Prevention of VTE in Nonsurgical Patients : Antithrombotic ...umg.umdnj.edu/gim/consult_manual/VTE...
102
DOI 10.1378/chest.11-2296 2012;141;e195S-e226S Chest Russell C. Klein, Hoang Le, Sam Schulman and M. Hassan Murad Francesco Dentali, Elie A. Akl, Deborah J. Cook, Alex A. Balekian, Susan R. Kahn, Wendy Lim, Andrew S. Dunn, Mary Cushman, Practice Guidelines Chest Physicians Evidence-Based Clinical Thrombosis, 9th ed: American College of Antithrombotic Therapy and Prevention of Prevention of VTE in Nonsurgical Patients : http://chestjournal.chestpubs.org/content/141/2_suppl/e195S.full.html services can be found online on the World Wide Web at: The online version of this article, along with updated information and e195S.DC1.html http://chestjournal.chestpubs.org/content/suppl/2012/02/03/141.2_suppl. Supplemental material related to this article is available at: ISSN:0012-3692 ) http://chestjournal.chestpubs.org/site/misc/reprints.xhtml ( written permission of the copyright holder. this article or PDF may be reproduced or distributed without the prior Dundee Road, Northbrook, IL 60062. All rights reserved. No part of Copyright2012by the American College of Chest Physicians, 3300 Physicians. It has been published monthly since 1935. is the official journal of the American College of Chest Chest © 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012 chestjournal.chestpubs.org Downloaded from
-
Upload
truongdiep -
Category
Documents
-
view
214 -
download
0
Transcript of Prevention of VTE in Nonsurgical Patients : Antithrombotic ...umg.umdnj.edu/gim/consult_manual/VTE...

DOI 10.1378/chest.11-2296 2012;141;e195S-e226SChest
Russell C. Klein, Hoang Le, Sam Schulman and M. Hassan MuradFrancesco Dentali, Elie A. Akl, Deborah J. Cook, Alex A. Balekian, Susan R. Kahn, Wendy Lim, Andrew S. Dunn, Mary Cushman, Practice GuidelinesChest Physicians Evidence-Based Clinical Thrombosis, 9th ed: American College ofAntithrombotic Therapy and Prevention of Prevention of VTE in Nonsurgical Patients :
http://chestjournal.chestpubs.org/content/141/2_suppl/e195S.full.html
services can be found online on the World Wide Web at: The online version of this article, along with updated information and
e195S.DC1.html http://chestjournal.chestpubs.org/content/suppl/2012/02/03/141.2_suppl.Supplemental material related to this article is available at:
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
written permission of the copyright holder.this article or PDF may be reproduced or distributed without the priorDundee Road, Northbrook, IL 60062. All rights reserved. No part of Copyright2012by the American College of Chest Physicians, 3300Physicians. It has been published monthly since 1935.
is the official journal of the American College of ChestChest
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

CHEST Supplement
www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e195S
ANTITHROMBOTIC THERAPY AND PREVENTION OF THROMBOSIS, 9TH ED: ACCP GUIDELINES
Background: This guideline addressed VTE prevention in hospitalized medical patients, outpa-tients with cancer, the chronically immobilized, long-distance travelers, and those with asymp-tomatic thrombophilia. Methods: This guideline follows methods described in Methodology for the Development of Anti-thrombotic Therapy and Prevention of Thrombosis Guidelines: Antithrombotic Therapy and Pre-vention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines in this supplement. Results: For acutely ill hospitalized medical patients at increased risk of thrombosis, we recom-mend anticoagulant thromboprophylaxis with low-molecular-weight heparin (LMWH), low-dose unfractionated heparin (LDUH) bid, LDUH tid, or fondaparinux (Grade 1B) and suggest against extending the duration of thromboprophylaxis beyond the period of patient immobilization or acute hospital stay (Grade 2B). For acutely ill hospitalized medical patients at low risk of throm-bosis, we recommend against the use of pharmacologic prophylaxis or mechanical prophylaxis (Grade 1B). For acutely ill hospitalized medical patients at increased risk of thrombosis who are bleeding or are at high risk for major bleeding, we suggest mechanical thromboprophylaxis with graduated compression stockings (GCS) (Grade 2C) or intermittent pneumatic compression (IPC) (Grade 2C). For critically ill patients, we suggest using LMWH or LDUH thromboprophylaxis (Grade 2C). For critically ill patients who are bleeding or are at high risk for major bleeding, we suggest mechanical thromboprophylaxis with GCS and/or IPC at least until the bleeding risk decreases (Grade 2C). In outpatients with cancer who have no additional risk factors for VTE we suggest against routine prophylaxis with LMWH or LDUH (Grade 2B) and recommend against the prophylactic use of vitamin K antagonists (Grade 1B). Conclusions: Decisions regarding prophylaxis in nonsurgical patients should be made after con-sideration of risk factors for both thrombosis and bleeding, clinical context, and patients’ values and preferences. CHEST 2012; 141(2)(Suppl):e195S–e226S
Abbreviations: APLA 5 antiphospholipid antibodies; ASA 5 acetylsalicylic acid; CVC 5 central venous catheter; GCS 5 graduated compression stockings; HIT 5 heparin-induced thrombocytopenia; HR 5 hazard ratio; INR 5 international normalized ratio; IPC 5 intermittent pneumatic compression; LDUH 5 low-dose unfractionated heparin; LMWH 5 low-molecular-weight heparin; PE 5 pulmonary embolism; RAM 5 risk assessment model; RCT 5 randomized controlled trial; RR 5 risk ratio; SCLC 5 small cell lung cancer; UFH 5 unfractionated heparin; VFP 5 venous foot pump; VKA 5 vitamin K antagonist
Prevention of VTE in Nonsurgical Patients Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Susan R. Kahn, MD; Wendy Lim, MD; Andrew S. Dunn, MD ; Mary Cushman, MD; Francesco Dentali, MD; Elie A. Akl , MD , MPH , PhD; Deborah J. Cook, MD , MSc ( Epi ); Alex A. Balekian , MD , MSHS ; Russell C. Klein, MD ; Hoang Le , MD , FCCP ; Sam Schulman, MD ; and M. Hassan Murad , MD , MPH
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e196S Prevention of VTE in Nonsurgical Patients
Revision accepted August 31, 2011 . Affi liations: From the Department of Medicine (Dr Kahn), McGill University, Montreal, QC, Canada; the Department of Medicine (Drs Lim and Cook), Division of Hematology and Thromboembolism (Dr Schulman), and the Department of Clin ical Epidemiology and Biostatistics (Drs Akl and Cook), McMaster University, Hamilton, ON, Canada; the Depart-ment of Medicine (Dr Dunn), Mount Sinai School of Medicine, New York, NY; the Department of Medicine (Dr Cushman), Uni-versity of Vermont and Fletcher Allen Health Care, Burlington, VT; the Department of Clinical Medicine (Dr Dentali), Univer-sity of Insubria, Varese, Italy; the Department of Medicine (Dr Akl), University at Buffalo, Buffalo, NY; the Division of Pul-monary and Critical Care Medicine (Dr Balekian), Keck School of Medicine, University of Southern California, Los Angeles, CA; the Huntington Beach Internal Medicine Group (Dr Klein), Newport Beach, CA; the Department of Pulmonary and Critical Care Medicine (Dr Klein), University of California Irvine School of Medicine, Orange, CA; the Hoag Memorial Hospital Presbyterian (Dr Le), Newport Beach, CA; the Pulmonary Division (Dr Le), Fountain Valley Regional Hospital, Fountain Valley, CA; and the Division of Preventive Medicine and the Knowledge and Evalua-tion Research Unit (Dr Murad), Mayo Clinic, Rochester, MN . Funding/Support: The Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines received support from the National Heart, Lung, and Blood Institute [R13 HL104758] and Bayer Schering Pharma AG. Support in the form of educational grants were also provided by Bristol-Myers Squibb; Pfi zer, Inc; Canyon Pharmaceuticals; and sanofi -aventis US. Disclaimer: American College of Chest Physician guidelines are intended for general information only, are not medical advice, and do not replace professional medical care and physician advice, which always should be sought for any medical condition. The complete disclaimer for this guideline can be accessed at http://chestjournal.chestpubs.org/content/141/2_suppl/1S. Correspondence to: M. Hassan Murad, MD, MPH, 200 First St SW, Rochester, MN 55905; e-mail: [email protected] © 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians ( http://www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.11-2296
Summary of Recommendations
Note on Shaded Text: Throughout this guideline, shading is used within the summary of recommenda-tions sections to indicate recommendations that are newly added or have been changed since the pub-lication of Antithrombotic and Thrombolytic Therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Recommendations that remain unchanged are not shaded.
2.3. For acutely ill hospitalized medical patients at increased risk of thrombosis, we recommend anticoagulant thromboprophylaxis with low-molecular-weight heparin [LMWH], low-dose unfractionated heparin (LDUH) bid, LDUH tid, or fondaparinux (Grade 1B) .
Remarks: In choosing the specifi c anticoagulant drug to be used for pharmacoprophylaxis, choices should be based on patient preference, compliance, and ease
of administration (eg, daily vs bid vs tid dosing), as well as on local factors affecting acquisition costs (eg, prices of various pharmacologic agents in individual hospital formularies).
2.4. For acutely ill hospitalized medical patients at low risk of thrombosis, we recommend against the use of pharmacologic prophylaxis or mechan-ical prophylaxis (Grade 1B) .
2.7.1. For acutely ill hospitalized medical patients who are bleeding or at high risk for bleeding, we recommend against anticoagulant thrombo-prophylaxis (Grade 1B) .
2.7.2. For acutely ill hospitalized medical patients at increased risk of thrombosis who are bleed-ing or at high risk for major bleeding, we suggest the optimal use of mechanical thrombo-prophylaxis with graduated compression stock-ings (GCS) (Grade 2C) or intermittent pneumatic compression (IPC) (Grade 2C) , rather than no mechanical thromboprophylaxis. When bleeding risk decreases, and if VTE risk persists, we sug-gest that pharmacologic thromboprophylaxis be substituted for mechanical thromboprophy-laxis (Grade 2B) .
Remarks: Patients who are particularly averse to the potential for skin complications, cost, and need for clinical monitoring of GCS and IPC use are likely to decline mechanical prophylaxis.
2.8. In acutely ill hospitalized medical patients who receive an initial course of thromboprophy-laxis, we suggest against extending the duration of thromboprophylaxis beyond the period of patient immobilization or acute hospital stay (Grade 2B) .
3.2. In critically ill patients, we suggest against routine ultrasound screening for DVT (Grade 2C) .
3.4.3. For critically ill patients, we suggest using LMWH or LDUH thromboprophylaxis over no prophylaxis (Grade 2C) .
3.4.4. For critically ill patients who are bleeding, or are at high risk for major bleeding, we sug-gest mechanical thromboprophylaxis with GCS (Grade 2C) or IPC (Grade 2C) until the bleeding risk decreases, rather than no mechanical throm-boprophylaxis. When bleeding risk decreases, we suggest that pharmacologic thromboprophy-laxis be substituted for mechanical thrombo-prophylaxis (Grade 2C) .
4.2.1. In outpatients with cancer who have no additional risk factors for VTE, we suggest against
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e197S
This article focuses on prevention of VTE in non-surgical populations. Because they are addressed
in other chapters in these guidelines, 1,2 we do not include prevention of VTE in patients with trauma and spinal cord injury and in patients with ischemic and hemorrhagic stroke.
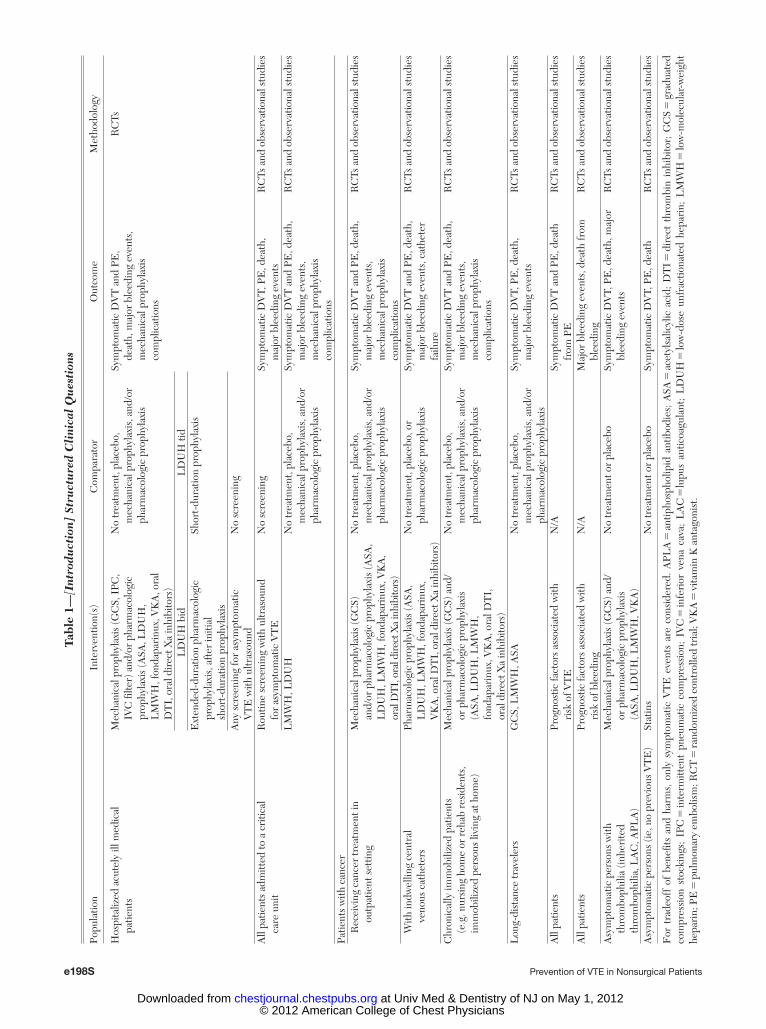
Adverse consequences of unprevented VTE include symptomatic DVT and pulmonary embolism (PE), fatal PE, chronic postthrombotic syndrome, and increased risk of recurrent VTE. We consider the desir-able and undesirable consequences of antithrombotic prophylaxis to prevent VTE in the following popula-tions/patient groups: (1) hospitalized acutely ill med-ical patients, (2) critically ill patients, (3) patients with cancer receiving cancer treatment in the outpatient setting, (4) patients with cancer with indwelling central venous catheters (CVCs), (5) Chronically immobilized patients, (6) long-distance travelers, and (7) asymptomatic persons with thrombophilia. We also consider the use of statins (HMG-CoA reduc-tase inhibitors) to prevent VTE. Table 1 describes the question defi nition (population, intervention, com-parator, and outcome) and eligibility criteria for studies considered in each section of this article.
1.0 Methods
The methodology of these guidelines follows the general approach of Methodology for the Development of Antithrombotic Therapy and Prevention of Thrombosis Guidelines. Antithrom-botic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines in this supplement. 3 In brief, panel members con-ducted literature searches to update the existing evidence base, seeking systematic reviews and trials published since the previous iteration of the guidelines, and rated the quality of the evidence using the Grading of Recommendations Assessment, Develop-ment, and Evaluation framework. The panel considered the bal-ance of benefi ts and harm, patients’ values and preferences, and patients’ context and resources to develop weak or strong recom-mendations. In this article, we identifi ed three areas with sparse high-quality evidence: (1) the benefi ts of prophylaxis as mea-sured by reduction of the incidence of symptomatic VTE events, (2) resource use and cost-effectiveness, and (3) the benefi ts of screening strategies for VTE in nonsurgical patients.
1.1 Outcomes of Interest
We selected similar patient-important outcomes across recom-mendations. These include symptomatic DVT, PE, death from PE, major bleeding, heparin-induced thrombocytopenia (HIT), and mechanical thromboprophylaxis complications (when appli-cable). In addition, for patients with CVCs, we include catheter failure as an outcome.
As the mortal outcome of greatest interest, when data were available, we have chosen treatment-related mortality (PE deaths, hemorrhagic deaths). For pharmacologic interventions, when available, we provide data on fatal bleeding and fatal intracranial
routine prophylaxis with LMWH or LDUH (Grade 2B) and recommend against the prophy-lactic use of vitamin K antagonists (Grade 1B) .
Remarks: Additional risk factors for venous throm-bosis in cancer outpatients include previous venous thrombosis, immobilization, hormonal therapy, angio-genesis inhibitors, thalidomide, and lenali domide.
4.2.2. In outpatients with solid tumors who have additional risk factors for VTE and who are at low risk of bleeding, we suggest prophylactic-dose LMWH or LDUH over no prophylaxis (Grade 2B) .
Remarks: Additional risk factors for venous throm-bosis in cancer outpatients include previous venous thrombosis, immobilization, hormonal therapy, angio-genesis inhibitors, thalidomide, and lenali domide.
4.4. In outpatients with cancer and indwelling central venous catheters, we suggest against routine prophylaxis with LMWH or LDUH (Grade 2B) and suggest against the prophylactic use of vitamin K antagonists (Grade 2C) .
5.1. In chronically immobilized persons resid-ing at home or at a nursing home, we suggest against the routine use of thromboprophylaxis (Grade 2C) .
6.1.1. For long-distance travelers at increased risk of VTE (including previous VTE, recent surgery or trauma, active malignancy, preg-nancy, estrogen use, advanced age, limited mobility, severe obesity, or known thrombo-philic disorder), we suggest frequent ambula-tion, calf muscle exercise, or sitting in an aisle seat if feasible (Grade 2C) .
6.1.2. For long-distance travelers at increased risk of VTE (including previous VTE, recent surgery or trauma, active malignancy, preg-nancy, estrogen use, advanced age, limited mobility, severe obesity, or known thrombo-philic disorder), we suggest use of properly fi tted, below-knee GCS providing 15 to 30 mm Hg of pressure at the ankle during travel (Grade 2C) . For all other long-distance travelers, we suggest against the use of GCS (Grade 2C) .
6.1.3. For long-distance travelers, we suggest against the use of aspirin or anticoagulants to prevent VTE (Grade 2C) .
7.1. In persons with asymptomatic thrombo-philia (ie, without a previous history of VTE), we recommend against the long-term daily use
of mechanical or pharmacologic thrombopro-phylaxis to prevent VTE (Grade 1C) .
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
e198S Prevention of VTE in Nonsurgical Patients
Tabl
e 1—
[Int
rodu
ctio
n] S
tru
ctu
red
Cli
nica
l Q
ues
tion
s
Popu
latio
nIn
terv
entio
n(s)
Com
para
tor
Out
com
eM
etho
dolo
gy
Hos
pita
lized
acu
tely
ill m
edic
al
patie
nts
Mec
hani
cal p
roph
ylax
is (G
CS,
IPC
, IV
C fi
lter)
and
/or
phar
mac
olog
ic
prop
hyla
xis
(ASA
, LD
UH
, L
MW
H, f
onda
pari
nux,
VK
A, o
ral
DT
I, o
ral d
irec
t Xa
inhi
bito
rs)
No
trea
tmen
t, pl
aceb
o,
mec
hani
cal p
roph
ylax
is, a
nd/o
r ph
arm
acol
ogic
pro
phyl
axis
Sym
ptom
atic
DV
T a
nd P
E,
deat
h, m
ajor
ble
edin
g ev
ents
, m
echa
nica
l pro
phyl
axis
co
mpl
icat
ions
RC
Ts
LD
UH
bid
LD
UH
tid
Ext
ende
d-du
ratio
n ph
arm
acol
ogic
pr
ophy
laxi
s, a
fter
initi
al
shor
t-du
ratio
n pr
ophy
laxi
s
Shor
t-du
ratio
n pr
ophy
laxi
s
Any
scr
eeni
ng fo
r as
ympt
omat
ic
VT
E w
ith u
ltras
ound
No
scre
enin
g
All
patie
nts
adm
itted
to a
cri
tical
ca
re u
nit
Rou
tine
scre
enin
g w
ith u
ltras
ound
fo
r as
ympt
omat
ic V
TE
No
scre
enin
gSy
mpt
omat
ic D
VT,
PE
, dea
th,
maj
or b
leed
ing
even
tsR
CTs
and
obs
erva
tiona
l stu
dies
LM
WH
, LD
UH
No
trea
tmen
t, pl
aceb
o,
mec
hani
cal p
roph
ylax
is, a
nd/o
r ph
arm
acol
ogic
pro
phyl
axis
Sym
ptom
atic
DV
T a
nd P
E, d
eath
, m
ajor
ble
edin
g ev
ents
, m
echa
nica
l pro
phyl
axis
co
mpl
icat
ions
RC
Ts a
nd o
bser
vatio
nal s
tudi
es
Patie
nts
with
can
cer
R
ecei
ving
can
cer
trea
tmen
t in
ou
tpat
ient
set
ting
Mec
hani
cal p
roph
ylax
is (G
CS)
an
d/or
pha
rmac
olog
ic p
roph
ylax
is (A
SA,
LD
UH
, LM
WH
, fon
dapa
rinu
x, V
KA
, or
al D
TI,
oral
dire
ct X
a in
hibi
tors
)
No
trea
tmen
t, pl
aceb
o,
mec
hani
cal p
roph
ylax
is, a
nd/o
r ph
arm
acol
ogic
pro
phyl
axis
Sym
ptom
atic
DV
T a
nd P
E, d
eath
, m
ajor
ble
edin
g ev
ents
, m
echa
nica
l pro
phyl
axis
co
mpl
icat
ions
RC
Ts a
nd o
bser
vatio
nal s
tudi
es
W
ith in
dwel
ling
cent
ral
ve
nous
cat
hete
rsPh
arm
acol
ogic
pro
phyl
axis
(ASA
, L
DU
H, L
MW
H, f
onda
pari
nux,
V
KA
, ora
l DT
I, o
ral d
irec
t Xa
inhi
bito
rs)
No
trea
tmen
t, pl
aceb
o, o
r ph
arm
acol
ogic
pro
phyl
axis
Sym
ptom
atic
DV
T a
nd P
E, d
eath
, m
ajor
ble
edin
g ev
ents
, cat
hete
r fa
ilure
RC
Ts a
nd o
bser
vatio
nal s
tudi
es
Chr
onic
ally
imm
obili
zed
patie
nts
(e.g
. nur
sing
hom
e or
reh
ab r
esid
ents
, im
mob
ilize
d pe
rson
s liv
ing
at h
ome)
Mec
hani
cal p
roph
ylax
is (G
CS)
and
/or
pha
rmac
olog
ic p
roph
ylax
is
(ASA
, LD
UH
, LM
WH
, fo
ndap
arin
ux, V
KA
, ora
l DT
I,
oral
dir
ect X
a in
hibi
tors
)
No
trea
tmen
t, pl
aceb
o,
mec
hani
cal p
roph
ylax
is, a
nd/o
r ph
arm
acol
ogic
pro
phyl
axis
Sym
ptom
atic
DV
T a
nd P
E, d
eath
, m
ajor
ble
edin
g ev
ents
, m
echa
nica
l pro
phyl
axis
co
mpl
icat
ions
RC
Ts a
nd o
bser
vatio
nal s
tudi
es
Lon
g-di
stan
ce tr
avel
ers
GC
S, L
MW
H, A
SAN
o tr
eatm
ent,
plac
ebo,
m
echa
nica
l pro
phyl
axis
, and
/or
phar
mac
olog
ic p
roph
ylax
is
Sym
ptom
atic
DV
T, P
E, d
eath
, m
ajor
ble
edin
g ev
ents
RC
Ts a
nd o
bser
vatio
nal s
tudi
es
All
patie
nts
Prog
nost
ic fa
ctor
s as
soci
ated
with
ri
sk o
f VT
EN
/ASy
mpt
omat
ic D
VT
and
PE
, dea
th
from
PE
RC
Ts a
nd o
bser
vatio
nal s
tudi
es
All
patie
nts
Prog
nost
ic fa
ctor
s as
soci
ated
with
ri
sk o
f ble
edin
gN
/AM
ajor
ble
edin
g ev
ents
, dea
th fr
om
blee
ding
RC
Ts a
nd o
bser
vatio
nal s
tudi
es
Asy
mpt
omat
ic p
erso
ns w
ith
thro
mbo
phili
a (in
heri
ted
thro
mbo
phili
a, L
AC
, APL
A)
Mec
hani
cal p
roph
ylax
is (G
CS)
and
/or
pha
rmac
olog
ic p
roph
ylax
is
(ASA
, LD
UH
, LM
WH
, VK
A)
No
trea
tmen
t or
plac
ebo
Sym
ptom
atic
DV
T, P
E, d
eath
, maj
or
blee
ding
eve
nts
RC
Ts a
nd o
bser
vatio
nal s
tudi
es
Asy
mpt
omat
ic p
erso
ns (i
e, n
o pr
evio
us V
TE
)St
atin
sN
o tr
eatm
ent o
r pl
aceb
oSy
mpt
omat
ic D
VT,
PE
, dea
thR
CTs
and
obs
erva
tiona
l stu
dies
For
tra
deof
f of
ben
efi ts
and
har
ms,
onl
y sy
mpt
omat
ic V
TE
eve
nts
are
cons
ider
ed.
APL
A 5
antip
hosp
holip
id a
ntib
odie
s; A
SA 5
acet
ylsa
licyl
ic a
cid;
DT
I 5 d
irec
t th
rom
bin
inhi
bito
r; G
CS
5 g
radu
ated
co
mpr
essi
on s
tock
ings
; IP
C 5
inte
rmitt
ent
pneu
mat
ic c
ompr
essi
on;
IVC
5 in
feri
or v
ena
cava
; L
AC
5 lu
pus
antic
oagu
lant
; L
DU
H 5
low
-dos
e un
frac
tiona
ted
hepa
rin;
LM
WH
5 lo
w-m
olec
ular
-wei
ght
hepa
rin;
PE
5 p
ulm
onar
y em
bolis
m; R
CT
5 ra
ndom
ized
con
trol
led
tria
l; V
KA
5 vi
tam
in K
ant
agon
ist.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e199S
supplementary tables not contained in the body of the article and available online. See the “Acknowledgments” for more informa-tion.). Also, there is uncertainty about the generalizability of trial results to other populations, as in many of the trials the ratio of patients screened to patients enrolled was very high (eg, � 100), and probable underestimation of absolute numbers of symptom-atic events, as patients diagnosed with asymptomatic DVT via trial-mandated screening tests are typically treated with anticoag-ulants. Incidence estimates from most observational studies were unsatisfactory because they were not stratifi ed by the use of thrombo-prophylaxis and were also reported in very heterogenous popula-tions (Table S2).
To estimate baseline risk for patients with low and high VTE risk, we used data from risk assessment models (RAMs). Several RAMs have been proposed for use in hospitalized medical patients (Table S3). 5-7 Limitations of most RAMs include lack of prospec-tive validation, applicability only to high-risk subgroups, inade-quate follow-up time, and excessive complexity.
In a prospective observational study of 1,180 inpatients, a predefi ned RAM (Padua Prediction Score, modifi ed after Kucher 8 ) assigned points to 11 common VTE risk factors ( Table 2 ) 9 and categorized hospitalized medical patients as low risk ( , 4 points; 60.3% of patients) or high risk ( � 4 points; 39.7% of patients) for VTE. Attending physicians were not notifi ed of their patients’ risk categories. Patients were followed for symp-tomatic VTE for 90 days. VTE occurred in 11.0% of high-risk patients who did not receive prophylaxis vs 0.3% of low-risk patients, a . 30-fold difference in risk (hazard ratio [HR], 32.0; 95% CI, 4.1-251.0). Among 711 low-risk patients, two (0.3%) developed VTE (1 PE, 1 PE with DVT). Among 283 high-risk patients who did not receive prophylaxis, the risk of DVT was 6.7%, nonfatal PE 3.9%, and fatal PE 0.4%. Hence, for base-line risk for low- and high-risk strata, we used risk estimates provided by the Padua Prediction Score. 9 Despite the limita-tions of this risk model (small number of events, suboptimal
bleeding as a subset of all-cause mortality, and for the outcome of major bleeding, when available, we provide data on intracranial bleeding and GI bleeding (the most common type of “critical organ” bleeding expected in nonsurgical populations). Given that anticoagulants used to prevent VTE are administered for short periods of time, major bleeding and fatal bleeding are likely to be rare events, except during critical illness.
1.2 Values and Preferences
Little is known about the distribution of patients’ values and preferences in the context of VTE prevention in nonsurgical set-tings. In developing the recommendations for this guideline, pan-elists made estimates of patients’ values and preferences often using indirect data from other settings (eg, values and preferences that pertain to anticoagulation in atrial fi brillation).
In our populations, the weights (relative importance) given to the harmful effects (disutilities) of the most representative types of critical organ bleeding, namely GI or, less commonly, intracranial bleeding, will greatly impact the tradeoff between desirable and undesirable consequences of antithrombotic therapy. There are limited data to guide us with respect to the relative impact of VTE events vs bleeding events on patient-perceived state of health; available evidence suggests values and preferences for treatments and for health states vary appreciably between individuals. 4
In a values rating exercise, Antithrombotic Therapy and Pre-vention of Thrombosis, 9th ed: American College of Chest Physi-cians Evidence-Based Clinical Practice Guidelines panelists used a “feeling thermometer” with anchors at 0 (representing death) and 100 (representing full health) to rate patient scenarios for var-ious clinical outcomes in terms of the value placed on a year in which the events depicted in the scenario occurred. 3 Median rat-ings were similar for the outcomes of symptomatic DVT, PE, and catheter thrombosis (80, 75, and 80, respectively) and severe GI bleeding (75), whereas the median rating for intracranial bleeding (stroke scenario) was 40. Therefore, we used 1:1 ratio of symp-tomatic VTE to major extracranial bleeding and 2.5:1 ratio of symptomatic VTE to intracranial bleeding for tradeoffs.
We considered that preventative and screening recommenda-tions require higher-quality evidence supporting benefi t than therapy recommendations. This decision is a value-based judg-ment. In making our recommendations, when there is uncertain benefi t and an appreciable probability of important harm or patient burden associated with treatment, we recommend against such treatments.
1.3 Estimating Baseline Risk
In making clinical recommendations, guideline developers need to consider the balance of benefi ts and harms in terms of absolute treatment effect on patient-important symptomatic events in addition to relative measures of risk. The panelists of the four articles dealing with VTE prevention faced challenges in fi nding these data and developed several possible approaches for estimating the effect of prophylaxis on the incidence of symptom-atic VTE events. In this article, we used two different approaches for hospitalized patients in non-critical care settings and for criti-cally ill patients, based on the availability of data.
1.3.1 Baseline Risk in Hospitalized Medical Patients: Since medical patients have a signifi cantly heterogeneous risk for VTE, the guideline panel sought to evaluate preventive strategies in two different strata of patients (low risk and high risk). We decided against simply using as the baseline estimate the pooled average risk of DVT (0.8%) and PE (0.4%) reported in the control arms of the randomized controlled trials (RCTs) of thromboprophylaxis in hospitalized medical patients, as it is evident from the trials’ eligi-bility criteria that patients with heterogeneous risk were enrolled (Table S1) (Tables that contain an “S” before the number denote
Table 2—Risk Factors for VTE in Hospitalized Medical Patients9
Risk Factor Points
Active cancera 3Previous VTE (with the exclusion of superfi cial vein
thrombosis)3
Reduced mobilityb 3Already known thrombophilic conditionc 3Recent (� 1 mo) trauma and/or surgery 2Elderly age (� 70 y) 1Heart and/or respiratory failure 1Acute myocardial infarction or ischemic stroke 1Acute infection and/or rheumatologic disorder 1Obesity (BMI � 30) 1Ongoing hormonal treatment 1
In the Padua Prediction Score risk assessment model, high risk of VTE is defi ned by a cumulative score � 4 points. In a prospective observational study of 1,180 medical inpatients, 60.3% of patients were low risk and 39.7% were high risk. Among patients who did not receive prophylaxis, VTE occurred in 11.0% of high-risk patients vs 0.3% of low-risk patients (HR, 32.0; 95% CI, 4.1-251.0). Among high-risk patients, the risk of DVT was 6.7%, nonfatal PE 3.9%, and fatal PE 0.4%.9 HR 5 hazard ratio.aPatients with local or distant metastases and/or in whom chemotherapy or radiotherapy had been performed in the previous 6 mo.bAnticipated bed rest with bathroom privileges (either because of patient’s limitations or on physician’s order) for at least 3 d.cCarriage of defects of antithrombin, protein C or S, factor V Leiden, G20210A prothrombin mutation, antiphospholipid syndrome.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e200S Prevention of VTE in Nonsurgical Patients
accounts for about one-fourth of all VTE events in the community. 17,18 Among hospitalized patients, 50% to 75% of VTE events, including fatal PE, occur in those hospitalized on the medical service. 16,19 Risk factors for VTE in hospitalized medical patients include intrinsic factors, such as increasing age (espe-cially . 70 years), previous VTE, known thrombo-philia, and various comorbid illnesses, such as cancer, heart failure, or respiratory failure, and extrinsic fac-tors, such as immobilization for � 3 days and hor-monal medications 5,20-22 ( Table 2 ). 9
2.2 Risk Factors for Bleeding in Hospitalized Medical Patients
A recent multinational observational study reported on risk factors at admission that were indepen-dently predictive of in-hospital bleeding (the analysis combined major and nonmajor clinically relevant bleeding) among 10,866 hospitalized medical patients. The strongest risk factors were active gastroduo-denal ulcer, bleeding in 3 months before admission, and platelet count , 50 3 10 9 /L, followed by age . 85 years, hepatic failure, severe renal failure, and ICU or critical care unit admission ( Table 3 ). 10 Although data on incidence of bleeding were not provided separately by use vs nonuse of prophylaxis (overall rate of major bleeding was 0.76%), the above vari-ables remained predictive of bleeding when the model was adjusted for pharmacologic prophylaxis. A bleeding risk score that included these and addi-tional variables was developed by the authors, who reported that more than one-half of all major bleeding episodes occurred in the 10% of hospital-ized medical patients who had a bleeding risk score � 7.0.
Although this risk score is complex and has not yet been validated, the panel considered patients to have an excessive risk of bleeding if they had multiple risk factors or had one of the three risk factors with
validation), this model provides the best available basis for judging hospitalized patients’ risk.
We considered a number of options for baseline risk of major bleeding. We considered bleeding events reported in the Padua prediction score study. However, this study stratifi ed bleeding events according to thrombosis risk, not bleeding risk (1 of 283 in the low VTE risk group [0.4%; 95% CI, 0.0-2.0] and 1 of 711 in the high VTE risk group [0.1%; 95% CI, 0.0-0.8]). 9 We also considered bleeding events in a large observational study by Decousus 10 ; however, this study did not report bleeding according to use of pharmacoprophylaxis. Therefore, we chose to use 0.4% (19 of 4,304) derived from the control arm of trials of thromboprophylaxis in medical patients as the estimate of baseline risk of major bleeding (section 2.1). Where possible, we presented data on intracranial bleeding separately from major bleeding events.
1.3.2 Baseline Risk in Critically Ill Patients: Critical care trials have routinely screened patients for asymptomatic DVT, which are usually promptly treated if detected. Hence, an accurate estimate of risk of symptomatic DVT is not available from trials of critically ill patients receiving no prophylaxis, and PE events are generally rare. We used two approaches to esti-mate the baseline risk and absolute risk difference in critically ill patients. When symptomatic events were reported, such as DVT in the trials by Shorr et al 11 and in PROTECT, 12 we used these data directly to estimate the baseline risk, relative risk (RR), and risk difference. When symptomatic events were not reported in the trials, such as the PE outcome in trials that compared unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) vs placebo, we opted to use a base-line risk derived from symptomatic PEs reported in three observational studies. 13-15 The risk ratio (RR) was derived from the trials in which events were likely a mix of symptomatic and asymptomatic events . The former approach has the advantage of directness but may suffer from imprecision and poor appli-cability. The latter approach requires imputations that make the evidence indirect.
2.0. Hospitalized Acutely Ill Medical Patients
2.1 Risk Factors for VTE in Hospitalized Medical Patients
Hospitalization for acute medical illness is associ-ated with an eightfold increased risk of VTE 16 and
Table 3—Independent Risk Factors for Bleeding in 10,866 Hospitalized Medical Patient10
Risk Factora Total Patients, No. (%) (N 5 10,866) OR (95% CI)
Active gastroduodenal ulcer 236 (2.2) 4.15 (2.21-7.77)Bleeding in 3 mo before admission 231 (2.2) 3.64 (2.21-5.99)Platelet count , 50 3 109/L 179 (1.7) 3.37 (1.84-6.18)Age � 85 y (vs , 40 y) 1,178 (10.8) 2.96 (1.43-6.15)Hepatic failure (INR . 1.5) 219 (2.0) 2.18 (1.10-4.33)Severe renal failure (GFR , 30 mL/min/m2) 1,084 (11.0) 2.14 (1.44-3.20)ICU or CCU admission 923 (8.5) 2.10 (1.42-3.10)Central venous catheter 820 (7.5) 1.85 (1.18-2.90)Rheumatic disease 740 (6.8) 1.78 (1.09-2.89)Current cancer 1,166 (10.7) 1.78 (1.20-2.63)Male sex 5,367 (49.4) 1.48 (1.10-1.99)
Data shown were obtained by multiple logistic regression analysis for characteristics at admission independently associated with in-hospital bleeding (major bleeding and clinically relevant nonmajor bleeding combined). GFR 5 glomerular fi ltration rate; INR 5 international normalized ratio.aAlthough not specifi cally studied in medical patients, one would also expect dual antiplatelet therapy to increase the risk of bleeding.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e201S
the strongest association with bleeding (OR . 3.0): active gastroduodenal ulcer, bleeding in 3 months before admission, and platelet count , 50 3 10 9 /L.
2.3 Any Anticoagulant vs None to Prevent VTE
We used data from three contemporary, high-quality systematic reviews to assess the benefi ts and harms of anticoagulant prophylaxis vs no prophylaxis in hospi-talized, acutely ill medical patients. 23-25 In general, the trials included acutely ill hospitalized patients (typi-cally, the mean age of enrolled patients was . 65 years) admitted for congestive heart failure, severe respi-ratory disease, or acute infectious, rheumatic, or infl ammatory conditions, who were immobilized and had one or more additional VTE risk factors including but not limited to age . 40 years, active cancer, pre-vious VTE, or serious infection (Table S2). Prophy-lactic anticoagulant regimens included low-dose unfractionated heparin (LDUH) tid, LDUH bid, var-ious LMWHs, and fondaparinux. Duration of use of prophylaxis ranged from 6-21 days or discharge from hospital, whichever came fi rst. In all trials, routine screening for DVT was performed.
Meta-analysis of these trials demonstrates that anticoagulant thromboprophylaxis is associated with signifi cant reduction in fatal PEs (RR, 0.41; 95% CI, 0.22-0.76; two fewer per 1,000 [95% CI, from one fewer to three fewer]). When we apply the relative effect of anticoagulant thromboprophylaxis obtained from these meta-analyses to baseline risks obtained from risk assessment models, we fi nd that throm-boprophylaxis is associated with a reduction in symp-tomatic DVT (RR, 0.47; 95% CI, 0.22-1; one fewer per 1,000 [95% CI, from one fewer to 0 fewer] in low-risk patients; 34 fewer per 1,000 [95% CI, from 51 fewer to 0 fewer] in high-risk patients). The effect on non-fatal PE, major bleeding, and all-cause mortality was not statistically signifi cant and is described in terms of relative and absolute effects ( Table 4 , Table S4). No trial reported the incidence of HIT.
Based on these data, the panel judged that moderate-quality evidence suggests that thromboprophylaxis is effective in reducing symptomatic DVT and fatal PE in acutely ill, hospitalized, immobilized medical patients who have characteristics similar to those enrolled in the above RCTs, and moderate-quality evidence suggests a modest relative and very small absolute increase in bleeding risk. Based on the above RCTs, the panel considered that providing prophy-laxis for 6 to 21 days, until full mobility is restored or until discharge from hospital, whichever comes fi rst, is a reasonable approach. The recommendation to prophylax applies only to the higher-risk patients ( Table 2 ). In low-risk patients, VTE is too infrequent to warrant prophylaxis.
Tabl
e 4—
[Sec
tion
2.3
] Su
mm
ary
of F
indi
ngs:
Sho
uld
Ant
icoa
gula
nt P
roph
ylax
is (
LM
WH
, UF
H, F
onda
pari
nux)
vs
Pla
ceb
o/N
o T
reat
men
t B
e U
sed
in
Hos
pita
lize
d M
edic
al P
atie
nts?
24-2
6
Out
com
es
Ant
icip
ated
Abs
olut
e E
ffec
ts
Rel
ativ
e E
ffec
t (95
% C
I)N
o. o
f Par
ticip
ants
(S
tudi
es) F
ollo
w-u
pQ
ualit
y of
the
Evi
denc
e (G
RA
DE
)B
asel
ine
Ris
kaR
isk
Diff
eren
ce W
ith A
ntic
oagu
lant
Pro
phyl
axis
(95%
CI)
Sym
ptom
atic
DV
TL
ow r
isk
RR
, 0.4
7 (0
.22-
1)5,
206
(4 R
CTs
) 1-1
4 d
Mod
erat
e du
e to
im
prec
isio
nb2
per
1,00
01
few
er p
er 1
,000
(fro
m 1
few
er to
0 m
ore)
Hig
h ri
sk67
per
1,0
0034
few
er p
er 1
,000
(fro
m 5
1 fe
wer
to 0
mor
e)N
onfa
tal p
ulm
onar
y em
bolis
mL
ow r
isk
RR
, 0.6
1 (0
.23-
1.67
)5,
206
(6 R
CTs
) 1-2
2 d
Mod
erat
e du
e to
im
prec
isio
nb2
per
1,00
01
few
er p
er 1
,000
(fro
m 1
few
er to
1 m
ore)
Hig
h ri
sk39
per
1,0
0015
few
er p
er 1
,000
(fro
m 3
0 fe
wer
to 2
6 m
ore)
Maj
or b
leed
ing
4 pe
r 1,
000
1 m
ore
per
1,00
0 (f
rom
1 fe
wer
to 6
mor
e)O
R, 1
.32
(0.7
3-2.
37)
8,60
5 (8
RC
Ts) 1
0-11
0 d
Mod
erat
e du
e to
im
prec
isio
nb
Ove
rall
mor
talit
y45
per
1,0
001
few
er p
er 1
,000
(fro
m 9
few
er to
8 m
ore)
OR
, 0.9
7 (0
.79-
1.19
)7,
355
(5 R
CTs
) 1-2
2 d
Mod
erat
e du
e to
im
prec
isio
nb
Thr
ombo
cyto
peni
a13
per
1,0
001
few
er p
er 1
,000
(fro
m 6
few
er to
7 m
ore)
OR
, 0.9
1 (0
.54-
1.53
)4,
624
(3 R
CTs
) 6-2
1 d
Low
due
to r
isk
of b
ias
and
impr
ecis
ionb
GR
AD
E 5
Gra
des
of R
ecom
men
datio
ns, A
sses
smen
t, D
evel
opm
ent,
and
Eva
luat
ion;
RR
5 ri
sk r
atio
; UF
H 5
unf
ract
iona
ted
hepa
rin.
See
Tab
le 1
lege
nd fo
r ex
pans
ion
of o
ther
abb
revi
atio
ns.
a Bas
elin
e ris
k fo
r DV
T a
nd P
E in
low
-risk
pop
ulat
ion
wer
e de
rived
from
the
RA
M b
y B
arba
r et a
l.9 Bas
elin
e ris
k fo
r mor
talit
y an
d bl
eedi
ng is
der
ived
from
the
cont
rol a
rm o
f med
ical
pat
ient
s in
a m
eta-
anal
ysis
(Den
tali
et a
l).24
b We
will
con
side
r th
e pr
esen
ce o
f ser
ious
impr
ecis
ion
whe
n th
ere
are
, 3
00 e
vent
s in
tota
l (ev
ents
in tr
eatm
ent a
nd c
ontr
ol p
atie
nts)
or
whe
n C
Is in
clud
e ap
prec
iabl
e ha
rms
and
bene
fi ts.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e202S Prevention of VTE in Nonsurgical Patients
of 15,156 acutely ill hospitalized medical patients enrolled at 52 hospitals in 12 countries, docu-mented marked variation in practices in dosing frequency of LDUH used to prevent VTE. LDUH was prescribed tid in 54% of patients from the United States compared with bid in 85% of non-US patients. 31
There have been no head-to-head trials comparing bid vs tid LDUH to prevent VTE in hospitalized medical patients. We conducted a mixed-treatment comparison meta-analysis of 16 RCTs that enrolled hospitalized nonsurgical patients at risk for VTE and compared LDUH bid, LDUH tid, or LMWH to each other or to an inactive control. 32 The RR and 95% credible intervals comparing LDUH tid to LDUH bid for DVT, PE, death, and major bleeding (all were indirect comparisons) were 1.56 (0.64-4.33), 1.67 (0.49-208.09), 1.17 (0.72-1.95), and 0.89 (0.08-7.05), respectively. Due to a lack of reporting, we could not perform this analysis for the outcome HIT. The low-quality evidence from these indirect comparisons provides no compelling evidence that LDUH tid dosing, compared with bid dosing, reduces VTE or causes more bleeding. A future randomized trial comparing these agents is unlikely, considering the large sample size that would be required to demon-strate a signifi cant difference, which, if it exists, is undoubtedly small. From a patient preference per-spective, twice daily injections are likely to be preferred and better tolerated than thrice daily injections.
2.4 LDUH vs LMWH to Prevent VTE
LDUH and LMWH (enoxaparin, nadroparin, or certoparin) have been directly compared in fi ve RCTs. 26-30 Eligibility criteria for RCTs of LDUH vs LMWH in hospitalized medical patients were sim-ilar to trials of any anticoagulant vs none to prevent VTE and are shown in Table S5. In all trials, routine screening for DVT was performed. Dosing of LDUH was tid in four trials and bid in one trial. 26
Pooled results failed to exclude benefi t or harm for LMWH vs LDUH for the outcomes DVT (RR, 0.77; 95% CI, 0.50-1.19), PE (RR, 1.00; 95% CI, 0.28-3.59), overall mortality (RR, 0.89; 95% CI, 0.65-1.23), and HIT (RR, 0.50; 95% CI, 0.05-5.48) ( Table 5 , Table S6). Pooled results for major bleeding suggest a large relative protective effect of LMWH (RR, 0.48; 95% CI, 0.24-0.99) and small absolute (fi ve fewer; 95% CI, 0-7 fewer) reduction in bleed-ing events per 1,000 patients treated. Evidence is consistent with a similar effect of LMWH and UFH on reduction in thrombosis in acutely ill hos-pitalized medical patients (though imprecision is such that effects could, in relative terms, be appre-ciably greater in one treatment or the other). The potential for less bleeding with LMWH represents a benefi t that is small, and it may be very small.
2.5 LDUH bid vs tid to Prevent VTE
The International Medical Prevention Registry on Venous Thromboembolism (IMPROVE), a registry
Table 5—[Section 2.4] Summary of Findings: Should Anticoagulant Prophylaxis With LMWH vs UFH be Used in Hospitalized Medical Patients?23,171
Outcomes No. of Participants (Studies) Follow-up
Quality of the Evidence (GRADE)
Relative Effect (95% CI)
Anticipated Absolute Effects
Risk With UFHa
Risk Difference With LMWH (95% CI)
Symptomatic DVT 5,371 (5 RCTs) 1-28 d Low due to imprecisionb and indirectnessc
RR, 0.77 (0.50-1.19) 3 per 1,000 1 fewer per 1,000 (from 2 fewer to 1 more)
Nonfatal pulmonary embolism
5,386 (5 RCTs) 1-28 d Low due to imprecisionb and indirectnessc
RR, 1.00 (0.28-3.59) 2 per 1,000 0 fewer per 1,000 (from 1 fewer to 5 more)
Major bleeding 5,597 (5 RCTs) 1-28 d Moderate due to imprecisionb
RR, 0.48 (0.24-0.99) 9 per 1,000 5 fewer per 1,000 (from 0 fewer to 7 fewer)
Overall mortality 5,597 (5 RCTs) 1-28 d Moderate due to imprecisionb
RR, 0.89 (0.65-1.23) 27 per 1,000 3 fewer per 1,000 (from 10 fewer to 6 more)
Heparin-induced thrombocytopenia
3,239 (1 RCT) 1-28 d Low due to risk of imprecisionb and reporting biasd
RR, 0.50 (0.05-5.48) 1 per 1,000 1 fewer per 1,000 (from 1 fewer to 1 more)
See Table 1 and 4 legends for expansion of abbreviations.aBaseline risk is derived from the median control group risk across studies.bWe will consider the presence of serious imprecision when there are , 300 events in total (events in treatment and control patients) or when confi dence intervals include appreciable harms and benefi ts.cThe RR used to estimate risk difference included a mix of symptomatic and asymptomatic events, whereas the baseline risk (risk with UFH) was derived from symptomatic events (Riess et al30).dOnly one study (Riess et al30) reported this outcome, suggesting possible reporting bias.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e203S
Medical Patients with Enoxaparin (MEDENOX) trial, which did not directly compare LMWH to LDUH 42 and enrolled a very small proportion of patients screened for eligibility, thereby limiting generalizability. Third, although the acquisition costs of LMWH are higher up front (or similar, depending on individual hospital formulary pricing), the eventual cost savings come from treating fewer adverse events—primarily HIT and, possibly, major bleeding—farther downstream. A recent thromboprophylaxis trial in 3,764 critically ill patients reported that the incidence of HIT was 0.3% in patients who received LMWH vs 0.7% in patients who received LDUH; 12 however, a meta-analysis of HIT in patients being treated for acute DVT or PE found no difference in incidence when using LMWH or LDUH. 43 Although the popu-lation of this meta-analysis is different from those in the critical care trial; adding the trial data to the meta-analysis does not change its conclusion (RR, 0.71; 95% CI, 0.45-1.11).
In summary, there is no clear evidence in the current literature to support choosing one form of pharma-coprophylaxis over another in the medical popula-tion based on outcomes or from a cost-effectiveness standpoint. It would be reasonable to make choices based on patient preference, compliance, and ease of
2.6 Anticoagulant Thromboprophylaxis in Acutely Ill Hospitalized Medical Patients From a Resource Perspective
Almost all cost-effectiveness analyses in this popu-lation have reported costs per VTE or death averted with the use of anticoagulant prophylaxis, but few studies have reported costs per quality-adjusted life-year gained to compare against preexisting bench-marks. Two studies that reported incremental costs of $65 to $2,534 per quality-adjusted life-year gained over no prophylaxis were both sponsored by the pharmaceutical industry. 33,34 In populations at suffi -ciently high risk ( Tables 2, 6 , Table S7), pharmaco-prophylaxis is likely to be favorable from a resource standpoint for preventing VTE. 35,36 The comparison between different types of prophylaxis, however, is less clear.
Several studies have suggested that choosing LMWH over LDUH is cost neutral, or even cost saving. 37-41 However, the quality of these analyses is moderate at best. First, many of the authors have had fi nancial disclosures with the pharmaceutical indus-try, and whether these ties infl uence the cost-neutral or cost-saving results of LMWH over LDUH is unclear. Second, the performance estimates used in most of these studies have been extracted from the
Table 6—[Section 2.6] Summary of Findings: Should Aspirin or Other Antiplatelet Drugs Be Used in Hospitalized Medical Patients?59
OutcomeParticipants (Studies)
Follow-upQuality of the
Evidence (GRADE)Relative Effect
(95% CI)
Anticipated Absolute Effects
Baseline Riska
Risk Difference With Aspirin Prophylaxis (95% CI)
Symptomatic DVT
Imputed data (1 RCT) up to 35 d
Low due to very serious indirectnessb
RR, 0.71 (0.52-0.97) Low risk2 per 1,000 1 fewer per 1,000
(from 1 fewer to 1 fewer)High risk
67 per 1,000 19 fewer per 1,000 (from 32 fewer to 2 fewer)
Nonfatal pulmonary embolism
Imputed data (64 RCTs) up to 35 d
Low due to very serious indirectnessb
RR, 0.47 (0.37-0.59) Low risk2 per 1,000 1 fewer per 1,000
(from 1 fewer to 1 fewer)High risk
39 per 1,000 21 fewer per 1,000 (from 25 fewer to 16 fewer)
Major bleeding Imputed data (1 RCT) up to 35 d
Low due to very serious indirectnessb
RR, 1.42 (1.16-1.74) 4 per 1,000 2 more per 1,000 (from 1 more to 3 more)
Overall mortality Imputed data (1 RCT) up to 35 d
Very low due to very serious indirectnessb and imprecisionc
RR, 0.97 (0.85-1.10) 45 per 1,000 1 fewer per 1,000 (from 7 fewer to 5 more)
See Table 1 and 4 legends for expansion of abbreviations.aBaseline risk for DVT and PE are derived from the RAM by Barbar et al.9 Baseline risk for mortality and bleeding is derived from the control arm of medical patients in a meta-analysis (Dentali et al).24
bEvidence is indirect because the relative effect is primarily derived from surgical patients (555 of the 26,890 patients included in PEP trial report meta-analysis were high-risk medical patients). DVT and PE baseline risk estimates are derived from a risk assessment model derived in a cohort with a small number of outcome events, hence have uncertainty about them. This uncertainty can be labeled as imprecision or indirectness. Some of the PE events in this meta-analysis may have been fatal.cWe will consider the presence of serious imprecision when there are , 300 events in total (events in treatment and control patients) or when CIs include appreciable harms and benefi ts.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e204S Prevention of VTE in Nonsurgical Patients
administration (eg, daily vs bid vs tid dosing), as well as on local factors affecting acquisition costs.
2.7 Mechanical Methods of Thromboprophylaxis in Hospitalized Medical Patients
Mechanical methods of thromboprophylaxis include graduated compression stockings (GCS), intermittent pneumatic compression devices (IPCs), and venous foot pumps (VFPs). These devices reduce venous stasis, a risk factor for VTE, by displacing blood from the superfi cial to the deep venous system via the per-forating veins, thereby increasing the velocity and volume of fl ow in the deep system. 44 Most studies of mechanical thromboprophylaxis have been conducted in surgical patients. The primary attraction of mechan-ical methods is that they do not cause bleeding; hence they may have advantages for patients at risk for VTE who cannot receive anticoagulant-based thrombo-
prophylaxis because they are bleeding or are at risk for bleeding.
2.7.1 Stockings to Prevent VTE: Direct evidence from hospitalized nonsurgical patients is available from three randomized trials that have evaluated the use of thigh-length GCS to prevent VTE in patients with myocardial infarction (one trial) 45 and stroke (two trials) 46,47 ( Table 7 , Table S8). In pooled analyses, results failed to demonstrate or exclude a benefi cial effect on symptomatic DVT or PE. Stocking use increased the risk of skin breaks/ulcers but failed to demonstrate or exclude an effect on lower limb ischemia or amputation. It is not known if hospital-ized medical patients have a similar risk of skin com-plications as hospitalized stroke patients.
In a recent multicenter RCT that compared knee-length to thigh-length GCS to prevent VTE in immo-bilized patients with acute stroke, proximal DVT
Table 7—[Section 2.7.1] Summary of Findings: Should Graduated Compression Stockings vs No Stockings Be Used in Hospitalized Medical Patients?45,47,48
OutcomeNo. of Participants (Studies) Follow-up
Quality of the Evidence (GRADE)
Relative Effect (95% CI)
Anticipated Absolute Effects
Baseline Riska
Risk Difference With Graduated Compression
Stockings (95% CI)
Symptomatic DVT 1,256 (1 RCT) 1-30 d Moderate due to imprecisionb
RR, 0.91 (0.63-1.29) Low risk2 per 1,000 1 fewer per 1,000
(from 1 fewer to 1 more)High risk
67 per 1,000 6 fewer per 1,000 (from 25 fewer to 19 more)
Nonfatal pulmonary embolism
1,256 (1 RCT) 1-30 d Low due to very serious imprecisionb
RR, 0.65 (0.33-1.31) Low risk2 per 1,000 1 fewer per 1,000
(from 1 fewer to 1 more)High risk
39 per 1,000 14 fewer per 1,000 (from 26 fewer to 12 more)
Overall mortality 1,321 (2 RCTs) 1-30 d Moderate due to imprecisionb
RR, 1.06 (0.94-1.20) 45 per 1,000 3 more per 1,000 (from 3 fewer to 9 more)
Skin breaks/ulcers/blisters/skin necrosis
1,256 (1 RCT) 1-30 d Very low due to imprecision,b indirectness,c and methodologic limitationsd
RR, 4.02 (2.34-6.91) 13 per 1,000 38 more per 1,000 (from 17 more to 75 more)
Lower limb ischemia/amputation
1,256 (1 RCT) 1-30 d Very low due to very serious imprecisionb and methodologic limitationsd
RR, 3.52 (0.73-16.90) 2 per 1,000 4 more per 1,000 (from 0 fewer to 25 more)
Number of participants is the number of patients who received graduated compression stockings. See Table 1 and 4 legends for expansion of abbreviations.aBaseline risk for DVT and PE are derived from the RAM by Barbar et al.9 Baseline risk for mortality and bleeding is derived from the control arm of medical patients in a meta-analysis (Dentali et al24). Baseline risk for lower leg ischemia and skin breaks (derived from the control arms of CLOTS trial 1).bWe will consider the presence of serious imprecision when there are , 300 events in total (events in treatment and control patients) or when confi dence intervals include appreciable harms and benefi ts. The exception is for low-risk patients in whom the absolute difference in PE and DVT is fairly small and precise.cData on skin breaks are from stroke patients.dAssessment of outcomes was based on case-note review and was not blinded to treatment allocation.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e205S
skin complications of IPC use, but one might plausi-bly expect rates to be similar to those of GCS. The panel considered that the evidence for the different outcomes should be rated down due to indirectness because the RR estimates are derived from surgical populations, in whom effects of IPC may be different than in medical patients, and from a mix of symptom-atic and asymptomatic events.
2.7.3 Mechanical Compression vs Heparin: There are no studies that have compared mechanical com-pression vs anticoagulants to prevent VTE in hos-pitalized medical patients. Indirect evidence from various orthopedic and nonorthopedic surgical popu-lations was provided in a recent meta-analysis by Eppsteiner of 16 trials (3,887 patients) of various compression modalities tested against LDUH or LMWH. 51 Pooled results for mechanical compres-sion compared with heparin failed to show or to exclude a benefi cial or detrimental effect for DVT (RR, 1.07; 95% CI, 0.72-1.61) or PE (RR, 1.03; 95% CI, 0.48-2.22). Mechanical compression was associated with a reduced risk of postoperative bleeding com-pared with heparin (RR, 0.47; 95% CI 0.31-0.70). The median rate of major bleeding within the study
(symptomatic or asymptomatic) occurred in 98 of 1,552 (6.3%) patients who received thigh-length stockings vs 138 of 1,562 (8.8%) who received below-knee stockings (RR, 0.71; 95% CI, 0.56-0.92), with no differences between groups in rates of deaths or PE. 48 Skin breaks occurred in 3.9% and 2.9% of patients allocated to thigh-length and knee-length GCS, respectively. These results are diffi cult to inter-pret alongside evidence from the CLOTS1 trial that thigh-length GCS were not effective to prevent VTE but suggest that if GCS are used, thigh length is pre-ferred to knee length. 49
2.7.2 Intermittent Pneumatic Compression Devices to Prevent VTE: An international registry of 15,156 hos-pitalized acutely ill medical patients found that 22% of US patients received IPC to prevent VTE compared with only 0.2% of patients in other coun-tries. 31 There are no published studies of IPC or VFP devices in hospitalized medical patients. Data are available from a meta-analysis of 22 trials that assessed IPC and VFP, primarily in surgical patients. 50 IPC devices failed to demonstrate or to exclude a benefi -cial effect on mortality or PE but reduced the risk of DVT ( Table 8 , Table S9). No data are available on
Table 8—[Section 2.7.2] Summary of Findings: Should Intermittent Pneumatic Compression Be Used in Hospitalized Nonsurgical Patients With Restricted Mobility?25,51,172,173
Outcome Source of Data
Quality of the Evidence (GRADE)
Relative Effect (95% CI)
Anticipated Absolute Effects
Baseline Riska
Risk Difference with IPC (95% CI)
Symptomatic DVT Imputed data Moderate due to serious indirectnessb
RR, 0.43 (0.32-0.58) Low risk8 per 1,000 1 fewer per 1,000
(from 1 fewer to 1 fewer)High risk
67 per 1,000 38 fewer per 1,000 (from 46 fewer to 28 fewer)
Nonfatal pulmonary embolism
Imputed data Low due to indirectnessb and imprecisionc
RR, 0.82 (0.41-1.62) Low risk4 per 1,000 1 fewer per 1,000
(from 1 fewer to 1 more)High risk
39 per 1,000 7 fewer per 1,000 (from 23 fewer to 24 more)
Overall mortality Imputed data Low due to indirectnessb and imprecisionc
RR, 1.03 (0.42-2.57) 45 per 1,000 1 more per 1,000 (from 76 fewer to 71 more)
Skin complications Not reported … … … …
See Table 1 and 4 legends for expansion of abbreviations.aBaseline risk for DVT and PE are derived from the RAM by Barbar et al.9 Baseline risk for mortality is derived from the control arm of medical patients in a meta-analysis (Dentali et al24).bSerious indirectness is considered because: RR for PE is derived from surgical patients (Roderick et al50). RR data are presented for IPC used as monotherapy because this is most relevant to the way IPCs are used in medical patients (ie, in patients who cannot receive anticoagulation). If IPCs are used alone or as adjunct to anticoagulant/antiplatelet therapy, RR is 0.77 (0.41-1.43). This does not change the conclusions of this evidence profi le. Another element of indirectness is that DVT in these surgical patients was primarily asymptomatic DVT as ascertained by systematic imaging tests. RR for proximal asymptomatic DVT was similar (0.52; 95% CI, 0.37-0.73). RR data are presented for IPC used as monotherapy because this is most relevant to the way IPCs are used in medical patients (ie, in patients who cannot receive anticoagulation). If IPCs are used alone or as adjunct to anticoagulant/antiplatelet therapy, RR is 0.49 (0.37-0.63). This does not change the conclusions of this evidence profi le.cWe will consider the presence of serious imprecision when there are , 300 events in total (events in treatment and control patients) or when CIs include appreciable harms and benefi ts.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e206S Prevention of VTE in Nonsurgical Patients
IPC devices are often not functioning when patients are out of bed or being transported, either due to improperly applied sleeves or nonfunctioning com-pression pump (not plugged in, power switch not turned on, or air hose compressed). Devices were properly functioning in , 50% of postoperative patients in one study 52 and only 19% of trauma patients in another. 53 Newer battery-powered por-table devices are available, and a recent study reported better compliance with these devices than with tra-ditional plug-in devices. 54
2.8 Extended-Duration Anticoagulant Thromboprophylaxis to Prevent VTE in Hospitalized Medical Patients
Hospitalized medical patients may have risk fac-tors for VTE that persist for weeks to months after hospital discharge. In a medical records review of 1,897 patients diagnosed with VTE in the Worcester, Massachusetts, area, 73.7% of episodes occurred in the outpatient setting; of these, 36.8% occurred in persons hospitalized for medical illness in the pre-ceding 3 months. Among these, two-thirds were diagnosed with VTE within 1 month after hospital-ization and one-third between 2 to 3 months after hospitalization. 18 In the MEDENOX RCT in which patients received enoxaparin prophylaxis or pla-cebo for up to 14 days, eight VTE events (8% of the total) occurred between days 15 and 110, of which four were fatal PEs. 42
Extended-duration thromboprophylaxis refers to prophylaxis that is continued beyond the initial (eg, 5-14 days) course, for up to approximately 35 days total. Evidence from RCTs in hospitalized surgical patients suggests that extended-duration thrombo-prophylaxis reduces VTE in patients undergoing hip replacement surgery, hip fracture surgery, and sur-gery for abdominal malignancy. 1,55
The Extended Prophylaxis for Venous Thrombo-embolism in Acutely Ill Medical Patients With Pro-longed Immobilization (EXCLAIM) study is the only published RCT of extended duration throm-boprophylaxis in hospitalized medical patients. 56 The study population consisted of 6,085 hospital-ized patients aged . 40 years with acute medical illness (eg, heart failure, respiratory insuffi ciency, infection) and reduced mobility. All patients received initial open-label enoxaparin (40 mg daily for 10 � 4 days ), and were then randomized to receive extended-duration enoxaparin (40 mg daily for 38 � 4 days) or placebo. Extended-duration enoxaparin, compared with placebo, reduced the incidence of overall VTE (composite of asymptomatic and symptomatic events) (RR, 0.62; 95% CI, 0.45-0.84) and symptomatic prox-imal DVT (RR, 0.25; 95% CI, 0.09-0.67) but failed to
populations was 1.5%, but bleeding rates were not provided by intervention. Subgroup analyses by hep-arin type suggested that LMWH may reduce risk of DVT compared with compression (RR for compres-sion, 1.80; 95% CI, 1.16-2.79), but remains associ-ated with increased bleeding risk.
2.7.4 Mechanical Compression and Pharmacologic Prophylaxis: Trials in postsurgical patients that com-pared the combination of intermittent pneumatic compression devices with a pharmacologic method to pharmacologic therapy used alone showed a strong trend toward fewer DVTs with combination therapy (OR, 0.45; 95% CI, 0.20-1.03). 1 Studies that compared the combination of elastic stockings and pharmaco-logic prophylaxis to pharmacologic therapy alone showed a reduction in symptomatic or asymptomatic DVT (OR, 0.40; 95% CI, 0.25-0.65), but this benefi t should be weighed against the increase in skin com-plications (RR, 4.18; 95% CI, 2.4-7.3) that has been observed in stroke patients treated with elastic com-pression stockings. 2,3,46
In summary, indirect data derived primarily from surgical populations suggest that GCS may be mod-estly effective at preventing asymptomatic DVT and possibly PE in hospitalized medical patients. Direct evidence of low to moderate quality in nonsurgical patients (primarily stroke patients) does not support benefi t, and their use in stroke patients is associated with a 5% risk of skin breakdown. IPCs failed to reduce PE in surgical patients but reduced DVT. Of the two methods, GCS has lower cost and greater ease of use and application than IPCs.
Despite the uncertain benefi t, mechanical throm-boprophylaxis with GCS or IPCs may be preferable to no prophylaxis in patients at appreciable risk for VTE who are also at high risk for bleeding, as the Eppsteiner meta-analysis showed similar effective-ness but reduced rates of bleeding with mechanical compared with heparin prophylaxis among surgical patients. 51 However, as subgroup analysis in that meta-analysis suggested that LMWH may be more effective than compression, and taking into account that the baseline rate of bleeding is lower among medical patients (average from RCTs, 0.4%) than surgical patients, if the bleeding risk is temporary and if patients remain at high risk of VTE ( Table 2 ), pharmacologic thromboprophylaxis should be initi-ated once the bleeding risk has decreased.
The panel also noted that the use of all mechanical methods of thromboprophylaxis are associated with costs related to purchase and maintenance and the time and vigilance required to ensure optimal com-pliance. Clinical staff must ensure that the correct size is used, that they are properly applied, and that they are worn at all times. Studies have shown that
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e207S
antiplatelet drugs to prevent VTE has been stud-ied in relatively few hospitalized medical patients (nine trials, total of 555 patients). These trial data are limited by small numbers of outcome events; report-ing of asymptomatic DVT of uncertain clinical rele-vance, often diagnosed with radiolabeled fi brinogen uptake testing, which has limitations in both sen-sitivity and specifi city; wide variety of antiplatelet drugs studied, including drugs that are no longer in use and that were administered for a mean of 8 weeks; and lack of reporting of rates of bleeding. 57 Among the nine trials, antiplatelet agents were asso-ciated with reduced risk of asymptomatic DVT (RR, 0.65; 95% CI, 0.45-0.94) based on 39 of 261 vs 61 of 266 events). Results failed to demonstrate or to exclude a benefi cial effect of antiplatelet agents on PE (RR, 0.38; 95% CI, 0.10-1.42) based on three of 275 vs eight of 280 events, respectively. Bleeding rates were not reported.
Our summary of ASA to prevent VTE in hospital-ized medical patients (section 2.9) is based on indi-rect evidence from the PEP (Pulmonary Embolism Prevention) trial, a multicenter trial of ASA 160 mg daily vs placebo for 35 days in hip fracture surgery or elective hip or knee arthroplasty patients 58 for the
exclude benefi ts or harm for fatal PE (RR, 0.34; 95% CI, 0.01-8.26) and overall mortality (RR, 1.00; 95% CI, 0.7-1.43). The risk of major bleeding was signifi cantly increased with extended-duration enox-aparin (RR, 2.51; 95% CI, 1.21-5.22), and there were four intracranial bleeding events (one fatal) in the extended enoxaparin group compared with none in the placebo group. In terms of absolute effects, extended-duration enoxaparin prevented six fewer symptomatic proximal DVT per 1,000 (95% CI, from three fewer to seven fewer) at a cost of fi ve more major bleeding events per 1,000 (95% CI, from one more to 14 more) ( Table 9 , Tables S10, S11). In addi-tion to the bleeding risk, extended prophylaxis also entails the burden and cost of daily injection.
2.9 Aspirin or Other Antiplatelet Drugs to Prevent VTE in Hospitalized Medical Patients
The contribution of platelet activation to the path-ogenesis of venous thrombosis is less clear than for arterial thrombosis. Although the use of acetylsali-cylic acid (ASA) for VTE prevention is appealing because of its low cost, oral administration, and low bleeding rates, the effectiveness of ASA or other
Table 9—[Section 2.8] Summary of Findings: Should Extended-Duration Thromboprophylaxis vs Standard Short-Duration Thromboprophylaxis Be Used for Prevention of VTE in Hospitalized Medical Patients With Reduced Mobility?57
OutcomeNo. of Participants (Studies) Follow-up
Quality of the Evidence (GRADE)
Relative Effect (95% CI)
Anticipated Absolute Effects
Risk With Standard Short-Duration
Thromboprophylaxis
Risk Difference With Extended-Duration
Prophylaxis (95% CI)
Symptomatic DVT 4,995 (1 RCT) 24-32 d
Moderate due to methodologic limitationsa
RR, 0.25 (0.09-0.67) 8 per 1,000 6 fewer per 1,000 (from 3 fewer to 7 fewer)
Nonfatal pulmonary embolism
Not reported … … … …
Fatal pulmonary embolism
4,995 (1 RCT) 24-32 d
Moderate due to methodologic limitationsa
RR, 0.34 (0.01-8.26) 1 per 1,000 1 fewer per 1,000 (from 1 fewer to 3 fewer)
Major bleeding 4,995 (1 RCT) 24-32 d
Moderate due to methodologic limitationsa
RR, 2.51 (1.21-5.22) 3 per 1,000 5 more per 1,000 (from 1 more to 14 more)
Overall mortality 4,995 (1 RCT) 24-32 d
Low due to methodologic limitationsa and imprecisionb
RR, 1.00 (0.7-1.43) 22 per 1,000 0 fewer per 1,000 (from 7 fewer to 9 more)
Heparin-induced thrombocytopenia
4,624 (1 RCT) 24-32 d
Very low due to methodologic limitationsa and very serious imprecisionb
RR, 3.01 (0.12-73.93) 0 per 1,000 0 more per 1,000 (from 0 fewer to 0 more)
ITT 5 intention to treat. See Table 1 and 4 legends for expansion of other abbreviations.aMethodologic limitations: change in eligibility criteria part way through the trial and seemed “data-driven”; did not use ITT analysis.bWe will consider the presence of serious imprecision when there are , 300 events in total (events in treatment and control patients) or when CIs include appreciable harms and benefi ts. We did not rate down for imprecision in the outcome of fatal PE because the absolute difference was small and precise.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e208S Prevention of VTE in Nonsurgical Patients
suggest that passive strategies, such as dissemination of guidelines or educational events, are ineffective. Multicomponent approaches, audit and feedback, and use of automatic reminders, such as preprinted orders, computer alerts, and human alerts, have been shown to be effective strategies; however, VTE prophylaxis continues to be underused or used inappropriately, even with such interventions. 8,64-66
Recommendations
2.3. For acutely ill hospitalized medical patients at increased risk of thrombosis ( Table 2 ), we recommend anticoagulant thromboprophylaxis With LMWH, LDUH bid, LDUH tid, or fonda-parinux (Grade 1B) .
Remarks: In choosing the specifi c anticoagulant drug to be used for pharmacoprophylaxis, choices should be based on patient preference, compliance, and ease of administration (eg, daily vs bid vs tid dosing), as well as on local factors affecting acquisition costs (eg, prices of various pharmacologic agents in individual hospital formularies).
2.4. For acutely ill hospitalized medical patients at low risk of thrombosis ( Table 2 ), we recom-mend against the use of pharmacologic prophy-laxis or mechanical prophylaxis (Grade 1B) .
2.7.1. For acutely ill hospitalized medical patients who are bleeding or at high risk for bleeding ( Table 3 ), we recommend against anti-coagulant thromboprophylaxis (Grade 1B) .
2.7.2. For acutely ill hospitalized medical patients at increased risk of thrombosis who are bleeding or at high risk for major bleeding, we suggest the optimal use of mechanical thromboprophylaxis with GCS (Grade 2C) or IPC (Grade 2C) , rather than no mechanical throm-boprophylaxis. When bleeding risk decreases, and if VTE risk persists, we suggest that pharmacologic thromboprophylaxis be sub-stituted for mechanical thromboprophylaxis (Grade 2B) .
Remarks: Patients who are particularly averse to the potential for skin complications, cost, and need for clinical monitoring of GCS and IPC use are likely to decline mechanical prophylaxis.
2.8. In acutely ill hospitalized medical patients who receive an initial course of thrombopro-phylaxis, we suggest against extending the dura-tion of thromboprophylaxis beyond the period
outcomes mortality, symptomatic DVT, and bleeding; and the PEP trial meta-analysis of 53 randomized trials (nine trials conducted in medical patients, as discussed above) of antiplatelet therapy to prevent VTE for the outcome PE. Use of ASA/antiplatelet drugs, compared with placebo, had little or no effect on mortality (RR, 0.97; 95% CI, 0.85-1.10) and was associated with a reduced risk of PE (RR, 0.47; 95% CI, 0.37-0.59), a reduced risk of DVT (RR, 0.71; 95% CI, 0.52-0.97), and an increased risk of nonsur-gical site-related bleeding events (RR, 1.42; 95% CI, 1.16-1.74).
The quality of the evidence was rated down for indirectness based on relative effects derived pri-marily from surgical patients (only 555 of the 26,890 patients included in PEP trial report meta-analysis were high-risk medical patients, and all PEP trials participants were orthopedic surgery patients). The panel judged that based on the low quality of available evidence pertaining to use of ASA to pre-vent VTE in hospitalized medical patients, no rec-ommendation could be made. There have been no studies of antiplatelet therapy compared with anti-thrombotic therapy to prevent VTE in acutely ill medical patients.
2.10 Screening for DVT in Hospitalized Medical Patients
Ultrasound screening in medical patients has not been systematically studied. Indirect evidence from hospitalized orthopedic patients 59 and spinal cord injury patients 60 suggests that routine screening is not of benefi t to reduce symptomatic VTE events. For example, in a population of patients who had joint arthroplasty and were receiving warfarin prophylaxis, screening compression ultrasonography with subse-quent treatment of identifi ed asymptomatic DVT did not reduce the rate of subsequent symptomatic VTE. 59 In a population with a low prevalence of DVT, such as medical patients, even with a highly-specifi c test such as ultrasound, one would anticipate a sub-stantial number of false-positive results. Moreover, even without considering false-positive results, rou-tine ultrasound screening would be associated with appreciable cost and inconvenience without evidence of benefi t.
2.11 Gaps in Care
Low rates of adherence to recommended thrombo-prophylaxis regimens have been documented world-wide. 31,61-64 In the last few years, research efforts have focused on evaluating strategies to improve uptake of evidence-based VTE prophylaxis regimens in hospi-talized patients, including medical patients. Results
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e209S
specifi cally evaluated prognostic factors associated with bleeding complications in critically ill patients ( Table 12 ). 70
3.4 Randomized Trials of Thromboprophylaxis
Five RCTs have examined pharmacologic prophy-laxis in critically ill patients: one of LDUH vs pla-cebo, 71 one of LMWH vs placebo, 69 and three of LDUH vs LMWH (one also included a placebo arm) 11,12,72 (Table S13). LDUH prophylaxis has been studied only in doses of 5,000 units bid.
The trial of LDUH vs placebo reported that LDUH was associated with a reduced risk of asymptomatic DVT (13% vs 29%, respectively; RR, 0.46; 95% CI, 0.22-0.99). Rates of bleeding, PE, and mortality were not reported. The trial of LMWH (nadroparin) vs placebo showed a trend toward reduced asymp-tomatic DVT with nadroparin (16% vs 28%, respec-tively; RR, 0.55; 95% CI, 0.30-1.00) but failed to demonstrate or exclude a benefi cial or detrimental effect of nadroparin on major bleeding (RR, 2.09; 95% CI, 0.54-8.16; 29 more per 1,000; 95% CI, from 12 fewer to 190 more) or mortality (RR, 1.01; 95% CI, 0.4-2.57). PE was not systematically evaluated.
As both of these trials routinely screened patients for asymptomatic DVT (which are usually treated if detected), and neither study reported PE, a direct estimate of effects on symptomatic VTE is only avail-able from one trial with a very small number of events. 11 For the comparison of LDUH vs placebo, results failed to demonstrate or exclude a benefi cial or detrimental effect on symptomatic DVT (RR, 0.89; 95% CI, 0.57-1.41; six fewer per 1,000; 95% CI, from 25 fewer to 24 more) or PE (RR, 0.48; 95% CI, 0.10-2.26; 22 fewer per 1,000 (95% CI, from 38 fewer to 53 more) (Table S14). Similarly, comparing LMWH
of patient immobilization or acute hospital stay (Grade 2B) .
3.0 Critically Ill Patients
3.1 Risk of VTE
The risk of VTE in patients who are admitted to an ICU varies, depending on their acute illness (eg, sepsis), chronic illnesses (eg, congestive heart failure), prehospi-tal diagnoses (eg, prior VTE), and ICU-specifi c expo-sures and events (eg, immobilization, surgery, and other invasive procedures [such as central venous catheteriza-tion] mechanical ventilation, and drugs such as vaso-pressors and paralytic agents) ( Table 10 , Table S12). 67 There are no validated risk assessment models to stratify VTE risk in critically ill patients.
3.2 Screening for VTE
There are no studies in critically ill patients of the effectiveness of screening compression ultrasonography and subsequent treatment of identifi ed DVT in reduc-ing the rate of subsequent symptomatic thromboem-bolic complications ( Table 11 ). Indirect evidence provides no support for ultrasonographic screening. 59,60
3.3 Risk of Bleeding
Although critically ill patients are at increased risk for VTE, they frequently develop bleeding complica-tions in the ICU. Up to 80% of critically ill patients have one or more episodes of bleeding, although most bleeding is minor. 68 The risk of major bleeding in the untreated arm of a prophylaxis trial in critical care patients was 2.7%, 69 but the range in practice is dependent on the case mix. Only few studies have
Table 10—[Section 3.1] Summary of Findings: Should Unfractionated Heparin vs Placebo Be Used for DVT Prevention in Critically Ill Adult Patients?71
OutcomeNo. of Participants (Studies) Follow-up
Quality of the Evidence (GRADE) Relative Effect (95% CI)c
Anticipated Absolute Effects
Baseline RiskRisk Difference With
UFH (95% CI)
Symptomatic DVT 1,457 (1 RCT) up to 28 d Moderate due to imprecisiona
RR, 0.89 (0.57-1.41) 58 per 1,000 6 fewer per 1,000 (25 fewer to 24 more)
Pulmonary embolus 1,457 (1 RCT) up to 28 d Low due to indirectnessb and imprecisiona
RR, 0.48 (0.10-2.26) 42 per 1,000 22 fewer per 1,000 (38 fewer to 53 more)
Death No data … … … …Major bleeding No data … … … …
See Table 1 and 4 legends for expansion of abbreviations.aWe will consider the presence of serious imprecision when there are , 300 events in total (events in treatment and control patients) or when CIs include appreciable harms and benefi ts.bPulmonary embolus baseline risk was obtained from observational studies whereas the relative risk is from RCT (mix of symptomatic and asymptomatic events)cRR estimated from a mix of symptomatic and asymptomatic events.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e210S Prevention of VTE in Nonsurgical Patients
The panel considered suggesting LMWH over LDUH; however, the benefi t was small enough in magnitude (eight PEs per 1,000 patients prevented by LMWH with lower boundary of the CI of 0.6 PE per 1,000), and the treatment effect was only driven by a difference of 16 events. In addition, this trial performed screening compression ultrasonography on all enrolled patients, which differs from real world practice. If DVTs detected on ultrasonog-raphy remained undiagnosed and untreated and progressed to symptomatic PE, the treatment effect would likely be different. The panel decided to not issue this recommendation in the absence of evi-dence from other future trials and reliable cost-effective data.
There are no randomized trials comparing mechan-ical methods of prophylaxis (GCS, IPC) with no pro-phylaxis in critically ill patients. Although combined mechanical and pharmacologic prophylaxis appears to be more effective in reducing symptomatic and asymptomatic VTE events than mechanical methods alone in surgical ICU patients, it is not known whether this is the same in medical ICU patients. 73
Recommendations
3.2. In critically ill patients, we suggest against routine ultrasound screening for DVT (Grade 2C) .
3.4.3. For critically ill patients, we suggest using LMWH or LDUH thromboprophylaxis over no prophylaxis (Grade 2C) .
3.4.4. For critically ill patients who are bleeding, or are at high risk for major bleeding ( Table 4 ), we suggest mechanical thromboprophylaxis
vs placebo, results failed to demonstrate or exclude a benefi cial or detrimental effect of LMWH on symptomatic DVT (RR, 0.82; 95% CI, 0.51-1.32), PE (RR, 1.01; 95% CI, 0.31-3.31), bleeding (RR, 2.09; 95% CI, 0.54-8.16), or mortality (RR, 1.01; 95% CI, 0.4-2.57) (Table S15). Combining data from the above com parisons, 11,69,71 the use of any heparin (LMWH or LDUH) compared with placebo was associated with similar risks of symptomatic DVT, symptom-atic PE, major bleeding, and mortality (Table S16; Table 13 ).
A large randomized, blinded, placebo-controlled trial compared the LMWH dalteparin 5,000 Inter-national Units daily vs LDUH 5,000 International Units bid in 3,764 critically ill patients expected to remain in the ICU for � 3 d. The trial failed to demonstrate or exclude difference in the rate of proximal leg asymptomatic DVT (5.1% vs 5.8%, respectively; HR, 0.92; 95% CI, 0.68-1.23). 12 PE was not systematically screened, and PE events were classifi ed by a blinded, independent adjudi-cation committee as defi nite, probable, possible, or absent. Symptomatic PE occurred in signifi cantly fewer patients receiving dalteparin compared with LDUH (22 of 1,873 [1.2%] vs 38 of 1,873 [2%]; RR, 0.58; 95% CI, 0.34-0.97). The study failed to show differences in major bleeding, rates of HIT, ICU mortality, and hospital mortality in the dalteparin and LDUH groups (major bleeding, 5.5% vs 5.6%; HR, 1.00; 95% CI, 0.75-1.34; HIT, 0.3% vs 0.6%; HR, 0.47; 95% CI, 0.16-1.35; ICU mortality, 15.2% vs 16.2%; HR, 0.97; 95% CI, 0.82-1.15; hospital mortality, 22.1% vs 24.5%; HR, 0.92; 95% CI, 0.80-1.05). Two other trials 11,72 conducted this com-parison with variable reporting of symptomatic outcomes ( Table 14 , Table S17).
Table 11—[Section 3.2] Summary of Findings: Should LMWH vs Placebo Be Used for DVT Prevention in Critically Ill Adult Patients?12,70
OutcomeNo. of Participants (Studies) Follow-up
Quality of the Evidence (GRADE) Relative Effect (95% CI)
Anticipated Absolute Effects
Baseline RiskRisk difference with LMWH (95% CI)
Symptomatic DVT 1,437 (1 RCT) 5-28 d
Moderate due to serious imprecisiona
RR, 0.82 (0.51-1.32) 58 per 1,000 6 fewer (from 23 fewer to 22 more)
Pulmonary embolus 1,437 (1 RCT) 5-28 d
Very low due to very serious imprecisionb and indirectnessc
RR, 1.01 (0.31-3.31) 42 per 1,000 1 more (from 29 fewer to 97 more)
Death 169 (1 RCT) 5-28 d
Low due to very serious imprecisiona
RR, 1.01 (0.40-2.57) 94 per 1,000 1 more per 1,000 (from 56 fewer to 148 more)
Major bleeding 221 (1 RCT) 5-28 d
Low due to very serious imprecisiona
RR, 2.09 (0.54 -8.16) 27 per 1,000 29 more per 1,000 (from 12 fewer to 190 more)
See Table 1 and 4 legends for expansion of abbreviations.aCIs include appreciable harms and benefi ts.b The RR of the outcome of PE is considered very imprecise due to small number of events (4 of 478 LMWH vs 8 of 959 placebo).cRR estimated from a mix of symptomatic and asymptomatic events.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
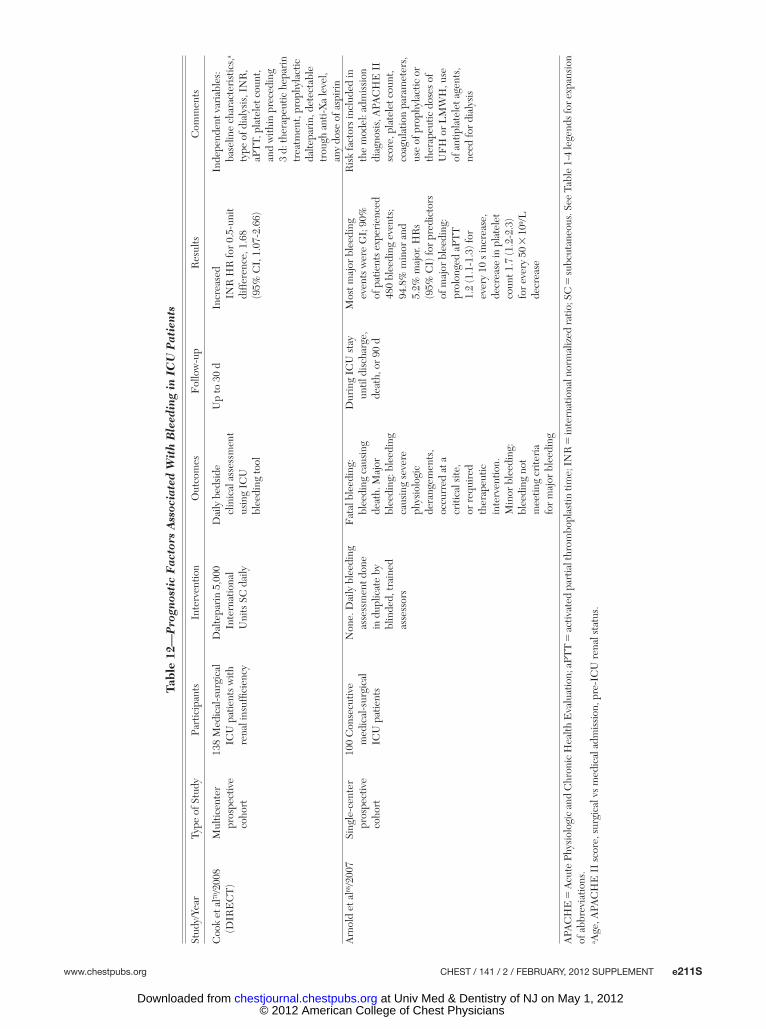
www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e211S
Tabl
e 12
—P
rogn
osti
c F
acto
rs A
ssoc
iate
d W
ith
Ble
edin
g in
IC
U P
atie
nts
Stud
y/Ye
arTy
pe o
f Stu
dyPa
rtic
ipan
tsIn
terv
entio
nO
utco
mes
Fol
low
-up
Res
ults
Com
men
ts
Coo
k et
al70
/200
8 (D
IRE
CT
)M
ultic
ente
r pr
ospe
ctiv
e co
hort
138
Med
ical
-sur
gica
l IC
U p
atie
nts
with
re
nal i
nsuf
fi cie
ncy
Dal
tepa
rin
5,00
0 In
tern
atio
nal
Uni
ts S
C d
aily
Dai
ly b
edsi
de
clin
ical
ass
essm
ent
usin
g IC
U
blee
ding
tool
Up
to 3
0 d
Incr
ease
d IN
R H
R fo
r 0.
5-un
it di
ffer
ence
, 1.6
8 (9
5% C
I, 1
.07-
2.66
)
Inde
pend
ent v
aria
bles
: ba
selin
e ch
arac
teri
stic
s,a
type
of d
ialy
sis,
IN
R,
aPT
T, p
late
let c
ount
, an
d w
ithin
pre
cedi
ng
3 d:
ther
apeu
tic h
epar
in
trea
tmen
t, pr
ophy
lact
ic
dalte
pari
n, d
etec
tabl
e tr
ough
ant
i-Xa
leve
l, an
y do
se o
f asp
irin
Arn
old
et a
l68/2
007
Sing
le-c
ente
r pr
ospe
ctiv
e co
hort
100
Con
secu
tive
med
ical
-sur
gica
l IC
U p
atie
nts
Non
e. D
aily
ble
edin
g as
sess
men
t don
e in
dup
licat
e by
bl
inde
d, tr
aine
d as
sess
ors
Fat
al b
leed
ing:
bl
eedi
ng c
ausi
ng
deat
h. M
ajor
bl
eedi
ng: b
leed
ing
caus
ing
seve
re
phys
iolo
gic
dera
ngem
ents
, oc
curr
ed a
t a
criti
cal s
ite,
or r
equi
red
ther
apeu
tic
inte
rven
tion.
M
inor
ble
edin
g:
blee
ding
not
m
eetin
g cr
iteri
a fo
r m
ajor
ble
edin
g
Dur
ing
ICU
sta
y un
til d
isch
arge
, de
ath,
or
90 d
Mos
t maj
or b
leed
ing
even
ts w
ere
GI;
90%
of
pat
ient
s ex
peri
ence
d 48
0 bl
eedi
ng e
vent
s;
94.8
% m
inor
and
5.
2% m
ajor
. HR
s (9
5% C
I) fo
r pr
edic
tors
of
maj
or b
leed
ing:
pr
olon
ged
aPT
T
1.2
(1.1
-1.3
) for
ev
ery
10 s
incr
ease
, de
crea
se in
pla
tele
t co
unt 1
.7 (1
.2-2
.3)
for
ever
y 50
3 1
09 /L
decr
ease
Ris
k fa
ctor
s in
clud
ed in
th
e m
odel
: adm
issi
on
diag
nosi
s, A
PAC
HE
II
scor
e, p
late
let c
ount
, co
agul
atio
n pa
ram
eter
s,
use
of p
roph
ylac
tic o
r th
erap
eutic
dos
es o
f U
FH
or
LM
WH
, use
of
ant
ipla
tele
t age
nts,
ne
ed fo
r di
alys
is
APA
CH
E 5
Acu
te P
hysi
olog
ic a
nd C
hron
ic H
ealth
Eva
luat
ion;
aPT
T 5
activ
ated
par
tial t
hrom
bopl
astin
tim
e; I
NR
5 in
tern
atio
nal n
orm
aliz
ed ra
tio; S
C 5
subc
utan
eous
. See
Tab
le 1
-4 le
gend
s for
exp
ansi
on
of a
bbre
viat
ions
.a A
ge, A
PAC
HE
II
scor
e, s
urgi
cal v
s m
edic
al a
dmis
sion
, pre
-IC
U r
enal
sta
tus.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e212S Prevention of VTE in Nonsurgical Patients
in the article about prevention of VTE in surgical patients in this supplement. 1
4.1 Risk of VTE
Patients with cancer have at least a sixfold increased risk of VTE, 16,74 and the development of DVT is asso ciated with a signifi cant reduction in survival in this population. 75-77 VTE risk is higher with certain cancers (malignant brain tumors; adenocarcinomas of the lung, ovary, pancreas, colon, stomach, prostate, and kidney; and hematologic malignancies). 78
Nonsurgical therapies for cancer, such as chemo-therapy and hormonal manipulation, also increase
with GCS (Grade 2C) or IPC (Grade 2C) until the bleeding risk decreases, rather than no mechan-ical thromboprophylaxis. When bleeding risk decreases, we suggest that pharmacologic throm-boprophylaxis be substituted for mechanical thromboprophylaxis (Grade 2C) .
4.0 Patients With Cancer in the Outpatient Setting
The role of thromboprophylaxis to prevent VTE in patients with cancer undergoing surgery is addressed
Table 13—[Section 3.4.3] Summary of Findings: Should Any Heparin (LDUH, LMWH) vs Placebo Be Used for DVT Prophylaxis in Critically Ill Adult Patients?12,70,71
Outcome
No. of Participants
(Studies) Follow-up Quality of the
Evidence (GRADE) Relative Effect (95% CI)
Anticipated Absolute Effects
Baseline RiskRisk Difference With Any
Heparin (95% CI)
Symptomatic DVT 1,935 (1 RCT) 5-28 d
Moderate due to serious imprecisiona
RR, 0.86 (0.59-1.25) 58 per 1,000 4 fewer per 1,000 (from 12 fewer to 8 more)
Pulmonary embolus 1,935 (1 RCT) 5-28 d
Low due to serious imprecisiona and indirectnessb
RR, 0.73 (0.26-2.11) 42 per 1,000 11 fewer per 1,000 (from 31 fewer to 47 more)
Death 169 (1 RCT) 5-28 d
Low due to very serious imprecisiona
RR, 1.01 (0.40-2.57) 94 per 1,000 1 more per 1,000 (from 56 fewer to 148 more)
Major bleeding 221 (1 RCT) 5-28 d
Low due to very serious imprecisiona
RR, 2.09 (0.54-8.16) 27 per 1,000 29 more per 1,000 (from 12 fewer to 190 more)
See Table 1 and 4 legends for expansion of abbreviations.aWe will consider the presence of serious imprecision when there are , 300 events in total (events in treatment and control patients) or when CIs include appreciable harms and benefi ts.bRR estimated from a mix of symptomatic and asymptomatic events.
Table 14—[Section 3.4.4] Summary of Findings: Should LMWH vs Unfractionated Heparin Be Used for DVT Prevention in Critically Ill Adult Patients?12,13,72
Outcome
Anticipated Absolute Effects
Relative Effect (95% CI)No. of Participants (Studies) Follow-up
Quality of the Evidence (GRADE)Risk with UFH
Risk Difference With LMWH (95% CI)
Symptomatic DVT 25 per 1,000 3 fewer per 1,000 (from 10 fewer
to 6 more)
RR, 0.87 (0.60-1.25) 4,722 (2 RCTs) 7-28 d Moderate due to imprecisiona
Symptomatic pulmonary embolism
20 per 1,000 8 fewer per 1,000 (13.2 fewer
to 0.6 fewer)
RR, 0.58 (0.34-0.97) 3,746 (1 RCT) 7 d Moderate due to imprecisiona
Major bleeding 55 per 1,000 2 fewer per 1,000 (from 14 fewer
to 14 more)
RR, 0.97 (0.75-1.26) 3,902 (2 RCTs) 7-47 d Moderate due to imprecisiona
Death 159 per 1,000 10 fewer per 1,000 (from 30 fewer
to 14 more)
RR, 0.94 (0.81-1.09) 3,902 (2 RCTs) 7-47 d Moderate due to imprecisiona
Heparin-induced thrombocytopenia
6 per 1,000 3 fewer per 1,000 (from 5 fewer
to 1 more)
RR, 0.42 (0.15-1.18) 3,746 (1 RCT) 7 d Moderate due to imprecisiona
See Table 1 and 4 legends for expansion of abbreviations.aWe will consider the presence of serious imprecision when there are , 300 events in total (events in treatment and control patients) or when CIs include appreciable harms and benefi ts.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e213S
one study and LMWH in the remaining studies; all studies used prophylactic doses. Type of chemo-therapy, duration of treatment, and duration of antithrombotic prophylaxis varied widely among the studies. A number of studies administered hep-arin for the duration of chemotherapy, whereas other studies administered it for fi xed durations of heparin (eg, 6 weeks, 12 months).
Overall, the effect of heparin therapy on mortality was not statistically signifi cant at 12 months (RR, 0.93; 95% CI, 0.85-1.02), but it was statistically signif-icant at 24 months (RR, 0.92; 95% CI, 0.88-0.97) ( Table 15 , Table S18). Heparin therapy also reduced symptomatic VTE (RR, 0.55; 95% CI, 0.37-0.82). The results failed to confi rm or to exclude benefi cial or detrimental effects of heparin therapy on major bleeding (RR, 1.30; 95% CI, 0.59-2.88), minor bleed-ing (RR, 1.05; 95% CI, 0.75-1.46), and quality of life (assessed in only one study 103 ). The quality of evi-dence was high for symptomatic VTE; moderate for mortality, major bleeding, and minor bleeding; and low for quality of life.
In a subgroup analysis of patients with small cell lung cancer (SCLC) 104,105 vs other types of cancer, the test for subgroup effect was statistically signifi cant for mortality at 12 months ( P 5 .03) (RR, 0.86; 95% CI, 0.75-0.98 for SCLC vs RR, 0.96; 95% CI, 0.86-1.07
the risk of VTE. 16,79-86 The rate of VTE increases by twofold to fi vefold among women whose breast cancer has been treated with the selective estrogen receptor modulator tamoxifen. 85,87 This risk was even greater in postmenopausal women when tamoxifen was combined with chemotherapy. 88 The use of aro-matase inhibitors anastrozole, letrozole, or exemes-tane is associated with about one-half the risk of VTE compared with tamoxifen. 89-92 Angiogenesis inhibitors have also been shown to increase thromboembolic complications in patients with cancer. 93 Thalidomide and lenalidomide increase the risk of venous throm-bosis, especially when combined with chemotherapy or high-dose dexamethasone. 94-97 A recent meta-analysis reported a high risk of VTE in patients with cancer receiving bevacizumab. 98 Finally, the presence of a CVC in patients with cancer predisposes to upper extremity DVT. 99-101
4.2 Parenteral Anticoagulants
A recent systematic review evaluated the effi cacy and safety of parenteral anticoagulants in outpa-tients with cancer. 102 The review identifi ed nine eligible RCTs enrolling 2,857 patients with meta-static or locally advanced solid cancers of different tissue types. The intervention consisted of UFH in
Table 15—[Section 4.2] Summary of Findings: Should Heparin Compared With No Heparin Be Used for Patients With Cancer Who Have No Other Therapeutic or Prophylactic Indication for Anticoagulation?102
Outcomes
Illustrative Comparative Risksa (95% CI)
Relative Effect (95% CI)
No. of Participants (Studies)
Quality of the Evidence (GRADE)
Assumed Risk, No Heparin
Corresponding Risk, Heparin
Mortality; follow-up: 12 mo
Medium-risk population RR, 0.93 (0.85-1.02) 2,531 (8) Moderateb-d
649 per 1,000 604 per 1,000 (552 to 662)Symptomatic VTE;
follow-up: 12 moMedium-risk population RR, 0.55 (0.37-0.82) 2,264 (7) Highb
29 per 1,000 16 per 1,000 (11 to 24)Major bleeding;
follow-up: 12 moMedium-risk population RR, 1.3 (0.59-2.88) 2,843 (9) Moderateb,e
7 per 1,000 9 per 1,000 (4 to 20)Minor bleeding;
follow-up: 12 wkMedium-risk population RR, 1.05 (0.75-1.46) 2,345 (7) Moderateb,e
27 per 1,000 28 per 1,000 (20 to 39)Health-related quality of
life: the Uniscale and the Symptom Distress Scale; better indicated by lower values. Follow-up: 12 mo
Not estimable Not estimable Not estimablef 0 (1) Lowg
See Table 4 legend for expansion of abbreviations.aThe basis for the assumed risk (eg, the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).bVast majority of studies had allocation concealment and used blinded outcome and adjudication. We did not downgrade, although there was some concern about lack of blinding in some studies; the overall risk of bias was believed to be very low.cThere is moderate heterogeneity among studies included in the analysis of death at 12 mo (I2 5 41%). The subgroup analysis for mortality at 12 mo was statistically signifi cant and suggested survival benefi t in patients with small cell lung cancer but not in patients with advanced cancer. Overall we decided to downgrade by one level when considering these issues along with imprecision.dCI interval includes effects suggesting benefi t as well as no benefi t.eCI includes possibility of both harms and benefi ts.fThe scores for the two scales were similar for the two study groups, both at baseline and at follow-up.gHigh risk of bias and only 138 patients enrolled.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e214S Prevention of VTE in Nonsurgical Patients
ing (RR, 4.24; 95% CI, 1.85-9.68; 23 more per 1,000 [from six more to 61 more]) and minor bleeding (RR, 3.34; 95% CI, 1.66-6.74). The quality of evidence was moderate for all outcomes ( Table 16 , Table S19). In summary, the absolute risk increase of bleeding with warfarin outweighs the absolute risk reduction of VTE.
4.4 Patients With Cancer With Indwelling CVCs
CVCs may result in arm swelling and discomfort, PE, predisposition to catheter-related sepsis, and the need to replace the catheter. 107,108 Peripherally inserted CVCs are associated with a greater risk of thrombosis than subclavian vein or internal jugular vein access. 109,110 If the CVC tip is placed in the upper superior vena cava or more peripherally, the DVT risk is higher than when placed at or just above the right atrium. 111 Other potential risk factors include left-sided CVC insertion, chest radiotherapy, more than one insertion attempt, and previous CVC insertion. 112,113
A systematic review identifi ed 12 eligible RCTs that enrolled 3,611 patients with cancer and an indwelling CVC 114 and compared prophylactic-dose heparin (LDUH or LMWH) or low-dose VKAs to each other or to no anticoagulation. Most studies administered treatments for a specifi ed fi xed period or until CVC removal or thrombosis diagnosis.
Prophylactic-dose heparin was associated with a trend toward reduction in symptomatic DVT (RR, 0.54; 95% CI, 0.28-1.05) ( Table 17 , Table S20). The results failed to confi rm or to exclude benefi cial or detrimental effects of prophylactic-dose heparin on
for other types of cancer) but not statistically signifi -cant at 24 months ( P 5 .88). In a subgroup analysis of patients with advanced cancer vs patients with non-advanced cancer, the review found no signifi cant dif-ference between the effects of heparin in the two subgroups ( P 5 .51).
In summary, there is moderate-quality evidence of a reduction in mortality and high-quality evidence of a reduction in VTE with larger absolute effects than any plausible increase in risk of major bleeding. There is a possible but not convincing increased mortality benefi t in the subgroup of patients with SCLC.
4.3 Oral Anticoagulants
A recent systematic review evaluated the effi cacy and safety of oral anticoagulants in patients with can-cer and no therapeutic or prophylactic indication for anticoagulation. 106 The review identifi ed fi ve eligible RCTs that enrolled 1,656 patients. The intervention consisted of warfarin in all fi ve studies; started within a month before, or at the time of, initiating chemo-therapy; and continued until the end of chemotherapy or up to a few weeks later.
Warfarin had little or no effect on reducing mortality at 6 months (RR, 0.96; 95% CI, 0.80-1.16), at 1 year (RR, 0.94; 95% CI, 0.8-1.03), at 2 years (RR, 0.97; 95% CI, 0.87-1.08), or at 5 years (RR, 0.91; 95% CI, 0.83-1.01). One study assessed the effect of warfarin on VTE and showed an RR reduction of 85% (RR, 0.15; 95% CI, 0.02-1.2; 25 fewer per 1,000 [from 28 fewer to six more]). Warfarin increased both major bleed-
Table 16—[Section 4.3] Summary of Findings: Should Oral Anticoagulation Be Used in Patients With Cancer With No Therapeutic or Prophylactic Indication for Anticoagulation?102
Outcomes
Illustrative Comparative Risksa (95% CI)
Assumed Risk, Control
Corresponding Risk, Oral Anticoagulation Relative Effect (95% CI)
No of Participants (Studies)
Quality of the Evidence (GRADE)
Death; follow-up: median 1 y
457 per 1,000 430 per 1,000 (398- 471) RR, 0.94 (0.87-1.03) 1,604 (5) Moderateb
VTE; follow-up: 1 y 43 per 1,000 6 per 1,000 (1-52) RR, 0.15 (0.02-1.2) 315 (1) Moderatec
Major bleeding; follow-up: median 1 y
22 per 1,000 93 per 1,000 (41-213) RR, 4.24 (1.85-9.68) 1,282 (4) Moderated
Minor bleeding; follow-up: 1 y
79 per 1,000 264 per 1,000 (131-532) RR, 3.34 (1.66-6.74) 851 (3) Moderated
Health-related quality of life: not reported
Not estimable Not estimable Not estimable … Not estimable
See Table 1 and 4 legends for expansion of abbreviations.aThe basis for the assumed risk (eg, the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).bWe downgraded because of lack of blinding of patients and providers in four out of fi ve studies, it was unclear whether allocation was concealed in two studies, and only one study clearly used ITT analysis.cWe downgraded because the precision of the estimate does not exclude a patient-important benefi t (the lower limit of RR still suggests a benefi t that might be relevant given the high baseline risk).dWe downgraded because lack of blinding of patients and providers in three out of four studies, it was unclear whether allocation was concealed in two studies, and only one study clearly used ITT analysis.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e215S
and low risk of bleeding are more likely to benefi t than be harmed from heparin prophylaxis.
Recommendations
4.2.1. In outpatients with cancer who have no additional risk factors for VTE, we suggest against routine prophylaxis with LMWH or LDUH (Grade 2B) and recommend against the prophylactic use of VKAs (Grade 1B) .
Remarks : Additional risk factors for venous thrombosis in outpatients with cancer include previous venous thrombosis, immobilization, hormonal therapy, angio-genesis inhibitors, thalidomide, and lenalidomide.
4.2.2. In outpatients with solid tumors who have additional risk factors for VTE and who are at low risk of bleeding, we suggest prophylactic-dose LMWH or LDUH over no prophylaxis (Grade 2B) .
Remarks : Additional risk factors for venous thrombosis in outpatients with cancer include previous venous thrombosis, immobilization, hormonal therapy, angio-genesis inhibitors, thalidomide, and lenalidomide.
4.4. In outpatients with cancer and indwelling CVCs, we suggest against routine prophylaxis with LMWH or LDUH (Grade 2B) and suggest against the prophylactic use of VKAs (Grade 2C) .
5.0 Chronically Immobilized Outpatients
5.1 Risk of VTE
The recognition that bedbound hospitalized patients are at increased risk for VTE has led many clinicians
death (RR, 0.85; 95% CI, 0.53-1.37), major bleeding (RR, 0.68; 95% CI, 0.10-4.78), thrombocytopenia (RR, 0.85; 95% CI, 0.49-1.46), and infection (RR, 0.91; 95% CI, 0.49-1.68). No data were available for HIT, heparin-induced thrombocytopenia and throm-bosis , PE, or catheter failure. The quality of evidence was moderate for all outcomes.
Results failed to confi rm or to exclude benefi cial or detrimental effects of low-dose VKAs on death (RR, 0.97; 95% CI, 0.82-1.15), symptomatic DVT (RR, 0.63; 95% CI, 0.35-1.11), or major bleeding (RR, 6.93; 95% CI, 0.86-56.08) ( Table 18 , Table S21). However, low-dose VKAs were associated with a statistically signifi cant reduction in asymptomatic DVT (RR, 0.42; 95% CI, 0.28-0.61).
Studies comparing heparin to VKA found no effects on any of the outcomes of interest. The quality of evidence was low for all these outcomes ( Table 19 , Table S22).
In summary, prophylactic-dose heparin in patients with cancer and CVCs is potentially associated with more benefi ts than harms. It is uncertain whether the potential benefi ts of low-dose VKAs outweigh the associated potential increase in bleeding.
Despite evidence of benefi t of prophylactic-dose heparin in some outpatients with cancer and some patients with cancer with CVCs, the substantial clin-ical heterogeneity of the patients studied (different cancer types, different cancer treatments, and dif-ferent durations of prophylaxis) raises questions about which groups of outpatients with cancer will benefi t. More evidence will be available over the next few years on the effectiveness, cost-effectiveness, and specifi c patient groups most likely to benefi t from prophylaxis. Considering the selection criteria of the studies, patients with solid cancer, high risk for VTE,
Table 17—[Section 4.4] Summary of Findings: Should Heparin Compared With No Heparin Be Used for Thrombosis Prophylaxis in Patients With Cancer With Central Venous Catheters?114
Outcomes
Illustrative Comparative Risksa (95% CI)
Relative Effect (95% CI)No. of Participants
(Studies)
Quality of the Evidence (GRADE)
Assumed Risk, No Heparin
Corresponding Risk, Heparin
Death 65 per 1,000 55 per 1,000 (34-89) RR, 0.85 (0.53-1.37) 1,192 (5) Moderateb-d
Symptomatic DVT 49 per 1,000 26 per 1,000 (14-51) RR, 0.54 (0.28-1.05) 1,173 (6) Moderateb-d
Major bleeding 5 per 1,000 3 per 1,000 (1-24) RR, 0.68 (0.1-4.78) 891 (4) Moderateb-d
Infection 71 per 1,000 65 per 1,000 (35-119) RR, 0.91 (0.49-1.68) 626 (3) Moderateb,c
Thrombocytopenia 66 per 1,000 56 per 1,000 (32-96) RR, 0.85 (0.49-1.46) 836 (3) Moderateb-d
Quality of life: not reported
Not estimable Not estimable Not estimable … Not estimable
See Table 4 for expansion of abbreviations.aThe basis for the assumed risk (eg, the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).bAllocation clearly concealed in three of the six studies. Four studies blinded patients and providers and all studies blinded outcome adjudicators. Three studies had no problem with incomplete data. None of the studies was suspected of selective reporting. Two studies clearly used ITT.cRelatively small number of events.dCI includes both values suggesting no effect and values suggesting either benefi t or harm.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e216S Prevention of VTE in Nonsurgical Patients
ical condition reducing mobility for at least 48 h. 115 Anticoagulant prophylaxis was administered to 35% of patients. The study found a 1.2% incidence of symptomatic VTE in the 3 weeks after the onset of the acute condition. This incidence is similar to studies examining patients hospitalized with acute medical conditions, but the pattern of immobility (acute rather than chronic) does not allow extrapolation to home-bound patients.
Several observational studies have examined the incidence of VTE in nursing home patients, including two large studies using the Minimum Data Set, a mandatory questionnaire completed for all Medicare-licensed long-term facilities in the United States. 116,117 Liperoti and colleagues retrospectively assessed 132,018 nursing home patients across fi ve states
to consider whether chronically immobilized outpa-tients are at similar increased risk, and whether they may also benefi t from VTE prophylaxis. The chroni-cally immobile population is large and includes patients who are homebound, as well as residents of nursing homes and postacute care facilities. Despite their similarities to medical inpatients, there have been few studies and no placebo-controlled trials investi-gating VTE prophylaxis for chronically immobilized outpatients.
Although the population at risk is clearly large, the scope of the problem and incidence of symptomatic VTE is uncertain. One study of outpatients examined the incidence of symptomatic VTE in 16,532 outpa-tients . 40 years of age (median age, 71 years) who were not immobile at baseline and had an acute med-
Table 18—[Section 4.5] Summary of Findings: Should VKA Compared With No VKA Be Used for Thrombosis Prophylaxis in Patients With Cancer With Central Venous Catheters?114
Outcomes
Illustrative Comparative Risksa (95% CI)
Relative Effect (95% CI)No. of Participants
(Studies)Quality of the
Evidence (GRADE)Assumed Risk,
no VKA Corresponding Risk, VKA
Death 312 per 1,000 303 per 1,000 (256-359) RR, 0.97 (0.82-1.15) 1,093 (2) Moderate due to imprecisionb,c
Symptomatic DVT 90 per 1,000 57 per 1,000 (31-100) RR, 0.63 (0.35-1.11) 1,235 (4) Moderate due to imprecisionb,c
Major bleeding 2 per 1,000 14 per 1,000 (2-112) RR, 6.93 (0.86-56.08) 1,093 (2) Moderate due to imprecisionb,c; high-quality evidence in other populations
See Table 1 and 4 legends for expansion of abbreviations.aThe basis for the assumed risk (eg, the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).bWe did not rate down for methodologic limitations. Allocation clearly concealed in three of the four studies. None of studies blinded patients, providers, or data collectors, and three studies blinded outcome adjudicators. Three studies had no problem with incomplete data. The presence of selective reporting was unclear in one study. Two studies clearly used ITT.cRelatively small number of events. CI includes both values suggesting no effect and values suggesting either benefi t or harm.
Table 19—[Section 4.6] Summary of Findings: Should LMWH Compared With VKA Be Used for Thrombosis Prophylaxis in Patients With Cancer With Central Venous Catheters?114
Outcomes
Illustrative Comparative Risksa (95% CI)
Relative Effect (95% CI)No. of Participants
(Studies)
Quality of the Evidence (GRADE)
Assumed Risk, VKA
Corresponding Risk, LMWH
Death 110 per 1,000 140 per 1,000 (61-326) RR, 1.27 (0.55-2.96) 343 (2) Lowb-d
Symptomatic DVT 22 per 1,000 28 per 1,000 (6-143) RR, 1.28 (0.25-6.5) 280 (2) Lowb-d
Major bleeding 0 per 1,000 0 per 1,000 (0-0) RR, 3.1 (0.13-73.14) 343 (2) Lowb-d
Thrombocytopenia 0 per 1,000 0 per 1,000 (0-0) RR, 5.17 (0.26-103.21) 59 (1) Lowb-d
Quality of life: not reported Not estimable Not estimable Not estimable … Not estimable
See Table 1 and 4 legends for expansion of abbreviations.aThe basis for the assumed risk (eg, the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).bAllocation clearly concealed in one of the two studies. None of the studies blinded patients, providers, or data collectors, but both studies blinded outcome adjudicators. One study did not address incomplete data reporting. None of the studies was suspected of selective reporting. One study clearly used ITT.cRelatively small number of events.dCI includes both values suggesting no effect and values suggesting either benefi t or harm.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e217S
6.0 Long-Distance Travel
6.1 Risk of VTE
Prolonged air travel results in a very small absolute incidence of VTE. A systematic review and meta-analysis of 14 studies (11 case-control, two cohort, and one case-crossover) of risk for VTE in travelers demonstrated a pooled RR of 2.8 (95% CI, 2.2-3.7). A dose-response relationship was identifi ed, with an 18% higher risk of VTE for each 2-h increase in travel duration. 122,123 However, the overall absolute inci-dence of a symptomatic VTE in the month following a fl ight . 4 h is 1 in 4,600 fl ights, 124 with a reported incidence of asymptomatic VTE on arrival from a trip ranging from 0% to 1.5%. 123 The incidence varies by the type and duration of travel and by individual risk factors. 125-127 Thrombosis risk also appears to be increased for travel by car, bus, or train. 128-130
The association between air travel and VTE is strongest for fl ights . 8 to 10 h 125-128,131-133 and is increased in the presence of VTE risk factors such as recent surgery. 123 For those on fl ights . 4 h, immo-bility during the fl ight and window seating (especially for obese persons) also increase the risk of VTE. 134 Especially tall or short passengers may have an increased risk. 130 There is no defi nitive evidence that dehydration, travel in economy class, and drink-ing alcoholic beverages on the fl ight are related to VTE risk.
Most individuals with travel-associated VTE have one or more known risk factors for thrombosis, including previous VTE, recent surgery or trauma, active malignancy, pregnancy, estrogen use, advanced age, limited mobility, severe obesity, or a thrombo-philic disorder. 129,130,132,135-140 Among healthy volunteers, coagulation activation observed after an 8-h fl ight was greater in carriers of factor V Leiden and in women taking oral contraceptives. 141 Case-control studies have reported an increased risk of VTE in travelers who have thrombophilia and use oral contraceptives. 130,136
We identifi ed a Cochrane review 142 of nine RCTs of thromboprophylaxis in long-distance air travelers (Tables S24, S25). All but one of these trials was con-ducted by a single group of investigators. 140,143-150 Trials enrolled a mix of low- and increased-risk subjects based on risk factors for VTE, and most studies included persons taking fl ights of . 7 h. Asymptomatic DVT detected by screening ultrasound examination was the primary end point. All of the trials have meth-odologic limitations that compromise their interpre-tation. Further, the UK General Medical Council’s Fitness to Practice Panel judged that these papers included coauthors who had not approved the papers and erased the principal investigator from the register of the General Medical Council. 151 Regardless, as there
and found a symptomatic VTE incidence of 0.91 per 100 person-years. Similarly, a retrospective study of 18,661 nursing home patients in Kansas found a VTE incidence of 1.30 per 100 person-years. 116 These studies suggest that the best estimate of the annual incidence of symptomatic VTE in nursing home patients is approximately 1%. The use of anticoagu-lant prophylaxis has not been examined adequately in this population to draw conclusions on whether the benefi ts outweigh the risks and costs.
The incidence of VTE in postacute care facil-ities was examined in a prospective cohort study of 3,039 patients admitted for rehabilitation after acute medical illness or surgery. 118 Reasons for admission to the facility included medical illness (54.7%), stroke (21.1%), and surgery (31.7%). Most patients (75.1%) received anticoagulant thromboprophylaxis, which was primarily LMWH. The incidence of symptom-atic VTE was 2.4% during the stay at the facility (median duration 26 days). Risk factors for VTE were cancer and prior VTE.
Two cross-sectional studies examined the preva-lence of asymptomatic DVT in elderly patients in postacute care facilities in France and detected asymptomatic DVT in 14.0% and 15.8% of patients, respectively. 119,120 A subsequent analysis that com-bined data from these two studies noted that although proximal DVT was not signifi cantly reduced among patients who received LMWH prophylaxis (5.7% vs 4.0%; P 5 .16), this difference became statistically signifi cant with the use of propensity analysis to con-trol for potentially confounding variables (OR, 0.56; P 5 .03). 121 These studies suggest that the incidence of asymptomatic DVT in elderly patients in postacute care facilities is similar to that of hospitalized patients. However, their observational designs and lack of patient-important end points does not allow for any conclusions to be drawn on whether thromboprophy-laxis is of benefi t in this population (Table S23).
The available data suggest that nursing home patients have an incidence of symptomatic VTE of 1% annually and postacute care patients have an incidence of 1.0% to 2.4% during their stay at the facility. These data offer some indirect support for prophylaxis of immobile patients in postacute or subacute care facilities, as their incidence of VTE may be similar to that of acutely ill hospitalized patients. Randomized trials are needed to determine if the benefi ts of anticoagulant thromboprophylaxis outweigh the risks in this population.
Recommendation
5.1. In chronically immobilized persons resid-ing at home or at a nursing home, we suggest against the routine use of thromboprophylaxis (Grade 2C) .
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e218S Prevention of VTE in Nonsurgical Patients
or trauma, active malignancy, pregnancy, estro-gen use, advanced age, limited mobility, severe obesity, or known thrombophilic disorder), we suggest frequent ambulation, calf muscle exercise or sitting in an aisle seat if feasible (Grade 2C) .
6.1.2. For long-distance travelers at increased risk of VTE (including previous VTE, recent surgery or trauma, active malignancy, preg-nancy, estrogen use, advanced age, limited mobility, severe obesity, or known thrombophilic disorder), we suggest use of properly fi tted, below-knee GCS providing 15 to 30 mm Hg of pressure at the ankle stockings during travel (Grade 2C) . For all other long-distance travelers, we suggest against the use of GCS (Grade 2C) .
6.1.3. For long-distance travelers, we suggest against the use of aspirin or anticoagulants to prevent VTE (Grade 2C) .
7.0 Thromboprophylaxis to Prevent VTE in Asymptomatic Persons
With Thrombophilia
7.1 Risk of VTE
Thrombophilia refers to inherited or acquired con-ditions, measurable in the blood, that are associated with an increased risk of developing venous throm-bosis. Inherited conditions include factor V Leiden (R506Q) mutation (average population prevalence, 5%; RR of a fi rst venous thrombosis, compared with the general population, 5-7), prothrombin gene (G20210A) mutation (2%; RR, 2-3), antithrombin defi ciency (0.04%; RR, 15-20), protein C defi ciency (0.3%; RR, 15-20), and protein S defi ciency (0.3%; RR, 15-20). Acquired thrombophilic conditions include antiphospholipid antibodies (APLA) (1%-5.6%; RR, 3-10), 9,152 which may be associated with both venous and arterial thrombosis.
Thrombophilia is most often tested for and detected in patients who have been diagnosed with VTE. However, in some situations, asymptomatic persons (ie, without a previous history of VTE) may undergo testing for thrombophilia for reasons potentially related (eg, family member had VTE) or unrelated (eg, as part of a workup for autoim-mune disease) to risk of VTE. The absolute annual incidence of VTE in asymptomatic persons with thrombophilia who are relatives of probands with VTE is low, ranging from 0.1% per year for carriers of factor V Leiden, to 1.7% per year for those with antithrombin defi ciency or mixed thrombophilic defects. 153,154
A pertinent clinical question is whether long-term antithrombotic therapy should be offered to such
was no evidence presented suggesting falsifi cation of data, we include discussion of these trials in this article.
A meta-analysis of the above trials found that among nine randomized trials, 142 the use of various brands of below-knee GCS (providing 15-30 mm Hg compression at the ankle) reduced the rate of asymp-tomatic DVT detected by screening from 3.6% (47 of 1,323 control subjects) to 0.2% (three of 1,314 stocking users) (RR, 0.10; 95% CI, 0.04-0.25); abso-lute estimated effects in a low-risk population were 4.5 fewer symptomatic DVT per 10,000 (95% CI, from four fewer to fi ve fewer) and 24 fewer PE per 1,000,000 (95% CI, from 20 fewer to 26 fewer), and in a high-risk population, 16.2 fewer symptomatic DVT per 10,000 (95% CI, from 14 fewer to 17.5 fewer) and 87 fewer PE per 1,000,000 (95% CI, from 76 fewer to 94 fewer) ( Table 20 , Table S26). Among eight trials that reported superfi cial throm-bophlebitis as an end point, results failed to show or exclude a benefi cial or detrimental effect of stockings (RR, 0.45; 95% CI, 0.18-1.13). Stockings reduced postfl ight leg edema in six trials in which this out-come was assessed; however, lack of blinding and use of unvalidated measures of edema reduce con-fi dence in this result.
In a small study of high-dose enoxaparin (1 mg/kg), administered once 2 to 4 h before travel lasting 7 to 8 h, vs aspirin, one dose daily for 3 days starting 12 h before the beginning of the fl ight, vs control, there were zero of 82, three of 84, and four of 83 asymp-tomatic DVT in the three groups, respectively, but no symptomatic DVT or PE events in any group, although follow-up ended after the subjects left the airport. 149
In summary, symptomatic VTE is rare in passen-gers returning from long fl ights. Travelers at increased risk of VTE, defi ned as persons with previous VTE, thrombophilic disorders, severe obesity, recently active cancer, or recent major surgery, who are trav-eling on fl ights . 6 h, may want to consider reducing their risk of VTE by frequent ambulation or sitting in an aisle seat if feasible and avoiding dehydration, although these measures have not been assessed in clinical trials. Light compression stockings appear to have a protective effect in reducing asymptomatic DVT in travelers, are inexpensive, and are unlikely to cause harm. Until further, methodologically appro-priate studies are available, decisions regarding phar-macologic thromboprophylaxis for travelers who are considered to be at particularly high risk for VTE must be made on an individual basis, considering that adverse effects may outweigh any benefi t.
Recommendations
6.1.1. For long-distance travelers at increased risk of VTE (including previous VTE, recent surgery
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
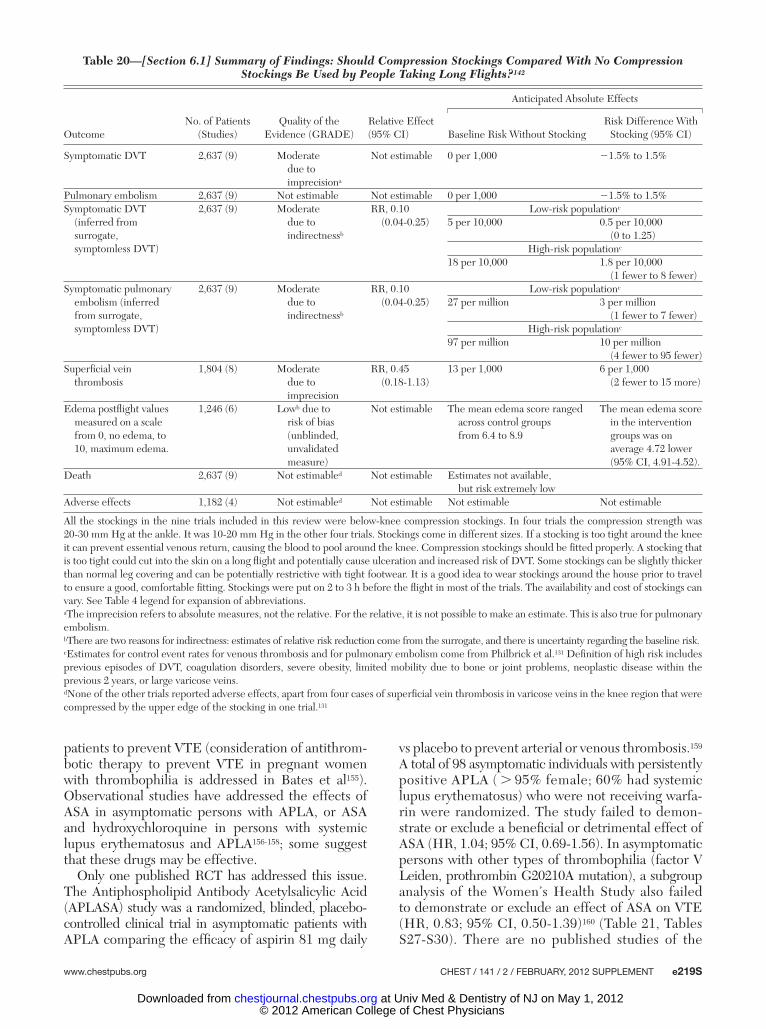
www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e219S
vs placebo to prevent arterial or venous thrombosis. 159 A total of 98 asymptomatic individuals with persistently positive APLA ( . 95% female; 60% had systemic lupus erythematosus) who were not receiving warfa-rin were randomized. The study failed to demon-strate or exclude a benefi cial or detrimental effect of ASA (HR, 1.04; 95% CI, 0.69-1.56). In asymptomatic persons with other types of thrombophilia (factor V Leiden, prothrombin G20210A mutation), a subgroup analysis of the Women’s Health Study also failed to demonstrate or exclude an effect of ASA on VTE (HR, 0.83; 95% CI, 0.50-1.39) 160 ( Table 21 , Tables S27-S30). There are no published studies of the
patients to prevent VTE (consideration of antithrom-botic therapy to prevent VTE in pregnant women with thrombophilia is addressed in Bates et al 155 ). Observational studies have addressed the effects of ASA in asymptomatic persons with APLA, or ASA and hydroxychloroquine in persons with systemic lupus erythematosus and APLA 156-158 ; some suggest that these drugs may be effective.
Only one published RCT has addressed this issue. The Antiphospholipid Antibody Acetylsalicylic Acid (APLASA) study was a randomized, blinded, placebo-controlled clinical trial in asymptomatic patients with APLA comparing the effi cacy of aspirin 81 mg daily
Table 20—[Section 6.1] Summary of Findings: Should Compression Stockings Compared With No Compression Stockings Be Used by People Taking Long Flights?142
OutcomeNo. of Patients
(Studies)Quality of the
Evidence (GRADE)Relative Effect (95% CI)
Anticipated Absolute Effects
Baseline Risk Without StockingRisk Difference With
Stocking (95% CI)
Symptomatic DVT 2,637 (9) Moderate due to imprecisiona
Not estimable 0 per 1,000 21.5% to 1.5%
Pulmonary embolism 2,637 (9) Not estimable Not estimable 0 per 1,000 21.5% to 1.5%Symptomatic DVT
(inferred from surrogate, symptomless DVT)
2,637 (9) Moderate due to indirectnessb
RR, 0.10 (0.04-0.25)
Low-risk populationc
5 per 10,000 0.5 per 10,000 (0 to 1.25)
High-risk populationc
18 per 10,000 1.8 per 10,000 (1 fewer to 8 fewer)
Symptomatic pulmonary embolism (inferred from surrogate, symptomless DVT)
2,637 (9) Moderate due to indirectnessb
RR, 0.10 (0.04-0.25)
Low-risk populationc
27 per million 3 per million (1 fewer to 7 fewer)
High-risk populationc
97 per million 10 per million (4 fewer to 95 fewer)
Superfi cial vein thrombosis
1,804 (8) Moderate due to imprecision
RR, 0.45 (0.18-1.13)
13 per 1,000 6 per 1,000 (2 fewer to 15 more)
Edema postfl ight values measured on a scale from 0, no edema, to 10, maximum edema.
1,246 (6) Lowb due to risk of bias (unblinded, unvalidated measure)
Not estimable The mean edema score ranged across control groups from 6.4 to 8.9
The mean edema score in the intervention groups was on average 4.72 lower (95% CI, 4.91-4.52).
Death 2,637 (9) Not estimabled Not estimable Estimates not available, but risk extremely low
Adverse effects 1,182 (4) Not estimabled Not estimable Not estimable Not estimable
All the stockings in the nine trials included in this review were below-knee compression stockings. In four trials the compression strength was 20-30 mm Hg at the ankle. It was 10-20 mm Hg in the other four trials. Stockings come in different sizes. If a stocking is too tight around the knee it can prevent essential venous return, causing the blood to pool around the knee. Compression stockings should be fi tted properly. A stocking that is too tight could cut into the skin on a long fl ight and potentially cause ulceration and increased risk of DVT. Some stockings can be slightly thicker than normal leg covering and can be potentially restrictive with tight footwear. It is a good idea to wear stockings around the house prior to travel to ensure a good, comfortable fi tting. Stockings were put on 2 to 3 h before the fl ight in most of the trials. The availability and cost of stockings can vary. See Table 4 legend for expansion of abbreviations.aThe imprecision refers to absolute measures, not the relative. For the relative, it is not possible to make an estimate. This is also true for pulmonary embolism.bThere are two reasons for indirectness: estimates of relative risk reduction come from the surrogate, and there is uncertainty regarding the baseline risk.cEstimates for control event rates for venous thrombosis and for pulmonary embolism come from Philbrick et al.131 Defi nition of high risk includes previous episodes of DVT, coagulation disorders, severe obesity, limited mobility due to bone or joint problems, neoplastic disease within the previous 2 years, or large varicose veins.dNone of the other trials reported adverse effects, apart from four cases of superfi cial vein thrombosis in varicose veins in the knee region that were compressed by the upper edge of the stocking in one trial.131
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e220S Prevention of VTE in Nonsurgical Patients
VTE in three prospective cohort studies, six case-control studies, and one clinical trial (Tables S31, S32). Considering DVT and PE together, the pooled risk estimate with statin use vs nonuse from several case-control studies 162-166 was 0.61 (95% CI, 0.48-0.81). Two observational studies based on administrative data 166,167 reported no signifi cant difference in the adjusted OR of VTE comparing statin users and nonusers. In contrast, another observational study 168 reported a lower risk of DVT with statin use, with an RR of 0.78 (95% CI, 0.69-0.87). The Heart and Estro-gen/Progestin Replacement (HERS) clinical trial 169 of women with coronary artery disease also reported a lower risk of VTE with statin use (not randomized) in women (HR, 0.45; 95% CI, 0.23-0.88).
A single RCT comparing statin to placebo reported a lower risk of VTE with the statin. 170 The Justifi ca-tion for the Use of Statins in Primary Prevention: an Intervention Trial Using Rosuvastatin (JUPITER) was designed to assess the effi cacy of rosuvastatin in preventing arterial vascular events in those not other-wise eligible for statins based on existing guidelines. Thus, it included a large sample of healthy people with low-density lipoprotein cholesterol , 130 mg/dL and C-reactive protein . 2 mg/L, without diabetes
effectiveness of thromboprophylaxis in asymptom-atic persons with thrombophilia types other than APLA, factor V Leiden, or prothrombin mutation, and no studies of anticoagulants such as LMWH, UFH, or VKA, or of mechanical thromboprophy-laxis such as GCS to prevent VTE in asymptomatic persons with thrombophilia.
Recommendation
7.1. In persons with asymptomatic thrombo-philia (ie, without a previous history of VTE), we recommend against the long-term daily use of mechanical or pharmacologic thrombopro-phylaxis to prevent VTE (Grade 1C) .
8.0 Statins to Prevent VTE in Asymptomatic Persons
8.1 Risk of VTE
Statins reduce coagulation potential by decreasing tissue factor expression and decreasing thrombin generation, 161 leading to consideration of statin use to prevent VTE. Statin use has been related to risk of
Table 21—[Section 7.1] Summary of Findings: Should Aspirin vs No Treatment Be Used for Prevention of VTE in Persons With Asymptomatic Thrombophilia?157-160
OutcomeNo. of Patients
(Studies) Follow-upQuality of the
Evidence (GRADE)
Relative Effect (95%
CI)
Anticipated Absolute Effects
Baseline RiskRisk Difference With
Aspirin (95% CI)
Symptomatic nonfatal DVT and PE
98 (2 RCTs) 2.3-10.1 y Low due to very serious imprecisiona
RR, 2.08 (0.20-22.23)
20 per 1,000 22 more per 1,000 (from 16 fewer to 425 more)
Mortality 98 (1 RCT) 2.3 y Very low due to very serious imprecisiona and methodologic limitationsb
RR, 1.04 (0.07-16.19)
21 per 1,000 1 more per 1,000 (from 19 fewer to 316 more)
Major bleeding 207 (3 Observational studies) 2.3-8 y
Very low due to very serious imprecisiona
Not estimable, no events in either arm
0 per 1,000 Not estimable
See Table 1 and 4 legends for expansion of abbreviations.aVery small number of events.bErkan et al159 terminated early as event rates were lower than expected and larger sample size was infeasible.
Table 22—[Section 8.1] Summary of Findings: Should Statins Be Used to Prevent VTE?170
OutcomeNo. of Patients
(Studies) Follow-upQuality of the
Evidence (GRADE) Relative Effect (95% CI)
Anticipated Absolute Effects
Baseline RiskRisk Difference With
Statins (95% CI)
Symptomatic DVT 17,802 (1 RCT) 1.9 y
High HR, 0.45 (0.25-0.79) 4 per 1,000 2 fewer per 1,000 (from 1 fewer to 3 fewer)
Nonfatal PE 17,802 (1 RCT) 1.9 y
High HR, 0.77 (0.41-1.45) 2 per 1,000 0 fewer per 1,000 (from 1 fewer to 1 more)
See Table 1 and 2 legends for expansion of abbreviations.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e221S
panies/orga nizations whose products or services may be dis-cussed in this article . Role of sponsors: The sponsors played no role in the develop-ment of these guidelines. Sponsoring organizations cannot recom-mend panelists or topics, nor are they allowed prepublication access to the manuscripts and recommendations. Guideline panel members, including the chair, and members of the Health & Sci-ence Policy Committee are blinded to the funding sources. Fur-ther details on the Confl ict of Interest Policy are available online at http://chestnet.org. Endorsements: This guideline is endorsed by the American Association for Clinical Chemistry, the American College of Clin-ical Pharmacy, the American Society of Health-System Pharma-cists, the American Society of Hematology, and the International Society of Thrombosis and Hematosis. Additional information: The supplemental Tables can be found in the Online Data Supplement at http://chestjournal.chestpubs.org/content/141/2_suppl/e195S/suppl/DC1.
References 1. Gould MK, Garcia DA, Wren SM, et al. Prevention of VTE
in nonorthopedic surgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2)(suppl):e227S-e277S.
2. Lansberg MG, O’Donnell MJ, Khatri P, et al. Antithrom-botic and thrombolytic therapy for ischemic stroke: anti-thrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2)(suppl):e601S-e636S.
3. Guyatt GH, Norris SL, Schulman S, et al. Methodology for the development of antithrombotic therapy and prevention of thrombosis guidelines: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physi-cians evidence-based clinical practice guidelines. Chest. 2012;141(2)(suppl):53S-70S.
4. MacLean S , Mulla S , Akl EA , et al . Patient values and pref-erences in decision making for antithrombotic therapy: a systematic review: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evi-dence-based clinical practice guidelines. Chest. 2012;141(2)(suppl):e1S-e23S.
5 . Cohen AT , Aikman R , Arcelus JI , et al . Assessment of venous thromboembolism risk and the benefi ts of thrombo-prophylaxis in medical patients . Thromb Haemost . 2005 ; 94 ( 4 ): 750 - 759 .
6 . Spyropoulos AC . Risk assessment of venous thromboembo-lism in hospitalized medical patients . Curr Opin Pulm Med . 2010 ; 16 ( 5 ): 419 - 425 .
7 . Spyropoulos AC , Anderson FA Jr , Fitzgerald G , et al . Predictive and associative models to identify hospitalized medical patients at risk for venous thromboembolism . Chest . 2011 ;140(3):706-714.
8 . Kucher N , Koo S , Quiroz R , et al . Electronic alerts to pre-vent venous thromboembolism among hospitalized patients . N Engl J Med . 2005 ; 352 ( 10 ): 969 - 977 .
9 . Barbar S , Noventa F , Rossetto V , et al . A risk assessment model for the identifi cation of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score . J Thromb Haemost . 2010 ; 8 ( 11 ): 2450 - 2457 .
10 . Decousus H , Tapson VF , Bergmann JF , et al ; IMPROVE Investigators . Factors at admission associated with bleeding risk in medical patients: fi ndings from the IMPROVE inves-tigators . Chest . 2011 ; 139 ( 1 ): 69 - 79 .
11 . Shorr AF , Williams MD . Venous thromboembolism in crit-ically ill patients. Observations from a randomized trial in sepsis . Thromb Haemost . 2009 ; 101 ( 1 ): 139 - 144 .
and other conditions. Considering symptomatic VTE, a secondary end point of the trial, assignment to the statin was associated with a 55% lower DVT risk and 23% lower PE risk. There was no increased risk of bleeding. The absolute rates of VTE were 2 per 1,000 in statin users compared with 4 per 1,000 in nonus-ers. The number needed to treat to prevent one DVT was 500 ( Table 22 , Table S33).
The panel considered that it was premature to issue a recommendation concerning the use of statins to prevent VTE in light of the paucity of data and the availability of more established effective treat-ments. In addition, the patients included in this trial were not at increased risk of thrombosis and are not the patients for whom thromboprophylaxis would be recommended.
This area is in need of further research. Trials that enroll patients at high risk of VTE (eg, those with previous VTE) who require thromboprophylaxis are needed. Such trials should have a comparative effec-tiveness design to better inform guideline developers; to that extent, these trials should have an active treat-ment of comparison, focus on symptomatic events that matter the most to patients, and report cost effec-tiveness analyses.
Acknowledgments Author contributions : As Topic Editor, Dr Murad oversaw the development of this article, including the data analysis and subse-quent development of the recommendations contained herein. Dr Murad: contributed as Topic Editor. Dr Kahn: contributed as Deputy Editor. Dr Lim: contributed as a panelist. Dr Dunn: contributed as a panelist. Dr Cushman: contributed as a panelist. Dr Dentali: contributed as a panelist. Dr Akl: contributed as a panelist. Dr Cook: contributed as a panelist. Dr Balekian: contributed as a resource consultant. Dr Klein: contributed as a frontline clinician. Dr Le: contributed as a frontline clinician. Dr Schulman: contributed as a panelist. Financial/nonfi nancial disclosures: The authors of this guide-line provided detailed confl ict of interest information related to each individual recommendation made in this article. A grid of these disclosures is available online at http://chestjournal.chestpubs.org/content/141/2_suppl/e195S/suppl/DC1. In summary, the authors have reported to CHEST the following confl icts of interest: Dr Kahn has received peer-reviewed and investigator-initi-ated industry research funding for projects related to venous thrombosis and postthrombotic syndrome prevention and treat-ment. She has received honoraria for industry-sponsored talks per-taining to venous thrombosis. Dr Balekian received industry research support and served as a consultant in areas relating to venous thrombosis. Dr Cook has received donated study drug (dalteparin) from Pfi zer for a Canadian government-funded trial of thrombo-prophylaxis in the ICU. Dr Cushman is the mentor on a mentored research grant from the Hemophilia and Thrombosis Research Society that is studying risk factors for venous thrombosis among medical inpatients, 2009-2011. No specifi c dollar amount goes toward her salary. Dr Akl is a prominent contributor to the GRADE Working Group. Dr Murad is a member of the GRADE Working Group. Drs Lim, Dunn, Dentali, Klein, Le, and Schulman have reported that no potential confl icts of interest exist with any com-
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e222S Prevention of VTE in Nonsurgical Patients
12. The PROTECT Investigators for the Canadian Critical Care Trials Group and the Australian and New Zealand Intensive Care Society Clinical Trials Group . Dalteparin versus unfractionated heparin in critically ill patients. N Engl J Med . 2011;364(14):1305-1314.
13 . Cook D , Attia J , Weaver B , McDonald E , Meade M , Crowther M . Venous thromboembolic disease: an observa-tional study in medical-surgical intensive care unit patients . J Crit Care . 2000 ; 15 ( 4 ): 127 - 132 .
14 . Lentine KL , Flavin KE , Gould MK . Variability in the use of thromboprophylaxis and outcomes in critically ill medical patients . Am J Med . 2005 ; 118 ( 12 ): 1373 - 1380 .
15 . Muscedere JG , Heyland DK , Cook D . Venous thromboem-bolism in critical illness in a community intensive care unit . J Crit Care . 2007 ; 22 ( 4 ): 285 - 289 .
16 . Heit JA , Silverstein MD , Mohr DN , Petterson TM , O’Fallon WM , Melton LJ III . Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study . Arch Intern Med . 2000 ; 160 ( 6 ): 809 - 815 .
17 . Heit JA , O’Fallon WM , Petterson TM , et al . Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study . Arch Intern Med . 2002 ; 162 ( 11 ): 1245 - 1248 .
18 . Spencer FA , Lessard D , Emery C , Reed G , Goldberg RJ . Venous thromboembolism in the outpatient setting . Arch Intern Med . 2007 ; 167 ( 14 ): 1471 - 1475 .
19 . Goldhaber SZ , Dunn K , MacDougall RC . New onset of venous thromboembolism among hospitalized patients at Brigham and Women’s Hospital is caused more often by prophylaxis failure than by withholding treatment . Chest . 2000 ; 118 ( 6 ): 1680 - 1684 .
20 . Alikhan R , Cohen AT , Combe S , et al ; MEDENOX Study . Risk factors for venous thromboembolism in hos-pitalized patients with acute medical illness: analysis of the MEDENOX Study . Arch Intern Med . 2004 ; 164 ( 9 ): 963 - 968 .
21 . Anderson FA Jr , Spencer FA . Risk factors for venous throm-boembolism . Circulation . 2003 ; 107 ( 23 suppl 1 ): I9 - I16 .
22 . Lijfering WM , Rosendaal FR , Cannegieter SC . Risk fac-tors for venous thrombosis - current understanding from an epidemiological point of view . Br J Haematol . 2010 ; 149 ( 6 ): 824 - 833 .
23 . Alikhan R , Cohen AT . Heparin for the prevention of venous thromboembolism in general medical patients (excluding stroke and myocardial infarction) . Cochrane Database Syst Rev . 2009 ;( 3 ): CD003747 .
24 . Dentali F , Douketis JD , Gianni M , Lim W , Crowther MA . Meta-analysis: anticoagulant prophylaxis to prevent symp-tomatic venous thromboembolism in hospitalized medical patients . Ann Intern Med . 2007 ; 146 ( 4 ): 278 - 288 .
25 . Lloyd NS , Douketis JD , Moinuddin I , Lim W , Crowther MA . Anticoagulant prophylaxis to prevent asymptomatic deep vein thrombosis in hospitalized medical patients: a sys-tematic review and meta-analysis . J Thromb Haemost . 2008 ; 6 ( 3 ): 405 - 414 .
26 . Bergmann JF , Neuhart E ; The Enoxaparin in Medicine Study Group . A multicenter randomized double-blind study of enoxaparin compared with unfractionated heparin in the prevention of venous thromboembolic disease in elderly in-patients bedridden for an acute medical illness . Thromb Haemost . 1996 ; 76 ( 4 ): 529 - 534 .
27 . Forette B , Wolmark Y . Calcium nadroparin in the preven-tion of thromboembolic disease in elderly subjects. Study of tolerance [in French] . Presse Med . 1995 ; 24 ( 12 ): 567 - 571 .
28 . Kleber FX , Witt C , Vogel G , Koppenhagen K , Schomaker U , Flosbach CW ; THE-PRINCE Study Group . Randomized comparison of enoxaparin with unfractionated heparin
for the prevention of venous thromboembolism in med-ical patients with heart failure or severe respiratory disease . Am Heart J . 2003 ; 145 ( 4 ): 614 - 621 .
29 . Lechler E , Schramm W , Flosbach CW ; The Prime Study Group . The venous thrombotic risk in nonsurgical patients: epidemiological data and effi cacy/safety profi le of a low-molecular-weight heparin (enoxaparin) . Haemostasis . 1996 ; 26 ( suppl 2 ): 49 - 56 .
30 . Riess H , Haas S , Tebbe U , et al . A randomized, double-blind study of certoparin versus unfractionated heparin to prevent venous thromboembolic events in acutely ill, non-surgical patients: CERTIFY study . J Thromb Haemost . 2010 ; 8 (6): 1209 - 1215 .
31 . Tapson VF , Decousus H , Pini M , et al ; IMPROVE Inves-tigators . Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: fi ndings from the International Medical Prevention Registry on Venous Thromboembolism . Chest . 2007 ; 132 ( 3 ): 936 - 945 .
32. Phung OJ , Kahn SR , Cook DJ , Murad MH. Dosing fre-quency of unfractionated heparin thromboprophylaxis: A meta-analysis. Chest. 2011;140(2):374-381.
33. Pechevis M , Detournay B , Pribil C , et al. Economic evalua-tion of enoxaparin vs. placebo for the prevention of venous thromboembolism in acutely ill medical patients. Value Health . 2000 ;3(6):389-396.
34. Nuijten MJ , Villar FA , Kosa J , et al. Cost-effectiveness of enoxaparin as thromboprophylaxis in acutely ill medical patients in Spain. Value Health . 2003 ;6(2):126-136.
35 . Lamy A , Wang X , Kent R , Smith KM , Gafni A . Economic evaluation of the MEDENOX trial: a Canadian perspec-tive. Medical Patients with Enoxaparin . Can Respir J . 2002 ; 9 ( 3 ): 169 - 177 .
36 . Pineo GF , Hull RD . Economic and practical aspects of thromboprophylaxis with unfractionated and low-molecular-weight heparins in hospitalized medical patients . Clin Appl Thromb Hemost . 2009 ; 15 ( 5 ): 489 - 500 .
37 . Leykum L , Pugh J , Diuguid D , Papadopoulos K . Cost utility of substituting enoxaparin for unfractionated heparin for prophylaxis of venous thrombosis in the hospitalized med-ical patient . J Hosp Med . 2006 ; 1 ( 3 ): 168 - 176 .
38 . Lloyd A , Anderson P , Quinlan D , et al . Economic evaluation of the use of enoxaparin for thromboprophylaxis in acutely ill medical patients . J Med Econ . 2001 ; 4 (1-4): 99 - 113 .
39 . McGarry LJ , Thompson D , Weinstein MC , Goldhaber SZ . Cost effectiveness of thromboprophylaxis with a low-molecular-weight heparin versus unfractionated heparin in acutely ill medical inpatients . Am J Manag Care . 2004 ; 10 ( 9 ): 632 - 642 .
40 . Offord R , Lloyd AC , Anderson P , Bearne A . Economic eval-uation of enoxaparin for the prevention of venous thrombo-embolism in acutely ill medical patients . Pharm World Sci . 2004 ; 26 ( 4 ): 214 - 220 .
41 . Shorr AF , Jackson WL , Weiss BM , Moores LK . Low-molecular weight heparin for deep vein thrombosis pro-phylaxis in hospitalized medical patients: results from a cost-effectiveness analysis . Blood Coagul Fibrinolysis . 2007 ; 18 ( 4 ): 309 - 316 .
42 . Samama MM , Cohen AT , Darmon JY , et al ; Prophylaxis in Medical Patients with Enoxaparin Study Group . A compar-ison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients . N Engl J Med . 1999 ; 341 ( 11 ): 793 - 800 .
43 . Morris TA , Castrejon S , Devendra G , Gamst AC . No differ-ence in risk for thrombocytopenia during treatment of pul-monary embolism and deep venous thrombosis with either low-molecular-weight heparin or unfractionated heparin: a metaanalysis . Chest . 2007 ; 132 ( 4 ): 1131 - 1139 .
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e223S
44 . Benkö T , Cooke EA , McNally MA , Mollan RA . Graduated compression stockings: knee length or thigh length . Clin Orthop Relat Res . 2001 ; 383 ( 383 ): 197 - 203 .
45 . Kierkegaard A , Norgren L . Graduated compression stock-ings in the prevention of deep vein thrombosis in patients with acute myocardial infarction . Eur Heart J . 1993 ; 14 ( 10 ): 1365 - 1368 .
46 . Dennis M , Sandercock PA , Reid J , et al ; CLOTS Trials Collaboration . Effectiveness of thigh-length graduated com-pression stockings to reduce the risk of deep vein thrombo-sis after stroke (CLOTS trial 1): a multicentre, randomised controlled trial . Lancet . 2009 ; 373 ( 9679 ): 1958 - 1965 .
47 . Muir KW , Watt A , Baxter G , Grosset DG , Lees KR . Ran-domized trial of graded compression stockings for pre-vention of deep-vein thrombosis after acute stroke . QJM . 2000 ; 93 ( 6 ): 359 - 364 .
48. CLOTS (Clots in Legs Or sTockings after Stroke) Trial Collaboration. Thigh-length versus below-knee stockings for deep venous thrombosis prophylaxis after stroke: a ran-domized trial. Ann Intern Med . 2010 ;153(9):553-562.
49. Kearon C , O’Donnell M. Should patients with stroke wear compression stockings to prevent venous thromboembo-lism? Ann Intern Med . 2010 ;153(9):610-611.
50. Roderick P , Ferris G , Wilson K , et al. Towards evidence-based guidelines for the prevention of venous thrombo-embolism: systematic reviews of mechanical methods, oral anticoagulation, dextran and regional anaesthesia as throm-boprophylaxis. Health Technol Assess . 2005 ;9(49): 1-78.
51 . Eppsteiner RW , Shin JJ , Johnson J , van Dam RM . Mechanical compression versus subcutaneous heparin therapy in post-operative and posttrauma patients: a systematic review and meta-analysis . World J Surg . 2010 ; 34 ( 1 ): 10 - 19 .
52 . Comerota AJ , Katz ML , White JV . Why does prophylaxis with external pneumatic compression for deep vein throm-bosis fail? Am J Surg . 1992 ; 164 ( 3 ): 265 - 268 .
53 . Cornwell EE III , Chang D , Velmahos G , et al . Compliance with sequential compression device prophylaxis in at-risk trauma patients: a prospective analysis . Am Surg . 2002 ; 68 ( 5 ): 470 - 473 .
54 . Murakami M , McDill TL , Cindrick-Pounds L , et al . Deep venous thrombosis prophylaxis in trauma: improved com-pliance with a novel miniaturized pneumatic compression device. J Vasc Surg . 2003 ;38(5):923-927.
55. Falck-Ytter Y, Francis CW, Johanson NA, et al. Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guide-lines. Chest. 2012;141(2)(suppl):e278S-e325S.
56 . Hull RD , Schellong SM , Tapson VF , et al ; EXCLAIM (Extended Prophylaxis for Venous ThromboEmbolism in Acutely Ill Medical Patients With Prolonged Immobilization) study . Extended-duration venous thromboembolism pro-phylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial . Ann Intern Med . 2010 ; 153 ( 1 ): 8 - 18 .
57 . Antiplatelet Trialists’ Collaboration . Collaborative overview of randomised trials of antiplatelet therapy—III: Reduction in venous thrombosis and pulmonary embolism by anti-platelet prophylaxis among surgical and medical patients. Antiplatelet Trialists’ Collaboration . BMJ . 1994 ; 308 ( 6923 ): 235 - 246 .
58 . Pulmonary Embolism Prevention (PEP) Trial Collaborative Group . Prevention of pulmonary embolism and deep vein thrombosis with low dose aspirin: Pulmonary Embolism Prevention (PEP) trial . Lancet . 2000 ; 355 ( 9212 ): 1295 - 1302 .
59 . Robinson KS , Anderson DR , Gross M , et al . Ultrasonographic screening before hospital discharge for deep venous throm-
bosis after arthroplasty: the post-arthroplasty screening study. A randomized, controlled trial . Ann Intern Med . 1997 ; 127 ( 6 ): 439 - 445 .
60. Furlan JC , Fehlings MG . Role of screening tests for deep venous thrombosis in asymptomatic adults with acute spi-nal cord injury: an evidence-based analysis. Spine (Phila Pa 1976) . 2007 ;32(17):1908-1916
61 . Cohen AT , Tapson VF , Bergmann JF , et al ; ENDORSE Investigators . Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multi-national cross-sectional study . Lancet . 2008 ; 371 ( 9610 ): 387 - 394 .
62 . Geerts WH , Bergqvist D , Pineo GF , et al ; American College of Chest Physicians . Prevention of venous thromboembo-lism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) . Chest . 2008 ; 133 ( 6 suppl ): 381S - 453S .
63 . Goldhaber SZ , Tapson VF ; DVT FREE Steering Committee . A prospective registry of 5,451 patients with ultrasound-confi rmed deep vein thrombosis . Am J Cardiol . 2004 ; 93 ( 2 ): 259 - 262 .
64 . Tooher R , Middleton P , Pham C , et al . A systematic review of strategies to improve prophylaxis for venous thromboem-bolism in hospitals . Ann Surg . 2005 ; 241 ( 3 ): 397 - 415 .
65 . Piazza G , Rosenbaum EJ , Pendergast W , et al . Physi-cian alerts to prevent symptomatic venous thromboembo-lism in hospitalized patients . Circulation . 2009 ; 119 ( 16 ): 2196 - 2201 .
66 . Schünemann HJ , Cook D , Grimshaw J , et al . Antithrombotic and thrombolytic therapy: from evidence to applica-tion: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy . Chest . 2004 ; 126 ( suppl 3 ): 688S - 696S .
67 . Cook D , Crowther M , Meade M , et al . Deep venous thrombosis in medical-surgical critically ill patients: preva-lence, incidence, and risk factors . Crit Care Med . 2005 ; 33 ( 7 ): 1565 - 1571 .
68 . Arnold DM , Donahoe L , Clarke FJ , et al . Bleeding during critical illness: a prospective cohort study using a new mea-surement tool . Clin Invest Med . 2007 ; 30 ( 2 ): E93 - E102 .
69 . Fraisse F , Holzapfel L , Couland JM , et al ; The Association of Non-University Affi liated Intensive Care Specialist Physi-cians of France . Nadroparin in the prevention of deep vein thrombosis in acute decompensated COPD . Am J Respir Crit Care Med . 2000 ; 161 ( 4 pt 1 ): 1109 - 1114 .
70 . Cook D , Douketis J , Meade M , et al ; Canadian Critical Care Trials Group . Venous thromboembolism and bleeding in critically ill patients with severe renal insuffi ciency receiving dalteparin thromboprophylaxis: prevalence, incidence and risk factors . Crit Care . 2008 ; 12 ( 2 ): R32 .
71 . Cade JF . High risk of the critically ill for venous throm-boembolism . Crit Care Med . 1982 ; 10 ( 7 ): 448 - 450 .
72 . De A , Roy P , Garg VK , Pandey NK . Low-molecular-weight heparin and unfractionated heparin in prophylaxis against deep vein thrombosis in critically ill patients undergoing major surgery . Blood Coagul Fibrinolysis . 2010 ; 21 ( 1 ): 57 - 61 .
73 . Kakkos SK , Caprini JA , Geroulakos G , Nicolaides AN , Stansby GP , Reddy DJ . Combined intermittent pneumatic leg compression and pharmacological prophylaxis for pre-vention of venous thromboembolism in high-risk patients . Cochrane Database Syst Rev . 2008 ;( 4 ): CD005258 .
74. Blom JW , Doggen CJ , Osanto S , Rosendaal FR . Malignancies, prothrombotic mutations, and the risk of venous thrombo-sis. JAMA . 2005 ;293(6):715-722.
75. Alcalay A , Wun T , Khatri V , et al. Venous thromboembolism in patients with colorectal cancer: incidence and effect on survival. J Clin Oncol . 2006 ;24(7):1112-1118.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

e224S Prevention of VTE in Nonsurgical Patients
76 . Chew HK , Wun T , Harvey D , Zhou H , White RH . Incidence of venous thromboembolism and its effect on survival among patients with common cancers . Arch Intern Med . 2006 ; 166 ( 4 ): 458 - 464 .
77 . Sørensen HT , Mellemkjaer L , Olsen JH , Baron JA . Prognosis of cancers associated with venous thromboembolism . N Engl J Med . 2000 ; 343 ( 25 ): 1846 - 1850 .
78 . Falanga A , Donati MB . Pathogenesis of thrombosis in patients with malignancy . Int J Hematol . 2001 ; 73 ( 2 ): 137 - 144 .
79 . Blom JW , Vanderschoot JP , Oostindiër MJ , Osanto S , van der Meer FJ , Rosendaal FR . Incidence of venous throm-bosis in a large cohort of 66,329 cancer patients: results of a record linkage study . J Thromb Haemost . 2006 ; 4 ( 3 ): 529 - 535 .
80 . Fisher B , Costantino J , Redmond C , et al . A randomized clin-ical trial evaluating tamoxifen in the treatment of patients with node-negative breast cancer who have estrogen-receptor-positive tumors . N Engl J Med . 1989 ; 320 ( 8 ): 479 - 484 .
81 . Fisher B , Costantino JP , Wickerham DL , et al . Tamoxifen for prevention of breast cancer: report of the National Sur-gical Adjuvant Breast and Bowel Project P-1 Study . J Natl Cancer Inst . 1998 ; 90 ( 18 ): 1371 - 1388 .
82 . Haddad TC , Greeno EW . Chemotherapy-induced throm-bosis . Thromb Res . 2006 ; 118 ( 5 ): 555 - 568 .
83 . Khorana AA , Francis CW , Culakova E , Fisher RI , Kuderer NM , Lyman GH . Thromboembolism in hospitalized neutropenic cancer patients . J Clin Oncol . 2006 ; 24 ( 3 ): 484 - 490 .
84 . Khorana AA , Francis CW , Culakova E , Lyman GH . Risk factors for chemotherapy-associated venous thromboem-bolism in a prospective observational study . Cancer . 2005 ; 104 ( 12 ): 2822 - 2829 .
85 . Lee AY , Levine MN . Venous thromboembolism and cancer: risks and outcomes . Circulation . 2003 ; 107 ( 23 suppl 1 ): I17 - I21 .
86 . Saphner T , Tormey DC , Gray R . Venous and arterial throm-bosis in patients who received adjuvant therapy for breast cancer. J Clin Oncol . 1991 ;9(2):286-294.
87 . Fisher B , Costantino JP , Wickerham DL , et al . Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study . J Natl Cancer Inst . 2005 ; 97 ( 22 ): 1652 - 1662 .
88 . Pritchard KI , Paterson AH , Paul NA , Zee B, Fine S, Pater J . Increased thromboembolic complications with concurrent tamoxifen and chemotherapy in a randomized trial of adju-vant therapy for women with breast cancer. National Cancer Institute of Canada Clinical Trials Group Breast Cancer Site Group. J Clin Oncol . 1996 ;14(10):2731-2737.
89 . Bonneterre J , Buzdar A , Nabholtz JM , et al ; Arimidex Writing Committee ; Investigators Committee Members . Anastrozole is superior to tamoxifen as fi rst-line therapy in hormone receptor positive advanced breast carcinoma . Cancer . 2001 ; 92 ( 9 ): 2247 - 2258 .
90 . Baum M , Budzar AU , Cuzick J , et al ; ATAC Trialists’ Group . Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: fi rst results of the ATAC randomised trial . Lancet . 2002 ; 359 ( 9324 ): 2131 - 2139 .
91 . Coombes RC , Hall E , Gibson LJ , et al ; Intergroup Exemestane Study . A randomized trial of exemestane after two to three years of tamoxifen therapy in postmenopausal women with pri-mary breast cancer . N Engl J Med . 2004 ; 350 ( 11 ): 1081 - 1092 .
92 . Thürlimann B , Keshaviah A , Coates AS , et al ; Breast International Group (BIG) 1-98 Collaborative Group . A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer . N Engl J Med . 2005 ; 353 ( 26 ): 2747 - 2757 .
93 . Johnson DH , Fehrenbacher L , Novotny WF , et al . Ran-domized phase II trial comparing bevacizumab plus carbo-platin and paclitaxel with carboplatin and paclitaxel alone
in previously untreated locally advanced or metastatic non-small-cell lung cancer . J Clin Oncol . 2004 ; 22 ( 11 ): 2184 - 2191 .
94 . Barlogie B , Tricot G , Anaissie E , et al . Thalidomide and hematopoietic-cell transplantation for multiple myeloma . N Engl J Med . 2006 ; 354 ( 10 ): 1021 - 1030 .
95 . Hussein MA . Thromboembolism risk reduction in multiple myeloma patients treated with immunomodulatory drug combinations . Thromb Haemost . 2006 ; 95 ( 6 ): 924 - 930 .
96 . El Accaoui RN , Shamseddeen WA , Taher AT . Thalidomide and thrombosis. A meta-analysis . Thromb Haemost . 2007 ; 97 ( 6 ): 1031 - 1036 .
97 . Palumbo A , Rus C , Zeldis JB , Rodeghiero F , Boccadoro M ; Italian Multiple Myeloma Network, Gimema . Enoxaparin or aspirin for the prevention of recurrent thromboembolism in newly diagnosed myeloma patients treated with melphalan and prednisone plus thalidomide or lenalidomide . J Thromb Haemost . 2006 ; 4 ( 8 ): 1842 - 1845 .
98 . Nalluri SR , Chu D , Keresztes R , Zhu X , Wu S . Risk of venous thromboembolism with the angiogenesis inhibitor bevacizumab in cancer patients: a meta-analysis . JAMA . 2008 ; 300 ( 19 ): 2277 - 2285 .
99 . Bona RD . Thrombotic complications of central venous catheters in cancer patients . Semin Thromb Hemost . 1999 ; 25 ( 2 ): 147 - 155 .
100 . Cunningham MS , White B , Hollywood D , O’Donnell J . Primary thromboprophylaxis for cancer patients with central venous catheters—a reappraisal of the evidence . Br J Cancer . 2006 ; 94 ( 2 ): 189 - 194 .
101 . Rosovsky RP , Kuter DJ . Catheter-related thrombosis in can-cer patients: pathophysiology, diagnosis, and management . Hematol Oncol Clin North Am . 2005 ; 19 ( 1 ): 183 - 202; vii .
102 . Akl EA , Gunukula S , Barba M , et al . Parenteral anticoagula-tion in patients with cancer who have no therapeutic or pro-phylactic indication for anticoagulation . Cochrane Database Syst Rev . 2011 ;(4): CD006652 .
103 . Sideras K , Schaefer PL , Okuno SH , et al . Low-molecular-weight heparin in patients with advanced cancer: a phase 3 clinical trial. Mayo Clin Proc . 2006 ; 81 (6): 758 - 767 .
104 . Altinbas M , Coskun HS , Er O , et al . A randomized clin-ical trial of combination chemotherapy with and without low-molecular-weight heparin in small cell lung cancer . J Thromb Haemost . 2004 ; 2 ( 8 ): 1266 - 1271 .
105 . Lebeau B , Chastang C , Brechot JM , et al . Subcutaneous heparin treatment increases survival in small cell lung can-cer. “Petites Cellules” Group . Cancer . 1994 ; 74 ( 1 ): 38 - 45 .
106 . Akl EA , Vasireddi SR , Gunukula S , et al . Oral antico-agulation in patients with cancer who have no therapeutic or prophylactic indication for anticoagulation . Cochrane Database Syst Rev . 2010 ;( 12 ): CD006466 .
107 . Randolph AG , Cook DJ , Gonzales CA , Andrew M . Benefi t of heparin in central venous and pulmonary artery cathe-ters: a meta-analysis of randomized controlled trials . Chest . 1998 ; 113 ( 1 ): 165 - 171 .
108 . Rooden CJ , Tesselaar ME , Osanto S , Rosendaal FR , Huisman MV . Deep vein thrombosis associated with cen-tral venous catheters—a review . J Thromb Haemost . 2005 ; 3 ( 11 ): 2409 - 2419 .
109 . Cheong K , Perry D , Karapetis C , Koczwara B . High rate of complications associated with peripherally inserted cen-tral venous catheters in patients with solid tumours . Intern Med J . 2004 ; 34 ( 5 ): 234 - 238 .
110 . Tesselaar ME , Ouwerkerk J , Nooy MA , Rosendaal FR , Osanto S . Risk factors for catheter-related thrombosis in cancer patients . Eur J Cancer . 2004 ; 40 ( 15 ): 2253 - 2259 .
111 . Cadman A , Lawrance JA , Fitzsimmons L , Spencer-Shaw A , Swindell R . To clot or not to clot? That is the question in central venous catheters . Clin Radiol . 2004 ; 59 ( 4 ): 349 - 355 .
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

www.chestpubs.org CHEST / 141 / 2 / FEBRUARY, 2012 SUPPLEMENT e225S
129 . Kesteven P , Robinson B . Incidence of symptomatic throm-bosis in a stable population of 650,000: travel and other risk factors . Aviat Space Environ Med . 2002 ; 73 ( 6 ): 593 - 596 .
130 . Cannegieter SC , Doggen CJ , van Houwelingen HC , Rosendaal FR . Travel-related venous thrombosis: results from a large population-based case control study (MEGA study) . PLoS Med . 2006 ; 3 ( 8 ): e307 .
131 . Philbrick JT , Shumate R , Siadaty MS , Becker DM . Air travel and venous thromboembolism: a systematic review . J Gen Intern Med . 2007 ; 22 ( 1 ): 107 - 114 .
132 . Schwarz T , Siegert G , Oettler W , et al . Venous thrombo-sis after long-haul fl ights . Arch Intern Med . 2003 ; 163 ( 22 ): 2759 - 2764 .
133 . ten Wolde M , Kraaijenhagen RA , Schiereck J , et al . Travel and the risk of symptomatic venous thromboembolism . Thromb Haemost . 2003 ; 89 ( 3 ): 499 - 505 .
134 . Schreijer AJ , Cannegieter SC , Doggen CJ , Rosendaal FR . The effect of fl ight-related behaviour on the risk of venous thrombosis after air travel . Br J Haematol . 2009 ; 144 ( 3 ): 425 - 429 .
135 . Arfvidsson B , Eklof B , Kistner RL , Masuda EM , Sato DT . Risk factors for venous thromboembolism following pro-longed air travel. Coach class thrombosis . Hematol Oncol Clin North Am . 2000 ; 14 ( 2 ): 391 - 400; ix .
136 . Martinelli I , Taioli E , Battaglioli T , et al . Risk of venous thromboembolism after air travel: interaction with throm-bophilia and oral contraceptives . Arch Intern Med . 2003 ; 163 ( 22 ): 2771 - 2774 .
137 . McQuillan AD , Eikelboom JW , Baker RI . Venous thrombo-embolism in travellers: can we identify those at risk? Blood Coagul Fibrinolysis . 2003 ; 14 ( 7 ): 671 - 675 .
138 . Paganin F , Bourdé A , Yvin JL , et al . Venous thromboem-bolism in passengers following a 12-h fl ight: a case-control study . Aviat Space Environ Med . 2003 ; 74 ( 12 ): 1277 - 1280 .
139 . Rege KP , Bevan DH , Chitolie A , Shannon MS . Risk fac-tors and thrombosis after airline fl ight . Thromb Haemost . 1999 ; 81 ( 6 ): 995 - 996 .
140 . Scurr JH , Machin SJ , Bailey-King S , Mackie IJ , McDonald S , Smith PD . Frequency and prevention of symptomless deep-vein thrombosis in long-haul fl ights: a randomised trial . Lancet . 2001 ; 357 ( 9267 ): 1485 - 1489 .
141 . Schreijer AJ , Cannegieter SC , Meijers JC , Middeldorp S , Büller HR , Rosendaal FR . Activation of coagulation sys tem during air travel: a crossover study . Lancet . 2006 ; 367 ( 9513 ): 832 - 838 .
142 . Clarke M , Hopewell S , Juszczak E , Eisinga A , Kjeldstrøm M . Compression stockings for preventing deep vein throm-bosis in airline passengers . Cochrane Database Syst Rev . 2006 ;( 2 ): CD004002 .
143 . Belcaro G , Cesarone MR , Nicolaides AN , et al . Prevention of venous thrombosis with elastic stockings during long-haul fl ights: the LONFLIT 5 JAP study . Clin Appl Thromb Hemost . 2003 ; 9 ( 3 ): 197 - 201 .
144 . Belcaro G , Cesarone MR , Rohdewald P , et al . Prevention of venous thrombosis and thrombophlebitis in long-haul fl ights with pycnogenol . Clin Appl Thromb Hemost . 2004 ; 10 ( 4 ): 373 - 377 .
145 . Belcaro G , Cesarone MR , Shah SS , et al . Prevention of edema, fl ight microangiopathy and venous thrombosis in long fl ights with elastic stockings. A randomized trial: The LONFLIT 4 Concorde Edema-SSL Study . Angiology . 2002 ; 53 ( 6 ): 635 - 645 .
146 . Belcaro G , Geroulakos G , Nicolaides AN , Myers KA , Winford M . Venous thromboembolism from air travel: the LONFLIT study . Angiology . 2001 ; 52 ( 6 ): 369 - 374 .
147 . Cesarone MR , Belcaro G , Errichi BM , et al . The LONFLIT4—Concorde Deep Venous Thrombosis and
112 . Lee AY , Levine MN , Butler G , et al . Incidence, risk fac-tors, and outcomes of catheter-related thrombosis in adult patients with cancer . J Clin Oncol . 2006 ; 24 ( 9 ): 1404 - 1408 .
113 . Verso M , Agnelli G , Kamphuisen PW , et al . Risk factors for upper limb deep vein thrombosis associated with the use of central vein catheter in cancer patients . Intern Emerg Med . 2008 ; 3 ( 2 ): 117 - 122 .
114 . Akl E , Vasireddi S , Gunukula S , et al . Anticoagulation for cancer patients with central venous catheters. Cochrane Database Syst Rev . 2011;(4):CD006468.
115 . Bosson JL , Pouchain D , Bergmann JF ; for the ETAPE Study Group . A prospective observational study of a cohort of outpatients with an acute medical event and reduced mobility: incidence of symptomatic thromboembolism and description of thromboprophylaxis practices . J Intern Med . 2006 ; 260 ( 2 ): 168 - 176 .
116 . Gomes JP , Shaheen WH , Truong SV , Brown EF , Beasley BW , Gajewski BJ . Incidence of venous thromboem-bolic events among nursing home residents . J Gen Intern Med . 2003 ; 18 ( 11 ): 934 - 936 .
117 . Liperoti R , Pedone C , Lapane KL , Mor V , Bernabei R , Gambassi G . Venous thromboembolism among elderly patients treated with atypical and conventional antipsychotic agents . Arch Intern Med . 2005 ; 165 ( 22 ): 2677 - 2682 .
118 . Scannapieco G , Ageno W , Airoldi A , et al ; TERSICORE Study Group . Incidence and predictors of venous thrombo-embolism in post-acute care patients. A prospective cohort study . Thromb Haemost . 2010 ; 104 ( 4 ): 734 - 740 .
119 . Bosson J-L , Labarere J , Sevestre MA , et al . Deep vein thrombosis in elderly patients hospitalized in subacute care facilities: a multicenter cross-sectional study of risk factors, prophylaxis, and prevalence . Arch Intern Med . 2003 ; 163 ( 21 ): 2613 - 2618 .
120 . Sellier E , Labarere J , Sevestre M-A , et al ; Association pour la Promotion de l’Angiologie Hospitalière . Risk factors for deep vein thrombosis in older patients: a multicenter study with systematic compression ultrasonography in postacute care facilities in France . J Am Geriatr Soc . 2008 ; 56 ( 2 ): 224 - 230 .
121 . Labarère J , Sevestre M-A , Belmin J , et al ; Association pour la Promotion de l’Angiologie Hospitalière . Low-molecular-weight heparin prophylaxis of deep vein thrombosis for older patients with restricted mobility: propensity analyses of data from two multicentre, cross-sectional studies . Drugs Aging . 2009 ; 26 ( 3 ): 263 - 271 .
122 . Chandra D , Parisini E , Mozaffarian D . Meta-analysis: travel and risk for venous thromboembolism . Ann Intern Med . 2009 ; 151 ( 3 ): 180 - 190 .
123 . Kuipers S , Schreijer AJ , Cannegieter SC , Büller HR , Rosendaal FR , Middeldorp S . Travel and venous thrombo-sis: a systematic review . J Intern Med . 2007 ; 262 ( 6 ): 615 - 634 .
124 . Kuipers S , Cannegieter SC , Middeldorp S , Robyn L , Büller HR , Rosendaal FR . The absolute risk of venous thrombosis after air travel: a cohort study of 8,755 employees of inter-national organisations . PLoS Med . 2007 ; 4 ( 9 ): e290 .
125 . Lapostolle F , Surget V , Borron SW , et al . Severe pulmo-nary embolism associated with air travel . N Engl J Med . 2001 ; 345 ( 11 ): 779 - 783 .
126 . Hughes RJ , Hopkins RJ , Hill S , et al . Frequency of venous thromboembolism in low to moderate risk long distance air travellers: the New Zealand Air Traveller’s Thrombosis (NZATT) study . Lancet . 2003 ; 362 ( 9401 ): 2039 - 2044 .
127 . Pérez-Rodríguez E , Jiménez D , Díaz G , et al . Incidence of air travel-related pulmonary embolism at the Madrid-Barajas airport . Arch Intern Med . 2003 ; 163 ( 22 ): 2766 - 2770 .
128 . Kraaijenhagen RA , Haverkamp D , Koopman MM , Prandoni P , Piovella F , Büller HR . Travel and risk of venous thrombosis . Lancet . 2000 ; 356 ( 9240 ): 1492 - 1493 .
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
e226S Prevention of VTE in Nonsurgical Patients
bolism: a randomized trial [Summary for patients in Ann Intern Med . 2007 Oct 16;147(8):I34; PMID: 17938386] . Ann Intern Med . 2007 ; 147 ( 8 ): 525 - 533 .
161 . Undas A , Brummel-Ziedins KE , Mann KG . Statins and blood coagulation . Arterioscler Thromb Vasc Biol . 2005 ; 25 ( 2 ): 287 - 294 .
162 . Doggen CJ , Lemaitre RN , Smith NL , Heckbert SR , Psaty BM . HMG CoA reductase inhibitors and the risk of venous thrombosis among postmenopausal women . J Thromb Haemost . 2004 ; 2 ( 5 ): 700 - 701 .
163 . Lacut K , Le Gal G , Abalain JH , Mottier D , Oger E . Dif-ferential associations between lipid-lowering drugs, statins and fi brates, and venous thromboembolism: role of drug induced homocysteinemia? Thromb Res . 2008 ; 122 ( 3 ): 314 - 319 .
164 . Ramcharan AS , Van Stralen KJ , Snoep JD , Mantel-Teeuwisse AK , Rosendaal FR , Doggen CJ . HMG-CoA reductase inhibitors, other lipid-lowering medication, antiplatelet therapy, and the risk of venous thrombosis . J Thromb Haemost . 2009 ; 7 ( 4 ): 514 - 520 .
165 . Sørensen HT , Horvath-Puho E , Søgaard KK , et al . Arterial cardiovascular events, statins, low-dose aspirin and subse-quent risk of venous thromboembolism: a population-based case-control study . J Thromb Haemost . 2009 ; 7 ( 4 ): 521 - 528 .
166 . Yang CC , Jick SS , Jick H . Statins and the risk of idiopathic venous thromboembolism . Br J Clin Pharmacol . 2002 ; 53 ( 1 ): 101 - 105 .
167 . Smeeth L , Douglas I , Hall AJ , Hubbard R , Evans S . Effect of statins on a wide range of health outcomes: a cohort study validated by comparison with randomized trials . Br J Clin Pharmacol . 2009 ; 67 ( 1 ): 99 - 109 .
168 . Ray JG , Mamdani M , Tsuyuki RT , Anderson DR , Yeo EL , Laupacis A . Use of statins and the subsequent development of deep vein thrombosis . Arch Intern Med . 2001 ; 161 ( 11 ): 1405 - 1410 .
169 . Grady D , Wenger NK , Herrington D , et al . Postmenopausal hormone therapy increases risk for venous thromboembolic disease. The Heart and Estrogen/progestin Replacement Study . Ann Intern Med . 2000 ; 132 ( 9 ): 689 - 696 .
170 . Glynn RJ , Danielson E , Fonseca FA , et al . A randomized trial of rosuvastatin in the prevention of venous thromboem-bolism . N Engl J Med . 2009 ; 360 ( 18 ): 1851 - 1861 .
171. Reiss H, Haas S, Tebbe U, et al. A randomized double-blind study of centoparin vs unfractionated heparin to prevent venous thromboembolic events in acutely ill, non-surgical patients: CERTIFY Study. J Thromb Haemost. 2009;8:1209-1215.
172. Naccarato M, ChiodoGrandi F, Dennis M, Sandercock PAG. Physical methods for preventing deep vein thrombosis in stroke. Cochrane Database of Systematic Reviews. 2010;8:CD001922.
173. Barbar S et al. A risk assessment model for the identifi cation of hospitalized medical patients at risk for venous thrombo-embolism: the Padua Prediction Score. J Thromb Haemost. 2010;8(11):2450-2457.
Edema Study: prevention with travel stockings . Angiology . 2003 ; 54 ( 2 ): 143 - 154 .
148 . Cesarone MR , Belcaro G , Nicolaides AN , et al . The LONFLIT4-Concorde—Sigvaris Traveno Stockings in Long Flights (EcoTraS) Study: a randomized trial . Angiology . 2003 ; 54 ( 1 ): 1 - 9 .
149 . Cesarone MR , Belcaro G , Nicolaides AN , et al . Venous throm-bosis from air travel: the LONFLIT3 study—prevention with aspirin vs low-molecular-weight heparin (LMWH) in high-risk subjects: a randomized trial . Angiology . 2002 ; 53 ( 1 ): 1 - 6 .
150 . Cesarone MR , Belcaro G , Nicolaides AN , et al . Prevention of venous thrombosis in long-haul fl ights with Flite Tabs: the LONFLIT-FLITE randomized, controlled trial . Angiology . 2003 ; 54 ( 5 ): 531 - 539 .
151. Report of the General Medical Council fi tness to practice panel. General Medical Council-UK. http://webcache.gmc-uk.org/minutesfi les/3313.HTML. June 15, 2007 .
152 . Metjian A , Lim W . ASH evidence-based guidelines: should asymptomatic patients with antiphospholipid antibodies receive primary prophylaxis to prevent thrombosis? Hematology (Am Soc Hematol Educ Program) . 2009 : 247 - 249 .
153 . Segal JB , Brotman DJ , Necochea AJ , et al . Predictive value of factor V Leiden and prothrombin G20210A in adults with venous thromboembolism and in family members of those with a mutation: a systematic review . JAMA . 2009 ; 301 ( 23 ): 2472 - 2485 .
154 . Vossen CY , Conard J , Fontcuberta J , et al . Risk of a fi rst venous thrombotic event in carriers of a familial thrombophilic defect. The European Prospective Cohort on Thrombophilia (EPCOT) . J Thromb Haemost . 2005 ; 3 ( 3 ): 459 - 464 .
155. Bates SM, Greer IA, Middeldorp S, Veenstra D, Prabulos A-M, Vandvik PO. VTE, thrombophilia, antithrombotic therapy, and pregnancy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2)(suppl):e691S-e736S.
156 . Erkan D , Yazici Y , Peterson MG , Sammaritano L , Lockshin MD . A cross-sectional study of clinical thrombotic risk factors and preventive treatments in antiphospholipid syndrome . Rheumatology (Oxford) . 2002 ; 41 ( 8 ): 924 - 929 .
157 . Hereng T , Lambert M , Hachulla E , et al . Infl uence of aspirin on the clinical outcomes of 103 anti-phospholipid antibodies-positive patients . Lupus . 2008 ; 17 ( 1 ): 11 - 15 .
158 . Tektonidou MG , Laskari K , Panagiotakos DB , Moutsopoulos HM . Risk factors for thrombosis and primary thrombosis prevention in patients with systemic lupus erythematosus with or without antiphospholipid antibodies . Arthritis Rheum . 2009 ; 61 ( 1 ): 29 - 36 .
159 . Erkan D , Harrison MJ , Levy R , et al . Aspirin for primary thrombosis prevention in the antiphospholipid syndrome: a randomized, double-blind, placebo-controlled trial in asymptomatic antiphospholipid antibody-positive individuals . Arthritis Rheum . 2007 ; 56 ( 7 ): 2382 - 2391 .
160 . Glynn RJ , Ridker PM , Goldhaber SZ , Buring JE . Effect of low-dose aspirin on the occurrence of venous thromboem-
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

Online Data SupplementCHEST
1 © 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians ( www . chestjournal . org / site / misc / reprints . xhtml ). DOI: 10.1378/chest.11-2296
Prevention of VTE in Nonsurgical Patients
Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Susan R. Kahn , MD ; Wendy Lim , MD ; Andrew S. Dunn , MD ; Mary Cushman , MD ; Francesco Dentali , MD ; Elie A. Akl , MD, MPH, PhD ; Deborah J. Cook , MD, MSc(Epi) ; Alex A. Balekian , MD, MSHS ; Russell C. Klein , MD ; Hoang Le , MD, FCCP ; Sam Schulman , MD ; and M. Hassan Murad , MD, MPH
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

2© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
—E
ligi
bil
ity
Cri
teri
a fo
r R
CT
s of
Thr
omb
opro
phyl
axis
vs
Pla
ceb
o/C
ontr
ol i
n H
ospi
tali
zed
Med
ical
Pat
ient
s
Stud
y/Ye
arIn
clus
ion
Cri
teri
aE
xclu
sion
Cri
teri
a
Gal
lus
et a
l 1 /197
3A
ge N
/S (S
tudy
par
ticip
ants
wer
e 43
-85
y; m
ean
age
not a
vaila
ble)
His
tory
of D
VT
or
PE w
ithin
pre
viou
s y
Hos
pita
lized
Ble
edin
g te
nden
cy
Hea
rt fa
ilure
Bel
ch e
t al 2 /1
981
Age
40-
80 y
(mea
n ag
e no
t ava
ilabl
e)B
ed r
est f
or .
2 d
bef
ore
adm
issi
on
Hos
pita
lized
DV
T o
r PE
on
adm
issi
on
Hea
rt fa
ilure
, che
st in
fect
ion,
or
both
Hig
h ri
sk fo
r bl
eedi
ng
Iodi
ne a
llerg
y/se
nsiti
vity
Dah
an e
t al 3 /1
986
Age
. 6
5 y
(mea
n �
SD
age
: tre
atm
ent g
roup
, 79.
9 �
6.8
y;
pl
aceb
o gr
oup,
80.
1 �
6.9
y)
Pred
icta
ble
shor
t-te
rm h
ospi
taliz
atio
n ( ,
7 d
)
Hos
pita
lized
Act
ive
blee
ding
Coa
gula
tion
diso
rder
Thy
roid
dis
ease
Ong
oing
ant
icoa
gula
nt o
r an
tipla
tele
t the
rapy
Iodi
ne a
llerg
y
Acu
te m
edic
al il
lnes
s: C
HF
(NYH
A I
II-I
V),
acut
e or
res
pira
tory
infe
ctio
us d
isea
se“A
utop
sy n
ot a
vaila
ble
if ne
cess
ary”
Ibar
ra-P
erez
et a
l 4 /198
8A
ge .
40
y (m
ean
age
not a
vaila
ble)
PE
Pred
icte
d im
mob
iliza
tion
. 3
dM
edic
al h
isto
ry o
f DV
T o
r PE
Hem
orrh
age
CVA
Vasc
uliti
s
Peri
card
itis
Coa
gula
tion
diso
rder
s
Rec
ent p
osto
pera
tive
stat
us
Use
of a
ntic
oagu
lant
s
Hos
pita
lized
Alle
rgy
to io
dine
Pulm
onar
y di
seas
ePa
tient
or
phys
icia
n’s
refu
sal t
o co
oper
ate
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
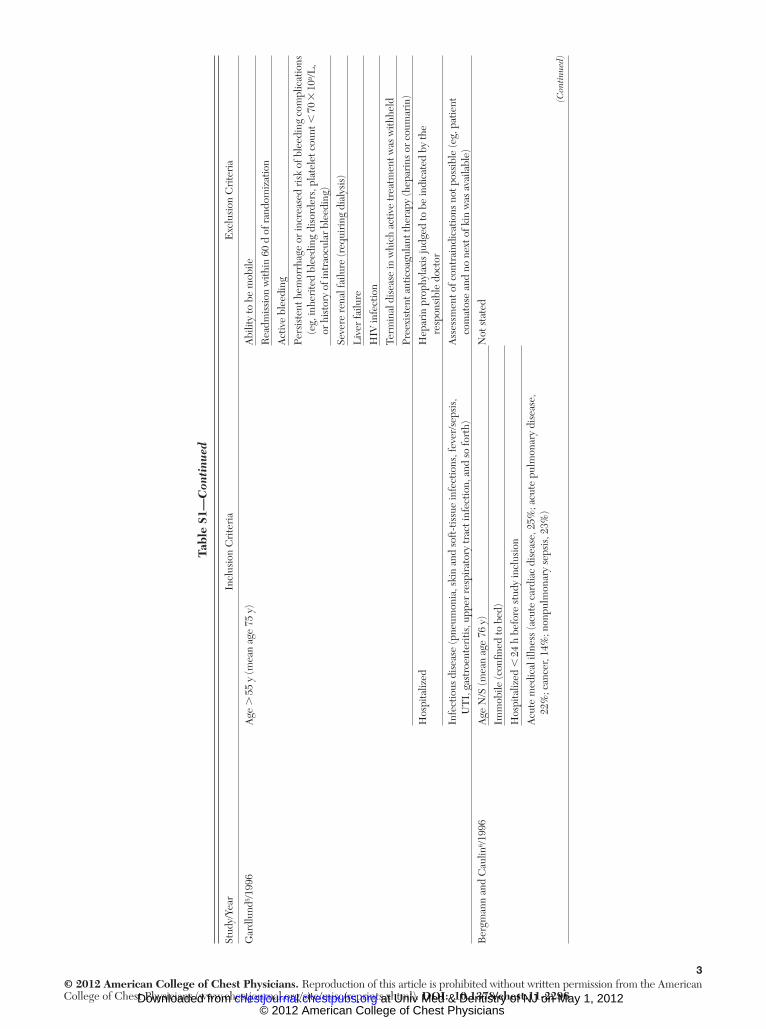
3© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arIn
clus
ion
Cri
teri
aE
xclu
sion
Cri
teri
a
Gar
dlun
d 5 /199
6A
ge .
55
y (m
ean
age
75 y
)A
bilit
y to
be
mob
ile
Rea
dmis
sion
with
in 6
0 d
of r
ando
miz
atio
n
Act
ive
blee
ding
Pers
iste
nt h
emor
rhag
e or
incr
ease
d ri
sk o
f ble
edin
g co
mpl
icat
ions
(eg,
inhe
rite
d bl
eedi
ng d
isor
ders
, pla
tele
t cou
nt ,
70
3 1
0 9 /L,
or h
isto
ry o
f int
raoc
ular
ble
edin
g)
Seve
re r
enal
failu
re (r
equi
ring
dia
lysi
s)
Liv
er fa
ilure
HIV
infe
ctio
n
Term
inal
dis
ease
in w
hich
act
ive
trea
tmen
t was
with
held
Pree
xist
ent a
ntic
oagu
lant
ther
apy
(hep
arin
s or
cou
mar
in)
Hos
pita
lized
Hep
arin
pro
phyl
axis
judg
ed to
be
indi
cate
d by
the
re
spon
sibl
e do
ctor
Infe
ctio
us d
isea
se (p
neum
onia
, ski
n an
d so
ft-t
issu
e in
fect
ions
, fev
er/s
epsi
s,
U
TI,
gas
troe
nter
itis,
upp
er r
espi
rato
ry tr
act i
nfec
tion,
and
so
fort
h)A
sses
smen
t of c
ontr
aind
icat
ions
not
pos
sibl
e (e
g, p
atie
nt
co
mat
ose
and
no n
ext o
f kin
was
ava
ilabl
e)
Ber
gman
n an
d C
aulin
6 /199
6A
ge N
/S (m
ean
age
76 y
)N
ot s
tate
d
Imm
obile
(con
fi ned
to b
ed)
Hos
pita
lized
, 2
4 h
befo
re s
tudy
incl
usio
n
Acu
te m
edic
al il
lnes
s (a
cute
car
diac
dis
ease
, 25%
; acu
te p
ulm
onar
y di
seas
e,
22
%; c
ance
r, 14
%; n
onpu
lmon
ary
seps
is, 2
3%)
Tabl
e S1
—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

4© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arIn
clus
ion
Cri
teri
aE
xclu
sion
Cri
teri
a
Sam
ama
et a
l, 7 ME
DE
NO
X S
tudy
/199
9A
ge .
40
y (m
ean
� S
D a
ge: 2
0 m
g en
oxap
arin
gro
up, 7
2.9
� 1
0.1
y; 4
0 m
g
enox
apar
in g
roup
, 73.
1 �
10.
8 y;
pla
cebo
gro
up, 7
4.1
� 1
0.6
y)K
now
n th
rom
boph
ilia
Imm
obili
zatio
n ,
3 d
at t
ime
of e
nrol
lmen
tSe
rum
cre
atin
ine
conc
entr
atio
n .
1.7
mg/
dL (1
50 m
mol
/L)
Proj
ecte
d ho
spita
l sta
y .
6 d
Unc
ontr
olle
d ar
teri
al h
yper
tens
ion
(sys
tolic
BP
. 2
00 m
m H
g,
di
asto
lic B
P .
120
mm
Hg,
or
both
)
Act
ive
pept
ic u
lcer
, bac
teri
al e
ndoc
ardi
tis, o
r ot
her
cond
ition
s
that
cou
ld in
crea
se th
e ri
sk o
f hem
orrh
age
Plat
elet
cou
nt ,
100
,000
/ m L
, pro
long
ed a
PTT,
pro
thro
mbi
n
ratio
of ,
50%
, or
INR
. 1
.2
HIV
Stro
ke/s
urge
ry w
ithin
pre
viou
s 3
mo
Intu
batio
n
Ant
icoa
gula
nt th
erap
y re
quir
ed/r
ecei
ved
any
type
of
an
ticoa
gula
nt th
erap
y fo
r .
48
h
Con
trai
ndic
atio
ns to
iodi
nate
d co
ntra
st m
edia
Hyp
erse
nsiti
vity
to h
epar
in o
r he
pari
n-in
duce
d
thro
mbo
cyto
peni
a
CH
F (N
YHA
III
-IV
), ac
ute
or c
hron
ic r
espi
rato
ry d
isea
se (i
f acu
te
re
spir
ator
y fa
ilure
doe
s no
t req
uire
ven
tilat
or s
uppo
rt);
or o
ne o
f the
fo
llow
ing
acut
e in
fect
ious
or
rheu
mat
olog
ic d
isea
se, i
f ass
ocia
ted
with
at
leas
t one
add
ition
al r
isk
fact
or a f
or V
TE
: acu
te in
fect
ion
with
out
sept
ic s
hock
; acu
te r
heum
atic
dis
orde
rs (i
nclu
ding
acu
te lu
mba
r pa
in o
r sc
iatic
a or
ver
tebr
al c
ompr
essi
on c
ause
d by
ost
eopo
rosi
s or
a tu
mor
), ac
ute
arth
ritis
of t
he le
gs, o
r an
acu
te e
piso
de o
f rh
eum
atoi
d ar
thri
tis in
the
legs
; or
an e
piso
de o
f in
fl am
mat
ory
bow
el d
isea
se
Preg
nant
/bre
astf
eedi
ng w
omen
Wom
en o
f chi
ldbe
arin
g ag
e no
t usi
ng c
ontr
acep
tion
Tabl
e S1
—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

5© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arIn
clus
ion
Cri
teri
aE
xclu
sion
Cri
teri
a
Fra
isse
et a
l 8 /200
0A
ge 4
0-80
y (m
ean
� S
D a
ge: t
reat
men
t gro
up, 6
9.4
� 7
.7 y
;
plac
ebo
grou
p, 6
6.8
� 8
.2 y
)Pa
tient
on
vent
ilato
r ,
48
h
Hos
pita
lized
(med
ical
IC
U)
His
tory
of a
con
fi rm
ed D
VT
with
in th
e pr
evio
us 6
mo
or
pre
senc
e of
sig
ns o
f a D
VT
on
the
Dop
pler
ul
tras
onog
raph
y at
incl
usio
n
Adm
itted
with
acu
te, r
espi
rato
ry-d
ecom
pens
ated
CO
PD,
an
d re
quir
ing
mec
hani
cal v
entil
atio
nO
rgan
ic le
sion
that
cou
ld b
leed
(ie,
an
activ
e ga
stro
duod
enal
ulce
r or
a r
ecen
t hem
orrh
agic
CVA
)
Wei
ght 4
5-10
0 kg
Seve
re li
ver
failu
re le
adin
g to
a d
ecre
ase
of th
e PT
to ,
50%
(nor
mal
val
ues
70%
-100
%)
Seve
re r
enal
impa
irm
ent (
seru
m c
reat
inin
e .
300
m m
ol/L
)
Con
fi rm
ed o
r un
cont
rolle
d hy
pert
ensi
on (d
iast
olic
BP
. 1
20 m
m H
g)
Con
geni
tal o
r ac
quir
ed c
oagu
latio
n di
sord
er
His
tory
of h
yper
sens
itivi
ty o
r th
rom
bocy
tope
nia
to a
ny ty
pe
of
hep
arin
Con
trai
ndic
atio
n to
ant
icoa
gula
nt th
erap
y, v
enog
raph
y,
or
ang
iogr
aphy
Rec
eivi
ng a
ny fo
rm o
f ace
tyls
alic
ylic
aci
d, ti
clop
idin
e,
or
ora
l ant
icoa
gula
nts
Lei
zoro
vicz
et a
l, 9 PR
EV
EN
T S
tudy
/200
4A
ge �
40
y (m
ean
� S
D a
ge, 6
8.5
� 1
1.7
y)H
igh
risk
of b
leed
ing
� 3
d o
f pre
viou
s im
mob
iliza
tion
Plat
elet
cou
nt ,
100
3 1
0 9 /L
Proj
ecte
d ho
spita
lizat
ion
� 4
dH
epat
ic in
suffi
cien
cy o
r ac
tive
hepa
titis
Acu
te c
oron
ary
synd
rom
e w
ithin
pre
viou
s m
o
Bac
teri
al e
ndoc
ardi
tis
Imm
obili
zed
low
er li
mb
due
to c
ast o
r fr
actu
re
Stro
ke w
ithin
last
3 m
o
Maj
or s
urgi
cal o
r in
vasi
ve p
roce
dure
per
form
ed in
prev
ious
mo
or to
be
unde
rtak
en w
ithin
nex
t 2 w
k
Hep
arin
or
LM
WH
pro
phyl
axis
. 4
8 h
befo
re r
ando
miz
atio
n
Con
trai
ndic
atio
n to
hep
arin
ant
icoa
gula
tion
Cre
atin
ine
. 2
.0 m
g/dL
Acu
te m
edic
al il
lnes
s: a
cute
CH
F (N
YHA
III
-IV
); or
acu
te r
espi
rato
ry fa
ilure
that
did
not
req
uire
ven
tilat
ory
supp
ort;
or a
ny o
f the
follo
win
g, if
com
bine
d w
ith �
1 a
dditi
onal
ris
k fa
ctor
for
VT
E b :
infe
ctio
n w
ithou
t sep
tic s
hock
, acu
te
rheu
mat
olog
ic d
isor
ders
, or
infl a
mm
ator
y bo
wel
dis
ease
Preg
nanc
y or
bre
astf
eedi
ng
Life
exp
ecta
ncy
, 1
mo
Tabl
e S1
—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

6© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arIn
clus
ion
Cri
teri
aE
xclu
sion
Cri
teri
a
Mah
e et
al 10
/200
5A
ge .
40
y (m
ean
age:
trea
tmen
t gro
up, 7
6.1
y; p
lace
bo g
roup
76.
5 y
Syst
olic
BP
. 2
40 m
m H
g, d
iast
olic
BP
. 1
20 m
m H
g
Imm
obili
zed
(una
ble
to w
alk
. 1
0 m
alo
ne)
Plat
elet
leve
l , 5
0,00
0/ m
m, T
CA
. c
ontr
ol 1
10
s
Hos
pita
lized
, 2
4 h
PT ,
50%
Act
ive
gast
rodu
oden
al u
lcer
Ren
al fa
ilure
(cre
atin
ine
leve
l . 3
00 m
mol
/L)
Con
ditio
ns r
equi
ring
full-
dose
ant
icoa
gula
tion
Stro
ke o
r m
ajor
sur
gery
with
in th
e pr
evio
us 3
0 d
Ant
icoa
gula
nt o
r an
tipla
tele
t the
rapy
with
in la
st 7
d
Acu
te m
edic
al il
lnes
s: C
HF
(NYH
A I
II-I
V),
acut
e or
res
pira
tory
dis
ease
,
nonp
ulm
onar
y se
psis
, can
cer
Preg
nanc
y
Led
erle
et a
l 11 /2
006
Age
� 6
0 (m
ean
� S
D a
ge: t
reat
men
t gro
up, 7
1.3
y; p
lace
bo g
roup
, 72.
1 y
Kno
wn
thro
mbo
cyto
peni
a (p
late
let c
ount
, 1
00,0
00/ m
m 3 )
Adm
itted
or
tran
sfer
red
to m
edic
al s
ervi
ceSy
stol
ic B
P .
220
mm
Hg
or d
iast
olic
BP
. 1
10 m
m H
g
Occ
urre
nce
with
in p
ast 3
0 d
of m
yoca
rdia
l inf
arct
ion,
str
oke,
maj
or s
urge
ry (d
efi n
ed a
s re
quir
ing
gene
ral,
spin
al,
or e
pidu
ral a
nest
hesi
a an
d la
stin
g .
30
min
), or
any
eye
sur
gery
Alr
eady
rec
eivi
ng o
r re
quir
ing
antic
oagu
latio
n fo
r re
ason
s
othe
r th
an V
TE
pro
phyl
axis
Oth
er c
ontr
aind
icat
ion
to lo
w-d
ose
hepa
rin
Prev
ious
ran
dom
izat
ion
into
the
stud
y
Pred
icte
d ho
spita
lizat
ion
� 3
d“S
uppo
rtiv
e/pa
lliat
ive
care
onl
y” s
tatu
s
Tabl
e S1
—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

7© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arIn
clus
ion
Cri
teri
aE
xclu
sion
Cri
teri
a
Coh
en e
t al, 12
AR
TE
MIS
Stu
dy/2
006
Age
� 6
0 y
(mea
n �
SD
age
: tre
atm
ent g
roup
, 75.
0 �
8.3
y;
pl
aceb
o gr
oup,
74.
4 �
8.3
y)
Hig
h ri
sk fo
r bl
eedi
ng
Pred
icte
d im
mob
iliza
tion
� 4
dSe
rum
cre
atin
ine
leve
l . 1
80 m
mol
/L in
wel
l-hyd
rate
d pa
tient
Hos
pita
lized
Acu
te b
acte
rial
end
ocar
ditis
Cer
ebra
l met
asta
sis
Rec
ent h
emor
rhag
ic o
r is
chem
ic s
trok
e
Bra
in, s
pina
l, or
oph
thal
mol
ogic
sur
gery
Indw
ellin
g in
trat
heca
l or
epid
ural
cat
hete
r
Ant
icip
ated
intu
batio
n .
24
h
Use
of a
ntith
rom
botic
s ,
48
h be
fore
ran
dom
izat
ion
Indi
catio
n fo
r an
ticoa
gula
nt p
roph
ylax
is o
r th
erap
y
Doc
umen
ted
hype
rsen
sitiv
ity to
con
tras
t med
ia
Acu
te m
edic
al il
lnes
s: C
HF
(NYH
A I
II-I
V);
or a
cute
res
pira
tory
illn
ess
in th
e
pres
ence
of c
hron
ic lu
ng d
isea
se; o
r cl
inic
ally
dia
gnos
ed a
cute
infe
ctio
ns
or in
fl am
mat
ory
diso
rder
s, s
uch
as a
rthr
itis,
con
nect
ive
tissu
e di
seas
es,
or in
fl am
mat
ory
bow
el d
isea
se
Life
exp
ecta
ncy
, 1
mo
aPT
T 5
act
ivat
ed p
artia
l thr
ombo
plas
tin ti
me;
CVA
5 c
ereb
rova
scul
ar a
ccid
ent;
INR
5 in
tern
atio
nal n
orm
aliz
ed r
atio
; LM
WH
5 lo
w-m
olec
ular
-wei
ght h
epar
in; N
/S 5
not
sta
ted
as in
clus
ion
crite
rion
; N
YHA
5 N
ew Y
ork
Hea
rt A
ssoc
iatio
n; P
T 5
pro
thro
mbi
n tim
e; T
CA
5 tr
ichl
oroa
cetic
aci
d; U
TI
5 u
rina
ry tr
act i
nfec
tion .
a A
dditi
onal
ris
k fa
ctor
s: a
ge .
75
y, c
ance
r, pr
evio
us V
TE
, obe
sity
(B
MI
� 3
0 fo
r m
en a
nd �
28.
6 fo
r w
omen
), va
rico
se v
eins
, hor
mon
e th
erap
y (a
ntia
ndro
gen
or e
stro
gen,
exc
ept
for
post
men
opau
sal
horm
one-
repl
acem
ent t
hera
py),
and
chro
nic
hear
t or
resp
irat
ory
failu
re.
b Add
ition
al r
isk
fact
ors
for
VT
E: a
ge �
75
y, c
ance
r, pr
evio
us V
TE
, obe
sity
, var
icos
e ve
ins
and/
or c
hron
ic v
enou
s in
suffi
cien
cy, h
orm
one
repl
acem
ent t
hera
py, h
isto
ry o
f CH
F, c
hron
ic r
espi
rato
ry fa
ilure
, or
mye
lopr
olife
rativ
e sy
ndro
me.
Tabl
e S1
—C
onti
nued
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

8© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
—O
bse
rvat
iona
l St
udi
es o
f R
isk
of V
TE
in
Acu
tely
Ill
or
Hos
pita
lize
d M
edic
al P
atie
nts
Stud
y/Ye
arPa
tient
sD
urat
ion
of F
ollo
w-u
pU
se o
f Thr
ombo
prop
hyla
xis
Sym
ptom
atic
VT
E
Eve
nts
No.
(%) C
umul
ativ
e In
cide
nce
[rat
e]
Bos
son
et a
l 13 /2
006
Patie
nts
� 4
0 y
with
an
acu
te m
edic
al
even
t, an
ticip
ated
to
hav
e re
duce
d m
obili
ty fo
r at
le
ast 4
8 h
(200
2-20
03)
1-28
dIn
itiat
ed in
35%
of
patie
nts
(n 5
5,7
82)
DV
T: c
onfi r
med
by
dup
lex
ultr
ason
ogra
phy
O
vera
ll12
8 (0
.77)
[0.5
eve
nts/
1,00
0 pa
tient
-day
s]
Man
aged
in th
e co
mm
unity
(out
patie
nts)
Tr
eate
d: n
5 4
,163
(h
igh
risk
: 1,6
64;
low
ris
k: 2
,499
)
77 (1
.85)
N 5
16,
532
Hig
h ri
sk 4
2 (2
.52)
Low
ris
k 35
(1.4
0)
U
ntre
ated
: n 5
8,2
47
(hig
h ri
sk: 1
,318
; lo
w r
isk:
6,8
43)
51 (0
.62)
Hig
h ri
sk 1
6 (1
.21)
Low
ris
k 35
(0.5
1)
PE
: con
fi rm
ed
by im
agin
g27
(0.2
)
[0.1
eve
nts/
1,00
0 pa
tient
-day
s]
Dar
ze e
t al 14
/200
5Pa
tient
s w
ith C
HF
(2
001-
2003
)N
ot r
epor
ted
70%
Rec
eive
d 40
mg
enox
apar
inPE
: con
fi rm
ed b
y hi
gh-
prob
abili
ty lu
ng
scin
tigra
phy
or p
ositi
ve
spir
al C
T
N 5
198
O
vera
ll18
(9.1
)
Tr
eate
d: n
5 1
3812
(8.7
)
Unt
reat
ed: n
5 6
06
(10.
0)
Gui
jarr
o et
al 15
/200
5A
ll ho
spita
l inp
atie
nts
(199
8-20
01)
Not
rep
orte
dN
o in
form
atio
n pr
ovid
edD
VT
as
the
seco
ndar
y
di
agno
sis
5,55
9 (0
.25)
N 5
2,2
28,8
94PE
as
the
seco
ndar
y di
agno
sis
at d
isch
arge
2,16
2 (0
.1)
Kis
him
oto
et a
l 16 /2
005
All
hosp
ital i
npat
ient
s (1
987-
1999
)H
ospi
tal s
tay:
mea
n le
ngth
of h
ospi
tal
stay
not
rep
orte
d
Nev
er o
r ra
rely
use
dD
VT:
dia
gnos
ed
by v
enog
raph
y or
ultr
asou
nd
128
(0.1
)
N 5
131
,060
Tim
e fr
om
adm
issi
on to
dia
gnos
is
(mea
n 1
SD
): 21
.3 1
21.
2 d
PE: d
iagn
osed
by
pulm
onar
y pe
rfus
ion
scin
tigra
phy
and/
or
cont
rast
-enh
ance
d C
T s
can
41 (0
.03)
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

9© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
—C
onti
nued
Stud
y/Ye
arPa
tient
sD
urat
ion
of F
ollo
w-u
pU
se o
f Thr
ombo
prop
hyla
xis
Sym
ptom
atic
VT
E
Eve
nts
No.
(%) C
umul
ativ
e In
cide
nce
[rat
e]
Skaf
et a
l 17 /2
005
Isch
emic
or
hem
orrh
agic
str
oke
(197
9-20
03)
Unt
il di
scha
rge
Not
ana
lyze
d; a
utho
rs
assu
me
mos
t pat
ient
s w
ith is
chem
ic s
trok
e re
ceiv
ed a
ntith
rom
botic
th
erap
y
DV
T: m
etho
d
of
dia
gnos
is
not r
epor
ted
Mea
n le
ngth
of
hosp
ital s
tay
not r
epor
ted
O
vera
ll12
6,00
0 (0
.8)
N 5
15,
715,
000
Is
chem
ic s
trok
e
pa
tient
s10
4,00
0 (0
.74)
14,1
09,0
00 (i
sche
mic
), 1,
606,
000
(hem
orrh
agic
)
Hem
orrh
agic
str
oke
patie
nts
22,0
00 (1
.37)
PE: m
etho
d of
dia
gnos
is
not r
epor
ted
O
vera
ll83
,000
(0.5
3)
Is
chem
ic s
trok
e
pa
tient
s72
,000
(0.5
1)
H
emor
rhag
ic s
trok
e
pa
tient
s11
,000
(0.6
8)
Spyr
opou
los
et a
l 18 /2
011
IMPR
OV
E r
egis
try
patie
nts:
� 1
8 y,
ad
mitt
ed to
the
hosp
ital f
or a
n ac
ute
med
ical
ill
ness
, hos
pita
l st
ay �
3 d
(200
2-20
06)
Up
to 3
mo
50%
Rec
eive
d th
rom
bopr
ophy
laxi
s (d
etai
ls p
rovi
ded
in T
apso
n et
al 19
)
VT
E: D
VT
and
PE
da
ta n
ot p
rese
nted
se
para
tely
, or
acco
rdin
g to
whe
ther
th
rom
bopr
ophy
laxi
s w
as r
ecei
ved
143
(0.9
)
N 5
15,
156
Spyr
opou
los
et a
l 20 /2
011
Insu
red
patie
nts
� 4
0 y,
ho
spita
lized
for
canc
er, C
HF,
se
vere
infe
ctio
us
dise
ases
, or
lung
di
seas
es (2
001-
2005
)
� 9
1 d
(rep
orte
d V
TE
by
30-
d w
indo
ws)
No
info
rmat
ion
prov
ided
VT
E: d
isch
arge
rec
ords
8,89
5 (5
.6):
3,22
5 (3
6.3)
ev
ents
occ
urre
d in
the
fi rst
30
d fo
llow
ing
hosp
italiz
atio
n; 4
,107
(46.
2)
even
ts o
ccur
red
. 3
mo
post
disc
harg
e 6,
300
(3.9
8)
(DV
T),
2,32
4 (1
.47)
(PE
), 27
1 (0
.17)
(DV
T/P
E)
DV
T: m
edia
n tim
e to
D
VT,
76
d
PE: m
edia
n tim
e
to
PE
, 73
d
N 5
158
,325
DV
T/P
E: m
edia
n tim
e
to
DV
T/P
E, 3
4 d
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

10© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arPa
tient
sD
urat
ion
of F
ollo
w-u
pU
se o
f Thr
ombo
prop
hyla
xis
Sym
ptom
atic
VT
E
Eve
nts
No.
(%) C
umul
ativ
e In
cide
nce
[rat
e]
Bar
bar
et a
l 21 /2
010
Patie
nts
� 1
8 y
adm
itted
to a
de
part
men
t of i
nter
nal
med
icin
e (2
007-
2008
)
3 m
o18
6 (3
9.7%
) of p
atie
nts
at
high
ris
k re
ceiv
ed
appr
opri
ate
prop
hyla
xis;
52
(7.3
%) o
f pat
ient
s at
lo
w r
isk
of V
TE
re
ceiv
ed p
roph
ylax
is
DV
T: c
ompr
essi
on
ultr
ason
ogra
phy
L
ow r
isk:
n 5
711
0 (0
)
H
igh
risk
: n 5
469
22 (4
.7)
Trea
ted:
n 5
186
3 (1
.6)
N 5
118
0
U
ntre
ated
: n 5
283
19 (6
.7)
PE: s
pira
l CT
or
/ s
can
L
ow r
isk:
n 5
711
2 (0
.3)
Trea
ted:
n 5
52
1 (1
.9)
Unt
reat
ed: n
5 6
591
(0.2
)
H
igh
risk
: n 5
469
13 (2
.8)
Trea
ted:
n 5
185
1 (0
.5) (
nonf
atal
)
Unt
reat
ed: n
5 2
8312
(4.2
) (11
non
fata
l w
ith o
r w
ithou
t D
VT,
1 fa
tal P
E)
Ris
k of
sym
ptom
atic
DV
T in
pat
ient
s ho
spita
lized
for
an a
cute
med
ical
eve
nt in
stu
dies
rep
orte
d he
re r
ange
from
0.1
%-6
.7%
. The
low
est e
stim
ate
(0.1
%) w
as d
eriv
ed fr
om a
stu
dy o
f hos
pita
lized
Jap
anes
e pa
tient
s w
ho a
re e
xpec
ted
to h
ave
low
rat
es b
ased
on
prev
ious
rep
orts
in J
apan
ese
pers
ons.
The
hig
hest
est
imat
e (6
.7%
) w
as r
epor
ted
in t
he B
arba
r et
al 21
stu
dy, w
hich
incl
uded
3 m
o of
fol
low
-up
and
repo
rted
eve
nts
with
in th
e tr
eate
d an
d un
trea
ted
grou
ps. T
he n
ext h
ighe
st e
stim
ate
(4.0
%) w
as r
epor
ted
in th
e Sp
yrop
oulo
s et
al 18
,20 s
tudy
, whi
ch a
lso
incl
uded
3 m
o of
follo
w-u
p bu
t did
not
rep
ort b
y pr
o-ph
ylax
is g
roup
. Exc
ludi
ng th
ese
thre
e st
udie
s, ra
tes r
ange
d fr
om 0
.25%
-0.8
%. R
ate
of D
VT
was
onl
y re
port
ed in
one
stud
y (B
osso
n et
al)
as 0
.5 e
vent
s/1,
000
patie
nt-d
ays.
Ris
k of
PE
in p
atie
nts h
ospi
taliz
ed
for a
n ac
ute
med
ical
eve
nt in
stud
ies r
epor
ted
here
rang
e fr
om 0
.03%
-10%
. The
low
est e
stim
ate
(0.0
3%) w
as d
eriv
ed fr
om a
stud
y of
hos
pita
lized
Japa
nese
pat
ient
s who
are
exp
ecte
d to
hav
e lo
w ra
tes b
ased
on
pre
viou
s re
port
s in
Jap
anes
e pe
rson
s. T
he h
ighe
st e
stim
ate
(10%
) was
rep
orte
d in
the
Dar
ze e
t al 14
stu
dy, w
hich
rep
orte
d ev
ents
with
in th
e tr
eate
d an
d un
trea
ted
grou
ps a
nd o
nly
incl
uded
pat
ient
s w
ith
seve
re c
onge
stiv
e he
art f
ailu
re w
ho h
ad h
igh
rate
s of
trad
ition
al r
isk
fact
ors.
The
sec
ond
high
est e
stim
ate
(4.2
%)
was
rep
orte
d in
the
Bar
bar
et a
l 21 s
tudy
, whi
ch in
clud
ed 3
mo
of fo
llow
-up
and
repo
rted
ev
ents
with
in t
he t
reat
ed a
nd u
ntre
ated
gro
ups.
Exc
ludi
ng t
hese
thr
ee s
tudi
es, r
ates
ran
ged
from
0.1
%-1
.5%
. Rat
e of
PE
was
onl
y re
port
ed in
one
stu
dy (
Bos
son
et a
l 13 )
as 0
.1 e
vent
/1,0
00 p
atie
nt-d
ays.
C
HF
5 co
nges
tive
hear
t fai
lure
; PE
5 p
ulm
onar
y em
bolis
m;
/ 5
ven
tilat
ion/
perf
usio
n. Ta
ble
S2—
Con
tinu
ed
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
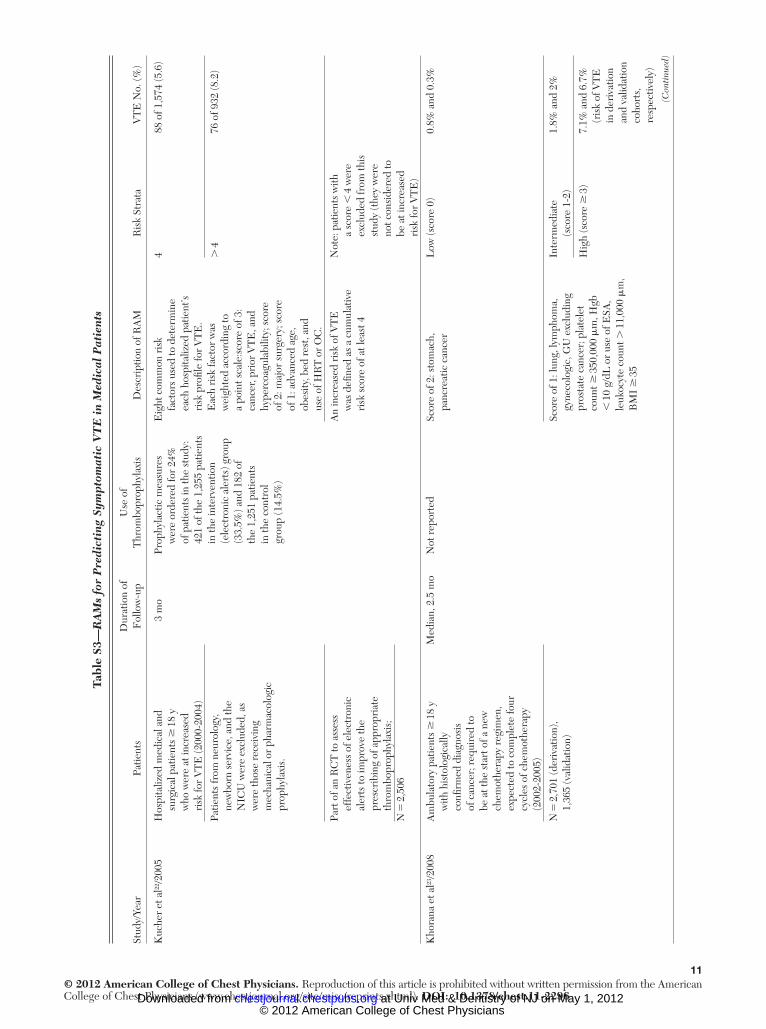
11© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S3
— R
AM
s fo
r P
redi
ctin
g Sy
mpt
omat
ic V
TE
in
Med
ical
Pat
ient
s
Stud
y/Ye
arPa
tient
sD
urat
ion
of
Fol
low
-up
Use
of
Thr
ombo
prop
hyla
xis
Des
crip
tion
of R
AM
Ris
k St
rata
VT
E N
o. (%
)
Kuc
her
et a
l 22 /2
005
H
ospi
taliz
ed m
edic
al a
nd
su
rgic
al p
atie
nts
� 1
8 y
who
wer
e at
incr
ease
d ri
sk fo
r V
TE
(200
0-20
04)
3 m
oPr
ophy
lact
ic m
easu
res
w
ere
orde
red
for
24%
of
pat
ient
s in
the
stud
y:
421
of th
e 1,
255
patie
nts
in th
e in
terv
entio
n (e
lect
roni
c al
erts
) gro
up
(33.
5%) a
nd 1
82 o
f th
e 1,
251
patie
nts
in th
e co
ntro
l gr
oup
(14.
5%)
Eig
ht c
omm
on r
isk
fa
ctor
s us
ed to
det
erm
ine
each
hos
pita
lized
pat
ient
’s ri
sk p
rofi l
e fo
r V
TE
. E
ach
risk
fact
or w
as
wei
ghte
d ac
cord
ing
to
a po
int s
cale
:sco
re o
f 3:
canc
er, p
rior
VT
E, a
nd
hype
rcoa
gula
bilit
y; s
core
of
2: m
ajor
sur
gery
; sco
re
of 1
: adv
ance
d ag
e,
obes
ity, b
ed r
est,
and
use
of H
RT
or
OC
.
488
of 1
,574
(5.6
)
Patie
nts
from
neu
rolo
gy,
ne
wbo
rn s
ervi
ce, a
nd th
e N
ICU
wer
e ex
clud
ed, a
s w
ere
thos
e re
ceiv
ing
mec
hani
cal o
r ph
arm
acol
ogic
pr
ophy
laxi
s.
. 4
76 o
f 932
(8.2
)
Part
of a
n R
CT
to a
sses
s
effe
ctiv
enes
s of
ele
ctro
nic
aler
ts to
impr
ove
the
pres
crib
ing
of a
ppro
pria
te
thro
mbo
prop
hyla
xis;
N
5 2
,506
An
incr
ease
d ri
sk o
f VT
E
w
as d
efi n
ed a
s a
cum
ulat
ive
risk
sco
re o
f at l
east
4
Not
e: p
atie
nts
with
a
scor
e ,
4 w
ere
excl
uded
from
this
st
udy
(the
y w
ere
not c
onsi
dere
d to
be
at i
ncre
ased
ri
sk fo
r V
TE
)
Kho
rana
et a
l 23 /2
008
Am
bula
tory
pat
ient
s �
18
y
with
his
tolo
gica
lly
confi
rm
ed d
iagn
osis
of
can
cer;
req
uire
d to
be
at t
he s
tart
of a
new
ch
emot
hera
py r
egim
en,
expe
cted
to c
ompl
ete
four
cy
cles
of c
hem
othe
rapy
(2
002-
2005
)
Med
ian,
2.5
mo
Not
rep
orte
dSc
ore
of 2
: sto
mac
h,
pa
ncre
atic
can
cer
Low
(sco
re 0
)0.
8% a
nd 0
.3%
N 5
2,7
01 (d
eriv
atio
n),
1,
365
(val
idat
ion)
Scor
e of
1: l
ung,
lym
phom
a,
gy
neco
logi
c, G
U e
xclu
ding
pr
osta
te c
ance
r; p
late
let
coun
t � 3
50,0
00 m
m, H
gb
, 1
0 g/
dL o
r us
e of
ESA
, le
ukoc
yte
coun
t . 1
1,00
0 m
m,
BM
I �
35
Inte
rmed
iate
(s
core
1-2
)1.
8% a
nd 2
%
Hig
h (s
core
� 3
)7.
1% a
nd 6
.7%
(ris
k of
VT
E
in d
eriv
atio
n an
d va
lidat
ion
coho
rts,
re
spec
tivel
y)
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

12© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arPa
tient
sD
urat
ion
of
Fol
low
-up
Use
of
Thr
ombo
prop
hyla
xis
Des
crip
tion
of R
AM
Ris
k St
rata
VT
E N
o. (%
)
Bar
bar
et a
l 21 /2
010 b
Con
secu
tive
patie
nts
� 1
8 y
ad
mitt
ed to
a d
epar
tmen
t of
inte
rnal
med
icin
e (2
007-
2008
)
3 m
o18
6 of
496
(39.
7%) o
f
patie
nts
at h
igh
risk
re
ceiv
ed a
ppro
pria
te
prop
hyla
xis
(the
re
mai
ning
283
rec
eive
d no
ne o
r in
appr
opri
ate
prop
hyla
xis)
; 52
of
711
(7.3
%) o
f pat
ient
s at
low
ris
k of
VT
E
rece
ived
pro
phyl
axis
Ele
ven
com
mon
ris
k fa
ctor
s
used
to d
eter
min
e ea
ch
hosp
italiz
ed p
atie
nt’s
risk
pr
ofi le
for
VT
E. E
ach
risk
fa
ctor
was
wei
ghte
d ac
cord
ing
to a
poi
nt s
cale
:
, 4
(low
ris
k):
2 of
711
(0.3
)
Scor
e of
3: a
ctiv
e ca
ncer
, pri
or
V
TE
, red
uced
mob
ility
, kno
wn
thro
mbo
phili
c co
nditi
on;
� 4
(hig
h ri
sk):
35 o
f 469
(7.5
)
Patie
nts
wer
e ex
clud
ed
if
they
wer
e on
full-
dose
an
ticoa
gula
tion
ther
apy,
ha
d co
ntra
indi
catio
ns to
ph
arm
acol
ogic
pro
phyl
axis
, or
wer
e pr
egna
nt
Scor
e of
2: r
ecen
t tra
uma
an
d/or
sur
gery
Rec
eive
d pr
ophy
laxi
s4
of 1
86 (2
.2)
N 5
1,1
80Sc
ore
of 1
: age
� 7
0 y,
hea
rt
an
d/or
res
pira
tory
failu
re, a
cute
M
I or
isch
emic
str
oke,
acu
te
infe
ctio
n an
d/or
rhe
umat
olog
ic
diso
rder
, obe
sity
, ong
oing
ho
rmon
al tr
eatm
ent
Did
not
rec
eive
prop
hyla
xis
31 o
f 283
(11.
8)
An
incr
ease
d ri
sk o
f VT
E w
as
de
fi ned
as
a cu
mul
ativ
e ri
sk
scor
e of
at l
east
4 c
Tabl
e S3
—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

13© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arPa
tient
sD
urat
ion
of
Fol
low
-up
Use
of
Thr
ombo
prop
hyla
xis
Des
crip
tion
of R
AM
Ris
k St
rata
VT
E N
o. (%
)
Spyr
opou
los
et a
l 18 /2
011
IMPR
OV
E s
tudy
19 p
atie
nts
ag
ed �
18
y, a
dmis
sion
fo
r an
acu
te m
edic
al
illne
ss, �
3 d
hos
pita
lizat
ion.
F
irst
10
elig
ible
acu
tely
ill
hos
pita
lized
med
ical
pat
ient
s sy
stem
atic
ally
enr
olle
d at
the
star
t of e
ach
mon
th a
t eac
h ho
spita
l.
3 m
oN
ot r
epor
ted
Two
mod
els
deve
lope
d: 4
-fac
tor
m
odel
bas
ed o
n fa
ctor
s av
aila
ble
at h
ospi
tal
adm
issi
on a
nd 7
-fac
tor
mod
el in
clud
ing
fact
ors
avai
labl
e du
ring
hos
pita
l st
ay. F
acto
r sc
ores
(1-3
) ba
sed
on lo
gari
thm
ic H
R.
4-fa
ctor
mod
el:
0 (l
owes
t ris
k)24
of 4
,981
(0.5
)
1
72 o
f 8,4
41 (1
.0)
2
20 o
f 1,1
66 (2
.1)
3
5 of
127
(4.0
)
4-fa
ctor
mod
el: o
lder
age
and
canc
er, 1
poi
nt e
ach;
kno
wn
thro
mbo
phili
a an
d pr
evio
us
VT
E, 3
poi
nts
each
.
4
16 o
f 376
(4.7
)
Patie
nts
excl
uded
if e
nrol
led
in a
ther
apeu
tic c
linic
al tr
ial o
r if
any
of th
e fo
llow
ing
appl
ied:
an
ticoa
gula
nt o
r th
rom
boly
tic
drug
use
at a
dmis
sion
or
with
in
48 h
aft
er a
dmis
sion
; maj
or
surg
ery
or tr
aum
a �
3 m
o be
fore
ad
mis
sion
; adm
issi
on fo
r D
VT
or
PE
(or
diag
nosi
s of
eith
er
with
in 2
4 h
of a
dmis
sion
); fo
llow
-up
deem
ed im
poss
ible
.
5
-8 (h
ighe
st r
isk)
6 of
65
(11)
7-fa
ctor
mod
el: o
lder
age
,
ICU
/CC
U s
tay,
im
mob
iliza
tion
� 7
d,
1 po
int e
ach;
cur
rent
can
cer,
curr
ent L
L p
aral
ysis
, kno
wn
thro
mbo
phili
a, 2
poi
nts
each
; pr
evio
us V
TE
3 p
oint
s.
7-fa
ctor
mod
el:
0 (l
owes
t ris
k)14
of 4
,029
(0.4
)
N 5
15,
156
1
33 o
f 6,3
50 (0
.6)
2
31 o
f 2,4
20 (1
.5)
3
18 o
f 1,3
35 (1
.6)
4
30 o
f 729
(4.8
)
5
-10
(hig
hest
ris
k)17
of 2
62 (8
.1)
Not
at A
CC
P ri
sk50
of 8
,227
(0.7
)
At A
CC
P ri
sk93
of 6
,898
(1.5
)
AC
CP
5 A
mer
ican
Col
lege
of
Che
st P
hysi
cian
s; C
CU
5 c
riti
cal c
are
unit
; ESA
5 e
ryth
ropo
iesi
s-st
imul
atin
g ag
ent;
GU
5 g
enit
ouri
nary
; Hgb
5 h
emog
lobi
n; H
R 5
haz
ard
rati
o; H
RT
5 h
orm
one
repl
acem
ent t
hera
py; L
L 5
low
er li
mb;
MI 5
myo
card
ial i
nfar
ctio
n; N
ICU
5 n
eona
tal I
CU
; OC
5 o
ral c
ontr
acep
tive;
RA
M 5
ris
k as
sess
men
t mod
el; R
CT
5 r
ando
miz
ed c
ontr
olle
d tr
ial .
Oth
er R
AM
s ou
tlin
ed in
Spy
ropo
ulos
24 b
ut e
xclu
ded
from
the
abov
e ta
ble
incl
ude
one
by L
utz
et a
l, 25 w
hich
was
reg
arde
d as
“no
t tho
roug
hly
evid
ence
-bas
ed o
r va
lidat
ed.”
Ano
ther
RA
M th
at w
as
excl
uded
fro
m t
he t
able
was
tha
t by
Coh
en e
t al
, 12 w
hich
was
not
val
idat
ed a
nd a
ssum
ed t
hat
all r
isk
fact
ors
conf
erre
d a
sim
ilar
leve
l of
VT
E r
isk.
Ano
ther
stu
dy e
xclu
ded
was
a v
alid
atio
n st
udy
by
Bah
l et a
l, 26 w
hich
use
d th
e C
apri
ni R
AM
but
was
onl
y as
sess
ed in
sur
gica
l pat
ient
s.
a An
inte
rven
tion
stud
y by
Pia
zza
et a
l 27 u
sed
the
Kuc
her
RA
M t
o cl
assi
fy p
atie
nts
as a
t ri
sk a
nd t
here
fore
elig
ible
for
incl
usio
n. S
ubje
cts
incl
uded
wer
e th
ose
with
a r
isk
scor
e �
4 a
nd t
he s
tudy
fou
nd a
cu
mul
ativ
e ri
sk o
f VT
E o
f 3%
in 9
0 d
of fo
llow
-up.
b B
arba
r et
al 8 :
Not
incl
uded
in th
e Sp
yrop
oulo
s 24 r
evie
w . T
he s
tudy
val
idat
es th
e Pa
dua
Pred
ictio
n Sc
ore
in m
edic
al in
patie
nts.
c N
otes
on
Bar
bar
et a
l 8 RA
M: (
1) a
ctiv
e ca
ncer
: loc
al o
r di
stan
t m
etas
tase
s an
d/or
che
mot
hera
py o
r ra
diot
hera
py in
the
pre
viou
s 6
mo;
(2)
pri
or V
TE
: exc
lude
s su
perfi
cia
l vei
n th
rom
bosi
s; (
3) r
educ
ed
mob
ility
: bed
res
t with
bat
hroo
m p
rivi
lege
s fo
r at
leas
t 3 d
; (4)
rec
ent t
raum
a an
d/or
sur
gery
, � 1
mo;
(5) o
besi
ty: B
MI
� 3
0.
Tabl
e S3
—C
onti
nued
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

14© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S4
—[S
ecti
on 2
.3]
Evi
denc
e P
rofi l
e: S
hou
ld A
ntic
oagu
lant
Pro
phyl
axis
(L
MW
H, U
FH
, Fon
dapa
rinu
x) v
s P
lace
bo/
No
Tre
atm
ent
Be
Use
d in
Hos
pita
lize
d M
edic
al P
atie
nts?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
sE
ffec
t
Qua
lity
No.
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
a Im
prec
isio
nO
ther
C
onsi
dera
tions
Ant
icoa
gula
nt
Prop
hyla
xis
(LM
WH
, UF
H,
Fon
dapa
rinu
x)Pl
aceb
o/N
o Tr
eatm
ent b
Rel
ativ
e (9
5% C
I)A
bsol
ute
Sym
ptom
atic
DV
T (f
ollo
w-u
p 1-
14 d
) c
4 c R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous e
Non
e…
0.15
%R
R, 0
.47
(0.2
2-1)
1 fe
wer
per
1,
000
(fro
m
1 fe
wer
to
0 fe
wer
)
Mod
erat
eC
ritic
al
6.7%
e 34
few
er p
er
1,00
0 (f
rom
51
few
er to
0
few
er)
Non
fata
l PE
(fol
low
-up
1-22
d) f
6 c , g
Ran
dom
ized
tr
ials
No
seri
ous
limita
tions
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s e N
one
…0.
15%
RR
, 0.6
1 (0
.23-
1.67
) h 1
few
er p
er
1,00
0 (f
rom
1
few
er to
1
mor
e
Mod
erat
eC
ritic
al
3.9%
e 15
few
er p
er
1,00
0 (f
rom
30
few
er to
26
mor
e)
Maj
or b
leed
ing
(fol
low
-up
10-1
10 d
)
8 c , i
Ran
dom
ized
tr
ials
No
seri
ous
limita
tions
No
seri
ous
inco
nsis
tenc
y j N
o se
riou
s in
dire
ctne
ssSe
riou
s d N
one
25 o
f 4,3
01
(0.6
%)
19 o
f 4,3
04
(0.4
%)
OR
, 1.3
2 (0
.73-
2.37
)1
mor
e pe
r 1,
000
(fro
m
1 fe
wer
to
6 m
ore)
Mod
erat
eC
ritic
al
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

15© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
sE
ffec
t
Qua
lity
No.
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
a Im
prec
isio
nO
ther
C
onsi
dera
tions
Ant
icoa
gula
nt
Prop
hyla
xis
(LM
WH
, UF
H,
Fon
dapa
rinu
x)Pl
aceb
o/N
o Tr
eatm
ent b
Rel
ativ
e (9
5% C
I)A
bsol
ute
Mor
talit
y (f
ollo
w-u
p 1-
22 d
) f
5 c , k
Ran
dom
ized
tr
ials
No
seri
ous
limita
tions
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s l N
one
158
of 3
,676
(4
.3%
)16
5 of
3,
679
(4.5
%)
OR
, 0.9
7 (0
.79-
1.19
)1
few
er p
er
1,00
0 (f
rom
9
few
er to
8
mor
e)
Mod
erat
eC
ritic
al
Thr
ombo
cyto
peni
a (f
ollo
w-u
p 6-
21 d
)
3 m
Ran
dom
ized
tr
ials
No
seri
ous
limita
tions
No
seri
ous
inco
nsis
tenc
y n N
o se
riou
s in
dire
ctne
ssSe
riou
s d N
one
28 o
f 2,3
16
(1.2
%)
31 o
f 2,3
08
(1.3
%)
OR
, 0.9
1 (0
.54-
1.53
)1
few
er p
er
1,00
0 (f
rom
6
few
er to
7
mor
e)
Mod
erat
eC
ritic
al
Bib
liogr
aphy
: D
enta
li F,
Dou
ketis
JD
, G
iann
i M
, L
im W
, C
row
ther
MA
. M
eta-
anal
ysis
: A
ntic
oagu
lant
pro
phyl
axis
to
prev
ent
sym
ptom
atic
ven
ous
thro
mbo
embo
lism
in
hosp
italiz
ed m
edic
al p
atie
nts.
A
nn I
nter
n M
ed .
2007
;146
(4):2
78-2
88.
Llo
yd N
S, D
ouke
tis J
D,
Moi
nudd
in I
, L
im W
, C
row
ther
MA
. A
ntic
oagu
lant
pro
phyl
axis
to
prev
ent
asym
ptom
atic
dee
p ve
in t
hrom
bosi
s in
hos
pita
lized
med
-ic
al p
atie
nts:
A s
yste
mat
ic r
evie
w a
nd m
eta-
anal
ysis
. J T
hrom
b H
aem
ost .
2008
;6(3
):405
-414
. Alik
han
R, C
ohen
AT.
Hep
arin
for
the
pre
vent
ion
of v
enou
s th
rom
boem
bolis
m in
gen
eral
med
ical
pat
ient
s (e
xclu
ding
stro
ke a
nd m
yoca
rdia
l inf
arct
ion)
. Coc
hran
e D
atab
ase
Syst
Rev
. 200
9;(3
):CD
0037
47. U
FH
5 u
nfra
ctio
nate
d he
parin
; RR
5 re
lativ
e ris
k. S
ee T
able
S1
and
S2 le
gend
s for
exp
ansio
n of
oth
er a
bbre
viat
ions
. a F
or m
any
of th
e tr
ials
, the
rat
io o
f pat
ient
s sc
reen
ed to
pat
ient
s in
clud
ed w
as v
ery
high
(eg,
� 1
00),
rais
ing
som
e co
ncer
ns a
bout
the
over
all r
epre
sent
ativ
enes
s of
the
tria
l pop
ulat
ions
. b B
asel
ine
risk
for
DV
T a
nd P
E (l
ow-r
isk
and
high
-ris
k po
pula
tions
) are
der
ived
from
the
RA
M b
y B
arba
r et
al. 8 B
asel
ine
risk
for
mor
talit
y an
d bl
eedi
ng is
der
ived
from
the
cont
rol a
rm o
f med
ical
pat
ient
s in
a m
eta-
anal
ysis
(Den
tali
et a
l).
c Dat
a de
rive
d fr
om D
enta
li et
al.
Stud
ies
som
etim
es r
epor
ted
outc
omes
for
a lo
nger
dur
atio
n of
follo
w-u
p; h
owev
er, t
he D
enta
li et
al r
evie
w o
nly
incl
uded
out
com
es d
urin
g th
e on
-tre
atm
ent p
erio
d.
d We
will
con
side
r th
e pr
esen
ce o
f ser
ious
impr
ecis
ion
whe
n th
ere
are
, 3
00 e
vent
s in
tota
l (ev
ents
in tr
eatm
ent a
nd c
ontr
ol p
atie
nts)
sin
ce it
is d
iffi c
ult t
o ob
tain
pre
cise
est
imat
es in
the
abse
nce
of a
suf
-fi c
ient
num
ber
of o
utco
mes
. e T
his
estim
ate
of th
e ri
sk o
f the
eve
nt in
hig
h-ri
sk p
atie
nts
was
der
ived
from
the
Bar
bar
et a
l 8 stu
dy, w
hich
str
atifi
ed p
atie
nts
acco
rdin
g to
the
Padu
a Pr
edic
tion
Scor
e. T
he e
stim
ate
show
n re
fl ect
s th
e ri
sk
amon
g pa
tient
s w
ho d
id n
ot r
ecei
ve p
roph
ylax
is (s
ympt
omat
ic D
VT
5 1
9 of
238
, non
fata
l PE
5 1
1 of
283
, fat
al P
E 5
1 o
f 283
). f F
atal
PE
: sev
en R
CTs
, ant
icoa
gula
nts
(14
of 9
,902
[0.
1%],
cont
rol 3
9 of
10,
051
[0.4
%];
RR
, 0.4
1 [0
.22-
0.76
]; fo
r lo
w-r
isk
patie
nts:
two
few
er p
er 1
,000
(fr
om o
ne fe
wer
to th
ree
few
er)
and
for
high
-ris
k pa
tient
s tw
o fe
wer
per
1,0
00 (
from
one
few
er to
thre
e fe
wer
). In
four
of t
he tr
ials
with
ava
ilabl
e da
ta th
ere
was
fata
l ble
edin
g in
18
of 8
,249
(0.
22%
) in
the
prop
hyla
xis
grou
p vs
sev
en o
f 8,3
65 (
0.08
%)
in
the
plac
ebo
grou
p.
g The
Den
tali
et a
l rev
iew
did
not
sep
arat
e no
nfat
al a
nd fa
tal P
E; t
here
fore
, we
wen
t to
the
orig
inal
stu
dies
to fi
nd w
hich
had
rep
orte
d no
nfat
al e
vent
s on
ly o
r bo
th n
onfa
tal a
nd fa
tal e
vent
s.
h The
RR
repo
rted
resu
lts fr
om a
met
a-an
alys
is u
sing
the
Der
Sim
onia
n-L
aird
rand
om e
ffec
ts m
odel
. Thi
s mod
el w
as c
hose
n du
e to
the
num
ber o
f stu
dies
( . 3
) and
bec
ause
ther
e w
as n
ot a
sing
le st
udy
that
do
min
ated
the
met
a-an
alys
is.
i GI
blee
ding
and
intr
acra
nial
ble
edin
g w
ere
not r
outin
ely
repo
rted
sep
arat
ely
from
maj
or b
leed
ing
even
ts in
the
indi
vidu
al c
ompo
nent
stu
dies
of t
he D
enta
li et
al s
yste
mat
ic r
evie
w; h
owev
er, a
t lea
st o
ne
stud
y (C
ohen
et a
l 12 ) r
epor
ted
that
GI
blee
ding
eve
nts
acco
unte
d fo
r ze
ro o
f tw
o to
tal a
nd in
trac
rani
al b
leed
ing
even
ts a
ccou
nted
for
zero
of t
wo
tota
l maj
or b
leed
ing
even
ts.
j The
re w
as s
ome
hete
roge
neity
det
ecte
d am
ong
indi
vidu
al s
tudi
es; I
2 5 3
0%.
k Alth
ough
the
Den
tali
et a
l rev
iew
did
not
rep
ort
fata
l ble
edin
g, s
ome
of t
he c
ompo
nent
stu
dies
did
: tw
o of
nin
e bl
eedi
ng o
utco
mes
in t
he t
reat
men
t gr
oup
and
one
of t
hree
in t
he p
lace
bo g
roup
of
the
Lei
zoro
vicz
et a
l 20 s
tudy
wer
e fa
tal b
leed
ing
even
ts. T
here
wer
e no
fata
l ble
edin
g ev
ents
in th
e C
ohen
et a
l 12 s
tudy
(ze
ro o
f tw
o m
ajor
ble
edin
g ou
tcom
es).
One
of s
ix b
leed
ing
outc
omes
in th
e tr
eatm
ent
grou
p an
d ze
ro o
f fou
r in
the
plac
ebo
grou
p of
the
Sam
ama
et a
l 7 stu
dy w
ere
fata
l ble
edin
g ev
ents
. l S
ince
the
confi
den
ce in
terv
al r
ange
s fr
om a
red
uctio
n in
dea
ths
to a
n in
crea
se in
dea
ths,
we
are
not a
ssur
ed th
at th
ere
is tr
uly
no e
ffec
t. m D
ata
deri
ved
from
the
Alik
han
and
Coh
en r
evie
w.
n The
re w
as s
ome
hete
roge
neity
det
ecte
d am
ong
the
indi
vidu
al s
tudi
es; I
2 5 4
2%.
Tabl
e S4
—C
onti
nued
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

16© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S5
—E
ligi
bil
ity
Cri
teri
a fo
r R
CT
s of
LD
UH
vs
LM
WH
Thr
omb
opro
phyl
axis
in
Hos
pita
lize
d M
edic
al P
atie
nts
Stud
y/Ye
arIn
clus
ion
Cri
teri
aE
xclu
sion
Cri
teri
a
For
ette
and
Wol
mar
k 28 /1
995
Age
N/S
(mea
n ag
e: 8
3 y)
Prev
ious
red
uced
mob
ility
Rec
ent t
rans
ient
red
uced
mob
ility
Exi
sten
ce o
f pre
viou
s D
VT,
con
fi rm
ed b
y ec
ho D
oppl
er 4
8 h
prio
r to
incl
usio
n in
stu
dy
Hos
pita
lized
for
. 4
wk
Acu
te m
edic
al il
lnes
sPr
evio
us D
VT
(with
in la
st 6
mo)
Prev
ious
PE
(with
in la
st y
)
Seve
re a
rter
ial h
yper
tens
ion
Cer
ebra
l hem
orrh
age
with
in p
revi
ous
6 m
o or
any
neu
rosu
rgic
al
inte
rven
tion
Ren
al in
suffi
cien
cy
Seve
re li
ver
dise
ase
Surg
ical
inte
rven
tion
(non
orth
oped
ic 8
d; o
rtho
pedi
c 28
d)
Rec
eivi
ng a
spir
in, t
iclo
pidi
ne, a
ntiin
fl am
mat
orie
s, h
epar
inoi
d,
or v
itam
in K
Con
trai
ndic
atio
n to
hep
arin
, or
veno
grap
hic
or a
ngio
grap
hic
inve
stig
atio
ns
Lec
hler
et a
l, 29 P
RIM
E/1
996
Age
. 1
8 y
(mea
n ag
e: 7
4 �
13
y)B
leed
ing
diso
rder
Exp
ecte
d im
mob
iliza
tion
. 1
/2 d
aytim
e fo
r w
hole
stu
dy p
erio
d (7
d)
Thr
ombo
cyto
peni
a ( ,
100
,000
3 1
0 9 /L)
Hos
pita
lized
Hem
orrh
agic
str
oke
duri
ng th
e pr
eced
ing
4 w
k
Acu
te m
edic
al il
lnes
s pl
us �
1 a
dditi
onal
thro
mbo
embo
lic r
isk
fact
or ( .
60
y, m
alig
nanc
y, o
besi
ty, f
orm
er th
rom
boem
bolic
eve
nt,
card
iac
insu
ffi ci
ency
, par
esis
of t
he lo
wer
lim
bs, h
emip
legi
a,
para
pleg
ia, o
r se
vere
infe
ctio
n)
Hea
d tr
aum
a in
pre
viou
s 6
mo
End
ocar
ditis
Seve
re r
enal
dis
ease
or
rena
l ins
uffi c
ienc
y
Thr
ombo
embo
lism
Reg
iona
l ane
sthe
sia
Trea
tmen
t with
ant
icoa
gula
nts,
ant
ipla
tele
ts o
r N
SAID
s in
the
prec
edin
g 7
d
Preg
nanc
y an
d la
ctat
ion
Part
icip
atio
n in
clin
ical
tria
l in
prec
edin
g 6
wk
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
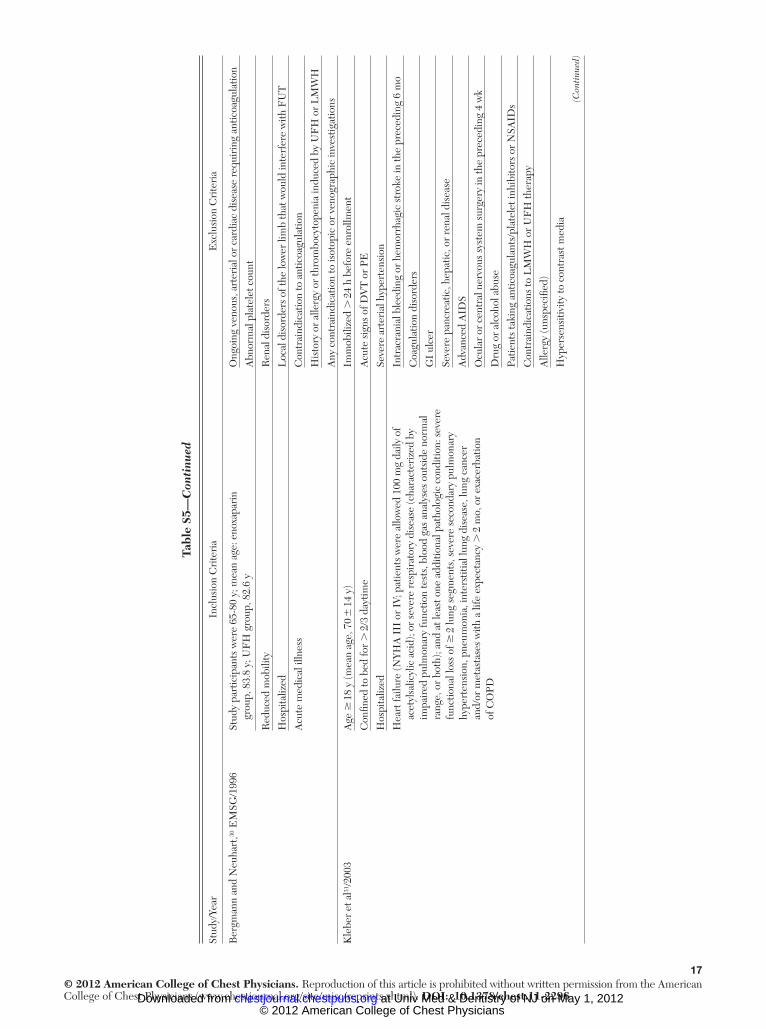
17© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arIn
clus
ion
Cri
teri
aE
xclu
sion
Cri
teri
a
Ber
gman
n an
d N
euha
rt, 30
EM
SG/1
996
Stud
y pa
rtic
ipan
ts w
ere
65-8
0 y;
mea
n ag
e: e
noxa
pari
n gr
oup,
83.
8 y;
UF
H g
roup
, 82.
6 y
Ong
oing
ven
ous,
art
eria
l or
card
iac
dise
ase
requ
irin
g an
ticoa
gula
tion
Abn
orm
al p
late
let c
ount
Red
uced
mob
ility
Ren
al d
isor
ders
Hos
pita
lized
Loc
al d
isor
ders
of t
he lo
wer
lim
b th
at w
ould
inte
rfer
e w
ith F
UT
Acu
te m
edic
al il
lnes
sC
ontr
aind
icat
ion
to a
ntic
oagu
latio
n
His
tory
or
alle
rgy
or th
rom
bocy
tope
nia
indu
ced
by U
FH
or
LM
WH
Any
con
trai
ndic
atio
n to
isot
opic
or
veno
grap
hic
inve
stig
atio
ns
Kle
ber
et a
l 31 /2
003
Age
� 1
8 y
(mea
n ag
e, 7
0 �
14
y)Im
mob
ilize
d .
24
h be
fore
enr
ollm
ent
Con
fi ned
to b
ed fo
r .
2/3
day
time
Acu
te s
igns
of D
VT
or
PE
Hos
pita
lized
Seve
re a
rter
ial h
yper
tens
ion
Hea
rt fa
ilure
(NYH
A I
II o
r IV
; pat
ient
s w
ere
allo
wed
100
mg
daily
of
acet
ylsa
licyl
ic a
cid)
; or
seve
re r
espi
rato
ry d
isea
se (c
hara
cter
ized
by
impa
ired
pul
mon
ary
func
tion
test
s, b
lood
gas
ana
lyse
s ou
tsid
e no
rmal
ra
nge,
or
both
); an
d at
leas
t one
add
ition
al p
atho
logi
c co
nditi
on: s
ever
e fu
nctio
nal l
oss
of �
2 lu
ng s
egm
ents
, sev
ere
seco
ndar
y pu
lmon
ary
hype
rten
sion
, pne
umon
ia, i
nter
stiti
al lu
ng d
isea
se, l
ung
canc
er
and/
or m
etas
tase
s w
ith a
life
exp
ecta
ncy
. 2
mo,
or
exac
erba
tion
of C
OPD
Intr
acra
nial
ble
edin
g or
hem
orrh
agic
str
oke
in th
e pr
eced
ing
6 m
o
Coa
gula
tion
diso
rder
s
GI
ulce
r
Seve
re p
ancr
eatic
, hep
atic
, or
rena
l dis
ease
Adv
ance
d A
IDS
Ocu
lar
or c
entr
al n
ervo
us s
yste
m s
urge
ry in
the
prec
edin
g 4
wk
Dru
g or
alc
ohol
abu
se
Patie
nts
taki
ng a
ntic
oagu
lant
s/pl
atel
et in
hibi
tors
or
NSA
IDs
Con
trai
ndic
atio
ns to
LM
WH
or
UF
H th
erap
y
Alle
rgy
(uns
peci
fi ed)
Hyp
erse
nsiti
vity
to c
ontr
ast m
edia
Tabl
e S5
—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

18© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arIn
clus
ion
Cri
teri
aE
xclu
sion
Cri
teri
a
Rei
ss e
t al, 32
CE
RT
IFY/
2010
Age
. 7
0 y
(mea
n �
SD
age
, 78.
8 �
6.3
y)
Imm
obili
zatio
n .
3 d
pri
or to
ran
dom
izat
ion
Sign
ifi ca
nt d
ecre
ase
in m
obili
ty (b
edri
dden
or
only
abl
e to
wal
k sh
ort d
ista
nces
) exp
ecte
d fo
r �
4 d
Imm
obili
zatio
n du
e to
cas
t or
frac
ture
Hos
pita
lized
A
cute
sym
ptom
atic
DV
T/P
E
Acu
te m
edic
al il
lnes
s (in
fect
ions
and
infe
stat
ions
, 28%
; car
diac
di
sord
ers,
22%
; res
pira
tory
, tho
raci
c, a
nd m
edia
stin
al
diso
rder
s, 1
7%; n
ervo
us s
yste
m d
isor
ders
, 7%
; and
so
fort
h)
Unc
ontr
olle
d hy
pert
ensi
on
Acu
te H
IT-I
I or
his
tory
of t
his
Hem
orrh
agic
str
oke
or in
trac
rani
al b
leed
ing
( , 1
2 m
o)
Acu
te n
onhe
mor
rhag
ic s
trok
e or
his
tory
of t
his
( , 3
mo)
Acu
te o
r on
goin
g in
trac
rani
al d
isea
se
Hig
h ri
sk o
f GI
blee
ding
Acu
te e
ndoc
ardi
tis
Kno
wn
activ
e re
tinop
athy
, or
intr
avitr
eal o
r ot
her
intr
aocu
lar
blee
ding
Seve
re s
epsi
s or
nee
d fo
r ve
ntila
tor
supp
ort (
cont
inuo
us p
ositi
ve a
irw
ay
pres
sure
, oxy
gen
mas
k, a
nd s
o fo
rth,
wer
e pe
rmitt
ed)
Seve
re r
enal
or
liver
dis
ease
Illn
ess
with
ver
y hi
gh a
cute
mor
talit
y ra
te ( .
30%
)
Spin
al o
r ep
idur
al a
nest
hesi
a or
lum
bar
punc
ture
with
in la
st 1
2 h
Exp
ecte
d to
und
ergo
maj
or s
urgi
cal/i
nvas
ive
proc
edur
e w
ithin
3
wk
follo
win
g ra
ndom
izat
ion
Rec
eive
d L
MW
H/h
epar
in fo
r .
48
h in
5 d
pri
or to
ran
dom
izat
ion
Indi
catio
ns fo
r an
ticoa
gula
tion
or th
rom
boly
sis
Life
exp
ecta
ncy
, 6
mo
FU
T 5
fi br
inog
en u
ptak
e; H
IT-I
I 5 h
epar
in-in
duce
d th
rom
bocy
tope
nia
type
2; L
DU
H 5
low
-dos
e un
frac
tiona
ted
hepa
rin;
NSA
IDs 5
ons
tero
idal
ant
iinfl a
mm
ator
y dr
ugs.
See
Tab
le S
1 an
d S2
lege
nds
for
expa
nsio
n of
oth
er a
bbre
viat
ions
.
Tabl
e S5
—C
onti
nued
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

19© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S6
—[S
ecti
on 2
.4]
Evi
denc
e P
rofi l
e: S
hou
ld A
ntic
oagu
lant
Pro
phyl
axis
Wit
h L
MW
H v
s U
FH
Be
Use
d in
Hos
pita
lize
d M
edic
al P
atie
nts?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
sE
ffec
t
Qua
lity
No.
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Oth
er
Con
sider
atio
ns
Ant
icoa
gula
nt
Prop
hyla
xis
With
LM
WH
UF
HR
elat
ive
(95%
CI)
Abs
olut
e
Sym
ptom
atic
DV
T (f
ollo
w-u
p, 1
-28
d)
5 a R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
Seri
ous b
Seri
ous c
Non
e…
0.33
%R
R, 0
.77
(0.5
0-1.
19)
1 fe
wer
per
1,0
00
(fro
m 2
few
er to
1 m
ore)
Low
Cri
tical
PE (f
ollo
w-u
p, 1
-28
d)
5 a R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
Seri
ous b
Seri
ous c
Non
e…
0.20
%R
R, 1
.00
(0.2
8-3.
59)
0 fe
wer
per
1,0
00
(fro
m 1
few
er to
5 m
ore)
Low
Cri
tical
Maj
or b
leed
ing
5 a , d R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous c
Non
e11
of 2
,795
(0.4
%)
26 o
f 2,8
02 (0
.9%
)R
R, 0
.48
(0.2
4-0.
99)
5 fe
wer
per
1,0
00
(fro
m 0
few
er to
7 fe
wer
)M
oder
ate
Cri
tical
Mor
talit
y
5 a , e R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous c
Non
e68
of 2
,795
(2.4
%)
77 o
f 2,8
05 (2
.7%
)R
R, 0
.89
(0.6
5-1.
23)
3 fe
wer
per
1,0
00
(fro
m 1
0 fe
wer
to 6
mor
e)M
oder
ate
Cri
tical
Hep
arin
-indu
ced
thro
mbo
cyto
peni
a
1R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous c , f
Rep
ortin
g bi
as g
1 of
1,6
24 (0
.06%
)2
of 1
,615
(0.1
2%)
RR
, 0.5
0 (0
.05-
5.48
)1
few
er p
er 1
,000
(f
rom
1 fe
wer
to 1
mor
e)L
owC
ritic
al
Bib
liogr
aphy
: A
likha
n R
, C
ohen
AT.
Hep
arin
for
the
pre
vent
ion
of v
enou
s th
rom
boem
bolis
m i
n ge
nera
l m
edic
al p
atie
nts
(exc
ludi
ng s
trok
e an
d m
yoca
rdia
l in
farc
tion)
. C
ochr
ane
Dat
abas
e Sy
st R
ev .
2009
;(3):C
D00
3747
. Rei
ss H
, Haa
s S, T
ebbe
U, e
t al.
A ra
ndom
ized
, dou
ble-
blin
d st
udy
of c
erto
pari
n vs
unf
ract
iona
ted
hepa
rin
to p
reve
nt v
enou
s thr
ombo
embo
lic e
vent
s in
acut
ely
ill, n
on-s
urgi
cal p
atie
nts:
C
ER
TIF
Y St
udy.
J T
hrom
b H
aem
ost.
2009
;8(6
):120
9-12
15. S
ee T
able
S1,
S2,
and
S5
lege
nds
for
expa
nsio
n of
abb
revi
atio
ns.
a One
stu
dy a
sses
sed
UF
H b
id; f
our
stud
ies
asse
ssed
UF
H ti
d.
b The
RR
is d
eriv
ed fr
om a
mix
of s
ympt
omat
ic a
nd a
sym
ptom
atic
eve
nts
and
the
base
line
risk
(ris
k w
ith U
FH
) is
deri
ved
from
sym
ptom
atic
eve
nts
from
the
Rie
ss e
t al s
tudy
. c W
e w
ill c
onsi
der
the
pres
ence
of s
erio
us im
prec
isio
n w
hen
ther
e ar
e ,
300
eve
nts
in to
tal (
even
ts in
trea
tmen
t and
con
trol
pat
ient
s), s
ince
it is
diffi
cul
t to
obta
in p
reci
se e
stim
ates
in th
e ab
senc
e of
a s
uf-
fi cie
nt n
umbe
r of
out
com
es.
d GI
blee
ding
and
intr
acra
nial
ble
edin
g w
ere
not r
outin
ely
repo
rted
sep
arat
ely
from
maj
or b
leed
ing
even
ts in
the
indi
vidu
al c
ompo
nent
stu
dies
of t
he A
likha
n an
d C
ohen
sys
tem
atic
rev
iew
; how
ever
, one
st
udy
(Lec
hler
et a
l 29 ) r
epor
ted
that
GI
blee
ding
eve
nts
acco
unte
d fo
r ni
ne o
f 30
tota
l maj
or b
leed
ing
even
ts, b
ut n
umbe
r of
eve
nts
was
not
rep
orte
d se
para
tely
by
trea
tmen
t gro
up.
e Fat
al b
leed
ing
even
ts n
ot r
epor
ted
sepa
rate
ly.
f Onl
y on
e st
udy
(CE
RT
IFY
tria
l) re
port
ed th
is o
utco
me
and
ther
e w
ere
only
thre
e oc
curr
ence
s of
thro
mbo
cyto
peni
a ov
eral
l; th
eref
ore,
the
sugg
estio
n of
a p
rote
ctiv
e ef
fect
of L
MW
H v
s U
FH
is n
ot w
ell
supp
orte
d.
g Sin
ce o
nly
one
stud
y re
port
ed th
is o
utco
me,
it is
pos
sibl
e th
at th
ere
was
sel
ectiv
e re
port
ing
of th
is o
utco
me,
whi
ch w
ould
indi
cate
pub
licat
ion
bias
.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
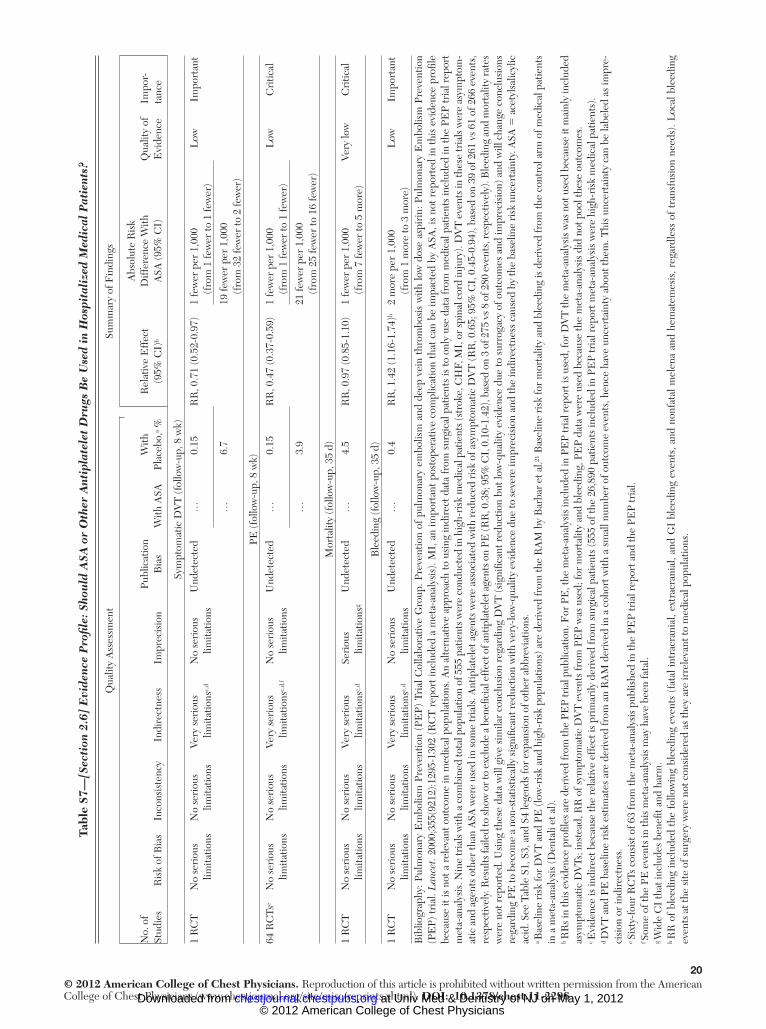
20© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S7
— [S
ecti
on 2
.6]
Evi
denc
e P
rofi l
e: S
hou
ld A
SA o
r O
ther
Ant
ipla
tele
t D
rugs
Be
Use
d in
Hos
pita
lize
d M
edic
al P
atie
nts?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
No.
of
Stud
ies
Ris
k of
Bia
sIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Publ
icat
ion
Bia
sW
ith A
SAW
ith
Plac
ebo,
a %R
elat
ive
Eff
ect
(95%
CI)
b
Abs
olut
e R
isk
Diff
eren
ce W
ith
ASA
(95%
CI)
Qua
lity
of
Evi
denc
eIm
por-
tanc
e
Sym
ptom
atic
DV
T (f
ollo
w-u
p, 8
wk)
1 R
CT
No
seri
ous
limita
tions
No
seri
ous
limita
tions
Very
ser
ious
lim
itatio
ns c , d
No
seri
ous
limita
tions
Und
etec
ted
…0.
15R
R, 0
.71
(0.5
2-0.
97)
1 fe
wer
per
1,0
00
(fro
m 1
few
er to
1 fe
wer
)L
owIm
port
ant
…6.
719
few
er p
er 1
,000
(f
rom
32
few
er to
2 fe
wer
)
PE (f
ollo
w-u
p, 8
wk)
64 R
CTs
e N
o se
riou
s lim
itatio
nsN
o se
riou
s lim
itatio
nsVe
ry s
erio
us
limita
tions
c , d , f N
o se
riou
s lim
itatio
nsU
ndet
ecte
d…
0.15
RR
, 0.4
7 (0
.37-
0.59
)1
few
er p
er 1
,000
(f
rom
1 fe
wer
to 1
few
er)
Low
Cri
tical
…3.
921
few
er p
er 1
,000
(f
rom
25
few
er to
16
few
er)
Mor
talit
y (f
ollo
w-u
p, 3
5 d)
1 R
CT
No
seri
ous
limita
tions
No
seri
ous
limita
tions
Very
ser
ious
lim
itatio
ns c , d
Seri
ous
limita
tions
g U
ndet
ecte
d…
4.5
RR
, 0.9
7 (0
.85-
1.10
)1
few
er p
er 1
,000
(f
rom
7 fe
wer
to 5
mor
e)Ve
ry lo
wC
ritic
al
Ble
edin
g (f
ollo
w-u
p, 3
5 d)
1 R
CT
No
seri
ous
limita
tions
No
seri
ous
limita
tions
Very
ser
ious
lim
itatio
ns c , d
No
seri
ous
limita
tions
Und
etec
ted
…0.
4R
R, 1
.42
(1.1
6-1.
74) h
2 m
ore
per
1,00
0 (f
rom
1 m
ore
to 3
mor
e)L
owIm
port
ant
Bib
liogr
aphy
: Pul
mon
ary
Em
bolis
m P
reve
ntio
n (P
EP)
Tri
al C
olla
bora
tive
Gro
up. P
reve
ntio
n of
pul
mon
ary
embo
lism
and
dee
p ve
in t
hrom
bosi
s w
ith lo
w d
ose
aspi
rin:
Pul
mon
ary
Em
bolis
m P
reve
ntio
n (P
EP)
tria
l. L
ance
t. 20
00;3
55(9
212)
:129
5-13
02 (
RC
T r
epor
t inc
lude
d a
met
a-an
alys
is).
MI,
an
impo
rtan
t pos
tope
rativ
e co
mpl
icat
ion
that
can
be
impa
cted
by
ASA
, is
not r
epor
ted
in th
is e
vide
nce
profi
le
beca
use
it is
not
a r
elev
ant o
utco
me
in m
edic
al p
opul
atio
ns. A
n al
tern
ativ
e ap
proa
ch to
usi
ng in
dire
ct d
ata
from
sur
gica
l pat
ient
s is
to o
nly
use
data
from
med
ical
pat
ient
s in
clud
ed in
the
PEP
tria
l rep
ort
met
a-an
alys
is. N
ine
tria
ls w
ith a
com
bine
d to
tal p
opul
atio
n of
555
pat
ient
s wer
e co
nduc
ted
in h
igh-
risk
med
ical
pat
ient
s (st
roke
, CH
F, M
I, o
r spi
nal c
ord
inju
ry).
DV
T e
vent
s in
thes
e tr
ials
wer
e as
ympt
om-
atic
and
age
nts
othe
r th
an A
SA w
ere
used
in s
ome
tria
ls. A
ntip
late
let a
gent
s w
ere
asso
ciat
ed w
ith r
educ
ed r
isk
of a
sym
ptom
atic
DV
T (R
R, 0
.65;
95%
CI,
0.4
5-0.
94),
base
d on
39
of 2
61 v
s 61
of 2
66 e
vent
s,
resp
ectiv
ely.
Res
ults
faile
d to
show
or t
o ex
clud
e a
bene
fi cia
l eff
ect o
f ant
ipla
tele
t age
nts o
n PE
(RR
, 0.3
8; 9
5% C
I, 0
.10-
1.42
), ba
sed
on 3
of 2
75 v
s 8 o
f 280
eve
nts,
resp
ectiv
ely)
. Ble
edin
g an
d m
orta
lity
rate
s w
ere
not r
epor
ted.
Usi
ng th
ese
data
will
giv
e si
mila
r co
nclu
sion
reg
ardi
ng D
VT
(sig
nifi c
ant r
educ
tion
but l
ow-q
ualit
y ev
iden
ce d
ue to
sur
roga
cy o
f out
com
es a
nd im
prec
isio
n) a
nd w
ill c
hang
e co
nclu
sion
s re
gard
ing
PE to
bec
ome
a no
n-st
atis
tical
ly s
igni
fi can
t red
uctio
n w
ith v
ery-
low
-qua
lity
evid
ence
due
to s
ever
e im
prec
isio
n an
d th
e in
dire
ctne
ss c
ause
d by
the
base
line
risk
unc
erta
inty
. ASA
5 a
cety
lsal
icyl
ic
acid
. See
Tab
le S
1, S
3, a
nd S
4 le
gend
s fo
r ex
pans
ion
of o
ther
abb
revi
atio
ns.
a Bas
elin
e ri
sk fo
r D
VT
and
PE
(low
-ris
k an
d hi
gh-r
isk
popu
latio
ns) a
re d
eriv
ed fr
om th
e R
AM
by
Bar
bar
et a
l. 21 B
asel
ine
risk
for
mor
talit
y an
d bl
eedi
ng is
der
ived
from
the
cont
rol a
rm o
f med
ical
pat
ient
s in
a m
eta-
anal
ysis
(Den
tali
et a
l).
b RR
s in
this
evi
denc
e pr
ofi le
s ar
e de
rive
d fr
om th
e PE
P tr
ial p
ublic
atio
n. F
or P
E, t
he m
eta-
anal
ysis
incl
uded
in P
EP
tria
l rep
ort i
s us
ed, f
or D
VT
the
met
a-an
alys
is w
as n
ot u
sed
beca
use
it m
ainl
y in
clud
ed
asym
ptom
atic
DV
Ts; i
nste
ad, R
R o
f sym
ptom
atic
DV
T e
vent
s fr
om P
EP
was
use
d; fo
r m
orta
lity
and
blee
ding
, PE
P da
ta w
ere
used
bec
ause
the
met
a-an
alys
is d
id n
ot p
ool t
hese
out
com
es.
c Evi
denc
e is
indi
rect
bec
ause
the
rela
tive
effe
ct is
pri
mar
ily d
eriv
ed fr
om s
urgi
cal p
atie
nts
(555
of t
he 2
6,89
0 pa
tient
s in
clud
ed in
PE
P tr
ial r
epor
t met
a-an
alys
is w
ere
high
-ris
k m
edic
al p
atie
nts)
. d D
VT
and
PE
bas
elin
e ri
sk e
stim
ates
are
der
ived
from
an
RA
M d
eriv
ed in
a c
ohor
t with
a s
mal
l num
ber
of o
utco
me
even
ts, h
ence
hav
e un
cert
aint
y ab
out t
hem
. Thi
s un
cert
aint
y ca
n be
labe
led
as im
pre-
cisi
on o
r in
dire
ctne
ss.
e Six
ty-f
our
RC
Ts c
onsi
st o
f 63
from
the
met
a-an
alys
is p
ublis
hed
in th
e PE
P tr
ial r
epor
t and
the
PEP
tria
l. f S
ome
of th
e PE
eve
nts
in th
is m
eta-
anal
ysis
may
hav
e be
en fa
tal.
g Wid
e C
I th
at in
clud
es b
enefi
t an
d ha
rm.
h RR
of
blee
ding
incl
uded
the
fol
low
ing
blee
ding
eve
nts
(fat
al in
trac
rani
al, e
xtra
cran
ial,
and
GI
blee
ding
eve
nts,
and
non
fata
l mel
ena
and
hem
atem
esis
, reg
ardl
ess
of t
rans
fusi
on n
eeds
). L
ocal
ble
edin
g ev
ents
at t
he s
ite o
f sur
gery
wer
e no
t con
side
red
as th
ey a
re ir
rele
vant
to m
edic
al p
opul
atio
ns.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

21© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S8
—[S
ecti
on 2
.7.1
] E
vide
nce
Pro
fi le:
Sho
uld
GC
S vs
No
GC
S B
e U
sed
in H
ospi
tali
zed
Med
ical
Pat
ient
s? a
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
No.
of P
atie
nts
Eff
ect
No.
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
isten
cyIn
dire
ctne
ssIm
prec
isio
nO
ther
C
onsid
erat
ions
GC
SC
ontr
ol a
Rel
ativ
e (9
5% C
I)A
bsol
ute
Qua
lity
Sym
ptom
atic
DV
T (p
roxi
mal
or d
ista
l) (f
ollo
w-u
p, 1
-30
d; c
onfi r
med
on
imag
ing)
1 b R
ando
miz
ed
tr
ials
No
seri
ous
lim
itatio
nsN
o se
riou
s
inco
nsist
ency
No
seri
ous
in
dire
ctne
ssSe
riou
s c N
one
…0.
15%
RR
, 0.9
1
(0.6
3-1.
29)
1 fe
wer
per
1,0
00 (f
rom
1
few
er to
1 m
ore)
Mod
erat
eIm
port
ant
6.7%
6 fe
wer
per
1,0
00 (f
rom
25
few
er to
19
mor
e)
PE (f
ollo
w-u
p, 1
-30
d; c
onfi r
med
on
imag
ing
or a
utop
sy)
1 b R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
isten
cyN
o se
riou
s in
dire
ctne
ssSe
riou
s c N
one
…0.
15%
RR
, 0.6
5 (0
.33-
1.31
)1
few
er p
er 1
,000
(fro
m
1 fe
wer
to 1
mor
e)L
owC
ritic
al
3.9%
14 fe
wer
per
1,0
00 (f
rom
26
few
er to
12
mor
e)
Mor
talit
y (f
ollo
w-u
p, 3
0 d)
2R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous c
Non
e13
1 of
1,3
21
(9.9
%)
4.5%
RR
, 1.0
6 (0
.94-
1.20
) d 3
mor
e pe
r 1,
000
(fro
m
3 fe
wer
to 9
mor
e)M
oder
ate
Cri
tical
Skin
bre
aks/
ulce
rs/b
liste
rs/s
kin
necr
osis
(fol
low
-up,
1-3
0 d;
cas
e-no
te r
evie
w)
1 b R
ando
miz
ed
tria
lsSe
riou
s e N
o se
riou
s in
cons
iste
ncy
Seri
ous
indi
rect
ness
b Se
riou
s c N
one
64 o
f 1,2
56
(5.1
%)
16 o
f 1,2
62
(1.3
%)
RR
, 4.0
2 (2
.34-
6.91
)38
mor
e pe
r 1,
000
(fro
m
17 m
ore
to 7
5 m
ore)
Very
low
Impo
rtan
t
Low
er li
mb
isch
emia
/am
puta
tion
(fol
low
-up,
1-3
0 d;
cas
e-no
te r
evie
w)
1 b R
ando
miz
ed
tria
lsSe
riou
s e N
o se
riou
s in
cons
iste
ncy
No
serio
us
indi
rect
ness
Very
se
riou
s c N
one
7 of
1,2
56
(0.6
%)
2 of
1,2
62
(0.2
%)
RR
, 3.5
2 (0
.73-
16.9
0)4
mor
e pe
r 1,
000
(fro
m
0 fe
wer
to 2
5 m
ore)
Very
low
Impo
rtan
t
Bib
liogr
aphy
: Kie
rkeg
aard
A, N
orgr
en L
. Gra
duat
ed c
ompr
essi
on s
tock
ings
in t
he p
reve
ntio
n of
dee
p ve
in t
hrom
bosi
s in
pat
ient
s w
ith a
cute
myo
card
ial i
nfar
ctio
n. E
ur H
eart
J . 1
993;
14(1
0):1
365-
1368
. M
uir
KW
, Wat
t A
, Bax
ter
G, G
ross
et D
G, L
ees
KR
. Ran
dom
ized
tri
al o
f gr
aded
com
pres
sion
sto
ckin
g fo
r pr
even
tion
of d
eep-
vein
thr
ombo
sis
afte
r ac
ute
stro
ke. Q
JM . 2
000;
93(6
):359
-364
. Den
nis
M,
Sand
erco
ck P
A, R
eid
J, e
t al
. The
CL
OT
S Tr
ials
Col
labo
ratio
n. E
ffec
tiven
ess
of t
high
-leng
th g
radu
ated
com
pres
sion
sto
ckin
gs t
o re
duce
the
ris
k of
dee
p ve
in t
hrom
bosi
s af
ter
stro
ke (
CL
OT
S tr
ial 1
): a
mul
ticen
ter,
rand
omiz
ed c
ontr
olle
d tr
ial.
Lan
cet .
2009
;373
(967
9):1
958-
1965
. GC
S 5
gra
duat
ed c
ompr
essi
on s
tock
ings
. See
Tab
les
S1 a
nd S
4 le
gend
s fo
r ex
pans
ion
of o
ther
abb
revi
atio
ns.
a Bas
elin
e ri
sk fo
r D
VT
and
PE
(lo
w-r
isk
and
high
-ris
k po
pula
tion
s) a
re d
eriv
ed fr
om th
e R
AM
by
Bar
bar
et a
l. 21 B
asel
ine
risk
for
mor
talit
y an
d bl
eedi
ng is
der
ived
from
the
cont
rol a
rm o
f med
ical
pa
tien
ts in
a m
eta-
anal
ysis
(Den
tali
et a
l). B
asel
ine
risk
for
low
er le
g is
chem
ia a
nd s
kin
brea
ks (d
eriv
ed fr
om th
e co
ntro
l arm
s of
CL
OT
S tr
ial 1
). b D
ata
from
CL
OT
S tr
ial 1
(str
oke
patie
nts)
; hen
ce, w
hen
resu
lts a
pplie
d to
med
ical
pat
ient
s, th
e qu
ality
of e
vide
nce
shou
ld b
e do
wng
rade
d du
e to
indi
rect
ness
c F
or t
he o
utco
mes
of
DV
T a
nd P
E, i
mpr
ecis
ion
refe
rs o
nly
to t
he h
igh-
risk
pat
ient
s (e
stim
ates
in lo
w-r
isk
patie
nts
are
asso
ciat
ed w
ith v
ery
smal
l abs
olut
e di
ffer
ence
tha
t is
fai
rly
prec
ise)
. Im
prec
isio
n ot
herw
ise
is d
ue to
wid
e C
I th
at in
clud
es a
ppre
ciab
le b
enefi
t an
d ha
rm a
nd o
vera
ll sm
all n
umbe
r of
eve
nts.
d T
he e
ffec
t est
imat
e sh
own
here
res
ults
from
a fi
xed-
effe
cts
met
a-an
alys
is o
f tw
o tr
ials
of g
radu
ated
com
pres
sion
sto
ckin
g fo
r pr
even
tion
of D
VT
in h
ospi
taliz
ed m
edic
al p
atie
nts.
The
Mui
r tr
ial r
epor
ted
deat
h in
nin
e of
65
patie
nts w
ith a
cute
stro
ke in
the
trea
tmen
t gro
up a
nd fo
ur o
f 32
patie
nts i
n th
e co
ntro
l gro
up. T
he C
LO
TS
tria
l 1 re
port
ed d
eath
in 1
22 o
f 1,2
56 p
atie
nts w
ith a
cute
stro
ke in
the
trea
tmen
t gr
oup
and
110
of 1
,262
pat
ient
s in
the
cont
rol g
roup
. Sto
ckin
gs w
ere
used
for
1 w
eek
in tw
o st
udie
s (K
ierk
egaa
rd a
nd N
orgr
en; M
uir
et a
l) an
d un
til th
e pa
tient
was
inde
pend
ently
mob
ile, w
as d
isch
arge
d,
refu
sed
to w
ear t
hem
, or d
evel
oped
skin
pro
blem
s in
one
stud
y (D
enni
s et a
l). T
he la
rges
t of t
he st
udie
s, th
e C
LO
TS1
Tri
al c
ondu
cted
in 2
,518
hos
pita
lized
stro
ke p
atie
nts,
was
the
only
one
to p
rovi
de d
ata
on a
dver
se e
ffec
ts o
f gra
duat
ed c
ompr
essi
on s
tock
ings
. e A
sses
smen
t of o
utco
mes
was
bas
ed o
n ca
se-n
ote
revi
ew a
nd w
as n
ot b
linde
d to
trea
tmen
t allo
catio
n.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

22© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S9
—[S
ecti
on 2
.7.2
] E
vide
nce
Pro
fi le:
Sho
uld
IP
C B
e U
sed
in H
ospi
tali
zed
Non
surg
ical
Pat
ient
s? S
etti
ngs:
Inp
atie
nts
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
No.
of P
atie
nts
Eff
ect
No
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Oth
er
Con
side
ratio
nsIP
CC
ontr
ol, a %
Rel
ativ
e (9
5% C
I)A
bsol
ute
Qua
lity
of
Evi
denc
e
Sym
ptom
atic
DV
T (f
ollo
w-u
p, 3
0 d)
19
Ran
dom
ized
tr
ials
No
seri
ous
limita
tions
No
seri
ous
inco
nsis
tenc
ySe
riou
s in
dire
ctne
ss b
No
seri
ous
impr
ecis
ion
Non
e…
0.15
RR
, 0.4
3 (0
.32-
0.58
)1
few
er p
er 1
,000
(f
rom
1 fe
wer
to 1
few
er)
Mod
erat
eIm
port
ant
6.7
38 fe
wer
per
1,0
00
(fro
m 4
6 fe
wer
to 2
8 fe
wer
)
PE (f
ollo
w-u
p, 3
0 d)
8R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
Seri
ous
indi
rect
ness
c Se
riou
s im
prec
isio
n d N
one
…0.
15R
R, 0
.82
(0.4
1-1.
62)
1 fe
wer
per
1,0
00 (f
rom
1
few
er to
1 m
ore)
Low
Cri
tical
3.9
7 fe
wer
per
1,0
00 (f
rom
23
few
er to
24
mor
e)
Mor
talit
y (f
ollo
w-u
p, 3
0 d)
2R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
Seri
ous
indi
rect
ness
e Se
riou
s im
prec
isio
n d N
one
…4.
5R
R, 1
.03
(0.4
2-2.
57)
1 m
ore
per
1,00
0 (f
rom
76
few
er to
71
mor
e)L
owC
ritic
al
Skin
com
plic
atio
ns (b
reak
s, u
lcer
s, b
liste
rs, a
nd n
ecro
sis)
, not
rep
orte
d in
any
pop
ulat
ion g
0…
……
……
Non
e…
……
…Im
port
ant
Bib
liogr
aphy
: Sys
tem
atic
rev
iew
in s
urgi
cal p
atie
nts:
Rod
eric
k P,
Fer
ris
G, W
ilson
K, e
t al.
Tow
ard
evid
ence
-bas
ed g
uide
lines
for
the
prev
entio
n of
ven
ous
thro
mbo
embo
lism
: sys
tem
atic
rev
iew
s of
mec
hani
cal m
etho
ds,
oral
ant
icoa
gula
tion,
dex
tran
and
reg
iona
l ane
sthe
sia
as t
hrom
bopr
ophy
laxi
s. H
ealth
Tec
hnol
Ass
ess.
200
5;9(
49):1
-78.
Sys
tem
atic
rev
iew
in s
trok
e pa
tient
s: N
acca
rato
M, C
hiod
o G
rand
i F, D
enni
s M
, San
derc
ock
PA.
Phys
ical
met
hods
for
prev
entin
g de
ep v
ein
thro
mbo
sis
in s
trok
e. C
ochr
ane
Dat
abas
e Sy
st R
ev. 2
010;
(8):
CD
0019
22. B
arba
r S,
Nov
enta
F, R
osse
tto
V, e
t al.
A r
isk
asse
ssm
ent m
odel
for
the
iden
tifi c
atio
n of
hos
pita
lized
m
edic
al p
atie
nts
at r
isk
for
veno
us th
rom
boem
bolis
m: T
he P
adua
Pre
dict
ion
Scor
e. J
Thr
omb
Hae
mos
t . 20
10;8
(11)
:245
0-24
57. D
enta
li F,
Dou
ketis
JD
, Gia
nni M
, Lim
W, C
row
ther
MA
. Met
a-an
alys
is: A
ntic
oagu
lant
pr
ophy
laxi
s to
pre
vent
sym
ptom
atic
ven
ous
thro
mbo
embo
lism
in
hosp
italiz
ed m
edic
al p
atie
nts.
Ann
Int
erna
l M
ed.
2007
;146
(4):2
78-2
88.
IPC
5 in
term
itten
t pn
eum
atic
com
pres
sion
. Se
e Ta
bles
S1,
S3,
and
S4
for
expa
nsio
n of
oth
er a
bbre
viat
ions
. a B
asel
ine
risk
for D
VT
and
PE
(low
-ris
k an
d hi
gh-r
isk
popu
latio
ns) a
re d
eriv
ed fr
om th
e R
AM
by
Bar
bar e
t al.
Bas
elin
e ri
sk fo
r mor
talit
y is
der
ived
from
the
cont
rol a
rm o
f med
ical
pat
ient
s in
a m
eta-
anal
ysis
(Den
tali
et a
l).
b RR
for
DV
T is
der
ived
from
sur
gica
l pat
ient
s (R
oder
ick
et a
l). A
noth
er e
lem
ent o
f ind
irec
tnes
s is
that
DV
T in
thes
e su
rgic
al p
atie
nts
was
pri
mar
ily a
sym
ptom
atic
DV
T a
s as
cert
aine
d by
sys
tem
atic
Im
agin
g te
sts.
RR
fo
r pr
oxim
al a
sym
ptom
atic
DV
T w
as s
imila
r (0
.52;
95%
CI,
0.3
7-0.
73).
RR
dat
a ar
e pr
esen
ted
for
IPC
use
d as
mon
othe
rapy
bec
ause
thi
s is
mos
t re
leva
nt t
o th
e w
ay I
PCs
are
used
in m
edic
al p
atie
nts
(ie, i
n pa
tient
s w
ho c
anno
t rec
eive
ant
icoa
gula
tion)
. If I
PCs
are
used
alo
ne o
r as
adj
unct
to a
ntic
oagu
lant
/ant
ipla
tele
t the
rapy
, RR
is 0
.49
(0.3
7-0.
63),
whi
ch le
ads
to a
bsol
ute
effe
ct p
er 1
,000
pat
ient
s of
one
few
er (
from
one
few
er to
on
e fe
wer
) in
low
-ris
k pa
tient
s an
d 32
few
er (f
rom
42
few
er to
25
few
er) i
n hi
gh-r
isk
patie
nts.
c R
R fo
r PE
is d
eriv
ed fr
om s
urgi
cal p
atie
nts
(Rod
eric
k et
al).
RR
dat
a ar
e pr
esen
ted
for
IPC
use
d as
mon
othe
rapy
bec
ause
this
is m
ost r
elev
ant t
o th
e w
ay I
PCs
are
used
in m
edic
al p
atie
nts
(ie, i
n pa
tient
s w
ho c
anno
t re
ceiv
e an
ticoa
gula
tion)
. If I
PCs
are
used
alo
ne o
r as
adj
unct
to a
ntic
oagu
lant
/ant
ipla
tele
t the
rapy
, RR
is 0
.77
(0.4
1-1.
43).
Thi
s do
es n
ot c
hang
e th
e co
nclu
sion
s of
this
evi
denc
e pr
ofi le
. d C
I in
clud
es n
eglig
ible
eff
ect,
appr
ecia
ble
bene
fi t, a
nd a
ppre
ciab
le h
arm
. e R
R is
der
ived
from
RC
Ts in
str
oke
(incl
udin
g on
e st
udy
of p
atie
nts
with
hem
orrh
agic
str
oke)
. RC
Ts o
f IPC
s in
oth
er p
opul
atio
ns d
id n
ot m
easu
re o
r re
port
mor
talit
y.
f Est
imat
es fo
r sk
in c
ompl
icat
ions
in m
edic
al p
atie
nts
usin
g IP
C a
re n
ot a
vaila
ble.
Dat
a fr
om g
radu
ated
com
pres
sion
sto
ckin
gs (s
ectio
n 2.
3) m
ay b
e in
dire
ctly
con
side
red.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

23© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
0 —E
xten
ded-
Du
rati
on P
roph
ylax
is i
n H
ospi
tali
zed
Med
ical
Pat
ient
s
Stud
y/Ye
arTi
tle, D
esig
nPa
tient
Typ
esE
xclu
ded
Patie
nts
Inte
rven
tion
Con
trol
Out
com
esR
esul
ts a
Len
gth
of
Fol
low
-up
Pote
ntia
l for
Bia
s
Hul
l et a
l 33 /2
010
Para
llel R
CT;
N
5 6
,085
Acu
tely
ill m
edic
al
patie
nts,
� 4
0 y
with
a li
fe
expe
ctan
cy o
f at
leas
t 6 m
o w
ith
rece
ntly
red
uced
m
obili
ty fo
r up
to
3 d
, defi
ned
as
req
uiri
ng
tota
l bed
res
t or
bein
g se
dent
ary
with
(lev
el 2
) or
with
out (
leve
l 1)
bath
room
pr
ivile
ges
Evi
denc
e of
an
activ
e bl
eedi
ng
diso
rder
Subc
utan
eous
en
oxap
arin
, 40
mg/
d fo
r 28
� 4
d
Plac
ebo
for
28 �
4 d
VT
E (c
ompo
site
of
sym
ptom
atic
pr
oxim
al D
VT,
as
ympt
omat
ic
prox
imal
DV
T
dete
cted
on
man
dato
ry b
ilate
ral
com
pres
sion
ul
tras
ound
at e
nd
of d
oubl
e-bl
ind
trea
tmen
t per
iod,
sy
mpt
omat
ic P
E,
or fa
tal P
E) d
urin
g do
uble
-blin
d tr
eatm
ent p
erio
d
VT
E a
t 28
d6
mo
Did
not
use
IT
T
anal
ysis
: –F
or s
afet
y, o
nly
incl
uded
thos
e w
ho h
as a
t lea
st
one
dose
of s
tudy
dr
ug (n
5 5
,963
) – F
or e
ffi ca
cy, o
nly
incl
uded
thos
e w
ho h
ad a
t lea
st
one
dose
of
stud
y dr
ug a
nd
had
an e
valu
able
ul
tras
onog
ram
(n
5 4
,995
)
E
: 61
of 2
,485
For
VT
E:
Aft
er in
itial
op
en-la
bel,
subc
utan
eous
en
oxap
arin
, 40
mg/
d fo
r 10
� 4
d
P:
100
of 2
,510
28 �
4 d
Sym
ptom
atic
prox
imal
DV
T90
� 1
0 d
E
: 5 o
f 2,4
85F
or d
eath
:
Maj
or s
urge
ry
with
in th
e pr
evio
us 3
mo
P:
20
of 2
,510
28 �
4 d
Aft
er in
itial
op
en-la
bel,
subc
utan
eous
en
oxap
arin
, 40
mg/
d fo
r 10
� 4
d
Fat
al P
E
90 �
10
d
E
: 0 o
f 2,4
85
P:
1 o
f 2,5
10
180
� 1
0 d
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

24© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arTi
tle, D
esig
nPa
tient
Typ
esE
xclu
ded
Patie
nts
Inte
rven
tion
Con
trol
Out
com
esR
esul
ts a
Len
gth
of
Fol
low
-up
Pote
ntia
l for
Bia
s
VT
E a
t 90
dC
onfl i
ct o
f int
eres
t: fu
nder
invo
lved
in
dat
a m
anag
emen
t, st
atis
tical
an
alys
is, a
nd
prep
arat
ion
of
the
artic
le fo
r pu
blic
atio
n
Spin
al o
r ep
idur
al
anal
gesi
a or
lu
mba
r pu
nctu
re
with
in th
e pr
evio
us 2
4 h
E
: 65
of 2
,485
P:
105
of 2
,510
Mor
talit
y di
d no
t si
gnifi
cant
ly
diff
er a
t 30,
90
, or
180
d K
now
n hy
pers
ensi
tivity
to
UF
H, L
MW
H,
or p
ork-
deri
ved
prod
ucts
Maj
or b
leed
ing
Did
not
rep
ort
num
ber
of
patie
nts
scre
ened
fo
r in
clus
ion
VT
E in
cide
nce
thro
ugh
3 m
o (d
ay 9
0 �
10)
E
: 25
of 2
,975
(4
intr
acra
nial
; 1
fata
l) H
isto
ry o
f he
pari
n-in
duce
d th
rom
bocy
tope
nia
or th
rom
bosi
s
Post
hoc
sub
grou
p an
alys
es
Mor
talit
y at
1 m
o (d
ay 2
8 � 4)
, 3 m
o (d
ay 9
0 �
10)
, an
d 6
mo
(day
18
0 �
10)
P:
10
of 2
,988
(0
intr
acra
nial
; 0
fata
l)
Cha
nge
in
elig
ibili
ty c
rite
ria
part
way
thro
ugh
the
tria
l and
“d
ata-
driv
en”
Tota
l ble
edin
g
E
: 186
of 2
,975
F
ollo
win
g an
am
endm
ent t
o th
e el
igib
ility
cr
iteri
a, p
atie
nts
with
leve
l 2
imm
obili
ty w
ere
requ
ired
to h
ave
at le
ast 1
VT
E
risk
fact
or
Tabl
e S1
0—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
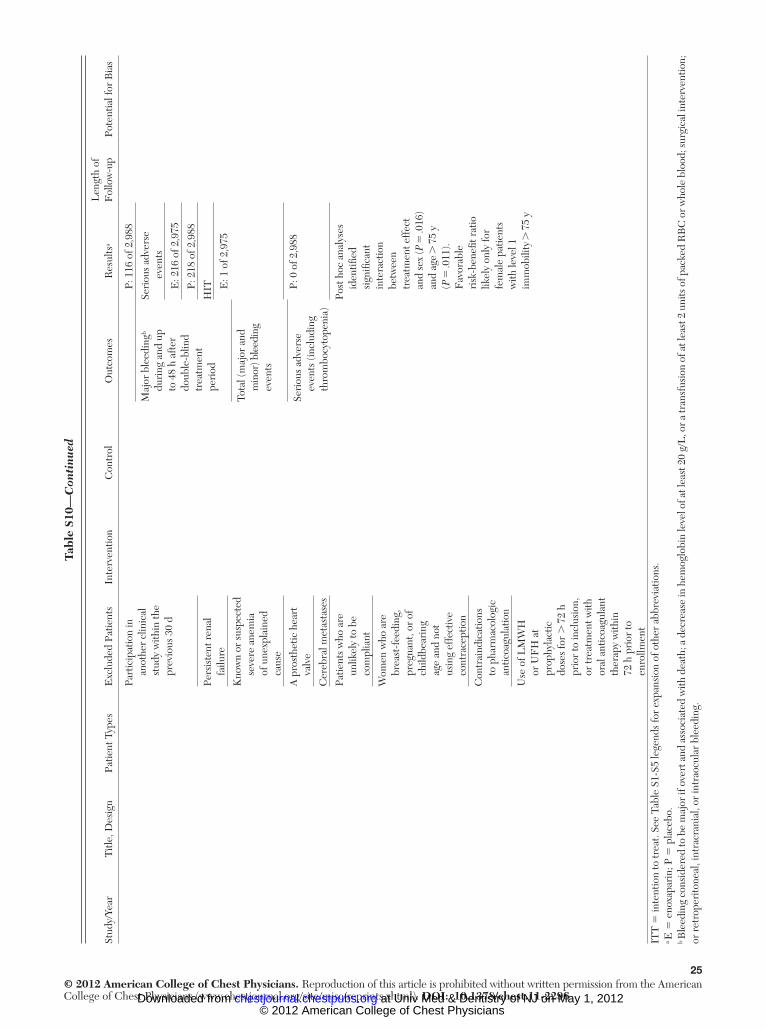
25© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arTi
tle, D
esig
nPa
tient
Typ
esE
xclu
ded
Patie
nts
Inte
rven
tion
Con
trol
Out
com
esR
esul
ts a
Len
gth
of
Fol
low
-up
Pote
ntia
l for
Bia
s
Part
icip
atio
n in
an
othe
r cl
inic
al
stud
y w
ithin
the
prev
ious
30
d
P:
116
of 2
,988
Maj
or b
leed
ing b
duri
ng a
nd u
p to
48
h af
ter
doub
le-b
lind
trea
tmen
t pe
riod
Seri
ous
adve
rse
ev
ents
E
: 216
of 2
,975
P:
218
of 2
,988
Pers
iste
nt r
enal
fa
ilure
HIT
E
: 1 o
f 2,9
75
Kno
wn
or s
uspe
cted
se
vere
ane
mia
of
une
xpla
ined
ca
use
Tota
l (m
ajor
and
m
inor
) ble
edin
g ev
ents
A p
rost
hetic
hea
rt
valv
e
P: 0
of 2
,988
Se
riou
s ad
vers
e ev
ents
(inc
ludi
ng
thro
mbo
cyto
peni
a)
Cer
ebra
l met
asta
ses
Patie
nts
who
are
un
likel
y to
be
com
plia
nt
Post
hoc
ana
lyse
s id
entifi
ed
sign
ifi ca
nt
inte
ract
ion
betw
een
trea
tmen
t eff
ect
and
sex
( P 5
.016
) an
d ag
e .
75
y ( P
5 .0
11).
Fav
orab
le
risk
-ben
efi t
ratio
lik
ely
only
for
fem
ale
patie
nts
with
leve
l 1
imm
obili
ty .
75
y
Wom
en w
ho a
re
brea
st-f
eedi
ng,
preg
nant
, or
of
child
bear
ing
age
and
not
usin
g ef
fect
ive
cont
race
ptio
n
Con
trai
ndic
atio
ns
to p
harm
acol
ogic
an
ticoa
gula
tion
Use
of L
MW
H
or U
FH
at
prop
hyla
ctic
do
ses
for
. 7
2 h
prio
r to
incl
usio
n,
or tr
eatm
ent w
ith
oral
ant
icoa
gula
nt
ther
apy
with
in
72 h
pri
or to
en
rollm
ent
ITT
5 in
tent
ion
to tr
eat.
See
Tabl
e S1
-S5
lege
nds
for
expa
nsio
n of
oth
er a
bbre
viat
ions
. a E
5 e
noxa
pari
n; P
5 p
lace
bo.
b Ble
edin
g co
nsid
ered
to b
e m
ajor
if o
vert
and
ass
ocia
ted
with
dea
th; a
dec
reas
e in
hem
oglo
bin
leve
l of a
t lea
st 2
0 g/
L, o
r a tr
ansf
usio
n of
at l
east
2 u
nits
of p
acke
d R
BC
or w
hole
blo
od; s
urgi
cal i
nter
vent
ion;
or
ret
rope
rito
neal
, int
racr
ania
l, or
intr
aocu
lar
blee
ding
.
Tabl
e S1
0—C
onti
nued
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
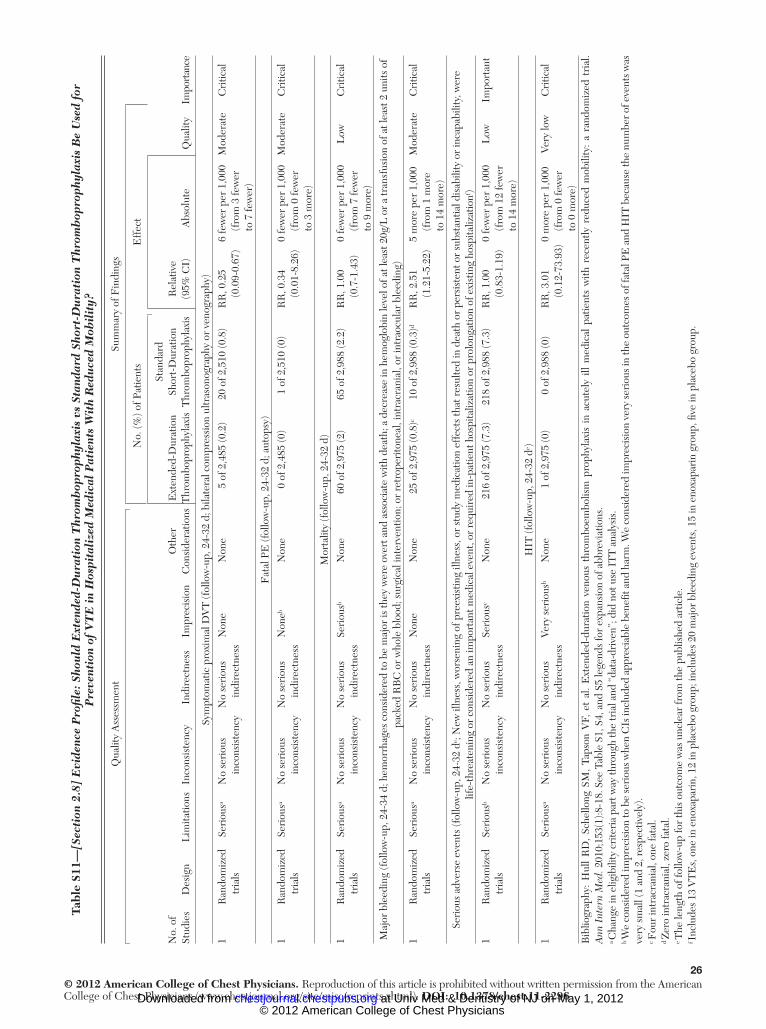
26© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
1 —[S
ecti
on 2
.8]
Evi
denc
e P
rofi l
e: S
hou
ld E
xten
ded-
Du
rati
on T
hrom
bop
roph
ylax
is v
s St
anda
rd S
hort
-Du
rati
on T
hrom
bop
roph
ylax
is B
e U
sed
for
Pre
vent
ion
of V
TE
in
Hos
pita
lize
d M
edic
al P
atie
nts
Wit
h R
edu
ced
Mob
ilit
y?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. (%
) of P
atie
nts
Eff
ect
No.
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Oth
er
Con
side
ratio
nsE
xten
ded-
Dur
atio
n T
hrom
bopr
ophy
laxi
s
Stan
dard
Sh
ort-
Dur
atio
n T
hrom
bopr
ophy
laxi
sR
elat
ive
(95%
CI)
Abs
olut
e Q
ualit
y
Sym
ptom
atic
pro
xim
al D
VT
(fol
low
-up,
24-
32 d
; bila
tera
l com
pres
sion
ultr
ason
ogra
phy
or v
enog
raph
y)
1R
ando
miz
ed
tria
lsSe
riou
s a N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Non
eN
one
5 of
2,4
85 (0
.2)
20 o
f 2,5
10 (0
.8)
RR
, 0.2
5 (0
.09-
0.67
)6
few
er p
er 1
,000
(f
rom
3 fe
wer
to
7 fe
wer
)
Mod
erat
eC
ritic
al
Fat
al P
E (f
ollo
w-u
p, 2
4-32
d; a
utop
sy)
1R
ando
miz
ed
tria
lsSe
riou
s a N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Non
e b N
one
0 of
2,4
85 (0
)1
of 2
,510
(0)
RR
, 0.3
4 (0
.01-
8.26
)0
few
er p
er 1
,000
(f
rom
0 fe
wer
to
3 m
ore)
Mod
erat
eC
ritic
al
Mor
talit
y (f
ollo
w-u
p, 2
4-32
d)
1R
ando
miz
ed
tria
lsSe
riou
s a N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous b
Non
e60
of 2
,975
(2)
65 o
f 2,9
88 (2
.2)
RR
, 1.0
0 (0
.7-1
.43)
0 fe
wer
per
1,0
00
(fro
m 7
few
er
to 9
mor
e)
Low
Cri
tical
Maj
or b
leed
ing
(fol
low
-up,
24-
34 d
; hem
orrh
ages
con
side
red
to b
e m
ajor
is th
ey w
ere
over
t and
ass
ocia
te w
ith d
eath
; a d
ecre
ase
in h
emog
lobi
n le
vel o
f at l
east
20g
/L o
r a
tran
sfus
ion
of a
t lea
st 2
uni
ts o
f pa
cked
RB
C o
r w
hole
blo
od; s
urgi
cal i
nter
vent
ion;
or
retr
oper
itone
al, i
ntra
cran
ial,
or in
trao
cula
r bl
eedi
ng)
1R
ando
miz
ed
tria
lsSe
riou
s a N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Non
eN
one
25 o
f 2,9
75 (0
.8) c
10 o
f 2,9
88 (0
.3) d
RR
, 2.5
1 (1
.21-
5.22
)5
mor
e pe
r 1,
000
(fro
m 1
mor
e to
14
mor
e)
Mod
erat
eC
ritic
al
Seri
ous
adve
rse
even
ts (f
ollo
w-u
p, 2
4-32
d e ;
New
illn
ess,
wor
seni
ng o
f pre
exis
ting
illne
ss, o
r st
udy
med
icat
ion
effe
cts
that
res
ulte
d in
dea
th o
r pe
rsis
tent
or
subs
tant
ial d
isab
ility
or
inca
pabi
lity,
wer
e lif
e-th
reat
enin
g or
con
side
red
an im
port
ant m
edic
al e
vent
, or
requ
ired
in-p
atie
nt h
ospi
taliz
atio
n or
pro
long
atio
n of
exi
stin
g ho
spita
lizat
ion f )
1R
ando
miz
ed
tria
lsSe
riou
s b N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous c
Non
e21
6 of
2,9
75 (7
.3)
218
of 2
,988
(7.3
)R
R, 1
.00
(0.8
3-1.
19)
0 fe
wer
per
1,0
00
(fro
m 1
2 fe
wer
to
14
mor
e)
Low
Impo
rtan
t
HIT
(fol
low
-up,
24-
32 d
e )
1R
ando
miz
ed
tria
lsSe
riou
s a N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Very
ser
ious
b N
one
1 of
2,9
75 (0
)0
of 2
,988
(0)
RR
, 3.0
1 (0
.12-
73.9
3)0
mor
e pe
r 1,
000
(fro
m 0
few
er
to 0
mor
e)
Very
low
Cri
tical
Bib
liogr
aphy
: H
ull
RD
, Sc
hello
ng S
M,
Taps
on V
F, e
t al
. E
xten
ded-
dura
tion
veno
us t
hrom
boem
bolis
m p
roph
ylax
is i
n ac
utel
y ill
med
ical
pat
ient
s w
ith r
ecen
tly r
educ
ed m
obili
ty:
a ra
ndom
ized
tri
al.
Ann
Int
ern
Med
. 201
0;15
3(1)
:8-1
8. S
ee T
able
S1,
S4,
and
S5
lege
nds
for
expa
nsio
n of
abb
revi
atio
ns.
a Cha
nge
in e
ligib
ility
cri
teri
a pa
rt w
ay th
roug
h th
e tr
ial a
nd “
data
-dri
ven”
; did
not
use
IT
T a
naly
sis.
b W
e co
nsid
ered
impr
ecis
ion
to b
e se
riou
s whe
n C
Is in
clud
ed a
ppre
ciab
le b
enefi
t an
d ha
rm. W
e co
nsid
ered
impr
ecis
ion
very
seri
ous i
n th
e ou
tcom
es o
f fat
al P
E a
nd H
IT b
ecau
se th
e nu
mbe
r of e
vent
s was
ve
ry s
mal
l (1
and
2, r
espe
ctiv
ely)
. c F
our
intr
acra
nial
, one
fata
l. d Z
ero
intr
acra
nial
, zer
o fa
tal.
e The
leng
th o
f fol
low
-up
for
this
out
com
e w
as u
ncle
ar fr
om th
e pu
blis
hed
artic
le.
f Inc
lude
s 13
VT
Es,
one
in e
noxa
pari
n, 1
2 in
pla
cebo
gro
up; i
nclu
des
20 m
ajor
ble
edin
g ev
ents
, 15
in e
noxa
pari
n gr
oup,
fi ve
in p
lace
bo g
roup
.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

27© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
2 —P
rogn
osti
c F
acto
rs A
ssoc
iate
d W
ith
VT
E i
n IC
U P
atie
nts
Stud
y/Ye
arTy
pe o
f Stu
dyPa
rtic
ipan
tsIn
terv
entio
nO
utco
mes
Fol
low
-up
Res
ults
Com
men
ts
Stud
ies
usin
g m
ultiv
aria
ble
anal
ysis
Shor
r et
al 34
/200
9M
ultic
ente
r R
CT
(X
PRE
SS)
1,93
5 se
psis
pat
ient
s re
ceiv
ing
DA
AL
MW
H (E
noxa
pari
n 40
mg
SC o
d), U
FH
5,
000
Inte
rnat
iona
l U
nits
SC
bid
or
plac
ebo
duri
ng D
AA
infu
sion
pe
riod
DV
T s
cree
ning
with
ul
tras
ound
be
twee
n da
ys 4
-6
28 d
RR
old
er p
atie
nts
(age
. 7
5 y)
, 1.
92 (9
5% C
I, 1
.22-
3.04
; P
5 .0
04);
hist
ory
of V
TE
, 4.
6 (2
.17-
9.79
, P ,
.001
); m
ultiv
aria
ble
anal
ysis
: his
tory
of
VT
E; O
R, 3
.66
(95%
CI,
1.
77-7
.56;
P 5
.005
)
Mul
tivar
iabl
e an
alys
is
adju
sted
for
age,
re
cent
sur
gery
, his
tory
of
VT
E, b
asel
ine
hepa
rin,
use
of
vaso
pres
sors
, nee
d fo
r m
echa
nica
l ven
tilat
ion
Coo
k et
al, 35
D
IRE
CT
/200
8M
ultic
ente
r pr
ospe
ctiv
e co
hort
138
med
ical
-sur
gica
l IC
U p
atie
nts
with
re
nal i
nsuf
fi cie
ncy
Dal
tepa
rin
5,00
0 In
tern
atio
nal U
nits
SC
od
DV
T s
cree
ning
with
ul
tras
ound
on
adm
issi
on a
nd
twic
e w
eekl
y
Up
to 3
0 d
Ele
vate
d A
PAC
HE
II
scor
e;
HR
for
10-u
nit i
ncre
ase,
2.
25 (9
5% C
I, 1
.03-
4.91
)
Inde
pend
ent v
aria
bles
: ba
selin
e V
TE
ris
k fa
ctor
s, a t
rans
fusi
on,
CV
C, i
notr
ope
or
vaso
pres
sor,
mec
hani
cal
vent
ilatio
n
Coo
k et
al, 36
V
ET
EC
/200
5Si
ngle
-cen
ter
pros
pect
ive
coho
rt
261
med
ical
-sur
gica
l IC
U p
atie
nts
Dal
tepa
rin
5,00
0 In
tern
atio
nal U
nits
SC
od
DV
T s
cree
ning
w
ith u
ltras
ound
on
adm
issi
on a
nd
twic
e w
eekl
y
Pers
onal
or
fam
ily h
isto
ry o
f V
TE
, HR
, 4.0
(95%
CI,
1.
5-10
.3);
end-
stag
e re
nal
failu
re, H
R, 3
.7%
(1.2
%-1
1.1%
); pl
atel
et tr
ansf
usio
n, H
R, 3
.2%
(1
.2%
-8.4
%);
vaso
pres
sor
use,
H
R, 2
.8%
(1.1
%-7
.2%
)
Inde
pend
ent v
aria
bles
: ba
selin
e V
TE
ris
k fa
ctor
s, e
xpos
ures
w
ithin
2 w
k an
d du
ring
IC
U a
dmis
sion
, da
ily I
CU
exp
osur
es b
Ibra
him
et a
l 37 /2
002
Pros
pect
ive
coho
rt11
0 m
edic
al I
CU
pa
tient
s re
quir
ing
mec
hani
cal
vent
ilatio
n .
7 d
Scre
enin
g du
plex
ul
tras
ound
of u
pper
an
d lo
wer
ext
rem
ities
ev
ery
7 d
DV
T, m
orta
lity;
als
o ho
spita
l and
IC
U
LO
S, d
urat
ion
of
mec
hani
cal
vent
ilatio
n
N/S
(whi
le
in I
CU
)D
urat
ion
of C
VC
pla
cem
ent
(1-d
incr
emen
ts),
RR
of
DV
T, 1
.04
(95%
CI,
1.
03-1
.05;
P ,
.001
)
Cox
pro
port
iona
l haz
ards
m
odel
Kol
lef 38
/199
8Si
ngle
-cen
ter
pros
pect
ive
coho
rt
323
med
ical
IC
U
patie
nts
Sem
iqua
ntita
tive
d-di
mer
VT
E (n
ot
syst
emat
ical
ly
scre
ened
)
N/S
(whi
le
in I
CU
)In
crea
sed
d-di
mer
inde
pend
ently
as
soci
ated
with
vas
cula
r th
rom
bosi
s, a
djus
ted
OR
, 5.0
6 (9
5% C
I, 2
.96-
8.65
; P 5
.003
)
Mul
tiple
logi
stic
re
gres
sion
Stud
ies
that
use
d un
ivar
iate
ana
lysi
s to
ide
ntify
ris
k fa
ctor
s fo
r V
TE
wer
e no
t in
clud
ed i
n th
e ta
ble.
34,3
9 A
PAC
HE
5 A
cute
Phy
siol
ogy
and
Chr
onic
Hea
lth E
valu
atio
n; C
VC
5 ce
ntra
l ve
nous
cat
hete
r;
DA
A 5
dro
trec
ogin
alfa
(act
ivat
ed);
LO
S 5
leng
th o
f sta
y; o
d 5
onc
e da
ily; S
C 5
subc
utan
eous
. See
Tab
le S
2, S
4, S
5, a
nd S
7 le
gend
s fo
r ex
pans
ion
of o
ther
abb
revi
atio
ns.
a Bas
elin
e ri
sk fa
ctor
s: p
erso
nal o
r fa
mily
his
tory
, kno
wn
thro
mbo
phili
c di
sord
er, c
urre
nt o
r re
cent
(with
in 5
y) m
alig
nanc
y.
b Bas
elin
e V
TE
ris
k fa
ctor
s: a
ge; g
ende
r; B
MI;
adm
issi
on d
iagn
osis
; med
ical
or
surg
ical
sta
tus;
APA
CH
E I
I sc
ore;
pre
-IC
U lo
catio
n; p
erso
nal o
r fa
mily
his
tory
of V
TE
; kno
wn
thro
mbo
phili
c di
sord
er; a
ctiv
e or
pre
viou
s m
alig
nanc
y; c
hron
ic c
ardi
ac, r
espi
rato
ry, r
enal
, or
CN
S di
seas
e; s
mok
ing;
hos
pita
lizat
ion
with
in 6
mo;
sur
gery
with
in 1
2 w
k; b
ed r
est o
f � 3
d in
pri
or 4
wk;
act
ivity
leve
l. E
xpos
ures
with
in 2
wk
befo
re I
CU
adm
issi
on a
nd d
aily
ther
eaft
er in
clud
ed C
VC
s, s
ubcu
tane
ous
UF
H, U
FH
for
cath
eter
pat
ency
, the
rape
utic
UF
H o
r L
MW
H, w
arfa
rin
ASA
, NSA
IDS,
ant
ipla
tele
t dru
gs, v
itam
in K
, tra
nsfu
sion
(R
BC
, pla
sma,
pla
tele
ts, c
ryop
reci
pita
te).
Dai
ly I
CU
var
iabl
es in
clud
ed v
asop
ress
ors,
mec
hani
cal v
entil
atio
n, p
ositi
ve e
nd-e
xpir
ator
y pr
essu
re, d
ialy
sis,
sur
gica
l int
erve
ntio
ns, M
ultip
le O
rgan
Dys
func
tion
scor
e, h
emog
lobi
n, p
late
let c
ount
, IN
R, a
PTT,
IV
sed
ativ
es/o
piat
es/p
aral
ytic
s.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

28© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
3 — D
escr
ipti
on o
f St
udi
es o
f P
roph
ylac
tic
Ant
icoa
gula
tion
in
ICU
Pat
ient
s
Stud
y/Ye
arTy
pe o
f Stu
dyPa
rtic
ipan
tsIn
terv
entio
nO
utco
mes
Fol
low
-up
Res
ults
Com
men
ts
UF
H v
s Pl
aceb
o
Cad
e 40 /1
982
Sing
le-c
ente
r R
CT
119
med
ical
-sur
gica
l IC
U p
atie
nts
UF
H 5
,000
Int
erna
tiona
l U
nits
SC
bid
vs
plac
ebo
DV
T d
etec
ted
by
fi bri
noge
n le
g sc
anni
ng fo
r m
edia
n 7
d (4
-10
d)
Not
spe
cifi e
d (w
hile
in I
CU
)D
VT:
UF
H, 1
3%
vs p
lace
bo 2
9%;
P ,
.05
57%
Dis
tal D
VT,
1/
3 bi
late
ral,
1/5
prox
imal
LM
WH
vs
Plac
ebo
Fra
isse
et a
l 8 /200
0M
ultic
ente
r, do
uble
-blin
d R
CT
223
mec
hani
cally
ve
ntila
ted
patie
nts
with
CO
PD
LM
WH
(nad
ropa
rin
� 6
5 In
tern
atio
nal U
nits
/kg
SC o
d) v
s pl
aceb
o
DV
T (d
etec
ted
by
veno
grap
hy b
efor
e da
y 21
), bl
eedi
ng,
mor
talit
y
Up
to 2
1 d
DV
T: L
MW
H, 1
3 of
84
(15.
5%) v
s pl
aceb
o,
24 o
f 85
(28.
2%);
P 5
.045
Wee
kly
ultr
asou
nd;
prox
imal
DV
T in
3
of 1
3 L
MW
H
and
7 of
24
plac
ebo
Maj
or b
leed
ing:
LM
WH
, 6
of 1
08 (5
.5%
) vs
pla
cebo
, 3 o
f 11
3 (2
.7%
); P
5 .2
8
Mor
talit
y: L
MW
H, 8
of
84 (9
.5%
) vs
plac
ebo,
8
of 8
5 (9
.4%
) (C
onti
nued
)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

29© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arTy
pe o
f Stu
dyPa
rtic
ipan
tsIn
terv
entio
nO
utco
mes
Fol
low
-up
Res
ults
Com
men
ts
LM
WH
vs
UF
H
PRO
TE
CT
in
vest
igat
ors 41
/201
1M
ultic
ente
r, do
uble
-blin
d R
CT
3,76
4 cr
itica
lly il
l pa
tient
s ex
pect
ed
to r
emai
n in
IC
U
for
� 3
d
LM
WH
(dal
tepa
rin
5,00
0 In
tern
atio
nal U
nits
SC
od)
vs
UF
H 5
,000
In
tern
atio
nal U
nits
SC
bid
Prox
imal
DV
T (d
etec
ted
by c
ompr
essi
on
ultr
asou
nd �
3 d
af
ter
rand
omiz
atio
n;
com
pres
sion
ultr
asou
nd
perf
orm
ed w
ithin
2
d of
adm
issi
on, t
wic
e w
eekl
y, a
nd a
s cl
inic
ally
in
dica
ted)
; sec
onda
ry
outc
omes
: any
DV
T,
PE, V
TE
, dea
th, m
ajor
bl
eedi
ng, H
IT
Whi
le in
IC
UPr
oxim
al D
VT:
LM
WH
, 96
of 1
,873
(5.1
%)
vs U
FH
, 109
of
1,87
3 (5
.8%
); H
R,
0.92
(95%
CI,
0.
68-1
.23;
P 5
.57)
All
DV
T o
utco
mes
w
ere
scre
ened
for
by u
ltras
ound
; PE
w
as n
ot s
cree
ned
for,
but w
as c
linic
ally
su
spec
ted
and
clas
sifi e
d as
pos
sibl
e,
prob
able
, or
defi n
ite
Any
DV
T: L
MW
H,
138
of 1
,873
(7.4
%)
vs U
FH
, 161
of
1,87
3 (8
.6%
); H
R, 0
.93
(95%
CI,
0.
72-1
.19;
P 5
.54)
PE: L
MW
H, 2
4 of
1,
873
(1.3
%) v
s U
FH
, 43
of 1
,873
(2.3
%);
HR
, 0.5
1 (9
5% C
I,
0.30
-0.8
8; P
5 .0
1)
VT
E: L
MW
H, 1
54 o
f 1,
873
(8.2
%) v
s U
FH
, 18
6 of
1,8
73 (9
.9%
); H
R, 0
.87
(95%
CI,
0.
69-1
.10;
P 5
.24)
Dea
th (I
CU
): L
MW
H,
284
of 1
,873
(15.
2%)
vs U
FH
, 304
of
1,87
3 (1
6.2%
); H
R, 0
.97
(95%
CI,
0.
82-1
.15;
P 5
.71)
Maj
or b
leed
ing:
LM
WH
, 10
3 of
1,8
73 (5
.5%
), U
FH
, 105
of
1,87
3 (5
.6%
)
HIT
: LM
WH
, 5 o
f 1,8
73
(0.3
%) v
s U
FH
, 12
of
1,87
3 (0
.6%
)
Tabl
e S1
3—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

30© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arTy
pe o
f Stu
dyPa
rtic
ipan
tsIn
terv
entio
nO
utco
mes
Fol
low
-up
Res
ults
Com
men
ts
Shor
r et
al 34
/200
9 M
ultic
ente
r R
CT
(XPR
ESS
)1,
935
seps
is p
atie
nts
rece
ivin
g D
AA
LM
WH
(eno
xapa
rin
40 m
g SC
od)
, UF
H 5
000
Inte
rnat
iona
l Uni
ts
SC b
id o
r pl
aceb
o du
ring
DA
A in
fusi
on
peri
od
DV
T (d
etec
ted
by
com
pres
sion
ul
tras
ound
bet
wee
n da
ys 4
-6)
28 d
VT
E: L
MW
H, 2
3 of
47
8 (5
.9%
), U
FH
, 26
of 4
98 (6
.3%
), pl
aceb
o, 5
6 of
95
9 (5
.8%
)
Mos
t DV
T c
linic
ally
si
lent
PE: L
MW
H, 4
of
478
(0.4
%),
UF
H, 2
of
498
(0.4
%),
plac
ebo,
8
of 9
59 (0
.8%
)
De
et a
l 42 /2
010
Sing
le-c
ente
r R
CT
N 5
156
, cri
tical
ly
ill s
urgi
cal p
atie
nts
unde
rgoi
ng m
ajor
su
rger
y
LM
WH
(eno
xapa
rin
40 m
g od
) vs
UF
H 5
,000
In
tern
atio
nal U
nits
SC
bid
DV
T (d
etec
ted
with
D
oppl
er b
etw
een
post
oper
ativ
e da
ys
5-7
and
clin
ical
su
spic
ion)
, ble
edin
g,
mor
talit
y
� 6
wk
DV
T: L
MW
H, 1
of
81 (1
.2%
) vs
UF
H,
2 of
75
(2.7
%),
Cau
se o
f dea
th n
ot
VT
E o
r bl
eedi
ng
Maj
or b
leed
ing:
LM
WH
, 1
of 8
1 (1
.2%
) vs
UF
H,
2 of
75
(2.7
%)
No
scre
enin
g ul
tras
ound
, D
oppl
er o
nly
Mor
talit
y: L
MW
H, 9
of
81 (1
1%) v
s 6
of 7
5 (8
%)
Sing
le-a
rm c
linic
al s
tudi
es u
sing
LM
WH
/UF
H
Dou
ketis
et a
l 43 /2
008
Mul
ticen
ter,
sin
gle-
arm
cl
inic
al tr
ial
138
criti
cally
ill
med
ical
-sur
gica
l pa
tient
s w
ith s
ever
e re
nal i
nsuf
fi cie
ncy
(CrC
l , 3
0 m
L/m
in)
LM
WH
(dal
tepa
rin
5,00
0 In
tern
atio
nal U
nits
SC
od)
un
til I
CU
dis
char
ge o
r 30
d
DV
T (d
etec
ted
by
twic
e-w
eekl
y sc
reen
ing
ultr
asou
nd),
blee
ding
Unt
il IC
U
disc
harg
e or
up
to 3
0 d
DV
T: 7
of 1
38 (5
.1%
; 95
% C
I, 2
.5%
-10.
1%)
All
DV
T a
sym
ptom
atic
an
d pr
oxim
al; 6
of
7 as
soci
ated
with
fe
mor
al c
athe
ters
M
ajor
ble
edin
g: 1
0 of
13
8 (7
.2%
; 95%
CI,
4.
0%-1
2.8%
)
Rab
bat e
t al 44
/200
5Si
ngle
-cen
ter
pros
pect
ive
coho
rt19
cri
tical
ly il
l m
edic
al-s
urgi
cal
patie
nts
with
C
rCl .
0 m
L/m
in
LM
WH
(dal
tepa
rin
5,00
0 In
tern
atio
nal U
nits
SC
od)
VT
E (t
wic
e w
eekl
y sc
reen
ing
ultr
asou
nd),
blee
ding
Med
ian
12 d
(4
-54
d)V
TE
: 1 o
f 19
(5.3
%)
1 In
tern
al ju
gula
r ve
in th
rom
bosi
s,
1 m
ajor
and
1 m
inor
bl
eedi
ng
Ble
edin
g: 2
of 1
9 (1
0.5%
)
Coo
k et
al 36
/200
5Si
ngle
-cen
ter
pros
pect
ive
coho
rt26
1 m
edic
al-s
urgi
cal
ICU
pat
ient
sU
FH
5,0
00 I
nter
natio
nal
Uni
ts S
C b
idD
VT
det
ecte
d by
co
mpr
essi
on u
ltras
ound
on
adm
issi
on a
nd tw
ice
wee
kly
Unt
il IC
U
disc
harg
e, d
eath
or
dev
elop
men
t of
DV
T
Inci
dent
DV
T: 2
5 of
261
(9
.6%
; 95%
CI,
6.
3%-1
3.8%
)
Mos
t DV
T a
sym
ptom
atic
(n
ot c
linic
ally
sus
pect
ed)
CrC
l 5 cr
eatin
ine
clea
ranc
e. S
ee T
able
S1-
S5 a
nd S
11 le
gend
s fo
r ex
pans
ion
of o
ther
abb
revi
atio
ns.
Tabl
e S1
3—C
onti
nued
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

31© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
4 —[S
ecti
on 3
.4.1
] E
vide
nce
Pro
fi le:
Sho
uld
UF
H v
s P
lace
bo
Be
Use
d fo
r D
VT
Pre
vent
ion
in C
riti
call
y Il
l A
dult
Pat
ient
s?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
N
o. o
f Pat
ient
sE
ffec
t
No.
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Oth
er
Con
side
ratio
nsU
FH
Plac
ebo
Rel
ativ
e (9
5% C
I)A
bsol
ute
Qua
lity
Sym
ptom
atic
DV
T (u
p to
28
d) a (
impo
rtan
t out
com
e)
1R
CT
Non
eN
one
Non
eSe
riou
s b N
one
26 o
f 498
(5.2
2%)
56 o
f 959
(5.8
4%)
RR
, 0.8
9 (0
.57-
1.41
)6
few
er p
er 1
,000
(f
rom
25
few
er to
24
mor
e)M
oder
ate
Sym
ptom
atic
PE
(up
to 2
8 d)
a (im
port
ant o
utco
me)
1R
CT
Non
eN
one
Seri
ous a
Seri
ous b
Non
e…
4.2%
RR
, 0.4
8 (0
.10-
2.26
)22
few
er p
er 1
,000
(f
rom
38
few
er to
53
mor
e)L
ow
Mor
talit
y (c
ritic
al o
utco
me)
No
data
……
……
……
……
……
…
Maj
or b
leed
ing
(impo
rtan
t out
com
e)
No
data
……
……
……
……
……
…
Bib
liogr
aphy
: Sh
orr
AF,
Will
iam
s M
D.
Veno
us t
hrom
boem
bolis
m i
n cr
itica
lly i
ll pa
tient
s. O
bser
vatio
ns f
rom
a r
ando
miz
ed t
rial
in
seps
is.
Thro
mb
Hae
mos
t. 20
09;1
01(1
):139
-144
. Se
e Ta
ble
S1 a
nd
S4 le
gend
s fo
r ex
pans
ion
of a
bbre
viat
ions
. a S
ympt
omat
ic D
VT
was
rep
orte
d in
Sho
rr a
nd W
illia
ms,
sym
ptom
atic
PE
was
not
rep
orte
d. T
here
fore
, we
estim
ated
PE
bas
elin
e ri
sk f
rom
obs
erva
tiona
l stu
dies
(4.
2%)
and
used
RR
fro
m S
horr
and
W
illia
ms,
whi
ch w
as li
kely
a m
ix o
f sym
ptom
atic
and
asy
mpt
omat
ic e
vent
s.
b Sm
all n
umbe
r of
pat
ient
s an
d sm
all n
umbe
r of
eve
nts
in e
ach
grou
p; C
I in
clud
e be
nefi t
and
har
m.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

32© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
5 — [S
ecti
on 3
.4.2
] E
vide
nce
Pro
fi le:
Sho
uld
LM
WH
vs
Pla
ceb
o B
e U
sed
for
DV
T P
reve
ntio
n in
Cri
tica
lly
Ill
Adu
lt P
atie
nts?
Set
ting
: IC
U
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
s (%
)E
ffec
t
No.
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Oth
er
Con
sider
atio
nsL
MW
HPl
aceb
oR
elat
ive
(95%
CI)
Abs
olut
e Q
ualit
y
Sym
ptom
atic
DV
T (5
-28
d) a
1R
CT
No
seri
ous
limita
tions
b N
one c
Non
eSe
riou
s d N
one
23 o
f 478
(4.8
1%)
56 o
f 959
(5.8
4%)
RR
, 0.8
2 (0
.51-
1.32
)9
few
er (f
rom
24
few
er
to15
mor
e)M
oder
ate
Impo
rtan
t
Sym
ptom
atic
PE
(5-2
8 d)
a
1R
CT
No
seri
ous
limita
tions
b N
one c
Seri
ous a
Very
se
riou
s d N
one
…4.
2 e R
R, 1
.01,
(0
.31-
3.31
)0
few
er (f
rom
29
few
er
to 9
7 m
ore)
Very
low
Impo
rtan
t
Maj
or b
leed
ing
(fol
low
-up
mea
n, 1
1.6
d)
1R
CT
No
seri
ous
limita
tions
b N
one c
No
seri
ous
indi
rect
ness
Very
se
riou
s d N
one f
6 of
108
(5.6
%)
3 of
113
(2.7
%)
RR
, 2.0
9 (0
.54
to 8
.16)
29 m
ore
per
1,00
0 (f
rom
12
few
er to
190
mor
e)Ve
ry lo
wIm
port
ant
Mor
talit
y (f
ollo
w-u
p m
ean,
11.
6 d)
1R
CT
No
seri
ous
limita
tions
b N
one c
No
seri
ous
indi
rect
ness
Very
se
riou
s d N
one f f
8 of
84
(9.5
%)
8 of
85
(9.4
%)
RR
, 1.0
1 (0
.4 to
2.5
7)1
mor
e pe
r 1,
000
(fro
m
56 fe
wer
to 1
48 m
ore)
Very
low
Cri
tical
Bib
liogr
aphy
: Fra
isse
F, H
olza
pfel
L, C
oula
nd J
M e
t al.
Nad
ropa
rin
in th
e pr
even
tion
of d
eep
vein
thro
mbo
sis
in a
cute
dec
ompe
nsat
ed C
OPD
. The
Ass
ocia
tion
of N
on-U
nive
rsity
Affi
liate
d In
tens
ive
Car
e Sp
ecia
list P
hysi
cian
s of
Fra
nce.
Am
J R
espi
r C
rit C
are
Med
. 200
0;16
1(4
pt 1
):110
9-11
14. S
horr
AF,
Will
iam
s M
D. V
enou
s th
rom
boem
bolis
m in
cri
tical
ly il
l pat
ient
s. O
bser
vatio
ns fr
om a
ran
dom
ized
tria
l in
sep
sis.
Thr
omb
Hae
mos
t . 20
09;1
01(1
):139
-144
. See
Tab
le S
1-S4
, S10
, and
S11
lege
nds
for
expa
nsio
n of
abb
revi
atio
ns.
a Sym
ptom
atic
DV
T w
as r
epor
ted
in S
horr
and
Will
iam
s sy
mpt
omat
ic P
E w
as n
ot r
epor
ted
in S
horr
et a
l (ze
ro e
vent
s in
bot
h st
udy
arm
s by
Fra
isse
et a
l). T
here
fore
, we
estim
ated
PE
bas
elin
e ri
sk fr
om
obse
rvat
iona
l stu
dies
(4.2
%) a
nd u
sed
RR
from
Sho
rr a
nd W
illia
ms,
whi
ch w
as li
kely
a m
ix o
f sym
ptom
atic
and
asy
mpt
omat
ic e
vent
s.
b Bot
h st
udie
s do
uble
-blin
d, I
TT
ana
lysi
s. F
rais
se e
t al
: ven
ogra
phy
coul
d no
t be
per
form
ed in
52
of 2
21 (
23.5
%)
of p
atie
nts;
the
se p
atie
nts
wer
e ex
clud
ed f
rom
the
effi
cacy
ana
lysi
s. S
horr
and
Will
iam
s:
stud
y as
sess
ed e
ffi ca
cy o
f pr
ophy
lact
ic d
oses
of
LM
WH
/UF
H in
pat
ient
s w
ith s
ever
e se
psis
onl
y w
hile
rec
eivi
ng d
rotr
ecog
in a
lfa. F
rais
se e
t al
: stu
dy s
uppo
rted
by
a gr
ant
from
San
ofi (
man
ufac
ture
r of
na
drop
arin
). c C
linic
al h
eter
ogen
eity
of t
he tr
ials
: (1)
Fra
isse
et a
l: N
adro
pari
n do
sed
acco
rdin
g to
wei
ght (
3,80
0 un
its fo
r 45
-70
kg; 5
,700
uni
ts fo
r 71
-110
kg)
; Sho
rr a
nd W
illia
ms:
enox
apar
in 4
0 m
g SC
od;
(2) F
rais
se e
t al:
Patie
nts
with
CO
PD e
xace
rbat
ion
requ
irin
g m
echa
nica
l ven
tilat
ion;
Sho
rr a
nd W
illia
ms:
1,9
35 s
epsi
s pa
tient
s re
ceiv
ing
drot
reco
gin
alfa
; (3)
Met
hod
of D
VT
ass
essm
ent:
Fra
isse
et a
l: ve
nogr
aphy
at e
nd
of s
tudy
per
iod
(max
21
� 1
d);
Shor
r an
d W
illia
ms:
com
pres
sion
ultr
ason
ogra
phy
betw
een
days
4 a
nd 6
; and
(4)
Fra
isse
et
al: r
esul
ts f
rom
Dop
pler
ultr
ason
ogra
phy
and
veno
grap
hy w
as d
iscr
epan
t, bu
t no
furt
her
info
rmat
ion
was
pro
vide
d. V
enog
raph
y (a
t the
end
of t
he s
tudy
per
iod)
was
use
d to
ass
ess
effi c
acy
in th
is s
tudy
, but
ultr
ason
ogra
phy
was
per
form
ed b
efor
e in
clus
ion
and
wee
kly.
d S
mal
l num
ber
of p
atie
nts
and
smal
l num
ber
of e
vent
s in
eac
h gr
oup;
CI
incl
ude
bene
fi t a
nd h
arm
. The
RR
of
the
outc
ome
of P
E is
con
side
red
very
impr
ecis
e du
e to
sm
all n
umbe
r of
eve
nts
(4 o
f 47
8 L
MW
H v
s 8
of 9
59 p
lace
bo).
e No
dire
ct e
vide
nce
rega
rdin
g sy
mpt
omat
ic P
E. T
here
fore
, we
estim
ated
bas
elin
e ri
sk fr
om o
bser
vatio
nal s
tudi
es (4
.2%
) and
use
d R
R fr
om S
horr
and
Will
iam
s, w
hich
was
like
ly a
mix
of s
ympt
omat
ic a
nd
asym
ptom
atic
eve
nts.
f M
ajor
ble
edin
g an
d m
orta
lity
wer
e on
ly a
sses
sed
in F
rais
se e
t al (
adju
dica
ted
by in
depe
nden
t com
mitt
ee).
Ble
edin
g w
as d
efi n
ed a
s ov
ert,
asso
ciat
ed w
ith d
ecre
ase
in H
gb o
f . 2
g/d
L, p
acke
d R
BC
tran
s-fu
sion
, ret
rope
rito
neal
or
intr
acra
nial
or
resu
lted
in d
isco
ntin
uatio
n of
pro
phyl
axis
. Mor
talit
y w
as m
ainl
y du
e to
car
diov
ascu
lar
com
plic
atio
ns a
ssoc
iate
d w
ith in
fect
ion
(not
due
to b
leed
ing)
.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
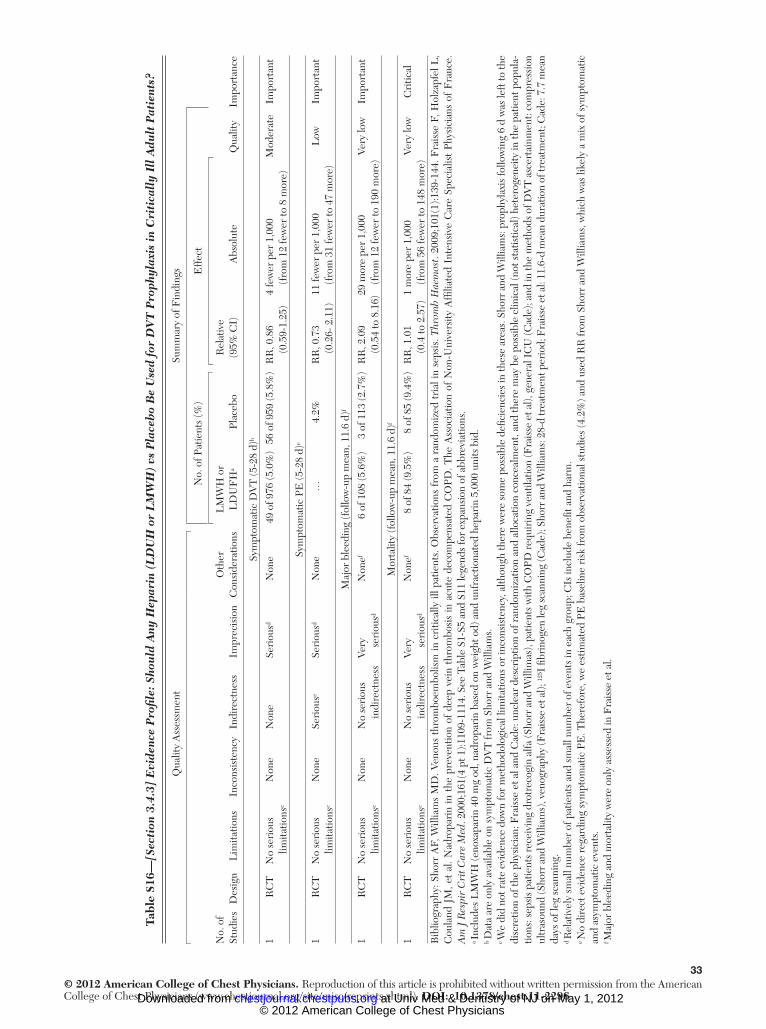
33© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
6 —[S
ecti
on 3
.4.3
] E
vide
nce
Pro
fi le:
Sho
uld
Any
Hep
arin
(L
DU
H o
r L
MW
H)
vs P
lace
bo
Be
Use
d fo
r D
VT
Pro
phyl
axis
in
Cri
tica
lly
Ill
Adu
lt P
atie
nts?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
s (%
)E
ffec
t
No.
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Oth
er
Con
side
ratio
nsL
MW
H o
r L
DU
FH
a Pl
aceb
oR
elat
ive
(95%
CI)
Abs
olut
eQ
ualit
y
Sym
ptom
atic
DV
T (5
-28
d) b
1R
CT
No
seri
ous
limita
tions
c N
one
Non
eSe
riou
s d N
one
49 o
f 976
(5.0
%)
56 o
f 959
(5.8
%)
RR
, 0.8
6 (0
.59-
1.25
)4
few
er p
er 1
,000
(f
rom
12
few
er to
8 m
ore)
Mod
erat
eIm
port
ant
Sym
ptom
atic
PE
(5-2
8 d)
e
1R
CT
No
seri
ous
limita
tions
c N
one
Seri
ous e
Seri
ous d
Non
e…
4.2%
RR
, 0.7
3 (0
.26-
2.1
1)11
few
er p
er 1
,000
(f
rom
31
few
er to
47
mor
e)L
owIm
port
ant
Maj
or b
leed
ing
(fol
low
-up
mea
n, 1
1.6
d) f
1R
CT
No
seri
ous
limita
tions
c N
one
No
seri
ous
indi
rect
ness
Very
se
riou
s d N
one f
6 of
108
(5.6
%)
3 of
113
(2.7
%)
RR
, 2.0
9 (0
.54
to 8
.16)
29 m
ore
per
1,00
0 (f
rom
12
few
er to
190
mor
e)Ve
ry lo
wIm
port
ant
Mor
talit
y (f
ollo
w-u
p m
ean,
11.
6 d)
f
1R
CT
No
seri
ous
limita
tions
c N
one
No
seri
ous
indi
rect
ness
Very
se
riou
s d N
one f
8 of
84
(9.5
%)
8 of
85
(9.4
%)
RR
, 1.0
1 (0
.4 to
2.5
7)1
mor
e pe
r 1,
000
(fro
m 5
6 fe
wer
to 1
48 m
ore)
Very
low
Cri
tical
Bib
liogr
aphy
: Sho
rr A
F, W
illia
ms
MD
. Ven
ous
thro
mbo
embo
lism
in c
ritic
ally
ill p
atie
nts.
Obs
erva
tions
fro
m a
ran
dom
ized
tri
al in
sep
sis.
Thr
omb
Hae
mos
t . 20
09;1
01(1
):139
-144
. Fra
isse
F, H
olza
pfel
L,
Cou
land
JM
, et
al. N
adro
pari
n in
the
pre
vent
ion
of d
eep
vein
thr
ombo
sis
in a
cute
dec
ompe
nsat
ed C
OPD
. The
Ass
ocia
tion
of N
on-U
nive
rsity
Affi
liate
d In
tens
ive
Car
e Sp
ecia
list
Phys
icia
ns o
f F
ranc
e.
Am
J R
espi
r C
rit C
are
Med
. 200
0;16
1(4
pt 1
):110
9-11
14. S
ee T
able
S1-
S5 a
nd S
11 le
gend
s fo
r ex
pans
ion
of a
bbre
viat
ions
. a I
nclu
des
LM
WH
(eno
xapa
rin
40 m
g od
, nad
ropa
rin
base
d on
wei
ght o
d) a
nd u
nfra
ctio
nate
d he
pari
n 5,
000
units
bid
. b D
ata
are
only
ava
ilabl
e on
sym
ptom
atic
DV
T fr
om S
horr
and
Will
iam
s.
c We
did
not r
ate
evid
ence
dow
n fo
r m
etho
dolo
gica
l lim
itatio
ns o
r in
cons
iste
ncy,
alth
ough
ther
e w
ere
som
e po
ssib
le d
efi c
ienc
ies
in th
ese
area
s. S
horr
and
Will
iam
s: p
roph
ylax
is fo
llow
ing
6 d
was
left
to th
e di
scre
tion
of th
e ph
ysic
ian;
Fra
isse
et a
l and
Cad
e: u
ncle
ar d
escr
iptio
n of
ran
dom
izat
ion
and
allo
catio
n co
ncea
lmen
t, an
d th
ere
may
be
poss
ible
clin
ical
(not
sta
tistic
al) h
eter
ogen
eity
in th
e pa
tient
pop
ula-
tions
: sep
sis
patie
nts
rece
ivin
g dr
otre
cogi
n al
fa (S
horr
and
Will
imas
), pa
tient
s w
ith C
OPD
req
uiri
ng v
entil
atio
n (F
rais
se e
t al),
gen
eral
IC
U (C
ade)
; and
in th
e m
etho
ds o
f DV
T a
scer
tain
men
t: co
mpr
essi
on
ultr
asou
nd (S
horr
and
Will
iam
s), v
enog
raph
y (F
rais
se e
t al);
125 I
fi br
inog
en le
g sc
anni
ng (C
ade)
; Sho
rr a
nd W
illia
ms:
28-
d tr
eatm
ent p
erio
d; F
rais
se e
t al:
11.6
-d m
ean
dura
tion
of tr
eatm
ent;
Cad
e: 7
.7 m
ean
days
of l
eg s
cann
ing.
d R
elat
ivel
y sm
all n
umbe
r of
pat
ient
s an
d sm
all n
umbe
r of
eve
nts
in e
ach
grou
p; C
Is in
clud
e be
nefi t
and
har
m.
e No
dire
ct e
vide
nce
rega
rdin
g sy
mpt
omat
ic P
E. T
here
fore
, we
estim
ated
PE
bas
elin
e ri
sk fr
om o
bser
vatio
nal s
tudi
es (4
.2%
) and
use
d R
R fr
om S
horr
and
Will
iam
s, w
hich
was
like
ly a
mix
of s
ympt
omat
ic
and
asym
ptom
atic
eve
nts.
f M
ajor
ble
edin
g an
d m
orta
lity
wer
e on
ly a
sses
sed
in F
rais
se e
t al.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

34© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
7 —[S
ecti
on 3
.4.4
] E
vide
nce
Pro
fi le:
Sho
uld
LM
WH
vs
UF
H B
e U
sed
for
DV
T P
reve
ntio
n in
Cri
tica
lly
Ill
Adu
lt P
atie
nts?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
sE
ffec
t
No.
of
Stud
ies a
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Oth
er
Con
sider
atio
nsL
MW
HU
FH
Rel
ativ
e (9
5% C
I)A
bsol
ute
Qua
lity
Sym
ptom
atic
DV
T (f
ollo
w-u
p 7-
28 d
) b
2R
CT
Non
e c N
o se
riou
s in
cons
iste
ncy
Non
eSe
riou
s d N
one
51 o
f 2,3
51 (2
.2%
)60
of 2
,371
(2.5
%)
RR
, 0.8
7 (0
.60-
1.25
) e 3
few
er p
er 1
,000
(f
rom
10
few
er to
6 m
ore)
Mod
erat
eIm
port
ant
Sym
ptom
atic
PE
(fol
low
-up
7-28
d)
1R
CT
Non
e c N
o se
riou
s in
cons
iste
ncy
Non
eSe
riou
s d N
one
22 o
f 1,8
73 (1
.2%
)38
of 1
,873
(2.0
%)
RR
, 0.5
8 (0
.34-
0.97
)8
few
er p
er 1
,000
(1
3.2
few
er to
0.6
few
er)
Mod
erat
eIm
port
ant
Maj
or b
leed
ing
(fol
low
-up
7-47
d)
2 f R
CT
Non
e c N
o se
riou
s in
cons
iste
ncy
Non
eSe
riou
s d N
one
104
of 1
,954
(5.3
%)
107
of 1
,948
(5.5
%)
RR
, 0.9
7 (0
.75-
1.26
) e 2
few
er p
er 1
,000
(f
rom
14
few
er to
14
mor
e)M
oder
ate
Impo
rtan
t
Mor
talit
y (f
ollo
w-u
p 7-
47 d
)
2R
CT
Non
e c N
o se
riou
s in
cons
iste
ncy
Non
eSe
riou
s d N
one
293
of 1
,954
(15.
0%)
310
of 1
,948
(15.
9%)
RR
, 0.9
4 (0
.81-
1.09
) e 10
few
er p
er 1
,000
(f
rom
30
few
er to
14
mor
e)M
oder
ate
Cri
tical
HIT
(7 d
)
1R
CT
Non
e c N
o se
riou
s in
cons
iste
ncy
Non
eSe
riou
s d N
one
5 of
1,8
73 (0
.3%
)12
of 1
,873
(0.6
%)
RR
, 0.4
2 (0
.15-
1.18
)3
few
er p
er 1
,000
(f
rom
5 fe
wer
to 1
mor
e)M
oder
ate
Impo
rtan
t
Bib
liogr
aphy
: PR
OT
EC
T I
nves
tigat
ors.
Dal
tepa
rin
vs u
nfra
ctio
nate
d he
pari
n in
cri
tical
ly il
l pat
ient
s. N
Eng
l J M
ed . 2
011;
364(
14):1
305-
1314
. Sho
rr A
F, W
illia
ms M
D. V
enou
s thr
ombo
embo
lism
in c
ritic
ally
ill
pat
ient
s. O
bser
vatio
ns fr
om a
ran
dom
ized
tria
l in
seps
is. T
hrom
b H
aem
ost.
2009
;101
(1):1
39-1
44. D
e A
, Roy
P, G
arg
VK
et a
l. L
ow-m
olec
ular
-wei
ght h
epar
in a
nd u
nfra
ctio
nate
d he
pari
n in
pro
phyl
axis
ag
ains
t dee
p ve
in th
rom
bosi
s in
cri
tical
ly il
l pat
ient
s un
derg
oing
maj
or s
urge
ry. B
lood
Coa
gul F
ibri
noly
sis .
201
0;21
(1):5
7-61
. IQ
R 5
inte
rqua
rtile
ran
ge. S
ee T
able
S1-
S5 a
nd S
11 le
gend
s fo
r ex
pans
ion
of
othe
r ab
brev
iatio
ns.
a The
out
com
e of
sym
ptom
atic
PE
was
rep
orte
d in
PR
OT
EC
T a
nd th
e ou
tcom
e of
sym
ptom
atic
DV
T w
as r
epor
ted
in P
RO
TE
CT
and
Sho
rr a
nd W
illia
ms
stud
ies.
The
out
com
es o
f ble
edin
g an
d m
orta
lity
wer
e re
port
ed in
PR
OT
EC
T a
nd D
e et
al s
tudi
es. T
he o
utco
me
of H
IT w
as re
port
ed in
PR
OT
EC
T. T
he in
terv
entio
ns w
ere:
PR
OT
EC
T: d
alte
pari
n 5,
000
Inte
rnat
iona
l Uni
ts S
C o
d; S
horr
and
Will
iam
s and
D
e et
al:
enox
apar
in 4
0 m
g SC
od;
UF
H 5
,000
uni
ts S
C b
id; a
nd a
ll st
udie
s inc
lude
d pl
aceb
o in
ject
ion.
PR
OT
EC
T: c
ompr
essi
on u
ltras
ound
per
form
ed w
ithin
2 d
of I
CU
adm
issi
on th
en tw
ice
wee
kly
whi
le
in I
CU
; Sho
rr a
nd W
illia
ms:
com
pres
sion
ultr
asou
nd p
erfo
rmed
bet
wee
n da
y 4
and
6 of
dro
trec
ogin
alfa
trea
tmen
t; D
e et
al:
Dop
pler
per
form
ed b
etw
een
post
oper
ativ
e da
y 5
and
7. P
opul
atio
n: P
RO
TE
CT:
3,
764
patie
nts
expe
cted
to r
emai
n in
IC
U a
t lea
st 3
d; S
horr
and
Will
iam
s: 1
,935
sep
sis
patie
nts
rece
ivin
g dr
otre
cogi
n al
fa; D
e et
al:
156
patie
nts
unde
rgoi
ng m
ajor
sur
gery
req
uiri
ng a
t lea
st 2
4 h
in I
CU
. b P
RO
TE
CT:
Med
ian
dura
tion
of s
tudy
per
iod:
7 d
(IQ
R 4
-12
d); S
horr
and
Will
iam
s: 2
8-d
stud
y pe
riod
; De
et a
l: M
edia
n fo
llow
-up:
47
d.
c De
et a
l: U
ncle
ar d
escr
iptio
n of
ran
dom
izat
ion
proc
ess,
blin
ding
, and
loss
es to
follo
w-u
p. P
RO
TE
CT
had
ade
quat
e bi
as p
rote
ctio
n m
easu
res.
d R
elat
ivel
y sm
all n
umbe
r of
eve
nts
and
wid
e C
Is th
at in
clud
e be
nefi t
and
har
m.
e Fix
ed e
ffec
t mod
el u
sed
for
met
a-an
alys
is.
f Maj
or b
leed
ing
defi n
ition
: PR
OT
EC
T: h
emor
rhag
e at
a c
ritic
al si
te, b
leed
ing
resu
lting
in n
eed
for t
hera
peut
ic in
terv
entio
n, c
ausi
ng h
emod
ynam
ic c
ompr
omis
e, re
quir
ing
2 un
its tr
ansf
usio
n or
resu
lting
in
deat
h. D
e et
al:
GI
blee
ding
dia
gnos
ed o
n st
ool t
estin
g or
upp
er G
I en
dosc
opy
or a
ny b
leed
ing
epis
ode
requ
irin
g re
oper
atio
n.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

35© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
8 —[S
ecti
on 4
.2]
Evi
denc
e P
rofi l
e: S
hou
ld H
epar
in v
s N
o H
epar
in B
e U
sed
in P
atie
nts
Wit
h C
ance
r W
ho H
ave
No
Oth
er T
hera
peu
tic
or P
roph
ylac
tic
Indi
cati
on f
or A
ntic
oagu
lati
on?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
sE
ffec
t
No.
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Oth
er
Con
sider
atio
nsH
epar
inN
o H
epar
in, %
Rel
ativ
e (9
5% C
I)A
bsol
ute
Qua
lity
Mor
talit
y (f
ollo
w-u
p, 1
2 m
o) a
8R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
ns b
Seri
ous c
No
seri
ous
indi
rect
ness
No
seri
ous
impr
ecis
ion d
Non
e73
5 of
1,4
64 (5
0.2%
)64
.9 e
RR
, 0.9
3 (0
.85-
1.02
)45
few
er p
er 1
,000
(f
rom
97
few
er to
13
mor
e)
Mod
erat
eIm
port
ant
Sym
ptom
atic
VT
E (f
ollo
w-u
p, 1
2 m
o)
7R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
ns b
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssN
o se
riou
s im
prec
isio
nN
one
38 o
f 1,3
38 (2
.8%
)2.
9 e R
R, 0
.55
(0.3
7-0.
82)
13 fe
wer
per
1,0
00
(fro
m 5
few
er to
18
few
er)
Hig
hC
ritic
al
Maj
or b
leed
ing
(fol
low
-up,
12
mo)
9R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
ns b
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s f N
one
30 o
f 1,6
24 (1
.8%
)0.
7 b R
R, 1
.3
(0.5
9-2.
88)
2 m
ore
per
1,00
0 (f
rom
3 fe
wer
to
13 m
ore)
Mod
erat
eIm
port
ant
Min
or b
leed
ing
(fol
low
-up,
12
wk)
7R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
ns b
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s f N
one
85 o
f 1,3
65 (6
.2%
)2.
7 e R
R, 1
.05
(0.7
5-1.
46)
1 m
ore
per
1,00
0 (f
rom
7 fe
wer
to
12 m
ore)
Mod
erat
eN
ot im
port
ant
Hea
lth-r
elat
ed q
ualit
y of
life
(fol
low
-up,
12
mo;
the
Uni
scal
e an
d th
e Sy
mpt
om D
istr
ess
Scal
e; b
ette
r in
dica
ted
by lo
wer
val
ues)
1R
ando
miz
ed
tria
lsSe
riou
s g N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous g
Non
eN
ot estim
able
h L
owIm
port
ant
Bib
liogr
aphy
: Akl
EA
, Gun
ukul
a SK
, van
Doo
rmaa
l FF,
et a
l. Pa
rent
eral
ant
icoa
gula
tion
in p
atie
nts
with
can
cer
who
hav
e no
ther
apeu
tic o
r pr
ophy
lact
ic in
dica
tion
for
antic
oagu
latio
n. C
ochr
ane
Dat
abas
e Sy
st R
ev . 2
011;
(4)C
D00
6652
. See
Tab
le S
4 le
gend
for
expa
nsio
n of
abb
revi
atio
n.
a The
out
com
es a
re r
epor
ted
at 1
2-m
o fo
llow
-up.
Mor
talit
y at
2-y
follo
w-u
p in
crea
ses
from
65%
to 8
6%.
b Vas
t m
ajor
ity o
f st
udie
s ha
d al
loca
tion
conc
ealm
ent
and
used
blin
ded
outc
ome
and
adju
dica
tion.
We
did
not
dow
ngra
de, a
lthou
gh t
here
was
som
e co
ncer
n ab
out
lack
of
blin
ding
in s
ome
stud
ies;
the
ov
eral
l ris
k of
bia
s w
as b
elie
ved
to b
e ve
ry lo
w.
c The
re is
mod
erat
e he
tero
gene
ity a
mon
g st
udie
s inc
lude
d in
the
anal
ysis
of d
eath
at 1
2 m
o ( I
2 5 4
1%).
The
subg
roup
ana
lysi
s for
mor
talit
y at
12
mo
was
stat
istic
ally
sign
ifi ca
nt a
nd su
gges
ted
surv
ival
ben
efi t
in p
atie
nts
with
sm
all c
ell l
ung
canc
er b
ut n
ot in
pat
ient
s w
ith a
dvan
ced
canc
er. O
vera
ll w
e de
cide
d to
dow
ngra
de b
y on
e le
vel w
hen
cons
ider
ing
thes
e is
sues
alo
ng w
ith im
prec
isio
n.
d CI
inte
rval
incl
udes
eff
ects
sug
gest
ing
bene
fi t a
s w
ell a
s no
ben
efi t.
e B
asel
ine
risk
is th
e m
edia
n of
ris
k in
con
trol
gro
ups
of tr
ials
incl
uded
in th
e sy
stem
atic
rev
iew
. f C
I in
clud
es p
ossi
bilit
y of
bot
h ha
rms
or b
enefi
ts.
g Hig
h ri
sk o
f bia
s an
d on
ly 1
38 p
atie
nts
enro
lled.
h T
he s
core
s fo
r th
e tw
o sc
ales
wer
e si
mila
r fo
r th
e tw
o st
udy
grou
ps, b
oth
at b
asel
ine
and
at fo
llow
-up.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

36© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S1
9 —[S
ecti
on 4
.3]
Evi
denc
e P
rofi l
e: S
hou
ld O
ral
Ant
icoa
gula
tion
Be
Use
d in
Pat
ient
s W
ith
Can
cer
Wit
h N
o T
hera
peu
tic
or P
roph
ylac
tic
Indi
cati
on f
or
Ant
icoa
gula
tion
?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
sE
ffec
t
No.
of
Stud
ies
Des
ign
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Oth
er
Con
side
ratio
nsO
ral
Ant
icoa
gula
tion
Con
trol
, %R
elat
ive
(95%
CI)
Abs
olut
e Q
ualit
y
Mor
talit
y (f
ollo
w-u
p m
edia
n, 1
y)
5R
ando
miz
ed
tria
lsSe
riou
s a N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
No
seri
ous
impr
ecis
ion
Non
e36
0 of
80
1 (4
4.9%
)64
.9 b
RR
, 0.9
4 (0
.87-
1.03
)39
few
er p
er 1
,000
(f
rom
84
few
er
to 1
9 m
ore)
Mod
erat
eIm
port
ant
Sym
ptom
atic
VT
E (f
ollo
w-u
p, 1
y)
1R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous c
Non
e1
of 1
54
(0.6
%)
2.9 b
RR
, 0.1
5 (0
.02-
1.2)
25 fe
wer
per
1,0
00
(fro
m 2
8 fe
wer
to
6 m
ore)
Mod
erat
eIm
port
ant
Maj
or b
leed
ing
(fol
low
-up,
med
ian
1 y)
4R
ando
miz
ed
tria
lsSe
riou
s d N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
No
seri
ous
impr
ecis
ion
Non
e72
of 6
50 (1
1.1%
)0.
7 b R
R, 4
.24
(1.8
5-9.
68)
23 m
ore
per
1,00
0 (f
rom
6 m
ore
to 6
1 m
ore)
Mod
erat
eIm
port
ant
Hea
lth-r
elat
ed q
ualit
y of
life
: not
rep
orte
d
0…
……
……
Non
e0
of 0
(0%
)0
……
Impo
rtan
t B
iblio
grap
hy: A
kl E
A, V
asir
eddi
S, G
unuk
ula
S, e
t al.
Ora
l ant
icoa
gula
tion
for
prol
ongi
ng s
urvi
val i
n pa
tient
s w
ith c
ance
r. C
ochr
ane
Dat
abas
e Sy
st R
ev . 2
010;
(12)
:CD
0064
66.
a We
dow
ngra
ded
beca
use
lack
of b
lindi
ng o
f pat
ient
s an
d pr
ovid
ers
in fo
ur o
ut o
f fi v
e st
udie
s; it
was
unc
lear
whe
ther
allo
catio
n w
as c
once
aled
in tw
o st
udie
s; a
nd o
nly
one
stud
y cl
earl
y us
ed I
TT
ana
lysi
s.
All
stud
ies
used
war
fari
n at
a d
ose
to in
crea
se P
T 1
.5 to
2 ti
mes
(fou
r st
udie
s) o
r to
kee
p IN
R b
etw
een
1.3
and
1.9.
See
Tab
les
S4 a
nd S
10 le
gend
s fo
r ex
pans
ion
of a
bbre
viat
ions
. b B
asel
ine
risk
is th
e m
edia
n of
ris
k in
con
trol
gro
ups
of tr
ials
incl
uded
in a
sys
tem
atic
rev
iew
of t
he e
ffec
ts o
f par
ente
ral a
ntic
oagu
latio
n in
pat
ient
s w
ith c
ance
r bu
t no
prop
hyla
ctic
or
ther
apeu
tic in
dica
tion
for
antic
oagu
latio
n (A
kl e
t al).
c W
e do
wng
rade
d be
caus
e th
e pr
ecis
ion
of th
e es
timat
e do
es n
ot e
xclu
de a
pat
ient
impo
rtan
t ben
efi t
(the
low
er li
mit
of R
R s
till s
ugge
sts
a be
nefi t
that
mig
ht b
e re
leva
nt g
iven
the
high
bas
elin
e ri
sk).
d We
dow
ngra
ded
beca
use
lack
of
blin
ding
of
patie
nts
and
prov
ider
s in
thr
ee o
ut o
f fo
ur s
tudi
es; i
t w
as u
ncle
ar w
heth
er a
lloca
tion
was
con
ceal
ed i
n tw
o st
udie
s; a
nd o
nly
one
stud
y cl
earl
y us
ed I
TT
an
alys
is.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
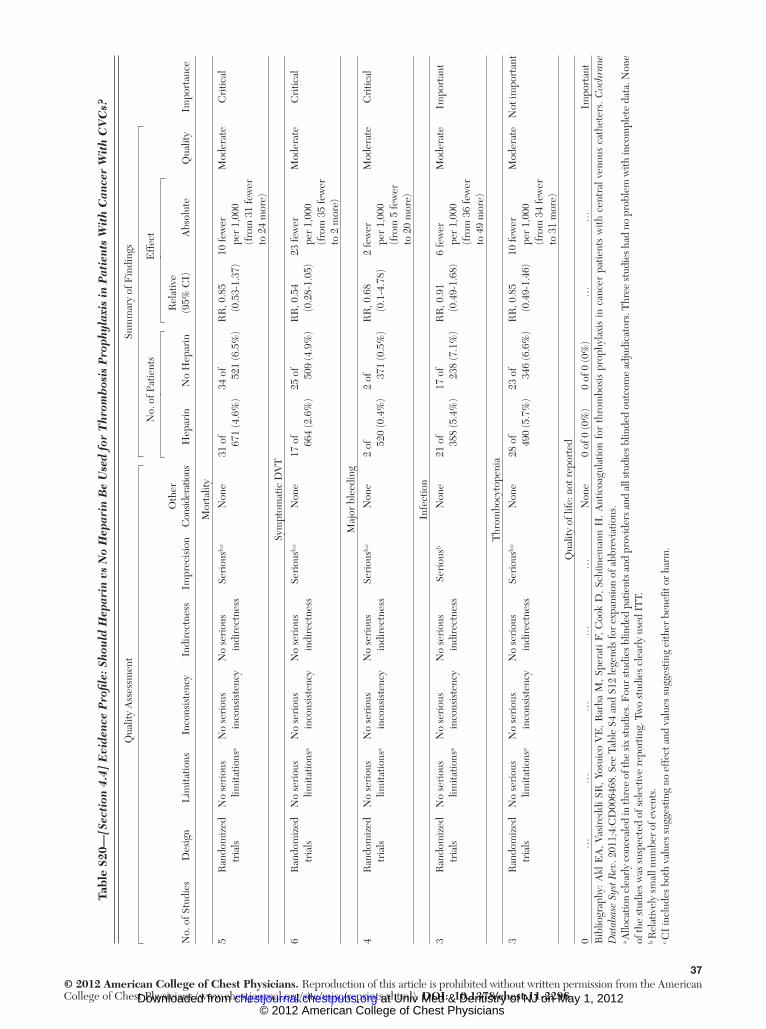
37© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
0 —[S
ecti
on 4
.4]
Evi
denc
e P
rofi l
e: S
hou
ld H
epar
in v
s N
o H
epar
in B
e U
sed
for
Thr
omb
osis
Pro
phyl
axis
in
Pat
ient
s W
ith
Can
cer
Wit
h C
VC
s?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
sE
ffec
t
Qua
lity
No.
of S
tudi
esD
esig
nL
imita
tions
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
C
onsid
erat
ions
Hep
arin
No
Hep
arin
Rel
ativ
e (9
5% C
I)A
bsol
ute
Mor
talit
y
5R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
ns a
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s b , c N
one
31 o
f 67
1 (4
.6%
)34
of
521
(6.5
%)
RR
, 0.8
5 (0
.53-
1.37
)10
few
er
per
1,00
0 (f
rom
31
few
er
to 2
4 m
ore)
Mod
erat
eC
ritic
al
Sym
ptom
atic
DV
T
6R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
ns a
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s b , c
Non
e17
of
664
(2.6
%)
25 o
f 50
9 (4
.9%
)R
R, 0
.54
(0.2
8-1.
05)
23 fe
wer
pe
r 1,
000
(fro
m 3
5 fe
wer
to
2 m
ore)
Mod
erat
eC
ritic
al
Maj
or b
leed
ing
4R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
ns a
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s b , c
Non
e2
of 520
(0.4
%)
2 of
371
(0.5
%)
RR
, 0.6
8 (0
.1-4
.78)
2 fe
wer
pe
r 1,
000
(fro
m 5
few
er
to 2
0 m
ore)
Mod
erat
eC
ritic
al
Infe
ctio
n
3R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
ns a
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s b N
one
21 o
f 38
8 (5
.4%
)17
of
238
(7.1
%)
RR
, 0.9
1 (0
.49-
1.68
)6
few
er
per
1,00
0 (f
rom
36
few
er
to 4
9 m
ore)
Mod
erat
eIm
port
ant
Thr
ombo
cyto
peni
a
3R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
ns a
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s b , c
Non
e28
of
490
(5.7
%)
23 o
f 34
6 (6
.6%
)R
R, 0
.85
(0.4
9-1.
46)
10 fe
wer
pe
r 1,
000
(fro
m 3
4 fe
wer
to
31
mor
e)
Mod
erat
eN
ot im
port
ant
Qua
lity
of li
fe: n
ot r
epor
ted
0…
……
……
Non
e0
of 0
(0%
)0
of 0
(0%
)…
…Im
port
ant
Bib
liogr
aphy
: Akl
EA
, Vas
ired
di S
R, Y
osui
co V
E, B
arba
M, S
pera
ti F,
Coo
k D
, Sch
ünem
ann
H. A
ntic
oagu
latio
n fo
r th
rom
bosi
s pr
ophy
laxi
s in
can
cer
patie
nts
with
cen
tral
ven
ous
cath
eter
s. C
ochr
ane
Dat
abas
e Sy
st R
ev . 2
011;
4:C
D00
6468
. See
Tab
le S
4 an
d S1
2 le
gend
s fo
r ex
pans
ion
of a
bbre
viat
ions
. a A
lloca
tion
clea
rly
conc
eale
d in
thre
e of
the
six
stud
ies.
Fou
r stu
dies
blin
ded
patie
nts a
nd p
rovi
ders
and
all
stud
ies b
linde
d ou
tcom
e ad
judi
cato
rs. T
hree
stud
ies h
ad n
o pr
oble
m w
ith in
com
plet
e da
ta. N
one
of th
e st
udie
s w
as s
uspe
cted
of s
elec
tive
repo
rtin
g. T
wo
stud
ies
clea
rly
used
IT
T.
b Rel
ativ
ely
smal
l num
ber
of e
vent
s.
c CI
incl
udes
bot
h va
lues
sug
gest
ing
no e
ffec
t and
val
ues
sugg
estin
g ei
ther
ben
efi t
or h
arm
.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

38© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
1 —[S
ecti
on 4
.5]
Evi
denc
e P
rofi l
e: S
hou
ld V
KA
vs
No
VK
A B
e U
sed
for
Thr
omb
osis
Pro
phyl
axis
in
Pat
ient
s W
ith
Can
cer
Wit
h C
VC
s?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
sE
ffec
t
Qua
lity
No.
of S
tudi
esD
esig
nL
imita
tions
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
C
onsi
dera
tions
VK
AN
o V
KA
Rel
ativ
e (9
5% C
I)A
bsol
ute
Mor
talit
y
2R
ando
miz
ed
tria
lsN
one a
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s b N
one
166
of
551
(30.
1%)
169
of
542
(31.
2%)
RR
, 0.9
7 (0
.82-
1.15
)9
few
er
per
1,00
0 (f
rom
56
few
er
to 4
7 m
ore)
Mod
erat
eC
ritic
al
Sym
ptom
atic
DV
T
4R
ando
miz
ed
tria
lsN
one a
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s b , c
Non
e37
of
621
(6%
)55
of
614
(9%
)R
R, 0
.63
(0.3
5-1.
11)
33 fe
wer
pe
r 1,
000
(fro
m 5
8 fe
wer
to
10
mor
e)
Mod
erat
eC
ritic
al
Maj
or b
leed
ing
2R
ando
miz
ed
tria
lsN
one a
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s b , c
Non
e7
of 551
(1.3
%)
1 of
542
(0.2
%)
RR
, 6.9
3 (0
.86-
56.0
8)11
mor
e pe
r 1,
000
(fro
m 0
few
er
to 1
02 m
ore)
Mod
erat
eC
ritic
al
Indi
rect
ev
iden
ce e
Hig
h
Bib
liogr
aphy
: Akl
EA
, Vas
ired
di S
R, Y
osui
co V
E B
arba
M, S
pera
ti F,
Coo
k D
, Sch
ünem
ann
H. A
ntic
oagu
latio
n fo
r thr
ombo
sis p
roph
ylax
is in
can
cer p
atie
nts w
ith c
entr
al v
enou
s cat
hete
rs. C
ochr
ane
Dat
abas
e Sy
st R
ev . 2
011;
4:C
D00
6468
. VK
A 5
vita
min
K a
ntag
onis
t. Se
e Ta
ble
S4 a
nd S
10 le
gend
s fo
r ex
pans
ion
of o
ther
abb
revi
atio
ns.
a Allo
catio
n cl
earl
y co
ncea
led
in t
hree
of
four
stu
dies
. Non
e of
stu
dies
blin
ded
patie
nts,
pro
vide
rs, o
r da
ta c
olle
ctor
s, a
nd t
hree
stu
dies
blin
ded
outc
ome
adju
dica
tors
. Thr
ee s
tudi
es h
ad n
o pr
oble
m w
ith
inco
mpl
ete
data
. The
pre
senc
e of
sel
ectiv
e re
port
ing
was
unc
lear
in o
ne s
tudy
. Tw
o st
udie
s cl
earl
y us
ed I
TT.
b R
elat
ivel
y sm
all n
umbe
r of
eve
nts.
c C
I in
clud
es b
oth
valu
es s
ugge
stin
g no
eff
ect a
nd v
alue
s su
gges
ting
eith
er b
enefi
t or
har
m.
d Alth
ough
dat
a in
this
pop
ulat
ion
are
of lo
wer
qua
lity,
indi
rect
dat
a fr
om m
any
othe
r po
pula
tions
that
use
d V
KA
dem
onst
rate
hig
h-qu
ality
evi
denc
e.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

39© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
2 —[S
ecti
on 4
.6]
Evi
denc
e P
rofi l
e: S
hou
ld L
MW
H v
s V
KA
Be
Use
d fo
r T
hrom
bos
is P
roph
ylax
is i
n P
atie
nts
Wit
h C
ance
r W
ith
CV
Cs?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
No.
of P
atie
nts
Eff
ect
Qua
lity
No.
of S
tudi
esD
esig
nL
imita
tions
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
C
onsi
dera
tions
LM
WH
VK
AR
elat
ive
(95%
CI)
A
bsol
ute
2R
ando
miz
ed
tria
lsSe
riou
s a N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous b ,
c N
one
22 o
f 170
(1
2.9%
)19
of 1
73 (1
1%)
RR
, 1.2
7 (0
.55-
2.96
)30
mor
e pe
r 1,
000
(fro
m
49 fe
wer
to
215
mor
e)
Low
Cri
tical
Sym
ptom
atic
DV
T
2R
ando
miz
ed
tria
lsSe
riou
s a N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous b ,
c N
one
4 of
142
(2.8
%)
3 of
138
(2.2
%)
RR
, 1.2
8 (0
.25-
6.5)
6 m
ore
per
1,00
0 (f
rom
16
few
er to
12
0 m
ore)
Low
Cri
tical
Maj
or b
leed
ing
2R
ando
miz
ed
tria
lsSe
riou
s a N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous b ,
c N
one
1 of
170
(0.6
%)
0 of
173
(0%
)R
R, 3
.1 (0
.13-
73.1
4)0
mor
e pe
r 1,
000
(fro
m
0 fe
wer
to 0
m
ore)
Low
Cri
tical
Thr
ombo
cyto
peni
a
1R
ando
miz
ed
tria
lsSe
riou
s a N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Seri
ous b ,
c N
one
2 of
29
(6.9
%)
0 of
30
(0%
)R
R, 5
.17
(0.2
6-10
3.21
)0
mor
e pe
r 1,
000
(fro
m
0 fe
wer
to 0
m
ore)
Low
Not
impo
rtan
t
Qua
lity
of li
fe -
not r
epor
ted
0…
……
……
Non
e0
of 0
(0%
)0
of 0
(0%
)…
…Im
port
ant
Bib
liogr
aphy
: Akl
EA
, Vas
ired
di S
R, Y
osui
co V
E D
, Bar
ba M
, Spe
rati
F, C
ook
D, S
chün
eman
n H
. Ant
icoa
gula
tion
for
thro
mbo
sis
prop
hyla
xis
in c
ance
r pa
tient
s w
ith c
entr
al v
enou
s ca
thet
ers.
Coc
hran
e D
atab
ase
Syst
Rev
. 201
1;4:
CD
0064
68. S
ee T
able
S2,
S4,
S10
, S12
, and
S21
lege
nds
for
expa
nsio
n of
oth
er a
bbre
viat
ions
. a A
lloca
tion
clea
rly
conc
eale
d in
one
of t
he tw
o st
udie
s. N
one
of th
e st
udie
s bl
inde
d pa
tient
s, p
rovi
ders
, or
data
col
lect
ors,
but
bot
h st
udie
s bl
inde
d ou
tcom
e ad
judi
cato
rs. O
ne s
tudy
did
not
add
ress
Inc
om-
plet
e da
ta r
epor
ting.
Non
e of
the
stud
ies
was
sus
pect
ed o
f sel
ectiv
e re
port
ing.
One
stu
dy c
lear
ly u
sed
ITT.
b R
elat
ivel
y sm
all n
umbe
r of
eve
nts.
c C
I in
clud
es b
oth
valu
es s
ugge
stin
g no
eff
ect a
nd v
alue
s su
gges
ting
eith
er b
enefi
t or
har
m.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

40© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
3 —O
bse
rvat
iona
l St
udi
es o
f O
utp
atie
nts
wit
h R
estr
icte
d M
obil
ity
and
Nu
rsin
g H
ome
Pat
ient
s
Stud
y/Ye
arTy
pe o
f Stu
dyPa
rtic
ipan
tsIn
terv
entio
nO
utco
mes
Fol
low
-up
Res
ults
Lab
arèr
e et
al 45
/200
9Tw
o cr
oss-
sect
iona
l st
udie
s (B
osso
n et
al47
an
d Se
llier
et a
l46) a
t 50
pos
t-ac
ute
care
fa
cilit
ies
in F
ranc
e
� 6
5 y;
866
LM
WH
and
73
7 no
n-L
MW
HPr
ophy
lact
ic-d
ose
LM
WH
vs
no
LM
WH
(32%
re
ceiv
ed
antip
late
let)
Prox
imal
DV
T b
y sc
reen
ing
ultr
asou
ndN
A; c
ross
-sec
tiona
l st
udy
Prox
imal
DV
T r
educ
ed b
y L
MW
H fr
om 5
.7%
to
4.0%
( P 5
.16)
; pro
pens
ity
anal
ysis
OR
, 0.5
6 ( P
5 .0
3)
Selli
er e
t al 46
/200
8C
ross
-sec
tiona
l stu
dy o
f 40
hos
pita
l-bas
ed
post
-acu
te c
are
faci
litie
s in
Fra
nce
812
Patie
nts
aged
� 6
5 y
Non
ePr
oxim
al D
VT
by
scre
enin
g ul
tras
ound
NA
; cro
ss-s
ectio
nal
stud
yD
VT:
113
of 8
12 (1
4%);
33
(4%
) had
pro
xim
al D
VT;
in
depe
nden
t ris
k fa
ctor
s ag
e .
80
y (O
R, 1
.71)
, pr
evio
us V
TE
(OR
, 2.0
3),
regi
onal
/met
asta
tic c
ance
r (2
.71)
, dep
ende
nt in
� 3
A
DL
(2.1
8), p
ress
ure
ulce
r (1
.85)
Bos
son
et a
l 47 /2
003
Cro
ss-s
ectio
nal s
tudy
of
36 h
ospi
tal-b
ased
pos
t-ac
ute
care
faci
litie
s in
F
ranc
e
852
Patie
nts
aged
� 6
5 y;
52
% h
ad �
2 V
TE
ris
k fa
ctor
s be
side
s ag
e
Non
ePr
oxim
al D
VT
by
scre
enin
g ul
tras
ound
NA
; cro
ss-s
ectio
nal
stud
yD
VT:
135
of 8
52 (1
5.8%
); 50
(5
.9%
) had
pro
xim
al D
VT;
pr
ophy
lact
ic a
ntic
oagu
lant
56
% (r
ange
20.
0%-8
6.9%
);
Bos
son
et a
1 13 /2
006
Pros
pect
ive
obse
rvat
iona
l co
hort
stu
dy16
,532
Out
patie
nts
. 4
0 y
(med
ian
age,
71
y) w
ith
an a
cute
med
ical
co
nditi
on r
educ
ing
mob
ility
for a
t lea
st 4
8 h;
35
% re
ceiv
ed p
roph
ylax
is
Non
eSy
mpt
omat
ic V
TE
3 w
k �
7 d
VT
E in
cide
nce:
197
of
16,5
32 (1
.2%
); re
ceiv
ing
prop
hyla
xis
asso
ciat
ed
with
incr
ease
d in
cide
nce
of V
TE
(con
foun
ding
by
indi
catio
n)
Ben
oist
et a
l 48 /1
994
(Fre
nch)
Cro
ss-s
ectio
nal s
tudy
96 I
nstit
utio
naliz
ed
elde
rly
patie
nts
Non
eD
VT
by
scre
enin
g ul
tras
ound
NA
13 o
f 96
(13.
5%) D
VT;
all
popl
iteal
Gat
t et a
l 49 /2
004
Ret
rosp
ectiv
e ch
art
revi
ew47
1 N
H p
atie
nts
Non
eSy
mpt
omat
ic V
TE
Med
ian,
2.7
5 y
(ran
ge, 0
.25-
18.3
3)26
Pat
ient
s de
velo
ped
DV
T
sym
ptom
s; in
cide
nce
sim
ilar
in im
mob
ile
and
mob
ile g
roup
s (1
3.9
and
15.8
per
1,
000
patie
nt-y
ears
)
Kro
psky
et a
l 50 /2
003
Ret
rosp
ectiv
e ch
art
revi
ew24
6 N
H p
atie
nts
taki
ng
meg
estr
olN
one
Sym
ptom
atic
DV
TN
ot r
epor
ted
10 o
f 246
(4.9
%) D
VT
Gom
es 51
/200
3R
etro
spec
tive
coho
rt
stud
y us
ing
Min
imum
D
ata
Set
18,6
61 N
H p
atie
nts
in
Kan
sas
1997
-199
8;
med
ian
age,
85
y; 9
5%
whi
te; 7
4% w
omen
Non
eSy
mpt
omat
ic V
TE
Med
ian
follo
w-u
p 25
2 d
155
Patie
nts
deve
lope
d V
TE
; 1.3
0 pe
r 1,
00
pers
on-y
ears
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

41© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
arTy
pe o
f Stu
dyPa
rtic
ipan
tsIn
terv
entio
nO
utco
mes
Fol
low
-up
Res
ults
Vald
erra
ma
et a
l 52 /2
006
Pros
pect
ive
obse
rvat
iona
l co
hort
stu
dy87
NH
pat
ient
sN
one
Asy
mpt
omat
ic D
VT
on
scre
enin
g ul
tras
ound
4 m
o3
of 8
7 (3
.4%
) had
DV
T o
n in
itial
scr
eeni
ng a
t tim
e of
NH
adm
issi
on; 0
of 8
7 (0
%) d
evel
oped
DV
T o
ver
the
stud
y pe
riod
Lip
erot
i et a
l 53 /2
005
Ret
rosp
ectiv
e co
hort
st
udy
usin
g M
inim
um
Dat
a Se
t
132,
018
NH
res
iden
ts in
fi v
e U
S st
ates
Non
eH
ospi
taliz
atio
n fo
r V
TE
6 m
oV
TE
hos
pita
lizat
ion
0.91
pe
r 10
0 pe
rson
-yea
rs; r
ate
was
incr
ease
d fo
r us
ers
of
atyp
ical
ant
ipsy
chot
ics
Hei
t et a
l 54 /2
000
Popu
latio
n-ba
sed
nest
ed
case
-con
trol
stu
dy62
5 Pa
tient
s (in
stitu
tiona
lized
w
ithou
t rec
ent s
urge
ry)
with
a fi
rst V
TE
and
62
5 m
atch
ed c
ontr
ols
with
out a
DV
T
Non
eR
isk
fact
ors
for
VT
EU
niva
riat
e: N
H c
onfi n
emen
t O
R, 1
0.64
; mul
tivar
iate
: “i
nstit
utio
naliz
atio
n w
ithou
t rec
ent s
urge
ry”
OR
, 7.9
8
Hei
t et a
l 55 /2
002
Popu
latio
n-ba
sed
nest
ed
case
-con
trol
stu
dy62
5 Pa
tient
s w
ith a
fi rs
t V
TE
and
625
mat
ched
co
ntro
ls w
ithou
t a D
VT
Non
eA
ttri
buta
ble
risk
of r
isk
fact
ors
for
VT
EN
H r
esid
ence
acc
ount
ed fo
r 13
% o
f cas
es o
f VT
E
Rod
rigu
ez-M
anas
et
al 56
/201
0Pr
ospe
ctiv
e ob
serv
atio
nal
coho
rt s
tudy
Ger
iatr
ic o
utpa
tient
ce
nter
s (n
5 3
58) o
r H
ospi
tal-a
t-H
ome
Uni
ts (n
5 1
49)
bedr
idde
n fo
r at
leas
t 4
d; m
ean
age,
82
y
LM
WH
(b
emip
arin
) 2,
500
or 3
,500
In
tern
atio
nal
Uni
ts/d
; no
cont
rol a
rm
Sym
ptom
atic
DV
T o
r PE
; maj
or b
leed
; m
inor
ble
ed,
thro
mbo
cyto
peni
a
3 m
oTh
ree
of 5
07 (0
.6%
) dev
elop
ed
DV
T; 2
(0.4
%) d
evel
oped
m
ajor
ble
edin
g; 8
(1.6
%)
deve
lope
d m
inor
ble
edin
g (e
xclu
ding
hem
atom
a).
Ove
rall
blee
d ra
te 2
.0%
. M
ild th
rom
bocy
tope
nia
inci
denc
e, 1
.4%
; non
e ,
100
,000
or
requ
ired
di
scon
tinua
tion
Lei
bson
et a
l 57 /2
008
Nes
ted
case
-con
trol
st
udy
with
in
popu
latio
n-ba
sed
coho
rt s
tudy
Olm
sted
Cou
nty
resi
dent
s (n
5 1
24,2
77).
Use
d (1
) M
CM
RP
(whi
ch w
as a
pr
ecur
sor
to th
e M
inim
um D
ata
Set i
n N
Hs)
, and
(2) R
EP
data
set
Non
eV
TE
dia
gnos
is b
ased
on
IC
D-9
cod
es.
Fol
low
ed u
ntil
date
of
last
kno
wn
vita
l st
atus
Yiel
ds a
n in
cide
nce
of V
TE
in
NH
pat
ient
s of 1
2-15
per
1,
000
patie
nt-y
ears
usin
g M
CM
RP
and
a hi
gher
rate
(3
6 pe
r 1,0
00 p
atie
nt-y
ears
) us
ing
RE
P. F
ound
risk
fa
ctor
s are
uni
que
in th
e N
H p
opul
atio
n an
d re
late
to
mob
ility
stat
us (i
e, re
quire
as
sista
nce
with
tran
sfer
ring,
ne
ed fo
r PT,
wou
nd c
are)
ra
ther
than
the
trad
ition
al
risk
fact
ors (
canc
er, C
HF
).
Prie
to 58
/200
7 (S
pani
sh)
0.9%
VT
E in
cide
nce
AD
5 ac
tiviti
es o
f da
ily l
ivin
g; I
CD
-9 5
Inte
rnat
iona
l St
atis
tical
Cla
ssifi
catio
n of
Dis
ease
s an
d R
elat
ed H
ealth
Pro
blem
s, 9
th e
d.; M
CM
RP
5 M
inne
sota
Cas
e M
ix R
evie
w P
rogr
am; N
A, n
ot a
pplic
able
; N
H 5
nur
sing
hom
e; R
EP
5 R
oche
ster
Epi
dem
iolo
gic
Proj
ect.
Tabl
e S2
3—C
onti
nued
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

42© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
4 —Su
mm
ary
Tab
le f
or T
rial
s of
Pha
rmac
olog
ic P
roph
ylax
is t
o P
reve
nt V
TE
in
Air
Tra
vele
rs
Stud
y/Ye
arIn
terv
entio
nsR
isk
Gro
up ,†
Flig
ht D
urat
ion
Patie
nts
Ana
lyze
d (%
)Ti
me
to
Scre
enin
gD
VT,
%, R
R
(95%
CI)
SVT,
%, R
R
(95%
CI)
Ede
ma,
M
ean
(SD
)‡C
omm
ents
LM
WH
vs
no th
rom
bopr
ophy
laxi
s
Ces
aron
e et
al 59
/200
2N
o th
rom
bopr
ophy
laxi
sH
igh,
7-8
hN
o th
rom
bopr
ophy
laxi
s:
83 o
f 100
(83)
On
arri
val
No
thro
mbo
prop
hyla
xis:
4
of 8
3 (5
)N
o th
rom
bopr
ophy
laxi
s:
2 of
83
(2)
NR
Wei
ght-
base
d L
MW
H
dosi
ng r
educ
es
feas
ibili
ty
Eno
xapa
rin:
1 m
g/kg
, 2-
4 h
prefl
ight
Eno
xapa
rin:
0 o
f 82
Eno
xapa
rin:
1 o
f 82
(1)
Eno
xapa
rin:
82
of 1
00 (8
2)R
R, 0
.11
(0.0
0-2.
06)
RR
, 0.5
1 (0
.05-
5.47
)
Asp
irin
vs
no th
rom
bopr
ophy
laxi
s
Ces
aron
e et
al 59
/200
2N
o th
rom
bopr
ophy
laxi
sH
igh,
7-8
hN
o th
rom
bopr
ophy
laxi
s:
83 o
f 100
(83)
On
arri
val
No
thro
mbo
prop
hyla
xis:
4
of 8
3 (5
)N
o th
rom
bopr
ophy
laxi
s:
2 of
83
(2)
NR
Asp
irin
: 400
mg
3 3
d,
star
ting
12 h
pre
fl igh
tA
spir
in: 8
4 of
100
(84)
Asp
irin
: 3 o
f 84
(4%
)A
spir
in: 3
of 8
4 (4
)
RR
, 0.7
4 (0
.17-
3.21
)R
R, 1
.48
(0.2
5-8.
64)
Pycn
ogen
ol (a
bio
fl avo
noid
) vs
plac
ebo
Bel
caro
et
al 60
/200
4Pl
aceb
o ad
min
iste
red
iden
tical
lyM
oder
ate
to h
igh,
7-
12 h
(m
ean,
8 h
)
Plac
ebo
adm
inis
tere
d id
entic
ally
97
of
105
(92)
, 1
20 m
inPl
aceb
o: 1
of 9
7 (1
.0)
Plac
ebo:
4 o
f 97
(4.1
)N
RIn
act
ive
trea
tmen
t gr
oup
1 cl
inic
al
SVT
see
n bu
t not
cl
assi
fi ed
as s
uch—
no th
rom
bosi
s se
en
on u
ltras
ound
Pycn
ogen
ol 2
00 m
g 2-
3 h
befo
re fl
ight
, 20
0 m
g 6
h la
ter,
100
mg
the
next
day
; al
l with
250
mL
wat
er.
Pycn
ogen
ol 2
00 m
g 2-
3 h
befo
re fl
ight
, 200
mg
6 h
late
r, 10
0 m
g th
e ne
xt d
ay; a
ll w
ith
250
mL
wat
er: 1
01 o
f 10
6 (9
5%)
Pycn
ogen
ol: 0
of 1
01 (0
)Py
cnog
enol
: 0 o
f 101
(0)
All
DV
T
asym
ptom
atic
. All
SVT
sym
ptom
atic
.
NR
5 n
ot r
epor
ted;
SV
T 5
supe
rfi c
ial v
ein
thro
mbo
sis.
See
Tab
le S
2 an
d S4
lege
nds
for
expa
nsio
n of
oth
er a
bbre
viat
ions
.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

43© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
5 —M
etho
dolo
gic
Qu
alit
y of
Tri
als
Usi
ng P
harm
acol
ogic
Pro
phyl
axis
to
Pre
vent
VT
E i
n A
ir T
rave
lers
Stud
y/Ye
arIn
terv
entio
nR
ando
miz
atio
n C
once
aled
Blin
ding
No
Out
com
e (%
)A
naly
sis
Com
men
ts
LM
WH
vs
no th
rom
bopr
ophy
laxi
s
Ces
aron
e et
al 59
/200
2N
o th
rom
bopr
ophy
laxi
sPr
obab
ly n
ot (N
R)
Subj
ects
: no
No
thro
mbo
prop
hyla
xis:
17
of 1
00 (1
7)Pe
r pr
otoc
olA
bstr
act r
epor
ts a
n ad
ditio
nal s
ubje
ct g
roup
(L
MW
H 1
sock
s) n
ot
men
tione
d in
pub
licat
ion
Subj
ect r
ecru
itmen
t pro
cess
N
R
Eno
xapa
rin
1 m
g/kg
, 2-4
h
prefl
ight
Out
com
e as
sess
ors:
pr
obab
ly n
otF
light
dur
atio
n N
R
Eno
xapa
rin:
18
of 1
00 (1
8)M
etho
d of
ran
dom
izat
ion
NR
DV
T s
cree
ning
test
not
va
lidat
ed
Sour
ce o
f fun
ding
NR
Asp
irin
vs
no th
rom
bopr
ophy
laxi
s
Ces
aron
e et
al 59
/200
2N
o th
rom
bopr
ophy
laxi
sPr
obab
ly n
ot (N
R)
Subj
ects
: no
No
thro
mbo
prop
hyla
xis:
17
of 1
00 (1
7)Pe
r pr
otoc
olA
bstr
act r
epor
ts a
n ad
ditio
nal s
ubje
ct g
roup
(L
MW
H 1
sock
s) n
ot
men
tione
d in
pub
licat
ion
Subj
ect r
ecru
itmen
t pro
cess
N
R
Asp
irin
400
mg
3 3
d,
star
ting
12 h
pre
fl igh
tO
utco
me
asse
ssor
s:
prob
ably
not
Asp
irin
: 16
of 1
00 (1
6)
Flig
ht d
urat
ion
NR
Met
hod
of r
ando
miz
atio
n N
R
DV
T s
cree
ning
test
not
va
lidat
ed
Sour
ce o
f fun
ding
NR
Pycn
ogen
ol v
s pl
aceb
o
Bel
caro
et a
l 60 /2
004
Plac
ebo
adm
inis
tere
d id
entic
ally
Unk
now
nU
nkno
wn
for
subj
ects
or
ass
esso
rsPl
aceb
o: 5
VT
(1 D
VT,
4 S
VT
[w
ith th
rom
bosi
s])
Per
prot
ocol
Out
com
e no
nsta
ndar
dize
d
Prefl
ight
(with
in 9
0 m
in)
and
post
fl igh
t (w
ithin
12
0 m
in) u
ltras
ound
don
e.
Pycn
ogen
ol: 0
DV
T, 1
SV
T b
ut
not c
lass
ifi ed
as
such
Inco
nsis
tent
rep
ortin
g of
com
plet
ion
rate
of
part
icip
ants
.
Pycn
ogen
ol 2
00 m
g 2-
3 h
befo
re fl
ight
, 20
0 m
g 6
h la
ter,
100
mg
the
next
day
; al
l with
250
mL
wat
er.
Exc
lude
d th
ose
. 9
0 kg
or
190
cm
See
Tabl
e S2
, S4,
and
S24
lege
nds
for
expa
nsio
n of
abb
revi
atio
ns.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

44© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
6 —[S
ecti
on 6
.1.1
] E
vide
nce
Pro
fi le:
Sho
uld
Peo
ple
Tak
ing
Lon
g F
ligh
ts U
se C
ompr
essi
on S
tock
ings
vs
No
Com
pres
sion
Sto
ckin
gs?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
No.
of P
atie
nts
RR
(95%
CI)
Abs
olut
e R
isk
Qua
lity
No.
of S
tudi
es
(Des
ign)
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Publ
icat
ion
Bia
s
With
out
Com
pres
sion
St
ocki
ngs a
With
C
ompr
essi
on
Stoc
king
sC
ontr
ol R
ate
Ris
k D
iffer
ence
(9
5% C
I)
Sym
ptom
atic
DV
T
Dir
ect e
vide
nce
9 (R
CT
)N
o se
riou
s lim
itatio
ns b
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s im
prec
isio
n c U
ndet
ecte
d0
of 1
,323
0 of
1,3
14N
ot e
stim
able
(n
o ev
ents
)0
per
1,00
00
per
1,00
0 ( 2
1.5
to 1
.5)
Mod
erat
e
Indi
rect
evi
denc
e (b
ased
on
sym
ptom
less
DV
T a
s a
surr
ogat
e ou
tcom
e fo
r sy
mpt
omat
ic D
VT
)
9 (R
CT
)N
o se
riou
s lim
itatio
ns b
No
seri
ous
inco
nsis
tenc
ySe
riou
s in
dire
ctne
ss d
No
seri
ous
impr
ecis
ion
Und
etec
ted
Surr
ogat
e sy
mpt
omle
ss
DV
T: 4
7 of
1,
323
Surr
ogat
e sy
mpt
omle
ss
DV
T: 3
of
1,31
4
RR
, 0.1
0 (0
.04-
0.25
)5
per
10,0
00L
ow r
isk
Mod
erat
e
4.5
per
10,0
00
(4 to
5)
18 p
er 1
0,00
0H
igh
risk
16.2
per
10,
000
(14
to 1
7.5)
PE
Dir
ect e
vide
nce
9 (R
CT
)N
o se
riou
s lim
itatio
ns b
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssN
o se
riou
s im
prec
isio
nU
ndet
ecte
d0
of 1
,323
0 of
1,3
14N
ot e
stim
able
(n
o ev
ents
)0
per
1,00
00
per
1,00
0 ( 2
1.5
to 1
.5)
Hig
h
Indi
rect
evi
denc
e (b
ased
on
sym
ptom
less
DV
T a
s a
surr
ogat
e ou
tcom
e fo
r sy
mpt
omat
ic D
VT
)
9 (R
CT
)N
o se
riou
s lim
itatio
ns b
No
seri
ous
inco
nsis
tenc
ySe
riou
s in
dire
ctne
ss d
No
seri
ous
impr
ecis
ion
Und
etec
ted
Surr
ogat
e sy
mpt
omle
ss
DV
T: 4
7 of
1,
323
Surr
ogat
e sy
mpt
omle
ss
DV
T: 3
of
1,31
4
RR
, 0.1
0 (0
.04-
0.25
)27
per
1 m
illio
nL
ow r
isk
Mod
erat
e
24 p
er 1
mill
ion
(20
to 2
6)
97 p
er 1
mill
ion
Hig
h ri
sk
87 p
er 1
mill
ion
(76
to 9
4)
SVT
8 (R
CT
)N
o se
riou
s lim
itatio
ns b
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s im
prec
isio
n c U
ndet
ecte
d12
of 9
014
of 9
03R
R, 0
.45
(0.1
8-1.
13)
13 p
er 1
,000
Not
sig
nifi c
ant
Mod
erat
e
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

45© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
6—C
onti
nued
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
No.
of P
atie
nts
RR
(95%
CI)
Abs
olut
e R
isk
Qua
lity
No.
of S
tudi
es
(Des
ign)
Lim
itatio
nsIn
cons
iste
ncy
Indi
rect
ness
Impr
ecis
ion
Publ
icat
ion
Bia
s
With
out
Com
pres
sion
St
ocki
ngs a
With
C
ompr
essi
on
Stoc
king
sC
ontr
ol R
ate
Ris
k D
iffer
ence
(9
5% C
I)
Ede
ma
(pos
tfl ig
ht v
alue
s m
easu
red
on a
sca
le fr
om 0
, no
edem
a, to
10,
max
imum
ede
ma)
6 (R
CT
)Ve
ry s
erio
us
limita
tions
e N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
No
seri
ous
impr
ecis
ion
Und
etec
ted
7- o
r 8-
h F
light
…W
eigh
ted
mea
n di
ffer
ence
: 2
4.7
2 ( 2
4.9
1 to
2 4
.52)
Low
Mea
n, 6
.4-6
.9M
ean,
2.2
-2.4
349
Part
icip
ants
348
Part
icip
ants
12-h
Flig
htF
avor
s st
ocki
ngs
Mea
n, 7
.9-8
.9M
ean,
2.6
-3.3
272
Part
icip
ants
277
Part
icip
ants
Adv
erse
eff
ects
f
4 (R
CT
)Ve
ry s
erio
us
limita
tions
e N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
No
seri
ous
impr
ecis
ion
Und
etec
ted
0 of
1,1
820
of 1
,182
Not
ava
ilabl
eT
he to
lera
bilit
y of
th
e st
ocki
ngs
was
des
crib
ed
as v
ery
good
w
ith n
o co
mpl
aint
s of
si
de e
ffec
ts
Low
Bib
liogr
aphy
: C
lark
e M
, H
opew
ell
S, J
uszc
zak
E,
Eis
inga
A,
Kje
ldst
rom
M.
Com
pres
sion
sto
ckin
gs f
or p
reve
ntin
g de
ep v
ein
thro
mbo
sis
in a
irlin
e pa
ssen
gers
. C
ochr
ane
Dat
abas
e Sy
st R
ev .
2006
; (2
):C
D00
4002
. Phi
lbri
ck J
T, S
hum
ate
R, S
iada
ty M
S, e
t al
. Air
tra
vel a
nd v
enou
s th
rom
boem
bolis
m: a
sys
tem
atic
rev
iew
. J G
en I
nter
n M
ed. 2
007;
22:1
07-1
14. A
ll th
e st
ocki
ngs
in t
he n
ine
tria
ls
incl
uded
in th
is r
evie
w w
ere
belo
w-k
nee
com
pres
sion
sto
ckin
gs. I
n fo
ur tr
ials
the
com
pres
sion
str
engt
h w
as 2
0 to
30
mm
Hg
at th
e an
kle.
It w
as 1
0 to
20
mm
Hg
in th
e ot
her
four
tria
ls. S
tock
ings
com
e in
di
ffer
ent s
izes
. If a
sto
ckin
g is
too
tight
aro
und
the
knee
it c
an p
reve
nt e
ssen
tial v
enou
s re
turn
cau
sing
the
bloo
d to
poo
l aro
und
the
knee
. Com
pres
sion
sto
ckin
gs s
houl
d be
fi tt
ed p
rope
rly.
A s
tock
ing
that
is
too
tight
cou
ld c
ut in
to th
e sk
in o
n a
long
fl ig
ht a
nd p
oten
tially
cau
se u
lcer
atio
n an
d in
crea
sed
risk
of D
VT.
Som
e st
ocki
ngs
can
be s
light
ly th
icke
r th
an n
orm
al le
g co
veri
ng a
nd c
an b
e po
tent
ially
res
tric
tive
with
tigh
t foo
t wea
r. It
is a
goo
d id
ea to
wea
r st
ocki
ngs
arou
nd th
e ho
use
prio
r to
trav
el to
ens
ure
a go
od, c
omfo
rtab
le fi
ttin
g. S
tock
ings
wer
e pu
t on
2 to
3 h
bef
ore
the
fl igh
t in
mos
t of t
he tr
ials
. The
ava
il-ab
ility
and
cos
t of s
tock
ings
can
var
y. S
ee T
able
S1,
S3,
S4,
and
S24
lege
nds
for
expa
nsio
n of
abb
revi
atio
ns.
a Est
imat
es f
or c
ontr
ol e
vent
rat
es f
or v
enou
s th
rom
bosi
s an
d fo
r PE
com
e fr
om P
hilb
rick
et
al . D
efi n
ition
of
high
ris
k in
clud
es p
revi
ous
epis
odes
of
DV
T, c
oagu
latio
n di
sord
ers,
sev
ere
obes
ity, l
imite
d m
obili
ty d
ue to
bon
e or
join
t pro
blem
s, n
eopl
astic
dis
ease
with
in th
e pr
evio
us 2
yea
rs, l
arge
var
icos
e ve
ins.
b W
e di
d no
t rat
e do
wn
for
met
hodo
logi
cal l
imita
tion,
alth
ough
ther
e w
as in
adeq
uate
con
ceal
men
t of a
lloca
tion
and
blin
ding
. c T
he im
prec
isio
n re
fers
to a
bsol
ute
mea
sure
s, n
ot th
e re
lativ
e. F
or th
e re
lativ
e, it
is n
ot p
ossi
ble
to m
ake
an e
stim
ate.
Thi
s is
als
o tr
ue fo
r PE
. d T
here
are
two
reas
ons
for
indi
rect
ness
. One
is th
at e
stim
ates
of R
R r
educ
tion
com
e fr
om th
e su
rrog
ate.
The
sec
ond
is th
at th
ere
is u
ncer
tain
ty r
egar
ding
the
base
line
risk
. e L
ack
of c
once
alm
ent a
nd b
lindi
ng c
onst
itute
d ve
ry s
erio
us li
mita
tions
in th
e co
ntex
t of a
n un
valid
ated
ede
ma
ratin
g an
d de
scri
ptio
n of
tole
rabi
lity
of s
tock
ings
. f N
one
of th
e ot
her
tria
ls r
epor
ted
adve
rse
effe
cts,
apa
rt fr
om fo
ur c
ases
of S
VT
in v
aric
ose
vein
s in
the
knee
reg
ion
that
wer
e co
mpr
esse
d by
the
uppe
r ed
ge o
f the
sto
ckin
g in
one
tria
l.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
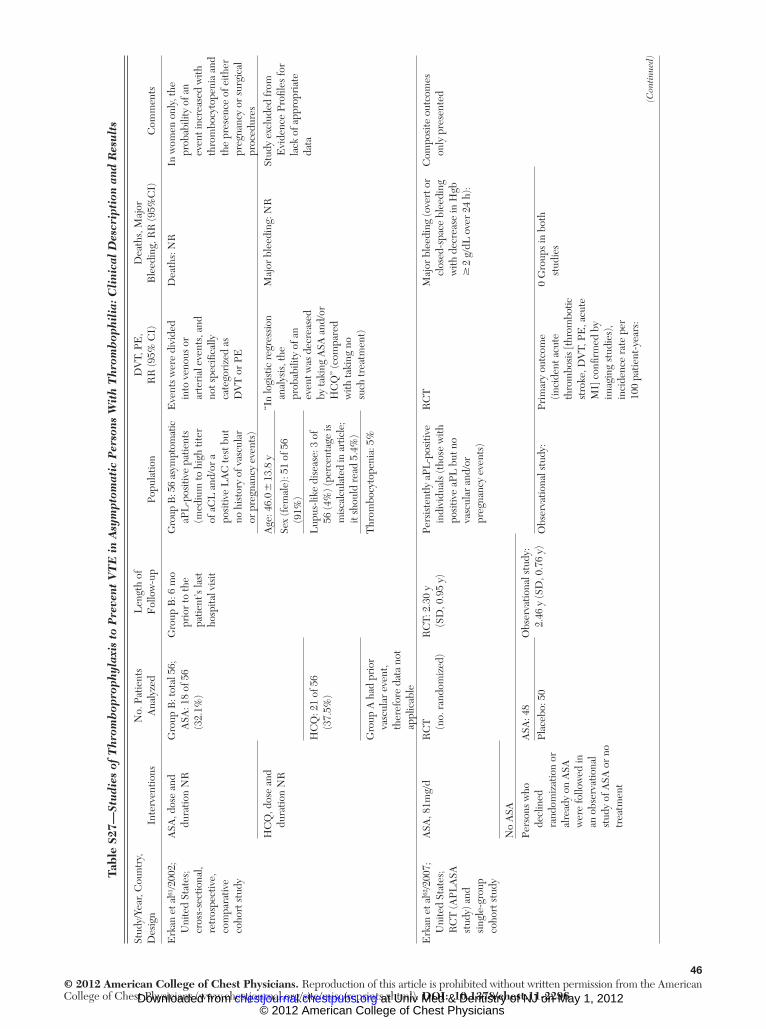
46© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
7 —St
udi
es o
f T
hrom
bop
roph
ylax
is t
o P
reve
nt V
TE
in
Asy
mpt
omat
ic P
erso
ns W
ith
Thr
omb
ophi
lia:
Cli
nica
l D
escr
ipti
on a
nd R
esu
lts
Stud
y/Ye
ar, C
ount
ry,
Des
ign
Inte
rven
tions
No.
Pat
ient
s A
naly
zed
Len
gth
of
Fol
low
-up
Popu
latio
nD
VT,
PE
, R
R (9
5% C
I)D
eath
s, M
ajor
B
leed
ing,
RR
(95%
CI)
Com
men
ts
Erk
an e
t al 61
/200
2;
Uni
ted
Stat
es;
cros
s-se
ctio
nal,
retr
ospe
ctiv
e,
com
para
tive
coho
rt s
tudy
ASA
, dos
e an
d du
ratio
n N
RG
roup
B: t
otal
56;
A
SA: 1
8 of
56
(32.
1%)
Gro
up B
: 6 m
o pr
ior
to th
e pa
tient
’s la
st
hosp
ital v
isit
Gro
up B
: 56
asym
ptom
atic
aP
L-p
ositi
ve p
atie
nts
(med
ium
to h
igh
titer
of
aC
L a
nd/o
r a
posi
tive
LA
C te
st b
ut
no h
isto
ry o
f vas
cula
r or
pre
gnan
cy e
vent
s)
Eve
nts
wer
e di
vide
d in
to v
enou
s or
ar
teri
al e
vent
s, a
nd
not s
peci
fi cal
ly
cate
gori
zed
as
DV
T o
r PE
Dea
ths:
NR
In w
omen
onl
y, th
e pr
obab
ility
of a
n ev
ent i
ncre
ased
with
th
rom
bocy
tope
nia
and
the
pres
ence
of e
ither
pr
egna
ncy
or s
urgi
cal
proc
edur
es
HC
Q, d
ose
and
dura
tion
NR
Age
: 46.
0 �
13.
8 y
“In
logi
stic
reg
ress
ion
anal
ysis
, the
pr
obab
ility
of a
n ev
ent w
as d
ecre
ased
by
taki
ng A
SA a
nd/o
r H
CQ
” (c
ompa
red
with
taki
ng n
o su
ch tr
eatm
ent)
Maj
or b
leed
ing:
NR
Stud
y ex
clud
ed fr
om
Evi
denc
e Pr
ofi le
s fo
r la
ck o
f app
ropr
iate
da
ta
Sex
(fem
ale)
: 51
of 5
6 (9
1%)
HC
Q: 2
1 of
56
(37.
5%)
Lup
us-li
ke d
isea
se: 3
of
56 (4
%) (
perc
enta
ge is
m
isca
lcul
ated
in a
rtic
le;
it sh
ould
rea
d 5.
4%)
Gro
up A
had
pri
or
vasc
ular
eve
nt,
ther
efor
e da
ta n
ot
appl
icab
le
Thr
ombo
cyto
peni
a: 5
%
Erk
an e
t al 62
/200
7;
Uni
ted
Stat
es;
RC
T (A
PLA
SA
stud
y) a
nd
sing
le-g
roup
co
hort
stu
dy
ASA
, 81m
g/d
RC
T
(no.
ran
dom
ized
)R
CT:
2.3
0 y
(SD
, 0.9
5 y)
Pers
iste
ntly
aPL
-pos
itive
in
divi
dual
s (t
hose
with
po
sitiv
e aP
L b
ut n
o va
scul
ar a
nd/o
r pr
egna
ncy
even
ts)
RC
TM
ajor
ble
edin
g (o
vert
or
clos
ed-s
pace
ble
edin
g w
ith d
ecre
ase
in H
gb
� 2
g/d
L o
ver
24 h
):
Com
posi
te o
utco
mes
on
ly p
rese
nted
No
ASA
Pers
ons
who
de
clin
ed
rand
omiz
atio
n or
al
read
y on
ASA
w
ere
follo
wed
in
an o
bser
vatio
nal
stud
y of
ASA
or
no
trea
tmen
t
ASA
: 48
Plac
ebo:
50
Obs
erva
tiona
l stu
dy:
2.46
y (S
D, 0
.76
y)
Obs
erva
tiona
l stu
dy:
Prim
ary
outc
ome
(inci
dent
acu
te
thro
mbo
sis [
thro
mbo
tic
stro
ke, D
VT,
PE
, acu
te
MI]
con
fi rm
ed b
y im
agin
g st
udie
s),
inci
denc
e ra
te p
er
100
patie
nt-y
ears
:
0 G
roup
s in
bot
h st
udie
s
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

47© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
7—C
onti
nued
Stud
y/Ye
ar, C
ount
ry,
Des
ign
Inte
rven
tions
No.
Pat
ient
s A
naly
zed
Len
gth
of
Fol
low
-up
Popu
latio
nD
VT,
PE
, R
R (9
5% C
I)D
eath
s, M
ajor
B
leed
ing,
RR
(95%
CI)
Com
men
ts
Obs
erva
tiona
l stu
dy
ASA
: 61
of 7
4 (8
2.4%
)
A
ge, m
ean
� S
D
ASA
: 2.7
5
A
SA: 4
7.8
� 1
4.8
y
No
ASA
: 0
No
ASA
: 13
of 7
4 (1
7.6%
)N
o A
SA: 4
6.2
� 1
4.1
yH
R, 1
.04
(95%
CI,
0.6
9-1.
56),
P 5
.83
Sex
(no.
wom
en),
Seco
ndar
y ou
tcom
e
(tra
nsie
nt is
chem
ic
atta
ck),
inci
denc
e ra
te
per 1
00 p
atie
nt-y
ears
:
ASA
: 58
of 6
1 (9
5%)
A
SA: 1
.83
No
ASA
: 13
of
13 (1
00%
)
No
ASA
: 0.8
6
H
R, 1
.08
(95%
CI,
0.
72-1
.62)
, P 5
.68
Obs
erva
tiona
l stu
dy
pr
imar
y ou
tcom
e (a
s ab
ove)
:
A
SA: 2
.70
N
o A
SA: 0
Seco
ndar
y ou
tcom
e:
0 bo
th g
roup
s
Gly
nn e
t al 63
/200
7;
Uni
ted
Stat
es; R
CT
(s
ubgr
oup
anal
yses
of
Wom
en’s
Hea
lth
Stud
y)
ASA
, 100
mg
ever
y 2
days
for
10 y
Tota
l No.
allo
cate
d in
Wom
en’s
Hea
lth S
tudy
:
Med
ian
follo
w-u
p,
10.2
y (I
QR
, 9.
7-10
.6 y
)
Tota
l pop
ulat
ion:
39,
876
initi
ally
hea
lthy
wom
en
age
� 4
5 y
Fac
tor
V L
eide
n pr
esen
t (u
nkno
wn
% h
ad p
rior
V
TE
):
NR
for
thro
mbo
phili
a su
bgro
up3%
of e
ntir
e st
udy
popu
latio
n ha
d pr
ior
VT
E, b
ut in
pop
ulat
ion
of in
tere
st (f
acto
r V
L
eide
n) a
n un
cert
ain
% h
ad p
rior
VT
E
No
ASA
ASA
: 19,
934
(5.2
%
had
fact
or V
L
eide
n 5
1,0
37)
Rat
e di
ffer
ence
per
1,
000
patie
nt-y
ears
, A
SA v
s pla
cebo
: 2 0
.50
(95%
CI,
2 2
.26
to
1.26
)
In p
atie
nts
with
fact
or
V L
eide
n or
the
prot
hrom
bin
mut
atio
n,
the
inci
denc
e of
VT
E
in th
e pl
aceb
o gr
oup
was
2.7
tim
es th
at o
f w
omen
in th
e pl
aceb
o gr
oup
with
out e
ither
ri
sk fa
ctor
No
ASA
: 19,
942
(5.1
% h
ad fa
ctor
V
Lei
den
5 1
,017
)
Tota
l with
fact
or V
L
eide
n pr
esen
t an
d da
ta fo
r A
SA
effe
ct: 1
,370
HR
, 0.8
1 (9
5% C
I,
0.42
-1.5
4)
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
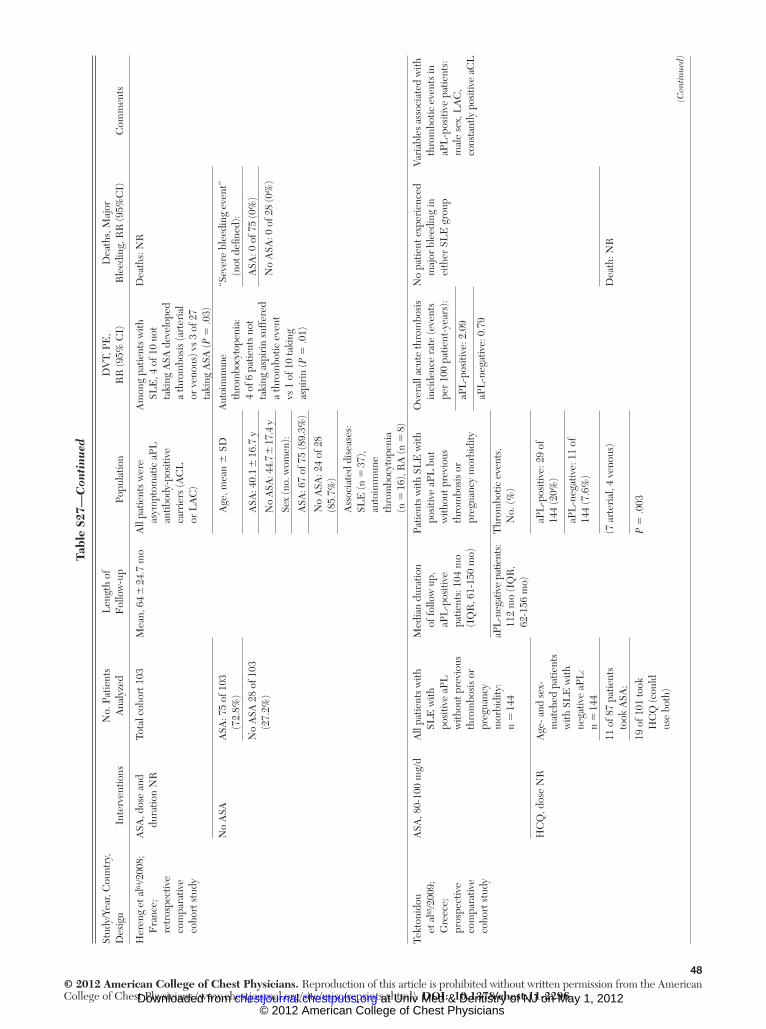
48© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
ar, C
ount
ry,
Des
ign
Inte
rven
tions
No.
Pat
ient
s A
naly
zed
Len
gth
of
Fol
low
-up
Popu
latio
nD
VT,
PE
, R
R (9
5% C
I)D
eath
s, M
ajor
B
leed
ing,
RR
(95%
CI)
Com
men
ts
Her
eng
et a
l 64 /2
008;
F
ranc
e;
retr
ospe
ctiv
e co
mpa
rativ
e co
hort
stu
dy
ASA
, dos
e an
d du
ratio
n N
RTo
tal c
ohor
t 103
Mea
n, 6
4 �
24.
7 m
oA
ll pa
tient
s w
ere
asym
ptom
atic
aPL
an
tibod
y-po
sitiv
e ca
rrie
rs (A
CL
or
LA
C)
Am
ong
patie
nts
with
SL
E, 4
of 1
0 no
t ta
king
ASA
dev
elop
ed
a th
rom
bosi
s (a
rter
ial
or v
enou
s) v
s 3
of 2
7 ta
king
ASA
( P 5
.03)
Dea
ths:
NR
No
ASA
ASA
: 75
of 1
03
(72.
8%)
Age
, mea
n �
SD
Aut
oim
mun
e th
rom
bocy
tope
nia:
4
of 6
pat
ient
s no
t ta
king
asp
irin
suf
fere
d a
thro
mbo
tic e
vent
vs
1 o
f 10
taki
ng
aspi
rin
( P 5
.01)
“Sev
ere
blee
ding
eve
nt”
(not
defi
ned
):
No
ASA
28
of 1
03
(27.
2%)
ASA
: 40.
1 �
16.
7 y
A
SA: 0
of 7
5 (0
%)
No
ASA
: 44.
7 � 17
.4 y
N
o A
SA: 0
of 2
8 (0
%)
Sex
(no.
wom
en):
ASA
: 67
of 7
5 (8
9.3%
)
No
ASA
: 24
of 2
8 (8
5.7%
)
Ass
ocia
ted
dise
ases
: SL
E (n
5 3
7),
auto
imm
une
thro
mbo
cyto
peni
a (n
5 1
6), R
A (n
5 8
)
Tekt
onid
ou
et a
l 65 /2
009;
G
reec
e;
pros
pect
ive
com
para
tive
coho
rt s
tudy
ASA
, 80-
100
mg/
dA
ll pa
tient
s w
ith
SLE
with
po
sitiv
e aP
L
with
out p
revi
ous
thro
mbo
sis
or
preg
nanc
y m
orbi
dity
: n
5 1
44
Med
ian
dura
tion
of fo
llow
up,
aP
L-p
ositi
ve
patie
nts:
104
mo
(IQ
R, 6
1-15
0 m
o)
aPL
-neg
ativ
e pa
tient
s: 11
2 m
o (I
QR
, 62
-156
mo)
Patie
nts
with
SL
E w
ith
posi
tive
aPL
but
w
ithou
t pre
viou
s th
rom
bosi
s or
pr
egna
ncy
mor
bidi
ty
Thr
ombo
tic e
vent
s,
No.
(%)
Ove
rall
acut
e th
rom
bosi
s in
cide
nce
rate
(eve
nts
per
100
patie
nt-y
ears
):
aP
L-p
ositi
ve: 2
.09
aP
L-n
egat
ive:
0.7
9
No
patie
nt e
xper
ienc
ed
maj
or b
leed
ing
in
eith
er S
LE
gro
up
Vari
able
s as
soci
ated
with
th
rom
botic
eve
nts
in
aPL
-pos
itive
pat
ient
s:
mal
e se
x, L
AC
, co
nsta
ntly
pos
itive
aC
L
HC
Q, d
ose
NR
Age
- and
sex
-m
atch
ed p
atie
nts
with
SL
E w
ith
nega
tive
aPL
: n
5 1
44
aP
L-p
ositi
ve: 2
9 of
14
4 (2
0%)
aP
L-n
egat
ive:
11
of
144
(7.6
%)
11 o
f 87
patie
nts
took
ASA
;(7
art
eria
l, 4
veno
us)
Dea
th: N
R
19 o
f 101
took
H
CQ
(cou
ld
use
both
)
P 5
.003
Tabl
e S2
7—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

49© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
ar, C
ount
ry,
Des
ign
Inte
rven
tions
No.
Pat
ient
s A
naly
zed
Len
gth
of
Fol
low
-up
Popu
latio
nD
VT,
PE
, R
R (9
5% C
I)D
eath
s, M
ajor
B
leed
ing,
RR
(95%
CI)
Com
men
ts
Una
djus
ted
RR
in
aPL
-pos
itive
pat
ient
s fo
r tr
eatm
ent:
ASA
vs
no A
SA fo
r th
rom
bosi
s:
HR
, 0.4
3; 9
5% C
I,
0.20
-0.9
1; P
5 .0
27
HC
Q: H
R, 0
.67
(95%
CI,
0.
31-1
.45)
, P 5
.30
Adj
uste
d an
alys
es: H
R
per
1 m
o in
aP
L-p
ositi
ve p
atie
nts
for
risk
of t
hrom
botic
ev
ents
:
ASA
vs
no A
SA: H
R, 0
.98
(95%
CI,
0.9
6-0.
99),
P 5
.05
HC
Q v
s no
ne: H
R, 0
.99
(95%
CI,
0.9
8 to
1.0
0),
P 5
.05
Com
bina
tion
ther
apy
resu
lts N
R
aCL
5 a
ntic
ardi
olip
in; a
PL 5
ant
ipho
spho
lipid
ant
ibod
ies;
HC
Q 5
hyd
roxy
chlo
roqu
ine;
LA
C 5
lupu
s an
ticoa
gula
nt; S
LE
5 s
yste
mic
lupu
s er
ythe
mat
osus
. See
Tab
le S
1, S
3, S
4, S
7, S
17, a
nd S
24 le
gend
s fo
r ex
pans
ion
of a
bbre
viat
ions
.
Tabl
e S2
7—C
onti
nued
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

50© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
8 —R
CT
s of
Thr
omb
opro
phyl
axis
to
Pre
vent
VT
E i
n A
sym
ptom
atic
Per
sons
Wit
h T
hrom
bop
hili
a: M
etho
dolo
gic
Qu
alit
y
Stud
y/Ye
arC
once
alm
ent o
f A
lloca
tion
Blin
ding
of P
atie
nts
Blin
ding
of
Hea
lth-c
are
Prov
ider
sB
lindi
ng o
f Dat
a C
olle
ctor
sB
lindi
ng o
f Out
com
e A
djud
icat
ors
Blin
ding
of D
ata
Ana
lyst
sSt
oppe
d E
arly
F
or B
enefi
tIT
T C
omm
ents
Erk
an e
t al 62
/200
7D
YD
YD
YD
YPY
PYD
YD
Y
Cen
tral
ized
al
loca
tion
with
co
mpu
ter-
gene
rate
d ra
ndom
izat
ion
tabl
e
“Inv
estig
ator
s,
coor
dina
tors
, pa
rtic
ipan
ts w
ere
blin
ded
to th
e tr
eatm
ent
assi
gnm
ents
”
Patie
nt r
ecru
itmen
t te
rmin
ated
ear
ly a
s lo
wer
-tha
n-ex
pect
ed
even
t rat
es in
bot
h gr
oups
; lar
ger
sam
ple
size
unf
easi
ble
Gly
nn e
t al 63
/200
7D
YD
YD
YD
YD
YD
YN
oD
Y
Subg
roup
ana
lysi
s of
R
CT
(Wom
en’s
Hea
lth s
tudy
)
Subg
roup
ana
lyse
s w
ere
pres
peci
fi ed.
In
pop
ulat
ion
of
inte
rest
(fac
tor
V
Lei
den)
an
unce
rtai
n %
had
pri
or V
TE
; in
over
all p
opul
atio
n 2.
9% h
ad p
rior
VT
E,
but i
n pa
tient
s w
ith
fact
or V
Lei
den
or
the
prot
hrom
bin
mut
atio
n th
e in
cide
nce
of V
TE
in
the
plac
ebo
grou
p w
as 2
.7 ti
mes
that
of
wom
en in
the
plac
ebo
grou
p w
ithou
t ei
ther
ris
k fa
ctor
D
Y 5
defi
nite
ly y
es; P
Y 5
pro
babl
y ye
s. S
ee T
able
S3
and
S10
lege
nds
for
expa
nsio
n of
oth
er a
bbre
viat
ions
.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

51© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S2
9 —O
bse
rvat
iona
l St
udi
es o
f T
hrom
bop
roph
ylax
is t
o P
reve
nt V
TE
in
Asy
mpt
omat
ic P
erso
ns W
ith
Thr
omb
ophi
lia:
Met
hodo
logi
c Q
ual
ity
Stud
y/Ye
arIn
terv
entio
n/C
ompa
rato
rSt
udy
Des
ign
Inte
rven
tion/
Con
trol
Se
ttin
g Si
mila
rIn
terv
entio
n/C
ontr
ol
Tim
e F
ram
e Si
mila
rA
djus
tmen
tE
ffec
tivel
y B
linde
d A
sses
smen
t of O
utco
me
Los
s to
Fol
low
-up
Erk
an e
t al 62
/200
7A
SA, 8
1 m
g/d
Pros
pect
ive
com
para
tive
coho
rt s
tudy
(RC
T
qual
ity is
ass
esse
d in
se
para
te ta
ble)
DY
DY
NR
PYA
SA: 2
of 6
1 (3
.3%
); 6
with
draw
als
No
ASA
Fol
low
-up
inte
rval
s si
mila
r, co
ntem
pora
neou
s da
ta c
olle
ctio
n
No
ASA
: 0 o
f 13
(0%
); 2
with
draw
als
Erk
an e
t al 61
/200
2B
oth
ASA
and
H
CQ
exa
min
ed
(stu
dy e
xclu
ded
from
E
vide
nce
Profi
le)
Cro
ss-s
ectio
nal,
retr
ospe
ctiv
e,
com
para
tive
stud
y
PYPY
NR
DN
NA
(ret
rosp
ectiv
e)
ASA
(dos
e an
d du
ratio
n N
R)
vs n
o tr
eatm
ent
HC
Q (d
ose
and
dura
tion
NR
) vs
no
trea
tmen
t
Gro
up A
had
had
an
eve
nt, G
roup
B
was
asy
mpt
omat
ic;
sign
ifi ca
nt d
iffer
ence
s be
twee
n th
e tw
o gr
oups
Her
eng
et a
l 64 /2
008
ASA
: dos
e an
d du
ratio
n N
RR
etro
spec
tive
com
para
tive
coho
rt s
tudy
PY (1
0 pa
tient
s w
ere
not f
ollo
wed
in
sam
e de
part
men
t)
DY
NR
DN
3 of
108
(27.
8%)
othe
r pa
tient
s re
ceiv
ed lo
ng-t
erm
an
ticoa
gula
tion
No
ASA
Gro
ups
diff
ered
on
%
aCL
, IgG
, and
IgM
( P
, .0
5), t
hus
diff
er
in th
rom
bosi
s ri
sk
Tekt
onid
ou e
t al 65
/200
9B
oth
ASA
and
H
CQ
exa
min
edPr
ospe
ctiv
e co
mpa
rativ
e co
hort
stu
dy
DY
DY
Sex,
LA
C,
age,
sm
okin
g,
com
orbi
d co
nditi
ons
PNC
ohor
t was
follo
wed
to
dat
e of
last
vis
it or
to e
vent
A
SA (8
0-10
0 m
g/d)
vs
no
trea
tmen
t
HC
Q (d
ose
NR
) vs
no
trea
tmen
tR
ecru
ited
from
sa
me
clin
ic
DN
5 d
efi n
itely
no;
PN
5 p
roba
bly
no. S
ee T
able
S7,
S24
, S27
, and
S28
lege
nds
for
expa
nsio
n of
abb
revi
atio
ns.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
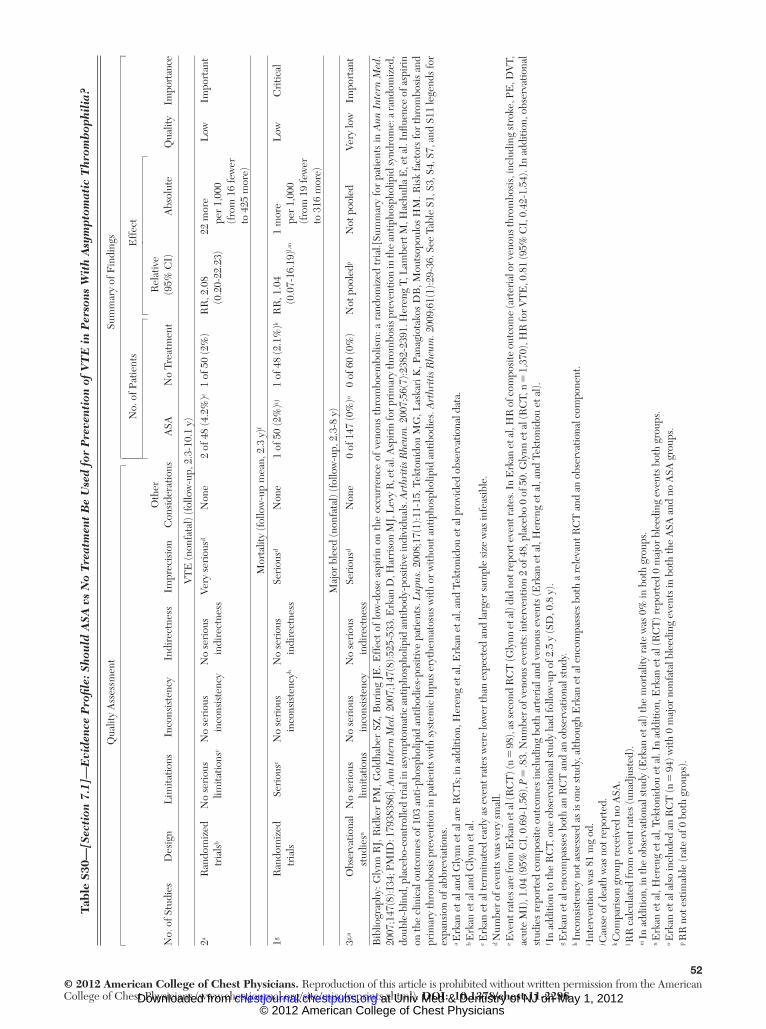
52© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S3
0 —[S
ecti
on 7
.1]—
Evi
denc
e P
rofi l
e: S
hou
ld A
SA v
s N
o T
reat
men
t B
e U
sed
for
Pre
vent
ion
of V
TE
in
Per
sons
Wit
h A
sym
ptom
atic
Thr
omb
ophi
lia?
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
N
o. o
f Pat
ient
sE
ffec
t
No.
of S
tudi
esD
esig
nL
imita
tions
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
C
onsi
dera
tions
ASA
No
Trea
tmen
tR
elat
ive
(95%
CI)
Abs
olut
e Q
ualit
y Im
port
ance
VT
E (n
onfa
tal)
(fol
low
-up,
2.3
-10.
1 y)
2 a R
ando
miz
ed
tria
ls b
No
seri
ous
limita
tions
c N
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
Very
ser
ious
d N
one
2 of
48
(4.2
%) e
1 of
50
(2%
)R
R, 2
.08
(0.2
0-22
.23)
22 m
ore
per
1,00
0 (f
rom
16
few
er
to 4
25 m
ore)
Low
Impo
rtan
t
Mor
talit
y (f
ollo
w-u
p m
ean,
2.3
y) f
1 g R
ando
miz
ed
tria
lsSe
riou
s c N
o se
riou
s in
cons
iste
ncy h
No
seri
ous
indi
rect
ness
Seri
ous d
Non
e1
of 5
0 (2
%) i , j
1 of
48
(2.1
%) k
RR
, 1.0
4 (0
.07-
16.1
9) l , m
1
mor
e pe
r 1,
000
(fro
m 1
9 fe
wer
to
316
mor
e)
Low
Cri
tical
Maj
or b
leed
(non
fata
l) (f
ollo
w-u
p, 2
.3-8
y)
3 g , n O
bser
vatio
nal
stud
ies n
No
seri
ous
limita
tions
No
seri
ous
inco
nsis
tenc
yN
o se
riou
s in
dire
ctne
ssSe
riou
s d N
one
0 of
147
(0%
) o 0
of 6
0 (0
%)
Not
poo
led p
Not
poo
led
Very
low
Impo
rtan
t
Bib
liogr
aphy
: Gly
nn R
J, R
idke
r PM
, Gol
dhab
er S
Z, B
urin
g JE
. Eff
ect
of lo
w-d
ose
aspi
rin
on t
he o
ccur
renc
e of
ven
ous
thro
mbo
embo
lism
: a r
ando
miz
ed t
rial
.[Sum
mar
y fo
r pa
tient
s in
Ann
Int
ern
Med
. 20
07;1
47(8
):I34
; PM
ID: 1
7938
386]
. Ann
Int
ern
Med
. 200
7;14
7(8)
:525
-533
. Erk
an D
, Har
riso
n M
J, L
evy
R, e
t al.
Asp
irin
for p
rim
ary
thro
mbo
sis p
reve
ntio
n in
the
antip
hosp
holip
id sy
ndro
me:
a ra
ndom
ized
, do
uble
-blin
d, p
lace
bo-c
ontr
olle
d tr
ial i
n as
ympt
omat
ic a
ntip
hosp
holip
id a
ntib
ody-
posi
tive
indi
vidu
als.
Art
hrit
is R
heum
. 200
7;56
(7):2
382-
2391
. Her
eng
T, L
ambe
rt M
, Hac
hulla
E, e
t al.
Infl u
ence
of a
spir
in
on th
e cl
inic
al o
utco
mes
of 1
03 a
nti-p
hosp
holip
id a
ntib
odie
s-po
sitiv
e pa
tient
s. L
upus
. 200
8;17
(1):1
1-15
. Tek
toni
dou
MG
, Las
kari
K, P
anag
iota
kos
DB
, Mou
tsop
oulo
s H
M. R
isk
fact
ors
for
thro
mbo
sis
and
prim
ary
thro
mbo
sis
prev
entio
n in
pat
ient
s w
ith s
yste
mic
lupu
s er
ythe
mat
osus
with
or
with
out a
ntip
hosp
holip
id a
ntib
odie
s. A
rthr
itis
Rhe
um. 2
009;
61(1
):29-
36. S
ee T
able
S1,
S3,
S4,
S7,
and
S11
lege
nds
for
expa
nsio
n of
abb
revi
atio
ns.
a Erk
an e
t al a
nd G
lynn
et a
l are
RC
Ts; i
n ad
ditio
n, H
eren
g et
al,
Erk
an e
t al,
and
Tekt
onid
ou e
t al p
rovi
ded
obse
rvat
iona
l dat
a.
b Erk
an e
t al a
nd G
lynn
et a
l. c E
rkan
et a
l ter
min
ated
ear
ly a
s ev
ent r
ates
wer
e lo
wer
than
exp
ecte
d an
d la
rger
sam
ple
size
was
infe
asib
le.
d Num
ber
of e
vent
s w
as v
ery
smal
l. e E
vent
rate
s are
from
Erk
an e
t al (
RC
T) (
n 5
98)
, as s
econ
d R
CT
(Gly
nn e
t al)
did
not r
epor
t eve
nt ra
tes.
In E
rkan
et a
l, H
R o
f com
posi
te o
utco
me
(art
eria
l or v
enou
s thr
ombo
sis,
incl
udin
g st
roke
, PE
, DV
T,
acut
e M
I), 1
.04
(95%
CI,
0.6
9-1.
56),
P 5
.83.
Num
ber
of v
enou
s ev
ents
: int
erve
ntio
n 2
of 4
8, p
lace
bo 0
of 5
0. G
lynn
et a
l (R
CT,
n 5
1,3
70),
HR
for
VT
E, 0
.81
(95%
CI,
0.4
2-1.
54).
In a
dditi
on, o
bser
vatio
nal
stud
ies
repo
rted
com
posi
te o
utco
mes
incl
udin
g bo
th a
rter
ial a
nd v
enou
s ev
ents
(Erk
an e
t al,
Her
eng
et a
l, an
d Te
kton
idou
et a
l).
f In
addi
tion
to th
e R
CT,
one
obs
erva
tiona
l stu
dy h
ad fo
llow
-up
of 2
.5 y
(SD
, 0.8
y).
g Erk
an e
t al e
ncom
pass
es b
oth
an R
CT
and
an
obse
rvat
iona
l stu
dy.
h Inc
onsi
sten
cy n
ot a
sses
sed
as is
one
stu
dy, a
lthou
gh E
rkan
et a
l enc
ompa
sses
bot
h a
rele
vant
RC
T a
nd a
n ob
serv
atio
nal c
ompo
nent
. i I
nter
vent
ion
was
81
mg
od.
j Cau
se o
f dea
th w
as n
ot r
epor
ted.
k C
ompa
riso
n gr
oup
rece
ived
no
ASA
. l R
R c
alcu
late
d fr
om e
vent
rat
es (u
nadj
uste
d).
m In
add
ition
, in
the
obse
rvat
iona
l stu
dy (E
rkan
et a
l) th
e m
orta
lity
rate
was
0%
in b
oth
grou
ps.
n Erk
an e
t al,
Her
eng
et a
l, Te
kton
idou
et a
l. In
add
ition
, Erk
an e
t al (
RC
T) r
epor
ted
0 m
ajor
ble
edin
g ev
ents
bot
h gr
oups
. o E
rkan
et a
l als
o in
clud
ed a
n R
CT
(n 5
94)
with
0 m
ajor
non
fata
l ble
edin
g ev
ents
in b
oth
the
ASA
and
no
ASA
gro
ups.
p R
R n
ot e
stim
able
(rat
e of
0 b
oth
grou
ps).
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

53© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S3
1 —St
udi
es E
xam
inin
g th
e E
ffec
t of
Exp
osu
re t
o St
atin
s on
DV
T, P
E, a
nd d
eath
: Cli
nica
l D
escr
ipti
on a
nd R
esu
lts:
RC
T a
nd C
ohor
t St
udi
es
Stud
y/Ye
ar; T
rial
Nam
e;
Cou
ntry
; Stu
dy D
esig
nIn
terv
entio
n an
d C
ompa
rato
rSa
mpl
e Si
zePo
pula
tion
Cha
ract
eris
tics
Len
gth
of
Fol
low
-up
Res
ults
Com
men
ts
Gra
dy e
t al 66
, 200
0;
Uni
ted
Stat
es;
Pros
pect
ive,
co
mpa
rativ
e co
hort
st
udy
from
H
ER
S tr
ial
Stat
in th
erap
y2,
763
Wom
en r
ando
miz
ed
in H
ER
S tr
ial
(1,3
80 r
ando
miz
ed
to r
ecei
ve e
stro
gen;
1,
383
to p
lace
bo)
Post
men
opau
sal w
omen
,
80
y, w
ith C
HD
but
no
pre
viou
s V
TE
and
no
hys
tere
ctom
y
HE
RS
tria
l: m
ean
follo
w-u
p 4.
1 y
(ran
ge 3
.6-5
.3 y
)
Clin
ical
eve
nts
acco
rdin
g
to s
tatin
use
dur
ing
the
HE
RS
tria
l:
Inte
ract
ion
betw
een
horm
one
repl
acem
ent
ther
apy
and
stat
in
use
for
1-y
even
ts:
P 5
.57
No
stat
in th
erap
y
Mea
n du
ratio
n of
fo
llow
-up:
3.3
yB
asel
ine
use
Mea
n ag
e �
SD
, y
Dur
atio
n of
follo
w-u
p fo
r w
omen
who
us
ed s
tatin
s fo
r � 3
y
(mea
n �
SD
): 5.
7 �
2.4
y
Stat
in th
erap
y: 1
,004
Stat
in th
erap
y: 6
6.9
� 6
.18
No
stat
in th
erap
y: 1
,467
No
stat
in th
erap
y:
66.5
� 7
.04
V
TE
s:
Sex:
100
% w
omen
N
o st
atin
use
: 32
of
1,
467
(5.5
a )
Dur
atio
n of
follo
w-u
p fo
r w
omen
who
use
d st
atin
s fo
r , 3
y
(mea
n �
SD
): 5.
7 �
2.4
y
Bas
elin
e st
atin
use
rs
tend
ed to
be
whi
te,
bett
er e
duca
ted,
he
alth
ier,
with
few
co
mor
bid
cond
ition
s an
d m
ore
likel
y to
ta
ke A
SA
St
atin
use
: 9 o
f
1,00
4 (2
.2 a )
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

54© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
ar; T
rial
Nam
e;
Cou
ntry
; Stu
dy D
esig
nIn
terv
entio
n an
d C
ompa
rato
rSa
mpl
e Si
zePo
pula
tion
Cha
ract
eris
tics
Len
gth
of
Fol
low
-up
Res
ults
Com
men
ts
A
djus
ted
HR
: 0.4
4
(95%
CI,
0.2
1-0.
94),
P 5
.033
A
ll-ca
use
mor
talit
y
N
o st
atin
use
: 159
of
1,
467
(26.
8 a )
S
tatin
use
: 75
of
1,
004
(18.
4 a )
A
djus
ted
HR
: 0.7
4
(95%
CI,
0.5
6-0.
99),
P 5
.040
Any
sta
tin u
se
V
TE
s:
N
o st
atin
use
: 28
of
1,
467
(6.1
a )
St
atin
use
: 13
of
1,
270
(2.5
a )
A
djus
ted
HR
: 0.4
5
(95%
CI,
0.2
3-0.
88),
P 5
.020
M
orta
lity
N
o st
atin
use
: 134
of
1,
467
(28.
4 a )
St
atin
use
: 100
of
1,
270
(18.
9 a )
A
djus
ted
HR
: 0.6
7
(95%
CI,
0.5
1-0.
87),
P 5
.003
Use
d st
atin
s .
3 y
A
ll-ca
use
mor
talit
y: H
R,
0.
70 (9
5% C
I 0.
52-0
.93)
, P
5 .0
1
V
TE
s: H
R, 0
.40
(9
5% C
I, 0
.18-
0.91
), P
5 .0
3
Tabl
e S3
1—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
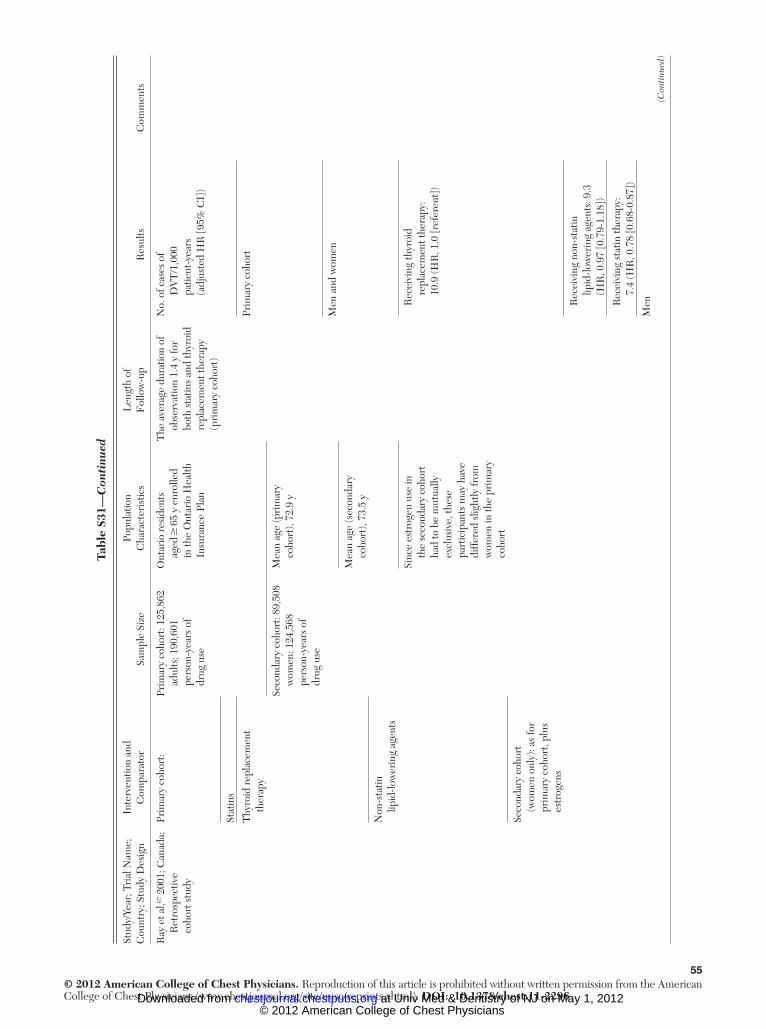
55© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S3
1—C
onti
nued
Stud
y/Ye
ar; T
rial
Nam
e;
Cou
ntry
; Stu
dy D
esig
nIn
terv
entio
n an
d C
ompa
rato
rSa
mpl
e Si
zePo
pula
tion
Cha
ract
eris
tics
Len
gth
of
Fol
low
-up
Res
ults
Com
men
ts
Ray
et a
l, 67 2
001;
Can
ada;
R
etro
spec
tive
coho
rt s
tudy
Prim
ary
coho
rt:
Prim
ary
coho
rt: 1
25,8
62
adul
ts; 1
90,6
01
pers
on-y
ears
of
drug
use
Ont
ario
res
iden
ts
aged
� 6
5 y
enro
lled
in th
e O
ntar
io H
ealth
In
sura
nce
Plan
The
ave
rage
dur
atio
n of
ob
serv
atio
n 1.
4 y
for
both
sta
tins
and
thyr
oid
repl
acem
ent t
hera
py
(pri
mar
y co
hort
)
No.
of c
ases
of
D
VT
/1,0
00
patie
nt-y
ears
(a
djus
ted
HR
[95%
CI]
)
Stat
ins
Thy
roid
rep
lace
men
t th
erap
yPr
imar
y co
hort
Seco
ndar
y co
hort
: 89,
508
wom
en; 1
24,5
68
pers
on-y
ears
of
drug
use
Mea
n ag
e (p
rim
ary
coho
rt),
72.9
y
Men
and
wom
en
Mea
n ag
e (s
econ
dary
co
hort
), 73
.5 y
Non
-sta
tin
lipid
-low
erin
g ag
ents
Sinc
e es
trog
en u
se in
th
e se
cond
ary
coho
rt
had
to b
e m
utua
lly
excl
usiv
e, th
ese
part
icip
ants
may
hav
e di
ffer
ed s
light
ly fr
om
wom
en in
the
prim
ary
coho
rt
R
ecei
ving
thyr
oid
re
plac
emen
t the
rapy
: 10
.9 (H
R, 1
.0 [r
efer
ent]
)
Seco
ndar
y co
hort
(w
omen
onl
y): a
s fo
r pr
imar
y co
hort
, plu
s es
trog
ens
R
ecei
ving
non
-sta
tin
lip
id-lo
wer
ing
agen
ts: 9
.3
(HR
, 0.9
7 [0
.79-
1.18
])
R
ecei
ving
sta
tin th
erap
y:
7.
4 (H
R, 0
.78
[0.6
8-0.
87])
Men
(C
onti
nued
)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

56© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S3
1—C
onti
nued
(Con
tinu
ed)
Stud
y/Ye
ar; T
rial
Nam
e;
Cou
ntry
; Stu
dy D
esig
nIn
terv
entio
n an
d C
ompa
rato
rSa
mpl
e Si
zePo
pula
tion
Cha
ract
eris
tics
Len
gth
of
Fol
low
-up
Res
ults
Com
men
ts
R
ecei
ving
sta
tin th
erap
y:
6.
7 (H
R, 0
.97
[0.7
8-1.
22])
Wom
en
R
ecei
ving
sta
tin th
erap
y:
8.
1 (H
R, 0
.72
[0.6
3-0.
82])
Seco
ndar
y co
hort
:
Thy
roid
rep
lace
men
t the
rapy
:
11.9
(HR
, 1.0
[ref
eren
t])
Stat
in th
erap
y: 7
.6
(H
R, 0
.68
[0.5
9-0.
79])
Smee
th e
t al 68
/200
9;
Uni
ted
Kin
gdom
; ob
serv
atio
nal s
tudy
, po
pula
tion
base
d
Vari
ous
stat
ins
(fi rs
t pre
scri
ptio
n)
com
pare
d w
ith
non-
stat
in u
sers
(n
o re
cord
of s
tatin
use
)
Tota
l N, 7
29,5
29T
HIN
dat
abas
e:
age
40-8
0 y
betw
een
Janu
ary
1995
and
D
ecem
ber
2006
Med
ian
follo
w-u
p af
ter
inde
x da
te
(dat
e of
fi rs
t use
of
sta
tin):
4.4
y
VT
E r
isk
in e
xpos
ed 1
.1%
,
unex
pose
d 1.
0%; H
R
adju
sted
for
age
and
sex,
1.
18 (9
5% C
I, 1
.06-
1.31
); H
R fu
lly a
djus
ted.
1.
02 (0
.88-
1.18
)
Stat
in u
sers
: 129
,288
Non
-sta
tin u
sers
: 600
,241
5.5
mill
ion
patie
nts
deri
ved
from
303
ge
nera
l pra
ctic
es
Gly
nn e
t al 69
/200
9;
Uni
ted
Stat
es
Ros
uvas
tatin
(20
mg/
d)To
tal:
17,8
02A
ppar
ently
hea
lthy
su
bjec
ts w
ith L
DL
ch
oles
tero
l ( ,
130
mg/
dL)
and
elev
ated
hi
gh-s
ensi
tivity
C
-rea
ctiv
e pr
otei
n ( �
2.0
mg/
L),
men
� 5
0 y
and
wom
en �
60
y
Med
ian
follo
w-u
p: 1
.9 y
(m
axim
um 5
.0 y
)Pr
imar
y ef
fi cac
y an
alys
is b
DV
T d
iagn
osed
with
ul
tras
ound
or
veno
gram
; PE
di
agno
sed
with
an
giog
ram
, CT
sca
n,
or
/ s
can
Ros
uvas
tatin
: 8,9
01
Rid
ker
et a
l 70 /2
008;
U
nite
d St
ates
Pl
aceb
o
Rid
ker
et a
l 71 /2
007;
U
nite
d St
ates
; JU
PIT
ER
tria
l; R
CT
Plac
ebo:
8,9
01
PE
(No.
pat
ient
s,
No.
eve
nts
per
100
pers
on-y
ears
)
Ros
uvas
tatin
: 17,
0.0
9
Plac
ebo:
22,
0.1
2
Am
ong
all 1
7,80
2
JUPI
TE
R p
atie
nts:
HR
(95%
CI)
: 0.7
7
(0
.41-
1.45
), P
5 .4
2
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
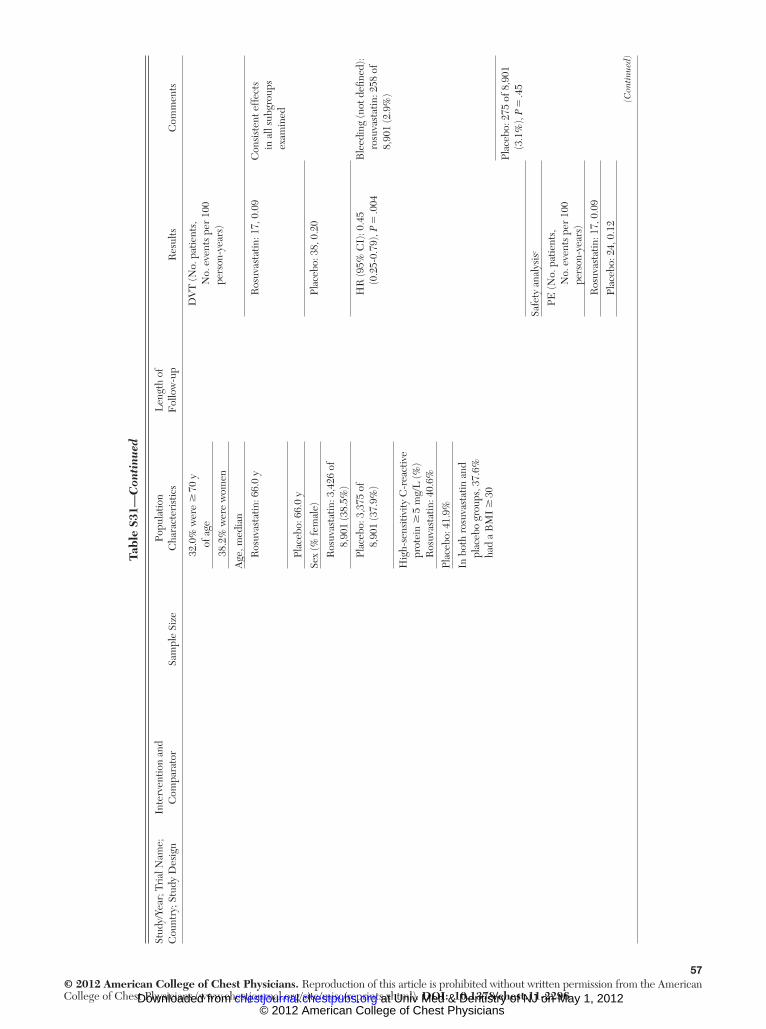
57© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S3
1—C
onti
nued
(Con
tinu
ed)
Stud
y/Ye
ar; T
rial
Nam
e;
Cou
ntry
; Stu
dy D
esig
nIn
terv
entio
n an
d C
ompa
rato
rSa
mpl
e Si
zePo
pula
tion
Cha
ract
eris
tics
Len
gth
of
Fol
low
-up
Res
ults
Com
men
ts
3
2.0%
wer
e �
70
y
of a
ge
DV
T (N
o. p
atie
nts,
N
o. e
vent
s pe
r 10
0 pe
rson
-yea
rs)
3
8.2%
wer
e w
omen
Age
, med
ian
R
osuv
asta
tin: 6
6.0
y
R
osuv
asta
tin: 1
7, 0
.09
Con
sist
ent e
ffec
ts
in a
ll su
bgro
ups
exam
ined
Pl
aceb
o: 6
6.0
y
Sex
(% fe
mal
e)
Pl
aceb
o: 3
8, 0
.20
R
osuv
asta
tin: 3
,426
of
8,
901
(38.
5%)
Pl
aceb
o: 3
,375
of
8,
901
(37.
9%)
HR
(95%
CI)
: 0.4
5
(0
.25-
0.79
), P
5 .0
04B
leed
ing
(not
defi
ned
): ro
suva
stat
in: 2
58 o
f 8,
901
(2.9
%)
Hig
h-se
nsiti
vity
C-r
eact
ive
prot
ein
� 5
mg/
L (%
) R
osuv
asta
tin: 4
0.6%
Plac
ebo:
41.
9%
In b
oth
rosu
vast
atin
and
pl
aceb
o gr
oups
, 37.
6%
had
a B
MI
� 3
0
Plac
ebo:
275
of 8
,901
(3
.1%
), P
5 .4
5
Safe
ty a
naly
sis c
PE
(No.
pat
ient
s,
No.
eve
nts
per
100
pers
on-y
ears
)
Ros
uvas
tatin
: 17,
0.0
9
Plac
ebo:
24,
0.1
2
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
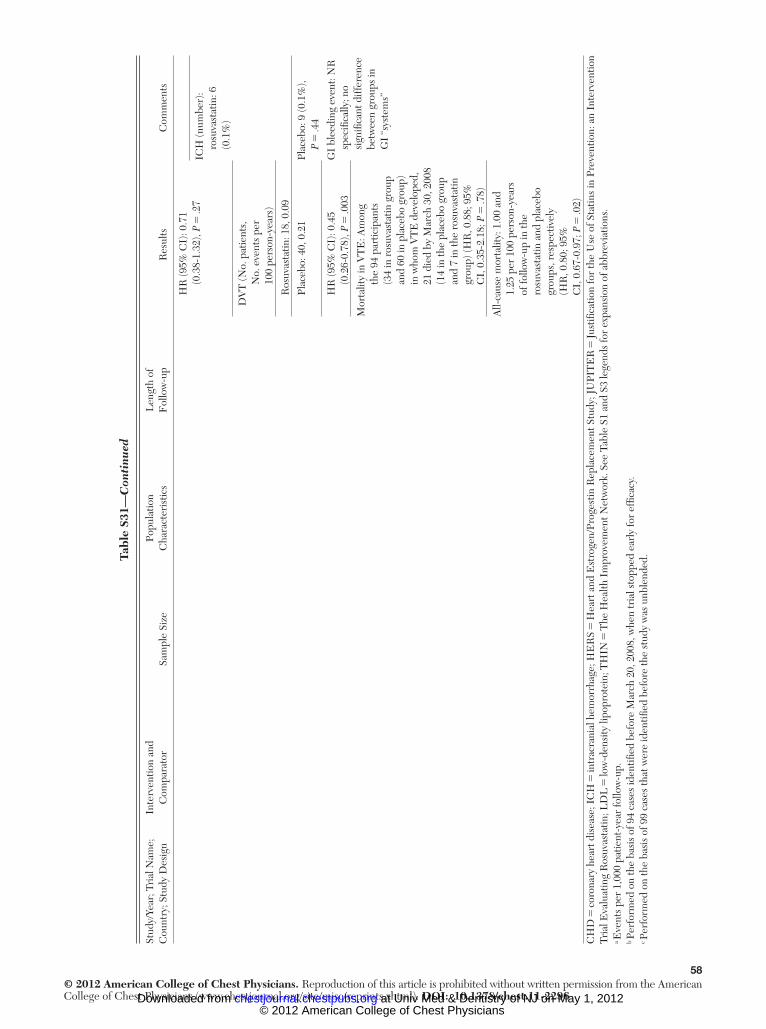
58© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
ar; T
rial
Nam
e;
Cou
ntry
; Stu
dy D
esig
nIn
terv
entio
n an
d C
ompa
rato
rSa
mpl
e Si
zePo
pula
tion
Cha
ract
eris
tics
Len
gth
of
Fol
low
-up
Res
ults
Com
men
ts
HR
(95%
CI)
: 0.7
1
(0
.38-
1.32
), P
5 .2
7 IC
H (n
umbe
r):
rosu
vast
atin
: 6
(0.1
%)
D
VT
(No.
pat
ient
s,
No.
eve
nts
per
100
pers
on-y
ears
)
Ros
uvas
tatin
: 18,
0.0
9
Plac
ebo:
40,
0.2
1Pl
aceb
o: 9
(0.1
%),
P 5
.44
HR
(95%
CI)
: 0.4
5
(0
.26-
0.78
), P
5 .0
03G
I bl
eedi
ng e
vent
: NR
sp
ecifi
cally
; no
sign
ifi ca
nt d
iffer
ence
be
twee
n gr
oups
in
GI
“sys
tem
s”
Mor
talit
y in
VT
E: A
mon
g
th
e 94
par
ticip
ants
(3
4 in
ros
uvas
tatin
gro
up
and
60 in
pla
cebo
gro
up)
in w
hom
VT
E d
evel
oped
, 21
die
d by
Mar
ch 3
0, 2
008
(14
in th
e pl
aceb
o gr
oup
and
7 in
the
rosu
vast
atin
gr
oup)
(HR
, 0.8
8; 9
5%
CI,
0.3
5-2.
18; P
5 .7
8)
All-
caus
e m
orta
lity:
1.0
0 an
d
1.25
per
100
per
son-
year
s of
follo
w-u
p in
the
rosu
vast
atin
and
pla
cebo
gr
oups
, res
pect
ivel
y (H
R, 0
.80;
95%
C
I, 0
.67-
0.97
; P 5
.02)
C
HD
5 co
rona
ry h
eart
dis
ease
; IC
H 5
intr
acra
nial
hem
orrh
age;
HE
RS
5 H
eart
and
Est
roge
n/Pr
oges
tin R
epla
cem
ent S
tudy
; JU
PIT
ER
5 Ju
stifi
catio
n fo
r th
e U
se o
f Sta
tins
in P
reve
ntio
n: a
n In
terv
entio
n Tr
ial E
valu
atin
g R
osuv
asta
tin; L
DL
5 lo
w-d
ensi
ty li
popr
otei
n; T
HIN
5 T
he H
ealth
Im
prov
emen
t Net
wor
k . S
ee T
able
S1
and
S3 le
gend
s fo
r ex
pans
ion
of a
bbre
viat
ions
. a E
vent
s pe
r 1,
000
patie
nt-y
ear
follo
w-u
p.
b Per
form
ed o
n th
e ba
sis
of 9
4 ca
ses
iden
tifi e
d be
fore
Mar
ch 2
0, 2
008,
whe
n tr
ial s
topp
ed e
arly
for
effi c
acy.
c P
erfo
rmed
on
the
basi
s of
99
case
s th
at w
ere
iden
tifi e
d be
fore
the
stud
y w
as u
nble
nded
. Tabl
e S3
1—C
onti
nued
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

59© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S3
2 —St
udi
es E
xam
inin
g th
e E
ffec
t of
Exp
osu
re t
o St
atin
s on
DV
T, P
E, a
nd D
eath
: Cli
nica
l D
escr
ipti
on a
nd R
esu
lts:
Cas
e-C
ontr
ol S
tudi
es
Stud
y/Ye
ar; T
rial
N
ame;
Cou
ntry
Inte
rven
tion
and
Com
para
tor
Sam
ple
Size
Popu
latio
n C
hara
cter
istic
sL
engt
h of
F
ollo
w-u
p, M
ean
Res
ults
Com
men
ts
Bro
phy
et a
l 72 /2
009;
U
nite
d St
ates
Stat
in u
se
vs n
o st
atin
use
Cas
es: 6
0A
ge:
NA
: cur
rent
st
atin
use
ass
esse
d by
sel
f-re
port
Stat
in u
se a
nd c
ases
of v
ascu
lar
acce
ss
thro
mbo
sis:
Con
trol
s: 4
1
Cas
es: p
atie
nts
who
(1) e
xper
ienc
ed
two
or m
ore
epis
odes
of
vas
cula
r ac
cess
th
rom
bosi
s in
12
mo
diag
nose
d by
ultr
asou
nd,
fi stu
logr
am, o
r ph
ysic
al
exam
inat
ion;
and
(2
) req
uire
d tw
o or
m
ore
new
dia
lysi
s ac
cess
pla
cem
ents
not
re
late
d to
infe
ctio
n in
2
y; o
r (3
) pat
ient
s w
ho
coul
d no
t mai
ntai
n a
pate
nt A
VG
or
AVF
w
ithin
2 m
o th
at
nece
ssita
ted
plac
emen
t of
a p
erm
anen
t cat
hete
r or
the
perm
anen
t co
nver
sion
to
peri
tone
al d
ialy
sis.
I:
53.
8 y
(S
D, 1
4.2
y)
Cas
es: 1
8
of 6
0 (3
1%)
C
ontr
ols:
8
of
41
(20.
5%)
P
5 .3
5
C
: 54.
8 y
(S
D, 1
0.2
y)M
ultiv
aria
ble
logi
stic
regr
essi
on fo
r va
scul
ar a
cces
s th
rom
bosi
s: O
R,
5.12
(95%
CI,
1.
25-2
0.90
); P
5 .0
2
P
5 .6
9
Sex,
fem
ale:
I:
27
(45%
)
C
: 16
(39%
)
P
5 .5
5
Rac
e, b
lack
:
I:
55
(92%
)
Con
trol
s: p
atie
nts
who
had
not
ex
peri
ence
d va
scul
ar
acce
ss th
rom
bosi
s in
at l
east
3 y
C
: 39
(95%
)
P
5 .4
9
All
patie
nts
had
st
age
5 ch
roni
c ki
dney
dis
ease
an
d re
ceiv
ed
mai
nten
ance
he
mod
ialy
sis
for .
3 y
(C
onti
nued
)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
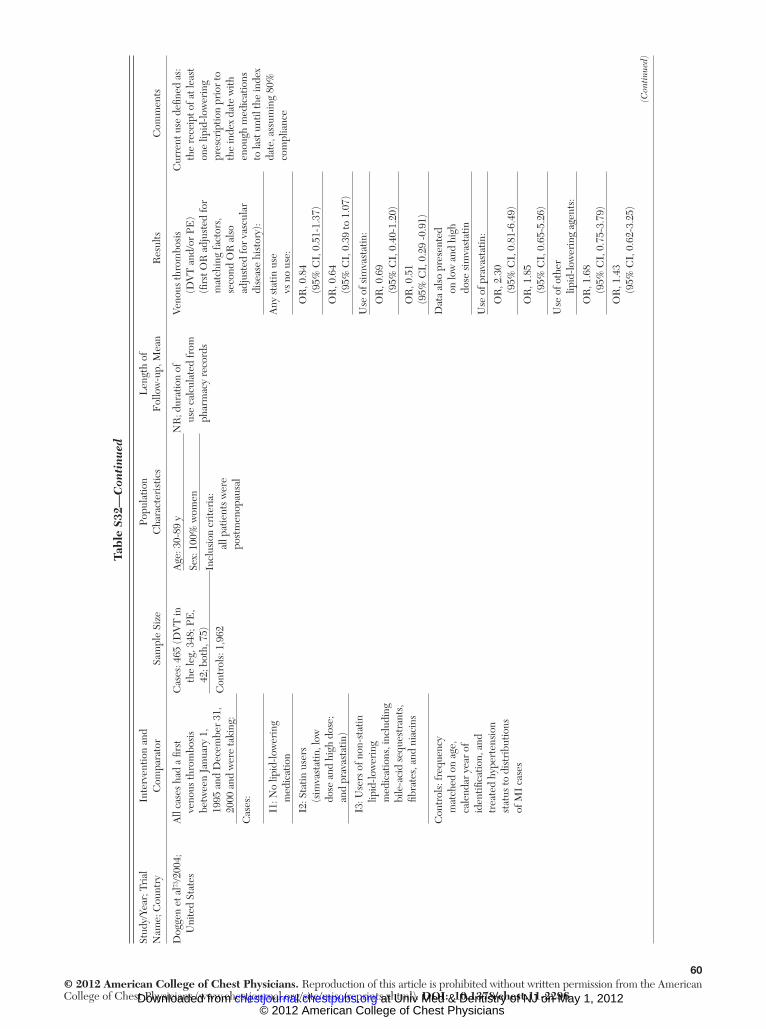
60© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
ar; T
rial
N
ame;
Cou
ntry
Inte
rven
tion
and
Com
para
tor
Sam
ple
Size
Popu
latio
n C
hara
cter
istic
sL
engt
h of
F
ollo
w-u
p, M
ean
Res
ults
Com
men
ts
Dog
gen
et a
l 73 /2
004;
U
nite
d St
ates
All
case
s ha
d a
fi rst
ve
nous
thro
mbo
sis
betw
een
Janu
ary
1,
1995
and
Dec
embe
r 31
, 20
00 a
nd w
ere
taki
ng:
Cas
es: 4
65 (D
VT
in
the
leg,
348
; PE
, 42
; bot
h, 7
5)
Age
: 30-
89 y
NR
; dur
atio
n of
us
e ca
lcul
ated
from
ph
arm
acy
reco
rds
Veno
us th
rom
bosi
s
(DV
T a
nd/o
r PE
) (fi
rst O
R a
djus
ted
for
mat
chin
g fa
ctor
s,
seco
nd O
R a
lso
adju
sted
for
vasc
ular
di
seas
e hi
stor
y):
Cur
rent
use
defi
ned
as:
th
e re
ceip
t of a
t lea
st
one
lipid
-low
erin
g pr
escr
iptio
n pr
ior
to
the
inde
x da
te w
ith
enou
gh m
edic
atio
ns
to la
st u
ntil
the
inde
x da
te, a
ssum
ing
80%
co
mpl
ianc
e
Sex:
100
% w
omen
Incl
usio
n cr
iteri
a:
al
l pat
ient
s w
ere
post
men
opau
sal
Con
trol
s: 1
,962
Cas
es:
I1
: No
lipid
-low
erin
g
med
icat
ion
Any
sta
tin u
se
vs
no
use:
I2
: Sta
tin u
sers
(sim
vast
atin
, low
dose
and
hig
h do
se;
an
d pr
avas
tatin
)
O
R, 0
.84
(9
5% C
I, 0
.51-
1.37
)
O
R, 0
.64
(9
5% C
I, 0
.39
to 1
.07)
I3: U
sers
of n
on-s
tatin
lipid
-low
erin
g
med
icat
ions
, inc
ludi
ng
bi
le-a
cid
sequ
estr
ants
,
fi bra
tes,
and
nia
cins
Use
of s
imva
stat
in:
O
R, 0
.69
(9
5% C
I, 0
.40-
1.20
)
O
R, 0
.51
(95%
CI,
0.2
9 -0
.91)
Con
trol
s: fr
eque
ncy
mat
ched
on
age,
ca
lend
ar y
ear
of
iden
tifi c
atio
n, a
nd
trea
ted
hype
rten
sion
st
atus
to d
istr
ibut
ions
of
MI
case
s
Dat
a al
so p
rese
nted
on lo
w a
nd h
igh
dose
sim
vast
atin
Use
of p
rava
stat
in:
O
R, 2
.30
(9
5% C
I, 0
.81-
6.49
)
O
R, 1
.85
(9
5% C
I, 0
.65-
5.26
)
Use
of o
ther
lipid
-low
erin
g ag
ents
:
O
R, 1
.68
(9
5% C
I, 0
.75-
3.79
)
O
R, 1
.43
(9
5% C
I, 0
.62-
3.25
)
Tabl
e S3
2—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

61© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
ar; T
rial
N
ame;
Cou
ntry
Inte
rven
tion
and
Com
para
tor
Sam
ple
Size
Popu
latio
n C
hara
cter
istic
sL
engt
h of
F
ollo
w-u
p, M
ean
Res
ults
Com
men
ts
Lac
ut e
t al 74
/200
4;
Fra
nce;
ED
ITH
Cas
es: p
atie
nts
with
doc
umen
ted
sym
ptom
atic
DV
T
of th
e lo
wer
lim
bs
(eith
er d
ista
l or
prox
imal
con
fi rm
ed b
y du
plex
ultr
ason
ogra
phy)
or
/and
an
obje
ctiv
ely
docu
men
ted
PE, n
ot
rela
ted
to a
maj
or
acqu
ired
ris
k fa
ctor
fo
r V
TE
Cas
es: 3
77 (D
VT,
252
; PE
, 46;
bot
h, 7
9)A
ge:
Con
trol
s fo
llow
ed fo
r up
to 3
mo
for
VT
ESt
atin
use
, cas
es o
f VT
E:
Popu
latio
ns in
L
acut
200
474 a
nd
2008
75 o
verl
ap. T
he
2008
pub
licat
ion
incl
uded
long
er
recr
uitm
ent p
erio
d bu
t on
ly in
clud
ed c
ases
w
ithou
t maj
or r
isk
fact
ors
for
VT
E,
whe
reas
Lac
ut 2
004
incl
uded
69
of
377
patie
nts
in e
ach
grou
p w
ith m
ajor
ac
quir
ed r
isk
fact
ors
for
VT
E
I:
20
of 3
77
C
: 44
of 3
77
O
R, 0
.42
(9
5% C
I, 0
.23-
0.76
); P
5 .0
02
Con
trol
s: 3
77
Cas
es: 6
8.0
y
(SD
, 16.
4 y)
C
urre
nt s
tatin
us
e w
as c
onsi
dere
d (w
ithin
pri
or 3
mo)
Stat
ins
incl
uded
pra
vast
atin
,
sim
vast
atin
, ato
rvas
tatin
; re
sults
not
str
atifi
ed b
y sp
ecifi
c st
atin
C: 6
8.1
y
(SD
, 16.
2 y)
Con
trol
s: h
ospi
taliz
ed
patie
nts
mat
ched
fo
r ag
e ( �
2 y
), se
x,
geog
raph
ical
ori
gin,
an
d m
ajor
acq
uire
d ri
sk fa
ctor
s of
VT
E,
and
no p
rior
VT
E
P 5
.90
Sex,
fem
ale:
St
ratifi
ed
anal
yses
of
vari
ous
leve
ls o
f ASA
us
e, C
AD
, sec
onda
ry
vs id
iopa
thic
VT
E,
age,
sex
did
not
si
gnifi
cant
ly in
tera
ct
with
odd
s of
VT
E
C
ases
: 211
(55.
9%)
C
: 211
(55.
9%)
Incl
usio
n cr
iteri
a:
Pa
tient
s . 1
8 y
of a
ge h
ospi
taliz
ed
betw
een
May
200
0 an
d M
ay 2
002
Tabl
e S3
2—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

62© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
ar; T
rial
N
ame;
Cou
ntry
Inte
rven
tion
and
Com
para
tor
Sam
ple
Size
Popu
latio
n C
hara
cter
istic
sL
engt
h of
F
ollo
w-u
p, M
ean
Res
ults
Com
men
ts
Lac
ut e
t al 75
/200
8;
Fra
nce;
ED
ITH
Cas
es: p
atie
nts
with
an
obje
ctiv
ely
confi
rm
ed
sym
ptom
atic
VT
E a
nd
no m
ajor
acq
uire
d ri
sk fa
ctor
for
VT
E
Cas
es: 6
77 (D
VT,
303
; PE
, 121
; bot
h, 2
56)
Age
:C
urre
nt s
tatin
use
(t
aken
with
in 1
wk)
Cur
rent
sta
tin u
se:
Con
trol
s: 6
77
Con
trol
s: p
atie
nts
mat
ched
by
age
( � 5
y)
and
sex
and
with
out
a pr
evio
us e
piso
de o
f ob
ject
ivel
y do
cum
ente
d V
TE
or
lifel
ong
antic
oagu
lant
ther
apy
I:
67.
9 y
(S
D, 1
7.0
y)
Cas
es: 5
5 (8
.1%
)
C
: 68.
0 y
(S
D, 1
7.0
y)
C: 9
1 (1
3.4%
)
Sex,
fem
ale:
OR
VT
E in
sta
tin
vs
non
use
r, 0.
53
(95%
CI,
0.3
7-0.
78)
I:
56.
7%A
djus
ted
OR
, 0.6
0
(0.3
9-0.
93)
C
: 56.
7%A
djus
ted
for
at
hero
thro
mbo
sis,
as
piri
n us
e, s
uspe
cted
as
the
mai
n co
nfou
ndin
g fa
ctor
s, a
nd c
hron
ic
pulm
onar
y di
seas
e,
BM
I, a
nd fa
mily
his
tory
of
VT
E
BM
I:
I:
26.
1 (S
D, 4
.7)
C
: 24.
7 (S
D, 5
.6)
P
, .0
001
Incl
usio
n cr
iteri
a,
case
s an
d co
ntro
ls:
patie
nts .
18
y of
age
hos
pita
lized
be
twee
n M
ay 2
000
and
Dec
embe
r 20
04,
with
out m
ajor
ac
quir
ed r
isk
fact
or o
f VT
E
(no
surg
ery
or p
last
er
cast
imm
obili
zatio
n in
the
past
3 m
o,
preg
nanc
y or
del
iver
y in
the
past
3 m
o,
or a
ctiv
e ca
ncer
)
Tabl
e S3
2—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
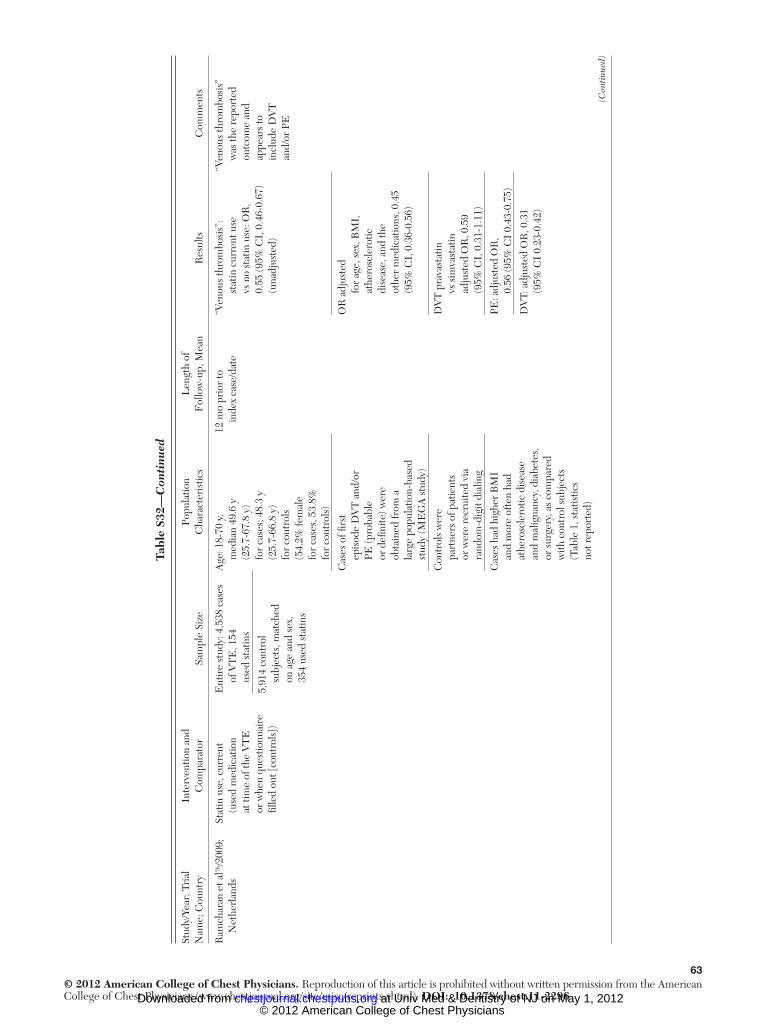
63© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
ar; T
rial
N
ame;
Cou
ntry
Inte
rven
tion
and
Com
para
tor
Sam
ple
Size
Popu
latio
n C
hara
cter
istic
sL
engt
h of
F
ollo
w-u
p, M
ean
Res
ults
Com
men
ts
Ram
char
an e
t al 76
/200
9;
Net
herl
ands
Stat
in u
se, c
urre
nt
(use
d m
edic
atio
n at
tim
e of
the
VT
E
or w
hen
ques
tionn
aire
fi l
led
out [
cont
rols
])
Ent
ire
stud
y: 4
,538
cas
es
of V
TE
, 154
us
ed s
tatin
s
Age
: 18-
70 y
, m
edia
n 49
.6 y
(2
5.7-
67.8
y)
for
case
s; 4
8.3
y (2
5.7-
66.8
y)
for
cont
rols
(5
4.2%
fem
ale
for
case
s, 5
3.8%
fo
r co
ntro
ls)
12 m
o pr
ior
to
inde
x ca
se/d
ate
“Ven
ous
thro
mbo
sis”
:
stat
in c
urre
nt u
se
vs n
o st
atin
use
: OR
, 0.
55 (9
5% C
I, 0
.46-
0.67
) (u
nadj
uste
d)
“Ven
ous
thro
mbo
sis”
w
as th
e re
port
ed
outc
ome
and
appe
ars
to
incl
ude
DV
T
and/
or P
E
5,91
4 co
ntro
l su
bjec
ts, m
atch
ed
on a
ge a
nd s
ex,
354
used
sta
tins
Cas
es o
f fi r
st
epis
ode
DV
T a
nd/o
r PE
(pro
babl
e or
defi
nite
) wer
e ob
tain
ed fr
om a
la
rge
popu
latio
n-ba
sed
stud
y (M
EG
A s
tudy
)
OR
adj
uste
d
for
age,
sex
, BM
I,
athe
rosc
lero
tic
dise
ase,
and
the
othe
r m
edic
atio
ns, 0
.45
(95%
CI,
0.3
6-0.
56)
Con
trol
s w
ere
part
ners
of p
atie
nts
or w
ere
recr
uite
d vi
a ra
ndom
-dig
it di
alin
g
DV
T p
rava
stat
in
vs
sim
vast
atin
ad
just
ed O
R, 0
.59
(95%
CI,
0.3
1-1.
11)
Cas
es h
ad h
ighe
r B
MI
and
mor
e of
ten
had
athe
rosc
lero
tic d
isea
se
and
mal
igna
ncy,
dia
bete
s,
or s
urge
ry, a
s co
mpa
red
with
con
trol
sub
ject
s (T
able
1, s
tatis
tics
not r
epor
ted)
PE: a
djus
ted
OR
,
0.56
(95%
CI
0.43
-0.7
5)
DV
T: a
djus
ted
OR
, 0.3
1
(95%
CI
0.23
-0.4
2)
Tabl
e S3
2—C
onti
nued
(Con
tinu
ed)
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

64© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Stud
y/Ye
ar; T
rial
N
ame;
Cou
ntry
Inte
rven
tion
and
Com
para
tor
Sam
ple
Size
Popu
latio
n C
hara
cter
istic
sL
engt
h of
F
ollo
w-u
p, M
ean
Res
ults
Com
men
ts
Sore
nsen
et a
l 77 /2
009;
D
enm
ark
Stat
in u
se in
last
1 y
5,82
4 Pa
tient
s w
ith
VT
E a
nd 5
8,24
0 co
ntro
ls m
atch
ed
on a
ge, s
ex, c
ount
y
Age
. 7
1 y:
47.
8%;
rang
e, 1
8-89
yN
APr
eval
ence
of s
tatin
use
in V
TE
pat
ient
s 4%
, co
ntro
ls 4
%
C
urre
nt u
se: �
90
d
F
orm
er u
se: 9
1-36
5 d
Fem
ale:
54.
7%
Cur
rent
sta
tin u
se:
3,36
6 W
ere
unpr
ovok
ed
(no
risk
fact
ors)
: 2,3
10
with
DV
T a
nd 1
,056
w
ith P
E
V
TE
: OR
, 0.7
4
(95%
CI,
0.6
3-0.
85
U
npro
voke
d V
TE
: OR
,
0.79
(95%
CI,
0.6
5-0.
96)
D
VT:
OR
, 0.8
1
(95%
CI,
0.6
8-0.
97)
PE
: OR
, 0.6
1
(95%
CI,
0.4
8-0.
78)
For
mer
sta
tin u
se:
V
TE
: OR
, 0.7
0 (0
.53-
0.92
)
U
npro
voke
d V
TE
: OR
,
0.97
(95%
CI,
0.69
-1.3
6)
All
OR
are
adj
uste
d
for
mul
tiple
pot
entia
l co
nfou
nder
s
Yang
et a
l 78 /2
002;
U
nite
d K
ingd
omC
urre
nt/r
ecen
t ( �
90
d)
and
past
. 9
0 d
stat
in u
se
Tota
l N 5
84,
093
(coh
ort s
tudy
)G
ener
al P
ract
ice
Res
earc
h D
atab
ase
was
use
d.
Coh
ort s
tudy
: 393
,756
pe
rson
-yea
rsC
ohor
t stu
dy
Ref
eren
ce g
roup
was
the
non-
hype
rlip
idem
ic
non-
stat
in u
sers
Cas
e-co
ntro
l stu
dyF
irst
idio
path
ic V
TE
, co
nfi r
med
or
prob
able
Cas
es: 7
2
C
ontr
ols:
432
C
ontr
ols:
6 m
atch
ed
cont
rols
: age
, sex
, ca
lend
ar ti
me,
tim
e in
dat
abas
e
Cas
e-co
ntro
l stu
dy:
NR
(tim
e of
po
tent
ial e
xpos
ure)
V
TE
and
cur
rent
stat
in u
se: A
djus
ted
rate
ra
tio, 0
.8 (9
5% C
I, 0.
3-2.
7)
A
djus
ted
RR
with
pas
t
stat
in u
se, 2
.4 (0
.6-1
0)
Cas
e-co
ntro
l stu
dy
V
TE
, cur
rent
/rec
ent s
tatin
use:
OR
adj
uste
d fo
r
smok
ing,
BM
I, an
d es
trog
en
us
e, 1
.1 (9
5% C
I, 0
.3-4
.3)
V
TE
: pas
t sta
tin u
se:
O
R a
djus
ted
for s
mok
ing,
B
MI,
and
estr
ogen
use
, 3.
7 (9
5% C
I, 0
.6-2
4)
AVF
5 ar
teri
oven
ous fi
stu
la; C
5 co
ntro
l; C
AD
5 co
rona
ry a
rter
y di
seas
e; E
DIT
H 5
Etu
des d
es D
éter
min
ants
et I
nter
actio
ns d
e la
Thr
ombo
se V
eine
use;
I 5
inte
rven
tion;
ME
GA
5 M
ultip
le E
nvir
onm
enta
l and
G
enet
ic A
sses
smen
t of R
isk
Fac
tors
for
Veno
us T
hrom
bosi
s. S
ee T
able
S1,
S3,
and
S7
lege
nds
for
expa
nsio
n of
oth
er a
bbre
viat
ions
.
Tabl
e S3
2—C
onti
nued
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

65© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
Tabl
e S3
3 —[S
ecti
on 8
.1]
Eff
ect
of S
tati
ns o
n R
isk
of V
TE
Qua
lity
Ass
essm
ent
Sum
mar
y of
Fin
ding
s
Impo
rtan
ce
N
o. o
f Pat
ient
sE
ffec
t
Qua
lity
No.
of S
tudi
esD
esig
nL
imita
tions
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
C
onsi
dera
tions
Stat
ins
No
Stat
in U
seR
elat
ive
(95%
CI)
Abs
olut
e
DV
T (f
ollo
w-u
p m
edia
n, 1
.9 y
; ultr
asou
nd o
r ve
nogr
am)
1R
ando
miz
ed
tria
ls a
No
seri
ous
limita
tions
No
seri
ous
inco
nsis
tenc
y b N
o se
riou
s in
dire
ctne
ss c
No
seri
ous
impr
ecis
ion d
Non
e17
of 8
,901
(0
.2%
)38
of 8
,901
(0
.4%
)H
R, 0
.45
(0.2
5-0.
79)
2 fe
wer
pe
r 1,
000
(fro
m 1
few
er
to 3
few
er)
Hig
hYe
s, c
linic
ally
di
agno
sed
DV
T
PE (f
ollo
w-u
p m
edia
n, 1
.9 y
; ang
iogr
am,
/ s
can,
or
CT
sca
n)
1R
ando
miz
ed
tria
lsN
o se
riou
s lim
itatio
nsN
o se
riou
s in
cons
iste
ncy
No
seri
ous
indi
rect
ness
No
seri
ous
impr
ecis
ion
Non
e17
of 8
,901
(0
.2%
)22
of 8
,901
(0
.2%
)H
R, 0
.77
(0.4
1-1.
45)
0 fe
wer
pe
r 10
0 (f
rom
0 fe
wer
to
0 m
ore)
Hig
hYe
s, c
linic
ally
di
agno
sed
PE
See
Tabl
e S1
and
S3
lege
nds
for
expa
nsio
n of
abb
revi
atio
ns.
a Bod
y of
evi
denc
e co
nsis
ts o
f one
RC
T. S
ix c
ase-
cont
rol s
tudi
es a
nd th
ree
obse
rvat
iona
l stu
dies
are
des
crib
ed in
the
text
. b I
ncon
sist
ency
is n
ot a
pplic
able
as
ther
e is
onl
y on
e st
udy.
Obs
erva
tiona
l dat
a w
ere,
how
ever
, con
sist
ent w
ith th
e tr
ial d
ata.
c T
he s
ingl
e R
CT
(JU
PIT
ER
, Gly
nn e
t al
69 )
was
a la
rge
inte
rnat
iona
l stu
dy in
clud
ing
heal
thy
subj
ects
with
out
diab
etes
, car
diov
ascu
lar
dise
ase,
or
kidn
ey d
isea
se, w
ith L
DL
cho
lest
erol
, 1
30 m
g/dL
and
C
-rea
ctiv
e pr
otei
n .
2 m
g/L
. Res
ults
may
then
be
appl
icab
le o
nly
to s
imila
r pe
rson
s.
d The
num
ber
of e
vent
s w
as lo
w f
or V
TE
(D
VT
1 P
E):
inte
rven
tion
34, c
ontr
ol 6
0, w
hich
is m
uch
less
tha
n th
e op
timal
info
rmat
ion
size
. How
ever
, the
tot
al s
ampl
e si
ze w
as la
rge
(8,9
01 e
ach
grou
p), s
o im
prec
isio
n no
t lik
ely.
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

66© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
References
1 . Gallus AS , Hirsh J , Tutle RJ , et al . Small subcutaneous doses of heparin in prevention of venous thrombosis . N Engl J Med . 1973 ; 288 ( 11 ): 545 - 551 .
2 . Belch JJ , Lowe GD , Ward AG , Forbes CD , Prentice CR . Pre-vention of deep vein thrombosis in medical patients by low-dose heparin . Scott Med J . 1981 ; 26 ( 2 ): 115 - 117 .
3 . Dahan R , Houlbert D , Caulin C , et al . Prevention of deep vein thrombosis in elderly medical in-patients by a low molecular weight heparin: a randomized double-blind trial . Haemostasis . 1986 ; 16 ( 2 ): 159 - 164 .
4 . Ibarra-Pérez C , Lau-Cortés E , Colmenero-Zubiate S , et al . Prevalence and prevention of deep venous thrombosis of the lower extremities in high-risk pulmonary patients . Angiology . 1988 ; 39 ( 6 ): 505 - 513 .
5 . Gärdlund B; The Heparin Prophylaxis Study Group . Ran-domised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious dis-eases . Lancet . 1996 ; 347 ( 9012 ): 1357 - 1361 .
6 . Bergmann JF , Caulin C . Heparin prophylaxis in bedridden patients . Lancet . 1996 ; 348 ( 9021 ): 205 - 206 .
7 . Samama MM , Cohen AT , Darmon JY , et al; Prophylaxis in Medical Patients with Enoxaparin Study Group . A compar-ison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients . N Engl J Med . 1999 ; 341 ( 11 ): 793 - 800 .
8 . Fraisse F , Holzapfel L , Couland JM , et al; The Association of Non-University Affi liated Intensive Care Specialist Physi-cians of France . Nadroparin in the prevention of deep vein thrombosis in acute decompensated COPD . Am J Respir Crit Care Med . 2000 ; 161 ( 4 Pt 1 ): 1109 - 1114 .
9 . Leizorovicz A , Cohen AT , Turpie AG , Olsson CG , Vaitkus PT , Goldhaber SZ ; PREVENT Medical Thromboprophylaxis Study Group . Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients . Circulation . 2004 ; 110 ( 7 ): 874 - 879 .
10 . Mahé I , Bergmann JF , d’Azémar P , Vaissie JJ , Caulin C . Lack of effect of a low-molecular-weight heparin (nadroparin) on mortality in bedridden medical in-patients: a prospective randomised double-blind study . Eur J Clin Pharmacol . 2005 ; 61 ( 5-6 ): 347 - 351 .
11 . Lederle FA , Sacks JM , Fiore L , et al . The prophylaxis of medical patients for thromboembolism pilot study . Am J Med . 2006 ; 119 ( 1 ): 54 - 59 .
12 . Cohen AT , Davidson BL , Gallus AS , et al; ARTEMIS Investigators . Effi cacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial . BMJ . 2006 ; 332 ( 7537 ): 325 - 329 .
13 . Bosson JL , Pouchain D , Bergmann JF; for the ETAPE Study Group . A prospective observational study of a cohort of outpatients with an acute medical event and reduced mobility: incidence of symptomatic thromboembolism and description of thromboprophylaxis practices . J Intern Med . 2006 ; 260 ( 2 ): 168 - 176 .
14 . Darze ES , Latado AL , Guimarães AG , et al . Incidence and clinical predictors of pulmonary embolism in severe heart failure patients admitted to a coronary care unit . Chest . 2005 ; 128 ( 4 ): 2576 - 2580 .
15 . Guijarro R , San Román CM , Perelló JI , Nuño E; Effi ciency Group of the Internal Medicine Services of Andalusia; Stra-tegic Plan of the SADEMI (Andalusia Society of Internal Medicine) . A study of hospital discharges for venous throm-boembolism in the south of Spain. An analysis of 19,170 cases from a regional database from 1998 to 2001 . Eur J Intern Med . 2005 ; 16 ( 4 ): 279 - 286 .
16 . Kishimoto M , Lim HY , Tokuda Y , et al . Prevalence of venous thromboembolism at a teaching hospital in Okinawa, Japan . Thromb Haemost . 2005 ; 93 ( 5 ): 876 - 879 .
17 . Skaf E , Stein PD , Beemath A , Sanchez J , Bustamante MA , Olson RE . Venous thromboembolism in patients with isch-emic and hemorrhagic stroke . Am J Cardiol . 2005 ; 96 ( 12 ): 1731 - 1733 .
18 . Spyropoulos A , Anderson FJ , FitzGerald G , et al . Pre-dictive and associative models to identify hospitalized medi-cal patients at risk for venous thromboembolism . Chest . 2011;140(3):706-714 .
19 . Tapson VF, Decousus H, Pini M, et al; IMPROVE Investi-gators. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: fi ndings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. 2007;132(3):936-945.
20 . Spyropoulos AC , Hussein M , Lin J , Battleman D . Rates of venous thromboembolism occurrence in medical patients among the insured population . Thromb Haemost . 2009 ; 102 ( 5 ): 951 - 957 .
21 . Barbar S , Noventa F , Rossetto V , et al . A risk assessment model for the identifi cation of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score . J Thromb Haemost . 2010 ; 8 ( 11 ): 2450 - 2457 .
22 . Kucher N , Koo S , Quiroz R , et al . Electronic alerts to pre-vent venous thromboembolism among hospitalized patients . N Engl J Med . 2005 ; 352 ( 10 ): 969 - 977 .
23 . Khorana AA , Kuderer NM , Culakova E , Lyman GH , Francis CW . Development and validation of a predictive model for chemotherapy-associated thrombosis . Blood . 2008 ; 111 ( 10 ): 4902 - 4907 .
24 . Spyropoulos AC. Risk Assessment of Venous Thromboembo-lism in Hospitalized Medical Patients. Curr Opin Pulm Med. 2010;16(5):419-425.
25 . Lutz L, Haas S, Hach-Wunderle V. Venous thromboembo-lism in internal medicine: risk assessment and pharmaceu-tical prophylaxis: publication for the specialist platform. Med Welt. 2002;53:231-234.
26 . Bahl V, Hu HM, Henke PK, Wakefi eld TW, Campbell DA, Jr, Caprini JA. A validation study of a retrospective venous thromboembolism risk scoring method. Ann Surg. 2010;251(2):344-350.
27 . Piazza G, Rosenbaum EJ, Pendergast W, et al. Physician alerts to prevent symptomatic venous thromboembolism in hospi-talized patients. Circulation. 2009; 119:2196-2201.
28 . Forette B , Wolmark Y . Calcium nadroparin in the preven-tion of thromboembolic disease in elderly subjects. Study of tolerance . Presse Med . 1995 ; 24 ( 12 ): 567 - 571 .
29 . Lechler E , Schramm W , Flosbach CW; The Prime Study Group . The venous thrombotic risk in non-surgical patients: epidemiological data and effi cacy/safety profi le of a low-molecular-weight heparin (enoxaparin) . Haemostasis . 1996 ; 26 ( Suppl 2 ): 49 - 56 .
30 . Bergmann JF , Neuhart E; The Enoxaparin in Medicine Study Group . A multicenter randomized double-blind study of enoxaparin compared with unfractionated heparin in the prevention of venous thromboembolic disease in elderly in-patients bedridden for an acute medical illness . Thromb Haemost . 1996 ; 76 ( 4 ): 529 - 534 .
31 . Kleber FX , Witt C , Vogel G , Koppenhagen K , Schomaker U , Flosbach CW; THE-PRINCE Study Group . Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease . Am Heart J . 2003 ; 145 ( 4 ): 614 - 621 .
32 . Riess H , Haas S , Tebbe U , et al . A randomized, double-blind study of Certoparin versus UFH to prevent venous
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from
67© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
thromboembolic events in acutely ill, non-surgical patients: CERTIFY study . J Thromb Haemost . 2010 ; 8 ( 6 ): 1209 - 1215 .
33 . Hull RD , Schellong SM , Tapson VF , et al; EXCLAIM (Extended Prophylaxis for Venous ThromboEmbolism in Acutely Ill Medical Patients With Prolonged Immobilization) study . Extended-duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial . Ann Intern Med . 2010 ; 153 ( 1 ): 8 - 18 .
34 . Shorr AF , Williams MD . Venous thromboembolism in criti-cally ill patients. Observations from a randomized trial in sep-sis . Thromb Haemost . 2009 ; 101 ( 1 ): 139 - 144 .
35 . Cook D , Douketis J , Meade M , et al; Canadian Critical Care Trials Group . Venous thromboembolism and bleeding in critically ill patients with severe renal insuffi ciency receiving dalteparin thromboprophylaxis: prevalence, incidence and risk factors . Crit Care . 2008 ; 12 ( 2 ): R32 .
36 . Cook D , Crowther M , Meade M , et al . Deep venous throm-bosis in medical-surgical critically ill patients: prevalence, inci-dence, and risk factors . Crit Care Med . 2005 ; 33 ( 7 ): 1565 - 1571 .
37 . Ibrahim EH , Iregui M , Prentice D , Sherman G , Kollef MH , Shannon W . Deep vein thrombosis during prolonged mechan-ical ventilation despite prophylaxis . Crit Care Med . 2002 ; 30 ( 4 ): 771 - 774 .
38 . Kollef MH , Zahid M , Eisenberg PR . Predictive value of a rapid semiquantitative D-dimer assay in critically ill patients with suspected venous thromboembolic disease . Crit Care Med . 2000 ; 28 ( 2 ): 414 - 420 .
39 . Marik PE, Andrews L, Maini B. The incidence of deep venous thrombosis in ICU patients. Chest. 1997;111:661-664.
40 . Cade JF . High risk of the critically ill for venous thromboem-bolism . Crit Care Med . 1982 ; 10 ( 7 ): 448 - 450 .
41 . The PROTECT Investigators for the Canadian Critical Care Trials Group and the Australian and New Zealand Intensive Care Society Clinical Trials Group . Dalteparin versus Unfrac-tionated Heparin in Critically Ill Patients . N Engl J Med . 2011;364(14):1305-1314.
42 . De A , Roy P , Garg VK , Pandey NK . Low-molecular-weight heparin and unfractionated heparin in prophylaxis against deep vein thrombosis in critically ill patients undergoing major surgery . Blood Coagul Fibrinolysis . 2010 ; 21 ( 1 ): 57 - 61 .
43 . Douketis J , Cook D , Meade M , et al; Canadian Critical Care Trials Group . Prophylaxis against deep vein thrombosis in critically ill patients with severe renal insuffi ciency with the low-molecular-weight heparin dalteparin: an assessment of safety and pharmacodynamics: the DIRECT study . Arch Intern Med . 2008 ; 168 ( 16 ): 1805 - 1812 .
44 . Rabbat CG , Cook DJ , Crowther MA , et al . Dalteparin thromboprophylaxis for critically ill medical-surgical patients with renal insuffi ciency . J Crit Care . 2005 ; 20 ( 4 ): 357 - 363 .
45 . Labarère J , Sevestre M-A , Belmin J , et al; Association pour la Promotion de l’Angiologie Hospitalière . Low-molecular-weight heparin prophylaxis of deep vein thrombosis for older patients with restricted mobility: propensity analyses of data from two multicentre, cross-sectional studies . Drugs Aging . 2009 ; 26 ( 3 ): 263 - 271 .
46 . Sellier E , Labarere J , Sevestre M-A , et al ; Association pour la Promotion de l’Angiologie Hospitalière . Risk factors for deep vein thrombosis in older patients: a multicenter study with systematic compression ultrasonography in postacute care facilities in France . J Am Geriatr Soc . 2008 ; 56 ( 2 ): 224 - 230 .
47 . Bosson J-L , Labarere J , Sevestre MA , et al . Deep vein thrombosis in elderly patients hospitalized in subacute care facilities: a multicenter cross-sectional study of risk factors, prophylaxis, and prevalence . Arch Intern Med . 2003 ; 163 ( 21 ): 2613 - 2618 .
48 . Benoist M , Barrellier MT , Gautier P , Hodara M , Alix M . Venous thromboembolic disease in a geriatric environment.
Importance of its detection and treatment. J Mal Vasc . 1994 ; 19 ( 4 ): 289 - 293 .
49 . Gatt ME , Paltiel O , Bursztyn M . Is prolonged immobilization a risk factor for symptomatic venous thromboembolism in elderly bedridden patients? Results of a historical-cohort study . Thromb Haemost . 2004 ; 91 ( 3 ): 538 - 543 .
50 . Kropsky B , Shi Y , Cherniack EP . Incidence of deep-venous thrombosis in nursing home residents using megestrol ace-tate . J Am Med Dir Assoc . 2003 ; 4 ( 5 ): 255 - 256 .
51 . Gomes JP , Shaheen WH , Truong SV , Brown EF , Beasley BW , Gajewski BJ . Incidence of venous thromboembolic events among nursing home residents . J Gen Intern Med . 2003 ; 18 ( 11 ): 934 - 936 .
52 . Valderrama A , Del Castillo J , DiazGranados CA , et al . Deep vein thrombosis in chronically bedridden elderly individuals . J Am Geriatr Soc . 2006 ; 54 ( 5 ): 866 - 867 .
53 . Liperoti R , Pedone C , Lapane KL , Mor V , Bernabei R , Gambassi G . Venous thromboembolism among elderly patients treated with atypical and conventional antipsychotic agents . Arch Intern Med . 2005 ; 165 ( 22 ): 2677 - 2682 .
54 . Heit JA , Silverstein MD , Mohr DN , Petterson TM , O’Fallon WM , Melton LJ III. Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study . Arch Intern Med . 2000 ; 160 ( 6 ): 809 - 815 .
55 . Heit JA , O’Fallon WM , Petterson TM , et al . Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study . Arch Intern Med . 2002 ; 162 ( 11 ): 1245 - 1248 .
56 . Rodríguez-Mañas L , Gómez-Huelgas R , Veiga-Fernández F , Ruiz GM , González JM ; ANCIANOS Investigators . Thrombo-prophylaxis with the low-molecular-weight heparin bemiparin sodium in elderly medical patients in usual clinical practice: the ANCIANOS study . Clin Drug Investig . 2010 ; 30 ( 5 ): 337 - 345 .
57 . Liebson CL , Petterson TM , Bailey KR , Melton LJ III , Heit JA . Risk factors for venous thromboembolism in nursing home residents . Mayo Clin Proc . 2008 ; 83 ( 2 ): 151 - 157 .
58 . Prieto SAJ . Efi cacia y seguridad de bemiparina en la preven-ción de la enfermedad tromboembólica venosa en pacientes de una residencia geriátrica . Rev Esp Geriatr Gerontol . 2007 ; 42 (1): 20 - 26 .
59 . Cesarone MR , Belcaro G , Nicolaides AN , et al . Venous throm-bosis from air travel: the LONFLIT3 study—prevention with aspirin vs low-molecular-weight heparin (LMWH) in high-risk subjects: a randomized trial . Angiology . 2002 ; 53 ( 1 ): 1 - 6 .
60 . Belcaro G , Cesarone MR , Rohdewald P , et al . Prevention of venous thrombosis and thrombophlebitis in long-haul fl ights with pycnogenol . Clin Appl Thromb Hemost . 2004 ; 10 ( 4 ): 373 - 377 .
61 . Erkan D , Yazici Y , Peterson MG , Sammaritano L , Lockshin MD . A cross-sectional study of clinical thrombotic risk factors and preventive treatments in antiphospholipid syndrome . Rheumatology (Oxford) . 2002 ; 41 ( 8 ): 924 - 929 .
62 . Erkan D , Harrison MJ , Levy R , et al . Aspirin for primary thrombosis prevention in the antiphospholipid syndrome: a randomized, double-blind, placebo-controlled trial in asymp-tomatic antiphospholipid antibody-positive individuals . Arthritis Rheum . 2007 ; 56 ( 7 ): 2382 - 2391 .
63 . Glynn RJ , Ridker PM , Goldhaber SZ , Buring JE . Effect of low-dose aspirin on the occurrence of venous thromboem-bolism: a randomized trial [Summary for patients in Ann Intern Med . 2007 Oct 16;147(8):I34] . Ann Intern Med . 2007 ; 147 ( 8 ): 525 - 533 .
64 . Hereng T , Lambert M , Hachulla E , et al . Infl uence of aspirin on the clinical outcomes of 103 anti-phospholipid antibodies-positive patients . Lupus . 2008 ; 17 ( 1 ): 11 - 15 .
65 . Tektonidou MG , Laskari K , Panagiotakos DB , Moutsopoulos HM . Risk factors for thrombosis and primary thrombosis prevention
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

68© 2012 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml). DOI: 10.1378/chest.11-2296
in patients with systemic lupus erythematosus with or with-out antiphospholipid antibodies . Arthritis Rheum . 2009 ; 61 ( 1 ): 29 - 36 .
66 . Grady D , Wenger NK , Herrington D , et al . Postmenopausal hormone therapy increases risk for venous thromboembolic disease. The Heart and Estrogen/progestin Replacement Study . Ann Intern Med . 2000 ; 132 ( 9 ): 689 - 696 .
67 . Ray JG , Mamdani M , Tsuyuki RT , Anderson DR , Yeo EL , Laupacis A . Use of statins and the subsequent development of deep vein thrombosis . Arch Intern Med . 2001 ; 161 ( 11 ): 1405 - 1410 .
68 . Smeeth L , Douglas I , Hall AJ , Hubbard R , Evans S . Effect of statins on a wide range of health outcomes: a cohort study validated by comparison with randomized trials . Br J Clin Pharmacol . 2009 ; 67 ( 1 ): 99 - 109 .
69 . Glynn RJ , Danielson E , Fonseca FA , et al . A randomized trial of rosuvastatin in the prevention of venous thromboembo-lism . N Engl J Med . 2009 ; 360 ( 18 ): 1851 - 1861 .
70 . Ridker PM , Danielson E , Fonseca FA , et al ; JUPITER Study Group . Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein . N Engl J Med . 2008 ; 359 ( 21 ): 2195 - 2207 .
71 . Ridker PM , Fonseca FA , Genest J , et al ; JUPITER Trial Study Group . Baseline characteristics of participants in the JUPITER trial, a randomized placebo-controlled primary pre-vention trial of statin therapy among individuals with low low-density lipoprotein cholesterol and elevated high-sensitivity C-reactive protein . Am J Cardiol . 2007 ; 100 ( 11 ): 1659 - 1664 .
72 . Brophy DF , Bukaveckas BL , Ferreira-Gonzalez A , Archer KJ , Martin EJ , Gehr TW . A pilot study of genetic polymorphisms and hemodialysis vascular access thrombosis . Hemodial Int . 2009 ; 13 ( 1 ): 19 - 26 .
73 . Doggen CJ , Lemaitre RN , Smith NL , Heckbert SR , Psaty BM . HMG CoA reductase inhibitors and the risk of venous throm-bosis among postmenopausal women . J Thromb Haemost . 2004 ; 2 ( 5 ): 700 - 701 .
74 . Lacut K , Oger E , Le Gal G , et al . Statins but not fi brates are associated with a reduced risk of venous thromboembolism: a hospital-based case-control study . Fundam Clin Pharmacol . 2004 ; 18 ( 4 ): 477 - 482 .
75 . Lacut K , Le Gal G , Abalain JH , Mottier D , Oger E . Differ-ential associations between lipid-lowering drugs, statins and fi brates, and venous thromboembolism: role of drug induced homocysteinemia? Thromb Res . 2008 ; 122 ( 3 ): 314 - 319 .
76 . Ramcharan AS , Van Stralen KJ , Snoep JD , Mantel-Teeuwisse AK , Rosendaal FR , Doggen CJ . HMG-CoA reductase inhibitors, other lipid-lowering medication, antiplatelet therapy, and the risk of venous thrombosis . J Thromb Haemost . 2009 ; 7 ( 4 ): 514 - 520 .
77 . Sørensen HT , Horvath-Puho E , Søgaard KK , et al . Arterial cardiovascular events, statins, low-dose aspirin and subse-quent risk of venous thromboembolism: a population-based case-control study . J Thromb Haemost . 2009 ; 7 ( 4 ): 521 - 528 .
78 . Yang CC , Jick SS , Jick H . Statins and the risk of idiopathic venous thromboembolism . Br J Clin Pharmacol . 2002 ; 53 ( 1 ): 101 - 105 .
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from

DOI 10.1378/chest.11-2296 2012;141; e195S-e226SChest
Hoang Le, Sam Schulman and M. Hassan MuradDentali, Elie A. Akl, Deborah J. Cook, Alex A. Balekian, Russell C. Klein,
Susan R. Kahn, Wendy Lim, Andrew S. Dunn, Mary Cushman, FrancescoPhysicians Evidence-Based Clinical Practice Guidelines
and Prevention of Thrombosis, 9th ed: American College of Chest Prevention of VTE in Nonsurgical Patients : Antithrombotic Therapy
May 1, 2012This information is current as of
http://chestjournal.chestpubs.org/content/suppl/2012/02/03/141.2_suppl.e195S.DC1.html View e-supplements related to this article at:
Supplementary Material
http://chestjournal.chestpubs.org/content/141/2_suppl/e195S.full.htmlUpdated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/141/2_suppl/e195S.full.html#ref-list-1This article cites 164 articles, 55 of which can be accessed free at:
References
http://chestjournal.chestpubs.org/content/141/2_suppl/e195S.full.html#related-urlsThis article has been cited by 5 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlfound online at: Information about reproducing this article in parts (figures, tables) or in its entirety can bePermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
"Services" link to the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the
Citation Alerts
PowerPoint slide format. See any online figure for directions. articles can be downloaded for teaching purposes inCHESTFigures that appear in Images in PowerPoint format
© 2012 American College of Chest Physicians at Univ Med & Dentistry of NJ on May 1, 2012chestjournal.chestpubs.orgDownloaded from