Polypill for primary and secondary preventions of cardiovascular
23
POLYPILL FOR PRIMARY AND SECONDARY PREVENTIONS OF CARDIOVASCULAR MORBIDITY AND MORTALITY 1 Dr. Bhaswat S. Chakraborty Sr. VP & Chair, R&D Core Committee Cadila Pharmaceuticals Ltd. Presented at the IACS Conference 'Translational Research in Cardiovascular Sciences” Anand, Gujarat, February 5-6, 2016
-
Upload
bhaswat-chakraborty -
Category
Health & Medicine
-
view
595 -
download
0
Transcript of Polypill for primary and secondary preventions of cardiovascular
POLYPILL FOR PRIMARY AND SECONDARY PREVENTIONS OF CARDIOVASCULAR MORBIDITY AND MORTALITY
1Dr. Bhaswat S. Chakraborty
Sr. VP & Chair, R&D Core Committee
Cadila Pharmaceuticals Ltd.
Presented at the IACS Conference 'Translational Research in Cardiovascular Sciences”
Anand, Gujarat, February 5-6, 2016
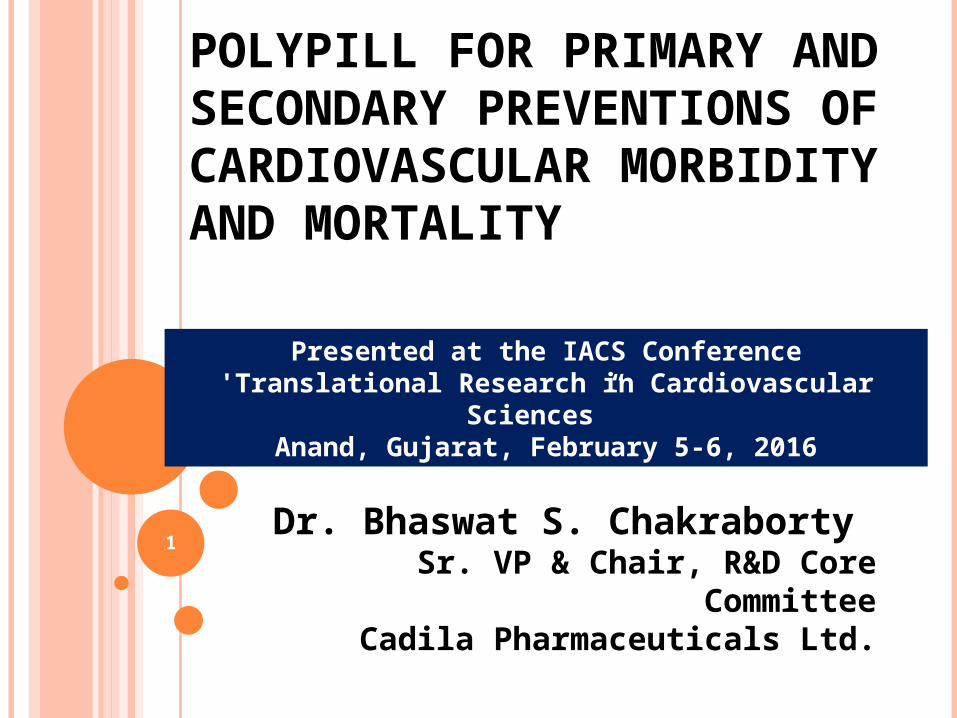
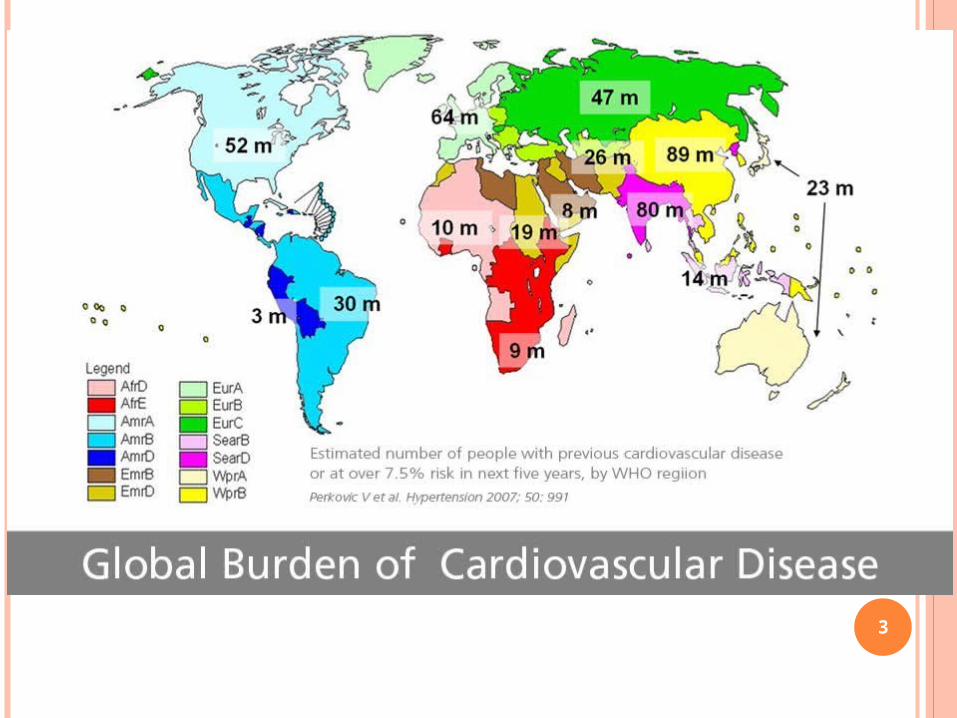
CVDS: CURRENT GLOBAL BURDEN
2
3
CVD RISK FACTORS Cardiovascular risk factors
Non-modifiable: Family history, ethnicity and age Modifiable: Hypertension, high cholesterol, obesity, physical
inactivity, diabetes, unhealthy diets, tobacco, and harmful use of alcohol
Modifiable risk factors Hypertension – biggest risk factor for stroke; significant role in
heart attacks; preventable & treatable Physical inactivity & obesity increases heart disease and stroke
risk by 50%. Type2 diabetes doubles coronary heart disease and stroke risk A diet high in saturated fat increases the risk of heart disease
and stroke Chronically stressful life, social isolation, anxiety and depression Up to 1 or 2 alcohol drinks OK but above this will damage the heart
muscle Certain medicines e.g., contraceptive pill and hormone
replacement therapy (HRT). Left ventricular hypertrophy (LVH)
4
WHAT ARE CVDS? Cardiovascular diseases (CVDs) are a group of disorders
of the heart and blood vessels and they include: Coronary heart disease – disease of the blood vessels
supplying the heart muscle Cerebrovascular disease – disease of the blood vessels
supplying the brain Peripheral arterial disease – disease of blood vessels supplying
the arms and legs Rheumatic heart disease – damage to the heart muscle and
heart valves from rheumatic fever, caused by streptococcal bacteria;
Congenital heart disease – malformations of heart structure existing at birth
Deep vein thrombosis and pulmonary embolism – blood clots in the leg veins, which can dislodge and move to the heart and lungs 5
COMMON SYMPTOMS OF CVDS Symptoms of heart attacks and strokes
Pain or discomfort in the centre of the chest Pain or discomfort in the arms, the left shoulder, elbows, jaw, or back Difficulty or shortness of breath; feeling sick or vomiting; feeling
light-headed or faint; breaking into a cold sweat; and becoming pale Women are more likely to have the above
Symptoms of stroke Sudden weakness of the face, arm, or leg, most often on one side of
the body Numbness of the face, arm, or leg, especially on one side of the body Confusion, difficulty speaking or understanding speech Difficulty seeing with one or both eyes Difficulty walking, dizziness, loss of balance or coordination Severe headache with no known cause Fainting or unconsciousness
6
PRIMARY PREVENTION OF CVDS Population level primary prevention:
Lowering the average risk factors like BP, LDL cholesterol, smoking and obesity in the entire population
Examples of population-wide interventions comprehensive tobacco control policies taxation to reduce the intake of foods that are high in fat,
sugar and salt building walking and cycle paths to increase physical activity strategies to reduce harmful use of alcohol providing healthy school meals to children.
Individual level 1o prevention: targeted those at high total cardiovascular risk or those with single risk factor levels above traditional
thresholds, e.g., hypertension and hypercholesterolemia7
PRIMARY PREVENTION OF CVDS
8
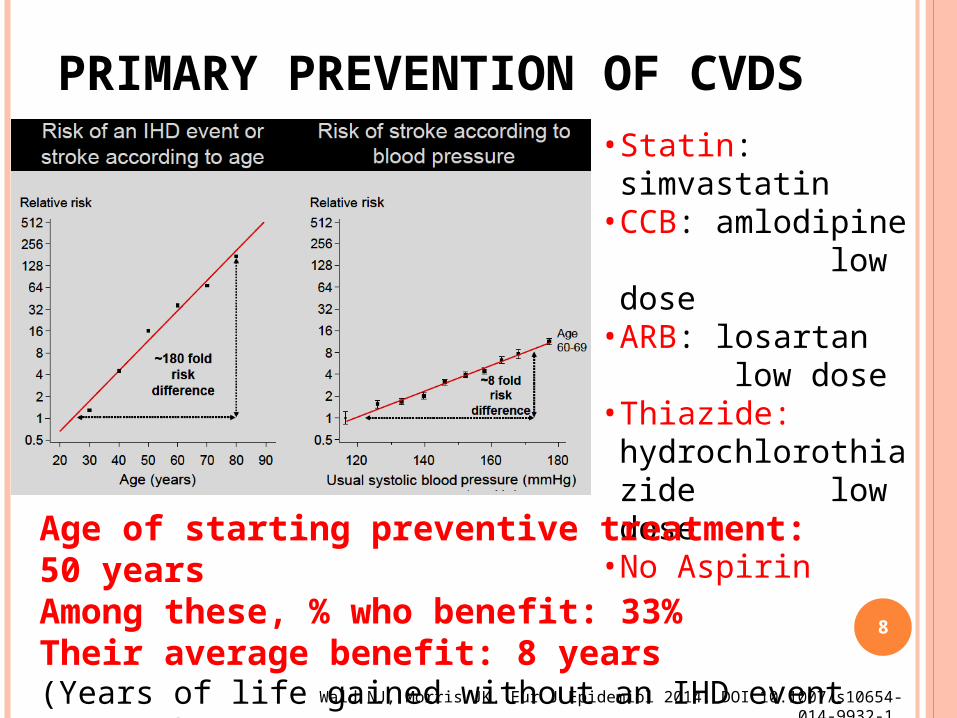
• Statin: simvastatin• CCB: amlodipine
low dose• ARB: losartan
low dose • Thiazide: hydrochlorothiazide low dose • No Aspirin
Wald NJ, Morris JK. Eur J Epidemiol 2014. DOI 10.1007/s10654-014-9932-1
Age of starting preventive treatment: 50 years Among these, % who benefit: 33% Their average benefit: 8 years (Years of life gained without an IHD event or stroke.)
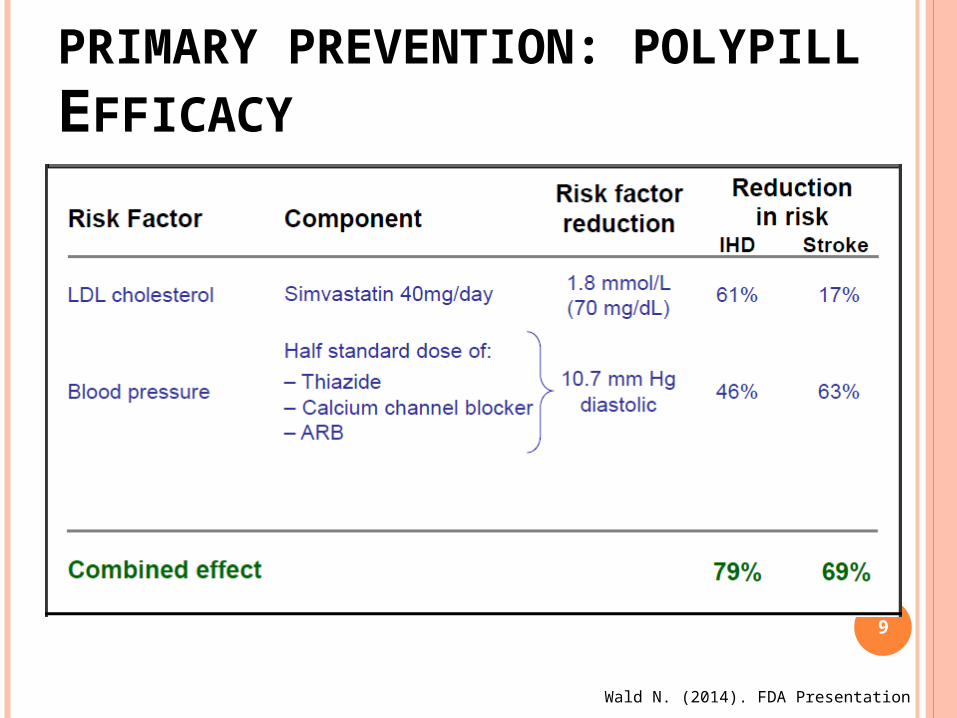
PRIMARY PREVENTION: POLYPILL EFFICACY
9
Wald N. (2014). FDA Presentation
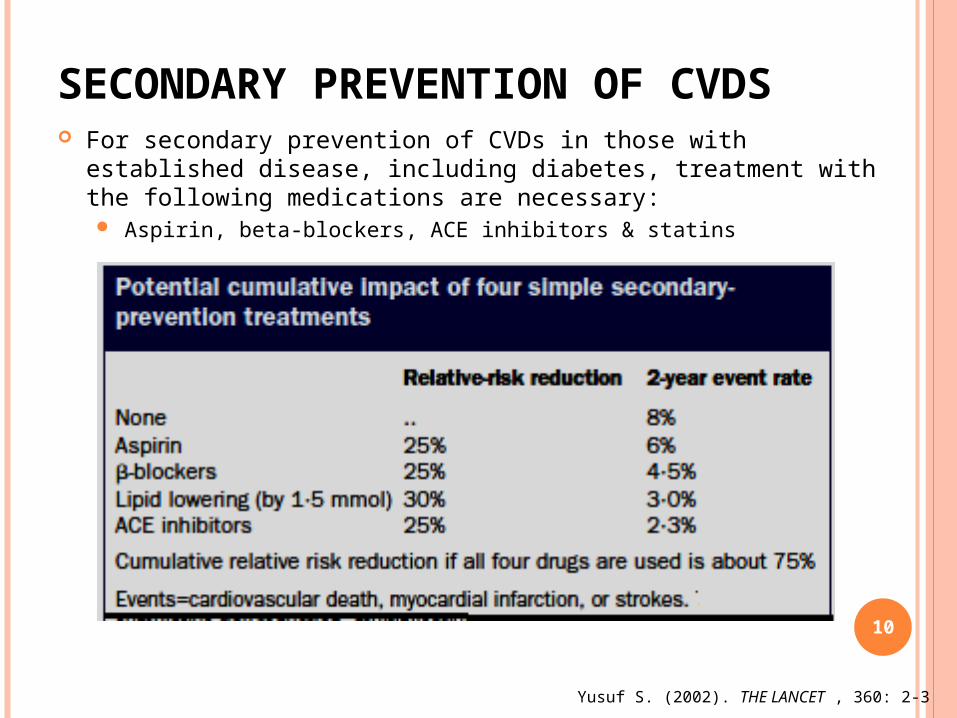
SECONDARY PREVENTION OF CVDS For secondary prevention of CVDs in those with established
disease, including diabetes, treatment with the following medications are necessary: Aspirin, beta-blockers, ACE inhibitors & statins
10
Yusuf S. (2002). THE LANCET , 360: 2-3
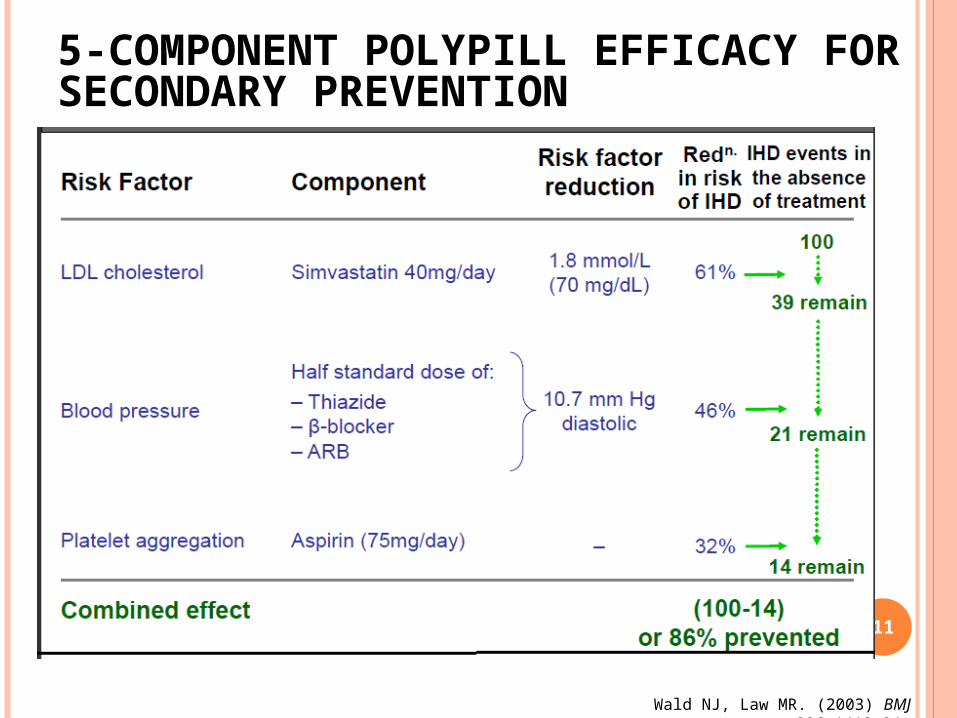
5-COMPONENT POLYPILL EFFICACY FOR SECONDARY PREVENTION
11
Wald NJ, Law MR. (2003) BMJ 326:1419-24
THE CADILA POLYCAPTM USED IN TIPS1 & PK STUDY Hydrochlorothiazide (12.5mg) Atenolol (50mg) Ramipril (5mg) Simvastatin (20mg) Acetyl Salicylic Acid (ASA)
(100mg, Enteric Coated)
In a 00 hard gelatin capsule 12
Reduction in
Heart Rate
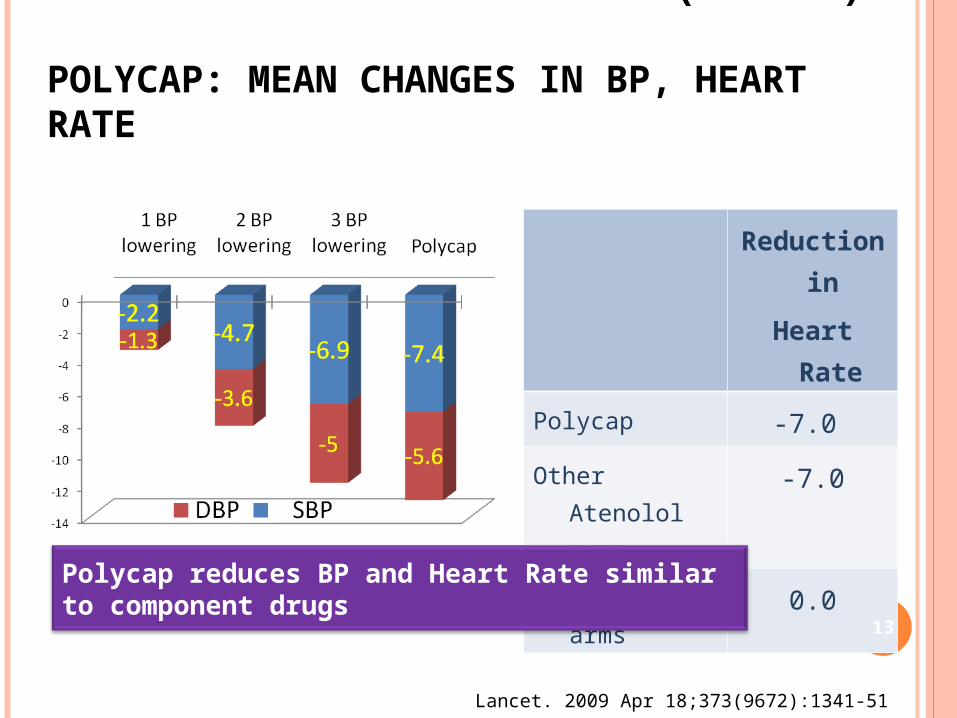
Polycap -7.0
Other Atenolol arms
-7.0
Non Atenolol arms 0.0
THE INDIAN POLYCAPTM STUDY (TIPS 1) POLYCAP: MEAN CHANGES IN BP, HEART RATE
Lancet. 2009 Apr 18;373(9672):1341-51
Polycap reduces BP and Heart Rate similar to component drugs
13
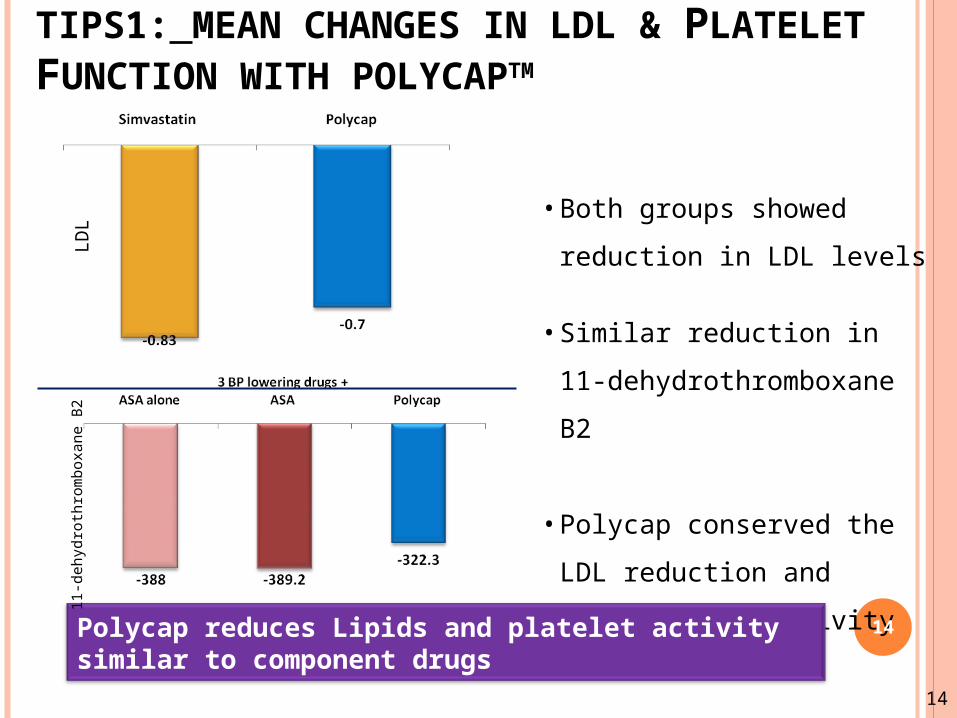
• Both groups showed reduction in LDL levels
• Similar reduction in 11-dehydrothromboxane B2
• Polycap conserved the LDL reduction and Antiplatelet activity
TIPS1: MEAN CHANGES IN LDL & PLATELET FUNCTION WITH POLYCAPTM
Polycap reduces Lipids and platelet activity similar to component drugs
14
LDL
11-d
ehyd
roth
rom
boxa
ne B
2
14
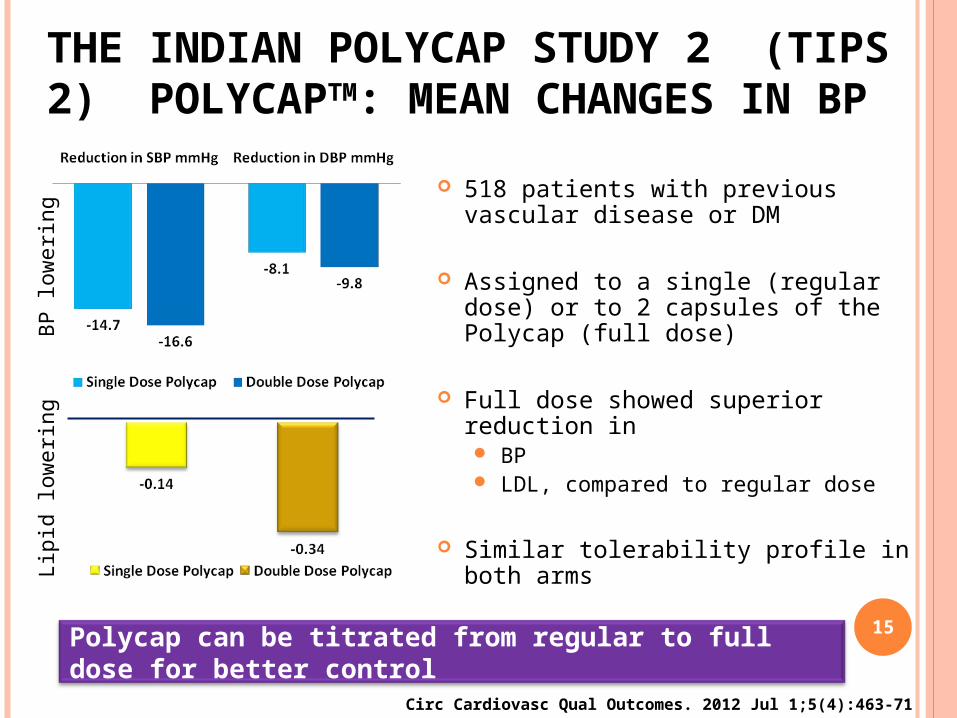
518 patients with previous vascular disease or DM
Assigned to a single (regular dose) or to 2 capsules of the Polycap (full dose)
Full dose showed superior reduction in BP LDL, compared to regular dose
Similar tolerability profile in both arms
THE INDIAN POLYCAP STUDY 2 (TIPS 2) POLYCAPTM: MEAN CHANGES IN BP
Circ Cardiovasc Qual Outcomes. 2012 Jul 1;5(4):463-71
Polycap can be titrated from regular to full dose for better control
Lipi
d lo
wer
ing
BP lo
wer
ing
15
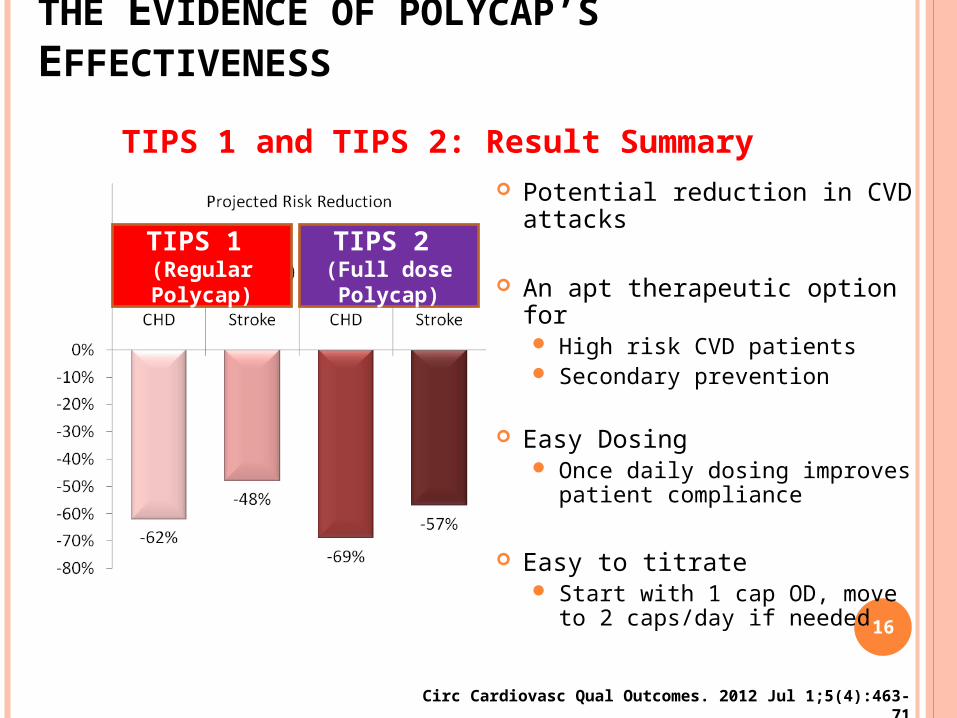
Potential reduction in CVD attacks
An apt therapeutic option for High risk CVD patients Secondary prevention
Easy Dosing Once daily dosing improves
patient compliance
Easy to titrate Start with 1 cap OD, move to
2 caps/day if needed
THE EVIDENCE OF POLYCAP’S EFFECTIVENESS
Circ Cardiovasc Qual Outcomes. 2012 Jul 1;5(4):463-71
TIPS 1 and TIPS 2: Result Summary
TIPS 1 (Regular Polycap)
TIPS 2 (Full dose Polycap)
16
ARE THE EFFECTS INDEPENDENT IN REDUCING RISK? YES Evidence
the mechanisms are different cohort studies randomised trials
e.g. Heart Protection Study, 2002; EUROPA trial, 2002; TIPS (2009)
So, when used together in appropriate patients, up to 80% future CV events can be prevented
Potential benefits of quitting smoking, diabetes control and exercise can virtually eliminate the entire CVD risk in in high-risk individuals 17
THE PHARMACOKINETIC (PK) ISSUES WITH POLYCAP While the efficacy of giving multiple proven drugs in a
single pill or capsule has been proven, the questions are: Is such a combination of several active drugs safe and
tolerable? Is there any drug-drug and drug-metabolite interaction?
Such interactions can lead to toxic or suboptimal levels of one or more ingredients (and metabolites), which may lead to increased adverse effects or alternatively decreased efficacy
Is the bioavailability of some or all its components preserved or getting altered?
While TIPS1 and TIPS2 studied the efficacy of risk factor reductions and clinical safety, we also studied the PK and drug-drug interaction of Polycap 18
Patel A., Shah T., ….Chakraborty B.S. (2010). Am J Cardiovasc Drugs, 10:95-103
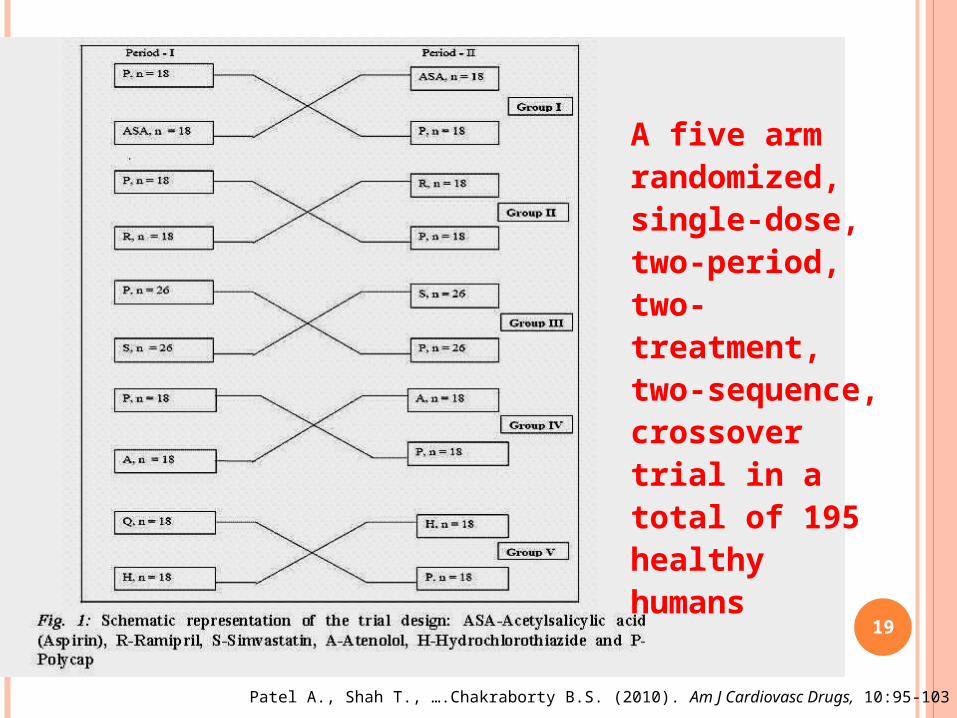
A five arm randomized, single-dose, two-period, two-treatment, two-sequence, crossover trial in a total of 195 healthy humans 19
Patel A., Shah T., ….Chakraborty B.S. (2010). Am J Cardiovasc Drugs, 10:95-103
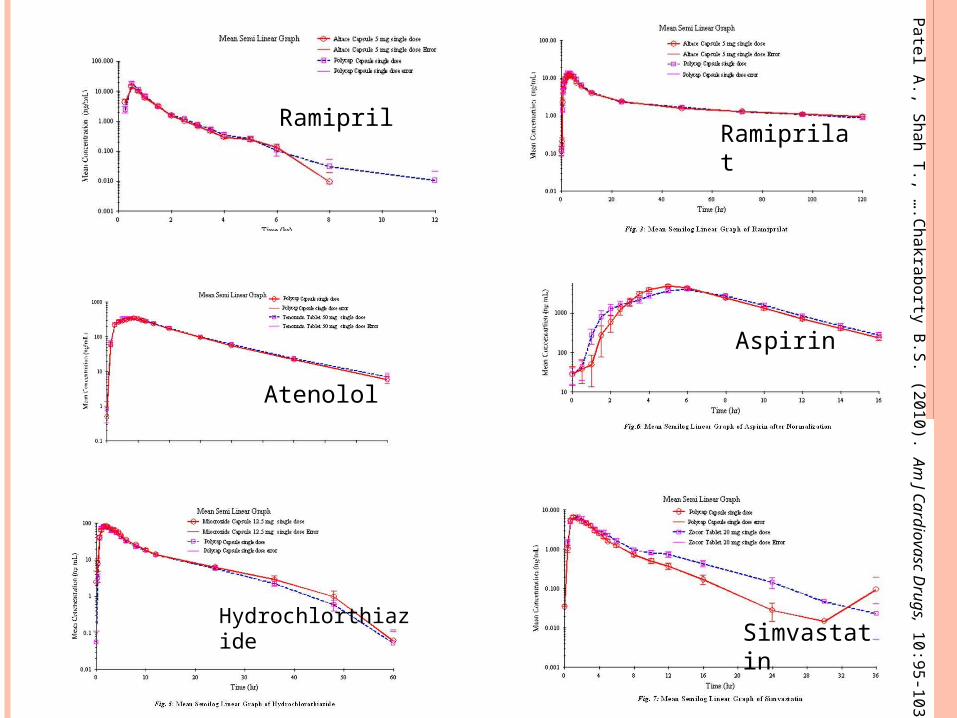
Ramipril Ramiprilat
Aspirin
Atenolol
Hydrochlorthiazide Simvastati
n20
Patel A., Shah T., ….Chakraborty B.S. (2010). Am
J Cardiovasc Drugs, 10:95-103
CONCLUSIONS OF THE POLYCAPTM PK STUDY Aspirin, ramipril, atenolol, and hydrochlorothiazide
from Polycap were absorbed with a comparable rate and extent with those of single ingredient formulations Preservation of bioavailabilty
There was no kinetic drug-drug interaction in vivo For simvastatin, there was a loss of bioavailability
(~20%) but >equal increase in bioavailability of simvastatin acid
The PK study of Polycap establishes the required bioavailability for all its component drugs, thus explaining its reported efficacy kinetically
21
Patel A., Shah T., ….Chakraborty B.S. (2010). Am J Cardiovasc Drugs, 10:95-103
FINAL REMARKS
22
Polycap provides potential primary reduction in CVD attacks
An apt therapeutic option for High risk CVD patients Secondary prevention
Once daily dosing improves patient compliance Easy to titrate
Start with 1 cap OD, move to 2 caps/day if needed No loss of bioavailability of individual
components when formulated as Polycap No drug-drug or drug-metabolite interaction Affordable in low income countries
THANK YOU VERY MUCH
23