Presentation of publication National and regional asthma programmes in Europe: a systematic review...
21
Presentation of publication National and regional asthma programmes in Europe: a systematic review by Olof Selroos, MD, PhD, Emeritus Professor SEMECO AB, Selroos Medical Consulting AB Ängelholm, Sweden
-
Upload
nicholas-marshall -
Category
Documents
-
view
217 -
download
5
Transcript of Presentation of publication National and regional asthma programmes in Europe: a systematic review...
Presentation of publication National and regional asthma programmes
in Europe: a systematic review
by
Olof Selroos, MD, PhD, Emeritus ProfessorSEMECO AB,
Selroos Medical Consulting ABÄngelholm, Sweden
Background
• In Europe 10 million people <45 years of age have asthma
• Prevalence within EU 8.2% in adults9.4% in children
The European Lung White Book, ERS 2013
• Direct costs €11 billion, indirect costs €14 billion
Lung Health in Europe, Facts and figures, ERS 2013

Disability Adjusted Life Years - DALYs
DALY: measure of overall disease burden, expressed as the number of years lost due to ill-health, disability or early death5.2 billion DALYs/year are lost within EU
Source: Institute for Health Metrics and Evaluation (IHME)

Aim of the project
• The European Asthma Research and Innovation Partnership (EARIP) aims to build on and harmonise existing asthma activities in order to generate interconnectivities in asthma management, to develop an approach to reduce asthma-related mortality and morbidity across Europe
• A systematic review of existing asthma programmes should form a part of the basis for future activities
Olof Selroos, Maciej Kupczyk, Piotr Kuna, Piotr Łacwik, Jean Bousquet,
David Brennan, Susanna Palkonen, Javier Contreras, Mark FitzGerald,
Gunilla Hedlin, Sebastian L. Johnston, Renaud Louis, Leanne Metcalf,
Samantha Walker, Antonio Moreno-Galdó, Nikos G. Papadapolous,
José Rosado-Pinto, Pippa Powell and Tari Haahtela
National and regional asthma programmes in Europe
Eur Respir Rev 2015;24:474-483
Methods
• To identify publications on national and regional initiatives in Europe that aimed to improve quality of asthma care in large populations
• Only papers published in English were considered
Systematic Search
• PubMed• Cochrane Database of Systematic Reviews• EMBASE• Web of Science• Science Citation Index• GARD and GAN documents• Asthma Health Outcome Project (AHOP)• Reference lists of publications

Result of the search
• 12 531 citations screened• 732 potentially relevant papers identified for
further evaluation• 412 abstracts evaluated • 147 publications found relevant for inclusion• 53 publications (19 European – 10 from
Finland) related to national asthma programmes
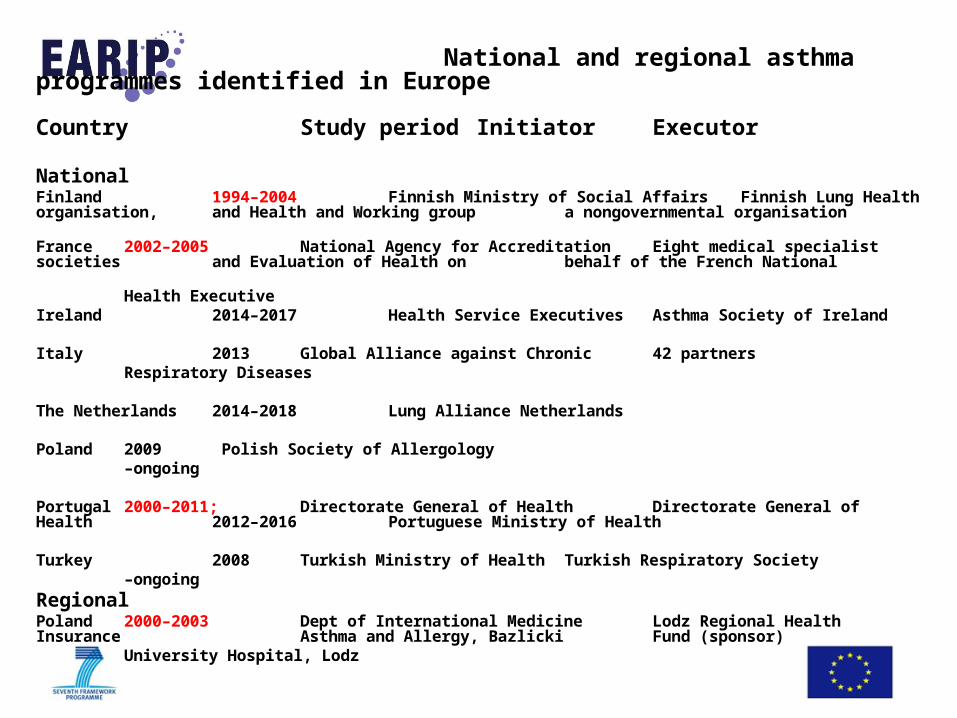
National and regional asthma programmes identified in Europe
Country Study period Initiator Executor National Finland 1994–2004 Finnish Ministry of Social Affairs Finnish Lung Health organisation,
and Health and Working group a nongovernmental organisation
France 2002–2005 National Agency for Accreditation Eight medical specialist societies and Evaluation of Health on behalf of the French National Health Executive
Ireland 2014–2017 Health Service Executives Asthma Society of Ireland
Italy 2013 Global Alliance against Chronic 42 partners Respiratory Diseases
The Netherlands 2014–2018 Lung Alliance Netherlands
Poland 2009 Polish Society of Allergology –ongoing
Portugal 2000–2011; Directorate General of Health Directorate General of Health
2012–2016 Portuguese Ministry of Health
Turkey 2008 Turkish Ministry of Health Turkish Respiratory Society –ongoing
Regional Poland 2000–2003 Dept of International Medicine Lodz Regional Health Insurance
Asthma and Allergy, Bazlicki Fund (sponsor) University Hospital, Lodz

Based on the Finnish programme we know that:
• The asthma burden can be reduced by relatively simple means via:
early diagnosis, effective anti-inflammatory
medication, guided self-management, and networking
• Asthma deaths are avoidable
• Hospitalizations can be reduced

The Finnish Asthma Programme 1994-2004
0
20
40
60
80
100
120
140
160
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Val
ue o
f the
inde
x
Share of asthmatics
Disability pensions
Patients attendingrehabilitation courses
Haahtela T, et al. Thorax 2006
Decrease in disability 76%
Increase the number of asthmatics on regular maintenance medication

Asthma Barometer Study in Finland 2001-2010Self-reported asthma severity and use of care during the last year
Kauppi P, et al. Asia Pac Allergy 2015
10%
4%
45%
62%
45%
34%

Total asthma costs in Finland 1987-2010.True costs in red.
Annual theoretical costs in blue and min costs in grey
Reissell E, et al. Asthma costs in Finland. A public health model to indicate cost effectiveness during 20 years. Finnish Medical Journal 2010.Haahtela T, et al. Reduction of asthma costs in Finland 1987-2010. A prevalence based cost of illness study Manuscript 2015.

● Strong public health-care (also good registries)
● Historical reasons to regard asthma as an inflammatory airway disease.
● Generally recognized and accepted need for a change
● Large national consensus (health-care, medical scientific societies, non-governmental organisations and authorities)
● Support from Ministry of Health and Social Affairs and National Public Health Institute
● Simple organizational structure for leadership and implementation of the programme
Success factors in the Finnish programme
Background
► NEW BODY OF KNOWLEDGE
• Disability caused by asthma can be prevented
► EPIDEMIOLOGY Morbidity Prevalence
► ECONOMY Costs
►EVIDENCE
• Implementation of best practices is highly cost-effective both on the patient and societal level
Generic Action Plan – to be adjusted for local and national needs
Example: The Finnish Asthma Programme 1994-2004

Background
► NEW BODY OF KNOWLEDGE
• Disability caused by asthma can be prevented
► EPIDEMIOLOGY Morbidity Prevalence
► ECONOMY Costs
►EVIDENCE
• Implementation of best practices is highly cost-effective both on the patient and societal level
► CONCLUSIONS
• Public health problem
• Need for broad consensus
• Need for action
• Identification of key stakeholders
• Focus on patients
• Focus on severe asthma to stop exacerbations/attacks
• Focus on effective use of available resources and registers
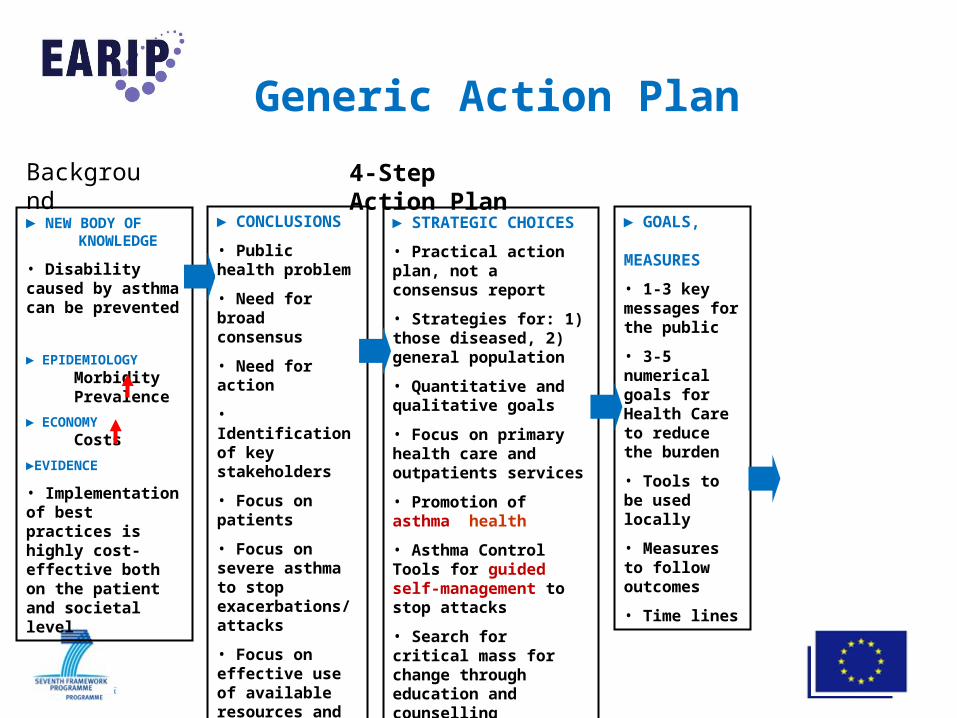
Generic Action Plan
4-Step Action Plan

Background
► NEW BODY OF KNOWLEDGE
• Disability caused by asthma can be prevented
► EPIDEMIOLOGY Morbidity Prevalence
► ECONOMY Costs
►EVIDENCE
• Implementation of best practices is highly cost-effective both on the patient and societal level
4-Step Action Plan
► CONCLUSIONS
• Public health problem
• Need for broad consensus
• Need for action
• Identification of key stakeholders
• Focus on patients
• Focus on severe asthma to stop exacerbations/attacks
• Focus on effective use of available resources and registers
► STRATEGIC CHOICES
• Practical action plan, not a consensus report
• Strategies for: 1) those diseased, 2) general population
• Quantitative and qualitative goals
• Focus on primary health care and outpatients services
• Promotion of asthma health
• Asthma Control Tools for guided self-management to stop exacerbations/attacks
• Search for critical mass for change through education and counselling
Generic Action Plan
Background
► NEW BODY OF KNOWLEDGE
• Disability caused by asthma can be prevented
► EPIDEMIOLOGY Morbidity Prevalence
► ECONOMY Costs
►EVIDENCE
• Implementation of best practices is highly cost-effective both on the patient and societal level
4-Step Action Plan
► CONCLUSIONS
• Public health problem
• Need for broad consensus
• Need for action
• Identification of key stakeholders
• Focus on patients
• Focus on severe asthma to stop exacerbations/attacks
• Focus on effective use of available resources and registers
► STRATEGIC CHOICES
• Practical action plan, not a consensus report
• Strategies for: 1) those diseased, 2) general population
• Quantitative and qualitative goals
• Focus on primary health care and outpatients services
• Promotion of asthma health
• Asthma Control Tools for guided self-management to stop attacks
• Search for critical mass for change through education and counselling
► GOALS, MEASURES
• 1-3 key messages for the public
• 3-5 numerical goals for Health Care to reduce the burden
• Tools to be used locally
• Measures to follow outcomes
• Time lines
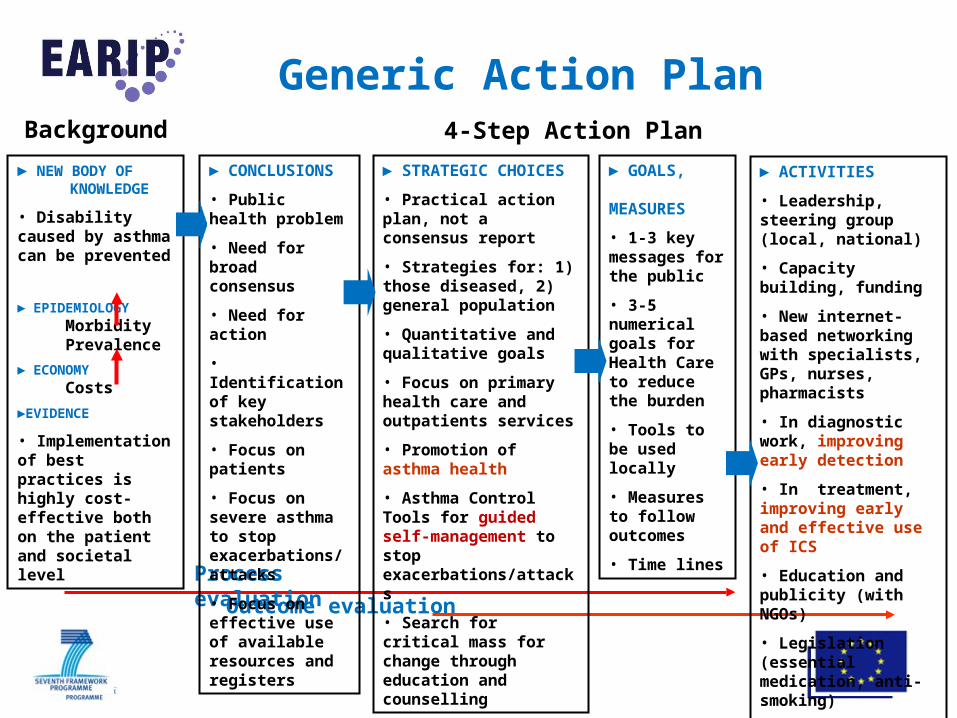
Generic Action Plan
Background
► NEW BODY OF KNOWLEDGE
• Disability caused by asthma can be prevented
► EPIDEMIOLOGY Morbidity Prevalence
► ECONOMY Costs
►EVIDENCE
• Implementation of best practices is highly cost-effective both on the patient and societal level
4-Step Action Plan
Process evaluation
Outcome evaluation
► CONCLUSIONS
• Public health problem
• Need for broad consensus
• Need for action
• Identification of key stakeholders
• Focus on patients
• Focus on severe asthma to stop exacerbations/attacks
• Focus on effective use of available resources and registers
► STRATEGIC CHOICES
• Practical action plan, not a consensus report
• Strategies for: 1) those diseased, 2) general population
• Quantitative and qualitative goals
• Focus on primary health care and outpatients services
• Promotion of asthma health
• Asthma Control Tools for guided self-management to stop exacerbations/attacks
• Search for critical mass for change through education and counselling
► GOALS, MEASURES
• 1-3 key messages for the public
• 3-5 numerical goals for Health Care to reduce the burden
• Tools to be used locally
• Measures to follow outcomes
• Time lines
► ACTIVITIES
• Leadership, steering group (local, national)
• Capacity building, funding
• New internet-based networking with specialists, GPs, nurses, pharmacists
• In diagnostic work, improving early detection
• In treatment, improving early and effective use of ICS
• Education and publicity (with NGOs)
• Legislation (essential medication, anti-smoking)
• Feedback, follow-up
Generic Action Plan

Generic Template for a Local Asthma Plan
Goals (e.g. 1-5 goals for next 5 years)
1. ....................................2. ....................................3. e.g. Prevent asthma attacks ► Indicator: emergency visits are reduced by 50%
4. .....................................5. ..................................... Main Messages
► e.g. Zero tolerance to asthma deaths► .....................................► .....................................
► .....................................► .....................................
Tasks Tools Outcomes
For each Goal: what to do (Tasks), how to do it (Tools), and what to measure (Outcomes)?
Quantitative (numerical) goals for health care professionals
For general public, decision makers

ConclusionsAsthma is still seriously neglectedThis can be changed by
higher awareness of asthma
higher on national priorities
advocacy for change
national asthma strategies
standard case management
more data and monitoring
“A community problem needs community solutions” Haahtela et al Thorax 2001;56:806-14