PPPM in Diabetes Care - COnnecting REpositories · 2017. 4. 5. · PPPM in Diabetes Care GERMAN...
12
ABSTRACT PPPM in Diabetes Care GERMAN FEDERATION OF DIABETICS—STATEMENT Hadder M Deutscher Diabetiker Bund (German Federation of Diabetics), Germany Dear Ladies and Gentlemen, As a representative of the German Federation of Diabetics (Deutscher Diabetiker Bund) in North Rhine-Westphalia I would like to communicate from the view of people being involved in the disease diabetes, how and to which scale Predictive, Preventive and Personalised Medicine in Germany has a chance to be integrated into the therapy of diseases. Predictive Medicine The German Federation of Diabetics believes that it is meaningful for people, living under the risk of suffering from a specific disease, to evaluate the risk factors more precisely by means of Predictive Medicine. On the other hand it might be ethically questionable to apply those methods in cases, in which serious consequences (e.g. death) can possibly be expected. For the patients this could be a situation of extraordinary mental stress. In those cases predictive methods or tests should only be applied, if a patient has given an explicit mandate. In our opinion results of such methods of testing should only be communicated to the patient by qualified medical specialists. However, when we are talking about disease patterns, in which a patient’ s behaviour, in combination with a qualified therapy, could avoid a worsening of the disease, the chances of Predictive Medicine should be employed. Prevention Prevention is not only a problem in our public healthcare system but also a problem of our society in general. Despite the fact that every third teenager carries the risk of diabetes there is almost no effort in prevention. This is even worse as genetic, family-related and socio-economic factors play a critical role in the further growing up of the adolescent persons. Hence prevention and working towards a healthy lifestyle should already start on the pre-school level, for example in the kindergarten or play school. The steadily increasing number of children and adolescents suffering from diabetes type 2 is significant. Normally information about the disease diabetes and a healthy lifestyle does not start before the manifestation of the disease took place. Especially for those patients, carrying a high risk, special risk-related measures of prevention should regularly be taken. Personalised Medicine The German Federation of Diabetics expects considerable success when Personalised Medicine is applied in the treatment of serious and/or chronic diseases. In Germany the influence of economic factors on political decisions on health care has been growing. The legislative organs and self-governing bodies impose strict regulations on doctors and therapists, which in most cases only allow standardised treatment. However, from our point of view individual treatment by means of biomarkers provides a lot of advantages: & Insufficient or even wrong treatment and therapies could be avoided & Risks or adverse reactions of pharmaceuticals and therapies could be avoided or limited & With individual treatment from the beginning, unnecessary cost for insufficient or wrong treatment could be eliminated & Patients could be protected from significant complica- tions of the disease and also from cost. POTENTIAL NEW STRATEGIES IN DIABETES THERAPEUTICS Sena CM Institute of Physiology, IBILI, Faculty of Medicine, University of Coimbra, Portugal EPMA Journal (2011) 2 (Suppl 1):S131–S142 DOI 10.1007/s13167-011-0120-z
Transcript of PPPM in Diabetes Care - COnnecting REpositories · 2017. 4. 5. · PPPM in Diabetes Care GERMAN...

ABSTRACT
PPPM in Diabetes Care
GERMAN FEDERATION OF DIABETICS—STATEMENTHadder MDeutscher Diabetiker Bund (German Federation of Diabetics),Germany
Dear Ladies and Gentlemen,
As a representative of the German Federation of Diabetics(Deutscher Diabetiker Bund) in North Rhine-Westphalia Iwould like to communicate from the view of peoplebeing involved in the disease diabetes, how and towhich scale Predictive, Preventive and PersonalisedMedicine in Germany has a chance to be integrated into thetherapy of diseases.
Predictive MedicineThe German Federation of Diabetics believes that it ismeaningful for people, living under the risk of sufferingfrom a specific disease, to evaluate the risk factors moreprecisely by means of Predictive Medicine. On the otherhand it might be ethically questionable to apply thosemethods in cases, in which serious consequences (e.g.death) can possibly be expected. For the patients this couldbe a situation of extraordinary mental stress. In those casespredictive methods or tests should only be applied, if apatient has given an explicit mandate. In our opinion resultsof such methods of testing should only be communicated tothe patient by qualified medical specialists.However, when we are talking about disease patterns, inwhich a patient’s behaviour, in combination with a qualifiedtherapy, could avoid a worsening of the disease, the chancesof Predictive Medicine should be employed.
PreventionPrevention is not only a problem in our public healthcaresystem but also a problem of our society in general. Despitethe fact that every third teenager carries the risk of diabetesthere is almost no effort in prevention. This is even worse
as genetic, family-related and socio-economic factors play acritical role in the further growing up of the adolescentpersons. Hence prevention and working towards a healthylifestyle should already start on the pre-school level, forexample in the kindergarten or play school. The steadilyincreasing number of children and adolescents sufferingfrom diabetes type 2 is significant. Normally informationabout the disease diabetes and a healthy lifestyle does notstart before the manifestation of the disease took place.Especially for those patients, carrying a high risk, specialrisk-related measures of prevention should regularly betaken.
Personalised MedicineThe German Federation of Diabetics expects considerablesuccess when PersonalisedMedicine is applied in the treatmentof serious and/or chronic diseases. In Germany the influence ofeconomic factors on political decisions on health care has beengrowing. The legislative organs and self-governing bodiesimpose strict regulations on doctors and therapists, which inmost cases only allow standardised treatment.However, from our point of view individual treatment bymeans of biomarkers provides a lot of advantages:
& Insufficient or even wrong treatment and therapies couldbe avoided
& Risks or adverse reactions of pharmaceuticals andtherapies could be avoided or limited
& With individual treatment from the beginning, unnecessarycost for insufficient or wrong treatment could be eliminated
& Patients could be protected from significant complica-tions of the disease and also from cost.
POTENTIAL NEW STRATEGIES IN DIABETESTHERAPEUTICSSena CMInstitute of Physiology, IBILI, Faculty of Medicine,University of Coimbra, Portugal
EPMA Journal (2011) 2 (Suppl 1):S131–S142DOI 10.1007/s13167-011-0120-z

The rising incidence of diabetes, metabolic syndrome, andsubsequent vascular diseases is a major public healthproblem in industrialized countries. Diabetes is a progres-sive disease with a complex pathophysiology that includesperipheral insulin resistance, declining β-cell function andmass, declining insulin secretion over time, inappropriateglucagon secretion and hepatic glucose production, anddeficiencies in amylin and glucagon-like peptide (GLP-1).The main pharmacological drugs that have been used inthe treatment of type 2 diabetes are: α-glucosidase
inhibitors, to delay intestinal carbohydrate absorption (e.g. acarbose); biguanides to target hepatic insulin resistance(e.g. metformin); insulin secretagogues or sulphonylureas,to increase pancreatic insulin secretion and also increaseglucose-induced insulin secretion (e.g. glibenclamide;gliclazide); insulin sensitisers or thiazolidinediones, totarget adipocyte and muscle insulin resistance (e.g.troglitazone; rosiglitazone); and intestinal lipase inhibi-tors, to inhibit fat absorption and promote weight loss inobese patients (e.g. orlistat) (Figure).
Observational studies have found that bariatric surgeryis effective in patients with obesity and diabetes,reinstating near normal glycaemia in 50–80% of patientsfor several years. Bariatric surgery is now an acceptedtreatment for obese patients with diabetes. The finding thatglycaemic control is promptly reinstated in most patients withdiabetes when less food passes through the stomach,duodenum, and proximal jejunum—independently of theamount of weight lost—has focused attention on researchinto gastrointestinal factors as a potential source of new drugsfor the treatment of type 2 diabetes. Several gastrointestinalpeptides (includingGLP-1, glucose dependent insulinotrophicpolypeptide, and peptide YY) could provide a basis for newtreatments in patients with obesity and diabetes.DPP-4 inhibitors and GLP-1 agonists stimulate glucose-mediated insulin secretion from pancreatic β cells andsuppress glucagon release; GLP-1 agonists also delaygastric emptying; and amylin agonists suppress gluca-gon release and delay gastric emptying. Combinationtherapy that includes drugs with complementary mech-
anisms of action is most effective and sometimespreferred.There is great potential for developing a new generationof therapeutics that offer better control of diabetes, itsco-morbidities and its complications. This contributionsummarizes current pharmacological approaches to treatdiabetes mellitus and will focus on novel therapies fordiabetes mellitus that are under development. Potentialnew treatments include analogues of intestinal andadipocyte hormones, inhibitors of renal glucose reab-sorption and cellular glucocorticoid activation, andactivators of cellular energy production.
INDICES OF DNA DAMAGE AS POTENTIALPREDICTIVE MARKERS OF DIABETICNEPHROPATHYMozaffari MS, Yao Liu J, El-Awady A, Baban BDepartment of Oral Biology, College of Dental Medicine,Georgia Health Sciences University, Augusta, Georgia 30912,USA
S132 EPMA Journal (2011) 2 (Suppl 1):S131–S142

The world-wide epidemic of obesity has fueled theincreasing incidence of type 2 diabetes mellitus. In turn,type 2 diabetes is associated with major target organcomplications with increased morbidity and mortality.Indeed, nephropathy is a prominent complication of type2 diabetes with end-stage renal failure which requires renaldialysis and/or renal transplantation. It is, therefore,imperative to identify novel diagnostic predictors for earlydetection, and monitoring progression, of target organpathologies such as nephropathy. A hallmark feature oftype 2 diabetes mellitus is hyperglycemia-induced oxidativestress and consequent DNA damage. Thus, identification ofindices of DNA injury that co-relate with disease progres-sion and manifestation of target organ pathologies areurgently needed. While the modified nucleoside, 8-hydroxydeoxyguanosine (8-OHdG), is a useful indexof oxidative DNA damage, γH2AX has emerged has asensitive index of double-strand DNA (dsDNA) breaks,the most severe form of DNA injury. Accordingly, thefocus of our recent studies was to examine the impactof insulin resistance/type 2 diabetes mellitus on urinaryand/or renal tissue 8-OHdG and γH2AX utilizing twohighly relevant animal models of the disease, namelythe obese Zucker rat (OZR) and db/db mouse (andtheir respective lean nondiabetic controls, LZR and db/m, respectively); these animal models lack the leptinreceptor and thus are markedly obese, insulin resistantand hyperglycemic. The OZR displayed mild hypergly-cemia but marked hyperinsulinemia in association withincreased albuminuria compared to the lean controls.Urinary excretion of 8-OHdG was significantly increasedin the OZR compared to LZR. Interestingly, however,renal tissue of OZR revealed similar 8-OHdG immunos-taining intensity and pattern to that of LZR. Subsequentstudies using the severely hyperglycemic obese diabeticdb/db mice revealed significant reduction in glomerularfunction but marked albuminuria than their lean db/mcontrols. Further, urinary excretion of 8-OHdG wasmarkedly increased in db/db, than db/m, group whilerenal tissue 8-OHdG immunostaining was similar be-tween the two groups. On the other hand, renal tissue ofdb/db mice displayed increased nuclear γH2AX immu-nostaining compared to the db/m group. SubsequentWestern blot analysis further confirmed increased renaltissue γH2AX level in db/db mice. Collectively, theresults suggest that while urinary 8-OHdG excretion is ahelpful predictive marker of whole body oxidative DNAdamage, renal tissue 8-OHdG immunostaining is anunlikely predictor of local oxidative DNA damage. Onthe other hand, renal tissue γH2AX is a more likelypredictor of local DNA injury.Supported by a grant from the National Institutes of Health.
RETINOPATHY SCREENING AS THE PROMOTEROFPREDICTIVE, PREVENTIVEANDPERSONALISEDMEDICINE IN TYPE 2 DIABETES CARESalminen LSchool of Medicine, University of Tampere, Finland
More than 75 % of patients who have diabetes mellitus formore than 20 years develop a kind of diabetic retinopathy(DR). In cohort studies, DR is prevented and treatedeffectively by strict control of HbA1c, hypertension andhypercholesterolaemia by lifestyle changes and medication.In clinical practice, DR is one primary endpoint and makerof suboptimal quality of diabetes treatment. DR is a leadingcause of visual impairment in working population. How-ever, diabetes related vision loss is greatest in the elderlywith type 2 diabetes (T2D). Digital fundus photography byaccredited workforce, image grading, quality assurance andIT considerations is the evidence based, sensitive andspecific method for DR screening and follow up. It is oneof the most cost effective health procedures to promotetimely treatment of patients with T2D from a public healthstandpoint.European countries differ considerably in type and qualityof T2D as well as DR prevention and treatments. It isassumed that few countries have been able to increaseresources for eye health since Liverpool Declaration in2005 (www.drscreening2005.org.uk). This contribution isfocused on numerical facts of T2D in Europe with incidenceand prevalence, prevention and care models. Factors likepersonal health practices (exercise, self-care), psychosocial(social support, internal locus of control), and healthcare use(access to care, type of care provided, belief in the ability ofthe healthcare system to help), diabetes registries, massimplication of preventive guidelines and programs, elec-tronic patient records with digital images are identifiedand outlined and road mapped. The unique opportunityof ophthalmologists to influence patient behavior andinform patient’s primary care physician is stressed. It issuggested that information technology and social mediawill play a central role in the redesign of the healthcarequality promoting predictive, preventive and personal-ized medicine for patients with T2D.
VISUAL LOSS IN DIABETIC PATIENTS—DO WEPREVENT IT OR DO WE TREAT ONLYTHE COMPLICATIONS?Josifova T, Henrich PB, Cybulska A, Flammer JUniversity Hospital Basel, Eye Clinic
There are two main reasons of visual loss in patientswith diabetes: diabetic maculopathy (DM) and prolif-erative diabetic retinopathy (PDR). The prevalence of
EPMA Journal (2011) 2 (Suppl 1):S131–S142 S133

PDR and DME is closely related to the duration ofdiabetes. During a life-time more then 50% of patientswith type 2 diabetes develop visual loss, versus 1/3 ofpatients with type 1 diabetes. Correlation betweenblood glucose and presence of PDR, in absence of Cpeptide determination is in close connection to thedevelopment of retinopathy. Two initial therapeuticapproaches are up to date in the treatment of PDR.The aim of the first one is to discourage proliferations,and second—to prevent and relieve the contraction ofthe fibroproliferative vitreoretinal membranes (Fig. 1).Laser photocoagulation (LFK)—retinal burns is still the“golden standard” in prevention and treatment of PDR.Destruction of the new vessels required burns involvethe full thickness retina and often lead to nerve fiberfield defects. Although being treated with LFK, someof the patients develop severe complications andunderwent surgical procedure. Recovery of good visionafter surgery in PDR in the early vitrectomy group isobserved only in 24.5% of the patients. The prevalenceof DM in type 2 diabetes after 5 years duration isabout 5% compared to 20% after 20 years of duration.The classification of DM is: diabetic macular edema(DME), ischaemic maculopathy and vitreomacularinterface changes. Improving the diagnostic techniques,a lot of ongoing studies have investigated differentmedications for intravitreal usage in conditions ofDME (Fig. 2). The grid LFK on the leaking micro-aneurisams in combination with focal LFK is still oneof the important treatments of DME. Up to datemedications include the corticosteroids and Anti-VEGF drugs. A lot of studies such as READ (Resolve,Restore and DRCR.net Study Group) have summarisedthe latest results. Improvement in findings does notalways match to visual acuity increase. The treatment ofthe vitreomacular interface changes is surgical, butwithout great improvement, and the changes are recur-rent. There is no effective treatment for ischemicmacular changes, which are always associated withsevere visual loss. Despite a lot of investigations run,there is still no any protocol elaborated for DMEtreatment.Considering the fact that about 26% of patients with type 1and 36% type 2 diabetic patients have never had their eyesexamined, the risk for different ocular complications is veryhigh: 32% of patients with diabetes at high-risk for visualloss never undergo an eye examination. When examinedalmost 61% of these patients are found to have diabeticretinopathy, cataract, glaucoma or other ocular pathologies.In order to prevent the ocular diabetic complications,
healthcare and eye-care delivery system on a personal-based level should be enhanced in societies. The only keyto success: focusing on “individuals” but not on “patients”with already manifested disorders to apply innovativeinvestigation approaches in the general population andgroups at risk.
ANKLE—BRACHIAL INDEX IN TYPE 2 DIABETESPATIENTS AND CARDIOVASCULAR RISKNussbaumerova B, Rosolova H, Sefrna F, Sipova I, Sifalda P2nd Medical Department, Charles University in Prague—Medical Faculty in Pilsen, Czech Republic
Purpose: The ankle—brachial index (ABI), i.e. the ratio ofsystolic blood pressure (SBP) measured on the ankle and onthe arm, is considered the diagnostic parameter for the
Fig. 1 Fundus foto of a PDR with preretinal haemorrhage
Fig. 2 OCT finding of DME
S134 EPMA Journal (2011) 2 (Suppl 1):S131–S142

peripheral occlusive artery disease and the marker ofcardiovascular (CV) risk. We measured ABI in patients withtype 2 diabetes (DM2) and evaluated its impact on the CVrisk.Method: A sample of 253 DM2 patients (135 males, 118females, average age 66±9 y.) was examined. The supineankle SBP was measured with the Doppler ultrasonographysond after a 5 minutes rest, with the 2 mmHg accuracy, SBPon the identical arm was measured the same way with thesame accuracy by the mercury sphygmomanometer. TheABI<0.9 suggests the arterial occlusion, on the contrary theABI ≥1.2 is nondiagnostic and suspected of mediocalci-nosis. The CV risk was evaluated according to up-to-dateguidelines; as the high risk patients were considered thepatients with manifested CV diseases (information from thepatients’ documentation), with elevated coronary calciumscore (CAC) evaluated by the Agatston’s score (101–400high risk, ≥401 very high risk) or according to the globalCV Risk Score≥5%. Used statistical method: Wilcoxon’sunpaired test, χ2 test, Spearman’s correlation, multiplelogistic regression.Results: The ABI<0.9 was found unilateral in 20 DM2 (8%), bilateral in 27 (11%), thus the ABI was decreased in 47(19%) DM2. Other 168 DM2 (66%) showed the normalABI and 38 (15%) the nondiagnostic ABI. There was nosignificant difference in the characteristics of DM2 patientswith the normal and the nondiagnostic ABI. The DM2patients with the ABI≤0.9 compared to the rest of thesample were older males with elevated total cholesterol,total homocystein and CAC and with the history of CVdiseases. Many CV and metabolic risk factors correlatedsignificantly positively with ABI<0.9: age, glycaemia, totalhomocystein, CAC (p<0.05), LDL-cholesterol (p<0.01)and SBP (p<0.01). The ABI<0.9 was significantly andindependently associated with age (p<0.001), smoking(p<0.01), LDL-cholesterol, total homocystein and CAC(p<0.05). The decreased ABI was a strong significantpredictor of ischemic stroke and symptomatic carotidstenosis for the next 3 years (p<0.001). The ABI<0.9correlated significantly neither with ultrasensitive C-reactiveprotein nor with presence of the metabolic syndrome inDM2.Conclusion: Decreased ABI<0.9 was found in 19% of DM2patients. It was in a significant and independent associationwith age, smoking, LDL-cholesterol, total homocystein andCAC.We evaluatedABI<0.9 as a strong predictor of ischemicstroke and symptomatic carotid artery stenosis. That is whythese patients need an individual, complex and intensiveintervention. Nondiagnostic ABI values were found in 15% ofthe sample; a high prevalence of mediocalcinosis in DM2patients is suspected.
CHARACTERISTICS OF INFLAMMATION COMMONTO BOTH DIABETES AND PERIODONTITIS:ARE PREDICTIVE DIAGNOSIS AND TARGETEDPREVENTIVE MEASURES POSSIBLE?Krishna R1, Hanes PJ21Department of Periodontics, Georgia Health SciencesUniversity, College of Dental Medicine, Augusta, GA30912, USA2Academic Affairs, Georgia Health Sciences University,College of Dental Medicine, Augusta, GA 30912, USA
In 2001, an NIH workgroup standardized the definition of abiomarker as “a characteristic that is objectively measured andevaluated as an indicator of normal biological processes,pathogenic processes, or pharmacologic responses to a thera-peutic intervention”.Diabetes has several effects on the oral cavity includingxerostomia, burning mouth, altered wound healing, andincreased incidence of periodontal diseases such as gingi-vitis and periodontitis. Diabetes and periodontitis arechronic inflammatory disorders that contribute to eachothers’ severity and worsen each others’ prognosis. Studieshave shown that patients with diabetes are at increased riskof developing periodontitis, and that diabetics with untreat-ed periodontitis have more difficulty controlling serumglucose. Although the primary etiology of periodontaldisease is the bacterial biofilm that is present on the surfaceof the teeth, 50% of the tissue destruction is attributed tohost response.Epidemiologic studies have shown a three to fourfoldincreased risk for progressive periodontal destruction indiabetic patients compared with individuals without diabe-tes. The factors suggested to explain this relationshipinclude altered immunoinflammatory response to bacterialpathogens, diminution of the formative aspects of connec-tive tissue metabolism, impaired wound healing, microvas-cular changes, and formation of advanced glycation end-products. Periodontal treatment that reduces gingivalinflammation aids in the control of hyperglycemia.Immune cell functions such as adherence, chemotaxisand phagocytosis, and monocytes/macrophage cell linethat is hyper-responsive to bacterial antigens resulting inincreased production of pro-inflammatory cytokines IL-1βand TNF-α.Periodontitis is accompanied by gingival bleeding and theproduction of an inflammatory exudate termed gingivalcrevicular fluid (GCF) that arises from the inflamedgingival tissues surrounding the teeth. GCF containsbyproducts of connective tissue degradation, enzymesfrom host and bacterial cells, cytokines and other
EPMA Journal (2011) 2 (Suppl 1):S131–S142 S135

inflammatory mediators, and has been studied for screen-ing blood glucose and for biomarkers of both diabetes andperiodontitis. Studies conducted to date suggest thatgingival crevicular fluid may be an acceptable substitutefor “finger stick” blood for determination of serumglucose levels and may therefore be a useful screeningtool in the dental office. Although the ideal immune-inflammatory biomarker is yet to be found, some of thepromising cytokines expressed in the GCF that areelevated in both periodontitis and diabetes include IL-1β, IL-6, PGE2, and VEGF. Further research is necessaryto clarify the usefulness of these potential biomarkers andto likewise investigate additional cytokines which have tobe studied in this regard.
ENDOTHELIAL DYSFUNCTION IN DIABETES:POTENTIAL APPLICATION OF CIRCULATINGMARKERS AS ADVANCED DIAGNOSTICAND PROGNOSTIC TOOLSAbebe W, Mozaffari MSDepartment of Oral Biology, College of Dental Medicine,Georgia Health Sciences University, Augusta, Georgia,USA
Diabetes mellitus is a common chronic metabolicdisease with a growing prevalence rate worldwide. Itis associated with vascular disorders, which contributeto as high as 80% of the 3.2 million annual deathsattributed to complications of diabetes. Endothelialdysfunction plays a crucial and an initiating role invascular disorders in both type 1 and type 2 diabetesand insulin resistance/prediabetes. In the majority ofdiabetic cases, it precedes the development of overthyperglycemia and its consequent complications.Assessing the status of the endothelium can serve as avaluable early diagnostic and prognostic tool forvascular diseases in diabetes. In human subjects,endothelial function/dysfunction has been evaluatedusing several in vivo techniques based on the measure-ment of the functional consequences of endothelialactivity (i.e., relaxation/lumen size alterations in bloodvessels). The commonly utilized techniques in thisFig. 2 Gingival Crevicular fluid flow in a periodontal pocket
Fig. 3 Clinical presentation of periodontitis in patient with undiag-nosed diabetes mellitus (type 1). History of multiple recurringperiodontal abscesses
Fig. 1 Histology of periodontitis lesion. Bacteria-induced inflammation hasresulted in loss of connective tissue attachment to the tooth, epithelialmigration, pocket formation, and loss of supporting bone.
S136 EPMA Journal (2011) 2 (Suppl 1):S131–S142

regard are plethysmography, ultrasound and/or dopplerdesigned to measure blood flow or lumen size incoronary arteries and peripheral blood vessels (e.g.,brachial arteries). While these techniques are used primarily forresearch purposes, some of them appear to be clinicallyrelevant for a limited scope of endothelial evaluations.However, certain limitations associated with the methods,particularly as related to technical difficulties and costs, haveprecluded their routine clinical applications.Recently, a number of endothelial-derived circulatingmarkers have been found to more directly indicate thestatus of the endothelium. The measurement of thesebiomarkers in the circulation is relatively easier and lesscostly. These potential circulating indicators include vonWillebrand factor, soluble thrombomodulin, soluble E-selectin, asymmetric dimethylarginine, tissue plasminogenactivator and endothelial microparticles. While the relativeimportance of each substance (or their combinations) forendothelial evaluation is not clearly defined, in most cases,the determination of these biomarkers has provided goodindications of endothelial damage/activation, as it occurs indiabetes. However, the validity of measuring these bio-markers for diagnosis and/or prognosis of endothelialdysfunction and the associated vascular disorders indiabetes has not yet been fully established for routineclinical applications. Other potential indicators of endothe-lial function/dysfunction in diabetes are circulating endo-thelial cells and circulating endothelial progenitor cells.However, only very few studies have investigated theclinical application of these cellular biomarkers, suggestingthe limited availability of information on their usefulnessfor diagnostic and/or prognostic purposes in humanpatients. Taken together, currently, the issue of circulatingendothelial markers is an area of intense research interestwith the potential to result in the development of clinicallyrelevant assessment techniques of the status of theendothelium and the vasculature. It is hoped that as moreresearch data become available, improved measurement ofcirculating endothelial indicators will make it possible toobtain valuable diagnostic and prognostic information onvascular events in diabetes and related conditions forroutine clinical testing.
INFLAMMATORY MARKERS AS POTENTIALPREDICTIVE INDICATORS FOR DIABETICNEPHROPATHYBaban B, El-Awady A, Yao Liu J, Mozaffari MSDepartment of Oral Biology, College of Dental Medicine,Georgia Health Sciences University, Augusta, Georgia30912, USA
Inflammatory pathways have emerged as major contributingmechanisms to the pathogenesis of insulin resistance/obesity/type 2 diabetes mellitus and associated chronic compli-cations such as nephropathy. Thus, indices of inflam-mation that co-relate with disease progression couldserve as potential predictive markers for the manifesta-tion of target organ pathologies. Accordingly, the focusof our recent studies was to determine the impact ofinsulin resistance/type 2 diabetes on urinary, renal tissueand/or blood levels of inflammatory markers. For thesestudies we used two highly relevant animal models ofthe disease, namely the obese Zucker rat (OZR) and db/db mouse (and their respective lean nondiabetic con-trols, LZR and db/m, respectively); OZR and db/dbmice lack the leptin receptor and thus are markedlyobese, insulin resistant and hyperglycemic. The OZRdisplayed mild hyperglycemia but marked hyperinsulinemiain association with changes in urinary excretion and renaltissue levels of inflammatory markers including a) increasedurinary monocyte chemoattractant protein-1 excretion and b)increased renal tissue levels of cyclooxygenase-2 and inter-cellular adhesion molecule-1 and c) increased renal tissueCD68 immunostaining. Subsequent studies using the severelyhyperglycemic db/db mice revealed significant reduction inglomerular function but marked albuminuria compared to theirlean db/m controls. Immunohistochemical studies revealedincreased expression of interleukin (IL)-6 and IL-17 in renaltubules of db/db compared to their db/m controls. Flowcytometry studies further confirmed pro-inflammatory changesin db/db mice as indicated by increased IL-17 positive cells inperipheral blood and renal cells of db/db than db/m mice; thestatus of IL-23 is currently under investigation. Collectively,the results indicate that urinary and/or tissue as well as bloodinflammatory markers can serve as potential predictiveindicators for progression of type 2 diabetic nephropathy.Supported, in part, by a grant from the National Institutes ofHealth.
DRUG DELIVERY SYSTEMS: ADVANCEDTECHNOLOGIES POTENTIALLYAPPLICABLEIN PERSONALIZED TREATMENTSCoelho JF, Ferreira PC, Alves P, Cordeiro R, Fonseca AC,Góis JR, Gil MHDepartment of Chemical Engineering, University of Coim-bra, 3030–290 Coimbra, Portugal
Advanced drug delivery systems (DDS) present indubitablebenefits for drug administration. Over the past threedecades, new approaches have been suggested for thedevelopment of novel carriers for drug delivery. In this
EPMA Journal (2011) 2 (Suppl 1):S131–S142 S137

presentation, general concepts and emerging research in thisfield based on multidisciplinary approaches aiming tocreate personalized treatment for a broad range of highlyprevalent diseases (e.g., cancer and diabetes) will bepresented. The information presented is organized in twoparts. The first part provides an overview on currentlyavailable drug delivery technologies including a briefhistory on the development of these systems and some of
the research strategies applied. The second part providesinformation about the most advanced drug delivery devicesusing stimuli responsive polymers. Their synthesis usingcontrolled-living radical polymerization strategy is pre-sented. In a near future it is predictable the appearance ofnew effective tailor-made DDS, resulting from knowledgeof different interdisciplinary sciences, in a perspective ofcreating personalized medical solutions.
CANCER PREDISPOSITION IN DIABETICS: RISKFACTORS CONSIDERED FOR PREDICTIVEDIAGNOSTICS AND TARGETED PREVENTIVEMEASURESCebioglu M, Schild HH, Golubnitschaja ODepartment of Radiology, Rheinische Friedrich-Wilhelms-University of Bonn, Bonn, Germany
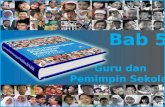
Cancer-related mortality in diabetics
According to the current worldwide statistics, every 10seconds one patient dies on Diabetes mellitus (DM) relatedconsequences. Once appeared, cancer outcomes have worseprognosis for diabetics compared to non-diabetic oncologicpatients (Figure 1).
73.191.2
1.48 1.44
1.43 1.30
1.20 1.24
0.99 1.25
1.05 1.11
1.07 0.90
0.82 1.12
1.27
1.02
0 0.5 1 1.5 2 2.5 3 3.5 4
liver
pancreas
bladder
colon
stomach
lung
rectal
kidney
breast
ovarian
Incr
ease
d m
orta
lity
Men
Women
Fig. 1. Increased mortality of diabetics versus non-diabetics for single cancer types as documented for patients treated in USA in years 1982–1998. Data taken from [1]
Fig—Overview of the polymers used in DDS
S138 EPMA Journal (2011) 2 (Suppl 1):S131–S142

The overall concept of cancer—predispositionin diabetics
Diabetics may be highly predisposed to cancer develop-ment specifically due to following contributors:
– strong stress factors (excessive metabolic alterations,disturbed glucose/insulin homeostasis, hormonal deregu-lation, insufficient detoxification) with consequentlyexcessive production of ROS.
– mitochondrial dysfunction with consequent low energyproduction, insufficient repair capacity and accumu-lating damage to both chromosomal and mitochondrialDNA.
– high risk for infectious disorders with consequentlyinduced viral proto-oncogenic activity as well asactivity of particular pathogenic bacterial forms suchas Helicobacter pylori.
Adequacy of stress response, repair capacity as well asimmune defence are highly individual for each patient andstrongly depend on risk factors such as genetic background,age, environmental factors, nutrition, body culture, lifestyle, etc.
OutlookCurrent biotechnology possesses sufficient power to estimatea severity of damage to sub-cellular structures, individualstress reactions and repair capacity. For example, bystress proteome profiling in peripheral leukocytes andblood plasma, individual stress reactions can be wellestimated. Advanced predictive diagnostic approachesare currently close to clinical application and allow toselect groups of risk and to estimate a predisposition tosevere complications in diabetics. Much attention shouldbe focused on targeted preventive arrangements indiabetes care, in order to restrict or even avoid severesecondary complications, such as cancer.
References
1. Cebioglu M, Schild HH, Lolubnitschaja O. Cancer predisposition indiabetics: risk factors considered for predictive diagnostics andtargeted preventive measures. EPMA J. 2010;1:130–7.
BARIATRIC MEDICINE: MULTIDISCIPLINARYAPPROACH FOR OBESITY PREVENTIONDimitrov DVMedical University Varna, Varna, Bulgaria
Obesity and its associated diseases are epidemic thatrepresent a major threat to human health. In the last twodecades an explosive increase in the number of people
diagnosed with diabetes has been observed worldwide andthe global figure of affected individuals is expected to risefrom currently 250 million to 350 million in 2025. Therapidly escalating number of affected patients at even veryyoung age poses a tremendous burden on the public healthsystem and a substantial reinforcement of research activitiesincluding transnational cooperation between scientists fromdifferent disciplines is urgently required to avoid asocioeconomic disaster. Dietary interventions and pharma-cological strategies, however, failed to deliver success, dueto side effects (e.g. sibutramine, rimonabant) or lack ofefficacy (e.g. lorcaserin, recombinant leptin). For patientswith obesity and type 2 diabetes, bariatric surgery is by farthe most effective treatment—it is, indeed, the only form oftreatment that can put patients into full long-term remission.This contribution reviews rise and fall of anti-obesitytreatments and highlights the importance of bariatricsurgery as the only way to cut diabetes costs at present.We discuss also public health implications. Until asuccessful non-surgical means for preventing and reversingobesity is developed, bariatric surgery appears to be theonly intervention that can result in a sustained reversal ofboth obesity and type 2 diabetes mellitus in most patientsreceiving it. One of the key recommendations is the needfor a multidisciplinary bariatric team to oversee the ongoingneeds of patients after surgery, as well as to build a weightmaintenance program. Beside surgeon, such bariatricmedicine team should include metabolic physicians,nutritionists, physical activities specialists, cardiologists, etc.
MSCS AS TOOLS FOR RESTORINGMORPHOFUNCTIONAL DEFICIENCYAND MODULATING IMMUNE RESPONSESAT THE PRECLINICAL STAGE OF T1D:MILESTONES AND HANDICAPSKostyushev DS1, Paltsev MA2, Suchkov SV1,3
1I.M. Sechenov First Moscow State Medical University,Moscow, Russia2National Research Center “Kurchatov Institute”, Moscow,Russia3Moscow State Medical Dentistry University, Moscow,Russia
Type 1 Diabetes (T1D) is a progressive autoimmunedisease associated with reduction of beta cell mass and,as a consequence, metabolic disturbances in peripheralblood glucose levels. Early diagnosis of T1D at the pre-diabetic stage allows for timely implementation ofefficient preventive and predictive measures includingcell-based technologies aimed at stabilization of thepatient’s immune status and reseeding the pancreas withnewly formed beta cells. Mesenchymal Stem Cells
EPMA Journal (2011) 2 (Suppl 1):S131–S142 S139

(MSCs) are among the most promising therapeutic toolsfor repairing the architectonics of the pancreas throughsecretion of a vast majority of paracrine factors ordirected trans-differentiation into beta cells. In addition,MSCs improve immune responses by acting upon the T celllink of immunity (increasing the population of CD4+CD25+FoxP3+ Tregs and Th2 and decreasing the population ofTh1), prevent the presentation of antigens by expressingnegative co-stimulatory molecules (PD-L1, PD-L2),induce revascularization of the pancreas and affordeffective anti-apoptotic protection of beta cells. Themost promising approaches to isolation of MSCs, theirtargeted delivery by directed homing, effects of secretedsoluble factors on pancreas regeneration and ways toincrease the proliferative activity of MSCs throughinduction of expression of a vast array of humoralfactors are considered. The totality of experimental dataon tumorogenesis in animal models after MSCs injec-tion is discussed in terms of their significance andpossibility of their extrapolation to human beings. Thiscontribution deals with the most promising approachesto preventing malignant growth in human beingsfollowing MSCs injection.
POLYMORPHIC GENETIC MARKERSARE OF SIGNIFICANCE FOR MONITORINGOF DISEASE PROGRESSION IN METABOLICSYNDROME PATIENTSVoytovich AN 1, Bogdanova MA1, Romashkina OS1, BystrovaAA2, Smirnov BI 3, Smirnov AM4, Demin GS 4, KrasilnikovaEI 2, Berkovich OA2, Shliakhto EV 2, Larionova VI11St. Petersburg State Pediatric Medical Academy, Saint-Petersburg, Russia2St. Petersburg State Pavlov Medical University, Saint-Petersburg, Russia3St. Petersburg State Electrotechnical University, Saint-Petersburg, Russia4Gene Ltd, Saint-Petersburg, Russia
Background: The metabolic syndrome (MS) is a cluster ofmetabolic abnormalities, such as abdominal obesity, arterialhypertension, and atherogenic dyslipidaemia, which areassociated with development of secondary complicationssuch as type 2 diabetes (DM2). Recently, many studiesshowed pathology-specific polymorphisms in apolipopro-tein genes that might be associated with the development ofDM2.Objective: To study a possible association of severalpolymorphisms of apo-genes APOA1 G-75A, APOA1C83T, APOC3 Sst1, APOE epsilon, APOA5 T-1131C, andAPOA5 S19W with DM2 in MS patients.
Study population: MS patients with DM2, including 100males and 264 females, average age 50.9±0.5, andcontrols, including 114 healthy males (average age 40.0±0.5)and 84 females (average age 85.9±0.5). All of themwere examined clinically, biochemically and genetically.Results: Among male MS patients with DM2, there was ahigher rate of carries of APOE e2-allele compared to thecontrols (22% vs. 13%, p=0.067). In addition, malepatients demonstrated a higher rate of carries of APOA519W-allele compared to the controls (13% vs. 3%, p=0.005). There was not a significant difference in genotypedistribution of the studied apo-genes between femalegroups. All studied groups were shown to correspond toHardy-Weinberg equilibrium.Conclusion: Gender (male) is considered as a risk factor ina diseases progression. Our results suggest that the APOEand APOA5 S19W polymorphisms are of significance inmale patients with DM2.
ASSOCIATION OF ACE I AND FABP2 GENESPOLYMORPHISM IN CASES WITH TYPE-2DIABETES MELLITUS IN NORTHERN INDIAMahdi F1, Banerjee D1, Rizvi N3, Sapkota R2, Saxena S3,Khan NA2, Raza ST11Era’s Lucknow Medical College & Hospital, Lucknow, India.2Baba Farid Institute of Technology, Dehradun, India.3Amity Institute of Biotechnology, Amity University,Lucknow, India
Background: India has the world’s largest diabetespopulation with an estimated 50.8 million people livingwith type 2 Diabetes Mellitus. Type 2 DM can shortenthe normal lifespan of an individual by up to one-fifthand is a complex disorder accounting for 90–95% of alldiabetes syndromes. Diabetes mellitus has a majorimpact on the cardiovascular and renal system, withthe main cause of death being directly related tocardiovascular disease.Angiotensin Converting Enzyme (ACE I), a key enzyme inthe renin-agiotensin system, is a zinc metallopeptidase,which catalyses the conversion of Angiotensin I toAngiotensin II, a potent vasoconstrictor, and throughprotease activity it also inactivates bradykinin, a potentvasodilator. Insertion/deletion (I/D) polymorphism of a287 bp Alu repeat sequence in intron 16 of the ACE geneis strongly associated with plasma and cellular ACE levelsand it indicates that the polymorphism may modulate theexpression of the ACE gene.Fatty acid–binding protein (FABP2) is involved in thetransport and metabolism of saturated and unsaturated long-chain fatty acids. The FABP2 gene has been proposed as a
S140 EPMA Journal (2011) 2 (Suppl 1):S131–S142

candidate gene for diabetes because the protein it codes foris involved in Fatty Acid absorption and metabolism andtherefore, affect insulin sensitivity and glucose metabolism.The Ala54Thr polymorphism is the most extensivelystudied FABP2 variant, as this variant seems the mostlikely candidate to alter the protein’s function.Material &Methods: Polymerase Chain Reaction—RestrictionFragment Length Polymorphism (PCR-RFLP) andGenotypingwas done to determine the ACE and FABP2 genepolymorphism in 75 cases and 57 controls.Results: The mean age of cases (n=75) in the study groupwas (48.29±11.89) years while in the control group (n=57)was (31.03±7.38) years. The frequencies of the genotypesDD, ID and II in the T2DM group were 16%, 55% and29% respectively while in the control group these frequen-cies were 20%, 78% and 2 %. The frequency of I and Dallele in the T2DM patients group was 57% and 43%respectively as compared to 51% and 49% in the controls.I/D genotype were significantly more frequent in healthycontrols while I/I genotype occurred with significantlymore frequency in patients with T2DM.The frequencies ofthe genotypes Ala54Ala, Ala54Thr and Thr54Thr in theT2DM group were 17%, 63% and 20% respectively whilein the control group these frequencies were 23%, 63% and14%. The frequency of Ala54 and Thr54 allele in theT2DM patients group was 48% and 52% respectively ascompared to 54% and 46% in the controls. FABP2 genepolymorphism shows no significant difference in Geno-types and allele frequencies found in cases and controls.Conclusion: It seems that the I/I allele frequency of ACE I/D gene polymorphism was significant in the T2DM casesas compared to controls. While the FABP2 gene polymor-phism shows no significant difference in Genotypes andallele frequencies found in cases and controls. It might berecommended that ACE gene I/D polymorphisms can be agood marker for the early identification of population atrisk of Type 2 diabetes mellitus.
MEASUREMENT OFANGIOGENESIS PROMOTORSAND CYTOKINES CONCENTRATIONSIN INTRAOCULAR FLUID OF PATIENTSWITH PROLIFERATIVE DIABETIC RETINOPATHYFORTREATMENT TAILORING POSSIBILITYVrzalova J, Kozova M, Rusnak S, Ricarova R , Topolcan OImmunoanalytic Laboratory and Eye Department of Uni-versity Hospital and Medical Faculty in Pilsen, E. Benese13, 305 99 Plzen, Czech Republic
Introduction: Proliferative Diabetic Retinopathy (PDR) isthe most common diabetic eye disease. It is caused bypathology-specific changes in the blood vessels of the retina.
It is a leading cause of blindness in adults that can affect bothcentral and peripheral vision. Vision loss can be reduced bytimely diagnosis and treatment. Nowadays ophthalmology isbased on determination of status quo solely by visual controlor imaging techniques. Our aim was to prove the suitability ofmultiplex analysis for measurement of changes of cytokinesand angiogenetic factors in intraocular fluid of patients withproliferative diabetic retinopathy (PDR) and to determine itsclinical applicability for a potential use in ocular medicine.Patient cohort: Patients with proliferative diabetic retinopa-thy, patients with retinal detachment and control group ofpatients before cataract surgery without any ocular pathologywere examined.Methods: Intraocular fluid samples were aspirated fromanterior chamber of patients with PDR.Concentrations of IL8, VEGF, EGF, IL 6, IP10, MCP1,PDGF, Rantes, BDNF, CNTF TGFb1 and IL 10 weremeasured simultaneously in intraocular fluid using multi-plex panel kits from Millipore (USA) and Luminex 100instrument (Luminex corp., USA). Levels of biomarkerswere compared between groups by Wilcoxon test and ROCanalysis was performed.Results: We were able to detect levels of EGF, IL6,VEGF, BDNF, CNTF, IL8, IP10, MCP1, PDGF AA, andTGFb. In PDR patients, VEGF and other angiogenetic factorsand antiangiogenetic factor (IP 10) were found to be higher inintraocular fluid compare to controls. In retinal detachmentpatients, intraoccular levels of inflammatory markers wereobserved to be higher compare to controls.Conclusion: Multiplex analysis enables an easy simulta-neous measurement of multiple markers in a very smallsample volume and so enables the use of biomarkeranalyses in intraocular fluid as a standard method.Support: Study was supported by the study projectNS10251-3.
NUTRITION OF PACIENTS WITH DIABETESMELLITUS TYPE 2 IN RELATION WITHSMOKING ADICTION—SURVEY POST-MONICA2008/2009 IN CZECH REPUBLICGalovcová M, Adámková V, Cífková R, Petržílková Z,Bruthans J, Lánská VDepartment of Preventive Cardiology, Institute for Clinicaland Experimental Medicine, Prague
Introduction: Tobacco smoking is one of the most importantrisk factors for cardiovascular disease (CVD). Smokers have2-fold higher risk of coronary heart disease, 95% contributesto a higher incidence of peripheral arterial disease. Smokingaffects not only alone, but synergistically with other riskfactors that potentiate the overall effect. The combination of
EPMA Journal (2011) 2 (Suppl 1):S131–S142 S141

smoking diabetics is a particular risk factor. However, stopsmoking is not a simple process: the main role plays strongmotivation. Some smokers argue with weight reduction. Aresmoking diabetics really slimmer?Objective: To compare nutritional parameters in smokers andnonsmokers diabetics type 2.Methods: 1% random population sample aged 25–64 yearswas selected from nine districts of the Czech Republic. Theexamination consisted of completing a standard question-naire, obtaining major anthropometric data, repeated bloodpressure measurements, and blood sampling.Results: We examined 3612 persons, whom 250 were type2 diabetics from.The experimental group included 162 (64.8%) male and 88(35.2%) femal diabetics.Therefrom, smokers were 52 (32%) men and 20 (23%)women. The average age of smokers was 54.4 ±8.6 yearsand 56.6 ±7.0 years of non-smokers (p<0,05).
SMOKERS NON-SMOKERS P
Age 54.4±8.6 56.6±7.0 *
sBP 136.8±19.6 138.9±20.0 n.s.
dBP 84.3±11.6 82.8±10.2 n.s.
BMI 31.8±6.1 33.1±5.8 n.s.
Waist 105.9±14.6 108.0±13.6 n.s.
TC 5.0±1.2 5.2±1.4 n.s.
TAG 2.4±1.6 2.4±1.9 n.s.
HDL-chol. 1.2±0.4 1.2±0.3 n.s.
LDL-chol. 2.8±1.0 3.0±1.1 n.s.
Glucose 8.6±3.0 9.1±3.0 n.s.
We found no indication that smoking diabetics have smallerBMI and waist. However, both groups demonstrated poorlycontrolled diabetes and higher blood pressure compared tonon-smoking diabetics.
S142 EPMA Journal (2011) 2 (Suppl 1):S131–S142