Primary open reduction and fixation compared with delayed ......Fracture-dislocations of the...
8
VOL. 90-B, No. 11, NOVEMBER 2008 1499 Primary open reduction and fixation compared with delayed corrective arthrodesis in the treatment of tarsometatarsal (Lisfranc) fracture dislocation S. Rammelt, W. Schneiders, H. Schikore, M. Holch, J. Heineck, H. Zwipp From University Hospital ‘Carl Gustav Carus’, Dresden, Germany S. Rammelt, MD, PhD, Attending Trauma and Orthopaedic Surgeon W. Schneiders, MD, Trauma Surgeon M. Holch, MD, Attending Trauma Surgeon J. Heineck, MD, Attending Trauma and Orthopaedic Surgeon H. Zwipp, MD, PhD, Professor of Trauma and Reconstructive Surgery, Head of Department Clinic of Trauma & Reconstructive Surgery University Hospital “Carl Gustav Carus” , Fetscherstrasse 74, 01307 Dresden, Germany. H. Schikore, MD, Trauma Surgeon Clinic of Hand Surgery Rhön-Klinikum AG, Salzburger Leite 1, 97616 Bad Neustadt/ Saale, Germany. Correspondence should be sent to Dr S. Rammelt; e-mail: [email protected] ©2008 British Editorial Society of Bone and Joint Surgery doi:10.1302/0301-620X.90B11. 20695 $2.00 J Bone Joint Surg [Br] 2008;90-B:1499-506. Received 3 January 2008; Accepted after revision 26 June 2008 Fracture-dislocations of the tarsometatarsal (Lisfranc) joints are frequently overlooked or misdiagnosed at initial presentation. This is a comparative cohort study over a period of five years comparing primary open reduction and internal fixation in 22 patients (23 feet) with secondary corrective arthrodesis in 22 patients (22 feet) who presented with painful malunion at a mean of 22 months (1.5 to 45) after injury. In the first group primary treatment by open reduction and internal fixation for eight weeks with Kirschner-wires or screws was undertaken, in the second group treatment was by secondary corrective arthrodesis. There was one deep infection in the first group. In the delayed group there was one complete and one partial nonunion. In each group 20 patients were available for follow-up at a mean of 36 months (24 to 89) after operation. The mean American Orthopaedic Foot and Ankle Society midfoot score was 81.4 (62 to 100) after primary treatment and 71.8 (35 to 88) after corrective arthrodesis (t-test; p = 0.031). We conclude that primary treatment by open reduction and internal fixation of tarsometatarsal fracture-dislocations leads to improved functional results, earlier return to work and greater patient satisfaction than secondary corrective arthrodesis, which remains a useful salvage procedure providing significant relief of pain and improvement in function. Dislocations and fracture-dislocations of the tarsometatarsal (Lisfranc) joints are relatively uncommon with a reported frequency of 0.1% to 0.9% of all fractures. 1,2 These estimates are possibly too low, because between 20% and 40% of these injuries are either overlooked or misdiagnosed as foot sprains or isolated frac- tures of the tarsal and metatarsal bones at first presentation. 3-7 If overlooked or not treated correctly tarsometatarsal fracture-dislocations frequently result in painful malunion and impaired function. 7-12 A broad spectrum of deformity is seen, depending on the type of pri- mary injury. Most commonly, planus or planovalgus deformities associated with fore- foot abduction are seen, 13,14 but cavus defor- mity with forefoot adduction may also be encountered. 9,12,15 Several studies have shown that the best pre- dictor of a satisfactory result after tarsometa- tarsal dislocations is primary anatomical reduction and internal fixation, 3,16-19 whereas closed reduction and plaster immobilisation often leads to an unacceptable result and frequent redisplacement. 7,16 The methods of operation recommended vary from closed reduction and percutaneous fixation 20 to open reduction and internal fixation with Kirschner (K)-wires or screws, 5,6,17,20,21 or even primary arthrodesis in cases of severe comminuted fractures 21-24 or ligamentous dislocations. 18,25 Calder, Whitehouse and Saxby 26 noted signifi- cantly inferior results if operative treatment was delayed for more than six months after injury. Over a period of five years nearly as many patients with painful residual deformity fol- lowing malunited tarsometatarsal fracture- dislocations presented to our department as were treated for fresh injuries. The aim of this cohort study was to compare the medium-term results of tarsometatarsal fracture-dislocations treated primarily by a standardised protocol of open reduction and internal fixation with those treated by secondary corrective tarso- metatarsal arthrodesis for painful malunion during the same period. The preliminary short- term results of this study have been reported previously. 27 Patients and Methods Between October 1993 and October 1998, 22 patients who presented with 23 acute tarso- metatarsal fracture-dislocations were treated by primary open reduction and internal
Transcript of Primary open reduction and fixation compared with delayed ......Fracture-dislocations of the...

VOL. 90-B, No. 11, NOVEMBER 2008 1499
Primary open reduction and fixation compared with delayed corrective arthrodesis in the treatment of tarsometatarsal (Lisfranc) fracture dislocation
S. Rammelt, W. Schneiders, H. Schikore, M. Holch, J. Heineck, H. Zwipp
From University Hospital ‘Carl Gustav Carus’, Dresden, Germany
S. Rammelt, MD, PhD, Attending Trauma and Orthopaedic Surgeon
W. Schneiders, MD, Trauma Surgeon
M. Holch, MD, Attending Trauma Surgeon
J. Heineck, MD, Attending Trauma and Orthopaedic Surgeon
H. Zwipp, MD, PhD, Professor of Trauma and Reconstructive Surgery, Head of DepartmentClinic of Trauma & Reconstructive SurgeryUniversity Hospital “Carl Gustav Carus”, Fetscherstrasse 74, 01307 Dresden, Germany.
H. Schikore, MD, Trauma SurgeonClinic of Hand SurgeryRhön-Klinikum AG, Salzburger Leite 1, 97616 Bad Neustadt/Saale, Germany.
Correspondence should be sent to Dr S. Rammelt; e-mail: [email protected]
©2008 British Editorial Society of Bone and Joint Surgerydoi:10.1302/0301-620X.90B11. 20695 $2.00
J Bone Joint Surg [Br] 2008;90-B:1499-506.Received 3 January 2008; Accepted after revision 26 June 2008
Fracture-dislocations of the tarsometatarsal (Lisfranc) joints are frequently overlooked or misdiagnosed at initial presentation. This is a comparative cohort study over a period of five years comparing primary open reduction and internal fixation in 22 patients (23 feet) with secondary corrective arthrodesis in 22 patients (22 feet) who presented with painful malunion at a mean of 22 months (1.5 to 45) after injury. In the first group primary treatment by open reduction and internal fixation for eight weeks with Kirschner-wires or screws was undertaken, in the second group treatment was by secondary corrective arthrodesis. There was one deep infection in the first group. In the delayed group there was one complete and one partial nonunion.
In each group 20 patients were available for follow-up at a mean of 36 months (24 to 89) after operation. The mean American Orthopaedic Foot and Ankle Society midfoot score was 81.4 (62 to 100) after primary treatment and 71.8 (35 to 88) after corrective arthrodesis (t-test; p = 0.031).
We conclude that primary treatment by open reduction and internal fixation of tarsometatarsal fracture-dislocations leads to improved functional results, earlier return to work and greater patient satisfaction than secondary corrective arthrodesis, which remains a useful salvage procedure providing significant relief of pain and improvement in function.
Dislocations and fracture-dislocations of thetarsometatarsal (Lisfranc) joints are relativelyuncommon with a reported frequency of 0.1%to 0.9% of all fractures.1,2 These estimates arepossibly too low, because between 20% and40% of these injuries are either overlooked ormisdiagnosed as foot sprains or isolated frac-tures of the tarsal and metatarsal bones at firstpresentation.3-7 If overlooked or not treatedcorrectly tarsometatarsal fracture-dislocationsfrequently result in painful malunion andimpaired function.7-12 A broad spectrum ofdeformity is seen, depending on the type of pri-mary injury. Most commonly, planus orplanovalgus deformities associated with fore-foot abduction are seen,13,14 but cavus defor-mity with forefoot adduction may also beencountered.9,12,15
Several studies have shown that the best pre-dictor of a satisfactory result after tarsometa-tarsal dislocations is primary anatomicalreduction and internal fixation,3,16-19 whereasclosed reduction and plaster immobilisationoften leads to an unacceptable result andfrequent redisplacement.7,16 The methods ofoperation recommended vary from closedreduction and percutaneous fixation20 to open
reduction and internal fixation with Kirschner(K)-wires or screws,5,6,17,20,21 or even primaryarthrodesis in cases of severe comminutedfractures21-24 or ligamentous dislocations.18,25
Calder, Whitehouse and Saxby26 noted signifi-cantly inferior results if operative treatment wasdelayed for more than six months after injury.
Over a period of five years nearly as manypatients with painful residual deformity fol-lowing malunited tarsometatarsal fracture-dislocations presented to our department aswere treated for fresh injuries. The aim of thiscohort study was to compare the medium-termresults of tarsometatarsal fracture-dislocationstreated primarily by a standardised protocol ofopen reduction and internal fixation withthose treated by secondary corrective tarso-metatarsal arthrodesis for painful malunionduring the same period. The preliminary short-term results of this study have been reportedpreviously.27
Patients and MethodsBetween October 1993 and October 1998, 22patients who presented with 23 acute tarso-metatarsal fracture-dislocations were treatedby primary open reduction and internal

1500 S. RAMMELT, W. SCHNEIDERS, H. SCHIKORE, M. HOLCH, J. HEINECK, H. ZWIPP
THE JOURNAL OF BONE AND JOINT SURGERY
fixation (group A) (Table I). During the same period, 22patients presented with residual deformity after tarso-metatarsal dislocation and were treated by secondary cor-rective tarsometatarsal arthrodesis at a mean of22 months (1.5 to 45) after the initial injury (group B)(Table I). The shortest time between injury and surgery ingroup B was six weeks in a patient who had alreadypresented with a fixed deformity at that time. Primarytreatment in group B consisted of open reduction and K-wire fixation in three patients, closed reduction and K-wire fixation in four, and closed reduction followed byimmobilisation in a plaster cast in seven. In eight of the 22patients the diagnosis had been missed on first presenta-tion and no specific treatment had been initiated.Conservative measures such as change of footwear, phys-ical therapy, pain medication and walking aids had allfailed to relieve symptoms prior to surgery.
Six of the patients in group A and five in group B hadmultiple injuries at the time of the accident, reflecting thehigh-energy type of injury often associated with tarso-metatarsal fracture-dislocations. Four patients in eachgroup also had an injury to the mid-tarsal (Chopart) joint.The overall pattern of injury was comparable between thetwo groups (Table I). Patients with crush injuries to thefoot, those with neurological disorders or pre-existingdeformity of the foot, and those who did not give theirconsent, were excluded from the study.
Standard radiographs in anteroposterior (the tubetilted20° caudally), lateral and oblique (45°) projections wereobtained in all patients with acute injuries.28,29 Weight-bearing radiographs of both feet in anteroposterior andlateral projections were obtained prior to secondarycorrective arthrodesis7 and at follow-up (Fig. 1).Primary open reduction and internal fixation (group A). Sur-gery was performed under general or spinal anaesthesia.The medial column of the tarsometatarsal joint wasapproached by a dorsal longitudinal incision centred overthe space between the first and second metatarsocuneiform
joints extending from the cuneiform bones to the proximalshaft of the metatarsals. In the presence of an acute com-partment syndrome the incision was extended to the distalextensor retinaculum to complete a dorsomedial fas-ciotomy.30 Reduction was begun at the second metatarso-cuneiform joint, which is considered the ‘keystone’ of thetarsometatarsal joints.1,7,31 If there was an additional frac-ture of the base of the second metatarsal, anatomical reduc-tion and fixation was attempted with 2.0 mm mini-fragment screws. Very small, irreducible fragments wereremoved. The second metatarsal was then brought intoalignment with the intermediate cuneiform and temporarilyfixed with a retrograde K-wire. The first and third meta-tarsals were then reduced and fixed in the same manner.Once reduction of the first to third metatarsocuneiformjoints was achieved, the position and stability of the fourthand fifth metatarsals was assessed. If the lateral metatarsalshad reduced spontaneously and were clinically stable, nofurther treatment was undertaken. If the fourth and fifthmetatarsals tended to sublux, they were fixed percutaneouslywith additional K-wires. If percutaneous reduction could notbe achieved because of additional fractures or soft-tissueinterposition, open reduction and internal fixation to thecuboid was carried out via a second, dorsolateral approachover the fourth intermetatarsal space.
Fixation was achieved with K-wires in 11 feet, with screwsin eight and small fragment plates (supplemented by screwsor K-wires) in four. In patients with multiple injuries andthose with severe soft-tissue damage, K-wire fixation waschosen as the definitive treatment, supplemented by tempo-rary external tibiometatarsal transfixation if there was grossinstability or soft-tissue laceration (Fig. 2). If K-wires wereused for definitive fixation, they were shortened and buriedsubcutaneously. If fixation with K-wires appeared inade-quate, they were replaced by 2.5 mm to 3.5 mm corticalscrews, depending on the size of the bone. The screws wereintroduced in a retrograde fashion from the base of the meta-tarsal to the corresponding cuneiform, and countersunk in
Table I. Patient characteristics
Group A (primary open reduction and temporary internal fixation)
Group B (secondary corrective arthrodesis)
Number of patients (feet) 22 (23) 22 (22)Male:female 17:5 15:7Mean age at time of injury (range) 35 (17 to 76) 39 (24 to 60)
Fracture classification (Quénu and Küss35)Homolateral 12 15Isolated 5 3Divergent 6 4
Polytrauma/multiple injuries 6 5Mean time to surgery in months (range) 0 22 (1.5 to 45)Time to follow-up in 20 available patients in each group inmonths (range)
37 (24 to 89) 35 (26 to 47)

PRIMARY OPEN REDUCTION COMPARED WITH DELAYED CORRECTIVE ARTHRODESIS IN FRACTURE DISLOCATION 1501
VOL. 90-B, No. 11, NOVEMBER 2008
order not to irritate the extensor tendons. Realignment of thetarsometatarsal joints was assessed with intra-operativelateral, oblique and dorsoplantar radiographs.
A short-leg cast was applied post-operatively for seven toten days. External fixation was used until soft-tissue swell-ing had subsided, usually for less than 14 days. After screwor plate fixation patients were mobilised in their own shoeswith a hard sole. After K-wire fixation a cast shoe wasapplied for six weeks. All patients were restricted to partialweight-bearing (20 kg) for eight weeks. The hardware wasremoved after that time and weight-bearing was graduallyincreased over the following two weeks.Secondary corrective arthrodesis (group B). In patients withresidual deformity the extent of the arthrodesis dependedon the number of affected joints and the degree of defor-mity. One or two parallel longitudinal dorsal incisionswere made over the first and fourth web spaces. Allfibrous and scar tissue, remaining cartilage, subchondraland non-viable bone was removed from the joints. Wherethere was substantial deformity or structural bone loss thedefect was filled with a tricortical bone graft from the ipsi-lateral iliac crest, and occasionally with local osteophytes.Axial malalignment and forefoot abduction/adductionwere corrected, starting with the first or secondmetatarsocuneiform joint. If realignment was satisfactoryas judged by intra-operative fluoroscopy, the medial col-umn was fused with compression screws, including theinter-cuneiform and naviculocuneiform joints if necessary.In 14 of 22 feet the fourth and fifth metatarsals could bereduced into the anatomical position once realignment ofthe medial column had been achieved (Fig. 3). They were
fused to the cuboid in the remaining eight feet when therewas severe damage to the fourth and fifth tarsometatarsaljoints. Final radiographs were taken in the three standardprojections described previously.
A short-leg cast was applied post-operatively for seven toten days and then replaced by a cast shoe that was worn foreight weeks. Full weight-bearing was allowed within thecast shoe except in patients with poor bone quality or afterbone grafting. These patients were restricted to partialweight-bearing (20 kg) for eight weeks.Follow-up. Patients were followed by a clinical examinationand gait function tests, such as toe- and heel-gait, squatting,jumping etc. The Maryland foot score16,32 and AmericanOrthopaedic Foot and Ankle Society (AOFAS) midfootscore33 were used to quantify the functional outcome. Bothinclude several objective and subjective criteria. Patientsfilled in a questionnaire on their level of activity, satisfac-tion with treatment and activities of daily living (ADL).Lateral and dorsoplantar weight-bearing radiographs aswell as 45° oblique views of the foot were taken.
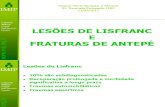
The following radiological measurements were used forevaluation: the talus-first metatarsal angle (in lateral anddorsoplantar views), the distance between the base of thefirst and second metatarsal in the dorsoplantar view, thealignment of the third metatarsal with the lateral cuneiformin the oblique view, and the distance between the base ofthe fifth metatarsal and cuboid in the lateral view(Fig. 1).28,34 Differences in outcome between the twogroups were evaluated with a two-sample Student’s t-testafter testing the groups for normality. Statisticalsignificance was assumed at p < 0.05.
Fig. 1b
Radiographs showing characteristics used for follow-up: TFMA, talus first metatarsal angle(dotted line, measured in lateral and anteroposterior weight-bearing radiographs: the latterwith 20° caudally tilted tube), distance between first and second metatarsal base (MT 1-2 dis-tance (mm), arrows in the anteroposterior view), and distance between plantar aspect of thefifth metatarsal base and the cuboid (Cuboid-MT 5 distance (mm), double-arrow in the lateralview).
Fig. 1a

1502 S. RAMMELT, W. SCHNEIDERS, H. SCHIKORE, M. HOLCH, J. HEINECK, H. ZWIPP
THE JOURNAL OF BONE AND JOINT SURGERY
ResultsComplications. In group A (22 patients, 23 feet) there wasone soft-tissue infection and one superficial wound edgenecrosis. Two patients developed a compartment syndromeof the foot which required fasciotomy within 24 hours of
injury. One patient had a sensory deficit of the dorsum ofthe midfoot after fasciotomy for compartment syndrome,indicating a lesion of the superficial peroneal nerve. Nohaematomas and no vascular injuries were seen. All frac-tures healed uneventfully with no sign of delayed or non-
Fig. 2g
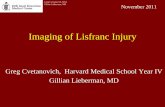
Radiographs showing a 21-year-old man who sustained a lateral dislocation of the whole tarsometatarsal joint (a-b) and a compartment syndromein a motorcycle accident.Fasciotomy, irrigation, open reduction and internal fixation were performed as an emergency. Because of the critical con-dition of the soft tissues, K-wires were used for fixation and supplemented by a tibiometatarsal external fixator for ten days (c-d). Secondary woundclosure was performed within five days. K-wires were removed at eight weeks. Seven years after the injury weight-bearing radiographs show goodalignment of the foot (e-f). Photograph showing satisfactory clinical outcome with an American Orthopaedic Foot and Ankle Society midfoot scoreof 90 and good foot function despite residual clawing of the toes secondary to the compartment syndrome (g).
Fig. 2a Fig. 2b Fig. 2c
Fig. 2d Fig. 2e
Fig. 2f

PRIMARY OPEN REDUCTION COMPARED WITH DELAYED CORRECTIVE ARTHRODESIS IN FRACTURE DISLOCATION 1503
VOL. 90-B, No. 11, NOVEMBER 2008
union. No implant failure was seen during the eight weeksof temporary fixation.
In group B (22 feet) there was one partial and one com-plete nonunion. The patient with the complete nonunionhad a soft-tissue infection after initial treatment withincomplete open reduction and K-wire fixation. Thispatient was not satisfied with the result of the arthrodesis,but declined further surgery. Another patient developed anisolated nonunion of the first metatarsocuneiform joint.However, he was satisfied with the result and declined fur-ther surgery. His overall functional result was fair. In onefoot a haematoma of the midfoot required decompressionon the second post-operative day, but the wound healeduneventfully. No superficial or deep infection and nowound necrosis were seen in this group. Implant failure ofone or two screws was observed in four of 22 patients, onein the patient with complete nonunion. Implant failure wasasymptomatic in the other three patients who had a solidunion on the radiographs and no further treatment wasundertaken.
Clinical results. In each group, 20 patients were followed upfor a mean of three years (two to 7.4) post-operatively. Themain clinical and radiographic findings are summarised inTable II. Subjectively, in group A all but one patient were sat-isfied with the result. In group B, two patients, among themone with complete nonunion, were not satisfied. Consideringthe severe functional limitation before secondary correctivearthrodesis, all but one of the 20 stated that, given the samecircumstances, they would undergo surgery again.
The mean Maryland foot score was 85.0 in group Acompared with 76.2 in group B (t-test; p = 0.027). In groupB the mean value before arthrodesis was 37.2 (18 to 66),indicating a significant functional improvement aftersurgery (t-test; p = 0.001). The mean AOFASmidfoot score was 81.4 in group A compared with 71.8 ingroup B (t-test; p = 0.031). Again, there was a substantialimprovement in the scores in the latter group, compared withthe mean value before surgery, which was 17.9 (0 to 55). Thedifference was highly significant (t-test; p = 0.001). Subjec-tively, the patients rated their functional results as excellent in
Fig. 3d
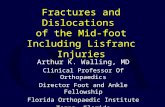
Radiographs showing a 60-year-old man who presented with painful deformity ten months after a homolateral fracture-dislocation sustained duringa fall from a ladder. The injury was initially diagnosed as a metatarsal fracture and treated conservatively. Note the plantar dislocation of the medialcuneiform and cuboid (arrow) with respect to the base of the fifth metatarsal in the lateral view (a) compared with the uninjured side (b), and theincreased distance between the first and second metatarsal base in the dorsoplantar view (c). Correction of the deformity was followed by fusion ofthe medial column. At 37 months after fusion, correction was maintained and the radiographic parameters were similar to those of the uninjured side(d-e). The patient reported significant pain relief and full return to work and activities of daily living.
Fig. 3c Fig. 3e
Fig. 3a Fig. 3b

1504 S. RAMMELT, W. SCHNEIDERS, H. SCHIKORE, M. HOLCH, J. HEINECK, H. ZWIPP
THE JOURNAL OF BONE AND JOINT SURGERY
seven, good in six, and fair in seven after primary openreduction and internal fixation. After secondary correctivearthrodesis the functional results were rated excellent inthree, good in nine, fair in six, and poor in two. In group B,given the numbers available, we found no difference in out-come between 13 patients treated by fusion of the medialcolumn only and seven patients with fusion of all thetarsometatarsal joints.Radiographic results. The measurements of the talus-firstmetatarsal angle in the anteroposterior and lateral weight-bearing radiographs, the distance between the base of thefirst and second metatarsals in the anteroposterior weight-bearing radiographs, and the distance between the base ofthe fifth metatarsal and the cuboid in the lateral weight-bearing radiographs were close to the normal values28 forboth groups (Table II). With the numbers available, no sta-tistically significant differences between the two groupswere seen for any of these observations.
DiscussionThe assessment and management of tarsometatarsal fracture-dislocations has changed considerably since the first system-atic studies by Quénu and Küss almost 100 years ago,35
although their classification is still in use today with somemodifications.2,16 Treatment has changed from closed reduc-tion with or without K-wire fixation1,36,37 to open reductionand internal fixation with either K-wires or screws.6,16-19,26
Fractures and dislocations of the tarsometatarsal(Lisfranc) joint are frequently overlooked or misdiag-nosed.7,9,12 In our experience this is because of the low inci-dence of these injuries, the variation in the pattern of injuryand clinical presentation. There is a lack of knowledge of
the specific clinical signs and radiological projections suchas the plantar ecchymosis sign,38 linked toe dislocation1
and the fleck sign at the base of the second metatarsal.16,39
Furthermore, tarsometatarsal injuries are often seen inpatients with multiple injuries.6,17,19 The importance ofcareful physical and radiological examination of thesepatients cannot be overestimated.29,30 As a result, over aperiod of five years, nearly as many patients presented toour department with painful residual deformities aftermalunion of tarsometatarsal fracture-dislocations as weretreated during the same period for acute injuries to the tar-sometatarsal joint. In more than one-third of the patients ingroup B the diagnosis of tarsometatarsal dislocation hadbeen missed completely at the initial examination. Thisobservation led us to prospectively follow-up the patientsfrom both groups with a standard protocol and to comparethe final outcome at a minimum of two years.
The patients who presented with painful arthritisand residual deformity after tarsometatarsal fracture-dislocation had been treated initially with open reductionand K-wire fixation in only three of the 22 cases. Closedreduction was attempted and followed by K-wire fixationin four and closed reduction followed by plaster immobili-sation in seven. We believe, as do other authors,6,16-20,26
that closed reduction is not sufficient to achieve anatomicalreduction in the majority of tarsometatarsal fracture-dislocations because of interposed soft tissue and smallbony fragments from fractures of the base of the meta-tarsals. Typically, a fracture of the base of the second meta-tarsal is associated with the homolateral type ofdislocation.16 Immobilisation in plaster alone is not ade-quate to maintain reduction.
Table II. Summary of main functional and radiographic results (20 patients of each group)
Group A (primary open reduction and temporary internal fixation)
Group B (secondary corrective arthrodesis) p-value (t-test)
AOFAS* midfoot scale (range) 81.4 (62 to 100) 71.8 (35 to 88) 0.031Pain 32.5 (20 to 40) 28.5 (20 to 40) 0.019Function 36.4 (27 to 45) 32.3 (24 to 42) 0.017Alignment 12.5 (8 to 15) 11.3 (0 to 15) NS†
Maryland foot score (range) 85.0 (70 to 100) 76.2 (39 to 92) 0.027Pain 39.8 (30 to 45) 35.8 (10 to 45) 0.048Function 34.0 (26 to 38) 30.4 (24 to 35) < 0.001Aspect 7.3 (2 to 10) 7.1 (2 to 10) NSMotion 3.9 (2 to 5) 2.9 (0 to 4) 0.013
Radiographic measurement (range)TFMA‡ in degrees (anteroposterior view)
6.9 (-3 to 16) 4.7 (-6 to 15) NS
TFMA in degrees (lateral view) 0.6 (-5 to 7) 0.3 (-20 to 16) NSMT§ 1-2 distance in mm 1.1 (0 to 3) 1.3 (0 to 3) NSCuboid - MT 5 distance in mm 5.2 (0 to 10) 5.7 (0 to 14) NS
* AOFAS, American Orthopaedic Foot and Ankle Society† NS, not significant‡ TFMA, talus first metatarsal angle (a negative value indicates abduction in the anteroposterior view and flat foot in the lateral view)§ MT, metatarsal base (see Figure 1 for detailed description)

PRIMARY OPEN REDUCTION COMPARED WITH DELAYED CORRECTIVE ARTHRODESIS IN FRACTURE DISLOCATION 1505
VOL. 90-B, No. 11, NOVEMBER 2008
Whether to use K-wires or screws for internal fixation iscontroversial. Although some authors prefer K-wire fixa-tion,2,3,40-42 others opt for screw fixation after open reduc-tion of tarsometatarsal fracture-dislocations.17-19,43-45
Although a few reports show a slightly higher failure rateafter K-wire fixation,9,17,19,46 there is no clear evidencefrom these studies on the superiority of either method oftreatment. We observed failure of previous K-wire fixationin three patients who presented for correction and thereforewe gradually shifted from K-wire to screw fixation for pri-mary treatment. However, we have shown no difference inoutcome between the patients treated with K-wires andscrews, and no loss of correction after K-wire fixation. Weprefer K-wires in patients with multiple injuries, in caseswhere the condition of the soft tissues is critical and whencomminuted fractures of the metatarsal bases do not allowadequate purchase for a screw.
There is no clear evidence on how long to maintain fixa-tion after primary open reduction. K-wires are usuallyremoved after eight weeks but screws are left in place forthree to 36 months.6,18,20 Some advocate their removal onlyin symptomatic patients.18,25,47 In our practice K-wires andscrews are removed eight weeks after surgery, and thenweight-bearing is increased gradually over the following twoweeks. With this regime no secondary displacement wasobserved in this study. We believe that eight weeks of fixationis sufficient to maintain reduction.
Secondary corrective arthrodesis resulted in a significantreduction of pain and an improvement in function after ini-tially overlooked or misdiagnosed tarsometatarsal fracture-dislocations, which is in accordance with recent studies.5,9,14
However, in the 20 of 22 patients in each group in this studyfollowed up at a mean of three years after treatment, primaryopen reduction and internal fixation gave significantly betterfunctional results and an earlier return to work than second-ary corrective arthrodesis. Because anatomical reconstruc-tion, as judged by the radiological parameters, could beachieved in both treatment groups, the difference in theresults must be attributed to other factors. Long-standingdeformity and soft-tissue contraction require extensive surgi-cal exposure and sometimes bone grafting, which may causea greater amount of scarring in the secondary arthrodesisgroup. Fusion of the tarsometatarsal joint results in increasedstiffness of the midfoot, whereas K-wires and screws wereremoved after eight weeks in the primary treatment group.This may lead to residual pain and functional impairment,such as difficulty in walking over uneven ground and altera-tions in footwear. This may be reflected by the scores shownin the subcategories in Table II. The main differencesbetween the two groups were in the pain and function scores,with no significant differences in alignment and aspect.
It has been suggested that results after fusion of the wholetarsometatarsal joint are inferior to those after fusion of thefirst to third metatarsocuneiform joints only because of theremaining mobility in the fourth and fifth metatarsocuboidjoints.5,9,46 In the author’s practice fusion was limited to the
medial column in the majority of cases (Fig. 2). However, inthe present study no difference in outcome was seen betweenpatients with fusion of the medial column and those withfusion of the whole tarsometatarsal joint.
The high satisfaction rate in 18 of the 20 patients in thesecondary arthrodesis group despite inferior functionalresults may be attributed to the relief of pain and significantfunctional improvement compared to the pre-operative state.Patients treated by secondary arthrodesis had an averageperiod of 22 months (1.5 to 45) with pain and poor functionof the foot, during which the majority were unable to work.The experience of a painful disability and the resulting socio-economic costs should not be underestimated in thesepatients. Therefore, a wait-and-see attitude should not beadopted when dealing with these injuries. Some earlierauthors13,36 have concluded even gross deformity after pri-mary conservative treatment of tarsometatarsal fracture-dislocations did not lead to functional impairment and resid-ual pain, and thus secondary arthrodesis was not required.The results of this study and the observations of otherauthors that anatomical reduction is the most important pre-dictor of good or excellent results after tarsometatarsal frac-ture-dislocations3,16-19,26,40 contradict these earlier studies.
ConclusionsPrimary treatment of tarsometatarsal (Lisfranc) fracture-dislocations with open reduction and internal fixation leadsto significant better functional results than does secondarycorrective arthrodesis for malunited fracture-dislocations.Care should be taken to not overlook the sometimes subtleclinical and radiographic signs of these injuries, as residualdeformities can lead to severe functional impairment. Ahigh index of suspicion is required in patients with multipleinjuries, who make up a considerable part of the patientcohort with tarsometatarsal injuries. Closed reduction ofcomplex tarsometatarsal dislocations is not encouraged,because anatomical reduction is an important predictor ofoutcome. In cases of painful malunion, secondary correc-tive arthrodesis provides significant relief of pain andimprovement in function.
No benefits in any form have been received or will be received from a commer-cial party related directly or indirectly to the subject of this article.
References1. English TA. Dislocations of the metararsal bone and adjacent toe. J Bone Joint Surg
[Br] 1964;46-B:700-4.2. Hardcastle PH, Reschauer R, Kutscha-Lissberg E, Schoffmann W. Injuries to
the tarsometatarsal joint: incidence, classification and treatment. J Bone Joint Surg[Br] 1982;64-B:349-56.
3. Goossens M, De Stoop N. Lisfranc’s fracture-dislocations: etiology, radiology, andresults of treatment: a review of 20 cases. Clin Orthop 1983;176:154-62.
4. Vuori JP, Aro HT. Lisfranc joint injuries: trauma mechanisms and associated injuries.J Trauma 1993;35:40-5.
5. Komenda GA, Myerson MS, Biddinger KR. Results of arthrodesis of the tarso-metatarsal joints after traumatic injury. J Bone Joint Surg [Am] 1996;78-A:1665-76.
6. Randt T, Dahlen C, Schikore H, Zwipp H. Dislocation fractures in the area of themiddle foot: injuries of the Chopart and Lisfranc joint. Zentralbl Chir 1998;123:1257-66 (in German).
7. Zwipp H, Rammelt S, Holch M, Dahlen C. Lisfranc arthrodesis after malunutedfracture healing. Unfallchirurg 1999;102:918-23 (in German).

1506 S. RAMMELT, W. SCHNEIDERS, H. SCHIKORE, M. HOLCH, J. HEINECK, H. ZWIPP
THE JOURNAL OF BONE AND JOINT SURGERY
8. Myerson M. The diagnosis and treatment of injuries to the Lisfranc joint complex.Orthop Clin North Am 1989;20:655-64.
9. Sangeorzan BJ, Veith RG, Hansen ST Jr. Salvage of Lisfranc’s tarsometatarsaljoint by arthrodesis. Foot Ankle 1990;10:193-200.
10. Petje G, Schiller C, Steinbock G. Mobile flatfoot as a sequela of dislocation injuryof the Lisfranc joint: a retrospective analysis of 13 patients. Unfallchirurg1997;100:787-91 (in German).
11. Mann RA, Prieskorn D, Sobel M. Mid-tarsal and tarsometatarsal arthrodesis forprimary degenerative osteoarthrosis or osteoarthrosis after trauma. J Bone Joint Surg[Am] 1996;78-A:1376-85.
12. Rammelt S, Schneiders W, Zwipp H. Corrective tarsometatarsal arthrodesis formalunion after fracture dislocation. Orthopäde 2006;35:435-42 (in German).
13. Brunet JA, Wiley JJ. The late results of tarsometatarsal joint injuries. J Bone JointSurg [Br] 1987;69-B:437-40.
14. Horton GA, Olney BW. Deformity correction and arthrodesis of the midfoot with amedial plate. Foot Ankle 1993;14:493-9.
15. Besse JL, Kasmaoui EH, Lerat J-L, Moyen B. Tarso-metatarsal fracture-disloca-tion: treatment by percutaneous pinning or open reduction (a report on 17 cases). FootAnkle Surg 2005;11:17-23.
16. Myerson MS, Fisher RT, Burgess AR, Kenzora JE. Fracture dislocations of thetarsometatarsal joints: end results correlated with pathology and treatment. FootAnkle 1986;6:225-42.
17. Arntz CT, Veith RG, Hansen ST Jr. Fractures and fracture-dislocations of the tarso-metatarsal joint. J Bone Joint Surg [Am] 1988;70-A:173-81.
18. Kuo RS, Tejwani NC, DiGiovanni CW, et al. Outcome after open reduction andinternal fixation of Lisfranc joint injuries. J Bone Joint Surg [Am] 2000;82-A:1609-18.
19. Richter M, Thermann H, Hüfner T, Schmidt U, Krettek C. Aetiology, treatmentand outcome in Lisfranc joint dislocations and fracture dislocations. Foot Ankle Surg2002;8:21-32.
20. Myerson MS. The diagnosis and treatment of injury to the tarsometatarsal jointcomplex. J Bone Joint Surg [Br] 1999;81-B:756-63.
21. Mulier T, Teynders P, Sioen W, et al. The treatment of Lisfranc injuries. ActaOrthop Belg 1997;63:82-90.
22. Granberry WM, Lipscomb PR. Dislocation of the tarsometatarsal joints. SurgGynecol Obstet 1962;114:467-9.
23. Jarde O, Trinquier Lautard JL, Filloux JF, de Lestang M, Vives P. Lisfranc’s frac-ture-dislocation. Rev Chir Orthop Reparatrice Appar Mot 1995;81:724-30 (in French).
24. Mulier T, Reynders P, Dereymaeker G, Broos P. Severe Lisfrancs injuries: primaryarthrodesis or ORIF? Foot Ankle Int 2002;23:902-5.
25. Ly TV, Coetzee JC. Treatment of primarily ligamentous Lisfranc joint injuries: primaryarthrodesis compared with open reduction and internal fixation: a prospective, ran-domized study. J Bone Joint Surg [Am] 2006;88-A:514-20.
26. Calder JD, Whitehouse SL, Saxby TS. Results of isolated Lisfranc injuries and theeffect of compensation claims. J Bone Joint Surg [Br] 2004;86-B:527-30.
27. Rammelt S, Schikore H, Holch M, Heinz P, Zwipp H. Primary vs delayed treat-ment of tarsometatarsal fracture dislocation. American Orthopaedic Foot and AnkleSociety, 19th Annual Summer Meeting, 2003:91.
28. Foster SC, Foster RR. Lisfranc’s tarsometatarsal fracture-dislocation. Radiology1976;120:79-83.
29. Suren EG, Zwipp H. Acute ligamentous injuries of the Chopart and Lisfranc jointline. Orthopäde 1986;15:479-86 (in German).
30. Zwipp H. Chirugie des Fusses. Wien: Springer-Verlag, 1994.
31. Hesp WL, van der Werken C, Goris RJ. Lisfranc dislocations: fractures and/or dis-locations through the tarso-metatarsal joints. Injury 1984;15:261-6.
32. Sanders R, Fortin P, DiPasquale A, Walling D. Operative treatment in 120 dis-placed intraarticular calcaneal fractures: results using a prognostic computed tomog-raphy scan classification. Clin Orthop 1993;290:87-95.
33. Kitaoka H, Alexander I, Adelaar R, et al. Clinical rating systems for the ankle,hindfoot, midfoot, hallux and lesser toes. Foot Ankle Int 1994;15:349-53.
34. Faciszewski T, Burks RT, Manaster BJ. Subtle injuries of the Lisfranc joint. JBone Joint Surg [Am] 1990;72-A:1519-22.
35. Quénu E, Küss G. Études sur les luxations du métatarse. Rev de Chir 1909;39:281-336, 730-91, 1094-145.
36. Aitken AP, Poulson D. Dislocations of the tarsometatarsal joint. J Bone Joint Surg[Am] 1963;45-A:246-60.
37. Resch S, Stenstrom A. The treatment of tarsometatarsal injuries. Foot Ankle1990;11:117-23.
38. Ross G, Cronin R, Hauzenblas J, Juliano P. Plantar ecchymosis sign: a clinical aid todiagnosis of occult Lisfranc tarsometatarsal injuries. J Orthop Trauma 1996;10:119-22.
39. Jeffreys TE. Lisfranc’s fracture-dislocation: a clinical and experimental study oftarso-metatarsal dislocations and fracture-dislocations. J Bone Joint Surg [Br]1963;45-B:546-51.
40. Pérez Blanco R, Rodrígues Merchán C, Canosa Sevillano R, Munuera Mar-tínez L. Tarsometatarsal fractures and dislocations. J Orthop Trauma 1988;2:188-94.
41. Tan YH, Chin TW, Mitra AK, Tan SK. Tarsometatarsal (Lisfranc’s) injuries: results ofopen reduction and internal fixation. Ann Acad Med Singapore 1995;24:816-19.
42. Dudko S, Kusz D, Pierchaa A. Lisfranc injury: fixation with Kirschner wires. FootAnkle Surg 2004;10:5-8.
43. Curtis MJ, Myerson M, Szura B. Tarsometatarsal joint injuries in the athlete. AmJ Sports Med 1993;21:497-502.
44. Rosenberg GA, Patterson BM. Tarsometatarsal (Lisfranc’s) fracture-dislocation.Am J Orthop 1995;Suppl:7-16.
45. Buzzard BM, Briggs PJ. Surgical management of acute tarsometatarsal fracturedislocation in the adult. Clin Orthop 1998;353:125-33.
46. Lin SS, Bono CM, Treuting R, Shereff MJ. Limited intertarsal arthrodesis usingbone grafting and pin fixation. Foot Ankle Int 2000;21:742-8.
47. Sands AK, Grose A. Lisfranc injuries. Injury 2004;35(Suppl 2):71-6.