Pneumonia - Community-Acquired (1 of 16)
16
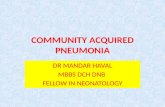
B167 Pneumonia - Community-Acquired (1 of 16) No Yes No Yes 1 Patient presents w/ probable community-acquired pneumonia (CAP) 2 DIAGNOSIS Is CAP highly suspected? 4 CLINICAL DECISION Should patient be admitted to hospital? ALTERNATIVE DIAGNOSIS 3 SEVERITY ASSESSMENT HOSPITAL ADMISSION See next page for treatment C Follow-up at 48-72 hours See next page A Supportive therapy B Pharmacological therapy Patient’s Age Empiric erapy for the Probable Cause of CAP (Oral) Bacteria Atypical Bacteria Influenza <5 years old • Amoxicillin • Alternative: - Co-amoxiclav • Azithromycin • Alternatives: - Clarithromycin - Erythromycin • Oseltamivir ≥5 years old • Amoxicillin ± macrolide 1 • Alternative: - Co-amoxiclav • Azithromycin • Alternatives: - Clarithromycin - Erythromycin - Doxycycline 2 • Oseltamivir • Zanamivir 2 1 For children w/ probable bacterial CAP w/ no clinical, laboratory, or radiographic evidence that differentiates bacterial CAP from atypical CAP 2 For children ≥7 years old Modified from: Bradley JS, Byington CL, Shah SS, et al. e management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guideline by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011 Oct;53(7):e10. Not all products are available or approved for above use in all countries. Specific prescribing information may be found in the latest MIMS. © MIMS Pediatrics 2020 © MIMS
Transcript of Pneumonia - Community-Acquired (1 of 16)

B167
Pneumonia - Community-Acquired (1 of 16)
No
YesNo
Yes
1Patient presents w/ probable
community-acquired pneumonia (CAP)
2DIAGNOSISIs CAP highly
suspected?
4CLINICAL DECISION
Should patient be admitted to
hospital?
ALTERNATIVE DIAGNOSIS
3SEVERITY ASSESSMENT
HOSPITAL ADMISSION See next page for treatment
CFollow-up at 48-72 hours
See next page
A Supportive therapy
B Pharmacological therapy
Patient’s Age
Empiric � erapy for the Probable Cause of CAP (Oral)Bacteria Atypical Bacteria Infl uenza
<5 years old
• Amoxicillin • Alternative:
- Co-amoxiclav
• Azithromycin • Alternatives:
- Clarithromycin- Erythromycin
• Oseltamivir
≥5 years old
• Amoxicillin ± macrolide1
• Alternative:- Co-amoxiclav
• Azithromycin • Alternatives:
- Clarithromycin- Erythromycin- Doxycycline2
• Oseltamivir• Zanamivir2
1For children w/ probable bacterial CAP w/ no clinical, laboratory, or radiographic evidence that diff erentiates bacterial CAP from atypical CAP
2For children ≥7 years old Modifi ed from: Bradley JS, Byington CL, Shah SS, et al. � e management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guideline by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011 Oct;53(7):e10.
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B168
Pneumonia - Community-Acquired (2 of 16)
NoYes
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
FOLLOWUP OF OUTPATIENTS W/ CAP
Did patient
improve?
2 DIAGNOSIS• Confi rm diagnosis
- Check for atypical microorganisms
• Assess possible complication
A Supportive therapy
B Pharmacological therapy• Adjust/shift antibiotic,
if necessary
ADVISE THE CAREGIVER• Complete the antibiotic
regimen
E Prevention• See page 8
MANAGEMENT OF HOSPITALIZED PATIENT
A Supportive therapy
B Pharmacological therapy
Patient’s Immunization Status & Local Penicillin Resistance Pattern
Empiric � erapy for the Probable Cause of CAP (Oral or IV) Bacteria Atypical Bacteria Infl uenza
• Complete vaccine• Minimal local
penicillin resistance
• Ampicillin• Penicillin G• Alternatives:
- Ceftriaxone- Cefotaxime- Plus, either:1
- Vancomycin- Clindamycin
• Azithromycin + β-lactam2
• Alternatives:- Clarithromycin- Erythromycin- Doxycycline3
- Levofl oxacin4
• Oseltamivir• Zanamivir3
• Incomplete vaccine• Signifi cant local
penicillin resistance
• Ceftriaxone• Cefotaxime
- Plus, either:1- Vancomycin- Clindamycin
• Alternative:- Levofl oxacin- Plus, either:1
- Vancomycin- Clindamycin
• Azithromycin + β-lactam2
• Alternatives:- Clarithromycin- Erythromycin- Doxycycline3
- Levofl oxacin4
• Oseltamivir• Zanamivir3
1For children w/ suspected community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)2For children w/ uncertain diagnosis of atypical pneumonia3For children ≥7 years old w/ macrolide-resistant mycoplasma infection (Doxycycline)4For children who have reached growth maturity or who cannot tolerate macrolides or w/ macrolide-resistant myco-plasma infection
Modifi ed from: Bradley JS, Byington CL, Shah SS, et al. � e management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guideline by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011 Oct;53(7):e10.
CFollow-up at 48-72 hours
See next page
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B169
Pneumonia - Community-Acquired (3 of 16)
NoYes
FOLLOWUP OF INPATIENTS W/ CAP
Did patient
improve?
2 DIAGNOSIS• Assess possible complication
A Supportive therapy
B Pharmacological therapy• Adjust/shift antibiotic, if
necessaryD Specialist referral
• If indicated
Discharge• Assess patient for possible
dischargeAdvise the caregiver• Complete the antibiotic regimen
E Prevention• See page 8
1 COMMUNITY-ACQUIRED PNEUMONIA (CAP)
• A previously healthy child presenting w/ signs & symptoms of lower respiratory tract infection (LRTI), acquired outside of the hospital
• � e most common bacterial cause of childhood pneumonia is Streptococcus pneumoniae - Usually causes about ⅓ of radiographically-confi rmed pneumonia in children <2 years of age - Pneumonia secondary to group A streptococcus & Staphylococcus aureus is more frequently associated w/
empyema or pediatric ICU admission• Viruses commonly aff ect children <1 year of age than those aged >2 years; respiratory syncytial viruses (RSV)
being the most frequently detected virus - Adenoviruses, bocavirus, human metapneumovirus, infl uenza A & B viruses, parainfl uenza viruses, coro-
naviruses & rhinovirus are less frequently identifi ed• Mixed infection may occur in 8-40% of CAP cases
2 DIAGNOSIS
• Diagnosis of CAP is primarily based on history & physical fi ndings (eg signs & symptoms of respiratory distress, fever)- Lab & radiographic exams may aid in the diagnosis of severe cases or in patients who failed to show clinical
improvement after initiation of antibiotic therapyHistory• Patient’s age, immunization status
- Age is a good predictor of the causative agent - Viruses are often linked in up to 50% of pneumonia in young children- S pneumoniae followed by atypical pneumonia (eg Mycoplasma & Chlamydia) is the most likely pathogen
in older children w/ pneumonia of bacterial origin- Immunization status is important because children fully immunized against Haemophilus infl uenzae type
b & S pneumoniae are less likely to be infected w/ these pathogens• Symptoms may include fever, dyspnea, cough, chest or abdominal pain w/ or without vomiting, headache
- Patients w/ cough or diffi culty of breathing w/ either lower chest indrawing, nasal fl aring, or grunting are considered to have severe pneumonia
- Patients w/ cough or diffi culty of breathing w/ either cyanosis, severe respiratory distress, inability to drink or vomits everything, or lethargy, unconsciousness, convulsions have very severe pneumonia
• Should also take note of the season of the year, daycare attendance, exposure to tobacco smoke or infectious diseases (eg tuberculosis), history of travel, or coexisting illnesses [ie cardiac or pulmonary disorders (eg history of severe or recurrent pneumonia, bronchopulmonary dysplasia, cystic fi brosis, congenital heart disease), immu-nodefi ciencies, neuromuscular diseases (eg severe cerebral palsy)]
Physical Exam• Combination of clinical fi ndings are more predictive in diagnosing CAP• Check for temperature
- Fever in viral pneumonia is generally lower than in bacterial pneumonia; bacterial pneumonia presents w/ persistent or recurrent temperatures of ≥38.5C over the prior 24-48 hours
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B170
Pneumonia - Community-Acquired (4 of 16)
2 DIAGNOSIS (CONT’D)
Physical Exam (Cont’d)• Respiratory rate (RR)
- Study shows signifi cant correlation between RR & oxygen saturation - Less sensitive & specifi c in the fi rst 3 days of illness- Criteria for tachypnea based on age as defi ned by World Health Organization (WHO):
- ≥60 breaths/minute in <2 months old- ≥50 breaths/minute in 2-11 months old- ≥40 breaths/minute in 1-5 years old- >20 breaths/minute in ≥5 years old
- Tachypnea may be a marker for respiratory distress &/or hypoxemia but may also be secondary to fever, dehydration or concurrent metabolic acidosis
- Increased work of breathing is associated w/ changes radiologically• Respiratory signs may include intercostal, subcostal, or suprasternal retractions, nasal fl aring, crackles or
wheezing on auscultation- Decreased breath sounds, scattered crackles, or rhonchi are usually heard over the aff ected lung fi eld in the
early course of illness- Dullness on percussion & decreased breath sounds are usually appreciated when increased consolidation &
complication developsLab Tests• May not be necessary in uncomplicated pneumonia Microbiology• Aids in determining the causative agent to provide a narrow-spectrum antimicrobial therapy that targets a
specifi c bacteria or virus• Blood culture is not routinely done in a nontoxic, fully immunized children w/ CAP
- Recommended in patients requiring hospitalization for presumed moderate to severe bacterial CAP, specifi cally those w/ complicated pneumonia
- Should also be performed in outpatients who do not show clinical improvement & in those w/ progressive symptoms or clinical deterioration even after starting the antibiotic therapy
- Follow-up blood culture is necessary to document resolution of bacteremia caused by S aureus, regardless of patient’s clinical status
• Sputum Gram stain & culture is recommended in hospitalized older children & adolescents w/ more severe disease or in those in whom outpatient therapy has failed
Tests for Viral Pathogens• Tests that are specifi c & sensitive to rapidly identify infl uenza virus & other respiratory viruses should be done
to evaluate children w/ CAP- Positive infl uenza test will guide appropriate antiviral agents to be used in both inpatient & outpatient settings,
& may also decrease the need for additional diagnostic studies & antimicrobial useTests for Atypical Bacteria• School-aged children & adolescents presenting w/ signs & symptoms of possible M pneumoniae should be
tested to identify the appropriate antibiotic to use- However, no single currently available test (ie culture, cold agglutinating antibodies, serology & molecular-based
methods) off ers the sensitivity & specifi city desired in a clinically relevant time frame Ancillary Diagnostic Tests• Complete blood count provides evaluation of white blood cells & determines presence of anemia or throm-
bocytopenia which may guide antimicrobial intervention & identify presence of hemolytic-uremic syndrome, a rare complication of pneumococcal pneumonia
• Acute-phase reactants (ie peripheral WBC count, erythrocyte sedimentation rate, C-reactive protein concen-tration, procalcitonin concentration) should not be routinely done in fully immunized patients w/ CAP- May provide useful information in managing patients requiring hospitalization or those w/ complications - May be helpful in assessing patient’s response to therapy in conjunction w/ clinical fi ndings
• Pulse oximetry gives an estimate of arterial oxygenation in a non-invasive manner - More directly relevant in evaluating severity of disease in CAP- Should be done in all children w/ pneumonia & suspected hypoxemia
- Presence of hypoxemia will determine the diagnostic tests needed & if hospitalization is warranted - Hypoxemia is a well established determinant for poor outcome in children & infants w/ systemic disease
- Usually monitored continuously in a child w/ increased work of breathing or signifi cant distress especially if the patient has a decreased level of activity or agitation
Imaging StudiesChest X-ray• Not necessary to confi rm suspected CAP in outpatient setting since diagnosis of CAP is strongly suspected
based on clinical fi ndings- Cannot diff erentiate viral from bacterial CAP nor among diff erent possible bacterial pathogens
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B171
Pneumonia - Community-Acquired (5 of 16)
2 DIAGNOSIS (CONT’D)
Chest X-ray (Cont’d)• Postero-anterior (PA) or lateral chest X-rays are indicated in patients w/ suspected or documented hypoxemia or
signifi cant respiratory distress, & in patients who did not respond to initial antibiotic therapy to confi rm presence of possible complications (ie empyema, parapneumonic eff usions, necrotizing pneumonia, pneumothorax)- Also recommended in hospitalized patients to determine the presence, size & character of parenchymal
infi ltrates, & to document possible complications • Daily chest X-ray is not required in stable patients w/ pneumonia complicated by parapneumonic eff usion
after chest tube placement or after video-assisted thoracoscopic surgery (VATS)• Follow-up chest X-ray should not be done routinely in patient who improved uneventfully from CAP but is
recommended in patients who do not show clinical improvement & in those w/ progressive symptoms or clinical deterioration within 48-72 hours after starting the antibiotic therapy- Should also be obtained in patients w/ complicated pneumonia who has worsening respiratory distress or
clinical instability or in those who are consistently febrile even after 48-72 hours of antibiotic use- Recommended after 4-6 weeks in patients w/ recurrent pneumonia in the same lobe & in patients w/ lobar
collapse at fi rst chest X-ray w/ suspicion of an anatomic anomaly, chest mass, or foreign body aspirationOther Imaging Studies• Chest ultrasound is the imaging study of choice to assess pleural fl uid loculations
- Chest ultrasound has no ionizing radiation; hence, considered a safer imaging procedure than computed tomography (CT)
- May be used as a guide in percutaneous needle aspiration for direct culture of infected lung tissue, chest tubing or thoracentesis
• CT may also be used to confi rm the presence & quantify the amount of pleural fl uid
3 SEVERITY ASSESSMENT
• Necessary to identify patients who may be eff ectively treated as outpatient & who may need hospitalization • Patient’s history, presentation & physical examination are the major determinants of the severity of illness &
appropriate site of care• Severity should be based on patient’s overall clinical appearance & behavior (eg degree of alertness & eagerness
to feed)
Infants Older ChildrenMild to
Moderate CAPSevere CAP Mild to
Moderate CAPSevere CAP
Temperature <38.5°C ≥38.5°C <38.5°C ≥38.5°C Respiratory rate
<50 breaths/minute
>70 breaths/minute <50 breaths/minute
>50 breaths/minute
Breathing eff ort
• Mild chest recession
• Moderate-severe chest recession
• Nasal fl aring• Cyanosis• Intermittent
apnea• Grunting
• Mild breathlessness
• Severe diffi culty in breathing
• Nasal fl aring• Cyanosis• Grunting
Other features
• Taking full feeds
• Not feeding• Increased heart
rate• Capillary refi ll
time ≥2 seconds
• No vomiting • W/ signs of dehydration
• Increased heart rate• Capillary refi ll time
≥2 secondsModifi ed from: Harris M, Clark J, Coote N, et al, on behalf of the British � oracic Society Standards of Care Committee. British � o-racic Society guidelines for the management of community acquired pneumonia in children: update 2011. � orax. 2011 Oct;66(2):ii16.
4 CLINICAL DECISIONIndications for Hospital Admission • Children & infants who have moderate to severe CAP, as defi ned by the presence of respiratory distress (ie
tachypnea, dyspnea, suprasternal/intercostal/subcostal retractions, grunting, nasal fl aring, apnea, altered mental status, pulse oximetry measurement <90% on room air)
• Patients <3-6 months old w/ possible bacterial CAP
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B172
Pneumonia - Community-Acquired (6 of 16)
1Adapted from: Bradley JS, Byington CL, Shah SS, et al. � e management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guideline by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011 Oct;53(7):e5.
2Adapted from: Harris M, Clark J, Coote N, et al, on behalf of the British � oracic Society Standards of Care Committee. British � oracic Society guidelines for the management of community acquired pneumonia in children: update 2011. � orax. 2011 Oct;66(2):ii16.
4 CLINICAL DECISION (CONT’D)Indications for Hospital Admission (Cont’d) • Children & infants w/ suspected or documented CAP caused by an agent w/ increased virulence (eg CA-MRSA)• Patients whom there is concern about careful observation at home or who may be unable to comply w/ medi-
cations or cannot be followed up• Presence of signifi cant comorbid conditions (eg cardiopulmonary disease, genetic syndromes)• Presence of dehydration, vomiting, inability to take oral medications • Patients w/ unsuccessful outpatient oral antimicrobial treatment, & those w/ new & progressive respiratory distressIndications for Intensive Care Unit (ICU) Admission1
• Patient w/ ≥1 major or ≥2 minor criteria should be transfered to an ICU or a unit w/ continuous cardiorespi-ratory monitoring - Major criteria: Invasive mechanical ventilation, fl uid refractory shock, acute need for noninvasive positive pressure
ventilation (NIPPV), hypoxemia requiring fraction of inspired oxygen (FiO2) > inspired concentration- Minor criteria: Tachypnea, apnea, retractions, dyspnea, nasal fl aring, grunting, arterial oxygen pressure
(PaO2)/FiO2 <250, multilobar infi ltrates, Pediatric Early Warning Score (PEWS) >6, altered mental status, hypotension, presence of eff usion, comorbid conditions, unexplained metabolic acidosis
• British � oracic Society indications for referral to a pediatric ICU2 include respiratory failure needing assisted ventilation & pneumonia w/ septicemia - Clinical features include presence of shock, raised RR & HR together w/ severe respiratory distress & exhaus-
tion w/ or without increased pCO2, slow irregular breathing or recurrent apnea, & inability to maintain oxygen saturations >92% with FiO2 60%
A SUPPORTIVE THERAPY• Parents of children who do not require hospitalization should be advised about:
- Use of antipyretics to manage fever- Preventing dehydration- Determining signs of deterioration or signs of other serious illness after 48 hours of antibiotic therapy
• Patients admitted in the hospital, whose oxygen saturation is <92% while breathing room air, should be given oxygen via nasal cannula, head box, or face mask to sustain oxygen saturation >95%
• Fluid therapy (eg IV fl uid replacement or nasogastric feeds) is recommended in patients who are unable to maintain their fl uid intake secondary to breathlessness, fatigue, or vomiting - Plasma sodium, potassium, urea &/or creatinine should be measured at baseline & at least daily in patients
on intravenous fl uids
B PHARMACOLOGICAL THERAPY• � erapy is usually empiric & is based on age-specifi c causes of CAP, disease severity & local resistance patterns
of predominant pathogens- If blood or respiratory tract specimen culture has identifi ed the causative agent, a safe, narrow-spectrum & eff ective
therapy should be given• Empiric treatment may be given for 7-10 days • Oral route is safe & eff ective for outpatients w/ bacterial pathogen that most commonly cause LRTIs• Parenteral route is preferred in patients w/ severe disease or are unable to tolerate oral drug intake (eg vomiting)
to ensure adequate blood & tissue concentrations• Antimicrobials are not warranted, may cause drug toxicity, & may facilitate development of antimicrobial
resistance in young patients w/ clinical features suggestive of upper & lower respiratory tract viral infections • Empiric therapy for some children require both antimicrobial & antiviral agentsPenicillinsAmoxicillin• 1st-line agent at any age if S pneumoniae is the likely pathogen
- May also be given to patients w/ pneumonia caused by β-lactamase-negative strains (eg H in� uenzae)• Has broader spectrum of activity, better oral pharmacokinetics (better absorption from gastrointestinal tract)
& tolerability (less frequent dosing & better taste) as compared w/ Penicillin• Preferred step-down oral therapy for hospitalized patients initially treated w/ Ampicillin for S pneumoniae or
β-lactamase-negative H in� uenzae infection- May also be given as step-down therapy in patients initially treated w/ broad-spectrum antimicrobials in
whom no cultures are obtained or were only obtained after starting antibiotics
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B173
Pneumonia - Community-Acquired (7 of 16)
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
B PHARMACOLOGICAL THERAPY (CONT’D)Ampicillin or Penicillin G• Recommended for hospitalized, fully immunized infants & school-aged children when local epidemiologic
data shows lack of resistance for invasive S pneumoniae- Also considered as 1st-line option in hospitalized patients w/ group A Streptococcus infections
• Ampicillin is the preferred agent for infections caused by β-lactamase negative H in� uenzae• Penicillin G represents the most narrow-spectrum & eff ective antibiotic for pneumococcal infections but
requires a more frequent dosing interval• Also active against S pyogenes that causes severe necrotizing pneumoniaAntistaphylococcal Penicillin • Eg Oxacillin (IV), Nafcillin (IV)• Used for patients admitted in the hospital for methicillin-susceptible S aureus (MSSA) infectionPenicillin w/ Beta-lactamase Inhibitor• Eg Amoxicillin/clavulanic acid, Ampicillin/sulbactam• Amoxicillin/clavulanic acid is the preferred oral step-down therapy for infections caused by β-lactamase
producing H in� uenzae- May also be given through intravenous route in patients w/ severe CAP which has been shown to be as
eff ective as Ceftriaxone for strains w/ Amoxicillin MIC of up to 2 mcg/mLMacrolides• Eg Azithromycin, Clarithromycin, Erythromycin, Roxithromycin • 1st-line agent in school-aged children & adolescents w/ atypical pneumonia eg M pneumoniae or C pneumoniae• Recommended 1st-line treatment for Penicillin-allergic pediatric patients • May be added at any age if without improvement w/ 1st-line therapy after 48 hours of treatment • Not advised as empiric therapy for pneumococcal CAP because currently isolated strains of S pneumoniae
have shown signifi cant resistance against macrolides • Azithromycin is the preferred agent for M pneumoniae, C pneumoniae or C trachomatis infectionsCephalosporins• 1st generation drugs (eg Cefazolin IV) may be used for inpatients w/ MSSA infection• 2nd generation (eg Cefuroxime) or 3rd generation (eg Ceftriaxone, Cefotaxime) agents are active against both
β-lactamase-negative & -positive strains- Parenteral Ceftriaxone or Cefotaxime are recommended in hospitalized infants & children that are incom-
pletely immunized, in places where local epidemiology shows lack of resistance for invasive S pneumoniae, or in infants & children w/ life-threatening infection (eg empyema) - Also the preferred agent for infections caused by β-lactamase producing H in� uenzae
- IV Ceftriaxone is the preferred agent for penicillin-resistant S pneumoniae - IM injection of Ceftriaxone may be given once a day as an outpatient therapy - Oral Cefpodoxime, Cefprozil or Cefuroxime may be considered as alternative agents in patients w/ allergies
to Amoxicillin• Also active against S pyogenes causing severe necrotizing pneumonia Quinolones• Eg Levofl oxacin• May be used as an alternative to patients w/ history of severe allergy to Amoxicillin• Have comparable eff ect as w/ macrolides & tetracyclines in treating patients w/ M pneumoniae infection• Preferred oral step-down therapy in patients infected w/ penicillin-resistant S pneumoniaeTetracyclines• Eg Doxycycline• For children >8 years w/ macrolide-resistant M pneumoniaeOther Antibiotics• Vancomycin is the 1st-line agent for infections caused by community-acquired methicillin-resistant S aureus
(CA-MRSA) • Linezolid is the preferred oral step-down therapy & an alternative parenteral agent for CA-MRSA infections
- Useful especially in patients w/ pre-existing renal impairment or is receiving other nephrotoxic drugs- May be given to children w/ severe allergy to β-lactam drugs who can not tolerate Vancomycin or Clindamycin
but should be used w/ caution since it has relatively high adverse eff ect profi le• IV Clindamycin may be used as an alternative agent in patients w/ infections caused by susceptible MSSA or
MRSA but is not recommended in patients w/ empyema
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B174
Pneumonia - Community-Acquired (8 of 16)
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
B PHARMACOLOGICAL THERAPY (CONT’D)Infl uenza Antiviral � erapy• Should be administered as soon as possible to patient w/ moderate to severe CAP caused by infl uenza virus
infection, specifi cally to those w/ clinically worsening CAP during outpatient visit• Should not wait for the results of confi rmation test since early treatment has been shown to provide maximal
advantage• May still be of benefi t when used after 48 hours of symptomatic infection in patients w/ more severe diseaseCombination � erapy• Macrolide plus β-lactam antibiotic may be given to inpatients w/ probable M pneumoniae & C pneumoniae• Vancomycin or Clindamycin should be added to β-lactam antibiotic in patients highly considered to have S aureus
infection, depending on local susceptibility data- Clindamycin plus β-lactam is recommended in children w/ toxic-like syndrome
Duration of � erapy• 10-day treatment course has been well studied but shorter period may be similarly eff ective for mild CAP• CA-MRSA infections may require longer treatment duration than those caused by S pneumoniae
C FOLLOW-UP• Predictors of treatment response are decrease in respiratory signs & defervescence within 48-72 hours of
antimicrobial therapy• Switch to oral therapy may be considered once there is improvement in fever, cough, tachypnea, supplemental
oxygen dependency, & increased activity & appetite, concurrent w/ decrease in WBC counts &/or CRP levels • Children who developed lobar collapse, round pneumonia, or radiographic fi ndings of CAP complications
may have an outpatient follow-up at 6-8 weeks w/ clinical evaluation & a chest X-ray
D SPECIALIST REFERRAL• Consultation w/ a pediatric pulmonologist or infectious diseases specialist is considered if the patient has
allergies, other coexisting illnesses or presence of complications (eg eff usion, empyema, bronchiectasis, hemolytic uremic syndrome, necrotizing pneumonia, sepsis)
E PREVENTIONVaccination• Children should be given vaccines against bacterial pathogens including S pneumoniae, H infl uenzae type b,
& Bordetella pertussis• Pneumococcal conjugate vaccine & combination vaccine against pertussis may be given as early as 6 weeks
old & infl uenza vaccine at 6 months of age as part of the recommended routine immunization schedule• Parents & caretakers of infants <6 months of age should be vaccinated against infl uenza virus & pertussis to
protect the infants from exposure to these pathogensInfl uenza vaccine1
• Children ≥6 months of age should be given infl uenza virus vaccine yearly• Two doses separated by a 4-week interval should be administered to children 6 months to 8 years receiving
infl uenza vaccine for the 1st time, then 1 dose yearly after initial dosePertussis vaccine1
• Given as part of the combination vaccine DTaP (diphtheria, tetanus, acellular pertussis) of the recommended routine immunization schedule & w/ the booster dose Tdap or Td annually for children w/ complete immunization
Pneumococcal vaccine1
• Introduction of pneumococcal vaccine greatly reduced the incidence of CAP in children caused by S pneumoniae • Pneumococcal 13-valent conjugate vaccine (PCV13) is recommended as a 3-dose series starting at 2 months
of age given at 8-week intervals w/ booster dose given at 12-15 months of age for primary immunization• Patients aged ≥2 years at high risk of invasive pneumococcal disease should be given pneumococcal 23-valent
polysaccharide vaccine (PPSV23) 8 weeks after PCV13 dose Immunotherapy• RSV-specifi c monoclonal antibody (eg Palivizumab) may be considered as prophylaxis during RSV season in
premature infants & in those w/ comorbid diseases (eg underlying lung pathology, congenital abnormalities of the airways, hemodynamically signifi cant congenital heart disease, neuromuscular diseases)
Other Preventive Measures• Frequent handwashing, breastfeeding, limiting exposure to other children, & reducing exposure to smoking
are important measures that should be done
1Recommendations for vaccination may vary between countries. Please refer to local guidelines.
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B175
Pneumonia - Community-Acquired (9 of 16)
All dosage recommendations are for children w/ normal renal & hepatic function unless otherwise stated.Not all products are available or approved for above use in all countries.
Products listed above may not be mentioned in the disease management chart but have been placed here based on indications listed in regional manufacturers’ product information.
Specifi c prescribing information may be found in the latest MIMS.
Dosage Guidelines
AMINOGLYCOSIDES
Drug Dosage Remarks
Amikacin 15 mg/kg/day IM/IV divided 8-12 hrlyNeonate: 10 mg/kg loading dose followed by 15 mg/kg/day divided 12 hrly
Adverse Reactions• Ototoxic eff ects (can cause irreversible ototoxicity
resulting in hearing loss, dizziness, vertigo); Renal eff ects (reversible nephrotoxicity, acute renal failure has been reported usually when other nephrotoxic drugs have also been administered); Neuromuscular eff ects (neuromuscular blockade resulting in resp depression & muscular paralysis especially after rapid IV infusion); Hypersensitivity reactions
Special Instructions• Ototoxicity & nephrotoxicity are most likely in patients
w/ renal impairment, in patients who are receiving high doses or for long periods or who are also receiving or have received other ototoxic/nephrotoxic drugs- Consider monitoring of serum concentrations &/or
peak serum concentrations/MIC ratio in these patients • Use w/ caution in neonates due to renal immaturity,
patients w/ conditions associated w/ muscle weakness, preexisting renal dysfunction, vestibular or cochlear impairment
Dibekacin 1-2 mg/kg/day IM divided 12-24 hrly
Gentamicin 6-7.5 mg/kg/day IM/IV divided 8 hrlyPremature/full-term neonate ≤1 wk:2.5 mg/kg IM/IV 12 hrly
Kanamycin 30-50 mg/kg/day IM divided 12-24 hrly
Netilmicin Premature/full-term neonate <1 wk: 6 mg/kg/day or 3 mg/kg IM/IV 12 hrly Neonate >1 wk to 1 yr: 7.5-9 mg/kg/day or 2.5-3 mg/kg IM/IV 8 hrly Childn >1 yr: 6-7.5 mg/kg/day or 2-2.5 mg/kg IM/IV 8 hrly
ANTIBACTERIAL COMBINATION
Drug Dosage Remarks
Co-trimoxazole [Sulfamethoxazole (SMZ) & Trimethoprim (TM)]
8-12 mg/kg/day PO divided 12 hrly based on TM
Adverse Reactions • GI eff ects (N/V, anorexia, diarrhea, rarely
antibiotic-associated diarrhea/colitis,); Dermatologic eff ects (rash, pruritus, photosensitivity); Hypersensitivity reactions can range from mild (eg rash) to severe/life-threatening (eg Stevens- Johnson syndrome, toxic epidermal necrolysis); Urogenital eff ect (crystallization in the urine)
• Rarely hematologic eff ects which may be more common if given for long periods or w/ high doses; Rarely hepatic, renal eff ects; Aseptic meningitis has occurred
Special Instructions• Maintain adequate fl uid intake• Contraindicated in patients <2 mth of age & patients w/
sulfonamide allergy• Use w/ extreme caution or not at all in patients w/
hematological disorders especially megaloblastic anemia due to folic acid defi ciency
• Use w/ caution in patients w/ renal impairment or severe hepatic dysfunction & in patients w/ folate defi ciency (may consider administration of calcium folinate)
• Use w/ caution in patients w/ G6PD defi ciency
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B176
Pneumonia - Community-Acquired (10 of 16)
All dosage recommendations are for children w/ normal renal & hepatic function unless otherwise stated.Not all products are available or approved for above use in all countries.
Products listed above may not be mentioned in the disease management chart but have been placed here based on indications listed in regional manufacturers’ product information.
Specifi c prescribing information may be found in the latest MIMS.
Dosage Guidelines
CEPHALOSPORINS
Drug Dosage Remarks
First GenerationCefalexin (Cephalexin)
25-50 mg/kg/day PO divided 6 hrly Adverse Reactions• Hypersensitivity reactions
(urticaria, pruritus, rash, severe reactions eg anaphylaxis can occur); GI eff ects (diarrhea, N/V, rarelyantibiotic-associated diarrhea/colitis); Other eff ects (candidal infections, inj site infl ammation)
• High doses may be associated w/ CNS eff ects (encephalopathy, convulsions); Rarely hematologic, hepatic & renal eff ects have occurred
Special Instructions• May be taken w/ food to
decrease gastric distress• Ceftriaxone is contraindicated
in hyperbilirubinemic neonates
• Avoid simultaneous administration of Ceftriaxone w/ IV Ca-containing soln
• Use w/ caution in patients allergic to Penicillin, there may be 10% chance of cross sensitivity; & patients w/ renal impairment & GI disease especially w/ history of colitis
Cefazolin 25-50 mg/kg/day IM/IV divided 6-8 hrly May be increased to 100 mg/kg/day in severe infections
Second GenerationCefaclor ≥1 mth: 20-40 mg/kg/day PO divided 8 hrly
Max dose: 1 g/dayCefuroxime ≥1 mth: 10-15 mg/kg PO 12 hrly or 75-100 mg/kg
IM/IV divided 8 hrlyMay be increased to 100-150 mg/kg IM/IV divided 8 hrly in severe infections
� ird GenerationCefditoren pivoxil ≥12 yr: 400 mg PO 12 hrly x 14 daysCefi xime >6 mth: 1.5-3 mg/kg PO 12 hrly
Severe infections: 6 mg/kg PO 12 hrly>30 kg: 50-100 mg PO 12 hrly
Cefotaxime Neonates ≤7 days 1.2-2 kg: 100 mg/kg/day IM/IV divided 12 hrly >2 kg: 100-150 mg/kg/day IM/IV divided 8-12 hrlyNeonates >7 days 1.2-2 kg: 150 mg/kg/day IM/IV divided 8 hrly>2 kg: 150-200 mg/kg/day IM/IV divided 6-8 hrly Infants & childn: 100-200 mg/kg/day IM/IV divided 6-12 hrly
Cefpodoxime 8-10 mg/kg/day PO divided 12-24 hrlyCeftazidime 30-100 mg/kg/day IM/IV divided 8-12 hrly
Max dose: 6 g/day IM/IV divided 8 hrly Neonates & infants: 25-60 mg/kg/day IM/IV divided 12 hrly
Ceftibuten 9 mg/kg PO 24 hrlyMax dose: 400 mg/day
Ceftizoxime ≥6 mth: 40-80 mg/kg/day IV divided 6-12 hrlyMay be increased to 120 mg/kg/day
Ceftriaxone ≤2 wk: 20-50 mg/kg/day IM/IV3 wk-12 yr: 20-80 mg/kg/day IM/IV
Fourth GenerationCefepime >2 mth & ≤40 kg: 50 mg/kg IM/IV 8-12 hrlyFifth GenerationCeftaroline fosamil
≥2 mth to <2 yr: 8 mg/kg/dose IV infusion over 5-60 min 8 hrly ≥2 yr to <18 yr:<33 kg: 12 mg/kg IV infusion over 5-60 min 8 hrly ≥33 kg: 600 mg IV infusion over 5-60 min 12 hrly
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B177
Pneumonia - Community-Acquired (11 of 16)
All dosage recommendations are for children w/ normal renal & hepatic function unless otherwise stated.Not all products are available or approved for above use in all countries.
Products listed above may not be mentioned in the disease management chart but have been placed here based on indications listed in regional manufacturers’ product information.
Specifi c prescribing information may be found in the latest MIMS.
Dosage Guidelines
CHLORAMPHENICOL
Drug Dosage Remarks
Chloramphenicol Neonates 0-7 days: 25 mg/kg/day IVNeonates >7 days: ≤2 kg: 25 mg/kg/day IV>2 kg: 50 mg/kg/day IV divided 12 hrlyInfants & childn: 50-100 mg/kg/day IV divided 6 hrly
Adverse Reactions• Hematologic eff ects (reversible bone-marrow
depression, rarely severe irreversible aplastic anemia); Hypersensitivity reaction (anaphylactoid reactions); CNS eff ects (optic atrophy or neuropathy paresthesias); GI eff ects (N/V, diarrhea, stomatitis, glossitis, bitter taste)
• Gray syndrome may occur in patients given high doses (abdominal distention, vomiting, ashen color, irregular respiration, circulatory collapse, death)
Special Instructions• Avoid in patients w/ preexisting
bone-marrow depression or blood dyscrasias• Use w/ caution in neonates & patients w/
G6PD defi ciency• Dosage must be adjusted for patients w/
hepatic or renal insuffi ciency • Due to narrow therapeutic/toxic ratio,
monitor serum levels if possible, particularly in patients w/ hepatic or renal disease
MACROLIDES
Drug Dosage Remarks
Erythromycin 30-50 mg/kg/day PO divided 6 hrly Adverse Reactions• GI eff ects (N/V, abdominal discomfort,
diarrhea & other GI disturbances, antibiotic-associated diarrhea/colitis, stomatitis, infantile hypertrophic pyloric stenosis); Other eff ects (candidal infections, headache)
• Hypersensitivity reactions are uncommon (urticaria, pruritus, rash, rarely anaphylaxis); Rarely cardiotoxicity, hepatotoxicity; Dose-related tinnitus/hearing loss have occurred w/ some macrolides
• Azithromycin & Clarithromycin tend to cause less GI disturbances than Erythromycin
• Clarithromycin may cause tooth & tongue discoloration, dysgeusia
Special Instructions• May take w/ food to decrease gastric distress• Use w/ caution in patients w/ hepatic
dysfunction
Midecamycin 30 mg/kg/day PO divided 6-8 hrly
Roxithromycin 5-8 mg/kg/day PO divided 12 hrly
Spiramycin 50-100 mg/kg/day PO divided 8-12 hrly
Advanced MacrolidesAzithromycin 10 mg/kg/day PO x 3 days
10 mg/kg/day PO x 1 day followed by 5 mg/kg/day PO x 4 days
Clarithromycin 15 mg/kg/day PO divided 12 hrly or>12 yr: 250 mg PO 12 hrly x 7 days
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B178
Pneumonia - Community-Acquired (12 of 16)
All dosage recommendations are for children w/ normal renal & hepatic function unless otherwise stated.Not all products are available or approved for above use in all countries.
Products listed above may not be mentioned in the disease management chart but have been placed here based on indications listed in regional manufacturers’ product information.
Specifi c prescribing information may be found in the latest MIMS.
Dosage Guidelines
OTHER ANTIBIOTICS
Drug Dosage Remarks
GlycopeptideVancomycin ≤1 wk: Initially, 15 mg/kg
slow IV followed by 10 mg/kg 12 hrly 1 wk-1 mth: Initially, 15 mg/kg slow IV followed by 10 mg/kg 8 hrly Infant >1 mth: 40 mg/kg/day slow IV divided 6-12 hrly
Adverse Reactions• Rapid infusion or high dose (≥15-20 mg/kg/hr) is
associated w/ red neck or red man syndrome (erythema multiforme-like reaction w/ intense pruritus, tachycardia, hypotension, rash in the face, neck, upper trunk, back & upper arms)
• CV eff ect (cardiac arrest); CNS eff ects (chills, fever); Dermatologic eff ects (urticaria, macular skin rash); GI eff ect (nausea); Hematologic eff ects (eosinophilia, neutropenia)
Special Instructions• Use w/ caution in patients w/ renal impairment or those
receiving other nephrotoxic or ototoxic drugsLincosamideClindamycin Childn >1 mth: 8-25 mg/
kg/day PO divided 6-8 hrly orNeonates <1 mth: 15-20 mg/kg/day IM/IV divided 6-8 hrly Childn >1 mth: 20-40 mg/kg/day IM/IV divided 6-8 hrly
Adverse Reactions• CV eff ects (hypotension, arrhythmia); CNS eff ects
(dizziness, headache); Dermatologic eff ects (dry skin, erythema, pruritus, rash); GI eff ects (abdominal pain, diarrhea, N/V, pseudomembranous colitis)
Special Instructions• Use w/ caution in patients w/ severe renal or hepatic
impairment, history of atopy, pseudomembranous colitis, regional enteritis, ulcerative colitis, or in patients on antiperistaltic agents (eg opiates, Diphenoxylate w/ atropines)
• Discontinue drug if patient develops signifi cant diarrheaOxazolidinoneLinezolid Infants & Childn <1 yr:
10 mg/kg/dose PO/IV 8 hrly for 10-14 days Childn ≥12 yr: 600 mg PO/IV 12 hrly for 10-14 days
Adverse Reactions• CNS eff ects (dizziness, headache); Dermatologic eff ects
(pruritus, rash); GI eff ects (abdominal pain, diarrhea, N/V, pseudomembranous colitis); Hematologic eff ects (anemia, eosinophilia, leukopenia, pancytopenia); Hepatic eff ects (increases ALT, AST, ALP); Other eff ects (blurred vision, loss of vision, anaphylaxis, dyspnea)
Special Instructions• Avoid use in patients w/ pheochromocytoma,
thyrotoxicosis, or taking sympathomimetics, vasopressive or dopaminergic or serotonergic agents
• Use w/ caution in patients w/ uncontrolled hypertension, history of seizures, severe renal hepatic impairment, pre-existing myelosuppression, phenylketonuria
• Monitor patient’s CBC wkly during therapy
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B179
Pneumonia - Community-Acquired (13 of 16)
All dosage recommendations are for children w/ normal renal & hepatic function unless otherwise stated.Not all products are available or approved for above use in all countries.
Products listed above may not be mentioned in the disease management chart but have been placed here based on indications listed in regional manufacturers’ product information.
Specifi c prescribing information may be found in the latest MIMS.
Dosage Guidelines
OTHER BETA-LACTAMS
Drug Dosage Remarks
CarbapenemsErtapenem 3 mth-12 yr: 30 mg/kg IM/IV
divided 12 hrlyMax dose: 1 g/day
Adverse Reactions• GI eff ects (diarrhea, N/V, antibiotic-associated
diarrhea/colitis, tongue/tooth discoloration, altered taste); Hypersensitivity reactions ranging from mild (eg rash) to severe (eg anaphylaxis) can occur; CNS eff ects (mental disturbances, confusion; Imipenem/cilastatin: Seizures & convulsions have been reported especially in patients w/ history of CNS lesions &/or renal dysfunction); Rarely severe dermatologic reactions (eg exfoliative dermatitis, Stevens-Johnson syndrome, etc) & hepatic eff ects
Special Instructions• Use w/ caution in patients allergic to penicillins,
cephalosporins or other beta-lactams, patients w/ renal impairment
• Imipenem/cilastatin is contraindicated in patients w/ CNS infections
Imipenem/cilastatin
≥3 mth: 50-100 mg/kg IV divided 6 hrlyMax dose: 2 g/day
Meropenem >3 mth-12 yr: 10-20 mg/kg IV 8 hrlyMax dose: 120 mg/kg/day divided over 3-4 doses
MonobactamAztreonam 90-120 mg/kg/day IV divided
6-8 hrlyMax dose: 120 mg/kg/day
Adverse Reactions• Hypersensitivity reactions (rash, urticaria,
pruritus, severe reactions eg anaphylaxis can occur); GI eff ects (diarrhea, N/V, antibiotic-associated diarrhea/colitis); Other eff ect (candidal infections)
Special Instructions• Use w/ caution in patients allergic to penicillins,
cephalosporins or other beta-lactams, & patients w/ renal impairment
OTHER ANTIBIOTICS (CONT’D)
Drug Dosage Remarks
Steroid AntibacterialNa fusidate (Sodium fusidate)
>12 yr: 500 mg PO 8 hrly
Adverse Reactions• GI eff ects (dyspepsia, N/V, epigastric pain, jaundice, change
of liver function); Other eff ect (anorexia)Special Instructions• Use w/ caution in patients w/ hepatic impairment, biliary
obstruction or disease, galactose intolerance, Lapp lactase defi ciency or glucose-galactose malabsorption
• Monitor liver function in patients w/ hepatic dysfunction, biliary pathway abnormalities, high-dose prolonged use, in combination w/ other antibiotics
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B180
Pneumonia - Community-Acquired (14 of 16)
1Dose & frequency are product specifi c & not all products are interchangeable. Please see the latest MIMS for specifi c prescribing information.
All dosage recommendations are for children w/ normal renal & hepatic function unless otherwise stated.Not all products are available or approved for above use in all countries.
Products listed above may not be mentioned in the disease management chart but have been placed here based on indications listed in regional manufacturers’ product information.
Specifi c prescribing information may be found in the latest MIMS.
Dosage Guidelines
PENICILLINS
Drug Dosage Remarks
Benzylpenicillin (Penicillin G, Penicillin G Na, Penicillin G K)
Mild-moderate infection: 25,000-50,000 U/kg/day IM/IV divided 6 hrlySevere infection: 250,000-400,000 U/kg/day IM/IV divided 4-6 hrly
Adverse Reactions• Hypersensitivity
reactions (rash, urticaria, pruritus, severe reactions eg anaphylaxis can occur); GI eff ects (diarrhea, N/V, rarelyantibiotic-associated diarrhea/colitis); Other eff ect (candidal infections)
• Rarely hematologic, renal & hepatic eff ects; High doses may be associated w/ CNS eff ects (encephalopathy, convulsions)
Special Instructions• Avoid in patients w/
Penicillin allergy• Use w/ caution in
patients w/ renal impairment
Phenoxymethylpenicillin (Penicillin V K, Penicillin V)
<12 yr: 25-50 mg/kg/day PO divided 6-8 hrlyMax dose: 3 g/day
Aminopenicillins w/ or without Beta-lactamase InhibitorsAmoxicillin (Amoxycillin) 20-45 mg/kg/day PO divided 8 hrly
High-dose: 80-90 mg/kg/dayAmoxicillin/clavulanic acid1 (Co-amoxiclav, Amoxicillin/clavulanate)
20-45 mg/kg/day PO divided 8-12 hrly based on Amoxicillin or≤3 mth: 60-90 mg/kg/day IV divided 8-12 hrly3 mth-12 yr: 90-120 mg/kg/day IV divided 6-8 hrly
Amoxicillin/sulbactam FC Tab ≥12 yr: 500 mg PO 8 hrly Susp 40-100 mg/kg/day PO divided 8-12 hrly >20 kg: 10-20 mL PO 8-12 hrly2-6 yr: 10 mL PO 8 hrly<2 yr & nursing infant: 5 mL PO 8 hrly or 7.5 mL PO 12 hrlyInj 1 yr or older weighing ≤40 kg: 60-150 mg/kg/day IV/IV infusion divided 8 hrlyMay be increased to 150 mg/kg/day for severe infections Max dose: 4 g Sulbactam/8 g Amoxicillin 24 hrly
Ampicillin 50-100 mg/kg/day PO divided 6 hrly or100-200 mg/kg/day IM/IV divided 6 hrly
Ampicillin/sulbactam (Sultamicillin: Pro-drug of Ampicillin/sulbactam)
<30 kg: 25-50 mg/kg/day PO divided 12 hrly based on Ampicillin≥30 kg: 220-440 mg PO 12 hrly based on Ampicillin or150-200 mg/kg/day IM/IV divided 6-8 hrly
Antistaphylococcal PenicillinsCloxacillin >1 mth & <20 kg: 50-100 mg/kg/day PO divided 6 hrlyFlucloxacillin 25 mg/kg/day PO divided 6 hrly or
<6 mth: 25 mg/kg IM/IV 6 hrly6 mth-2 yr: 25-50 mg/kg IM/IV 6 hrly2-10 yr: 125-250 mg IM/IV 6 hrly
Oxacillin ≥1 mthMild-moderate infection: 100-150 mg/kg/day IM/IV divided 6 hrlySevere infection: 150-200 mg/kg/day IM/IV divided 6 hrly
Antipseudomonal Penicillin w/ or without Beta-lactamase InhibitorPiperacillin/tazobactam <6 mth: 150-300 mg/kg/day IV divided 6-8 hrly
based on Piperacillin≥6 mth: 240 mg/kg/day IV divided 8 hrly based on Piperacillin
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B181
Pneumonia - Community-Acquired (15 of 16)
All dosage recommendations are for children w/ normal renal & hepatic function unless otherwise stated.Not all products are available or approved for above use in all countries.
Products listed above may not be mentioned in the disease management chart but have been placed here based on indications listed in regional manufacturers’ product information.
Specifi c prescribing information may be found in the latest MIMS.
Dosage Guidelines
QUINOLONE
Drug Dosage Remarks
Levofl oxacin 500 mg PO 24 hrly for 7 days
Adverse Reactions• GI disturbances, pruritus, rash, headache, dizziness, vertigo,
drowsiness, insomnia, eosinophilia, leukopenia, astheniaSpecial Instructions• Avoid in patients w/ history of tendon disorder related to
fl uoroquinolones, epilepsy, & G6PD defi ciency• Should be given in childn >18 yr of age• Excessive/direct sun exposure should be avoided
TETRACYCLINES
Drug Dosage Remarks
Doxycycline >8 yr & ≤45 kg:4.4 mg/kg PO 24 hrly on day 1Followed by 2.2 mg/kg PO 24 hrly on subsequent days
Adverse Reactions• GI eff ects (N/V, diarrhea, antibiotic-associated diarrhea/
colitis has occurred, discoloration of teeth, dysphagia, esophageal ulceration has occurred when taken w/ an insuffi cient amount of liqd); Other eff ects (candidal infections, interference w/ skeletal development & bone growth, photosensitivity)
• Rarely renal dysfunction, hepatotoxicity, hematologic eff ects, intracranial pressure w/ headache & visual disturbances; Hypersensitivity reactions have occurred
Special Instructions• Avoid long exposure to sunlight or tanning beds• Take w/ plenty of fl uid while sitting/standing & before bedtime• Avoid in patients ≤8 yr of age• Use w/ caution in renal or hepatic impairment
Tetracycline >8 yr: 25-50 mg/kg/day PO divided 6 hrly
© MIMS Pediatrics 2020
© MIM
S

PNEU
MON
IA (C
AP)
B182
Pneumonia - Community-Acquired (16 of 16)
All dosage recommendations are for children w/ normal renal & hepatic function unless otherwise stated.Not all products are available or approved for above use in all countries.
Products listed above may not be mentioned in the disease management chart but have been placed here based on indications listed in regional manufacturers’ product information.
Specifi c prescribing information may be found in the latest MIMS.Please see the end of this section for the reference list.
Dosage Guidelines
VACCINES
Drug Dosage Remarks
Vaccine, pneumococcal [Pneumococcal polysaccharide conjugate vaccine, 10-valent (PCV10)]
0.5 mL/dose IM3-dose primary series: 3 doses at 1-mth intervals beginning at 2 mth1 of ageBooster dose given at least 6 mth after the last primary dose & preferably between 12th & 15th mth2-dose primary series: 1st dose at 2 mth, 2nd dose 2 mth later; booster dose same as 3-dose primary series7-11 mth, previously unvaccinated: 1st 2 doses given 1 mth apart followed by 3rd dose in the 2nd yr w/ at least 2-mth interval12-23 mth, previously unvaccinated: 2 doses at least 2 mth apart1-5 yr, previously vaccinated: 2 doses at least 2 mth apart
Adverse Reactions• Inj site reactions,
irritability, fever, loss of appetite
Special Instructions• Administer in
anterolateral aspect of thigh or deltoid muscle of upper arm- Administer SC in
patients w/thrombocytopenia or bleeding disorder
• Contraindicated in patients w/ hypersensitivity to any vaccine component
• Defer vaccination for patients w/ acute severe febrile illness
• Use w/ caution in immunodefi cient patients or in patients on immunosuppressive treatment
Vaccine, pneumococcal [Pneumococcal polysaccharide conjugate vaccine, 13-valent (PCV13)]
0.5 mL/dose IMInfant3-dose primary series: 3 doses at 2-mth intervals beginning at 2 mth1 of ageBooster dose between 12-15 mth of age2-dose primary series: 1st dose at 2 mth, 2nd dose 2 mth laterBooster dose between 11-15 mth of age7-11 mth, previously unvaccinated: 1st 2 doses given 1 mth apart followed by 3rd dose in the 2nd yr at least 2 mth after 2nd doseChildn12-23 mth, previously unvaccinated: 2 doses at least 2 mth apart12-23 mth incompletely vaccinated w/ 1 dose of PCV13 <12 mth: 2 doses at least 2 mth apart12-23 mth incompletely vaccinated w/ 2-3 doses of PCV13 <12 mth: 2 doses at least 2 mth apart24-71 mth incompletely vaccinated w/ PCV13: 1 dose at least 2 mth from the 1st dose2-17 yr, previously unvaccinated: Single doseInfant & ChildnPreviously vaccinated w/ pneumococcal 7-valent vaccine: May switch at any point in the schedule
Vaccine, pneumococcal [Pneumococcal polysaccharide vaccine, 23-valent (PCV23)]
0.5 mL/dose IM/SC ≥2 yr: Single dose & at least 2 mth after the fi nal dose of PCV13 Revaccination: 5 yr after the 1st dose in immunocom-promised patients
1May be given as early as 6 wk old
© MIMS Pediatrics 2020
© MIM
S