Presentazione di PowerPoint · Hepatorenal syndrome P. Angeli, Dept. of Medicine, Unit of Internal...
58
Hepatorenal syndrome P. Angeli, Dept. of Medicine, Unit of Internal Medicine and Hepatology (UIMH), University of Padova (Italy) [email protected] UIMH 37 th Vicenza Course on AKI & CRRT Vicenza (Italy) May 28-30 th , 2019
Transcript of Presentazione di PowerPoint · Hepatorenal syndrome P. Angeli, Dept. of Medicine, Unit of Internal...

Hepatorenal syndrome
P. Angeli, Dept. of Medicine, Unit of Internal Medicine and Hepatology (UIMH),
University of Padova (Italy)[email protected]
UIMH
37th Vicenza Course on AKI & CRRTVicenza (Italy) May 28-30th, 2019
Disclosures
•2014- 2018: Sequana Medical AG Advisory Board
•2016-2018: Biovie Advisory Board and patent application
•2016: Gilead (Italy): Advisory Board and grant
•2014-2018: Bhering: speaker invitation and travel grant
•2016: Kedrion speaker invitation
•2018: Ferring: Advisory Board
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

0
20
40
60
80
100
AKI AKI+CKD CKD
N.S. Warner et al. J. Investig. Med. 2011 ; 59 : 1244-1251.
Prevalence of AKI and CKD in patients with cirrhosis admitted to the hospital
%
70 %
17 %13 %
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Definition and staging of Acute Kidney Injury (AKI)
KDIGO AKI Work Group Kidney Int. Suppl. 2012 ; 2 : 1-138
KDIGO criteria = an abrupt (within 48 hours) reduction in kidney function currently definedas an absolute increase in serum creatinine of more than or equal to 0.3 mg/dl ( 26.4μmol/l), or a percentage increase in serum creatinine of more or equal to 50 % (1.5-fold frombaseline) in less than 7 days.
Stage Serum creatinine criteria
1°Increase in serum creatinine of more than or equal to 0.3 mg/dl ( 26.4μmol/l) or a percentage increase in serum creatinine of more or equal to 50 %(< 2 fold from baseline).
2°Increase in serum creatinine to more than 200% to 300% (> 2- to 3-fold) from baseline
3°
Increase in serum creatinine to more than 300 % (> 3-fold) from baseline or serum creatinine of more or equal to 4.0 mg/dl ( 354 μmol/l) with an acute increase of at least 0.5 mg/dl (44 μmol/l) or need for renal replacementtherapy
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Criteria Sensibility95 % CI
Specificity95% CI
PPV95% CI
NPV95% CI
LR+95% CI
LR-95% CI
Conventional criteria 0.5152(0.33 - 0.69)
0.9450(0.90 - 0.97)
0.6071(0.40 - 0.78)
0.9220(0.87 - 0.95)
9.3664(4.8 - 18.17)
0.5131(0.36 - 0.73)
KDIGO criteria 0.6667(0.48 - 0.82)
0.8100(0.74 - 0.86)
0.3667(0.24 - 0.50)
0.9364(0.88 - 0.96)
3.5088(2.41 - 5.10)
0.4115( 0.25 - 0.66)
KDIGO withProgression
0.5455(0.36 - 0.71)
0.9450(0.90 - 0.97)
0.6207(0.42 - 0.79)
0.9265(0.88 - 0.95)
9.9174(5.15 - 19.06)
0.4810(0.33 - 0.70)
Accuracy of conventional criterion vs KDIGO criteria in the prediction of in-hospital mortality in a series of 233 patients with cirrhosis and ascites
S. Piano et al. J. Hepatol. 2013 ; 59 : 482-489
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

P <0.001
P <0.0001
P <0.0001
P=N.S.P <0.025
P <0.01
Initial AKI stage≠ and in-hospital mortality
S. Piano et al. J. Hepatol. 2013 ; 59 : 482-489
%
0
20
40
60
80
100
No AKI AKI stage 1 AKI stage 2 AKI stage 3
# = AKI stage at the first fulfillement of KDIGO criteria
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Survival of in hospitalized patients with cirrhosis according to Acute Kidney Injury (AKI).
C. Fagundes et al. J. Hepatol. 2013 ; 59 : 474–481# = with peak creatinine level <1.5 mg/dl, * = with peak creatinine level 1.5 mg/dl
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
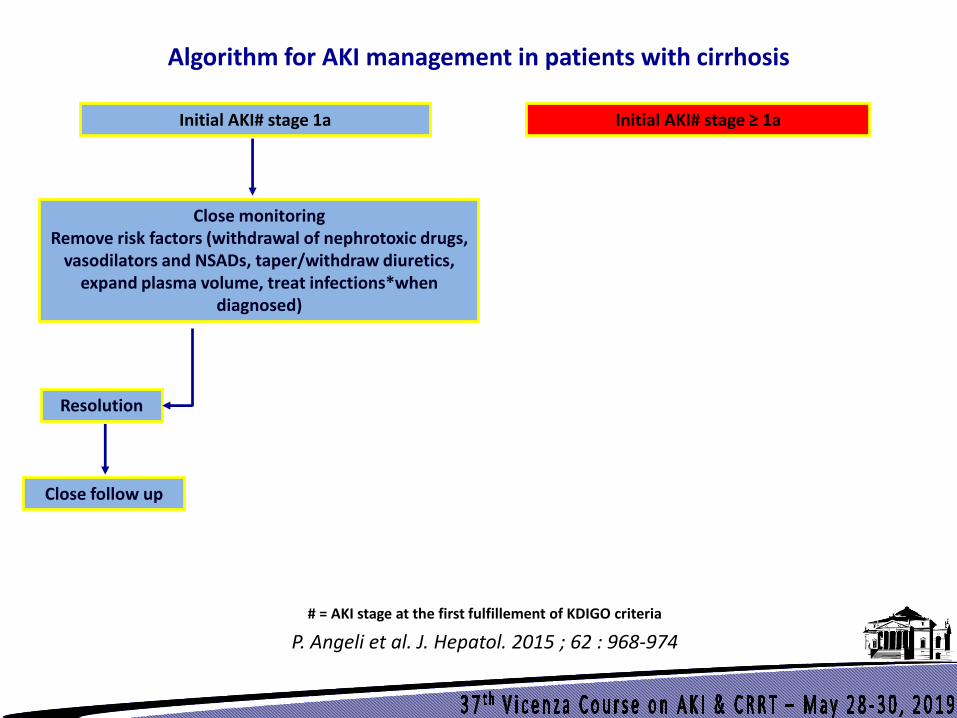
Algorithm for AKI management in patients with cirrhosis
Initial AKI# stage ≥ 1aInitial AKI# stage 1a
# = AKI stage at the first fulfillement of KDIGO criteria
Close monitoringRemove risk factors (withdrawal of nephrotoxic drugs,
vasodilators and NSADs, taper/withdraw diuretics, expand plasma volume, treat infections*when
diagnosed)
Resolution
Close follow up
P. Angeli et al. J. Hepatol. 2015 ; 62 : 968-974
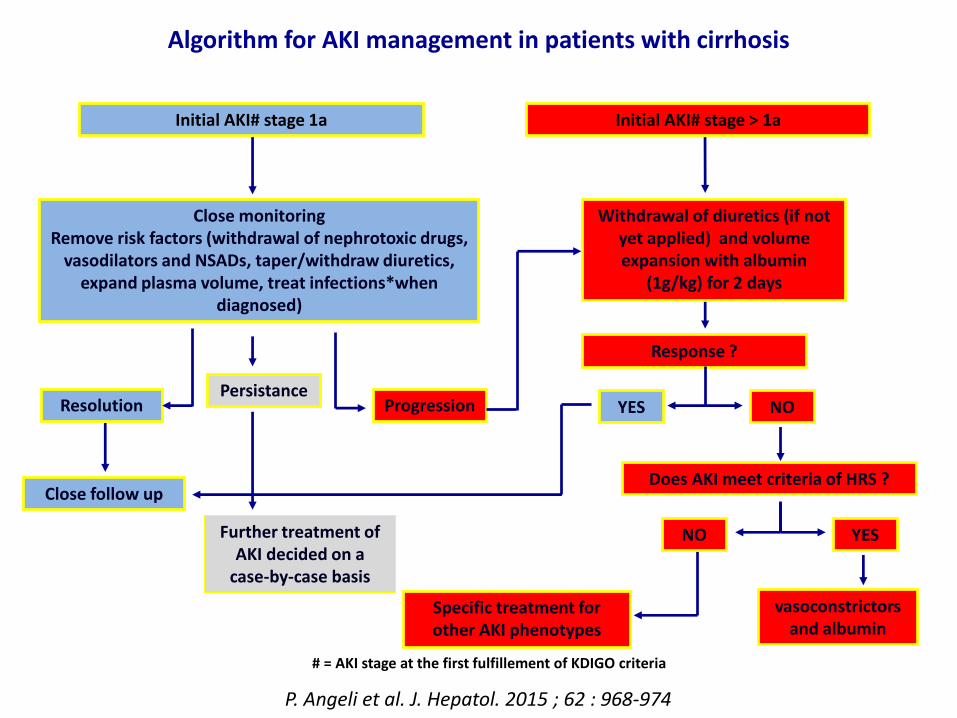
Algorithm for AKI management in patients with cirrhosis
Initial AKI# stage > 1aInitial AKI# stage 1a
Close monitoringRemove risk factors (withdrawal of nephrotoxic drugs,
vasodilators and NSADs, taper/withdraw diuretics, expand plasma volume, treat infections*when
diagnosed)
Resolution
Close follow up
Response ?
NO
Does AKI meet criteria of HRS ?
Specific treatment for other AKI phenotypes
NO
Persistance
Further treatment of AKI decided on a
case-by-case basis
Withdrawal of diuretics (if notyet applied) and volume expansion with albumin
(1g/kg) for 2 days
Progression YES
P. Angeli et al. J. Hepatol. 2015 ; 62 : 968-974
# = AKI stage at the first fulfillement of KDIGO criteria
vasoconstrictorsand albumin
YES
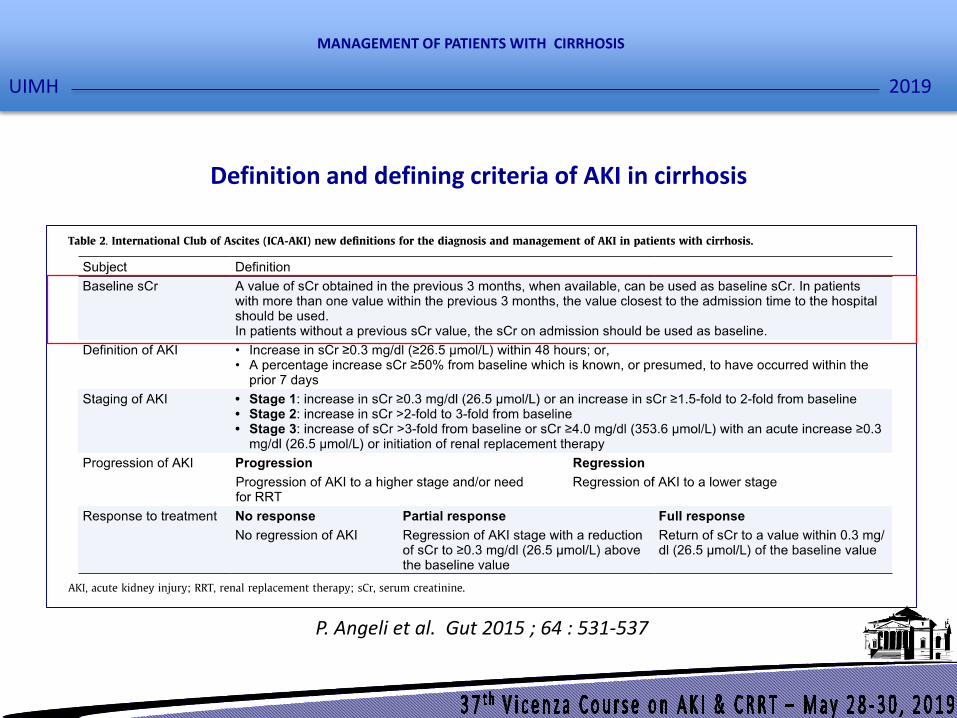
Definition and defining criteria of AKI in cirrhosis
P. Angeli et al. Gut 2015 ; 64 : 531-537
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
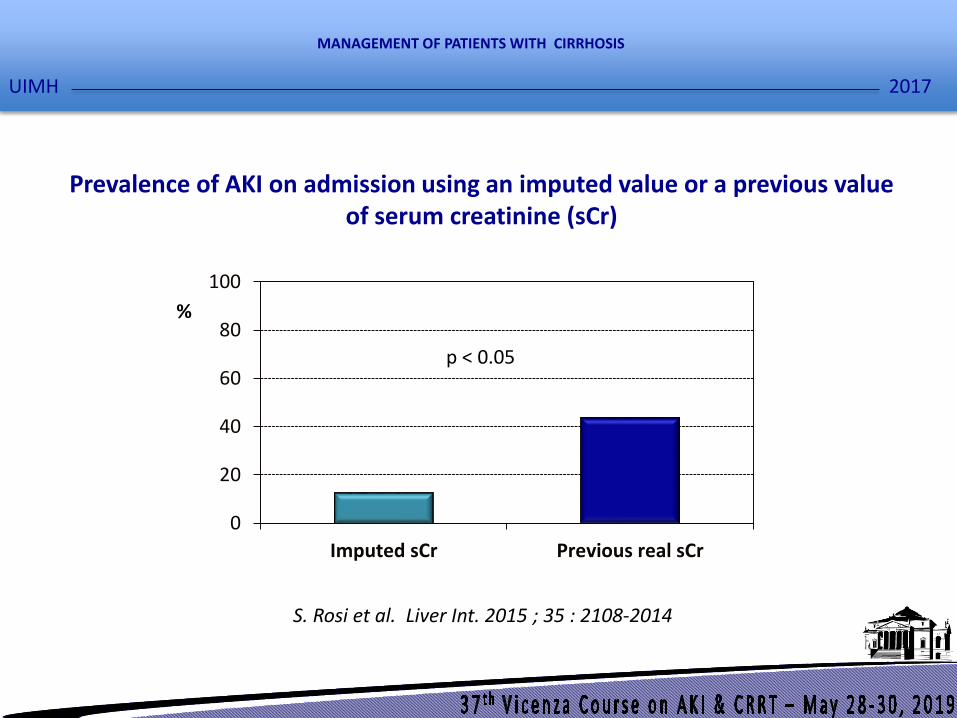
Prevalence of AKI on admission using an imputed value or a previous valueof serum creatinine (sCr)
p < 0.05
2017
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
S. Rosi et al. Liver Int. 2015 ; 35 : 2108-2014
%
0
20
40
60
80
100
Imputed sCr Previous real sCr

Definition and staging of Acute Kidney Injury (AKI)
KDIGO AKI Work Group Kidney Int. Suppl. 2012 ; 2 : 1-138
KDIGO urine output criteria = an urinary output < 0.5 ml/kg B.W./hr x 6-12 hours
Stage Serum creatinine criteria
1°an urinary output < 0.5 ml/kg B.W./hr x 6-12 hours
2°an urinary output < 0.5 ml/kg B.W./hr x 12 -24 hours
3°an urinary output < 0.5 ml/kg B.W./hr x 24 or more hours or anuria per 12 hr
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

AKI sCr + UO
2854 (82.5%)
AKI only sCr
2002 (57.9%)
AKI only UO
2553 (73.8%)
Patients
2997
Critically ill patients with cirrhosis and AKI diagnosed by KDIGO criteria
R. Amathhieu et al. Hepatology 2017 ; 66 : 1592-1600
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
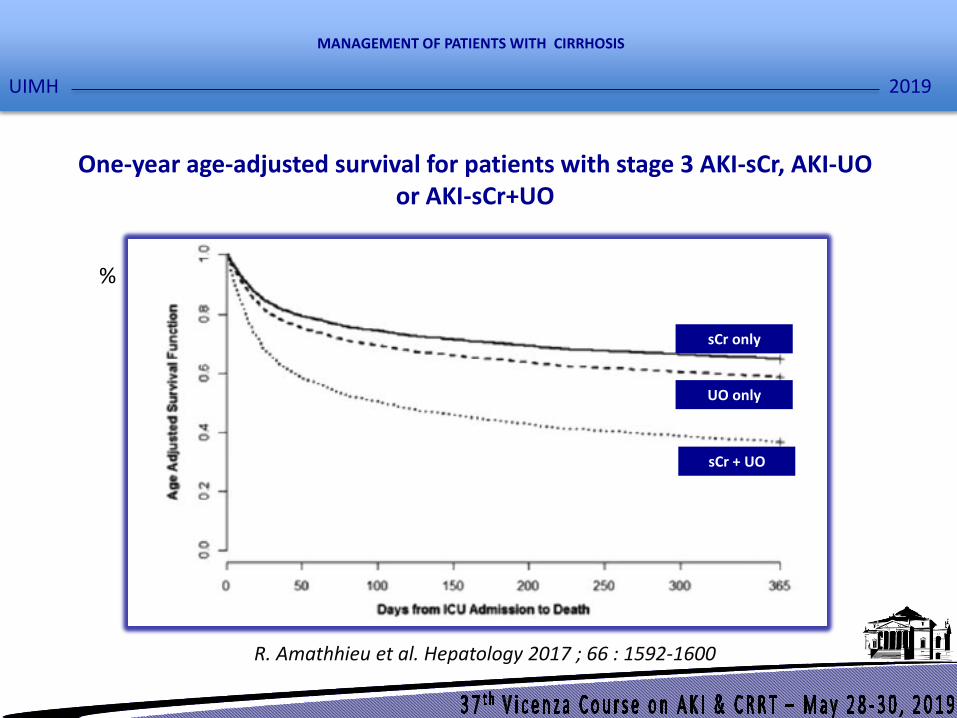
One-year age-adjusted survival for patients with stage 3 AKI-sCr, AKI-UO or AKI-sCr+UO
R. Amathhieu et al. Hepatology 2017 ; 66 : 1592-1600
%
sCr only
UO only
sCr + UO
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
• Acute tubular necrosis (ATN-AKI) (41.7%)
• Prerenal failure (Prenal-AKI) (38%)
• Hepatorenal syndrome (HRS-AKI) (20%)
• Postrenal failure (Postrenal AKI) (0.3%)
Types of AKI in patients with cirrhosis and ascites
R. Moreau et al. Hepatology 2003 ; 37 : 233-243.
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
HRS is a functional renal failure caused by intrarenal vasoconstrictionwhich occurs in patients with end stage liver disease as well as inpatients with acute liver failure or alcoholic hepatitis.HRS is characterized by impaired renal function, marked alterations incardiovascular function, and overactivity in the endogenousvasoactive systems.
Definition of hepatorenal syndrome (HRS)
F. Salerno et al. Gut 2007 ; 56 : 1310-1318
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
1. Cirrhosis with ascites;
2. Serum creatinine > 133 µmol/l (1.5 mg/dl);
3. No sustained improvement of serum creatinine (decrease to a level of 133 µmol/l or
less) after at least two days of diuretic withdrawal and volume expansion with
albumin. The recommended dose of albumin is 1 g/kg of body weight per day to a
maximum of 100 g/day;
4. Absence of shock
5. No current or recent treatment with nephrotoxic drugs;
6. Absence of parenchimal disease as indicated by proteinuria >500 mg/day,
microhematuria (>50 red blood cells per high power field) and/or abnormal renal
ultrasonography.
Current diagnostic criteria of HRS
F. Salerno, et al. Gut 2007 ; 56 : 1310-1318.
Deleted
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Biomarkers No AKI Prerenal AKI HRS-AKI ATN-AKI P
NGAL (μg/g sCr) 30 (17-41) 36 (26-125) 104 (58-208) 1807 (494-3716) <0.0001
IL-18 (ng/g sCr) 21 (16-35) 16 (14-36) 18 (10-29) 150 (58-259) <0.0001
Albumin (mg/g sCr) 3 (1-7) 9 (1-77) 16 (8-46) 324 (53-380) <0.0001
TFF-3 (μg/g sCr) 582 (367-1665) 2300 (323-2720) 1893 (840-2715) 5810 (4019-14466) < 0.0001
MCP-1 (μg/g sCr) 0.2 (0.1-1.4) 0.9 (0.2-2.5) 3 (1-6) 4 (1-14) <0.0001
Ostepontin (μg/g sCr) 1456 (715-3210) 2914 (1847-8382) 5471 (2959-11983) 83337 (4019-14466) < 0.0001
Calbindin (μg/g sCr) 71 (26-150) 5 (2-34) 25 (8-58) 118 (37-324) 0.010
GST-TT (μg/g sCr) 3 (1-16) 3 (1-7) 4 (2-21) 50 (9-169) 0.012
KIM-1 (μg/g sCr) 0.5 (0.3-1.4) 0.5 (0.1-1.1) 1.2 (0.5-2.8) 1.7 (0.9-5.1) 0.015
Cistatin C (μg/g sCr) 24 (12-435) 21 (15-53) 27 (10-47) 115 (39-1552) 0.023
Values of urinary biomarkers in patients categorized according to the absence or presence of AKI and phenotype of AKI
X. Ariza et al. Plos One 2015 ; 10 [Epub ahead of print]
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
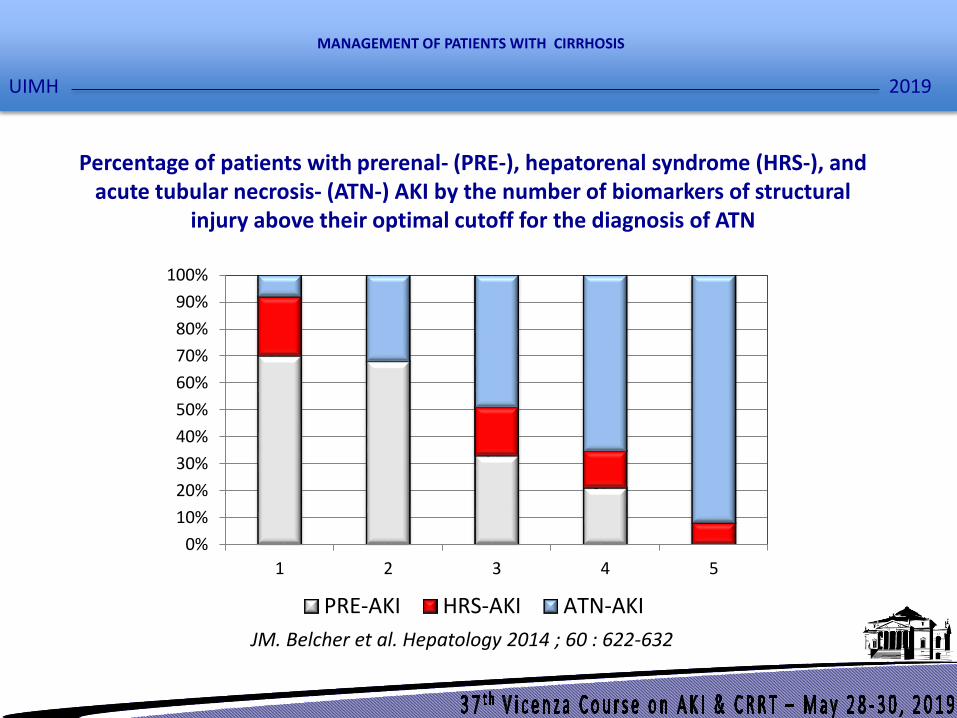
JM. Belcher et al. Hepatology 2014 ; 60 : 622-632
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2 3 4 5
PRE-AKI HRS-AKI ATN-AKI
Percentage of patients with prerenal- (PRE-), hepatorenal syndrome (HRS-), and acute tubular necrosis- (ATN-) AKI by the number of biomarkers of structural
injury above their optimal cutoff for the diagnosis of ATN
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
20
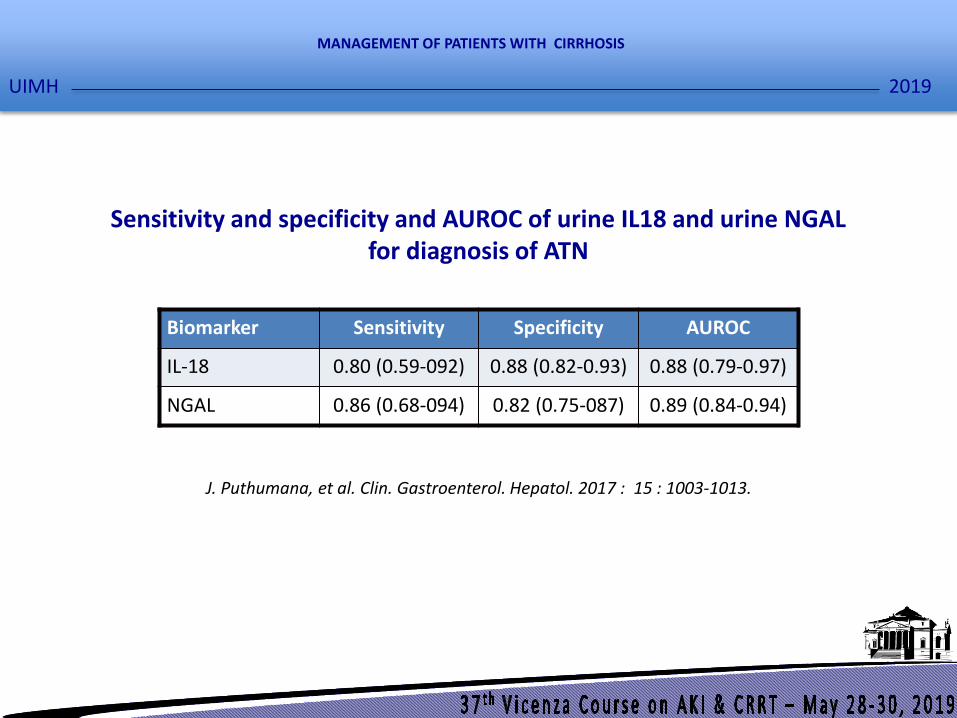
J. Puthumana, et al. Clin. Gastroenterol. Hepatol. 2017 : 15 : 1003-1013.
Sensitivity and specificity and AUROC of urine IL18 and urine NGAL for diagnosis of ATN
Biomarker Sensitivity Specificity AUROC
IL-18 0.80 (0.59-092) 0.88 (0.82-0.93) 0.88 (0.79-0.97)
NGAL 0.86 (0.68-094) 0.82 (0.75-087) 0.89 (0.84-0.94)
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

21
P. Huelin et al. J. Hepatol. 2017 ; 66 : S10-S11 (Abstract).
Urinary NGAL values in patients with cirrhosis and hepatorenal syndrome (HRS-), and acute tubular necrosis- (ATN-) AKI
0
200
400
600
800
1000
1200
1400
1600
ATN-AKI HRS-AKI
μg
/g c
reat
inin
e
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
Pharmacologic therapy for HRS
• Albumin (20-40 g/day intravenously)
• Terlipressin (0.5-2 mg/4-6hr intravenously)
J. Uriz et al. J. Hepatol. 2000 ; 33 : 43-48.
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Rate of response in patients with type 1 HRS according to the schedule of i.v. administration of terlipressin
55,88
45,95
20,59 18,9
0
20
40
60
80
100
I.V. Continuous Infusion I.V. Boluses
Complete response Partial response
% P = N.S.
M. Cavallin et. al. 2016 ; 63 : 983-992
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
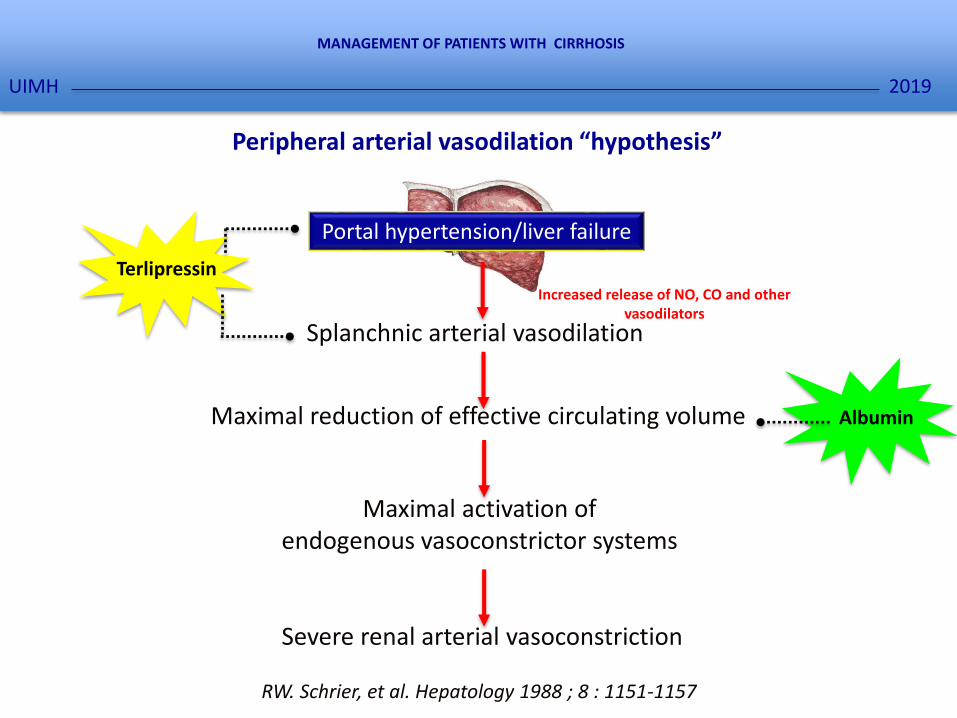
Peripheral arterial vasodilation “hypothesis”
Maximal activation of endogenous vasoconstrictor systems
Severe renal arterial vasoconstriction
RW. Schrier, et al. Hepatology 1988 ; 8 : 1151-1157
Maximal reduction of effective circulating volume
Terlipressin
Albumin
Portal hypertension/liver failure
Splanchnic arterial vasodilation
Increased release of NO, CO and other vasodilators
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
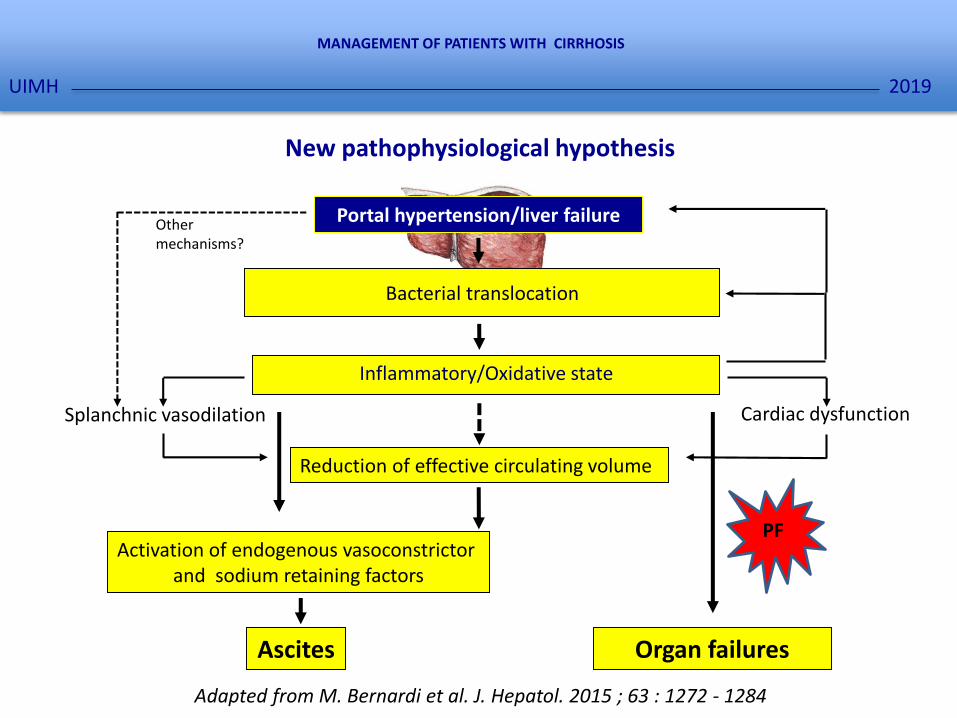
Cardiac dysfunctionSplanchnic vasodilation
Inflammatory/Oxidative state
Reduction of effective circulating volume
Activation of endogenous vasoconstrictorand sodium retaining factors
Ascites
Adapted from M. Bernardi et al. J. Hepatol. 2015 ; 63 : 1272 - 1284
New pathophysiological hypothesis
Other mechanisms?
Organ failures
PF
Portal hypertension/liver failure
Bacterial translocation
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Renal hypoperfusion
Mechanisms of renal injury potentially involved in AKI in patients with liverdisease
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Renal hypoperfusion
Microvascular dysfunction
Mechanisms of renal injury potentially involved in AKI in patients with liverdisease
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
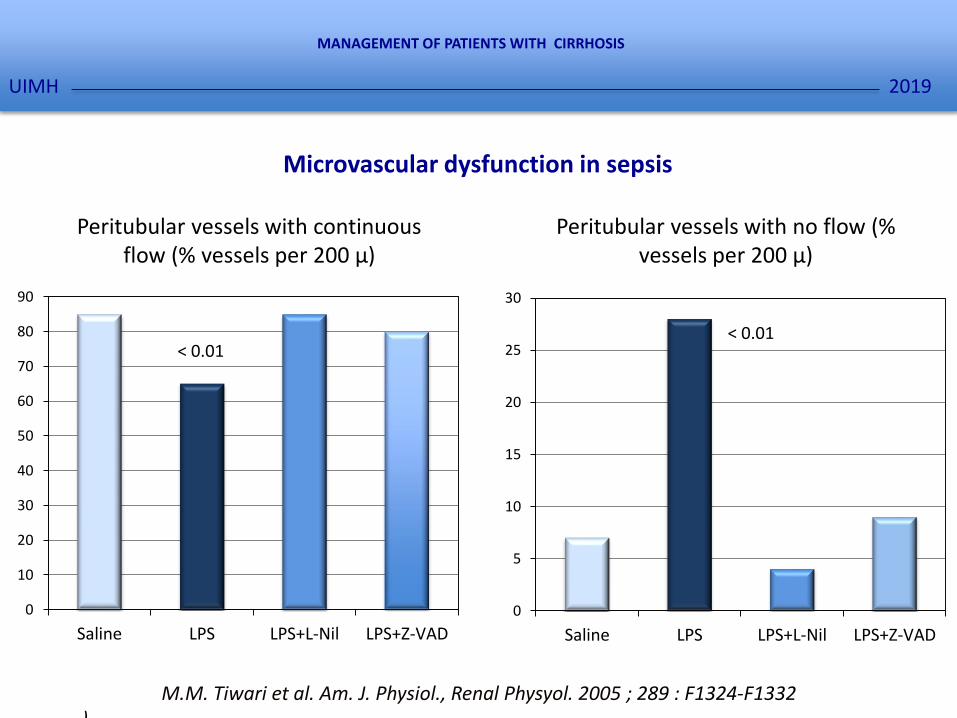
Microvascular dysfunction in sepsis
0
10
20
30
40
50
60
70
80
90
Saline LPS LPS+L-Nil LPS+Z-VAD
0
5
10
15
20
25
30
Saline LPS LPS+L-Nil LPS+Z-VAD
Peritubular vessels with continuousflow (% vessels per 200 μ)
Peritubular vessels with no flow (% vessels per 200 μ)
< 0.01< 0.01
M.M. Tiwari et al. Am. J. Physiol., Renal Physyol. 2005 ; 289 : F1324-F1332).
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
Direct tubular damage
Mechanisms of renal injury potentially involved in AKI in patients with ALF
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
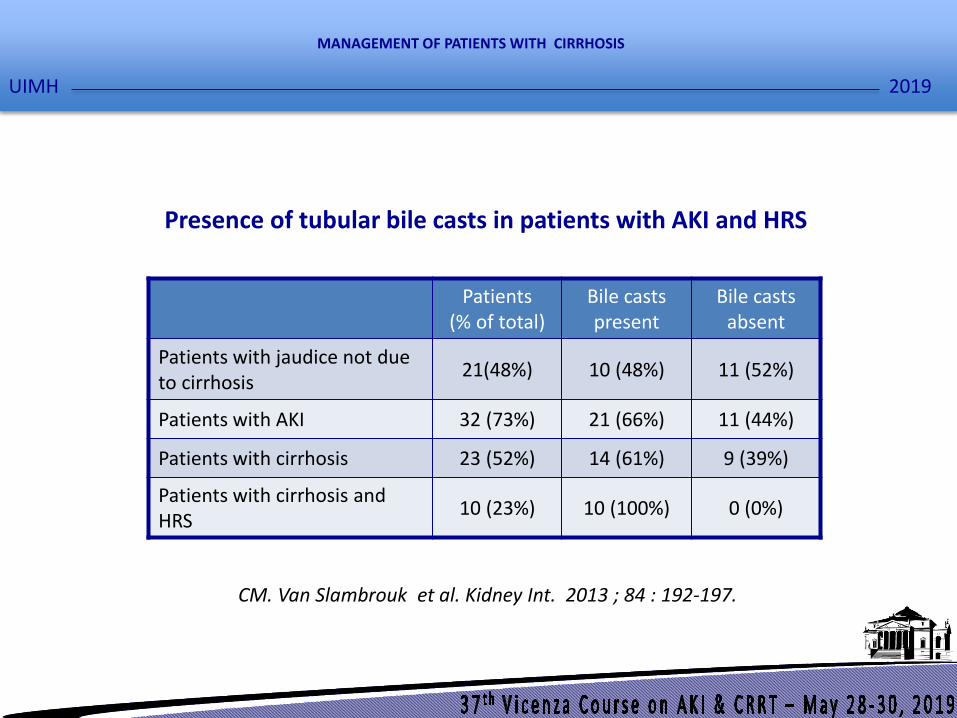
CM. Van Slambrouk et al. Kidney Int. 2013 ; 84 : 192-197.
Presence of tubular bile casts in patients with AKI and HRS
Patients(% of total)
Bile castspresent
Bile castsabsent
Patients with jaudice not due to cirrhosis
21(48%) 10 (48%) 11 (52%)
Patients with AKI 32 (73%) 21 (66%) 11 (44%)
Patients with cirrhosis 23 (52%) 14 (61%) 9 (39%)
Patients with cirrhosis and HRS
10 (23%) 10 (100%) 0 (0%)
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
Mechanisms of renal injury potentially involved in AKI in patients with ALF
Dangersignal/Inflammation
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
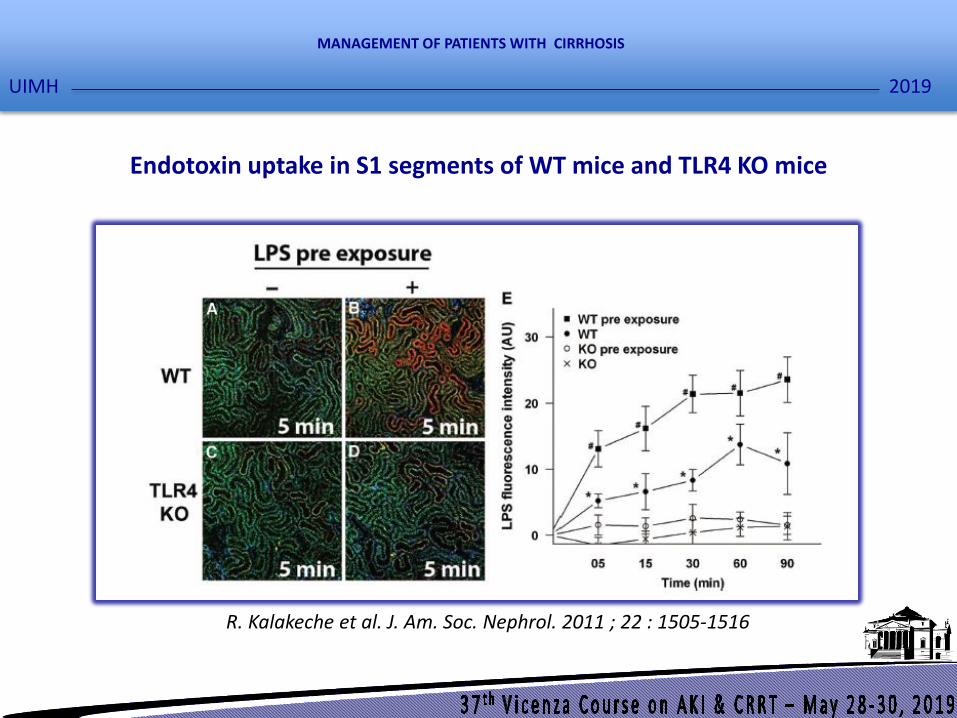
Endotoxin uptake in S1 segments of WT mice and TLR4 KO mice
R. Kalakeche et al. J. Am. Soc. Nephrol. 2011 ; 22 : 1505-1516
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
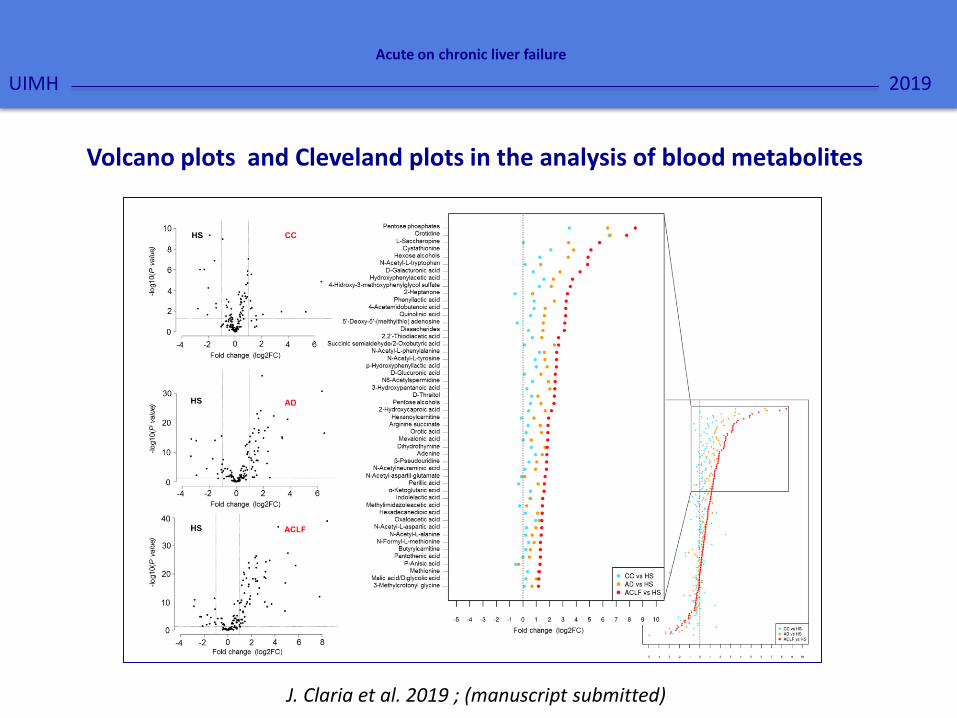
Volcano plots and Cleveland plots in the analysis of blood metabolites
2019
Acute on chronic liver failure
UIMH
J. Claria et al. 2019 ; (manuscript submitted)

Channeling of intracellular glucose in Acute on Chronic Liver Failure
2019
Acute on chronic liver failure
UIMH
J. Claria et al. 2019 ; (manuscript submitted)
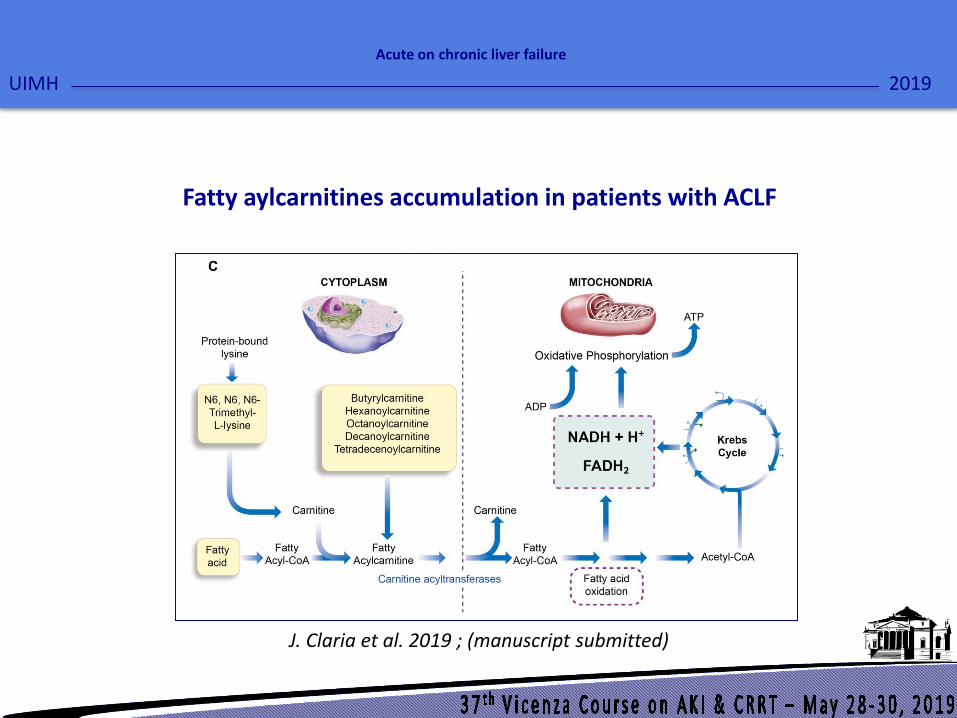
Fatty aylcarnitines accumulation in patients with ACLF
2019
Acute on chronic liver failure
UIMH
J. Claria et al. 2019 ; (manuscript submitted)

Renal hypoperfusion
Direct tubular damage
Dangersignal/Inflammation
Microvascular dysfunction
Mechanisms of renal injury potentially involved in AKI in patients with liverdisease
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Inflammation in patients with ACLF
* p<0.05 with respect to No ACLF
** p<0.001 with respect to No ACLF
C-reactive Protein
R. Moreau et al. Gastroenterology 2013 ; 144 : 1426-1437
0
10
20
30
40
50
60
70
No ACLF ACLF grade 1 ACLF grade 2 ACLF grade 3
***
**
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
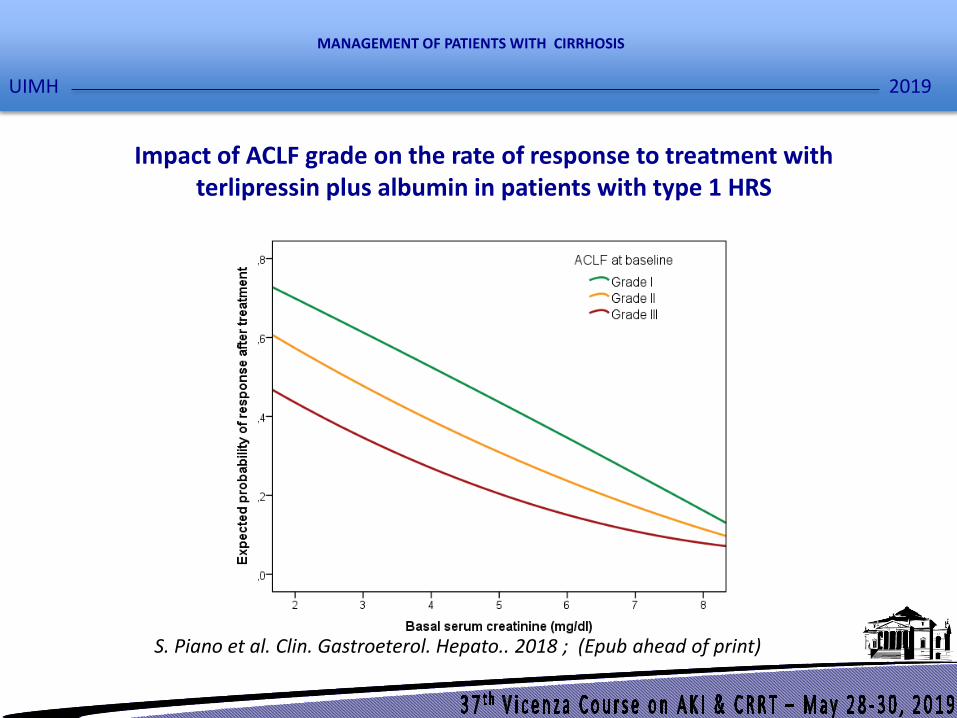
Impact of ACLF grade on the rate of response to treatment with terlipressin plus albumin in patients with type 1 HRS
S. Piano et al. Clin. Gastroeterol. Hepato.. 2018 ; (Epub ahead of print)
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
Clinical types of HRS
Type 1 HRS : rapidly progressive reduction of renal function asdefined by a doubling of the initial serum creatinine to a level> 226 µmol/l or 2.5 mg/dl in less than two weeks. It mayoccurs spontaneously, but it can also follow a precipitatingevent.
Clinical pattern: acute renal failure
Type 2 HRS: is characterized by moderate renal failure (serumcreatinine from 133 to 226 µmol/l or 1.5 to 2.5 mg/dl) with asteady or slowly progressive course.
Clinical pattern: refractory ascites
F. Salerno, et al. Gut 2007 ; 56 : 1310-1318.
HRS-AKI
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
Pharmacologic therapy for HRS
• Albumin (20-40 g/day intravenously)
• Terlipressin (0.5-2 mg/4-6hr intravenously)
J. Uriz et al. J. Hepatol. 2000 ; 33 : 43-48.
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Rate of response in patients with type 1 HRS according to the schedule of i.v. administration of terlipressin
55,88
45,95
20,59 18,9
0
20
40
60
80
100
I.V. Continuous Infusion I.V. Boluses
Complete response Partial response
% P = N.S.
M. Cavallin et. al. 2016 ; 63 : 983-992
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
42
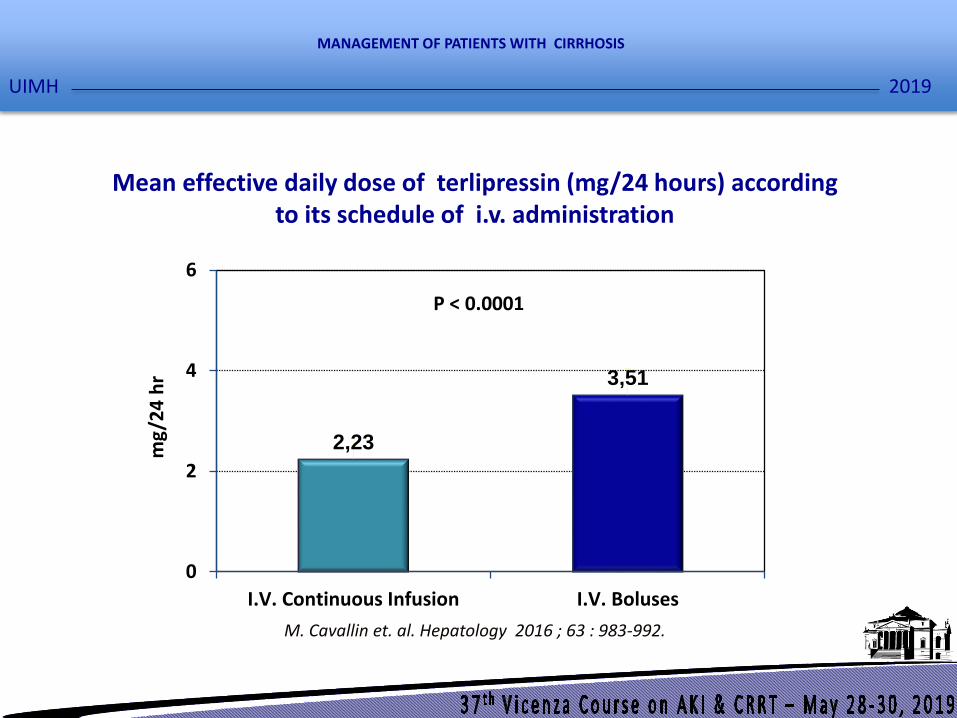
2,23
3,51
0
2
4
6
I.V. Continuous Infusion I.V. Boluses
mg
/24
hr
Mean effective daily dose of terlipressin (mg/24 hours) accordingto its schedule of i.v. administration
M. Cavallin et. al. Hepatology 2016 ; 63 : 983-992.
P < 0.0001
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Type I.V. Continuous infusion
(n° = 34)
I.V. Boluses
(n° = 37)
P
Total: pts (%) 7 (20.58 %) 16 (43.24 %) < 0.05
Suspected intestinal ischemia : pts
- 3 --
Peripheral ischemia: pts 1 - --
Circulatory overload: pts 2 5 --
Angina pectoris: pts 3 3 --
Arrhythmia: pts - 1 --
Arterial hypertension: pts 1 - --
Persistent diarrhea: pts - 2 --
Others: pts - 2 --
Severe treatment-related adverse events (defined as need to withdraw terlipressin) according to the schedule of i.v. administration of terlipressin
M. Cavallin et. al. Hepatology 2016 ; 63 : 983-992
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

TD. Boyer et al. Liver Transpl. 2011 ; 17 : 1328-1332
Survival in patients according to the treatment of type 1 HRS
%LT
Responders to terlipressin and albumin
Non responders to terlipressin and albumin
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
• Patients with advanced liver disease frequently show an acute impairmentof renal function (AKI).
• The KDIGO criteria should be applied for the diagnosis of AKI.• A new algorithm has been developed for a more rationale application of
the therapeutic resources (avoiding of potentially dangerous consequencesof an overtreatment of AKI as a consequence of an uncritical application ofthe KDIGO criteria)
• The definitive removal of the cut off of serum creatinine from the criteriafor diagnosis and treatment of HRS in the setting of AKI (HRS-AKI).
• The differential diagnosis between HRS-AKI and ATN-AKI is complex.• New biomarkers of glomerular filtration rate and parenchymal kidney
damage are promising tools in refining the evaluation of renal function inthese patients.
• Terlipressin plus albumin is an effective treatment for HRS-AKI.• RRT should be used in nonresponders when indicated.
Summary
S. Piano et al. Liver Int. 2017 ; 37 (Suppl 1) : 116-122
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
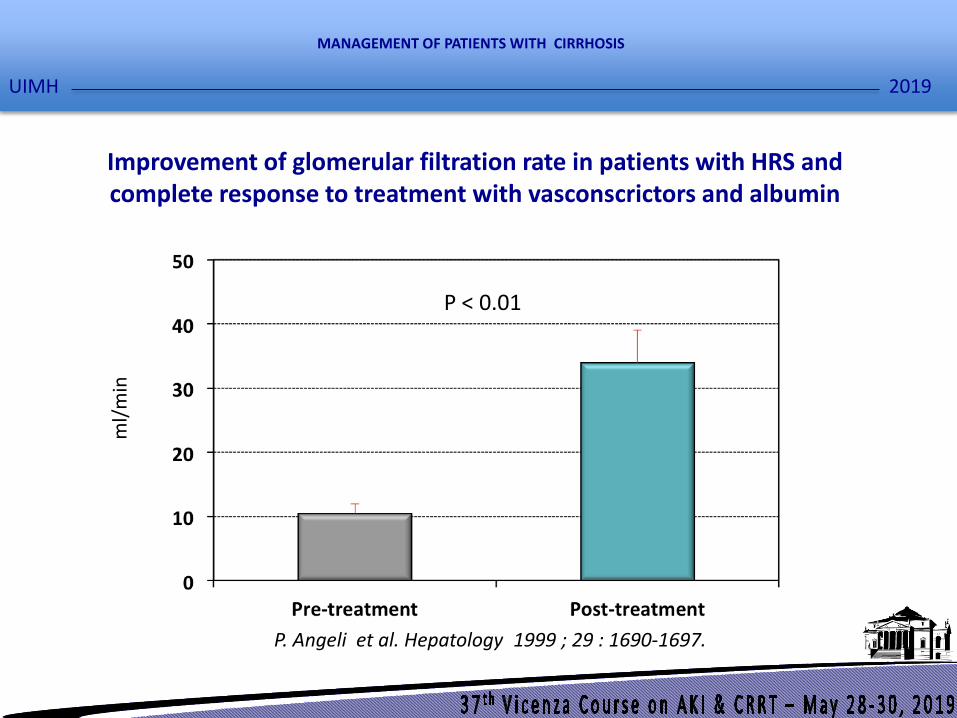
ml/
min
P < 0.01
P. Angeli et al. Hepatology 1999 ; 29 : 1690-1697.
Improvement of glomerular filtration rate in patients with HRS and complete response to treatment with vasconscrictors and albumin
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
M. Hultström et al. Physical. Genomics 2018 ; 50 ; 127-141.
The hierachical network of 114 connected genes in common in 6 different models of AKI
MyC
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
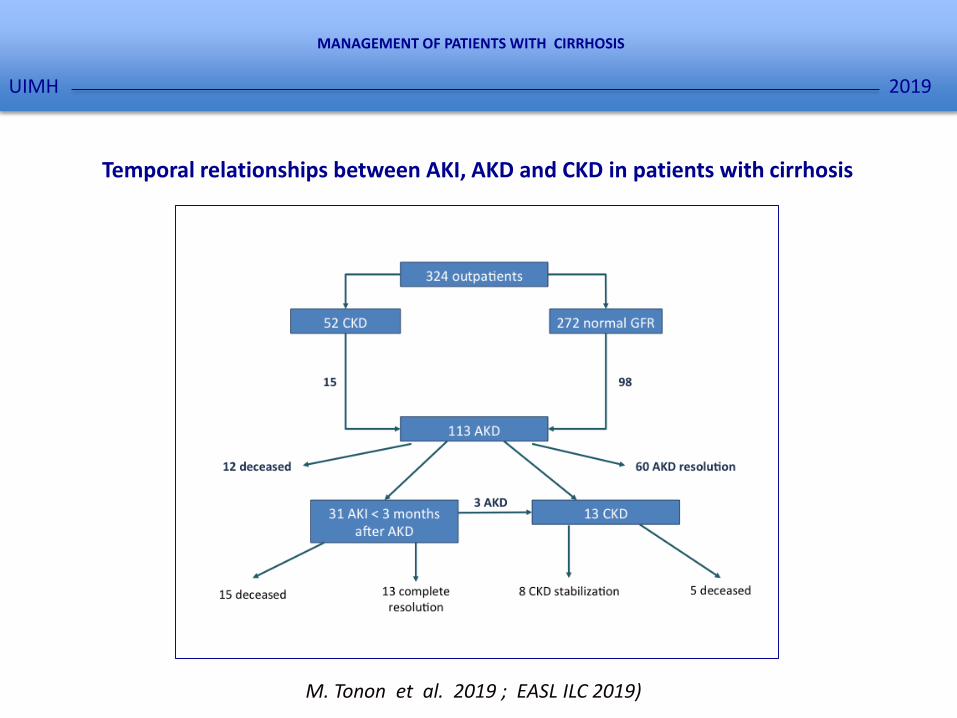
Temporal relationships between AKI, AKD and CKD in patients with cirrhosis
M. Tonon et al. 2019 ; EASL ILC 2019)
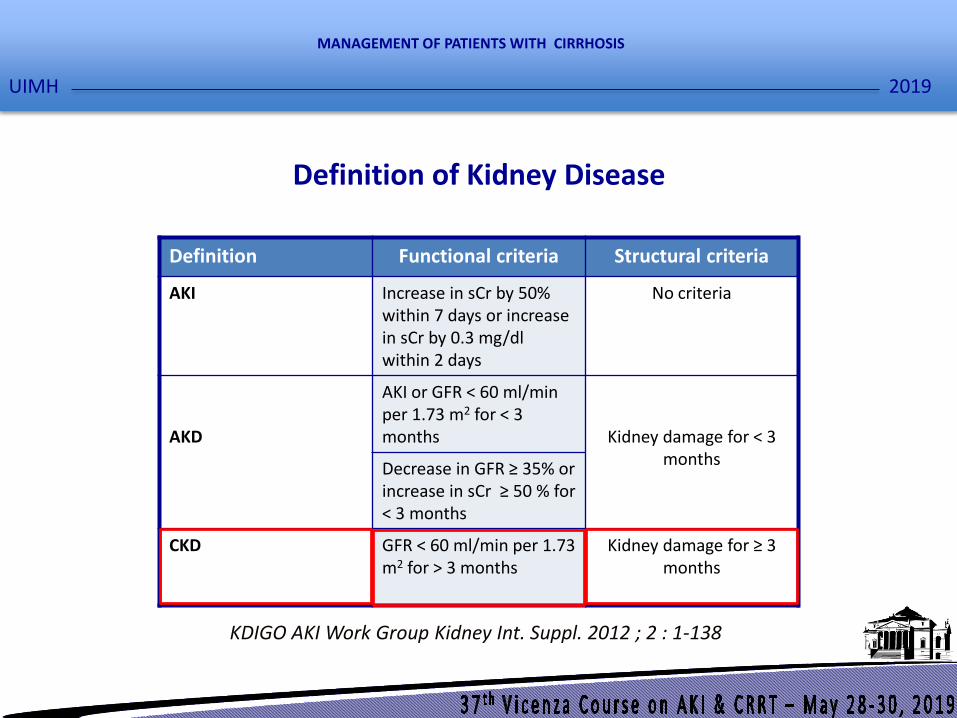
KDIGO AKI Work Group Kidney Int. Suppl. 2012 ; 2 : 1-138
Definition Functional criteria Structural criteria
AKI Increase in sCr by 50%within 7 days or increasein sCr by 0.3 mg/dl within 2 days
No criteria
AKD
AKI or GFR < 60 ml/minper 1.73 m2 for < 3 months Kidney damage for < 3
monthsDecrease in GFR ≥ 35% or increase in sCr ≥ 50 % for < 3 months
CKD GFR < 60 ml/min per 1.73 m2 for > 3 months
Kidney damage for ≥ 3 months
Definition of Kidney Disease
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
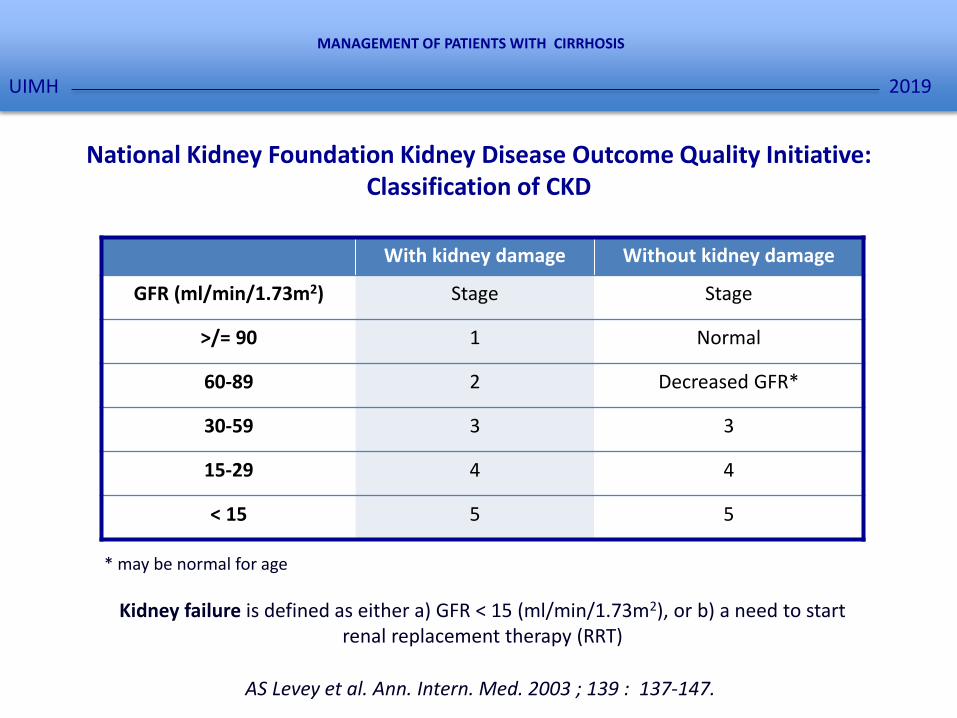
National Kidney Foundation Kidney Disease Outcome Quality Initiative: Classification of CKD
With kidney damage Without kidney damage
GFR (ml/min/1.73m2) Stage Stage
>/= 90 1 Normal
60-89 2 Decreased GFR*
30-59 3 3
15-29 4 4
< 15 5 5
* may be normal for age
Kidney failure is defined as either a) GFR < 15 (ml/min/1.73m2), or b) a need to start renal replacement therapy (RRT)
AS Levey et al. Ann. Intern. Med. 2003 ; 139 : 137-147.
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
0 20 40 60 80 100 120
Stage 1
Stage 2
Stage 3
Stage 4
Stage 5
mGFR
CKD-EPI
MDRD4
MDRD7
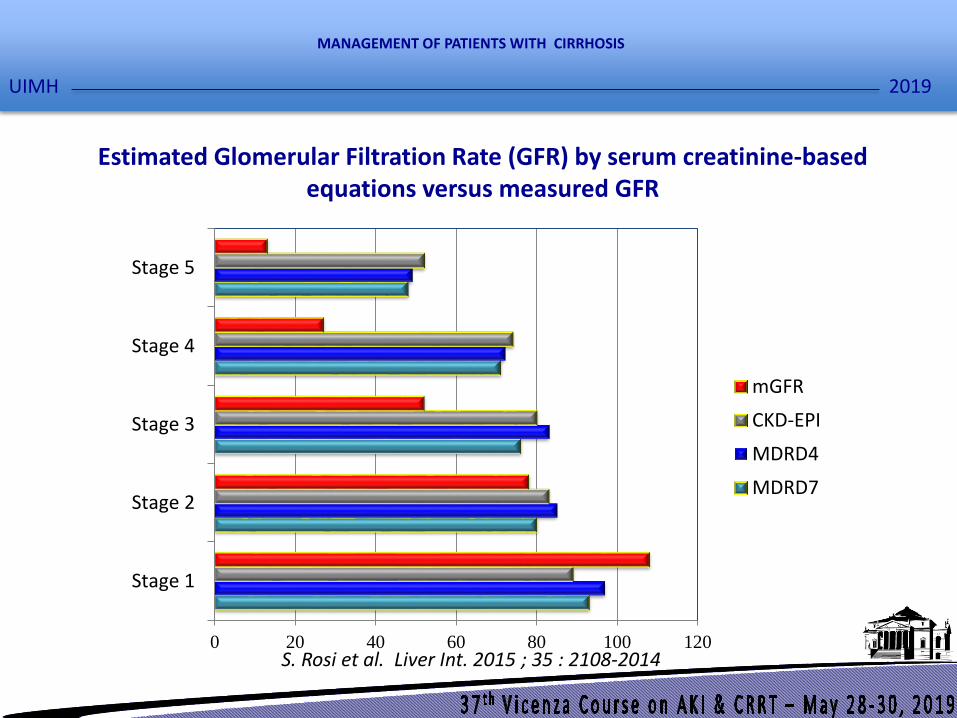
Estimated Glomerular Filtration Rate (GFR) by serum creatinine-basedequations versus measured GFR
S. Rosi et al. Liver Int. 2015 ; 35 : 2108-2014
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

KDIGO AKI Work Group Kidney Int. Suppl. 2012 ; 2 : 1-138
Definition Functional criteria Structural criteria
AKI Increase in sCr by 50%within 7 days or increasein sCr by 0.3 mg/dl within 2 days
No criteria
AKD
AKI or GFR < 60 ml/minper 1.73 m2 for < 3 months Kidney damage for < 3
monthsDecrease in GFR ≥ 35% or increase in sCr ≥ 50 % for < 3 months
CKD GFR < 60 ml/min per 1.73 m2 for > 3 months
Kidney damage for ≥ 3 months
Definition of Kidney Disease
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

M. Tonon et al. 2019 ; EASL ILC 2019)
0,00
0,20
0,40
0,60
0,80
0 12 24 36 48 60
AKD
No AKD
Five-year probability of survival according to the diagnosis of AKD in patients with cirrhosis
%
< p < 0.01
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
Clinical types of HRS
Type 1 HRS : rapidly progressive reduction of renal function asdefined by a doubling of the initial serum creatinine to a level> 226 µmol/l or 2.5 mg/dl in less than two weeks. It mayoccurs spontaneously, but it can also follow a precipitatingevent.
Clinical pattern: acute renal failure
Type 2 HRS: is characterized by moderate renal failure (serumcreatinine from 133 to 226 µmol/l or 1.5 to 2.5 mg/dl) with asteady or slowly progressive course.
Clinical pattern: refractory ascites
F. Salerno, et al. Gut 2007 ; 56 : 1310-1318.
HRS-AKI
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

Proposal of a new classification of hepatorenal syndrome
P. Angeli et al 2019 (manuscript submitted)
Old classification New classification Criteria
Type 1 HRS HRS-AKI a) Absolute increase in sCr ≥ 0.3 mg/dl within 48 hours
and/or
b) Urinary output ≤ 0.5ml/Kg B.W. ≥ 6 hours*
or
b) Percent increase in sCr ≥ 50 % using the last availablevalue of outpatient sCr within 3 months as the baselinevalue
Type 2 HRS HRS-NAKI HRS without the criteria for AKI
• HRS-AKD Decrease in GFR ≥ 35% or eGFR <60 mL/min per 1.73 m2
for < 3 months in the absence of other (structural) causes
• HRS-CKD eGFR < 60 mL/min per 1.73 m2 for 3 months in the absence of other (structural) causes
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
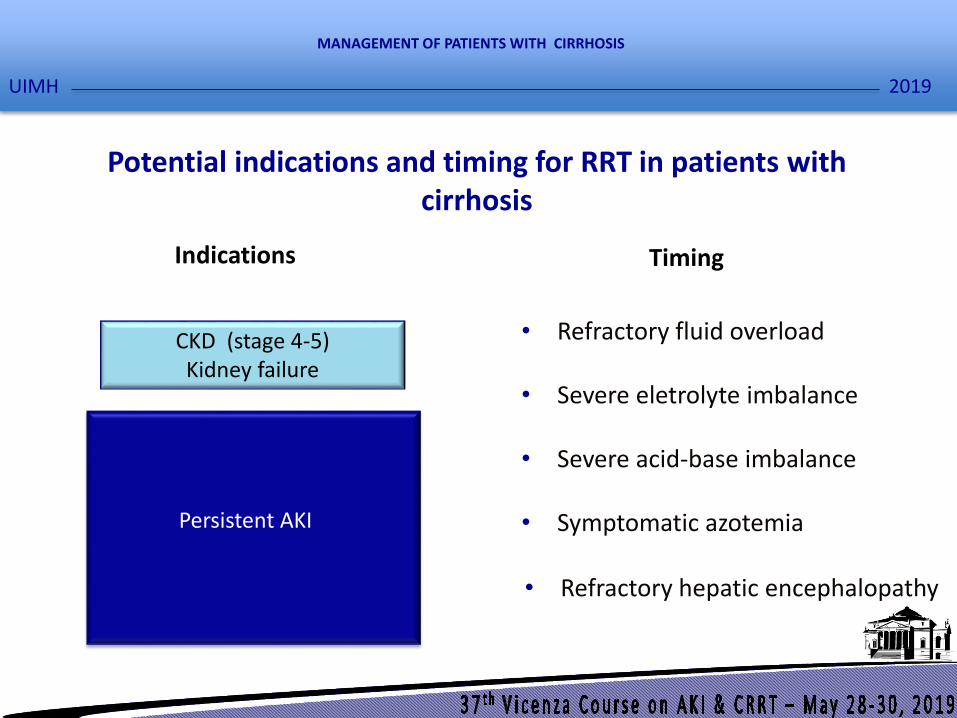
Potential indications and timing for RRT in patients with cirrhosis
CKD (stage 4-5)Kidney failure
AKI-ATN(stage 2 or 3)
AKI-HRS(stage 2 or 3) with no response to terlipressin
plus albumin
• Refractory fluid overload
• Severe eletrolyte imbalance
• Severe acid-base imbalance
• Symptomatic azotemia
• Refractory hepatic encephalopathy
Indications Timing
Persistent AKI
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH

80
100
120
140
160
180
200
0 1 24
Changes in arterial ammonia concentration after CVVH in patients with cirrhosis
AJ. Slak, et al. Liver Int. 2014 ; 34 : 42-48
hr
μm
ol/
l
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH
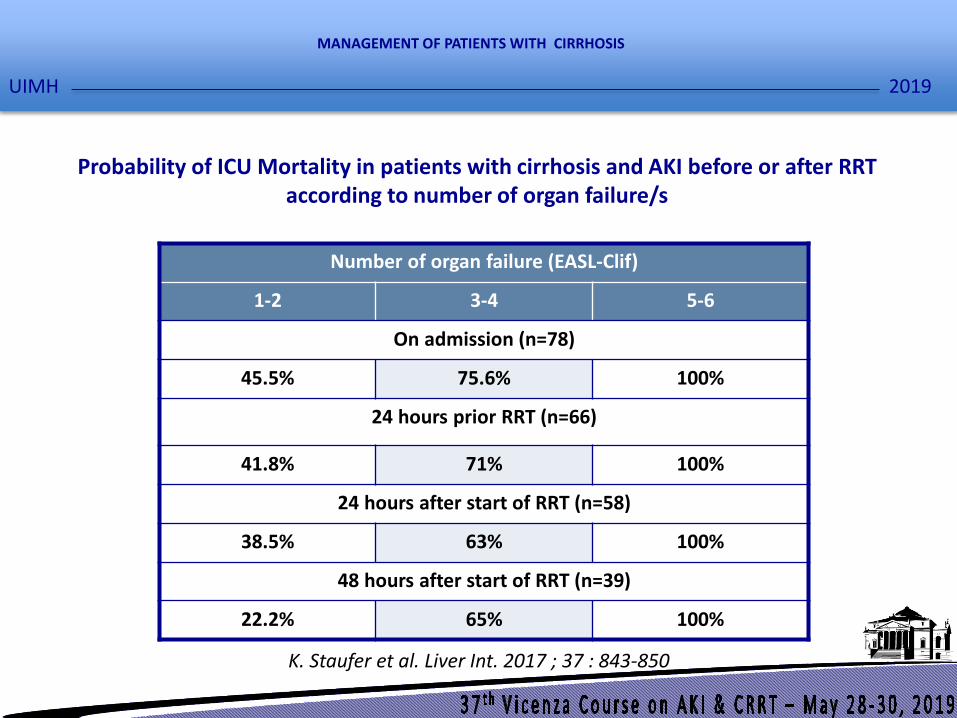
Probability of ICU Mortality in patients with cirrhosis and AKI before or after RRT according to number of organ failure/s
K. Staufer et al. Liver Int. 2017 ; 37 : 843-850
Number of organ failure (EASL-Clif)
1-2 3-4 5-6
On admission (n=78)
45.5% 75.6% 100%
24 hours prior RRT (n=66)
41.8% 71% 100%
24 hours after start of RRT (n=58)
38.5% 63% 100%
48 hours after start of RRT (n=39)
22.2% 65% 100%
2019
MANAGEMENT OF PATIENTS WITH CIRRHOSIS
UIMH