Preparedness for Emerging Infections and Bioterrorism:...
102
AVG 1 Preparedness for Emerging Infections and Bioterrorism: Are We There Yet? Adi Gundlapalli, MD, PhD Wasatch Homeless Health Care, Inc. Infectious Diseases University of Utah Hospital & Clinics Salt Lake City, Utah
Transcript of Preparedness for Emerging Infections and Bioterrorism:...
AVG 1
Preparedness for Emerging Infections and Bioterrorism:
Are We There Yet?
Adi Gundlapalli, MD, PhDWasatch Homeless Health Care, Inc.
Infectious DiseasesUniversity of Utah Hospital & Clinics
Salt Lake City, Utah
2AVG
One bright sunny day…
A child is brought in for evaluationFever and URI for 2 daysBy the way…She has a skin rash

3AVG
This is her hand…
Courtesy: Michael Anderson, The New York Times
4AVG
And this is her pet…
5AVG
This is a true story
The New York Times, April 18, 2004 • By Gretchen Reynolds (NYT) 5347 words
Late Edition - Final , Section 6 , Page 32 , Column 1
“Why Were Doctors Afraid to Treat Rebecca McLester?”

6AVG
Unknown Skin Lesion
The worry: smallpox-like lesionsThe problem: who would see her?To find smallpox vaccinated health care workers

7AVG
Unknown Skin Lesion
The child had monkeypox!Transmitted from prairie dogs that came in contact with a sick African rat
In a small town in Illinois

8AVG
Are We Prepared?
Why are we concerned?What are some of those diseases?What can we do?
9AVG
Is There a Problem?http://www.ahrq.gov/clinic/epcindex.htm#healthcare
Training of Clinicians for Public Health Events Relevant to Bioterrorism Preparedness 2001“Modest” evidence: detect and manage infectious disease outbreaksVery little evidence: bioterrorism preparedness

10AVG
Is there a problem?
Provider Perspective“On the Front Lines: Family Physicians’Preparedness for Bioterrorism”
•FM Chen et al, J Fam Pract, 2002:745-750

11AVG
Provider Perspective
Oct 2001: 976 Family Physicians63% response!26% felt preparedTraining would be welcomed
12AVG
Is there a problem?
“Ready and Willing? Physicians’ Sense of Preparedness for Bioterrorism”
•Alexander and Wynia, Health Affairs (Millwood), 2003;22(5):189-97
13AVG
Physician Perspective
526 of 1000 Physicians responded21% felt prepared80% were willing to do what it takes – even at the risk of becoming ill

14AVG
Is There a Problem?
National Assoc. of Comm. Health Centers, Inc.Nov 2001: HC Preparedness Survey
137 Health Centers
15AVG
Community Health Centers
91%Inadequately prepared for a pubic health emergency involving bioterrorism
84%Identified training as a key component
16AVG
Patient Perspective
Are our patients at risk?Why not?
17AVG
Our patients
No different from other patientsHigher risk sub-categories
Foreign Born (migrant/refugees)• TB: esp. multi-resistant• “Exotic” imported diseases
Homeless
18AVG
Higher Risk?
Delay in seeking care• Care Without Coverage: Too Little Too Late
• IOM Report 2002, National Academy Press
With regard to infectionsMore severe illness before seeking careMay be transmitted to othersOutbreak before you know it!
19AVG
Higher Risk?NACHC Issue Brief #75, July 2003PL 107-188: Public Health Security and BioTPreparedness and Response Act of 2002
Awaiting a report by HHS SecretaryFactors that may make underserved areas more vulnerable to biological attacks
20AVG
Most Recent Survey
NACHC 2003: PreparednessResults not published yetNot fully prepared?Better prepared than 2001?

21AVG
So…
We are not fully preparedOur patients are at risk
22AVG
What are we facing?
Emerging infectionsNatural disease outbreaks
Avian InfluenzaMonkey poxSARSWest Nile VirusMulti-drug resistant TBCommunity Associated MRSA

23AVG
What are we facing?
Agents of Bio-TerrorismCategory A: easiest to transmit
AnthraxBotulismPlagueSmallpoxTularemiaViral Hemorrhagic fevers
24AVG
Recognition of agents
Easier said than doneEmerging infections & Bio-T agents
Similar presentationClusters of illness?
25AVG
Recognition
Nothing specificGeneral symptom complex
Most have respiratory componentMany have fever and rash
26AVG
Non-outbreak Situation
We will all miss the first few casesBe aware of clusters of illnessAre you seeing more than one patient with similar illnesses?Are others noting the same?
27AVG
Non-Outbreak Situation
Anything common among patients?Exposure?
Same householdSame animalSame substanceSick contactSame travel
28AVG
Outbreak Situation
Heightened awarenessKnow what is circulating in your communityGlobal Village
Your local health districtYour stateYour countryWorld
29AVG
Epidemiologic Clues
Travel HistorySARSTBMeasles (airplane)
Any sick contactsSARSTB
30AVG
Epidemiologic Clues
Any contact with animalsTularemiaPlagueMonkeypoxAvian Influenza
Mosquito exposureWest Nile Virus

31AVG
Some emerging infections
32AVG
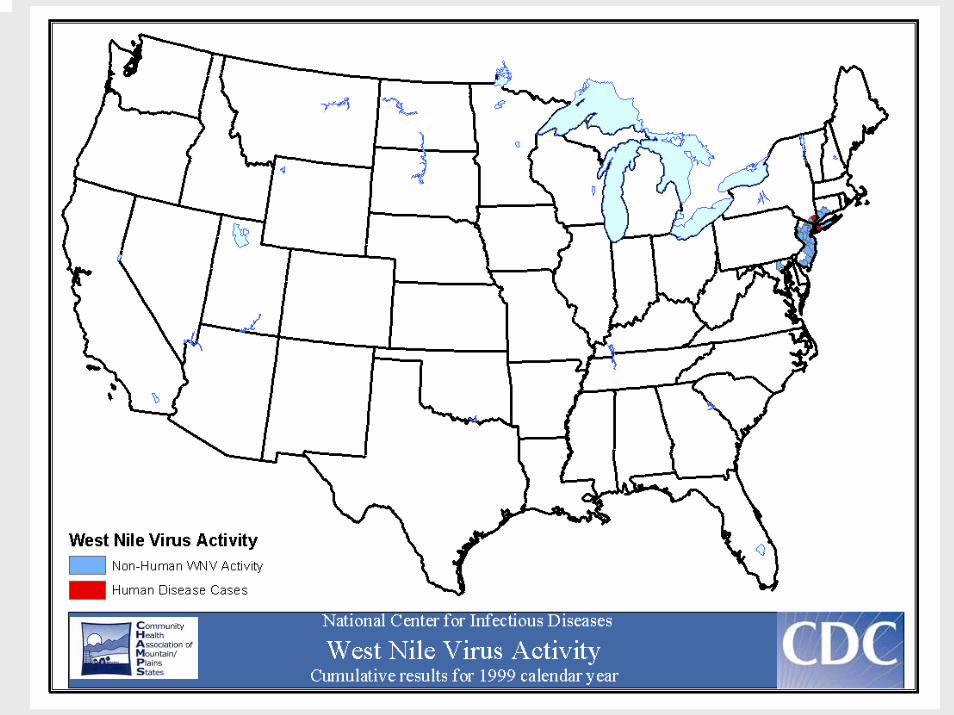
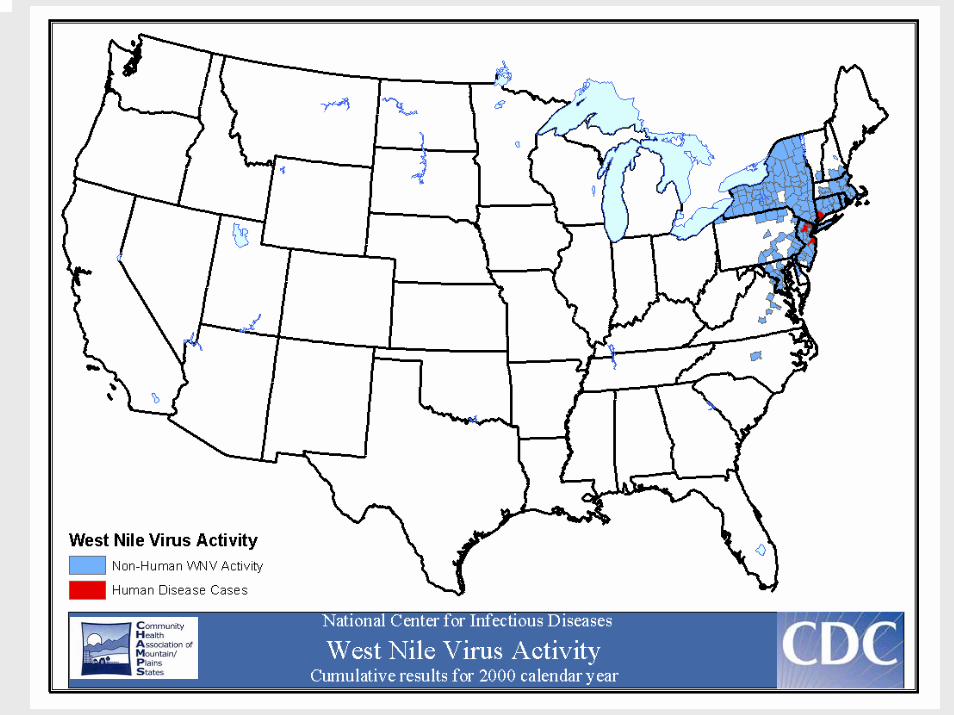
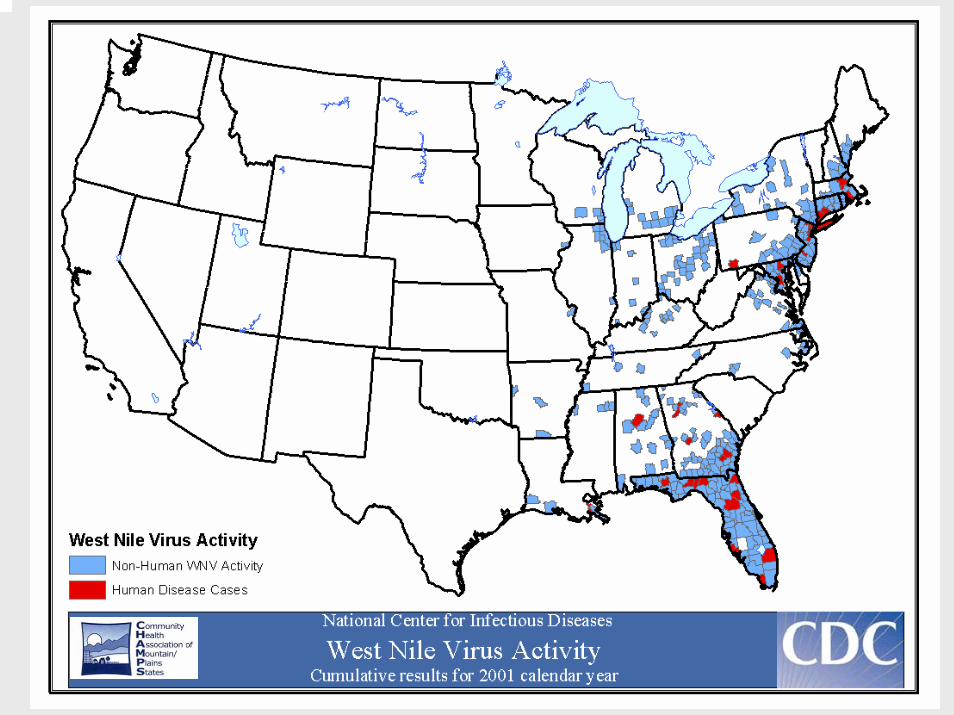
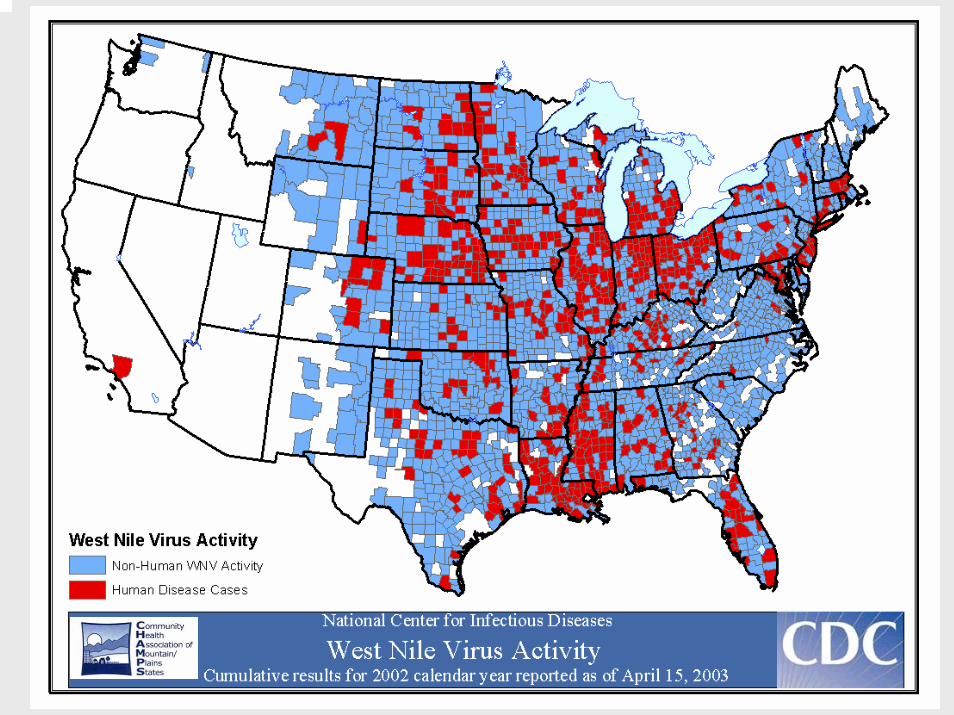
West Nile Virus
1937: Uganda1950s: Egypt and Israel1999: First seen in the USHow did it get here?
33AVG
34AVG
35AVG
36AVG

AVG 37
38AVG
West Nile
How do you get it?
39AVG
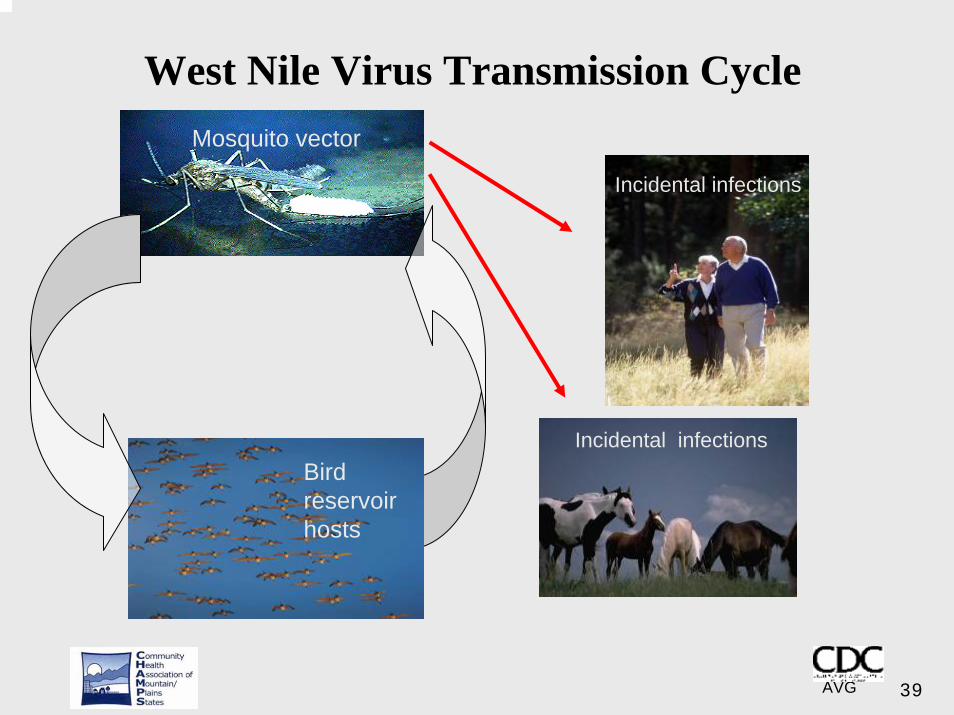
West Nile Virus Transmission CycleMosquito vector
Incidental infections
Bird reservoir hosts
Incidental infections

40AVG
West Nile Virus
Fortunately, most are mild illnessesWest Nile Fever
Acute Febrile Illness• Sudden onset• Malaise, headache, anorexia • Myalgia, nausea and vomiting• Rash, lymphadenopathy, eye pain
41AVG
West Nile
NeurologicalMost dreaded manifestation, 1 in 150EncephalitisMeningitis less commonOther neurological signs• Flaccid paralysis (looks like polio)
42AVG
West Nile
DiagnosisHigh index of suspicion in the summerKnow what is in your backyardAppropriate testing (serum, CSF)

43AVG
West Nile
ManagementSupportiveNo specific treatment
44AVG
Anthrax
Described in history worldwideForms
SkinGastro-intestinalRespiratory system
Inhalation Anthrax (US): 20th cent.
45AVG
Anthrax
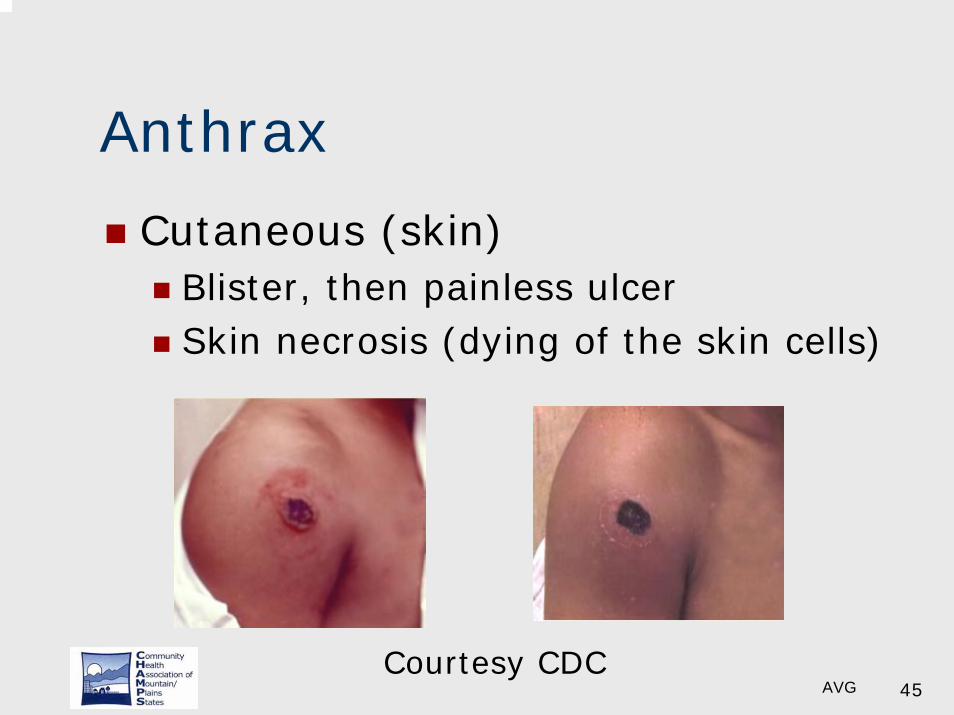
Cutaneous (skin)Blister, then painless ulcerSkin necrosis (dying of the skin cells)
Courtesy CDC
46AVG
Inhalational anthrax
Patients are sickerMortality is highPresents like the fluThen pneumoniaNO PERSON to PERSON SPREAD
47AVG
Diagnosis of anthrax
Microbiology specimensAlert the lab!Seek expert consultation
48AVG
Management
Actually it can be treatedCiprofloxacin, doxycycline, pen GTreatmentProphylaxis for exposed personsThere is a vaccine
Used mostly in the military
49AVG
Monkeypox
1958 : lab monkeys1970:first reported human caseSporadic cases in AfricaSurge after smallpox vaccination was stopped?
Did the vaccine protect?

50AVG
US Monkeypox Outbreak
June 2003In the news: mid-westSick African rats were importedContact with local prairie dogsTransmitted illness to petsThen to humans

51AVG
Monkeypox features
A rather long incubation periodUpto 12 days
Fever, muscle aches, headacheJust like the flu!Lymph node swellingRash a few days later
52AVG
Diagnosis and Management
Diagnosis by suspicion onlyMay look like smallpoxNeeds special diagnostic testsNo specific treatmentSmallpox vaccine for the exposed
The CDC does recommend this
53AVG
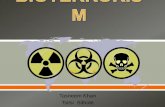
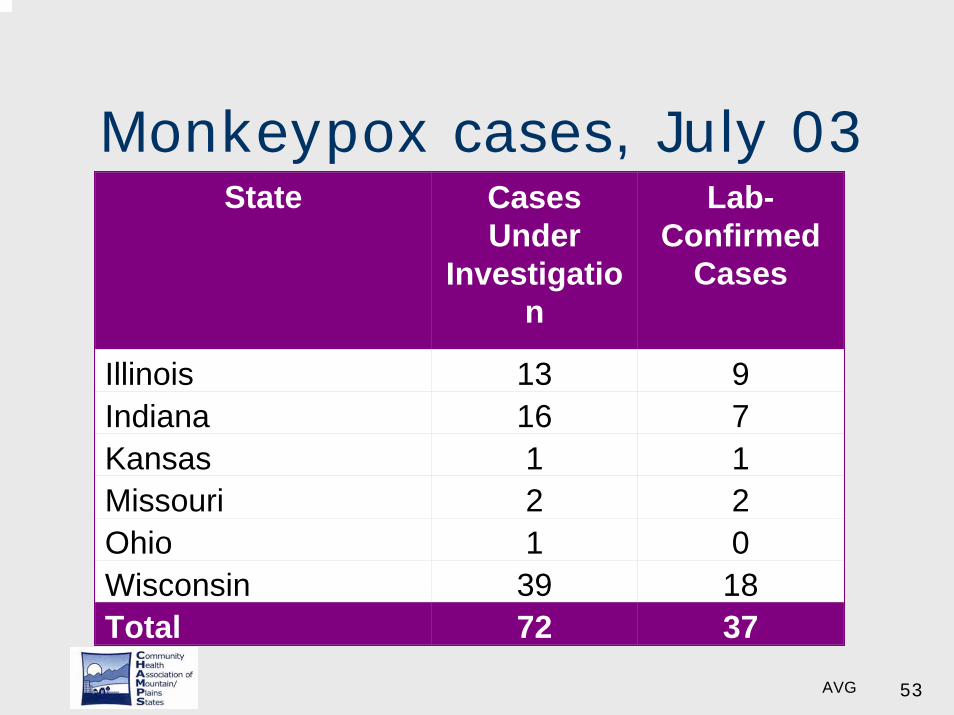
Monkeypox cases, July 03State Cases
Under Investigatio
n
Lab-Confirmed
Cases
Illinois 13 9Indiana 16 7Kansas 1 1Missouri 2 2Ohio 1 0Wisconsin 39 18Total 72 37
54AVG
Monkeypox
Animal to humanPerson to person possible
Large respiratory dropletsClose contact requiredSecretions from skin lesionContaminated bedding/objects
55AVG
SARS
Severe Acute Respiratory SyndromeThis is truly an emerging infectionNot known to exist before 2003Knowledge is still “emerging”Current thinking
Animal reservoirCivet cats in China?
56AVG
SARS
Caused by a coronavirusA mutant cousin of the cold virus!
Highly communicablePerson to personLarge droplet: close contact neededFrom inanimate objects?
57AVG
SARS
2003: 8098 cases with 774 deathsThe US was largely sparedUnlucky: Southeast Asia & Canada2004: Handful of cases
ChinaLab accidents
58AVG
SARS
Presents like the fluNo specific treatmentHighly contagiousWill it become seasonal?
59AVG
What does SARS look like?
InfluenzaAvian influenzaOther viral respiratory illnessesSevere pneumonia
60AVG
Now that we have discussed some diseases…
61AVG
What Constitutes Preparedness?
No right answerSome common denominatorsStart with the Disaster Plan
Everyone has one
Review the communicable disease section

62AVG
Please hold on…
Courtesy AVG Family

63AVG
Now – Here is THE plan you need…

64AVG

65AVG
Not so fast…
66AVG
I can’t write YOUR plan!
We are all the same…Yet differentWe are
Urban Community Health CentersRural Health CentersHomeless HealthMigrant Health

67AVG
We are different
Different trainingDifferent expertiseResources are variableOur disasters are different!
Natural disasters: EarthquakesChemicalNear Port-of-Entry
68AVG
Basic PrinciplesAwarenessTriage areaWaiting room
Can you isolate ill from the well?
Prompt identification of ill patientsCan you take them into a private room?
69AVG
Respiratory Etiquette (CDC)
Basic infection controlSurgical mask for coughing patientsMasks for front office/intake team
70AVG
Other Basics
Personal Protective Equipment (PPE)N95 Mask with fit-testingGowns, gloves, face shields
71AVG
Other Basics
Room cleaningGood disinfectant- hospital grade
Medical Waste DisposalLaundry Facilities

72AVG

73AVG
Now…
We have equipped our clinic and ourselves

74AVG
Increase our awareness
Some suggestionsDisclaimer
These are only suggestionsNot validated yet
75AVG
Syndromic Surveillance
Look for groups of symptoms“Syndrome”Not specific for anythingMAY suggest an illness
76AVG
Syndromic Surveillance
Best Example – ValidatedInfluenza-like illness (ILI) surveillanceLooking for either
Fever AND Cough ORFever AND Sore throat
During flu seasonPatient with ILI most likely has the flu!
77AVG
A Suggestion
Syndromic surveillanceIn the season: Influenza-like illnessOther times:
Fever with Cough and SOBModify for West Nile: fever + HA
Rash with Fever
78AVG
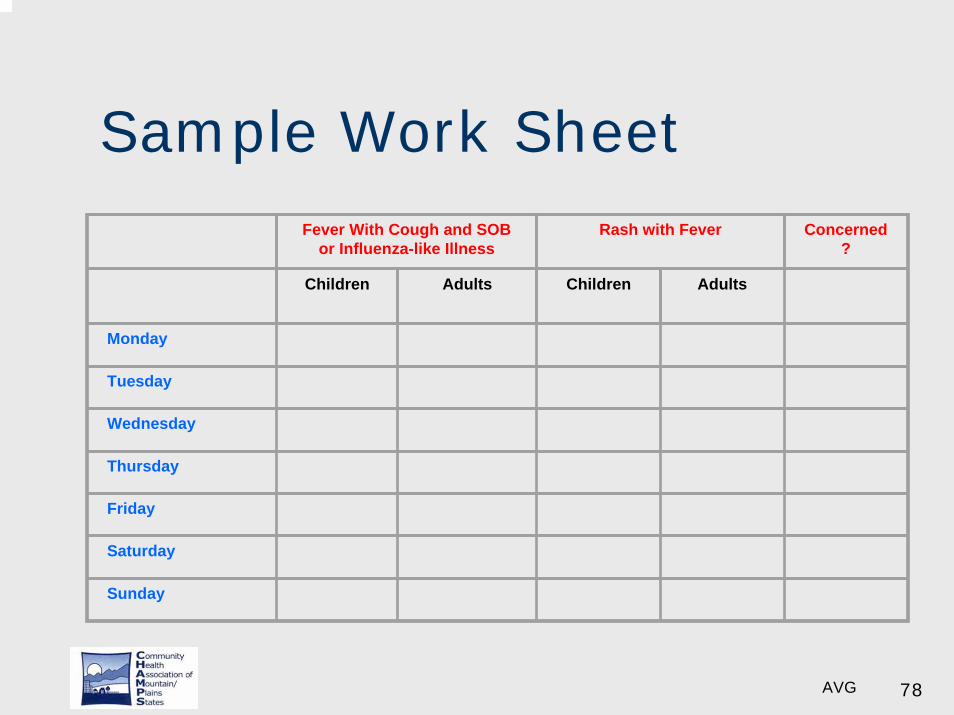
Sample Work SheetFever With Cough and SOB
or Influenza-like IllnessRash with Fever Concerned
?
Children Adults Children Adults
Monday
Tuesday
Wednesday
Thursday
Friday
Saturday
Sunday

79AVG
Sample work sheet
What will this alert you to?Most of the time
The usual suspects!
Influenza in the winterChildhood illnesses
ChickenpoxMeasles
80AVG
When would I use this?
Not all the time!Large outbreak in the world (SARS)Unusual activity in my communityWhen threat level is raised to Orange?
Otherwise we do not do anything differently
81AVG
Seen anything unusual?
Notification Local health departmentTechnical assistance from them
82AVG
Partnerships
Build bridges before the flood!Do you know how to contact
Your local health departmentYour State health department
Do they know you?

83AVG
Partnerships
Do you have consult services?Can you call someone?Where can you refer your patients?
84AVG
Communication is the key
Bi-directionalCurrent information
Accurate and timelyWhere will you get it?• Health departments
You will hear a lot from the mediaRumors/Panic
85AVG
Communication is the key
Information TO public healthYou are their eyes and ears!They depend on you!
86AVG
Challenges
No one size fits all!Basic plan: You all have oneTailor to your specific needs
87AVG
Challenges
RESOURCESTrainingQuick access to
InformationSpecialistsPublic health
Build bridges now
88AVG
Scenario 1: Rebecca
What happened to Rebecca?Emergency smallpox vaccinationAdmitted to isolation roomSupportive careGood outcome
89AVG
Scenario 2
36 year old womanPresents with fever and coughSlowly progressingWalks in to the waiting roomShe is actively coughing
90AVG
Scenario 2
No travel historyNo risk factors for TBBy the way…
91AVG
Scenario 2
Live-in NannyThe employer is also sickThe employer just returned from a business trip to China
92AVG
Scenario 2: Respiratory
What would you do?
93AVG
Scenario 2
You are concernedDifferential includes
SARSInfluenza: avian and humanOther viral diseaseOther bacterial diseaseA new disease?
94AVG
Scenario 2: Respiratory
Mask for patient and providersIsolate in private roomBasics: Is she stable?What does her employer have?Call local HD and local ERWho are her contacts?

95AVG
Acknowledgements
My colleaguesWasatch Homeless Health Care, Inc.University of Utah School of Medicine• Hospital Epidemiology and Inf Diseases
Local Homeless Service ProvidersNorth York General Hospital, Toronto

96AVG
Acknowledgements
CHC ColleaguesKeith Horwood, MD, SLCMel Ray, PA-C, Green River, Utah
Colleagues at CHAMPSGina AstorinoDarci Martinez

97AVG
This is where we work…

98AVGAnd this is where we play…

99AVG

100AVG
Questions and Comments
101AVG
Resources
Local HD and State HD websiteswww.cdc.govhttp://www.bt.cdc.gov/Other government sitesMajor university sitesNational associations (NACHC)
Adi Gundlapalli, MD, PHD
Dr. Gundlapalli is board certified in internal medicine and infectious diseases and has received training in both basic and clinical research. His research interests include issues in infection control, epidemiology of upper respiratory infections, public health surveillance for emerging infections and agents of bioterrorism, and health care for the homeless. He is actively involved in research and teaching at the University of Utah School Of Medicine and has presented his work at national and international meetings. Dr. Gundlapalli has also been invited by several local and national organizations to lecture on topics relating to infectious diseases and public health.
Adi Gundlapalli received his basic medical training in India and graduate training in immunology at the University of Connecticut Health Center in Farmington, CT. He then completed an internal medicine residency at the University of Connecticut and moved to the University of Utah School Of Medicine where he completed a fellowship in infectious diseases and hospital epidemiology. He is currently the medical director of Wasatch Homeless Health Care, Inc. in Salt Lake City, Utah and adjunct assistant professor of medicine at the University of Utah School Of Medicine .