Principles of Prescription Writing · Principles of Prescription Writing CHAPTER 3 M.ASHOKKUMAR...
39
Principles of Prescription Writing CHAPTER 3 M.ASHOKKUMAR DEPT OF PHARMACY PRACTICE SRM COLLEGE OF PHARMACY SRM UNIVERSITY
Transcript of Principles of Prescription Writing · Principles of Prescription Writing CHAPTER 3 M.ASHOKKUMAR...

Principles of Prescription Writing
CHAPTER 3
M.ASHOKKUMARDEPT OF PHARMACY PRACTICESRM COLLEGE OF PHARMACY
SRM UNIVERSITY
HistoryPrescriptions have been in use since ancient times
Latin adopted as standard language“Rx” = prescription“Sig.” = directions
Federal Food, Drug, and Cosmetic Act (1938)
Non – prescriptionPrescription
Legend drugs Controlled drugs

Classification of DrugsPrescription drug
drug that requires a prescription because it is considered potentially harmful if not used under the supervision of a licensed health care practitionerKnown synonymously as a legend drug because the label of the drug bears the legend, “Caution: Federal Law Prohibits Dispensing without a Prescription” or “Rx only.”

Classification of Drugs
Controlled or scheduled drug a prescription drug whose use and distribution is tightly controlled because of its abuse potential or riskControlled drugs are classified into schedules
Schedules CI, CII, CIII, CIV, and CVPrescriptions for controlled substances have additional requirements by law

Definition and FormatA prescription is a written, verbal, or electronic order from a practitioner or designated agent to a pharmacist for a particular medication for a specific patient.
Writing PrescriptionsWho can write a Rx?
Practitioners Physicians, veterinarians, dentists, podiatrists
Mid-level practitioners nurse practitioners, physician assistants, optometrists, pharmacists
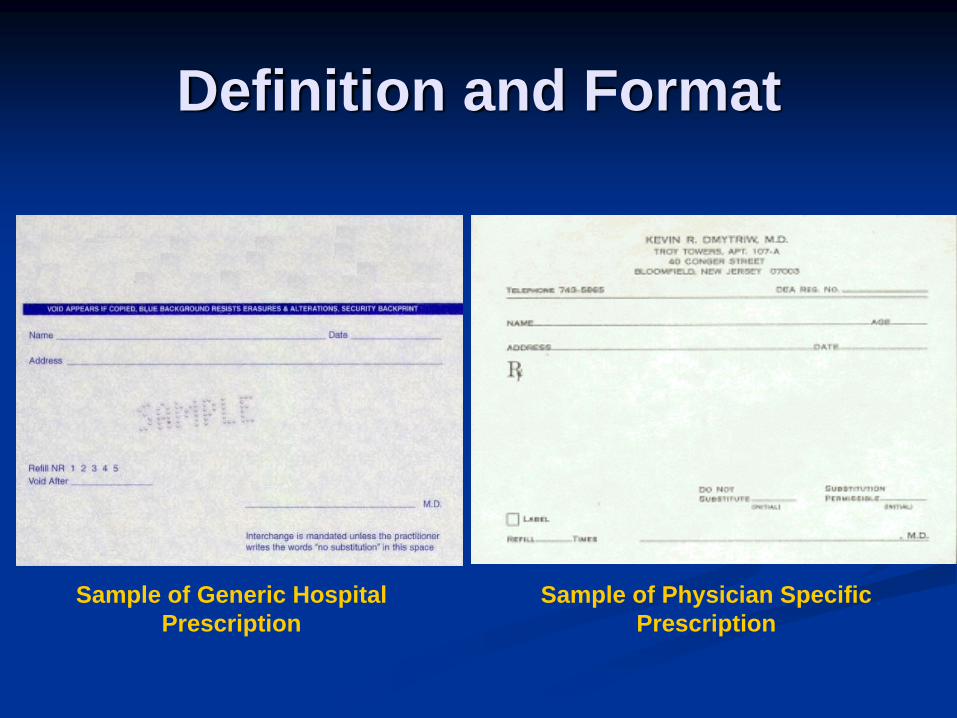
Definition and Format
Sample of Generic Hospital Prescription
Sample of Physician Specific Prescription

Contents of the PrescriptionUnder Texas State Law, all prescriptions should have the following essential elements:
Date of the orderPatient Name and AddressIf the drug is prescribed for an animal, the species of the animalName of the drugStrength of the drugQuantity of the drugDirections for useIntended use of the drug, unless practitioner feels indication is not in best interest of patientPractitioner Name, Address, Telephone number
Contents of the PrescriptionDate
Date the prescription is issued or writtenAllows the determination of the life of the prescription to validate refills
Legend drugs – expire 1 year from date issuedControlled drugs
CIII-CV – expire 6 months from date issuedCII – expire 7 days from date issued
Ensures continual patient supervisionPromotes patient follow - up

Contents of the Prescription
Patient Name and AddressFull first and last name
Middle initial may be helpfulFull addressDOB – not required, but will be helpful in further identifying the correct patient to prevent medication errors
Contents of the PrescriptionSelecting the drug
Medication AllergiesAvailability
UTMB Outpatient FormularyRestrictions
Medicaid Formulary (Handout 1)Outside Pharmacy
CostUTMB Tier Categories
A Drug - $10B Drug - $25C Drug - $45D drug – Full price
Full payment
Contents of the PrescriptionSelecting the drug
Determine if controlled drug or non-controlled drugControlled drugs will have additional law requirements
Determine preference for brand or generic productBrand vs. genericBioequivalent – same amount of active ingredient is delivered to body and will produce identical effect in terms of duration and intensityIs Brand always better? NOIf practitioner prefers brand, must indicate in print, “Brand Necessary” or “Brand Medically Necessary”

Sample Prescription- “Brand Necessary”

Contents of the Prescription
Name of the drug USE WITH CAUTION:
Look Alike/Sound Alike drug names Massive number of new drug releasesMassive number of reformulationsDrug marketing strategy
Build on established namesNew combination drugs – Use converged names
Handout 2

Look Alike/Sound Alike Names
CASE # 1:Serzone (nefazodone) vs. Seroquel (quetiapine)
(antidepressant) (antipsychotic)
Similar overlapping strengths (100 mg and 200 mg)Similar dosage forms (tablets)Similar dosing interval (BID)Similar titration scheduleOften stocked in close proximity on pharmacy shelf
Prescribing and dispensing errors have led to a number ofadverse events (N/V, hallucinations, AMS, lethargy,seizures, death)

Contents of the PrescriptionName of the drugAVOID THE USE OF:
AbbreviationsMany drugs identified with abbreviations
EX: HCTZ for hydrochlorothiazide, MSO4 for morphine sulfate
Attempts to standardize abbreviations have been unsuccessfulJCAHO (January 1, 2004): “Do Not Use” List: Abbreviations, Acronyms, and SymbolsHandout 3

Abbreviation Potential Problem Preferred Term
U (unit) Mistaken as zero, four, or cc Write “unit”
IU (international unit) Mistaken as IV or 10 Write “international unit”
Q.D., Q.O.D. Mistaken for each other. Period after Q and O after Q can be mistaken for “I”
Write “daily” and “every other day”
Trailing zero and lack of leading zero
Decimal point missed Never write a zero by itself after a decimal point, and always use a zero before a decimal point
MS, MSO4, MgSO4 Confused for one another Write “morphine sulfate” or “magnesium sulfate”
List of dangerous abbreviations, acronyms, and symbols JCAHO MINIMUM REQUIRED LIST
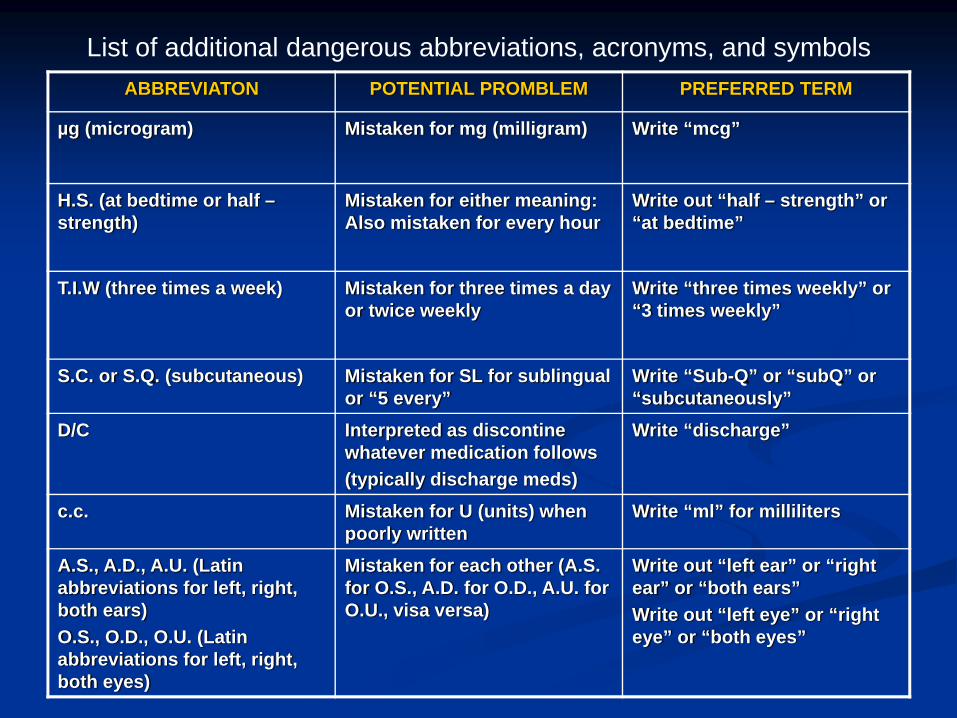
List of additional dangerous abbreviations, acronyms, and symbolsABBREVIATON POTENTIAL PROMBLEM PREFERRED TERM
µg (microgram) Mistaken for mg (milligram) Write “mcg”
H.S. (at bedtime or half –strength)
Mistaken for either meaning: Also mistaken for every hour
Write out “half – strength” or “at bedtime”
T.I.W (three times a week) Mistaken for three times a dayor twice weekly
Write “three times weekly” or “3 times weekly”
S.C. or S.Q. (subcutaneous) Mistaken for SL for sublingual or “5 every”
Write “Sub-Q” or “subQ” or “subcutaneously”
D/C Interpreted as discontine whatever medication follows(typically discharge meds)
Write “discharge”
c.c. Mistaken for U (units) when poorly written
Write “ml” for milliliters
A.S., A.D., A.U. (Latin abbreviations for left, right, both ears)O.S., O.D., O.U. (Latin abbreviations for left, right, both eyes)
Mistaken for each other (A.S. for O.S., A.D. for O.D., A.U. for O.U., visa versa)
Write out “left ear” or “right ear” or “both ears”Write out “left eye” or “right eye” or “both eyes”
Contents of the PrescriptionName of the drug
Multiple drugs per prescription can add to confusionKEEP IT SIMPLE

Contents of the PrescriptionStrength of the drug
Be familiar with drugs and their various dosing strengths and dosage forms
When in doubt, use references or call pharmacy for help Be familiar with dosing units and their corresponding abbreviations (Handout 4)Weight – based dosing
Always convert patient weight to correct units (kg)Liquid medications
One product may be available in a number of concentrationsBe familiar with various product concentrationsIndicate BOTH concentration and dose of medicationExample: Cephalexin suspension 125 mg/ 5 ml
1 teaspoon (5 ml) every 6 h200 ml

Contents of the Prescription
Strength of the drugDecimal points
Avoid trailing zeros. EX. 5 mg vs. 5.0 mg; can be mistaken for 50 mg or 0.7 g vs. .70 g; can be mistaken for 70 gAlways use leading zeros. EX. 0.8 ml vs. .8 ml; can be mistaken for 8 ml

Contents of the Prescription
Quantity of the drugPrescribe only necessary quantityWrite for specific quantities rather than time period (for example: dispense #30 vs. dispense for 1 month)Calculate: quantity = frequency per day x treatment daysWriting out “Dispense # X” is helpful

Contents of the Prescription
Directions for useWrite out in full English or use Latin abbreviations (Handout 5)Latin abbreviations – more convenient, more potential for mistakes
Avoid Dangerous Abbreviations (Handout 3)Provide clear and specific directions
Avoid “Take as Directed.”

Contents of the PrescriptionIndication
Encouraged, seldom practicedHelps confirm appropriateness of medicationReminds patient of drug’s purposeFacilitates communication between health care providers

Contents of the PrescriptionPractitioner’s Name, Address, and Phone number
Validates prescriptionProvides contact information to clarify any questionsInformation based on practitioner’s usual place of business
Contents of the PrescriptionRefills
Refills are not requiredTo avoid interrupting maintenance therapy, practitioners can authorize refills on a written prescriptionNon-controlled substances - No limit to number of refills allowed. Use Discretion.Refills authorized are valid only for life of the prescription – 1 yearPRN – Refill as needed for 1 year

Controlled Substances
Definition - a prescription drug whose use and distribution is tightly controlled because of its abuse potential or riskRegulation is more strictFederal law and State law regulate the storage, use, and disposal of controlled substances
Federal vs. State laws

Controlled SubstancesControlled drugs are divided into Schedules according to abuse potential
Schedule I (C-I) – Highest abuse risk. No safe medical use in U.S. Examples: heroin, marijuana, LSD, PCP, and crack cocaine.Schedule II (C-II) – High abuse risk but have safe and accepted medical use. Examples: morphine, oxycodone, methylphenidate, dextroamphetamine. Schedule III (C-III) – Abuse risk less than C-II and safe and accepted medical use. Examples: Acetaminophen/Codeine (Tylenol #3), acetaminophen/hydrocodone (Vicodin), propoxyphene (Darvon).Schedule IV (C-IV) – Abuse risk less than C-III and safe and accepted medical use. Examples: diazepam (Valium), alprazolam (Xanax), phenobarbital, chloral hydrate. Schedule V (C-V) – Abuse risk less than C-IV and safe and accepted medical use. Mainly consist of preparations containing limited quantities of certain stimulant and narcotic drugs for antitussive and antidiarrheal purposes.
Controlled SubstancesAdditional Law Requirements
RegistrationEvery practitioner must register with DEA and DPS.Exemptions – all of the following may prescribe CIII-CV drugs if acting in the course of employment for a DEA registered hospital
Interns or residents Physicians on staff at VA hospitalIndividual practitioner
DEA identification number will be assigned to registrants and must be provided on EVERY prescription for controlled substance.

Controlled SubstancesAdditional Law Requirements
For CIII – CV prescription drugsQuantity must be written out numerically and as a word
Vicodin, Dispense #20 (twenty)Number of refills – Limit of 5 refills within 6 monthsExpires in 6 months from date of issuance.
Controlled SubstancesAdditional Law Requirements
For CII prescription drugsEvery practitioner must register with DEA and DPS
Exemptions do not apply for outpatient prescriptions
Special prescriptions requiredTriplicateOfficial Prescription Form
Refills – No refills allowedExpiration – Expires 7 days after issuance

DPS-issued Triplicate Prescription

DPS – issued Official Prescription Form
Controlled SubstancesAdditional Law Requirements
DPS – issued Official Prescription FormAvailable since March 1, 2002Security features
Control numberPantographThermochromatic ink – “SAFE”DPS seal
Controlled SubstancesAdditional Law Requirements
DPS – issued Official Prescription FormPractitioner Responsibilities
Patient’s complete Name, Address (including city, state, zip code), and age or DOBDate the prescription is written (can not be post-dated)Controlled substance prescribedQuantity of drug, written numerically and as a wordIndication, if not deemed detrimentalPreference for brand, if necessary
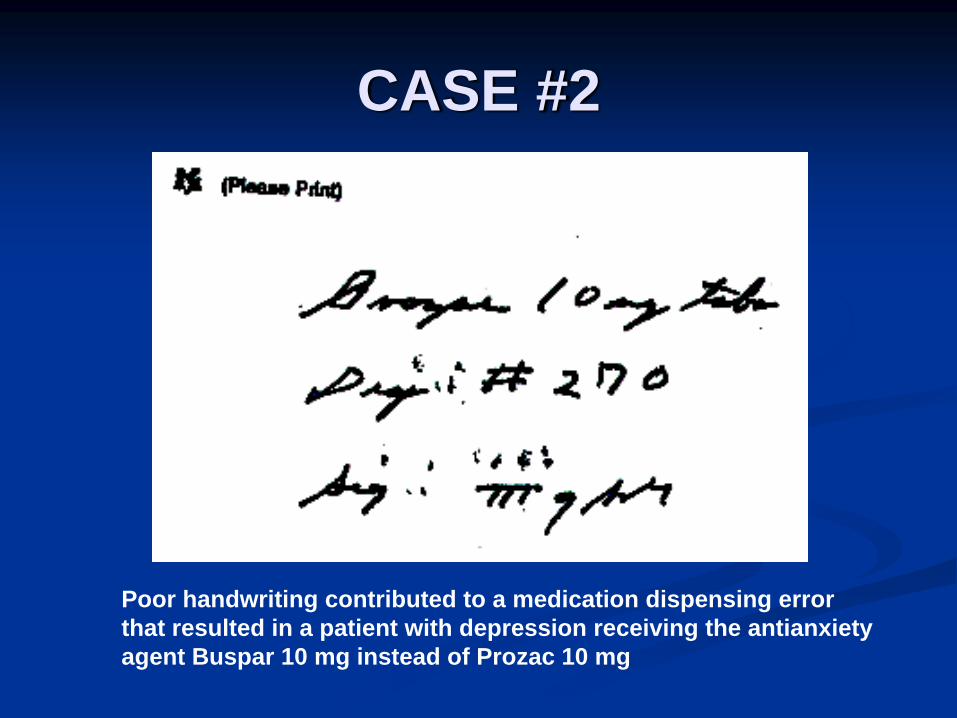
CASE #2
Poor handwriting contributed to a medication dispensing error that resulted in a patient with depression receiving the antianxiety agent Buspar 10 mg instead of Prozac 10 mg

CASE #3
A hypertensive patient accidentally received Vantin 200 mg instead of Vasotec 20 mg when a pharmacist misread this prescription
MAXIMIZE PATIENT SAFETY
ALWAYS write legibly.ALWAYS space out words and numbers to avoid confusion.ALWAYS complete medication orders.AVOID abbreviations.When in doubt, ask to verify.