Presentation1
38
Altered mental status in a patient post-BMT Sushma Bellamkonda PGY-2 Neurology
-
Upload
sushma-bellamkonda -
Category
Health & Medicine
-
view
69 -
download
2
Transcript of Presentation1

Altered mental
status in a patient
post-BMT
Sushma Bellamkonda
PGY-2 Neurology
bull 21 yo caucasian female with NHL sp MSD BMT day + 35
pw fever + neutropenia on 1123
bull Evening of 1123 Episode of confusiondisorientation
difficulty expressing herself as in misinterpretation of things
along with forgetfulness One of the episodes was
accompanied by bowel incontinenceThis went on for the
next week and Neurology was consulted
bull Patient was aware of these episodes and was increasingly
upset and anxious
HPI
CC Altered mental status
bull As per mothertremulousness of her BUE noted which she
thought was secondary to weakness lsquoIntermittent
widening of her eyesrsquo with dilated pupils but no
alteration of consciousness during these episodes
bull ROS Shoulder and neck painanxiety with
irritabilitynauseavomiting
PMH Non Hodgkinrsquos LymphomaPeripheral NeuropathyShoulder joint
arthritis
PSH Total hip arthroplasty
SH No ETOHsmokingdrug abuse
Allergies Vancomycin (red manrsquos)
Meds AcyclovirAzithromycinMicafunginSeptra Mycophenolate
mofetilSirolimusVoriconazoleGabapentinAmlodipinePantoprazole
PRN BenadrylDilaudidZofran
EXAM
Vitals
Gen Patient tearful and anxiousWell-nourishedCo-operative
HEENT NCAT Neck supple
Neuro AAO X 3Speech clear and coherentNo dysarthria
Pupils 5 mmreactive to light and accomodation
bilaterallyEOMIGaze intactNo nystagmus
No facial droop notedOther CN intact as well
Muscle tone WNL
Strength testing BUE limited secondary to painbut spontaneous
antigravity movements present45 BLE
DTR 1+ and symmetric throughoutPlantar Flexor BLE
Co-ordination intact
Sensation to pin-prick diminished distal BLEintact to vibration
and proprioception
Gait not assessed
PERTINENT LABS
Pancytopenia(+) ndash WBC 36HH 1030Platelet 41
ANC 828
BMP significant for BUN 38Cr 18
Mg 17Phosphorus 24
LDH 398
Thiamine 38
LFT AST 56Rest normal
BNP 5637
CRP 3
TSHFree T4 WNL
Aspergillus antigen negative
CSF analysis
ClearcolorlessWBC 0RBC 62Glucose 55Protein 42
Cytology negative for any tumor cells
CSF gram stain negativeCSF culture NGTD
CSF for CMVEBVVZVHSVAdenovirusParecho virus - Negative
MRI Head (1202)
New non specific well defined T2 HYPERINTENSE white matter
lesion 7mm in diameter in right posterior subinsularperitrigonal
area
EEG (1203)
Diffuse slowing of background with no seizure activity
Hospital course
bull Bilateral shoulder pain requiring dilaudid and flexeril which
can also interfere with mentation
bull Gabapentindose decreased post 1123
bull Prophylactic voriconazole held after elevated level
bull Marinol held post 1123 after altered mental status
bull Thiamine level found to be 38started on thiamine supp 1126
bull With all above interventionspatientrsquos mentation continued to
improve over her hospitalization
bull Follow up in Neurology clinic in 2 months with fu MRI
Post-BMT neurological complications
NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

bull 21 yo caucasian female with NHL sp MSD BMT day + 35
pw fever + neutropenia on 1123
bull Evening of 1123 Episode of confusiondisorientation
difficulty expressing herself as in misinterpretation of things
along with forgetfulness One of the episodes was
accompanied by bowel incontinenceThis went on for the
next week and Neurology was consulted
bull Patient was aware of these episodes and was increasingly
upset and anxious
HPI
CC Altered mental status
bull As per mothertremulousness of her BUE noted which she
thought was secondary to weakness lsquoIntermittent
widening of her eyesrsquo with dilated pupils but no
alteration of consciousness during these episodes
bull ROS Shoulder and neck painanxiety with
irritabilitynauseavomiting
PMH Non Hodgkinrsquos LymphomaPeripheral NeuropathyShoulder joint
arthritis
PSH Total hip arthroplasty
SH No ETOHsmokingdrug abuse
Allergies Vancomycin (red manrsquos)
Meds AcyclovirAzithromycinMicafunginSeptra Mycophenolate
mofetilSirolimusVoriconazoleGabapentinAmlodipinePantoprazole
PRN BenadrylDilaudidZofran
EXAM
Vitals
Gen Patient tearful and anxiousWell-nourishedCo-operative
HEENT NCAT Neck supple
Neuro AAO X 3Speech clear and coherentNo dysarthria
Pupils 5 mmreactive to light and accomodation
bilaterallyEOMIGaze intactNo nystagmus
No facial droop notedOther CN intact as well
Muscle tone WNL
Strength testing BUE limited secondary to painbut spontaneous
antigravity movements present45 BLE
DTR 1+ and symmetric throughoutPlantar Flexor BLE
Co-ordination intact
Sensation to pin-prick diminished distal BLEintact to vibration
and proprioception
Gait not assessed
PERTINENT LABS
Pancytopenia(+) ndash WBC 36HH 1030Platelet 41
ANC 828
BMP significant for BUN 38Cr 18
Mg 17Phosphorus 24
LDH 398
Thiamine 38
LFT AST 56Rest normal
BNP 5637
CRP 3
TSHFree T4 WNL
Aspergillus antigen negative
CSF analysis
ClearcolorlessWBC 0RBC 62Glucose 55Protein 42
Cytology negative for any tumor cells
CSF gram stain negativeCSF culture NGTD
CSF for CMVEBVVZVHSVAdenovirusParecho virus - Negative
MRI Head (1202)
New non specific well defined T2 HYPERINTENSE white matter
lesion 7mm in diameter in right posterior subinsularperitrigonal
area
EEG (1203)
Diffuse slowing of background with no seizure activity
Hospital course
bull Bilateral shoulder pain requiring dilaudid and flexeril which
can also interfere with mentation
bull Gabapentindose decreased post 1123
bull Prophylactic voriconazole held after elevated level
bull Marinol held post 1123 after altered mental status
bull Thiamine level found to be 38started on thiamine supp 1126
bull With all above interventionspatientrsquos mentation continued to
improve over her hospitalization
bull Follow up in Neurology clinic in 2 months with fu MRI
Post-BMT neurological complications
NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

bull As per mothertremulousness of her BUE noted which she
thought was secondary to weakness lsquoIntermittent
widening of her eyesrsquo with dilated pupils but no
alteration of consciousness during these episodes
bull ROS Shoulder and neck painanxiety with
irritabilitynauseavomiting
PMH Non Hodgkinrsquos LymphomaPeripheral NeuropathyShoulder joint
arthritis
PSH Total hip arthroplasty
SH No ETOHsmokingdrug abuse
Allergies Vancomycin (red manrsquos)
Meds AcyclovirAzithromycinMicafunginSeptra Mycophenolate
mofetilSirolimusVoriconazoleGabapentinAmlodipinePantoprazole
PRN BenadrylDilaudidZofran
EXAM
Vitals
Gen Patient tearful and anxiousWell-nourishedCo-operative
HEENT NCAT Neck supple
Neuro AAO X 3Speech clear and coherentNo dysarthria
Pupils 5 mmreactive to light and accomodation
bilaterallyEOMIGaze intactNo nystagmus
No facial droop notedOther CN intact as well
Muscle tone WNL
Strength testing BUE limited secondary to painbut spontaneous
antigravity movements present45 BLE
DTR 1+ and symmetric throughoutPlantar Flexor BLE
Co-ordination intact
Sensation to pin-prick diminished distal BLEintact to vibration
and proprioception
Gait not assessed
PERTINENT LABS
Pancytopenia(+) ndash WBC 36HH 1030Platelet 41
ANC 828
BMP significant for BUN 38Cr 18
Mg 17Phosphorus 24
LDH 398
Thiamine 38
LFT AST 56Rest normal
BNP 5637
CRP 3
TSHFree T4 WNL
Aspergillus antigen negative
CSF analysis
ClearcolorlessWBC 0RBC 62Glucose 55Protein 42
Cytology negative for any tumor cells
CSF gram stain negativeCSF culture NGTD
CSF for CMVEBVVZVHSVAdenovirusParecho virus - Negative
MRI Head (1202)
New non specific well defined T2 HYPERINTENSE white matter
lesion 7mm in diameter in right posterior subinsularperitrigonal
area
EEG (1203)
Diffuse slowing of background with no seizure activity
Hospital course
bull Bilateral shoulder pain requiring dilaudid and flexeril which
can also interfere with mentation
bull Gabapentindose decreased post 1123
bull Prophylactic voriconazole held after elevated level
bull Marinol held post 1123 after altered mental status
bull Thiamine level found to be 38started on thiamine supp 1126
bull With all above interventionspatientrsquos mentation continued to
improve over her hospitalization
bull Follow up in Neurology clinic in 2 months with fu MRI
Post-BMT neurological complications
NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

PMH Non Hodgkinrsquos LymphomaPeripheral NeuropathyShoulder joint
arthritis
PSH Total hip arthroplasty
SH No ETOHsmokingdrug abuse
Allergies Vancomycin (red manrsquos)
Meds AcyclovirAzithromycinMicafunginSeptra Mycophenolate
mofetilSirolimusVoriconazoleGabapentinAmlodipinePantoprazole
PRN BenadrylDilaudidZofran
EXAM
Vitals
Gen Patient tearful and anxiousWell-nourishedCo-operative
HEENT NCAT Neck supple
Neuro AAO X 3Speech clear and coherentNo dysarthria
Pupils 5 mmreactive to light and accomodation
bilaterallyEOMIGaze intactNo nystagmus
No facial droop notedOther CN intact as well
Muscle tone WNL
Strength testing BUE limited secondary to painbut spontaneous
antigravity movements present45 BLE
DTR 1+ and symmetric throughoutPlantar Flexor BLE
Co-ordination intact
Sensation to pin-prick diminished distal BLEintact to vibration
and proprioception
Gait not assessed
PERTINENT LABS
Pancytopenia(+) ndash WBC 36HH 1030Platelet 41
ANC 828
BMP significant for BUN 38Cr 18
Mg 17Phosphorus 24
LDH 398
Thiamine 38
LFT AST 56Rest normal
BNP 5637
CRP 3
TSHFree T4 WNL
Aspergillus antigen negative
CSF analysis
ClearcolorlessWBC 0RBC 62Glucose 55Protein 42
Cytology negative for any tumor cells
CSF gram stain negativeCSF culture NGTD
CSF for CMVEBVVZVHSVAdenovirusParecho virus - Negative
MRI Head (1202)
New non specific well defined T2 HYPERINTENSE white matter
lesion 7mm in diameter in right posterior subinsularperitrigonal
area
EEG (1203)
Diffuse slowing of background with no seizure activity
Hospital course
bull Bilateral shoulder pain requiring dilaudid and flexeril which
can also interfere with mentation
bull Gabapentindose decreased post 1123
bull Prophylactic voriconazole held after elevated level
bull Marinol held post 1123 after altered mental status
bull Thiamine level found to be 38started on thiamine supp 1126
bull With all above interventionspatientrsquos mentation continued to
improve over her hospitalization
bull Follow up in Neurology clinic in 2 months with fu MRI
Post-BMT neurological complications
NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

EXAM
Vitals
Gen Patient tearful and anxiousWell-nourishedCo-operative
HEENT NCAT Neck supple
Neuro AAO X 3Speech clear and coherentNo dysarthria
Pupils 5 mmreactive to light and accomodation
bilaterallyEOMIGaze intactNo nystagmus
No facial droop notedOther CN intact as well
Muscle tone WNL
Strength testing BUE limited secondary to painbut spontaneous
antigravity movements present45 BLE
DTR 1+ and symmetric throughoutPlantar Flexor BLE
Co-ordination intact
Sensation to pin-prick diminished distal BLEintact to vibration
and proprioception
Gait not assessed
PERTINENT LABS
Pancytopenia(+) ndash WBC 36HH 1030Platelet 41
ANC 828
BMP significant for BUN 38Cr 18
Mg 17Phosphorus 24
LDH 398
Thiamine 38
LFT AST 56Rest normal
BNP 5637
CRP 3
TSHFree T4 WNL
Aspergillus antigen negative
CSF analysis
ClearcolorlessWBC 0RBC 62Glucose 55Protein 42
Cytology negative for any tumor cells
CSF gram stain negativeCSF culture NGTD
CSF for CMVEBVVZVHSVAdenovirusParecho virus - Negative
MRI Head (1202)
New non specific well defined T2 HYPERINTENSE white matter
lesion 7mm in diameter in right posterior subinsularperitrigonal
area
EEG (1203)
Diffuse slowing of background with no seizure activity
Hospital course
bull Bilateral shoulder pain requiring dilaudid and flexeril which
can also interfere with mentation
bull Gabapentindose decreased post 1123
bull Prophylactic voriconazole held after elevated level
bull Marinol held post 1123 after altered mental status
bull Thiamine level found to be 38started on thiamine supp 1126
bull With all above interventionspatientrsquos mentation continued to
improve over her hospitalization
bull Follow up in Neurology clinic in 2 months with fu MRI
Post-BMT neurological complications
NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

PERTINENT LABS
Pancytopenia(+) ndash WBC 36HH 1030Platelet 41
ANC 828
BMP significant for BUN 38Cr 18
Mg 17Phosphorus 24
LDH 398
Thiamine 38
LFT AST 56Rest normal
BNP 5637
CRP 3
TSHFree T4 WNL
Aspergillus antigen negative
CSF analysis
ClearcolorlessWBC 0RBC 62Glucose 55Protein 42
Cytology negative for any tumor cells
CSF gram stain negativeCSF culture NGTD
CSF for CMVEBVVZVHSVAdenovirusParecho virus - Negative
MRI Head (1202)
New non specific well defined T2 HYPERINTENSE white matter
lesion 7mm in diameter in right posterior subinsularperitrigonal
area
EEG (1203)
Diffuse slowing of background with no seizure activity
Hospital course
bull Bilateral shoulder pain requiring dilaudid and flexeril which
can also interfere with mentation
bull Gabapentindose decreased post 1123
bull Prophylactic voriconazole held after elevated level
bull Marinol held post 1123 after altered mental status
bull Thiamine level found to be 38started on thiamine supp 1126
bull With all above interventionspatientrsquos mentation continued to
improve over her hospitalization
bull Follow up in Neurology clinic in 2 months with fu MRI
Post-BMT neurological complications
NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

CSF analysis
ClearcolorlessWBC 0RBC 62Glucose 55Protein 42
Cytology negative for any tumor cells
CSF gram stain negativeCSF culture NGTD
CSF for CMVEBVVZVHSVAdenovirusParecho virus - Negative
MRI Head (1202)
New non specific well defined T2 HYPERINTENSE white matter
lesion 7mm in diameter in right posterior subinsularperitrigonal
area
EEG (1203)
Diffuse slowing of background with no seizure activity
Hospital course
bull Bilateral shoulder pain requiring dilaudid and flexeril which
can also interfere with mentation
bull Gabapentindose decreased post 1123
bull Prophylactic voriconazole held after elevated level
bull Marinol held post 1123 after altered mental status
bull Thiamine level found to be 38started on thiamine supp 1126
bull With all above interventionspatientrsquos mentation continued to
improve over her hospitalization
bull Follow up in Neurology clinic in 2 months with fu MRI
Post-BMT neurological complications
NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

MRI Head (1202)
New non specific well defined T2 HYPERINTENSE white matter
lesion 7mm in diameter in right posterior subinsularperitrigonal
area
EEG (1203)
Diffuse slowing of background with no seizure activity
Hospital course
bull Bilateral shoulder pain requiring dilaudid and flexeril which
can also interfere with mentation
bull Gabapentindose decreased post 1123
bull Prophylactic voriconazole held after elevated level
bull Marinol held post 1123 after altered mental status
bull Thiamine level found to be 38started on thiamine supp 1126
bull With all above interventionspatientrsquos mentation continued to
improve over her hospitalization
bull Follow up in Neurology clinic in 2 months with fu MRI
Post-BMT neurological complications
NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Hospital course
bull Bilateral shoulder pain requiring dilaudid and flexeril which
can also interfere with mentation
bull Gabapentindose decreased post 1123
bull Prophylactic voriconazole held after elevated level
bull Marinol held post 1123 after altered mental status
bull Thiamine level found to be 38started on thiamine supp 1126
bull With all above interventionspatientrsquos mentation continued to
improve over her hospitalization
bull Follow up in Neurology clinic in 2 months with fu MRI
Post-BMT neurological complications
NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Post-BMT neurological complications
NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

NEUROLOGICAL COMPLICATIONS POST-BMT
Yoshida S Hayakawa K Yamamoto A et al
INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

INFECTIOUS DISEASES
Most common CNS complication (22-14)
ASPERGILLOSIS
PNSLUNGBRAIN
Vasculopathy Septic infarcts Hemorrhage and Abscess
formation
Difficult to diagnose as rarely cultured from CSF
Imaging T2WI Low-intermediate density lesion surrounded by high
intensity
No ring like enhancement in abscesses as decreased immune
response in these patients
Yoshida S Hayakawa K Yamamoto A et al
manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

manifestations of central nervous system infection following allogeneic
bone marrow transplantationYamada K Shrier DA Rubio A et al
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU
HHV-6 encephalitis
Reactivation of latent virus in immunosuppressed
Anterograde amnesiaaltered mentationfeverHAdrowsiness
Diagnosis by CSF PCR of HHV-6
Imaging
T2WIFLAIR abnormal symmetrical hyperintensities in limbic
system(Medial temporal lobes)
Coley SC Jager HR Szydlo RM et al
Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Coley SC Jager HR Szydlo RM et al
Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Bacterial infections
Phase 1 Gram negative bacteria
Phase 2 Gram positive bacteria
Phase 3 Encapsulated bacteria
Most common MRSAMRSEListeria monocytogenes
Imaging
MRI Abnormal thickening and enhancement of leptomeninges
Fukui MB Williams RL Mudigonda S et al
Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Fukui MB Williams RL Mudigonda S et al
Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Progressive Multifocal Leukoencephalopathy
Seen in phase 3
Pediatric cases rareMore common in adults
Progressive decline in mental functionAtaxiaVisual
disturancesensory deficitsparalysis
Imaging
T2WIFLAIR Multiple subcortical white matter lesions
Osorio S Camara R Golbano N et al
Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Osorio S Camara R Golbano N et al
Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Vasculopathy
38-8 prevalence
SDHSAHIPH mostly secondary to thrombocytopenia
Infarctionsthrombotic events secondary to endocarditis
Phase 2 and 3 CNS angiitis
Wiznitzer M Packer RJ August CSBurkey ED
Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Wiznitzer M Packer RJ August CSBurkey ED
Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Drug induced neurotoxicity
Immunosuppressants such as MTXCyclosporineTacrolimus and
steroids
bull PRES
bull MTX induced leukoencephalopathy
bull Disseminated Necrotizing leukoencephalopathy
Yoshida S Hayakawa K Yamamoto A et al
Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Posterior Reversible Encephalopathy Syndrome
bull Cyclosporine ATacrolimusSteroids
bull Disruption of BBBinterference with cerebral autoregulationreversible vasogenic edemairreversible
cytotoxic edema
bull HeadacheAMSseizures
Imaging
CTH ndash Hypodense lesions in posterior parieto-occipital regions
MRI gt CTH
MRI FLAIR most sensitive ndash Symmetrical hyperintense lesions in
parieto-occipital and posterior frontal cortical and subcortical
WM bilaterally
Mckinney AM Short J Truwit CL et al
Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Mckinney AM Short J Truwit CL et al
MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

MTX ndash induced leukoencephalopathy
16-69 prevalence
Dose of IV MTX correlates with incidence of leuko-
encephalopathy
Imaging
T2WIFLAIR Hyperintense lesions in central and periventricular
WM
Sparing of subcortical WMcorpus callosumHippocampal
commissureanterior commissure
Reddick WE Glass JO Helton KJ et al
Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Reddick WE Glass JO Helton KJ et al
Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Disseminated Necrotizing leukoencephalopathy
Usually seen after intra-thecal administration of MTX
Rapidly progressive deterioration ndash drowsinessconfusion seizure
ataxia and dementia
Imaging
T1T2 hyperintensities usually in deep white matter surrounded by
edema
Post contrast may show irregular ring like enhancement secondary
to BBB disruption
Pande AR Ando K Ishikura R et al
Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Pande AR Ando K Ishikura R et al
Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Marty FM Lowry CM Cutler CS Campbell BJ Fiumara K Baden LR
Antin JH
Voriconazole and Sirolimus Coadministration after Allogeneic HSCT
is relatively contra-indicated as azoles cause CYP450 inhibition
leading to sirolimus toxicity Recommendation is to empirically
reduce the sirolimus dosage by 90 and regular monitoring of
trough levels
As per literature sirolimus can cause PML though itrsquos very rare(McCalmont V Bennett K et al)
Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Metabolic disturbances following BMT
bull Wernickersquos encephalopathy 55
bull Central Pontine Myelinolysis even more rare
bull Hypothalamic-pituitary dysfunction ndash growth retardationdelay in
puberty and deficiency of secondary sex characters
Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Wernickersquos Encephalopathy
Due to thiamine deficiency
Primary risk factor Prolonged use of TPN
Other causes Decreased oral intake secondary to
anorexiastomatitisGI infections
Triad of acute mental confusionataxiaophthalmoplegia(only
13 of patients)
Imaging
MRI T2 hyperintense lesions in medial thalami and mamillary
bodies
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo
Kang Chul Won Choi
Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Yoon Ji Choi Seh Jong Park Jung Sun Kim Eun Joo Kang Chul Won Choi
Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Post BMT carcinogenesis
Post-transplantation lymphoproliferative disorder (PTLD)
therapy-induced neoplasmCNS relapse can appear in
the late phase after BMT
Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Post-transplant Lymphoproliferative disorder
Spectrum of unregulated lymphoid expansion
Polyclonal B-cell expansion monoclonal malignant
lymphoma
Risk factors Allogenic BMTEBV infection immunosuppression
CNS involvement less commonbut poorer prognosis
Imaging
MRI shows solitary periventricular subcortical mass with necrosis
and hemorrhage
Post contrast ring like enhancement may be present as well
Scarsbrook AF Warakaulle DRDattani M Traill Z
Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

Scarsbrook AF Warakaulle DRDattani M Traill Z
C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

C de Brabander J CornelissenP A E Sillevis Smitt Ch J Vecht M
J van den Bent
Increased incidence of neurological complications in patients
receiving an allogenic BMT from alternative donors ( HLA matched
unrelated donorMismatched related donor)
Probably secondary to more profound and prolonged
immunosuppression used here
In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

In short
The frequency of various CNS complications after BMT differs
according to the period after BMT
Imaging plays an important role in diagnosis T2WI and FLAIR
images are useful because of their higher sensitivity for detecting
white matter lesions compared with other sequences
THANK YOU

THANK YOU

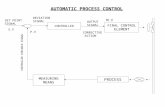










![Presentation1.ppt [โหมดความเข้ากันได้] · Title: Microsoft PowerPoint - Presentation1.ppt [โหมดความเข้ากันได้]](https://static.fdocuments.net/doc/165x107/5ec776d210d7bd5f6f00774b/aaaaaaaaaaaaaaaaaa-title-microsoft-powerpoint.jpg)