Prognostic factors for ARDS: clinical, physiological and ...
12
RESEARCH ARTICLE Open Access Prognostic factors for ARDS: clinical, physiological and atypical immunodeficiency Min Song 1,2 , Yijie Liu 1 , Zhiwen Lu 3 , Hong Luo 1,2* , Hong Peng 1,2 and Ping Chen 1,2 Abstract Background: Risk factors affecting the prognosis of acute respiratory distress syndrome (ARDS) in adults were investigated. The aim was to identify new predictors for ARDS patient prognosis, including those with clinical, pathophysiological, and atypical immunodeficiency. Methods: ARDS patients were retrospectively included. The patients were grouped and analysed according to different oxygenation index grades and prognosis, and factors influencing prognosis and survival were examined. Adolescent patients, patients with typical immunodeficiency and patients who died within 24 h after being diagnosed with ARDS were excluded. The predictive value for mortality was determined by Cox proportional hazard analysis. Results: In total, 201 patients who fulfilled the Berlin definition of ARDS were included. The severity of critical illness on the day of enrolment, as measured by the Acute Physiology and Chronic Health Evaluation (APACHE) II score (P = 0.016), Sequential Organ Failure Assessment (SOFA) score (P = 0.027), and PaO 2 /FiO 2 (P = 0.000), worsened from mild to severe ARDS cases. Compared with survivors, non-survivors were significantly older and had higher APACHE II and SOFA scores. Moreover, significantly lower lymphocyte/neutrophil ratios and leukocyte counts were found among non-survivors than survivors (P = 0.008, P = 0.012). A moderate positive correlation between the lymphocyte/ neutrophil and PaO 2 /FiO 2 ratios (P = 0.023) was observed. In predicting 100-day survival in patients with ARDS, the area under the curve (AUC) for the lymphocyte/neutrophil ratio was significantly higher than those for the PaO 2 / FiO 2 ratio alone, body mass index (BMI) alone, and the lymphocyte count alone (P = 0.0062, 0.0001, and 0.0154). Age (per log 10 years), BMI < 24, SOFA score, leukocyte count, and the lymphocyte/neutrophil ratio were independent predictors of 28-day mortality in ARDS patients. Additionally, ARDS patients with a lymphocyte/ neutrophil ratio < 0.0537 had increased 28-day mortality rates (P = 0.0283). Old age affected both 28-day and 100- day mortality rates (P = 0.0064,0.0057). (Continued on next page) © The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data. * Correspondence: [email protected] 1 Department of Pulmonary and Critical Care Medicine, The Second Xiangya Hospital, Central South University, No.139 Renmin Road, Changsha 410011, Hunan, China 2 The Respiratory Disease Research Institute of Hunan Province; The Respiratory Disease Diagnosis and Treatment Center of Hunan Province, No.139 Renmin Road, Changsha 410011, Hunan, China Full list of author information is available at the end of the article Song et al. BMC Pulmonary Medicine (2020) 20:102 https://doi.org/10.1186/s12890-020-1131-0
Transcript of Prognostic factors for ARDS: clinical, physiological and ...

RESEARCH ARTICLE Open Access
Prognostic factors for ARDS: clinical,physiological and atypicalimmunodeficiencyMin Song1,2, Yijie Liu1, Zhiwen Lu3, Hong Luo1,2*, Hong Peng1,2 and Ping Chen1,2
Abstract
Background: Risk factors affecting the prognosis of acute respiratory distress syndrome (ARDS) in adults wereinvestigated. The aim was to identify new predictors for ARDS patient prognosis, including those with clinical,pathophysiological, and atypical immunodeficiency.
Methods: ARDS patients were retrospectively included. The patients were grouped and analysed according todifferent oxygenation index grades and prognosis, and factors influencing prognosis and survival were examined.Adolescent patients, patients with typical immunodeficiency and patients who died within 24 h after beingdiagnosed with ARDS were excluded. The predictive value for mortality was determined by Cox proportionalhazard analysis.
Results: In total, 201 patients who fulfilled the Berlin definition of ARDS were included. The severity of critical illnesson the day of enrolment, as measured by the Acute Physiology and Chronic Health Evaluation (APACHE) II score(P = 0.016), Sequential Organ Failure Assessment (SOFA) score (P = 0.027), and PaO2/FiO2 (P = 0.000), worsened frommild to severe ARDS cases. Compared with survivors, non-survivors were significantly older and had higher APACHEII and SOFA scores. Moreover, significantly lower lymphocyte/neutrophil ratios and leukocyte counts were foundamong non-survivors than survivors (P = 0.008, P = 0.012). A moderate positive correlation between the lymphocyte/neutrophil and PaO2/FiO2 ratios (P = 0.023) was observed. In predicting 100-day survival in patients with ARDS, thearea under the curve (AUC) for the lymphocyte/neutrophil ratio was significantly higher than those for the PaO2/FiO2 ratio alone, body mass index (BMI) alone, and the lymphocyte count alone (P = 0.0062, 0.0001, and 0.0154).Age (per log10 years), BMI < 24, SOFA score, leukocyte count, and the lymphocyte/neutrophil ratio wereindependent predictors of 28-day mortality in ARDS patients. Additionally, ARDS patients with a lymphocyte/neutrophil ratio < 0.0537 had increased 28-day mortality rates (P = 0.0283). Old age affected both 28-day and 100-day mortality rates (P = 0.0064,0.0057).
(Continued on next page)
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] of Pulmonary and Critical Care Medicine, The Second XiangyaHospital, Central South University, No.139 Renmin Road, Changsha 410011,Hunan, China2The Respiratory Disease Research Institute of Hunan Province; TheRespiratory Disease Diagnosis and Treatment Center of Hunan Province,No.139 Renmin Road, Changsha 410011, Hunan, ChinaFull list of author information is available at the end of the article
Song et al. BMC Pulmonary Medicine (2020) 20:102 https://doi.org/10.1186/s12890-020-1131-0

(Continued from previous page)
Conclusions: Age (per log10 years), BMI < 24, SOFA score, lymphocytes, and the lymphocyte/neutrophil ratio wereindependent predictors of 100-day mortality in patients with ARDS. The lymphocyte/neutrophil ratio may representa potential molecular marker to evaluate atypical immunosuppression or impairment in patients with ARDS.
Keywords: Acute respiratory distress syndrome, Morbidity, Outcome assessment, Prognostic
BackgroundAcute respiratory distress syndrome (ARDS) is a life-threatening respiratory disease with a high mortality ratein critically ill patients [1, 2]. Although many in-depthstudies on ARDS have been conducted, the specificpathogenesis and prognostic factors of the disease re-main unclear. Indeed, despite improvements in ventila-tory techniques and extensive research to date, ARDScontinues to be associated with high mortality [3, 4].Nonetheless, clinical and animal studies have shown
that the activation of multiple inflammatory cells andthe release of inflammatory mediators play importantroles in the development and outcome of ARDS [5]. Theinvolvement of immune cells, including neutrophils [6,7] lymphocytes [8], and regulatory T-cell [9, 10], has be-come an active topic of research in ARDS pathogenesis.To date, few clinical studies on the immune status ofARDS patients have focused on aetiology, treatment andprognosis [11]. Immunocompromised individuals repre-sent a significant proportion of ARDS patients [11, 12],these patients do not have the ability to respond nor-mally to an infection due to an impaired or weakenedimmune system. Some studies have shown that ARDSoccurs in patients with previous immunodeficiencies,such as haematologic malignancies, active solid tu-mours, solid organ transplantation, and acquired im-munodeficiency syndrome, as well as in patientstaking long-term or high-dose corticosteroids or im-munosuppressants, and those who use extra-corporealmembrane oxygenation (ECMO) may have a betterprognosis [13]. Compared with immunocompetentsubjects, ARDS patients with typical immunodefi-ciency have higher mortality regardless of ARDS se-verity [11]. In addition, atypical immunosuppression isfrequently found among ARDS patients, and virus in-fections are also increasingly being reported in ARDSpatients without typical immunosuppression [13].Overall, there is currently a lack of uniform molecularmarkers for patients with atypical immunosuppressionor impaired status. Furthermore, it is not well knownwhether the status of atypical immunodeficiency af-fects the prognosis of ARDS. Managing patients withatypical immunosuppression in intensive care unit(ICU) can be challenging, updated epidemiologicaland outcomes studies are needed to evaluate the con-dition of these patients.
This aim of our study was to identify a convenient andeasy-to-use molecular biomarker to detect and evaluatethe status of patients with atypical immunosuppressionin ARDS patients.
MethodsStudy design and patientsThis retrospective observational cohort study was con-ducted with ARDS patients hospitalized in the criticalcare centre of a university-based tertiary care hospital(The Second Xiangya Hospital of Central South Univer-sity) in Hunan, China, from January 2011 to August2018. Institutional approval was provided by the SecondXiangya Hospital of Central South University BiomedicalResearch Ethics Committee (Hunan, China). Written in-formed consent was waived because of the retrospectiveobservational design. All patient data were anonymouslyrecorded to ensure confidentiality.
Inclusion and exclusion criteriaPatients admitted to the critical care centre with a diag-nosis of ARDS based on the 2012 Berlin definition [14]were included in our study if they met the inclusion cri-teria and none of the exclusion criteria. All eligible pa-tients were over 18 years old with available neutrophiland lymphocyte count results within 24 h after ICU ad-mission. Patients who were repeatedly admitted to theICU, lack of neutrophil and lymphocyte records, hadchronic haematological disorders, were under the age of18 years, or died within 24 h of receiving a diagnosis ofARDS were excluded. In addition, we excluded patientswho were defined as having an immunodeficiency withthe following aetiologies: (1) haematological malignan-cies, (2) active solid tumours or specific anti-tumourtreatment within a year, (3) solid organ transplant, (4)acquired immunodeficiency syndrome (AIDS), or (5)long-term or high-dose corticosteroid (CS) or immuno-suppressant (IS) therapy. Long-term CS therapy was de-fined as > 7.5 mg of prednisone/day for > 3 months, anda high dose was defined as > 1mg/kg for > 1 week withinthe previous 3 months. According to the PaO2/FiO2 ra-tio, patients were categorized as mild (200 mmHg<PaO2/FiO2 ≤ 300 mmHg, n = 31), moderate (100 mmHg<PaO2/FiO2 ≤ 200 mmHg, n = 61), and severe (PaO2/FiO2 ≤ 100mmHg, n = 109) groups. In addition, 201 patients wereincluded and divided into a survivor group (n = 80) and
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 2 of 12

a non-survivor group (n = 121) according to the finalclinical results.
Data extraction and outcomeDemographic and baseline characteristics such as age,sex, body mass index (BMI), ARDS risk factors, severityof illness upon admission to the ICU (Acute Physiologyand Chronic Health Evaluation (APACHE) II score)[15], and the Sequential Organ Failure Assessment(SOFA) score [16] were recorded and analysed. We re-corded routine blood examination results within 24 hand within 3 days after ICU admission. Two authorscompleted the data collection independently. The pri-mary outcome was mortality, and the secondary out-comes were ICU mortality and hospital mortality. Wealso calculated 28-day mortality and 100-day mortalityrates.
Blood measurements and flow cytometric analysisThe white blood cell count, C-reactive protein (CRP)level and procalcitonin (PCT) level were measured.Serum levels of haemoglobin, albumin, immunoglobulins(IgG, IgA, IgM, IgE), and complement components (C3,C4) (R&D Systems, USA) was determined by enzyme-linked immunosorbent assay (ELISAs) in accordancewith the manufacturer’s instructions. To analyse T-lymphocytes, cell staining kit (BD ingen™, USA) was usedto detect CD4 + CD8 + CD3 + cells according to themanufacturer’s protocol. Briefly, peripheral blood mono-nuclear cells (PBMCs) were incubated with a mixture ofluciferin isothiocyanate anti-CD4 and apc anti-CD8 at4 °C for 30 min. Facscalibur flow cytometry (BD Biosci-ences, USA) and CellQuest software (BD Biosciences,USA) were used for flow cytometry analysis. A homo-type control was used to ensure antibody specificity [17,18].
Statistical analysisWe used the Kolmogorov-Smirnov test to assess distri-bution normality. The continuous variables were re-ported as the mean ± SD or median (IQR). Anindependent samples t-test was used to evaluate nor-mally distributed data, and the Mann-Whitney test wasemployed to evaluate non-normally distributed datawhen comparing two groups. In multi-group compari-sons, one-way ANOVA and Kruskal-Wallis test wereused to analyze the normal and non-normal distributiondata respectively, and the P-values adjusted by Bonfer-roni were used for multiple groups of comparison. Clas-sification data number (percentage) aggregation, andChi-square or Fisher’s exact test. Spearman’s rank cor-relation was adopted to determine correlations amongvariables. Area under the curve operating characteristic(ROC) was used to evaluate the prognostic value of the
subject properties, diagnostic and test parameters. Thecut-off point was obtained by determining the optimalden index (sensitivity+specificity-1). We used Kaplan-Meier plots and log-rank tests to compare the survivalrate of each group. To calculate an independent pre-dictor of mortality of 100 days, with a stepwise binary lo-gistic regression variables for the regression values ofP < 0.05 (one variable was entered when P < 0.05, andone was deleted when P > 0.10). The odds ratio (OR), P-value and 95% CI were used to represent results. Alltests were double-tailed, and P < 0.05 was consideredstatistically significant. All analyses were performededusing IBM SPSS 22.0 and MedCalc v.11.0.
ResultsBaseline characteristics and patient outcomeA total of 201 patients meeting the Berlin definitionof ARDS from January 2011 to August 2018 were in-cluded in this study. Characteristics at enrolment andoutcomes of the study population are shown inTable 1 and Table 2. There were no statistically sig-nificant differences in age, sex or BMI among themild, moderate and severe ARDS groups. The mostcommon aetiologies of ARDS were pneumonia, sepsisand pancreatitis. According to the APACHE II score(P = 0.016), SOFA score (P = 0.027), and PaO2/FiO2
(P = 0.000), it can be seen that the severity of criticalillness on the day of enrolment worsened from mildto severe ARDS, as shown in Tables 1 and 2. The100-day mortality rate for patients with ARDS was60.2% (121/201). Compared to non-survivors, the sur-vivors were significantly younger, with relatively lowscores for APACHE II and SOFA. Survivors hadhigher BMIs and PaO2/FiO2 ratios than did non-survivors.
Correlations of the lymphocyte/neutrophil ratio withdisease severity and outcomeCompared with the mild group, the frequencies oflymphocyte cells were decreased in severe ARDS pa-tients (P = 0.025). Moreover, the lymphocyte/neutro-phil ratio decreased progressively with increasingARDS severity (P = 0.001). Among non-survivors, asignificantly lower lymphocyte/neutrophil ratio wasfound compared with that of survivors (P = 0.008)(Table 2), the frequencies of lymphocyte cells werelower than those in survivors (P = 0.025) (Table 2),andthe frequencies of leukocytes and neutrophil cellswere both higher than those in survivors (P = 0.012,0.016) (Table 2). There were no significant differencesamong the three severity groups in terms of the fre-quencies of leukocytes and neutrophils (Table 1).
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 3 of 12

Table 1 Baseline characteristics of the enrolled study population. Normally distributed quantitative data are expressed as means±standard deviation. Non-normally distributed quantitative data are expressed as medians (IQR)
Variables Acute respiratory distress syndrome ΔP-value
Total Mild Moderate Severe
Number 201 31 61 109
Age,years 54.24 ± 16.35 55.38 ± 15.60 52.43± 54.93 ± 16.03 0.579
Sex,male/female,n 130/71 19:12 40/21 71/38 0.415
BMI,kg/m2 23.90 ± 3.82 24.22 ± 3.93 23.83 ± 4.05 23.90 ± 3.82 0.896
Cause of ARDS
Pneumonia 125 19 37 69
Non-pulmonary spesis 38 6 15 17
Pancreatitis 15 4 7 4
Trauma 7 0 0 7
Aspiration 2 0 0 2
Others 14 2 2 10
APACHE II score 14.19(7.69 to 31.00) 12.74(7.69 to 24.37) 14.52 (9.86 to 27.69) 14.34 (9.68 to 31.00)* 0.016
SOFA score 4.98(4.65 to 5.30) 4.59(3.97 to 5.20) 5.11 (4.71 to 5.53) 5.26 (4.89 to 5.63) 0.027
PaO2/FiO2,mmHg 123 (112 to 134) 280 (267 to 294) 140 (132 to 146)* 69 (65 to 72)* # 0.000
CRP,mg/L 129.82 (129.82 to169.91)
110.09 (76.59 to143.59)
163.90 (138.67 to189.14)*
203.33 (115.97 to290.68)*
0.011
PCT,ng/ml 12.20 (8.12 to 16.29) 9.37 (5.45 to 13.30) 10.15 (1.51 to 18.80) 17.05 (7.58 to 27.73)* 0.175
Albumin,g/L 27.67 ± 5.82 27.13 ± 3.17 27.07 ± 6.05 28.10 ± 6.05* 0.759
Hemoglobin,g/L 107.67 ± 28.32 104.04 ± 23.76 107.29 ± 28.05 108.82 ± 29.73 0.759
Leukocytes,109/L 11.33(10.12 to 12.54) 10.98 (8.67 to 13.28) 10.91 (9.62 to 12.22) 13.65 (8.65 to 18.64) 0.298
Lymphocytes,109/L 1.10 (0.95 to 1.26) 1.28 (0.86 to 1.75) 1.10 (8.67 to 13.28) 1.07 (0.87 to 1.27)* 0.025
Neutrophils,109/L 10.78 (8.38 to 13.18) 8.35 (6.91 to 9.78) 11.66 (7.59 to 15.74) 13.03 (7.31 to 18.76) 0.371
Lymphocyte/Neutrophil ratio 0.19 ± 0.03 0.35 ± 0.23 0.17 ± 0.03* 0.15 ± 0.02* 0.001
Virus infection,n,% 23(11.44%) 1(3.23%) 10(16.39%) 12(11.0%)
28-day mortality,n,% 103(51.24%) 13(41.94%) 31(50.82%) 59(54.13%)
100-day mortality,n,% 121(60.20%) 15(48.39%) 37(60.66%) 69(63.30%)
Immunoglobulin
IgG,g/L 10.87 ± 1.86 11.71 ± 4.96 10.82 ± 1.94 10.59 ± 5.36 0.095
IgA,g/L 1.98 ± 0.24 1.92 ± 1.09 1.85 ± 0.72 2.11 ± 1.40 0.270
IgM,g/L 1.05 ± 0.86 1.32 ± 1.18 1.02 ± 0.92 1.00 ± 0.72 0.598
IgE,ng/mL 620.36 ± 145.11 1426.20 ± 119.89 640.55 ± 32.45 356.87 ± 78.73* 0.025
Complement components
C3 5.62 ± 1.78 12.27 ± 1.83 7.13 ± 3.14 0.84 ± 0.33* 0.186
C4 1.33 ± 0.58 0.25 ± 0.13 0.24 ± 0.11 2.25 ± 0.95* 0.663
T-lymphocytes subsets
CD3+ cells,% 62.75 ± 15.29 71.00 ± 13.78 63.35 ± 12.44 60.62 ± 17.11 0.229
CD4+ cells,% 35.15 ± 15.48 36.40 ± 13.69 34.10 ± 11.14 35.66 ± 8.47 0.951
CD4+ cells count (PCS/ul) 383.20 ± 67.18 176.50 ± 67.18 383.67 ± 94.79 434.08 ± 78.66 0.708
CD8+ cells,% 27.33 ± 13.46 34.33 ± 6.37 25.60 ± 11.59 26.92 ± 14.01 0.275
CD8+ cells count (PCS/ul) 212.33 ± 64.30 134.00 ± 30.63 286.67 ± 51.72 178.91 ± 70.96 0.409
CD4+/CD8+ ratio 1.95 ± 0.26 1.29 ± 0.23 1.91 ± 0.93 2.14 ± 0.48 0.623
B-lymphocytes
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 4 of 12

Alterations in inflammatory biomarkers,immunoglobulins, complement components, circulatingT-lymphocyte cells, B-lymphocyte cells and NK cells inARDSCRP levels progressively increased with increasingARDS severity (P = 0.011). The PCT level of patientswith severe ARDS was higher than that of patientswith mild ARDS (P = 0.002). Interestingly, thelymphocyte count decreased as the severity of ARDSincreased (P = 0.025) (Table 1). In addition, comparedwith survivors, non-survivors were older (P = 0.004),and had higher leukocyte and neutrophil counts (P =0.012, 0.016) and lower BMI, lymphocyte counts andlymphocyte/neutrophil ratios (P = 0.027, 0.025, and0.008) (Table 2). CRP and PCT levels in the twogroups were similar (Table 2).The peripheral blood immunoglobulin IgE and
complement C3 levels in patients with mild ARDSwere significantly higher than those in patients withsevere ARDS (P = 0.023, 0.019). Moreover, the levelsof immunoglobulin IgE and complement C3 in non-survivors were lower than in survivors (P = 0.009,0.018) (Table 2). Peripheral blood complement C4levels in patients with mild ARDS were significantlylower than those in patients with severe ARDS (P =0.026) (Table 1), but the level of complement C4was similar between survivors and non-survivors(Table 2).The level of peripheral blood B-lymphocyte cells was
significantly lower in non-survivors than in survivors(P = 0.009), as was the level of peripheral blood CD8+cells (P = 0.024), though the levels of both peripheralblood B-lymphocyte cells and CD8+ cells were similar inthe three groups (Table 1). In addition, the proportionsof CD3+ cells, CD4+ cells, and NK cells and the CD4+/CD8+ ratio in peripheral blood showed no significantdifferences among the three groups of ARDS patientsstratified by oxygenation index or between the survivorand non-survivor groups.
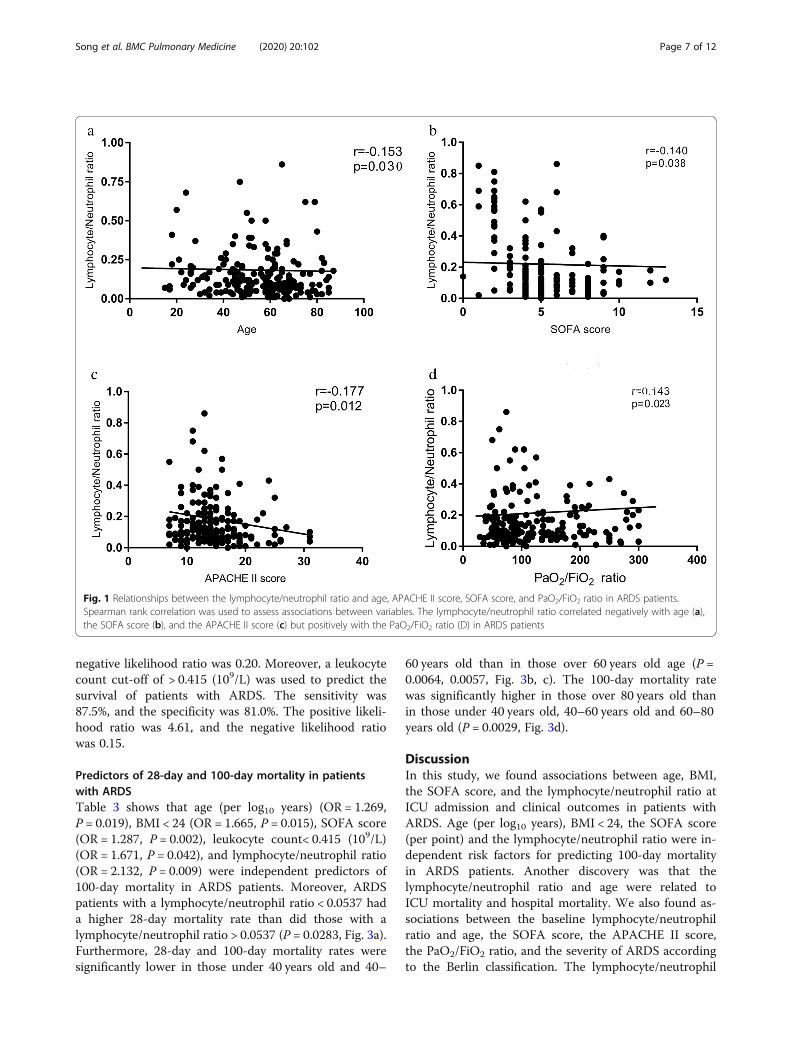
Correlations of lymphocytes, the lymphocyte/neutrophilratio, immunoglobulin IgE levels, complement C3 levels,T-CD8+ lymphocyte levels and B-lymphocyte levels withdisease severity and outcomeWe noted that in all ARDS patients, the lymphocyte/neutrophil ratio was moderately negatively correlatedwith age (r = − 0.153, P = 0.030, Fig.1a), SOFA score (r =− 0.140, P = 0.038, Fig.1b), and the APACHE II score(r = − 0.177, P = 0.012, Fig.1c). We also observed that,there is a moderate positive correlation between thelymphocyte/neutrophil ratio and PaO2/FiO2 ratio (r =0.143, P = 0.023, Fig.1d). Moreover, significant mild posi-tive correlations were found between the lymphocytecount and BMI (r = 0.145, P = 0.041), the lymphocytecount and the PaO2/FiO2 ratio (r = 0.110, P = 0.121), theimmunoglobulin IgE level and the PaO2/FiO2 ratio (r =0.288, P = 0.036), the C3 level and BMI (r = 0.342, P =0.026), the T-CD8+ lymphocyte count and the lympho-cyte count (r = 0.755, P = 0.001), the B-lymphocyte countand BMI (r = 0.588, P = 0.013), and the B-lymphocytecell count and lymphocyte count (r = 0.582, P = 0.014).The area under the ROC curve (AUC) for the lympho-
cyte/neutrophil ratio for the prediction of 100-day sur-vival in ARDS patients was 0.721 (95% CI 0.653 to0.782) and was significantly higher than the AUC for thePaO2/FiO2 ratio alone (0.625, 95% CI 0.554 to 0.692,P = 0.0062,), the AUC for BMI alone (0.593, 95% CI0.521 to 0.661, P = 0.0001) or the AUC for the lympho-cyte count alone (0.592,95% CI 0.520 to 0.660, P =0.0154) (Fig.2). The AUC for the lymphocyte/neutrophilratio in combination with the lymphocyte count for theprediction of 100-day survival in ARDS patients was0.723 (95% CI 0.656 to 0.784), which was larger thanboth the AUC for the lymphocyte/neutrophil ratio alone(P = 0.8601) and the lymphocyte/neutrophil ratio incombination with the PaO2/FiO2 ratio (0.719, 95% CI0.651 to 0.780, P = 0.7734) (Fig.2). In predicting survivalin patients with ARDS, the AUC for the lymphocyte/neutrophil ratio in combination with the lymphocyte
Table 1 Baseline characteristics of the enrolled study population. Normally distributed quantitative data are expressed as means±standard deviation. Non-normally distributed quantitative data are expressed as medians (IQR) (Continued)
Variables Acute respiratory distress syndrome ΔP-value
Total Mild Moderate Severe
B-lymphocytes,% 30.25 ± 17.28 18.00 ± 3.24 26.20 ± 7.81 33.36 ± 7.81 0.598
B-lymphocytes cell count (PCS/μl)
301.05 ± 73.77 69.01 ± 8.89 413.20 ± 41.42 271.18 ± 78.37 0.665
NK cell
NK cells,% 8.76 ± 5.91 17.00 ± 4.41 9.40 ± 0.81 7.73 ± 4.58 0.331
NK cell count (PCS/ul) 68.77 ± 46.46 68.20 ± 7.66 82.60 ± 14.82 62.55 ± 15.15 0.751
Qualitative data are presented as numbers (%). ΔP-value for the three groups (mild, moderate, and severe ARDS groups); *P < 0.05 versus mild ARDS; #P < 0.05versus moderate ARDS. BMI body mass index, APACHE Acute Physiology and Chronic Health Evaluation SOFA Sequential Organ Failure Assessment, CRP C-reactiveprotein, PCT procalcitonin
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 5 of 12

count was significantly higher than those for the PaO2/FiO2 ratio alone (P = 0.0060), BMI alone (P = 0.0001),and lymphocyte count alone (P = 0.0067), and the AUCfor the lymphocyte/neutrophil ratio in combination withthe PaO2/FiO2 ratio was significantly higher than those
for the PaO2/FiO2 ratio alone (P = 0.0014), BMI alone(P = 0.0001), and lymphocytes alone (P = 0.0162).A cut-off value of the lymphocyte/neutrocyte ratio of
> 0.0537 was used to predict the survival of ARDS pa-tients. The sensitivity was 83.8%, and the specificity was80.2%. The positive likelihood ratio was 4.23, and the
Table 2 Comparison of clinical characteristics of ARDS patients according to survival status. Normally distributed quantitative dataare expressed as means±standard deviation. Non-normally distributed quantitative data are expressed as medians (IQR)
Variables Non-survivors(n = 121) Survivors(n = 80) P-value
Age,years 56.96 ± 17.09 50.16 ± 14.33 0.004
Sex,male/female,n 76/45 54/26 0.496
BMI,kg/m2 23.41 ± 3.88 24.69 ± 3.93 0.027
APACHE II score 14.96(14 to 16) 13.51 (13 to 15) 0.036
SOFA score 5.42 (5 to 6) 4.15 (4 to 5) 0.000
PaO2/FiO2,mmHg 115 (102 to 188) 135 (115 to 154) 0.042
CRP,mg/L 152.20 (126.50 to 177.89) 146.32 (113.27 to 179.37) 0.778
PCT,ng/Ml 13.67 (5.49 to 21.89) 11.30 (6.90 to 15.70) 0.577
Hemoglobin,g/L 105.63 ± 27.68 110.41 ± 30.74 0.298
Albumin,g/L 27.24 ± 5.68 28.33 ± 6.02 0.223
Leukocytes,109/L 12.19 (10.41 to 13.97) 10.80 (9.47 to 12.14) 0.012
Lymphocytes,109/L 1.03 (0.86 to 1.20 1.21 (0.92 to 1.50) 0.025
Neotrophils,109/L 9.80 (8.29 to 11.31) 8.80 (7.64 to 9.95) 0.016
Lymphocyte/Neotrophil ratio 0.15 ± 0.05 0.20 ± 0.28 0.008
Virus infection 12(9.91%) 11(13.75%)
Immunoglobulin
IgG,g/L 9.95 ± 2.37 12.42 ± 3.88 0.169
IgA,g/L 1.80 ± 0.53 2.29 ± 1.04 0.156
IgM,g/L 0.90 ± 0.25 1.22 ± 0.33 0.163
IgE,ng/mL 351.97 ± 80.27 1030.29 ± 220.94 0.009
Complement component
C3 3.27 ± 0.91 10.31 ± 2.06 0.018
C4 1.84 ± 0.46 0.25 ± 0.10 0.170
T-lymphocyte subsets
CD3+ cells,% 61.90 ± 15.49 63.83 ± 15.29 0.647
CD4+ cells,% 33.93 ± 16.06 36.67 ± 14.93 0.521
CD4+ cell count (PCS/μl) 328.85 ± 72.23 487.86 ± 65.04 0.512
CD8+ cells,% 29.47 ± 5.42 24.38 ± 9.75 0.190
CD8+ cell count (PCS/μl) 152.75 ± 22.66 331.50 ± 95.71 0.024
CD4+/CD8+ ratio 1.79 ± 0.09 1.78 ± 0.12 0.428
B-lymphocytes
B-lymphocyte cells,% 29.81 ± 8.89 31.33 ± 5.49 0.169
B-lymphocyte cell count (PCS/μl) 113.27 ± 29.45 601.33 ± 52.26 0.009
NK cell
NK cells,% 9.19 ± 3.28 8.00 ± 1.67 0.708
NK cell count (PCS/μl) 56.55 ± 12.87 91.17 ± 19.79 0.134
BMI body mass index, APACHE Acute Physiology and Chronic Health Evaluation, SOFA Sequential Organ Failure Assessment, CRP,C-reactive protein,PCT procalcitonin
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 6 of 12
negative likelihood ratio was 0.20. Moreover, a leukocytecount cut-off of > 0.415 (109/L) was used to predict thesurvival of patients with ARDS. The sensitivity was87.5%, and the specificity was 81.0%. The positive likeli-hood ratio was 4.61, and the negative likelihood ratiowas 0.15.
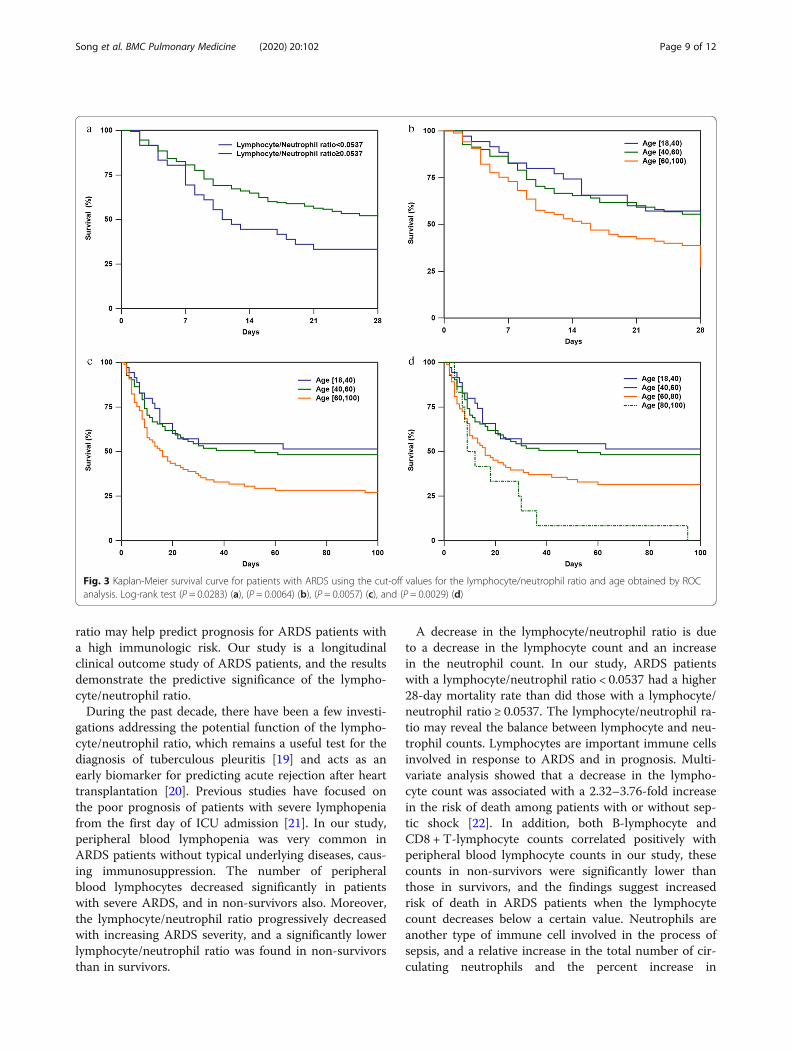
Predictors of 28-day and 100-day mortality in patientswith ARDSTable 3 shows that age (per log10 years) (OR = 1.269,P = 0.019), BMI < 24 (OR = 1.665, P = 0.015), SOFA score(OR = 1.287, P = 0.002), leukocyte count< 0.415 (109/L)(OR = 1.671, P = 0.042), and lymphocyte/neutrophil ratio(OR = 2.132, P = 0.009) were independent predictors of100-day mortality in ARDS patients. Moreover, ARDSpatients with a lymphocyte/neutrophil ratio < 0.0537 hada higher 28-day mortality rate than did those with alymphocyte/neutrophil ratio > 0.0537 (P = 0.0283, Fig. 3a).Furthermore, 28-day and 100-day mortality rates weresignificantly lower in those under 40 years old and 40–
60 years old than in those over 60 years old age (P =0.0064, 0.0057, Fig. 3b, c). The 100-day mortality ratewas significantly higher in those over 80 years old thanin those under 40 years old, 40–60 years old and 60–80years old (P = 0.0029, Fig. 3d).
DiscussionIn this study, we found associations between age, BMI,the SOFA score, and the lymphocyte/neutrophil ratio atICU admission and clinical outcomes in patients withARDS. Age (per log10 years), BMI < 24, the SOFA score(per point) and the lymphocyte/neutrophil ratio were in-dependent risk factors for predicting 100-day mortalityin ARDS patients. Another discovery was that thelymphocyte/neutrophil ratio and age were related toICU mortality and hospital mortality. We also found as-sociations between the baseline lymphocyte/neutrophilratio and age, the SOFA score, the APACHE II score,the PaO2/FiO2 ratio, and the severity of ARDS accordingto the Berlin classification. The lymphocyte/neutrophil
Fig. 1 Relationships between the lymphocyte/neutrophil ratio and age, APACHE II score, SOFA score, and PaO2/FiO2 ratio in ARDS patients.Spearman rank correlation was used to assess associations between variables. The lymphocyte/neutrophil ratio correlated negatively with age (a),the SOFA score (b), and the APACHE II score (c) but positively with the PaO2/FiO2 ratio (D) in ARDS patients
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 7 of 12

Fig. 2 Receiver operating characteristic (ROC) curves for predicting 100-day survival in patients with acute respiratory distress syndrome (ARDS).The area under the curve (AUC) was 0.721 (95% CI 0.656 to 0.784) for the lymphocyte/neutrophil ratio, 0.625 (95% CI 0.554 to 0.692) for the PaO2/FiO2 ratio, 0.593 (95% CI 0.521 to 0.661) for the BMI, 0.592 (95% CI 0.520 to 0.660) for the lymphocyte count, 0.723 (95% CI 0.656 to 0.784) for thelymphocyte/neutrophil ratio combined with the lymphocyte count and 0.719 (95% CI 0.651 to 0.780) for the lymphocyte/neutrophil ratio incombined with the PaO2/FiO2 ratio. The AUC was 0.369 (95% CI 0.292 to 0.446) for age, 0.425 (95% CI 0.345 to 0.505) for the APACHE II score, and0.355 (95% CI 0.278 to 0.433) for the SOFA score (not shown)
Table 3 Logistic regression analysis of the prediction of mortality for patients with acute respiratory distress syndrome (ARDS)
Variables Univariate analysis Multivariate analysis
Odds ratio (95% CI) P-value Odds ratio (95% CI) P-value
Age,per log10(years) 1.269(1.040,1.548) 0.019 2.982(2.073,4.654) 0.007
BMI,< 24 1.665(0.883,3.137) 0.015
APACHE II score,per point 1.016(0.940,1.098) 0.059
SOFA score,per point 1.287(1.098,1.509) 0.002 2.560(1.457,5.430) 0.005
PaO2/FiO2,per log10(mmHg) 0.652(0.280,1.004) 0.067
PCT,per log10(ng/mL) 1.028(0.797,1.810) 0.063
CRP,> 150(mg/L) 1.256(0.618,2.553) 0.059
Lymphocytes,< 0.415 × 109/L 1.671(1.252,1.787) 0.042
Lymphocyte/Neutrophil ratio,< 0.0537 4.137(1.452,6.832) 0.002 3.726(2.754,5.195) 0.003
BMI body mass index, APACHE Acute Physiology and Chronic Health Evaluation, SOFA Sequential Organ Failure Assessment, PCT procalcitonin, CRPC-reactive protein
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 8 of 12
ratio may help predict prognosis for ARDS patients witha high immunologic risk. Our study is a longitudinalclinical outcome study of ARDS patients, and the resultsdemonstrate the predictive significance of the lympho-cyte/neutrophil ratio.During the past decade, there have been a few investi-
gations addressing the potential function of the lympho-cyte/neutrophil ratio, which remains a useful test for thediagnosis of tuberculous pleuritis [19] and acts as anearly biomarker for predicting acute rejection after hearttransplantation [20]. Previous studies have focused onthe poor prognosis of patients with severe lymphopeniafrom the first day of ICU admission [21]. In our study,peripheral blood lymphopenia was very common inARDS patients without typical underlying diseases, caus-ing immunosuppression. The number of peripheralblood lymphocytes decreased significantly in patientswith severe ARDS, and in non-survivors also. Moreover,the lymphocyte/neutrophil ratio progressively decreasedwith increasing ARDS severity, and a significantly lowerlymphocyte/neutrophil ratio was found in non-survivorsthan in survivors.
A decrease in the lymphocyte/neutrophil ratio is dueto a decrease in the lymphocyte count and an increasein the neutrophil count. In our study, ARDS patientswith a lymphocyte/neutrophil ratio < 0.0537 had a higher28-day mortality rate than did those with a lymphocyte/neutrophil ratio ≥ 0.0537. The lymphocyte/neutrophil ra-tio may reveal the balance between lymphocyte and neu-trophil counts. Lymphocytes are important immune cellsinvolved in response to ARDS and in prognosis. Multi-variate analysis showed that a decrease in the lympho-cyte count was associated with a 2.32–3.76-fold increasein the risk of death among patients with or without sep-tic shock [22]. In addition, both B-lymphocyte andCD8 + T-lymphocyte counts correlated positively withperipheral blood lymphocyte counts in our study, thesecounts in non-survivors were significantly lower thanthose in survivors, and the findings suggest increasedrisk of death in ARDS patients when the lymphocytecount decreases below a certain value. Neutrophils areanother type of immune cell involved in the process ofsepsis, and a relative increase in the total number of cir-culating neutrophils and the percent increase in
Fig. 3 Kaplan-Meier survival curve for patients with ARDS using the cut-off values for the lymphocyte/neutrophil ratio and age obtained by ROCanalysis. Log-rank test (P = 0.0283) (a), (P = 0.0064) (b), (P = 0.0057) (c), and (P = 0.0029) (d)
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 9 of 12

neutrophils with immature morphology are also closelyrelated to sepsis [23, 24]. Compared with counts in sur-vivors, higher neutrophil counts were found in patientswho eventually died as a result of sepsis-induced ARDS,and excessive accumulation of neutrophils in patientswith ARDS may therefore contribute to disease progres-sion [6, 8]. Therefore, the combination of lymphopeniaand neutrophilia contributes to the outcome of ARDS,which may explain why the lymphocyte/neutrophil ratioin our study was a strong independent predictor ofprognosis.Although the clinical scores, such as APACHE II [25],
SOFA [26] and the PaO2/FiO2 ratio [27], have beenwidely used to predict the results of clinical practice pa-tients of ARDS. We further found that the lymphocyte/neutrophil ratio AUC was higher than the PaO2/FiO2 ra-tio, BMI, APACHE II score, and SOFA score alone inpredicting 100-day survival in ARDS patients. In com-bination with the lymphocyte count slightly increasedthe AUC of the lymphocyte/neutrophil ratio in predict-ing 100-day survival, yet there was no difference com-pared with the lymphocyte/neutrophil ratio alone.Moreover, ARDS patients with a lymphocyte/neutrophilratio ≥ 0.0537 had a lower 28-day mortality rate, and sig-nificantly moderate negative correlations were found be-tween the lymphocyte/neutrophil ratio and age, theSOFA score, and the APACHE II score. In addition, amoderate positive correlation between the lymphocyte/neutrophil ratio and the PaO2/FiO2 ratio was beennoted. These results suggest that the lymphocyte/neutro-phil ratio can comprehensively and plausibly reflect thepatient’s physiological, pathophysiological and respira-tory oxygenation index status. Taken together, our find-ings strongly suggest that the lymphocyte/neutrophilratio is a potential indicator and good indicator for prog-nosis evaluation among ARDS patients.There have been many clinical studies on ARDS pa-
tients with typical immunodeficiency [13, 28], and im-munodeficiency in ARDS patients is usually atypical.Although it does not reach the level found in typical im-munodeficiency, there is already a degree of immune im-pairment. Nonetheless, there are few studies on atypicalimmune deficiency or impaired immunity in ARDS pa-tients, and there is no uniform scale or biomarker tomeasure immune impairment in ARDS patients and itsrelationship with prognosis. A consensus has not beenreached regarding whether viral infection causes im-mune deficiency, though it is commonly thought to in-duce immune impairment but not to the extent ofimmune deficiency. In our study, there was no signifi-cant difference in viral infection status between the sur-vivor and non-survivor groups. However, we did observethat the lymphocyte/neutrophil ratio in the survivorgroup were higher than those in the non-survivor group.
We hypothesize that a low lymphocyte/neutrophil ratiomay be a marker of this atypical immunodeficiency inARDS patients, affecting their prognosis. There are norecognized biomarkers to date that can be used to iden-tify the immune status of ARDS patients. Accordingly,we propose a new biomarker for the identification ofatypical immune status in patients with ARDS. This sta-tus may be due to abnormal inhibitors that have been beactivated. We hope that by observing the association ofthe early lymphocyte/neutrophil ratio with prognosismay result in better detection and more timely treat-ment of an abnormal immune status.Our findings must be understood in view of the fol-
lowing limitations. First, this study had a relatively smallsample size, even though it was the first study to explorethe prognostic value of the lymphocyte/neutrophil ratiofor prognosis in ARDS patients. Second, there may be aselection bias because only patients for whom absolutelymphocyte and neutrophil counts were measured soonafter ARDS diagnosis were included. Third, the currentstudy was not pre-specified but is a post hoc analysisfrom a retrospective controlled trial. Therefore, furtherprospective studies are needed.
ConclusionsWe found age (per log10 years), BMI < 24, the SOFAscore, the lymphocyte count, and the lymphocyte/neu-trophil ratio to be independent predictors of 100-daymortality in patients with ARDS. We also observed amoderate negative correlations between the lymphocyte/neutrophil ratio and age, the SOFA score, and the APA-CHE II score, and a significant mild positive correlationbetween the lymphocyte count and BMI was also found.However, we detected a moderate positive correlationbetween the lymphocyte/neutrophil ratio and the PaO2/FiO2 ratio in all patients with ARDS. The AUC wasgreatest for the lymphocyte/neutrophil ratio combinedwith the lymphocyte count for the prediction of 100-daysurvival in ARDS. In addition, the 28-day mortality rateof ARDS patients with a lymphocyte/neutrophil ratio <0.0537 was higher than that with a ratio of lymphocyte/neutrophil ≥0.0537. The lymphocyte/neutrophil ratiowas also revealed to be a strong and independent pre-dictor of prognosis in ARDS patients, particularly inthose with atypical immunodeficiency.
AbbreviationsARDS: Acute respiratory distress syndrome; APACHE: Acute Physiology andChronic Health Evaluation; AUC: Area under the curve; BALF: Bronchoalveolarlavage fluid; BMI: Body mass index; CI: Confidence interval; CRP: C-reactiveprotein; ICU: Intensive care unit; LDH: Lactate dehydrogenase; MOF: Multipleorgan failure; OR: Odds ratio; PCT: Procalcitonin; ROC: Receiver operatingcharacteristic; SAPS: Simplified Acute Physiology Score; SD: Standarddeviation; SOFA: Sequential Organ Failure Assessment
AcknowledgementsNot applicable.
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 10 of 12

Author contributionsAll authors participated in the interpretation of the study results and reviewof the manuscript. MS designed and conducted all experiments, drafted themanuscript, and performed the statistical analyses. HL planned the study anddrafted the manuscript. YJ L and ZW L participated in the data collection. HPand PC contributed to the study design and the revision of the manuscript.All authors read and approved the final manuscript.
FundingThis work was supported by grants from by the National Natural ScienceFoundation of China (Grant number 81770002 and 81670062). Financialsupport was mainly provided for the collection and analysis of data and forstaff costs.
Availability of data and materialsThe datasets used and analysed during the current study are available fromthe corresponding author on reasonable request.
Ethics approval and consent to participateThe study protocol was approved by the ethics committee of the SecondXiangya Hospital, Central South University (approval number: 2019150), andwritten informed consent was waived because of the retrospective design.All personal identification data were anonymized before analysis.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Author details1Department of Pulmonary and Critical Care Medicine, The Second XiangyaHospital, Central South University, No.139 Renmin Road, Changsha 410011,Hunan, China. 2The Respiratory Disease Research Institute of Hunan Province;The Respiratory Disease Diagnosis and Treatment Center of Hunan Province,No.139 Renmin Road, Changsha 410011, Hunan, China. 3School ofMathematics and Statistics, Hunan Normal University, Changsha 410081,Hunan, China.
Received: 12 July 2019 Accepted: 2 April 2020
References1. Thompson BT, Chambers RC, Liu KD. Acute respiratory distress syndrome. N
Engl J Med. 2017;377:562–72.2. Definition Task Force ARDS, Ranieri VM, Rubenfeld GD, Thompson BT,
Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratorydistress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–33.https://doi.org/10.1001/jama.2012.5669.
3. Pipeling MR, Fan E. Therapies for refractory hypoxemia in acute respiratorydistress syndrome. JAMA. 2010;304:2521e2527.
4. Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, Mercier E,Badet M, Mercat A, Baudin O, Clavel M, Chatellier D, Jaber S, Rosselli S,Mancebo J, Sirodot M, Hilbert G, Bengler C, Richecoeur J, Gainnier M, BayleF, Bourdin G, Leray V, Girard R, Baboi L, Ayzac L, PROSEVA Study Group.Prone positioning in severe acute respiratory distress syndrome. N Engl JMed. 2013;368(23):2159–68. https://doi.org/10.1056/NEJMoa1214103.
5. Matthay MA, Ware LB, Zimmerman GA. The acute respiratory distresssyndrome. J Clin Invest. 2012;122:2731–40.
6. Williams AE, Chambers RC. The mercurial nature of neutrophils: still anenigma in ARDS? Am J Physiol Lung Cell Mol Physiol. 2014;306:L217–30.
7. Williams AE, José RJ, Mercer PF, Brealey D, Parekh D, Thickett DR, O'Kane C,McAuley DF, Chambers RC. Evidence for chemokine synergy duringneutrophil migration in ARDS. Thorax. 2017;72(1):66–73. https://doi.org/10.1136/thoraxjnl-2016-208597.
8. Steinberg KP, Milberg JA, Martin TR, Maunder RJ, Cockrill BA, Hudson LD.Evolution of bronchoalveolar cell populations in the adult respiratorydistress syndrome. Am J Respir Crit Care Med. 1994;150(1):113–22.
9. Grudzinska FS, Sapey E. Friend or foe? The dual role of neutrophils in lunginjury and repair. Thorax. 2018;73(4):305–7. https://doi.org/10.1136/thoraxjnl-2017-211253.
10. Adamzik M, Broll J, Steinmann J, Westendorf AM, Rehfeld I, Kreissig C, PetersJ. An increased alveolar CD4 + CD25 + Foxp3 + T-regulatory cell ratio inacute respiratory distress syndrome is associated with increased 30-daymortality. Intensive Care Med. 2013;39(10):1743–51. https://doi.org/10.1007/s00134-013-3036.
11. Cortegiani A, Madotto F, Gregoretti C, Bellani G, Laffey JG, Pham T, VanHaren F, Giarratano A, Antonelli M, Pesenti A, Grasselli G, LUNG SAFEInvestigators and the ESICM Trials Group. Immunocompromised patientswith acute respiratory distress syndrome: secondary analysis of the LUNGSAFE database. Crit Care. 2018 Jun 12;22(1):157. https://doi.org/10.1186/s13054-018-2079-9.
12. Azoulay E, Soares M, Benoit D. Focus on immunocompromised patients.Intensive Care Med. 2016;42(3):463–5. https://doi.org/10.1007/s00134-016-4224-8.
13. Schmidt M, Schellongowski P, Patroniti N, Taccone FS, Reis Miranda D,Reuter J, Prodanovic H, Pierrot M, Dorget A, Park S, Balik M, Demoule A,Crippa IA, Mercat A, Wohlfarth P, Sonneville R, Combes A; InternationalECMO Network (ECMONet), the REVA Research Network and the IDEA StudyGroup. Six-month Outcome of Immunocompromised Severe ARDS PatientsRescued by ECMO. An International Multicenter Retrospective Study. Am JRespir Crit Care Med. 2018. doi: https://doi.org/10.1164/rccm.201708-1761OC.
14. Force ADT, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, CaldwellE, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: theBerlin Definition. JAMA. 2012;307(23):2526–33.
15. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity ofdisease classification system. Crit Care Med. 1985;13:818–29.
16. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H,Reinhart CK, Suter PM, Thijs LG. The SOFA (Sepsis-related organ failureassessment) score to describe organ dysfunction/failure. On behalf of theworking group on Sepsis-related problems of the European Society ofIntensive Care Medicine. Intensive Care Med. 1996;22(7):707–10.
17. Nguyen CQ, Yin H, Lee BH, Carcamo WC, Chiorini JA, Peck AB. Pathogeniceffect of interleukin-17A in induction of Sjögren’s syndrome-like diseaseusing adenovirus-mediated gene transfer. Arthritis Res Ther. 2010;12:R220.
18. Anderson KC, Roach JA, Daley JF, Schlossman SF, Nadler LM. Dualfluorochrome analysis of human B lymphocytes: phenotypic examination ofresting, anti-immunoglobulin stimulated, and in vivo activated B cells. JImmunol. 1986;136(10):3612–8.
19. Burgess LJ, Maritz FJ, Le Roux I, Taljaard JJ. Combined use of pleuraladenosine deaminase with lymphocyte/neutrophil ratio. Increasedspecificity for the diagnosis of tuberculous pleuritis. Chest. 1996;109(2):414–9.
20. Choi DH, Kobayashi Y, Nishi T, Luikart H, Dimbil S, Kobashigawa J, Khush K,Fearon WF. Change in lymphocyte to neutrophil ratio predicts acuterejection after heart transplantation. Int J Cardiol. 2018;251:58–64. https://doi.org/10.1016/j.ijcard.2017.10.060.
21. Bonizzoli M, Arvia R, di Valvasone S, Liotta F, Zakrzewska K, Azzi A, Peris A.Human herpesviruses respiratory infections in patients with acuterespiratory distress (ARDS). Med Microbiol Immunol. 2016;205(4):371–9.https://doi.org/10.1007/s00430-016-0456-z.
22. Güell E, Martín-Fernandez M, De la Torre MC, Palomera E, Serra M, MartinezR, Solsona M, Miró G, Vallès J, Fernández S, Cortés E, Ferrer V, Morales M,Yébenes JC, Almirall J, Bermejo-Martin JF. Impact of Lymphocyte andNeutrophil Counts on Mortality Risk in Severe Community-AcquiredPneumonia with or without Septic Shock. J Clin Med. 2019 May 27;8(5).https://doi.org/10.3390/jcm8050754.
23. Brown KA, Brain SD, Pearson JD, Edgeworth JD, Lewis SM, Treacher DF.Neutrophils in development of multiple organ failure in sepsis. Lancet. 2006;368(9530):157–69.
24. Shen XF, Cao K, Jiang JP, Guan WX, Du JF. Neutrophil dysregulation duringsepsis: an overview and update. J Cell Mol Med. 2017;21(9):1687–97. https://doi.org/10.1111/jcmm.13112 Epub 2017 Feb 28.
25. Mouillaux J, Allam C, Gossez M, Uberti T, Delwarde B, Hayman J, Rimmelé T,Textoris J, Monneret G, Peronnet E, Venet F. TCR activation mimicsCD127lowPD-1high phenotype and functional alterations of T lymphocytesfrom septic shock patients. Crit Care. 2019;23(1):131. https://doi.org/10.1186/s13054-018-2305-5.
26. Zhu G, Liu Y, Zhang W, Huang Y, Li K. CD27+TIM-1+ memory B cellspromoted the development of Foxp3+ Tregs and were associated withbetter survival in acute respiratory distress syndrome. Immunol Res. 2018;66(2):281–7. https://doi.org/10.1007/s12026-017-8983-2.
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 11 of 12

27. Festic E, Bansal V, Kor DJ, Gajic O. US critical illness and injury trials group:lung injury prevention study investigators (USCIITG–LIPS). SpO2/FiO2 ratioon hospital admission is an indicator of early acute respiratory distresssyndrome development among patients at risk. J Intensive Care Med. 2015;30(4):209–16. https://doi.org/10.1177/0885066613516411.
28. Azoulay E, Mokart D, Pène F, Lambert J, Kouatchet A, Mayaux J, Vincent F,Nyunga M, Bruneel F, Laisne LM, Rabbat A, Lebert C, Perez P, Chaize M,Renault A, Meert AP, Benoit D, Hamidfar R, Jourdain M, Darmon M,Schlemmer B, Chevret S, Lemiale V. Outcomes of critically ill patients withhematologic malignancies: prospective multicenter data from France andBelgium--a groupe de recherche respiratoire en reanimation onco-hematologique study. J Clin Oncol. 2013;31:2810–8.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Song et al. BMC Pulmonary Medicine (2020) 20:102 Page 12 of 12