Presented by, Lynn Handy - Managed Resources
105
Presented by, Lynn Handy (CPC, CPC-I, COC, CCS-P, LPN) 1
Transcript of Presented by, Lynn Handy - Managed Resources

Presented by, Lynn Handy (CPC, CPC-I, COC, CCS-P, LPN)
1

Your Presenter
Lynn HandyCPC, CPC-I, COC, CCS-P, LPN
2

Agenda
3
Inpatient E&M Services
Same Day Admit/Discharge
Observation
Nursing Facility Services
Pre-Op Services
Split/Shared Services
Teaching Physician Guidelines

In Patient Services

Inpatient Services
Initial (3 of 3 Key Components)
• 99221• 99222• 99223
Subsequent (2 of 3 Key Components)
• 99231• 99232• 99233
Discharge (Time)
• 99238 <30• 99239 >30

Initial In-Patient Services
Detailed History and Exam will be the minimum requirements for the lowest level of service.
99221 Detailed History/Detailed Exam SF/Low MDM99222 Comprehensive Hx/Comprehensive Ex Moderate MDM99223 Comprehensive Hx/Comprehensive Ex High MDM
Inpatient Admissions with less than Detailed History and Exam will be coded as subsequent hospital services. https://www.cms.gov/Regulations-and-
Guidance/Guidance/Transmittals/downloads/R2282CP.pdf
6
99221 Detailed History/Detailed Exam SF/Low MDM
99222 Comprehensive History/Comprehensive Exam Moderate MDM
99223 Comprehensive History/Comprehensive Exam High MDM

History
DETAILED (99221)
COMPREHENSIVE (99222/99223)
4 HPI 4 HPI
2 Review of System (ROS)
10+ Review of Systems
Past, Family & Social History
• Only 1 required
Past, Family & Social History
• All 3 required

Chief Complaint
A chief complaint is a required element for all E/M services. A CC is a concise statement describing the symptom, problem,
condition, diagnosis, or other factor that is the reason for the encounter. Usually stated in the patient’s words. Chief Complaint will help to establish the “medical necessity” for the
visit.NOTE: Chief Complaint is often missing from the documentation for
subsequent hospital visits.
8

ROS Tips The E/M documentation guidelines state that for a
complete ROS those systems with positive or pertinent negatives responses must be individually documented. For the remaining systems, a notation such as “all other systems were reviewed and are negative” is permissible. Variations of language may also be acceptable if they clearly imply the same
o In the absence of such a notation at least ten systems must be individually documented
o The following are examples of allowed statements:
– All other systems are negative
– A complete ROS is negative
Examples of phrases/documentation that are not allowed:
o “Other ROS non-contributory”
o “All ROS negative” (without documenting the pertinent positive and/or negative responses related to the presenting problem)
o “The rest of the ROS is negative”
o “No other complaints”
9

Family History Use of “non-contributory” as the sole notation in regards to all or part of
PFSH (e.g., “Family History – non-contributory”) should not be credited. If the PFSH or a portion of the PFSH is reviewed by the physician and deemed non-contributory, a statement is required in the documentation to qualify it for a complete or partial PFSH. o Example: “Reviewed PFSH, non-contributory to current condition”
(or a similar statement indicating that the history was in fact reviewed)
o Example: “Family History non-contributory to heart disease”
Do not allow the following statements: o Family History: “reviewed and non-contributory” without mention
of the current condition o “Family History reviewed and negative” o “Family History none”

Unable to Obtain a History
If the physician is unable to obtain a history from the patient or other source, the record should describe the patient’s condition or other circumstance which precludes obtaining the history
If the patient’s condition or other circumstance is clearly documented in the medical record, and the physician notes what elements of the history are unobtainable, the coder may give the provider credit for a Comprehensive History if the severity of the nature of the presenting problem warrants a comprehensive history. The physician must still document all elements, but he/she can simply note “unobtainable due to patient being intubated.” o Example: “PFSH and ROS are unobtainable as patient presents in a coma”
11

2019 MPFS Proposed Rule
CMS has proposed to allow practitioners to simply review and verify certain information in the medical record that is entered by ancillary staff or the beneficiary, rather than re-entering it.
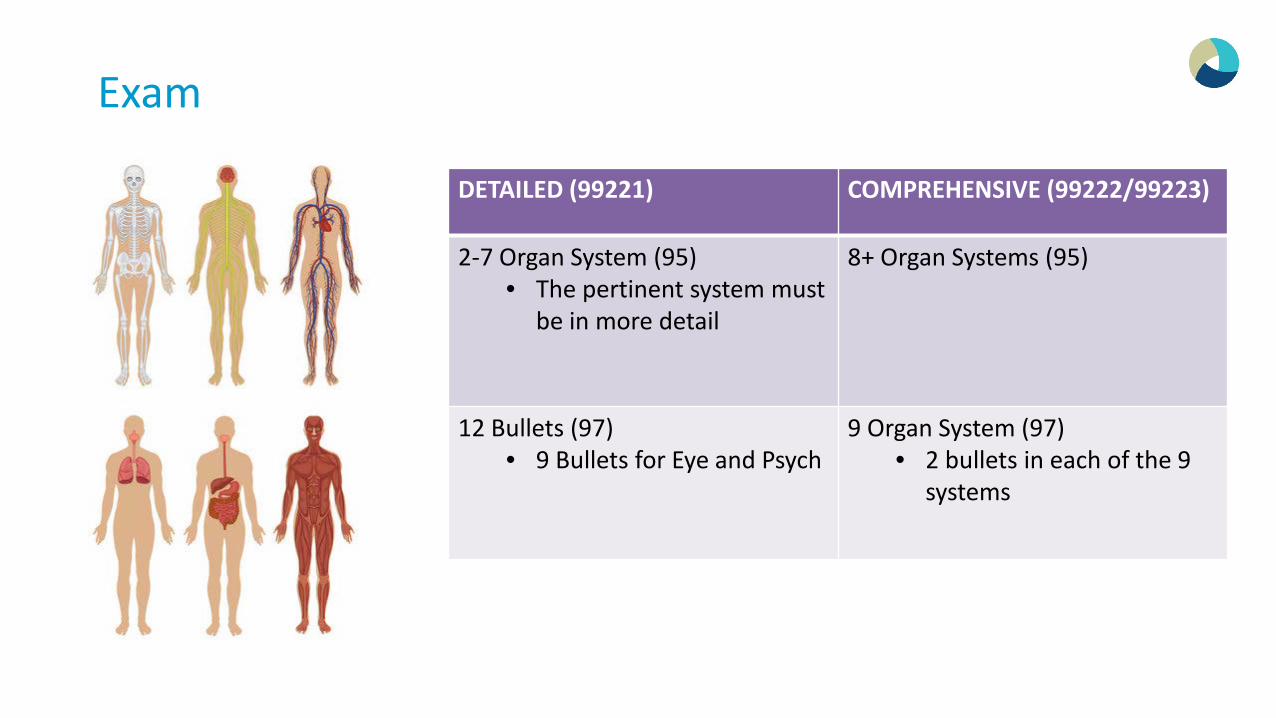
Exam
DETAILED (99221) COMPREHENSIVE (99222/99223)
2-7 Organ System (95)• The pertinent system must
be in more detail
8+ Organ Systems (95)
12 Bullets (97)• 9 Bullets for Eye and Psych
9 Organ System (97)• 2 bullets in each of the 9
systems

1995 Examination Guidelines
14
PROBLEM FOCUSED EXAM
• Defined as “a limited examination of the affected body area or organ system.”
EXPANDED PROBLEM FOCUSED EXAM
• Defined as “a limited examination of the affected body area or organ system and other symptomatic of related organ system(s)” (2-7 BA/OS)
DETAILED EXAM
• Defined as “an extendedexamination of the affected body area or organ system and other symptomatic or related organ system(s)” (2-7 BA/OS)
COMPREHENSIVE EXAM
• Defined as general multi-system examination or complete examination of a single organ system. (8+ OS)

Medical Decision Making
Start with medical decision making and work “backward” from the problem. After determining medical decision making through a simple, tabular formula, the correct code will be identified and all necessary supporting documentation can be captured.
This is arguably the most important of the three key components because the Medical Decision-Making ( MDM ) reflects the intensity of the cognitive labor performed by the physician.
Medical decision making can help to drive medical necessity and, therefore, should be one of the two components that drives the level of service for subsequent patient services and the basis for leveling any E/M service.
15

Complexity of Medical Decision Making
Straightforward
Low
Moderate
High
16
Diagnosis Data Risk

Medical Decision Making
High
• 99223 (Initial)• 99233 (Subsequent visit)
Moderate
• 99222 (Initial)• 99232 (Subsequent visit)

Medical Decision Making
New Problem –Is additional work-up planned?o The term “work-up” is meant as any additional testing services that may be performed
(during a future visit) that will assist the physician in determining a condition or extent of a condition that would help him effectively manage the patient.
• Labs, Radiology, etc.• Consultation (requesting advise/opinion of another physician) is considered additional
work-up• Decision for surgery/procedure:
Diagnostic work-up
Therapeutic not a work-up
Established Problem(s): Is it stable or unstable?
18

Amount and/or Complexity of Data Reviewed
Refers to information gathered from sources other than the history and physical exam. The point values assigned in the documentation guidelines are for types of data (e.g., lab tests, review
of old records etc.), not for quantities of data. Data:
o Review and order of diagnostic studies.o Discussions with other physicians.o Interpretations of films or tracing brought in by the patient from an outside source (independent
visualization).o Review of old records (summary of findings must be documented).
Q: In the amount and/or complexity section, what is the difference between Decision to "obtain history from someone other than the patient" equals to 1 point verses Review & summary of old records and/or "obtaining history from someone other than patient" equals to 2 points.
19

Presenting Problem: Moderate or High Risk
One or more chronic illnesses with mild
exacerbation
Patient with Asthma comes
in wheezing
COPD with Shortness of
Breath
Diabetes with increased
blood sugar
Undiagnosed New Problem
FUO
Shortness of Breath
One or more chronic illnesses with severe
exacerbation
Patient with Asthma comes in with Respiratory Distress and is
admitted to the hospital
Patient with severe
dehydration and disoriented
Acute or Chronic illness or injury that may pose a threat to life or bodily function
Organ System Failure (ESRD)
Head injury with altered
mental status
Diabetic with Ketoacidosis
20

Management Options
Elective Major surgeryoWith no identified risk factors (Moderate risk)oWith identified risk factors (High risk)
– These risk factors are above and beyond the risk of the procedure/surgery– Physician must mention the additional factor as a heightened risk i.e. Diabetes, COPD/Emphysema, etc Patient has increased risk due to diabetes and COPD

Drug Therapy requiring intensive monitoring for toxicity (High Risk)
22
DRUG LEVEL MONITORING IS MAY NOT BE REQUIRED DRUG LEVEL MONITORING MAY BE REQUIRED
For drugs with a well-defined clinical response and a high therapeutic index (i.e., low toxicity), intensive therapeutic drug monitoring is not necessary
Administration of cytotoxic chemotherapy is always considered high risk under management options when monitoring of blood cell counts is used as a surrogate for toxicity.
For acute or short-term drug therapy, there is no advantage to monitoring drug levels
Drugs that have a narrow therapeutic window and a low therapeutic index may exhibit toxicity at concentrations close to the upper limit of the therapeutic range and may require intensive clinical monitoring.
For treatment of chronic disorders such as antihypertensive therapy, if the desired response can be readily assessed by a noninvasive technique, such as blood pressure monitoring, serial drug level monitoring is not medically necessary
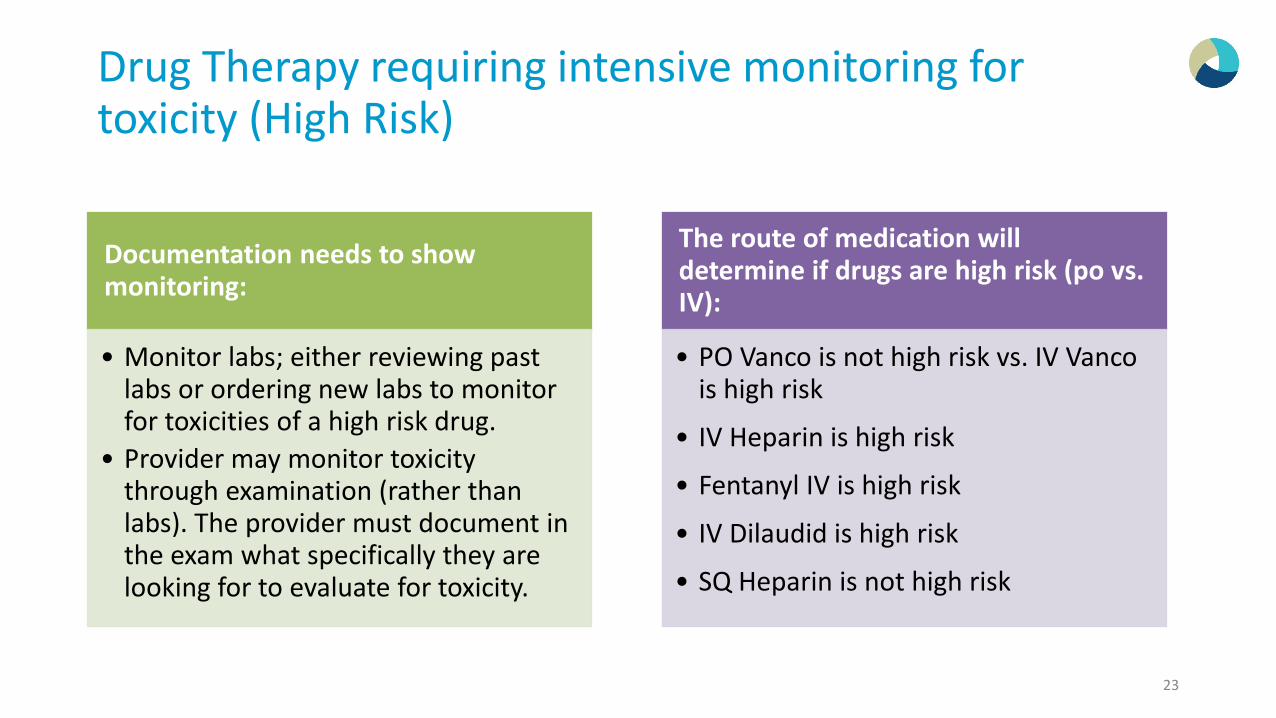
Drug Therapy requiring intensive monitoring for toxicity (High Risk)
23
Documentation needs to show monitoring:
• Monitor labs; either reviewing past labs or ordering new labs to monitor for toxicities of a high risk drug.
• Provider may monitor toxicity through examination (rather than labs). The provider must document in the exam what specifically they are looking for to evaluate for toxicity.
The route of medication will determine if drugs are high risk (po vs. IV):
• PO Vanco is not high risk vs. IV Vancois high risk
• IV Heparin is high risk
• Fentanyl IV is high risk
• IV Dilaudid is high risk
• SQ Heparin is not high risk

Risk assessment is based on: Disease process anticipated between present encounter and next. Risk during and following any procedures or treatment. Co-morbidities that increase complexity of medical decision due to risk of
complications, morbidity, mortality. Type of surgical or invasive diagnostic procedure ordered or performed
during encounter. Referral for or decision to perform an urgent surgical or invasive diagnostic
procedure. Decision for major surgery is not high risk unless there are additional risk
factors involved. If not, decision for major surgery is moderate risk. Prescription drug management includes more than reviewing prescriptions.
Documentation must support prescribing, ordering , altering or directing instructions regarding prescription.
24
Table of Risk
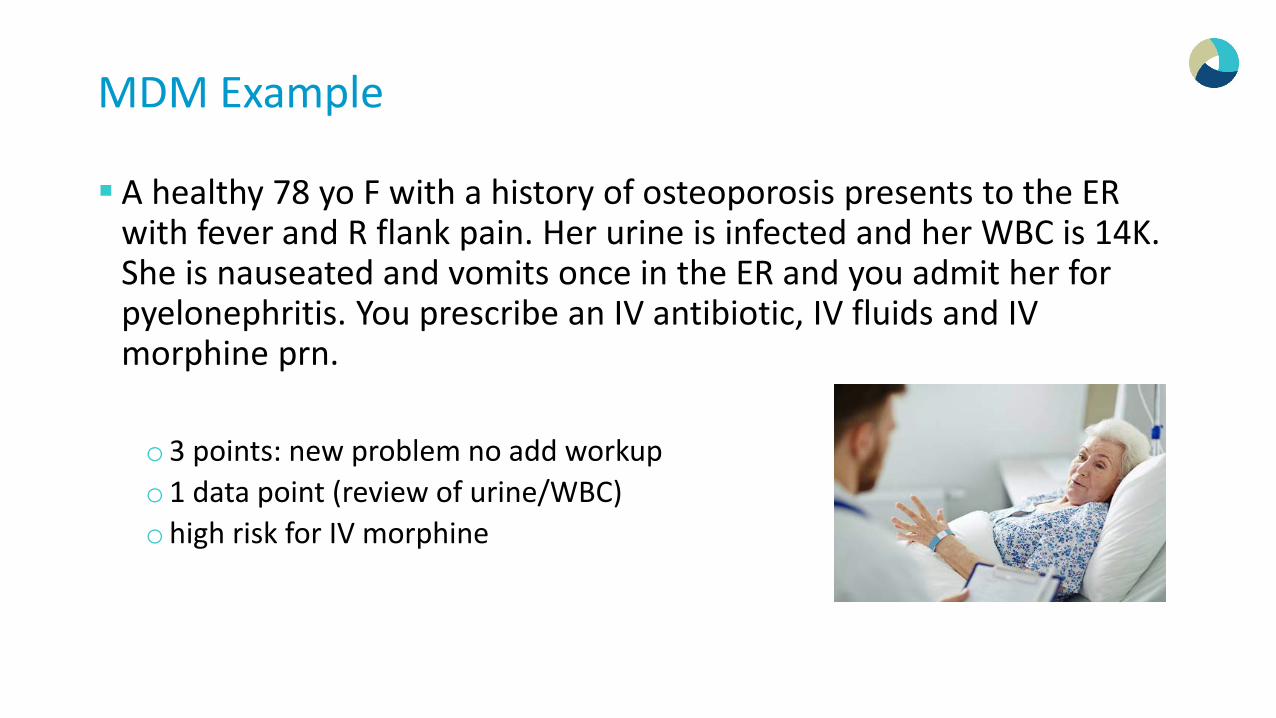
MDM Example
A healthy 78 yo F with a history of osteoporosis presents to the ER with fever and R flank pain. Her urine is infected and her WBC is 14K. She is nauseated and vomits once in the ER and you admit her for pyelonephritis. You prescribe an IV antibiotic, IV fluids and IV morphine prn.
o3 points: new problem no add workupo1 data point (review of urine/WBC)ohigh risk for IV morphine

MDM Examples
A 92 yo M with dementia, aspiration pneumonia, ARF and DM is doing poorly. His labs and chest x-ray get worse each day. You discuss the option of comfort measures with the family who are in agreement with that plan.
o4 points for dx, o2 points in dataohigh risk for deescalating care

Coding by Time
27

Counseling & Coding by Time
Counseling includes:oDiagnostic results, impressions, and/or recommended diagnostic studies.oPrognosis.oRisks and benefits of treatment options.o Instructions for treatment and/or follow-up.o Importance of compliance with chosen treatment options.oRisk factor reduction.oPatient and family education.
28

Documenting Time and Content of Counseling When counseling and/or coordination of care makes up more than 50% of the total time
spent with the patient during an encounter, time can be used as the key factor in choosing a level of service. Documentation must include:
o Total time spent.o % of time spent in counseling.o What was discussed in counseling. No canned or pre-set template statement when this appears to
be cloned. Can be coded by time:
o I spent 25 minutes with the patient, greater than 50% of the time was spent discussing her new diagnosis, conservative treatment options and reassurance.
Cannot be coded by time:o A long discussion was held with the patient as to his underlying diagnosis. Course of treatment
plan from conservative management to lesion excision was discussed with the patient.
29

Rounding the Time
30
Sequential Time Coding• The physician spends 31 minutes
counseling a patient in the hospital and the discussion is more than 50% of the total encounter
• 99232 is for 25 minutes and 99233 is for 35 minutes
• You would code 99233 since it is closest to the actual time
Family Discussions• Time spent with the family can be
included IF the discussion results in a treatment or management decision. That outcome must be documented in the medical records within the face to face visit note.
Coordination of Care• Time spent discussing the patient
with other providers and nursing staff may also be included in the total time.

Date of Service on H & P Dictation
Issue: DOS is missing from inpatient dictation. The admit date is not always the DOS you are documenting and billing for. Resolution: Dictate the date you are seeing the patient in the
beginning of your dictation or within your Teaching Physician Attestation note.
*Note Example: “Patient (or insert patient name) seen on xx/xx/xxxxfor …….”

Subsequent Inpatient Services

33
Subsequent In-Patient Services (99231-99233)
A subsequent hospital service and a hospital discharge may not be reported on the same calendar date by the same provider. If a consulting physician sees a patient on the day of discharge, the
subsequent hospital codes should be reported, unless the attending physician has transferred the care of the patient to you.Hospitalist/Consultants may report subsequent hospital services for a
surgical patient during the post operative period only if it is unrelated to the post op care of the patient and the name of the requesting physician is documented
33

If you are in one of the following states, CMS requires post op care 99024 to be reported, effective July 1, 2017
Global Surgery Data Collection: Postoperative Care
• New Jersey• Kentucky• Louisiana• Nevada
• North Dakota• Ohio• Oregon• Rhode Island
CMS is currently collecting data on the number of post op visits for specific types of surgery and who is performing those post op visits.
Practitioners who only practice in practices with fewer than 10 practitioners are exempted from required reporting, but are encouraged to report if feasible.
The list of 293 procedure codes that require 99024 to be reported is located at this CMS websiteo https://www.cms.gov/Medicare/Medicare-Fee-
for-Servie-Payment/PhysicianFeeSched/Global-Surgery-Data-Collection-.html
2019 CMS Proposal Rule
In these nine states, from July 1, 2017 through December 31, 2017, there were 990,581 postoperative visits reported using CPT code 99024. Of the 32,573 practitioners who furnished at least one of the 293 procedures during this period and who, based on Tax Identification Numbers in claims data, were likely to meet the practice size threshold, only 45 percent reported one or more visit using CPT code 99024 during this 6-month period. The share of practitioners who reported any CPT code 99024 claims varied by specialty.o Among 90-day global procedures performed from July 1, 2017 through December 31,
2017, where it is possible to clearly match postoperative visits to specific procedures, 67 percent had one or more matched visit reported using CPT code 99024.
o Among 10-day global procedures performed from July 1, 2017 through December 31, 2017, where it is possible to clearly match postoperative visits to specific procedures, only 4 percent had one or more matched visit reported with CPT code 99024

The Nature of the Presenting Problem
The nature of the presenting problem usually determines the levels of history and physical exam required.oCPT code 99231 usually requires documentation to support that the patient is
stable, recovering, or improving.oCPT code 99232 usually requires documentation to support that the patient is
responding inadequately to therapy or has developed a minor complication. Such minor complication might call for careful monitoring of comorbid conditions requiring continuous, active management.
oCPT code 99233 usually requires documentation to support that the patient is unstable or has a significant new problem or complication.
Subsequent Inpatient Level 2 versus Level 3
Level 2 (99232)o Subsequent hospital care visit for
a 62-year-old female with congestive heart failure, who remains dyspneic and febrile.
– This could be a level 3 if the patient has other co morbid conditions that complicate the care of the patient and raise the risk level
Level 3 (99233)o Subsequent hospital visit for a
type 1 diabetes mellitus patient with a new onset of fever, change in mental status, and a diffuse petechial, purpuric eruption.

Multiple visits Same Day, Same Patient, But Different Physicians
Question: Can multiple subsequent visits with different diagnoses (different chronic conditions) from many physicians be billed on the same day for SNF visits (99307-99310) or Acute hospital visits (99231-99233)?
• Are they in the same specialty group?• Is it Medically necessary for multiple physicians to see the same patient on the same day?
• CMS says:• In a hospital inpatient situation involving one physician covering for another, if physician A
sees the patient in the morning and physician B, who is covering for A, sees the same patient in the evening, contractors do not pay physician B for the second visit. The hospital visit descriptors include the phrase “per day” meaning care for the day.
• If the physicians are each responsible for a different aspect of the patient’s care, pay both visits if the physicians are in different specialties and the visits are billed with different diagnoses. There are circumstances where concurrent care may be billed by physicians of the same specialty
• 2019 MPFS Proposed Rule:• CMS will solicit public comment on potentially eliminating a policy that prevents payment for
same-day E/M visits by multiple practitioners in the same specialty within a group practice.

Discharge Day Management

40
In-Patient Discharge Day Management (99238/99239) Hospital discharge management is a face to face service between the attending
physician and the patient. Only the attending physician of record (or physician acting on behalf of the
attending physician) shall report the Hospital discharge codes (subsequent hospital services may not be reported by the attending on the same day as discharge).o Documentation of “Acceptance of Transfer of Care” is required for the Consulting Hospitalist
to bill a discharge.
The provider shall report the Discharge for the date of the actual visit even if the patient is discharged on a different calendar date (no visit on the day of discharge) 99239 must document over 30 minutes spent discharging the patient
40

41
Death Summaries
Only the physician who personally performs the pronouncement of death shall bill for the face-to-face Hospital Discharge Day Management. The date of the death pronouncement shall
reflect the date of service on the calendar date it was performed even if the paperwork is delayed to a subsequent date. If the patient was seen in the morning and
expired later that day, but the provider did not do the pronouncement of death, a subsequent hospital code would be billed (even though the hospital requires a death summary to be dictated)
41

Hospital Discharge and SNF Admit Same Day
Medicare will pay the hospital discharge code (codes 99238 or 99239) in addition to a nursing facility admission code when they are billed by the same physician with the same date of service.Documentation requirements:
o Two separate notes are required: Hospital Discharge Summary and a SNF H & P.
Reference: CMS Manual System: Section 30.6.9.2Q: Can Critical Care and a Discharge both be billed on the same day?

Observation Services

44
Observation
Observation services are only reimbursable by Medicare when they are provided by the order of a physician or another individual authorized to admit patients to the hospital or order outpatient tests.
The order may simply state o “Place patient in outpatient Observation”, with documentation of the medical
necessity.
Only the admitting physician can report Observation codes.
44

Same Day Admit/Discharge Coding
45
Observation or inpatient hospital care, for the evaluation & management of a patient including admission and discharge on the same date which requires 3 key components.
These codes would be reported when the patient is in observation for a minimum of 8 hours to 24 hours.
These codes should also be used for In-patient admission and Discharge on the same calendar date if the above Observation guidelines are met.
If the patient is admitted to the Hospital for a minimum of 8 hours, maximum of 24 hours the admitting provider may bill these codes
HISTORY EXAM MEDICAL DECISION MAKING99234 Detailed or Comprehensive Detailed or Comprehensive SF or Low MDM
99235 Comprehensive Comprehensive Moderate MDM99236 Comprehensive Comprehensive High MDM

Documentation Requirements for Same Day Admit/Discharge
The physician shall satisfy the E/M documentation guidelines for furnishing observation care or inpatient hospital care. In addition to meeting the documentation requirements for history, examination, and medical decision making, documentation in the medical record shall include: oDocumentation stating the stay for observation care or inpatient hospital care
involves 8 hours, but less than 24 hours; oDocumentation identifying the billing physician was present and personally
performed the services; and oDocumentation identifying the order for observation services, progress notes,
and discharge notes were written by the billing physician.

Initial Observation Care (when discharge occurs on a different day)
47
The following codes are used to report an encounter by the supervising physician with the patient when designated as “Observation status”. This includes the initiation of observation status, supervision of the care plan for observation and performance of periodic reassessments.
These codes would be reported when Observation care is less than 8 hours on the same calendar date (Observation discharge would not be reported).
All 3 key components must be documented.
HISTORY EXAM MEDICAL DECISION MAKING
99218 Detailed or Comprehensive Detailed or Comprehensive SF or Low MDM
99219 Comprehensive Comprehensive Moderate MDM
99220 Comprehensive Comprehensive High MDM

Outpatient/ED to Observation
All other outpatient services (hospital emergency department, physician’s office, nursing facility) provided to the patient on the same date as admitted to observation are considered part of the initial observation care. Only the Observation code would be reported. Patient seen in ED and admitted to Observation
but an OBS bed is not available.oObservation starts when the order is written. (not
when they are transferred out of the ED)
48

Observation transfer to Inpatient Status If the same physician who ordered hospital outpatient observation services also
admits the patient to inpatient status before the end of the date on which the patient began receiving hospital outpatient observation services, Medicare will pay only an initial hospital visit for the evaluation and management services provided on that date. Medicare payment for the initial hospital visit includes all services provided to the patient on the date of admission by that physician, regardless of the site of service. The physician may not bill an initial or subsequent observation care code for
services on the date that he or she admits the patient to inpatient status. If the patient is admitted to inpatient status from hospital outpatient observation care subsequent to the date of initiation of observation services, the physician must bill an initial hospital visit for the services provided on that date. The physician may not bill the hospital observation discharge management code
(code 99217) or an outpatient/office visit for the care provided while the patient received hospital outpatient observation services on the date of admission to inpatient status.
49

Observation transfer to Inpatient Status
Day 1: Patient is admitted to Observation
Provider codes 99218-99220Day 2: Patient meets inpatient criteria
Provider can bill the Initial Inpatient codes if the patients conditions requires it and the documentation supports• If the minimum documentation requirements
are not met for the Initial inpatient codes than the subsequent inpatients codes should be billed
Provider must write another order to admit the patient to inpatient status
50

Inpatient transfer to Observation
If IP is ordered, and the hospital wishes to change the patient to OBS, this can be done using condition code (CC) 44, if the practitioner responsible for the care of the patient agrees to the change and the patient is notified prior to discharge. A new order must be written to admit the patient to OBS status
51

Inpatient transfer to Observation
Example:
Day 1
Patient admitted to inpatientDay 2
Clinical Review Nurses notifies the physician the patient did not meet inpatient criteria on Day 1 and wants to change the patient to Observation. • The Inpatient code must be changed
to OBS for Day 1
52
Subsequent Observation
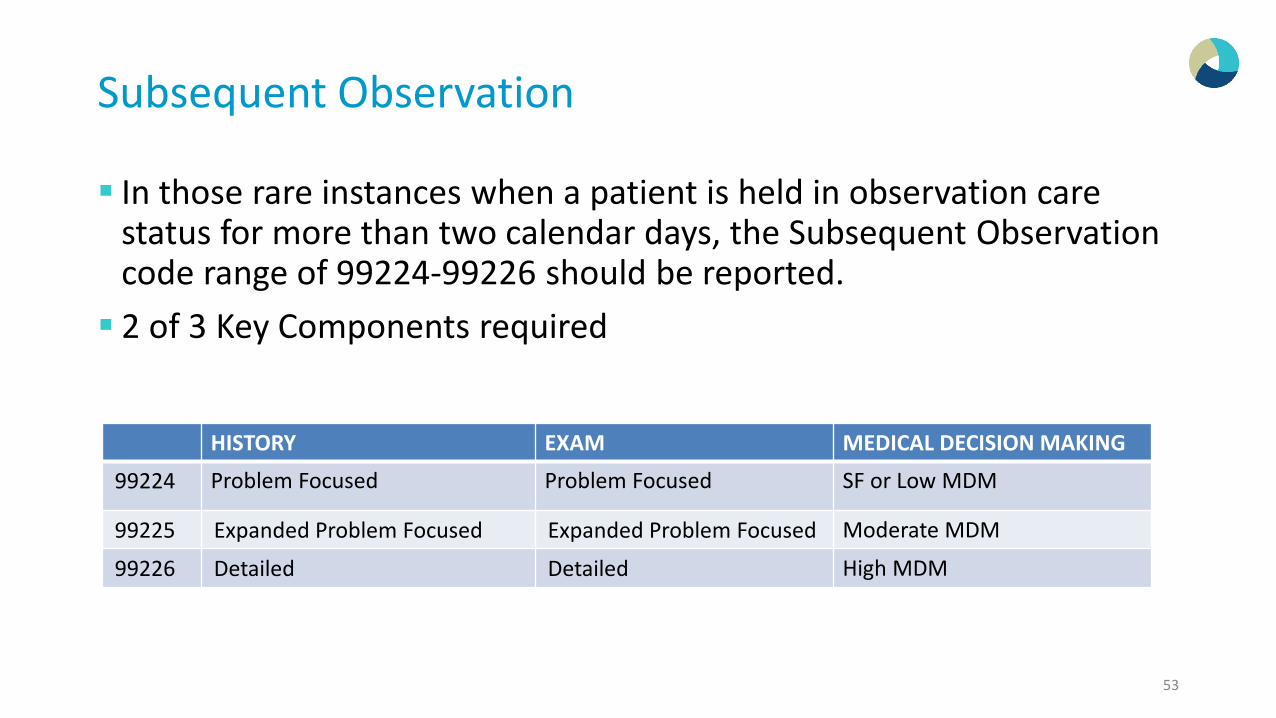
In those rare instances when a patient is held in observation care status for more than two calendar days, the Subsequent Observation code range of 99224-99226 should be reported. 2 of 3 Key Components required
53
HISTORY EXAM MEDICAL DECISION MAKING
99224 Problem Focused Problem Focused SF or Low MDM
99225 Expanded Problem Focused Expanded Problem Focused Moderate MDM
99226 Detailed Detailed High MDM

Two-Midnight Rule
This rule established Medicare payment policy regarding the benchmark criteria that should be used when determining whether inpatient admission is reasonable and payable under Medicare Part A. In general, the Two-Midnight rule stated that:
o Inpatient admissions will generally be payable under Part A if the admitting practitioner expected the patient to require a hospital stay that crossed two midnights and the medical record supports that reasonable expectation.
oMedicare Part A payment is generally not appropriate for hospital stays not expected to span at least two midnights.
54

Observation Care Discharge (day management)
99217 o This code is to be utilized by the physician to report all services provided to a
patient on discharge from “observation status” if the discharge is on other than the initial date of “observation status”.
oObservation care discharge of a patient from “observation status” includes final examination of the patient, discussion of the hospital stay, instructions for continuing care, and preparation of discharge records.
55

Hospital Observation Services During Global Surgical Period
The global surgical fee includes payment for hospital observation (codes 99217, 99218, 99219, 99220, 99224, 99225, 99226, 99234, 99235, and 99236) services unless the criteria for use of CPT modifiers “-24,” “-25,” or “-57” are met. Contractors must pay for these services in addition to the global
surgical fee only if both of the following requirements are met:o The hospital observation service meets the criteria needed to justify billing it
with CPT modifiers “-24,” “-25,” or “-57” (decision for major surgery); and o The hospital observation service furnished by the surgeon meets all of the
criteria for the hospital observation code billed.
Time Coding Observation Services
Outpatient time coding rules apply to Observation servicesoOnly face to face time by the billing provider will be applied to the total time
for time coding E & M services.
Inpatient services time also incudes nurse and floor time discussing the patient with the nursing staff.
57

Counseling & Coding by Time
When counseling makes up more than 50% of the total time spent with the patient during an encounter, time can be used as the key factor in choosing a level of service. Counseling includes:
oDiagnostic results, impressions, and/or recommended diagnostic studies.oPrognosis.oRisks and benefits of treatment options.o Instructions for treatment and/or follow-up.o Importance of compliance with chosen treatment options.oRisk factor reduction.oPatient and family education.
58

Documenting Time and Content of Counseling Documentation must include:
o Total time spent.o% of time spent in counseling.oWhat was discussed in counseling. No canned or pre-set template statement
when this appears to be cloned. Can be coded by time:
o I spent 25 minutes with the patient, greater than 50% of the time was spent discussing her new diagnosis, conservative treatment options and reassurance.
Cannot be coded by time:oA long discussion was held with the patient as to his underlying diagnosis.
Course of treatment plan from conservative management to lesion excision was discussed with the patient.
59

Time Coding Observation
Code History Exam MDM Nature of Presenting Problem Time
99234 Detailed or Comprehensive Detailed or Comprehensive
SF or Low MDM Low Severity 40 Minutes
99235 Comprehensive Comprehensive Moderate MDM Moderate Severity 50 Minutes
99236 Comprehensive Comprehensive High MDM High Severity 55 Minutes
99218 Detailed or Comprehensive Detailed or Comprehensive
Sf or Low MDM Low Severity 30 Minutes
99219 Comprehensive Comprehensive Moderate MDM Moderate Severity 50 Minutes
99220 Comprehensive Comprehensive High MDM High Severity 70 Minutes
99224 Detailed or Comprehensive Detailed or Comprehensive
SF or Low MDM Stable or recovering 15 minutes
99245 Expanded Problem Focused Expanded Problem Focused
Moderate MDM Responding to therapy or has developed a minor complication
25 Minutes
99246 Detailed Detailed High MDM Unstable or significant complications
35 Minutes
60

Consultation Guidelines
A type of service provided by a physician whose opinion or advice regarding a specific problem is requested by another physician or appropriate source. A physician consultant can initiate diagnostic and/or therapeutic
services. Request and need for consultation must be documented in the
patient’s medical record.o The name of the requesting provider must be in the consultants note
The consultant physician’s opinion must be communicated in writing to the requesting physician.
61

Coding Consultations for Medicare and other payers that do not reimburse Consultation Codes
Place of Service Category Codes
Office Consultations New Patient Codes 99201-99205
Established Patient Codes if seen in the same specialty group within the last 3 years
99211-99215
Inpatient Consultations Initial Inpatient Codes 99221-99223
Observation (Consulting) New Patient Codes 99201-99205
Established Patient Codes if seen in the same specialty group within the last 3 years
99211-99215
Emergency Room Consults Patient is admitted 99221-99223
Patient is NOT admitted 99281-99285

Pre-op Consultation Pre-Op Clearance Consultations
Medical Necessity: There must be a reason for the patient to be sent to you for consultation (beyond the reason for surgery)o Chronic/Co-Existing Conditions
– Be sure to include HPI about the Chronic Conditions– Be sure to document the Chronic Conditions in the Assessment– Be sure to document the status of the Chronic Conditions– Be sure to document the management of the Chronic Conditions
Request: From the Surgeon
Report: Written report back to the Surgeon. Is the patient cleared for surgery?
Note Example:o “Patient being seen for Pre-Op Clearance Consultation requested by Dr. Surgeon. The patients risk
factors include, Hypertension and Diabetes.”63

Emergency Department Services3 of the 3 criteria (Hx, Exam, MDM) must be met for that level
3 of 3 History Exam MDM Presenting Problem
99281
Problem FocusedHPI: 1-3
ROS: nonePFSH: none
Problem Focused95: 1 BA/OS
Straight ForwardDx/Tx options: min 1
Amt/Complex data: min 1Risk: minimal 1
Self limited or minor
99282
Expanded Problem FocusedHPI: 1-3ROS: 1
PFSH: none
Expanded Problem Focused2-5 OS or BA limited
Low ComplexityDx/Tx options: limited 2
Amt/Complex data: limited 2Risk: low 2
Low to moderate severity
99283
Expanded Problem FocusedHPI: 1-3ROS: 1
PFSH: none
Expanded Problem Focused2-5 OS or BA limited
Moderate ComplexityDx/Tx options: Multiple 3
Amt/Complex data: Multiple 3Risk: Moderate 3
Moderate severity
99284
DetailedHPI: 4+
ROS: 2-9PFSH: 1
Detailed6-7 OS or BA extended
Moderate ComplexityDx/Tx options: Multiple 3
Amt/Complex data: Multiple 3Risk: Moderate 3
High severity with an urgent evaluation by
the provider
99285
ComprehensiveHPI: 4+
ROS: 10+PFSH: 2
Comprehensive>8 organ systems
High ComplexityDx/Tx options: Extensive 4
Amt/Complex data: Extensive 4Risk: High 4
High severity and pose an immediate significant threat to life or physiologic
function
64

Nature of the Presenting Problem(s)99281- Self-limited or minor problem
o Patient didn’t need to present to the EDo Symptoms resolving or resolved by the time they are seen in the EDo Discharged
99282- Low to moderate severity
o Acute uncomplicated injuryo OTC medicationo Discharged
99283- Moderate severity
o Acute condition that requires prescription managemento Head Injury, no loss of consciousnesso Mild exacerbation of a chronic conditiono Potential drug overdose, patient alert, anxious, given IV fluids then
dischargedo Discharged
99284- High severity, urgent evaluation, does not pose immediate threat to
life or physiologic function, admit to observation, telemetry or inpatient status (i.e. pancreatitis, kidney stones, pyelonephritis, abdominal pain, pneumonia, fracture requiring surgery)
o Chest pain unknown etiology requiring extensive monitoring, admit to observation
o Abdominal pain, multiple tests, IV pain medicine, admit to inpatient status.
o Drug overdose, conscious but neuro deficitso MVA, multiple lacerations, brief loss of consciousness, admit to
observation
99285- High severity, pose an immediate significant threat to life or
physiologic function and is admitted as inpatient status.o Acute MIo Acute kidney injuryo Acute appendicitis requiring surgeryo Drug overdose, unconsciouso MVA, multiple & severe trauma, admito Chest pain, multiple tests ordered, patient admitted for pulmonary
embolismo Active upper gastrointestinal bleeding, inpatient admito Admitted to ICU, documentation does not support critical care
65

Nursing Facility Services

Nursing Facility Services
Identifying the correct Place of Service is needed to correctly code Nursing Facility Services.o Inpatient: 21o Skilled Nursing Facility: 31o Nursing Facility: 32o Custodial Care Facility: 33
Does your Hospital utilize “Swing Beds”?o What POS is a Swing Bed?
A Swing Bed can represent an inpatient service or a SNF service. It depends on how the hospital is billing Medicare for its services.
Always check with the Hospital to align your professional services.

Initial Nursing Facility The initial comprehensive assessment visit performed by the physician includes:
o a thorough assessment, o develops a plan of care and o writes or verifies admitting orders for the nursing facility resident.
For Survey and Certification requirements, a visit must occur no later than 30 days after admission. Only a physician may report these codes for an initial visit performed in a SNF Split/Shared visits may not be reported in the SNF/NF setting
68
HISTORY EXAM MEDICAL DECISION MAKING
99304 Detailed or Comprehensive Problem Focused SF or Low MDM
99305 Comprehensive Comprehensive Moderate MDM
99306 Comprehensive Comprehensive High MDM
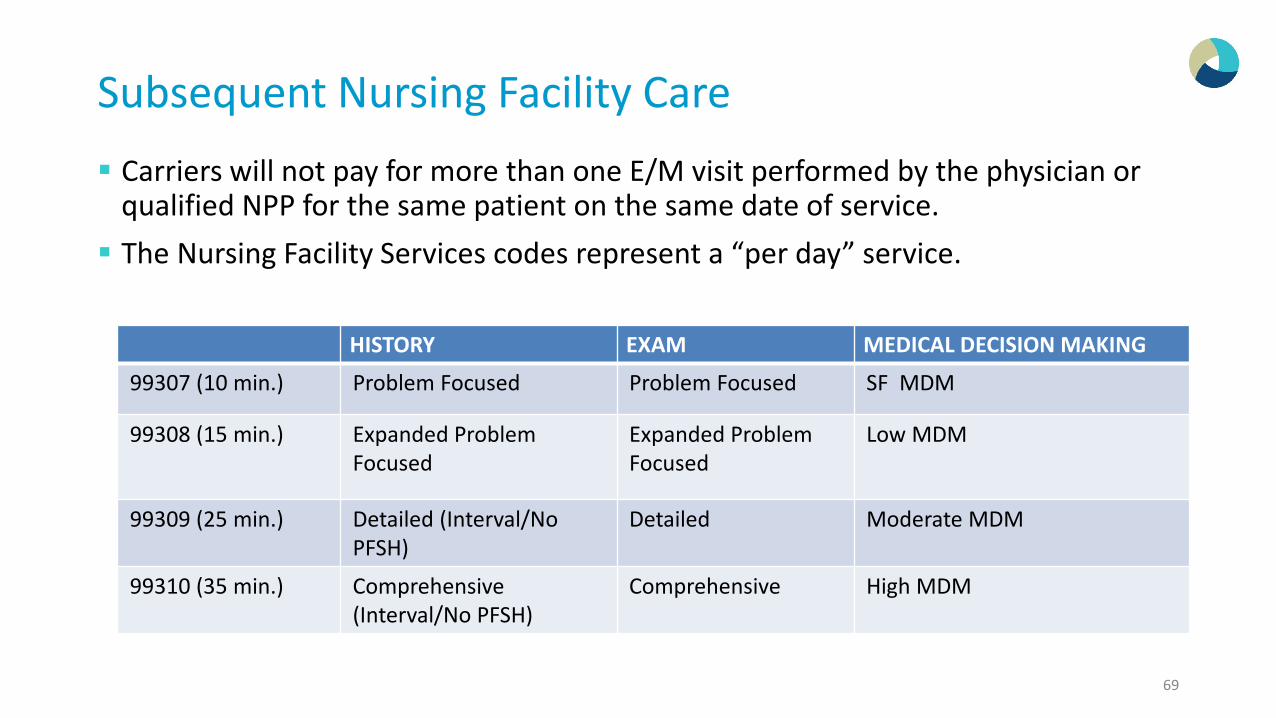
Subsequent Nursing Facility Care Carriers will not pay for more than one E/M visit performed by the physician or
qualified NPP for the same patient on the same date of service. The Nursing Facility Services codes represent a “per day” service.
69
HISTORY EXAM MEDICAL DECISION MAKING
99307 (10 min.) Problem Focused Problem Focused SF MDM
99308 (15 min.) Expanded Problem Focused
Expanded Problem Focused
Low MDM
99309 (25 min.) Detailed (Interval/No PFSH)
Detailed Moderate MDM
99310 (35 min.) Comprehensive (Interval/No PFSH)
Comprehensive High MDM

Visits to Comply With Federal Regulations
Payment is made under the physician fee schedule by Medicare Part B for federally mandated visits.
Following the initial visit by the physician, payment shall be made for federally mandated visits that monitor and evaluate residents at least once every 30 days for the first 90 days after admission and at least once every 60 days thereafter.
The federally mandated E/M visit may serve also as a medically necessary E/M visit if the situation arises (i.e., the patient has health problems that need attention on the day the scheduled mandated physician E/M visit occurs).
99307-99310 are used to report federally mandated physician visits and other medically necessary visits.
70

Nursing Facility Discharge
Nursing facility discharge day management codes are to be used to report the total duration of time spent by a physician for the final nursing facility discharge of a patient.
The codes include, as appropriate, final examination of the patient, discussion of the nursing facility stay, instructions for continuing care to all relevant caregivers and preparation of discharge records, prescriptions and referrals.
If the patient is admitted to the Hospital, a Nursing Facility Discharge may NOT be reported on the same day.
Face to Face Service Required
71
99315 99316Time 30 minutes or less More than 30 minutes (time must be documented)

Annual Nursing Facility Assessment
Do not report 99318 on the same date of service as nursing facility service codes 99304-99316
The Annual Assessment is payed once per year and may be used as a Mandated visit.
This Annual Assessment may be performed by an MD or an NPP, but may not be billed as a shared service or incident to service
72
99318
History Detailed Interval (no PFSH)
Exam Comprehensive
Medical Decision Making Low to Moderate

Home Services
In the 2019 POFS Proposed Rule: CMS has proposed to eliminate the requirement to justify the medical necessity of a home visit in lieu of an office visit.

NPP Services“Split/Shared”

75
NPP Billing Guidelines
Key Factors to consider when working with Non Physician Practitioners (NPP’s)What Place of Service are they working?
oOffice (POS 11)oOutpatient Clinic (POS 19, 22 & 23) o In-Patient (POS 21)

POS 19/21/22/23: Split / Shared Services
A split/shared visit is a medically necessary encounter with a patient, where the physician and a qualified NPP each personally perform a substantive portion of an E/M visit face-to-face with the same patient on the same date of service.
Note: It is NOT sufficient for MD to note “seen and agree” or simply countersign; he/she must specifically document what he/she has personally done. o A portion of the key components must be documented by both. Both notes may be
combined together to establish the level of service.
Documentation showing NPP performs a portion of the E/M encounter and physician performs a part of the encounter with signatures by both.
76

Medicare Info
Medicare allows only certain types of services to be shared between a physician and NPP.
When reviewing documentation, the medical review clinician (RAC auditors) are not always able to differentiate who the rendering provider is, as well as, if the incident-to or shared/split service requirements have been met.
77
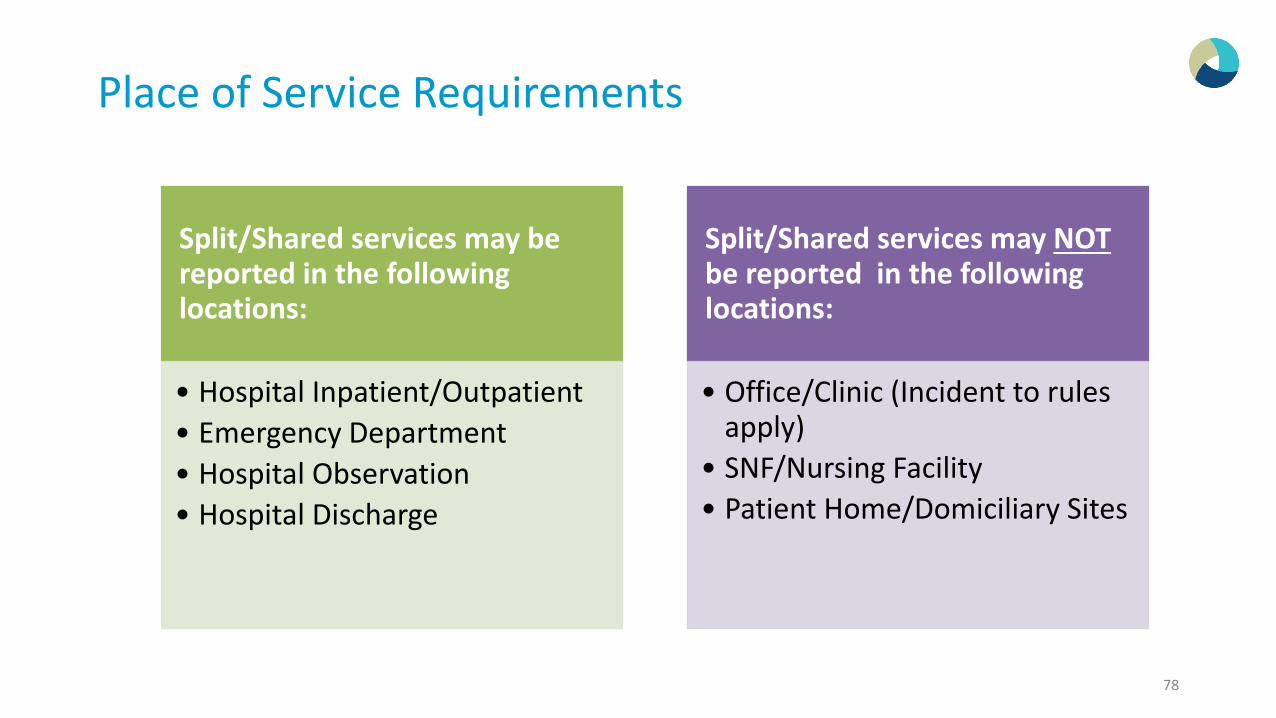
Place of Service Requirements
78
Split/Shared services may be reported in the following locations:
• Hospital Inpatient/Outpatient • Emergency Department • Hospital Observation • Hospital Discharge
Split/Shared services may NOTbe reported in the following locations:
• Office/Clinic (Incident to rules apply)
• SNF/Nursing Facility• Patient Home/Domiciliary Sites

Rules!
The service provided must be reasonable and medically necessary, must be within the NPP's scope of practice as defined in state law where he/she practices; and performed in collaboration with a physician.
Physician & NPP are from the same group practice OR employed by the same employer. o They cannot be employed by the hospital
79

What must be documented by the Physician and NPP?
The documentation by the physician must specifically say what he/she has personally done. oA portion of the key components must be documented by both. Both notes
may be combined together to establish the level of service.
Documentation showing NPP performs a portion of the E/M encounter and physician performs a part of the encounter with signature by both. Collaboration must be documented by either the NPP or MD
o “I have seen the patient with the NP/PA today”o “Refer to the NP/PA note who also saw the patient today”o “I have seen the patient with Dr. XXX today”
80

What is “substantive portion”?
Substantive portion of the EM service must be documented by both the NPP and MDoUsually not a problem for the NPP as they are usually documenting the
majority of the visit.oPhysician “substantive portion” requires
– A physician face to face encounter with documentation to support– The physician must document at least one element of the key components
oNote: The exam will satisfy the face to face requirement (include the exam findings) for all services as well as the following statements:
– “I have examined the patient today”– “I have discussed with the patient today…”– “Patient seen today with COPD exacerbation, continue xxx meds”
81

Services That Cannot be Reported as Split / Shared:
Consultation services (no longer reimbursed by Medicare) Critical Care services Procedures
*The provider that performs these services must be the provider that bills the services
82

CMS Q&A On Split / Shared Services
83
Q: If split/shared visit (ED) and unable to determine if provider performed any part (face-to-face) how will the service be denied (not rendered, insufficient documentation, or cut back to 85%?)
• A: Denied as “Payment adjusted as not furnished directly to the patient and/or not documented.”

CMS Q&A On Split / Shared Services
84
Q: If split/shared visit with NPP signature & MD signature & different handwriting and the medical reviewer can distinguish who performed what part of the E/M encounter, will the full (combined) E/M visit be allowed, or only the portion that the MD performed & documented?
• A: The full (combined) E/M visit will be allowed.

Teaching Physician Documentation
The teaching physician must personally document at least the following:
o That they performed the service or were physically present during the key or critical portions of the service when performed by the resident
o The participation of the teaching physician in the management of the patient
*When assigning the codes to services billed by teaching physicians, the reviewer will combine the documentation of both the resident and the teaching physician.
85

Teaching Physician Presence
Documentation by the resident of the presence and participation of the teaching physician (TP) is not sufficient to establish the presence and participation of the teaching physician 2019 MPFS Proposed Rule:
o For E/M visits furnished by teaching physicians, we also propose to eliminate potentially duplicative requirements for notations in medical records that may have previously been included in the medical records by residents or other members of the medical team.
86

Minimally Acceptable Documentation
87
Admitting Note: “I performed a H & P exam of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.
Follow-up Note: “Hospital Day #3. I saw and evaluated the patient. I agree with the findings and the plan of care as documented by the resident’s note”.

Minimally Acceptable Documentation
88
Initial or Follow-up visit: “I was present with the
resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the
resident’s note”.
Follow-up visit: “I saw the patient with the resident
and agree with the resident’s findings and
plan”.
Initial Visit: “I saw and evaluated the patient. I reviewed the resident’s
note and agree, except that picture is more consistent
with pericarditis than myocardial ischemia. Will
begin NSAID’s”.

Unacceptable Documentation
“Agree with above”, followed by countersignature or identity
“Rounded, Reviewed, Agree”, followed by countersignature or identity
“Discussed with resident, Agree” followed by countersignature or identity
“Seen and agree”, followed by countersignature or identity
“Patient seen and evaluated”, followed by countersignature or identity
A legible countersignature or identity alone
89

Late Night Admits
If a patient is admitted, the resident may perform the H & P The teaching physician has 24 hours to review information obtained with the
resident and see the patient ( in that order)
When the resident sees the patient and the teaching physician sees the patient later on the following day (after midnight or next day)o Attending (TP) has conversation with the Resident as he admits the patient (via phone)o Attending (TP) see the patient the next dayo Attending (TP) documents the following:
– “I discussed the patient with the resident and agree with his note from 10/24/17. I saw and examined the patient on 10/25/17 and agree with the resident (or insert resident’s name) assessment and plan”
– Also document any additional clinical information about the patients conditions from resident visit to your visit the next day

Late Night Admits: Medicare Rules The teaching physician must document that he/she personally saw the patient and participated in
the management of the patient. The teaching physician may reference the resident's note in lieu of re-documenting the history of present illness, exam, medical decision-making, review of systems and/or past family/social history provided that the patient's condition has not changed, and the teaching physician agrees with the resident's note.
The teaching physician's note must reflect changes in the patient's condition and clinical course that require that the resident's note be amended with further information to address the patient’s condition and course at the time the patient is seen personally by the teaching physician.
The teaching physician’s bill must reflect the date of service he/she saw the patient and his/her personal work of obtaining a history, performing a physical, and participating in medical decision-making regardless of whether the combination of the teaching physician’s and resident’s documentation satisfies criteria for a higher level of service. For payment, the composite of the teaching physician’s entry and the resident’s entry together must support the medical necessity of the billed service and the level of the service billed by the teaching physician.

Implications for Surgical Care
92
Minor Surgery
• For procedures that take only a few minutes (5 minutes or less) and involve little decision making once the need for the operation is determined, the TP must be present for the entire procedure in order to bill for the procedure. (no change)
Endoscopy Procedures
• In order to bill, TP must be present during the entire viewing. Entire viewing starts at the time of insertion of the endoscope and ends at the time of removal of the endoscope. Viewing through a monitor in another room does not meet the TP presence requirements. (clarifies that rule excludes endoscopic surgery that follows the surgery section rules)

Diagnostic Procedures A teaching physician need not be present during diagnostic services
(i.e., radiology)oThe interpretation of diagnostic radiology and other diagnostic
tests are reimbursed if performed by or reviewed with a teaching physician
oMedicare does not pay if the TP just countersigns the resident’s interpretation
oThe TP must indicate that he reviewed the image and the resident’s interpretation and either agrees with or edits the findings.
93

Time-Based Services When billing time based codes the TP must be present during the entire time that is
being billed Time spent by the resident in the absence of the TP should not be included in the total
time billed Types of time based services:
o Individual Medical Psychotherapyo Critical Care Serviceso Hospital Discharge day managemento E/M codes which counseling and/or coordination of care dominates more than 50%
of the encountero Prolonged Serviceso Care Plan Oversight
94

Medical Student Documentation
The Centers for Medicare & Medicaid Services (CMS) is revising the Medicare Claims Processing Manual, Chapter 12, Section 100.1.1, to update policy on Evaluation and Management (E/M) documentation to allow the teaching physician to verify in the medical record any student documentation of components of E/M services, rather than re-documenting the work. Students may document services in the medical record. However, the teaching physician must verify in the medical record all
student documentation or findings, including history, physical exam and/or medical decision making. The teaching physician must personally perform (or re-perform) the
physical exam and medical decision making activities of the E/M service being billed, but may verify any student documentation of them in the medical record, rather than re-documenting this work.
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM10412.pdf
95

Primary Care Exception
“Teaching physicians providing E/M services with a GME program granted a primary care exception may bill Medicare for lower and mid-level E/M services provided by residents.” “Teaching physicians may submit claims for services furnished by
residents in the absence of a teaching physician.”

Primary Care Exception The resident should have completed more than 6 months in an approved residency
program The TP may not direct more than 4 residents at one given time TP must:
– Be immediately available if necessary– Not have other responsibilities at the time the service was provided by the
resident– Have the primary medical responsibility for the patient’s care by the resident– Ensure that the care provided was reasonable and necessary– Review the care provided by the resident during or immediately after each
visit– Document the extent of his/her own participation in the review and direction
of the services furnished to each patient

Primary Care Exception
The following conditions must be met:oServices located in hospital OP department or free standing setting where
time spent by resident is included in Part A payments to the hospitaloServices are provided to patients who use the facility as their continuing
source of healthcareoServices are furnished under the direction of a teaching physician
Residency Programs that qualify include:oFamily Practice, General Internal Medicine, Geriatric Medicine, Pediatrics,
and OBGYN.oUnder special situations some Psychiatric facilities may qualify
Primary Care Exception
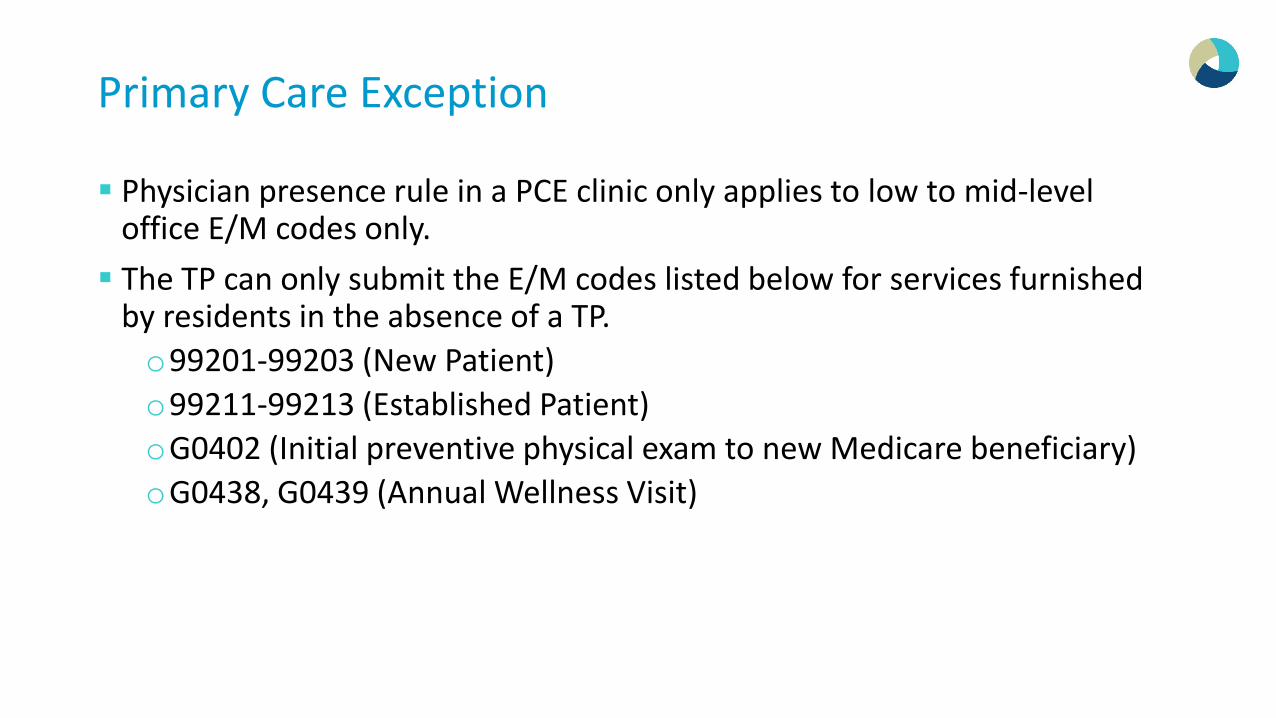
Physician presence rule in a PCE clinic only applies to low to mid-level office E/M codes only. The TP can only submit the E/M codes listed below for services furnished
by residents in the absence of a TP.o99201-99203 (New Patient)o99211-99213 (Established Patient) oG0402 (Initial preventive physical exam to new Medicare beneficiary)oG0438, G0439 (Annual Wellness Visit)

Primary Care Exception TP must review the care provided by the resident during or immediately
after each visit. This must include a review of the patient’s:oMedical historyo Exam findingsoDiagnosis o Treatment plan.
TP must be on-site, provide a real time discussion of findings/plan of care and have discussion with the resident PRIOR to the patient leaving, should changes need to be made in plan of care. TP must document the extent of his/her participation in the review and
direction of the services furnished to each patient.

Primary Care Exception
“While the patient was in clinic I reviewed the patient’s medical history, the resident’s physical examination, and the patient’s diagnosis and treatment plan with the resident and agree with the information documented.” “Immediately following the patient leaving the clinic I reviewed the
patient’s medical history, the resident’s physical examination, and the patient’s diagnosis and treatment plan with the resident and agree with the information documented.”

Physical Presence in the Primary Care Clinic
Code appropriately for the service that is rendered and documented. It is not appropriate to bill a 99213 when a 99214 level of service is
performed. o99213 (Low complexity Medical Decision Making) o99214 (Moderate complexity Medical Decision Making)
TP physical presence is required for 99214 and above.o TP attestation must show physical presence (saw and/or examined the
patient). o If TP physical presence is not documented, the service is unbillable.

Medi-Cal Patients
Medi-Cal does not follow the Medicare Primary Care Exception Rule The teaching physician must see the patient for all levels of service for
all Medi-Cal patients
Reference: Medi-Cal Online Manual, Section: Evaluation and Management (E&M), Teaching Physician Billing Requirements for Evaluation and Management Services, pages 22 and 23.
103

Stay Up-to-date on Upcoming Webinars
104
www.linkedin.com/company/codingaid www.facebook.com/CodingAIDLongBeach
www.managedresourcesinc.com/news/events

Thank You!
Coding Support ◦ Coding Audit & Compliance Clinical Documentation Improvement ◦ Recruitment
Education & Training Clinical Appeals ◦ Charge Audit 105