Professor Munir Pirmohamed Digital Health Assembly 2015
17
16/02/2015 1 My Risks, My Treatment: Stratified Medicine Munir Pirmohamed NHS Chair of Pharmacogenetics Department of Molecular and Clinical Pharmacology Institute of Translational Medicine University of Liverpool Hypertension ACE inhibitor β‐blocker Calcium channel blocker Diuretic Choice of 1 st line treatment Age Level of BP Renal function Concomitant Medication Concurrent disease (diabetes, gout etc) Current Clinical Practice: A Hypothetical Patient Personalisation of treatment
-
Upload
dha2015 -
Category
Healthcare
-
view
60 -
download
5
Transcript of Professor Munir Pirmohamed Digital Health Assembly 2015

16/02/2015
1
My Risks, My Treatment:Stratified Medicine
Munir PirmohamedNHS Chair of Pharmacogenetics
Department of Molecular and Clinical Pharmacology
Institute of Translational Medicine
University of Liverpool
Hypertension
ACE inhibitor
β‐blocker
Calcium channel blocker
Diuretic
Choice of 1st line treatment
Age
Level of BP
Renal function
Concomitant Medication
Concurrent disease (diabetes, gout etc)
Current Clinical Practice: A Hypothetical Patient
Personalisation of treatment
16/02/2015
2
Current Clinical Practice
The best drug for the patient (according to current clinical practice and clinical judgement) to treat a disease
Relatively unsophisticated: cannot predict
whether the patient will improve
whether the patient will develop side effects
“One Dose Fits All” – Variability In Improvement
Condition Efficacy Rate (%)
Alzheimer’s 30Asthma 60Diabetes 57HCV 47Cancer 25Osteoporosis 48Rheumatoid arthritis 50Schizophrenia 60
“The vast majority of drugs - more than 90 per cent –only work in 30 or 50 per cent of the people,”
Source: Physicians Desk Reference

16/02/2015
3
Adverse Drug Reactions (Side Effects)
• Adverse drug reactions are common• Vary in severity
TOXIC EPIDERMAL NECROLYSIS
“The tailoring of medical treatment to the individual
characteristics of each patient. The ability to classify
individuals into subpopulations that differ in
their susceptibility to a particular disease or their response to a specific
treatment. Interventions can then be concentrated on those
who will benefit, sparing expense and side effects for
those who will not”.

16/02/2015
4
Personalised Medicine
Need for Personalised Medicine
Society
Individual
16/02/2015
5
Arguments against Personalised Medicine
Public health initiatives such as flu vaccine produce greater benefits
Developing drugs for a proportion will cost more, and will only target a minority
Rescuing the pharmaceutical industry
Personal genetic tests have only been recommended for 4% of patients (US, 2012)
We Medicine vs Me Medicine
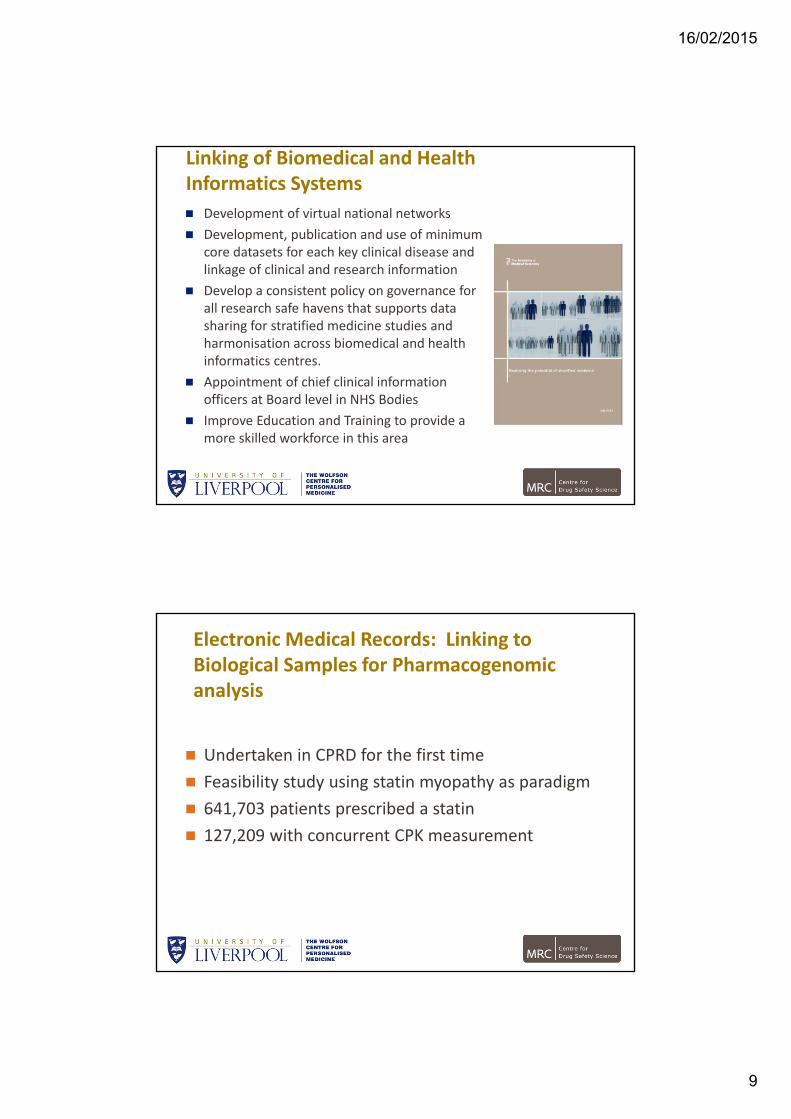
Malignant Melanoma and BRAF Inhibitor: Baseline and 2 Weeks After

16/02/2015
6
Source: Academy of Medical Sciences Report
New CF drug, ivacaftor
Targets G551D mutation in the CFTR gene
Seen in 4% of the CF population
Fantastic innovation with increases in FEV1 ~10%
Cost $294,000 per year in the US

16/02/2015
7
Technology‐Based Reduction in the Burden of ADRs: The Case of Abacavir Hypersensitivity
Association with HLA-B*5701
Clinical genotype
CH2OH
H2N
N
NN
N
NH
Case Studies Represent Different Models for Implementation
Vemurafenib – malignant melanoma
Early and co‐ordinated interaction between drug developers and diagnostics industry allowed simultaneous development
Ivacaftor – cystic fibrosis
Most specialised CF clinics have undertaken genetic testing and will have results in case records
No need for additional testing
Abacavir – hypersensitivity reactions
Developed after drug licensed
HLA testing done in different labs, and provision of test left to NHS or private providers

16/02/2015
8
“it is crucial that information technology and use of electronic patient records is addressed, as is linking biosamples, biological and clinical data to health records”
Increase pace of progress which is only possible through involvement of many stakeholders
Linking of biomedical and health informatics systems
Incentives to develop stratified medicine products
Adoption
Need for collaboration
16/02/2015
9
Linking of Biomedical and Health Informatics Systems
Development of virtual national networks
Development, publication and use of minimum core datasets for each key clinical disease and linkage of clinical and research information
Develop a consistent policy on governance for all research safe havens that supports data sharing for stratified medicine studies and harmonisation across biomedical and health informatics centres.
Appointment of chief clinical information officers at Board level in NHS Bodies
Improve Education and Training to provide a more skilled workforce in this area
Electronic Medical Records: Linking to Biological Samples for Pharmacogenomic analysis
Undertaken in CPRD for the first time
Feasibility study using statin myopathy as paradigm
641,703 patients prescribed a statin
127,209 with concurrent CPK measurement

16/02/2015
10
Governance
Sponsor – University of Liverpool
Ethics Committee approval – 1
Independent Scientific Advisory Committee – 1
R & D Departments in Primary Care NHS Trusts
132 approvals
Over 55 pages long – different questions (not in their remit)
Wanted changes to PILs (not in their remit)
Timelines for approval varied
The R&D Governance Burden
Statin myopathyIdentified via CPRDLink to DNA samples
132 R&D approvals

16/02/2015
11
Statin Use in CPRD and Risk of Muscle Toxicity
Simvastatin was most frequently prescribed (66.3%) followed by atorvastatin (24.4%).
Concomitant prescribing of CYP3A4 inhibitors increased risk of rhabdomyolysis (OR 3.71, 95% CI 1.18‐11.61)
Dose also associated with risk.
recent clinical record of myalgia was associated with an increased OR of 4+x ULN CPK (OR 1.73, 95% CI 1.37‐2.18).
In patients who were rechallenged to statins and had repeat CPK measurements after 4+x ULN CPK abnormalities, 54.8% of the repeat CPK values were within normal range, 32.1% between 1‐3x and 13.0% 4+x ULN
Recruitment

16/02/2015
12
Cumulative Recruitment
Cases
Controls
1. Implicated SNP is in the SLCO1B1 gene (transporter)2. Shown with simvastatin 40mg and 80mg

16/02/2015
13
Clin Pharmacol Ther. 2013 Dec;94(6):695‐701
Nature. 2013 Oct 17;502(7471):377‐80.
Nature. 2014 Sep 18;513(7518):E1
Nature. 2014 Sep 18;513(7518):E1‐3
LACK OF REPLICATION

16/02/2015
14
Linking eHRs to Biobanks: Example of the UK Biobank Q1/2015:
Web‐based questionnaire data on cognitive function
Genotyping data available for first 150,000 participants
Q2/2015:
Web‐based questionnaire data on occupational history
Some primary care data
Biochemistry assay data for urinary biomarkers (for all participants)
Objective measures of built environment available (for all participants)
Q3/2015: Genotyping data available for remaining participants
Q4/2015: Imaging data available for some participants
Q1/2016: Data collection completed for physical activity monitor for 100,000 participants
Q2/2016: Biochemistry assay data available for plasma and serum (for all participants
http://biobank.ctsu.ox.ac.uk/crystal/exinfo.cgi?src=future_timelines
BioVu
Vanderbilt900 samples per week192,000 samples

16/02/2015
15
16/02/2015
16
Can CPRD be Used for Stratified Medicine Trials?
Use for pragmatic trials already demonstrated
Stratified medicine trial is not usually a pragmatic trial
Requires the use of a diagnostic test to determine which therapeutic should be prescribed
Challenges:
Local governance approvals
MHRA CTA approval
Confidentiality and consent
Ability to undertake testing in a suitable timeframe (point‐of‐care, or central laboratory)
Feeding result back to GP
Need to avoid delay in prescribing
Vanderbilt – patients pre‐emptively genotyped for a panel of actionable pharmacogenomic variants
Results entered into electronic medical record
Advantages:
Most patient carry at least one pharmacogenomic variant
Data are available at point of care
Substantial reduction in testing burden compared with a reactive strategy

16/02/2015
17
Conclusions
Linking EHRs to biological samples is important in facilitating stratified medicine
EHRs can be used for both efficacy and safety end‐points, and will be particularly valuable in identifying rare events
The governance burden associated with undertaking such research needs to be improved
Stratified medicine trials likely to face additional challenges which also need the development of simpler pathways
AcknowledgementsSERIOUS ADVERSE EVENT CONSORTIUM
Funders:
Dept of Health (NHS Chair of Pharmacogenetics)
MRC, WT, DH, NIHR, EU‐FP7
The University of Liverpool
• B Kevin Park, Dan Carr and many others
Tjeerd van Staa and others involved in programme on pragmatic trials
CPRD for providing access to records and initial work on linking to biological samples