Prescribing Opioids in the Emergency Department...Prescribing Opioids in the Emergency Department...
32
Prescribing Opioids in the Emergency Department Dr. Maureen Allen BN,CCFP-EM(PC) Assistant Professor Dalhousie University Emergency Medicine October 2017 2015-2016 1
Transcript of Prescribing Opioids in the Emergency Department...Prescribing Opioids in the Emergency Department...

Prescribing Opioids in the Emergency Department
Dr. Maureen Allen BN,CCFP-EM(PC)
Assistant Professor Dalhousie University
Emergency Medicine
October 2017
2015-2016 1

No Disclosures
2015-2016 2

What I hope you learn from this session
• A comprehensive approach to pain that helps you manage the risk associated with prescribing high risk pain pharmacology.
• Better understanding of tolerance and dependency and how this differs from addiction (and why it matters).
• Strategy for safe dispensing of opioid analgesics.

“Houston we have a problem”
•Opioids have been a game changer
• But so have Benzodiazepines
• Prescription drug mortality has increased 6 fold since 1980’s
• National Opioid Use Guidelines for the safe and Effective Use of Opioids for Chronic Non-Cancer Pain. Hamilton: National Opioid Use Guideline Group; 2010.• Volkow ND, McLellan AT. Opioid abuse in Chronic pain. Misconceptions and Mitigation Strategies. NEJM. 374;13. March 2016.• CDC Guidelines for prescribing Opioids for Chronic Pain-United States 2016. Morbidity and Mortality weekly Report. March 18, 2016.

Benzodiazepines
• 45,000 Nova Scotian’s take them
• 25% take more than 2 BZD
• 20% on BZD are also taking opioids
• 25% who use BZD and Opioids take > 90mg MEDD
2015-2016 5
BZD often prescribed for unrecognized withdrawal
which can manifest as increase anxiety, increase pain and poor
sleep

“Opioid Crisis”
2015-2016 6
RECREATIONAL USE
PRESCRIPTION USE
“Pain”
• Forces that drive use different than recreational use (Talking points)
• De novo addiction (5-16%)• Problematic use (28-29%)• Diversion ?
• Legitimate scripts (Diverted )
• Illicit marketplace• Canada Post (Fentanyl)
Fentanyl
Hydromorphone

What’s driving the epidemic
• Legitimate script’s (FP, NP, Dentists, Vet’s, Specialists including CP and PC)
• Illicit (Canada post, organized crime)
• Lack of affordable access to alternative treatment for chronic pain or psychological pain
• Problematic use not addressed early or if addressed at all is often mislabeled as addiction (OUD)
• Poverty, elder abuse (Diversion)
Barnett ML, Olenski AR, Jena AB. Opioid-Prescribing Patterns of Emergency Physicians and Risk of Long-Term Use. NEJM. 376;7 February 16, 2017.Volkow ND, McLellan TA, Cotto JH. Characteristics of Opioid Prescriptions in 2009. JAMA 2011; 305(13): 1299-1301.

0
5
10
15
20
25
30
35
40
45
2011 2012 2013 2014
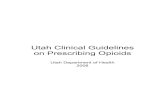
Percentage of deaths attributed to specific opioid in Nova Scotia
Hydromorphone Oxycodone Methadone
Morphine Fentanyl Codeine
HYDROMORPHONE
METHADONE
MORPHINE
OXYCODONE
FENTANYL
CODEINE
NS Medical examiner’s office, accessed Nov 2015

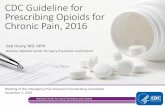
8%
92%
Drugs Found in overdose deaths in Nova Scotia 2007- 2014
NS Medical examiner’s office, accessed Nov 2015
Illicit
Prescription

Fact checking in 2017
• Opioid analgesic are effective in acute pain
• Limited effectiveness in Chronic pain
• Extended release dosing of >100mg MEDD increase mortality and morbidity
• They are widely diverted and improperly used
• Risk of opioid related complications including death increase when sedatives (BZD) are added
• Some individuals and conditions are more vulnerable than others to these risks
2015-2 10
Volkow ND, McLellan T. Opioid Abuse in Chronic Pain-Misconceptions and Mitigation Strategies. N Engl J Med 374;13. March 31, 2016.Chou R, Deyo R, Devine B et al. The effectiveness and risks of long-term opioid treatment of chronic pain: Evidence Report/Technology Assessment. AHRQ 2014.

Reality check
• Many physicians admit they are not confident about how to prescribe opioids safely, how to detect abuse or emerging addiction or even how to discuss these issues with their patients.
2015-2016 11
Hagemeier NE, Gray JA, Pack RP. Prescription drug abuse: a systematic review and critical appraisal of guidelines for chronic pain.Ann Intern Med 2014; 160:38-47.

Question #1
• Legitimate pain protects patients from addiction to their opioid. (Cancer pain, fracture pain etc.)
2015-2016 12
• TRUE• FALSE

Opioid Addiction
• Is a Life-threatening complication of opioid use NOT a moral failing
• Cause of pain doesn’t matter
• Risk factors do
2015-2016 13

2015-2016 14
90% will start before 35 years
85% before 18 years“Pediatric illness”
Don’t leave them on IV to
long“Clinical inertia”
OPIOID RISK TOOL

Question #2
• Addiction is the same as tolerance and dependency.
2015-2016 15
• TRUE• FALSE• It depends

2015-2016 16
have addiction
100%

3. Prescribing opioids: What we need to know: Talking point
• Opioids• Tolerance• Dependency• Withdrawal
100% will gets this
PROBLEMATICUSE
“Unstable angina”
ADDICTION“AMI”
This is NOT ADDICTION
PREVENTION MONITORING
RECOVERY(Opioid
stabilization)
• Pain• Energy • OST
LINE IN THE SAND
Why do you use
opioids?

Physiological processes associated with opioids
2015-2016 18
*CNCP: Chronic non-cancer pain*OIP: Opioid Induced Pain
• Servick K. Primed for pain: Do opioids make chronic pain users more sensitive to pain? SCIENCE. November 2016. Vol 354 Issue 6312.• Volkow ND, McLellan T. Opioid Abuse in Chronic Pain-Misconceptions and Mitigation Strategies. N Engl J Med 374;13. March 31, 2016.• Chou R, Deyo R, Devine B et al. The effectiveness and risks of long-term opioid treatment of chronic pain: Evidence Report/Technology Assessment. AHRQ 2014
DEPENDENCY0-5 days
*SENSITIZATION< 8 days
ADDICTION(Months)

What is “Problematic use”?
More Predictive for ADDICTION
• Selling drugs
• Forging prescriptions
• Stealing prescriptions pads
• Altering a delivery route
• Buying from an illicit source
• Abusing illicit drug
• Multiple dose escalations
• Multiple lost prescriptions
More Predictive for “PROBLEMATIC USE”
• Request more or stronger opioids
• Hoarding drugs when symptoms improve
• Request specific drugs
• Acquiring analgesics from more than one source
• Unapproved dose escalation once or twice
• Unapproved use of analgesia to treat other symptoms
• Porteroy RK. Opioid prescriptions for chronic non-cancer pain: Clinical perspectives. J Law Med Ethics. 1996;24:301
PROBLEMATIC USE IS NOT ADDICTION

Addiction and the 4 C’s:
•Compulsive use•Cravings•Continued use
despite consequences•*Altering a route
(chewing, injecting)

Important difference between tolerance, dependency and addiction
• Addiction IS NOT a predictable result of opioid prescribing whereas tolerance and dependency are
• Molecular mechanisms underlying addiction are distinct from those responsible for tolerance and physical dependence in that they evoke much more slowly, last much longer, and disrupt multiple brain processes
• Once addiction develops it is a separate often chronic medical illness that will not remit simply with opioid discontinuation and will carry a high risk of relapse for years without proper treatment
2015-2016 21
• Volkow ND, McLellan T. Opioid Abuse in Chronic Pain-Misconceptions and Mitigation Strategies. N Engl J Med 374;13. March 31, 2016.

2015-2016 22

OPIOID ANALGESICS
• Important family of medications
• Inherent risks
• Opioid induced pain
• Opioid addiction (OUD)
• Opioid diversion
2015-2016 23

Location of Mu receptors
• Human brain
• Brain stem
• Spinal cord
• Peripheral terminals
• Small intestine (gut motility)
2015-2016 24

Opioid analgesics: Therapeutic and abuse-producing effects
• Produce analgesia and euphoria
• Pavlovian conditioning (Learned association between pain and drug relief)
• Conditioned urge (panic) for relief often leads to early, inappropriate use
2015-2016 25

Putting it together in 6 steps
• LISTEN to the patient’s pain story
• ACKNOWLEDGE suffering
• EXAM carefully for any new pathology or progression of a pre-existing disease
• MAXIMIZE non-opioid and non-cannabinoid therapies
• RISK STRATIFY for harm if opioid analgesics and cannabinoid are used to manage pain
• MANAGE the risk by MAPing out an approach to opioids and cannabinoids
Allen MA. Opioid Analgesics: Is it time for risk stratification Prior to Use? CJEM. 2017; 19(5): 414.

MAPing
• MONITOR use (UDT, PMP, Screening, UDR-MS, aberrant behaviour)
• ADJUST approach (immediate)
• PRESCRIBE using principles of HARM REDUCTION
Allen MA. Opioid Analgesics: Is it time for risk stratification Prior to Use? CJEM. 2017; 19(5): 414.

Key Harm reduction strategy’s
• Avoid prescribing extended release, long acting preparations of opioids as first line.
• Avoid prescribing opioids to patients who are already taking sedatives, particularly benzodiazepines.
• Avoid prescribing opioids to patients with alcohol dependency, or patients who are regular benzodiazepine or sedative users, especially if they have a known substance abuse history or history of mental illness.
• If prescribing opioids, prescribe a small number of short-acting pills to last the patient 2-3 days.
2015-2016 28

Key Harm reduction strategy’s
• Do not give known IV drug user’s oral opioids. There is a risk that these patients will crush the tablets and use them intravenously, which can result in infectious and thrombotic complications.
• Recurrent abdominal pain and vomiting: Consider opioid withdrawal or Hyperemesis Cannabinoid Syndrome
• Tell patients to discard unused pills to pharmacy especially if they have adolescents living with them.
• Never let your patient tell you how to prescribe a dangerous drug

Acute Pain (Opioid naïve and tolerant)
• 3 day supply of low dose, short-acting opioids (10-20 tablets)
• Avoid acetaminophen containing opioids
• Yes…..Tramadol is a mu agonist
2015-2016 30
*SHORT-ACTING OPIOID MORPHINE EQUIVALENCY
ORAL DOSING
Morphine (Caution with renal
insufficiency)5mg 2.5mg 1mg
Codeine (Caution with renal
insufficiency)50mg 25mg 10mg
Hydromorphone 1mg 0.5mg ~0.25mg
Oxycodone 2.5mg 1.25mg 0.5mg
Tramadol (Caution with SSRI) 50mg 25mg ~10mg
• Institute for Clinical Systems Improvement. Acute Pain assessment and Opioid Prescribing Protocol. www.icsi.org. January 2014• CDC: https://www.cdc.gov/drugoverdose/pdf/guidelines_factsheet-a.pdf

Summary
• Opioid use should be about SAFETY NOT moral or ethical reasoning
• Never let a patient tell you how to prescribe a dangerous drug
• Let them know you “care enough” to set boundaries
• Problematic substance use is not addiction
• Opioid addiction is a life threatening complication of opioid use

On line (Youtube) and community resources
• Brainman stops his opioids
• Brainman understands pain in less than 5 minutes
• Never, ever give up. Arthur’s transformation
• TED talk
• Addiction services
• Pain self-management program