
PRESENTED BY-DR. POOJA MODERATOR – DR.DARA SINGH CIRCLE SYSTEM AND LOW FLOW ANESTHESIA.
48
PRESENTED BY-DR. POOJA MODERATOR – DR.DARA SINGH CIRCLE SYSTEM AND LOW FLOW ANESTHESIA
-
Upload
annabella-charles -
Category
Documents
-
view
213 -
download
0
Transcript of PRESENTED BY-DR. POOJA MODERATOR – DR.DARA SINGH CIRCLE SYSTEM AND LOW FLOW ANESTHESIA.

PRESENTED BY-DR. POOJAMODERATOR – DR.DARA SINGH
CIRCLE SYSTEM AND LOW FLOW ANESTHESIA

CIRCLE SYSTEM DEFINITION AND COMPONENTS
Named so because gases flow in a circular pathway through separate inspiratory and expiratory channels
Its primary components are-1. Fresh gas inlet2. Inspiratory and expiratory unidirectional valves3. Inspiratory and expiratory corrugated tubes4. Y-piece connector5. APL valve6. Reservoir bag7. Canister containing CO2 absorbent

Other components included in circle system are-
Respiratory gas monitor sensorAirway pressure monitor sensorRespirometerPEEP valveFiltersHeated humidifierBag ventilator selector switch

FRESH GAS INLET
connected to common gas outlet on anesthesia machine by flexible tubing
ASTM standards require that inlet port has an inside diameter of atleast 4.0mm and fresh gas delivery tube has an inside diameter of atleast 6.4mm
On newer machines, direct connection between machine outlet and breathing system so user does not see a fresh gas hose.

UNIDIRECTIONAL VALVES(flutter, one-way, check, directional, dome, flap, nonreturn, inspiratory, and expiratory)
direction of intended gas flow permanently marked on the valve housing or near its associated port with either a directional arrow or with the marking inspiration or expiration so that it is visible to the user

Valves ensure that gas flows in one direction only
Gases enter at the bottom raising the disc from its seat.gas then passes under dome and through breathing system
Reversing gas flow causes disc to contact seat preventing retrograde flow One or both unidirectional valves may become incompetent
A unidirectional valve may jam, obstructing gas flow

Each tube connects to a port on the absorber at one end and the Y-piece at the other
The dead space extends from Y-piece to patient
Length of tubes does not affect the dead space
Longer tubes allow the anesthesia machine to be located farther from the patient's head
BREATHING TUBES

The inspiratory port has a 22-mm male connector downstream of the inspiratory unidirectional valve through which gases pass toward the patient during inspiration
The expiratory port has a 22-mm male connector upstream of the unidirectional valve through which gases pass during exhalation

Y-PIECE
Three-way tubular connector with two 22-mm male ports for connection to the breathing tubes and a 15-mm female patient connector for a tracheal tube or supraglottic airway device
Patient connection port usually has a coaxial 22-mm male fitting to allow direct connection between Y-piece and face mask


APL VALVE
During spontaneous breathing, the valve is left fully open and gas flows through the valve during exhalation
When manually assisted or controlled ventilation is used, the APL valve should be closed enough that the desired inspiratory pressure can be achieved
When this pressure is reached, the valve opens and excess gas is vented to the scavenging system during inspiration
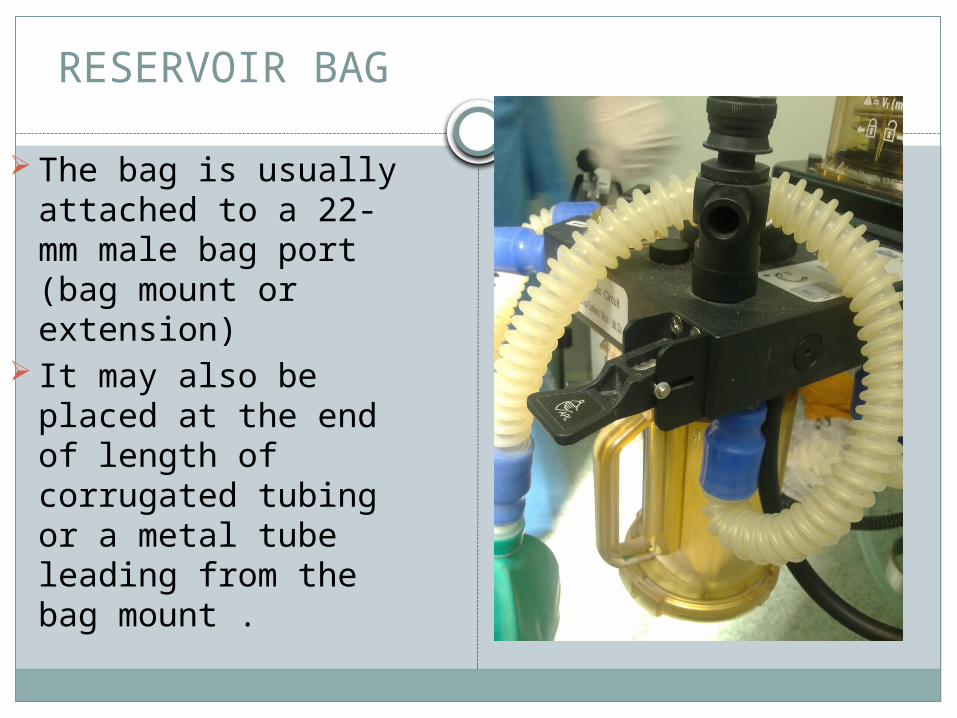
RESERVOIR BAG
The bag is usually attached to a 22-mm male bag port (bag mount or extension)
It may also be placed at the end of length of corrugated tubing or a metal tube leading from the bag mount .

CANISTERS( CO2–ABSORBENT CONTAINERS, CHAMBERS, UNITS, CARTRIDGES)
Transparent side wallScreen at bottom which holds absorbentThere may be 2 canisters in series or 1
single canisterSIZESmall canisters are used more frequentlyFrequent changes help to provide fresh
absorbent Internal volume of the breathing system is
reduced

CANISTER

First absorption occurs at the inlet and along canister sides. As this absorpion is exhausted, CO2 absorption occurs further downstream
No difference whether gases enter at the top or bottom


Spaces at the top and bottom of absorber for incoming gases to disperse before passing through the absorbent or for outgoing gases to collect before passing on through the circle
Canister is attached to housing that incorporates valves that will close the entrance and exit from the canister when the canister is removed.
Allows breathing system continuity to be maintained when the canister is changed.

COMPOSITION OF ABSORBENTS
HIGH ALKALI ABSORBENTS Soda lime – KoH -1 % ,NaOH- 4%, H2O-15% Ca(OH)2-80%
and silica Keiselguhr is used as hardening agent When desiccated, form CO with anesthetics Sevoflurane - Compound A is formed. LOW ALKALI ABSORBENTS Barylime- barium hydroxide-20%,Ca(OH)2-80%ALKALI FREE ABSORBENTS Calcium hydroxide ,CaCl2 with other agents like CaSO4
and polyvinylpyrolidine , inc porosity and hardness No CO , compound A formation Indicator changes color on drying CO2 absorption capacity is less

CO2 absorption employs general principle of base neutralizing acid
Acid is carbonic acid formed by reaction of CO2 with water.
CO2+H2O=H2CO3H2CO3+2NaOH=NaCO3+2H2O+HeatNa2CO3+Ca(OH)2=CaCO3+2NaOH

An indicator is added to absorbent to signify whether its ability to absorb CO2 has exhausted
Its an acid or base whose colour depends on pH


SIZE AND SHAPE Pellets or small granules provide greater surface area Size is measured by mesh number-no of openings per
linear inch in a sieve through which granular particles can pass
4-mesh strainer has four openings per square inch , 8 mesh has eight openings per square inch
Mostly 4-8 mesh size is usedHARDNESS Some granules fragment easily, producing dust Excessive powder produces channeling, resistance to
flow small amounts of a hardening agent are added Coating of granules is done with film

PRODUCTS OF RXN B/W ABSORBENT AND ANESTHETIC AGENT
HALOALKENE FORMATIONCompound A – vinyl ether Sevoflurane decomposes to produce compound A More so when prolonged anesthesia Dry absorbent lower fresh gas flows Higher temperature Higher concentration of sevoflurane Absorbets containing KOH or NaOH

Carbon Monoxide-Highest levels are seen with desflurane
followed by enflurane and isofluraneWhen absorbent is dryHigh temperatureAbsorbents with KOH or NaOHSmall patient sizeHigh fresh gas flow

PREVENTION
- All fresh gas flow should be turned off after each case.
- Vaporizers should be turned off .anesthetic system flushed with fresh gas
- Absorbent should be changed regularly - Practice of supplying O2 through circle
system should be discouraged when not receiving GA
- Temperature should be monitored-Integrity of absorbent packaging should be
tested

Excessive heat and fires-more so with dessicated Baralyme and sevoflurane
Sodalime results in less elevated temperature

WHEN TO CHANGE
Appearance of CO2 in inspired gasIndicator colour change-a phenomenon of
regeneration is noticed. Exhausted colour show reversal on rest but absorption capacity will be low and colour will reappear after brief exposure to CO2
Heat in canister

RESPIRATORY GAS MONITOR SENSOR
Oxygen analyzer-ASA standards require use of O2 analyzer on breathing circuits with alarms
-to detect hypoxic mixture inspiration
-to detect leaks and disconnections-to detect hypoventilationPARAMAGNETIC and ELECTROCHEMICAL O2
Analyzers-when a gas containing O2 is passed through magnetic field,gas will expand and contract causing a pressure wave proportional to O2 partial pressure

In electrochemical , sensor contains a cathode and anode surrounded by electrolyte. Gel is held in place by membrane permeable to O2
O2 diffuses through membrane to cathode where it is reduced causing current to flow . The rate of O2 entering membrane is proportional to partial pressure of O2
Display is usually in percent O2


CO2 monitors –diverting and non divertingDiverting type uses a pump to aspirate gas from
sampling site to the sensor through a sampling tubeSampling flow rate less than 150ml/min should not be
usedDuring low flow techniques flow should be returned to
circuitBased on infrared technology-gases with 2 or more
dissimilar atoms have specific absorpion spectra. Since amount of infrared light absorbed is proportional to concentration of absorbing molecules its conc. Is determined by comparing with known standard



ADVANTAGES AND DISADVANTAGES
Low flow can be used with its advantagesUseful for malignant hyperthermiaDISADVANTAGESChances of disconnections and leaksBulkyDifficult to cleanToxic product formation

CIRCLE SYSTEM TEST
To check the integrity of circle system spanning from common gas outlet to Y-piece
Leak test and Flow test-Closing pop-off valve, occluding y-piece, pressurizing the
circuit to 30cm of H2O with oxygen flush valve.Value on pressure gauge will remain fixed for atleast 10sec.
Flow test check integrity of unidirectional valve .By removing Y-piece and breathing through 2 tubes individually. The valves should move appropriately.operator should be able to inhale not exhale through inspiratory limb and vice-versa.
Alternately by using breathing bag and ventilator

LOW FLOW ANESTHESIA
Inhalation technique in which circle system with absorbent is used with a fresh gas inflow of less than patient,s alveolar minute volume
- less the 1 or 1.5 l/min- 3L or less-0.5-2l/min-0.5-1l/minInhalation technique via a rebreathing system in
which rebreathing fraction amounts to atleast 50% i.e.atleast 50% of exhaled gas volume is led back to patient after CO2 absorption.

Closed system anesthesia is a low flow anesthesia in which fresh gas flow equals uptake of anesthetic gases and oxygen by the patient ,system and gas sampling.
No gas is vented through APL valve.

FLOW TECHNIQUE NOMENCLATURE
High flow- >1l/min Low flow anesthesia-1l/minMinimal flow anesthesia-500ml/minBasal metabolic-250ml/minUptake-140-180ml/min

Based on fact that O2 consumption is equal to basal metabolic consumption under anesthesia
Nitrous oxide consumption depends on alveolar-arterial pressure gradient. Requirement decreases when peripheral tissues are saturated
Newer inhalation agents are minimally metabolized. They are mainly exhaled into the breathing system

Requirements can be calculated by-VO2=10 x Kg3/4
N2O=o.7x0.47x%N2Ox QInhalation agents=G(b/G)x C(A-V)xQ

EQUIPMENT
Standard anesthesia machine with flowmeters providing low flow.
Vaporizers –in-circle vaporizers,calibrated vaporizers or liquid injection
Monitors-continuous measurement of oxygen mandatory.

TECHNIQUE
Induction-Intavenous induction-By injection of liquid anesthetic in expiratory
limb but takes prolonged time to establish concentration
-By using high flow initially to allow denitrogenation, establish anesthetic agent concentration. After gas exchange low fresh gas flow are used.

MAINTENANCE
Nitrous oxide, oxygen flows and vaporizer settings should be adjusted to maintain a satisfactory oxygen concentration and desired level of anesthesia.
Constant circuit volume is achieved by-constant reservoir bag size(increasing FGF if bag size decreases, decreasing FGF if bag size increases)
Ventilator with ascending bellows-FGF is adjusted so that bellows is below the top of its housing at the end of exhalation
Ventilator with descending bellows-bellows just reaches the bottom of its housing at the end of exhalation

High flows should be used for 1-2min atleast once an hour to eliminate gases such as nitrogen and carbon monoxide that have accumulated in system.
EMERGENCE-anesthetic administration is stopped toward end of operation and circuit is maintained with enough oxygen flow to maintain end tidal volume of the reservoir bag(coasting)

CONTRAINDICATIONS
Malignant hyperthermiaSmoke or gas intoxicationUncompensated diabetesAcute alcohol intoxicationChronic alcoholismGas volume deficiencyInsufficient depth of anesthesiaInsufficient dinitrogenationSodalime exhausionFailure of O2 monitor

ADVANTAGES
Economy Reduced operating room pollutionReduced environmental pollutionEstimation of anesthetic agent uptake and
oxygen consumptionBuffered changes in inspired concentrationHeat and humidity conservationLess danger of barotrauma

DISADVANTAGES
More attention requiredInability to alter inspired concentration
quicklyDanger of hypercarbiaAccumulation of undesirable gases in the
system- CO, compound A, acetone, methane,hydrogen, argon,nitrogen acrylic monomer when joint prosthesis is cemented
Faster absorbent exhaustionUncertainty about inspired concentration

THANK YOU


















