnatural tooth overdenture abutments or in theform of dental implants. A series of studiesfrom McGill University compared patient sat-isfaction with implant-supported overdenturescompared with conventional dentures. Typi-cally, scores for satisfaction with stability of theimplant-supported denture were around 30%higher than those for conventional dentures(Thomason et al. 2003). Although there are nodata for these differences with natural overden-ture abutments, there is little reason to believethat they would be markedly different.
Mastication
Complete dentures certainly help in the controland breaking up of a bolus of food, but theirchewing efficiency is considerably lower thanthat of natural teeth. This is due to the followingreasons:
� Natural teeth are firmly attached to the sur-rounding bone, whereas dentures are merelysitting on the mucosa and, thus, must be ac-tively controlled by the patient.
� The pain threshold of the denture-bearingmucosa is relatively easily exceeded so thatthe biting force, which is closely correlatedwith chewing efficiency of complete den-tures, is reduced and may be only one-sixthof that of dentate patients.
Although a higher intake of essential nutri-tional factors is associated with an efficient nat-ural dentition, the wearing of complete den-tures does not mean that nutrition will be de-ficient. Modern food production methods tech-nically enable an adequate diet to be obtainedin a form that is readily assimilated despite themost inefficient dentitions. However, as notedlater in this chapter, the situation may becomecritical within certain groups of older people.
Of particular importance is the fact that theenjoyment of eating depends upon the abilityto chew, thus making the most of the flavourof the food whilst it is in the mouth. Further-more, the sense of touch within the oral cavityenables us to distinguish the textures of differ-ent foods, a process which heightens the enjoy-ment of a meal. Such pleasure in eating encour-ages people to maintain an interest in food. Ifcomplete dentures are painful or if their controlbecomes a problem, eating a meal becomes achore. In addition, coverage of the palate by theupper denture prevents the full appreciation ofthe texture and temperature of the food. Peo-ple with complete dentures are thus more likelyto lose interest in eating and switch from suchthings as meat, fruit and salads to less demand-ing foods.
People with a natural dentition have beenshown to eat more fruit and vegetables thanthe edentulous. A patient’s perception of limita-tions in chewing ability with complete denturesmight be one of the factors influencing this di-etary choice, but of greater importance mightbe the subject’s attitude to, and knowledge of,the benefits of an appropriate diet. Indeed, sim-ply improving the quality of a prosthesis doesnot suddenly cause an improvement in that pa-tient’s diet (Moynihan et al. 2000). It may well

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
An Appraisal of the Complete Denture Situation 9
be that the quality of the denture is importantfor the personal enjoyment of eating, but tohave a good chance of improving the diet ofdenture-wearers psychosocial factors, as well asperceived chewing ability, must be addressed(Bradbury et al. 2008). There is clear evidencethat to make this change a dietary interventionprogramme is required which ideally runs inparallel with the denture provision (Bradburyet al. 2006).
In spite of the limitations of dentures, themajority of patients manage well and are onthe whole relatively happy to have a substi-tute for what may have been decayed, mobileand painful natural teeth. After all, it must beremembered that the most likely alternative tocomplete dentures is ‘no dentures’.
There are, however, other alternatives thathave been alluded to above; overdentures (overtooth roots or implants) or ‘fixed’ rehabilita-tions (bridges) constructed on dental implants.Many now regard overdentures supported bytwo implants to be the most appropriate mini-mal standard that should be offered to the eden-tulous in an affluent society (Feine et al. 2002;Thomason et al. 2009) – but there is a longway to go before this concept is universallyaccepted. There is only poor epidemiologicaldata regarding the prevalence of dental implanttreatment. It has been suggested that towardsthe end of the twentieth century, somethinglike 1/1000 edentulous and partially edentu-lous patients had been treated using implant-supported prostheses (Carlsson 1998), and themajority of these are likely to have been in thepartially edentulous. Sweden probably still hasthe highest penetration rate of implant treat-ment in the world (Carlsson 2006), but evenhere only some 8% of the edentulous popu-lation has received any form of implant ther-apy (Osterberg et al. 2000), the other 92% beingmanaged by conventional means. Whilst thereis a better alternative to conventional completedentures, there is still a long way to go be-fore this alternative becomes the ‘normal’ treat-ment. The need for this change is clear and
exemplified by the observation that a signifi-cant number of people find complete denturestroublesome to the extent that, in one large na-tional survey, over a quarter experienced diffi-culty in eating and drinking (Walker & Cooper2000).
One of the fortunate consequences of thesedevelopments is that it is becoming increas-ingly rare that one meets patients whose mis-guided attitude towards dental disease is thatthe best approach is to have all the natural teethextracted electively, when they are restorable,and be replaced by complete dentures. Indeed,bizarre as it now seems, only a few generationsago it used to be a common practice in someareas of the UK for this treatment to be car-ried out for a bride-to-be in the belief that itwould reduce her future dental problems andwould avoid saddling her new husband withmajor dental expenses! Fortunately, this atti-tude is no longer prevalent and there is rarelyany justification for undertaking such a drasticstep in early adulthood. Even though the firstfew years of edentulous life may well be rela-tively free of problems, it is impossible to pre-dict whether an individual patient will retainan adequate bony foundation and maintain asatisfactory level of comfort and function, orwill proceed to a state where denture problemssignificantly reduce the patient’s quality oflife.
The older edentulous patientEarlier in the chapter, it was pointed out that theprovision of complete dentures now, and evenmore so in the future, will largely be directed atthe older patient. In recent years, a great dealhas been written about this group of people.The purpose of this section of the book is tohighlight some of the significant points that re-late particularly to complete denture treatment.For a more detailed presentation of the topic,the reader is referred to the bibliography at theend of the chapter, which cites textbooks andpapers that were used to compile this summary.

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
10 Prosthetic Treatment of the Edentulous Patient
Demographic changes
The life expectancy of those in the developedworld has been increasing at the incredible rateof 5 hours per day for the past 200 years. There-fore, it is hardly surprising that we are see-ing a change in the age profile of our soci-ety, and with it a change in the expectationof those we used to call old. Studies of age-ing have brought a generally accepted under-standing that ageing is not programmed intoeach person but comes about by a lifelong ac-cumulation of ‘faults’ in our cellular make-up.The events causing these faults can be affectedsurprisingly easily so that delaying damage byreducing exposure to events or boosting ourdefences will help to postpone the age-relateddecline which represents old age. This reducedexposure probably explains why the health ofour older populations is so much improved –and indeed why the ‘old’ can now be describedas the ‘new middle aged’! The improvements inthe conditions of our society in terms of hous-ing, nutrition and working conditions may eachhave contributed to this reduction in accumu-lated damage and may also go some way toexplain the life expectancy differences betweenbetter-off and economically deprived areas ofour communities.
At one time, an ‘elderly person’ was com-monly defined as someone over the age of65. Many people have found this label faintlyinsulting even though the pill may be maderather sweeter if it is pointed out that the la-bel is attached to those who are of pension-able age (Harkins 2002). The term ‘older per-son’ has become more acceptable and will beused throughout the rest of the text.
Throughout the world, the older populationis growing rapidly. Figure 1.7 shows the pro-portion of the total population aged 60 yearsand over living in selected regions. The figureswere produced at the World Health Organiza-tion (WHO) World Assembly on Aging in 1982.It can be seen that there is a big difference be-tween areas which contain industrialised coun-
25
20
15
10
5
1950 1975 2000 2025
Western AfricaEastern Africa
Middle AmericaNorthern Africa
Caribbean
TemperateSouth America
Northern AmericaAustralia andNew Zealand
Western Europe
Northern Europe
Year
Pro
port
ion
of th
e to
tal p
opul
atio
n 60
yea
rs a
nd o
ver
(%)
Figure 1.7 The growth of elderly populations in var-ious regions of the world.
tries and those which are composed largely ofless developed countries.
It is expected that in the first quarter of thetwenty-first century more than a fifth of thepopulation in industrialised countries will beover the age of 65. Those undergraduates read-ing this book will realise that most of their prac-tising life will be influenced by this pattern. Theproportion of edentulous adults in each age co-hort will fall during this time, but the effect ofthe upwards shift in the age profile of our soci-ety associated with ageing ‘baby boomers’ willmean that the number of edentulous adults re-maining in our society will remain significant(Mojon et al. 2004). In the UK, the proportion ofolder people in the population will continue toincrease over the next 50 years. The effect of in-creased life expectancy on the population pro-file will mean that the greatest increase will beamongst those 85 years and over; their numberwill almost triple. The increase in the 65–74 and

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
An Appraisal of the Complete Denture Situation 11
75–84 age groups will be a little less dramatic(MacMahon & Battle 2002).
The vast majority of older and significantlyolder people live in the community. A smallpercentage, estimated at between 12% and 14%,are housebound because of physical or men-tal handicap. In Northern Europe, between 4%and 7% live in some form of institution. Thesefigures are of particular relevance with respectto the delivery of care. Those people living insome form of institution do have the advantagethat their carers are in a position to recogniseproblems and to seek advice on their behalf.Of course, this presupposes that the carers havesome knowledge of prosthetic problems. Thoseolder people who have some form of hand-icap and are living at home are perhaps themost vulnerable when it comes to dealing withprosthetic difficulties; frequently, the responsi-bility for initiating help and seeking treatmenthas not been accepted by any particular per-son. Valuable guidelines which cover the careof long-stay patients and of those who needtreatment on a domiciliary basis have been pub-lished (Fiske & Lewis 2000; Fiske et al. 2000).
Some changes seen in olderpeopleThis section describes some of the more rele-vant changes that occur in older people.
Older people typically remain alert and con-tinue to have sound judgement; however, amodest decrease in mental agility occurs. Withincreasing age there is often seen slight impair-ment of the abilities to learn and to memorise.With increasing age, there is a progressive lossof neurones and synapses in the cerebral cor-tex. As a result, there is a slowing of the centralprocessing facility with a consequential length-ening of reaction times and response to sensorystimuli.
Within the sensory system, age brings abouta deterioration of the senses of smell and taste,the former being more affected. Hearing is im-
paired in approximately 25% of people over theage of 65 years and in 80% of those in the agerange 75–79 years.
With respect to the motor system, there tendsto be impairment of balance and some postu-ral tremor, indicating deterioration of cerebel-lar function and of the extrapyramidal system.With increasing age, there is less precision incontrolling the contraction of muscles, such asthe masseter muscles. It takes more time andefforts before new dentures can be controlledautomatically. Of course, an older person has agreat deal of experience to fall back on, and ifa new task is given, which utilises previouslyacquired skills, difficulties will be minimised.However, problems are more likely to arise ifthe new task is more demanding than decliningabilities are able to cope with. For example, pre-vious denture experience can be of the greatestassistance when having to cope with new den-tures, providing that major changes to the de-sign of the dentures have not been introduced(see Chapter 8).
Research has shown that the masseter andmedial pterygoid muscles suffer a decrease incross-sectional area and in muscle density as aconsequence of advancing age; the decrease ismore apparent in edentulous people (Newtonet al. 1993). Such changes might, in individualcases, be responsible for complaints of difficultyin eating and of eating more slowly than the restof the family. Of course, these problems can bedue to the simple fact that eating with denturesis just more difficult than eating with naturalteeth anyway!
Age also brings about deterioration of thedenture-bearing tissues. The epithelium be-comes thinner, the connective tissue is less re-silient and the ability of the mucosa to healis impaired. Osteoporosis is a common prob-lem in older people, particularly affecting post-menopausal women, occurring in about one-third of women over 60 years. Not only is theskeleton affected, but the lower jaw will alsoshow a decrease in bone density. The severityof osteoporosis is related not only to hormonal

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
12 Prosthetic Treatment of the Edentulous Patient
changes but also to long-term calcium defi-ciency and to loss of normal function. Thereis no evidence to suggest that the rate of sali-vary secretion decreases with age per se, but aswill be seen later, normal salivation can be ad-versely affected by drug therapy.
Systemic disease
The following problems, which commonly oc-cur in older people, can cause complicationsspecifically related to the care and treatment ofthe edentulous patient.
Psychiatric disorders
Depression is the most common mental disor-der in later life. The prevalence of depressionrequiring clinical intervention in the over 65-year-olds is between 13% and 16% (Banerjeeet al. 2002). This condition can result in poorappetite and weight loss and can adversely af-fect motivation and self-care. It is not a normalconsequence of ageing and is treatable. With re-gard to prosthetic treatment, the condition mayreduce the patient’s ability to make an effort toaccommodate to new dentures.
Dementia is found in 5%–6% of people overthe age of 65 and in 20% of those over 80 yearsold and can result in conditions such as intellec-tual impairment, a poor memory (particularlyfor recent events), poor concentration and a re-duced level of self-care. The situation can de-teriorate to such a level that dentures, particu-larly the lower, cannot be worn.
Additional problems may arise from thedrug therapy given to these patients; they arediscussed in the next section and in Chapter 16.
Parkinson’s disease
This condition, as well as other tremors thatare likely to occur in the older person, canadversely affect the precise control of themandible, making it more difficult to obtainan accurate recording of the jaw relation-
ship. Parkinsonism can also cause difficulty inswallowing, leading to pronounced dribbling,which can be very distressing for the patient.
Cerebrovascular accident
The occurrence of a ‘stroke’ may result in uni-lateral paralysis of the facial muscles, makingit more difficult for the patient to control den-tures, especially the lower denture. The patientmay also have difficulty clearing food whichhas lodged in the buccal sulcus. Speech may beaffected, making it difficult for the patient tocommunicate with the dentist. Ways in whichprosthetic treatment can help these patientshave been described by Wright (1997).
Angina
Angina can cause pain that is experiencedaround the left body of the mandible or eventhe left side of the palate. This usually occursin association with chest pain and the onset isusually related to physical exertion.
Congestive heart failure, chronicbronchitis and emphysema
Older patients with these conditions are likelyto become breathless if the dental chair istipped back into the supine position.
Diabetes
Type 2 diabetes occurs commonly in later life.It predisposes to infection in the mouth by Can-dida albicans, is a cause of a ‘burning mouth’ andcan result in troublesome dryness of the oralmucosa.
Osteoporosis
Although this condition has already been men-tioned with respect to the denture-bearing tis-sues, it is appropriate to mention that it canlead to a hunched posture, or kyphosis, which

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
An Appraisal of the Complete Denture Situation 13
requires the dentist to ensure that work is un-dertaken with the patient in the sitting positionwith the head and neck adequately supported.
Arthritis
Older patients may suffer from osteoarthritisor rheumatoid arthritis. Either condition mayhave reached such an advanced state that thepatient finds it extremely difficult, or even im-possible, to attend the dental surgery. If eitherof these conditions affects the hands, it becomesincreasingly difficult for the patient to cleandentures adequately. The patient can be helpedby increasing the thickness of the brush handleso that it can be gripped without discomfort, byproviding brushes which can be attached to awashbasin and by recommending an effectivecleansing solution which reduces the relianceon mechanical means of plaque removal.
Nutritional deficiencies
Deficiencies of the vitamin B complex, folic acidand iron are not uncommon in the older person.As will be described in later chapters, these de-ficiencies can lead to pathology of the mucosaand to widespread discomfort or burning.
Drug therapy
It has been reported that older patients are pre-scribed an average of 2.8 drugs per person.Poor compliance with medication is found inbetween 50% and 60% of patients; this is a par-ticular problem among older people who are ofcourse taking more drugs and may have somedegree of intellectual impairment or poor recall.
The commonest drugs prescribed for olderpeople, in descending order of frequency,are diuretics, analgesics, hypnotics, sedatives,anxiolytics, antirheumatics and beta-blockers.Many of these drugs have side effects thatare relevant to the dentist about to undertakeprosthetic treatment. Xerostomia is producedby certain antidepressants, diuretics, antihyper-
tensives and antipsychotics, with some drugshaving a more profound effect on secretion thanothers. Lack of saliva adversely affects the re-tention of dentures, increases the possibility oforal infection, and through the absence of lu-brication, can result in generalised soreness oreven a burning sensation.
Certain drugs, such as steroid inhalers usedin the treatment of asthma, immunosuppres-sive drugs and broad-spectrum antibiotics usedover a long period, can alter the oral flora, thuspredisposing to candida infection.
Tardive dyskinesia is a condition charac-terised by spasmodic movements of the oral,lingual and facial muscles. These uncontrol-lable movements can make it extremely diffi-cult, or even impossible, to provide stable den-tures. The condition is brought on by extensiveuse of drugs such as antipsychotics and tricyclicantidepressants. It will occur in 20%–40% ofpatients who have been taking the drugs forlonger than 6 months. In approximately 40% ofsufferers, the condition is not reversible, even ifthe drug therapy is stopped.
Psychological changes
Advancing age leads to certain inevitablechanges that must be taken into account whentreating older patients. For example, the patientfinds it more difficult to perform tasks that de-pend upon rapid movements. Such tasks maywell include the need to suddenly control adenture that has become destabilised duringnormal function. It should also be realised thatolder people take rather longer to learn to per-form new tasks or to remember new informa-tion which is not put over clearly or which maynot appear to be immediately relevant.
As mentioned earlier, depression is a com-mon condition. One frequent cause is thechanging role brought about by increasing age.For example, children are no longer dependentupon the parent, retirement brings about a newlife with reduced income, life changes dramat-ically as a result of the death of the spouse,

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
14 Prosthetic Treatment of the Edentulous Patient
health deteriorates and the person is less ableto care for him or herself. The greater the num-ber of these life events, the more the person hasto cope with. Of course, if the person is able toadapt to the changes, there is a reduced risk ofdepression developing.
Older people are less able to accept new situ-ations, be they a change in denture shape, a newdentist or even the appointment time for treat-ment. It will be appreciated that the clinicianmust take many aspects of the life of the patientinto account when investigating a complaint.Of course, many problems will be straightfor-ward, but some will be complicated by factorsthat are far removed from the oral cavity andthe existing dentures. Unless their presence issuspected, there is a risk that prosthetic treat-ment alone will fail to deal with a problem (seeChapter 16).
Nutrition
A great deal has been written on the relation-ship between nutrition and the efficiency of thedentition, be it natural or artificial. It is notappropriate in this text to rehearse all the ar-guments. Instead, some of the more importantconclusions will be listed.
Although overt malnutrition is relativelyrare, it should be pointed out that an inad-equate diet can lead to reduced tolerance ofthe oral tissues to normal wear and tear andthat this reduced resistance, in turn, can resultin poor adaptation to dentures. Those peoplemore likely to have nutritional problems are thehousebound living at home, those with handi-caps that make shopping and cooking difficult,alcoholics, people who suffer from mental ill-ness or those who have been recently bereaved.As indicated below, those living in long-stay in-stitutions are a particularly vulnerable group.
Our knowledge of the link between oralhealth, diet and nutritional status in older peo-ple has been improved by the publication ofa national diet and nutrition survey of peopleaged 65 years and over (Steele et al. 1998). In
this survey, comparisons were made betweenthose people living at home (the free-livingsample) and those in long-term care (the insti-tutional sample). Findings that relate particu-larly to edentate people are as follows:
� Fifty per cent of the free-living group wereedentate as compared with 79% of the insti-tutional group.
� Those living at home wore old dentures witha mean age of 17 years. The complete den-tures of the institutional group were olderstill and had more faults.
� Edentate people reported greater difficultyin eating certain foods than did the dentate.These foods included tomatoes, raw carrots,lettuce, well-done steaks, apples and nuts.The difficulties could be so great that thefoods were not eaten at all. Those peoplewho reported dry mouths had greater dif-ficulties with those foods which requiredchewing. Those living in institutions re-ported significantly greater restrictions.
� Edentate people had lower plasma levels ofvitamins A, C and E than the dentate. Thoseliving in institutions had a disturbingly lowlevel of vitamin C that was at the bottom endof the normal range.
Finally, the point should be made that, in theabsence of an effective dentition and an ade-quate supply of saliva, there is a greater risk of aperson choking on a large bolus of food that hasnot been adequately broken up. Preparation forsafe swallowing is an important consideration.
The condition of denturesMost edentulous people over the age of 65years are wearing dentures that are more than10 years old, and as a result, mucosal changesare present in between 44% and 63% of cases.The need for treatment, based on clinical judge-ment, suggests that 40% of 5-year-old denturesand 80% of 10-year-old dentures should be

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
An Appraisal of the Complete Denture Situation 15
replaced. However, the picture is not that sim-ple. Need can be measured in a variety of ways:
� ‘Normative need’ is the need defined by ex-pert or professional opinion.
� ‘Felt need’ is the patient’s subjective desire.� ‘Expressed need’ is recorded when the ‘felt
need’ is activated through the patient seek-ing treatment.
One estimate of ‘normative need’ has al-ready been described. Others indicate that70%–85% of older people’s dentures require at-tention and that such need far exceeds the ‘ex-pressed need’. Older people are likely to con-sider that treatment is required as a result ofexperiencing pain, difficulty in chewing, a de-teriorating appearance, or because the existingdentures are broken or have been lost. How-ever, the ‘felt need’ may not be activated for avariety of reasons, including the following:
� The dental problem is low on the list of pri-orities compared with other problems.
� Inertia on the part of the patient.� Ignorance of available services.� Fear of treatment that may be required. It is
important to remember that a large propor-tion of today’s edentulous patients experi-enced dental treatment in less sophisticatedtimes when pain was a frequent accompani-ment.
� Inability to travel to a surgery because of illhealth or problems of transportation.
� A feeling that nothing can be done anywayand that the dental problem is just one of theinconveniences of old age.
� Finance.
The effectiveness of some or all of these ‘bar-riers to care’ can be gauged from one surveywhich reported that of a group of 75-year-oldpeople living independently, nearly half had anoral problem, one-third had pain and the major-ity had not visited a dentist for at least 10 years,and what’s more, did not plan to do so.
Caring for the older patient:some practical pointsMany of the subsequent chapters of the bookrefer to modifications to clinical techniques orapproaches that may be required to meet theparticular needs of the significantly older pa-tient. When dealing with these significantlyolder patients who may be frail, all membersof the surgery team must have a sound under-standing of the problems of this older groupand be sympathetic to their needs. The sectionswhich follow mention some aspects of manage-ment that naturally follow on from the previousdiscussion.
Mobility
There are many causes of immobility, whichmay arise from disorders of the musculoskele-tal system, neurological disorders, cardiovascu-lar and pulmonary disease, the consequence ofdrug therapy and psychological problems. Thewhole story for an individual patient may bequite complex and the consequences may befar reaching. For example, a person’s immobil-ity may result in depression, which itself causesloss of appetite, and ultimately, malnutrition(Walsh et al. 1999). It requires little imaginationto realise that the added complication of poorlyfitting or painful dentures can only worsen thesituation.
It should be stressed that to encourage olderedentulous patients to attend for dental treat-ment, it is important to ensure that there isready access to the surgery. A ground floor lo-cation is ideal, and both doors and corridorsshould be wide enough to provide access forwheelchairs. Once the patient has arrived in thesurgery, sufficient time needs to be spent ex-plaining the routine in order to put the patientat his or her ease. When settling the patient inthe dental chair, it is important to warn the pa-tient in advance of any movements of the chairthat are about to be made and to remember that

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
16 Prosthetic Treatment of the Edentulous Patient
most older people will be more comfortable inthe sitting rather than the supine position.
Communication
It should be recognised that the patient is likelyto be anxious and also unclear as to what mightbe involved at the first visit to the surgery. Itis imperative to develop appropriate communi-cation skills so that the patient’s problems canbe assessed as accurately as possible, a realistictreatment plan evolved, and the patient madefully aware of what will be done and more par-ticularly what may be the limitations of treat-ment. To this end, it is vital to carry out the dis-cussion in a quiet, unhurried environment, toface the patient when talking and, if the patienthas a hearing impairment, to speak slowly andclearly but without undue exaggeration. As theimpairment is likely to mean that higher fre-quencies can no longer be perceived, it is im-portant not to speak too loudly. It is also ex-tremely important to allow plenty of time forlistening to the patient’s account of any prob-lems so that he or she feels that sufficient op-portunity has been given for matters of concernto be adequately explained to the dentist.
When information is being given to the pa-tient, it should be relayed reasonably slowly, ina carefully structured manner, and without dis-traction or interruption. It is useful to back upverbal comment with written advice, recognis-ing that the print should be large enough forthose whose eyesight has deteriorated.
When obtaining a history, it is important toremember that older people have an increas-ing number of ‘aches and pains’, but regard-ing these problems as being a normal conse-quence of ageing can result in a risk of under-diagnosing. It must also be appreciated thatchronic pain and depression commonly go to-gether, so it is important to establish any predis-posing factors. For example, widespread painunder a lower denture might be due to a clench-ing habit which has bruised the mucosa, andwhich has been initiated by worry at home;
the pain is no less real, whatever the cause. Insuch circumstances, prosthetic treatment on itsown is unlikely to offer long-term success. Ef-fective care is likely to require communicationbetween the dentist and the patient’s medicalpractitioner.
Planning treatment
When deciding upon a course of treatmentfor an older patient, one must always havethe original complaint at the forefront of one’smind and plan a programme of care that canbe achieved in the particular circumstances. Forexample, the request to see the patient maycome from a relative who has become increas-ingly embarrassed that dentures are not beingworn on social occasions. The health of the pa-tient may have deteriorated to such an extentthat successful control of a new lower dentureis clearly out of the question. It may be con-cluded that realistic treatment is the provisionof an upper denture only, which will be wornfor appearance’s sake rather than for function.In such circumstances, it can be argued that thedentist is treating the relative as well as the pa-tient, a course of action that surely is entirelyjustified. Although this particular illustrationmay be thought of as an extreme one, it is byno means uncommon in long-stay care homesand does serve to make the point that success-ful treatment is the ‘art of the possible’.
Postscript
In this section of the chapter dealing with theolder and significantly frailer patient, we havedrawn attention to conditions that are likely toinfluence overall care. The reader should notprogress to the remainder of the book withthe impression that prosthetic treatment of theolder patient is invariably going to be compli-cated by a long list of problems. It is impor-tant to put things in perspective by appreciatingcharacteristics of normal ageing. Many of thesecharacteristics are widely recognised but some

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
An Appraisal of the Complete Denture Situation 17
have been less well accepted. Certain featuresthat are well recognised include the following:
� The majority of older people are not senile,nor do they feel miserable for most of thetime.
� Most older people can learn new things.� Older peoples’ reaction times tend to be
slower.� Physical strength tends to decline with age,
but about 80% of individuals are healthyenough to carry out normal activities.
� The majority like some kind of work to do.
Those features which are less well recog-nised include the following:
� All five senses tend to decline with age.� Most older people are not set in their ways;
they do, however, take longer to learn some-thing new.
� The majority are seldom bored and are nei-ther socially isolated nor lonely.
� The majority of old people are seldom irri-tated or angry.
References and additionalreadingAnon. (1990) Elderly people: their medicines and
their doctors. Drugs and Therapeutic Bulletin, 20,77–9.
Atwood, D.A. (1971) Reduction of residual ridges: amajor oral disease entity. Journal of Prosthetic Den-tistry, 26, 266–79.
Baillie, S. & Woodhouse, K. (1988) Medical aspects ofageing. Dental Update, 15, 236–41.
Baker, K.A. & Ettinger, R.L. (1985) Intra-oral effectsof drugs in elderly persons. Gerodontics, 1, 111–16.
Banerjee, S., Wedgewood, F. & Ha, Y. (2002) Old agepsychiatry. In: Elderly Medicine – A Training Guide(eds G.S. Rai & G.P. Mulley), pp. 111–25. MartinDunitz, London.
Bradbury, J., Thomason, J.M., Jepson, N.J.A, Walls,A.W.G, Allen, P.F., & Moynihan, P.J. (2006) Nutri-tion counseling increases fruit and vegetable intakein the edentulous. Journal of Dental Research, 85(5),463–8.
Bradbury, J., Thomason, J.M., Jepson, N.J.A., Walls,A.W.G., Mulvaney, C.E., Allen, P.F. & Moynihan,P.J. (2008) Perceived chewing ability and intake offruit and vegetables. Journal of Dental Research, 87,720–5.
Budtz-Jørgensen, E. (1999) Prosthodontics for the El-derly: Diagnosis and Treatment. Quintessence Pub-lishing Co., Chicago.
Carlsson, G.E. (1998) Clinical morbidity and seque-lae of treatment with complete dentures. Journal ofProsthetic Dentistry, 79, 17–23.
Carlsson, G.E. (2006) Facts and fallacies: an evi-dence base for complete dentures. Dental Update,33, 134–42.
Christensen, J. (1988) Domiciliary care for the elderlypatient. Dental Update, 15, 284–90.
Douglass, C.W., Shih, A. & Ostry, L. (2002) Will therebe a need for complete dentures in the UnitedStates in 2020? Journal of Prosthetic Dentistry, 87,5–8.
Drummond, J.R., Newton, J.P. & Yemm, R. (1988)Dentistry for the elderly: a review and an assess-ment of the future. Journal of Dentistry, 16, 47–54.
Feine, J.S., Carlsson, G.E., Awad, M.A., Chehade,A., Duncan, W.J., Gizani, S., Head, T., Heydecke,G., Lund, J.P., MacEntee, M., Mericske-Stern, R.,Mojon, P., Morais, J.A., Naert, I., Payne, A.G.,Penrod, J., Stoker, G.T., Tawse-Smith, A., Taylor,T.D., Thomason, J.M., Thomson, W.M. & Wismei-jer, D. (2002) The McGill consensus statement onoverdentures. Mandibular two-implant overden-tures as first choice standard of care for edentulouspatients. Journal of Prosthetic Dentistry, 88, 123–4.
Fiske, J., Dougall, A. & Lewis, D. (2009) A ClinicalGuide to Special Care Dentistry. British Dental As-sociation, London.
Fiske, J., Gelbier, G. & Watson, R.M. (1990) The ben-efit of dental care to an elderly population as-sessed using a sociodental measure of oral hand-icap. British Dental Journal, 168, 153–6.
Fiske, J., Griffiths, J., Jamieson, R. & Manger, D. (2000)Guidelines for oral health care for long-stay pa-tients and residents. Gerodontology, 17, 55–64.
Fiske, J. & Lewis, D. (2000) The development ofstandards for domiciliary dental care services:guidelines and recommendations. Gerodontology,17, 119–22.
Grabowski, M. & Bertram, U. (1975) Oral health sta-tus and need of dental treatment in the elderlyDanish population. Community Dentistry and OralEpidemiology, 3, 108–14.

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
18 Prosthetic Treatment of the Edentulous Patient
Hamilton, F.A., Sarll, D.W., Grant, A.A. & Worthing-ton, H.V. (1990) Dental care for elderly people bygeneral dental practitioners. British Dental Journal,168, 108–12.
Haraldson, T., Karlsson, U. & Carlsson, G.E. (1979)Bite force and oral function in complete denturewearers. Journal of Oral Rehabilitation, 6, 41–8.
Harkins, K. (2002) Social gerodontology. In: ElderlyMedicine – A Training Guide (eds G.S. Rai & G.P.Mulley), pp. 9–12. Martin Dunitz, London.
Heath, M.R. (1972) Dietary selection by elderly per-sons, related to dental state. British Dental Journal,132, 145–8.
Hoad-Reddick, G., Grant, A.A. & Griffiths, C.S.(1987) Knowledge of dental services provided: in-vestigations in an elderly population. CommunityDentistry and Oral Epidemiology, 15, 137–40.
Holm-Pedersen, P. & Loe, H. (1986) Geriatric Den-tistry. Munksgaard, Copenhagen.
MacEntee, M.I. (1985) The prevalence of edentulismand diseases related to dentures – a literature re-view. Journal of Oral Rehabilitation, 12, 195–207.
MacEntee, M.I., Dowell, T.B. & Scully, C. (1988) Oralhealth concerns of an elderly population in Eng-land. Community Dentistry and Oral Epidemiology,16, 72–4.
MacMahon, D.G. & Battle, M. (2002) Developing andplanning services. In: Elderly Medicine – A TrainingGuide (eds G.S. Rai & G.P. Mulley), pp. 19–28. Mar-tin Dunitz, London.
Mojon, P., Thomason, J.M. & Walls, A.W. (2004) Theimpact of falling rates of edentulism. InternationalJournal of Prosthodontics, 17, 434–40.
Moynihan, P.J., Butler, T.J., Thomason, J.M. & Jepson,N.J.J. (2000) Nutrient intake in partially dentate pa-tients: the effect of prosthetic rehabilitation. Journalof Dentistry, 28, 557–63.
Murphy, W.M., Morris, R.A. & O’Sullivan, D.C.(1974) Effect of oral prostheses upon texture per-ception of food. British Dental Journal, 137, 245–9.
Newton, J.P., Yemm, R. & Abel, R.W. (1993) Changesin human jaw muscles with age and dental state.Gerodontology, 10, 16–22.
O’Mullane, D. & Whelton, H. (1992) Oral Healthof Irish Adults 1989–1990. The Stationery Office,Dublin.
Osterberg, T., Carlsson, G.E. & Sundh, V. (2000)Trends and prognoses of dental status in theSwedish population: analysis based on interviewsin 1975 to 1997 by Statistics Sweden. Acta Odonto-logica Scandinavica, 58, 177–82
Owall, B., Kayser, A.F. & Carlsson, G.E. (1996)Prosthodontics – Principles and Management Strate-gies. Mosby-Wolfe, London.
Rai, G.S. & Mulley, G.P. (2002) Elderly Medicine – ATraining Guide. Martin Dunitz, London.
Seymour, R. A. (1988) Dental pharmacology prob-lems in the elderly. Dental Update, 15, 375–81.
Shapiro, S., Bomberg, T.J. & Hamby, C.L. (1985) Post-menopausal osteoporosis: dental patients at risk.Gerodontics, 1, 220–5.
Smith, J.M. & Sheiham, A. (1979) How dental con-ditions handicap the elderly. Community Dentistryand Oral Epidemiology, 7, 305–10.
Steele, J.G., Sheiham, A., Marcenes, W. & Walls,A.W.G. (1998) National Diet and Nutrition Sur-vey: People aged 65 years and over. Vol. 2, Reportof the oral health survey. The Stationery Office,London.
Steele, J.G., Treasure, E., Pitts, N.B., Morris, J. & Brad-nock, G. (2000) Total tooth loss in the United King-dom in 1998 and its implications for the future.British Dental Journal, 189, 598–603.
Strayer, M.S., DiAngelis, A.J. & Loupe, M.J. (1986)Dentists’ knowledge of aging in relation to per-ceived elderly patient behavior. Gerodontics, 2,223–7.
Thomason, J.M, Feine, J., Exley, C., Moynihan, P.,Muller, F., Naert I., Ellis, J.S., Barclay, C., But-terworth, C., Scott B., Lynch, C., Stewardson, D.,Smith, P., Welfare, R., Hyde, P., McAndrew, R., Fen-lon, M., Barclay, S. & Barker, D. (2009) Mandibulartwo implant-supported overdentures as the firstchoice standard of care for edentulous patients –the York Consensus Statement. British Dental Jour-nal, 207, 185–6.
Thomason, J.M., Lund, J.P., Chehade, A. & Feine,J.S. (2003) Patient satisfaction with mandibularimplant overdentures and conventional dentures6 months after delivery. International Journal ofProsthodontics, 16, 467–73.
Walker, A. & Cooper, I. (2000) Adult Dental HealthSurvey. Oral Health in the United Kingdom 1998. TheStationery Office, London.
Walls, A.W.G. & Barnes, I.E. (1988) Gerodontology:the problem? Dental Update, 15, 186–91.
Walsh, K., Roberts, J. & Bennett, G. (1999) Mobility inold age. Gerodontology, 16, 69–74.
WHO (1982) Introductory Document: DemographicConsiderations. World Assembly on Aging, Vienna.
WHO (1992) Country Profiles on Oral Health in Eu-rope 1991. WHO, Regional Office for Europe,Copenhagen.

P1: JZP Trim: 246mm X 189mmc01 BLBK351-Basker December 17, 2010 17:17 Printer Name: Yet to Come
An Appraisal of the Complete Denture Situation 19
Wright, S.M. (1997) Denture treatment for the strokepatient. British Dental Journal, 183, 179–84.
Xie, Q., Ainamo, A. & Tilvis, R. (1997a) Associationof residual ridge resorption with systemic factorsin home-living elderly subjects. Acta OdontologicaScandinavica, 55, 299–305.
Xie, Q., Narhi, T.O., Nevalainen, J.M., Wolf, J. &Ainamo, A. (1997b) Oral status and prostheticfactors related to residual ridge resorption in el-derly subjects. Acta Odontologica Scandinavica, 55,306–13.

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
2Factors Influencing the Outcomeof Prosthetic Treatment
The successful outcome of prosthetic treatmentdepends upon the combined efforts of threepeople:
� The clinician – who makes a diagnosis, pre-pares a treatment plan and undertakes theclinical work.
� The dental technician – who constructs thevarious items, which culminate in the fin-ished dentures.
� The patient – who is faced with comingto terms with the loss of all the naturalteeth, having to adapt to the dentures andaccepting and accommodating their limita-tions.
This chapter will:
� focus on the patient’s contribution to the suc-cess of complete denture treatment,
� review the information on the success rate ofthis treatment, and
� consider whether it is possible to predicttreatment outcome.
The patient’s contributionThe patient needs to know, with the clinician’shelp, what to expect when new dentures areprovided and to be motivated to wear themlong enough for adaptation to take place. Thiswillingness, even determination, of the patientto persevere with new prostheses in the faceof initial difficulties – so that adaptation canoccur – is vital to success for two main reasons:
� There is nothing ‘normal’ about having towear conventional complete dentures. Thechange to the oral environment when twolarge foreign bodies are inserted into themouth is so great that a substantial positiveeffort has to be made to come to terms withit.
� The wearing of these foreign bodies is un-der the complete control of the patient.When difficulties are experienced with thenew dentures they can be removed fromthe mouth, considered, discussed, comparedand even set aside. If this is the patient’smain response to the feeling of strangeness
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
20

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
Factors Influencing the Outcome of Prosthetic Treatment 21
then adaptation will not occur and the treat-ment is likely to fail.
To cope with the drastic change within theoral cavity, the patient must:
� be able to come to terms with the loss of thenatural teeth and their artificial replacement,
� become accustomed to the sensation of thedentures, a process known as habituation,
� learn to control the dentures, and� accept and hopefully appreciate the new
appearance.
The psychological effects oftooth loss
Chapter 1 discussed the effect that tooth losshad on the residual ridges. Whereas a lot of re-search work has been undertaken on that topic,it is only in more recent years that investiga-tions have been carried out to discover the ef-fect of tooth loss on people’s feelings (Fiskeet al. 1998; Davis et al. 2000; Hyland et al. 2009).
In an investigation of patients receivingprosthetic treatment, most having lost their re-maining natural teeth several years previouslyand seeking replacement dentures, 45% admit-ted to having found it difficult to accept the loss(Davis et al. 2000).
Many of those who had difficulties tooklonger than a year to get over the loss, andmore than one-third had still not acceptedit by that time. They expressed feelings ofsadness, anger and depression and many feltthat these last extractions had made them feelprematurely old and that they had lost a partof themselves. There was loss of confidence,a restriction in choice of food and a loweredenjoyment of that food. Relationships with oth-ers were affected and many patients avoidedlooking at themselves without their dentures inplace. The impact of the limitations of completedentures imposed on edentulous patientswas also highlighted in a qualitative studycomparing patients treated with either conven-tional complete dentures or implant-supported
overdentures (Hyland et al. 2009). The find-ings again demonstrated that the functionallimitations of complete dentures often imposesignificant restrictions on edentulous patients,particularly in terms of limiting social partici-pation with family and friends and in the choiceof foods, especially when eating with others.
The disturbing picture for edentulous pa-tients painted by these studies was reinforcedby findings from a national survey of adult den-tal health (Walker & Cooper 2000), which re-vealed that 61% of those who still retained theirnatural teeth found the idea of complete den-tures a very upsetting one. More women wereupset than men and those people who attendedtheir clinicians on a regular basis were morelikely to be troubled than those who did not.Interestingly, the older the dentate person themore likely they were to find the idea of com-plete dentures very upsetting. It is as if thelonger a person has been able to put off the evilday the more troubled they will be if, in spite ofevery effort, they succumb.
From the above account, it may be con-cluded that total tooth loss has a profound ef-fect on a significant proportion of the edentu-lous population and may well introduce addedcomplications to the process of successful reha-bilitation. The following points clearly emergefrom the research work:
� Prevent total tooth loss if possible.� If total loss is inevitable, plan the transition
from the remains of the natural dentition tothe artificial dentition with great care (seeChapter 3).
� Ensure that the patient is properly preparedfor treatment and that everything possible isdone to reduce the inevitable feeling of anx-iety.
� Remember that many wearers of completedentures are still likely to have profoundworries some considerable time after becom-ing edentulous, and that if these worries areaddressed in a sympathetic and encouragingmanner, there will be a greater chance of thecourse of treatment being successful.

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
22 Prosthetic Treatment of the Edentulous Patient
Habituation
Habituation has been defined as follows: ‘Agradual diminution of responses to continuedor repeated stimuli.’
When new dentures are placed in themouth, they stimulate mechanoreceptors inthe oral mucosa. Impulses arising from thesereceptors, which record touch and pressure,are transmitted to the sensory cortex with theresult that the patient can ‘feel’ the dentures.For the first-time denture wearer this bombard-ment of the sensory nervous system almostinevitably results in pronounced salivationwhich, fortunately, only lasts for a few hours.The continuing stimulation of these receptorsdoes not result in a corresponding continuousstream of impulses. The receptors adapt to thisstimulation and as a consequence the patientbegins to lose conscious awareness of the newshapes in the mouth. Of course, if replacementdentures are constructed whose shape is dis-similar to existing ones, a new set of stimuliwill be evoked and the process of habituationstarts all over again. This concept is one of themain reasons for copying dentures, using amethod such as that described in Chapter 8.
In addition to the mechanoreceptors in theoral mucosa being stimulated by the shape ofthe new dentures, further stimulation arises asa result of contact between the occlusal sur-faces during function. The forces generated bycontraction of the muscles of mastication aretransmitted through the dentures to the under-lying tissues, resulting in a pattern of stimula-tion of the mechanoreceptors which enables thepatient to recognise the presence or absence ofocclusal harmony. This is dealt with in greaterdetail in Chapter 14.
Control of the dentures
A discussion of the behaviour of sensory recep-tors is equally relevant when considering thepatient’s ability to control dentures. This is be-cause the successful manipulation of dentures
depends upon purposeful and effective muscu-lar activity, which in turn is dependent on ad-equate sensory feedback. When sensory nerveendings in the oral cavity are anaesthetised,the retention of complete lower dentures is re-duced. In other words, loss of sensory input re-sults in a lower level of purposeful muscle ac-tivity directed at keeping the dentures in place.
The patient’s ability to control dentures in-volves a learning process that, initially, is a con-scious endeavour. The first few faltering stepsof the inexperienced denture wearer are oftendiscouraging both to the patient and to the clin-ician. However, it is comforting to realise thatthe vast majority of these patients return to thesurgery after a few days showing few signs oftheir initial difficulty. The learning process hascome to the rescue. As a result of repetition,new reflex arcs have been set up in the cen-tral nervous system and the conscious efforthas been replaced by a subconscious behaviourpattern. Constant repetition of impulses low-ers the synaptic resistance and facilitates theformation of conditioned reflexes. At the sametime, however, it must be realised that thesynaptic resistance will be increased in the ab-sence of these repeated stimuli. In other words,practice makes perfect whilst idleness leads todecay.
The observation that the first few falteringsteps are usually quickly overcome does notprovide a license to ignore a more staged transi-tion to the edentulous state through both partialdentures and more particularly overdentures asoutlined in Chapter 3.
Appearance
The patient’s perception
‘Beauty is in the eye of the beholder’, and inthe prosthetic context one is concerned withthe patient assessing the appearance of thenew dentures in a mirror. Because a pleasingappearance is a subjective evaluation, there isobviously room for the clinician and patient

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
Factors Influencing the Outcome of Prosthetic Treatment 23
to have differing opinions. However, opendisagreement does not predispose to successfultreatment and so it is vitally important thatthe clinician should take careful notice of apatient’s views on appearance. However, thisdoes not mean that the clinician should blindlyfollow the patient’s requests if they are likely tolead to a poor aesthetic result. Indeed, adviceand particularly demonstration may wellsucceed in convincing the patient that a morepleasing appearance can be obtained by intro-ducing features such as slight irregularities inthe positioning of the anterior teeth and a morenatural shade. However, if demonstration ofsuch modifications fails to convince the patientof their merits then it is likely that the patient’smind is made up and that success will beobtained only if an appearance is producedwhich conforms to the original request.
The clinician’s judgement
Although the patient clearly has the final wordon the appearance of the dentures, there aresome situations in which clinical judgement isparticularly important. Examples of these are asfollows:
� The patient may be tolerating an upper den-ture whose tooth position has been placedtoo near the crest of the resorbed ridge. It isoften possible to improve the appearance ofreplacement dentures by a judicious expan-sion of the upper dental arch. However, ifthe dental arch is expanded too far, the in-creased lip pressure on the labial face of theupper denture can lead to instability.
� Patients may request that new dentures aredesigned to ‘iron out’ creases around themouth or generally to provide more facialsupport. Occasionally under such circum-stances, it is possible to reduce the creasesand so improve the appearance by expan-sion of the upper dental arch or by thicken-ing the denture border as mentioned above.In both these situations, if it has proved pos-
sible to expand the upper arch the possibil-ity of placing the mandibular denture teethfurther buccally and/or labially arises andso avoids, or reduces, the dangers of ‘tonguecramping’.
� The clinician may recognize that therewould be an advantage in constructing re-placement dentures with a lower occlusalplane so that the tongue, by resting on theocclusal surface of the mandibular denture,can be more effective in stabilising it. How-ever, this lowering of the occlusal plane willalter the appearance and may lead to objec-tions from the patient.
On occasions such as those described above,it is advisable for the clinician to explain, testand demonstrate the possible denture changesto the patient. This demonstration can be car-ried out on the patient’s old dentures at thefirst appointment; wax additions can be madeto simulate the possible changes to see if thealterations are likely to achieve the hoped-forbenefits, or whether they are likely to have anydetrimental effects such as instability. An exam-ple of success is shown in Fig. 8.8, whilst Fig. 2.1is an example where the patient’s wishes couldnot be met.
The value of compromise
On all these occasions where it is necessary toseek a compromise between function and ap-pearance, the ability of the patient to accept themodified appearance will depend just as muchon the persuasiveness of the clinician’s expla-nation as on the deeds. Having said this, onemust always be aware of the occasional patientwho will not accept advice. In this case, the clin-ician has the choice of refusing to undertakea form of treatment that is unlikely to satisfythe patient’s objectives of both appearance andfunction, or of making the dentures conformto the patient’s request after warning the pa-tient of the possible outcome and ensuring thathe or she accepts responsibility for the design.

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
24 Prosthetic Treatment of the Edentulous Patient
a b
Figure 2.1 (a) The patient requested that replacement dentures be made to eliminate marked creasing at theangles of the mouth. (b) Possible alterations in design were demonstrated by addition of wax to the existingdentures; the dental arches were expanded and the occlusal vertical dimension increased. With the modifieddentures in the mouth, it was possible to show the patient that her request could not be met and that the creaseswere, in fact, an age change.
Occasionally, it may be possible to satisfy thedemanding patient by constructing two sets ofdentures, one set with which to eat and one setin which to be seen! Needless to say it is vitallyimportant that the eventual decision and rea-sons for that decision are noted in the patient’streatment record.
One further aspect of appearance is worthyof consideration. It is not uncommon for pa-tients to seek replacement dentures in circum-stances where the existing set has deterioratedto such an extent that a great deal of occlusalvertical dimension and lip support has beenlost. In such circumstances, the patients com-monly seek treatment to improve appearance.Replacement dentures that correct the aestheticfaults in the old dentures will undoubtedlymake a dramatic change in appearance – achange hopefully appreciated by the patient.However, there is the risk that the change in ap-pearance is so marked that it will be noticed bythe patient’s friends and relatives. The patient’sinitial enthusiasm for the new image is likelyto be dampened if people stare rather point-edly, or even ask somewhat tactless questionsabout the new dentures. Such unwelcome com-
ments can undermine the patient’s confidencebecause they indicate that the friend recognisesthat the patient is a denture wearer. When ob-vious but necessary changes in appearance arebeing made, it is, therefore, a wise policy towarn the patient in advance of possible reac-tions from friends so that he or she is mentallyprepared for them, and therefore, less likely tobe discouraged.
Success rate of treatmentThe discussion so far has ranged around theconcept of the patient adapting to new den-tures. The degree of success with which pa-tients cope with the inevitable limitations of anartificial replacement varies enormously. For-tunately, the majority of patients have surpris-ingly little difficulty in adapting to an artificialdentition. However, it has been reported thatabout 15% of patients are dissatisfied with theirnew dentures (van Waas 1990a; Al Quran et al.2001) and that this level may rise to 20% wheretreatment is being provided for patients whohave had persistent problems (Lechner et al.1995). It has also been shown that even if very

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
Factors Influencing the Outcome of Prosthetic Treatment 25
high levels of satisfaction are recorded immedi-ately after new dentures have been fitted, a sig-nificant deterioration occurs after 1 year (Berg1988; Mersel et al. 1995). Most of the recurringdissatisfaction is blamed on the fit and comfortof the lower denture and the inability to eat ef-fectively. This comment emphasises the impor-tance of recalling patients and maintaining thedentures (Chapter 15). For example, relining orreplacing dentures can readily restore chewingability and the level of enjoyment when eat-ing (Garrett et al. 1996). In addition, many pa-tients simply accept a range of limitations asinevitable and ‘learn to live with them’ eventhough their general satisfaction and quality oflife is adversely affected. In spite of these dif-ficulties, such patients may not admit to themunless the relevant questions are put directly tothem in a sympathetic manner (Hyland et al.2009). Some patients present very consider-able difficulties that can in fact be treated suc-cessfully by using special techniques. How-ever, there remain a few patients who neverbecome successful denture wearers. Can theybe identified before treatment commences?The next section attempts to answer thisquestion.
Predicting treatment outcomeHow can one predict the outcome of completedenture treatment? Various attempts have beenmade to select various factors which, over theyears, have been thought, either individuallyor collectively, to influence the eventual out-come of treatment. These factors include thefollowing:
� Age of the patient� Quality of care provided and previous com-
plete denture experience� The patient’s expectations and attitude to-
wards dentures� Opinion of a third party� General health
A review of the literature has led to the con-clusion that there are still no reliable methods topredict the outcome of complete denture treat-ment (Carlsson 1998) and that satisfaction withdentures for most patients is individually de-termined, and for clinician and patient, is of-ten unpredictable (van Waas 1990a). Neverthe-less, the research offers some helpful pointers,and just as importantly, debunks some cher-ished beliefs.
The various factors will now be consideredbriefly.
Age of the patient
Age has not been found to be an accurate pre-dictor of success or failure to adapt to newdentures (Beck et al. 1993). In general, as pa-tients grow older, it takes longer for them toadapt successfully to new dentures for the rea-sons already discussed in Chapter 1. As the rateof ageing varies greatly between individuals,the actual age of a patient may be an unreli-able guide to adaptive potential. A better basisfor this assessment is the biological age, whichmay be estimated by judging how old the pa-tient looks. It is not uncommon for the bio-logical and actual ages to differ markedly. Forexample, when comparing the two people inFig. 2.2, one would not expect the woman tohave greater difficulty in adapting to the den-tures in spite of the fact that she is 23 years olderthan the man. Increasing age should be lookedat as offering a particular advantage in that thepatient is likely to be able to draw upon pre-vious denture experience, which, if favourable,can play an extremely valuable part in achiev-ing ultimate success.
At this point, there should be a word ofwarning. Little is yet known about the abilityof elderly people to adapt to the change fromwhat remains of the natural dentition to a to-tally artificial one. With advances in preventivedentistry and an increased expectancy of life,one can foresee the possibility of people beingfaced with their first set of complete dentures

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
26 Prosthetic Treatment of the Edentulous Patient
a b
Figure 2.2 Variation of biologicalage with actual age. The woman,aged 89, is 23 years older than theman.
much later in life. The problems of adaptationwith which prosthetic dentistry will be facedcould well increase in the future for reasonsmentioned earlier in this chapter.
The quality of care and previousdenture experience
A survey of the literature shows inconsis-tency in identifying a positive association be-tween patient satisfaction and denture qual-ity. Whereas some researchers have reportedno correlation (Vervoorn et al. 1988; de Baatet al. 1997), others have reported moderate cor-relation (van Waas, 1990a,b; Garrett et al. 1996)and still others have shown positive associa-tion with patient satisfaction (Reeve et al. 1984;Smith & Hughes 1988; Beck et al. 1993; Lambet al. 1994; Fenlon et al. 2000; Fenlon & Sherriff2008).
We conclude that of all the predictors of suc-cess which have been investigated, the qualityof the prosthetic care provided stands out asthe factor which is most strongly linked withpatient satisfaction. This conclusion should notreally be surprising and it highlights the fun-
damental importance of routinely adoptingthe best possible clinical and technical prac-tices and of continually seeking to enhance thequality of care. These points are emphasisedthroughout this book.
The significance of the past dental history,its link with quality and with adaptability, canbe illustrated by considering two common yetcontrasting situations. There are those patientswho seek new dentures to replace existing onesthat have been worn for very many years. Sooften it is apparent that the old dentures arenow ill-fitting and the occlusion is no longerbalanced, and yet the patient has tolerated anincreasing inadequacy for some time. Althoughthis state of affairs may well indicate initial highdenture quality and a well-marked ability toadapt to dentures and to overcome difficulties,such a level of perseverance can be dangerous,as it can result in accelerated resorption of theunderlying bone and may induce pathologicalchanges in the mucosa. This picture of stoicismis in marked contrast to the second group, madeup of patients who have been provided withseveral sets of dentures in a short period oftime. Such a story of repeated failure may at

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
Factors Influencing the Outcome of Prosthetic Treatment 27
first sight indicate a patient who is unable orunwilling to accept complete dentures. How-ever, there is another potent reason for repeatedfailure of prosthetic treatment and this may be-come apparent during examination of the var-ious old dentures as obvious errors in designand construction are identified in each of them.If patients receive inadequate treatment on oneor more occasions and are told that the prob-lems experienced are due to them, confidencein prosthetic treatment is lost rapidly and amental barrier is built up against dentures.
At first thought, it might seem commonsense that there would be an obvious rela-tionship between patient satisfaction and thequality of the denture-bearing tissues. In otherwords, it is easier to achieve success for a pa-tient who has well-formed ridges on which toplace dentures and vice versa. However, not allthe investigations support such a relationship –perhaps because those patients who have poorridges have learned to accept the inevitable lim-itations and have adapted particularly well tothe handicap (van Waas 1990a; de Baat et al.1997).
Nevertheless, in the cases where examina-tion of the mouth indicates that the prognosisfor dentures is poor, it is essential for the clini-cian to warn the patient in advance of the dif-ficulties and to describe the steps that will betaken to minimise them. If a patient is not ad-vised of the limited prognosis in the particu-lar circumstances, any shortcomings in perfor-mance may be blamed on the dentures and thepatient becomes discouraged prematurely.
It should also be remembered, as stated atthe beginning of the chapter, that there is noth-ing ‘normal’ about having to wear conventionalcomplete dentures. As such we should not besurprised that patients have difficulties accom-modating to them and that this accommoda-tion may only be partial. Thus, the possibilityof other treatment alternatives, such as the useof dental implants for denture support, shouldbe actively considered as a means of enhancingthe possible success rates.
The patient’s expectations andattitude towards dentures
Patients requesting replacement dentures gen-erally do so for reasons of function and ap-pearance; function includes fit and comfort ofthe dentures as well as the ability to eat effec-tively. As mentioned earlier, a satisfactory out-come to treatment is generally related to thelevel of function achieved and to the technicalquality of the dentures (Fenlon & Sherriff 2008).It is of interest to note that concern over ap-pearance seems to be under-reported, both be-fore and after treatment. If functional require-ments have been satisfied by the new dentures,patients may be inclined to look more closelyat appearance. If they are unhappy with whatthey see, there is occasionally a reluctance tocomplain directly. Instead, patients may resortto making complaints about function to drawthe clinician’s attention to their real concernin a somewhat roundabout way. Functionalcomplaints that seem to have no logical causeshould always be considered in this particularlight.
One study (van Waas 1990b) has pointed outthat a patient’s attitude to dentures can be auseful predictor of satisfaction or dissatisfac-tion. Agreement or disagreement to the follow-ing statements might be obtained from a patientbefore commencing treatment:
� I expect to have problems with my new den-tures.
� I think I’ll soon get used to my new dentures.� I think it is difficult to make good dentures
for me.� I think they’ll manage to make good den-
tures for me.� I did not receive dentures that like me.
The ‘wrong’ answers should at least make oneaware of the possibility of an unsatisfactoryoutcome.
Nevertheless, it should also be noted thatthe patient’s expectations of what conventional

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
28 Prosthetic Treatment of the Edentulous Patient
complete dentures are capable of may not ac-tually be realizable and that implant-supporteddentures may be a more reliable way of satisfy-ing the patients’ wishes. One recent study hassuggested that post-treatment satisfaction withconventional complete dentures was signifi-cantly lower than the patients’ pre-treatmentexpectations, whereas the pre-treatment expec-tations of implant-supported overdenture werelargely met (Heydecke et al. 2008). It may bethe initial unrealistic expectation of what can beachieved with conventional complete denturesthat ultimately leads to some patients’ dissatis-faction with dentures even though constructedto a high standard.
The opinion of a third party
Earlier in the chapter, we drew attention to po-tential complications which might arise follow-ing critical comments about the new denturesfrom friends and relations. It has been shownthat such comments, which are mostly centredon appearance, show a highly significant cor-relation with acceptance of the dentures by thepatient (Berg et al. 1985). Negative commentscan cause disappointment and rejection of theprostheses, whilst positive comments can pro-mote cheerful acceptance of the treatment.
Health of the patient
Significant impairment of general bodily ormental health may affect the learning processadversely, with the result that the patient be-comes discouraged because of major difficul-ties in mastering new dentures. In this respect,it should be remembered that the chances ofimpairment of health increase as people growolder. Therefore, when assessing a patient, it isvery important to note details of the medicalhistory, such as a chronic debilitating illness,which may reduce the patient’s stamina to suchan extent that there is little left to cope withthe demands of new dentures. For example, pa-tients suffering from any form of arthritis may
be persistently troubled with pain to the extentthat it becomes a depressing and overwhelmingpart of life. The ability to manipulate denturesmay be reduced severely by various neurologi-cal disorders, such as the muscle tremor and re-duced muscular power of Parkinson’s disease,and the muscle weakness of myasthenia gravisor bulbar palsy.
It has long been believed that any set of cir-cumstances which impairs mental health maycreate a situation whereby anxiety, depressionor other neurotic states may result in the pa-tient being unable or unwilling to tolerate newdentures. Clues that such adverse psychologi-cal factors exist may be supplied by the medicalhistory; for example, the patient may be takingtranquillisers or sedatives. To assist cliniciansin recognising behavioural problems, variousquestionnaires have been designed to measurecharacteristics of personality and the levels ofanxiety or depression.
The results of studies in this area areequivocal, whereas some point towards alink between, for example, neuroticism anddissatisfaction with the outcome of prosthetictreatment, others do not (Beck et al. 1993; AlQuran et al. 2001). At the beginning of thechapter, attention was drawn to the negativefeelings shared by many people who had losttheir remaining natural teeth. When comingacross a patient who has had persistent dis-satisfaction with complete dentures, it wouldseem sensible, at the very least, to discovertheir feelings and attitudes to prosthetic treat-ment, to offer advice or seek help from a dentalor medical colleague as appropriate.
Readers may reasonably conclude at the endof this chapter that the pre-treatment assess-ment of a patient with respect to the level ofultimate success is far from being an exact sci-ence. They would be correct.
Clinical prosthetic experience is littered withpleasant surprises and with disappointments.Our review of current knowledge leads usto conclude that as long as a high standardof treatment is provided the disappointments,

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
Factors Influencing the Outcome of Prosthetic Treatment 29
though inevitable, will at least be kept to aminimum.
References and additionalreadingAl Quran, F., Clifford, T., Cooper, C. & Lamey, P.-J.
(2001) Influence of psychological factors on the ac-ceptance of complete dentures. Gerodontology, 18,35–40.
Beck, C.B., Bates, J.F., Basker, R.M., Gutteridge, D.L.& Harrison, A. (1993) A survey of the dissatisfieddenture patient. European Journal of Prosthodonticsand Restorative Dentistry, 2, 73–8.
Berg, E. (1984) The influence of some anamnestic, de-mographic, and clinical variables on patient accep-tance of new complete dentures. Acta OdontologicaScandinavica, 42, 119–27.
Berg, E. (1988) A 2-year follow-up study of patientsatisfaction with new complete dentures. Journal ofDentistry, 16, 160–5.
Berg, E., Backer Johnsen, T. & Ingebretsen, R. (1984)Patient motives and fulfillment of motives in re-newal of complete dentures. Acta OdontologicaScandinavica, 42, 235–40.
Berg, E., Backer Johnsen, T. & Ingebretsen, R. (1985)Social variables and patient acceptance of com-plete dentures. Acta Odontologica Scandinavica, 43,199–203.
Berry, D.C. & Mahood, M. (1966) Oral stereognosisand oral ability in relation to prosthetic treatment.British Dental Journal, 120, 179–85.
Brill, N., Tryde, G. & Schubeler, S. (1959) The role ofexteroceptors in denture retention. Journal of Pros-thetic Dentistry, 9, 761–8.
Brill, N., Tryde, G. & Schubeler, S. (1960) The role oflearning in denture retention. Journal of ProstheticDentistry, 10, 468–75.
Carlsson, G.E. (1998) Clinical morbidity and seque-lae of treatment with complete dentures. Journal ofProsthetic Dentistry, 79, 17–23.
Crum, R.J. & Loiselle, R.J. (1972) Oral perception andproprioception: a review of the literature and itssignificance to prosthodontics. Journal of ProstheticDentistry, 28, 215–30.
Davis, D.M., Fiske, J., Scott, B. & Radford, D.R.(2000) The emotional effects of tooth loss: a prelim-inary quantitative study. British Dental Journal, 188,503–6.
de Baat, C., van Aken, A.A., Mulder, J. & Kalk, W.(1997) ‘Prosthetic condition’ and patients’ judge-
ment of complete dentures. Journal of ProstheticDentistry, 78, 472–8.
Fenlon, M.R. & Sherrif, M. (2008) An investigation offactors influencing patients’ satisfaction with newcomplete dentures using structural equation mod-eling. Journal of Dentistry, 36, 427–34.
Fenlon, M.R., Sherrif, M. & Walter, J.D. (2000) Aninvestigation of factors influencing patients’ useof new complete dentures using structural equa-tion modelling techniques. Community Dentistryand Oral Epidemiology, 28, 133–40.
Fish, S.F. (1969) Adaptation and habituation to fulldentures. British Dental Journal, 127, 19–26.
Fiske, J., Davis, D.M., Frances, C. & Gelbier, S. (1998)The emotional effects of tooth loss in edentulouspeople. British Dental Journal, 184, 90–3.
Garrett, N.R., Kapur, K.K. & Perez, P. (1996) Effects ofimprovements of poorly fitting dentures and newdentures on patient satisfaction. Journal of ProstheticDentistry, 76, 403–13.
Heydecke, G., Thomason, J.M., Awad, M.A., Lund,J.P. & Feine, J.S. (2008) Do mandibular implantoverdentures and conventional complete denturesmeet the expectations of edentulous patients?Quintessence International, 39, 803–9.
Hyland, R., Ellis, J., Thomason, M., El-Feky, A. &Moynihan, P. (2009) A qualitative study on patientperspectives of how conventional and implant-supported dentures affect eating. Journal of Den-tistry, 37, 718–23.
Lamb, D.J., Ellis, B. & Kent, G. (1994) Measurement ofchanges in complete mandibular denture securityusing visual analogue scales. International Journal ofProsthodontics, 7, 30–4.
Lechner, S.K., Champion, H. & Tong, T.K. (1995)Complete denture problem solving: a survey. Aus-tralian Dental Journal, 40, 377–80.
Mersel, A., Babayof, I., Berkey, D. & Mann, J. (1995)Variables affecting denture satisfaction in Israelielderly: a one year follow-up. Gerodontology, 12,89–94.
Reeve, P.E., Watson, C.J. & Stafford, G.D. (1984) Therole of personality in the management of completedenture patients. British Dental Journal, 156, 356–62.
Smith, J.P. & Hughes, D. (1988) A survey of re-ferred patients experiencing problems with com-plete dentures. Journal of Prosthetic Dentistry, 60,583–6.
van Waas, M.A.J. (1990a) Determinants of dissatisfac-tion with dentures: a multiple regression analysis.Journal of Prosthetic Dentistry, 63, 569–72.

P1: JZP Trim: 246mm X 189mmc02 BLBK351-Basker December 17, 2010 10:1 Printer Name: Yet to Come
30 Prosthetic Treatment of the Edentulous Patient
van Waas, M.A.J. (1990b). The influence of clinicalvariables on patients’ satisfaction with completedentures. Journal of Prosthetic Dentistry, 63, 307–10.
van Waas, M.A.J. (1990c). The influence of psycho-logic factors on patient satisfaction with completedentures. Journal of Prosthetic Dentistry, 63, 545–8.
Vervoorn, J.M., Duinkerke, A.S., Luteijn, F. & van dePoel, A.C. (1988) Assessment of denture satisfac-tion. Community Dentistry and Oral Epidemiology,16, 364–7.
Walker, A. & Cooper, I. (eds) (2000) Adult DentalHealth Survey. Oral Health in the United Kingdom1998. The Stationery Office, London.
Weinstein, W., Schuchman, J., Lieberman, J. & Rosen,P. (1988) Age and denture experience as determi-nants in patient denture satisfaction. Journal of Pros-thetic Dentistry, 59, 327–9.
Zigmond, A.S. & Snaith, R.P. (1983) The HospitalAnxiety and Depression Scale. Acta PsychiatricaScandinavica, 67, 361–70.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
3Transition from the Naturalto the Artificial Dentition
The loss of the remaining natural teeth and pro-vision of an artificial dentition is a major and ir-reversible procedure for the patient. The enor-mity of the change raises the question – why isit not more common to use overdentures overnatural tooth remnants, at least as a stagingpost, in the transition to the edentulous state?This is particularly the case as such overden-tures may last for so long that the patient isable to continue having the denture supportedby these natural abutments for the rest of hisor her life. The question as to why this transi-tion is not more frequently used is brought intosharp focus when one considers the improve-ments seen in patient satisfaction and qualityof life provided by implant-supported overden-tures when compared with conventional den-tures (Thomason 2007). Before discussing thevarious ways of making the transition, it ishelpful to consider just how common is thesudden, complete transition to the edentulousstate and the typical reaction that patients haveto the prospect.
Regular national surveys of the dental healthof adults enable us to examine the changing
state of dentitions and the attitudes of peo-ple to their dental status (Todd & Lader 1991;Walker & Cooper 2000). The general improve-ment in oral health has already been describedin Chapter 1. With respect to the transition,there have been parallel improvements with theloss of natural teeth becoming an increasinglygradual process. For example, whereas in 1978two-thirds of those who had lost the remainderof their teeth had 12 or more teeth extracted atthe final stage, this proportion was reduced tonearly half in the next decade and to a quarterin the 1990s.
The level of anxiety with which people facethe prospect of losing all their teeth and hav-ing to rely on complete dentures can be seenin Fig. 3.1. Nearly two-thirds of those peo-ple who did not wear dentures of any kindfound the thought of having to wear com-plete dentures very upsetting. The concern wasfelt more by women than by men and moreby those people who were regular attendersfor dental treatment. It is important that theclinician appreciates that the transition can bea cause of great concern to the patient and
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
31

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
32 Prosthetic Treatment of the Edentulous Patient
62%
24%
14% 22%
39%
39%
Anticipatingcomplete dentures
Anticipatingpartial dentures
Very upsetting A little upsetting Not at all upsetting
Figure 3.1 The attitude of adults(%) with only natural teeth to thethought of having complete den-tures or a removable partial den-ture. (From Todd & Lader, 1991.)
takes the opportunity not only to manage thistransition with understanding but also to of-fer alternatives to simply rendering the patientedentulous.
It can also be seen in Fig 3.1 that the con-cern about having complete dentures is muchgreater than that about partial dentures. An-other important point to make is that this at-titude had become more widespread over a10-year period between surveys to the extentthat the proportion of those who viewed thethought of having complete dentures as a veryupsetting experience had gone up by 10%.
The level of concern felt by the general pub-lic can be examined in another way (Fig. 3.2).Here the level of anxiety was gauged amongstthose who thought they were likely to needcomplete dentures within 5 years, those whowould need complete dentures at sometime inthe future and those who felt they would neverrequire complete dentures. As expected, theproportion of those who were very upset about
19%
26%
55% 48%
27%
25%
66%
23%
11%
(a) Within 5 years Likelihood of complete dentures:
(b) Sometime (c) Never
Very upsetting A little upsetting Not at all upsetting
Figure 3.2 The attitude of adults(%) with only natural teeth to thethought of having complete denturesby the likelihood that they will needthem. (From Todd & Lader, 1991.)
the prospect of having complete dentures in-creased as their expectations of keeping theirnatural teeth increased. But even amongst thosewho thought they would need complete den-tures in the next 5 years, one in five viewed theprospect as a very upsetting experience.
What is quite apparent is that a significantproportion of people who may have to havetheir remaining teeth extracted and completedentures provided view the prospect with agreat deal of concern and anxiety, thus mak-ing their acceptance of treatment much harder(see Chapter 2). The aim of this chapter is tooutline the principles of treatment contribut-ing to a successful transition either when forcedto remove all the remaining tooth elements, orbetter still when at least some roots can be re-tained as overdenture abutments. The use ofimplants in place of tooth roots to support andstabilise the lower denture is also considered.Details of clinical techniques are, in the main,omitted.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 33
Methods of transitionThe various methods of making the transitionfrom natural to artificial dentition may be con-sidered under the following headings.
Transitional partial dentures
Transitional partial dentures restore existingedentulous areas. They may be worn for a shortperiod of time before the remaining naturalteeth are extracted and the dentures are con-verted accordingly.
Overdentures
Overdentures are fitted over retained roots andderive some of their support and, if appropri-ately contoured, some stability from that cov-erage. Special attachments may be fixed to theroot faces to provide mechanical retention forthe denture which will further increase the den-ture stability. If, in due course, the roots have tobe extracted, the overdenture can be convertedinto a mucosally-supported complete denture.In addition, overdentures can be supported andretained by implants.
Immediate dentures
Immediate dentures are constructed before theextraction of the natural teeth and are in-serted immediately after removal of those teeth.An immediate denture can be either a con-ventional complete denture without supportfrom the tooth roots, or a complete immediateoverdenture.
Clearance of remaining naturalteeth before making dentures
This approach differs from all those mentionedpreviously in that, after the extractions, time isallowed for initial healing and alveolar boneresorption to occur before providing completedentures.
Factors influencing the decisionof whether to extract all theremaining teeth or to retainsome teeth or tooth rootsWhen the patient’s dentition has reached thestage where it appears that complete dentureswill be necessary in the foreseeable future, theclinician must consider carefully the timing ofextraction of the remaining teeth and if it wouldbe possible to retain some tooth roots, even ifonly in the short term. The following consider-ations will influence the decision.
The condition of the teeth andsupporting tissues
The prognosis for each remaining tooth shouldbe assessed carefully. Useful teeth can be re-tained if:
� it is feasible to undertake appropriate treat-ment to eliminate any disease present;
� if there is confidence in the patient’s abilityto maintain good, or even reasonable, oralhealth.
The presence of gross caries or advanced peri-odontal disease, coupled with an inability of thepatient to maintain an acceptable level of oralhygiene, makes the decision of whether or notto extract the teeth a much simpler one; earlyextraction in such circumstances is probably ad-visable. Such a decision is perhaps especiallyimportant in the case of advanced periodon-tal disease where any undue delay will resultin further destruction of what will become thebony denture foundation. Nevertheless, manypatients who would be unwilling or unable tomanage reasonable oral hygiene around multi-ple teeth, can often manage to clean two sim-ple overdenture abutments, or at least to cleanthem well enough to delay significant short-term bone loss.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
34 Prosthetic Treatment of the Edentulous Patient
The position of the teeth
Natural teeth opposing an edentulousridge
The situation in which one arch only is ren-dered edentulous can lead to major prostheticcomplications. The combination most com-monly found is a complete upper denture op-posed by a number of lower natural teeth. Amost unfavourable situation can develop inwhich the natural teeth generate high occlusalloads and excessive displacement of the den-ture, which may result in:
� rapid destruction of the denture-bearingbone;
� the production of a flabby ridge (see Chapter16);
� complaints of a loose denture;� a deteriorating appearance as the denture
sinks into the tissues;� fracture of the denture base.
The problems are accentuated in the lower jawbecause the denture-bearing area is smaller.
Serious consideration must be given to pre-venting these problems from developing. Thefirst step is to warn the patient of the possibleconsequences and arrange for regular inspec-tion and maintenance to reduce the possibil-ity of rapid, damaging resorption. If sufficientthought has been given to the problem in ad-vance, it may be possible to utilise selected teethas overdenture abutments so as to improve theloading on the underlying bone. It would bevery rare for the clinician to consider trying toreduce the occlusal loads by extracting soundteeth in the opposing arch.
Over-eruption of the teeth
Extraction of over-erupted teeth may be re-quired because they:
� excessively reduce the vertical space avail-able for the opposing prosthesis;
� have a poor appearance.
In appropriate cases, endodontic therapy fol-lowed by decoronation of over-erupted teeth(so that they can be used as overdenture abut-ments) might be the preferred alternative ap-proach. This also has the marked advantagethat decoronating the tooth markedly improvesits crown–root ratio and, therefore, creates amore favourable loading, usually resulting in aconsiderable reduction in mobility.
Age and health of the patient
As mentioned in Chapter 2, advancing years,frequently coupled by worsening health, mayreduce the patient’s ability to adapt success-fully to complete dentures. This places the clin-ician on the horns of a dilemma when planningthe timing of the extraction of teeth that have anuncertain prognosis:
� Extract the remaining teeth earlier? On the onehand, the teeth may be expected to have afew more years of useful life, but delayingextractions until they are unavoidable maypostpone the patient’s first experience ofcomplete dentures to a time when ageinghas seriously reduced adaptive capability.As a result, the patient may find it difficult,or even impossible, to cope with completedentures when they are eventually fitted.It may therefore be argued that the bestapproach under such circumstances is toextract the teeth sooner rather than later sothat the patient stands a better chance ofadapting successfully to complete dentures.Better still, though, would be a plannedprogression through transitional partialdentures, the undertaking of endodontics onselected teeth for later overdenture supportand eventually the conversion of the partialdenture to a simple complete overdenture.
� Extract the remaining teeth later? As the rateof biological ageing and reduction in adap-tive capability vary greatly from one patientto another, it is not possible to identify ac-curately a cut-off point in years at which

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 35
extractions should be carried out for the rea-son outlined above. It is true that early ex-tractions may reduce problems of adapta-tion to dentures, but this advantage must bebalanced against the immediate probabilityof reduced oral function and comfort in apatient who may be happy with a few re-maining natural teeth and, perhaps, a partialdenture.
The correct way out of the dilemma of whetheror not to take the irrevocable step of a dentalclearance may be determined by delaying thedecision and placing the patient on a pro-gramme of regular review appointments. Ateach appointment, an assessment can be madeof the rate of deterioration of the patient’s den-tition, and thus a clearer picture will emergeof the probable life of the teeth and their valueto the patient. A somewhat crude judgementis to assess the health of the patient and theteeth and try to answer the question, ‘Is thepatient likely to outlive the remaining usefulnatural teeth, or is the reverse more likely tooccur?’ When it seems probable that the patientwill outlive the remaining teeth in their currentform, the first step should be the considerationof a staged transition, from partial denturesthrough to overdentures and, only if necessary,to conventional complete dentures. This wayany decision to take action can be moderatedby the patient’s response to each phase oftreatment.
It is important to remember that in the veryelderly patient any elective alteration of oralstatus must be made only when absolutely nec-essary. On balance, extractions should proba-bly be carried out only when they are unavoid-able, not as an elective procedure in the hopethat this will reduce adaptive difficulties later.In fact, those difficulties are likely to be presentalready.
To this end, there is a strong argument thatevery effort should be made to retain useful,strategic teeth which may either help to sta-bilise a partial denture or be converted into
overdenture abutments. The argument may beextended by saying that if these last remainingteeth are extracted, and the patient experiencesenormous problems with the complete den-tures, the only way of minimising these prob-lems is to provide an implant-retained over-denture. Such treatment is more costly. Thus,retaining these few natural teeth may well savethe patient considerable trouble and expenseand the clinician no little heartache.
The patient’s wishes
The patient will often have views aboutwhether or not the remaining teeth should beextracted and these views must of course begiven high priority. If the views coincide withthe clinician’s judgement all is well. However,the following two scenarios occur occasionallyand might cause the clinician some difficulty.
Hopeless teeth that the patient wantsto retainThe clinician should carefully explain to thepatient about the condition of the teeth andthe possible harmful consequences of retainingthem. If in spite of this the patient persists inwanting to retain the teeth, the clinician can dolittle apart from carefully noting the situation inthe patient’s record. A decision may still have tobe made on whether to proceed with an alter-native treatment plan, such as the provision oftransitional partial dentures or an overdenture,or whether to withdraw from treatment.
Sound, useful teeth that the patientwants extractedAgain, the clinician’s primary responsibility isto explain to the patient the nature of the clin-ical situation and to emphasise the harm thatunnecessary extraction of the remaining teethwould cause. If this is done with care, the ma-jority of patients will be persuaded of the valueof keeping the teeth, or the tooth roots wherethis would be more appropriate. Judging from

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
36 Prosthetic Treatment of the Edentulous Patient
the relatively small number of tooth-supportedoverdentures it would appear that this is anarea that the dental profession has probablynot promoted sufficiently in the past. However,even after careful explanation a few patientswill not accept the case for retaining the teeth;the appropriate action by the clinician is mostlikely to be withdrawal from the case, as toextract the teeth without clinical justificationwould be unethical.
Transitional partial denturesTransitional partial dentures are of particularvalue in those cases where problems of adap-tation to, or tolerance of, complete dentures areanticipated. Wearing a transitional partial den-ture provides:
� an opportunity to complete any denture ad-justments found necessary to provide com-fort and adequate function, before the re-maining teeth are extracted or decoronated;
� a training period that allows the patient todevelop some denture control and toleranceunder circumstances made less demandingby the stabilising effect of the remainingteeth.
However true this may be, a study of unsuc-cessful and successful complete denture wear-ers did not conclude that a history of wearing apartial denture had any influence on the even-tual outcome (Beck et al. 1993).
The chance of success of a transitional partialdenture is influenced to a large extent by theparticular teeth that remain in the mouth. Forexample, stability of a lower denture will be in-creased if an anterior saddle is present becausethe existence of the labial flange and contactswith the mesial surfaces of the abutment teethwill resist posterior displacement. Also, if thedenture carries anterior teeth, the patient willbe better motivated by the wish to retain a gooddental appearance to persevere with the den-ture in the face of any initial difficulties. Suc-cess is also more likely if the denture design in-
corporates clasps (and preferably rests) to max-imise retention and support. Although transi-tional partial dentures are a potentially valu-able means of smoothing the passage from thepartially dentate to the edentulous state, theycan compound the difficulties of subsequentcomplete dentures unless they are correctly de-signed and adequately maintained. A partialdenture that is under-extended, poorly fittingor which has an incorrect occlusion is likelyto be unstable and uncomfortable, thus un-dermining the patient’s confidence in denturewearing. Also, if the patient perseveres hero-ically with the partial denture in spite of thedifficulties, destruction of the denture-bearingtissues is likely to occur, creating a more un-favourable foundation for subsequent completedentures. Whilst traditionally these transitionalpartial dentures have been supported only bythe soft tissues (so called tissue-borne) there isno reason why this should be the case. The im-portant advantage of a transitional denture isthat it can be added to when teeth need to beextracted; this usually means that the connec-tor needs to be constructed from acrylic resin.It should be remembered that the transitionalpartial denture is the type of prosthesis usuallyprovided for a patient whose dental awarenessis highly suspect. In this situation, increasedplaque formation and lack of adequate supportcan combine to cause severe tissue destructionin a relatively short time (Fig. 3.3). In such a
Figure 3.3 Severe tissue destruction caused by atissue-borne partial denture.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 37
case, a high-risk denture is provided for a high-risk patient.
Tooth-supported overdenturesIn the transitional dentition the overdenture,like the partial denture, can be used to provide atraining period, allowing the patient to preparefor the more demanding task imposed by futureconventional complete dentures. If the life ofthe teeth is limited, treatment should normallybe kept as simple as possible. However, eventhe simplest overdenture treatment usually en-tails root filling and decoronating two or threeabutment teeth. As the loading of the teethis more advantageous once they are decoro-nated, the simple overdenture may well extendthe life of these remaining abutments. There-fore with tolerably acceptable oral hygiene, thetooth supported complete overdenture can be along-term treatment option for many patients.
Advantages of tooth-supportedoverdentures
Preservation of the ridge form
Retaining the roots and periodontal tissues ofthe abutment teeth reduces resorption of thesurrounding bone. This is the most importantadvantage of overdentures, particularly for thelower jaw where it has been shown that pre-serving the canine roots can reduce the rate ofresorption in that region by a factor of 8. Thispreservation of alveolar bone has obvious ben-efits in providing support and promoting sta-bility of dentures. If the retained roots are in theanterior region, the preservation of bone willalso help to maintain support of the lips andthus will contribute to facial appearance.
Minimising horizontal forces on theabutment teeth
The reduction in crown length of the abutmentteeth and the production of a domed shape tothe root face reduces the mechanical advan-
tage of potentially damaging horizontal forces.As mentioned above, the life of the abutmentteeth may therefore actually be prolonged, andteeth that were very mobile before treatmentcommonly become firmer. This change in mo-bility is partly due to the improvement in thecrown–root ratio. In addition, the absence ofteeth on either side of these overdenture abut-ments facilitates oral hygiene measures whichcan be especially helpful for those who havefound this a challenge in the past.
Proprioception
It has been suggested that while the roots andtheir periodontal ligaments remain, periodon-tal mechanoreceptors allow a finer discrimina-tion of food texture, tooth contacts and levelsof functional loading. A better appreciation offood and a more precise control of mandibu-lar movements may therefore be possible thanis provided for by receptors in the denture-bearing mucosa of edentulous patients. In the-ory this may mean that natural tooth roots mayserve better in this regard than dental implantswhich are devoid of periodontal mechanore-ceptors.
Correction of occlusion and aesthetics
Overdentures have a particular advantage overpartial dentures in those cases where thecrowns of the remaining few teeth are not idealeither in terms of occlusion or appearance. Re-moval of the offending crowns and covering ofthe roots with an overdenture provide the free-dom in artificial tooth arrangement necessaryto correct the undesirable features.
Denture retention
As mentioned earlier, more positive retention ofthe denture to the root faces may be obtainedby means of precision attachments (Fig. 3.4).However, in many instances, such additionalretention seems not to be needed. Indeed whilstprecision attachments may make a positive

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
38 Prosthetic Treatment of the Edentulous Patient
Figure 3.4 Stud attachments on the abutment teethare engaged by spring clips within the overdenture toprovide positive retention.
contribution to retention on roots with goodbone support, they are contraindicated foroverdentures provided as a transitional stage oflimited duration en route to conventional com-plete dentures for the following reasons:
� The increased height of the abutment arisingfrom the precision attachment will adverselyaffect the crown–root ratio of the tooth. Asa result, the tooth root will be subjected tolarger horizontal forces.
� Attachments are relatively expensive and,therefore, may not be cost-effective if usedon abutment teeth with a poor prognosis.
� The retention achieved with attachments canbe too good, thus inhibiting the develop-ment of the patient’s neuromuscular skillsthat will be required to control the futureconventional complete dentures when theloss of these roots is inevitable.
An alternative method of augmenting reten-tion is to use rare earth magnets located inthe overdenture with the keepers incorporatedinto the abutment teeth (Fig. 3.5). These de-vices are less expensive than many precision at-tachments and provide effective retention. Asa magnet applies less lateral force to the abut-ment tooth than does a precision attachment, it
Figure 3.5 Keepers have been placed in the abut-ment teeth. The rare earth magnets are located withinthe overdenture.
can be used in situations where more advancedperiodontal destruction has occurred.
The disadvantage of early designs of rareearth magnets is that they corroded in the oralenvironment. There has been significant im-provement in this regard over the last decadewith magnets now encased in a relatively inertcapsule of titanium or stainless steel. In spite ofthis, corrosion can still be an occasional prob-lem with some magnets when the oral fluidsdiffuse through the epoxy seal of the capsule(Riley et al. 1999). Longevity is improved if themagnet is enclosed in a laser-welded stainlesssteel casing (Thean et al. 2001).
Psychological benefits
The complete, irrevocable loss of all teeth canbe a serious blow to a patient’s morale as itsignals, perhaps, that a major milestone in lifehas been reached. The retention of remnants ofthe natural dentition in the form of overden-ture abutments can soften the blow and allowa period of mental adjustment before the eden-tulous state is reached. The patient’s attitude totreatment and to conventional complete den-tures may thus be more favourable. This par-ticular benefit is not, in the authors’ opinion, acommon one. However, when it does arise, itcan be of considerable value to both patient andclinician.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 39
Disadvantages of tooth-supportedoverdentures
Root canal therapy
The preservation of roots as overdenture abut-ments usually necessitates endodontic treat-ment, thus extending the course of treatmentand increasing its cost. The technical difficultyof achieving a satisfactory root filling may beincreased because of partial obliteration of theroot canal by secondary dentine due to ageingor in response to excessive loss of tooth sub-stance. On the other hand, the same obliterationof the root canal may mean that the tooth maybe shortened sufficiently without the need forendodontic treatment.
Caries
Covering root faces with an overdenture in-creases the risk of carious attack on these sur-faces. The conclusions from a number of sur-veys reveal a caries prevalence ranging from15% to 36%. Therefore, preventive measuresare of great importance and comprise thefollowing:
� Oral and denture hygiene instruction.� Dietary advice.� Careful smoothing and polishing of the
domed root face to facilitate plaque removal.� Sealing the root canal coronally with a glass-
ionomer cement, as this material releasesfluoride.
� Regular topical applications of fluoride us-ing a fluoride varnish in the surgery and afluoride toothpaste at home.
� Use of dentine bonding agents (Fenton1998).
Periodontal disease
Covering the gum margins of abutment teethwith an overdenture has the potential for ini-tiating periodontal disease or aggravating anyexisting disease process. There have been re-ports of gingival bleeding around all abutment
teeth after 4 years and of obvious inflammationaround 12% of abutment teeth after 3 years. Thereduced number of teeth and their simple shap-ing may well mean that patients who found ad-equate home care a significant challenge maynow be able to accomplish sufficient plaque re-moval to reduce the risk of these problems.
Budtz-Jørgensen (1995) has demonstratedthat it is possible to maintain overdenture abut-ment teeth in older people who initially hadpoor periodontal and caries status by initial in-tensive treatment followed by four to five recallvisits per year.
Technique for tooth-supportedoverdentures
The summary that follows outlines a simpletechnique appropriate for the construction of acomplete overdenture.
Selection of abutments
As the mandibular residual ridge providesa less favourable foundation for a completedenture than the maxillary ridge and hardpalate, the indications for retaining roots asoverdenture abutments are greater in the lowerjaw. Although any tooth amenable to root canaltherapy may be retained as an overdentureabutment, single-rooted teeth are preferable onthe grounds of simplicity. Teeth such as the ca-nines, lower first premolars and upper centralincisors are thus particularly suitable. Lowerincisors and upper lateral incisors are not idealabutments because of their smaller periodontalligament area. Extraction of these teeth may,in fact, facilitate the task of cleaning adjacentabutments. Such extractions will usually becarried out at the appointment for fitting theoverdenture.
Clinical and laboratory stages
After endodontic treatment of the abutmentteeth has been carried out, the production of an

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
40 Prosthetic Treatment of the Edentulous Patient
overdenture follows the stages of conventionalpartial denture technique until the try-in stagehas been completed.
Modifying the castThe working cast is then modified by cuttingoff the crowns of the chosen abutment teethand under-trimming the root faces to producea domed preparation slightly larger and moresupragingival than is intended for the actualroot faces. It is useful to measure the heightfrom the top of the dome to a fixed point at thegingival margin with dividers and to note thismeasurement in order to guide the preparationof the natural tooth at the next clinical visit. Thecrowns of any teeth to be extracted at the timeof fitting the denture are also cut off the castand the gingival contour modified to simulateany collapse likely to occur following tooth ex-traction. The denture is then processed in thenormal way.
Fitting the dentureAt the appointment for fitting the denture,the crowns of the teeth selected as overden-ture abutments are removed and the root facesare domed, using the measurement made onthe working cast. The openings of the rootcanals are then sealed with glass-ionomer ce-ment or possibly amalgam, although the lat-ter material does not have the advantage ofcaries inhibition resulting from fluoride release.The other teeth are extracted and the immediateoverdenture is fitted.
Relining the dentureWhen the denture is checked at the next ap-pointment, the restorations and the root facesare polished and fluoride varnish is applied tothe dentine. An accurate fit of the denture tothe root faces is achieved by using a cold-curingdenture relining material based on acrylic resinwithin the recesses in the impression surfacecorresponding to the roots. Correct seating ofthe denture under occlusal pressure is facili-tated by drilling a hole from each of the recesses
Excess acrylic resin
Vent
Glass-ionomer restoration
Figure 3.6 Cross-section of overdenture and abut-ment tooth showing correction of fit by addition ofcold-curing acrylic resin.
to the polished surface to allow escape of anyexcess acrylic resin (Fig. 3.6).
Maintenance of tooth-supportedoverdentures
It is important to arrange a programme of re-view appointments to allow proper mainte-nance of the overdenture. This will involvemaintaining oral and denture hygiene and re-inforcing when necessary. Regular applicationsof topical fluoride should be made to the abut-ments. Temporary or permanent relining proce-dures will be required to compensate for alveo-lar resorption in regions where extractions werecarried out at the time of fitting the denture.If caries of the root faces poses a problem inspite of topical fluoride applications, gold cop-ings can be considered as a secondary proce-dure. If the patient is unable to control the den-ture as well as had been anticipated, magnets

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 41
or stud attachments may be placed on the abut-ments to enhance retention. In one long-termstudy it was reported that treatment needs weregreatest after 6 years. By that time, 36% of loweroverdentures had lost stability but as few as 6%of upper and lower dentures had to be remade(Ettinger & Jakobsen 1997).
Implant-supportedoverdenturesOsseointegrated implant-supported overden-tures are not generally an appropriate optionfor the short-term transition from the dentatestate to that of complete denture wearing. Nev-ertheless, it is relevant to consider osseointe-grated implants in this section of the book asboth tooth roots and implants provide similarpotential benefits for the enhanced support andretention of complete dentures.
Development of osseointegratedimplants
Osseointegrated implants were developed inthe second part of the twentieth century byProfessor Per-Ingvar Branemark. He was work-ing in the early 1950s, using titanium-viewingchambers to examine blood flow in the boneof rabbits. When it became time to remove thechambers at the end of the experiment, the bonewas firmly attached to the chamber. The phe-nomenon was termed osseointegration and de-scribes the direct connection between vital boneand the implant without the presence of inter-vening connective tissue. It was later defined as‘direct structural and functional connection be-tween ordered, living bone and the surface of aload carrying implant’.
Design
The vast majority of dental implants placed to-day are osseointegrated root-form titanium im-plants. These implants come in a wide variety
Figure 3.7 Examples of different types of implantdesign.
of designs (Fig. 3.7), but they all have certainbasic components in common. These are:
� A submerged portion (usually referred to asthe fixture) to which the bone integrates.
� A supra-bony portion that emerges throughthe mucosa into the mouth (the transmu-cosal element) to which various attachmentscan be added to support and retain the sub-sequent prosthesis (Fig. 3.8).
Success rates
Osseointegrated implants provide a successfuland predictable way of replacing missing teethwhich achieves a long-term survival, especiallyin the anterior part of the mandible where it isin excess of 98% after 20 years (Ekelund et al.2003). Even so, the complications associatedwith such long-term restorations are probablygreater than for the restoration of natural teeth(Pjetursson et al. 2007). The success of implanttreatment has been followed by an explosionin the number of implant manufacturers eachwith their own specific designs.
Through the decades of development of os-seointegrated prostheses for edentulous pa-tients, the fixed restoration has been regardedas the ‘gold standard of treatment’. The re-movable option tended to be considered only

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
42 Prosthetic Treatment of the Edentulous Patient
Attachment
Transmucosalelement
Fixture
Figure 3.8 The three component parts of an im-plant.
where there were anatomical or financial re-straints that excluded the fixed option. Never-theless, work by various research groups hasconvincingly shown that even the provisionof just two implants placed in the mandiblecan provide marked improvement both in pa-tient satisfaction with a removable prosthesisand in oral health-related quality of life. Thesedata have been summarised by Thomason et al.(2007).
There is an increasing body of researchwhich provides support for the argument thatan implant-supported mandibular overdentureshould be offered as the preferred treatmentoption to edentulous patients. This view hasgained momentum and is the key outcomestatement from both the McGill Consensus
statement (Feine et al. 2002) and the York Con-sensus statement (Thomason et al. 2009).
Barriers to implant treatment
It is difficult to overestimate the potential forimproved treatment that dental implants offer.This potential has only been partially fulfilledhowever because of the low rates of uptake ona global basis, the greatest barriers being thoseof cost and training. The number of edentulouspatients worldwide who have received implanttreatment is probably less than 1% (Carlsson2009) and for the majority of the world’s eden-tulous patients the cost will continue to be aninsurmountable barrier for the foreseeable fu-ture. Interestingly, even when offered implants‘free of charge’, a significant proportion of pa-tients have chosen to refuse the option for avariety of reasons (Walton & MacEntee 2005;Allen et al. 2006).
Implant placement
Traditionally, implants are inserted as a two-stage procedure. The first stage involves plac-ing the implant, or fixture, within the alveolarand basal bone. A site for the implant is pre-pared in the bone with sets of graded drillsso that it carefully matches the dimensions ofthe fixture. Great care must be taken to avoidincreasing the temperature of the bone to apoint that would cause necrosis and so preventosseointegration. The fixtures are then placedinto the prepared site and covered with thesoft tissues. After a period for osseointegration,which is typically 3 months in the mandible and6 months in the maxilla, the fixture is surgicallyexposed and the second stage or transmucosalelement is attached to the fixture. After a shorthealing period the implants are restored witha fixed or removable prosthesis. More recently,the usual practice for simple overdentures hasbeen to use a one-stage rather than a two-stageprocedure and to attach the transmucosal ele-ment at the time of implant placement (Fig. 3.9).

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 43
Figure 3.9 Non-submerged osseointegrated im-plants inserted as a single-stage procedure for the sup-port and retention of a mandibular overdenture.
An attachment is subsequently added to theimplant to provide support and retention forthe overdenture (Fig. 3.10). There is a wide va-riety of attachments available and the numberof designs continues to increase (Fig. 3.11). Theattachments on each implant can be kept sepa-rate, or the implants can be linked together witha bar (Figs. 3.12a and 3.12b).
Impressions
It is critical for implant-supported denturesthat the position of the implant abutments isrecorded with great precision. This usually in-
Figure 3.10 The attachment driver (patient’s right)is used to carry the abutment to the fixture and secureit in place as seen on the patient’s left.
Figure 3.11 The photographs show two differenttypes of abutments widely used for implant-supportedmandibular overdentures.
volves some form of transfer impression whichallows abutment-analogues (which are repli-cas of the abutment, or ‘dummies’) to be in-corporated into the stone models on whichthe dentures will be constructed (Fig. 3.15).This can be achieved by taking an impres-sion in a heavy bodied elastic impression mate-rial which includes the attachments on the im-plants. Then, when the impression is removedfrom the mouth, the abutment analogues can beinserted into the impressions of the attachmentsbefore the stone model is poured. Alternatively,transfer copings can be placed on the implantsin the mouth (Fig. 3.13) which are then ‘pickedup’ in the impression. Abutment replicas areplaced onto the copings in the impression(Fig. 3.14) so that they will be incorporatedinto the master model (Fig. 3.15) on which the

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
44 Prosthetic Treatment of the Edentulous Patient
a
b
Figure 3.12 (a) shows two implants linked with agold bar. (b) shows a retainer within the denture basewhich clips onto the bar.
denture is constructed allowing accurate posi-tioning of the retainer within the denture base(Fig. 3.16).
Training
Whilst the placement of implants remains theprovince of those with appropriate additionaltraining, the actual construction of overden-tures supported by two implants is a straight-forward procedure comparable to providingdentures supported by two tooth roots. Initialreports suggest that newly qualified clinicianswith little implant experience can achieve veryfavourable results when restoring implantswith overdentures (Esfandiari et al. 2006). As
Figure 3.13 Two transfer copings have beenplaced on the implant abutments prior to impression-taking. The extension of the copings occlusally will beenveloped by the impression material so that when theimpression is removed from the mouth the copings willbe removed with it.
a result, there is an inevitable pressure tobring an understanding of the placementof implants and even clinical experience ofthe restoration and management of implantprostheses into the undergraduate curriculum(McAndrew 2010).
Immediate denturesIf the provision of overdentures is not possible,then providing a patient with a conventional
Figure 3.14 Abutment replicas have been insertedinto transfer copings “picked up” in the impression ofthe denture bearing area.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 45
Figure 3.15 Abutment replicas incorporated intothe master model on which the denture will be con-structed.
immediate denture is the most effective way ofmaking the transition from the natural to theartificial dentition (Jonkman et al. 1997). It wasonce said that this method was the appropri-ate treatment for those in the professions wherethey could not do without teeth for any lengthof time. The typical list would usually includevicars, doctors and business people – dentistswere never mentioned! Thankfully, times andoutlooks have changed and today the preser-vation of appearance is an almost universalwish.
Figure 3.16 Retainers located accurately within thedenture base.
Advantages of immediatedentures
Related to the patient� Maintenance of dental appearance and facial
contour.� Minimising disturbances of mastication and
speech.� Facilitating adaptation to dentures. Difficul-
ties with adaptation occur more commonlyif the patient experiences an edentulous pe-riod of several months before dentures arefitted.
� Maintenance of the patient’s physical andmental well-being.
� Provides a ‘protective bandage’ for the sur-gically traumatised area.
Related to the clinician� Transfer of the jaw relationship. If the jaw re-
lationship determined by the occlusion ofthe remaining natural teeth is acceptable inboth horizontal and vertical planes, it can betransferred to the immediate dentures withreasonable accuracy. This obviates the needfor the inspired guesswork of rest positionestimation that is required if the patient isedentulous.
� Achieving a good appearance. The form andarrangement of the natural teeth can bereproduced in the immediate denture ifthe patient likes their appearance. Whenthe appearance of the natural teeth is poor,or when their positions are likely to causeinstability of the denture, planned im-provements relative to the existing naturalanterior tooth arrangement can be carriedout. However, when such changes are an-ticipated, it is important to avoid radicalchanges in incisal relationship which mayresult in the undesirable consequences, asdescribed in Chapter 12.
� Reduction in ridge resorption. It has beensuggested that the rate of ridge resorption

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
46 Prosthetic Treatment of the Edentulous Patient
following extractions is less if immediatedentures are worn than if no dentures are fit-ted. However, the evidence for this is incon-clusive.
� Haemostasis. An immediate denture coversthe sockets as a “protective bandage” andthus encourages haemostasis. It also sup-ports and protects the clot during the im-mediate post-extraction period, reducing thechance of its mechanical dislodgement, forexample, by food particles.
Disadvantages of immediatedentures
It is extremely important for the clinician tofully explain to the patient the following limita-tions of immediate dentures (Seals et al. 1996).Treatment should not normally be started un-less the patient fully appreciates and acceptsthese limitations. Failure to achieve such an un-derstanding is a common cause of complaint bypatients against clinicians and can also result infailure of treatment:
� Inability to complete a comprehensive trial stage.As the trial stage is carried out while theremaining natural teeth are still present thetry-in prosthesis consists of a partial den-ture restoring the existing edentulous spacesonly. Therefore, artificial teeth that will even-tually replace the natural teeth cannot beassessed. This is a particular disadvantagewhen anterior teeth are being replaced be-cause neither the patient nor the clinician canmake a full evaluation of the appearance ofthe dentures in situ.
� Increased maintenance. A number of visits arerequired after extraction of the teeth to allowfor maintenance of the immediate dentures.Such maintenance may include:� relining with soft or hard materials;� occlusal adjustment;� addition of a labial flange to an open-face
denture. If the dentures are not properlymaintained, it usually results in exten-
sive destruction of the denture-bearingtissues.
� Short service life. An immediate denture willnot normally last as long as a conventionalcomplete denture. After 6–12 months of theadjustments outlined above, together withmorphological changes in the oral environ-ment, an immediate denture will commonlyneed replacing. Therefore, patients are likelyto have to face the financial and time com-mitments associated with the provision ofa replacement denture sooner than theywould normally expect.
In spite of the disadvantages listed above, theadvantages of conventional immediate den-tures are normally overwhelming comparedwith tooth extraction and delayed denture fab-rication after healing. This form of treatmentshould therefore be offered to the vast majorityof patients for whom the transition from nat-ural to artificial dentition must be made andwhere overdentures are not a possibility. Withthis caveat, there are relatively few circum-stances in which the immediate denture is con-traindicated.
Types of immediate completedenture
There are basically two types of immediatecomplete denture (Fig. 3.17).
FlangedThis design can be subdivided into:
� Complete flange – labial flange fully ex-tended to the depth of the sulcus.
� Partial flange – labial flange usually finishedwith the border extended about 1 mm be-yond the maximum bulbosity of the ridge.
Open-facedThere is no labial flange and the anterior teethextend a few millimetres into the labial aspectof the sockets of their natural predecessors.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 47
a b c
Figure 3.17 Types of immediatedenture: (a) complete flange; (b) par-tial flange; (c) open face.
Comparison of flanged and open-facedentures
Appearance� The appearance of a flanged denture does
not alter after fitting whereas the appearanceof an open-face denture, although good ini-tially, can deteriorate rapidly as resorptioncreates a gap between the necks of the teethand the ridge.
� The flange design allows considerable free-dom in positioning the anterior teeth for op-timum effect, whereas the anterior teeth onthe open-face denture have to be positionedwith their necks in the sockets of their natu-ral predecessors.
StabilityA flange on an upper denture creates a moreeffective border seal, and therefore better reten-tion, than is achieved with an open-face design.In the lower denture a border seal is not nor-mally so significant. However, stability is of thegreatest importance and this is improved by alabial flange because it helps to resist posteriordisplacement of the denture.
Strength� The presence of a labial flange produces a
stronger denture, which is less likely to frac-ture as a result of accidental impacts or highocclusal loads.
� A labial flange will also make the denturestiffer so that the likelihood of a midlinefatigue fracture caused by repeated flexingacross the midline is reduced.
Maintenance� As the bone resorbs following extraction of
the teeth, the immediate denture becomesloose and a reline is required. The presenceof a labial flange makes it easier to add eithera short-term soft lining material or a cold-curing polybutylmethacrylate relining mate-rial as a chairside procedure.
� As the colour of some of the chairside re-line materials is not always ideal, they maybe visible and unsightly when used with anopen-face denture, but discreetly concealedby a flange.
Haemostasis� The flanged denture covers the clots com-
pletely and protects them more effectivelythan does an open-face denture.
� The flanged denture also exerts pressureon both lingual and labial gingivae, reduc-ing the likelihood of post-extraction haem-orrhage.
Remodeling of the ridgeThere is always the danger that the patientwill fail to attend for a maintenance appoint-ment. The consequent wearing of an ill-fitting

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
48 Prosthetic Treatment of the Edentulous Patient
Figure 3.18 Tissue damage produced by an open-face lower immediate denture.
denture can, if it is open-faced, produce a scal-loped ridge in the region of the extracted teeth(Fig. 3.18). This danger is avoided in the caseof a flanged denture, which also has the advan-tage of distributing the functional loads morefavourably to the underlying ridge, thus min-imising bone resorption. For this reason alone,the authors would discourage the use of anopen-faced denture in the upper arch and donot advocate its use in the lower arch at all.
Tolerance of replacement denturesA significant clinical problem can be the diffi-culty that patients commonly experience in ac-cepting a labial flange on a replacement denture
Path of insertion
Path of insertion
a b
Figure 3.19 Diagram of aflanged immediate denture showingthe effect of the path of insertionon the placement of the flange:(a) path of insertion parallel tothe labial surface of the ridge –flange position favourable; (b) pathof insertion at right angles to theocclusal plane – flange positionunfavourable.
when they have got used to an open-face imme-diate denture. Although a correctly designedflange only replaces bone that has resorbed, itspresence in the richly innervated oral cavity fre-quently promotes a complaint of ‘fullness’ ofthe upper lip. If a flanged denture has beenworn from the very beginning, this problemdoes not occur.
For the reasons listed above, the flange de-sign is usually preferable; however, it is essen-tial that the flange is kept thin and positionedcorrectly against the labial surface of the ridge,otherwise over-distension of the lip will resultin poor facial appearance. In this context, selec-tion of the correct path of insertion of the den-ture is essential (Fig. 3.19).
Where the ridge morphology produces adeeply undercut area, it may not be possible tofit a full labial flange unless there is surgical re-duction of that undercut. Under such circum-stances, a partial flange may be acceptable un-less the patient has a smile line high enough toreveal the edge of the flange.
An outline of relevant clinical andtechnical procedures
The essential steps in the construction of im-mediate dentures follow the same sequence asthose for conventional partial dentures until

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 49
after the try-in stage. The subsequent conver-sion of the try-in to the complete denture re-quires modification of the cast in the laboratory.
Impressions for immediate dentures can beproblematic if the remaining teeth are particu-larly mobile as a result of terminal periodon-tal disease. Under such circumstances, a con-ventional alginate impression can even act asan instrument of extraction with some or all ofthe remaining teeth coming out in the impres-sion. The risk of such an undesirable and poten-tially upsetting accident can be minimised byeither:
� Loosening the ‘grip’ of the impression on theloose teeth. One way that this can be achievedif there are several teeth adjacent to eachother is by moulding soft red carding waxinto the sub-contact point spaces and aroundthe necks of the teeth so that the alginate isprevented from locking into the undercuts.Solitary teeth can be protected by placing aloose-fitting copper band over them beforetaking the impression.
� Temporarily strengthening the attachment of thevulnerable teeth. A stronger attachment ofthe loose teeth can be produced by splint-ing them to adjacent teeth with compositeresin.
The nature of the modification depends uponwhether the denture is to be flanged or open-face. The extent of the adjustment will be in-fluenced by clinical assessment of the bone lev-els around the teeth to be extracted and on theamount of surgical reshaping of the ridge that isrequired. Therefore, as a general rule it is highlydesirable for the cast to be modified by the clin-ician rather than by the dental technician.
Flanged dentures
Extraction without alveolar surgeryIf the arrangement of the natural anterior teethis to be reproduced in the denture, a record of
Figure 3.20 Position of the anterior teeth recordedby a silicone putty index.
their position must be obtained in one of the fol-lowing ways:
(i) Produce a labial index of the natural teethbefore they are cut off the cast. The indexcan be produced quite simply by mould-ing silicone putty against the labial sur-face of the teeth and ridge on the cast(Fig. 3.20). The artificial teeth are then setinto the index while it is held against thecast.
(ii) Remove teeth singly from the cast and im-mediately wax an artificial tooth into po-sition so that the adjacent teeth serve asa guide to the position of the artificial re-placement.
(iii) Scribe guidelines on the cast recording theposition, angulation and incisal level of thenatural teeth (Fig. 3.21).
Once the artificial teeth have been positioned,the flange is added in wax before the denture isprocessed.
Alveolotomy following interseptalalveolectomyThis procedure is intended to eliminate mod-erate labial alveolar undercuts so that a flangeddenture can be used without that flange distort-ing the upper lip unduly.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
50 Prosthetic Treatment of the Edentulous Patient
Figure 3.21 Long axes of the teeth marked on thecast to assist in placing the artificial teeth in similarpositions. The location of incisal edges can be deter-mined by direct measurement with dividers.
The denture is constructed on a working castwhich is trimmed to the anticipated contour ofthe ridge after surgery as follows:
(i) The gingival margins are marked and theteeth removed.
(ii) Guidelines are drawn on the cast (Fig.3.22).� A line is drawn on the crest of the ridge,
passing across the centre of the soc-kets of the incisors and through thejunction of the labial third and palataltwo-thirds of the canine sockets.
Figure 3.22 Alveolotomy following interseptal alve-olectomy: lines drawn on the cast to guide model trim-ming (see text for details).
� A second line is drawn horizontallyalong the labial aspect of the ridge; it isplaced approximately two-thirds downthe length of the shortest root, usuallythe lateral incisor, and is continuousaround all the teeth at that level.
(iii) All that part of the cast contained withinthese two lines is trimmed away and theedges are rounded over.
(iv) A clear acrylic template is processed on aduplicate of this cast and is used as a guideto control the amount of bone removal atoperation.
The surgical procedure involves the following:
(i) Extraction of the teeth.(ii) Removal of the associated interseptal
bone.(iii) Collapse of the labial cortical plate of bone
and mucoperiostium, back into the result-ing ‘gutter’.
(iv) Insertion of the clear acrylic template tocheck if bone removal has been sufficient.Blanching of the mucosa is clearly seen be-neath the template in any area where thereis excessive pressure.
(v) Further bone removal, if necessary, untilre-insertion of the template ceases to causeblanching.
(vi) Suturing of the sockets and insertion of theimmediate denture.
AlveolectomyThe most common indication for an alveolec-tomy in association with the fitting of imme-diate dentures is the reduction of a prominentpremaxilla to allow a more favourable placingof anterior teeth on the dentures.
A clear acrylic template is processed on a du-plicate of the working cast trimmed to producethe desired ridge form. The template is used asa guide to bone removal during surgery in thesame way as described for an alveolotomy fol-lowing interseptal alveolectomy.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 51
Open-face dentures
The purpose of extending the labial aspectof the necks of the denture teeth into thesockets, just enough to compensate for thegingival retraction that occurs immediatelyafter extractions, is to maintain an acceptableappearance in the immediate post-extractionperiod. Without this, an unsightly gap wouldsoon appear between tooth and mucosa. Theamount of gingival retraction will depend onthe degree of pocketing and bone loss that ispresent around the natural teeth. These aspectsshould therefore be assessed before decidingwhether the necks of the denture teeth shouldbe placed sub-gingivally to a depth of 2 mm, orwhether a greater anticipated gingival collapseindicates that they should be placed moredeeply. When this decision has been taken,the teeth are cut off the cast and a recess of therequired depth is cut in the labial aspects ofthe sockets. No recessing of the palatal aspectsof the sockets is undertaken. The artificialteeth are carefully positioned in the preparedrecesses and the denture is processed.
Contraindications to immediatedentures
Patients at risk from a bacteraemia
Some clinicians believe that movement of animmediate denture can disturb the clots andsurrounding tissues sufficiently to precipitate abacteraemia. They are therefore opposed to theprovision of immediate dentures for patientswhere such a bacteraemia may be perceived asa danger. Nevertheless, it can be argued that thepotential for clot disturbance in the absence ofa baseplate covering the wounds may be evengreater.
Patients with a genuine history ofpost-extraction haemorrhage
As multiple extractions of anterior teeth aregenerally required when immediate dentures
are fitted, such treatment is inappropriate whenthere is a proven history of post-extractionhaemorrhage that has been difficult to control.A more cautious approach is indicated, involv-ing the extraction of a few teeth at a time fol-lowed by suturing the sockets. Dentures arethen fitted at a later date when the initial heal-ing is complete.
The presence of gross oral sepsis
Although it is possible to provide immediatedentures for a neglected mouth, it is generallyunwise to do so. The anterior teeth are oftenunsightly because of surface deposits, caries,gingival inflammation or recession; therefore,their retention for aesthetic reasons is unjus-tified. Furthermore, a patient who has ne-glected the mouth in this way may be less con-cerned about appearance anyway. The benefitsof an immediate denture are therefore reducedsignificantly.
Clearance of teeth withoutimmediate provision ofdenturesWhen a decision is taken to extract the remain-ing teeth before denture construction, it is acommon practice to allow a period of severalmonths for healing and initial alveolar mod-elling. This delay before taking impressions willproduce more stable supporting areas for thedentures, although resorption will continue in-definitely but at a slower rate. The main ad-vantage of this method, that the dentures retaintheir fit for a longer period, is outweighed bythe following disadvantages:
� Loss of masticatory function and appearanceduring the healing period.
� The undesirable mental and physical effectsthat the absence of teeth creates on a patient.
� Tongue and cheeks may invade the futuredenture space, making adaptation to subse-quent dentures more difficult.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
52 Prosthetic Treatment of the Edentulous Patient
� Difficulty in assessing vertical and horizon-tal jaw relationships when constructing newdentures.
� The difficulty in restoring appearance if allinformation on the natural dentition hasbeen lost.
It is surprising, in view of the disadvantageslisted above, that the more efficient alterna-tive method of making the transition fromthe natural to the artificial dentition via im-mediate dentures is not used routinely unlessdefinite contraindications exist. The authorswould strongly advocate that, where possible,long-term planning should encompass transi-tion through partial dentures and then over-dentures, thus avoiding the very abrupt “leap”from the dentate to the edentulous state. Anadditional benefit of this step-by-step approachis that it provides flexibility in the long-termtreatment plan, allowing it to be modified ap-propriately in response to changes in clinicalcircumstances.
PostscriptA well-managed transition from what remainsof the natural dentition to the totally artificialdentition carries a good level of success. Withregard to the more problematic lower denture,studies have shown that, after 1 year, 85% of pa-tients were satisfied both with complete imme-diate conventional dentures and with completeimmediate overdentures (Jonkman et al. 1995;van Wass et al. 1997). This result was the con-sequence of careful clinical and technical pro-cedures and a considerable amount of interimcare.
Implant supported overdentures, as an alter-native to conventional complete dentures, arebecoming much more widely accepted as theynow provide a realistic option for edentulouspatients (Thomason et al. 2009). The availabledata convincingly show that patients are moresatisfied with implant-supported mandibularoverdentures than conventional dentures – typ-
ically by some 30%. There is also strong ev-idence that oral health-related quality of lifecan be significantly improved by this treatment(Thomason et al. 2007). However, whilst highsatisfaction ratings have been reported for max-illary implant prostheses, the overall ratingsgiven to them have not been shown to be anygreater than for maxillary conventional den-tures. Despite the positive improvements pro-vided by mandibular implant overdentures theoverall uptake of this treatment remains low,even in affluent countries and in the UK in par-ticular (see above and Chapter 1). For manyyears to come, the most common treatmentalternative for edentulous individuals world-wide will be conventional complete dentures(Carlsson 2006). This is in no small part dueto the additional expense involved in implanttreatment – even though this is relatively mod-est for two-implant overdentures, particularlywhen spread over the life of the patient (Hey-decke et al. 2005). The relatively slow uptakeof implant treatment is also a consequence ofa need for further training of the dental work-force, both for implant placement and for reha-bilitation. Fortunately, for the latter, the prin-ciples of implant-supported complete dentureconstruction and conventional complete den-ture construction are similar. Therefore, thosewell trained in conventional denture provisionare also well prepared for the provision of im-plant supported complete dentures.
References and additionalreadingAllen, P.F., Thomason, J.M., Jepson, N.J., Nohl, F.,
Smith, D.G. & Ellis, J. (2006) A randomized con-trolled trial of implant-retained mandibular over-dentures. Journal of Dental Research, 85, 547–51.
Basker, R.M., Harrison, A., Ralph, J.P. & Watson, C.J.(1993) Overdentures in general dental practice, 3rdedn. British Dental Association, London.
Beck, C.B., Bates, J.F., Basker, R.M., Gutteridge, D.L.& Harrison, A. (1993) A survey of the dissatisfieddenture patient. European Journal of Prosthodonticsand Restorative Dentistry, 2, 73–8.

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
Transition from the Natural to the Artificial Dentition 53
Budtz-Jørgensen, E. (1995) Prognosis of overdentureabutments in elderly patients with controlled oralhygiene. A 5 year study. Journal of Oral Rehabilita-tion, 22, 3–8.
Carlsson, G.E. (2006) Facts and fallacies: an evi-dence base for complete dentures. Dental Update,33, 134–42.
Carlsson, G.E. (2009) Critical review of some dogmasin prosthodontics. Journal of Prosthodontic Research,53, 3–10.
Ekelund, J.A., Lindquist, L.W., Carlsson, G.E. & Jemt,T. (2003) Implant treatment in the edentulousmandible: a prospective study on Branemark sys-tem implants over more than 20 years. InternationalJournal of Prosthodontics, 16, 602–8.
Esfandiari, S., Lund, J.P., Thomason, J.M., Dufresne,E., Kobayashi, T., Dubois, M. & Feine, J.S. (2006)Can general dentists produce successful implantoverdentures with minimal training? Journal ofDentistry, 34, 796–801.
Ettinger, R.L. & Jakobsen, J. (1997) Denture treatmentneeds of an overdenture population. InternationalJournal of Prosthodontics, 10, 355–65.
Feine, J.S. & Carlsson, G.E. (eds) (2003) Implant Over-dentures: The Standard of Care for Edentulous Patients.Quintessence Publishing, Chicago.
Feine, J.S., Carlsson, G.E., Awad, M.A., Chehade, A.,Duncan, W.J., Gizani, S., Head, T., Heydecke, G.,Lund, J.P., MacEntee, M., Mericske-Stern, R., Mo-jon, P., Morais, J.A., Naert, I., Payne, A.G., Pen-rod, J., Stoker, G.T., Tawse-Smith, A., Taylor, T.D.,Thomason, J.M., Thomson, W.M. & Wismeijer, D.(2002) The McGill consensus statement on over-dentures. Mandibular two-implant overdenturesas first choice standard of care for edentulous pa-tients. Journal of Prosthetic Dentistry, 88, 123–4.
Fenton, A.H. (1998) The decade of overdentures:1970–1980. Journal of Prosthetic Dentistry, 79, 31–6.
Heydecke, G., Penrod, J.R., Takanashi, Y., Lund,J.P., Feine, J.S. & Thomason, J.M. (2005) Cost-effectiveness of mandibular two-implant overden-tures and conventional dentures in the edentulouselderly. Journal of Dental Research 84, 794–9.
Johnson, K. (1977) A study of the dimensionalchanges occurring in the maxilla following open-face immediate denture treatment. Australian Den-tal Journal, 22, 451–4.
Johnson, K. (1978) Immediate denture treatment forpatients with class II malocclusions. AustralianDental Journal, 23, 383–8.
Jonkman, R.E., van Waas, M.A., van’t Hof, M.A.& Kalk, W. (1997) An analysis of satisfaction
with complete immediate (over)dentures. Journal ofDentistry, 25, 107–11.
Jonkman, R.E.G., van Wass, M.A.J. & Kalk, W. (1995)Satisfaction with complete immediate denturesand complete immediate overdentures. A 1 yearsurvey. Journal of Oral Rehabilitation, 22, 791–6.
McAndrew, R., Ellis, J., Lynch, C.D. & Thomason, M.(2010) Embedding implants in undergraduate den-tal education. British Dental Journal 2010, 208, 9–10.
Murphy, W.M., Huggett, R., Handley, R.W. & Brooks,S.G. (1986) Rigid cold curing systems for direct usein the oral cavity. British Dental Journal, 160, 391–4.
Mushimoto, E. (1981) The role in masseter muscleactivities of functionally elicited periodontal af-ferents from abutment teeth under overdentures.Journal of Oral Rehabilitation, 8, 441–55.
Nairn, R.I. & Cutress, T.W. (1967) Changes inmandibular position following removal of the re-maining teeth and insertion of immediate com-plete dentures. British Dental Journal, 122, 303–6.
Pjetursson, B.E., Braggur, U., Lang, N.P. & Zwalen,M. (2007) Comparison of survival and complica-tion rates of tooth-supported fixed dental prosthe-ses (FDPs) and implant-supported FDPs and singlecrowns (SCs). Clinical Oral Implants Research, 3, 97–113.
Preiskel, H.W. (1996) Overdentures Made Easy,Quintessence Publishing, London.
Quinn, D.M., Yemm, R., Ianetta, R.V., Lyon, F.F. &McTear, J. (1986) A practical form of pre-extractionrecords for construction of complete dentures.British Dental Journal, 160, 166–8.
Ralph, J.P. & Basker, R.M. (1989) The role of overden-tures in gerodontics. Dental Update, 16, 353–60.
Riley, M.A., Williams, A.J., Speight, J.D., Walmsley,A.D. & Harris, I.R. (1999) Investigations into thefailure of dental magnets. International Journal ofProsthodontics, 12, 249–54.
Seals, R.R., Kuebker, W.A. & Stewart K.L. (1996) Im-mediate complete dentures. Dental Clinics of NorthAmerica, 40, 151–67.
Tallgren, A., Lang, B.R., Walker, G.F. & Ash, M.M.(1980) Roentgen cephalometric analysis of ridgeresorption and changes in jaw and occlusal rela-tionships in immediate complete denture wearers.Journal of Oral Rehabilitation, 7, 77–94.
Thean, H.P.Y., Khor, S.K.L. & Loh, P.-L. (2001) Via-bility of magnetic denture retainers: a 3-year casereport. Quintessence International, 32, 517–20.
Thomason, J.M, Feine, J., Exley, C., Moynihan,P., Muller, F., Naert I., Ellis, J.S., Barclay, C.,Butterworth, C., Scott B., Lynch, C., Stewardson,

P1: JZP Trim: 246mm X 189mmc03 BLBK351-Basker January 4, 2011 7:43 Printer Name: Yet to Come
54 Prosthetic Treatment of the Edentulous Patient
D., Smith, P., Welfare, R., Hyde, P., McAndrew,R., Fenlon, M., Barclay, S. & Barker, D. (2009)Mandibular two implant-supported overdenturesas the first choice standard of care for edentulouspatients – the York Consensus Statement. BritishDental Journal, 207, 185–6.
Thomason, J.M., Heydecke, G., Feine, J.S. & Ellis, J.S.(2007) How do patients perceive the benefit of re-constructive dentistry with regard to oral health re-lated quality of life and patient satisfaction? Clini-cal Oral Implants Research, 18, 168–88.
Todd, J.E. & Lader, D. (1991) Adult Dental Health 1988United Kingdom. HMSO, London.
van Wass, M.E.J., Kalk, W., van Zetten, B.L. & vanOs, J.H. (1997) Treatment results with immediateoverdentures. An evaluation of 4.5 years. Journal ofProsthetic Dentistry, 76, 153–7.
Walker, A. & Cooper, I. (eds) (2000) Adult DentalHealth Survey Oral Health in the United Kingdom1998. The Stationery Office, London.
Walton, J.N. & MacEntee, M.I. (2005) Choosing or re-fusing oral implants: a prospective study of eden-tulous volunteers for a clinical trial. InternationalJournal of Prosthodontics, 18, 483–8.

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
4Stability of Dentures
A stable denture is one that moves little in re-lation to the underlying bone during function.It is perhaps surprising that what we now re-fer to as conventional dentures stay in placeat all, as they simply rest on mucous mem-brane and lie within a very active muscular en-vironment. They stay in place if the retentiveforces acting on the dentures exceed the dis-placing forces and the dentures have adequatesupport. Clearly, when complete dentures aresupported by implants, this balance betweenretentive and displacing forces is greatly tippedin favour of the denture staying in place. Forconventional complete dentures, this support isdetermined by the form and consistency of thedenture-bearing tissues and the accuracy of fitof the denture. The relationship of these factorsis summarised in Fig. 4.1.
Retentive forcesRetentive forces offer resistance to verticalmovement of a denture away from the underly-ing mucosa and act through the three surfaces
of a denture. These surfaces may be defined asfollows:
(1) Occlusal surface: that portion of the surfaceof a denture which makes contact or nearcontact with the corresponding surface ofthe opposing denture or dentition.
(2) Polished surface: that portion of the surfaceof a denture which extends in an occlusaldirection from the border of the dentureand which includes the palatal surface. It isthat part of the denture base which is usu-ally polished, includes the buccal and lin-gual surfaces of the teeth, and is in contactwith the lips, cheeks and tongue.
(3) Impression surface: that portion of the surfaceof a denture that had its shape determinedby the impression. It includes the bordersof the denture and extends to the polishedsurface.
The retentive forces that act upon each ofthese surfaces (Fig. 4.2) are of two main types,muscular forces and physical forces:
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
55

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
56 Prosthetic Treatment of the Edentulous Patient
+ = STABILITYRetentive
forcesDisplacing
forces> Adequatesupport Figure 4.1 Relationship of factors
contributing to denture stability.
1. Muscular forces. These forces are exerted bythe muscles of the lips, cheeks and tongueupon the polished surface of the dentureand by the muscles of mastication indirectlythrough the occlusal surface.
2. Physical forces. These rely on the presence ofan intact film of saliva between the dentureand mucosa. They act primarily between theimpression surface of the denture and theunderlying mucosa, and are to a large extentdependent on the maintenance of a seal be-tween the mucosa and the border regions ofthe denture and upon the accuracy of fit.
Muscular forces
Patients who wear their dentures successfullydo so primarily because they have learnt to con-trol them with the muscles of their lips, cheeksand tongue. This skill may be developed tosuch a high degree that a denture which ap-pears loose to the clinician may be perfectly sat-
isfactory from the patient’s point of view. Thereare even instances of patients who can eat with-out difficulty in spite of the fact that the denturehas broken into two or more pieces.
Cineradiographic studies show that manycomplete dentures move several millimetres inrelation to the underlying tissues during mas-tication. Consequently loss of physical reten-tion occurs frequently during mastication, asmovement of this extent breaks the border sealupon which physical retention depends. Mus-cular control is therefore extremely important,particularly in the case of the lower denturewhere the reduced area of the impression sur-face and the difficulty of obtaining a border sealreduce the influence of physical retention.
The successful muscular control of denturesdepends on two factors:
1. The design of the dentures.2. The ability of the patient to acquire the nec-
essary skill.
Occlusalsurface
Polishedsurface
Impressionsurface
Borderregions
Mucosa
Saliva
1
223
Figure 4.2 Retaining forces act-ing on a denture: (1) force ofthe muscles of mastication actingthrough the occlusal surface; (2)muscular forces of lips, cheeks andtongue acting through the polishedsurface; (3) physical forces actingthrough the impression surface.

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
Stability of Dentures 57
a b
Figure 4.3 Influence of soft tissueforces on dentures: (a) seating thedentures when the polished surfacesare correctly shaped; (b) displacingthe dentures when the polished sur-faces are incorrectly shaped.
Design of dentures
During mastication the muscles of the cheeks,lips and tongue control the bolus of food, moveit around the oral cavity and place it betweenthe occlusal surfaces of the teeth. In doing so,they press against the polished surfaces of thedentures. If these surfaces are correctly shapedwith the buccal and lingual surfaces converg-ing in an occlusal direction, this muscular forcewill seat the dentures on the underlying mu-cosa (Fig. 4.3a). In addition to this active mus-cular fixation of the dentures during function,there will be a certain amount of passive fix-ation when the muscles are at rest, as the re-laxed soft tissues ‘sit’ on the dentures, therebymaintaining them in position. Conversely anincorrectly shaped denture results in the mus-cular force dislodging that denture (Fig. 4.3b).In short, the muscles can either help or hinderdenture stability.
Patient’s skill
The patient’s ability to acquire the necessaryskills to control new dentures tends to be re-lated to biological age. In general, the older thepatient, the longer the learning period. In theextreme case, the older or senile patient may
not be able to acquire this skill at all and so newdentures may fail even though they are tech-nically satisfactory. It is for this reason that re-placement dentures for an older patient shouldnormally be constructed in such a way that thepatient’s skill in controlling the previous den-ture shapes can be transferred directly to the re-placements. This is achieved by copying the olddentures as closely as possible, ideally using atechnique such as that described in Chapter 8.
A specific example of the muscular con-trol of dentures is seen when a patient incises(Fig. 4.4). The forces tend to tip the upper den-ture, causing the posterior border to drop. Thismovement is normally resisted by the dorsumof the tongue, which presses against the den-ture and reseats it. Patients who complain ofdifficulty when incising with dentures, whichotherwise appear to be satisfactory, should beexamined very carefully to establish whetheror not tongue control is present. If it is not,it is essential for the clinician to draw the pa-tient’s attention to the problem and to instituteappropriate training (Basker & Watson 1991).This takes the form of explaining the centralrole of the tongue, lips and cheeks in control-ling the denture and giving specific advice –such as supporting the posterior border of theupper denture with the tongue when incising.

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
58 Prosthetic Treatment of the Edentulous Patient
Figure 4.4 As the patient incises,the upper denture is controlled bythe tongue pressing against the pos-terior border.
A reduction in displacing forces to bring themwithin the ability of the patient to control thedentures can be achieved by offering advice,for example, cutting food into smaller piecesbefore inserting them into the mouth, chewingon both sides of the dental arch simultaneouslyand starting with softer ‘easier’ foods beforeprogressing to more challenging morsels. Un-less purposeful muscular activity is learnt, re-placement dentures will fail to overcome thepatient’s complaint.
When dentures are first fitted, muscular con-trol takes some time to develop and is there-fore likely to be inefficient in the early stages.Thus, it is during this initial learning periodthat the physical forces of retention are partic-ularly important. The stronger these forces are,the smaller will be the demand on the patient’sskill in controlling the dentures. If the prospectsfor physical retention are poor, the resultinglooseness of the dentures may lead to their re-jection by the patient. In difficult cases it maybe helpful to advise the use of a denture fix-ative, as improved retention and stability willgive the patient confidence during the periodof adaptation (Grasso et al. 1994). There are realphysical limitations of conventional completedentures, particularly the lower denture, and as
such it is not surprising that some patients areunhappy with their function despite apparentlyseeming to have learned to control them well.As an example, such a patient may be awareof movements of the dentures during functionalthough these movements are undetectable tothe observer. This may lead to dissatisfactionand concerns for the patient which may ulti-mately impact on their interaction with otherpeople (Thomason et al. 2009).
As alveolar resorption progresses, the fit ofthe dentures deteriorates with a consequent re-duction in physical retention. However, thiswill not necessarily result in a reduction in theoverall retention, as there will have been a com-pensating increase in the level of muscular con-trol. Nevertheless, the fit may eventually be-come so poor that complete compensation is nolonger possible and movement of the denturesbegins to increase. The degree of denture mo-bility that elicits a complaint of looseness willvary considerably between individuals; somepatients are quite happy with dentures whichperform ‘acrobatics’ in the mouth while otherscomplain bitterly about dentures which hardlymove at all.
The topic of the patient’s skill is consideredfurther in Chapter 2.

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
Stability of Dentures 59
Physical forces
The contribution of physical forces to the reten-tion of a denture is heavily dependent upon thepresence of a continuous thin film of saliva be-tween denture and mucosa, which wets bothsurfaces. The forces of adhesion and cohesionplay a part in achieving this condition.
Adhesion
Adhesion is the force of attraction between dis-similar molecules such as saliva and acrylicresin or saliva and mucosa, which promotes thewetting of the denture and mucosal surfaces.
Cohesion
Cohesion is the force of attraction between likemolecules, which maintains the integrity of thesaliva film. These intermolecular forces of adhe-sion and cohesion may be thought of as form-ing a chain between the denture and the mu-cosa (Fig. 4.5).
Surface tension
Surface tension is the result of cohesive forcesacting at the surface of a fluid. It has been sug-gested that in the case of saliva these cohe-sive forces result in the formation of a concavemeniscus at the surface of the saliva in the bor-der region of the denture. When a fluid filmis bounded by a concave meniscus, the pres-sure within the fluid is less than that of the sur-rounding medium; thus, in the intra-oral situ-ation a pressure differential will exist betweenthe saliva film and the air (Fig. 4.6). The size ofthis pressure differential is inversely related tothe diameter of the meniscus, i.e. the closer thefit of the denture to the tissues the stronger theretentive force attributable to surface tension.This is discussed further in the section below,‘Obtaining optimum physical retention’.
Salivamolecules
Mucosa
Adhesion
Cohesion
Adhesion
Denture
Figure 4.5 The chain of intermolecular forces be-tween the denture and the mucosa contributing toretention.
Saliva film (pressure = Ps)
Air(pressure = Pa)
MeniscusRetentive force = Pa – Ps
Figure 4.6 Retention due to the pressure differentialbetween the saliva film and the air.

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
60 Prosthetic Treatment of the Edentulous Patient
a b
Figure 4.7 Relationship betweenthe width of the buccal channel andresistance to flow of saliva: (a) widechannel, rapid flow, poor retention;and (b) narrow channel, slow flow,good retention.
Viscosity
As a denture is pulled away from the tissues,saliva is drawn into the space being created be-neath the denture. A retentive force is gener-ated by a resistance to this flow of saliva, result-ing from the viscous properties of the saliva andthe dimensions of the channel through whichit flows (Fig. 4.7). It follows that the narrowerthe channel and the greater the viscosity of thesaliva, the more effective should be the reten-tion. This certainly holds true clinically for thedimensions of the channel, but it appears thatvery viscous saliva is associated with relativelypoor retention. It may be that retention is lowin this instance because the excessive viscos-ity of the saliva results in a thick and discon-tinuous film between the denture and the mu-cosa. Any discontinuities, such as air bubbles,in the saliva film reduce retention dramaticallybecause air flows infinitely more readily thansaliva and therefore offers very little resistanceto denture displacement.
It is important to appreciate that the wallsof the buccal channel through which the salivaflows differ from each other. The denture flangeis rigid while the soft tissues of the cheeks orlips are movable. If the denture is displaced,the pressure within the saliva film drops andthe mucosa is drawn tightly against the den-
ture surface so that the channel between thetwo becomes very narrow indeed. This causesa greatly increased resistance to the flow ofsaliva and a corresponding increase in retention(Fig. 4.8). Incidentally, this will also increase re-tention due to surface tension, because narrow-ing of the channel between denture and mu-cosa will reduce the diameter of the meniscus
Displacingforce
Figure 4.8 Drop in pressure of the saliva film be-neath the denture causing impaction of the buccal mu-cosa and greatly increased retention.

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
Stability of Dentures 61
and therefore increase the pressure differentialbetween the saliva film and air. If, however,the denture is constructed with flanges whichare too thin, resulting in a wide buccal channel(Fig. 4.7a), impaction of the buccal mucosa willnot occur, and saliva and air will be rapidlydrawn towards the impression surface as thedenture is displaced. Retention in this instancewill be poor.
The retentive mechanism resulting from theviscosity of the saliva and the valve-like actionof the soft tissues is best able to resist largedisplacing forces of short duration. Small forcesacting over an extended period of time, such asthe influence of gravity on the upper denture,result in a much smaller pressure differentialbetween the saliva film and the air becausethey allow saliva to be drawn gradually intothe space being created beneath the prosthesis.If the effect of gravity is unopposed, a pro-gressive downwards movement of the upperdenture is likely to occur until eventuallyall retention is lost and the denture drops.However, in this situation, occlusal forces areimportant in restoring the denture to its formerposition. Whenever the patient occludes (e.g.during swallowing), excess saliva which hasaccumulated beneath the denture is squeezedout again, the denture is re-seated and retentionis re-established.
Obtaining optimum physicalretentionThe aspects of complete dentures that influencethe amount of physical retention obtained are:
� Border seal� Area of impression surface� Accuracy of fit
Border seal
For optimum retention, the denture bordershould be shaped so that the channel betweenit and the sulcus tissues is as small as possible.
Resting level of sulcus
Lowest functionallevel of sulcus
Area offacial seal
Figure 4.9 Lateral extension of the buccal flange toproduce a facial seal.
It is not possible to maintain a close approx-imation between the border of a denture andthe mucosal reflection in the sulcus at all timesbecause the depth of the sulcus varies duringfunction. The denture has to be constructedso that the border conforms to the shallowestpoint that the sulcus reflection reaches duringnormal function. This means that for some ofthe time when the patient is at rest the denturewill be slightly under-extended. If the denturewere extended further in an attempt to producea more consistent seal in this area, displacementmight occur when the sulcus tissues move dur-ing function. The problem of achieving a con-stant border seal is overcome by extending theflanges of the denture laterally so that they con-tact and slightly displace the buccal and labialmucosa to produce a facial seal (Fig. 4.9).
It is not possible to produce a facial sealalong the posterior border of the upper dentureas it crosses the palate. In this area, the solu-tion to achieving the smallest possible space be-tween denture and mucosa is to create a post-dam – a raised lip along the posterior borderwhich becomes embedded a little way into thepalatal mucosa. One way of producing this is

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
62 Prosthetic Treatment of the Edentulous Patient
to cut a groove into the working cast wherethe posterior border of the denture is to be lo-cated which is normally at the vibrating line(Figs. 10.1 and 10.3).
Alternatively, the post-dam may be devel-oped during the first stage of the master im-pression by using a mucocompressive impres-sion material along the posterior border of theimpression tray to displace the mucosa locallyin the post-dam area (p. 145).
However, although an enhanced posteriorseal is achieved with a post-dam it differs fromthe facial seal against the flanges in that, evena small downwards movement of the posteriorborder of the denture is likely to break the sealwith a resultant loss of retention. If the post-dam has width as well as depth, the basic re-tention of the denture will be improved.
Area of impression surface
The degree of physical retention is proportionalto the area of the impression surface. It is impor-tant therefore to ensure maximum extension ofthe dentures so that the optimum retention fora particular patient may be obtained.
The denture on the right side in Fig. 4.10 waspoorly retained because the thin flanges failedto create a facial seal, and the palatal coverage
Figure 4.10 Right: denture poorlyretained because the thin flangesfailed to create a facial seal andthe palatal coverage did not makethe most of the area available.Left: the replacement denture cor-rected these errors and as a resulthad excellent retention.
did not make the most of the area available. Thereplacement denture on the left corrected theseerrors and as a result had excellent retention.
Accuracy of fit
The thinner the saliva film between the dentureand underlying mucosa, the greater the forcesof retention; therefore, it is important that the fitof the dentures is as accurate as possible. A poorfit will increase the thickness of the saliva filmand increase the likelihood of air bubbles occur-ring within the film. These bubbles will furtherreduce the retention of the denture. In addition,as the pressure of the saliva film drops due todisplacing forces acting on the denture, the airbubbles will expand and may extend to the bor-der area, resulting in a breaking of the borderseal.
Other factors
Bony undercuts
If bony undercuts exist, retention may be en-hanced by designing a denture that utilisesthese undercut areas. In order to achieve thiswithout traumatising the mucosa on insertionand removal of the denture, special care is

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
Stability of Dentures 63
Path ofinsertion
a
First pathof insertion
Second path of insertion
b
Figure 4.11 Selection of path ofinsertion to improve retention by util-ising undercuts: (a) single path ofinsertion to engage labial undercut;(b) dual path of insertion to engageunilateral undercut.
required in planning the path of insertion(Fig. 4.11).
Retention aids
In exceptional cases, such as surgical or congen-ital defects of the hard palate, it may not be pos-sible to obtain the required retention by routineclinical techniques. In such circumstances, theuse of denture fixatives, long-term soft liners,springs or implants may be of value.
Denture fixativeA denture fixative can be an invaluable aid toretention, particularly under difficult anatom-ical circumstances. Fixatives come in powder,paste or sheet form, the latter having the ad-vantage of staying longest between the denture
and mucosa. The more adhesive that can be in-corporated in the sheet of material, the betterthe retention (Uysal et al. 1998). It should benoted that there is a potential health risk as-sociated with long-term, excessive use of zinc-containing denture adhesives; high levels ofzinc in the body have been associated withsymptoms such as numbness or tingling in thearms and legs, difficulties with walking andbalance, and anaemia. As a result these prod-ucts have been currently withdrawn from themarket.
Long-term soft linersSoft liners enable free, flexible margins to ex-tend into the anatomical defect and engage tis-sue undercuts. The liner can be constructed asan integral part of the denture base or as a

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
64 Prosthetic Treatment of the Edentulous Patient
separate obturator section retained on the den-ture base by rare earth magnets. Long-termsoft lining materials are considered further inChapter 16.
Denture springsDenture springs are usually of coil type andare attached by pivots to the buccal flanges ofupper and lower dentures in the premolar re-gion. The springs are often partially coveredby acrylic flanges, or ‘hooded’, to stabilise thesprings and reduce irritation of the buccal mu-cosa. The springs exert a force which acts to sep-arate the dentures and thus helps to maintainthe dentures in contact with the supporting tis-sues. These devices are rarely used but can oc-casionally be of value when the anatomical cir-cumstances are exceptionally unfavourable ascan be the case in a patient who has undergonea maxillectomy.
ImplantsIt was proposed in the McGill Consensus State-ment (Feine et al. 2002) and again in the YorkConsensus statement (Thomason et al. 2009)that 2-implant supported overdentures shouldbe the minimum offered to edentulous patientsas the first choice of treatment. Available datastrongly support this suggestion in terms ofpatient satisfaction and Quality of Life out-comes (Thomason et al. 2007). The available ev-idence has resulted in this form of treatmentbeing recognised and provided under privateand state administered insurance schemes ina number of different countries over the lastfew years. The situation currently in the UK re-mains with almost all implant provision occur-ring privately or to a limited extent in the sec-ondary care environment.
Displacing forcesActing through the occlusal surface
Occlusal imbalance
If, when the dentures occlude, tooth contact onone side of the dental arch is not balanced by
Figure 4.12 Tipping of the denture due to an un-balanced occlusal contact.
contact on the other side the dentures will tip,causing the border seal to break, with conse-quent loss of retention (Fig. 4.12). When themandible moves into lateral or protrusive oc-clusal positions, interference between opposingteeth resulting from interlocking cusps or anexcessively deep overbite can cause horizon-tal displacement and tipping of the dentures.This type of instability can be minimised by re-ducing or eliminating the occlusal interferences(pp. 167–171). It should be borne in mind thatocclusal displacing forces can be dramaticallyincreased in patients exhibiting parafunctionalactivity such as bruxism.
Mastication
Forces related to the posterior teethDuring mastication, pressure exerted by thefood on the teeth tends to displace the den-ture. This problem may influence the position-ing of artificial posterior teeth. For example, sta-bility of the lower denture can be improvedby careful consideration of the posterior exten-sion of the occlusal table. If that table extendsto the steeply sloping part of the ridge posteri-orly, pressure from the bolus will tend to makethe denture slide forwards (Fig. 4.13). There-fore the occlusal table should terminate on the

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
Stability of Dentures 65
Figure 4.13 Pressure from thebolus on the posterior part of thelower occlusal table, which overliesa sloping part of the ridge, causesthe lower denture to slide forwards.
relatively horizontal part of the ridge whereeffective support is available and displace-ment prevented. It may be necessary to reducethe number of posterior teeth to achieve thisaim.
Forces related to the anterior teethOccasionally, the problem of occlusal displace-ment can create a conflict of interests betweenthe requirements of optimum appearance anddenture stability. This is illustrated by the ex-ample of the experienced denture wearer whoexpresses a strong preference for having up-per anterior teeth placed close to the crest ofthe ridge where strong incising forces can beapplied with minimal leverage effects, despitethe fact that lip support and appearance wouldbe compromised. In the face of such a clearlystated preference it is usually wise for the clin-ician to comply with the patient’s request. Butit is important that the likely aesthetic penaltyis explained to, and accepted by, the patient be-fore treatment is started.
During the opening phase of the masticatorycycle, when the teeth begin to separate afterpenetrating a bolus of food, the adhesive prop-erties of the food generate a displacing forcein an occlusal direction. Sticky foods there-fore tend to move the dentures away from themucosa.
Acting through the polishedsurface
The muscles of the lips, cheeks and tongue, inaddition to being of fundamental importancein the retention of dentures, are also capable ofcausing denture instability. Displacement willoccur, as mentioned earlier, if the polished sur-faces have an unfavourable slope (Fig. 4.3b)and also if the denture interferes with the ha-bitual posture and functional activity of thesurrounding musculature. For example, distalmovement of a lower denture may be producedby the lower lip if the anterior teeth are placedtoo far labially (Fig. 4.14). The teeth shouldtherefore be placed just far enough lingually toprevent this displacement but not so far as toallow excessive tongue pressure to develop.
It is not uncommon to see lower denturesthat are unstable because the posterior teethhave been placed too far lingually; under suchconditions of restricted tongue space, move-ment of the tongue during function will tendto lift the denture. There is an area betweenthe tongue on the one side and the cheeks andlips on the other where the muscular displacingforces acting on a denture are least. This area isknown as the neutral zone or zone of minimalconflict. Positioning a prosthesis within thiszone is most important for the lower dentureas the physical retentive forces are normally

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
66 Prosthetic Treatment of the Edentulous Patient
Figure 4.14 Distal displacement of the lower den-ture caused by placing teeth too far labially.
small and can do little to resist muscular dis-placement.
Post-extraction changes may lead to a grad-ual shifting of the neutral zone. For example,it is common for posterior teeth to be extractedsome considerable time before the anteriorteeth. If a partial denture is not fitted, thetongue spreads laterally into the edentulousspace. This, in effect, moves the neutral zonelaterally as well as reducing its bucco-lingualdimension so that there is a reduced space inwhich to place a denture. This space mightbe re-established, at least in part, when anew complete denture is fitted. However, themodification in tongue posture and behaviourrequired to achieve this, increases the demandon the patient’s ability to adapt. Some patientsmay find it difficult or even impossible to meetthis challenge and so the denture could fail.
Changes in the neutral zone also occur be-tween the lower lip and the tongue as a result ofpost-extraction changes affecting the mentalismuscle. Resorption of the alveolar bone leads tothe superior fibres of the origin of the mentalismuscle lying on top of the residual ridge and alingual migration of the neutral zone. Certainly,in these circumstances, it is no longer possibleto position the artificial teeth where once thenatural ones were situated.
A further disturbance of muscle balance canarise as a consequence of incorrect tongue pos-ture. If the tongue takes up a ‘defensive pos-ture’ towards the back of the mouth a lowerdenture, of whatever design, will be unstable.It is necessary to explain matters to the patientand train the tongue to touch the lingual sur-faces of the lower incisors in order to restorethe lingual balancing force and, thus, stability(Likeman 1997).
Gravity
The effect of gravity on an upper denture hasbeen described on p. 61. In order to minimisethis effect, it is important that the upper dentureis of light construction. Heavy denture base ma-terials, such as cobalt-chromium alloy, shouldbe avoided unless other requirements, such asstrength, are of overwhelming importance.
SupportThis chapter has shown that stability of den-tures can be obtained only if retentive forces ex-ceed displacing forces. However, there is onemore factor in the equation, that of adequatesupport for the dentures by the underlying tis-sues. A reduction in support promotes instabil-ity, as indicated in the following examples:
� Instability of an upper denture follows re-sorption of the supporting bone. This resorp-tion is largely confined to the region of thealveolar ridges, as there is remarkably littleresorption of bone in the centre of the palate.Thus, after a period of time, the denture willbe well supported by the hard palate, butthere will be limited contact between the im-pression surface of the denture and the alve-olar ridges. In these circumstances, occlusalcontact readily produces tipping, with thedenture pivoting about the mid-line of thepalate.
� Support will be inadequate if the ridges aresmall because resistance to lateral displacingforces will be poor.

P1: JZP Trim: 246mm X 189mmc04 BLBK351-Basker January 18, 2011 13:25 Printer Name: Yet to Come
Stability of Dentures 67
� Support will be reduced if the ridges areflabby (p. 242). The denture will move con-siderably during function even though theretention may be good and contact with themucosal surface is maintained.
References and additionalreadingBasker, R.M. & Watson, C.J. (1991) Tongue control of
upper complete dentures – a clinical hint. BritishDental Journal, 170, 449–50.
Brill, N. (1967) Factors in the mechanism of full den-ture retention – a discussion of selected papers.Dental Practitioner and Dental Record, 18, 9–19.
Culver, P.A.J. & Watt, I. (1973) Denture movementsand control – a preliminary study. British DentalJournal, 135, 111–16.
Darvell, B.W. & Clark, R.K.F. (2000) The physicalmechanisms of complete denture retention. BritishDental Journal, 189, 248–52.
Davenport, J.C. (1984) Clinical and laboratory proce-dures for the production of a retentive silicone rub-ber obturator for the maxillectomy patient. BritishJournal of Oral and Maxillofacial Surgery, 22, 378–86.
Feine, J.S., Carlsson, G.E., Awad, M.A., Chehade, A.,Duncan, W.J., Gizani, S., Head, T., Heydecke, G.,Lund, J.P., MacEntee, M., Mericske-Stern, R., Mo-jon, P., Morais, J.A., Naert, I., Payne, A.G., Pen-rod, J., Stoker, G.T., Tawse-Smith, A., Taylor, T.D.,Thomason, J.M., Thomson, W.M. & Wismeijer, D.(2002) The McGill consensus statement on over-dentures. Mandibular two-implant overdenturesas first choice standard of care for edentulous pa-tients. Journal of Prosthetic Dentistry, 88, 123–4.
Grasso, J.E., Rendell, J. & Gay, T. (1994) Effect of den-ture adhesive on the retention and stability of max-illary dentures. Journal of Prosthetic Dentistry, 72,399–405.
Jagger, D.C. & Harrison, A. (1996) Denture fixatives –an update for general dental practice. British DentalJournal, 180, 311–13.
Kelsey, C.C., Lang, B.R. & Wang, R.F. (1997) Examin-ing patients’ responses to the effectiveness of fivedenture adhesive pastes. Journal of the AmericanDental Association, 128, 1532–8.
Likeman, P.R. (1997) Tongue control of lower com-plete dentures: a clinical hint. British Dental Journal,182, 229–30.
Lindstrom, R.E., Pawelchak, J., Heyd, A. & Tarbet,W.J. (1979) Physical–chemical aspects of dentureretention and stability. A review of the literature.Journal of Prosthetic Dentistry, 42, 371–5.
Sheppard, I.M. (1963) Denture base dislodgementduring function. Journal of Prosthetic Dentistry, 13,462–8.
Slaughter, A., Katz, R.V. & Grasso, J.E. (1999) Profes-sional attitudes toward denture adhesives. Journalof Prosthetic Dentistry, 15, 159–65.
Thomason, J.M, Feine, J., Exley, C., Moynihan, P.,Muller, F., Naert I., Ellis, J.S., Barclay, C., But-terworth, C., Scott B., Lynch, C., Stewardson, D.,Smith, P., Welfare, R., Hyde, P., McAndrew, R., Fen-lon, M., Barclay, S. & Barker, D. (2009) Mandibulartwo implant-supported overdentures as the firstchoice standard of care for edentulous patients-theYork Consensus Statement. British Dental Journal,207, 185–6.
Thomason, J.M., Heydecke, G., Feine, J.S. & Ellis, J.S.(2007) How do patients perceive the benefit of re-constructive dentistry with regard to oral health re-lated quality of life and patient satisfaction? Clini-cal Oral Implants Research, 18, 168–88.
Tyson, K.W. (1967) Physical factors in retention ofcomplete upper dentures. Journal of Prosthetic Den-tistry, 18, 90–7.
Uysal, H, Altay, O.T., Alparslan, N. & Bilge, A. (1998)Comparison of four different denture cushion ad-hesives – a subjective study. Journal of Oral Rehabil-itation, 25, 209–13.

P1: JZP Trim: 246mm X 189mmc05 BLBK351-Basker January 4, 2011 7:46 Printer Name: Yet to Come
5Jaw Relations – Theoretical Considerations
The clinical procedure of recording the jawrelationship enables the clinician to providethe dental technician with the followinginformation:
� An appropriate vertical and horizontal rela-tionship of the mandible to the maxilla.
� The required shape of the dentures.
This information is given to the dental tech-nician in the form of wax record rims, whichhave been adjusted by the clinician, to enablethe casts to be mounted on an articulator. Theshape of the record rims provides the dentaltechnician with a blueprint on which to base thedesign of the trial dentures.
This chapter is devoted to a discussion of thetheoretical background to occlusion. The pointsarising from the discussion are used to justifythe clinical techniques described in Chapter 11.
Basic mandibular positions� Rest position. The rest position can be de-
fined as the vertical and horizontal position
the mandible assumes when the mandibu-lar musculature is relaxed and the patientis upright. When the mandible is in the restposition there is a space between the oc-clusal surfaces of the teeth which is knownas the freeway space or interocclusal restspace. This space is wedge-shaped, beinglarger anteriorly where the separation be-tween the teeth is most commonly withinthe range 2–4 mm, although there can beconsiderable variation between individualsand within an individual depending on theparticular circumstances operating at thetime.
� Muscular position. The muscular position isthe vertical and horizontal position of themandible produced by balanced muscle ac-tivity raising the mandible from the rest po-sition into initial tooth contact.
� Intercuspal position. The intercuspal positionis the vertical and horizontal position ofthe mandible in which maximum occlusalcontact occurs. In the denture wearer, theintercuspal and muscular positions shouldcoincide.
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
68

P1: JZP Trim: 246mm X 189mmc05 BLBK351-Basker January 4, 2011 7:46 Printer Name: Yet to Come
Jaw Relations – Theoretical Considerations 69
OVD RVD
Freeway space
Figure 5.1 The difference betweenthe rest vertical dimension (RVD) andthe occlusal vertical dimension (OVD)is the freeway space.
The distance between two selected points,one related to the maxilla and one relatedto the mandible, when the upper and lowerteeth are in contact is known as the occlusalvertical dimension. When the mandible is inits resting position, this distance is the restvertical dimension (Fig. 5.1). The differencebetween the measurements is the freewayspace.
� Retruded contact position. With light toothcontact maintained, movement of themandible in a posterior direction from theintercuspal position is usually possible. Thisposterior position is known as the retrudedcontact position and is separated fromthe intercuspal position by approximately1 mm. Further retrusion of the mandible isprevented by the lateral ligaments of thetemporomandibular joints.
With the condyles maintained in theretruded position, the movement of themandible as it opens is hinge-like until jawseparation in the incisal region is approxi-mately 2 cm. The path taken by the mandibleup to this point is known as the retruded arcof closure. Further opening of the mandibleresults in a forwards and downwards trans-lation of the condyles.
The interrelationship of the mandibular po-sitions is shown in Fig. 5.2.
In the past, there has been confusion with re-gard to the associated nomenclature. The termsused in this book, together with the alternativescommonly used elsewhere in the dental litera-ture, are shown in Table 5.1.
The rest position
Clinical significance� Constructing or assessing dentures. The rest
position is used as a reference position whendetermining the appropriate occlusal verti-cal dimension for new complete dentures orchecking the occlusal vertical dimension ofexisting dentures. The clinical procedure isto measure the rest vertical dimension andthe occlusal vertical dimension and then cal-culate the freeway space.
� Relaxation of the masticatory apparatus. Whenthe mandible is in the rest position and theteeth are out of contact, the tissues whichsupport the dentures are not loaded, thereis no strain on the temporomandibular jointcapsules and only minimal, if any, activityin the elevator and depressor muscles of themandible.
If new dentures have no freeway space, thedenture-bearing tissues are subjected to exces-sive loading, the elevator muscles are unable to

P1: JZP Trim: 246mm X 189mmc05 BLBK351-Basker January 4, 2011 7:46 Printer Name: Yet to Come
70 Prosthetic Treatment of the Edentulous Patient
Muscular+
intercuspalpositions
Retrudedcontactposition
Restposition
1 mm
2–4 mm
Retrudedarc of
closure
ANTERIOR POSTERIOR
Figure 5.2 Diagrammatic repre-sentation of the basic positions of themandible in the sagittal plane.
return to their normal resting length, and thecontinuous muscular activity results in an accu-mulation of metabolites and subsequent pain inthe affected muscles.
If, on the other hand, an excessive freewayspace is provided, the load on the tissues is ofcourse reduced. However, there is a reductionin masticatory efficiency and the patient’s ap-pearance is usually adversely affected.
Table 5.1 Nomenclature for basic mandibularpositions.
Terms used inthis book Alternative terms
Rest position Physiologic rest position
Muscular position Habitual position
Intercuspal position Centric occlusionMaximum intercuspationTooth position
Retruded contactposition
Centric occlusionCentric relationLigamentous positionPosterior border position
Freeway space Inter-occlusal rest space
Control of the rest position
The rest position of the mandible at any onetime is the result of a balance of forces as shownin Fig. 5.3. Both passive and active forces are de-scribed. The relative importance of active andpassive forces in determining the rest positionis a controversial issue. One school of thoughtmaintains that active forces are the major fac-tor, another that passive forces alone are re-sponsible for the true rest position, while yeta third school suggests that the rest position isthe product of both active and passive forces incombination.
Passive forcesPassive forces are derived from the following:
� Muscles attached to the mandible. Passiveforces arising from the muscles attached tothe mandible result from the elastic natureof the muscle fibres and of the connectivetissue elements. Although it has been sug-gested that, in the truly relaxed state, thepassive forces inherent in the muscles areable to maintain the rest position, this state israrely evident and variables such as changein posture or emotional state affect the

P1: JZP Trim: 246mm X 189mmc05 BLBK351-Basker January 4, 2011 7:46 Printer Name: Yet to Come
Jaw Relations – Theoretical Considerations 71
Elevator muscles (active and passive)
Reduced air pressure (passive)
Gravity(passive)
Depressor muscles (active and passive)
Capsule andligaments(passive)
Figure 5.3 Forces which determine the rest positionof the mandible.
equilibrium, resulting in the introduction ofactive forces.
� The elastic properties of the capsules and lig-aments of the temporomandibular joints. Theelastic properties of the capsules and liga-ments of the temporomandibular joints exertforces on the condyles that tend to returnthem to a central position within the glenoidfossae. Thus, these passive forces will en-courage the mandible to adopt the restposition.
� Reduced intra-oral air pressure. A contribu-tion to the balance of forces acting on themandible in the rest position may come froma reduction in intra-oral air pressure.
When the mandible is in the rest posi-tion, the lips are together and the patient isbreathing through the nose, the oral cavityis a closed ‘box’ sealed anteriorly by the lipsand posteriorly by contact between the softpalate and the posterior surface of thetongue. There is a tendency for the spaceinside this closed box, between the dorsum
of the tongue and the hard palate, to beincreased by the weight of the mandiblepulling downwards. It has been suggestedthat the pressure in this closed space isthus reduced and that the resulting differ-ential between the intra-oral pressure andatmospheric pressure helps to support themandible in the rest position.
� Gravity. The force of gravity is a constant fac-tor. However, its influence on the balance offorces acting on the mandible varies with theposition of the head in the gravitational fieldand with the mass of the mandible. Thus,the gravitational effect is reduced when thepatient is supine, when lower teeth are ex-tracted or when a lower denture is removedfrom the mouth.
Active forcesActive forces influencing the rest positionare generated by continuous low-grade mo-tor unit activity in the muscles attached to themandible. This activity is seen predominantlyin the elevator muscles and is influenced by thefollowing factors:
� Mass of the mandible. Activation of the stretchreflex increases motor unit activity. If themass of the mandible is increased by the in-sertion of a lower denture or record block,the mandible will tend to drop and the ele-vator muscles will be stretched. Muscle spin-dles within the stretched muscles are acti-vated and initiate impulses which increasemotor unit activity in the same muscles andinhibit activity in the depressor muscles.This activity acts to oppose the displacingeffect of the lower denture and returns themandible towards its original rest position.
� Changes in position of the mandible. Othermechanoreceptors which may play a partin influencing the rest position followingchanges in position of the mandible, or of thehead as a whole, are to be found in the tem-poromandibular joint, the middle ear andthe cervical spine.

P1: JZP Trim: 246mm X 189mmc05 BLBK351-Basker January 4, 2011 7:46 Printer Name: Yet to Come
72 Prosthetic Treatment of the Edentulous Patient
� Pain, drugs and emotional stress. External fac-tors are able to facilitate or inhibit motor unitactivity via the reticular system. For exam-ple, the amount of jaw separation at rest isreduced by pain, drugs such as adrenalinand caffeine, and emotional stress. Emo-tional stress itself may be caused by factorsin the patient’s own domestic environment,or by disturbing visual, auditory or olfactorystimuli in the dental surgery. Jaw separationis increased during sleep or by drugs such astranquillisers and sedatives.
An alternative explanationThe rest position of the mandible has been con-sidered from an entirely different viewpoint –its association with the function of respiration(Fish 1964). When a patient is at rest, respirationis the primary function affecting the oral region.It has been suggested that the rest position ofthe mandible is determined by the demands ofthe tongue in performing its respiratory func-tion of completing the anterior wall of the pha-ryngeal part of the respiratory tract (Fig. 5.4a).Following extraction of teeth and resorption ofthe alveolar bone, the tongue spreads laterallyinto the edentulous space. When the resorp-tion of bone is extensive, the tongue spreads tosuch a degree that the posterior oral seal cannotbe maintained (Fig. 5.4b). The response of themandible in this situation is to rise, thus allow-ing the posterior oral seal to be re-established(Fig. 5.4c). A lower denture replaces the naturalteeth and alveolar bone and, when inserted intothe mouth, controls the lateral tongue spreadand allows the mandible to return to a lowerresting position while still maintaining the pos-terior seal.
Variation in the rest position
At one time, the rest position of the mandiblewas thought to be constant throughout life.From the foregoing discussion, it is apparentthat this is not so. The rest position of the eden-tulous patient can be affected by the short-term
Posterior oral seal
Posterior oral sealbroken
Posterior oral sealre-established
a
b
c
Figure 5.4 The association of the tongue with res-piration and its influence on the rest position of themandible: (a) posterior oral seal established betweenthe soft palate and the tongue – lower denture in situ;(b) the tongue spreads into the area vacated by thedenture; the posterior oral seal cannot be maintained;(c) the mandible is raised so that the posterior oralseal can be re-established (the rest vertical dimensionwhen the denture is in the mouth is therefore largerthan when it is removed) (Fish 1964).
variables listed in Table 5.2, and by long-termvariables. However, these variables in no wayreduce the value of the rest position as a refer-ence point in establishing the occlusal verticaldimension.
Short-term variablesThe short-term variables can reduce the repro-ducibility of the rest vertical dimension while

P1: JZP Trim: 246mm X 189mmc05 BLBK351-Basker January 4, 2011 7:46 Printer Name: Yet to Come
Jaw Relations – Theoretical Considerations 73
Table 5.2 Short-term variables that may affect therest position of the edentulous patient.
VariableRest verticaldimension
Patient supine Reduced
Head tilted back Increased
Head tilted forwards Reduced
Insertion of lower denture orrecord block
Increased
Stress Reduced
Pain Reduced
Drugs Variable
the clinician is attempting to record it, but thatinfluence can be minimised by careful clinicaltechnique as discussed in Chapter 11.
Long-term variablesProsthetic treatment has an important long-term influence on the rest position of themandible. If the same dentures are worn formany years and are not maintained, a reduc-tion in the occlusal vertical dimension occursas a result of alveolar resorption and occlusalwear. The rest position of the mandible adaptsto this change and takes up a position closer tothe maxilla. Longitudinal studies of the changein the vertical dimension have been undertakenand it has been shown that an average 7-mmreduction in occlusal vertical dimension occursin as many years (Fig. 5.5). The rest verticaldimension responds in a similar manner, al-though to a lesser degree. As a result, the free-way space becomes larger. Where these changeshave taken place in young patients, it is oftenpossible to recover much of the lost vertical di-mension when new dentures are constructed.However, with the older patient, any attemptto restore the occlusal vertical dimension to itsoriginal level may be met with problems thatare discussed more fully in Chapter 8. The long-term variables will not affect the reproducibility
of the rest vertical dimension during the periodof a dental appointment, but their likely effecton the recorded rest vertical dimension needsto be recognised by the clinician and allowedfor, if appropriate.
The muscular and intercuspalpositions
The precise nature of the muscular and inter-cuspal positions in a dentate subject dependsupon the arrangement of the natural teeth andthe proprioceptive impulses arising from re-ceptors in the periodontal ligaments and mus-cles of mastication. The muscular position isnot constant and may be modified by sensoryfeedback resulting from changes in intercus-pal position. For example, a protrusive relation-ship may be adopted following loss of poste-rior teeth and consequent restriction of mas-tication to the incisal region. A similar situa-tion can develop where an edentulous patienthas been wearing dentures whose pattern of oc-clusal contact has been altered through toothwear and resorption of underlying bone. In thisinstance, altered sensory input from receptorsin the denture-bearing mucosa and muscles en-courages the mandible to adopt a protrusiveposition closer to the maxilla. The resulting clin-ical picture is one of uneven occlusal contact, re-duction in the occlusal vertical dimension andprotrusion of the mandible. Such a modifica-tion of the muscular position will complicatethe provision of new dentures. Although theposition will appear to be reproducible, it is un-wise to set up the new dentures in relation to itbecause once they are fitted the muscular posi-tion is likely to change yet again in response tothe new sensory feedback initiated by the im-proved occlusion. Muscular position and inter-cuspal position will then no longer be coinci-dent. This is a highly undesirable situation be-cause it increases the likelihood of damage tothe denture-bearing tissues and discomfort inthe muscles of mastication. The situation can beavoided by recording the retruded jaw relation

P1: JZP Trim: 246mm X 189mmc05 BLBK351-Basker January 4, 2011 7:46 Printer Name: Yet to Come
74 Prosthetic Treatment of the Edentulous Patient
FWS
RVD
OVD
1 2 3 4 5 6 7
Years
0
Denture insertion
Ver
tical
dim
ensi
on
Figure 5.5 Average changes inocclusal and rest vertical dimen-sions after fitting complete dentures.(Modified after Tallgren (1966).)
rather than the muscular position, as discussedbelow.
The retruded jaw relation
This relation is determined by the lateral lig-aments of the temporomandibular joints anddoes not depend upon the presence of teeth.Therefore, it does not alter when the naturalteeth are extracted or when a new occlusalsurface replaces an unsatisfactory one. It hasbeen suggested that the retruded position haspractical significance during normal functionalmovements, as tooth contact in this positionis the termination of the heavy masticatorystrokes needed to break up pieces of hard food.
Reference positions of themandible to be used whenrecording the jaw relationshipWhen providing complete dentures, the rela-tionship of the mandible to the maxilla in bothhorizontal and vertical planes must be deter-mined.
In the vertical plane, it is of prime impor-tance that the occlusal vertical dimension of the
dentures allows for an adequate freeway space.If existing dentures have been entirely satisfac-tory from this point of view their occlusal ver-tical dimension may be copied in the new pros-theses. Otherwise the occlusal vertical dimen-sion must be calculated with reference to therest position.
The issue is perhaps less clear-cut with re-spect to the jaw relationship in the horizon-tal plane. Some authorities prefer to record theantero-posterior relationship of the mandibleto the maxilla in the muscular position,while others describe techniques for obtainingthe retruded position.
Evidence indicates that it is possible torecord the retruded position with greater con-sistency than the muscular position. It has beenshown that variation of the muscular positionin the antero-posterior plane is especially af-fected by the posture of the patient, whereasthe reproducibility of the retruded position re-mains high. In addition, it is quite possible thatthe muscular position may have been influ-enced by an abnormal occlusion and may al-ter once the new occlusal surface has been pro-vided. Because the retruded jaw relationshipis more consistent than the muscular position,and because the former is known to be close to

P1: JZP Trim: 246mm X 189mmc05 BLBK351-Basker January 4, 2011 7:46 Printer Name: Yet to Come
Jaw Relations – Theoretical Considerations 75
an acceptable intercuspal position, the authorsrecommend using the retruded position as thepoint of reference in the horizontal plane. How-ever, when positioning the artificial teeth, al-lowance must be made for the patient to adoptthe muscular position. This concept is consid-ered further on p. 170.
References and additionalreadingBrill, N. & Tryde, G. (1974) Physiology of mandibular
positions. Frontiers of Oral Physiology, 1, 199–237.Brill, N., Lammie, G.A., Osborne, J. & Perry,
H. (1959) Mandibular positions and mandibularmovements. A review. British Dental Journal, 106,391–400.
Crum, R.J. & Loiselle, R.J. (1972) Oral perception andproprioception: a review of the literature and itssignificance to prosthodontics. Journal of ProstheticDentistry, 28, 215–30.
Faigenblum, M.J. (1966) Negative oral pressures.A research report. Dental Practitioner and DentalRecord, 16, 214–16.
Fish, S.F. (1961) The functional anatomy of the restposition of the mandible. Dental Practitioner andDental Record, 2, 178–88.
Fish, S.F. (1964) The respiratory associations of therest position of the mandible. British Dental Journal,116, 149–59.
Helkimo, M., Ingervall, B. & Carlsson, G.E. (1971)Variation of retruded and muscular position ofmandible under different recording conditions.Acta Odontologica Scandinavica, 29, 423–37.
Nairn, R.I. & Cutress, T.W. (1967) Changes inmandibular position following removal of the re-maining teeth and insertion of immediate com-plete dentures. British Dental Journal, 122, 303–6.
Posselt, U. (1952) Studies in the mobility of the hu-man mandible. Acta Odontologica Scandinavica, 10(Suppl. 10).
Preiskel, H.W. (1965) Some observations on the pos-tural position of the mandible. Journal of ProstheticDentistry, 15, 625–33.
Tallgren, A. (1957) Changes in adult face heightdue to ageing, wear and loss of teeth and pros-thetic treatment. Acta Odontologica Scandinavica, 15(Suppl. 24).
Tallgren, A. (1966) The reduction in face heightof edentulous and partially edentulous subjectsduring long-term denture wear. Acta OdontologicaScandinavica, 24, 195–239.
Yemm, R. (1969) Variations in the electrical activity ofthe human masseter muscle occurring in associa-tion with emotional stress. Archives of Oral Biology,14, 873–8.
Yemm, R. (1972) Stress-induced muscle activity: apossible etiologic factor in denture soreness. Jour-nal of Prosthetic Dentistry, 28, 133–40.
Yemm, R. & Berry, D.C. (1969) Passive control inmandibular rest position. Journal of Prosthetic Den-tistry, 22, 30–6.

P1: JZP Trim: 246mm X 189mmc06 BLBK351-Basker December 17, 2010 10:34 Printer Name: Yet to Come
6Introductory Remarks to the Clinical Chapters
A preview of the clinicalchaptersIt is much more common for a dentist to haveto provide complete dentures as replacementsfor existing dentures than to provide them for apatient who has not worn dentures before.
What is the reason for this pattern of treat-ment? Clearly, one of the main factors is thatthe average life expectancy of patients receivingcomplete dentures for the first time is consider-ably greater than the average life expectancy ofthe dentures themselves. This is, of course, par-ticularly the case if the patient’s first completedentures were immediate restorations whoseuseful life is relatively short. Thus, dentures arelikely to be replaced several times during thelife of the patient.
The remaining chapters of this book arelargely concerned with clinical procedures and,because of the pattern of demand mentionedabove, the major emphasis is placed on thetreatment of patients requiring replacementdentures.
Chapter 7 deals with the first stage of treat-ment, i.e. history, examination and treatmentplanning. Then in Chapter 8, the use of old den-tures is discussed as their existence affects treat-ment from the outset. The next logical step is toconsider the measures that may be required toprepare the oral tissues (Chapter 9) before con-tinuing with the stages of denture construction(Chapters 10–15). The book concludes with adiscussion of some clinical problems and theirpossible solutions (Chapter 16).
Of course, there are patients who requirecomplete dentures, who have not had den-tures before. In these cases the initial assess-ment is usually a less complicated procedure.After mouth preparation, the conventional clin-ical stages of treatment are followed, as de-scribed in the appropriate chapters.
Quality of treatment – itscontrol and enhancementIn recent years much emphasis has been placedon measures designed to evaluate and improve
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
76

P1: JZP Trim: 246mm X 189mmc06 BLBK351-Basker December 17, 2010 10:34 Printer Name: Yet to Come
Introductory Remarks to the Clinical Chapters 77
the quality of care. This has led to the activepromotion of two concepts:
1. Clinical audit2. Peer review
Clinical audit
Clinical audit has been defined as:
the systematic, critical analysis of thequality of dental care, including the pro-cedures and processes used for diagno-sis, intervention and treatment, the use ofresources and the resulting outcome andquality of life as assessed by both profes-sionals and patients.
(Clinical Audit and Peer Review in theGeneral Dental Services, April 2001)
The aim of the concept is self-examinationby the clinician. For example, criteria are estab-lished to judge the quality of outcome of a pro-cedure, the actual outcome is measured againstthe criteria and, where the criteria have notbeen fully met, changes are made to improvethe procedure and the audit cycle is repeatedafter a convenient time.
Peer review
Peer review
provides an opportunity for groups ofdentists to get together to review aspectsof practice. The aim is to share experi-ences and identify areas in which changescan be made with the objective of im-proving the quality of service offered topatients.
(Clinical Audit and Peer Review in TheGeneral Dental Services, April 2001)
We hope that this textbook will be seen asproviding a useful foundation on which qualityinitiatives can be built. As a contribution to the
thinking behind clinical audit and peer reviewwe have included short sections in the clinicalchapters entitled ‘Quality control and enhance-ment’ where we offer ideas on clinical topicswhich might be examined more closely withinan audit cycle.
The clinician/dental technicianinterfaceThe quality of care provided for the edentulouspatient is heavily dependent upon effectivecommunication between the dental clinicianand dental technician and a mutual under-standing of the objectives for each clinical stage.
Previous studies have indicated that thestandard of communication between a dentalclinician and a dental technician can be veryvariable (Basker et al. 1993; Barsby et al. 1995).Even in those cases when the instructions fromthe dentist are clear they are not necessarily fol-lowed by the dental technician, as shown inthe survey of quality of complete dentures byBarsby et al. (1995), where the actual positionof the postdam on the finished dentures onlycoincided with the correct position which hadbeen clearly marked previously by the clinicianin 65 of the 101 instances.
The outcome of a study into the quality ofcopy dentures (Kippax et al. 1998) strongly sug-gested that the objectives behind the procedurewere not fully understood by either clinician ordental technician with the result that the den-tures produced were poor ‘copies’.
To emphasise the importance of clear com-munication, we have included specific sectionson the topic at the end of each appropriatechapter. We have not included such basic itemsas names and addresses of the patient and thedentist and the date when the next item of workis required. Rather, we have listed the mini-mum amount of information that the dentaltechnician requires in order to provide what isreally wanted by the clinician.
At this point it is worth noting that the ac-curacy of the clinician’s prescription and the

P1: JZP Trim: 246mm X 189mmc06 BLBK351-Basker December 17, 2010 10:34 Printer Name: Yet to Come
78 Prosthetic Treatment of the Edentulous Patient
way it is acted upon by the dental technicianare fruitful areas for clinical audit and peer re-view. A greater understanding of each other’srole would foster this communication and maybe best built on joint training and shared edu-cation (Clark et al. 2010).
The control of cross-infectionMuch has been written about cross-infectioncontrol in the last decade. It is not appropriatein this book to go into any detail about tech-niques that should be used. Rather, we simplymake the point that the reader will find up-to-date information provided by professional,governmental and statutory bodies as well asin the dental literature and in information pro-vided by the manufacturers of dental products.
We restrict ourselves to a brief discussion onthree points:
1. The surgery/laboratory interface2. Impression materials3. Avoiding contamination of stock materials
The surgery/laboratory interface
The dental technician is an integral memberof the dental team, and the dental laboratory,wherever it is situated, is an integral part of thedental environment. Therefore, it is essentialthat cross-infection policies are fully discussed,understood and agreed on by both dental tech-nician and clinician. Without this close coopera-tion, the chain upon which cross-infection con-trol depends will be broken and the mutual pro-tection lost.
Cross-infection within the dental laboratorycan be a problem. One study attributed a highprevalence of eye infections among dental tech-nicians to contaminated pumice. It was foundthat the pumice was heavily infected but thatthe bacterial count could be significantly re-duced by mixing up the slurry with a solutionof a commercially available disinfectant. It wasconcluded that untreated pumice slurries pre-
sented an unacceptable risk of cross-infection(Witt & Hart 1990).
The key to preventing transmission of infec-tion between the two areas is a disinfectant ‘bar-rier’ through which all items must pass beforebeing dispatched in either direction. The pre-cise nature of this barrier will vary according tothe item involved. Prior to dispatch of an itemfrom the clinic to the laboratory the responsi-bility for disinfection lies solely with the clini-cian. It is a good practice to agree the protocolto be used with the laboratory and this wouldbroadly consist of rinsing the item, immersingit in an ultrasonic bath if it is grossly contam-inated, disinfecting it with an approved prod-uct and then rinsing again before packing. Thepackage should be labelled to indicate its disin-fection status. When items are being returnedfrom the laboratory to the clinic, they shouldbe similarly disinfected before dispatch (BritishDental Association, 2009).
Impression materials
The basic point is that the dentist must choose acombination of impression material and disin-fectant where the latter is not only effective butwill not adversely affect the dimensional stabil-ity and surface accuracy of the impression.
Care needs to be taken not to breach cross-infection procedures when using impressioncompound. This material is commonly soft-ened in a thermostatically controlled water-bath. However, these baths must be regardedas contaminated once the impression has beencompleted, and therefore must be emptied,cleaned and disinfected before being used foranother patient – a cumbersome procedure. Abetter and simpler procedure is to use a bowlin which hot water is poured and which can beautoclaved after use.
Handling materials
When handling prosthetic materials, it is im-portant to develop a regimen that avoids

P1: JZP Trim: 246mm X 189mmc06 BLBK351-Basker December 17, 2010 10:34 Printer Name: Yet to Come
Introductory Remarks to the Clinical Chapters 79
contamination of stocks and unacceptable lev-els of wastage. Careful advanced planning foreach prosthetic appointment so that, as far aspossible, all the required materials and instru-ments are placed ready, is the key to min-imising the chance of contaminating stock.However, even then it is difficult to avoidthe situation in which it is necessary to col-lect additional items during a procedure. Thiscan be done only by changing the gloves,or by placing a barrier between the contam-inated gloves of the clinician and the stock.This barrier may take the form of a ‘clean’dental nurse to hand the item to the clini-cian, cheap vinyl over-gloves which are subse-quently discarded, or sterile forceps. Rummag-ing through stocks with contaminated glovesclearly creates a breach in any cross-infectionpolicy.
It is important for economic reasons to min-imise wastage. Dispensing prosthetic materials(such as the various waxes) in portions appro-priate for single use keeps the residue of un-used materials to a level at which they can bediscarded without incurring an unacceptable fi-nancial penalty.
References and additionalreadingBarsby, M.J., Hellyer, P.H. & Schwarz, W.D. (1995)
The qualitative assessment of complete den-tures produced by commercial dental laboratories.British Dental Journal, 179, 51–7.
Basker, R.M., Ogden, A.R. & Ralph, J.P. (1993) Com-plete denture prescription – an audit of perfor-mance. British Dental Journal, 174, 278–84.
British Dental Association (2009) Infection Controlin Dentistry (England). Advice sheet A12. BDA,London.
Clark, R.K.F., Radford, D.R. & Juszczyk, A.S. (2010)Current trends in complete denture teaching inBritish Dental Schools. British Dental Journal, 208,214-15.
Croser, D. & Chipping, J. (1989) Cross-infection con-trol in general dental practice – a practical guide for thewhole dental team. Quintessence, London.
Department of Health (2001) Clinical Audit and PeerReview in the General Dental Services. Department ofHealth, London.
Kippax, A., Watson, C.J., Basker, R.M. & Pentland,J.E. (1998) How well are complete dentures copied?British Dental Journal, 185, 129–33.
Witt, S. & Hart, P. (1990) Cross-infection hazards as-sociated with the use of pumice in dental laborato-ries. Journal of Dentistry, 18, 281–3.

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
7Assessment of the Patient
A thorough and systematic history and exami-nation of the patient will ensure that all relevantdetails are recorded so that the clinician can de-termine the following:
� Diagnosis� Treatment plan� Prognosis
The purpose of this chapter is to describe asystematic approach to this all-important stagepreceding treatment. The significance of the in-formation obtained is discussed more fully inother chapters of the book.
HistoryReason for attendance
After noting personal particulars such as name,address, age and occupation, the clinicianshould record the concern or complaint in thepatient’s own words. For example, if the pa-tient says that the denture is loose, it may bepositively misleading if the clinician records the
comment as ‘the denture lacks retention’. Thedenture may, in fact, exhibit excellent physicalretention but is being displaced by an unevenocclusal contact.
History of the present complaint
It is essential to obtain full details of any com-plaint. If, for example, the complaint is of painin relation to a denture, the location, characterand timing of the pain should be determined;relieving and aggravating factors should alsobe recorded. It is important to ascertain the re-lationship of the time of onset of the symptomswith the time that the present set of dentureswas fitted.
If a denture is loose, it is necessary to enquirewhen the looseness was first noticed. If the den-ture has been worn satisfactorily for severalyears before trouble developed, it indicates thatthe dentures were initially satisfactory and thatsubsequent changes such as resorption of theresidual ridges or wear of the occlusal surfacesare responsible for the problem. In this situa-tion, it is essential – in addition to identifying
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
80

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
Assessment of the Patient 81
the cause of the complaint – to note the goodfeatures of the denture, as it is usually sensibleto replicate these in the replacement dentures.
On the other hand, if the looseness waspresent from the time the denture was fitted,the cause may be attributed to a basic designfault in the denture, to unfavourable anatom-ical factors or perhaps to the inability of thepatient to adapt to dentures. Until an exami-nation is made, it is not possible to distinguishbetween these causes.
Dental history
When obtaining a patient’s dental history, it isnecessary to determine:
� when the natural teeth were extracted;� the reasons for the extractions;� the occurrence of any surgical complications;� how many dentures have been worn subse-
quently;� the degree of success or failure with the
dentures.
This history can provide important informationon the following:
� The rate of bone resorption. The history of toothloss provides a basis on which to make anassessment of the current rate of bone re-sorption. If extractions were carried out inthe previous few months, resorption will stillbe continuing at a rapid rate, so that if den-tures are provided at this time they will soonbecome loose and require rebasing. The pa-tient should therefore be warned of this like-lihood. If, however, the teeth were extractedseveral years ago, the alveolar bone willhave reached a relatively stable state and thelife of a replacement denture will be consid-erably extended.
� Retained roots. If there is a history of difficultextractions, it is advisable to obtain radio-graphs in order to check for the presence andlocation of retained roots.
� The adaptive capability of the patient. Cluescan be obtained as to the adaptive capa-bility of the patient. For example, if threesets of dentures have been worn success-fully over a period of 15 years, it may be as-sumed that adaptation has been satisfactory,whereas if the same number have been pro-vided over the last 2 or 3 years – and eachhas been troublesome – the ability to adaptwill be suspect. However, it is vitally impor-tant not to jump to conclusions and to putthe blame on the patient until one is satis-fied that the complaint cannot be related todefects in the design of previous dentures(see Chapter 2). It is thus a wise practice toask the patient to bring all available sets ofdentures when attending the initial assess-ment, as inspection of them can yield valu-able clues and increase the accuracy of thediagnosis.
Medical history
Notes should be made of a patient’s past andpresent medical history that is relevant tofuture dental treatment. Information shouldinclude particulars of drug therapy and thename of the patient’s medical practitioner. Apatient for whom sedatives and tranquillisersare being prescribed may have a reduced ca-pacity in adapting to dentures, as may a personsuffering from a protracted chronic disability. Itshould also be noted that many antidepressantsand tranquillisers produce xerostomia. Thiscondition may reduce the physical retentionof a denture and may cause a generalisedsoreness of the denture-bearing mucosa. It hasalso been reported that certain antidepressantsand tranquillisers may adversely affect thetonicity of the facial muscles and may producefacial grimacing and trismus or bizarre tonguemovements.
It can be helpful when taking a medi-cal history to work with a questionnaire tomake certain that no significant aspect is over-looked.

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
82 Prosthetic Treatment of the Edentulous Patient
Figure 7.1 Both patients arewearing complete dentures whichare in occlusion. The man showsobvious signs of a gross loss ofocclusal vertical dimension; thefreeway space is approximately10 mm. On the other hand, thewoman’s facial appearance leadsone to suspect that the occlusalvertical dimension of her dentures isexcessive.
Social history
When entering into a discussion with somepatients, it may be helpful to explain thatone is not being ‘nosy’ but that there areimportant reasons for such an enquiry. Forexample:
� A history of domestic worries may welltie in with the medication that has beenprescribed or with a parafunctional habitwhich is resulting in pain under an existinglower denture.
� If the patient has been widowed, preparingfood and eating alone can well take all theenjoyment out of mealtimes and an unbal-anced diet could lead to tissue changes in theoral cavity.
� Because the clinician has a responsibility forthe health of the patient, it is important toobtain information on risk factors related tooral cancer such as smoking or chewing to-bacco, a high alcohol consumption, a priorhistory of cancer, familial or genetic predis-position. Age on its own is not a risk factorbut exposure to other risks clearly increaseswith age.
ExaminationExamination of the patient
Extra-oral examination of the patient
Simply by talking to the patient, and makingcareful observations at the same time, the clin-ician may obtain important information thatwill help in treatment planning:
� Discrepancy between actual and biological ages.Any discrepancy between the actual age andbiological age should be noted as this canbe important in assessing the likely adaptivecapability, an aspect discussed more fully inChapter 2.
� Skeletal relationship. The skeletal relation-ship of the patient should be assessedbecause this will indicate the appropriateincisal relationship of the planned dentures(Chapter 12).
� Occlusal vertical dimension. The facial appear-ance provides valuable information aboutthe occlusal vertical dimension of existingdentures (Fig. 7.1). If loss of occlusal verti-cal dimension is noted, correction may be re-quired before the provision of new denturesis started (p. 93).

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
Assessment of the Patient 83
� Dental appearance. If the patient already hasdentures, the dental appearance should beevaluated at this stage of the examination. Itis particularly important that the appearanceof the dentures is assessed during speakingand smiling. Features such as inadequate lipsupport or poor appearance of the anteriorteeth should be noted. If the patient has acomplaint regarding the appearance of thecurrent dentures it is essential that the de-tails are carefully recorded when obtainingthe history of the complaint.
� Extra-oral lesions. Inflammation and fissuringat the corners of the mouth (angular stom-atitis) may be present; the significance andtreatment of this condition are described onp. 119.
� Intolerance or other difficulties with the dentures.While the patient is speaking it may be pos-sible to detect any obvious looseness of den-tures, or whether the patient is having diffi-culty in controlling the prostheses.
Intra-oral examination of the patient
The broad objectives of this part of the exami-nation are to determine:
� whether there is any pathology in the mouth(Figs. 7.2a and 7.2b);
� what the prospects are for the new denturesproviding a satisfactory level of comfort andfunction.
Detecting systemic diseaseThe mouth has been aptly described as a mir-ror which reflects the state of health of the in-dividual. When systemic disease develops, thepowerful combination of microorganisms, nor-mal wear and tear, and moisture and warmthpresent in the mouth frequently result in vis-ible changes in the oral tissues before signsof disease are evident elsewhere in the body.Investigation of these changes may allow an
a
b
Figure 7.2 (a) The swelling in the left molar regionshould be reviewed for associated pathology. (b) Aradiograph showed an unerupted third molar.
early diagnosis of the systemic condition to bemade. For example, there may be a change inthe population of papillae on the tongue; thischange occurs first on the tip and sides, theareas of maximum trauma. The filiform papil-lae are progressively lost so that the fungiformpapillae become more noticeable and producethe appearance of a ‘pebbly’ tongue; eventu-ally, the fungiform papillae also disappear andthe tongue becomes smooth (Fig. 7.3). Thesechanges should lead the clinician to suspect de-ficiencies such as iron, vitamin B12 and folicacid. Diagnosis may be confirmed by the appro-priate haematological investigations.
Screening for oral cancerClinicians, because of their training, experienceand equipment, are uniquely qualified to exam-ine the oral cavity thoroughly and to recognise

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
84 Prosthetic Treatment of the Edentulous Patient
Figure 7.3 Reduction in population of filiform andfungiform papillae as a result of a folic acid deficiency.
any features which are outside the range ofnormal variation. Large numbers of peopleare examined dentally each year; the cliniciantherefore plays the central role in screening thepopulation for oral manifestations of systemicdisease. Of particular relevance in the olderpatient with complete dentures is the presenceof oral malignancy. It has been reported that theoral cavity and pharynx combined, constitutethe sixth commonest site for cancer and thatoral cancer is increasing in a number of coun-tries in both the developed and developingworld. Although the overall prevalence of oralcancer is low, 95% of cases, excluding salivarygland tumours, occur in patients who are over45 years of age. Early detection by the clinicianincreases the chance that treatment may affect
Figure 7.4 The ulcer in the upper right canine re-gion has a raised, rolled margin; there was no historyof trauma. Biopsy confirmed a malignant change.
a cure. Any ulceration, change in character ofthe mucosa or swelling, whose presence cannotbe readily explained, should be regarded withsuspicion (Fig. 7.4). In all instances, appropriatesteps such as radiographic examination, biopsyor immediate referral should be undertaken.There is widespread agreement that oppor-tunistic screening for oral cancer should bepart of every dental examination procedure(British Dental Association 2000; Conway et al.2002). There is evidence that this is particu-larly effective in developing countries with ahigh incidence of the disease (Downer et al.2006). However, there is a concern that theindividuals who are at the highest risk tend notto be regular dental attenders and, therefore,additional strategies are needed to also allowscreening of this group (Yusof et al. 2006).
Other assessmentsIf there are no signs of systemic disease, thefindings of the intra-oral examination assume aprimarily local significance by helping to diag-nose the patient’s dental complaint, to formu-late a treatment plan and to determine a prog-nosis. Features of interest are:
� The shape and size of ridges and hard palate.� The depth and width of the sulci, including
the presence of prominent frena.

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
Assessment of the Patient 85
� The degree of compressibility of the denture-bearing mucosa determined by palpation.
� The size of the tongue.� Any pathology such as mucosal inflam-
mation, ulceration, hyperplasia, sinuses orswellings. If pathological conditions of theunderlying bone are suspected, radiographsmust be taken. These conditions, describedin Chapter 9, should normally be treatedbefore starting prosthetic treatment so thata stable and healthy denture foundation isproduced.
� The quality and quantity of saliva. The rele-vance of such observations to the stability ofcomplete dentures is discussed more fully inChapters 4 and 16.
Examination of the dentures
Extra-oral examination of the dentures
The dentures are removed from the mouth anda detailed and systematic extra-oral examina-tion is made of their impression, polished andocclusal surfaces. Any relevant findings arerecorded.
Impression surface� The presence or absence of a post-dam
(p. 153) and palatal relief (p. 162).� Width of borders.� The amount and distribution of plaque,
an important cause of denture stomatitis(Chapter 9). Painting disclosing solution onthe impression surface will help to visualisethe plaque (Fig. 14.10).
� Evidence of adjustments, relines or repairs.� Surface roughness.
Polished surface� Shape and inclination. In essence, is the
shape such that it will allow the muscles tohelp rather than hinder the control of thedenture?
� Condition and general cleanliness of thedenture material.
Occlusal surface� Amount of wear; presence of shiny facets.� Teeth – size, shape and colour.
Intra-oral examination of the dentures
The first point to make in this section is thatthe clinicians’ judgements of the quality ofdentures often do not match the level of sat-isfaction reported by patients. For example,a denture border which is judged clinicallyto be under-extended, may not necessarilyhave led the patient to complain of loosenessbecause the denture foundation is particularlyfavourable. Furthermore, the point needs tobe made that clinicians may well vary in theirjudgements of quality.
This insecurity has prompted the develop-ment of an approach which judges the follow-ing important aspects of upper and lower den-tures (Corrigan et al. 2002):
� Occlusal vertical dimension� Occlusion� Retention of upper denture� Tongue control of upper denture� Stability of upper denture� Stability of lower denture
Occlusal vertical dimensionEvery effort should be made to obtain an ac-curate estimation of the freeway space at thisstage because the result will be of fundamentalimportance both in the diagnosis and in the for-mulation of a treatment plan; the clinical tech-niques for obtaining this information are de-scribed in Chapter 11. However, it should beremembered that an assessment of the freewayspace at this stage may, in some instances, onlybe a rough estimate because it may be impossi-ble to induce a relaxed state at the patient’s firstvisit. Further estimations will be made whenthe occlusion is recorded and will serve to checkon the accuracy of the original assessment.

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
86 Prosthetic Treatment of the Edentulous Patient
OcclusionHaving asked the patient ‘to close gently onthe back teeth’ several times from a relaxedand slightly open position, occlusal contact isjudged to be either satisfactory (when thereis even meeting of teeth and consistent re-turn to an intercuspal position) or unsatisfac-tory (when there is uneven contact, an inconsis-tent return to the intercuspal position or a slidegreater than 4 mm).
Retention of the upper dentureTests of retention are usually only of value inassessing the upper denture as the physical re-tention of lower dentures is often minimal. Twofunctional tests are of particular value for theupper denture:
1. Seat the upper denture and attempt to dis-lodge it by pulling vertically downwardswith the thumb and first finger on the buccalaspects of the right and left premolar teeth.Lack of resistance indicates poor retention.
2. Seat the upper denture and ask the patient toopen the mouth until the incisal separation isabout 2 cm. If this degree of opening causesthe denture to drop, an error in either the im-pression or the polished surface should besuspected.
Tongue control of the upper dentureThis is particularly important because, in its ab-sence, a complaint of looseness when biting ona piece of food is unlikely to be cured (Culver &Watt 1973; Basker & Watson 1988). A cottonwool roll is inserted between the incisors andthe patient is instructed to initially hold the rollgently and then, when instructed, to bite on itas if it were a piece of food. This test can be re-peated three times and a check made on the lastoccasion as to whether or not the tongue hasbeen raised to stabilise the posterior border ofthe denture (Fig. 7.5).
Figure 7.5 From this position the patient is asked tobite on the cotton wool roll. The clinician is in a positionto judge whether or not the tongue has pushed itselfagainst the back edge of the upper denture so as tostabilise it.
Stability of the upper dentureThe upper denture is seated in the mouth andan attempt made to rotate it in the horizontalplane. Any resulting lateral movement of themidline is noted. Some movement is inevitablebecause of the compressibility of the mucosa,but a movement of 3 mm or more either side ofthe midline is an indication of loss of fit or thepresence of a flabby ridge. A similar conclusioncan be drawn if an attempt to rock the dentureacross the midline results in clearly detectablemovement of the prosthesis with the centre ofthe hard palate acting as a fulcrum.
Stability of the lower dentureThis can be judged in four ways:
1. With the upper denture in place to sup-port the muscles of the cheeks, the patient isasked to open the mouth by about 2 cm. Ajudgement can then be made as to whetherthe denture stays on the tissues or has beennoticeably displaced in an occlusal direc-tion. This judgement can be made only ifthe tongue is brought forwards so that itstip lightly contacts the lingual surfaces of theanterior teeth (Fig. 7.6).

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
Assessment of the Patient 87
Figure 7.6 The tongue is in a retruded position andthus it is impossible to assess if the denture is in theneutral zone. The tip of the tongue should touch the lin-gual aspect of the anterior teeth before the judgementis made.
2. The stability of a lower denture can be fur-ther investigated by seeing if it stays seatedon the ridge when the patient is instructed tomove the tongue so that the tip rests gentlyat the angle of the mouth, first one side andthen the other. Lack of tongue space withinthe arch of teeth will readily result in move-ment of the denture (Fig. 7.7).
3. The lower denture is held against the ridgeby a finger and thumb in the incisor re-gion and an attempt is made to move itin an antero-posterior direction. Pronounced
Figure 7.7 The tongue movement has producedmarked instability of the denture. There is inadequatespace for the tongue.
movement is highly suggestive of lack ofextension of the denture base over the all-important pear-shaped pads and into theretromylohyoid fossa.
4. It is also advisable to assess the height of theocclusal plane of the lower denture and de-termine whether it is in such a position thatthe tongue is able to rest on the occlusal sur-face and thus play a part in stabilising thedenture.
Border extensionHaving completed the functional assessmentof the dentures, there will usually be a needto focus on the border extension of the den-tures so as to link functional concerns with de-sign errors. Under-extension of the upper andlower denture buccally, labially and at the post-dam can be determined by direct vision. Over-extension is present if the denture moves oc-clusally when the muscles are gently pulled.Lingual extension is less easy to assess. Ante-riorly a mouth mirror can help, and overex-tension can be inferred if the lower denturelifts when the tongue is raised. A fully bor-der moulded alginate wash impression withinthe denture can be very informative, indicat-ing either over- or under-extension. The cor-rect extension of a denture base is described inChapter 10.
AppearanceHaving completed the functional assessment ofthe dentures, a further assessment of the ap-pearance of the dentures should be made. Thelips can be retracted and features such as ori-entation of the occlusal plane, and the colour,shape and arrangement of the anterior teeth canbe noted. The findings at this stage will supple-ment those obtained during the extra-oral ex-amination of the patient described previously.
Special tests
It may be necessary to take radiographs, or-ganise blood tests, arrange for microbiological

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
88 Prosthetic Treatment of the Edentulous Patient
examination of swabs or smears, or to carry outdiagnostic modifications of existing dentures.The reasons for undertaking any of these pro-cedures are discussed in the relevant sectionsof the book.
DiagnosisBy correlating the findings of the examinationand special tests with the patient’s history, thecause or causes of the complaint should beidentified and recorded. It is important to re-alise that, unless a diagnosis is made, there islittle prospect of solving a patient’s problems byproviding new dentures, and in some cases, it isunwise to embark on such treatment.
Treatment planFollowing the diagnosis, a treatment plan is for-mulated. Possible treatment options include thefollowing:
� No treatment� Preparatory treatment such as denture ad-
justment or a short-term reline (Chapter 8)� Definitive denture modifications such as re-
line, rebase (Chapter 15), repair or cleaning� Replacement dentures
If replacement dentures are to be made, it canbe of great value to write down a ‘shopping list’in the patient’s records that clearly identifiesthose features in the existing dentures whichwill be:
� Modified in the replacement dentures in or-der to overcome the patient’s complaint. Anindication of the nature of the modificationsshould also be included.
� Copied and incorporated in the replacementdentures because these features have provedsuccessful previously. Such written com-ments serve as an invaluable reminder andchecklist during subsequent clinical stages.
There are several approaches to designing andconstructing complete dentures. The clinicianshould make a positive decision at the treat-ment plan stage as to which is appropriate forthe patient:
� Carving record rims. The shape, or design, ofthe dentures may be determined by the clin-ician carving the record rims as described inChapter 11.
� Copy dentures. Where dentures have pro-vided satisfactory service for the patient inthe past, it may be advisable to base the de-sign of replacement dentures on the well-accepted features of the old ones. Althoughsuch an approach is particularly appropriatefor the treatment of older patients who havea reduced ability to adapt, it can also be ofvalue in a number of other clinical situations.A potentially accurate method of maintain-ing the well-accepted features of existingdentures is to use a copy technique (Chap-ter 8).
� Biometric guides. Another approach to de-sign involves the use of biometric guides –measurements from certain anatomical land-marks which allow the denture teeth andbase to be placed in positions similar to thoseformerly occupied by the natural teeth andalveolar bone. The desirability of so doinghas been a source of controversy for manyyears but has received a considerable mea-sure of support. Anatomical guidelines havenow been researched which assist the clin-ician in trying to achieve this aim (Chapter10).
� Functional neutral zone impression. Whenthere are particular problems in achievingstability of a lower denture – for example, ifthere is abnormal muscular activity or intra-oral anatomy – the clinician can record theneutral zone by getting the patient to moulda soft record rim into a position of stabil-ity between the tongue and cheeks and lipsby means of swallowing and speaking. Alower denture is then produced whose shape

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
Assessment of the Patient 89
Tonguecrowding
Inefficientfacial seal
Crest of residual maxillary ridge
Crest of residual mandibular ridge
Position formerly occupied by the naturalteeth and supporting bone
Figure 7.8 Pattern of resorptionin the maxilla and mandible follow-ing loss of the natural teeth. A mech-anistic upper denture (heavy outline)has been produced with teeth on thecrest of the residual ridge. Occlu-sion with the lower denture has beenachieved by producing a cross-biteon the patient’s right and excessivelingual placement of the lower teethon the left.
is derived from the neutral zone impression.This clinical technique has been shown toenhance the tongue’s retentive ability overa conventional design (Miller et al. 1998).Details of this technique are described inChapter 12.
All these approaches to complete denture de-sign are based on sound clinical principles andrequire an adequate prescription to be sent bythe clinician to the laboratory. In the absenceof such a prescription, the technician may betempted to produce a denture design which isessentially mechanistic with the teeth placed onthe crest of the ridge. The greater the amountof resorption that has occurred, the greater theproblem this approach can create. This is be-cause the pattern of bone resorption of theresidual ridges is not uniform. For example, inthe maxilla the bone loss is predominantly fromthe buccal and labial aspects of the ridge, caus-ing its crest to progressively migrate palatally.Setting the upper teeth on the crest of the ridge
as shown in Fig. 7.8 has the following undesir-able consequences:
� Poor facial appearance due to inadequate lipand cheek support.
� Reduced physical retention associated withan inefficient or absent facial seal.
� Encroachment on tongue space, resultingin denture instability, tongue soreness andinterference with tongue function duringspeech and food transport.
� Problems in achieving a satisfactory occlusalrelationship with the lower denture. For ex-ample, in Fig. 7.8 the alternatives are to ac-cept a posterior cross-bite or place the lowerteeth so far lingually that instability of thelower denture is bound to result.
In view of these undesirable consequences, itcan be argued that a mechanistic approachwhich results from the clinician failing to sup-ply a design prescription to the laboratory isan avoidance of professional responsibilities by

P1: JZP Trim: 246mm X 189mmc07 BLBK351-Basker January 18, 2011 13:13 Printer Name: Yet to Come
90 Prosthetic Treatment of the Edentulous Patient
the clinician, who alone has the clinical infor-mation necessary to make an informed decisionon the design.
PrognosisThe findings of the history and examinationwill enable the clinician to assess the degree ofsuccess the proposed line of treatment is likelyto achieve. If problems are anticipated, theyshould be explained to the patient before treat-ment proceeds. The patient is then more likelyto accept and to cope with the unavoidable lim-itations of the new dentures.
References and additionalreadingBasker, R.M. & Watson, C.J. (1991) Tongue control
of upper complete dentures. British Dental Journal,170, 449–50.
Boyle, P., Macfarlane, G.J., Maisonneuve, P., Zheng,T., Scully, C. & Tedesco, B. (1990) Epidemiology ofmouth cancer in 1989: a review. Journal of the RoyalSociety of Medicine, 83, 724–30.
British Dental Association (2000) Opportunistic OralCancer Screening. BDA, London.
Conway, D.I., Macpherson, L.M.D., Gibson, J. & Bin-nie, V.I. (2002) Oral cancer: prevention and detec-tion in primary dental healthcare. Primary DentalCare, 9, 119–23.
Corrigan, P.J., Basker, R.M., Farrin, A.J. Mulley, G.P. &Heath, M.R. (2002) The development of a method
for functional assessment of dentures. Gerodontol-ogy, 19, 41–5.
Culver, P.A.J. & Watt, I. (1973) Denture movementsand control: a preliminary study. British DentalJournal, 135, 111–6.
Downer, M.C., Moles, D.R., Palmer, S. & Speight,P.M. (2006) A systematic review of measures of ef-fectiveness in screening for oral cancer and pre-cancer. Oral Oncology, 42, 129–31.
Duxbury, A.J., Leach, F.N. & Smart, T.E. (1982) Oraldyskinesia induced by Tryptizol. Dental Update, 9,299–302.
Lamey, P.J. & Lewis, M.A.O. (1999) A Clinical Guideto Oral Medicine, 2nd edn. British Dental Journal,London.
Likeman, P.R & Watt, D.M. (1974) Morphologicalchanges in the maxillary denture bearing area. BritishDental Journal, 136, 500–3.
Miller, W.P., Monteith, B. & Heath, M.R. (1998)The effect of variation of the lingual shapeof mandibular complete dentures on lingualresistance to lifting forces. Gerodontology, 15,113–19.
Watt, D.M. (1977) Tooth positions on com-plete dentures. Journal of Dentistry, 6,147–60.
Watt, D.M. & Likeman, P.R. (1974) Morphologicalchanges in the denture bearing area following theextraction of maxillary teeth. British Dental Journal,136, 225–35.
Yusof, Z.Y., Netuveli, G., Ramli, A.S. & Sheiham, A.(2006) Is opportunistic oral cancer screening bydentists feasible? An analysis of the patterns ofdental attendance of a nationally representativesample over 10 years. Oral Health and PreventiveDentistry, 4, 165–71.

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
8The Relevance of Existing Dentures
This chapter makes the following key points:
� Existing dentures are often invaluable for di-agnosis and treatment planning. For this athorough assessment of the dentures, as de-scribed in Chapter 7, is essential. Most exist-ing dentures, whether or not they have beenworn successfully, can provide important in-formation for all stages of treatment. There-fore they should be referred to regularly astreatment proceeds.
� Existing dentures are often very useful whencarrying out certain treatment procedures.
� Most complete denture provision is con-cerned with the construction of replacement,rather than first dentures.
� The copy technique is an effective way oftransferring design information accuratelyfrom existing to replacement dentures.
� As with most prosthetic treatments, goodclinician/dental technician teamwork is ofthe utmost importance in achieving a suc-cessful outcome.
To summarise, existing dentures can play animportant part in the following:
� Diagnosis� Treatment planning� Preparation of the mouth� Impression procedures� Recording the jaw relationship� Denture copying
DiagnosisA thorough assessment of a patient’s denturehistory and of the dentures themselves will pro-vide key information which leads to a sounddiagnosis and an effective treatment plan. Pa-tients requesting replacement dentures fall intothree broad categories.
Those wearing immediate dentures
Patients requesting replacement of their imme-diate dentures usually do so because the post-extraction resorption of bone has led to a loss ofretention and stability. Apart from a desire forbetter fitting dentures, many of these patientsare anxious that the appearance of the originaldentures should be maintained. The clinician
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
91

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
92 Prosthetic Treatment of the Edentulous Patient
needs to satisfy these demands if a successfuloutcome is to be achieved. Improving the fit isseldom a major problem, but considerable careis needed to maintain the other well-acceptedcharacteristics, such as position and arrange-ment of the artificial teeth. This challenge maybest be met by using a copying technique, asdescribed later in this chapter.
Those whose most recent dentures havebeen worn successfully for a significantperiod of time
It is important when providing new denturesfor those patients whose previous dentureshave been satisfactory for a number of yearsthat the features considered to have contributedto that success are incorporated into the newprostheses. Failure to conform to this principle,which is particularly relevant to the treatmentof older patients, who may adapt to changevery slowly or be unable to adapt, is likelyto lead to the construction of dentures whichare poorly tolerated. Such failures account fora proportion of patients in the third group,who have experienced persistent dentureproblems.
Those with dentures that havecaused persistent problems from thevery beginning
For those patients with chronic denture prob-lems, it is again vitally important to establish anaccurate diagnosis. This is best achieved by ask-ing the patient to bring in all sets of dentures intheir possession so that the previous attemptscan be analysed.
Within each of the three groups described,clinical situations may occur in which the clini-cian observes a shortcoming in the denture de-sign which has not troubled the patient. Thereis then the dilemma – should the shortcomingbe corrected or not? This can be a very diffi-cult question to answer and possible pitfalls arediscussed more fully under ‘Category (f)’ on
p. 103. It is impossible to be dogmatic aboutthis, particularly when treating older patients.In all instances, the clinician should considerwhether it is likely to be possible to make suc-cessful new dentures if the error is retained. Ifit is decided to make an alteration, then it isessential to explain the reasons for this to thepatient.
Treatment planHaving assessed the patient’s dentures and re-lated problems, the treatment plan is likely tofall into one of the following categories:
� Make temporary modifications to the exist-ing dentures to test a diagnosis.
� Make permanent modifications to the exist-ing dentures (e.g. rebase or modify the oc-clusion).
� Construct replacement dentures using con-ventional techniques.
� Construct replacement dentures using acopy technique for one or both dentures.
� No treatment, or referral for specialist ad-vice. Such a decision may be made when theclinician assesses that new dentures will notovercome the patient’s complaint or wherea diagnosis cannot be established with con-fidence, and thus there is a real risk of newdentures being no more successful than anyof the existing ones.
Preparation of the mouthBefore commencing any of the treatment planslisted above, it is often necessary to carry outpreparatory treatment to improve the condi-tion of the mouth so that it is in the optimumstate to receive the new prostheses. The exist-ing dentures are often of value in carrying outthis preparatory treatment – for example, whentreating inflammation of the denture-bearingmucosa or when modifying an unsatisfactoryjaw relationship.

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
The Relevance of Existing Dentures 93
Treatment of inflammation of thedenture-bearing mucosa
The commonest causes of this condition aretrauma from an existing denture and the pro-liferation of microorganisms on the impressionsurface of the denture. Denture trauma maybe the result of an ill-fitting denture, an unbal-anced occlusion, or lack of freeway space.
It is important that the inflammation of themucosa is resolved before final impressions forthe new dentures are taken. If not, the better fit-ting and more hygienic new dentures are likelyto affect some improvement in the condition.Then, as the inflammation resolves, the shape ofthe denture-bearing mucosa will change caus-ing the fit of the new dentures to deteriorate,re-establishing one of the causative factors ofthe original inflammation. Although the sim-plest method of treatment is to ask the patientnot to wear the old dentures, such advice is un-acceptable to the majority of patients. In suchcases the dentures need to be corrected beforethe definitive treatment is started.
The fit of a denture can be improved quicklyand effectively by temporarily relining with ashort-term soft lining material (p. 234).
Occlusal imbalance can be corrected eitherby adjusting the occlusal surface through selec-tive grinding or by applying a layer of cold-curing acrylic to the posterior teeth, providedthis addition leaves an adequate freeway space.
Methods of eliminating infection by mi-croorganisms are described on p. 117.
Modification of an unsatisfactoryjaw relationship
Some patients still believe that once completedentures have been provided there is no needfor further treatment. This is borne out by a na-tional survey of adult dental health in the UKwhich included information on the age of den-tures being worn by edentulous people (Walker& Cooper 2000). A total of 39% were wear-ing a denture provided at least 20 years ago.
Added to this was the fact that although 41%of complete denture wearers had some prob-lem, only 13% were planning to visit a den-tist. As a result, cases are seen where, throughlack of maintenance, there have been consider-able changes in occlusal vertical dimension andin the intercuspal position. Severe wear of theacrylic occlusal surface and resorption of alveo-lar bone leads to a situation where the freewayspace may be 10 mm or more. Patients seekingnew dentures at this advanced stage of occlusalderangement may make such statements as ‘Ican’t chew my food so well’, or ‘My teeth don’tshow as much as they used to’. Little imagina-tion is required on the part of the clinician to ap-preciate the basis of their complaints (Fig. 8.1).
Figure 8.1 The patient is occluding on his completedentures. Lack of maintenance has led to gross lossin occlusal vertical dimension and protrusion of themandible.

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
94 Prosthetic Treatment of the Edentulous Patient
However, patients are not usually aware of theproblems produced in allowing the occlusion todeteriorate to such a degree.
There are two major uncertainties concern-ing the jaw relationship when providing re-placement dentures:
1. What increase in occlusal vertical dimension islikely to be tolerated? If one attempts to re-duce the freeway space to 3 mm in situ-ations like those described above, the oc-clusal vertical dimension has to be increasedby 7 mm or more. This may exceed a pa-tient’s ability to adapt. For example, sucha magnitude of change can result in in-creased masticatory stress being transmittedto the denture-bearing mucosa which mighthave atrophied to the extent that it is nolonger able to accept such stress. Further-more, a patient possessing a generous free-way space has been able to eat large mouth-fuls of food without having to open themandible much beyond the rest position. Ifthe same dietary habits continue once thenew dentures are fitted, difficulties in eat-ing are likely and the increased opening ofthe jaw to accommodate the large mouth-fuls may well produce pain in the muscles ofmastication.
2. What is the correct jaw relationship in the hori-zontal plane? The reduction in occlusal verti-cal dimension and the unbalanced occlusionresult in protrusion of the mandible. Thismandibular protrusion is partly anatomicaland partly habitual and generally makes itdifficult, sometimes impossible, to record theretruded position. A reduction in the appar-ent protrusion of the mandible is, to somedegree, automatic on restoration of the oc-clusal vertical dimension, because the hinge-like nature of the temporomandibular jointcauses the chin to move posteriorly as theocclusal vertical dimension is increased (Fig.8.2). Correcting the habitual element is usu-ally a more gradual process. If the protrusivehabit is not corrected before constructing the
Figure 8.2 Movement of the chin posteriorly as theocclusal vertical dimension is increased.
new dentures the subsequent gradual reduc-tion in the protrusive posture will result ina long programme of occlusal adjustment tothese new dentures.
The uncertainties may be minimised bymodifying the old dentures. The occlusal ver-tical dimension is increased by adding a layerof cold-curing acrylic resin to the occlusal sur-face of one of the dentures (Fig. 8.3). The newocclusal pattern initiates the breakdown of thehabitual protrusion of the mandible as well asallowing an assessment of the patient’s abilityto accept the chosen increase in occlusal verti-cal dimension and the change in appearance.The temporary occlusal surface can be mod-ified to accommodate the gradual change inthe jaw relationship. New dentures can then beconstructed when it becomes apparent that theplanned increase in vertical dimension is ac-ceptable and the protrusion of the mandible hasbeen corrected.

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
The Relevance of Existing Dentures 95
Figure 8.3 Occlusal vertical dimension correctedby the addition of a layer of cold-curing acrylic resinapplied to the occlusal surface of the lower denture.
Impression proceduresUnder certain circumstances an existing lowerdenture may be used as an impression tray toobtain the following types of master impres-sion:
� Functional impression� ‘Wash’ impression� Copy of the existing impression surface of
the old denture
Functional impression
A functional impression is one that is obtainedby placing in the denture an impression ma-terial that exhibits plastic flow over a periodof several hours. During this period the den-ture is worn and subjected to functional loads,e.g. during mastication. As a result the impres-sion material records the shape of the denture-bearing tissues during function. This contrastswith the conventional impression techniquesdescribed in Chapter 10, which are in effect‘snapshots’ of the shape of the denture-bearingtissues obtained at a single point in time. Suchimpressions are produced under conditions ofloading applied by the clinician as the tray is
seated which bear little, if any, relationship tothose occurring in normal function.
An additional advantage of the functionalimpression technique is that it allows an assess-ment of the patient’s reaction to a new impres-sion surface before proceeding with definitivetreatment. For example, a patient may presentwith a history of persistent discomfort beneatha denture that has not responded to previousadjustments. If, after a careful evaluation of thesituation, the clinician concludes that the prob-lem is due to errors in the impression surface, itcan be helpful to the clinician and reassuring tothe patient to be able to test the hypothesis be-fore being committed to definitive treatment. Inthe case described this can be achieved by cor-recting the fit of the denture with a short-termsoft lining material. If the patient commentsfavourably on the result at the next visit, theoperator has gained valuable evidence thatthe new impression surface is compatible withthe comfortable, normal function and that a re-base or a replacement denture made to this newsurface is likely to be equally well tolerated. Ifthe patient does not comment favourably on theresult the clinician can look for other possiblecauses of the complaint and, if necessary, re-move the ineffective functional impression ma-terial. Using this approach, one is following thedictates of the saying, ‘The proof of the puddingis in the eating’. It is very important, however,to sound a note of caution here. There are sit-uations in which a patient has persistent prob-lems with a number of dentures in which it maybe very unwise to alter the existing dentures inany way. This is discussed further in the section‘Category (f)’ on p. 103. The short-term soft lin-ing materials used for functional impressionsare discussed more fully in Chapter 16.
The ‘wash’ impression technique
In some instances an old denture can act as avery satisfactory special impression tray. Thisavoids the need for a separate appointment totake a preliminary impression in a stock tray

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
96 Prosthetic Treatment of the Edentulous Patient
b ca
Zinc oxide
impression paste
Alveolar bone
Mucosa Stone model
Figure 8.4 (a) Undercuts not removed from the impression surface. (b) Mucosal compressibility allows removalof the denture from the mouth. (c) Subsequent removal from the cast is impossible without damage.
in order to construct a special tray. However,it must be appreciated that corrections of anyover- or under-extension of the old denture willbe required before taking the master impres-sion. If it is necessary to increase the extensionof the border by more than 2 mm, it is advisableto use one of the rigid border-trimming materi-als which are discussed on p. 145.
It will be appreciated that if there are signifi-cant undercuts in the impression surface of thedenture they have to be removed before tak-ing the impression for the reason described inFig. 8.4. In most cases it is unwise to tamperwith such a denture in this way for fear ofmaking it too loose or uncomfortable to wear.Fortunately, most of the dentures for whichthe technique might be considered appropriatewill have been originally constructed on well-resorbed ridges where undercuts do not exist.
The impression surface of the dentureshould be dried thoroughly to ensure that theimpression material adheres firmly to the den-ture. Either a low viscosity silicone impressionmaterial or a zinc oxide-eugenol impression
paste may be used to record the detail of thedenture-bearing mucosa. Both materials are ac-curate when used in thin section but the for-mer has the advantages of being tasteless, elas-tic and relatively clean to use. The denture isreturned to the patient after the cast has beenpoured and the impression material has beenremoved.
Copying the existing impressionsurface of the lower denture
There are occasions when a new lower denturehas been provided to replace an old ill-fittingone and the patient returns to the surgery withthe comment that ‘the old denture was muchmore comfortable’.
The impression surface of the old denturemay only contact the mucosa along its bor-ders (Fig. 8.5). However, the reactions of the pa-tient and the appearance of the mucosa showthat this state of affairs is perfectly acceptable.Why do the reactions of the patient differ fromthe evidence of the clinical examination? It is

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
The Relevance of Existing Dentures 97
Figure 8.5 The impression surface of a lower den-ture which still provides comfort and stability after 10years of wear. The border areas are well polished bycontinual contact with the border tissues. The middle ofthe impression surface is covered with calculus and isheavily stained, indicating that the denture no longerfits the tissues in that area.
because the denture-bearing tissues have grad-ually adapted to the progressive loss of fit of theold denture and the uneven distribution of loadthat is the result. It is also likely that the pro-gressive loss of fit has been adequately compen-sated by the muscular control of the denture.
If a new denture is constructed with an accu-rate impression surface, the masticatory forceswill be transmitted to tissues which have notbeen loaded for a long time. The mucosa over-lying the ridge may no longer be able to ac-cept the forces, so discomfort is experienced.Therefore, if one is faced with an old denturewhose impression surface is well tolerated bythe patient and which has not caused mucosaldamage, an option which should be seriouslyconsidered is to pour dental stone directly intothe impression surface and construct the newdenture on the cast produced. In this way thecomfortable fit of the old denture will be repro-duced in the new one.
Recording jaw relationsIf replacement dentures are being made byconventional techniques, reference to previ-
ous dentures is particularly rewarding whenrecording jaw relations. During this clinicalstage, the clinician produces a blueprint, forexample, by shaping the record rims so thatthe dental technician can construct denturesthat faithfully follow the design concepts de-cided at the treatment planning stage. In thecase of a patient requiring replacement den-tures, the clinician has the advantage of aprevious blueprint, the old dentures, whichwill yield valuable information on featuresto be copied or changed in the replacementdentures.
Assessing occlusal verticaldimension
Simply determining the occlusal vertical di-mension by reference to the rest position alonecan be rather imprecise. Thus, it is advisable totry to improve the reliability of this assessmentby using several indicators. These include fa-cial appearance, speech and the patient’s expe-rience with existing dentures.
If it is apparent from the patient’s commentsand the clinician’s own observations that theexisting dentures have an adequate freewayspace, the occlusal vertical dimension can berecorded and copied in the new dentures.
On the other hand, if the patient complainsof symptoms which signify a lack of freewayspace and this is confirmed by clinical as-sessment, the clinician can still record the oc-clusal vertical dimension and then use the re-sult for comparative purposes to ensure thatthe height of the record blocks is reduced by anamount sufficient to provide the required free-way space.
Where there is excessive freeway space, itmay be advisable to correct this on the old den-tures by adding a resin onlay, as described pre-viously. Then, when the occlusal vertical di-mension for the new dentures is determined, itis possible to refer directly to the successfullymodified old dentures.

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
98 Prosthetic Treatment of the Edentulous Patient
Shaping the upper record block
When replacing an existing upper denturewhich has provided several years of satisfac-tory wear, it is usually advantageous to carvethe record block to a shape very similar to thatof the denture so that the key details of de-sign are passed on to the dental technician forincorporation into the new prosthesis. Partic-ular attention should be paid to the followingaspects.
Shape and width of the dental arch,together with its relationship to theunderlying ridge
The shape and width of the dental arch de-termine the amount of tongue space withinthe confines of the upper denture. As thetongue is accustomed to functioning within agiven space, a reduced space on the replace-ment denture is liable to induce speech diffi-culties, problems when manipulating a bolusof food, a sore tongue and a general difficultyin adapting to the new shape of the denture.The well-accepted shape of the old denture isconveniently reproduced by first assessing theoverbite–overjet relationship of the buccal andlabial segments on the old dentures. Then theupper record block is carved until, on occludingwith the old lower denture in the mouth, thesame relationship is produced. This procedureestablishes the overall width of the dental arch.The palatal aspect of the record block is thenadjusted to produce an occlusal table whichis similar in width to that of the old denture(Fig. 8.6).
Labial contour and lip support
The labial contour of the upper denture deter-mines the amount of support provided for theupper lip. If the lip support provided by the ex-isting upper denture is acceptable, it is usuallyappropriate to shape the labial aspect of the up-per record block to provide the same amount of
support. The lip support provided by an upperrecord block is the product of three factors:
� The position of the incisal edge in the hori-zontal plane,
� The position of the incisal edge in the verti-cal plane,
� The inclination of the labial surface of therecord rim.
The first two factors can be controlled accu-rately if the incisal relationship on the previousdentures is copied by following the method ofshaping the upper rim as described previously.
An alternative and effective way of estab-lishing the position of the incisal edge in thevertical plane is to measure the distance on theexisting denture between the incisive papillaand the incisal edge with a specially designedgauge (Fig. 8.7). With the denture resting on thetable of the gauge, and the locating needle po-sitioned in the concavity produced by the inci-sive papilla, the relationship of the central in-cisors in both horizontal and vertical planes canbe read on the scales attached to the gauge. Therecord rim is then shaped and the relationshipof its midline to the incisive papilla is checkedon the gauge.
Level and orientation of theocclusal plane
The level and orientation of the occlusalplane are critical for both the appearance andthe function of dentures. The patient’s experi-ence with the existing dentures will again pro-vide invaluable information on whether or notthe occlusal plane is satisfactory. If the experi-ence has been a happy one the level of the oc-clusal plane can be reproduced by shaping therecord blocks as described above. If there havebeen problems with the existing dentures thatcan be attributed to the positioning of the oc-clusal plane then reference to the old dentureswill allow measured changes to be introduced.

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
The Relevance of Existing Dentures 99
Previous dentures
Upper record block adjusted to lowerdenture
Lower recordblock adjusted toupper dentureTongue
space
Overallarch width
a
b
c
Figure 8.6 Procedure for repro-ducing the overall arch width and thetongue space on replacement den-tures: (a), (b) and (c) illustrate the con-secutive stages of the procedure.
Shaping the lower record block
It is essential that adequate tongue space is pro-vided within the confines of the lower dentureso that tongue function is unimpaired and thetongue can help rather than hinder the stabil-ity of the prosthesis. To maintain such a spacewhen replacing a well-tolerated lower denture,the following aspects must be borne in mindwhile shaping the lower rim:
� The shape of the dental arch and its relation-ship to the underlying ridge;
� The width of the occlusal table;� The height of the occlusal plane.
The method of shaping the upper record blockhas already been described. Continuing thisprocess allows the transfer of the characteristicsof the arch width and occlusal width of the oldlower denture to the rim (Fig. 8.6).
If the replacement dentures are being madeto a similar occlusal vertical dimension as theold denture, and the height of the upper rim hasbeen correctly established, the desired height of

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
100 Prosthetic Treatment of the Edentulous Patient
Figure 8.7 The incisal relationship measured in ver-tical and horizontal planes with an Alma gauge (seetext for further details).
the occlusal plane will be determined automati-cally once the lower rim is adjusted to the upperrim.
On many occasions, however, it is neces-sary to increase the occlusal vertical dimen-sion to compensate for wear of the old occlusalsurfaces and resorption of the alveolar bone,which allows the lower denture in particular tosink.
Should the increase be made on the upper orlower rim or shared between both? Each clinicalcase must be treated on its merits when makingsuch a decision. It is necessary to have a clearidea of the magnitude of change required andto decide whether such an increase, if addedto the upper rim, will improve or detract fromthe appearance of the patient or, if added to thelower rim, will so increase the height of the oc-clusal plane that the stability of the lower den-ture will be impaired. However, the patternsof bone resorption occurring in the upper andlower denture-bearing areas differ and it is usu-ally the lower denture that has sunk most as aresult. The upper denture benefits from contin-ued support from the hard palate, which is rel-atively stable. Therefore, if the upper occlusalplane is to be kept unchanged and the lowerocclusal plane is restored to its former level itis the lower denture that most commonly hasto be increased in height.
Selecting artificial teeth
Unless careful thought is given to this very im-portant matter, the time given to the other as-pects of denture construction is likely to bewasted because if incorrect choices are madethe patient may reject the new dentures on thegrounds of an unacceptable change in appear-ance. Decisions to be made at this stage con-cerning the artificial teeth are about the:
� Shade� Mould� Material� Arrangement
When choosing the shade and mould of the up-per anterior teeth, it is naturally very importantto obtain the patient’s thoughts on the appear-ance of the existing dentures. If, as a result ofdiscussion, it is planned to maintain a similarappearance with the new dentures, it is neces-sary to choose the same or similar mould andshade for the upper anterior teeth. By takingan impression of the teeth of the old denture, itis possible to furnish the technician with a castwhich provides guidance as to the arrangementof the teeth. However, it must be rememberedthat the cast only indicates the relationship be-tween the artificial teeth and does not show theposition of these teeth in relation to the under-lying ridge. This latter relationship can only beobtained by correctly shaping the record rim.
There are occasions, of course, where it isnecessary to alter the mould, shade or arrange-ment of the existing teeth. For example, thecrown length may have been severely reducedby occlusal wear or the colour may have beenaltered by bleaching or staining. There is noproblem if the patient has recognised thedeterioration and requests an improvement.However, if the clinician is the first personto notice this state of affairs, it is importantto explain and demonstrate the reason for aproposed change very carefully. If the groundis well prepared for an alteration in appearance

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
The Relevance of Existing Dentures 101
and the patient’s full agreement has beenobtained, the change is likely to be accepted.It is particularly important to warn the patientthat members of the family or close friendsmay comment on a change in facial appearanceor even, tactlessly, enquire whether new den-tures have been provided. Such comments arecapable of turning the patient against the newdentures unless the ground has been preparedadequately in advance.
Positioning the posterior border ofthe upper denture
The clinician will normally wish to position theposterior border of the upper denture at the vi-brating line. However, if an existing denture isunder-extended in this region there may be un-certainty as to whether the patient can toleratethe desired correction of the under-extension.Under such circumstances, if a fully extendednew denture is fitted which subsequently can-not be tolerated, the palate of the replacementdenture will have to be shortened. As a result,the posterior palatal seal will be lost and the re-tention of the denture reduced. As an insuranceagainst this eventuality it is a wise practice toproduce two post-dam lines, one in the positionof that on the old denture and one at the vibrat-ing line. If, after wearing the new denture for afew days, the patient reports that the new po-sition of the posterior border is intolerable, theextension of the palate can be cut back to theold post-dam line without the danger of break-ing the continuity of the border seal.
Denture copying – clinicalindicationsSo far in this chapter, discussion has been re-stricted to ways in which existing dentures canbe used as a guide in the construction of re-placement prostheses by conventional clinicalprocedures. However, none of these methodsallow the features of an existing denture to becopied exactly. The ability to do this can be ex-
tremely useful, particularly in the treatment ofolder patients.
With increasing age, there is a progressivereduction in the ability to learn the new pat-terns of muscular behaviour upon which thesuccessful control of complete dentures largelydepends. An older person may therefore havedifficulty in controlling a replacement dentureif its shape differs from that of the old one.As more older patients are likely to requirereplacement dentures, a technique for copyingthe shape of dentures and so avoiding theseproblems of adaptation becomes increasinglyvaluable.
It must be stressed that it is rarely appropri-ate to copy all aspects of an old denture exactly.Strictly speaking therefore, ‘copy technique’ issomething of a misnomer. Usually the methodis used to copy selected aspects of denture de-sign, which the clinician judges to be importantto the success of treatment, while correctingother aspects which are considered to be un-satisfactory. For example, the overall shape ofthe dental arches and polished surfaces may becopied while a loss of fit and a worn occlusionare corrected.
The appropriate clinical work is undertakenon a copy of the old denture. This copy maybe described as the copy template. The finishedproduct becomes the copy denture.
Indications for copying dentures
It cannot be overemphasised that the correct ap-plication of a copying technique depends uponan accurate diagnosis, which itself is dependentupon a careful evaluation of the three surfacesof the existing denture. This examination al-lows a decision to be reached on the adequacyor otherwise of each surface and thus whetheror not a copying technique is a feasible propo-sition, and, if it is, how best to employ thattechnique.
In general terms, an assessment of the threesurfaces will allow the dentures to be placedinto one of the categories shown in Table 8.1.

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
102 Prosthetic Treatment of the Edentulous Patient
Table 8.1 Assessment of the adequacy of the three surfaces of the existing denture.
Polished surface Occlusal surface Impression surface Category
a
b
c
d
e
f
g
KEY Satisfactory Questionable Unsatisfactory
Category (a) – all denture surfacessatisfactory
In this category, where all the denture surfacesare satisfactory, is the patient who is perfectlyhappy with existing dentures but wishes tohave the added security of a ‘spare set’. Thecopying technique may be used to produce theextra dentures.
Category (b) – deficiencies in theimpression surface
Where an error is found only on the impres-sion surface, the patient’s complaint is normallybest treated by relining or rebasing the denture(Chapter 15).
Category (c) – deficiencies in theocclusal surface
If a patient’s complaint can be localised to asmall defect on the occlusal surface, treatment
may involve simple occlusal adjustment. If thedefect is the result of general occlusal wear ofposterior teeth, it may be advisable to avoidmaking new dentures, especially when treat-ing patients whose advanced age and poor stateof health suggest that there are advantages inreducing the number and complexity of treat-ment visits. Instead, the occlusal relationshipcan be recorded, the dentures articulated andthe worn teeth replaced by new ones whichare positioned in the corrected occlusal rela-tionship and ultimately attached to the denturebase with cold-curing resin.
Category (d) – deficiencies in theimpression and occlusal surfaces
This category is perhaps the most common onewhere, over the years, there has been progres-sive wear of the occlusal surfaces and loss of fitas a consequence of bone resorption. A copy-ing technique may be the ideal approach whenproviding new dentures that eliminate these

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
The Relevance of Existing Dentures 103
faults. In this way, the well-accepted overallshape of the polished surface can be accuratelyretained. The clinical and technical stages re-quired to deal with this situation will be de-scribed later in the chapter.
Category (e) – deficiencies in thepolished surface
If it is concluded that a major error exists in thepolished surface and that the denture is not po-sitioned in the neutral zone, there is unlikely tobe an indication for employing a copying tech-nique. Having said this, a case can be argued fora modified copy technique in certain circum-stances. For example, if a complaint of a looselower denture is judged to be due to the loweranterior teeth being positioned too far labially,the desired change can be made on the waxreplica teeth of the copy template and the ef-fect of that change can be judged in the mouth.If the result is a more stable denture, the newwell-defined prescription can be passed to thelaboratory for the construction of trial dentures.An example whereby a copy technique allowschanges in overall shape to be carefully con-trolled is shown in Figs. 8.8a–d.
Category (f) – the chronic denturepatient with multiple deficienciesin the dentures
The typical scenario in this category is the pa-tient who has experienced problems with manydentures and who is just about managing towear a set which might be described as theleast unsatisfactory of the collection. The clini-cian might conclude, not unreasonably, that ob-vious faults with the dentures are the cause ofthe problems and be tempted to try to correctthem by adjusting the troublesome dentures.However, such a course of action can be mis-guided and a shortcut to disaster because, insuch cases, it can never be guaranteed that thecorrections will achieve the hoped-for result.They may even, as far as the patient is con-
cerned, make things worse. The very difficultsituation then arises of the patient who was justabout managing with just one of the many setsof problematic dentures and now cannot man-age any of them. Unfortunately, it is not usuallypossible to save the day by undoing the alter-ations that have failed in an attempt to returnthe denture to its original state.
Such a catastrophe can be avoided if the olddentures are first copied without any correc-tions being carried out. The copy dentures arethen modified as appears to be appropriate andworn for a trial period. If the patient reportsthat the problems have been eliminated all iswell and good. However, if the modificationsdo not work the patient still has the originaldenture to fall back on, so at the very least noharm has been done.
Category (g) – the older denture patientwith deficiencies in the impression andocclusal surfaces
The patient with the following characteristicsfalls into this category:
� Older, and judged by the clinician to havea very limited ability to adapt to majorchanges in denture shape.
� Wearing dentures which have been success-ful for many years, but which have grad-ually deteriorated to the point where theynow have a combination of faults creatingproblems for the patient.
A ‘one-step’ approach to the correction of thedenture faults by providing new dentures mayfail because of the very limited ability of thepatient to adapt to the relatively substantialchanges. This problem might be avoided byintroducing the changes gradually. For exam-ple, the occlusal vertical dimension can be in-creased over a period by the repeated additionof small increments of cold cure acrylic resinto the occlusal surfaces. A new increment ofresin is not added until the patient has adapted

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
104 Prosthetic Treatment of the Edentulous Patient
a
b
c d
Figure 8.8 (Continued)

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
The Relevance of Existing Dentures 105
successfully to the previous one. Once the de-sired endpoint has been reached, the dentureswith all their additions look rather like a patch-work quilt (Fig. 8.9). The copy technique canthen be used to convert the corrected but un-tidy old dentures into the replacements.
To copy or not to copy?
In concluding this section, it should be stressedthat a copying technique is but one approachto treatment – albeit a most valuable one.In general terms, the older the patient, thestronger the reasons for using the technique. Infact, this method of treatment may prove to bethe only way of realising success for a patientwhose powers of adaptation have deterioratedmarkedly. However, the copy technique mustnot be regarded by either clinician or dentaltechnician as a shortcut to denture constructionwhere relatively little care is needed. In fact,unless the decision to use the method is basedon a sound diagnosis, and the clinical andtechnical procedures are undertaken with thegreatest care, the course of treatment is highlylikely to fail.
If the copy technique is used with care, acomprehensive prescription for the design of
←--------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
Figure 8.8 (a) This woman had worn the same set of dentures for many years. She requested replacementswhich would fit more satisfactorily and which would provide more support for her face. (b) A radiograph confirmedthe extensive resorption of the lower ridge. Additionally, the upper ridge was flabby. The retained lower thirdmolar was an incidental finding and did not require surgical extraction as it was causing no symptoms. Theprosthetic risk was that if a significant increase in the occlusal vertical dimension was introduced and the dentalarches expanded to support the facial muscles the resulting increase in the bulk of the new dentures would makethem unstable. As part of the assessment, wax was added to the old dentures to mimic the changes that might bemade. The patient was asked her opinion on the new appearance and whether she had noted any increase inlooseness of the dentures. As she made no adverse comments it was concluded that the proposed changes werefeasible. (c) Copy templates were made and wax was added to them as in Figure 2.1. This procedure ensuredthat changes to the denture shape were made in a controlled manner and that a detailed prescription was givento the dental technician. The trial denture stage was a routine matter. Wash impressions were taken in upper andlower copy templates before returning them to the laboratory for processing. (d) The finished copy dentures werestable and retentive and provided an improvement in appearance which was appreciated by the patient. Thecopy technique had provided a relatively easy solution to a potentially difficult clinical problem.
2 1 Original extensionof dentures beforemodification
4 5
63
Figure 8.9 Diagram showing examples of diagnos-tic modifications which may be made to old den-tures. (1) Addition to the posterior palatal border toextend the denture to the vibrating line. (2) Modi-fications to upper buccal flanges to: (a) correct un-derextension; (b) improve facial seal; (c) produce aform favourable for neuromuscular control of the den-ture. (3) Posterior occlusal additions to: (a) correct oc-clusal imbalance; (b) increase occlusal vertical dimen-sion; (c) prevent postural protrusion of the mandible.(4) Extension of lower buccal flange to: (a) improvedistribution of occlusal loads to the residual ridge;(b) increase resistance to posterior displacement bycontact with the retromolar pad. (5) Hollowing thelabial flange to reduce displacement by the men-talis muscle. (6) Additions to the incisal edges to:(a) improve appearance; (b) facilitate speech; (c) allowincision.

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
106 Prosthetic Treatment of the Edentulous Patient
the replacement dentures is produced and thedental technician receives ample informationfor the decisions made at the treatment plan-ning stage to be carried out reliably.
Scott et al. (2006) compared conventionaland copy techniques for providing replacementof complete upper and lower dentures. They re-ported that the copy technique resulted in pa-tients reporting greater improvement in func-tional satisfaction of lower dentures made withthe copy technique as against the conventionalapproach. Clark et al. (2004) warned that thechances of losing control of the occlusion werepotentially high if both upper and lower den-tures were being copied.
A final point is worth making. As the lowerdenture is usually more dependent on mus-cular control than the upper, there are oftenstronger indications for copying it so that suchfeatures as the polished surface and the tonguespace can be faithfully carried through to thereplacement. In addition, it will be appreciatedthat the presence of the lower copy will help theclinician to shape the upper record rim to pro-duce an appropriate arch shape for the upperdenture which is being constructed in the con-ventional manner at the same time.
Denture copying – practicalproceduresVarious methods of constructing copy dentureshave been described in the literature (Duthieet al. 1978; Davenport & Heath 1983; Murray &Wolland 1986); each one requires the exist-ing denture to be invested in an elastic ma-terial which is adequately supported in somesort of container. Two different methods willbe described. In both, the objective is to pro-duce a copy template of existing dentures withwax teeth and acrylic resin bases using mate-rials which are readily available in the dentalsurgery. Thus the first stage becomes a chairside procedure and not one which relies on lab-oratory facilities.
Figure 8.10 Soapbox suitable as a container forthe copy technique.
Preparation of the copy template
Method 1
The patient’s denture is invested in alginate,which is supported in a container such as asoapbox. A window is cut into its side to pro-vide an exit for sprues as shown in Fig. 8.10. Thetechnique is summarised in Fig. 8.11. A varia-tion of this method utilises a specially designedaluminium flask (Fig. 8.12) (Murray & Wolland1986).
After polymerisation, the copy is removedfrom the mould and the sprues are cut off. Theresulting copy template has a rigid acrylic basetogether with wax teeth, which make the jobof the dental technician very much easier whensetting up teeth on the trial dentures. It has beenshown that accurate copies can be constructedwith this technique, the maximum dimensionalchange being –2.12% (Heath & Basker 1978).
Method 2
This technique uses stock impression trays andsilicone putty (Duthie et al. 1978). First, the oc-clusal and polished surfaces of the denture areembedded in a mix of silicone putty held in anupper tray. The impression surface is then in-vested in a second mix of putty, which is sup-ported on the reverse surface of another tray

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
The Relevance of Existing Dentures 107
2 4
5
61
3
Figure 8.11 Diagrammatic summary of the copydenture technique. (1) First mix of alginate to obtain animpression of polished and occlusal surfaces. Adhesiveis not applied to the walls of the container. (2) Alginateis trimmed at the level of the upper border of the boxand just below the denture periphery. Petroleum jellyis smeared on the surface of the alginate to facilitateseparation of the two halves of the mould. (3) Sec-ond mix of alginate to obtain a record of the impres-sion surface. (4) Soap box closed on to stops. Dentureremoved when alginate set. Sprue channels cut withwax knife into heels of polished surface impression.(5) Wax poured to above level of gingival margin.Mould closed and held together with rubber band. (6)Base poured in a fluid mix of cold-curing acrylic resin.
(Fig. 8.13). Once the putty has set, the two im-pressions are separated and the denture is re-moved. Sprue holes are cut into the heels of theimpression, and the copy template is producedas described above.
Figure 8.12 Specially designed aluminium flask forthe copy technique (Murray & Wolland 1986).
Figure 8.13 Silicone putty mould used for copymethod 2 (Duthie et al.1978) (see text for details).
Stages in copy denture production
The various clinical and technical stages aresummarised in Table 8.2. It may be possibleto undertake more than one clinical stage atthe same appointment. It can be seen fromTable 8.2 that the various stages are similarto those followed when constructing denturesin the conventional manner. Of course, if theocclusal surface is not to be altered and thecopy templates can be interdigitated accurately,stage 4 (recording the occlusion) would not berequired.
Communication with thedental technicianThere is evidence to suggest that unless boththe clinician and the dental technician have aclear understanding of the rationale behind thecopy technique, and why the technique is be-ing used for a particular patient, it is likelythat the prescription will not be followed ac-curately by the dental laboratory (Kippax et al.1998). The same study showed that not onlycan the quality of the copies be poor, but alsothat the replacement teeth are not positioned asrequested.

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
108 Prosthetic Treatment of the Edentulous Patient
Stage Clinical Remarks Technical
1
2
3 Wax teeth on rigid bases
4If the impression surface deficiency issuch that the copy templates areunstable in the mouth, bordermodifications and impressions in lowviscosity silicone should be taken beforerecording the occlusion (Fig. 8.14)
5
6 If impressions were taken at Stage 4,sufficient silicone material will still beattached to the bases to ensureacceptable stability of the trial dentures (Fig. 8.15)
7
8
9
Diagnosis and treatmentplan
Invest dentures to becopied
Construct copytemplates
Finish dentures
Record occlusion
Pour casts.Articulate copy templates.Make trial dentures.
Assess trial dentures.Take impression in lowviscosity silicone if not donein stage 4.
Fit dentures
Recall
List those aspects of the existing denturesthat will be modified and those aspectsthat will be copied
It is important to remove only one or twowax teeth at a time so that the remainder act as effective guides to accurate positioning of the new denture teeth
It will be necessary to remove the acrylicpalate of the upper trial denture and to lay down a wax palate of correctthickness before investing the denture.The remaining cold-curing resin andimpression material are discarded andthe flask is packed with heat-curing resin.
Table 8.2 Summary of clinical and technical stages of the copy denture technique.
It can hardly be stressed enough that thehigh quality of technical work needed to takea copy denture through to a successful comple-tion is dependent upon a mutual appreciationof the benefits of the technique, an accurate pre-scription and a precise attention to detail of thetechnical work.
Quality control andenhancementTo audit the reaction of patients to replace-ment dentures the following questions mightbe asked of the patient at the appropriate stageof treatment:

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
The Relevance of Existing Dentures 109
Figure 8.14 Wash impressions taken in the copydentures at the stage of recording the occlusion.
� Do you prefer the new dentures to the oldones?
� How different do the new dentures feel?What particular difference do you notice?
� How similar to the old dentures do the newcopy dentures feel?
� How long did it take you to get used to thenew dentures?
The following questions might be asked of thedental technician:
� With regard to copy dentures, were yougiven sufficient information to allow you to
Figure 8.15 The trial dentures are stabilised by thewash impressions taken at the stage of recording theocclusion.
position the new artificial teeth in the correctposition?
� With regard to copy dentures, were yougiven a clear indication of the objectives oftreatment?
From a collection of patients’ record cards thefollowing points might be reviewed:
� Did the treatment plans clarify those aspectsof the design of the existing dentures thatrequired alteration and those aspects whichshould remain unchanged in the replace-ment dentures?
� Were the objectives of the treatment plansfulfilled?
References and additionalreadingClark, R.F.F., Radford, D.R. & Fenlon, M.R. (2004) The
future of teaching complete denture constructionto undergraduates in the UK: is a replacement den-ture technique the answer? British Dental Journal,196, 571–5.
Davenport, J.C. & Heath, J.R. (1983) The copy den-ture technique – variables relevant to general den-tal practice. British Dental Journal, 155, 162–3.
Duthie, N. & Yemm, R. (1985) An alternative methodfor recording the occlusion of the edentulous pa-tient during the construction of replacement den-tures. Journal of Oral Rehabilitation, 12, 161–71.
Duthie, N., Lyon, F.F., Sturrock, K.C. & Yemm,R. (1978) A copying technique for replacementof complete dentures. British Dental Journal, 144,248–52.
Heath, J.R. & Basker, R.M. (1978) The dimensionalvariability of duplicate dentures produced in analginate investment. British Dental Journal, 144,111–14.
Heath, J.R. & Davenport, J.C. (1982) A modification ofthe copy denture technique. British Dental Journal,153, 300–2.
Heath, J.R. & Johnson, A. (1981) The versatility of thecopy denture technique. British Dental Journal, 150,189–93.
Kippax, A., Watson, C.J., Basker, R.M. &. Pentland,J.E. (1998) How well are complete dentures copied?British Dental Journal, 185, 129–33.

P1: JZP Trim: 246mm X 189mmc08 BLBK351-Basker January 4, 2011 10:41 Printer Name: Yet to Come
110 Prosthetic Treatment of the Edentulous Patient
Murray, I.D & Wolland, A.W. (1986) New denturesfor old. Dental Practice, 24, 1–6.
Osborne, J. (1960) The full lower denture. British Den-tal Journal, 109, 481–97.
Scher, E.A. & Ritchie, G.M. (1978) Prosthodontictreatment of the elderly by incremental modifica-tions to old dentures. Quintessence International, 8,47–53.
Scott, B.J.J., Forgie, A.H. & Davies, D.M. (2006) Astudy to compare the oral health impact profile
and satisfaction before and after having replace-ment complete dentures constructed by either thecopy or the conventional technique. Gerodontology,23, 79-86.
Walker, A. & Cooper, I. (eds) (2000) Adult DentalHealth Survey. Oral Health in the United Kingdom1998. The Stationery Office, London.
Watt, D.M. & Lindsay, K.N. (1972) Occlusalpivot appliances. British Dental Journal, 132,110–12.

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
9Preparation of the Mouth
Preparation of the mouth is often necessary be-fore dentures are made and may involve theelimination of pathology within the denture-bearing tissues or the creation of a morefavourable anatomical environment.
The various conditions requiring treatmentmay be considered in two sections, those in-volving the oral mucosa and those involvingbone.
(1) Conditions involving the oral mucosa� Denture stomatitis� Inflammatory papillary hyperplasia of
the palate� Angular stomatitis (angular cheilitis)� Shallow sulci� Denture-induced hyperplasia� Prominent frena
(2) Conditions involving the bone� Pathology within the bone� Sharp and irregular bone� Undercut ridges� Prominent maxillary tuberosities� Tori
Conditions involving the oralmucosaDenture stomatitis
Clinical appearance
The clinical appearance of denture stomatitisvaries from a patchy to a diffuse inflammationof the mucosa covered by a denture (Fig. 9.1).Newton (1962) classified denture stomatitis intothree types on the basis of its clinical appear-ance:
� Type I: Pinpoint hyperaemia� Type II: Diffuse inflammation� Type III: Granular (palatal inflammatory
papillary hyperplasia (p. 118)
The condition typically involves the mucosa ofthe maxillary denture-bearing area and doesnot extend beyond the borders of the den-ture. It may occur alone but is sometimesseen with two associated conditions, inflamma-tory palatal papillary hyperplasia and angularstomatitis.
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
111

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
112 Prosthetic Treatment of the Edentulous Patient
Figure 9.1 Denture stomatitis. The characteristicallysharp delineation of the diffuse palatal inflammation bythe borders of the denture is seen at the junction of thehard and soft palate, where the line separating the in-flamed from normal tissue corresponds to the posteriorborder of the denture.
Nomenclature
In spite of the lesion’s rather angry appearancethe patient rarely complains of soreness, there-fore the term ‘denture sore mouth’, which hasbeen used in the past to describe this condition,is inappropriate. Other terms currently used inthe literature to describe the condition are:
� Denture-related stomatitis.� Denture-induced stomatitis – however, it has
been argued that as the denture is rarely theprimary aetiological agent this term is sel-dom appropriate.
� Stomatitis prothetica.� Chronic atrophic candidiasis – for this and
the following term to be appropriate it isnecessary that a microbiological investiga-tion should have confirmed the presence ofcandida.
� Candida-related stomatitis
Prevalence
Denture stomatitis is a common condition, hav-ing been reported in 10–60% of patients wear-ing complete dentures. However, in the gen-eral complete denture-wearing population the
prevalence of the condition is likely to be closerto the lower limit of this range than to the upper(Radford et al. 1999).
Predisposing factors
AgeDenture stomatitis has been found to be morecommon in the elderly, particularly if hyposali-vation is present (Figueiral et al. 2007; Campisiet al. 2008).
GenderDenture stomatitis occurs more frequently in fe-males than in males, the ratio being approxi-mately 4:1 (Davenport 1970; Pires et al. 2002).Although the cause of this predisposition todenture stomatitis in females is not known,possible explanations include endocrine imbal-ance, iron deficiency anaemia, vaginal carriageof candida, a higher oral carrier rate of candidaand a greater inclination than males to weardentures at night.
Night wearing of denturesIt appears that behavioural factors, such aswearing the dentures at night and poor den-ture hygiene, are of major importance in the ae-tiology of denture stomatitis (Jeganathan et al.1997; Sakki et al. 1997; Saulman et al. 2006).Wearing the dentures at night can aggravatethe effect of both denture plaque and den-ture trauma by increasing the exposure of thepalatal mucosa to both aetiological factors.
Poor denture hygienePoor denture hygiene allows the build-up ofdenture plaque containing candida and othermicroorganisms. A strong association betweenpoor denture hygiene and denture stomatitishas been identified (Khasawneh & Al-Wahadni2002; Kulak-Ozkan et al. 2002).
High-carbohydrate dietDentures with a reduced masticatory efficiencymay encourage a patient to adopt a relatively

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
Preparation of the Mouth 113
easily managed high-carbohydrate diet, whichfavours the growth of candida and increasesthe adhesion of the microorganism to thedenture surface. An increase in the amount andfrequency of intake of relatively inexpensivecarbohydrates may also be encouraged by thepatient’s economic circumstances.
Systemic factorsSystemic conditions which can predispose todenture stomatitis include immunological defi-ciencies (Golecka et al. 2006), hormonal imbal-ance, e.g. diabetes, and nutritional deficiencies,e.g. vitamin B complex, vitamin C and iron.
Aetiology
Many different local and systemic factors havebeen incriminated in the aetiology of denturestomatitis, which is now widely accepted tobe multifactorial in origin. The relative impor-tance of microorganisms, in particular Candidaalbicans, and trauma from the dentures is stilldebated. However, the bulk of the relevantliterature supports the view that the presenceof candida organisms within plaque on theimpression surface of the denture is the keylocal factor.
In 1885, G.V. Black, commenting on thecondition we now know as denture stomatitis,stated that, ‘Fungi grow readily under anyplate irrespective of the material of what it ismade. They produce acids which if the mouthand palate are not properly cleaned will causesore mouth’. He sampled microorganismsfrom under the dentures of patients withthis condition and expressed surprise at theirabundance. He concluded that ‘plates are notcleaned often enough and that cleanliness isthe chief preventive measure’. Thus, well over100 years ago Black summarised the modernview of both the aetiology and management ofdenture stomatitis.
In a study of 3450 patients wearing at leastone removable denture the main risk factors as-sociated with denture stomatitis were found to
be wearing the dentures continuously, low lev-els of vitamin A and smoking (Shulman et al.2005). The authors recommended improveddenture cleaning and removing the dentures atnight.
Candida albicansThe evidence suggests that the most impor-tant local causative factor of denture stomati-tis is the presence of microorganisms withinplaque on the impression surface of the denture(Davenport 1970; Budtz-Jørgensen 1974; Olsen1974; Khasawneh et al. 2002; Ramage et al.2004). The plaque is present in significant quan-tities because of inadequate denture hygieneand its effects are maximised if the patientwears the dentures at night. The fungus, Can-dida albicans (Fig. 9.2), is the organism mostcommonly associated with denture stomatitisand which has received the most attention inthe literature, although other candida speciesmay also be present (Marcos-Arias et al. 2009).This fungus is dimorphic, occurring as bothyeast-like blastospores and filamentous pseu-dohyphae. In denture stomatitis, large num-bers of both forms are usually found in plaqueon the impression surface of the denture. Rela-tively few candida organisms are found on the
Figure 9.2 Mycelial and yeast forms of Candidaalbicans obtained from the impression surface of adenture.

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
114 Prosthetic Treatment of the Edentulous Patient
mucosa and there is no evidence that candidalinvasion of the mucosa occurs.
BacteriaAlthough the evidence for a causal relation-ship between candida and denture stomatitis isstrong, it has been suggested that a variety ofbacteria may also play a part in the condition(Kulak et al. 1997).
Denture traumaIt has been proposed that trauma to the oralmucosa is a cause of denture stomatitis (Emamiet al. 2008). Dentures can traumatise the mu-cosa either because of the presence of faultsin the prostheses such as loss of fit or oc-clusal imbalance or because the patient exhibitsparafunctional activity, such as bruxism, whichoverloads the tissues. It is sometimes arguedthat if trauma from the dentures was a ma-jor factor in the development of denture stom-atitis then the condition would be more com-monly seen under mandibular than maxillarydentures. This is because the area of mucosalsupport for the prosthesis is much less in themandible than in the maxilla and thereforethe load per unit area and potential degree oftrauma is significantly greater in the mandiblethan in the maxilla. However, the widespreadinflammation characteristic of denture stomati-tis that is seen clinically is a feature of themaxillary, not the mandibular, denture-bearingmucosa.
Other factorsIt should be remembered that palatal inflamma-tion under dentures is a non-specific responseto a variety of injurious agents. Therefore dif-fused inflammation of the denture-bearing mu-cosa may occasionally be seen, which is notthe result of denture plaque or trauma. Forexample:
� Raised residual monomer. A faulty curing cyclewhen the dentures are processed can resultin a residual monomer content high enough
to produce mucosal inflammation (p. 116)(Austin & Basker 1980). This, unlike the clas-sical denture stomatitis resulting from poordenture hygiene, is characteristically associ-ated with discomfort from the inflamed mu-cosa.
� Self-medication. Palatal inflammation issometimes caused by patients using topicalagents in an inappropriate way. Certainmouthwashes, ointments, or other sub-stances which are normally free of adverseeffects in the mouth, can cause mucosaldamage when applied beneath a denture.Examples of preparations that can behavein this way are chlorhexidine gel, salicylateointments and even whisky – with whichsome more ingenious patients have beenknown to bathe their sore mucosa. Thedamage occurs because the exposure tothe agents is increased by their being heldagainst the mucosa for extended periodsby the denture and because they are notdiluted or washed away by the saliva. Also,a vicious cycle may be established in whichthe patient initially uses the preparationin a misguided attempt to relieve somediscomfort; the preparation then causesfurther mucosal damage which increasesthe soreness and so the patient applies evenmore of the injurious agent.
Aetiological interactionsThe possible interaction of the various predis-posing and aetiological factors is complex anduncertain, but a possible scenario which is com-patible with the bulk of the relevant literature isas follows (Fig. 9.3).
Toxins produced by the candida cells left onthe denture surface by deficient hygiene mea-sures, together with trauma from the dentureinitiate an inflammatory reaction. A resultingthinning of the epithelium results in increasedpermeability and escape of inflammatory ex-udates. The exudates, together with desqua-mated mucosal cells, form a favourable nutri-ent medium, which promotes the growth of

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
Preparation of the Mouth 115
Dentureplaque
Mucosa
Toxins
INFLAMMATION
Exudate andsquames
Sucrose-rich dietSalivaryanti-candidalantibody
Trauma
Denturebase
Mucosal thinning andincreased permeability
Candidal growth and adhesionCandidal growth and adhesionCandidal growth and adhesion
Figure 9.3 Possible aetiological interactions in denture stomatitis (see text for fuller explanation). (Reproducedwith permission from Stephen Hancock. c© 2000 British Dental Journal.)
Candida albicans. In addition, these exudatesand the sucrose-rich diet which may result fromthe dietary selection sometimes associated withthe wearing of dentures, may contribute to thecondition by increasing the adhesiveness of thecandidal cells, and thus encouraging the for-mation of denture plaque. As candidal prolif-eration occurs, the rate of production of potenttoxins by the microorganisms increases. Thepassage of these toxins into the tissues is facili-tated by the thinning and increased permeabil-ity of the mucosa. Aggravation of the inflam-matory response occurs and so a vicious circleis set up. Anti-candidal antibody is secreted inparotid saliva but the denture base may restrictaccess of the antibody to the candida cells.
Diagnosis
The diagnosis of denture stomatitis is essen-tially a clinical one made on the basis of the ap-
pearance of the palatal mucosa. Identificationof the aetiological factors responsible for a par-ticular case may be achieved by noting the fol-lowing.
Night-wearing of denturesIt should be noted routinely from the historywhether or not the dentures are worn both dayand night.
Denture hygieneDetails of the patient’s denture cleaning regimeshould be obtained, including the method andfrequency of cleaning together with the typeof immersion cleanser used. The amount ofplaque on the impression surface of the den-ture should be recorded. This assessment of thequantity and distribution of denture plaque ismade easier by applying a disclosing solutionto the denture (Fig. 14.10). In those cases whereonly a little plaque is seen, it should be realised

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
116 Prosthetic Treatment of the Edentulous Patient
that a patient will sometimes have made an ef-fort to clean the dentures in readiness for thevisit to the dentist, which is atypical of theirnormal denture hygiene regimen.
Denture traumaThe degree of denture trauma should be as-sessed. This can be estimated from the relativefunctional adequacy of the dentures in terms ofocclusion and fit, and from evidence of the pres-ence or absence of parafunctional activity.
Other local factors� Raised residual monomer. If palatal inflamma-
tion and discomfort occur shortly after a newdenture has been fitted, or an existing den-ture repaired or relined, then a raised resid-ual monomer content might be suspected.
� Self-medication. Questioning the patient abo-ut any current oral medication such asmouthwashes or ointments might indicateif the condition is iatrogenic, resulting frommucosal irritation by these preparations.
� Diet. A dietary assessment can be carried outif it is suspected that a high carbohydratediet is contributing to the condition.
Systemic factorsThe medical history may provide clues that sys-temic factors are playing a part. If this is thecase, or if the condition subsequently fails to re-spond to local treatment, appropriate investiga-tions should be arranged.
It is important to obtain details of drugtherapy in case a particular medication iscausing conditions such as a dry mouth (seeChapter 16).
Treatment
Although denture stomatitis is symptomlessand the patient is often unaware of its presence,it should be treated before new dentures areconstructed because of the following:
� Swelling of the oral mucosa will have oc-curred as a result of the inflammation. Pro-ducing a new denture from an impressionof the mucosa in this condition will compro-mise the fit of the prosthesis, especially if thenew well-fitting denture brings about someresolution of the swelling.
� The mouth may be the source of candida or-ganisms and other microorganisms respon-sible for infection in other parts of the body,such as nailbeds, the pharynx and the larynx(Nikawa et al. 1998). In debilitated patients,systemic spread of candida from the mouthcan occur with fatal consequences.
There is increasing evidence that theoral cavity, particularly in denture wearers,can be a reservoir for methicillin-resistantStaphylococcus aureus (MRSA) which clearlyhas serious implications for both patientsand their carers (Lee et al. 2009). Commonlyemployed denture-cleaning solutions havebeen shown to be effective against MRSA invitro (Maeda et al. 2007).
As behavioural factors are so important inthe aetiology of denture stomatitis, appropri-ate modification of the patient’s behaviour is es-sential for long-term success. Therefore the pri-mary objectives of local treatment of denturestomatitis (Lombardi & Budtz-Jørgensen 1993)are to improve denture hygiene and discouragethe patient from wearing the dentures at night.
In addition, in those cases where denturefaults are identified and which could be trau-matising the denture-bearing tissues, correctionof the faults should be undertaken.
Improve denture hygiene� Motivating, instructing and monitoring the
patient. It is vital that the clinician convincesthe patient of the need for meticulouscleaning of the dentures. The methods forcarrying it out should be discussed usingappropriate language, clearly demonstrated,subsequently monitored and reinforced ifnecessary. Once a high level of denture

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
Preparation of the Mouth 117
hygiene has been achieved it is essential thatit is maintained otherwise recurrence of thedenture stomatitis is likely (Cross et al. 2004).
� Laboratory cleaning of the dentures. Where de-posits are heavy and possibly partly calci-fied, and where the surface polish of thedenture has deteriorated, it is recommendedthat laboratory cleaning and polishing of thedenture is carried out before home care bythe patient is instituted.
� Disinfection of the dentures. The denturesshould be regularly immersed by the patientin a suitable disinfectant. Two solutions havebeen shown to be effective in controllingdenture plaque: alkaline hypochlorite andaqueous chlorhexidine gluconate (Hutchins& Parker 1973; Altman et al. 1979; Budtz-Jørgensen 1979; Abelson 1985; Webb et al.1998c; Barnabe et al. 2004). The formersolution has been shown to be effective inremoving denture plaque while the latterinhibits its formation. Overnight immersionis necessary if either a hypochlorite solutioncontaining 0.08% available chlorine or 0.1%aqueous chlorhexidine gluconate is used.When it is impossible to persuade a patientto leave the denture out at night, immersionin a hypochlorite solution containing 0.16%available chlorine for 20 minutes daily or in2% aqueous chlorhexidine gluconate for ap-proximately 5 minutes daily are alternatives.Before immersion, the denture should bebrushed thoroughly to remove most of theplaque and then, if chlorhexidine is tobe used, rinsed carefully to remove anysoap which would otherwise inactivate thechlorhexidine. Patches of brown stainingusually appear on a denture that has beenimmersed in chlorhexidine solution. As arule, the staining is not severe and canbe removed by subsequent immersion in ahypochlorite cleaner. The presence of a metaldenture base complicates matters becausehypochlorite can cause corrosion of the base.However, the recommended short immer-sion period can be used with safety.
Disinfection of dentures by short exposure tomicrowave irradiation has also been shownto be effective (Baysan et al. 1998; Webb et al.1998c; Dixon et al. 1999; Webb et al. 2005).However the practicality of this approach re-mains uncertain: the procedure kills the or-ganisms but does not remove the plaque,and there is the possibility that overexposureto the irradiation could have adverse effectson the denture materials.
Ultrasonic cleaning devices have beenshown to be potentially useful for cleaningdentures (Hashiguchi et al. 2009; Arita et al.2005).
Correction of denture faults� Occlusal faults. An unbalanced occlusion
should be corrected by occlusal adjustmentor by the addition of cold-curing acrylicresin to the occlusal surfaces of the dentures(p. 95).
� Impression surface faults. Lack of fit in a den-ture can be corrected by applying a short-term soft lining material to the impressionsurface (p. 234). However, caution should beexercised in selecting this option as the pres-ence of a temporary lining will make it muchmore difficult for the patient to maintain theall-important high level of denture hygiene.It has been reported that certain of these lin-ing materials exhibit antifungal activity invitro, but it is unlikely that this activity is sig-nificant in vivo.
Leaving the dentures out at nightAll patients should be strongly advised to leavetheir dentures out as much as possible, ideallyat night, although some will feel unable to con-form to this timing for a variety of reasons. Insome instances, successful treatment will not bepossible unless the patient follows this advice.This regimen reduces the period the mucosais in contact with denture plaque, reduces theintra-oral population of candida and other or-ganisms (Williamson 1972), provides an oppor-tunity for prolonged immersion of the dentures

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
118 Prosthetic Treatment of the Edentulous Patient
in a disinfectant and, for those cases where den-ture trauma is a contributory factor, reduces theperiod over which mucosal damage can occur.
Antifungal preparationsAntifungal agents such as nystatin, ampho-tericin B, fluconazole, itraconazole and micona-zole have been advocated for the treatment ofdenture stomatitis and they have been shown tobe effective in the short term. They are used top-ically as lozenges, mouthwashes or ointmentsapplied to the denture and to the lesion. Whereproblems with patient compliance are antici-pated, some of these agents can be applied tothe denture by the clinician incorporating theminto a tissue conditioner or a lacquer (Budtz-Jørgensen & Carlino 1994; Konsberg & Axell1994; Parvinen et al. 1994; Truhlar et al. 1994;Dias et al. 1997; Chow et al. 1999; Geerts et al.2008). However, these preparations do nothingto modify the oral conditions and patient be-haviour responsible for the inflammation in thelong term. Clinical studies have shown that arapid relapse usually follows the cessation ofsuch antifungal therapy if this is the sole treat-ment employed. There is no difference at 1 yearfollowing start of treatment between patientstreated with antifungal antibiotics in combina-tion with denture hygiene instruction and cor-rection compared with those treated by denturemeasures alone (Bergendal 1982; Bissell et al.1993; Webb et al. 1998c). The recurrence of den-ture stomatitis in patients who maintain a highlevel of denture cleanliness is low (Cross et al.2004). The prescription of antifungal agents inthe treatment of denture stomatitis is thereforenot supported by the available evidence.
Systemic therapyAn appropriate combination of the simple ther-apeutic measures described above will usuallyeffect a cure within 2–3 weeks if there are no un-derlying systemic factors. Therefore, if a cure isnot achieved in this time, and if persistent lo-cal factors cannot be identified, systemic causes
Figure 9.4 Inflammatory papillary hyperplasia ofthe palate.
should be suspected and the patient referred toa medical practitioner for further investigation.
Inflammatory papillaryhyperplasia of the palate
This condition, alternatively known as hyper-plastic or granular denture stomatitis, involvesthe palatal mucosa and appears as multipleelevations, usually bright red in colour. It is‘raspberry-like’ in appearance and may involvethe whole or part of the hard palate (Fig. 9.4). Atone time, it was suggested that this conditionmight be premalignant; but malignant transfor-mation has not been reported, nor is it asso-ciated with the cytological signs of dysplasia(Kaplan et al. 1998).
Aetiology
The condition is closely related to the simpleatrophic form of denture stomatitis and sharesthe same aetiology (Kaplan et al. 1998). In addi-tion, the presence of a relief chamber in an up-per denture may predispose to this hyperplasticchange (Ettinger 1975).
Treatment
Treatment may be considered to have twophases, as described in the following.

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
Preparation of the Mouth 119
a
b
Mucosa
Denture
Figure 9.5 The impression surface of the denture inpalatal inflammatory papillary hyperplasia: (a) sharpspicules of acrylic penetrate the fissures between thehyperplastic papillae if the impression surface is notmodified after processing; (b) the spicules of acrylicmay be lightly stoned before fitting the denture to re-duce the amount of trauma.
Elimination of the mucosal inflammationTreatment of the inflammatory component ofthis condition is the same as that describedfor denture stomatitis. Antifungal agents havebeen reported to reduce the inflammatory com-ponent but the hyperplasia remains (Salonenet al. 1996).
Prosthetic or surgical managementof the hyperplasiaWhen the inflammation has been successfullytreated the hyperplastic nodules will still re-main, although they will now be pale in colourand reduced in size. A decision then has to bemade whether to construct a denture on thisfoundation or to remove the nodules surgicallybeforehand. The approach adopted in a partic-ular case will depend on factors such as the sizeof the nodules, and the patient’s age and medi-cal history.
If an acrylic denture is constructed withoutprior surgical removal of the nodules, sharpspicules of acrylic resin will penetrate the fis-sures of the lesion (Fig. 9.5a). As all dentures
move to a certain extent during function, thesespicules have an abrasive effect on the mucosaand inflammation will recur. To prevent thishappening, the spicules should be lightly pol-ished to reduce their sharpness before fittingthe denture (Fig. 9.5b).
Angular stomatitis
Angular stomatitis, sometimes described as an-gular cheilitis, is an erythematous, often ero-sive, non-vesicular skin lesion radiating fromthe angles of the mouth. It is usually bilateral,frequently painful and is rarely seen except indenture wearers (Fig. 9.6). It has been foundto occur in 28% of long-term hospitalised el-derly denture-wearers. It is more common in fe-males. If left untreated, it can result in unsightlyscarring. The majority of patients with angu-lar stomatitis also have an associated denturestomatitis.
Aetiology
Common local and systemic factors which maycontribute to the development of angular stom-atitis are as follows.
Local� Infection� Inadequate lip support� Maceration of the skin
Figure 9.6 Angular stomatitis – clinical appearancebefore treatment.

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
120 Prosthetic Treatment of the Edentulous Patient
Reduced lipsupport
Reduced occlusalvertical dimension Age changes
Angularcreasing Saliva
Systemic factors
Macerationof the skin
Reduced resistanceto infection
Micro-organisms
Infection
ANGULARSTOMATITIS Figure 9.7 The multifactorial aeti-
ology of angular stomatitis.
Systemic� Iron deficiency� Vitamin B and C deficiency� Insulin-dependent diabetes mellitus
The aetiological factors listed above are closelyinterrelated as indicated in Fig. 9.7. Macerationresults from the continuous bathing by saliva ofthe skin at the corners of the mouth, which low-ers the resistance of the skin to infection. Mac-eration is encouraged by the presence of skincreases which draw saliva from the mouth bycapillary action and which may be due to inad-equate lip support being provided by the up-per denture or to the presence of an excessivefreeway space. However, an increased freewayspace should never be assumed to be presentsimply on the evidence of angular stomatitis.
Microorganisms may be carried in the salivato the lips from intra-oral sites, of which themain ones are the denture and the dorsum ofthe tongue. The significance of microbial plaqueon the dentures is demonstrated by the obser-vation that if patients with angular stomatitisdo not wear their dentures, a complete cureusually results in 2 weeks even though all den-tal support to the lips has been lost. Candidaalbicans is frequently isolated from the lesionof angular stomatitis where denture stomatitisis also present. However, if angular stomati-tis occurs alone, Staphylococcus aureus is recov-ered from the lesion twice as often as candida(McFarlane & Helnarska 1976) In such cases,the nose may be the source of secondary in-fection with carriage on the fingers being themethod of transmission.

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
Preparation of the Mouth 121
Treatment
The treatment of angular stomatitis in the firstinstance involves the elimination of local infec-tion and the reduction of the intra-oral popula-tion of micro-organisms.
Denture hygieneDenture hygiene instruction and immersion ofthe dentures in a hypochlorite denture cleaner,as described for denture stomatitis, should beinstituted. In many cases, such simple measureswill effect a cure in about 2 weeks.
Antimicrobial agentsImproved denture hygiene may be supple-mented where necessary by prescribing oneof the broad-spectrum antimicrobial agents,such as miconazole oral gel or a tetra-cycline/nystatin ointment, which are activeagainst both fungi and bacteria. However, itis not advisable to prescribe one of the manycompound skin preparations which containsteroids, as topical steroids have been shown tobe the commonest cause of perioral dermatitisand may therefore aggravate the condition.
If specific antimicrobial therapy is to be em-ployed, a swab from the angles of the lipsshould be cultured to allow identification of theresponsible organisms. If the cultures are pos-itive for candidal organisms, amphotericin Blozenges (10 mg) or nystatin pastilles (100 000units) may be sucked four times a day. Thesepreparations are of value in the treatment ofangular stomatitis because candidal organismsnot only grow in large numbers on the den-ture but also proliferate on the dorsum of thetongue. Both reservoirs could be contributingto the high salivary count predisposing to theangular stomatitis.
If swabs from the lesion indicate that abacterial infection is present, benefit may begained from the topical application of a tetracy-cline ointment or miconazole gel (an antifungalwith some antibacterial properties). Treatmentshould be continued for 2–4 weeks.
Denture modificationsWhen it appears that the skin folds are due toa reduced occlusal vertical dimension or inade-quate lip support, the existing dentures can bemodified to test the diagnosis. This can be doneby temporarily correcting the suspect denturesurface by the addition of wax to see whether asubsequent permanent correction would elimi-nate or reduce the folds. If the temporary waxmodification does result in an improvement,new dentures should be made accordingly. Asan interim measure, it is sometimes possible tocorrect the existing dentures in the short termby the addition of cold-curing acrylic resin atthe chair side (p. 95). If the occlusal vertical di-mension of the old dentures is reduced it can becorrected by adding tooth-coloured resin to theocclusal surfaces of the posterior teeth.
However, if the temporary modificationshave little, or no effect on the folds, it mustbe accepted that they are the result of an ir-reversible tissue change, such as loss of tissuetone associated with ageing. The persistence ofthe folds makes treatment more difficult and re-currence of the condition more likely.
Failure to respond to local measures sug-gests that systemic factors are playing a partand that further investigations are required.
A suggested interrelation between the localcausative factors leading to denture stomatitis,angular stomatitis and inflammatory papillaryhyperplasia is shown in Fig. 9.8.
Shallow sulci
The problems characteristically created by ashallow sulcus are twofold:� Denture instability� Unfavourable load distribution – a problem
occurring primarily in the lower jaw
Treatment
Prosthetic treatmentThe main approach to treatment is prosthetic –to go over the dentures again with a fine

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
122 Prosthetic Treatment of the Edentulous Patient
DENTURE STOMATITIS
INFLAMMATORY PAPILLARY
HYPERPLASIA
ANGULAR STOMATITIS
Skin folds
Saliva
Micro-organisms on denture
Micro-organisms on tongue
Trauma
Bacteria from an extra-oral
source, e.g. nose
Figure 9.8 A suggested relationshipbetween the local causative factorsleading to denture stomatitis, angularstomatitis and inflammatory palatal hy-perplasia.
toothcomb and to undertake any correctionsthat offer the possibility of improving stabilityor obtaining more tissue coverage. Where over-loading has resulted in persistent discomfort along-term soft lining may be provided (p. 238).
Surgical treatment
If prosthetic measures fail, then surgery toimprove the quality of the denture-bearingtissues might be of benefit. The most obvi-ous interventions currently undertaken are im-plants to support the prostheses. Other formsof pre-prosthetic surgery have largely fallenout of favour because the advanced alveolarresorption which commonly creates the needalso limits what can be achieved by surgicalintervention.
Soft tissue surgery is now largely confinedto removal of denture hyperplasia and, less fre-quently, frenectomy to reduce prominent frena.
Denture-induced hyperplasia
Denture-induced hyperplasia takes the form ofsingle or multiple flaps of fibrous tissue relatedto the border of a denture (Fig. 9.9). It is foundin up to 10% of denture wearers (Axell 1976;Budtz-Jørgensen 1981).
Aetiology
The primary cause of this condition is overex-tension of the denture border causing chronicirritation of the sulcus tissues. The lesioncharacteristically develops slowly as a result ofthe gradual resorption of alveolar bone caus-ing the denture to sink so that its borders diginto the mucosa. The chronic nature of the pro-cess means that discomfort is often not a promi-nent feature and therefore the patient contin-ues wearing the offending denture for far toolong. Hyperplastic lesions of considerable size
Figure 9.9 Denture-induced hyperplasia – the flapof fibrous tissue is situated in the lower labial sulcus.

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
Preparation of the Mouth 123
can develop before the patient becomes awareof the need for treatment.
This situation contrasts with tissue dam-age produced by overextension present whena denture is first fitted. Here mucosal injury oc-curs rapidly, usually within a day or two, andpresents commonly in the form of frank ulcer-ation with associated pain. Because of the dis-comfort, the patient seeks treatment to alleviatethe problem before hyperplasia has had time todevelop.
Treatment
Treatment should be undertaken in the follow-ing sequence:
(i) Eliminate denture trauma. The hyperplastictissue diminishes in size if the denture isnot worn for a period of time or if theflange is cut away from the affected area.Other denture adjustments to reduce thelevel of trauma may be indicated, such asapplying a short-term soft lining materialto improve the fit and stability of the den-ture, or correcting occlusal imbalance.
(ii) Review at 2 weeks. In some cases, the degreeof resolution resulting from the elimina-tion of denture trauma is sufficient to al-low satisfactory dentures to be made with-out the necessity for surgical intervention.
(iii) Surgical excision if required. If the size ofthe lesion remaining after correction of thedenture is still too large to allow adequateextension of the denture, surgical removalis indicated. It must be remembered thatthe swelling of an oral malignancy in thesulcus could masquerade as a denture-induced hyperplasia and therefore all ex-cised hyperplastic tissue should routinelybe sent for histological examination.
Prominent frena
These are bands of fibrous tissue whose attach-ments are close to the crest of the alveolar ridge.
Figure 9.10 A prominent frenum attached tothe crest of the ridge in the lower left premolarregion.
Prominent frena may be found in both jawslabially and buccally in the premolar regions(Fig. 9.10). In order to accommodate this fibroustissue, it is necessary to make a deep notch inthe denture flange. The stress concentrationswhich are set up at the apex of the notch predis-pose to fracture of the denture base. In addition,there may be difficulty in achieving an efficientborder seal.
Surgical excision of a prominent frenum maybe necessary in extreme cases.
Conditions involving the bonePathology within the bone
Pathology within the bone should be sus-pected if one or more of the following arepresent:
� A sinus� A swelling� Irregularity of the shape of the ridge
Radiographs should not usually be taken ofedentulous patients in the absence of signs orsymptoms. However, the existence of clinicalevidence, such as that listed above, justifies thetaking of full-mouth radiographs to confirmor allay the suspicion that there is pathology

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
124 Prosthetic Treatment of the Edentulous Patient
within the bone. For this purpose, panoramicradiography has the advantage of a relativelylow-radiation dosage to the patient comparedwith a full set of intra-oral films.
Treatment
Radiographic surveys have revealed the pres-ence of such items as unerupted teeth, retainedroots and dental cysts in 30–40% of edentu-lous patients. However, this finding should bequalified with the fact that the significant di-agnostic yield in these surveys was low, asonly a small percentage of these patients actu-ally required surgical treatment. For example,if an unerupted tooth is deeply embedded inhealthy bone with no associated pathology evi-dent, future complications are unlikely. Surgicalremoval is not only unnecessary but positivelycontraindicated, as it would involve a consider-able loss of alveolar bone. On the other hand, atooth or tooth fragment lying close to the sur-face should usually be removed, because thepressure from a denture is likely to induce re-sorption of the overlying bone so that the toothor fragment is exposed to the oral cavity (Fig.9.11).
Figure 9.11 A radiograph showing a tooth deeplyembedded in bone and a root on the surface.Before making complete dentures, removal of theroot is essential: the tooth, however, should be leftundisturbed.
Sharp and irregular bone
Bony spicules
Where sharp spicules of bone are present onthe crest of a ridge which is covered by thin at-rophic mucosa, pain may be produced by pres-sure from a denture. One reason for the pres-ence of the sharp spicules is that insufficientcare was taken when the teeth were extracted,such as the failure to compress the sockets ad-equately. Another possible reason is irregularbone resorption resulting from previous peri-odontal disease. The most common area forthese spicules to occur is in the lower anteriorregion.
TreatmentThe insertion of a short-term soft lining mate-rial into an existing denture may be sufficient torelieve the symptoms; if so, the material can bereplaced by a long-term soft lining material. Oc-casionally, however, prosthetic treatment is un-successful and it becomes necessary to smooththe bone surgically. A conservative approachto bone removal is recommended, as in manycases excessive resorption has already occurredand little ridge remains.
Mylohyoid ridges and genial tubercles
Bony prominences associated with muscle at-tachments are another cause of discomfort be-neath dentures. The prominences that occasion-ally cause trouble are:
� The mylohyoid ridges� The genial tubercles
When the natural teeth are present these bonyprojections are well down in the depths ofthe sulci, but after the teeth are extracted andthe associated alveolar bone is resorbed theprojections come to lie within the denture-bearing area and become progressively moreprominent with increasing age. Discomfort iscaused by the denture exerting pressure on the

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
Preparation of the Mouth 125
thin layer of mucosa covering these sharp bonyprojections.
Treatment(i) Prosthetic treatment. Prosthetic measures to
resolve the problem should be attemptedfirst. These include the following:� A thorough re-appraisal of the dentures
and correction of any design faults.� Reducing masticatory load on the
denture-bearing tissues by reducing thearea of the occlusal table, for example,by reducing the width of the posteriorteeth so that they penetrate the bolus offood more easily.
� Localised relief or adjustment of the im-pression surface of the denture in the re-gion of the bony projections.
� Smoothing the impression surface of thedenture so that movement of the den-ture is less traumatic to the mucosa.
� Placing a soft lining.(ii) Surgical treatment. If prosthetic treatment of
the condition is unsuccessful surgical re-moval of the bony projections may be re-quired.
Undercut ridges
If ridges are grossly undercut (Fig. 9.12), com-plete seating of a denture may be impossiblewithout extensive cutting back of the flangeand the risk of reduced retention. To avoidthis problem, surgical reduction of the undercutmay be necessary. In some instances, the reduc-tion can be carried out unilaterally so as to al-low the denture to be rotated into position (seeFig. 4.11).
Prominent maxillary tuberosities
These may be composed of either fibrous tissueor bone and may in extreme cases be so largeas to completely eliminate the inter-alveolarspace. In such cases, it is impossible for fully
Figure 9.12 There is a large bony undercut buccalto the right tuberosity. A denture can be inserted onlyif the flange is extensively reduced or the undercuteliminated surgically.
extended denture bases to be accommodatedand so retention and support of the dentures islikely to be compromised.
Treatment
Prosthetic treatment(i) Re-assessment of the occlusal vertical dimen-
sion. This re-assessment should be car-ried out routinely, because, if the patientis able to accept a small increase in oc-clusal vertical dimension, sufficient inter-alveolar space might be created to allowfull extension of the denture bases.
(ii) Accept posterior under-extension of both up-per and lower dentures. This might well besuccessful for the upper denture becausethe ridges are normally well developed sothe denture is well retained and stable asa result. However, the approach is muchmore likely to compromise the lower den-ture and therefore should not be adoptedin this case.
(iii) Use a thin denture base. It may be possibleto extend the dentures fully if a very thinmetal base is used in the area of the re-duced inter-alveolar space.

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
126 Prosthetic Treatment of the Edentulous Patient
a b
Figure 9.13 Prominent tori. (a) A palatine torus; (b) mandibular tori situated lingually in left and right premolarareas.
Tori
Tori are developmental bony prominences oc-curring in the maxilla and mandible that canadversely affect denture function and comfort.
Palatine torus
A palatine torus occurs in the midline of thehard palate and when covered by a thin, rela-tively incompressible layer of mucosa may leadto problems of discomfort, instability and mid-line fracture of the upper denture (Fig. 9.13a).
TreatmentIf it is considered that a palatine torus is likelyto give rise to the difficulties mentioned abovea palatal relief is commonly placed in the den-ture. This approach is discussed further onp. 162. Only in exceptional cases would surgi-cal removal of the torus be contemplated.
Mandibular tori
Mandibular tori usually occur bilaterally onthe lingual aspect of the mandible, frequentlyin the premolar region; they are situated closeto the mucosal reflection in the lingual sulcus(Fig. 9.13b). Their presence may make it diffi-cult to provide comfortable dentures as the bor-
der of the denture readily traumatises the mu-cosa overlying the bony protuberances. In suchinstances, surgical removal of the tori may benecessary.
References and additionalreadingAbelson, D.C. (1985) Denture plaque and denture
cleansers. Gerodontics, 1, 202–6.Altman, D.M., Yost, K.G. & Pitts, G. (1979) A spec-
trofluorometric protein assay of plaque on den-tures and of denture cleaning efficiency. Journal ofProsthetic Dentistry, 42, 502–6.
Arendorf, T.M. & Walker, D.M. (1987) Denture stom-atitis: a review. Journal of Oral Rehabilitation, 14,217–27.
Arita, M., Nagayoshi, M., Fukuizumi, T., Okinaga, T.,Masumi, S., Morikawa, M., Kakinoki, Y. & Nishi-hara T. (2005) Microbicicidal efficacy of ozonatedwater against Candida albicans adhering to acrylicdenture pales. Oral Microbiology and Immunology,20, 206–10.
Austin, A.T. & Basker, R.M. (1980) The level of resid-ual monomer in acrylic denture base material.British Dental Journal, 149, 281–6.
Axell, T. (1976) A prevalence study of oral mucosallesions in an adult Swedish population. Odontolo-gisk Revy, 27 (Suppl. 36), 1–103.
Barnabe W., de Mendonca N., Pimenta F., PegoraroL. & Scolaro J. (2004) Efficacy of sodium hypochlo-rite and coconut soap used as disinfecting agents

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
Preparation of the Mouth 127
in the reduction of denture stomatitis, Streptococcusmutans and Candida albicans. Journal of Oral Rehabil-itation, 31, 453–9.
Baysan, A., Whiley, R. & Wright, P.S. (1998) Use ofmicrowave energy to disinfect a long-term soft lin-ing material contaminated with Candida albicans orStaphylococcus aureus. Journal of Prosthetic Dentistry,79, 454–8.
Bergendal, T. (1982) Status and treatment of denturestomatitis patients – a 1 year follow-up study. Scan-dinavian Journal of Dental Research, 90, 227–38.
Bergendal, T., Hiemdahl, A. & Isacsson, G. (1980)Surgery in the treatment of denture-related inflam-matory papillary hyperplasia of the palate. Interna-tional Journal of Oral Surgery, 9, 312–19.
Bissell, V., Felix, D.H. & Wray, D. (1993) Compara-tive trial of fluconazole and amphotericin in thetreatment of denture stomatitis. Oral Surgery, OralMedicine, Oral Pathology, 76, 35–9.
Black, G.V. (1885) Sore mouth under plates. DentalItems of Interest, 7, 492.
Brook, I.M. & Lamb, D.J. (1987) Treatment of denture-induced hyperplasia. Dental Update, 14, 288–95.
Budtz-Jørgensen, E. & Carlino, P. (1994) A micona-zole lacquer in the treatment of Candida-associateddenture stomatitis. Mycoses, 37, 131–5.
Budtz-Jørgensen, E. (1974) The significance ofCandida albicans in denture stomatitis. ScandinavianJournal of Dental Research, 82, 151–90.
Budtz-Jørgensen, E. (1979) Materials and methods forcleaning dentures. Journal of Prosthetic Dentistry, 42,619–23.
Budtz-Jørgensen, E. (1981) Oral mucosal lesions as-sociated with the wearing of removable dentures.Journal of Oral Pathology, 10, 65–80.
Campisi, G., Panzarella, V., Matranga, D., Calvino,F., Pizzo, G., Lo Muzio, L., & Porter, S. (2003)Risk factors of oral candidosis: a twofold approachof study by fuzzy logic and traditional statistic.Archives of Oral Biology, 53, 388–97.
Chow, C.K., Matear, D.W. & Lawrence, H.P. (1999)Efficacy of antifungal agents in tissue conditionersin treating candidiasis. Gerodontology, 16, 110–18.
Cross, L., Williams, D., Sweeney, C., Jackson, M.,Lewis, M. & Bagg, J. (2004) Evaluation of the recur-rence of denture stomatitis and Candida coloniza-tion in a small group of patients who received itra-conazole. Oral Surgery Oral Medicine Oral PathologyOral Radiology and Endodontics, 97, 351–8.
Davenport, J.C. (1970) The oral distribution ofCandida in denture stomatitis. British Dental Journal,129, 151–6.
Davenport, J.C. (1972) The denture surface. BritishDental Journal, 133, 101–5.
Dias, A.P., Samaranayake, L.P. & Lee, M.T. (1997)Miconazole lacquer in the treatment of denturestomatitis: clinical and microbiological findings inChinese patients. Clinical Oral Investigations, 1, 47–52.
Dixon, D.L., Breeding, L.C. & Faler, T.A. (1999) Mi-crowave disinfection of denture base materials col-onized with Candida albicans. Journal of ProstheticDentistry, 81, 207–14.
Emami, P., de Grandmont, P., Rompre, P., Barbeau,J., Pan, S. & Feine, J. (2008) Favouring trauma asan etiological factor in denture stomatitis. Journalof Dental Research, 87, 440–4.
Ettinger, R.L. (1975) The etiology of inflammatorypapillary hyperplasia. Journal of Prosthetic Den-tistry, 34, 254–259.
Figueiral, M.H., Azul, A., Pinto, E., Fonseca, P.A.,Branco, F.M. & Scully, C. (2007) Denture-relatedstomatitis: identification of aetiological and predis-posing factors – a large cohort. Journal of Oral Reha-bilitation, 34, 448–55.
Geerts, G., Stuhlinger, M. & Basson, N. (2008) Effectof an antifungal denture liner on the saliva yeastcount in patients with denture stomatitis – a pilotstudy. Journal of Oral Rehabilitation. 35: 664–9.
Golecka, M., Oldakowska-Jedynak, U., Mierzwinska-Nastalska, E. & Adamczyk-Sosinska, E. (2006)Candida-associated denture stomatitis in patientsafter immunosupression therapy. TransplantationProceedings. 38: 155–6.
Hashiguchi, M., Nishi, Y., Kania, T., Ban, S. &Nagaoka, E. (2009) Bactericidal efficacy of glycine-type amphoteric surfactant as a denture cleanerand its influence on properties of denture baseresins. Dental Materials Journal. 28: 307–14.
Hopkins, R. (1987) A Colour Atlas of Pre-prostheticSurgery. Wolfe, London.
Hopkins, R., Stafford, G.D. & Gregory, M.C. (1980)Preprosthetic surgery of the edentulous mandible.British Dental Journal, 148, 183–8.
Hutchins, D.W. & Parker, W.A. (1973) A clinical eval-uation of the ability of denture cleaning solutionsto remove dental plaque from prosthetic devices.New York State Dental Journal, 39, 363–7.
Infanta-Cossio, P., Martinez-de-Fuentes, R., Torres-Carranza, E. & Gutierrez-Peerez, J.L. (2007) BritishJournal of Oral and Maxillofacial Surgery, 45, 658–60.
Jeganathan, S., Payne, J.A. & Thean, H.P. (1997) Den-ture stomatitis in an elderly edentulous Asian pop-ulation. Journal of Oral Rehabilitation, 24, 468–72.

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
128 Prosthetic Treatment of the Edentulous Patient
Kaplan, I., Vered, M., Moskona, D., Buchner, A. &Dayan, D. (1998) An immunohistochemical studyof p53 and PCNA in inflammatory papillary hy-perplasia of the palate: a dilemma of interpretation.Oral Diseases, 4, 194–9.
Keur, J.J., Campbell, J.P.S., McCarthy, J.F. & Ralph,W.J. (1987) Radiological findings in 1135 edentulous patients. Journal of Oral Rehabilitation, 14,183–91.
Khasawneh, S. & Al-Wahadni, A. (2002) Control ofdenture plaque and mucosal inflammation in den-ture wearers. Journal of the Irish Dental Association,48: 132–8.
Konsberg, R. & Axell, T. (1994) Treatment of Candida-infected denture stomatitis with a miconazole lac-quer. Oral Surgery, Oral Medicine, Oral Pathology, 78,306–11.
Kulak, Y., Arikan, A. & Kazazoglu, E. (1997) Exis-tence of Candida albicans and micro-organisms indenture stomatitis patients. Journal of Oral Rehabili-tation, 24, 788–90.
Kulak-Ozkan, Y., Kazazoglu, E. & Arikan, A. (2002)Oral hygiene habits, denture cleanliness, presenceof yeasts and stomatitis in elderly people. Journal ofOral Rehabilitation. 29: 300–4.
Lamey, P.J. & Lewis, M.A.O. (1989) Oral medicinein practice: angular cheilitis. British Dental Journal,187, 15–18.
Lee, D., Howlett, J., Pratten, J., Mordan, N., McDon-ald, A., Wilson, M. & Ready, D. (2009) Susceptibil-ity of MRSA biofilms to denture-cleansing agents.FEMS Microbiology Letters. 291: 241–6.
Lombardi, T. & Budtz-Jørgensen, E. (1993) Treatmentof denture-induced stomatitis: a review. EuropeanJournal of Prosthodontics & Restorative Dentistry, 2,17–22.
MacFarlane, T.W. & Helnarska, S.J. (1976) The micro-biology of angular cheilitis. British Dental Journal,140, 403–6.
Maeda, Y., Kenny, F., Coulter, W., Loughrey, A.,Nagano, Y., Goldsmith, C., Millar, B., Dooley, J.,Lowery, C., Rooney, P., Matsuda, M. & Moore,J. (2007) Bactericidal activity of denture-cleaningformulations against planktonic health-care as-sociated and community-associated methicillin-resistant Staphylococcus aureus. American Journal ofInfection Control, 35: 619–22.
Marcos-Arias, C., Vicente, J., Sahand, I., Eguia, A.,De-Juan, A., Madariaga, L., Aguirre, J., Eraso, E. &Quindos, G. (2009) Isolation of Candida dubliniensisin denture stomatitis. Archives of Oral Biology, 54:127–31.
Moore, T.C., Smith, D.E. & Kenny, G.E. (1984) San-itization of dentures by several denture hygienemethods. Journal of Prosthetic Dentistry, 52, 158–63.
Nikawa, H., Hamada, T. & Yamamoto, T. (1998) Den-ture plaque – past and recent concerns. Journal ofDentistry, 26, 299–304.
O’Driscoll, P.M. (1965) Papillary hyperplasia of thepalate. British Dental Journal, 118, 77–80.
Olsen, I. (1974) Denture stomatitis – occurrence anddistribution of fungi. Acta Odontologica Scandinav-ica, 32, 329–33.
Parvinen, T. Kokko, J. & Yli-Urpo, A. (1994) Micona-zole lacquer compared with gel in treatment ofdenture stomatitis. Scandinavian Journal of DentalResearch, 102, 361–6.
Peltola, P., Vehkalahti, M. & Wuolijoki-Saaristo, K.(2004) Oral health and treatment needs of the long-term hospitalized elderly. Gerodontology, 21: 93–9.
Pires, F.R., Santos, E.B.D., Bonan, P.R.F., De Almeida,O.P. & Lopez, M.A. (2002) Denture stomatitis andsalivary Candida in Brazilian edentulous patients.Journal of Oral Rehabilitation, 29: 1115–9.
Radford, D.R., Challacombe, S.J. & Walter, J.D. (1999)Denture plaque and adherence of Candida albicansto denture-base materials in vivo and in vitro. Crit-ical Reviews in Oral Biology & Medicine, 10, 99–116.
Ralph, J.P. & Stenhouse, D. (1972) Denture-inducedhyperplasia of the oral soft tissues. British DentalJournal, 132, 68–70.
Ramage, G., Tomsett, K., Wickes, B., Lopez-Ribot, J.& Redding, S. (2004) Denture stomatitis – a role forCandida biofilms. Oral Sugery, Oral medicine, OralPathology Oral Radiology & Endodontics. 98: 53–9.
Sachdeo, A., Haffajee, A.D. & Socranski, S.S. (2008)Biofilms in the edentulous oral cavity. Journal ofProsthodontics, 17, 348–56
Sakki, T.K., Knuuttila, M.L., Laara, E. & Anttila, S.S.(1997) The association of yeasts and denture stom-atitis with behavioral and biologic factors. OralSurgery, Oral Medicine, Oral Pathology, Oral Radiol-ogy, & Endodontics, 84, 624–9.
Salonen, M.A., Raustia, A.M. & Oikarinen, K.S. (1996)Effect of treatment of palatal inflammatory papil-lary hyperplasia with local and systemic antifungalagents accompanied by renewal of complete den-tures. Acta Odontologica Scandinavica, 54, 87–91.
Samaranayake, L.P. & MacFarlane, T.W. (1981) A ret-rospective study of patients with recurrent chronicatrophic candidosis. Oral Surgery, Oral Medicine,Oral Pathology, 52, 150–3.
Samaranayake, L.P. (1986) Nutritional factors andoral candidosis. Journal of Oral Pathology, 15, 61–5.

P1: JZP Trim: 246mm X 189mmc09 BLBK351-Basker January 4, 2011 7:51 Printer Name: Yet to Come
Preparation of the Mouth 129
Shulman, J.D., Rivera-Hidalgo, F. & Beach, M.M.(2005) Risk factors associated with denture stom-atitis in the United States. Journal of Oral Pathologyand Medicine, 34: 340–6.
Theilade, E. & Budtz-Jørgensen, E. (1988) Predomi-nant cultivable microflora on removable denturesin patients with denture-induced stomatitis. OralMicrobiology and Immunology, 3, 8–13.
Truhlar, M.R., Shay, K. & Sohnle, P. (1994) Use of anew assay technique for quantification of antifun-gal activity of nystatin incorporated in denture lin-ers. Journal of Prosthetic Dentistry, 71, 517–24.
Webb, B.C., Thomas, C.J. & Whittle, T. (2005) Atwo-year study of Candida-associated stomatitistreatment in aged care patients. Gerodontology, 22,168–76.
Webb, B.C., Thomas, C.J., Willcox, M.D., Harty, D.W.& Knox, K.W. (1998a) Candida-associated denturestomatitis. Aetiology and management: a review.
Part 1. Factors influencing distribution of Candidaspecies in the oral cavity. Australian Dental Journal,43, 45–50.
Webb, B.C., Thomas, C.J., Willcox, M.D., Harty, D.W.& Knox, K.W. (1998b) Candida-associated denturestomatitis. Aetiology and management: a review.Part 2. Oral diseases caused by Candida species.Australian Dental Journal, 43, 160–6.
Webb, B.C., Thomas, C.J., Willcox, M.D., Harty, D.W.& Knox, K.W. (1998c) Candida-associated denturestomatitis. Aetiology and management: a review.Part 3. Treatment of oral candidosis. AustralianDental Journal, 43, 244–9.
Williamson, J.J. (1972) Diurnal variation of Candida al-bicans counts in saliva. Australian Dental Journal, 17,54–60.
Wilson, J. (1998) The aetiology and managementof denture stomatitis. British Dental Journal, 185,380–4.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
10Impressions
This chapter describes the clinical techniquesnecessary for obtaining accurate preliminaryand master impressions. The information pre-sented here is directly related to the theoreticaldiscussion on stability in Chapter 4.
A denture is constructed on a cast of thedenture-bearing tissues. Before this cast can bemade, an impression, or negative likeness, ofthese tissues is obtained. The impression mate-rial, which is held against the tissues and sup-ported by an impression tray, exhibits plasticflow in the initial stages and then subsequentlyhardens or sets. Either plaster of Paris or modelstone is then poured into the impression to formthe cast, or positive likeness, of the denture-bearing tissues.
If maximum accuracy of the casts is tobe achieved, a two-stage impression proce-dure is required. First, preliminary impressionsare taken using stock ‘off the peg’ impres-sion trays and second, the more accurate mas-ter impressions are taken using trays whichhave been ‘tailor-made’ for a particular pa-tient on casts obtained from the preliminaryimpressions.
The denture-bearing areasThe surface anatomy of the denture-bearing ar-eas is illustrated in Figs. 10.1 and 10.2.
The upper denture is normally extendedposteriorly to the vibrating line, which is thejunction between the moving tissues of the softpalate and the static tissues anteriorly (Fig.10.3). Two small depressions in the mucosalsurface, the foveae palatinae, common collect-ing ducts from minor salivary glands, are oftenseen in this region and are therefore a usefullandmark for this junction.
The fibrous band running along the resid-ual ridge is the vestige of the palatal gingivaeand, like the incisive papilla, remains relativelyconstant in position during the remodelling ofthe ridge which follows extraction of the nat-ural teeth. These two structures can thereforebe used as landmarks allowing teeth on com-plete dentures to be placed in positions similarto those of their natural predecessors (Fig. 10.4).This biometric approach also requires specificdesign features to be incorporated into the im-pression trays – for details of these the reader
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
130

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
Impressions 131
••
Hamular notch
Vibrating line
Fovea palatinae
Torus palatinus
Mucogingival line
Buccalsulcus
Buccalfrenum
Labialsulcus
Labial frenum
Incisive papilla
Palatal rugae
Palatal gingivalvestige
Figure 10.1 Surface anatomy ofthe upper denture-bearing area. Thevibrating line indicates the normalposterior extension of the upper den-ture.
is referred to the relevant bibliography (Watt &MacGregor 1976).
In the lower jaw, the denture should extendover the pear-shaped pads. These pads are veryimportant as buttresses helping to resist distalmovement of the denture.
As explained in Chapter 4, it is importantthat the borders of the denture conform to thefunctional form of the sulci so that a good fa-cial seal can be produced and maximum phys-
Retromolar pad
Buccal sulcus
Labial sulcus
Labial frenum Buccal frenum
Lingual frenum
Lingual sulcus
Pear-shaped pad
Buccal shelf
Figure 10.2 Surface anatomy of the lower denture-bearing area. The heavy dotted line indicates the nor-mal posterior extension of the lower denture.
ical retention obtained. Broad coverage of thetissues by the denture also ensures that theocclusal loads are distributed as widely aspossible.
Anatomy of the sulcus tissues
When recording the functional shape of thesulci, it is necessary to have an understand-ing of the anatomical structures that influencethis shape. These are shown diagrammaticallyin Figs. 10.5–10.10.
The form of the sulcus changes markedlyduring function and the shape of the denturemust make allowance for these changes, oth-erwise discomfort or displacement of the den-ture is likely to result. The required shape ofthe denture borders is obtained by careful bor-der moulding of the impression. The followingareas require particular attention.
Mentalis muscle
Contraction of the mentalis muscle raises thesoft tissues of the chin, thus reducing the depthand width of the labial sulcus (Fig. 10.7). If therehas been marked resorption of the underlyingbone, this muscle can exert considerable pres-sure on the labial flange, resulting in its poste-rior and upward displacement.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
132 Prosthetic Treatment of the Edentulous Patient
Vibrating line Figure 10.3 Longitudinal sectionthrough the palate showing correctrelationship of the posterior borderof the upper denture to the junctionbetween the moving and static tis-sues (vibrating line).
Modiolus
The area of strong muscle activity in the lowerlabial sulcus is bounded distally on each sideby the modiolus, a decussation of muscle fi-bres at the corner of the mouth (Fig. 10.8). Nar-rowing of the lower denture base related tothe modiolus is usually necessary to avoid dis-placement (Fig. 10.5). The muscles contribut-ing to the modiolus are able to move or fixthe corner of the mouth in any required posi-tion during function. For example, approxima-
Incisive papilla
Position of canine tip
Palatal gingivalvestige
Furthest horizontal extent of thebuccal polished surface of the denture
X X
A
A = 6 mm
DD = 12 mm
B
B = 8 mmC
C = 10 mm
Figure 10.4 Diagram of the up-per arch showing average distancesfrom the palatal gingival vestige ofthe furthest horizontal extent of thepolished surface of the denture inthe incisal (A), canine (B), premo-lar (C) and molar (D) regions (thebiometric approach). The line (X–X)passing through the posterior bor-der of the incisive papilla can beused as a guide to positioning thetips of the canines.
tion of the modiolus to the buccal surface of thedenture closes the buccal sulci anteriorly dur-ing mastication, so helping to contain the bolusof food as it is being crushed between the pos-terior teeth.
Masseter muscle
On clenching the teeth the anterior borderof the masseter muscle bulges into the disto-buccal sulcus area (Fig. 10.5).

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
Impressions 133
Pterygo-mandibular raphe
Superior pharyngealconstrictor m.
Retromolar pad
Pear-shapedpad
Masseter m.
Buccinator m.
Modiolus
Obicularis oris m.
Palato-glossus m.
Figure 10.5 The buccal and dis-tal anatomical relations of the lowerdenture.
Floor of mouth
When the tongue is elevated, the sublingualfolds are raised and may greatly reduce thedepth and width of the lingual sulcus. This phe-nomenon is most marked when advanced re-sorption of the ridge has occurred.
Zygomatic process of the maxilla
The anatomical structures determining theform of the sulcus in the upper jaw are shownin Fig. 10.9. Particular care must be taken toavoid vertical over-extension in the first mo-lar region, as mucosal injury may result from a
Mylohyoid m.
Palatoglossus m. Sub-lingualsalivary gland
Origin ofgenioglossus m.
Origin ofgeniohyoid m.
Lingual frenum
Origin of buccinator andsuperior pharyngealconstrictor muscles
Figure 10.6 The lingual anatom-ical relations of the lower denture.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
134 Prosthetic Treatment of the Edentulous Patient
Orbicularis oris m.
Depressor labii inferioris m.
Mentalis m.
Figure 10.7 Section through the lower lip showingthe muscles which influence the shape of the labialsulcus.
sandwiching of the soft tissues between thedenture border and the zygomatic process ofthe maxilla.
Coronoid process
Buccal to the tuberosities, the sulcus oftenreaches its deepest point; however, its width isreduced when the mouth is opened because ofthe close proximity of the coronoid process ofthe mandible (Fig. 10.9). If the buccal flangesof the eventual denture are too wide posteri-orly, they will either restrict mandibular open-ing or be displaced by the coronoid process.Thus, the borders of the impression in this re-
Zygomaticusmajor m.
Buccinator m.
Depressoranguli oris m.
Upper incisive m.
Levatoranguli oris m.
Lower incisive m.
Orbicualrisoris m.
Figure 10.8 The muscles con-tributing to the modiolus (dotted cir-cle).
gion should be moulded to the correct widthby the patient moving the mandible from sideto side when the mouth is open.
Buccinator muscle
A certain amount of lateral displacement of thebuccinator muscle by the denture in other ar-eas can occur without causing instability of thedenture. In fact, such displacement can be de-sirable as it can increase retention by improv-ing the facial seal (Fig. 10.10). It can also makeit easier to create a favourable slope of the pol-ished surface for effective muscular control ofthe denture.
The preliminary impressionStock trays
Stock trays are available in a range of sizes andshapes. These trays are constructed in metal orplastic and may be perforated or unperforated.Certain types of plastic trays are intended to bedisposable.
Ideally, a stock tray should cover the en-tire denture-bearing area and allow a uniformspace of a few millimetres in between it and theunderlying mucosa (Fig. 10.11).
However, as the range of sizes and shapesof stock trays is limited and the shape of thedenture-bearing areas so varied, the fit of the

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
Impressions 135
Buccal frenum
Zygomatic process ofthe maxilla
Buccinator m.
Hamular notch
Incisive m.
Compressornares m.
Depressorsepti m.
Labial frenum
Coronoid processin the open position
Figure 10.9 The buccal anatomical relations of the upper denture.
Form of unsupportedbuccal sulcus
Palatal gingival vestigeFigure 10.10 Lateral displace-ment of the buccinator muscle by thedenture to improve facial seal.
Figure 10.11 The ideal relationship of a stock tray to the sulci and denture-bearing mucosa.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
136 Prosthetic Treatment of the Edentulous Patient
tray is usually less than perfect. The tray maybe too wide or too narrow; it may not coverthe denture-bearing tissues posteriorly; the trayflange may be under-extended, finishing shortof the mucosal reflection in the sulcus, or maybe over-extended so that it digs into and dis-torts the sulcus tissues.
It is a common misconception amongstnovice clinicians that accuracy of the prelimi-nary impressions is not particularly importantas it is assumed, incorrectly, that any faults canbe easily corrected when obtaining the mas-ter impressions. However, this is far from thetruth. It is very important that the preliminaryimpression is as accurate as the limitations ofthe stock tray allow, because the more faultsthere are in this impression, the more time-consuming and difficult will be the modifica-tions of the special trays at the next visit. Asa result the quality of the master impression islikely to be compromised.
When it has been decided to use a relativelylow viscosity impression material such as algi-nate for the preliminary impression it is oftennecessary to modify the extension of the stocktray. Under-extension of the tray can be cor-rected by the addition of impression compoundor pink wax to the deficient flange, while over-extension can be corrected, if the tray is plastic,by trimming back the flange with a bur.
Impression materials andtechniques
As even a correctly selected and modified stocktray is very unlikely to have a perfect relation-ship to the denture-bearing tissues, it is de-sirable for the impression material chosen fora preliminary impression to have a relativelyhigh viscosity, as this allows it to compensatebetter for the shortcomings in fit and extensionof the stock tray.
Alginate
Alginates vary considerably in their viscosityand the high viscosity type is most suitable
for preliminary impressions. Alternatively, thepowder–water ratio of the more fluid alginatescan be increased to achieve the required consis-tency.
Retention of alginate to the impressiontrayAlginate does not adhere to the tray surfaceand so retention must be provided by means ofa perforated tray or an adhesive. Perforationsallow alginate to flow through and ‘rivet’ thebody of the impression to the tray. If adhesiveis used, it should be applied thinly to the entireinner surface of the tray and also carried overthe peripheries to include a few millimetres ofthe outer surface. Time should be allowed af-ter application of the adhesive for it to becometacky, a process which can be speeded up con-siderably by dispersing the adhesive over thesurface of the tray with a stream of air from atriple syringe.
Border moulding the lower impressionThe lower impression is usually taken first as itis easier for the patient to tolerate than the up-per. When the impression is seated in the mouththe patient is asked to raise the tongue to con-tact the upper lip and to sweep the tongue totouch each cheek in turn before returning tomaintain contact with the upper lip until thealginate has set. This tongue movement willraise the floor of the mouth and tense the lin-gual frenum, causing the alginate in the over-extended parts of the lingual periphery to bemoulded to conform more closely to the func-tional depth of the sulcus. If the tongue is al-lowed to relax and fall back into the floor ofthe mouth while the impression material is stillfluid, the material may flow down into the floorof the mouth and the impression will becomeoverextended once more. Buccal and labial bor-der moulding is achieved by firm stretchingof the relaxed lips and cheeks with the fin-gers. It is essential that the clinician supportsthe tray carefully during these border mouldingmanoeuvres.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
Impressions 137
Border moulding the upper impressionIf the sulci buccal to the maxillary tuberositiesare deep, air may be trapped as the loaded im-pression tray is inserted. To overcome this prob-lem, these areas can be pre-packed with algi-nate before seating the tray. The tray is firstloaded and placed to one side; then with thecheek reflected and the patient’s mouth halfclosed, alginate is placed into the buccal sul-cus with a spatula or finger. The loaded trayis then quickly inserted into the mouth, po-sitioned over the ridge and seated with suf-ficient pressure to cause the alginate to flowand record the shape of the tissues. Excess al-ginate will flow into the sulci, producing anover-extended impression. This over-extensionmust be corrected by carrying out bordermoulding.
Removing the impression from the mouthWhen the border moulding is complete, thetray must be kept perfectly still until the algi-nate has set, otherwise strains will be inducedin the impression. Then when the impressionhas been removed from the mouth, gradual re-lease of these strains will take place, causingdistortion. In order to remove the set impres-sion from the mouth, the border seal must bebroken. This is achieved by first asking the pa-tient to half close the mouth; the cheek is thenreflected away from the buccal surface of theimpression on one side to allow access of airto the periphery, and a sharp jerk is applied tothe tray handle. If the impression is removedslowly, distortion of the alginate is more likelyto occur.
The completed impressionSaliva should be removed from the impres-sion surface by rinsing briefly under a coldtap. Excess water is shaken off and the im-pression is inspected carefully. A satisfactorycompleted impression will include the entiredenture-bearing area. The surface of the im-pression should be smooth and show evidence
Figure 10.12 A lower impression in alginate show-ing a border which has been molded by the adjacenttissues. Correct extension in the lingual pouches hasbeen achieved by suitable extension of the tray. Theline drawn on the impression provides a useful guidewhen the cast is trimmed.
of having been moulded by the tissues (Fig.10.12). The border areas should be rounded andinclude impressions of the frenal attachments.
The dimensional instability of alginateAn alginate impression is particularly suscep-tible to dimensional change developing as a re-sult of an increase or a decrease in its water con-tent. These two processes are:
1. Imbibition – the absorption of water2. Syneresis – the loss of water
If water is left on the surface of the impressionimbibition will take place causing the alginateto swell. If the impression is left in a dry at-mosphere syneresis will occur with consequentshrinkage of the alginate. Therefore it is essen-tial that a satisfactory impression is rinsed, dis-infected, covered as soon as possible with adamp napkin and placed in a plastic bag. Castsshould be poured as soon as possible. Whilethe impression is waiting to be poured, it mustnot be allowed to rest on any surplus alginatewhich has flowed over the posterior border ofthe tray, as this will cause distortion.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
138 Prosthetic Treatment of the Edentulous Patient
Impression compound
This is a thermoplastic material which softenswhen heated in a water-bath to temperaturesbetween 55◦C and 70◦C. The high viscosity ofthe material and the fact that it becomes rigidwhen chilled make it unnecessary to correct anyunder-extensions of a stock tray before takingthe impression.
Preparing the materialAs the impression compound softens in thewater-bath, a portion of sufficient size to takethe planned impression is kneaded with the fin-gers by folding the material inwards from theperiphery of the mass to the centre. This pro-duces a smooth, crease-free, surface on one sideof the compound; it also improves flow andhelps to give the material a uniform consis-tency.
Obtaining the lower impressionThe lower impression is usually obtained be-fore the upper. The portion of compound isformed into a cylinder and then extended to thelength of the tray by pulling on either end. Thiscreates a dumb-bell-shaped specimen whichdistributes the material along the tray in a fash-ion corresponding to the width of the denture-bearing area to be recorded – narrow anteri-orly and broad posteriorly. The compound isplaced in the dried tray so that the smooth sidewill be towards the tissues and is then mouldedwith the fingers to the approximate shape ofthe ridge. The surface of the compound canbe lightly flamed to improve its flow and thentempered in warm water to avoid burning thepatient. Coating with petroleum jelly is some-times recommended to improve surface flow.The tray is then seated firmly in the mouthand supported while border moulding is car-ried out as described for the alginate prelimi-nary impression. However, in this instance, asthe impression compound is more viscous thanalginate, the moulding must be executed withgreater firmness, otherwise over-extension of
the impression will occur. When the impres-sion has cooled and hardened, it is removedfrom the mouth and inspected. If minor faultsare present, corrections can be carried out bytrimming away excess material with a hot waxknife, or by adding new compound to repairdeficiencies and then resoftening the surface ofthe impression before reseating it in the mouth.If there are major faults, for instance in posi-tioning the tray, the impression is retaken. Oncea satisfactory impression has been obtained, itmust be hardened by thoroughly chilling it incold water.
Obtaining the upper impressionThe impression for the upper jaw is obtainedby placing a golf-ball-sized portion of softenedcompound into the centre of a dried tray andpre-forming it with the fingers to the shapeof the ridge and palate. The procedure then isas described for the lower impression. Com-pleted impressions in compound are shown inFig. 10.13.
The alginate wash impression techniqueA satisfactory impression in compound is oftenquite adequate for producing a cast on which toconstruct a special tray. However, there are oc-casions when the clinician might require a moreaccurate picture of the mucosa so that the po-tential denture-bearing area can be visualisedmore easily. This can be achieved by refiningthe initial compound impression with a washimpression in alginate as follows:
� Obtain the best possible impression in com-pound and dry it thoroughly.
� Trim back the borders of the impression by1–2 mm with a heated wax knife.
� Apply a thin layer of alginate adhesive to theimpression surface.
� Load the compound impression with a smallamount of low viscosity alginate, seat it fullyon the tissues and complete border trimmingas before.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
Impressions 139
Figure 10.13 Upper and lowerimpressions taken in impressioncompound.
The completed impressionsThe completed satisfactory impressions are dis-infected before being sent to the laboratory.
Communication with the dentaltechnician
In order to achieve the best possible treatmentoutcome, it is essential that the clinician anddental technician work together as a team. Anadequate understanding of each other’s workand contribution, together with effective two-way communication, are of paramount impor-tance in achieving success. The clinician there-fore needs to ensure that at the end of each clini-cal stage, when sending items to the laboratory,all the information required by the dental tech-nician is provided together with a clear indica-tion of the clinician’s requirements for the nextclinical stage. This communication traditionallytakes the form of a comprehensive written pre-scription, but on occasion the dental technicianwill need additional information or clarifica-tion. Under such circumstances, the value ofdiscussing the case face to face, or on the tele-phone cannot be underestimated. Increasingly,electronic links are likely to play a significant
part in contributing to effective communicationbetween the dental surgery and the laboratory.
The laboratory prescription
After the preliminary impressions have beenobtained, the following information shouldnormally be entered on the laboratory prescrip-tion by the clinician:
� Confirmation that all items sent from theclinic to the laboratory have been disin-fected.
� Materials to be used for the special trays.� Details of the design of the special trays in-
cluding:◦ Spaced or close fitting.◦ Size and location of any stops to be pre-
formed in spaced special trays.◦ Perforated or not.◦ Type of handle and any finger rests.◦ Any special requirements, e.g. a special
tray for a flabby ridge.� The written prescription can be sup-
plemented by the clinician marking therequired extension of the special trays on thepreliminary impressions with an indelible

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
140 Prosthetic Treatment of the Edentulous Patient
Mucosa
Denture base
Bone
Figure 10.14 Occlusal loadstransmitted by the denture to themucosa will tend to be greatest(arrows) where the mucosa isthinnest.
pencil if the impression is in alginate, orwith the tip of a wax knife if the impressionis in impression compound.
Quality control and enhancement
An audit of the quality of this clinical stage canbe most fruitful if the quality of the end product– the special tray – is assessed. The audit mightinclude the following:
� Is there avoidable over-extension or under-extension of the special tray, particularly inthe ‘high risk’ areas such as the upper pos-terior border and tuberosity regions and, inthe lower, the pear-shaped pads and lingualpouches?
� Has the dental technician been providedwith sufficient information in the prescrip-tion?
� Has the dental technician produced whatwas asked for?
The master impressionMucostatic and mucodisplaciveimpression techniques
The clinician’s goal when taking master im-pressions is to record as accurately as possiblethe shape of the mucosa overlying the alveo-lar ridges and hard palate together with thefunctional depth and width of the sulci. How-ever, there is some disagreement as to the bestmethod of achieving this goal.
Mucostatic impression
The mucosa overlying the alveolar ridges andhard palate is not of uniform thickness. Con-sequently, if the clinician uses a mucostatictechnique which applies minimal pressure tothe tissues, and therefore records their restingshape, there is a possibility that the subsequentdistribution of occlusal loads by the finisheddentures will be uneven (Fig. 10.14). However,as the impression surface of the denture con-forms closely to the mucosa surface of the un-derlying mucosa, both when the denture is un-der load and when it is not, physical retentionwill be optimal.
Mucodisplacive impression
The alternative approach, a mucodisplacivetechnique, applies pressure to the mucosa dur-ing the impression-taking procedure so that theshape of the tissues under load is recorded. Thisapproach may have the advantage that occlusalloads are more evenly dispersed over the tis-sues, but has the disadvantage that the physi-cal retention of the denture when the teeth areapart is likely to be less than that obtained witha mucostatic impression technique (Fig. 10.15).
Selecting the appropriate impressiontechnique
Should the mucosa be recorded in its restingstate or in its displaced state? In most cases,it will be found that the best results may bemost simply obtained by a mucostatic tech-nique. Pressure on the tissues is reduced as far

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
Impressions 141
Resting shapeof mucosa
Displaced shapeof mucosa
Denture base
a
b
c
Figure 10.15 The mucodisplac-ive impression technique: (a) the dif-ference in the shape of the mucosalsurface produced by a mucostatictechnique (dotted line) and a mu-codisplacive technique (continuousline); (b) the impression surface, ob-tained by a mucodisplacive tech-nique, fits the mucosa closely whenthe denture is under occlusal load;(c) when the occlusal load is re-moved the mucosa returns to its rest-ing shape and the denture ceases tofit accurately.
as possible by using an impression material oflow viscosity. Impression plaster, zinc oxide-eugenol impression paste and low viscosity al-ginate or silicone rubber are examples of suit-able materials.
In some patients, a moderate variation inmucosal compressibility may be present anda mucostatic impression, particularly in thecase of the lower jaw, results in a denture thatdistributes the occlusal loads unevenly withconsequent mucosal injury and associated dis-comfort. In this situation, it may be advis-able to record the shape of the mucosa in adisplaced state by using an impression mate-rial of high viscosity. The load applied dur-ing the impression-taking procedure should bethe same as that occurring during function.A method which fulfils these requirements isknown as a functional impression techniqueand is described on p. 237.
Special trays
To ensure accuracy of the master impressionspecial trays must be made of a material that isdimensionally stable and rigid enough not todeform under the stresses of impression taking.Light-cured or cold-curing acrylic resins satisfythese requirements and are the tray materialsof choice.
Spaced trays
In order to avoid permanent distortion of anelastic impression material as it is withdrawnfrom undercut areas, an adequate uniformthickness of the material is required. Thespecial tray should be constructed on thepreliminary cast after a spacer of appropriatethickness for the planned impression materialhas been adapted to it (Fig. 10.16). Alginate

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
142 Prosthetic Treatment of the Edentulous Patient
Spacer Tray material
Figure 10.16 A spaced special tray is constructedby adapting the tray material over a spacer which hasbeen applied to the cast.
is the most commonly used elastic impres-sion material for edentulous patients and thisrequires a spacer of about 3 mm. The elastomershave a better elastic recovery than alginate andso require less spacing of the special tray.
Close-fitting trays
Close-fitting trays are used with impressionmaterials that are used in thin section such aszinc oxide-eugenol impression paste and light-bodied elastomers.
It is an advantage if a lower acrylic close-fitting tray has vertical pillars in the premo-lar regions to act as finger rests (Fig. 10.17).
Figure 10.17 A lower close-fitting acrylic trayshowing the position of the finger rests in the premolarregions.
These rests keep the fingers, which stabilise thetray and support the impression, well clear ofcritical border areas of the impression while itsets. If this is not done, inaccuracies will resultfrom the fingers restricting the border mould-ing movements of the soft tissues. They canalso displace excess impression material intothe sulci. The anterior stub handle is for hold-ing and manipulating the tray. Its shape avoidsinterference with the lower lip which otherwisecan make placement of the tray difficult andcan hinder border trimming of the impressionin that area.
The use of stopsIf an unmodified spaced special tray is tried inthe mouth to check its border extension, it willbe seated in contact with the underlying mu-cosa (Fig. 10.18a). In this position, the borders ofthe tray bear a different relationship to the sul-cus to the one that will exist when the impres-sion is taken. In this latter instance, the tray willbe separated from the mucosa by a few millime-tres of impression material (Fig. 10.18b). Thus, aborder that appears to be correctly extended onfirst inspection may be under-extended whenthe impression is taken.
Placing stops in the tray before checking andcorrecting the borders will overcome this prob-lem, ensuring a uniform thickness of about 2–3mm of impression material, and stabilising thetray during impression taking.
In the lower tray these stops are placed in theincisal region and over the pear-shaped pads. In
ba
Figure 10.18 (a) Tray in contact with the mucosa –the border appears to be correctly extended. (b) Trayseparated from the mucosa by the impression mate-rial – tray border under-extended.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
Impressions 143
the upper tray the stops are placed in the incisalregion and along the line of the post-dam.
There are several ways that stops can be pro-duced:
� During construction of an acrylic tray in the lab-oratory. Windows are cut in the wax spacerat appropriate locations on the cast used tomanufacture the impression tray (Fig. 10.19).The stops are produced by the acrylic doughflowing into these windows and contactingthe model. This is the preferred method ofproducing stops as it is accurate and saveschair side time.
� At the chair side in the mouth. Tracing com-pound is applied to the tray and tem-pered in warm water to avoid burning themucosa. The tray is then seated in the mouthto mould the tracing compound to the ridge
Figure 10.19 The upper cast and wax spacer,showing where the stops will be created (see text fordetails).
tissues creating the required space betweenthe tray and mucosa.
� At the chair side on the cast. Tracing compoundis applied to the tray as in the previous para-graph and the tray is then seated on the wetcast. This approach has the advantage thatit is easier to visually check that the tray iscentred correctly on the ridge while the stopsare being formed than it is when seating thetray in the mouth.
Once the stops have been prepared the borderextension of the tray is checked intra-orally.
Checking the special tray
As a special tray is made on a cast poured froma relatively inaccurate preliminary impression,it will commonly be found on checking the trayin the mouth that the periphery does not con-form to the shape of the sulcus tissues in allareas. Both over-extension and under-extensionmay be present.
Visual assessmentThe tray can be checked visually in most ar-eas of the mouth with the exception of thelingual sulcus where the tongue obscures theview in the posterior regions. Over-extension inthese regions is present if the tray is displacedupwards when the patient raises the tongueto contact the upper lip. However, as under-extension is the more common fault, it is wiseto assume its presence if over-extension cannotbe demonstrated.
The diagnostic impressionA rapid and effective way of checking tray ex-tension is to take a diagnostic impression withalginate. For this it is not necessary to applyadhesive to the tray, which simplifies subse-quent removal of the impression material fromthe tray once it has served its purpose. Care-ful border moulding of the diagnostic impres-sion is carried out and subsequent inspection

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
144 Prosthetic Treatment of the Edentulous Patient
of the completed impression gives a very clearrecord of the accuracy of the tray extensionin all areas. The tray can then be corrected asnecessary.
Correcting the special tray
Correction of over-extensionOver-extension must be corrected by trimmingaway the offending acrylic resin with a bur orstone until the height of the flange has beenreduced by the appropriate amount. If over-extension of the special tray is not corrected, thesulcus tissues will be stretched and the masterimpression will be over-extended. If this faultis not recognised before the denture is finished,the over-extended flange will injure the tis-sues; in addition, elastic recoil of the displacedsulcus tissues will cause instability of thedenture.
Correction of under-extensionUnder-extension is corrected by extending thetray in the region of the deficiency with aborder-trimming material. These additions tothe tray must then be carefully border moulded.It should be remembered that the common ar-eas of under-extension of the upper denture arethe posterior border and around the tuberosi-ties, while the lower denture is often under-extended in the regions of the pear-shaped padsand lingual pouches (Basker et al. 1993). Sowhatever technique is used, the greatest caremust be taken to ensure that the impression in-cludes these vital areas.
If an under-extended tray is not corrected,there are two possible sequelae:
1. The impression material is not carried to thefull depth of the sulcus, so that the finisheddenture is under-extended.
2. The impression material reaches the fullfunctional depth of the sulcus but is not sup-ported by the under-extended tray. Whenthe cast is poured, the weight of the artifi-
Figure 10.20 Distortion of unsupported elastic im-pression material by the artificial stone.
cial stone will distort the unsupported partof the elastic impression material, resultingin a denture which is an inaccurate fit (Fig.10.20).
In order to obtain the best possible recording ofthe lingual sulcus, it is essential to train the pa-tient to make the following tongue movementsbefore making additions lingually to the lowertray: the tip of the tongue is placed in one cheekand then swept round anteriorly to the othercheek; this is repeated two or three times andthen the tongue is raised to contact the upperlip. The tongue should not be protruded furtherthan the lip as such a movement is rarely usedin normal function and only results in an exces-sive and unnecessary reduction in depth of thelingual flange of the eventual denture. Anotheruseful technique is to ask the patient to push thetongue against the hard palate. This movementactivates the muscles in the floor of the mouthand assists in obtaining accurate border exten-sion.
If biometric guides (mentioned briefly onp. 130), are being followed in the design of adenture, a border-trimming material should beused to extend the tray flanges laterally to sup-port the cheek and lips in the positions shownin Fig. 10.4.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
Impressions 145
Creating a post-damIf the post-dam (p. 101) is to be created by com-pressing the mucosa while obtaining the finalimpression, rather than by cutting a groove intothe palate of the master cast, the following pro-cedure is adopted. Firstly, tracing compound isplaced along the posterior border on the inneraspect of the adjusted tray so that when thetray is seated with sufficient pressure, the mu-cosa will be compressed by the tracing material.Secondly, after trimming the tracing compoundback to the posterior border of the tray, a rel-atively low viscosity impression material is se-lected for the definitive impression. The tray isthen inserted with enough pressure to displacethe impression material from over the tracingcompound. If this has been done correctly thetracing compound will be visible through a thinveneer of the set impression material. This com-pression caused during impression taking willresult in a permanent denture base which has araised lip along the posterior border on its im-pression surface. This projection, the post-dam,compresses the palatal mucosa once the den-ture is placed in the mouth and thus creates theborder seal.
Border trimming materials
Materials available for the correction of under-extended impression trays include tracing com-pound and high viscosity elastomers.
Tracing compound, which is thermoplastic,has the advantage that it can be progressivelycorrected, by resoftening or by adding furthermaterial, until the tray extension is satisfactory.The setting of the high viscosity elastomers, onthe other hand, is by an irreversible chemical re-action and requires a ‘one shot’ approach; thus,if the border trimming is deficient at the firstattempt the entire procedure will have to be re-peated.
The technique for using tracing compoundis summarised in Fig. 10.21. The tracing com-pound should be applied in increments to thetray border, with each increment being border
a b
c d
Figure 10.21 A method of applying tracing com-pound for correction of under-extension: (a) the trac-ing compound is softened and placed on the outersurface of the tray – sufficient bulk of material shouldbe used to allow a broad area of attachment and toretain heat so that there is an adequate working timefor border moulding; (b) the compound is tempered inwarm water and moulded with the fingers to produce aflange; (c) border moulding is carried out and then thetray is chilled in cold water; (d) finally, the space be-tween the tracing compound and the alveolar ridge isre-established by removing material with a wax knife.
moulded before the next addition is made. Ifadequate moulding has not been achieved atthe first attempt, the over-extended compoundis resoftened using a fine flame, tempered inwarm water to avoid burning the mucosa,and border moulded once more. When theadjustment is complete, the tracing compoundis chilled in cold water. The finished result isshown in Fig. 10.19.
Impression materials andtechniques
Alginate
This material is elastic when set and therefore isindicated where bony undercuts are present.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
146 Prosthetic Treatment of the Edentulous Patient
Figure 10.22 A satisfactory upper alginate impres-sion.
Whereas high viscosity alginates are indi-cated for the preliminary impression, they arenot recommended for master impressions asthey readily cause mucosal displacement, par-ticularly in the border areas. Thus, a low vis-cosity type should be used.
The procedures for manipulating the algi-nate and obtaining the impression are the sameas those described for the alginate preliminaryimpression (p. 134).
Figure 10.22 shows a satisfactory impressionin which the borders are rounded and well de-fined.
It is important that having carefully recordedthe shape of the borders this valuable informa-tion is reproduced on the cast. A useful guidecan be given to the dental technician by draw-ing a line on the alginate with indelible pencil3–4 mm beyond the border of the impression(Fig. 10.23). This line is transferred to the castmaterial and acts as a landmark, discouragingover-trimming of the cast which would other-wise result in loss of information concerningthe functional width of the sulcus (Fig. 10.24).
Zinc oxide-eugenol impression paste
This excellent impression material is rigid whenset and is dimensionally stable, so it is preferredto alginate in all cases where there are no bonyundercuts. Other advantages of this material
Figure 10.23 An alginate impression showing theposition of the indelible pencil line placed as a guideto subsequent trimming of the cast.
accrue from the fact that it is used in a close-fitting, rather than a spaced tray, i.e.:
� The overall bulk of the impression is kept toa minimum and so is better tolerated by thepatient.
� Where the sulcus is narrow, it is easier toavoid displacement of the buccal mucosa(Fig. 10.25).
� It is easier to obtain an impression of a re-sorbed lower ridge without the mucosa ofthe floor of the mouth becoming trappedwithin the border of the tray.
Checking and correcting the trayextensionAs zinc oxide-eugenol impression paste is usedin a thin film, stops are not added to thespecial tray. Instead, the borders should be
a b
Figure 10.24 Cross section through (a) a correctlytrimmed and (b) an overtrimmed cast.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
Impressions 147
b a
Figure 10.25 (a) A spaced tray may displace thebuccal mucosa laterally from its normal position. (b) Amore accurate recording of the sulcus width is possiblewith a close-fitting tray.
checked with the tray held in contact withthe mucosa. Again a diagnostic impression inlow viscosity alginate is an excellent way ofcarrying out a comprehensive check on thetray extension. Over-extension of acrylic traysmay be corrected with an acrylic bur, whileunder-extension may be corrected with anyof the border-trimming materials mentionedpreviously. The procedure differs from thatdescribed for spaced trays in that when theborder-trimming material has set, a space doesnot need to be re-created in that area.
A completed impression is shown in Fig.10.26. A clear guide to the correct trimming ofthe cast is created by the wax beading which ad-heres easily to the impression paste (Fig. 10.27).
Figure 10.26 A satisfactory lower zinc oxide-eugenol impression paste impression.
Figure 10.27 The addition of a wax beading toguide the cast trimming.
Impression plaster
Impression plaster is a good impression ma-terial primarily for the upper edentulous jawwhere there are no bony undercuts. A spacedspecial tray should be used so that the impres-sion has adequate strength when set, and anyfragments which break off when the impressionis removed from the mouth are large enough tobe relocated accurately and to be attached to themain part of the impression.
Impression plaster has the following proper-ties which are clinically relevant:
� Rigid when set. However, if small bony un-dercuts are present the use of impressionplaster is not ruled out. The material whichenters the undercut area will break off whenthe impression is removed from the mouthand can then be re-attached to the impres-sion as mentioned above.
� Dimensionally stable.� Low viscosity. Impression plaster is therefore
a good material to use when a mucostaticimpression is required.
� Susceptible to excess saliva. It is difficult to ob-tain a satisfactory lower impression in pa-tients who salivate profusely because thesaliva mixes with the plaster and a rough,friable surface is produced.

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
148 Prosthetic Treatment of the Edentulous Patient
Figure 10.28 An upper plaster master impressionon which a pencil line has been drawn at the posteriorborder to indicate the position of the post-dam.
A satisfactory plaster impression is shown inFig. 10.28 and the position of the post dam hasbeen indicated on the impression with an in-delible pencil. The completed impression is dis-infected before being sent to the laboratory.
Elastomers
The elastomers include the following impres-sion materials:
� Condensation-cured silicone rubbers� Addition-cured silicone rubbers� Polysulphide rubbers� Polyethers
The silicone materials are relatively expensive,but in spite of the modest cost penalty com-pared with alginate and zinc oxide-eugenol im-pression paste they are becoming increasinglypopular for complete denture impressions. Thesilicone elastomers have the following desir-able clinical properties:
� Excellent elastic recovery.� Excellent dimensional stability.� A wide range of viscosities. The silicone materi-
als vary from heavy-bodied putties to light-bodied perfecting pastes, creating a versatilegroup of materials suitable for a wide variety
of clinical applications. These range from theuse of putties for border trimming to perfect-ing pastes for wash impressions.
� They are clean and easy to handle.� A wide range of working and setting times.
This versatility makes them appropriate formost techniques. For example, some ma-terials with an extended setting time aresuitable for functional impressions of boththe denture-bearing mucosa and the neu-tral zone. Other materials with short settingtimes allow conventional impressions to betaken rapidly and thus reduce patient dis-comfort.
� Non-adherence to dry mucosa. The low viscos-ity silicone materials are preferred alterna-tives to zinc oxide-eugenol impression pastefor patients with dry mouths, as the lattermaterial can adhere to and irritate the drymucosa.
Communication with the dentaltechnicianThe laboratory prescription
After the master impressions have been ob-tained the following information should nor-mally be entered on the laboratory prescriptionby the dental clinician:
� Confirmation that all items sent from theclinic to the laboratory have been disin-fected.
� Materials to be used for the bases of therecord blocks. Normally, these are acrylicresin or shellac. The relative merits of thesematerials and the indications for their useare discussed at the beginning of the nextchapter.
� The written prescription can be supple-mented by the dental clinician delineatingthe borders of the impression with a pencilline or wax beading to indicate to the dentaltechnician the required limit of cast trim-ming. It is worth emphasising in this context

P1: JZP Trim: 246mm X 189mmc10 BLBK351-Basker January 19, 2011 13:12 Printer Name: Yet to Come
Impressions 149
Figure 10.29 Upper cast with the full depth andwidth of sulci carefully maintained.
that the best prescription for the eventualdenture border is an accurately trimmed castwhich has been produced from a carefullytaken impression (Fig. 10.29).
Quality control andenhancementAn audit of a series of cases at the appropriatetime might include the following:
� Did the recording of the functional widthand depth of the sulcus ensure that the bor-ders of the eventual denture covered themaximum area?
� Did the borders of the bases of the recordblocks/eventual dentures require no morethan minimal adjustment?
� Did the dental technician maintain the fullsulcus depth and width on the master casts?
Were the bases of the record blocks extendedto the full depth of the sulcus on the mastercast?
� Was the dental technician provided with allthe information necessary to provide thenext item of work?
References and additionalreadingBasker, R.M., Ogden, A.R. & Ralph, J.P. (1993)
Complete denture prescription – an audit ofperformance. British Dental Journal, 174, 278–84.
Lawson, W.A. (1978) Current concepts and practicein complete dentures. Impressions: principles andpractice. Journal of Dentistry, 6, 43–58.
Nairn, R.I. (1964) The posterior lingual area of thecomplete lower denture. Dental Practitioner andDental Record, 15, 123–30.
Shannon, J.L. (1972) The mentalis muscle in relationto edentulous mandibles. Journal of Prosthetic Den-tistry, 27, 477–84.
Strang, R., Whitters, C.J., Brown, D., et al. (1998) Den-tal materials: 1996 literature review. Part 2. Journalof Dentistry, 26, 273–91.
Watt, D.M. (1978) Tooth positions on complete den-tures. Journal of Dentistry, 6, 147–60.
Watt, D.M. & MacGregor, A.R. (1976) Designing Com-plete Dentures. W.B. Saunders, Philadelphia.
Wilson, H.J. (1966a) Elastomeric impression materi-als. Part 1: The setting material. British Dental Jour-nal, 121, 277–83.
Wilson, H.J. (1966b) Elastomeric impression materi-als. Part 2: The set material. British Dental Journal,121, 322–8.
Wilson, H.J. (1966c) Some properties of alginate im-pression materials relevant to clinical practice.British Dental Journal, 121, 463–7.

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
11Recording Jaw Relations – Clinical Procedures
This chapter describes the basic technique forrecording the jaw relationship. This clinicalstage is, in fact, concerned with far more thanestablishing the relationship between maxillaand mandible. It is the process by which the in-formation essential for the production of newdentures is transferred from the patient to thedental laboratory so that the dental technicianis provided with what amounts to a blueprintfor the prostheses.
This chapter focuses primarily on recordingthe jaw relationship for patients without exist-ing dentures. However, in Chapter 8 the pointwas made that most patients require replace-ment dentures, and that the existing ones pro-vide a great deal of information which will beinvaluable at this clinical stage. Therefore werecommend that the reader also refer to Chap-ter 8 to obtain a more comprehensive picture ofthe clinical procedure.
Measuring the rest verticaldimensionThe rest vertical dimension is recorded to pro-vide a point of reference from which the oc-clusal vertical dimension of the dentures canbe calculated by subtracting the required free-way space (usually approximately 3 mm). De-termining the rest vertical dimension is one ofthe more difficult tasks in dentistry, as indicatedby the large number of denture problems thatcan be attributed to errors in this dimension.
To reduce the chance of error and to coaxthe mandible into the rest position, the patientmust be completely relaxed. This can be encour-aged by paying particular attention to the fol-lowing points:
� Many patients are apprehensive whenthey enter a dental surgery. The clinician
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
150

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 151
therefore needs to make every effort toreassure the patient and allay any feelingsof anxiety.
� The patient should be seated in a com-fortable, upright position in the dentalchair.
� External stimuli should be reduced to aminimum, as disturbing noises, or a brightlight shining in the patient’s eyes, are likelyto increase activity of the mandibular mus-culature and thus reduce the rest verticaldimension.
� Relaxation may be further promoted if thepatient’s eyes are closed, although it is im-portant that the clinician explains what is tobe done at the time, otherwise this exercisemay achieve quite the opposite effect and in-duce a state of apprehension.
� Some patients are helped if they are asked toswallow, lick their lips, or make the sound‘m’ before trying to relax the mandible.
Before measuring the rest vertical dimension,the clinician must be satisfied that the patientis truly relaxed. Visual assessment of facial fea-tures and proportions assists the clinician injudging the progressive development of thisstate of mind. It is pointless making a measure-ment if the patient appears tense, or if the lowerthird of the face is clearly reduced or increasedin height.
The rest vertical dimension is measured asthe distance between two selected points, onerelated to the upper jaw and one to the lowerjaw. Two methods are commonly used to makethis measurement, the Willis gauge and the‘two-dot’ technique (Fig. 11.1). It is most impor-tant to appreciate the inherent inaccuracies ofboth measuring methods. As a general rule, itis advisable to repeat measurements of the restvertical dimension on several occasions dur-ing the appointment. This gives the clinicianan idea of the reproducibility and reliability ofthe recordings. Above all, it should be borne inmind that all clinical methods of measuring therest vertical dimension are based to a greater
a
b
Figure 11.1 Two methods of measuring the rest ver-tical dimension and the occlusal vertical dimension. (a)The Willis gauge. (b) The two-dot technique; the dis-tance between the dots is measured with a pair ofdividers.
or lesser extent on what is in reality intelligentguesswork.
The Willis gauge
In the case of the Willis gauge, three points re-quire attention to minimise the potential errorsof this technique.
The position of the fixed arm under thenose
If the patient has a well-defined naso-labialangle, the fixed arm can be positioned with

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
152 Prosthetic Treatment of the Edentulous Patient
a b
Figure 11.2 (a) The shape of the naso-labial angleallows the fixed arm of the Willis gauge to be locatedaccurately. (b) A location mark may be used where thenaso-labial angle is obtuse.
reasonable accuracy. However, if the naso-labial angle is obtuse, positioning of the gaugebecomes less precise. Under these circum-stances it helps if a small mark is made on theskin at the angle so that the fixed arm can bepositioned in relation to it (Fig. 11.2).
The position of the sliding arm underthe chin
The sliding arm should be moved so that it onlyjust touches the under-surface of the chin, be-cause if pressure is applied to the sub-mentaltissues by the gauge, errors will result fromthe mandible being pushed upwards. Also, thetissues will be compressed by an amount thatwill be impossible to reproduce consistentlyon subsequent measurements. Further inaccu-racies may arise if the shape of the chin is suchthat it prevents positive location of the slidingarm. However, this difficulty can be avoided bymodifying the gauge to reduce the length of thearm and to alter its angle (Fig. 11.3).
The vertical orientation of the gauge
The vertical orientation of the gauge should besuch that it makes contact with the face both
a b
Figure 11.3 (a) The shape of the chin prevents pos-itive location of the sliding arm of the Willis gauge. (b)Sliding arm modified to allow more accurate position-ing.
above and below the lips. The handle contactsthe upper lip under the nose and also contactsthe chin in the mental region, so that its longaxis is in line with the long axis of the face.This keeps any variation in vertical orientationof the gauge to a minimum during successivemeasurements (Fig. 11.4). However, consistentorientation of the gauge is difficult to achievewith facial profiles associated with full lips or asevere skeletal class II jaw relationship, becausethe handle of the gauge cannot be placed in con-tact with the chin.
The two-dot technique
When the two-dot technique is used, the dot re-lated to the upper jaw is best placed on the tipof the nose and not on the upper lip becausethe latter is too mobile to provide a reliable lo-cation. The rest vertical dimension is then mea-sured using dividers. This technique has beenshown to be particularly subject to error. Thecause is usually movement of the dot on thechin due to an inability by the patient to thor-oughly relax the muscles of facial expression.

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 153
a b c
Figure 11.4 (a) Incorrect; (b) and(c) correct positioning and orienta-tion of the Willis gauge.
A particular complication is that an increasein occlusal vertical dimension will not necessar-ily be associated with a corresponding increasein the distance between the dots because, asthe mandible moves down away from the max-illa, there is a tendency for the patient to try tomaintain a lip seal. The effort by the circum-oralmusculature needed to keep the lips togetherpulls the dot on the chin upwards.
However, in spite of these limitations, thetechnique remains a useful one to have inreserve for certain types of facial profile andfor bearded patients for whom consistentpositioning of the Willis gauge may be difficultor impossible.
The post-damBefore discussing the construction of recordblocks, it is helpful to consider a related subject,the post-dam.
The physical forces of retention are createdand maintained in the sulci by a valve-like sealbetween the flange of the denture and the mu-cosa. Obviously, this kind of seal cannot be pro-duced along the posterior border of the upperdenture as it crosses the palate and so it has tobe completed by other means.
To obtain this posterior seal, either a grooveis cut into the palate of the master cast, or themucosa in this area is compressed during im-pression taking so that when the permanent
denture base is processed a raised lip is cre-ated on its impression surface. This projection,the post-dam, compresses the palatal mucosaonce the denture is placed in the mouth andthus creates a border seal. At the same time,the polished surface of the denture can be bev-elled in this region so that the edge of the den-ture is not so noticeable to the patient’s tongue(Fig. 11.5).
When cutting the post-dam it should nor-mally be completed at the appointment forrecording the jaw relationship so that the post-dam will be incorporated into the trial denture.However, when problems with retention of the
Figure 11.5 The post-dam region of an upper den-ture. Inset: the bevelled polished surface allows thedenture to merge with the mucosa.

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
154 Prosthetic Treatment of the Edentulous Patient
upper record blocks are anticipated, it is advan-tageous to have a post-dam on the upper recordblock. In such cases the post-dam will need tobe prepared on the master cast before the recordblock is constructed.
It is the clinician, rather than the dental tech-nician, who should be responsible for creat-ing the post-dam because only the clinician canmake the essential clinical assessments regard-ing its position and depth.
The position of the post-dam
The orthodox position of the post-dam is at thejunction of the moving tissues of the soft palateand the static tissues of the hard palate ante-riorly (Fig. 11.3). It should extend laterally tothe mucosa overlying the hamular notches. Ifthe border of the denture is taken further pos-teriorly, the patient may well complain of nau-sea. Furthermore, the continual movement ofthe soft palate in relation to the posterior bor-der of the denture will repeatedly break theseal and is likely to result in inflammation andeven ulceration of the mucosa. If the post-damis placed anteriorly to the junction, it termi-nates on relatively incompressible tissue. It isthen impossible to achieve a reasonable depthto the post-dam and, as a result, the seal is lessefficient.
RigidityEase of
RetentionmanufactureEase ofmodification
Light-curingacrylic resinHeat-curingacrylic resin
Shellac
SatisfactoryGoodKEY
Table 11.1 A comparison of materials used in the construction of bases for record rims.
The depth of the post-dam
The depth to which a post-dam can be cut de-pends upon the compressibility of the mucosaand this varies across the palate. For exam-ple, the mucosa in the midline of the palateis bound tightly to the underlying periosteum,while laterally the presence of a submucosagives rise to much greater compressibility. Suchvariation is detected clinically by palpationand the depth of the post-dam is modifiedaccordingly.
The record blocksIt is essential that the wax record rims should beplaced on well-fitting rigid bases. A non-rigidwax base is likely to change shape during therecording procedure and thus prevent accuratelocation both in the mouth and subsequently onthe casts.
Suitable materials for the bases are:
� Light-curing acrylic resin� Heat-curing acrylic resin� Shellac
Aspects of the advantages and disadvantagesof the materials compared in Table 11.1 are dis-cussed below:

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 155
Rigidity and strength
Although both types of acrylic resin are morerigid than shellac, the latter material is rigidenough to use as a base for upper blocks. How-ever, where the lower ridge is narrow in cross-sectional shellac is unreliable as it may easilydeform or fracture in use.
Ease of manufacture
Light-curing acrylic is the quickest and easiestof the materials for the dental technician to use.
Accuracy of fit
Heat-curing acrylic resin bases provide the bestfit and allow maximum retention to be estab-lished. Thus, when the rims have been carvedto their final shape, it should be possible to en-gage the patient in conversation without theblocks becoming dislodged. Observing a pa-tient talking is of immense value in judgingthe occlusal vertical dimension, as discussed in‘Adjusting the lower record rim’ later in thischapter.
A heat-curing acrylic base can be particu-larly valuable when the prognosis for retentionin the upper jaw is very poor. It helps to first trythe denture base in the mouth alone. Any per-fecting of the extension of the base can then becompleted and a baseline estimate of retentionobtained. The wax rim can then be added. If theretention is significantly reduced the most ob-vious cause is that the superstructure of the rimis not in muscle balance and must therefore bemodified.
Ease of modification
Before positioning a post-dam the clinicianneeds to be confident about the patient’s tol-erance to that degree of posterior extension.Where there is uncertainty about tolerance theuse of a shellac base allows the base extensionto be modified easily at the chairside.
Where the inter-ridge distance is small thethinness and adjustability of a shellac base canmake life easier for both the clinician, whenrecording the jaw relationship, and the dentaltechnician, when setting up the teeth for thetrial denture.
It will be appreciated that the matters justdiscussed need to be considered immediatelyafter the master impressions have been taken,as they will influence the prescription for thematerial to be used by the dental technician toconstruct the record blocks.
Adjusting the upper record rimBefore starting any adjustment, upper andlower record blocks should be placed in themouth in turn and checked for stability, re-tention, extension and comfort. It is impor-tant to appreciate that a loose or uncomfortablerecord block will almost certainly disturb nor-mal mandibular movement and invoke such afeeling of insecurity in the patient that the es-sential relaxation is not achieved and is perhapsthe strongest reason for suggesting the use of‘permanent’ acrylic bases. If there are problemswith any of these aspects it is essential that cor-rections are carried out before proceeding anyfurther.
There are two basic objectives when adjust-ing the upper record rim:
� To establish the correct orientation and levelof the occlusal plane.
� To produce the correct shape for the labial,buccal and palatal surfaces.
Although the procedures are described belowin sequence, in practice the final form of therecord blocks is most often achieved as a resultof a coordinated process in which earlier adjust-ments are reviewed and modified in the light ofthe results of later adjustments.

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
156 Prosthetic Treatment of the Edentulous Patient
Figure 11.6 A Fox’s occlusal plane indicator; theintra-oral portion is held against the occlusal surfaceof the upper record block; the extra-oral extension al-lows the clinician to judge the orientation of the oc-clusal plane with the interpupillary line and with theala-tragal line. The latter line is indicated by the rulerheld against the patient’s face.
Establishing the orientation of theocclusal plane
The orientation of the occlusal plane of the up-per rim is conveniently judged by using a Fox’socclusal plane indicator (Fig. 11.6) or a dispos-able wooden tongue spatula. The intra-oral partof the instrument rests on the occlusal surfaceof the record rim while the extra-oral extensionallows the clinician to judge the relationship ofthe plane to the facial guidelines.
Adjustment in the coronal plane
The rim is adjusted so that the occlusal planeis parallel to the interpupillary line, or alterna-tively, at right angles to the long axis of the pa-tient’s face. Failure to follow these guidelines,which ensure that the occlusal plane appearshorizontal in relation to the general symmetryof the face, will result in an unsightly, lopsidedappearance of the finished dentures.
Adjustment in the sagittal plane
A useful guideline for sagittal orientation of theocclusal plane is the ala-tragal line, an imagi-
nary line joining the lower border of the ala ofthe nose with the midpoint of the tragus of theear, to which the occlusal plane is made paral-lel (Fig. 11.6). Failure to conform to this guide-line is likely to detract from the aesthetic result.It can also have adverse consequences for sta-bility; for example, if the occlusal plane on thelower denture is tilted up posteriorly it may be-come so high that the denture is displaced bythe tongue rather than being controlled by it.
Establishing the level of theocclusal plane
The incisal level of the upper rim is related tothe upper lip, but it is impossible to describehard and fast rules for determining this rela-tionship. For example, whereas a patient with along upper lip may show very little of the upperteeth during normal function, the patient witha short upper lip is likely to display more of theteeth. For those patients who don’t have exist-ing dentures, a baseline from which to start is tomodify the incisal edge so that it is just visiblewhen the lip is at rest. As the rim is then eitherreduced or added to, errors in appearance areeasy enough to identify. It is important, as partof this assessment, to look at the relationshipof the rim to the lip during function by gettingthe patient to smile and say a few words whilstwearing the record block. The eventual answercomes as the result of trial and error and by ex-ercising a little visual common sense.
Correct shaping of the labial,buccal and palatal surfaces of thewax rim
Shaping the labial surface
Adequate lip support depends upon the posi-tion and inclination of the labial face of the waxrim. The biometric guides mentioned in Chap-ter 10 can help in achieving the correct shape.For example, the incisal edges of the upper cen-tral incisors can be placed up to 1 cm in front

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 157
Figure 11.7 (a) An upper recordblock providing inadequate supportto the upper lip – the naso-labial an-gle is obtuse. (b) Addition of wax tothe labial face of the upper recordblock providing more support for theupper lip – the naso-labial angle is90◦.
of the centre of the incisive papilla to compen-sate for the resorption of the alveolar ridge.Another useful guide is the naso-labial angle.A study of dentate adults (Brunton & McCord1993) suggests that if the angle is within therange 102◦–116◦ the upper lip is adequatelysupported by the record block (Fig. 11.7). It isessential that the position of the labial surfaceof the rim is compatible with the stability ofthe record block. The further forward the rimthe greater will be the displacing force of thelip muscles acting on the labial surface. Also,it should be remembered that the displacingforce occurring on incising food when the fin-ished denture is worn will also be increased. Ifthe prognosis for retention of the upper dentureis unfavourable as a result of extensive post-extraction resorption of bone, it may be neces-sary to effect a compromise between functionand appearance by positioning the rim furtherpalatally if this gives greater stability.
Shaping the buccal surface
The record rim posteriorly should be shaped sothat it fills the buccal sulcus and slightly dis-
places the buccal mucosa laterally as shown forthe denture in Fig. 11.10. This will contributeto retention by achieving an efficient facial seal.The rim itself will usually be buccal to the crestof the ridge by an amount proportional to theamount of resorption that has occurred. Refer-ence to the biometric guides (Chapter 10) willhelp to identify an appropriate position. How-ever, care should be taken not to place the rimtoo far buccally, as it will then be outside theneutral zone and increased force from the buc-cinator muscle will cause displacement. Thebuccal and palatal surfaces of the rim shouldbe shaped to converge occlusally so that pres-sure from the cheeks and tongue has a resultantforce towards the ridge, thus aiding neuromus-cular control.
Shaping the palatal surface
It is essential to create adequate space for thetongue by ensuring that the rim is not placedtoo far lingually and by reducing the width ofthe rim where necessary by removing wax fromthe palatal aspect until it corresponds to thewidth of the artificial teeth which will replace it.

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
158 Prosthetic Treatment of the Edentulous Patient
If the record block is too bulky, the constrictionof the tongue and the resulting abnormal sen-sory feedback is likely to influence mandibularposture and so lead to inaccuracies in recordingthe jaw relationship. In addition, speech qual-ity, which can be most valuable in confirmingthe accuracy of jaw relationship recordings, canonly make a contribution to this assessment ifthe dimensions of the rims are similar to thoseof the eventual dentures.
Adjusting the lower record rimThe adjustment of the lower rim may be con-sidered to have three aspects, as discussed inthe following.
Adjusting the height of the rim tothe required occlusal verticaldimension
The orientation of the occlusal plane has al-ready been established on the upper rim, whilethe overall height of the lower rim will begoverned by the existing height of the upperand the need to fit both into the required oc-clusal vertical dimension. However, the clini-cian should be prepared to modify the upperocclusal plane further if problems arise whenshaping the lower one. For example, if it be-comes increasingly apparent that the lower rimis going to be so high that stability will be poor,or so low that there will be no room for theteeth, then appropriate modifications must becarried out on the upper block.
Shaping the labial, buccal andlingual surfaces to conform to theneutral zone
These surfaces of the rim are shaped to accom-modate the surrounding musculature, becausethe lower rim will be unstable until it is posi-tioned in the neutral zone. First, it is necessaryto adjust the buccal and labial surfaces of the
rim so that they lie close to, but do not displace,the cheek and lip mucosa. Second, it is vital toallow adequate tongue space by carving the rimon the lingual side so that it is of a width similarto the denture teeth that will eventually replaceit. Failure to adequately carve the lower rim tothe neutral zone is a common error resulting ininstability, inaccurate recording of the jaw rela-tionship and an incomplete prescription for thedental technician.
When judging the relationship of the rim tothe neutral zone, it is important that the tonguetakes up a normal resting position forwards inthe mouth with the tip contacting the lingualsurface of the rim anteriorly. This may bedifficult to achieve clinically because as soon asthe tongue is mentioned to the patient there isa tendency for it to take on a ‘life of its own’.Occasionally, the tongue is drawn towards theback of the mouth to adopt a posture which hasbeen aptly described as a ‘defensive tongue’.This is probably the result of a subconsciouswish to guard the pharynx against the foreignbody in the mouth. It is impossible to achievemuscular balance with such tongue behaviourand therefore it is necessary to coax the patientto position the tongue in a more anterior posi-tion before the stability of the record block canbe assessed adequately.
Re-assessment of the occlusalvertical dimension
Having largely completed the adjustment ofthe record blocks, it is vital to undertake a re-assessment of their occlusal vertical dimensionbefore finalising the recording of the jaw rela-tionship. This is achieved by the following:
� Measuring the rest vertical dimension. Refer-ence was made on pp. 72–73 to the in-crease in the rest vertical dimension thattakes place when a lower denture is insertedinto the mouth. The observation is of partic-ular significance at the stage now reached.Once the lower rim has been adjusted to the

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 159
oral musculature and its shape and size arejudged to be comparable to the new denturewhich will eventually replace it, the record-ing of the rest vertical dimension must be re-checked with the lower block in situ. If, asis likely, the rest vertical dimension is foundto have increased, the new reading shouldbe used to re-calculate the occlusal verticaldimension. The record blocks are then ad-justed accordingly.
� Assessment of facial proportion. With therecord blocks in occlusion the clinicianshould make a judgement as to whether thefacial proportions look correct, or whetherthe lower third of the face appears too long(excessive occlusal vertical dimension), ortoo short (reduced occlusal vertical dimen-sion). Noting other facial features such ascreases at the corner of the mouth, loss of redmargin of the lips, incompetence of the lipsand degree of mandibular protrusion willalso provide clues to help in this assessment.With increasing clinical experience it is notunusual for a clinician to rely more and moreon an assessment of facial appearance ratherthan direct measurement to decide whetheror not a satisfactory occlusal vertical dimen-sion has been produced.
� Assessing speech with the record blocks in situ.If the record rims have been constructedon well-fitting, stable bases and have beenshaped correctly it should be possible to en-gage the patient in conversation. Frequentcontact of the rims during speech indicatesthat the occlusal vertical dimension is ex-cessive. On the other hand, if the patientcan talk without making such contacts, theclosest speaking distance has not been oblit-erated and the clinician has obtained ad-ditional valuable evidence that the occlusalvertical dimension is not too great.
� Reference to previous dentures. Where previousdentures exist the patient’s experience withthem will often provide clues as to whethertheir occlusal vertical dimension is satisfac-tory or not (Chapter 8). Depending upon the
findings, the occlusal vertical dimension ofthe record blocks can be adjusted to copy ormodify the freeway space of these dentures.
If the patient has no existing dentures to whichone can refer to for additional information, it isacceptable to initially establish the occlusal ver-tical dimension approximately 3 mm less thanthe rest vertical dimension. The freeway spaceso produced is satisfactory for the vast major-ity of patients. However, this should then bere-evaluated having observed speech and facialappearance.
Recording the retruded jawrelationshipThe next stage is to establish even occlusalcontact between the record rims at the chosenvertical dimension with the mandible in theretruded position.
Preparation of the patient
Every effort is made to get the patient to relaxso that jaw muscle activity is reduced as muchas possible. By adopting a relaxed manner, bygently guiding the mandible and by giving in-structions such as, ‘close together on your backteeth’, the clinician is most likely to encouragethe mandible to fall back into its retruded po-sition. An additional procedure which may beof help in obtaining the retruded position is toask the patient to curl the tongue to the back ofthe mouth and to touch the posterior border ofthe upper record block while closing. The pa-tient may be assisted in this by placing a smallblob of wax in the centre of the posterior bor-der to act as a ‘target’ for the tongue so that thepatient will be aware of when it is in the correctposition. Whatever technique is used, it is wiseto get the patient to close from an open positionof around 1 cm only as the condyle will be moreeasily located in the glenoid fossa and closurewill be a rotational rather than a translationalmovement

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
160 Prosthetic Treatment of the Edentulous Patient
Check�lines�
Premature�contact�
Figure 11.8 Record blocks lo-cated extra-orally by using checklines showing premature contact be-tween the bases posteriorly. Theshaded areas indicate where waxcan be removed from the bases toeliminate the premature contact.
Preliminary recording
Initially, in order to make large adjustments toa lower rim, the occlusal surface of the rimshould be thoroughly softened and the pa-tient asked to close together. Closure is stoppedwhen the occlusal vertical dimension appearsto be correct. However, as a means of makingthe final recording of the retruded position, thismethod is fraught with danger. Unless the pa-tient is able to close into a surface of uniformsoftness, there is every chance that contact ona harder portion of wax will create an error inthe recording by causing uneven compressionof the underlying mucosa and effectively caus-ing the record blocks to tip. In addition, contacton the harder wax is likely to result in an ab-normal path of closure. It is necessary thereforeto separate the two rims after chilling and cutaway the excess wax that has been squeezedout. The record blocks are then reinserted andeven occlusion is checked by asking the patientto close very gently into initial contact.
After any necessary corrections have beencarried out, three check lines are drawn witha wax knife from one rim to the other, one inthe midline and one either side in the premo-lar regions. These lines enable the blocks to belocated outside the mouth to establish whetherthere is any premature contact on the posterior
aspects of the rims or bases (Fig. 11.8). In addi-tion, the check lines allow the clinician to judgewhether the patient continues to close in a con-sistent manner.
The patient may be further encouraged atthis stage to make contact in the retruded po-sition by reducing the height of the lower rimanteriorly by about 1 mm so that the rims oc-clude only in the premolar and molar regions(Fig. 11.9)
Definitive recording
Before the rims are finally located together, it iswise to consider five basic questions:
1. Are the rims stable?2. Is there adequate freeway space?3. Has a consistent retruded jaw relationship
been established?4. Is there even occlusal contact?5. With the rims in the mouth and the lips
brought together, is there a pleasing appear-ance?
Bearing in mind that the record rims are theblueprint for the eventual dentures, if any faultis left uncorrected at this stage, it will re-appearon the trial dentures.

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 161
Prematurecontacteliminated��
Anterior�lower�rimreduced�by�1�mm��
Figure 11.9 The premature con-tact between the bases posteriorlyhas been eliminated and the lowerrim has been reduced in height toencourage the patient to occlude inthe retruded position.
For the definitive recording it is advisableto use a recording medium which initially isof low viscosity, thus offering little resistanceto closure of the jaws, but which subsequentlyhardens sufficiently not to be distorted whenthe casts are mounted on the articulator. Suit-able materials include a zinc oxide-eugenol oc-clusal registration paste, silicone registrationpaste, impression plaster and a wax containingfine metal particles.
The clinical procedure is as follows:
� Two locating notches are cut into the occlusalsurface of the upper rim, one either side ofthe arch in the premolar areas.
� If a zinc oxide-eugenol paste is being usedthe occlusal surface of the upper rim iscoated with a thin film of petroleum jellywhich acts as a separating medium. If us-ing a silicone registration paste this step isnot required, but additional notches shouldbe placed in the lower rim to allow accuratelocalisation.
� The registration medium is applied to thepremolar and molar regions of the lowerrim and the patient is guided into theretruded position. The patient must keep themandible absolutely still until the registra-tion medium has set – a requirement that canbe a problem for older patients.
An alternative technique
An alternative, very rapid method for record-ing the jaw relationship is to start by reducingthe lower rim to two occlusal pillars about 1 cmin length in the second premolar region. Thesepillars can be adjusted quickly by softeningor adding wax to achieve balanced occlusalcontact in the retruded jaw relation at theappropriate occlusal vertical dimension. Themissing sections of the lower rim are thenreconstructed by placing impression plasterinto the spaces with a spatula and getting thepatient to close into the plaster until the waxpillars occlude with the upper rim (Fig. 11.10).This particular technique has the advantagethat the clinician has only two small areasof wax to adjust in order to establish evenocclusal contact. As the contact is restricted tothe premolar/molar region it encourages thepatient to close in the retruded jaw relationshipand also helps to stabilise the lower recordblock.
Having recorded the jaw relationship, thefollowing questions need to be answered:
� Is a palatal relief chamber required, and if sowhat is its location and extent?
� What artificial teeth are appropriate?

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
162 Prosthetic Treatment of the Edentulous Patient
a
b
Figure 11.10 (a) Lower record block with occlusalcontact area restricted to the premolar areas. Impres-sion plaster is being applied to fill the spaces posteri-orly. (b) Completed registration. Note that the impres-sion plaster has filled locating notches (arrows) cut intothe upper rim.
Palatal reliefIf a relief chamber is required but has not beenprescribed at the master impression stage thenit should be done here. Very occasionally, whenthe upper denture-bearing tissues are palpated,the mucosa covering the ridge will be found tobe more compressible than the mucosa in themiddle of the palate. If an impression recordsthese tissues in an undistorted state and a den-ture is constructed on the resulting cast then,when the denture is fitted, the compressibleridges will offer less support than the centre of
the palate. As a result, occlusal contact will re-sult in pivoting and flexing of the denture aboutthe midline. Initially, this pivoting may causeloss of border seal or inflammation of the mu-cosa. Over a longer period of time, the contin-ual flexing of the denture is likely to producefatigue of the acrylic resin resulting in a midlinefracture (p. 246).
There are two ways of avoiding these prob-lems. A more viscous impression material maybe used for the master impression so that theshape of the tissues over the ridge is recordedin a compressed state. Alternatively, if a lessviscous impression material is used, a sheet oftin foil, trimmed to correspond to the area ofincompressible mucosa, may be cemented tothe resulting cast in the midline so that whenthe denture is processed, a relief chamber iscreated. That part of the denture base overly-ing the incompressible midline will stand awayfrom the mucosal surface and will only con-tact the tissues when the ridge mucosa is com-pressed.
As the authors favour an impression tech-nique which records the shape of the mucosawith minimal distortion, for reasons discussedon p. 146, they prefer to use relief as a means ofovercoming the problem of varying compress-ibility. However, this approach has its draw-back because air may be trapped in the reliefchamber, so potentially reducing the physicalforces of retention. For this reason, it is im-portant that relief is provided only when pos-itively indicated. For example, although a pala-tine torus might be present, there is no need toprovide a palatal relief over it unless the cov-ering mucosa is found to be less compressiblethan that over the ridges.
The decision as to whether to provide arelief is the responsibility of the clinician, notthe dental technician. If the clinical situationwarrants a palatal relief, the size and shapeof the area requiring it should be identifiedby palpation. The corresponding area on thecast is then outlined as a guide to the dentaltechnician when laying down the tin foil of

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 163
appropriate thickness. If a heat-cured acrylicbase is to be used for the upper record block,a decision on palatal relief must be made afterthe working impression has been taken. If apalatal relief is required the relevant area canbe marked on the impression with an indeliblepencil. This mark is transferred to the mastercast and acts as a guide to the laying downof the tin foil before the permanent base isconstructed.
It should be said that the occasions when re-lief is not needed far exceed the occasions whenit is required.
Choice of teethThe information required to produce a pleasingand natural appearance for complete denturesincludes the following:
� Incisal level� Amount of lip support provided by the an-
terior teeth and labial flange� Occlusal vertical dimension� Colour, shape, size and material of the artifi-
cial teeth� Arrangement of the artificial teeth
Incisal level, lip support and occlusal verticaldimension are indicated by the shape of theadjusted record rims as discussed previously.A decision on the colour, shape, size and ma-terial of the teeth must now be made. Withthis information, the technician is able to pro-duce a basic set-up for the trial dentures. Thefinal stage in refining the appearance, creatingthe detailed arrangement of the anterior teethwithin the dental arch, is completed on thetrial dentures at the chairside as discussed inChapter 13.
The comments which follow, with the excep-tion of those concerned with the choice of ma-terial of the denture teeth, are concerned pri-marily with the selection of anterior rather thanposterior teeth.
Colour of teeth
An appropriate colour of artificial tooth is se-lected from a shade guide. When making thechoice, it is advisable to moisten the teeth withwater and hold them just inside the patient’sopen mouth. Care should be taken to avoid let-ting the patient view the teeth against a lightbackground such as pale clothing. Under suchconditions the shade will appear darker thanit will when the denture is eventually in themouth. As a result, the patient is likely tochoose a shade that is too light; indeed for thisreason alone, there is a lot to say in favour ofthe patient seeing the teeth against a dark back-ground when viewing them out of the mouth.
It is, of course, important that a decision oncolour should be influenced by the patient’scomments and by the patient’s opinion of pre-vious dentures. However, as it is often difficultfor the patient to forecast the final result fromthe appearance of one tooth positioned in themouth, the clinician should offer guidance onthe colour that is likely to be most suitable.
It is not possible to provide hard and fastrules on choice of colour in view of the varia-tion in the natural dentition. However, the fol-lowing comments are offered as useful guide-lines:
� Natural teeth tend to become darker with in-creasing age. Therefore, it is appropriate tochoose a shade of denture tooth which is inkeeping with the patient’s age.
� A more natural appearance is likely to be ob-tained if people with dark complexions areprovided with darker teeth, while those withpaler complexions are given lighter teeth.
Shape and size of teeth
Because of the enormous variation found in thenatural dentition, it is possible to offer onlyvery general guidelines for choosing the shapeand size of artificial teeth.

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
164 Prosthetic Treatment of the Edentulous Patient
Shape
Age, sex and personalityOver the years several papers have offeredguidance on the choice and arrangement of ar-tificial teeth to reflect the sex, age and person-ality of the patient (Chapter 13). As a gener-alisation, it has been stated that masculinityis associated with ‘vigour, boldness and hard-ness’ while femininity, in contrast, is describedin terms of ‘roundness, softness and smooth-ness’. Whereas larger and more angular toothshapes indicate strength and masculinity, a del-icate and more feminine impression is createdby moulds that have curved outlines and aresomewhat smaller. There is only limited hardevidence to suggest that these stereotypes aregenetically derived and probably owe moreto years of social conditioning. Anterior den-ture teeth can and probably should be made toreflect advancing years by introducing incisalgrinding to simulate tooth wear.
Facial morphologyOne cannot state categorically that patientswith large faces and strong features have largeteeth, or vice versa, because jaw size and toothsize have different genetic origins (which is aprimary reason for the need for orthodontists).Nevertheless, when choosing artificial replace-ments in the absence of any other information,a large tooth mould is usually appropriate forthose patients with a heavier skeletal makeup,and vice versa.
A further suggestion that has been madeis that the shape of the upper anterior teethshould complement the shape of the patient’sface. Three basic facial shapes have been de-scribed – square, ovoid and tapering – and cor-responding tooth moulds have been producedwhich are an inverted version of these shapes.
A recent review of the literature (Sellen et al.1999) concluded that there was no scientificbasis for any of these proposals. Neverthelessthese guidelines are worth bearing in mind onpurely aesthetic grounds when selecting den-
ture teeth, as their application can increase thechance of creating dentures which harmonisewith the patient’s facial appearance.
Size
Crown widthIt is possible to use photographs of the patient(taken when still dentate) to calculate the widthof the central incisor by measuring the widthof that tooth and the interpupillary distance onthe photograph and the interpupillary distanceon the patient and then substituting the valuesin the following equation:
Calculatedwidth ofincisor
=photographic
width of incisor× actual PD
photographic PD
where PD is the interpupillary distance. It hasbeen shown that this technique is of provenvalue only if the pre-extraction photograph is afull-face portrait and of sufficient size, approxi-mately 13 cm × 18 cm (Bindra et al. 2001).
Two further suggestions are offered as guid-ance when choosing the width of the anteriorteeth:
1. The combined width of the two central in-cisors is frequently similar to the width ofthe philtrum of the upper lip (Fig. 11.11).
2. The projection of a line drawn from the in-ner canthus of the eye to the ala of the nosepasses through the upper canine tooth (Fig.11.11). These lines can be scribed onto thecorrectly contoured record block and thenaflexible ruler curved around the labial sur-face of the rim to measure the distance be-tween the lines. Tooth moulds which will fitinto this distance can be identified from achart.
Crown lengthThe crown length of the upper artificial teeth isindicated by the distance between inferior andsuperior reference points:

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 165
Figure 11.11 The combinedwidth of the two central incisorstends to be similar to the width ofthe philtrum of the upper lip. Theprojection of a line from the innercanthus of the eye to the ala of thenose passes through the tip of theupper canine tooth.
1. The inferior reference point is the incisallevel of the recording rim that has beencarved to produce an appropriate relation-ship to the upper lip.
2. The superior reference point is the level towhich the upper lip is raised on smiling. Thefurther the necks of the teeth are placed be-low this ‘smile line’ the more gum will beshown when smiling. If an excessive amountof gum is displayed this can appear un-sightly.
Mould guides
The choice of mould for the upper anterior teethcan be made from actual samples of mouldsavailable, or from a printed mould guide. If theclinician has a selection of upper tooth mouldsset in conventional tooth arrangements, theycan be positioned inside the upper lip. It ispreferable to use only half the anterior seg-ment so that the set-up can be rotated in themouth to follow the shape of the dental arch(Fig. 11.12). The full complement of anteriorteeth may be so unlike the shape of the den-tal arch that the appearance resembles the teethfound in a Christmas cracker and thus offers lit-tle guidance to the clinician and even less to thepatient.
Tooth arrangement
Patient history
Having recorded the information on colour andshape of the artificial teeth, it is advisable to askpatients if they remember any particular char-acteristic in the arrangement of the natural teethwhich they would like to be included in the ar-tificial set-up. For example, if a request is madeto reproduce a fondly remembered median di-astema or imbricated incisors this can be passedto the dental technician for inclusion in the trial
Figure 11.12 Choosing the mould for the anteriorteeth. More guidance on the width of the teeth can begained from trying in three anterior teeth only ratherthan a set-up of all six whose arch shape may be quiteinappropriate for the patient.

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
166 Prosthetic Treatment of the Edentulous Patient
dentures. However, it is commonly found thatthis line of questioning is of limited help. Sooften, patients remember only gross irregular-ities, which in any case they want modified inthe artificial dentition.
Pre-extraction records
Most of the process of tooth selection andarrangement is a matter of inspired, creativeguesswork helped by applying principles ofproven clinical value. The uncertainty of thisapproach underlines the value of pre-extractionrecords, such as good-quality photographs,notes and dental casts. Immediate dentures arealso an excellent way of transferring the de-sirable features of the natural dentition to theartificial one. Whenever possible, records suchas these should be included in the decision-making process.
Tooth material – a comparison ofacrylic and porcelain teeth
As consideration should be given as to whetheracrylic or porcelain teeth should be used, it isappropriate to consider their respective quali-ties at this stage. However, it should be pointedout that very few porcelain teeth are usednowadays.
Appearance
A very satisfactory appearance can be obtainedfrom both good-quality acrylic and porcelainteeth. In the manufacture of both types of teeth,it is possible to produce a satisfactory gradationof colour throughout the length of the crownand to introduce striations and stains to mimicthe imperfections of natural teeth. However, theacrylic tooth may deteriorate more rapidly insome patients’ mouths because of its lower re-sistance to wear.
Attachment to the denture base
The attachment of acrylic teeth to the denturebase is by chemical union, while porcelain teeth
are retained by means of pins or holes. Undernormal circumstances, both methods work per-fectly satisfactorily. However, in cases wherethe inter-ridge distance is small, it may be nec-essary to reduce the length of the tooth so muchthat, in the case of porcelain, the retentive el-ement is removed. Under these circumstancesacrylic teeth must be used. As a denture coolsfollowing processing, the denture base polymercontracts 20 times more than porcelain. Thismeans that around the necks of porcelain teeth,where contraction is restricted, areas of strainare set up, which reduce the resistance of thepolymer to fracture.
Transmission of masticatory forces
Porcelain teeth transmit a greater proportion ofthe masticatory forces to the underlying mu-cosa. This is because of the widely differing val-ues in the modulus of elasticity of the two ma-terials, that for porcelain being about nine timesgreater than the value for acrylic resin. Thus,the use of porcelain teeth can be a disadvantagein those patients whose denture-bearing tissuesare less able to tolerate the higher forces.
Response to function
NoiseAs porcelain teeth are approximately ten timesharder than acrylic teeth they can make morenoise on contact. In spite of this, as only a smallpercentage of patients complain of noise fromporcelain teeth, it is a point of little importance.Possible reasons for this are that during mas-tication, a layer of food separates the two oc-cluding surfaces for much of the time, and be-fore the teeth eventually make contact there isalways a deceleration of the mandible whichlimits the force on impact. In addition, duringspeech the teeth do not come into contact witheach other at all provided an adequate freewayspace has been provided.
Resistance to chippingAs acrylic resin has a lower modulus of elas-ticity than porcelain, it will absorb much more

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 167
energy before fracturing; thus, a sudden impactis more likely to chip porcelain teeth.
Occlusal wearThe resistance of the two materials to occlusalwear is perhaps the most significant differencebetween the two types of teeth from a clini-cal standpoint. As porcelain teeth are so muchharder, their occlusal surfaces wear out onlyvery slowly. Thus, the established jaw relation-ship in both horizontal and vertical planes ismaintained for longer. Some people believe thatthe more rapid wear of acrylic teeth allows thepatient to ‘grind in’ a personal occlusal pat-tern. This may be a justifiable view in the earlystages of wear. However, further deteriorationof the occlusal surfaces leads to irregular oc-clusal contact and loss of the original jaw re-lationship. Another argument put forward infavour of acrylic teeth is that the masticatoryforces wear the teeth away rather than cause re-sorption of the underlying bone. However, any-thing more than minimal occlusal wear can re-sult in an unbalanced occlusion which is itself apotent cause of resorption.
Obtaining balanced occlusalcontact during functionThe remainder of this chapter deals with theimportant topic of the relevance of balanced oc-clusion and the role played by the articulator.But first, it may be of help to the reader to havean understanding of a few definitions.
Definition of terms
Balanced occlusion
Balanced occlusion is present when there aresimultaneous contacts between opposing arti-ficial teeth on both sides of the dental arches.This term describes a static situation and ap-plies when upper and lower dentures meet inany position.
Balanced articulation
Balanced articulation is a dynamic situation inwhich there are bilateral, simultaneous contactsof opposing teeth in central and eccentric po-sitions as the mandible moves into and awayfrom the intercuspal position.
Working and non-working sides
The working side is that to which the mandiblemoves, for example, in order to break up a bo-lus of food. The opposite side of the arch istermed the non-working, or balancing side.
Condylar path
The condylar path (Fig. 11.13) is the route takenby the mandibular condyle as it moves for-wards and downwards from the glenoid fossato the articular eminence.
Condylar angle
The condylar angle (Fig. 11.13) is the anglebetween the condylar path and the Frankfortplane.
Condylar axis
The condylar axis (Fig. 11.13) is a line betweenthe mandibular condyles close to a hinge axisaround which the mandible can rotate withouttranslatory movement.
Advantages of occlusal balance
If occlusal balance exists, the masticatory forcesare transmitted as widely as possible over thedenture-bearing tissues. Furthermore, the even,bilateral contact positively assists in retainingthe dentures. As the patient closes together, bi-lateral contact actively seats the dentures onthe underlying tissues. Occlusal contact on onlyone side will usually result in either or bothdentures tipping with resultant loss of reten-tion. In addition, if the occlusion is unbalanced,

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
168 Prosthetic Treatment of the Edentulous Patient
Glenoid fossa
Frankfort plane
Condylar axis
Condylar path Articular eminence
Condylar angle
Figure 11.13 Diagrammatic rep-resentation of the relationship of theFrankfurt plane, the condylar pathand the condylar angle.
the masticatory forces are transmitted initiallyto a reduced area of tissue. The likely conse-quences of this are inflammation of the mucosa,discomfort and, ultimately, an increased rate ofresorption of the underlying bone.
It is important to make the point that bal-anced occlusion and articulation are relevantonly when the teeth make contact. This situa-tion occurs during the so-called ‘empty mouthcontacts’ while swallowing saliva, clenching orgrinding the teeth. During mastication, in theearly stages of the chewing process, the bolusis generally too large or too firm for the up-per and lower teeth to penetrate fully and tocome into contact. Thus, occlusal balance doesnot operate at this stage, a situation reflected inthe old adage, ‘Enter bolus, exit balance.’ It isonly in the later stages of comminution of thebolus that the food is broken down and soft-ened enough for the teeth to contact and for oc-clusal balance to come into play.
Articulators
If complete dentures are to be constructed witha balanced articulation, the articulator on whichthey are constructed has to be capable of repro-ducing certain basic characteristics of the pa-tient, namely:
� The condylar angle� The relationship of the maxilla to the condy-
lar axis
Examples of three types of articulators com-monly used are shown in Fig. 11.14.
The simple hinge articulator
If complete dentures are constructed on a sim-ple hinge articulator, all that can be producedwith certainty is balanced occlusion in theposition in which the jaw relationship wasrecorded.
The average-movement articulator
The value for the condylar angle and therelationship of the maxilla to the hinge axis onthis type of articulator are fixed to conform toaverage measurements obtained from manypatients. The upper arm can be moved inthe horizontal plane; thus, on the articulatorthe technician is able to simulate lateral andprotrusive movements of the mandible andcheck that the arrangement of the artificialteeth provides a balanced articulation.

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 169
a b c
Figure 11.14 Examples of three articulators (a) a simple hinge articulator; (b) an average-movement articulator;and (c) a semi-adjustable articulator.
The semi-adjustable articulator
The semi-adjustable articulator allows themounting of the casts in the anatomically cor-rect relationship to the condylar axis using aface bow record. Also, by obtaining an interoc-clusal record of the jaw relationship with themandible in protrusion the condylar path canbe adjusted so that it more closely correspondsto that of the patient. Lateral and protrusivemovements of the mandible can therefore besimulated on the articulator, allowing denturesto be constructed with occlusal balance in ec-centric positions.
Limitations of articulators
Hinge articulatorIn spite of the limitations of the simple hinge ar-ticulators, many dentures are made on this in-strument and function quite satisfactorily. Thelikely reason for success is the ability of mostpatients to adapt to the limitations of the oc-clusal surface. The patient recognises that cer-
tain functional movements cause instability ordiscomfort and cease to make them. It will, ofcourse, be apparent that such dentures may failin those patients whose ability to adapt is morerestricted.
Semi-adjustable articulatorAlthough the semi-adjustable articulator is amore complex instrument, there are features ofits design which prevent it from reproducingmandibular movement with complete accu-racy. For example, when a patient’s mandiblemoves in protrusion, the head of the condylesmove downwards, forwards and mediallyalong an articular surface whose shape is a sig-moid curve. In contrast, the condylar spheres ofthe articulator move forwards, downwards andmedially along a straight path. It should also bepointed out that the successful use of this typeof articulator is dependent upon the accuracyof the face-bow record and the inter-occlusalrecord. In this respect it is worth emphasisingthe point that the accuracy is restricted to a

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
170 Prosthetic Treatment of the Edentulous Patient
degree by the varying compressibility of themucosa on which the record rim sits
Average movement articulatorThe average-movement articulator may be con-sidered as lying somewhere between the twoother instruments. As far as clinical tasks areconcerned, it is less complicated to use than thesemi-adjustable articulator whilst, at the sametime, allowing the dental technician to positionartificial teeth in such a way as to produce an ar-ticulation that has a level of balance which willsatisfy most patients.
Selecting an articulator
Faced with the alternative approaches men-tioned above, which articulator is mostappropriate for the edentulous patient? Is thesophistication of the semi-adjustable articula-tor justified for all patients, or can satisfactoryresults be obtained with the less complicatedinstruments?
To help answer these questions, it is logicalto consider what actually happens to completedentures during normal function.
The first point to realise is that althougha perfectly balanced articulation may be pro-duced on the articulator when the dentures arefixed rigidly to the underlying casts, the situa-tion is likely to be very different in the mouth.Once in the mouth, dentures are placed on acompressible foundation and they inevitablymove when occlusal contact is made. Even ifthe mucosa is firm, there is the possibility of upto 1 mm of movement in the horizontal plane.With increasing compressibility, greater move-ment will occur.
The stability of complete dentures has re-ceived considerable attention in the literature.Research has shown that, during normal func-tion, complete dentures are remarkably unsta-ble. During incision, the posterior border of anupper denture usually drops. When the bolusof food is transferred to the posterior teeth forchewing, the upper denture commonly slides
towards the working side and the balancingside tends to drop. The lower denture is oftenseen to lift bodily. Muscular control of the den-tures comes to the rescue and enables reason-ably normal function to be established. This setof circumstances is probably one of the reasonsbehind the observation that long-term successof dentures does not appear to be related to so-phisticated articulator systems (Carlsson 2006).The frequency of occlusal contact increases asthe bolus of food is broken down. It appearsthat most of this contact occurs in the proximityof the retruded position. The results of these ex-perimental observations may now be applied tothe clinical situation and the following conclu-sions drawn and recommendations made.
� Due to the compressibility of the denturefoundation and the inevitable movement ofthe dentures, the apparent precision of themore sophisticated semi-adjustable articula-tor seems to be superfluous. The use of anaverage-movement articulator makes for asimpler technique, while at the same timeproviding the facility to produce a level ofbalanced articulation that is acceptable formost patients.
� As it appears that functional tooth contactoccurs in the region of the retruded position,it is usually sufficient to develop an occlu-sion which minimises the possibility of im-balance in an area 2–3 mm lateral and ante-rior to this position.
� In lateral occlusion, there should be contacton the working side and a balancing contact,or contacts, on the opposite side (Fig. 11.15a).It is important to avoid a premature contactor complete lack of contact on the balancingside (Figs. 11.15b and 11.15c).
� In protrusive occlusion, it would seem wiseto aim for bilateral balancing contacts on oneor more posterior teeth (Fig. 11.15d). It maybe more difficult to produce a balancing con-tact in instances where the anterior tooth ar-rangement appropriate for the patient ne-cessitates an anterior deep vertical overlap

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 171
B S
a c
b d
Workingside
Balancingside
W S B S
W S Figure 11.15 (a) Balanced occlu-sion with contact on the working side(left) and on the balancing side (right).The arrows indicate the direction ofmovement of the mandible as it returnsto the intercuspal position. (b) A prema-ture contact on the balancing side. (c) Apremature contact on the working side.(d) Balancing contact on posterior teethin protrusion.
(Chapter 12). However, within the zone inwhich balance is advantageous, the problemis frequently solved by a slight reduction inheight of the lower incisors.
Selecting posterior teeth
With regard to the choice of posterior teeth,studies into patients’ satisfaction and abilityto chew tougher foods with cusped or cusp-less types have indicated preference for the for-mer (Heydecke et al., 2007; Sutton & McCord,2007). It has been argued that cuspless teeth arebetter able to accommodate positional changesof the dentures relative to the supporting tis-sues brought about by resorption of alveolarbone and that cuspless teeth might be particu-larly suitable for older patients because an in-creased variation in occlusal contact positions ischaracteristic of this group. However, others ar-gue that the positive interdigitation offered bycusped teeth helps to reduce the variation andthat this can provide functional benefits for the
older patient. If it is considered desirable to cre-ate a fully balanced articulation, than cuspedteeth will facilitate the task.
Communication with the dentaltechnicianThe technician requires a detailed blueprintfrom which the trial dentures can be con-structed. The following information should beincluded:
� Confirmation that all items sent from theclinic to the laboratory have been disin-fected.
� The adjusted record blocks to indicate thefollowing:– Jaw relationship– Relationship of the teeth to the underlying
ridges– Arch relationship in both the anterior and
posterior regions– Overall shape of the dentures

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
172 Prosthetic Treatment of the Edentulous Patient
� Location, shape and depth of the post-dam.� The location, size and shape of palatal relief
if required.� Type of articulator required.� Face bow and protrusive interocclusal
records if required.� Shade, mould and material of anterior and
posterior teeth.� Any special instructions, e.g. regarding ap-
pearance and the setting of anterior teeth.
Quality control andenhancementThe accuracy with which this clinical stage hasbeen accomplished, and how well the informa-tion has been transferred from the patient in thedental chair to the dental technician in the labo-ratory, can be judged at the subsequent stage oftrial dentures.
Suggestions for topics that might be investi-gated in a series of cases include the following:
� In what percentage of cases was the amountof freeway space found to be appropriateand correct?
� In what percentage of cases was even oc-clusal contact established and a consistentantero-posterior jaw relationship recorded?
� In what percentage of cases did the posteriorteeth appear to be positioned correctly in theneutral zone?
� In what percentage of cases had the prescrip-tion for the appearance of the anterior teethbeen followed satisfactorily?
� In what percentage of cases was the den-tal technician satisfied with the informationprovided in the record rims and in the writ-ten prescription?
References and additionalreadingBindra, B., Basker, R.M. & Besford, J.S. (2001) A study
of the use of photographs for denture tooth se-
lection. International Journal of Prosthodontics, 14,173–7.
Brewer, A.A., Reibel, P.R. & Nassif, N.J. (1967) Com-parison of zero degree teeth and anatomic teeth oncomplete dentures. Journal of Prosthetic Dentistry,17, 28–35.
Brill, N. (1957) Reflexes, registrations, and prosthetictherapy. Journal of Prosthetic Dentistry, 7, 341–60.
Brunton, P.A. & McCord, J.F. (1993) An analysis of na-siolabial angles and their relevance to tooth posi-tion in the edentulous patient. European Journal ofProsthodontics and Restorative Dentistry, 2, 53–6.
Carlsson, G.E. (2006) Facts and fallacies: An evi-dence base for complete dentures. Dental Update,33, 134–42.
Feldmann, E.E. (1971) Tooth contacts in denture oc-clusion – centric occlusion only. Dental Clinics ofNorth America, 15, 875–87.
Harcourt, J.K. (1974) Accuracy in registration andtransfer of prosthetic records. Australian DentalJournal, 19, 182–90.
Helkimo, M., Ingervall, B. & Carlsson, G.E. (1973)Comparison of different methods in active andpassive recording of the retruded position of themandible. Scandinavian Journal of Dental Research,81, 265–71.
Heydecke, G., Akkad, A.S., Wolkewitz, M., Vogeler,M., Turp, J.C. & Strub, J.R. (2007) Patient ratingsof chewing ability from a randomised crossovertrial: lingualised vs. first premolar/canine-guidedocclusion for complete dentures. Gerodontology, 24,77–86.
Kobowicz, W.E. & Geering, A.H. (1972) Transferof maxillomandibular relations to the articulator.In: International Prosthodontic Workshop on CompleteDenture Occlusion (eds B.R. Lang & C.C. Kelsey).Ann Arbor, Michigan.
McMillan, D.R. & Imber, S. (1968) The accuracy offacial measurements using the Willis bite gauge.Dental Practitioner and Dental Record, 18, 213–17.
McMillan, D.R., Barbenel, J.C. & Quinn, D.M. (1969)Measurement of occlusal face height by dividers.Dental Practitioner and Dental Record, 20, 177–9.
Nairn, R.L. (1973) Lateral and protrusive occlusions.Journal of Dentistry, 1, 181–7.
Preiskel, H.W. (1967) Anteroposterior jaw relations incomplete denture construction. Dental Practitionerand Dental Record, 18, 39–44.
Sellen, P.N, Jagger, D.C. & Harrison, A. (1999) Meth-ods used to select artificial anterior teeth for theedentulous patient: a historical overview. Interna-tional Journal of Prosthodontics, 12, 51–8.

P1: JZP Trim: 246mm X 189mmc11 BLBK351-Basker January 18, 2011 13:20 Printer Name: Yet to Come
Recording Jaw Relations – Clinical Procedures 173
Sutton, A.F. & McCord, J.F. (2007) A randomizedclinical trial comparing anatomic, lingualized, andzero-degree posterior occlusal forms for completedentures. Journal of Prosthetic Dentistry, 97, 292–8.
Tryde, G., McMillan, D.R., Christensen, J. & Brill, N.(1976) The fallacy of facial measurements of oc-
clusal face height in edentulous subjects. Journal ofOral Rehabilitation, 3, 353–8.
Yurkstas, A.A. & Kapur, K.K. (1964) Factors in-fluencing centric relation records in edentulousmouths. Journal of Prosthetic Dentistry, 14, 1054–65.

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
12Dentures and Muscles
Earlier in the book (Chapter 2), mention wasmade of the importance of the muscular con-trol of dentures. Success in achieving this, as inso many aspects of prosthetic dentistry, is de-pendent upon the efforts of three people:
(1) The clinician – in recognising the importanceof muscular control as well as designingand prescribing the shapes of dentures to becompatible with oral function.
(2) The dental technician – in also appreciatingthe importance of muscular control, follow-ing the clinician’s prescription accuratelyand translating it into correctly designeddentures.
(3) The patient – in literally getting to gripswith the final product and, with the clini-cian’s support, persevering with the often-challenging task of learning the techniquesfor controlling the prostheses.
This chapter focuses on two aspects of denturedesign which are important in influencing howdentures function within the muscular environ-ment into which they are placed:
� The positioning of incisor teeth� Recording the position of the neutral zone
The relevance of a patient’snatural incisal relationshipIn dental publications it is common for pho-tographs of dentitions or casts to depict a ClassI incisal relationship and consequently there isa temptation to think, mistakenly, of this as thenorm. A key objective of this chapter is to makethe point that if such a relationship is providedfor all complete dentures, treatment will fail in asizeable proportion of patients. To prevent thisfrom happening, there is a need to assess thepatient carefully so as to establish a diagnosis ofthe skeletal relationship and the former incisalclassification as both will influence the subse-quent clinical and technical procedures.
A consideration of natural and artificial in-cisal relationships reveals a close similarity be-tween orthodontic and prosthetic knowledge.At first thought, the two specialities might ap-pear to be poles apart, as they are concernedlargely with patients from opposite ends of
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
174

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
Dentures and Muscles 175
the age range. However, a study of the fac-tors which govern the development of the nat-ural occlusion – particularly the influence ofthe surrounding muscles – reveals fundamentalsimilarities. Furthermore, it becomes increas-ingly apparent that prosthetic dentistry can bepractised successfully only if this orthodonticknowledge is applied to the clinical prostheticsituation.
Development of the naturalocclusion
As teeth erupt into the oral environment, theirposition is influenced by the activity and pos-ture of the surrounding muscles, the size, shapeand relationship of the jaws, and the occlusalforces produced by tooth contact. The shapeand size of the jaws are inherited and, aftergrowth has ceased, cannot be changed otherthan by surgical intervention. The functionalbehaviour of the muscles is partly inherited butmay also be modified by treatment. It is impor-tant to consider the muscles and jaws as oneunit because the muscles function from theirskeletal origins and insertions.
The position of natural teeth is influencedmore by the long-term forces associated withmuscle posture than by the short-term forcesoccurring during function. As the teeth erupt
Class III -
4%
Class I -
44%
Class II division 1 -27%
Class II unclassified -
7%
Class II division 2 -
18%
Figure 12.1 Percentages of thedental arch relationships occurringin English school children. (AfterFoster & Walpole Day 1974.)
into a mould of muscular tissue created by thelips, cheeks and tongue, they eventually takeup positions of relative stability related to therelaxed posture of these muscles. This situa-tion contrasts with that occurring with com-plete dentures, which are all too readily dis-placed both by the short-term functional forcesand also perhaps by the long-term posturalforces. The design of complete dentures, partic-ularly that of the lower prosthesis, therefore hasto take muscular displacement into account ifstability is to be achieved.
The prosthetic problem
When both clinician and dental technician arefirst taught to set up artificial teeth for com-plete dentures, it is traditional to position themin a Class I incisal relationship with a horizontaloverlap of 2 mm and a vertical overlap of 2 mm.But for how many edentulous patients does this‘normal’ incisal relationship resemble the pre-vious natural dentition? In a survey of Englishschool children aged 11–12 years, the percent-ages for the various dental arch relationshipsassessed on a modified Angle’s classificationwere as shown in Fig. 12.1 (Foster & WalpoleDay 1974). Thus, 52% of the children pos-sessed a Class II incisal relationship. Of course,it is possible to correct some of the incisal

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
176 Prosthetic Treatment of the Edentulous Patient
Skeletal class I -41%
Skeletal class II -54%
Skeletal class III -5%
Figure 12.2 Percentages of theskeletal patterns occurring in En-glish school children. (After Foster &Walpole Day 1974.)
relationships, but it must be remembered thatthe success of such treatment depends uponthe underlying jaw relationship. The greater thediscrepancy in jaw size and relationship, theharder it is to produce an ideal incisal relation-ship. More significant, therefore, are the resultsof the survey showing the variation in skeletalpattern, as shown in Fig. 12.2 (Foster & WalpoleDay 1974).
It must be pointed out that these figuresare representative of a group of young adoles-cents and that further growth of the mandiblemay reduce the number of those possessing askeletal Class II pattern in a small percentageof cases; however, in the majority of patientsthe underlying Class II skeletal pattern is main-tained into adulthood. The point being made isthat parity will not be established between thisgroup and the skeletal Class I group.
The results of the surveys suggest that, in theUK, the most common occlusion is a Class IItooth relationship superimposed upon a skele-tal Class II jaw relationship. As a result, itwould be expected that if all edentulous pa-tients were provided with dentures which hada Class I incisal relationship, many such artifi-cial dentitions would be in a different class fromthe previous natural ones. Some modificationof the artificial arrangement is, of course, per-missible and even requested by the patient –just as orthodontic treatment can be undertakento modify a malocclusion where the prognosisis favourable. Of the remainder, the patient willeither adapt to the dentures with difficulty or
find them quite intolerable. However, as dis-cussed fully in Chapter 2, the success of pros-thetic treatment depends so much upon theadaptability of a patient that if additional de-mands are made by creating an incisal relation-ship completely divorced from the natural statethe chances of prosthetic treatment succeedingare reduced. The reasons for possible failurewill be discussed in the next section, after whichways of preventing failure will be described.
Reasons for failure of treatment
To discover why prosthetic treatment may failas a result of providing dentures with an incor-rect incisal relationship, it is logical to considereach type of incisal relationship in turn and askthe following questions:
� How can a Class I artificial incisal relation-ship be produced?
� What is likely to happen as a result?
Class I
Figure 12.3 illustrates the tracing from a lateralskull radiograph of a dentate adult subject pos-sessing a Class I incisal relationship. Of course,if complete dentures are constructed with thesame incisal relationship, the artificial occlusionwill be similar to the previous natural one, andfew problems will be expected.

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
Dentures and Muscles 177
Figure 12.3 Tracing from a lateral skull radiographof a dentate patient showing a Class I incisal relation-ship.
Class II division I
In order to convert a Class II division 1 incisalrelationship (Fig. 12.4a) into a Class I relation-ship, it is necessary to modify the horizontal in-cisor overlap and, if there is an increased over-bite, the vertical overlap as well. The horizontal
a b c
Figure 12.4 (a) Class II division1 natural incisal relationship. (b) Up-per artificial teeth placed in the sameposition as the natural ones; lowerteeth proclined forwards. (c) Lowerartificial teeth placed in the same po-sition as the natural ones althoughthe crown length is reduced; upperteeth moved back.
overlap may be reduced by moving either thelower incisors labially or the upper incisorspalatally. If there is a deep overbite the verticaloverlap can be altered by reducing the crownlength or increasing the occlusal vertical dimen-sion of the dentures. This latter option wouldmean that the freeway space is substantially re-duced or eliminated altogether and so is notfeasible. Complications which are likely to arisewhen following the other possibilities becomeapparent when considering the example in thesame figure.
In Fig. 12.4b, the upper artificial teeth areplaced in the same position as the natural oneswhile the lower teeth are placed further for-wards. The result of this modification is to po-sition the lower labial segment anterior to theneutral zone. The force exerted by the lower lipis no longer balanced by that of the tongue andso the lower denture becomes unstable. This er-ror is not an uncommon one and is illustratedby the clinical case shown in Fig. 12.5.
In Fig. 12.4c, the lower incisors are placedin the position of the natural teeth and the up-per anterior segment is moved backwards. Thistreatment may be quite acceptable if the skele-tal relationship is favourable, just as orthodon-tic treatment in the natural dentition may suc-cessfully reduce a large horizontal overlap.However, there is the possibility of a markedchange in appearance – including reduced sup-port for the upper lip – which might be forthe worse, as shown in Fig. 12.6, where the

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
178 Prosthetic Treatment of the Edentulous Patient
Figure 12.5 Top left: the incisal relationship of a patient complaining of a loose lower denture. Bottom left: thelower anterior teeth are positioned forwards of the neutral zone. Pressure from the lip results in mobility of thedenture. Bottom right: replacement denture with the lower incisors placed in muscle balance. Top right: as a resultof this change in incisal position, a Class II division 1 relationship is produced.
anterior teeth and upper lip almost appear tobe strangers. A treatment possibility that canbe explored to overcome these problems is toretrocline the upper incisors rather than movethem palatally. This produces a Class II divi-sion 2 relationship, which reduces the horizon-tal overlap while retaining a realistic relation-ship of the necks of the teeth to the underlyingridge.
If the natural horizontal incisal overlap waslarge, allowing the lower lip to fall behind theupper incisors, a partial reduction of the over-lap in the subsequent dentures may result in avery unsatisfactory ‘half-way house’ where thelower lip is unable to take up a comfortable po-sition either behind or in front of the incisors.
This results in the persistent irritation of the lipby the incisal edge.
There is a group of patients possessing a se-vere skeletal Class II relationship, which is theresult of a prominent maxilla rather than an un-derdeveloped mandible, where treatment canbe carried out to correct a horizontal overlapwhich may be in the region of 10–20 mm. Al-though a combination of prosthetic treatmentand surgical removal of bone from the promi-nent premaxilla may improve the situation, itis frequently impossible to reduce the discrep-ancy completely and the patient will retaina Class II division 1 incisal relationship withthe overlap reduced to perhaps 5–10 mm. Anyfurther reduction may be impossible because

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
Dentures and Muscles 179
a
b
Figure 12.6 (a) Unsatisfactory relationship of up-per teeth to the upper lip produced by the top denturein (b). (b) The lower of the two dentures is a replace-ment with the anterior teeth placed further labially toimprove their relationship with the lip.
the amount of bone to be removed would to-tally eliminate the alveolar ridge anteriorly. Inaddition, it is important to realise that the alve-olar bone provides the upper lip with someof its support. If too radical an approach ischosen, the loss of lip support may be suchthat the change in appearance is anything butacceptable.
Class II division 2
The deep vertical overlap mentioned in theClass II division 1 case also occurs commonlyin Class II division 2 patients; the vertical over-
a b
Figure 12.7 (a) Class II division 2 natural incisalrelationship. (b) Artificial teeth placed in the same po-sition as the natural ones; the crown length of both theupper and lower teeth has been reduced.
lap can be reduced either by shortening thecrowns or by increasing the occlusal vertical di-mension. For the reasons already stated, any in-crease in occlusal vertical dimension is virtuallynever a viable option.
The deep vertical overlap shown in Fig. 12.7may be altered by reducing the crown lengthof the upper artificial teeth. However, the pa-tient with this type of natural incisal relation-ship rarely complains about the appearance ofthe teeth and so a change in incisal level is un-likely to be accepted. Fortunately, the situationregarding the lower teeth is not so critical andit is usually possible to reduce the crown lengthwithout detriment to appearance.
Class III
Two extremes of skeletal pattern are recognised.In the first the maxilla is small and the
Frankfort-mandibular plane angle is large (Fig.12.8). The prognosis for retention of an up-per denture is often poor because of the smalldenture-bearing area. If the upper anterior teethare moved labially to establish a Class I incisalrelationship, the force of the upper lip on thelabial face of the denture may be so great asto tip the balance between adequate stabilityand complete failure. Also the tipping forces

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
180 Prosthetic Treatment of the Edentulous Patient
O
Frankfort plane
Mandibular plane
Figure 12.8 A lateral skull tracing from a patientwith a skeletal Class III relationship and a largeFrankfort-mandibular plane angle.
generated during incision may be too great forthe patient to control the denture successfullyduring mastication. At best, it is usually advis-able to create no more than an edge-to-edge in-cisal relationship, although on occasion a lessambitious reverse horizontal overlap will haveto be accepted if a stable upper denture is to beproduced.
In the second, the maxilla has devel-oped normally, the mandible is large and theFrankfort-mandibular plane angle is small. Be-cause of a favourable palatal shape and size, theprognosis for retention of an upper denture isusually good and thus greater latitude may bepresent for positioning the artificial teeth.
Anterior open bite
The act of swallowing involves the productionof an anterior oral seal, which is normally madeby the lips meeting and the tongue remain-ing within the dental arches. However, in somepeople the seal is made by the tongue thrust-ing between the upper and lower anterior teethand contacting the lips. In the majority of cases,this behavioural pattern is adaptive. For exam-ple, if the upper incisors are unduly protrusive,the lower lip finds it extremely hard to move
around this dental barrier and meet the up-per lip; therefore, the anterior oral seal is mademore economically by the tongue meeting thelower lip. If the dental barrier is removed byorthodontic or prosthetic treatment so that thelips are able to come together, the tongue givesup its adaptive thrust and returns to more nor-mal function.
There remains a very small number of peo-ple, calculated as 0.6% of the population, wherethe tongue thrust appears to be the result ofan innate neuromuscular behavioural pattern(Tulley 1969). This so-called endogenoustongue thrust is frequently associated with asevere lisp and is resistant to treatment. Ifartificial teeth are positioned in a Class Irelationship, a dental barrier will have beenerected against the tongue as it continues toprotrude. The outcome of such treatment willbe instability of both upper and lower dentures,the likelihood of a sore tongue and a completeinability of the patient to adapt to such aforeign incisal arrangement. An example of atypical patient is shown in Fig. 12.9.
Prevention of failureTreatment failure due to an inappropriate re-lationship of the dentures to the surroundingmusculature can be prevented if particular careis taken in the assessment of the patient, inidentifying and recording the optimum posi-tion of the denture teeth and in subsequent lab-oratory procedures.
Assessment of the patient
The task of assessing the edentulous patientand deciding upon the classification of the pre-vious natural incisal relationship becomes moredifficult the longer the patient has been edentu-lous. The reasons are as follows:
� The patient’s own fading memory of the re-lationship of the natural teeth.

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
Dentures and Muscles 181
a
b
Figure 12.9 (a) This dentate patient has a largelower face height. Considerable muscular effort is re-quired to bring the lips together. (b) The anterior oralseal is made between the tongue and the lower lip,resulting in the anterior open occlusion shown here.
� Resorption of the alveolar bone leads to lossof support for the lips and cheeks and con-sequent changes in the facial features uponwhich the clinician depends for vital clues.
� An alteration in the jaw relationship follow-ing loss of teeth will occur through change inmandibular posture. Loss of tooth supportallows the mandible to move closer to the
maxilla and assume a more protrusive posi-tion which might falsely suggest a skeletalClass III relationship (Fig. 12.10).
� Increased activity of the lower portion of theorbicularis oris and mentalis muscles occursin long-term denture wearers. This changein muscle activity may cloud the clinician’sjudgement when assessing the patient.
Nevertheless, in spite of these difficulties, or-thodontic knowledge does allow the clinician toseek for clues in the edentulous patient:
Class I
Patients in this group have competent lips, askeletal Class I jaw relationship and an obtuselabiomental groove.
Class II division 1
A patient who possesses a Class II division1 incisal relationship superimposed upon askeletal Class II base is relatively easy to diag-nose. Typical features to observe are a retrusivemandible, an oval face, an acute labiomentalgroove and frequently a small lower face height(Fig. 12.11).
Class II division 2
A patient with a Class II division 2 incisal re-lationship possesses certain features which aredistinctive in the dentate patient and may stillbe clearly seen in the edentulous state (Fig.12.12). These features include a small lower faceheight, an acute labiomental groove, a smallFrankfort-mandibular plane angle, a prominentmental region of the mandible, a square go-nial angle and prominent zygoma. It is commonfor this type of patient to have a less markedskeletal discrepancy than is sometimes seen inthe Class II division 1 subject. It is necessaryto stress, however, that these features are not

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
182 Prosthetic Treatment of the Edentulous Patient
a b
Figure 12.10 (a) A patient in oc-clusion wearing her old dentureswhich have become badly worn.She appears to have a skeletal ClassIII jaw relationship. (b) The true jawrelationship once the occlusal ver-tical dimension has been restoredwith new dentures. The patient, infact, possesses a skeletal Class IIjaw relationship.
necessarily diagnostic outside the UK. For ex-ample, such a facial structure is commonly seenin Scandinavia and is not associated with aClass II division 2 incisal relationship.
Figure 12.11 An edentulous patient. The retrusivemandible, small lower face height and acute labiomen-tal groove point to the fact that the patient probablypossessed a Class II division 1 natural incisal relation-ship.
Class III
An edentulous patient who possesses a Class IIIocclusal relationship on one of the two skele-tal Class III base types is perhaps the easiestto diagnose. In the first type there may be ev-idence of the large lower face height, the ob-tuse Frankfort-mandibular plane angle and theoverall length of the face (Fig. 12.13). The sec-ond type with a normal maxilla and overdevel-oped mandible is also readily recognised.
Anterior open bite
In the dentate subject possessing an ante-rior open bite associated with an endogenoustongue thrust, circumoral muscular activity isseen during swallowing and there is often acharacteristic lisp. Neither of these diagnosticclues is reliable in the edentulous patient, be-cause the absence of teeth leads to indistinctspeech while the absence of lip support re-sults in abnormal muscular behaviour duringswallowing. However, a combination of thesefactors may point the way to the correct as-sessment. Without doubt, this small group of

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
Dentures and Muscles 183
Figure 12.12 The upper picturesare of a dentate subject possessinga Class II division 2 incisal relation-ship and illustrate the characteris-tic facial features described in thetext. The similar features of the eden-tulous woman shown in the lowerpictures suggest that she once pos-sessed a Class II division 2 naturalincisal relationship.
patients creates considerable problems in as-sessment and diagnosis.
Reliable information on the degree of lipcompetence is more likely to be obtained if thepatient is encouraged to relax completely andis then assessed from a distance. If the patient isseemingly unobserved, there is more likelihoodof natural lip activity being encouraged.
Adjusting the record rims
Remembering that one of the objectives ofrecording the occlusion is to show the dentaltechnician where the artificial teeth are to beplaced, it is vital that the record rims are shapedso that they reproduce the incisal relation-ship appropriate for the particular patient. In

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
184 Prosthetic Treatment of the Edentulous Patient
Figure 12.13 An edentulous patient. The combi-nation of large lower face height, obtuse Frankfort-mandibular plane angle and obtuse labiomentalgroove indicate that he possesses a skeletal Class IIIjaw relationship.
patients where only a horizontal overlap is re-quired, the procedure is relatively simple.
Complications arise in the skeletal ClassIII patient if the clinician underestimates the
a b
Figure 12.14 Effect of change inocclusal vertical dimension on askeletal Class III jaw relationship. (a)A reduction in occlusal vertical di-mension accentuating the Class IIIjaw relationship. (b) Restoration ofthe occlusal vertical dimension al-lowing a more acceptable incisal re-lationship to be produced.
required occlusal vertical dimension. The rela-tive protrusion of the mandible becomes morepronounced as the mandible approaches themaxilla with the result that the production ofan acceptable incisal relationship becomes in-creasingly difficult. Thus, the possibility of po-sitioning the labial segment in front of the neu-tral zone is increased (Fig. 12.14).
For a skeletal Class II patient, a horizontaloverlap is automatically produced if the rou-tine objectives of recording the occlusion aresatisfied, namely the rims being shaped to pro-vide satisfactory lip support and positioned inthe neutral zone to achieve stability. However,difficulties arise where a marked vertical over-lap is required. If the incisal level of each rim isadjusted to produce a pleasing appearance andthe same height maintained over the entire oc-clusal surface, it is likely that the occlusal ver-tical dimension will be excessive. The reasonsfor this become apparent when considering theocclusal plane of the natural dentition shownin Fig. 12.15, where it can be seen that the verti-cal overlap is the product of a particularly steepcurve in the occlusal plane. If this curve is re-produced on the record block, then it is possibleto provide the dental technician with the exact

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
Dentures and Muscles 185
Figure 12.15 A sagittal section through casts of aClass II division 1 incisal relationship. The vertical over-lap is the result of a steeply curved occlusal plane.
information on incisal relationship and heightof occlusal plane. One method of achieving thisis described in the following section.
Adjusting the rims for a Class IIdivision 1 incisal relationship
First, the upper rim is carved labially and in-cisally to indicate the correct position for theanterior teeth. Palatally, the rim is reduced inthickness to correspond to the size of the den-ture teeth. The lower rim is then shaped to theneutral zone and to the correct incisal height.The height of the lower rim in the buccal re-gion is reduced so that the correct occlusal ver-tical dimension is established. When the patientcloses together on the rims, the lower labial seg-ment will fit in behind the upper one and so es-tablish the required vertical overlap (Fig. 12.16).In some instances, it will be necessary to reducethe height of the upper buccal segments as well,in order to gain adequate freeway space.
At this stage, a somewhat artificial step hasbeen created between labial and buccal seg-ments of each rim. This abrupt step is softenedwhen the rim is replaced by the artificial teeth,but the overall curvature of the occlusal plane,as found in the natural dentition, is retained.
Figure 12.16 Recording the jaw relationship for apatient who possessed a Class II division 1 incisal re-lationship. Correct incisal levels and the degree of ver-tical overlap are produced by creating a step on thelower rim.
Positioning lower anterior teeth
Placing the lower anterior teeth in the neutralzone is crucial, especially if there has been con-siderable resorption of the mandible and thementalis muscle is particularly active. As a gen-eral rule, the necks of the artificial teeth shouldbe placed close to the crest of the residual ridge,otherwise it is likely that the muscle activity ofthe lower lip will displace the denture. Havingmade this point, it should also be mentionedthat it is frequently possible to give the incisorsa slight labial tilt. Such a proclination can helpto establish a favourable incisal relationship,while ensuring that the incisors remain in a po-sition of muscle balance between the lower lipand the tongue.
Recording the neutral zone
So far, the descriptions of recording the neu-tral zone in this chapter and in Chapter 11 havebeen restricted to the conventional methodwhereby the wax record rim is shaped so thatit lies within the neutral zone and is thus stable.For the vast majority of patients, this techniqueis perfectly satisfactory.

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
186 Prosthetic Treatment of the Edentulous Patient
There are, however, a few patients for whoma functional recording of the neutral zone is in-dicated. These patients may give a history ofnumerous unstable lower dentures and on ex-amination the clinician may anticipate that it isgoing to be difficult to identify the neutral zoneby simply carving the record rims. There maybe instances where the intraoral anatomy is soaltered – for example, as a result of surgery –that many of the usual anatomical landmarksno longer exist. In other cases it may be theamount and strength of activity of the oral mus-culature which suggests that a functional recor-ding of the neutral zone would be helpful. Insuch cases the clinical technique is as follows.
At the stage of recording the occlusion, theupper rim is shaped carefully so that it sup-
a b
c d
Figure 12.17 (a) Lower base for neutral zone impression. (b) Occlusal contact between the lower base andthe upper trial denture checked before the addition of the impression material. (c) Neutral zone impression whichhas been moulded by the muscles of the lips, cheeks and tongue. (d) Buccal and lingual indices in silicone putty.
ports the muscles of the cheeks and upper lipand fulfils all the criteria listed on pp. 155–158.The lower rim is trimmed so that a recording ofthe correct jaw relationship can be made. Thisstage can be accomplished quickly if the oc-clusal contact is restricted to a limited area inthe premolar-molar region as described on p.161. After the casts have been articulated, theupper trial denture is constructed.
A lower base is made in cold-curing acrylicresin. Molar pillars on the base are made to oc-clude with the upper denture at the correct oc-clusal vertical dimension. A thin spine, whichwill help to support the recording material, canbe added to the rest of the base and left clearof occlusal contact (Fig. 12.17a). In exceptionalcases the molar pillars and the spine can get

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
Dentures and Muscles 187
in the way of the investing muscles and there-fore affect the recording. In such cases a sim-ple acrylic base is produced, and molar pillarsare created intra-orally using a chairside relinematerial. During its plastic phase this materialwill be shaped by the muscles into the neutralzone. Once it has set the clinician can adjust theheight of the pillars to the required occlusal ver-tical dimension.
At the stage of recording the position of theneutral zone, checks are made of the upper trialdenture and of the occlusal contact with the mo-lar pillars (Fig. 12.17b). A mouldable material,with an extended setting time of several min-utes, is applied to the lower base which is thenreinserted in the mouth. The bulk of the addedmaterial must be carefully judged so that therim produced does not exceed the anticipatedthickness of the finished denture. The patientis instructed to alternately sip water and talk.In this way, the surrounding muscles shape therecording material (Fig. 12.17c).
When the material has set, the recording ofthe denture space is returned to the laboratorywhere it is seated on the master cast and in-dices are constructed around the buccal and lin-gual surfaces (Fig. 12.17d). The dental techni-cian now has a recording of the denture spaceenabling the artificial teeth to be positionedwithin its boundaries.
The benefit of a lower denture shaped bythe neutral zone impression technique has beenshown in a study measuring the magnitude offorce needed to lift the denture away from itssurrounding musculature. A larger force wasrequired to remove the ‘neutral zone’ denturethan the conventional denture (Miller et al.1998). For some patients this enhanced reten-tive ability of the tongue acting through the spe-cially shaped polished surface may make thedifference between success and failure.
Care in the dental laboratory
It is, of course, essential that the dental tech-nician accurately follows the blueprint of the
record blocks or neutral zone recording whensetting up the trial dentures. This is bestachieved if the artificial teeth are set into therim with only a small portion of the rim beingcut away each time. The remaining rim acts asa guide to the overall arch shape.
A postscript – pre-extractionrecordsHaving read this chapter, the reader may con-clude that the designing of complete denturesis to a large extent a matter of deduction andguesswork. This is in fact true when one is facedwith an edentulous patient and no record ofthe previous natural dentition. However, theamount of guesswork can be considerably re-duced if pre-extraction records of the naturaldentition are available. Many methods of ob-taining pre-extraction records have been de-scribed. Certainly, good-quality photographsand occluded casts of the natural dentitionprovide information about the incisal relation-ship. However, the casts do not indicate the all-important relationship of the teeth to the under-lying jaws and the surrounding musculature.In rare cases a lateral cephalogram radiographmay be available showing the true underlyingskeletal pattern. However, in the majority ofcases, such information can be obtained only bythe recording rims being shaped in the mouth.
The best method of transmitting the charac-teristics of the natural dentition through to theartificial one is undoubtedly by means of imme-diate dentures. The patient should be advisedthat these will always be a valuable source ofinformation to a clinician for the constructionof replacement dentures and therefore shouldnever be discarded.
It can be argued that if all edentulous pa-tients possessed their original immediate den-tures, the number of prosthetic problems wouldbe reduced considerably. For although imme-diate dentures will cease to fit the mouth ac-curately after a few years, and post-extraction

P1: JZP Trim: 246mm X 189mmc12 BLBK351-Basker January 4, 2011 7:57 Printer Name: Yet to Come
188 Prosthetic Treatment of the Edentulous Patient
changes in the jaws and muscles will result ina shifting of the neutral zone, the clinician stillhas evidence of tooth shape, tooth position andincisal relationship – without doubt informa-tion that can be invaluable in achieving a suc-cessful outcome.
Communication with the dentaltechnicianBoth the clinician and the dental technicianshould have a clear understanding of the prin-ciples which lie behind the provision of den-tures with the correct incisal relationship andrelationship to the neutral zone.
The record rims should be shaped accuratelyso as to provide an accurate blueprint for thedental technician.
It is essential to reinforce this blueprint bymeans of a written prescription.
Quality control andenhancementThe following themes might be consideredwhen instituting a review of performance in aseries of patients:
� In what percentage of patients’ records isthere a clear indication that an assessment ofthe appropriate incisal relationship has beenmade?
� In what percentage of cases has the dentaltechnician been given a clear prescription ofthe incisal relationship and neutral zone?
� When comparing old dentures with the re-placements, in how many instances has asignificant change been made to the incisalrelationship? In how many cases has thechange resulted in an improvement in ap-pearance, stability and function?
References and additionalreadingBerry, D.C. & Wilkie, J.K. (1964) Muscle activity in
the edentulous mouth. British Dental Journal, 116,441–7.
Foster, T.D. & Walpole Day, A.J. (1974) A survey ofmalocclusion and the need for orthodontic treat-ment in a Shropshire school population. BritishJournal of Orthodontics, 1, 73–8.
Liddelow, K.P. (1964) Oral muscular behaviour. Den-tal Practitioner and Dental Record, 15, 109–13.
Miller, W.P., Monteith, B. & Heath, M.R. (1998) Theeffect of variation of the lingual shape of mandibu-lar complete dentures on lingual resistance to lift-ing forces. Gerodontology, 15, 113–19.
Murphy, W.M. (1964) Pre-extraction records in fulldenture construction. British Dental Journal, 116,391–5.
Neill, D.J. & Glaysher, J.K.L. (1982) Identifying thedenture space. Journal of Oral Rehabilitation, 9,259–77.
Richardson, A. (1965) The pattern of alveolar boneresorption following extraction of anterior teeth.Dental Practitioner and Dental Record, 16, 77–80.
Tallgren, A. (1963) An electromyographic study ofthe behaviour of certain facial and jaw muscles inlong-term complete denture wearers. OdontologiskTidskrift, 71, 425–44.
Tulley, W.J. (1969) A critical appraisal of tongue-thrusting. American Journal of Orthodontics, 55,640–50.

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
13Try-in Procedures
Trial dentures are constructed by setting updenture teeth on shellac or acrylic resin (tem-porary or permanent) bases. This stage is usedto check the accuracy of the registration stageand to assess the appearance of the dentures sothat any appropriate modifications can be car-ried out. This clinical stage may be regarded asthe ‘dress rehearsal’.
The trial dentures should be examined firston the articulator and then in the mouth.
Assessment on the articulatorAn efficient and reliable examination of the trialdentures is more likely to be achieved if the op-erator inspects each of the denture surfaces inturn, checking the aspects listed below.
General appearance
The trial dentures as supplied from the dentallaboratory should be neat, clean and tidy. It isimportant to ensure that all requests includedin the prescription completed at the previousclinical stage have been taken through to thetrial dentures.
Impression surface
Fit
The bases of the trial dentures should be ac-curately adapted to the casts such that there isno movement when finger pressure is appliedto the occlusal surfaces. If the trial denturesare on permanent acrylic bases the impressionsurfaces should be checked for any sharp pro-jections, roughness or excessive extension intoundercuts.
Extension
The border regions of the dentures should beshaped to conform to the depth and width ofthe sulci on the casts. In the upper jaw, the baseshould normally be extended posteriorly to thepost-dam cut or formed in the cast, and in thelower jaw over the pear-shaped pads.
Relief chamber
If a relief chamber has been requested, a checkshould be made that it is present and of the
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
189

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
190 Prosthetic Treatment of the Edentulous Patient
b a
Figure 13.1 Occlusal view of twolower dentures: (a) the teeth followthe crest of the ridge; (b) markeddiscrepancies between the positionof the teeth and the crest of theridge are present, suggesting thatthe teeth will not be in the neutralzone.
required size and shape. If it has been left withsharp margins these will need to be rounded.
Polished surface
Position of the lower teeth
The teeth on a lower denture should normallybe positioned to conform fairly closely to thecrest of the mandibular ridge. If there are grossdiscrepancies between the position of the teethand the ridge (Fig. 13.1), the teeth may not be inthe neutral zone (p. 65) and could become thecause of instability in the mouth. However, thisis not invariably the case, so final judgement onthis aspect must be delayed until the dentureshave been examined in the mouth.
Position of the upper teeth
If a biometric approach is being adopted in thedesign of the upper denture (Chapter 10), theposition of the teeth and the polished surfacesshould be checked in relation to the palatal gin-gival vestige and incisive papilla. The trial den-ture can also be compared with the record rimif this is still available, or with the positions ofthe teeth on the existing denture if this has beenused as a reference.
Inclination of the polished surfaces
The buccal and lingual aspects of the polishedsurfaces should converge occlusally so that
pressure from the surrounding muscles of thecheeks, lips and tongue contributes to retentionrather than displacement (Fig. 4.3). The excep-tion to this rule is found in the upper anteriorregion where the labial surface of the flange of-ten faces upwards and outwards (Fig. 12.6b).
Surface contour
The polished surface of the denture should nor-mally be smooth for optimum comfort and tofacilitate plaque removal. This is particularlyimportant around the necks of the teeth. Wherethe requirements of appearance make it desir-able the polished surface may be contoured andstippled to simulate the mucosal surface. Thisis usually only indicated for the upper labialflange.
Comparison with previous dentures
If the patient already has dentures, they shouldbe compared with the trial dentures to seewhether any planned similarities or changes,such as arch shape or arrangement of the an-terior teeth, have been reproduced correctly.
Occlusal surface
There should normally be bilateral even contactin the intercuspal position. Opposing cuspedteeth should interdigitate accurately. Wherean average movement or semi-adjustablearticulator has been used excursions should

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
Try-in Procedures 191
be checked to see if balanced articulation ispresent.
Assessment in the mouthThe dentures should first be assessed individu-ally for:
� physical retention;� stability;� extension of the denture bases;� relationship to the neutral zone.
Details of the clinical procedures are describedin Chapter 7. The dentures should then be as-sessed together for:
� evenness of occlusal contact;� occlusal vertical dimension;� appearance.
Physical retention
If the prognosis for retention in the upper jawis good, dislodgement should be expected to bedifficult. In the case of the lower denture, re-tention is often poor because of the relativelysmall denture-bearing area and the difficulty inobtaining an efficient border seal. If the physi-cal retention of an upper trial denture is not asgood as would be expected from the anatomicalconditions existing in a particular patient, thecause should be identified and, if found to be afault in the denture, must be corrected. Denturefaults may include the absence of a border sealresulting from:
� under-extension;� inadequate width of flange;� ineffective seal at the posterior border;� poor fit of the denture base.
Stability
Movement of either denture of more than 2 mmsuggests lack of stability of the denture. A
judgement then needs to be made as to whetherthis is due to:
� lack of fit of the denture; or� displaceability, or unfavourable shape, of the
denture-bearing tissues.
Extension of the denture bases
The accuracy with which the denture bordersconform to the depth and width of the sulcimust be determined. The all-important poste-rior extension of the dentures over the pear-shaped pads in the lower jaw and to the junc-tion of the hard and soft palate in the upper jawmust also be checked.
If marked over-extension of the dentureflanges is present, stretching of the sulcus tis-sues will occur when the denture is insertedinto the mouth and their subsequent elastic re-coil will cause dislodgement of the denture.Therefore, if the denture is displaced immedi-ately after being seated, over-extension shouldbe suspected. A small degree of over-extensionmay cause dislodgement of the denture whenthe clinician gently manipulates the lips andcheeks or when the patient raises the tongue.The exact location of such an error can be deter-mined only by carrying out a careful intra-oralexamination. When over-extension is present inareas where the visibility is good, displacementof the sulcus tissues will be seen as the dentureis seated. However, in the lingual pouches, vis-ibility is poor, so the clinician will have to makean assessment based on the behaviour of thelower denture as the tongue is moved. Correc-tion of over-extension is by reducing the depthof the offending flange. If this is not carried out,the finished dentures will traumatise the mu-cosa in that area and will be unstable becauseof the large displacing forces exerted by the softtissues.
The presence of under-extension is deter-mined primarily by intra-oral examination,when the depth of the sulcus will be seen tobe greater than that of the denture flange. In

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
192 Prosthetic Treatment of the Edentulous Patient
a b
Figure 13.2 The relationship ofthe lower posterior teeth to thecheeks and tongue: (a) correct – buc-cal surfaces of the teeth are in closeproximity to the buccal mucosa; thelevel of the occlusal plane allows thetongue to rest on the occlusal sur-faces; (b) incorrect.
the case of the upper denture, however, a pre-liminary indication of under-extension will begiven by the existence of poor physical reten-tion. Correction of any under-extension willusually entail taking a new impression in thetrial denture. Failure to do this will result inreduced physical retention of the finished den-tures and inadequate distribution of load to thetissues.
Relationship to the neutral zone
The positioning of teeth in the neutral zoneis of particular importance in the case of thelower denture because the physical retentionis relatively weak. Identification of the neu-tral zone will have been attempted while shap-ing the record block at the earlier visit andnow the trial denture must be checked to seeif that assessment was correct and has beentransferred accurately to the denture. When thelower denture is inserted, it should remain inplace when the mouth is half open and thetongue is positioned so that its tip lies just be-hind the lower anterior teeth. The tongue mustnot be allowed to adopt the retracted ‘defensivetongue’ posture otherwise it will not be possi-ble to make the required assessment. A useful‘rule of thumb’ is that the lower denture willusually be stable if narrow teeth are used and
are placed as far buccally, or labially, as possiblewithout displacing the cheek and lip tissues. Bythis means, maximum tongue room is providedwithin the limits dictated by the lips and cheeks(Fig. 13.2a). If there is space between the buccalsurfaces of the posterior teeth and the mucosaof the cheek (Fig. 13.2b), it is almost certain thatthere is inadequate tongue space.
If displacement of the denture does occur,the cause must be identified and the den-ture modified to correct the instability. An areawhere this difficulty commonly arises is thelower anterior region where the lip may ex-ert excessive pressure, causing the denture tomove upwards and distally. Correction of thistype of fault should be carried out at the chair-side so that the effect of the alterations can beassessed in the patient’s mouth. The offendingteeth may be reset in the correct relationship tothe soft tissues or they may be removed and re-placed with a wax rim which is shaped witha wax knife until a stable denture is produced.The dental technician is then asked to reset theteeth in the position indicated by the rim.
If the dentures being constructed are replace-ments for dentures which have given good ser-vice in the past, it may usually be assumedthat the relationship of the old denture to thecheeks, lips and tongue is satisfactory and thatconsequently this relationship should be copied

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
Try-in Procedures 193
in the trial dentures. Both old and new den-tures should be compared in the mouth to seewhether this relationship has been faithfully re-produced.
While assessing the position of the lowerteeth relative to the soft tissues, the height of theocclusal plane in relation to the tongue shouldbe noted. When the tongue is relaxed, it shouldbe able to rest on the occlusal surfaces of theteeth – a situation which favours retention ofthe lower denture (Fig. 13.2a).
Occlusal vertical dimension
Assessment of the occlusal verticaldimension
MeasurementThe lower trial denture should be inserted andthe rest vertical dimension measured. Then,after inserting the upper denture and measur-ing the rest and occlusal vertical dimensions,an initial impression can be gained of the ad-equacy or otherwise of the freeway space. If anegative freeway space is suspected then it isworth reassessing the rest vertical dimension,this time without the lower denture.
Facial appearanceThe initial impression regarding the freewayspace should be backed up by an assessment ofthe patient’s appearance. If the patient’s facialproportions and contact between upper andlower lips appear to be appropriate when theteeth are occluded, it suggests that the occlusalvertical dimension is correct. This assessmentcan be broadened by asking the patient to oc-clude and then to relax the mandible severaltimes while the clinician assesses the freewayspace by observing the amount of mandibularmovement. Changes in facial proportions, lipposture and jaw relations during these move-ments will also help the observer to decidewhether the occlusal vertical dimension is ac-ceptable.
SpeechFinally, the patient should be asked to speakwhile wearing the trial dentures. The teeth donot normally contact during speech but ap-proach most closely when the ‘S’ sound ismade. The separation is known as the closestspeaking distance and is usually about 1 mm. Ifthe occlusal vertical dimension of the trial den-tures is excessive, the space may be absent; cor-respondingly, it will be increased if the occlusalvertical dimension is too small. This assessmentcan be made by asking the patient to count outloud from ‘sixty’ to ‘seventy’.
Correction of the occlusal verticaldimension
Occlusal vertical dimension too smallWhen the freeway space is too large, it is cor-rected by adding the appropriate thickness ofwax to the occlusal surfaces of the posteriorteeth on one of the dentures, adjusting the waxto produce an even occlusion at the desired oc-clusal vertical dimension and then re-recordingthe jaw relationship in the retruded contact po-sition.
Occlusal vertical dimension too largeWhen the freeway space is too small, or absentaltogether, teeth will have to be removed fromone of the dentures and be replaced with a waxrim before the new recording can be made. Thedecision as to which denture should be reducedin height will depend on how much more free-way space needs to be created, the relation-ship that the corrected height of occlusal planewould have to the tongue (Fig. 13.2) and theeffect any change in height would have on ap-pearance. It is often sufficient to remove just theposterior teeth for this purpose, but it may alsobe necessary to remove the anterior teeth wherethe horizontal overlap is such that further clo-sure would be prevented by anterior toothcontact.

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
194 Prosthetic Treatment of the Edentulous Patient
Evenness of occlusal contact
When a shellac or temporary acrylic base hasbeen used, there may be some looseness of theupper trial denture which may make it impos-sible to carry out an accurate assessment of theocclusion in patients, especially where anatom-ical factors are unfavourable. In these circum-stances, application of a denture fixative to theimpression surface can provide a solution. Thisshould, though, be done only if all other causesof instability have been eliminated.
A bowl of cold water should be available atthe chair side so that frequent chilling of thetrial dentures can be carried out. If the denturesare left in the mouth for more than a few min-utes at a time, softening and distortion of thewax will occur.
Retruded contact positionThe occlusion should first be checked withthe mandible in the retruded contact position.The patient closes slowly so that the cliniciancan observe the initial occlusal contact. Thisfirst contact should not be on one or 2 teethbut should be a widespread and even contactaround the arch. The final occlusal relationshipis not so reliable for assessment, as the earlycontact of one or 2 teeth may have been maskedby compression of the mucosa beneath the den-ture, tipping of the denture or posturing of themandible.
Lateral and protrusive positionsThese positions will already have been exam-ined on the articulator. If further assessment iscarried out in the mouth the patient must bestrongly advised to only use very light toothcontact, as the excursive movements can read-ily displace the denture teeth from the wax.
Methods of occlusal assessment
VisualIf a relatively large occlusal discrepancy ispresent, the clinician will be able to see this
without any difficulty. However, the existenceof smaller faults may be deduced from evidencesuch as slight tipping or lateral movement ofthe dentures as they occlude.
Patient perceptionThe patient should be asked if the dentures arecontacting evenly. Many patients are able to de-tect occlusal unevenness which is so slight thatit could be overlooked by the clinician.
Articulating paperThe use of articulating paper is not indicated atthis stage because of the following reasons:
� Teeth are readily displaced from the waxby the pressure required to make the papermark the teeth.
� Direct visual checking of the occlusion to-gether with the patient’s comments are usu-ally sufficient to allow the clinician to an-swer the key question – ‘Are there any errorsin the occlusion large enough to require re-recording of the jaw relationship, or are theyso small that their correction is best left untilthe dentures are processed and the teeth arefirmly anchored in the acrylic bases?’
Correction of occlusal faults
Both vertical and horizontal discrepancies inthe occlusion may occur.
Vertical occlusal discrepancyA vertical occlusal discrepancy may take theform of a unilateral, anterior or posterior openocclusion. If this type of fault is present, theretruded position should be re-recorded aftermodifying one or both of the dentures to pro-duce an even occlusion at the correct occlusalvertical dimension. There are several ways inwhich this may be achieved, the choice ofmethod depending on the occlusal vertical di-mension of the trial dentures (Fig. 13.3). Be-fore carrying out the modifications, the clin-ician should determine whether or not the

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
Try-in Procedures 195
(a) OVDtoo small
Waxadditions
Waxaddition
Recordblocks
(b) OVDcorrect
(c) OVDtoo large
Figure 13.3 Methods of correct-ing a unilateral open occlusion at thetry-in stage: (a) if the occlusal verti-cal dimension is too small, an appro-priate thickness of wax is added tothe upper or lower denture on bothsides of the dental arch; (b) if the oc-clusal vertical dimension is correct,wax is added to the side with theopen occlusion to produce even bi-lateral occlusal contact; and (c) ifthe occlusal vertical dimension is toolarge, the teeth on one of the den-tures are removed and replaced witha wax rim reduced in height by anappropriate amount. Final recordingof the retruded contact position maybe made in each case using a suit-able registration material placed onboth sides of the arch.
orientation of the occlusal plane of the upperdenture is correct in lateral and anteroposteriorplanes; if it is, the alterations will be carriedout on the lower denture. If the plane is wrong,the upper denture will also have to be modi-fied by resetting the anterior teeth, or replacingthe teeth with a wax rim, to indicate to the den-tal technician the correct position of the occlusalplane.
Horizontal occlusal discrepancyAn occlusal discrepancy in the horizontal planemay be detected by observing that the upperand lower centre lines are not coincident, thatthe posterior tooth relationship is not symmet-rical, or that the horizontal overlap is not thesame in the mouth as it is on the articulator. Anew recording of the retruded contact positionshould be obtained after the teeth from one ofthe dentures have been removed and replacedwith a wax rim. If the teeth are not removed,there is a danger that the cusps will guide the
mandible back into the incorrect intercuspalposition.
AppearanceThe appearance must be assessed by both clini-cian and patient.
The clinician’s assessment
At the try-in stage, the clinician must re-assessthe information concerning the appearance ofthe dentures which was acquired at the ap-pointment for recording occlusion. This in-cludes the following:
� Shade of the teeth� Mould of the teeth� Size of the teeth� Orientation and level of the occlusal plane� Position of the centre line� Degree of lip support

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
196 Prosthetic Treatment of the Edentulous Patient
A check on basic aspects of the trial dentures,such as orientation of the occlusal plane andposition of the centre line, can best be made ifthe upper lip is reflected so that a clear view ofthe maxillary teeth is obtained. However, thismethod of examination is not appropriate whenassessing the overall aesthetic effect. To makethis latter judgement, the teeth should be ob-served during function by the clinician engag-ing the patient in conversation and, if possi-ble, encouraging the patient to smile naturally.This functional assessment is very importantbecause dentures which have a pleasant ap-pearance in repose may suddenly become glar-ingly unsuitable as soon as the patient’s lipsmove in speech.
The patient’s assessment
The patient must be given ample opportunityto see the dentures in situ and form an opin-ion regarding their appearance. This stage is ofparamount importance and is not uncommonlyallotted too little time. It is, of course, essentialthat the patient’s requirements regarding theappearance of the dentures should be discussedfully, not only at the try-in stage but also duringthe preceding stages of the course of treatment.The clinician’s role in these discussions shouldbe that of an adviser who ensures that thepatient is in possession of all the informationrequired to make a sensible decision. For exam-ple, some patients will request that their den-tures have anterior teeth which are small, whiteand even – a combination which will almostguarantee that the dentition is easily recognisedas being an artificial one. However, these pa-tients will often change their minds if given theopportunity at the try-in stage of seeing the im-provement that even a small amount of alter-ation can make.
If a patient has strongly held views abouthow the dentures should look, the clinicianshould take great care not to be too persuasiveso that the patient accepts an arrangement ofanterior teeth which conflicts with these views.
If this happens, the patient is likely to be dis-satisfied with the finished dentures and could,with complete justification, request that they beremade.
Sometimes it is difficult for a patient to forma clear opinion regarding the appearance of thedentures in the relatively strange surroundingsof the dental surgery. If a friend or relative isavailable to offer an opinion, this can be of con-siderable help to the patient, particularly if theclinician leaves the room so that they are able todiscuss the appearance in an uninhibited man-ner. In the absence of a friend, discussing theappearance with the dental nurse can be verybeneficial.
It is preferable for the patient to assess theappearance of the dentures by looking at themin a wall mirror at a normal viewing distance,rather than using a hand mirror which may beheld too close to the face and give an unreal-istic view. In exceptional cases, where there isparticular difficulty in determining what an ac-ceptable appearance is, it may even be neces-sary to permit the patient to take the trial den-tures home for a short time provided the fragilenature of the trial dentures is made quite clear.
Achieving a natural appearance
The final appearance is created by:
� detailed arrangement of the anterior teeth;� shaping the gingival margins;� grinding the incisal edges where necessary.
If the arrangement of the anterior teeth requirescorrection, the modifications should ideally becarried out at the chair side, so that the altereddentures can be tried in the mouth and the ef-fectiveness of the changes assessed by both theclinician and the patient. If the dental techni-cian does need to be involved it is of immensevalue for him or her to be present in the surgeryto see the situation directly rather than relyingon written or telephoned instructions.

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
Try-in Procedures 197
a b
Figure 13.4 (a) Imbalance produced by inclining the vertical axes of the anterior teeth in the same direction.(b) The improvement in appearance produced by counterbalancing the inclination of the axes on one side of themouth with those on the other.
The clinician should attempt to create theillusion of natural teeth when finalising theappearance. In order to carry out this visual de-ception successfully, the appearance of the den-tures should be appropriate for the patient inquestion and also appropriate for the popula-tion from which the patient comes. If these re-quirements are fulfilled, the teeth will appear to‘belong’ to the patient and the deception will becomplete.
Introducing irregularityIt should be remembered that the prevalence ofirregularity or crowding of natural teeth is high.Therefore, if dentures are constructed with a‘perfect’ arrangement, the risk of the result-ing appearance seeming artificial is consider-able. As a general rule, imperfection in the an-terior tooth arrangement is a basic requirementin creating the illusion of natural teeth. Com-plete symmetry should be avoided: for exam-ple, the anterior teeth should not be placed sothat the incisal edges are all at the same level.Some form of crowding, which may vary in de-gree from minimal irregularity to marked over-lapping of the teeth, should usually be incor-porated into the anterior tooth arrangement.When producing irregularity, care should betaken to ensure that a general impression of bal-ance is maintained even though the two sidesof the dental arch may not be identical. For ex-ample, if the centre line of the teeth is somedistance from the midline of the face, or if theincisal level is not horizontal, a sense of im-
balance will result and the appearance will bepoor. The vertical axes of the anterior teeth canbe varied, but if the inclination of these axes onone side of the mouth does not approximatelybalance that on the other, an unsatisfactory ap-pearance will result (Fig. 13.4).
Incisal relationshipThe method of determining an incisal relation-ship which is appropriate for an edentulous pa-tient’s skeletal relationship has been discussedin Chapter 12. If a patient is provided with den-tures which have an inappropriate incisal rela-tionship, for example, a Class I incisal relation-ship on a marked skeletal Class II base, there isa risk that, in addition to problems with stabil-ity, the dentures will appear incongruous andthe aesthetic result will be poor.
AgeChanges in the shape of the crowns of natu-ral teeth commonly occur as a result of increas-ing age. These alterations in crown shape areproduced by incisal wear and gingival reces-sion. Anterior teeth on dentures can thereforebe given a definitely youthful, or aged, appear-ance by incisal grinding where appropriate andcorrect shaping of the gingival margins (Fig.13.5). If a ‘young’ dental appearance is pro-vided for an older patient, or vice versa, it willbe only too apparent that the patient is wearingdentures.

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
198 Prosthetic Treatment of the Edentulous Patient
Figure 13.5 Use of incisal grinding and gingivalcontouring to convert a youthful appearance UR3-UR1to an aged one UL1-UL3.
SexWhen determining the appearance of dentures,the sex of the patient should also be taken intoaccount. Although there is no evidence that theform and arrangement of natural teeth are re-lated to the sex of the individual, there is aview that artificial teeth can be arranged tocreate either a so-called ‘feminine’ or ‘mascu-line’ appearance (Fig. 13.6) (Hyde et al. 1999).Masculinity can be suggested by increasing theirregularity of the arrangement and by usingsquarish moulds with obvious surface charac-ter while, conversely, a more even arrangementof rounded, smooth-surfaced anterior teeth willimpart a feminine quality to the appearance.Rotation of the incisors in a vertical plane may
Figure 13.6 (a) An example of a ‘masculine’ ante-rior tooth arrangement. (b) An example of a ‘feminine’anterior tooth arrangement.
Table 13.1 Features that can help to determine the‘sex’ of dentures.
Male Female
Large teeth Small teeth
Square moulds Rounded moulds
Characterised labialsurface
Smooth surface
Irregularity Even arrangement
Distal margins labially Distal margins palatally
Significant wear ofincisal edges
Minimal wear ofincisal edges
Diastemas Closed contact points
Prominent canines Canines not prominent
also help to ‘sex’ the dentures; moving the dis-tal margins labially will increase the vigour andmasculinity of the appearance and vice versa.
Features that help to determine the ‘sex’ ofdentures are summarised in Table 13.1.
Arrangement of the lower anterior teethOnce the upper anterior teeth have been ad-justed, consideration should be given to thelower teeth. These, in some patients, will notmake such an important contribution to theappearance; nevertheless, they should not beignored. In many patients, they will be dis-played more during function than the upperteeth and therefore may be a dominant factorin determining the patient’s dental appearance.Again, the same general rules regarding perfec-tion and evenness of tooth arrangement whichhave been discussed previously should beapplied.
Labial flangeIn some patients, the upper labial flange willbe visible during speech and smiling. If this isthe case, a natural appearance will be achievedonly if the acrylic flange is contoured to resem-ble natural gum, and if the surface of the flangeis slightly irregular or stippled to break up any

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
Try-in Procedures 199
reflections (Fig. 13.5). If melanotic pigmentationof the mucosa is present, a pale pink flange willseem out of place. The technician should there-fore be requested to tint the labial flange duringprocessing.
Denture markingMarkers in dentures can be of immense valuefor the identification of the following:
� Dentures – in dental laboratories, hospitalsand care homes.
� Individuals – following loss of conscious-ness, memory or life.
Identification of dentures in dentallaboratories
This is important in dental laboratories wherelarge numbers of dentures are being processed.This procedure is widely practised by dentaltechnicians and does not require instructionsfrom the clinician.
Identification of dentures in hospitalsand care homes
The ability to identify dentures is of great valuein hospitals and care homes because older andconfused patients, and sometimes staff, notinfrequently misplace the dentures (Michaeliet al. 2007). Losses are particularly regrettablebecause the dentures may be virtually irre-placeable as a result of an older person’s diffi-culty in adapting to new dentures of differentdesign. And yet, surveys into the marking ofdentures in care homes showed that this hadbeen done in only 35–47% of cases (Bengtssonet al. 1996; Stenberg & Borrman 1998). In a morerecent study, whereas over 80% of prosthodon-tic specialists believed that the marking of den-tures was a worthwhile procedure, yet just overhalf actually carried it out routinely; none of thecare homes included in the study followed suit(Murray et al. 2007).
An identification mark allows a misplaceddenture and its owner to be reunited. The
following steps should be taken routinely toreduce the considerable number of dentureswhich are actually lost:
� The care programme for the patient shouldrecord whether the patient possesses den-tures, whether they are usually worn andwhether they are with the patient rather thanbeing looked after by relatives.
� There should be an understanding withinthe care team that dentures are normally inone of two places – either in the patient’smouth or in a clearly labelled denture pot.If not, a search must be made urgently asthe precious dentures could easily have beenwrapped up in dirty linen or be languishingin a waste-paper basket.
Identification of individuals
Dentures can be marked to allow identifica-tion of patients following loss of consciousness,memory or life. For this system to be fully ef-fective, the marker needs to be indestructibleand to incorporate a code which is universallyacceptable. As the latter requirement has notbeen fulfilled at the present time, such markersare not widely used in general dental practice.However, they are routinely used in the ArmedForces and are regulated by law in Sweden, Ice-land and in many states in the USA (Borrmanet al. 1999). Requirements for denture markersused for this purpose include that they are:
� Biologically inert� Inexpensive� Widely available� Easy to inscribe� Retrievable after an accident� Able to survive elevated temperatures� Visually acceptable to the patient (Richmond
& Pretty 2009)
Identification marks fall into two broad cate-gories, surface markers and inclusion markers.

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
200 Prosthetic Treatment of the Edentulous Patient
Surface markers
Scribing the cast
Marks may be produced on the impression sur-face of the denture by scribing the cast beforeprocessing the denture. The irregularities pro-duced on the denture surface are clinically un-desirable and therefore should be reserved foridentifying dentures in laboratories after pro-cessing. The marks should be removed beforedelivering the denture to the patient.
Pen or pencil
Marks on a denture can be made by writingwith either a spirit-based pen or a fine pencil.However, pencil marks require protection witha polymer varnish. Both techniques offer rel-atively short-term benefits. Exposure of spiritpen marks to hypochlorite cleaners can resultin rapid fading. Also, there can be a rapid lossof definition of both pencil and spirit pen marksif an abrasive cleaner is used. Thus, unless themarks are checked at regular intervals and re-newed as necessary, the methods are perhapssuitable only for the identification of denturesbelonging to patients admitted to hospital for ashort stay.
Inclusion markers
Names can be written or typed on metallicmarkers, such as the stainless steel strip of theSwedish ID-band, which has become an in-ternational standard and FDI-accepted denturemarking system (Thomas et al. 1995). Alter-native non-metallic materials that have beenused include tissue paper and ceramic materi-als. More recently, embedded radio frequencyidentification microchips have been described(Richmond & Pretty 2009).
Inclusion markers can either incorporatedinto a denture at the time of processing (Fig.13.7) or inserted into the processed denture bycutting a recess, inserting the marker and cov-ering with clear cold-curing acrylic resin. They
Figure 13.7 Inclusion marker inserted into lingualsurface at time of processing.
should be placed posteriorly in the lingual orpalatal areas of the dentures. In this position,the stresses induced by the markers are unlikelyto cause significant weakening of the dentures.Furthermore, the markers are less likely to bedestroyed in the event of the patient’s death byburning.
If identification marks of the inclusion typeare required, the appropriate request must bemade to the technician when the trial denturesare sent for processing.
Communication with the dentaltechnicianThe following topics might need to be includedin the clinician’s prescription to the laboratory:
� Confirmation that all items sent from theclinic to the laboratory have been disin-fected.
� It must be made quite clear whether the den-tures are to be processed, modified and thenprocessed or modified and returned to theclinician for a further trial stage. If there areany lingering doubts, or there has been sig-nificant adjustment to the occlusion or theposition of the teeth, a further trial stage isrecommended. It is better to be safe than tobe sorry.

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
Try-in Procedures 201
� If the original recording of the jaw relation-ship was wrong, it will be necessary for thetechnician to re-articulate one or both castsand to reset a number of teeth. Very clearinstructions must be given on the necessaryprocedures. A retry will be required.
� The use of the split-cast technique (p. 205) tocorrect any errors in occlusion resulting fromprocessing.
� The elimination of unwanted undercuts, orthe addition of a palatal relief when indi-cated, if instructions regarding these havenot yet been given. (The post-dam should al-ready have been carved into the cast wherenecessary by the clinician, p. 153.)
� Any special finish, such as stippling, to beapplied to the surface of the labial flanges,if this has not already been produced on thewax-work of the trial denture.
� The shade of acrylic resin to be used if thestandard shade would be unsightly. The pro-vision of a diagram of any stains to be incor-porated into the pink resin to simulate areasof melanotic pigmentation if this is required.
� The provision of some form of identificationmarker to be incorporated into the denturesshould be considered.
Quality control andenhancementAt the conclusion of the try-in stage, and beforethe dentures are returned to the dental techni-cian for processing, the clinician needs to havehad positive answers to the following:
� Are the dentures retentive and stable?� Is the occlusion balanced?� Is there adequate freeway space?� Is the patient happy with the appearance?� Has the original treatment plan been ful-
filled with respect to the design of the den-tures?
Topics which might be investigated in an as-sessment of a series of patients include the fol-lowing:
� In how many cases was the dental techni-cian provided with appropriate informationat the conclusion of the trial stage?
� In what proportion of cases was a secondtry-in procedure required? What were thereasons for this? Could the number of theseoccasions have been reduced?
References and additionalreadingBengtsson, A., Olsson, T., Rene, N., Carllson, G.E.,
Dahlbom, U. & Borrman, H. (1996) Frequency ofedentulism and identification marking of remov-able dentures in long-term units. Journal of Oral Re-habilitation, 23, 520–3.
Borrman, H.I., DiZinno, J.A., Wasen, J. & Rene, N.(1999) On denture marking. Journal of ForensicOdonto-Stomatology, 17, 20–6.
Deb, A.K. & Heath, M.R. (1979) Marking dentures ingeriatric institutions – the relevance and appropri-ate methods. British Dental Journal, 146, 282–4.
De Van, M.M. (1957) The appearance phase of den-ture construction. Dental Clinics of North America, 1,255–68.
Engelmeyer, R.L. (1996) Complete denture aesthetics.Dental Clinics of North America, 40, 71–84.
Frush, J.P. & Fisher, R.D. (1958) Dynesthetic interpre-tation of dentogenic concept. Journal of ProstheticDentistry, 8, 558–81.
Harrison, A. (1986) A simple denture marking sys-tem. British Dental Journal, 160, 89–91.
Heath, J.R. (1987) Denture identification – a simpleapproach. Journal of Oral Rehabilitation, 14, 147–63.
Hyde, T.P., McCord, F., Macfarlane, T. & Smith, J.(1999) Gender aesthetics in the natural dentition.European Journal of Prosthodontics and RestorativeDentistry, 7, 27–30.
Lombardi, R.E. (1973) The principles of visual per-ception and their clinical application to dentureaesthetics. Journal of Prosthetic Dentistry, 29, 358–82.
Michaeli, L., Davis, D.M. & Foxton, R. (2007) Dentureloss: an 8-month study in a community dental set-ting. Gerodontology, 24, 117–20.

P1: JZP Trim: 246mm X 189mmc13 BLBK351-Basker January 18, 2011 13:17 Printer Name: Yet to Come
202 Prosthetic Treatment of the Edentulous Patient
Murray, C.A., Boyd, P.T., Young, B.C., Dhar, S., Dick-son, M. & Currie, J.N.W. (2007) A survey of dentureidentification marking within the United King-dom. British Dental Journal, 203, E24.
Oliver, B. (1989) A new inclusion denture markingsystem. Quintessence International, 20, 21–5.
Richmond, R. & Pretty, I.A. (2009) A range of post-mortem assault experiments conducted on a va-riety of denture labels used for the purpose ofidentification of edentulous individuals. Journal ofForensic Sciences, 54, 411–4.
Schwarz, W.D. (1963) Improving full denture ap-
pearance. Dental Practitioner and Dental Record, 8,319–27.
Stenberg, I. & Borrman, H.I. (1998) Dental conditionand identification marking of dentures in homesfor the elderly in Goteborg, Sweden. Journal ofForensic Odonto-Stomatology, 16, 35–7.
Thomas, C.J., Mori, T., Miyakawa, O. & Chung, H.G.(1995) In search of a suitable denture marker. Jour-nal of Forensic Odonto-Stomatology, 13, 9–13.
Wright, S.M. (1974) Prosthetic reproduction of gin-gival pigmentation. British Dental Journal, 136,367–72.

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
14Fitting Complete Dentures
Objectives of this clinical stageThe overall objective when fitting completedentures is to ensure that the patient is giventhe best possible start with the new prostheses.This may be achieved by checking that:
� there is no pain when the dentures are in-serted and removed from the mouth, orwhen the teeth are brought into occlusal con-tact;
� the teeth meet evenly;� the dentures stay in place when inserted and
during normal opening of the mouth;� the patient understands:
◦ how to control the dentures;◦ what to expect of them;◦ how to clean them.
As a result of this preparation the patientshould be reasonably confident when meetingfamily and friends. It should be rememberedthat to achieve this satisfactory outcome with apatient who has not worn dentures previouslywill require very careful advice and instructionby the clinician.
The main changes in the dentures since thetry-in stage are in the impression and occlusalsurfaces. This chapter will focus on the assess-ment and correction of these two surfaces.
Assessment and correction ofthe impression surfaceBefore inserting the new dentures for the firsttime, the impression surface must be carefullychecked for any potential causes of pain. Iffound these must be eliminated to ensure pa-tient comfort and also to avoid the adoptionof abnormal paths of closure of the mandible,which may be followed to avoid occlusal pres-sure at the site of discomfort.
The common causes of pain arising from theimpression surface of a denture are shown inFig. 14.1:
� Acrylic nodules and spicules. These are pro-duced by acrylic resin being processed intoindentations or porosity in the cast. These ar-eas of roughness can be detected by obser-vation of the dried denture surface and by
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
203

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
204 Prosthetic Treatment of the Edentulous Patient
3
2
1
1
Figure 14.1 Common causes of pain arising fromthe impression surface of a denture are indicated bynumbers (1) surface roughness associated with sharpprojections and acrylic nodules; (2) sharp edge of re-lief chamber; (3) overextension into bony undercuts.
passing a gauze napkin or cotton wool rollover the surface so that the threads catch onthe offending areas. They should be carefullyremoved with a stone without modifying thefit of the denture.
� Sharp acrylic margins. Sharp edges can becaused by the presence of a tin-foil relief onthe cast and can be identified by direct ob-servation. Bevelling of these edges should becarried out.
� An undercut flange. A good indication ofwhether or not an undercut flange is likelyto cause pain or mucosal injury can oftenbe obtained by a careful visual inspection ofthe impression surface. A disclosing mate-rial, such as soft wax or silicone rubber, canthen be used to locate the offending area pre-cisely. A thin, even layer of the disclosingmaterial is applied to the suspect area andthe denture is gently inserted until the pa-tient just begins to experience slight discom-fort, and is then removed. The location of theundercut producing the discomfort is shownup as an area of acrylic from which the dis-closing material has been displaced.
Retention and stabilityThe retention and stability of new denturesshould be carefully evaluated at the fit stage.This may be achieved as follows.
Retention
The dentures are inserted and, after a short in-terval during which the denture becomes en-veloped by a saliva film, they should normallystay in place during moderate opening of themouth. The upper denture should offer resis-tance when pulled downwards by finger andthumb gripping the incisors. The lower den-ture, however, will not normally offer signifi-cant resistance to attempted displacement be-cause it has a relatively inefficient border seal.
Stability
Neither denture should rock when finger pres-sure is applied alternately to either side of theocclusal surfaces in the first molar region. Hori-zontal displacement should not result in a shiftof the centre line of more than 2 mm.
Further discussion of retention and stabilitycan be found in Chapters 4 and 13.
Assessment of the occlusalsurfaceThe occlusion of the dentures is checkedonce completion of the adjustments mentionedabove have ensured that:
� each denture can be inserted and removedfrom the mouth without discomfort;
� firm pressure can be applied to the occlusalsurface without eliciting pain.
Before discussing the methods of occlusal ad-justment the possible causes of occlusal errorarising from the laboratory processing of thedentures will be considered.

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
Fitting Complete Dentures 205
1
2
3 4
2
Figure 14.2 Laboratory causesof occlusal error (for a descriptionof the causes, see the text).
Laboratory occlusal errors
Causes of errors
Poor laboratory technique (Fig. 14.2) can resultin the movement of individual teeth or in anincrease in occlusal vertical dimension of thedenture.
(1) Excessive packing pressures resulting in theartificial teeth being forced into the invest-ing plaster. This can occur:� If the acrylic resin has reached an ad-
vanced dough stage and thus offers in-creased resistance to closure of the flask.Excessive pressure will then be neededto bring the two halves of the flasktogether.
� If the two halves of the flask are closedtoo quickly, resulting in a rapid build-upof pressure in the flask.
(2) Normal packing pressures breaking the in-vesting plaster and causing movement ofthe teeth when the layer of investing plas-ter is weakened as a result of:� porosity in the mix;� the use of an incorrect powder–water
ratio;� an inadequate thickness of plaster be-
tween the walls of the flask and thedenture.
(3) If pressure on the flask is released duringthe curing cycle, the two halves are likely toseparate, thus increasing the occlusal verti-cal dimension of the completed denture.
(4) Separation of the two halves of the flask bya layer of excess resin which should havebeen removed during trial closure of theflask. This ‘flash’ results in an increased oc-clusal vertical dimension of the denture.
In spite of taking all due precautions to preventthe errors just described, small occlusal inaccu-racies invariably occur. It has been shown that aprocessed denture exhibits an average increasein height of 0.5 mm and a shift in tooth con-tact towards the posterior region. These errorscan be corrected in the laboratory if a split-castmounting technique is used.
Correction of errors
Laboratory occlusal errors can be effectivelycorrected by using the split-cast technique.This technique involves replacing the processeddentures, still on their casts, back on to the ar-ticulator in exactly the same jaw relationship aswhen the trial dentures were produced (Figs.14.3–14.5). Any deflective occlusal contacts re-sulting from displacement of individual teeth

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
206 Prosthetic Treatment of the Edentulous Patient
Figure 14.3 Split-cast mountingtechnique (1). The trial dentureshad been mounted on an averagemovement articulator. Before themaster casts were plastered tothe articulator, location grooveswere cut into each cast. A filmof petroleum jelly was applied tothe location grooves and to theperipheral areas of each cast; as aresult, the master casts were readilydetached from the topping plasterbefore processing.
can then readily be seen. An overall increase inocclusal vertical dimension will be indicated bythe incisal pin failing to make contact with theincisal table.
There is evidence to show that if completedentures are processed by injection mouldingrather than the more common compression-moulding technique there is significantly lessincisal pin opening and generally fewer oc-clusal inaccuracies (Nogueira et al. 1999).
Figure 14.4 Split-cast mounting technique (2). Inthe laboratory, the denture, still seated on the cast, hasbeen removed from the investing plaster after process-ing. It can now be relocated onto the topping plastervia the locating grooves.
Clinical occlusal errors
If all appropriate precautions have been takenwhile processing the dentures, any remainingocclusal errors detected when the dentures areplaced in the mouth are likely to be primarily ofclinical origin and to have passed undetected atthe trial stage.
The objectives of adjusting the occlusion onthe finished dentures are to achieve:
Figure 14.5 Split-cast mounting technique (3). Inthe laboratory, the master casts, on which the den-tures are still seated, have been accurately relocatedon the topping plaster and secured with sticky wax.The occlusion can now be refined.

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
Fitting Complete Dentures 207
� occlusal balance in the intercuspal position;� a balanced articulation.
Occlusal errors can be identified and subse-quently corrected by occlusal adjustment withor without remounting the dentures on anarticulator.
Occlusal adjustment withoutremounting the dentures onan articulator
In general, small occlusal discrepancies in theabsence of a horizontal slide can be correctedeffectively by chair side adjustment following athorough intra-oral assessment using the meth-ods described in the following.
Identification of occlusal errors(i) Visual assessment. Visual assessment of oc-
clusal contact relationships of the denturesby the clinician can be an effective wayof recognising obvious deflective occlusalcontacts and slides which occur after theinitial contact. It is essential that the clin-ician bases an assessment of the occlu-sion on the initial contact of the denturesrather than on the final occlusal relation-ship, as the latter can be the product of thedentures tipping and of mucosal displace-ment.
(ii) Feedback from mucosal mechanoreceptors. Ausually reliable guide to identifying oc-clusal imbalance in dentures is the pa-tient’s sensory nervous system, as themechanoreceptors in the oral mucosa arecapable of fine pressure discrimination.They are generally able to detect the pres-ence of a deflective occlusal contact, butmay not precisely identify the specific sitethat should be adjusted. This will usuallyrequire the use of articulating paper.
(iii) Articulating paper. When searching for de-flective contacts with articulating paper,using the technique described in the nextsection, it should be remembered that ar-
ticulating paper marks can be very mis-leading. False marks can readily be createdbecause of the following reasons:� Even thin articulating paper may fill the
space between non-occluding teeth andmark areas of the occlusal surfaces thatare not actually contacting.
� Mucosal displacement and tipping ofthe dentures can bring non-occludingteeth into contact with the articulatingpaper.
� The vertical overlap of teeth associ-ated with cusp/fossa relationships andvertical overlap of anterior teeth can‘crimp’ the articulating paper and pro-duce false marks (Fig. 14.6).
Correction of occlusal errorsThis may be undertaken as a two-stage process:
(i) Produce a balanced occlusion in the muscularposition.� When the dentures have been made
comfortable, the patient is encouragedto relax and is then instructed to openand close without making occlusal con-tact. In this way, the pattern of jawmovement is largely determined by sen-sory input from the temporomandibu-lar joint receptors and from the musclespindles in the muscles of mastication.
� Sensory input from the mechanorecep-tors in the denture-bearing mucosa isthen introduced by asking the patientto continue opening and closing in a re-laxed manner but to make initial, lightcontact on the teeth and to report onthe location of that contact. It is essen-tial that the patient refrains from heavycontact; this ensures that the joint sen-sory input prevails and thus preventsalteration to the path of closure of themandible. In addition, it should be re-membered that heavy contact is likely tocompress the underlying mucosa, or tip

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
208 Prosthetic Treatment of the Edentulous Patient
Articulatingpaper
a b
Figure 14.6 Articulating papercan mark the teeth that are notin contact when it is ‘crimped’by a deep vertical overlap or byposterior teeth with cusps.
the dentures, and so mask the presenceof the deflective contact.
The majority of patients are able to of-fer such comments as ‘The dentures aremeeting on the left side first of all’, or ‘Iam meeting on the back teeth only’. Thisdiscrimination comes from stimulationof the mechanoreceptors in the denture-bearing mucosa. It is the clinician’s taskto interpret this evidence, and with theassistance of additional tests eliminatethe deflective contacts.
� A piece of thin horseshoe-shaped artic-ulating paper is inserted between theteeth and the patient is asked to repeatthe jaw movements. A single strip of ar-ticulating paper should not be placed ononly one side of the dental arch as thisis likely to induce jaw movement to thatside.
� Instructing the patient how to occludeonto the articulating paper needs to becarried out with care. The request to‘bite together’ is not advisable as it en-courages protrusion of the mandible to-wards an edge-to-edge incisal relation-
ship and consequently an incorrect re-sult. On the other hand, ‘close on yourback teeth’ will encourage a normal clo-sure pattern. Once the desired positionhas been obtained the patient is re-quested to tap the teeth together severaltimes in that position in order to markthe occlusal surfaces.
� Adjustment of the occlusal surfacesshould be made only on those markingsmade by the articulating paper whichcoincide with the patient’s comments.The process is repeated until the patientreports that the teeth meet evenly.
(ii) Produce a balanced articulation. Having es-tablished a balanced occlusion in the mus-cular position, the clinician should nor-mally check that there is an area of bal-anced articulation 1–2 mm around this po-sition. Articulating paper is again used tomark interfering contacts requiring adjust-ment. With a horseshoe of articulating pa-per between the teeth the patient closesinto intercuspal position and then slidesthe mandible into the lateral or protrusiveposition being assessed.

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
Fitting Complete Dentures 209
a
b c
d
Buccal Lingual
Supporting cusps
B L
B L B L
Figure 14.7 (a) Contact be-tween supporting cusps maintainsthe occlusal vertical dimension andocclusal balance in tooth position.(b) Deflective contact betweenbuccal cusps on the working sidein lateral occlusion is corrected bygrinding the buccal upper cusp.(c) Deflective contact betweenlingual cusps on the working sidein lateral occlusion is corrected bygrinding the lingual lower cusps. (d)Deflective contact on the balancingside is corrected by reducing theinterfering contact on one or otherof the supporting cusps.
The occlusal vertical dimension and oc-clusal balance in intercuspal and muscu-lar position normally depend on contactbetween the palatal upper cusps and thebuccal lower cusps of the posterior teeth(Fig. 14.7a). These cusps are thereforeknown as supporting cusps.
Having established even occlusal contactin muscular position, further adjustment ofthese supporting cusps should be avoidedwherever possible. Thus, if, in a lateral oc-clusal position, a deflective contact is de-tected on the working side between a buc-cal upper and buccal lower cusp, it is thebuccal upper cusp (BU) that should be re-duced. Similarly, if interference is observed
on the working side in lateral occlusion be-tween a palatal upper and lingual lowercusp, it is the lingual lower cusp (LL) thatshould be reduced (Figs. 14.7b and 14.7c).This approach to correcting the occlusionon the working side is known as the BULLrule.
However, this rule cannot be applied tothe correction of deflective contacts on thebalancing side, because here both upperand lower supporting cusps are in opposi-tion (Fig. 14.7d). It is usually possible in thissituation to reduce the interfering contactwithout eliminating the supporting con-tact. If this is not possible, it is necessaryto adjust one of the offending cusps and to

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
210 Prosthetic Treatment of the Edentulous Patient
accept loss of supporting contact in thisarea. Overall balance in muscular positionwill not be lost as a result.
Occlusal adjustment with remountingof the dentures on an articulator – thecheck record
Adjusting an occlusal discrepancy that is largeenough to be visible clinically can be a time-consuming and rather inaccurate exercise if at-tempted in the manner just described. This isespecially so if the error produces an antero-posterior or lateral slide after the initial occlusalcontact. It is therefore recommended that thecheck record procedure, in which the denturesare remounted on an articulator, is used for any-thing other than relatively minor occlusal cor-rections. There is, in fact, evidence to suggestthat it is advantageous to undertake a checkrecord as a routine procedure on the groundsthat its use results in fewer post-insertion com-plaints of discomfort (Firtell et al. 1987).
When a satisfactory occlusion has beenachieved in this way it should be recognisedthat the situation does not remain stable indefi-nitely. Post-insertion changes in the masticatorysystem such as mucosal displacement, neu-romuscular adjustment, bone resorption andwear of the acrylic teeth tend to result in a grad-ual deterioration of the occlusion (see Chapter15). When such a deterioration is recognised arepeat check record is likely to be the most ef-fective way of correcting it, as long as the post-insertion change has not been so dramatic thatthere is gross occlusal wear and a significantloss in occlusal vertical dimension.
A laboratory check record will usually re-quire an additional appointment for the patientas it is unusual for the dental laboratory to beon the surgery premises. This inconvenienceacts as a disincentive to the use of the techniqueand is the reason why a chair side check recordwas devised. Stages of the check record proce-dure are illustrated in Fig. 14.8.
Both techniques are described below.
a
b
c
Figure 14.8 Stages of the check record proce-dure: (a) a recording of the jaw relationship with themandible in the retruded position and with the den-tures out of occlusion; (b) the dentures are articulated,the occlusal record removed, the incisal pin raised andocclusal contact made; (c) view of the dentures on thearticulator to show an occlusal error.

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
Fitting Complete Dentures 211
Recording the jaw relationshipAfter the denture bases have been made com-fortable, a recording is made of the jaw re-lationship with the mandible in the retrudedposition and with the dentures just out of occlu-sion. This procedure, described below, ensuresthat normal jaw closure and the relationship ofthe dentures to the supporting tissues are notinfluenced by uneven occlusal contact:
(i) A wax containing fine metal particles isuseful as a recording material. The soft-ened wax is placed on the posterior teethof one of the dentures, care being takento confine it to the occlusal surface. Ifan excessive amount of material is used,sensory nerve endings in the tongue andcheek mucosa are stimulated and the sen-sory input may influence jaw movementadversely.
(ii) After initial closure in the retruded po-sition, the dentures are removed and thewax is inspected to ensure that there hasbeen no penetration of the wax by the arti-ficial teeth.
(iii) Once an apparently satisfactory record hasbeen obtained the wax is chilled and thentrimmed using a sharp blade to minimisethe chance of distortion. Buccal excess isremoved because it obscures the contactrelationship of opposing teeth with thewax record, making a visual check on ac-curacy impossible.
(iv) Occlusal excess is removed until only theindentations made by the tips of the op-posing cusps are visible. This is neces-sary because deep occlusal indentationsincrease the likelihood of denture dis-placement and mandibular deviation.
(v) Once the excess wax has been removed, adefinitive intra-oral check on the accuracyof the record can be made.
(vi) Accuracy is crucial to the success of theprocedure and therefore it is a commonpractice to verify the accuracy of the all-
important record before committing one-self to the occlusal adjustment. This in-volves obtaining more than one record andthen only proceeding with mounting thedentures on an articulator and their sub-sequent occlusal correction if the recordsagree.
If the dentures are mounted on an average-movement articulator without using a face bow,the relationship of the upper denture to thearticulator’s hinge axis conforms to the aver-age value for the relationship of the maxillato the condylar axis. However, if the clinicianwishes to record this latter relationship moreaccurately for a particular patient a facebowrecord is obtained and used to mount the upperdenture on the articulator; this is commonly un-dertaken on a semi-adjustable articulator, butcan be done equally effectively on those aver-age movement articulators able to accept a facebow.
Articulating the denturesThe task of mounting the dentures on an articu-lator is conventionally carried out by the dentaltechnician using routine laboratory procedures.However, the time required to mount the den-tures on the articulator may act as a disincen-tive to the use of the check record procedure,particularly if there is no dental technician onthe premises. The process can be speeded upconsiderably if the laboratory is requested to re-turn the finished dentures with the upper den-ture already on a plaster-holding cast on the ar-ticulator. It is then a quick and simple matter forthe clinician to mount the lower denture againstthe upper when the check record has been ob-tained. Of course, this variation is possible onlyat the stage of fitting the dentures. If the checkrecord is to be undertaken at a later visit, whenthe articulator is no longer available, one of theother techniques will have to be used.
The time required for the laboratory re-mounting of the dentures on an articulatorcan be reduced to about 10 minutes by using

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
212 Prosthetic Treatment of the Edentulous Patient
a
b
Figure 14.9 (a) Acrylic mounting platforms at-tached to an average-movement articulator to allowa rapid check record procedure at the chairside. (b)The jaw relationship having been recorded, the den-tures are fixed to the acrylic mounting platforms withimpression plaster. When the plaster has set the pro-cedure for adjusting the occlusion follows the stagesdescribed already.
an instrument which has special acrylic plat-forms fixed to the upper and lower arms.These platforms have small locating notches cutinto them and provide convenient tables ontowhich quick-setting impression plaster can bepoured (Oliver & Basker 1994). The stages ofthe mounting procedure are shown in Fig. 14.9.
Adjusting the occlusionBefore starting the occlusal adjustment, theinter-occlusal wax record is removed, the in-cisal pin raised and the articulator closed un-
til initial tooth contact is made. The occlusionis then adjusted until even occlusal contact isobtained.
If there is a gross error in the jaw relation-ship, it may be necessary to remove the arti-ficial teeth and set up new ones in the cor-rect position. In such a situation, the trial stageshould normally be repeated. When the jaw re-lationship is at last correct, the new teeth can beattached to the denture base with cold-curingacrylic resin.
Advice to the patientThe ultimate success of new dentures dependsto a large extent upon the quality of advice of-fered by the clinician. Sensible advice put overin a clear manner gives confidence to the newdenture wearer, ensures that the patient startsoff on the right footing and increases patientsatisfaction. It is often more effective to stressparticular points by the spoken rather than thewritten word. Thus, the clinician should spendtime in explaining the intricacies of denturewearing. This advice must be supplementedwith printed instructions, which will act as a re-minder for the patient.
With regard to advice on cleaning dentures,especially when given to older patients, verbalinformation alone is unlikely to result in anymore than a short-term improvement. Long-term change in behaviour is likely to occur onlyif verbal information is subsequently followedup by practice and reinforcement (Burnett et al.1993).
Although advice to the patient is consideredin this chapter on fitting dentures, it is impor-tant to explain the relevant points repeatedlyduring the earlier stages of treatment so thatonly reinforcement of this information is re-quired when the dentures are inserted. Infor-mation must be remembered and assimilated ifit is to be effective. If new dentures have justbeen placed in the mouth, the patient is won-dering how to control them, how to cope withthe new sensation and possibly what to do withthe sudden outpouring of saliva. The patient

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
Fitting Complete Dentures 213
is therefore too preoccupied to fully appreciatewhat is being explained by the clinician. Thisthought is even more relevant if the patient isolder and cannot readily assimilate new infor-mation. If, however, the basic information hasalready been given, repetition at the stage of fit-ting the dentures can help to reinforce the ear-lier message. For some older patients it maybe particularly helpful to give the advice to thecarer.
The advice given to the patient may be con-sidered under the following headings.
Limitations of dentures
When the patient was examined initially, anassessment of the prognosis for denture treat-ment should have been made. It is of the utmostimportance that if anatomical and, perhaps,adaptive problems indicate the possibility of fu-ture difficulties with dentures, the patient is in-formed of this at the outset. It is crucial thatrealistic expectations of dentures are created inthe patient before treatment is actually started.If the information is first given after the den-tures have been fitted and when complaintshave already been made, it is likely that the pa-tient will believe that the valid explanation is,in fact, an excuse for inadequate clinical work.
Controlling dentures
It should be explained to patients that oncethe dentures have been fitted, new muscularbehaviour must be developed in order tocontrol them. It is helpful to reassure patientsthat although it takes time the required skillsare usually acquired in due course and that it isimportant not to be discouraged by any earlydifficulties. It has been reported that althoughapproximately 60% of experienced denturewearers were able to eat and speak satisfacto-rily within a week of the replacement denturesbeing fitted, a further 20% of these patientsrequired up to 1 month to become proficient(Bergman & Carlsson 1972). A few patients takeeven longer.
The clinician can facilitate the learning pro-cess by giving appropriate advice. Simple tasksshould be mastered before advancing to morecomplex skills. Thus, the patient should be ad-vised to take small mouthfuls of non-stickyfood and to chew on both sides of the mouth atonce during the initial stages. Such well-knownphrases as ‘learn to walk before you run’ and‘practice makes perfect’ convey the sense ad-mirably. For first-time denture wearers and sig-nificantly older people, there may be benefit intheir being advised to commence with soft foodfor the first 2–3 days followed by the gradualintroduction of more challenging foods (Clearyet al. 1997).
Appearance
If the new dentures make an obvious changeto the appearance of the patient, as for exam-ple when restoring a loss of vertical dimension,it is very important to warn the patient in ad-vance that friends and relatives may look twiceand even pass a remark on a change in appear-ance. Unless this warning is given, there is arisk that the patient will interpret a chance re-mark or a second glance as realisation by thefriend that new dentures have been provided.Whereas most people are more than happy thatnew clothes or new hairstyles are admired, theymay be particularly sensitive to new denturesbeing recognised. As there is a danger that suchrecognition may bias the patient against thedentures, it is wise to remind him or her ofthe original aims of the treatment and that themuch-needed improvement in appearance maybe noticed. The patient should be encouraged toappreciate that friends and relatives, as well asthe patient, may require a period of adaptationto the new dentures.
Initial sensations
It is wise to reassure the patient regarding theimmediate changes that may be noticed whenthe dentures are inserted. For example, some

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
214 Prosthetic Treatment of the Edentulous Patient
inexperienced denture wearers salivate exces-sively and thus find it extremely difficult tospeak. Reassurance that this outpouring usu-ally settles down within several hours and thatthe strange sensations disappear within a fewdays helps to boost morale.
Soreness
In spite of all the care that is taken through-out all the stages of treatment, it is not unusualfor the patient to experience some soreness dur-ing the first few days of wearing new dentures.Helpful advice can be given as follows:
� If the discomfort is minimal and of short du-ration the patient should be advised that thedentures should continue to be worn andthat adjustments will be made at the recallvisit.
� If the discomfort is considerable and per-sistent the patient may need to discontinuewearing the new dentures and revert to theold ones before the recall appointment. It isimportant to make it clear to the patient thatif it is at all possible the new dentures shouldbe reinserted a few hours before the recallappointment so that the area of trauma canbe accurately pin-pointed and appropriatetreatment provided.
Wearing dentures at night
If new dentures are worn at night for at leastthe first two weeks after they have been fitted,the continuous stimulation of the mechanore-ceptors in the oral mucosa helps to speed upadaptation. After this initial period of adapta-tion has been successfully completed, the den-tures should ideally be left out at night becauseit has been shown that coverage of the denture-bearing mucosa day and night has the follow-ing significant disadvantages:
� Preventing cleaning of the mucosa by thetongue and saliva.
� Stimulating the growth of denture plaque.� Prolonging the exposure of the mucosa to
denture plaque.� Not accommodating an extended period of
immersion of the dentures in a cleanser.� Creating the possibility for parafunctional
clenching and grinding of the teeth duringsleep thus traumatising the denture-bearingmucosa.
If the dentures are not worn at night, the mu-cosa is allowed a rest period to recover fromthe day’s activity. This is especially relevant forthose patients with a thin atrophic mucosa andwith a reduced ability to repair tissue, featurescommonly found in the older patient. However,the clinician’s advice to leave the dentures outat night is frequently ignored because, as hasbeen said, ‘To leave the dentures in a glass inthe bathroom or at the bedside all night is anunattractive thought to most people, even ifthey sleep alone, or with partners whose capac-ity for simple domestic pleasures and skills hasfallen off’. Advice to take dentures out just be-fore sleep rather than leaving them out at nightis a subtle variation which can prove moreacceptable to some patients. Alternatively, ad-vice that the dentures are removed for a periodwhen patients are by themselves during the daymay be more acceptable.
Cleaning dentures – its importance
A variety of deposits form on dentures, such as:
� Microbial plaque� Calculus� Food debris
These deposits may be responsible for a num-ber of problems:
� Denture stomatitis (p. 111).� Angular stomatitis (p. 119).� Unpleasant tastes and odours.� Unsightly appearance because of staining.

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
Fitting Complete Dentures 215
� Accelerated deterioration of some denturematerials such as short-term and long-termsoft lining materials.
� Systemic disease and the infection of others,e.g. carers, by organisms such as methicillin-resistant Staphylococcus aureus (MRSA)(Glass et al. 2001). Fortunately immersiondenture cleansers have been shown to beeffective against MRSA (Lee et al. 2009;Maeda et al. 2007; Murakami et al. 2002).
The effective cleaning of dentures is therefore ofgreat importance to the patient’s general well-being and oral health and, potentially, also totheir carers or contacts.
The importance of giving advice onthe cleaning of dentures cannot be over-emphasised. Unfortunately, there is evidencethat a high proportion of patients appear notto have been given such instruction (Jagger &Harrison 1995).
Brushing will remove the majority of theplaque and will tend to disrupt the remainder,thus facilitating its subsequent penetration byan immersion cleanser. The objective of soakingdentures in an immersion cleanser is to removeany plaque left behind on the denture surface asa result of difficulty in brushing inaccessible ar-eas or because of a patient’s visual impairmentor lack of manual dexterity.
Brushing
When new dentures are fitted, the patientshould be advised to carefully brush them reg-ularly using soap, water and a soft nylon toothbrush the head of which is small enough toreach into all areas of the denture surface. Manycommercially available denture brushes haveheads which are too large to reach into all thenooks and crannies of the denture surface. Alsotheir bristles are often so stiff that they can-not conform satisfactorily to the contours of thedenture and can also cause significant abrasionof the acrylic resin.
Figure 14.10 Microbial plaque stained by disclos-ing solution applied to the impression surface.
Older patients with arthritic hands can findit difficult to hold and manipulate a conven-tional toothbrush. For such patients there arebrushes with handles designed for easy grip-ping or simple modifications that can be madeto the handle of a conventional toothbrush.
The importance of removing all deposits, notjust the more obvious stains and food parti-cles, should be emphasised. Disclosing solu-tions may be used by the patient at home toindicate when complete removal of dentureplaque has been achieved. Food dyes are suit-able for this purpose as long as their correct usehas been explained. If the clinician needs to re-inforce denture hygiene procedures and moti-vate the patient at a later stage, a commercialdisclosing agent may be used (Fig. 14.10).
Some patients prefer to brush their dentureswith a paste rather than with soap and wa-ter. Both conventional toothpastes and pastesdesigned specifically for dentures are used bypatients. The former have been shown to bemore abrasive for acrylic resin than the latter(Freitas-Pontes et al. 2009). Overzealous brush-ing of the denture with a stiff brush and anabrasive paste can cause marked abrasion of theacrylic resin, both of the denture base and ofthe teeth (Fig. 14.11). This can result in a sig-nificant deterioration in the appearance and fitof the dentures. Studies have shown that pastes

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
216 Prosthetic Treatment of the Edentulous Patient
Figure 14.11 Denture showing severe abrasion ofthe acrylic resin as a result of over-enthusiastic brush-ing.
containing dicalcium phosphate are less abra-sive than those containing calcium carbonate,but that the amount of wear that occurs evenwith the latter group of pastes is insignificantprovided that the brushing load is not excessive(Murray et al. 1986a,b).
Immersion
Patients should be advised to regularly sup-plement the careful brushing of their dentureswith periodic soaking in an immersion cleanser.Combining these two cleaning methods hasbeen shown to be a particularly effective strat-egy for denture plaque control (Paranhos et al.2007)
There has been some concern that immer-sion cleansers might damage materials used inthe construction or maintenance of dentures.Most of the adverse changes reported have oc-curred in soft linings or chair side relining ma-terials and usually take the form of increasedroughness and colour change (Benting et al.
2005; Handa et al. 2008; Haywood et al. 2003; Jinet al. 2003; Mese 2007). However, these changesare usually slight and are unlikely to be signifi-cant clinically.
It should also be remembered that if immer-sion cleansers are not used and the dentureplaque control is not therefore maintained at ahigh level, rapid degradation of soft linings canoccur as a result of microbial invasion of thematerial.
Types of cleanser
There are several different types of liquidcleansers into which a denture can be im-mersed:
� Bleaches – e.g. sodium hypochlorite.� Effervescent solutions – e.g. alkaline perox-
ides, perborates and persulphates.� Acid cleansers.
Hypochlorite cleansers
Although investigations into the relative effec-tiveness of the various denture cleansers for re-moving denture plaque have produced someconflicting results in the case of the effervescentcleansers, there is widespread agreement as tothe effectiveness of the hypochlorite prepara-tions (Lima et al. 2006). These cleansers arenot only effective disinfectants, but unlike someothers, good at removing non-viable organismsand other organic deposits from the denturesurface. They are not effective for the removalof calculus. Immersion of the dentures in ahypochlorite cleanser for periods in excess of6 hours will result in removal of plaque andheavy staining. Bleaching of the acrylic resinhas not been reported but corrosion of cobalt-chromium has been seen when hypochloritecleansers have been used. These cleansers maycause some loss of colour of acrylic and siliconesoft lining materials but neither softness norelasticity of the linings is affected significantly(Davenport et al. 1986). In addition, microbial

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
Fitting Complete Dentures 217
invasion, a common cause of soft lining fail-ure, is prevented. Some of the commonly usedshort-term soft lining materials are compatiblewith hypochlorite cleansers; in fact, the regularuse of such a cleanser can extend the useful lifeof a tissue conditioner from a few days to sev-eral months.
Effervescent cleansers
These may take the form of alkaline peroxides,perborates or persulphates. They are the mostwidely used type of immersion cleanser. Theircleaning action is largely due to the forma-tion of small bubbles which dislodge loosely at-tached material from the denture surface. Theyare not particularly effective cleansers and thereis evidence that their ability to remove micro-bial plaque is limited. They are safe, pleasantto use and do not damage acrylic resin or themetals used in denture construction. However,it has been demonstrated that they are capableof causing rapid deterioration of certain short-term soft lining materials (Harrison et al. 1989).Severe bleaching of acrylic resin resulting in awhite denture has been reported; however, thishas been shown to occur because the manufac-turer’s recommendations for use of the cleanserhave not been followed and excessively hot wa-ter has been added to the cleaning agent (Craw-ford et al. 1986; Robinson et al. 1987).
Acid cleansers
One type of acid cleanser contains sulphamicacid. Immersion in this solution helps to con-trol the formation of calculus on dentures. Thecompatibility of this agent with the commonlyused denture materials, including the metals,appears to be good.
Another type of acid cleanser contains 5%hydrochloric acid. This cleanser is applied tothe denture surface to wet the calculus andsoften it so that it can be removed by brush-ing. Care is necessary as damage to clothingcan result if the solution is spilled accidentally.
Corrosion of stainless steel or cobalt-chromiumpalates can occur if there is frequent and pro-longed contact with the acid.
Other denture cleaning methods
Enzymes
There are a number of commercial preparationsfor cleaning dentures that contain enzymes,but they have not been proven to be effective(Hashiguchi et al. 2009; Lima et al. 2006).
Ultrasonic cleansers
Ultrasonication has been found to be as effec-tive as immersion in denture cleansers for re-ducing the population of Candida albicans onacrylic resin plates in vitro (Arita et al. 2005;Hashiguchi et al. 2009).
Microwave exposure
This has been found to be effective whenused in conjunction with an immersion cleanser(Goodson et al. 2003). Even when used on itsown, microwave exposure is still likely to killmicroorganisms on the denture; however, itwill not remove the residual film of organicmatter.
Recall procedures
When the dentures are fitted, it should bestressed that a recall visit within the next fewdays is necessary. To help boost the patient’sconfidence, it is useful to make the points thatsmall problems may be experienced, that theseare part and parcel of the adaptation processand that where appropriate these will be dealtwith at the recall appointment.
To reduce the risk of mucosal damage andbone resorption, a check should be made everyyear. It is important that the patient is not un-der the mistaken belief that once the artificialsubstitute for the natural teeth has been pro-vided there will be no further problems, and

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
218 Prosthetic Treatment of the Edentulous Patient
no need for further maintenance. Treatment car-ried out at subsequent visits is discussed in thenext chapter.
Quality control andenhancement� At the stage of fitting the dentures keep
a record of the amount of occlusal adjust-ment that was found to be necessary and themethod used to make the adjustment.
The effectiveness of this stage of treatmentcan also be assessed at the first recall appoint-ment. The following topics might be part of aclinical audit undertaken on a series of patients.Patients can be asked at recall:
� ‘After the dentures had been fitted at the lastvisit, did you then find that you had worrieswhich had not been dealt with by the adviceand instructions given to you?’ ‘What werethose worries?’
� ‘Did you feel confident with your new den-tures when you left the surgery at the lastvisit?’ If the answer is negative, find outwhat the problem was.
References and additionalreadingAltman, M.D., Yost, K.G. & Pitts, G. (1979) A spec-
trofluorometric protein assay of plaque on den-tures and of denture cleaning efficiency. Journal ofProsthetic Dentistry, 42, 502–6.
Ambjornsen, E. & Rise, J. (1985) The effect of ver-bal information and demonstration on denture hy-giene in elderly people. Acta Odontologica Scandi-navica, 43, 19–24.
Arita, M., Nagayoshi, M., Fukuizumi, T., Okinaga, T.,Masumi, S., Morikawa, M., Kakinoki, Y. & Nishi-hara, T. (2005) Microbicidal efficacy of ozonatedwater against Candida albicans adhering to acrylicresin denture plates. Oral Microbiology & Immunol-ogy, 20, 206–10.
Benting, D., Pesun, I. & Hodges, J. (2005) Compli-ance of resilient denture liners immersed in effer-
vescent denture cleansers. Journal of Prosthodontics,14, 175–83.
Bergman, B. & Carlsson, G.E. (1972) Review of54 complete denture wearers. Patients’ opinions1 year after treatment. Acta Odontologica Scandinav-ica, 30, 399–414.
Budtz-Jørgensen, E. (1979) Materials and methods forcleaning dentures. Journal of Prosthetic Dentistry, 42,619–23.
Burnett, C.A., Calwell, E. & Clifford, T.J. (1993) Ef-fect of verbal and written education on denturewearing and cleansing habits. European Journal ofProsthodontics and Restorative Dentistry, 2, 79–83.
Cleary, T.J., Hutter, L., Blunt-Emerson, M. & Hutton,J.E. (1997) The effect of diet on the bearing mucosaduring adjustment to new complete dentures: a pi-lot study. Journal of Prosthetic Dentistry, 78, 479–85.
Crawford, C.A., Lloyd, C.M., Newton, J.P. & Yemm,R. (1986) Denture bleaching: a laboratory simu-lation of patients’ cleaning procedures. Journal ofDentistry, 14, 258–61.
Davenport, J.C. (1972) The denture surface. BritishDental Journal, 133, 101–5.
Davenport, J.C., Wilson, H.J. & Basker, R.M. (1978)The compatibility of tissue conditioners with den-ture cleaners and chlorhexidine. Journal of Den-tistry, 6, 239–46.
Davenport, J.C., Wilson, H.J. & Spence, D. (1986) Thecompatibility of soft lining materials and denturecleansers. British Dental Journal, 161, 13–17.
Firtell, D.N., Finzen, F.C. & Holmes, J.B. (1987) The ef-fect of clinical remount procedures on the comfortand success of complete dentures. Journal of Pros-thetic Dentistry, 57, 53–7.
Freitas-Pontes, K., Silva-Lovato, C. & Paranhos, H.(2009) Mass loss of four commercially availableheat-polymerised acrylic resins after toothbrush-ing with three different dentifrices. Journal of Ap-plied Oral Science, 17, 116–21.
Glass, R., Goodson, L., Bullard, J. & Conrad, R. (2001)Comparison of the effectiveness of several denturesanitizing systems. Compendium of Continuing Edu-cation in Dentistry, 22, 1093–6.
Goodson, L, Glass, R., Bullard, J. & Conrad, R. (2003)A statistical comparison of denture sanitation us-ing a commercially available denture cleanser withand without microwaving. General Dentistry, 51,148–51.
Guckes, A.D., Smith, D.E. & Swoope, C.C. (1978)Counselling and related factors influencing sat-isfaction with dentures. Journal of Prosthetic Den-tistry, 39, 259–67.

P1: JZP Trim: 246mm X 189mmc14 BLBK351-Basker January 4, 2011 8:1 Printer Name: Yet to Come
Fitting Complete Dentures 219
Handa, R., Jagger, D. & Vowles, R. (2008) Denturecleansers, soft lining materials and water temper-ature: what is the effect? Primary Dental Care, 15,53–8.
Harrison, A., Basker, R.M. & Smith, I. (1989) Thecompatibility of temporary soft materials with im-mersion denture cleansers. International Journal ofProsthodontics, 2, 254–8.
Hashiguchi, M., Nishi, Y., Kanie, T., Ban, S. & Na-gaoka, E. (2009) Bactericidal efficacy of glycine-type amphoteric surfactant as a denture cleanserand its influence on properties of denture baseresins. Dental Materials Journal, 28, 307–14.
Haywood, J., Wood, D., Gilchrist, A., Basker, R. &Watson, C. (2003) A comparison of three hardchairside denture reline materials. Part II. Changesin colour and hardness following immersion inthree commonly used denture cleansers. EuropeanJournal of Prosthodontics and restorative Dentistry, 11,165–9.
Hutchins, D.W. & Parker, W.A. (1973) A clinical eval-uation of the ability of denture cleaning solutionsto remove dental plaque from prosthetic devices.New York State Dental Journal, 39, 363–7.
Jagger, D.C. & Harrison, A. (1995) Denture cleans-ing – the best approach. British Dental Journal, 178,413–17.
Jin, C., Nikawa, H., Makihira, S., Hamada, T., Fu-rukawa, M. & Murata, H. (2003). Changes in sur-face roughness and color stability of soft denturelining materials caused by denture cleansers. Jour-nal of Oral Rehabilitation, 30, 125–30.
Lee, D., Howlett, J., Pratten, J., Mordan, N., McDon-ald, A., Wilson, M. & Ready, D. (2009) Susceptibil-ity of MRSA biofilms to denture-cleansing agents.FEMS Microbiology Letters, 291, 241–6.
Lima, E., Moura, J., Del Bel Cury, A., Garcia, R. &Cury, J. (2006) Effect of enzymatic and NaOCltreatments on acrylic roughness and on biofilmaccumulation. Journal of Oral Rehabilitation, 33,356–62.
Maeda, Y., Kenny, F., Coulter, W., Loughrey, A.,Nagano, Y., Goldsmith, C., Millar, B., Dooley, J.,James, S., Lowery, C., Rooney, P., Matsuda, M. &Moore, J. (2007) Bactericidal activity of denture-cleaning formulations against planktonic healthcare–associated and community-associated methi-cillin resistant Staphylococcus aureus. American Jour-nal of Infection Control, 35, 619–22.
Mese, A. (2007) Effect of denture cleansers on thehardness of heat- or auto-cured acrylic- or silicone-based soft denture liners. American Journal of Den-tistry, 20, 411–5.
Murakami, H., Mizuguchi, M., Hattori, M., Ito, Y.,Kawai, T. & Hasegawa, J. (2002) Effect of denturecleanser using ozone against methicillin resistantStaphylococcus aureus and E coli T1 phage. DentalMaterials Journal, 21, 53–60.
Murray, I.D., McCabe, J.F. & Storer, R. (1986a) Abra-sivity of denture cleaning pastes in vitro and insitu. British Dental Journal, 161, 137–41.
Murray, I.D., McCabe, J.F. & Storer, R. (1986b) Therelationship between the abrasivity and clean-ing power of the dentifrice-type denture cleaners.British Dental Journal, 161, 205–8.
Nogueira, S.S., Ogle, R.E. & Davis, E.L. (1999)Comparison of accuracy between compression-and injection-molded complete dentures. Journal ofProsthetic Dentistry, 82, 291–300.
Oliver, O. & Basker, R.M. (1994) Check records – achairside mounting procedure. Quintessence Inter-national, 25, 763–6.
Paranhos, H., Silva-Lovato, C., Souza, R., Cruz, P.,Freitas, K. & Peracini, A. (2007) Effect of me-chanical and chemical methods on denture biofilmaccumulation. Journal of Oral Rehabilitation, 34,606–12.
Robinson, J.G., McCabe, J.F. & Storer, R. (1987) Den-ture bases: the effects of various treatments on clar-ity, strength and structure. Journal of Dentistry, 15,159–65.

P1: JZP Trim: 246mm X 189mmc15 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
15Recall Procedures
In this chapter, we stress the importance ofplanning a programme of recall appointmentsafter fitting complete dentures, to ensure thatthe tissues are not being damaged and that thedentures are functioning efficiently and com-fortably. A recall visit also gives the patient anopportunity to seek advice over any concerns.
Short-term and long-term recalls are consid-ered separately.
Short-term recallThe first recall appointment should be nolonger than 1 week after fitting the dentures. Atthis visit it is necessary to obtain a careful his-tory of any complaint, such as pain or loosenessof the dentures, and to undertake a thoroughexamination.
The patient’s complaints
The clinician should routinely enquire aboutthe patient’s progress during the first weekof denture wearing. This is important becausethe more timid patient may need positive en-
couragement before being willing to commentabout a matter of concern. Of course, there areother patients who require no such invitationand will have already composed a list of diffi-culties. However, even then the routine enquiryabout progress is likely to be welcomed as anexample of a caring ‘after-sales service’.
Whatever the type of patient response, ad-vice and explanation by the clinician may beall that are needed to overcome certain dentureproblems, particularly if the patient is an inex-perienced denture wearer. Other problems willrequire intervention to modify the dentures.
Problems with the dentures may be causedby faults that passed unnoticed at the fit stage,or by changes occurring in the mouth since thattime. There can also be persistent difficultiescaused by insurmountable hurdles related tounfavourable anatomy, unrealistically high pa-tient expectations, or lack of adequate denturecontrol skills.
The more common complaints are:
� Discomfort� Looseness
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
220

P1: JZP Trim: 246mm X 189mmc15 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Recall Procedures 221
� Appearance� Speech
The first two problems occur most frequently.The last two are dealt with elsewhere in thebook.
Discomfort
Examples of injury to the mucosa which arisefrom faults on the impression surface includemucosal damage in the sulcus due to over-extension, and on the most bulbous part of aridge where the denture base has been inade-quately relieved from a bony undercut. Wherethere is a clear relationship between mucosaldamage and the impression surface, appropri-ate correction of the denture should be under-taken. It may be tempting to assume that allmucosal damage is directly related to faults inthe impression surface. However, such an as-sumption would be fraught with danger as thedamage could be equally due to faults in theocclusion causing movement of the denture orconcentrations of occlusal pressure. It is impor-tant to appreciate that the occlusal error causinga problem may be some distance from the siteof inflammation (Fig. 15.1). It is also importantto remember that when there is a complaint ofdiscomfort an assessment of the occlusion mustalways be made before any adjustment of theimpression surface is carried out.
a b
Figure 15.1 (a) A posterior pre-mature contact, resulting in forwardmovement of the lower denture (dot-ted arrow), produces inflammationof the mucosa on the lingual aspectof the alveolar ridge in the ante-rior region. (b) Lateral displacementof the lower denture produces in-flammation of the mucosa in areasclosely related to the occlusal error.
Looseness
Looseness of the dentures may occur becausethe patient has not, as yet, learned to controlthe new shapes in the mouth, rather than be-ing due to denture faults or anatomical short-comings. Thus, a check must be made on thepatient’s progress in adapting to the new den-tures. Bearing in mind that 20% of experienceddenture wearers require up to a month in whichto become proficient with their new dentures(Bergman & Carlsson 1972), it is likely that asignificant number of patients will benefit fromthe offer of further advice, reassurance andfollow-up.
Routine checks and treatment
Checks that should always be made at the re-call appointment when carrying out an exami-nation of the patient’s mouth and dentures are:
� Occlusion� Tissue health� Denture cleanliness
Occlusion
It must be remembered that because new den-tures are seated on a surface which is compress-ible and liable to change, the initial few days offunction may have caused an alteration in theocclusion. Such an alteration is a potent cause of

P1: JZP Trim: 246mm X 189mmc15 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
222 Prosthetic Treatment of the Edentulous Patient
mucosal injury, and it can also lead to problemswith the masticatory muscles. Patients attemptto adapt to an uneven occlusion by altering thenormal pattern of mandibular movement. Suchan attempt is liable to produce muscular disor-ders which, in the short term, may pass unno-ticed by the patient, but in the longer term cangive rise to significant discomfort. Methods ofcarrying out occlusal adjustment are describedin Chapter 14.
Tissue health
Even if the patient expresses complete satisfac-tion and reports perfect comfort, it is essentialto carry out a thorough examination to check ontissue health. This is because occasionally theremay be mucosal injury, even frank ulceration,without the patient apparently being aware ofit. The absence of a complaint under such cir-cumstances may be due to a high pain thresh-old or a desire to please. With the informationgleaned from the history and an examination, adiagnosis of any problem should be establishedand appropriate treatment decided upon.
The impression surface of the dentureshould never be adjusted in an empirical man-ner. Once any occlusal faults have been elimi-nated, a further check of the impression surfaceshould be made using a pressure-disclosingmedium. If this sequence is not carried out, it isdifficult to judge whether an area of inflamma-tion is due either to an impression surface de-fect or to an occlusal error. Pressure-disclosingmedia suitable for this purpose include siliconerubber materials formulated for the purpose,pressure-disclosing paste or wax and low vis-cosity alginate.
If the mucosal damage has been diagnosedas being due to a fault with the impression sur-face and is localised, a disclosing material is ap-plied to the impression surface of the denturein the suspect area. The denture is then seatedfirmly for a few seconds and on removal anypressure points are indicated by the pink den-ture base showing through the material. Ad-
justment of the impression surface can then becarried out in a relatively precise manner.
If the mucosal damage is more generalised,an alternative technique which is simple, quickand revealing is to obtain a wash impressionover the whole of the impression surface usinga low viscosity mix of alginate or silicone rub-ber. The set impression gives a clear picture ofpressure points and base extension. Any pres-sure points can be marked with a pencil be-fore the material is removed allowing their pre-cise correction. If adhesive has not been appliedto the denture beforehand, the impression canthen be quickly and cleanly removed from thedenture after the adjustments have been com-pleted.
Denture cleanliness
A check on denture plaque control can bemade by direct visual inspection assisted wherenecessary by the use of a disclosing solution.If there are significant deposits it is essentialto discover what cleaning technique the pa-tient is using. Reinforcement of advice at thisstage may prevent the development of denture-induced stomatitis, angular stomatitis, stain-ing of the dentures and mouth odour. If therehave been significant problems at the first re-call appointment, a further appointment forshort-term review should be made to check onprogress. The clinician can also ensure that anymodification to the dentures has been success-ful. The patient should be advised about the im-portance of a review in a year’s time for reasonsthat will become apparent in the next section ofthis chapter. Thereafter reviews at intervals of2–3 years will usually be appropriate.
Long-term recallAll the checks carried out for the short-termrecall should also be completed at long-termrecall appointments. However, the followingpoints will be discussed further.

P1: JZP Trim: 246mm X 189mmc15 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Recall Procedures 223
Mucosal changes
In Chapter 7 the need to carry out periodicchecks with respect to oral cancer was stressed(Craig & Johnson 2000; Conway et al. 2002).In 2007, in the UK, there were 5325 new casesand 1841 deaths, with an increased prevalencein deprived communities (Chadwick 2009). Itshould be emphasised that the typical eden-tulous patient falls into a risk group, as a ret-rospective study of patients with oral cancershowed that 59% were edentulous, tended tobe older than 60 years, were tobacco and al-cohol users, had a lower socioeconomic statusand had a somewhat negative attitude to re-call appointments (Guggenheimer & Hoffman1994; Craig & Johnson 2000).
Bone resorption
The long-term changes in shape of the residualridges and the consequent effect on dentureshave been studied extensively. A continuing re-duction in height of the alveolar ridges over aperiod of 25 years has been observed. There ap-pears to be a marked reduction in the first yearof denture wearing and in the next few yearsa continuing loss averaging 1 mm each year.Over periods of time, the loss in height of theanterior lower ridge is four times that of the up-per (Tallgren 1972; Douglass et al. 1993). As thelower denture covers a much smaller area, thefunctional stress transmitted to the underlyingtissues is greater than that to the upper tissues;thus, it is likely that the greater loss of mandi-bular bone is due to the physiological limit ofthis tissue being exceeded. The resorption ofbone brings in its wake a loss of both occlusalvertical dimension and rest vertical dimension.The former dimension is reduced to a greaterextent and thus the freeway space is increased.
Occlusal changes
The progressive loss of fit of dentures, result-ing from resorption of bone, also leads to de-
Wear ofocclusal surface
Loss of fitof denture
Mucosaltrauma
Loss ofocclusal balance
Resorptionof bone
Figure 15.2 Cycle of tissue damage resulting fromlack of denture maintenance.
terioration in occlusal balance. In the case ofdentures with acrylic teeth this occlusal dete-rioration can be aggravated by occlusal wear.The combination of loss of fit and occlusal im-balance encourages mucosal inflammation andfurther bone resorption, thus establishing a vi-cious cycle (Fig. 15.2). It is clearly important, iforal health and function are to be maintained,that this cycle is broken by regular denture re-view and effective maintenance.
Adaptation of the patient
The progressive long-term deterioration of den-tures that has been described is not invariablyassociated with a complaint. This is becauseadaptive changes can occur and a tolerance candevelop which allows patients to continuewearing the dentures. Thus, a considerableamount of tissue damage can go unnoticed.Whereas successful adaptation to new denturesis a prerequisite for success, a patient who toler-ates slowly developing faults beyond a certainpoint will store up troubles for the future. In ad-dition to the likelihood of tissue damage, reduc-tion in rest vertical dimension and the adoptionof abnormal mandibular postures create prob-lems for both the clinician and the patient whenreplacement dentures are eventually required(Chapter 8).

P1: JZP Trim: 246mm X 189mmc15 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
224 Prosthetic Treatment of the Edentulous Patient
Dental health surveys
Deterioration in both the dentures and thehealth of the mouth is the result of patients notseeking regular denture maintenance. The sizeof the problem has been highlighted by nationalsurveys of adult dental health which reportedthat, whereas 40% of complete denture wear-ers reported problems with eating, drinking,speaking and appearance, only 13% plannedto seek advice (Walker & Cooper 2000). It ap-pears that the longer patients have been eden-tulous the less inclined they are to seek treat-ment. In an earlier survey it was reported thata third of the edentulous population had hadtheir current dentures for over 20 years and aquarter of them had not visited a dental clin-ician for more than 20 years (Todd & Lader1991). Clearly, many patients do not have a real-istic perception of what is required to maintaintheir dentures and mouth in good condition.
Having made these comments, which almostsuggest a laissez-faire attitude amongst com-plete denture wearers, it is worth making thepoint that people who express satisfaction withold dentures, even though they are ill-fitting,can in fact appreciate the benefits of new den-tures. This is suggested by the fact that patientsreported that chewing with their new dentureswas more enjoyable than with their old onesand that they had discovered they had a greaterfood choice (Garrett et al. 1996).
Long-term recall schedule
The importance of the clinician convincing thepatient of the need to seek regular denturemaintenance is obvious in the light of this dis-cussion. It should be explained that the firstlong-term recall appointment should be madeno more than a year after the dentures werefirst fitted. Thereafter, an appointment every2 or 3 years to check on tissue health andquality of the dentures is a realistic arrange-ment, on the mutual understanding that thepatient will attend sooner if problems develop
in the meantime. The clinician should makethe point that the dentures have a limited lifeand should stress to the patient the potentialdangers of wearing dentures that have becomeinadequate.
At this stage it is worth sounding a warn-ing note. The clinician can be faced with adilemma if, at review, it is apparent that a den-ture fault has developed but there is no concernexpressed by the patient, nor any signs of tissuedamage. The clinician has to decide whether ornot to correct the deficiency. In the absence ofboth signs and symptoms, it will often be fool-hardy to tamper with well-accepted denturesjust because a minor shortcoming has devel-oped. Absence of current signs and symptomsis not the only consideration, however, as theclinician needs to consider whether the pres-ence of the problem, even though undetectedby the patient, is likely to give rise to significantdifficulties in the future.
Treatment required at long-term recall ap-pointments will be one, or a combination, of thefollowing:
� Adjustment of the impression surface� Correction of denture base extension� Occlusal adjustment with or without a check
record� Reline or rebase of the dentures� Construction of replacement dentures.
Relining and rebasing will now be consideredin more detail, and the other procedures in thelist having already been considered in previouschapters.
Clinical procedures for reliningor rebasing
Relining
In simple terms, a reline involves a straight-forward substitution of the layer of impres-sion material within the denture by a layer ofnew acrylic resin (Fig. 15.3a). Such a method is

P1: JZP Trim: 246mm X 189mmc15 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Recall Procedures 225
New acrylic resin
a
b
Figure 15.3 Cross section throughupper dentures that have been (a)relined and (b) rebased.
quite satisfactory for a lower denture but willincrease the thickness of the palate of an up-per denture, the degree of increase dependingupon the impression material used. The moreviscous zinc oxide-eugenol impression pastesare likely to produce an unacceptable thickness,while minimal change will occur with light-bodied silicone impression materials.
Rebasing
Rebasing entails the replacement of most ofthe original acrylic base of the denture withheat-curing acrylic resin (Fig. 15.3b). A rebas-ing technique does not suffer from the disad-vantage just mentioned and is thus preferredby many for correcting the impression surfaceof an upper denture. Certainly, a rebase shouldbe undertaken when the existing denture basematerial has deteriorated or when there is a his-tory of previous fractures of the palate. What-ever laboratory technique is requested, the ba-sic principles of the clinical method remain thesame.
Diagnosis and treatment planning
It is apparent that as the reline/rebase altersthe impression surface of a denture, it will beof benefit only when a patient’s complaint canbe attributed to a defect in that surface. Thecommon history a patient gives is one of re-cent looseness following a period of trouble-free denture wearing. If the complaint of loose-ness is the result of defects in the other surfaces,such as an unbalanced occlusion, it is quite use-less to reline/rebase the denture.
Preparatory procedures
Three routine preparatory procedures are car-ried out whatever reline/rebase technique isfollowed:
(i) The occlusion must be balanced to ensurethat, when the impression is taken, unevencontact does not bring about a bodily shiftor tilt of the denture when the patient isasked to occlude.
(ii) Any over- or under-extension of the bor-ders must be corrected.

P1: JZP Trim: 246mm X 189mmc15 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
226 Prosthetic Treatment of the Edentulous Patient
Figure 15.4 Escape routes for ex-cess impression material.
(iii) Undercuts within the impression surfaceof the denture must be eliminated so thatthe technician can remove the denturefrom the cast.
Impression procedures
When an impression is taken within an existingdenture, care must be taken to ensure that thejaw relationship in the horizontal plane is notaltered. This is achieved by taking great carein seating the denture and checking the accu-racy of this by getting the patient to occludein the intercuspal position. Inevitably, the oc-clusal vertical dimension is increased slightlyby the thickness of the impression material. Un-less there has been a corresponding reductionin occlusal vertical dimension during the lifeof the dentures this increase should be keptto a minimum. It is usual, therefore, to choosean impression material which can be reducedto a thin film as the denture is seated andis accurate in thin section. Low viscosity sil-icone elastomers and zinc oxide-eugenol im-pression pastes are good examples of materialsof this type. The more fluid silicone will pro-duce the least change in occlusal vertical di-mension. When an impression is taken withina lower denture, excess material in the middleof the impression surface has only a short dis-tance to travel before it escapes at the periph-ery. Thus, the force needed to extrude the ma-terial and seat the denture is small, and the riskof displacing the underlying tissues or of alter-ing the occlusal relationship is minimal. The sit-
uation is obviously somewhat different in theupper jaw as the excess material has a longerand more circuitous route to follow (Fig. 15.4).Greater force is therefore needed to seat theupper denture, bringing with it the potentialcomplication of undue displacement of the mu-cosa with consequent reduction in retention ofthe relined/rebased denture. Also, unless greatcare is taken, the denture may not be seated cor-rectly in the antero-posterior plane; too muchimpression material may be left under the labialflange resulting in the relined/rebased denturebeing positioned too far anteriorly. This bringswith it inevitable occlusal and aesthetic compli-cations. Creating a series of small perforationsin the palate of the denture will facilitate the es-cape of excess impression material and reducethe chance of the above problems occurring.
Intra-oral reline
It will be appreciated that the above proceduresrequire the patient to be without the denture fora period of time while the laboratory work isbeing completed. If this approach is unaccept-able for any reason it is possible to carry out areline as a one-stage chair side procedure. Thesematerials are discussed further in Chapter 16.
References and additionalreadingBergman, B. & Carlsson, G.E. (1972) Review of
54 complete denture wearers. Patients’ opinions1 year after treatment. Acta Odontologica Scandinav-ica, 30, 399–414.

P1: JZP Trim: 246mm X 189mmc15 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Recall Procedures 227
Bergman, B., Carlsson, G.E. & Ericson, S. (1971) Effectof differences in habitual use of complete dentureson underlying tissues. Scandinavian Journal of Den-tal Research, 79, 449–60.
Chadwick, B. (2009) Oral cancer annual evi-dence update. NHS Evidence – oral health NICE,www.evidence.nhs.uk
Conway, D.l, Macpherson, L.M.D., Gibson, J. & Bin-nie, V.I. (2002) Oral cancer: prevention and detec-tion in primary dental healthcare. Primary DentalCare, 9, 119–23.
Craig, G. & Johnson, N. (ed) (2000) Opportunisitic oralcancer screening – a management strategy for dentalpractice. British Dental Association, London.
Douglass, J.B., Meader, L., Kaplan, A. & Ellinger,C.W. (1993) Cephalometric evaluation of thechanges in patients wearing complete dentures.A 20-year study. Journal of Prosthetic Dentistry, 69,270–5.
Garrett, N.R., Kapur, K.K. & Perez, P. (1996) Effects ofimprovements of poorly fitting dentures and newdentures on patient satisfaction. Journal of ProstheticDentistry, 76, 403–13.
Guggenheimer, J. & Hoffman, R.D. (1994) The impor-tance of screening edentulous patients for oral can-cer. Journal of Prosthetic Dentistry, 72, 141–3.
Jackson, R.A. & Ralph, W.J. (1980) Continuingchanges in the contour of the maxillary resid-
ual alveolar ridge. Journal of Oral Rehabilitation, 7,245–8.
Shaffer, F.W. & Filler, W.H. (1971) Relining completedentures with minimum occlusal error. Journal ofProsthetic Dentistry, 25, 366–70.
Sheppard, I.M., Schwartz, L.R. & Sheppard, S.M.(1971) Oral status of edentulous and completedenture-wearing patients. Journal of the AmericanDental Association, 83, 614–20.
Sheppard, I.M., Schwartz, L.R. & Sheppard, S.M.(1972) Survey of the oral status of complete den-ture patients. Journal of Prosthetic Dentistry, 28,121–6.
Tallgren, A. (1972) The continuing reduction of theresidual alveolar ridges in complete denture wear-ers: a mixed-longitudinal study covering 25 years.Journal of Prosthetic Dentistry, 27, 120–32.
Todd, J.E. & Lader, D. (1991) Adult Dental Health 1988United Kingdom. HMSO, London.
Walker, A. & Cooper, I. (eds) (2000) Adult DentalHealth Survey – Oral Health in the United Kingdom1998. The Stationery Office, London.
Yusof, Z.Y., Netuveli, G., Ramli, A.S. & Sheiham, A.(2006) Is opportunistic oral cancer screening bydentists feasible? An analysis of the patterns ofdental attendance of a nationally representativesample over 10 years. Oral Health and PreventiveDentistry, 4, 165–71.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
16Some Clinical Problems and Solutions
The topics that will be covered in this chapterare:
� Pain and instability� Lack of saliva� Hard and soft materials for modifying the
impression surface of dentures� The flabby ridge� Denture breakages� Gagging� The burning mouth syndrome� Disturbance of speech
Pain and instabilityThe most common problems associated withcomplete dentures are pain and instability ofthe dentures (Lechner et al. 1995). Many of thecauses have been described in earlier chaptersbut to give a simplified picture they are sum-marised in Table 16.1. The most likely maincomplaints have been indicated in each case.However, it should be remembered that there isconsiderable overlap between the two columns,
as any cause of instability may additionallygive rise to a complaint of pain. It should also bestressed that there may be more than one causeof a complaint.
Persistent painThis problem is more often seen in the lowerjaw where the area available for distribution ofthe occlusal load is relatively small. As notedin Table 16.1, there are many possible causes ofthis complaint, which may be attributed to thedenture design and to the patient.
A diagnostic flow chart is shown in Fig. 16.1.The clinician may find it helpful to base the his-tory and examination on this chart in order toarrive at a diagnosis. An example of the diag-nostic process is presented in Table 16.2.
Discomfort can arise from overloading of themucosa as a result of clenching or grinding theteeth. These occlusal habits are caused by in-creased activity of the masticatory muscles pro-duced during stressful situations. Clues to sucha diagnosis come from the absence of errors in
Prosthetic Treatment of the Edentulous Patient, Fifth Edition, C© R.M. Basker, J.C. Davenport and J.M. ThomasonPublished 2011 by Blackwell Publishing Ltd.
228

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 229
CAUSE COMPLAINT
DENTURE FAULTSImpression surface
LPtfietaruccanILPnoisnetxe-revOLPnoisnetxe-rednULlaeslaicafrofetauqedanihtdiwegnalF
Post-dam absent LLPderiuqertubtnesbarebmahcfeileR
PssenhguoRPgnissecorperofebdegamadtsaCPstucrednuynobotninoisnetxE
Polished surfaceDenture not in neutral zone L
LlortnocelcsumrofelbaruovafnuepahSOcclusal surface
LPdecnalabnunoisulccOLPecnerefretnilapsuC
Occlusal plane too high LPecapsyaweerfetauqedanI
LPediwootelbatlasulccO
PATIENT FACTORSBruxism/parafunction PLow pain tolerance PPoor neuromuscular control
L)tneitapylredle.g.e(noitatpadafoetarwolSL)msinosnikraP.g.e(sredrosidralucsumorueN
MucosaFlabby L
PcihportABone
PselucipsprahSP)selcrebutlaineg,irot,segdirdioyholym(secnenimorP
Advanced resorption LPegdirfotsercraennemaroflatneMPenobehtnihtiwygolohtaP
SalivaLPtnesbarotneicfieD
Systemic diseasePaimeanaycneicfied-norI
Table 16.1 Summary of the causes of pain (P) and looseness (L)
denture design together with evidence of shinywear facets on the occlusal surface of the teeth.It is helpful to ask the patient, ‘When you arenot eating are your upper and lower teeth nor-
mally in contact or out of contact?’ It is not un-usual for such patients to reply that their teethare usually together and for them to assumethat this is quite normal.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
230 Prosthetic Treatment of the Edentulous Patient
Causes of pain beneath dentures(NB multiple aetiology possible)
Patient factors
Chemical irritation, e.g. raised residual
monomer
Generalisedpain
Overload of denture-bearing tissues
Localisedpain
Local factors, e.g. roots,
bony spicules,undercuts
Reducedtolerance
Reduceddenture-
bearing area
Function Parafunction
Design faults
Highocclusalforces
Denture factors
Polishedsurface
Occlusalsurface
Impressionsurface
Atrophic mucosa
Xerostomia
Low pain threshold
Psychogenic
Systemic factors
Figure 16.1 A diagnostic flow chart of the various possible causes of pain beneath dentures.
In treating parafunction, the patient must bemade aware of the problem and should be toldthat teeth should be out of contact for mostof the time. It is important to reassure the pa-tient, describe the link between stress, para-function and pain under dentures and point outthat there is no sinister change in the oral mu-cosa. The importance of conscious relaxationshould be emphasised and the patient should
be strongly encouraged to leave both dentures,or at least the lower denture, out at night.
Lack of salivaFunctions of saliva
Saliva possesses the following functions in theedentulous patient (Lewis, 2009):

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Table 16.2 The history taking and possible significance of the patientís answers are presented for an elderlyperson complaining of persistent pain in the lower denture-bearing area. The objective of the table is to stressthat (1) many denture problems are multifactorial; (2) a seemingly simple complaint may have widerramifications – especially with older patients; (3) a correct diagnosis is unlikely to be established unless aproperly structured history and examination are undertaken.
CLINICIAN’S QUESTIONS SUMMARY OF ANSWERS SIGNIFICANCE
COMPLAINT‘What’s your problem?’ ‘I can’t eat with my dentures’ A common answer reflecting a
common concern, but it tells uslittle.
‘Why do you have difficulty ineating?’
‘Because my lower gum hurts’ We now know that pain ratherthan instability of the denture is theproblem.
‘How long have you had theproblem?’
‘For about 1 year’
‘How long have you had this set ofdentures?’
‘For the same time’ This could suggest that a DENTUREFAULT is contributing to theproblem, or it could be acoincidence.
‘Where is the pain?’ ‘All round the lower gum’‘What’s the pain like?’ ‘A continuing soreness – severe at
times’‘How often do you get the pain?’ ‘All day, every day’‘Does anything make it better orworse?’
‘Worse after eating. Better if thelower denture is removed. I nowalways leave it out at night’
Answers to the last four questionspaint a picture of tissue overload.A DENTURE FAULT is onepossibility.
‘When you wore the lower dentureat night, how was the lower gumwhen you woke in the morning?’
ytilibissopehtstseggusgnimitehT’erosyreV‘of PARAFUNCTION.
‘When you are wearing thedentures (and not eating) are yourupper and lower teeth usuallyapart or together?’
‘Usually together’ Suggests LACK OF FREEWAYSPACE and/or PARAFUNCTION.
PAST DENTAL HISTORY‘How long have you been wearingcomplete dentures?’
‘About 10 years’
‘How many sets have you had inthat time?’
‘Three’
‘Tell me about them’ First set was fitted immediatelyafter the teeth were taken out. Oneyear later a further set made. Wornsuccessfully for eight years. Thirdset are the troublesome ones.
Suggests DENTURE FAULT with thelatest prostheses. But could be dueto deterioration of the supportingTISSUES.
It is important to examine thesuccessful dentures and comparethem with the most recent ones toclarify this.
(Continued)

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
232 Prosthetic Treatment of the Edentulous Patient
Table 16.2 (Continued)
CLINICIAN’S QUESTIONS SUMMARY OF ANSWERS SIGNIFICANCE
‘Why did you decide to seekreplacements for the successfulset?’
‘The teeth were worn down and myface was beginning to look old’.
There might have been anINCREASE IN OVD in thetroublesome dentures which cannotbe tolerated.
MEDICAL HISTORY
A full history is taken including aquestion on current medication.
‘For how long have you beentaking these tablets?’
‘I’m taking an anti-depressant anda diuretic’.
‘One year’
DRY MOUTH is a possiblecontributory factor to the oralcomplaint.
SOCIAL HISTORY
‘Why were you prescribed theanti-depressant tablets?’
‘Last year my wife was found tohave Alzheimer’s. I have had torearrange my life to look after her.I retired early’.
It is possible that worry and anxiety(and a degree of frustration) haveled to PARAFUNCTION.
Comment: The history has revealed a number of possible causes of the persistent pain. The diagnosis can be established only after acareful examination of the patient, the mouth and the various sets of dentures in order to confirm or eliminate the various possibilities. Thepoint should be made that unless a full history is obtained some of the possible causes might never be identified. The provision of newdentures would do little to resolve the problem if the persistent pain was due to a dry mouth and/or parafunction.
� Denture retention – saliva is an essential com-ponent in the physical retention of completedentures.
� Lubrication – the glycoproteins in saliva fa-cilitate movement of the soft tissues duringspeech, mastication and the swallowing offood.
� Cleansing – saliva physically washes foodand other debris from the soft tissues andfrom the polished surfaces of prostheses.
� Taste – flavours are perceived only whensubstances are in solution in saliva or otherfluids.
� Digestion – digestion begins during mastica-tion when salivary amylase starts to breakdown glucose.
� Antimicrobial – there are antimicrobial com-ponents, such as antibodies, in saliva whichhelp to maintain a normal balance of the oralflora.
Problems of reduced salivary flow
A reduction or absence of saliva, known as xe-rostomia, is responsible for a range of symp-toms resulting from an interference with someor all of the functions of saliva listed above.As a result, a general and significant reduc-tion in the quality of life can result. Reducedretention of dentures can be a particular prob-lem for edentulous patients. However, the lit-erature is inconclusive about whether or nottreating the hyposalivation has a beneficial ef-fect on denture retention (Turner et al. 2008).There may also be an increased susceptibil-ity to denture trauma resulting in complaintsof pain and in some cases the burning mouthsyndrome, discussed later in this chapter (Sohet al. 2007). A complaint of dry mouth can oc-cur in the absence of the clinical signs of dry-ness (‘symptomatic xerostomia’). Under such

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 233
circumstances the physical retention of the den-tures would not be expected to be diminished.
Aetiology of reduced salivary flow
Old age per se probably does not result in re-duced salivary flow rates (Scott & Baum 1990).The condition is more common in females thanin males (Flink et al. 2008) and is relatively com-mon in middle-aged and older people, the maincandidates for complete dentures, with up toa third of adults complaining of a dry mouth(Locker 1995; Field et al. 2001; Marton et al.2008; Johansson et al. 2009). This relatively highprevalence of xerostomia is likely to be due tothe fact that older individuals are more likelyto be suffering from systemic disease or to betaking drugs that can reduce salivary flow (vonBultzingslowen et al. 2007).
The most common causes of dry mouth(Niedermeier et al. 2000; Field et al. 2001;Guggenheimer & Moore, 2003) are:
� Adverse effects of drug therapy – over 500 med-ications have been implicated in xerostomia,e.g. tricyclic antidepressants, beta-blockers,diuretics, recreational drugs such as ecstasy.
� Auto-immune disease (Sjogren’s syndrome) –this affects 1-3% of the UK population, par-ticularly middle-aged females.
� Poorly controlled diabetes – reduced salivaryflow results from raised blood sugar, and in-creased micturition which can lead to dehy-dration.
� Radiotherapy – an increasing number of pa-tients with malignant disease of the headand neck receive radiotherapy as part oftheir treatment. Salivary tissue is very sen-sitive to radiation and so, in spite of strate-gies to limit exposure of the salivary glandsreduction in salivary flow often follows.
� Other causes – these include depression,chronic anxiety, dehydration, mouth breath-ing and smoking.
Management of dry mouth
In clinical xerostomia there are intra-oral signsof dryness such as a dry, atrophic mucosa andlack of saliva pooling in the floor of the mouth.The clinician can check the dryness of thebuccal mucosa simply and quickly during theexamination of the patient by carrying outthe ‘mirror test’. For this the clinician lightlypresses the face of the mirror against the buccalmucosa and then tries to remove it. If the mirrorcomes away easily the mucosa is still coveredby a substantial film of saliva; if the mucosaadheres to the mirror then it is dry. Referralto the patient’s general medical practitioner orto a specialist in oral medicine is likely to benecessary if a more thorough investigation isindicated.
Measures for managing xerostomiamay be local or systemic
Local measures� Artificial saliva. In cases where the salivary
flow rate cannot be improved, limited re-lief may sometimes be obtained by the useof artificial saliva (Ship et al. 2007; Oh et al.2008). These preparations are usually basedon either carboxymethylcellulose or mucin.But it should be remembered that as themucin preparations are of animal origin,they may not be acceptable to vegetarians orto some religious groups. Some patients withdry mouth find that frequent sips of wa-ter or milk are equally, or even more, effec-tive than artificial saliva in alleviating theirsymptoms.
� Denture and oral hygiene. It is very impor-tant for a denture patient with a dry mouthto maintain an excellent level of denturehygiene. The likelihood of the proliferationof Candida albicans and other microorgan-isms is increased in xerostomia and there-fore unless denture hygiene is maintained ata high level the denture is likely to be rapidlycolonised by the microorganism, increas-

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
234 Prosthetic Treatment of the Edentulous Patient
ing the likelihood of oral disease (Almstahlet al. 2008; Leung et al. 2008). Motivationand instruction of the patient, followed bymonitoring the quality of denture hygiene,are essential.
� Denture retention. In cases where an in-tractable dry mouth gives rise to a persistentproblem of loose dentures a denture adhe-sive will usually provide some improvementin denture function.
Systemic measures� Treatment of an underlying disease. It might be
possible, for example, to change an existingxerostomic drug to one less liable to reducesalivary flow. Also if the patient is diabetic,an improved glycaemic control will alleviatethe xerostomia.
� Increasing fluid intake. As there is a relation-ship between fluid intake and secretory per-formance, it is essential that the patient iskept well hydrated.
� Sialogogues. Pilocarpine can stimulate sali-vary flow where some functional salivarytissue remains, particularly in drug-relatedxerostomia, but it commonly has unpleasantside effects such as increased sweating. Thedry mouth may also be occasionally allevi-ated by sialogogues such as chewing gum orglycerine and lemon mouthwash.
Hard and soft materials formodifying the impressionsurface of denturesIn a chapter dealing with problems and solu-tions it is logical to consider materials whichcan be used to modify the impression surfaceof a denture to overcome some of these prob-lems; these materials can be either applied bythe clinician at the chair side or constructed bythe dental technician in the laboratory.
The materials may be classified as follows:
� Hard materials� Short-term soft lining materials� Long-term soft lining materials
Hard materials
Recent years have seen the development of agroup of useful materials, frequently describedas chair side reline materials, which can be usedto modify the impression surface of an existingdenture.
Composition
Commonly these materials consist of a pow-der containing polyethylmethacrylate togetherwith a liquid monomer, butylmethacrylate. Theimportant point to make is that monomericmethylmethacrylate, a tissue irritant, is avoi-ded. Many of the products include a bondingagent to enhance the adhesion of the material tothe existing denture polymer (Mutluay, 2005).The available materials vary in working time,setting time and viscosity.
Clinical applications
These materials can be immensely useful for re-lining dentures. As they can be used at the chairside a ‘one-stop’ reline technique can be em-ployed. This has great benefits in the followingsituations:
� A laboratory reline would require the patientto be without any denture for an inconvenientlength of time. This is likely to include pa-tients who only have one set of dentures thatthey can wear and who find being withoutdentures for any period of time socially un-acceptable. In particular, immediate denturepatients usually fall into this category. Thematerials can be used to improve the fit of animmediate denture that has become loose as

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 235
a consequence of bone resorption. This hardmaterial is usually added after initial heal-ing of the residual ridge has occurred. In theearly days following the extraction of teethit is more likely that a short-term soft liningmaterial will be used (see below). The greatadvantage in changing from the short-termsoft lining material to the hard material af-ter the initial healing period is that the lat-ter can be trimmed and polished for a high-quality finish and is much more durable. The‘one-stop’ reline technique can also be veryuseful when treating older patients, particu-larly when a domiciliary service is being pro-vided.
� A reline is required, but it is not necessary for itto last for much longer than a year. After thisperiod of time the hard chair side reliningmaterial is likely to have deteriorated to thepoint when replacement is required. Again,the immediate denture patient is likely to fallinto this category, as after a year the chairside reline will usually need replacing by apermanent rebase or by a replacement den-ture.
� Where a direct technique is indicated. A chairside reline is a direct technique that doesnot involve the intermediate stages of im-pression taking, cast pouring and laboratoryprocessing. There are therefore fewer oppor-tunities for errors to creep into the processand consequently there is the potential forgreater accuracy.
Clinical performance
Clinical trials have shown that the best ofthis group of materials are convenient to useand provide immediate improvement of fit andcomfort. Over a period of time there is a loss ofmaterial, especially at the borders of the den-ture; this loss is more apparent in the lowerdenture. However, the loss does not appearto cause marked deterioration of fit or com-fort (Hayward et al. 2003). The better materials
should be regarded as having a working life ofabout one year. The surface can be cleaned inthe normal manner and there is relatively littlediscolouration (Hayward et al. 2003).
Short-term soft lining materials
Composition
Most materials are supplied in a powder/liquidform. An alternative presentation is in a ready-to-use sheet form which can be found in oneproduct available to the dental profession andin several ‘over the counter’ products avail-able directly to the general public. The methodof self-treatment is to be discouraged, exceptas an emergency measure, as it is not basedon a sound clinical diagnosis and can resultin severe tissue destruction. It is essential thattraumatised tissue is examined by the clini-cian and that rational, rather than empirical,treatment is prescribed. The composition of thepowder/liquid types is as follows:
� Powder – polyethylmethacrylate, or copoly-mers of polyethyl/methylmethacrylate.
� Liquid – a mixture of an aromatic ester, suchas dibutyl phthalate, which acts as a plasti-ciser, and ethyl alcohol.
The setting process
After the powder and liquid have been mixed,the ethyl alcohol causes swelling of the poly-mer particles and permits penetration by theester so that a gel is formed. This is a physi-cal change; there is no chemical reaction. Thepresence of ethyl alcohol is necessary to initi-ate this process and the amount present in theliquid is related to the particle size and molec-ular weight of the polymer; the higher the alco-hol content, the shorter the gelling time (Murataet al. 1994). If particle size and molecular weightare low, then the ethyl alcohol content can be

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
236 Prosthetic Treatment of the Edentulous Patient
kept to a minimum. This state of affairs is desir-able as large amounts of ethyl alcohol producean unpleasant taste and sensation in the mouth.
Some materials suffer from dimensionalchange as a consequence of water absorptionand solubility of the material (Murata et al.2001). The ethyl alcohol and plasticiser areleached out reducing the flow of the materialwith time and causing the material to hardenand shrink. The more ethyl alcohol there is inthe formulation, the quicker is the rate of hard-ening. The rate can also be accelerated by di-etary solvents found in fatty foods and foodscontaining alcohol (Jepson et al. 2000).
Clinical applications
Short-term soft lining materials are placed inexisting dentures for the following reasons:
� Tissue conditioning. For tissue conditioning,the material is applied for a period of a fewdays to the impression surface of a den-ture when the denture-bearing mucosa istraumatised and inflamed. The tissue con-ditioner acts as a cushion absorbing the oc-clusal loads, improving their distributionto the supporting tissues and encouraginghealing of the inflamed mucosa.
� Temporary soft reline. A short-term soft liningmaterial can be used to improve the fit andcomfort of a denture, typically an immediaterestoration.
� Diagnosis. A short-term soft lining materialcan be used as a diagnostic aid where theclinician wishes to check the reaction of thepatient and the tissues to an improvementin fit of a denture. If the patient is happywith the change made by the short-term lin-ing material, the clinician has first-hand evi-dence of the degree of improvement that canbe expected if a long-term soft reline is tobe inserted. An important advantage of thisapproach is that the information has beenobtained by a reversible procedure. If the pa-
tient is unhappy the lining can be removedand the denture returned to its original state.
� Functional impression. A short-term soft lin-ing material can be used as a functional im-pression material applied to the impressionsurface of a denture for the purpose of secur-ing an impression under functional stresses.
� Recording the neutral zone. The ability of thesematerials to be moulded by the oral mus-culature over an extended period of severalminutes allows them to be used to record theneutral zone (p. 185).
It is probably true to say that these productsare used less as functional impression materialsthan as tissue conditioners and temporary softlining materials.
Relevant properties
The properties of soft lining materials which areof particular clinical relevance are:
� Softness. This property of the set materialalters with time. The longer the powder/liquid types are left in the mouth, the harderthey become. However, those with a low al-cohol content remain softer for longer andare thus more effective as tissue condition-ers.
� Viscoelasticity. The current range of availablematerials varies considerably with respectto viscoelastic behaviour and each materialcan be modified in this respect by alteringthe powder/liquid ratio, although the scopefor doing this is limited. The gelling mate-rial should have sufficient flow to allow itto adapt accurately to the mucosal surface,but should not flow so readily that most ofit is squeezed out when the patient occludeson the dentures. Those materials with a lowalcohol content exhibit plastic behaviour forthe first few hours after mixing. Elasticity in-creases as the materials age, but some of thepowder/liquid materials are elastic from the

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 237
start and are therefore unsuitable as func-tional impression materials.
� Dimensional stability. Those materials witha low alcohol content exhibit good dimen-sional stability for the first few hours aftermixing. Thus they are the materials of choiceif a functional impression is being obtained(see below). It is apparent that these proper-ties vary from brand to brand, and the clin-ical importance of each varies with the par-ticular use to which the material is being put.Therefore it is important for the clinician tobe able to select the best material for the jobin hand. This topic is discussed further in thenext section ‘Clinical implications’.
Clinical applications
Tissue conditioning
A material used for this purpose should ideallybe soft and elastic so that it provides a goodcushioning effect.
If a tissue conditioner is applied to the im-pression surface of an old denture, it will helpto resolve inflammation of the denture-bearingtissues. However, as the inflammation is re-duced the traumatised mucosa will alter inshape so that the lining ceases to be accuratelyadapted to the mucosa, thus slowing the rate ofhealing. Of course, if the material remains softand elastic, its deformation by relatively smallforces in the mouth will adapt it to the tissueswhile it is under load. Nevertheless, it is a wisepractice to replace the tissue conditioner withnew material after a few days to ensure that thetraumatised tissue reverts to a healthy state asrapidly as possible.
If one of the less viscous products is chosen,it is particularly important to instruct the pa-tient to close on the dentures with the lightestpossible contact while the material gels so that athickness of at least 2 mm is maintained. Need-less to say, it is essential to check that the free-way space of the dentures allows a lining of thisthickness to be inserted.
It must be emphasised that a course of tissueconditioning will not be effective unless othertraumatic factors, such as an unbalanced occlu-sion, under-extension and overextension of thebase are corrected before applying the condi-tioning material to the impression surface.
Functional impression
A material used for this purpose should ideally:
� Exhibit plastic flow – so that it can bemoulded to the denture-bearing tissues dur-ing function.
� Be dimensionally stable after theimpression-taking period – so that it re-tains its shape while the cast is poured.
As many of the materials available for func-tional impressions exhibit elastic recovery evenafter several hours, there is the danger that inthe time interval between removing the denturefrom the mouth and pouring the cast, the im-pression will change shape. The following regi-men is suggested as the best way of minimisingthis potential problem:
(i) The impression surface and borders of thedenture are inspected. Where there is obvi-ous over- or under-extension the bordersare adjusted so that a gap of 1–2 mm iscreated between the acrylic border and thefunctional depth of the sulcus. This size ofgap allows the functional impression ma-terial to be moulded by the sulcus tissuesand at the same time provides adequatesupport for the impression when the castis made.
(ii) If an undercut ridge is present, it is wiseto remove between 2 and 3 mm of the im-pression surface of the denture in the re-gion of the undercut. This allows for an in-creased thickness of functional impressionmaterial so that the shape of the tissue un-dercut is recorded more accurately.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
238 Prosthetic Treatment of the Edentulous Patient
(iii) The impression surface of the denture iscleaned and dried to ensure good adhe-sion. The functional impression material ismixed according to the manufacturer’s in-structions and placed in the denture. Af-ter the denture is inserted into the mouth,the patient is instructed to close gently to-gether so that the normal occlusal relation-ship is maintained. Natural movements ofthe tongue, cheek and lip musculature areencouraged to achieve border moulding ofthe impression.
(iv) Once the material has gelled sufficientlyfor there to be little risk of it distorting, thedenture is removed with care and exces-sive impression material is cut away fromthe polished surfaces with a scalpel, takingcare to maintain the full border shape.
The functional impression material is ap-plied to the denture approximately 1 hour be-fore the patient is due to have a meal and thepatient is asked to return to the surgery afterthat meal. If the patient’s report is favourableand the impression is satisfactory a cast ispoured immediately. In this way, the risk ofelastic recovery is reduced to a minimum, anda more accurate cast can be obtained (Murataet al. 2001). Attention to detail will lead to goodresults being obtained from this most usefultechnique.
Temporary soft lining
When a short-term soft lining material is usedas a temporary reline to improve the fit of a den-ture it is essentially acting simply as a space-filler. Ideally the material should gel within areasonably short time and be elastic so that itremains within the denture and can be insertedand removed over undercuts without result-ing in significant permanent deformation. Theavailable materials vary in their softness. If thelining is to be inserted into an immediate den-ture soon after the extraction of teeth, a rela-tively soft type should be selected as it will be
more comfortable for the patient. On the otherhand, if a reasonable amount of healing has oc-curred, a harder material can be chosen.
Cleaning
Beneath the surface the short-term soft liningmaterials are porous. If cleaning is ineffectiveplaque readily penetrates the lining which thentakes on the unsavoury appearance of what hasaptly been described as ‘an infected sponge’.Any tissue conditioning effect is rapidly lostand mucosal inflammation is aggravated as aresult. Thus it is essential when using these ma-terials to give the patient detailed instructionson how to keep them clean.
A brush should not be used on the lining as itis likely to damage the surface. Frequent swab-bing and rinsing of the lining should be carriedout together with daily soaking in a compatibleimmersion cleanser. Studies have shown thatcertain immersion denture cleanser/short-termlining combinations are compatible while oth-ers can be very damaging to the surface of thelining (Harrison et al. 1989). Alkaline hypochlo-rite cleansers, which are particularly efficient atremoving plaque, are compatible with most ofthe soft materials and should normally be thetype of cleanser recommended. Patients shouldbe informed which specific cleansers will dam-age their particular lining and warned not touse them.
Long-term soft lining materials
Long-term soft lining materials distribute stressmore evenly under dentures than do the harddenture base materials. They also absorb im-pacts that can arise from masticatory function(Kawano et al. 1997a). They can therefore besaid to have a shock-absorbing or cushioningeffect. Consequently it has been shown that theaddition of a long-term soft lining to a com-plete lower denture improves the ability to biteand chew and provides general improvementin comfort when compared with hard relines

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 239
(Bhat & Wright 2001; Kimoto, 2004; Mutluayet al. 2008); the lining has also been shown toimprove masticatory performance (Hayakawa2000). Heat-cured silicone materials seem to beparticularly beneficial in these respects.
Indications for use� Persistent pain under a denture� Thin atrophic mucosa� Parafunction
It is useful to consider the first three indica-tions together, as a complaint of persistent painmay be due to the poor quality of the denture-bearing mucosa or to the patient’s inability toregulate gripping or grinding habits. The wholeproblem may be exacerbated by gross resorp-tion of the mandible which results in the normalmasticatory forces being distributed over a re-duced area. It is important to make two points:first, the problem is almost always found in thelower jaw and, second, it is essential to ensurethat all existing denture faults have been elim-inated before deciding to proceed with a long-term soft lining:
� Replacing an existing denture which has a softlining. Once a patient has successfully worna lower denture with a soft lining and hasgot used to its ‘feel’ it is often wise to repeatthe prescription. If this is not done and thenew denture is made with a hard base thepatient may have problems in adapting to itand reject the prosthesis as a result.
� Sharp bony ridges or spicules. The pattern ofresorption of the mandible may result insharp ridges or spicules of bone on whichthe denture-bearing mucosa, in essence, be-comes impaled. The problem might be over-come, at least in the short term, by surgicallysmoothing the bone. However, there are of-ten occasions where poor health or a strongpreference by the patient to avoid surgery,are contraindications to this approach. Thereis also the danger that surgical interference
with the mandible will speed up resorptionof the bone, resulting in further destructionof the denture-bearing area. An alternative,conservative approach is to provide a softlining, which often provides an acceptablelevel of comfort under these circumstances.
� Superficially placed mental nerve. Another con-sequence of advanced resorption of themandible is that the mental foramen andmental nerve may become superficiallyplaced within the denture-bearing area sothat the nerve is traumatised during func-tion. This typically gives rise to a complaintof a severe, sharp, stabbing pain from thearea of the mental foramen which is broughton by biting. A soft lining restricted to theproblem area may provide relief. However,it is not uncommon to find that a superficialmental nerve requires greater pressure reliefthan can be provided by a soft lining. If thisis the case it may be necessary to cut the den-ture away in the area of the nerve to elimi-nate pressure on the nerve altogether.
Types of long-term soft liningmaterials
Soft linings are made either of silicone rubber orsoft acrylic. The silicone materials may be cold-curing or heat-curing. The soft acrylics are heat-curing; cold-curing soft acrylics have a verylimited lifespan and are best thought of as tem-porary soft linings.
Cold-curing silicone rubber materialsOne of the most important variations in com-position is the percentage of filler content. Asthe content increases, so does the level of wa-ter sorption with resultant worsening of dimen-sional stability. The rupture properties of thesematerials can be poor so that the soft liningis liable to tear and to become detached fromthe denture base. In isolated instances, the com-monly used catalyst, dibutyltin dilaurate hasbeen found to be a mucosal irritant. The abra-sion resistance of these materials is poor.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
240 Prosthetic Treatment of the Edentulous Patient
Heat-curing silicone rubber materialsIn contrast to the cold-curing silicones, the wa-ter absorption of these materials is low. As a re-sult, the dimensional stability is improved andaccuracy of fit is little affected by the oral envi-ronment. Improvements in rupture propertiesand adhesion to the denture base complete thepicture of superiority.
Acrylic resin materialsMost of the materials use polyethylmethacry-late or polybutylmethacrylate as the basic poly-mer. The materials are heavily plasticised to cre-ate softness.
A comparison of silicone and acryliclong-term soft lining materials
The following properties are of particular clini-cal importance:
� Elasticity. As shown in Fig. 16.2, silicone rub-ber materials react quite differently from softacrylic resins when a load is applied througha penetrometer. The heat-curing silicone ma-terial responds almost immediately to theapplication and removal of a load; it is elas-tic in nature. In contrast, the heat-curing softacrylic material shows a more gradual re-sponse; it is viscoelastic (McCabe et al. 1996).The elastic nature of the silicone soft liningmaterial is responsible for its ability to ab-sorb shock more effectively than the acryliclining and is no doubt the reason why it hasbeen shown to be better at enhancing masti-catory performance.
� Ageing. The properties of some long-termsoft lining materials alter dramatically withage and with immersion in water. Whereasthe softness and elastic behaviour of heat-curing silicone materials have been shownto remain stable with time (Dootz et al. 1993;Jepson et al. 1993; Kawano et al. 1997a) softacrylic materials become harder with timeand with immersion in water as a conse-
quence of the plasticiser leaching out into theliquid medium.
� Bonding. Heat-curing silicone and heat-curing soft acrylic materials have similarbond strengths to the hard denture basepolymer, whereas some cold-curing siliconesoft liners have lower values. This problemof low bond strength appears to be restrictedto those materials with a high filler con-tent. Of particular significance is the fact thathigher bond strengths are found if the softlining is processed against polymerisedpolymethylmethacrylate than against theunpolymerised material. In practice thismeans that it is better to add a soft lining toan existing hard denture base than to processboth materials at the same time (Kawanoet al. 1997b).
Further practical considerations
DurabilityThere has been a reluctance to prescribe softlinings because of the belief that their clini-cal life is too short. It is possible that such aviewpoint stems from the observed hardeningof soft acrylic materials and the debonding ofheavily filled cold-curing silicone materials. Ev-idence from clinical surveys supports the long-term benefit of a heat-curing silicone soft lining.In one of the surveys (Wright 1994), a numberof linings had been in situ for up to 8 years.Patients sought replacement dentures, not be-cause of problems with the soft linings but be-cause the acrylic teeth had worn down. Anothersurvey (Jepson et al. 1994) showed that the sur-vival time of a heat-curing silicone soft liningwas better than a heat-curing soft acrylic resin.This last study also showed that survival timewas related to thickness of the lining but thatthere was no benefit in increasing the thicknessbeyond 2 mm.
Midline fractureA frequently reported complication is fractureof the lower denture. As the soft lining must be

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 241
Load off
Load off
Typical penetration/recovery curve(Coe Super Soft @ 23C)
Typical penetration/recovery curve(Molloplast B @ 23C)
0.5
0.4
0.3
0.2
0.1
0.00 15 30 45
Time (secs)P
enet
ratio
n (m
m)
60 75
0.6
0.5
0.4
0.3
0.2
0.1
0.00 15 30 45
Time (secs)
a
b
Pen
etra
tion
(mm
)
60 75
Figure 16.2 Penetration/recoverycurves showing: (a) the gradual responseof a heat-curing soft acrylic lining material;(b) the rapid response of a heat-curing sili-cone soft lining material to the applicationand removal of a load.
at least 2 mm thick if its beneficial properties areto be fully effective, a corresponding reductionin the thickness of the hard acrylic resin of thedenture base is necessary to make room for thelining, which weakens the denture. Finite ele-ment analysis of lower dentures has shown thepresence of high stress concentrations linguallyin the lower canine areas and also around thearea of the labial notch (Shim & Watts 2000). Toreduce the risk of fracture a strengthener in theform of a cobalt-chromium lingual plate may beadded to the denture (Fig. 16.3).
CleaningSome soft lining materials suffer from high lev-els of water sorption. When the lining is placedin the mouth it absorbs saliva and can be in-vaded by oral microorganisms. It is perhapsthis set of circumstances that has led to the be-lief that soft linings may cause infections of theoral mucosa. Whilst soft linings do not activelysupport the growth of yeasts such as Candida al-bicans they do permit it and can in fact encour-age it due to the ready availability of nutrientsand to the difficulty of cleaning the surface of

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
242 Prosthetic Treatment of the Edentulous Patient
Figure 16.3 A lower denture with a cobalt-chromium lingual plate strengthener.
the lining (Wright et al. 1998). Effective clean-ing is more difficult if the surface of the lining isrough. With respect to the retention of Candidaalbicans a rough silicone lining is worse thana rough soft acrylic lining (Verran & Maryan1997).
It is therefore essential to achieve a smoothsurface to the lining (see below), and to givethe patient detailed instructions on how best toclean the lining (Davenport et al. 1986). This in-formation should stress that the manufacturer’srecommendation with respect to temperature ofthe water used with denture cleansers shouldbe followed; if not, there is a risk that there maybe a detrimental effect on colour of the liningand creation of surface roughness (Handa et al.2008).
Dietary advice, such as avoiding frequentintake of carbohydrates to restrict the supplyof nutrients to the microorganisms, may alsobe of value. A sodium hypochlorite denturecleanser is effective in eliminating Candida albi-cans and Staphylococcus aureus from the lining(Baysan et al. 1998; Yilmaz et al. 2005; Ferri-era et al. 2009), while not adversely affectingthe mechanical properties of the lining itself.However, it will cause some loss of colour andmight cause corrosion of a metal lingual platestrengthener. Microwave irradiation has beenshown to inhibit colonisation by Candida albi-
cans (Buergers et al. 2008) but should not beused if the denture has a metal lingual plate.
AdjustmentLong-term soft linings can be difficult to ad-just unless the burs and stones designed specif-ically for trimming these materials are used.After any reshaping has been completed it isimportant to leave as smooth a surface as pos-sible.
The flabby ridgeThe flabby ridge is most frequently seen in theanterior maxillary region and has been reportedin up to a quarter of edentulous patients (Carls-son, 1998). The bone is grossly resorbed, some-times up to the level of the anterior nasal spine,and is partly replaced by fibrous tissue. As a re-sult of this mobile fibrous tissue, the supportfor a complete denture is poor in the affectedregion leading to instability of the prosthesis.Both function and appearance can be heavilycompromised.
Aetiology
It has long been believed that the condition,sometimes called the ‘combination syndrome’,is the result of wearing a maxillary completedenture opposed only by lower natural anteriorteeth. This unfavourable relationship encour-ages tipping of the denture, overloading of theanterior maxillary ridge and rapid resorption ofalveolar bone (Lynch & Allen 2006). However,an assessment of controlled studies does not re-veal strong evidence to support this conclusion(Carlsson 1998). This is probably not surpris-ing when the many factors that influence bonemetabolism are considered. Nevertheless it isprobably wise to keep such patients under reg-ular review to ensure that damage to the ridgeis not occurring.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 243
Management
Approaches to treatment
Surgical� Excision of the fibrous tissue to try and cre-
ate a firm foundation for the prosthesis.� Osseo-integrated implants with, or without
bone grafting.
There are frequently contraindications to thesurgical approach:
� The patients are often older, or have a med-ical history, or a preference which makessurgery inappropriate.
� Removal of the fibrous tissue will reduce theextent and volume of the denture bearingarea. This can reduce denture retention andwill require replacement of the excised tissuewith denture-base material making the pros-thesis bulky and heavy.
� There will usually be too little alveolar boneleft for the placing of implants, so to adoptthis approach is likely to require furthersurgical intervention in the form of bonegrafting.
It is the opinion of the authors that in the vastmajority of cases a satisfactory denture can bemade without resorting to surgery.
Non-surgicalA key aspect in the non-surgical managementof the flabby ridge is the choice of impressiontechnique employed:
� To employ a mucodisplacive impressiontechnique which compresses the flabby tis-sue in order to try and obtain maximum sup-port from it or,
� To use a mucostatic impression techniquewith the aim of achieving maximum reten-tion.
There is little published evidence in the litera-ture that one approach produces better results
b
a
Figure 16.4 (a) Under occlusal pressure, the upperdenture is seated and the flabby anterior ridge dis-placed. (b) When the teeth are apart, the flabby tissuerecoils and displaces the denture downwards.
than the other. However, it is the authors’ clin-ical experience that it is more effective to usea mucostatic impression technique which doesnot displace the flabby tissue. This is because,if the fibrous tissue is distorted by a mucodis-placive impression, the denture will fit onlywhen seated by occlusal pressure (Fig. 16.4).When the teeth move out of occlusion and thepressure is released the compressed tissues re-bound and displace the denture.
If, however, the denture is constructed on acast obtained from a mucostatic impression ofthe flabby ridge in its resting position, the den-ture maintains its contact with the tissues whenthe teeth are out of occlusion. Retention willtherefore be optimal for the case in question.Support will be gained primarily from the hard

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
244 Prosthetic Treatment of the Edentulous Patient
palate and firm areas of the ridge rather thanfrom the flabby tissue.
Recommended impression techniques forthe flabby ridge are as follows:
� Preliminary impressions are taken in a stocktray using an alginate of low viscosity.This material will cause less tissue displace-ment than if impression compound wereused, with the result that less modifica-tion of the special tray will subsequently berequired.
� In many cases, it will be found that thetraumatised denture-bearing mucosa is in-flamed. Resolution of this inflammationshould be achieved before the working im-pressions are taken. This might be achievedby leaving the dentures out for several daysbeforehand, or by a combination of appro-priate modifications to the existing denturessuch as occlusal adjustment or the applica-tion of a short-term soft lining material to theimpression surface.
� Where the degree of mucosal displacementis only slight, a satisfactory result may beachieved by taking a working impressionin a spaced tray using an impression ma-terial of low viscosity. Suitable impressionmaterials for this purpose are low viscos-ity silicone rubber, alginate or impressionplaster. If desired, pressure on the displace-able tissue can be further reduced by usinga tray with perforations in the region cov-ering the flabby ridge. A technique of thistype has been described by Lynch and Allen(2006).
� Where the risk of displacement of the flabbyridge is high, a two-part impression tech-nique can be very effective:
(i) A preliminary impression is obtainedas described above. The area of flabbytissue, determined by intra-oral palpa-tion, should be marked out on the pre-liminary cast.
(ii) A cold-curing acrylic resin special trayis constructed that is close-fitting in the
Figure 16.5 A close-fitting acrylic tray cut away touncover the flabby anterior ridge. The tray is spacedfrom the mucosa along its anterior edge. The rim han-dle prevents the unset plaster falling into the mouthwhen the patient is supine.
firm denture-bearing area and leavesthe flabby ridge uncovered (Fig. 16.5).
(iii) The tray is tried in the mouth, checked,and if necessary adjusted so that it is notdisplacing the flabby tissue. It is a majoradvantage of this type of tray that directvision can be used to make absolutelycertain that the tray does not displacethe flabby ridge when it is fully seated.The borders of the tray are corrected inthe normal way.
(iv) An impression is taken of the firmdenture-bearing area using zinc oxide–eugenol impression paste or siliconerubber.
(v) If this first part of the impression provesto be satisfactory, it is replaced in themouth, the patient is tipped back intothe supine position and an impressionof the flabby tissue, left uncovered bythe tray, is obtained by applying a thinmix of impression plaster with a spat-ula, brush or syringe. As the impressionplaster sets rigidly there is no need tosupport it on the labial aspect.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 245
Once a satisfactory mucostatic impressionhas been obtained it is advisable to produce aheat-cured clear acrylic base from the mastercast. This base is checked in the mouth to as-sess its accuracy and subsequently provides op-timum retention and stability for the recordingof the jaw relationship.
Denture breakagesPrevious investigations into the size of theproblem in the UK reveal that the NationalHealth Service spent £7 million each yearon denture repairs. This figure did not takeinto account the cost of repairs undertakenprivately outside this government-financedscheme. Midline fracture of the complete upperdenture accounted for 29% of all repair work indental laboratories, whilst teeth debonded fromcomplete dentures accounted for 33% (Darbaret al.1994; Jagger et al. 1999). These two com-mon problems will now be considered.
Types of fracture
Fatigue of the acrylic resin
Fatigue fracture results from repeated flexingof the denture by forces too small to fractureit directly. Failure of the denture base is dueto the progressive growth of a crack originat-ing from a point on the surface where an abruptchange in the surface profile causes a localisedconcentration of stress many times that appliedto the bulk of the denture. The crack often startspalatally to the upper central incisors, growsslowly at first but undergoes an enormously in-creased rate of growth just before the denturefractures. A failure of this type most commonlyoccurs in dentures that are about 3 years old.
Midline fracture due to fatigue is the com-monest type of denture breakage and will bethe primary focus of the discussion which fol-lows.
Impact
Denture breakage might occur, for example, ifthe patient accidentally drops the denture whilecleaning it. It might also result from an acci-dent in which the patient receives a blow to themouth.
Whenever possible, the cause, or causes, ofthe fracture must be identified before the den-ture is repaired or replaced. Unless this is doneand the cause attended to, the denture is likelyto fracture again within a short period of time.
Causes of fracture
Denture factors
Stress concentratorsChanges in the surface profile of the dentureacting as stress concentrators include scratches,a median diastema and a deep frenal notch. In-clusions within the denture base such as poros-ity, plaster, dust, nylon filaments and relativelyflexible metal mesh ‘strengtheners’ may predis-pose to fracture and also contribute to the rapidgrowth of the crack. Stress concentration canalso develop around the pins of porcelain teeth.
Absence of a labial flangeAn open-face denture is not as stiff as a flangeddenture. Flexing will therefore be more markedand fatigue fracture more likely as a conse-quence. If this appears to be the primary causeof a fracture, and the anatomy of the anterioralveolus prevents the addition of a labial flangeto the replacement denture, a metallic denturebase is indicated.
Incomplete polymerisation of theacrylic resinIf the original curing cycle of the denturehad not included a terminal heating period at100◦C, the maximum degree of polymerisationwill not have been attained and the strength ofthe denture base will have been reduced fromits normally expected value.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
246 Prosthetic Treatment of the Edentulous Patient
Figure 16.6 Wear of acrylic posterior teeth result-ing in a wedge effect on the upper denture.
Previous repairWhen a denture has fractured previously in themidline and has been repaired with cold-curingacrylic resin, a further fracture may occur be-cause the cold-curing material is more suscep-tible to fatigue than the heat-cured resin. In ad-dition, the original denture base material on ei-ther side of the fracture line will already be fa-tigued.
Shape of the teeth on the dentureWhen acrylic posterior teeth are set up with anormal buccal overjet, they may wear and pro-duce the situation shown in Fig. 16.6, where awedging action on the upper denture resultsfrom occlusion of the teeth. Locking of the oc-clusion also appears to predispose to midlinefracture.
Poor fitWhen resorption of the alveolar ridge has takenplace beneath an upper denture, support willbe provided primarily by the hard palate. As aresult, flexing of the denture will occur whenthe teeth occlude. To correct this fault, the den-ture should be rebased after it has been re-paired. By this process, the old highly stressedresin is replaced by stronger heat-curing resin.
Lack of adequate reliefIf the mucosa overlying the crest of the ridge ismore compressible than that covering the cen-tre of the hard palate, flexing of the denture
will occur when the teeth occlude. To compen-sate for this variation in mucosal compressibil-ity, and to prevent the flexing, a palatal reliefchamber should be incorporated in the denture(p. 162).
Patient factors
Anatomical factorsCertain features of the patient may give rise todenture factors, already discussed, which pre-dispose to fracture. For example, a prominentlabial frenum will require a deep notch in theflange resulting in stress concentration in thatarea.
High occlusal loadsThese may occur in patients with powerfulmuscles of mastication, or whose natural lowerteeth are still present, or who are bruxists.
Repairing a denture
An informative and comprehensive review ofthis subject has been published by Seo et al.(2007).
If a broken denture appears to be serviceablea repair would usually be attempted if only be-cause the patient is likely to want the appear-ance restored as a matter of urgency. A repaircan be effective, cheaper and, of course, quickerthan remaking the denture.
An attempt should be made at the chair sideto relocate the parts of the broken denture. Ifthis can be achieved convincingly, the parts canthen be secured by using either hard stickywax or a cyanoacrylate adhesive before send-ing the denture to the laboratory for repair. Astudy by Goiato et al. (2009) has indicated thatcyanoacrylate adhesive is more accurate thansticky wax for this purpose.
If, after the two pieces of the denture havebeen located accurately and securely, a lack offit is diagnosed, one option is to reline or rebasethe denture (p. 224). It is possible to take a washimpression at the patient’s first visit rather than

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 247
waiting for the repaired denture to be returnedfor an impression to be taken at a subsequentappointment.
A repair should have:
� adequate strength;� dimensional stability;� a good colour match with the original den-
ture base.
Choice of repair material
The choice of repair material is not straightfor-ward.
Cold-curing acrylic resinThis is the material most commonly used, butits transverse strength is relatively poor (about60–65% of the strength of the original heat-curing base material) making a repeat fracturemore likely.
Light-cured acrylic resinsThese materials appear to be even weaker thancold-curing acrylic resin.
Microwave–cured acrylic resinsThese resins have a transverse strength compa-rable to a heat-cured material, but the process-ing can distort the original denture base. Thereis little information in the literature on the clin-ical use of microwave-cured acrylic resins fordenture repair.
Heat-cured acrylic resinThis has significantly better mechanical proper-ties, but requires more complex laboratory pro-cedures and higher costs.
Increasing the strength of repair
The strength of a repair can be increased by thefollowing:
Choice of repair materialThe best available repair material for the orig-inal denture base material should be selected.
For example, if time and cost do not rule it out,the use of a heat-cured material will give a su-perior repair to a cold-curing material.
The design of the repair surfaceA common technique is for the fractured sur-faces to be bevelled and slightly roughened tostrengthen the bond between repair and origi-nal resin by increasing the bonding area.
Chemical treatment of the repair surfaceThe repair resin bonds more strongly to the re-pair surface if the latter is wetted with methylmethacrylate monomer, dichloromethane orethyl acetone (Seo et al. 2007).
The use of reinforcementsThese reinforcements include carbon, glass oraramid fibres, or metal wire (p. 249). Recentstudies have indicated that when reinforcing,wires are air-abraded with alumina and treatedwith a metal conditioner to increase the adhe-sion of acrylic resin to them, and provided theyare correctly positioned in the denture, they canbe one of the most effective ways of strength-ening cold-curing repair resin (Kostoulas et al.2008; Shimizu et al. 2008).
Elimination of wax or salivacontaminationCareful technique is essential to avoid contam-ination of the repair surface by wax or saliva.
Replacing a broken denture with astronger prosthesis
A repaired denture may be made stronger byaltering its design or construction as indicatedpreviously. However, when no such improve-ments are possible – yet fracture remains aproblem, usually because of exceptionally highocclusal loading – a stronger denture basematerial is often indicated. Materials that maybe used for this purpose are described brieflybelow.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
248 Prosthetic Treatment of the Edentulous Patient
Cobalt–chromium alloy
Although cobalt–chromium alloy provides astrong and well-fitting denture base it has cer-tain disadvantages:
WeightUpper dentures with cobalt–chromium palatestend to be heavier than those with acrylic bases;therefore, in cases where anatomical factors areunfavourable for retention, there is an increasedlikelihood that the denture will drop.
Lack of adjustabilityCobalt–chromium alloy as a denture basematerial is far less adjustable than acrylicresin. For example, if a post-dam (which is anintegral part of the casting) requires modifica-tion, this can only be achieved to a very minorextent.
The problems of lack of adjustability andof increased weight can be minimised by re-stricting the cobalt-chromium component to ahorseshoe-shaped palatal strengthener set intothe acrylic base (Fig. 16.7). This design results inan impression surface of acrylic resin and thuspreserves the advantage of adjustability.
If it is judged that greater strength is re-quired than can be provided by a horseshoestrengthener, a more extensive metal base can
Figure 16.7 Upper denture with cobalt–chromiumhorseshoe-shaped strengthener.
Figure 16.8 Cobalt–chromium palate with poste-rior mesh to which an acrylic post-dam will be at-tached.
be used and still retain the advantage of anadjustable post-dam if the design shown inFig. 16.8 is employed. Acrylic resin, added tothe mesh at the posterior border, becomes thematerial in contact with the mucosa; this ma-terial can be modified should the need arise.When constructing this type of denture base,the dental technician has to take great care tominimise the step between metal and acrylic atthe finishing line. One way of achieving this isto dispense with the rather bulky spaced meshaltogether and to use a meta-resin for the post-dam region. This type of material adheres di-rectly to cobalt–chromium alloy and thereforedoes not require the mechanical retention of-fered by the mesh.
Modified polymeric denture basematerials
Polymeric materials can be modified and rein-forced. Examples of polymer modification in-clude the addition of elastomers or the creationof acrylic-elastomer copolymers. The elastomerabsorbs the energy of impact and therefore pro-vides protection for the acrylic resin. Such im-pact polymers are more expensive than conven-tional denture base polymers.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 249
Reinforcement of denture basematerials
The following fibres have been used to re-inforce and stiffen conventional denture basepolymers. It is important that when reinforcingfibres are used they are positioned and shapedto achieve optimum performance. They may beconditioned to improve bonding to the denturebase material. They should be positioned inthe areas of maximum stress, at right angles tothe anticipated line of fracture, and they shouldbe fully enclosed within the denture base sothat the fibres do not irritate the mucosa.
Carbon fibresTechniques have been described by which con-ventional upper dentures are reinforced by theinclusion of carbon fibre inserts in the palate toreduce the flexibility of the denture base. Thisapproach was reported to have reduced the in-cidence of fracture in a high-risk group of pa-tients, but a disadvantage of the method is theblack colour of the insert.
Ultra-high-modulus polyethylenefibres (UHMPE)In recent years there have been reports of den-ture bases being reinforced with ultra-high-modulus polyethylene fibre (Karacaer et al.2001). This material may be added either asa discrete woven insert into the denture baseor as chopped fibre incorporated in the poly-mer powder before the resin is mixed (Bradenet al. 1988; Gutteridge 1988). The fibre is trans-parent and its inclusion in the polymer aschopped fibre at a loading of 1% has resultedin an increase in impact strength exceedingthat of commercially available ‘high impact’resins. When the material is inserted as a wo-ven mat, loadings of 20–30% are reported. Bothapproaches can be used when a new denturebase is to be constructed, but the inclusion of awoven mat requires an additional technicalstage.
Glass fibresThe inclusion of glass fibres into acrylic resinhas been shown to improve fatigue resistance,flexural strength and impact strength (Kimet al. 2004). The fibres are produced either asa woven mat and inserted into the whole den-ture, or as individual fibres which are laid outin the region of a previous weakness. To obtainthe full benefit, care must be taken to positionthe fibres correctly. Effective adhesion of the fi-bres to the surrounding denture base polymeris achieved by pre-impregnating the fibres withpolymer before they are positioned (Narva et al.2001; Kostoulas et al. 2008).
‘Metal strengtheners’Metal mesh is occasionally included in a den-ture as a ‘so-called’ strengthener, but has notbeen shown to effectively reinforce a denturebase (Narva et al. 2001) and in fact mightweaken it by acting as a stress concentrator.This finding conflicts with the more recent re-sults for the effectiveness of wire strengthen-ers mentioned above. A possible explanationis that the wires are stiffer than the mesh andhave been treated to create a good bond withthe acrylic resin of the repair.
Debonding of teeth
Causes
Debonding of teeth from the denture base oc-curs more commonly on upper anterior teeth.In the presence of an existing weak bond theupward and outward force arising from contactby the lower anterior teeth causes bond failure.
The usual reasons for a weak bond betweentooth and denture base are:
� The presence of tin-foil substitute on theridge-lap surface of the tooth.
� The presence of residual wax on the samesurface.
� The use of cross-linked teeth which are in-compatible with the particular denture basepolymer.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
250 Prosthetic Treatment of the Edentulous Patient
All the above factors prevent effective chemicalunion between the teeth and the denture baseand the production of an acceptable interwovenpolymer network (Cunningham & Bennington1999; Takahashi et al. 2000).
Prevention
The literature is not unanimous about how bestto achieve the maximum bond strength be-tween teeth and denture base. The variable andsometimes conflicting results are possibly dueto the different combinations of denture teethand denture base polymers that were used inthe studies. Of the various recommendationsthat have been made for minimising the risk ofdebonding the following have received fairlywidespread support (Buyukyilmaz & Ruyter1997; Cunningham & Bennington 1999; Taka-hashi et al. 2000; Dalal et al. 2009):
Selection of compatible artificial teethand denture base polymerThis compatibility should be checked from in-formation sheets provided with the products,or by seeking information from the manufactur-ers. Conventional denture teeth tend to achievea higher bond strength than cross-linked teeth.
Removal of all traces of wax and tin-foilsubstitute from the teethThe complete removal of wax before packingthe mould is not consistently achieved withboiling water alone and so for optimum bondstrength the use of a wax solvent is recom-mended (Cunningham & Bennington 1997).
Mechanical preparation of the teethGrinding and sandblasting the bonding surfaceof the teeth enhances the bond strength sig-nificantly (Chung et al. 2008). Small channelsdrilled into the palatal surface of the teeth willincrease the area available for the curing den-ture base resin. However, it needs to be remem-bered that such recesses in the ridge-lap surfaceof the teeth can make complete wax removal
more difficult. Therefore particular care needsto be taken when removing the wax; otherwise,the adjustments can result in a weaker, ratherthan a stronger bond.
Chemical preparation of the teethApplying methyl methacrylate monomer(Barbosa et al. 2009), or a solvent such asdichloromethane or ethyl acetone to the ridge-lap surface of the teeth creates microscopicpores and channels which promote diffusion ofthe polymerisable materials and increase bondstrength.
Use of a heat-curing denture basepolymerThis material polymerises more slowly than acold-curing material and ensures better pen-etration into the tooth substance. Medium orlong curing cycles have been shown to result inhigher tensile bond strengths between denturebase material and acrylic teeth than the use ofshort curing cycles (Dalal et al. 2009).
GaggingGagging is a protective reflex to stop un-wanted entry of substances into the mouth andoropharynx (Dickinson & Fiske 2005).
Aetiology of gagging
There are a number of causes of gagging thatmay be conveniently grouped together as fol-lows.
SomaticThe term ‘somatic’ covers those situationswhere the reflex is triggered by tactile stimu-lation of the soft palate, posterior third of thetongue and fauces. Included in this group arenumerous iatrogenic causes related to the de-sign of dentures.
Some patients begin to gag when new den-tures are inserted, but in most cases this reflexsoon disappears as they adapt to the dentures.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 251
However, the reflex may persist if there arefaults with the dentures such as an excessive oc-clusal vertical dimension, or if the dentures arestimulating the sensitive areas of the soft palateand tongue directly. This stimulation may becaused by palatal over-extension, a posteriorborder which is too thick or poorly adapted, theteeth encroaching on tongue space or indeedby any factor producing denture instability. Anupper denture whose posterior border is under-extended posteriorly can provoke gagging be-cause as the edge of the denture terminates onrelatively incompressible mucosa a satisfactorypost-dam cannot be produced. This results inpoor retention, which increases denture insta-bility, stimulates the tongue and palate, andcauses apprehension in the patient. When thisdiagnosis is established, it requires a very care-ful explanation by the clinician to convince thepatient that to cure the problem it will be nec-essary to cover more, rather than less of thepalate.
PsychogenicPsychogenic causes may arise from sight,sound or thought. They include the sight of im-pression material being mixed or the sound ofanother patient gagging. The patient may be ex-tremely apprehensive because of an unhappyfirst-hand experience of dental procedures oras a result of disturbing stories from friends. Inrare instances, gagging may be a manifestationof a psychological disturbance which is not pri-marily related to the patient’s dental treatment.It is within this group one finds the most severeproblems.
SystemicLess frequently, the causative factor may be sys-temic disease, particularly conditions affectingother regions of the gastrointestinal tract; forexample, the link between gagging and alco-holism may be related to the persistent gastritisfound in such patients. Persistent catarrh willprevent nose breathing and may contribute tothe problem of gagging. A link between smok-
ing and gagging has been described (Wright1979).
Patient management
Assessment of the severity of theproblem
A carefully taken history and an examinationof the patient will reveal the patient’s con-cerns and fears, what procedures have previ-ously been tried and with what result. The find-ings will allow the clinician to gauge the sever-ity of the problem and provide clues as to thecause. For example, a situation where a patienthas been able to tolerate the clinical stages ofdenture construction but then has difficulty inwearing the finished dentures points to an ia-trogenic cause which should be treated rela-tively simply by correcting the error in denturedesign. At the other extreme is the patient whogags as soon as a mouth mirror is brought up tothe mouth.
Impressions
All but the most phlegmatic of individuals findimpression taking unpleasant. However, gag-ging can usually be prevented by the following.
Reassurance and relaxationIt is very important that the clinician has a con-fident, relaxed and sympathetic chair side man-ner. It is essential that the anxious patient isreassured and encouraged to relax both phys-ically and mentally. The dental nurse can alsoplay a major role in creating an appropriatestate of mind in the patient.
Position of the patientThe dental chair should be adjusted so that thepatient is sitting comfortably in the upright po-sition.
Breathing through the noseInstructing the patient to breathe through thenose while the impression tray is being tried in

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
252 Prosthetic Treatment of the Edentulous Patient
Figure 16.9 The tongue in its guarding position dur-ing the taking of an upper impression.
the mouth or the impression is being taken isone of the most helpful methods of preventingretching. During nasal breathing the soft palateremains stationary in a low position and makescontact with the tongue in its ‘guarding’ posi-tion, thus closing off the oral cavity from thenasopharynx (Fig. 16.9); this arrangement pro-tects the nasopharynx from the perceived threatof the foreign body in the mouth. If the patientbreathes through the mouth, the soft palate israised and this protective feeling may well belost.
A refinement of this technique is where thepatient is instructed in a regime of controlledbreathing which must be practised for 1 or2 weeks before impression taking. Breathingshould be slow, deep and even; the requiredsteady rhythm can be ensured by asking the pa-tient to link it mentally to a well-known tune.
Impression techniqueImpression trays should be as well fitting aspossible. As close-fitting special trays are lessbulky than spaced trays, they are better toler-ated and should be used whenever possible.When trying trays in the mouth, firm, positive,confident movements should be used. Most pa-tients tolerate the lower impression better thanthe upper one, so if the lower impression istaken first, the success of the procedure is likelyto reassure the patient. The impression materialshould be mixed or prepared out of sight of the
patient and the amount placed in the tray keptto the minimum necessary to record the rele-vant structures. A saliva ejector should be usedif copious amount of saliva collects in the floorof the mouth.
DistractionIt is during the insertion of the impression andwhile the material is setting that it is partic-ularly important to distract the patient’s at-tention from what is going on. This may beachieved by the clinician talking about some-thing that is known to be of particular interestto the patient, or by reinforcing the requirementthat the patient continues to breathe slowly andsteadily through the nose. It has even been sug-gested that the patient be asked to raise one legand to concentrate on not lowering it until theimpression has set!
The severe gagging reflex
The first challenge when treating a patient whohas this problem is to obtain an accurate im-pression so that a well-fitting denture base canbe constructed. The second challenge is to pro-vide a prosthesis that can be worn by the pa-tient for a reasonable length of time. The fol-lowing approaches to the management of thisdifficult problem have been found to be useful:
The training dentureThe training denture approach may be of valuewhen treating any patient with a long historyof difficulties which suggest frank denture in-tolerance, including gagging. The rationale forthis approach is that as new stimuli are intro-duced gradually, the patient has to cope withonly one small step at a time and does notadvance to the next stage in treatment un-til the previous stage has been mastered. Therate of progress is therefore under the patient’scontrol, a feature which can increase patientconfidence. This approach whereby intra-oralstimuli are gradually increased is known as

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 253
desensitisation (Bassi et al. 2004). A possibleclinical progression is as follows:
(i) The impressions may be obtained by oneof the techniques outlined above. Alter-natively, primary impressions can oftenbe successfully produced using impres-sion compound because insertion, bordermoulding and removal of this type of im-pression can be completed so quickly thatthe gagging reflex does not have time todevelop. As the compound is still soft onremoval from the mouth it must be chilledimmediately and thoroughly under coldwater to prevent distortion. Training basesare constructed on the models obtainedfrom the compound impressions and theirfit is refined in the mouth using a chair siderelining material. The close fit and smalldimensions of the bases are much moreeasily tolerated than a conventional im-pression.
(ii) The upper training base is constructedwith a posterior extension judged to beappropriate for a particular patient. Thiswill vary from the minimum extensionof a horseshoe, palateless design to con-ventional extension to the vibrating line.To help the patient to control the lowerbase, a spine of a polybutylmethacrylateresin may be added in the mouth so thatthe muscles of the tongue and cheeks restagainst it.
(iii) It is often advisable for the patient to startby wearing just one of the bases. The baseshould be worn for as long as the patientcan tolerate, but should be removed fromthe mouth before gagging occurs. This isbecause the objective of treatment is to ex-tinguish the gag reflex, but if the patientis too heroic and persists in wearing theprosthesis until frank gagging occurs thereflex may in fact be reinforced. After a restperiod, the base should be reinserted andan attempt made to increase the period ofwear. This process is repeated until the pa-
Figure 16.10 Training bases with the addition ofanterior teeth and a spine of cold-curing polybutyl-methacrylate resin.
tient reports that the base can be worn suc-cessfully. Some patients find that it helpsthem get through this difficult early stageif they suck a boiled sweet while wearingthe training base.
(iv) Once the first major challenge of wearingthe initial training base for reasonable pe-riods of time has been met successfully,further additions can be progressively in-troduced. For example, more courageousextensions can be developed with chairside relining materials and anterior teethcan be added (Fig. 16.10). Eventually, ifprogress is maintained, the complete den-tures are developed and because the mul-tiple additions make these look rather likea patchwork quilt, a copying techniquemay be used to produce the replacementprostheses. The training base approach tocomplete denture treatment is inevitablya complicated and long drawn-out affair.However, if all other more conventionaltechniques have failed, the approach maybe the one remaining chance of providinga successful outcome.
Relative analgesiaRelative analgesia has been found to be a help-ful technique in that it will allow the clinicianto obtain a satisfactory impression whilst at

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
254 Prosthetic Treatment of the Edentulous Patient
the same time reducing patient embarrassment(Packer et al. 2005). However, the technique willonly put off the evil hour; although it may in-deed be possible to obtain a reasonable impres-sion, ultimately the patient must meet the chal-lenge of wearing a denture in an unsedatedstate. Of particular importance, though, are theregulations that govern this method of pain andanxiety control. The regulations in force in theparticular country must be followed precisely.
AcupunctureThe gag reflex has been shown to be capable ofbeing controlled by acupuncture (Fiske & Dick-inson 2001; Rosted et al. 2006).
HypnosisHypnosis has been used in the treatment of se-vere cases (Barsby 1994). Its success is depen-dent upon the patient being well motivated andbeing able to practise self-hypnosis, thus en-abling a denture to be worn outside the dentalsurgery.
Gagging is a serious problem in a minor-ity of patients only. From the foregoing accountthe reader will appreciate that treatment can belengthy and that a great deal of patience andperseverance are required by both clinician andpatient. Further details on aetiology and man-agement can be obtained elsewhere (Bassi et al.2004; Dickinson & Fiske, 2005).
The burning mouth syndromeThe burning mouth syndrome (BMS) can bevery troublesome to the sufferer, presents prob-lems of diagnosis and often involves prolongedtreatment (Basker et al. 1978; Maresky et al.1993). The symptoms occur in 5–7% of the adultpopulation. Of those who seek treatment, thereis a predominance of women, with a mean ageof approximately 60 years. The most commonsites of the complaint are the tongue and theupper denture-bearing tissues. Rather less com-mon are the lips and lower denture-bearing tis-
Figure 16.11 Severe blistering of the mucosa re-sulting from a residual monomer content of 3.2%.
sues. The oral mucosa typically appears nor-mal. However, those cases due to a high levelof residual monomer are the exception as themucosa is inflamed (Fig. 16.11).
Many BMS patients have consulted numer-ous health care professionals before seekinghelp from the clinician or dental specialist. Theyrarely know of others with the complaint andcan therefore feel quite isolated. If several pro-fessionals have stated that the mouth looks nor-mal the patient may feel that ‘it is all in themind’. The level of anxiety is commonly raisedand cancerophobia may develop.
Classification
Three types of BMS have been described(Lamey & Lewis 1989). The classification is use-ful as it points the way towards appropriatetreatment and a probable prognosis.
Type 1There are no symptoms on waking. A burn-ing sensation then commences and becomesworse as the day progresses. This patternoccurs every day. Approximately 33% of pa-tients fall into this category and are likely toinclude those with haematinic deficiencies anddefects in denture design.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 255
Type 2Burning is present on waking and persiststhroughout the day. This pattern occurs everyday. About 55% of patients are placed in thiscategory, a high proportion of who have chronicanxiety and are the most difficult to treat suc-cessfully.
Type 3Patients have symptom-free days. Burning oc-curs in less usual sites such as the floor of themouth, the throat and the buccal mucosa. Thiscategory is made up of the remaining 12% ofpatients. A study of this group has shown thatthe main causative factors are allergy and emo-tional instability (Lamey et al. 1994). The in-vestigation of these patients is likely to includepatch testing.
Aetiology
BMS has been attributed to a multitude ofcauses which may be placed conveniently intothree groups:
1. Local irritants, including denture faults2. Systemic factors3. Psychogenic factors
Local irritation
Denture faultsErrors in denture design which cause a dentureto move excessively over the mucosa, which in-crease the functional stress on the mucosa orwhich interfere with the freedom of movementof the surrounding muscles may initiate a com-plaint of burning rather than frank soreness.Denture design errors have been discovered in50% of BMS patients.
Residual monomerHigh levels of residual monomer in the den-ture base have been reported and the tissuedamage produced is considered to be the
result of chemical irritation rather than a trueallergy (Fig. 16.11) (Austin & Basker 1980). It ispossible that high levels of residual monomer,which have ranged from three to ten times thenormal value, are due to errors inadvertentlyintroduced into the short curing cycles whichare popular with manufacturers and dentallaboratories. If the requisite curing temperatureof 100◦C is not achieved in the relevant partof the short curing cycle, there is a marked in-crease in residual monomer content (Austin &Basker 1982). This content can be measuredby specialised analytical techniques such asgas chromatography and high-pressure liquidchromatography. Recent work (Zissis et al.2008) has confirmed that higher levels ofresidual monomer are found in cold-curing asopposed to heat-curing resins. The cold-curingmaterials release significant amounts of resid-ual monomer in the first few weeks of storagein water.
Some authorities may not consider a reac-tion to residual monomer to be an exampleof BMS where, classically, the mucosa looksnormal. However, a patient who reacts to ahigh level of the chemical complains of a burn-ing sensation and so we feel justified in inclu-ding it.
MicroorganismsThe role of microorganisms in burning mouthsyndrome is controversial and studies have notshown a link between the presence of Candidaalbicans and the complaint.
Smoking and mouthwashesSmoking and the regular use of some mouth-washes are irritants that have been implicatedin BMS.
Systemic causes
Nutritional deficienciesContributions from nutritional deficienciessuch as iron, vitamin B complex and folic acid

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
256 Prosthetic Treatment of the Edentulous Patient
Figure 16.12 A burning tongue: note the smoothsurface of the dorsum.
should be highlighted. An example of BMScaused by a deficiency is shown in Fig. 16.12.
Iron deficiencies have been found in 8% andfolic acid deficiencies in 6% of BMS patients.Low blood levels of vitamin B1 and B6 werefound in 40% of patients (Lamey 1998).
Endocrine disordersWhat is apparent is the relative unimportanceof the climacteric as a causative factor, a con-temporary viewpoint which is at variance withpast clinical opinion.
On rare occasions, the symptoms are foundto be linked with an undiagnosed diabetes mel-litus. Treatment of the medical condition resultsin resolution of BMS.
XerostomiaXerostomia, frequently associated with BMS,has many causes as mentioned earlier in thischapter. One that should be highlighted hereis drug-induced xerostomia. Recent investiga-tions have produced evidence of a link betweenType 2 BMS, antidepressant medication andreduced parotid gland function (Lamey et al.2001).
It should be recognised that the presence of adry mouth is capable of accentuating the symp-toms initiated by any of the causes of local irri-
tation. This is an example of the multifactorialnature of BMS.
HypersensitivityTrue hypersensitivity to constituents of denturebase polymer is rare and typically results in lo-cal symptoms such as burning or itching. In oneinstance where there were systemic symptomsof nausea, dizziness and general malaise the pa-tient was found to have reacted to dyes usedto colour the polymer. Dentures made of clearpolymer proved successful (Barclay et al. 1999).
In a study of Type 3 patients the avoidance inthe diet of such food additives as benzoic acid,propylene glycol and cinnamon products ren-dered a significant number of patients asymp-tomatic. Interestingly, those patients who werenot cured had higher levels of psychiatric ill-ness (Lamey et al. 1994).
Parkinson’s diseaseIt has been reported that the prevalence of BMSwas 24% in people suffering from Parkinson’sdisease; this is five times that found in surveysof general populations (Clifford et al. 1998).
Psychogenic causes
The more common psychiatric disorders associ-ated with BMS are anxiety, depression, cancero-phobia and hypochondriasis. The associatedparafunctional activities such as bruxism andabnormal and excessive tongue movements arecapable of inducing mucosal irritation. Onestudy showed that parafunctional habits werepresent in 61% of patients with BMS (Patersonet al. 1995).
Management
Faced with a multitude of causative factors, itwill be recognised that the process of diagno-sis and treatment is usually a time-consumingaffair. It is beyond the scope of this book to dis-cuss management in any detail, but the pointshould be made that establishing a diagnosis

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 257
entails a very careful and systematic approachto history-taking and examination, and usuallyinvolves the need for a battery of special tests.The establishment of a multi-disciplinary cliniccomprising a dental clinician, doctor, derma-tologist and psychiatrist, together with experttechnical assistance, is desirable in order to ef-fectively follow the regimen outlined in the fol-lowing:
(i) Initial assessment (history/examination/special tests)
(ii) Provisional diagnosis(iii) Initial treatment (e.g. elimination of lo-
cal irritants and investigating and treatinghaematinic deficiencies)
(iv) Assessment of initial treatment(v) Definitive diagnosis
(vi) Definitive treatment (local/systemic cor-rection/psychological therapy)
(vii) Follow-up
Outcome
With regard to outcome, analysis of variousstudies suggests that about two-thirds of BMSpatients are either cured or improved to such anextent that the burning sensation is no longer anoverwhelming problem. There remains a groupof patients for whom the current state of knowl-edge can offer relatively little benefit. Somein this small group remain totally resistant totreatment. However, it should be rememberedthat even in these refractory cases BMS is notnecessarily a life sentence as spontaneous re-missions can eventually occur for no apparentreason.
The above account is a simplification ofmuch work undertaken over the years. A de-tailed resume may be found elsewhere (Klasseret al. 2008).
Disturbance of speechThe presence of complete dentures can modifyspeech by affecting articulation and by altering
the degree of oral resonance (Lawson & Bond1968, 1969; Carr et al. 1985; Seifert et al. 1999). Anumber of sounds are articulated by contact ofthe tongue with the palate and with the teeth.A change in speech that may be quite markedwhen the dentures are first inserted will usu-ally disappear completely within a few days.However, if changes in the position or shape ofcontact surfaces on the denture require a modi-fication of tongue behaviour that is beyond theadaptive capability of an individual patient, aspeech defect will persist. It should also be re-membered that the tongue of a patient who iswearing complete dentures has a dual functionto take part in speech articulation and to con-trol the dentures. If the dentures are loose, thedemands of this latter function may be so greatthat there is a general deterioration in the qual-ity of speech. As mentioned on p. 232, a drymouth is likely to result in looseness of denturesand will also affect speech due to the loss of sur-face lubrication of the oral mucosa. The follow-ing relationships are particularly important tothe production of clear speech.
Tip of the tongue to the palate
Contact between the tip of the tongue and thepalate is required in the production of /s/, /z/, /t/,/d/ and /n/. Consequently, a change in the shapeor thickness of the denture contact surface re-sulting from the fitting of new dentures willrequire a modification of tongue behaviour inorder to produce sounds which are the same asbefore. In the vast majority of cases, the neces-sary modification occurs without any difficultyin a relatively short period of time.
The sound most commonly affected in thisway is /s/, a sound which is generally producedwith the tongue tip behind the upper anteriorteeth. A narrow channel remains in the centre ofthe palate through which air hisses (Fig. 16.13).If the palate is too thick at this point, or if theincisors are positioned too far palatally, the /s/may become a /th/. If the denture is shaped sothat it is difficult for the tongue to adapt itself

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
258 Prosthetic Treatment of the Edentulous Patient
s
th
Air
sh
Figure 16.13 The position of thetongue for producing the sounds /th/,/s/ and /sh/.
closely to the palate, a channel narrow enoughto produce the /s/ sound will not be producedand a whistle or /sh/ sound may result. This ismost likely to be the consequence of excessivepalatal thickening laterally in the canine region(Fig. 16.14)
Lower lip to incisal edges of upperanterior teeth
The lower lip makes contact with the incisaledges of the upper anterior teeth when thesounds /f/ and /v/ are produced. If the positionof these teeth on a replacement denture is dra-
matically different from that on the old denturethere is likely to be a disturbance in speech.
Lateral margin of the tongue toposterior teeth
Contact between the lateral margins of thetongue and the posterior teeth is necessary toproduce the English consonants /th/, /t/, /d/, /n/,/s/, /z/, /sh/, /zh/ (as in measure), /ch/, /j/ and /r/(as in red). Air is directed forwards over thedorsum of the tongue and may be modified bymovement of the tongue against the teeth or an-terior slope of the palate to produce the finalsound. If the contact can only be achieved with
S sh
a b
Figure 16.14 (a) The polished surface of the denture palatal to UR3 and UL3 is correctly shaped so that thetongue can form a narrow channel in the midline for producing the /s/ sound. (b) Excessive thickening of thepalate laterally prevents close adaptation of the tongue to the palate so that the /s/ becomes /sh/.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 259
difficulty, movement of the tip of the tonguemay be restricted with consequent impairmentof speech. This difficulty arises if the posteriorcontact surfaces are too far from the resting po-sition of the tongue as a result of the occlusalplane being too high, the occlusal vertical di-mension too great or the posterior teeth placedtoo far buccally. In extreme cases, it may not bepossible for the tongue to produce a completelateral seal so that air leaks out laterally duringthe production of /s/ and /z/ resulting in what issometimes known as a lateral sigmatism.
The relationship of mandibleto maxilla
The mandible moves closest to the maxilla dur-ing speech when the sounds /s/, /z/, /ch/ and /j/are made. Normally, at this time, there will bea small space between the occlusal surfaces ofthe teeth. However, if the occlusal vertical di-mension of the dentures is too great, the teethmay actually come into contact so that the pa-tient complains that the teeth clatter.
References and additionalreadingAlmstahl, A., Wikstrom, M. & Fagerberg-Mohlin, B.
(2008) Microflora in oral ecosystems in subjectswith radiation-induced hyposalivation. Oral Dis-eases, 14, 541–9.
Austin, A.T. & Basker, R.M. (1980) The level of resid-ual monomer in acrylic denture base material.British Dental Journal, 149, 281–6.
Austin, A.T. & Basker, R.M. (1982) Residualmonomer levels in denture bases: the effectsof varying short curing cycles. British DentalJournal, 153, 424–6.
Barbosa D.B., Monteiro D.R., Barao V.A., Pero A.C. &Compagnoni M.A. (2009) Effect of monomer treat-ment and polymerisation methods on the bondstrength of resin teeth to denture base material.Gerodontology, 26, 225–31.
Barclay, S.C., Forsyth, A., Felix, D.H. & Watson, I.B.(1999) Case report – hypersensitivity to denturematerials. British Dental Journal, 187, 350–52.
Barsby, M.J. (1994) The use of hypnosis in the man-agement of ‘gagging’ and intolerance to dentures.British Dental Journal, 176, 97–102.
Basker, R.M., Sturdee, D.W. & Davenport, J.C. (1978)Patients with burning mouths. British Dental Jour-nal, 145, 9–16.
Bassi, G.S, Humphris, G.M & Longman, L.P. (2004)The aetiology and management of gagging: a re-view of the literature. Journal of Prosthetic Dentistry,91, 459–67.
Baysan, A., Whiley, R. & Wright, P.S. (1998). Use ofmicrowave energy to disinfect a long-term soft lin-ing material contaminated with Candida albicans orStaphylococcus aureus. Journal of Prosthetic Dentistry,79, 454–8.
Bhat, J. & Wright, P.S. (2001) The clinical acceptabilityof chairside soft lining materials. European Journalof Prosthodontics and Restorative Dentistry, 9, 46.
Braden, M., Davey, K.W.M., Parker, S., Ladizesky,N.H. & Ward, I. (1988) Denture base poly(methylmethacrylate) reinforced with ultra-high modu-lus polyethylene fibres. British Dental Journal, 164,109–13.
Branemark, P.-I., Zarb, G.A., & Albrektsson, T. (eds)(1985) Tissue integrated prostheses. Quintessence,Chicago.
Buergers, R., Rosentritt, M., Schneider-Brachert, W.,Behr, M., Handel, G. & Hahnel, S. (2008) Efficacyof denture disinfection methods in controlling Can-dida albicans colonization in vitro. Acta OdontologicaScandinavica, 66, 174–80.
Buyukyilmaz, S. & Ruyter, I.E. (1997) The effects ofpolymerization temperature on the acrylic resindenture base-tooth bond. International Journal ofProsthodontics, 10, 49–54.
Carlsson, G. (1998) Clinical morbidity and seque-lae of treatment with complete dentures. Journal ofProsthetic Dentistry, 79, 17–23.
Carr, L., Wolfaardt, J.F. & Haitas, G.P. (1985) Speechdefects in prosthetic dentistry. Part II – Speechdefects associated with removable prosthodontics.Journal of the Dental Association of South Africa, 40,387–90.
Chung K.H., Chung C.Y., Chung C.Y. & Chan D.C.N.(2008) Effect of pre-processing surface treatmentsof acrylic teeth on bonding to the denture base.Journal of Oral Rehabilitation, 35, 268–75.
Clifford, T.J., Warsi, M.J., Burnett, C.A. & Lamey, P.J.(1998) Burning mouth in Parkinson’s disease suf-ferers. Gerodontology, 15, 73–8.
Cunningham, J.L. & Benington, I.C. (1997) A surveyof the pre-bonding preparation of denture teeth

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
260 Prosthetic Treatment of the Edentulous Patient
and the efficiency of dewaxing methods. Journal ofDentistry, 25, 125–8.
Cunningham, J.L. & Bennington, I.C. (1999) An in-vestigation of the variables which may affect thebond between plastic teeth and denture base resin.Journal of Dentistry, 27, 129–35.
Dalal, A., Juszczyk, S., Radford, D.R. & Clark, R.F.K(2009). Effect of curing cycle on the tensile strengthof the bond between heat cured denture baseacrylic resin and acrylic resin denture teeth. Eu-ropean Journal of Prosthodontics and Restorative Den-tistry, 17, 146–9
Darbar, U.R., Huggett, R. & Harrison, A. (1994) Den-ture fracture – a survey. British Dental Journal, 176,342–5.
Davenport, J.C. (1970) An adverse reaction to a sili-cone rubber soft lining material. British Dental Jour-nal, 128, 545–6.
Davenport, J.C., Wilson, H.J. & Spence, D. (1986) Thecompatibility of soft lining materials and denturecleansers. British Dental Journal, 161, 13–17.
Dickinson CM & Fiske J. (2005). A review of gaggingproblems in dentistry: 1. Aetiology and classifica-tion. Dental Update, 32, 26–32
Dickinson, C.M. & Fiske J. (2005) A review of gaggingproblems in dentistry: 2. Clinical assessment andmanagement. Dental Update, 32, 74–80.
Dootz, E.R., Koran, A. & Craig, R.G. (1993) Physicalproperty comparison of 11 soft denture lining ma-terials as a function of accelerated aging. Journal ofProsthetic Dentistry, 69, 114–19.
Ferreira, M.A., Pereira-Cenci, T., Rodrigues de Vas-concelos, L.M., Rodrigues-Garcia, R.C. & Del BelCury, A.A. (2009). Efficacy of denture cleansers ondenture liners contaminated with Candida species.Clinical Oral Investigations, 13, 237–42.
Field, E.A., Fear, S., Higham, S.M., Ireland, R.S.,Rostron, J. & Willetts, R.M. (2001) Age andmedication are significant risk factors for xe-rostomia in an English population, attend-ing general dental practice. Gerodontology, 18,21–4.
Fiske, J. & Dickinson, C. (2001) The role of acupunc-ture in controlling the gagging reflex using a re-view of ten cases. British Dental Journal, 190, 611–13.
Flink, H., Bergdahl, M., Tegelberg A., Rosenblad,A. & Lagerlof, F. (2008) Prevalence of hyposaliva-tion in relation to general health, body mass in-dex and remaining teeth in different age groupsof adults. Community Dentistry & Oral Epidemiology,36, 523–31.
General Dental Council. Maintaining Standards. Gen-eral Dental Council, London.
Goiato M.C., Pesqueira A.A., Vedovatto E., dos San-tos D.M. & Gennari F.H. (2009) Effect of differentrepair techniques on the accuracy of reposition-ing the fractured denture base. Gerodontology, 26,237–41
Guggenheimer G. & Moore P. (2003) Xerostomia.Etiology, recognition and treatment. Journal of theAmerican Dental Association, 134, 61–9
Gutteridge, D.L. (1988) The effect of including ultra-high-modulus polyethylene fibre on the impactstrength of acrylic resin. British Dental Journal, 164,177–80.
Handa, R.K., Jagger, D.C. & Vowles, R.W. (2008) Den-ture cleansers, soft lining materials and water tem-perature: what is the effect? Primary Dental Care, 15,53–8.
Hargreaves, A.S. (1975) Polymethyl methacrylate asdenture base material in service. Journal of Oral Re-habilitation, 2, 97–104.
Harrison, A., Basker, R.M. & Smith, I.S. (1989). Com-patibility of temporary soft lining materials withimmersion denture cleansers. International Journalof Prosthodontics, 2, 254–8.
Hayakawa, I., Hirano, S., Takahashi, Y. & Keh, E.N.(2000) Changes in the masticatory function of com-plete denture wearers after relining the mandibu-lar denture with a soft denture liner. InternationalJournal of Prosthodontics, 13, 227–31.
Haywood, J. Basker, R.M. Watson, C.J. & Wood, D.J.(2003) A comparison of three hard chairside relinematerials. Part I. Clinical evaluation. European Jour-nal of Prosthodontics and Restorative Dentistry, 11,157–163.
Haywood, J. Wood, D.J. Gilchrist, A. Basker, R.M.,& Watson, C.J. (2003). A comparison of threehard chairside reline materials. Part II. Changes incolour and hardness following immersion in threecommonly used denture cleansers. European Jour-nal of Prosthodontics and Restorative Dentistry, 11,165–9.
Hemmings, K.W., Schmitt, A. & Zarb, G.A. (1994)Complications and maintenance requirements inthe edentulous mandible. International Journal ofOral and Maxillofacial Implantology, 9, 191–6.
Jagger, D.C., Harrison, A. & Jandt, K.D. (1999) Thereinforcement of dentures. Journal of Oral Rehabili-tation, 26, 185–94.
Jepson, N.J.A., McCabe, J.F. & Storer, R. (1993). Agechanges in the viscoelasticity of permanent soft lin-ing materials. Journal of Dentistry, 21, 171–8.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 261
Jepson, N.J.A., McCabe, J.F. & Storer, R. (1994) Theclinical serviceability of two permanent denturesoft linings. British Dental Journal, 177, 11–16.
Jepson N.J., McGill, J.T. & McCabe, J.F. (2000) In-fluence of dietary simulating solvents on the vis-coelasticity of temporary soft lining materials. Jour-nal of Prosthetic Dentistry, 83, 25–31.
Johansson, A.K., Johansson, A., Unell L, Ekback, G.,Ordell, S. & Carlsson, G. E. (2009) A 15-yr longitu-dinal study of xerostomia in a Swedish populationof 50-yr-old subjects. European Journal of Oral Sci-ences, 117, 13–19.
Karacaer, O., Dogan, O.M., Tincer, T. & Dogan, A.(2001). Reinforcement of maxillary dentures withsilane-treated ultra high modulus polyethylenefibers. Journal of Oral Science, 43, 103–7.
Kawano, F., Dootz, E.R., Koran, A. & Craig, R.G.(1997b) Bond strength of six soft denture liners pro-cessed against polymerised and unpolymerisedpoly(methyl methacrylate). International Journal ofProsthodontics, 10, 178–82.
Kawano, F., Koran, A., Nuryanti, A. & Inoue, S.(1997a) Impact absorption of four processed softdenture liners as influenced by accelerated aging.International Journal of Prosthodontics, 10, 55–60.
Kim, S.H. & Watts, D.C. (2004). The effect of rein-forcement with woven E-glass fibers on the im-pact strength of complete dentures fabricated withhigh-impact acrylic resin. Journal of Prosthetic Den-tistry, 91, 274–80.
Kimoto, S., Kitamura, M., Kodaira, M., Yamamoto, S.,Ohno, Y., Kawai, Y., Kawara, M. & Kobayashi, K(2004) Randomized controlled clinical trial on sat-isfaction with resilient denture liners among eden-tulous patients. International Journal of Prosthodon-tics, 17, 236–40.
Klasser, G.D., Fischer, D.J. & Epstein J.B. (2008) Burn-ing mouth syndrome: recognition, understanding,and management. Oral and Maxillofacial SurgeryClinics of North America, 20, 255–71
Kostoulas I.E., Kavoura V.T., Frangou M.J. & PolyzoisG.L. (2008) The effect of length parameter on therepair strength of acrylic resin using fibres or metalwires. General Dentistry, 56, 51–5.
Lamey, P.J. (1998) Burning mouth syndrome: ap-proach to successful management. Dental Update,25, 298–300.
Lamey, P.J. & Lamb, A.B. (1988) Prospective studyof aetiological factors in burning mouth syndrome.British Medical Journal, 296, 1243–6.
Lamey, P.J., Lamb, A.B., Hughes, A., Milligan, K.A.& Forsyth, A. (1994) Type 3 burning mouth syn-
drome: psychological and allergic aspects. Journalof Oral Pathology & Medicine, 23, 216–19.
Lamey, P.J. & Lewis, M.A.O. (1989) Oral medicine inpractice: burning mouth syndrome. British DentalJournal, 167, 197–200.
Lamey, P.J., Murray, B.M., Eddie, S.A. & Freeman,R.E. (2001) The secretion of parotid saliva as stim-ulated by 10% citric acid is not related to precipi-tating factors in burning mouth syndrome. Journalof Oral Pathology & Medicine, 30, 121–4.
Lawson, W.A. & Bond, E.K. (1968) Speech and its re-lation to dentistry. Speech and speech defects. Den-tal Practitioner and Dental Record, 19, 75–81.
Lawson, W.A. & Bond, E.K. (1968) The influence oforal structures on speech. Dental Practitioner andDental Record, 19, 113–18.
Lawson, W.A. & Bond, E.K. (1969) The effects onspeech of variations in the design of dentures. Den-tal Practitioner and Dental Record, 19, 150–6.
Lechner SK, Champion, H. & Tongue, T.K. (1995)Complete denture problem solving – a survey. Aus-tralian Dental Journal, 40, 377–80.
Leung, K.C.M., McMillan, A.S., Cheung, B.P.K &Leung, W.K. (2008) Sjogren’s syndrome sufferershave increase oral yeast levels despite regular oralcare. Oral Diseases, 14, 163–73.
Lewis, M. (2009) An essential guide to xerostomia.Oral Health Report, 2, 2–6.
Locker, D. (1995) Xerostomia in older adults: a longi-tudinal study. Gerodontology, 12, 18–25.
Loney, R.W. & Moulding, M.B. (1993). The effect offinishing and polishing on surface roughness of aprocessed resilient denture liner. International Jour-nal of Prosthodontics, 6, 390–6.
Lynch, C.D. & Allen, P.F. (2006) Management ofthe flabby ridge: using contemporary materials tosolve an old problem. British Dental Journal, 200,258–261.
Maresky, L.S., van der Bijl, P. & Gird, I. (1993)Burning mouth syndrome. Evaluation of multi-ple variables among 85 patients. Oral Surgery, OralMedicine, Oral Pathology, 75, 303–7.
Marton, K., Madlena, M., Banoczy, J., Varga, G., Fe-jerdy, P., Shreebny, L.M. & Nagy, G. (2008) Unstim-ulated whole saliva flow rate in relation to siccasymptoms in Hungary. Oral Diseases, 14, 472–7.
McCabe, J.F., Basker, R.M., Murata, H. & Wollwage,P.G.F. (1996) The development of a simple testmethod to characterise the compliance and vis-coelasticity of long-term soft lining materials. Eu-ropean Journal of Prosthodontics and Restorative Den-tistry, 4, 77–81.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
262 Prosthetic Treatment of the Edentulous Patient
Murata, H. Kawamura, M., Hamada, T., Saleh, S.,Kresnoadi, U. & Toki, K. (2001) Dimensional stabil-ity and weight changes of tissue conditioners. Jour-nal of Oral Rehabilitation, 28, 918–23.
Murata, H., Murakami, S., Shigeto, N. & Hamada, T.(1994) Viscoelastic properties of tissue condition-ers – influence of ethyl alcohol content and typeof plasticizer. Journal of Oral Rehabilitation, 21, 145–56.
Mutluay, M.M. & Ruyter, I.E. (2005) Evaluation of ad-hesion of chairside hard relining materials to den-ture base polymers. Journal of Prosthetic Dentistry,94, 445–52.
Mutluay, M.M., Ogus, S., Floystrand, F., Saxegaard,E., Dogan, A., Bek, B. & Ruyter, I.E. (2008) Aprospective study on the clinical performance ofpolysiloxane soft liners: one-year results. DentalMaterials Journal, 27, 440–7.
Narva, K.K., Vallittu, P.K., Helenius, H. & Yli-Urpo,A. (2001) Clinical survey of acrylic resin removabledenture repairs with glass-fiber reinforcement. In-ternational Journal of Prosthodontics, 14, 219–24.
Niedermeier, W., Huber, M., Fischer, D., Beier, K.,Muller, N., Schuler, R., Brininger, A., Fartasch, M.,Diepgen, T., Matthaeus, C., Meyer, C. & Hector,M.P. (2000) Significance of saliva for the denture-wearing population. Gerodontology, 17, 104–18.
Oh, D.J., Lee, J.Y., Kim, Y.K. & Kho, H.S. (2008) Ef-fects of carboxymethylcellulose (CMC-based) ar-tificial saliva in patients with xerostomia. Interna-tional Journal of Oral and Maxillofacial Surgery, 37,1027–31.
Osborne, J. (1960) The full lower denture. British Den-tal Journal, 109, 481–97.
Packer M.E., Joarder, C. & Lall, B.A. (2005) The use ofrelative analgesia in the prosthetic treatment of the‘gagging’ patient. Dental Update, 32, 544–6.
Paterson, A.J., Lamb, A.B., Clifford, T.J. & Lamey, P.J.(1995) Burning mouth syndrome: the relationshipbetween the HAD scale and parafunctional habits.Journal of Oral Pathology & Medicine, 24, 289–92.
Rosted, P., Bundgaard, P., Fiske, J. & Pedersen, A.M.L.(2006) The use of acupuncture in controlling thegag reflex in patients requiring an upper alginateimpression: an audit. British Dental Journal, 201,721–5.
Scott, J. & Baum B.J. (1990) Oral effects of ageing. In:Oral Manifestations of Systemic Disease, 2nd ed., (edsJ.H. Jones & D.K. Mason), pp. 311–38. Balliere Tin-dall, London.
Seifert E., Runte, C., Riebandt, M., Lambrecht-Dinneses, A. & Bollmann, F. (1999) Can dental
prostheses influence voice parameters? Journal ofProsthetic Dentistry, 81, 579–85.
Seo R.S., Neppelenbroek K.H. & Filho J.N. (2007) Fac-tors affecting the strength of denture repairs. Jour-nal of Prosthodontics, 16, 302–10.
Shim, J.S. & Watts, D.C. (2000) An examination ofthe stress distribution in a soft-lined acrylic resinmandibular complete denture by finite elementanalysis. International Journal of Prosthodontics, 13,19–24.
Shimizu, H., Kakigi, M., Fujii, J., Tsue, F. & Takahashi,Y. (2008) Effect of surface preparation using ethylacetate on the shear bond strength of repair resinto denture base resin. Journal of Prosthodontics, 17,451–5.
Shimizu, H., Mori, N. & Takahashi, Y. (2008) Useof metal conditioner on reinforcement wires. NewYork State Dental Journal, 74, 26–8.
Ship, J.A., McCutcheon, J.A., Spivakovsky, S. & Kerr,A.R. (2007) Safety and effectiveness of topical drymouth products containing olive oil, betaine andxylitol in reducing xerostomia for polypharmacy-induced dry mouth. Journal of Oral Rehabilitation,34, 724–32.
Soh, K.I., Lee, J.Y., Chung, J.W., Kim, Y.K. & Kho H.S.(2007) Relationship between salivary flow rate andclinical symptoms and behaviours in patients withdry mouth. Journal of Oral Rehabilitation, 34, 739–44.
Svensson, P. & Kaaber, S. (1995) General health fac-tors and denture function in patients with burn-ing mouth syndrome and matched control sub-jects. Journal of Oral Rehabilitation, 22, 887–95.
Takahashi, Y., Chai, J., Takahashi, T. & Habu, T.(2000) Bond strength of denture teeth to denturebase resins. International Journal of Prosthodontics,13, 59–65.
Turner, M., Jahangiri, L. & Ship, J.A. (2008) Hypos-alivation, xerostomia and the complete denture: asystematic review. Journal of the American DentalAssociation, 139, 146–50.
van der Waal, I. (1990) The burning mouth syndrome.Munksgaard, Copenhagen.
Verran, J. & Maryan, C.J. (1997) Retention of Candidaalbicans on acrylic resin and silicone of differentsurface topography. Journal of Prosthetic Dentistry,77, 535–9.
von Bultzingslowen, I., Sollecito, T.P., Fox, P.C.,Daniels, T., Jonsson, R., Lockhart, P.B., Wray,D., Brennan, M.T., Carrozzo, M., Gandera, B.,Fujibayashi, T., Navazesh, M., Rhodus, N.L. &Schiodt, M. (2007) Salivary dysfunction associatedwith systemic diseases: systematic review and

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come
Some Clinical Problems and Solutions 263
clinical management recommendations. OralSugery, Oral Medicine, Oral Pathology, Oral Radiol-ogy & Endodontics, 103, Suppl S57, e1–15.
Wilson, H.J. & Tomlin, H.R. (1969) Soft lining materi-als: some relevant properties and their determina-tion. Journal of Prosthetic Dentistry, 21, 244–50.
Wright, P.S. (1984) The success and failure of denturesoft lining materials in clinical use. Journal of Den-tistry, 12, 319–27.
Wright, P.S. (1994) Observations on long-term use of asoft-lining material for mandibular complete den-tures. Journal of Prosthetic Dentistry, 72, 385–92.
Wright, P.S., Young, K.A., Riggs, P.D., Parker, S. &Kalachandra, S. (1998) Evaluating the effect of softlining materials on the growth of yeast. Journal ofProsthetic Dentistry, 79, 404–9.
Wright, S.M. (1979) An examination of factors asso-ciated with retching in dental patients. Journal ofDentistry, 7, 194–207.
Yemm, R. (1972) Stress-induced muscle activity: apossible etiologic factor in denture soreness. Jour-nal of Prosthetic Dentistry, 28, 133–40.
Yilmaz, H., Aydin, C., Bal, B.T. & Ozcelik, B. (2005)Effects of disinfectants on resilient denture-liningmaterials contaminated with Staphylococcus au-reus, Streptococcus sobrinus and Candida albicans.Quintessence International, 36, 373–81.
Zissis, A., Yannikakis, S., Polyzois, G. & Harrison,A. (2008) A long term study on residual monomerrelease from denture materials. European Jour-nal of Prosthodontics and Restorative Dentistry, 16,81–4.

P1: JZP Trim: 246mm X 189mmc16 BLBK351-Basker January 4, 2011 8:3 Printer Name: Yet to Come

P1: JZP Trim: 246mm X 189mmind BLBK351-Basker November 30, 2010 21:33 Printer Name: Yet to Come
Index
abrasion, 215acid cleaners, 217adhesion, 59advice to patient, 212
appearance, 213cleaning dentures, 214controlling dentures, 213initial sensations, 213limitations of dentures, 213soreness, 214wearing dentures at night, 214
ala-tragal line, 180alginate, 136–7, 145–6alkaline peroxide cleaners, 217Alma gauge, 98, 100alveolectomy, 50alveolotomy, 49angular stomatitis (angular cheilitis), 119–21antifungal preparations, 118appearance
assessing in trial dentures, 196–9creating a natural appearance, 196–9influencing outcome of treatment, 22–4lip support, 98obvious change in, 213
articulating paper, 207–8articulators, 194–9attitudes to tooth loss and dentures,
31–2
balanced articulation, 207–9balanced occlusion, 193–4, 200–01, 207–8Bennett angle, 197biometric design, 88bone (see also mandible; maxilla)
genial tubercles, 124–5mylohyoid ridge, 124–5pathology within, 123–4resorption
causes of, 5–7long-term changes, 223reducing risk, 6
sharp, irregular, 124tooth unerupted, 124tori, 126undercut ridges 62, 125
border seal, 61–2bruxism. See parafunctionBULL rule, 209burning mouth syndrome, 254–7
cancer, 83–4, 223Candida albicans, 113, 120, 233, 241–7, 255check record, 210–12
articulating the dentures, 211recording jaw relations, 211
cleaning dentures, 214–7, 238, 241–2immersion cleansers, 216mechanical cleaning, 215
265

P1: JZP Trim: 246mm X 189mmind BLBK351-Basker November 30, 2010 21:33 Printer Name: Yet to Come
266 Index
cleaning dentures (cont.)types of cleanser, 216
acid, 217effervescent, 217hypochlorite, 216other, 217
clearance of teeth, 33without immediate provision of dentures,
51–2clinical audit, 82closest speaking distance, 193cohesion, 59condylar angle, 193condylar axis, 193condylar path, 193copy dentures
communication with dental technician, 107copy template, 106–7indications, 22, 88, 104–6quality control and enhancement, 108–9stages of treatment, 107
coronoid process, 134cross-infection control, 78–9
dental health surveys, 224dental laboratory
communication with, 77, 107, 139, 148, 171cross-infection control, 83–4
denture(s) See copy dentures; existing dentures;immediate dentures; overdentures
abrasion of, 215adapting to, 21–4, 223advice to patient, 212–7appearance, 195–9base, hypersensitivity to, 256base materials, 247–9
cobalt-chromium, 248modified polymeric, 248reinforced, 248
breakagescauses, 215–6debonding of teeth, 249–50fatigue fracture, 245impact fracture, 245mid-line fracture, 245
cleansers, 128, 216–7
cleanliness, 222control of, 23, 58–9, 174, 213deposits on, 214designing, approaches to, 88disinfection, 117faults, 229fixative, 63fracture. See breakageshyperplasia, 122identification markers, 199–200
inclusion markers, 200surface markers, 200
immediate. See immediate denturesimpression surface, 85inclusion markers, 200instability, 228–9limitations
mastication, 8–9replacing bone, 5restoring appearance, 7
marking dentures. See identificationmarkers
mid-line fracture, 142, 245need for treatment, 15occlusal surface, 85, 204pain under, 228–32plaque, 125, 127, 222polished surface, 85predicting outcome of treatment,
25–28rebasing, 225relining, 224repairing, 246–7success rate of treatment, 24–5surfaces
impression, 85occlusal, 85polished, 85
surface markers, 200training, 252–3transitional partial, 36trial, 189–201wearing at night, 214
denture-bearing areas, 130–35assessment of, 84
denture-induced hyperplasia, 122–3

P1: JZP Trim: 246mm X 189mmind BLBK351-Basker November 30, 2010 21:33 Printer Name: Yet to Come
Index 267
denture stomatitis, 111–8diabetes, 12, 113,
edentulousness. See total tooth losselderly people. See older peopleexisting dentures, use of in
diagnosis, 91–2examination of, 85–7impression procedures, 95–7modifying a jaw relationship, 93–5positioning post-dam, 101recording jaw relations, 97–100selecting teeth, 100treatment of inflammation, 93
extraction of teeth, factors influencing decision,33–5
face bow, 169facial seal, 61fitting dentures, 203–19
impression surface assessment, 203–4objectives, 203occlusal surface assessment, 204
clinical errors, 206laboratory errors, 205
quality control and enhancement, 218retention and stability assessment, 204
flabby ridge, 242–5causes, 242management, 243–5
floor of mouth, 133folic acid deficiency, 13, 83foveae palatinae, 131Fox’s occlusal plane indicator, 156Frankfort plane, 167,freeway space. See mandibular positionsfrena, prominent, 123fixative, 63functional impression materials. See soft lining
materials
gagging, 250–54genial tubercles, 124
habituation, 22hamular notch, 131, 135
hyperplasiadenture-induced, 122–3palatal inflammatory papillary, 118
hypochlorite cleanser, 216, 238, 284, 241–2
imbibition, 137immediate dentures, 44–51
advantages, 45clinical and technical procedures, 48–50
alveolectomy, 50–51alveolotomy, 49–50flanged dentures, 49–50impressions, 49open-face dentures, 48
contraindications, 51disadvantages, 46types of, 46–8
flanged, 46–8open face, 46–8
implant-supported overdentures, 41–4implant design, 41impression technique, 43–4placement of implants, 42–3success rates, 41–2
impressions, 130–49master impressions, 140–49
alginate, 145–6border-trimming materials, 145elastomers, 148impression materials/techniques, 145impression plaster, 147–8mucostatic/mucodisplacive techniques,
140–41special trays, 141–5
border-trimming materials, 145checking, 143close fitting, 142correction, 143–4diagnostic impression, 143spaced, 142stops, 142–3
preliminary impressions, 152–8impression material and techniques,
136–9alginate, 136–7
dimensional instability, 137

P1: JZP Trim: 246mm X 189mmind BLBK351-Basker November 30, 2010 21:33 Printer Name: Yet to Come
268 Index
impressions (cont.)imbibition, 137syneresis, 137
alginate wash technique, 138border moulding, 136–7impression compound, 138
laboratory prescription, 139quality control and enhancement, 140stock trays, 134, 136
‘wash’ impression, 95zinc oxide-eugenol paste, 166–8
impression plaster, 168–9impression surface, 55–6, 85, 203incisal relationship, 174–80
causes of failure due to, 174–80communication with dental technician, 188quality control and enhancement, 188preventing failure by
adjusting the record rims, 183–5assessing the patient, 180–83
pre-extraction records, 187relevance of natural, 174–6
incisive papilla, 147–8inclusion markers, 200injection moulding, 206intercuspal position, 68, 70inter-occlusal rest space, 70interpupillary line, 156iron deficiency, 13, 83, 113, 120, 229, 255
jaw relations, recording, 150–61communication with dental technician, 172lower record rim adjustment, 158occlusal vertical dimension, reassessing, 158quality control and enhancement, 172record blocks, 154–5rest vertical dimension, 150–3
two-dot technique, 152Willis gauge, 151–2
retruded jaw relationship, recording,159–61
upper record rim adjustment, 155–8
magnets, 38mandible. See also bone
tori, 141–3
mandibular positions, basic, 68–70centric occlusion, 70centric relation, 70freeway space (inter-occlusal rest space), 70intercuspal position, 70, 73muscular position, 70, 73–4reference positions, 74rest position, 70–73
clinical significance, 69control of, 70–72tongue effect on, 72variables effecting 72–3
retruded arc of closure, 72–3retruded contact position, 69–70, 74retruded jaw relation, 74
marking dentures, 199–200inclusion markers, 200surface markers, 200
masseter muscle, 132maxilla. See also bone
pattern of resorption, 89prominent tuberosities, 125
mentalis muscle, 131modiolus, 132mouth. See oral cavitymucodisplacive impression techniques, 140–41mucostatic impression techniques, 140–41mylohyoid ridge, 124
nasolabial angle, 157neutral zone (zone of minimal conflict), 65
assessing in trial dentures, 192impression, 88, 185–7
nutrition, 14, 112
occlusal errorclinical causes, 206–12
correction, 207–12identification, 207
laboratory causes, 205correction, 205–6
occlusal surface, 55, 85assessment of, 204
occlusal vertical dimension, 69–70, 73–4, 183assessing in trial dentures, 193inadequate, 134

P1: JZP Trim: 246mm X 189mmind BLBK351-Basker November 30, 2010 21:33 Printer Name: Yet to Come
Index 269
older peopleage changes in systems, 11
in denture-bearing tissues, 12in muscles, 12
biological age, 27–8, 87characteristics of normal ageing, 18communication, 17–18condition of dentures, 16demographic changes, 9–10drug therapy, 14nutrition, 15, 126practical points in care, 16–18psychiatric disorders, 13psychological changes, 14–15systemic diseases, 12–13
oral cavitycancer, 83–4, 223preparation of, 111–26reduced air pressure, 71
overdenturesadvantages, 37–8disadvantages, 39implant-supported 41–4maintenance, 40–41technique, 39–40tooth-supported, 33, 37–40
palatal gingival vestige, 130–32, 135palatal inflammatory papillary hyperplasia,
118–19palatal relief, 126, 162–3palatal rugae, 131palatine torus, 131parafunction, 228–30, 256Parkinson’s disease, 12, 256patient assessment, 80–90
complaints, 220–21diagnosis, 88examination,82–7
dentures, 85–8extra-oral, 82–3, 221–2intra-oral, 83–5
history, 80–82dental, 80–81medical, 81social, 82
prognosis, 90treatment plan, 88–9
pear-shaped pad, 131, 133, 140, 142, 144, 189peer review, 77polished surface, 55, 85post-dam, 61–2, 101, 153–4pre-extraction records, 187pressure-disclosing materials, 222
radiographs, 124rebasing, 225–6recall procedures, 217, 220–26
long-term recall, 222–4short-term recall, 220–22
relief (palatal), 126, 162–3relining, 224–6relining materials, 226–42
hard, 226, 234–5soft long term, 238–42soft short term, 235–8
residual monomer, 126, 255rest vertical dimension, 69, 73–4retention, 56–62, 204
muscular forces, 56designing dentures for, 57patient skills, 57–8
physical forces, 59–61adhesion, 59cohesion, 59obtaining optimum, 61–2
accuracy of fit, 62area of impression surface, 62bony undercuts, 62border seal, 61facial seal, 61–2fixative, 63post-dam, 61–2soft liners, 63springs, 64
surface tension, 59viscosity, 60
retromolar pad, 131, 133
saliva, 14artificial, 233functions of, 230–32

P1: JZP Trim: 246mm X 189mmind BLBK351-Basker November 30, 2010 21:33 Printer Name: Yet to Come
270 Index
saliva (cont.)influence on retention, 59–61lack of, 230–34
associated with burning mouth syndrome,256
viscosity, 60soft lining materials
assisting retention, 63long term, 238–42
adjustment, 242cleaning, 241–2comparison of types, 240indications for use, 239types, 239
short term, 235–8cleaning, 238clinical applications, 237–8composition, 235functional impression, 95, 237–8relevant properties, 236–7temporary soft lining, 238tissue conditioning, 237
special tray, 141–4speech disturbance, 257–9split-cast technique, 205–6stability, 56–70
assessing, 86–7displacing forces, 64–6
gravity, 66through the occlusal surface,
64–5through the polished surface,
65–6neutral zone, 65zone of minimal conflict, 65
retentive forces, 55–60support, 66–7
Staphylococcus aureus, 120stock tray, 134–6sulci, shallow, 121–2
prosthetic treatment, 121surgical treatment, 122
sulcus tissues, anatomy, 131supporting cusps, 209surface markers, 200surface tension, 59
syneresis, 137systemic disease, detecting, 83
tardive dyskinesia, 13teeth, artificial
arrangement, 165–6choice of, 163–5debonding, 249–50material, 166–7selection of posterior, 171use of existing denture, 100
tissue-conditioning materials. See soft liningmaterials
tonguedefensive, 192papillary changes, 83tongue thrust endogenous, 182
tori, 126total tooth loss
adults in 1998, 1–2in other countries, 4mental barriers to, 2psychological effects, 22rate of, 2trends over 30 years, 3
transition from natural to artificialdentition
methods, 33reaction of patient, 32
try-in procedures, 189–201assessment, articulator, 189–91
impression surface, 189occlusal surface, 190polished surface, 190
assessment, mouth, 191–9appearance, 196–9base extension, 191neutral zone, 192occlusal vertical dimension, 193occlusion, 194–5retention and stability, 191
communication with dental technician,200
quality control and enhancement,200
two-dot technique, 152–3

P1: JZP Trim: 246mm X 189mmind BLBK351-Basker November 30, 2010 21:33 Printer Name: Yet to Come
Index 271
vibrating line, 131–2viscosity of saliva, 60–61vitamin B complex deficiency, 13, 83, 113, 255vitamin C deficiency, 15, 113, 120
Willis gauge, 151–2
xerostomia. See saliva
zinc oxide-eugenol paste, 146, 226zone of minimal conflict (neutral zone), 65,
88–9, 192zygomatic process, 135