Please Silence Your Cell Phones Meeting (CM)/CM10-15/DDx Fatty Liver...• Ranges from hepatocytes...
63
Please Silence Your Cell Phones Thank You
Transcript of Please Silence Your Cell Phones Meeting (CM)/CM10-15/DDx Fatty Liver...• Ranges from hepatocytes...

Please Silence Your Cell Phones
Thank You

Disclosure of Relevant Financial Relationships
The USCAP requires that anyone in a position to influence or control the content of all CME activities disclose any relevant relationship(s) which they or their spouse/partner have,
or have had within the past 12 months with a commercial interest(s) [or the products or services of a commercial interest] that relate to the content of this educational activity and create a conflict of interest. Complete disclosure information is maintained in the USCAP
office and has been reviewed by the CME Advisory Committee.
Dr. (Elizabeth Brunt) declares consulting work for Rottapharm.

Ddx of Fatty Liver Disease:
Not the Usual Culprits
Elizabeth M. Brunt
Department of Pathology and Immunology
Hans Popper HepatopathologyCompanion Society
March 22, 2015

Outline• Why is this important to discuss?
– Epidemiology of fatty liver
• What are the usual culprits– IR– Alcohol
• What are the Not-So-Usual culprits?

What is NAFLD, 2015
• Fatty infiltration– ? Tumoral infiltrates?– ? Primary or Mets?
• Simple steatosis– What is it about metabolic pathways
that result in triglyceride accumulation is simple?
• Puhleeeeezzzz don’t say:

What is NAFLD, 2015
• A spectrum of liver diseases with macrofat– NOT related to excess
alcohol intake
• Ranges from hepatocytes with >5% macrovesicularsteatosis– Large and small droplet
• PLUS inflammation– Lobular +/- portal
• PLUS hepatocyte injury (ballooning)
• +/- fibrosis in varying patterns of distribution

What is NAFLD, 2015
• A spectrum of liver diseases with macrofat– NOT related to excess
alcohol intake
• +/- liver cell injury• +/- cirrhosis• +/- liver carcinoma
– HCC– Any primary liver carcinoma
with or without cirrhosis
• Ranges from hepatocytes with >5% macrovesicularsteatosis– Large and small droplet
• PLUS inflammation– Lobular +/- portal
• PLUS hepatocyte injury (ballooning)
• +/- fibrosis in varying patterns of distribution

NAFLD, 2015: Epidemiology• Purists: require biopsy for liver fat >5%, NASH• Imagers: trust various modalities
– Ultrasound– CT – MR
• Proton MR spectroscopy (1H-MRS)• PDFF: standardized MR-based biomarker of tissue fat
concentration; uses MRS or MRI (Reeder, Hu, Sirlin*)
• Reviewers: gov-based population studies• Realists:
*JMRI 2012; 36:1011-1014

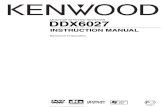
NAFLD, 2015: EpidemiologyPurists
• Outpatients to Brooke Army Medical Base400
outptsenrolled
328 completed
US
156 pos: 48%
NAFLD
LIVER BIOPSY:
5 were NORMAL
22 refused liver biopsy
Williams, et al. Gastroenterol 2011;140:124-131

NAFLD, 2015: EpidemiologyPurists
• Outpatients to Brooke Army Medical Base48% with
NAFLD
Hispanics (58%) > Caucasians (44% ) > African Americans (35%)
Men: 59%Obese: 68%Older
Williams, et al. Gastroenterol 2011;140:124-131

NAFLD, 2015: EpidemiologyPurists
• Outpatients to Brooke Army Medical Base48% with NAFLD
NASH
by bx: n=40
12.2% total
29.9% US pos
Fibrosis St 2-4:
2.7% of cohort
NASH Prevalence amongst all 328:
12.2%
Men 65%Higher BMI, IR, ALT, AST
Hispanics (19.4%) > African Americans (13.5%) >Caucasians (9.7%)
Williams, et al. Gastroenterol 2011;140:124-131

NAFLD, 2015: EpidemiologyPurists
• Outpatients to Brooke Army Medical Base48% with
NAFLD
NASH by bx: 29.9%
Fibrosis St 2-4:
2.7% of cohort
54 Diabetics
74% had NAFLD
22% had NASH
NASH Prevalence amongst all 328:
12.2%
Men 65%Higher BMI, IR, ALT, AST
Hispanics (19.4%) > African Americans (13.5%) >Caucasians (9.7%)
Williams, et al. Gastroenterol 2011;140:124-131
0
50
100
150
200
250
300
350
400
450
TotalEnrolled
CompletedQ-R, US
NAFLD NASH
OutPatientColumn1Psoriasis#REF!
NAFLD, 2015: EpidemiologyPurists
Williams, et al. Gastroenterol 2011;140:124-131; Roberts, et al. Aliment Pharm Therap 2015;41:293-300.

0102030405060708090
OutPtPsoriasis
NAFLD, 2015: EpidemiologyPurists
%
Williams, et al. Gastroenterol 2011;140:124-131; Roberts, et al. Aliment Pharm Therap 2015;41:293-300.

NAFLD, 2015: EpidemiologyImagers: US
• Ultrasound– Noninvasive– Least expensive, most
available– Low sensitivity, specificity
• Difficult to ddx steatosis, fibrosis
– Machine and operator dependent
– Doesn’t reliably detect steatosis < 30%
• In United States, prevalence of NAFLD by US is…17-51% *(yikes!)– Obesity: 90%*
– T2DM: 69%**
– Hispanic men: 45%***
Chalasani, Hepatology 2012 Vernon, Alimen Pharm Therap 2011 Browning, Hepatology 2004

• Quantitative US– One study published
to date; from UCSD– Comparator group
was MRI-PDFF– 2 year study of 204
subjects randomized to training and validation sets
– NAFLD in each group was 69%
• Back scatter calculation of QUS v MRI-PDFF
Spearman P 0.8, p<0.0001AUC (training): 0.98
• QUS is inexpensive, algorithms in place to reduce operator, machine error sources
• Can be done on any US machine
NAFLD, 2015: EpidemiologyImagers: QUS
Lin et al, Clin Gastro Hepatol 2015, epub accepted manuscript
Training Validation
Sensitivity 93% 87%Specificity 97% 91%Pos Predict Value 99% 95%Neg Predict Value 86% 76%
• Noninvasive, but involves radiation
• 100% specificity at >30% steatosis, but difficult to quantify steatosis
NAFLD, 2015: EpidemiologyImagers: CT

NAFLD, 2015: EpidemiologyImagers: 1H-MR Spectroscopy
Urban population, Dallas County 34% prevalence
0%
10%
20%
30%
40%
50%
60%
Population
IHTG >5.5%
Browning, et al. Hepatology 2004;40:1387-1395.
(2,240)

NAFLD, 2015: EpidemiologyImagers: 1H-MR Spectroscopy
Urban population, Dallas County 34% prevalence
0%
10%
20%
30%
40%
50%
60%
Population
IHTG >5.5%
Browning, et al. Hepatology 2004;40:1387-1395.
(2,240)
0%10%20%30%40%50%60%70%80%90%
Population
IHTG >5.5%
Wong, et al. Gut 2012;61:409-415
(900)
Urban population, Hong Kong 27.3% prevalence

• Proton-density fat fraction – maps the entire liver– correlates well in adults
for quantitative measurements of hepatic steatosis
– PDFF was better than biopsy for steatosis over time in clinical trials1
– Costly– Not widely available
NAFLD, 2015: EpidemiologyImagers: MRI-PDFF
1Noureddin, et al. Hepatology 2013; 58:1930-1940

• ? “American Exceptionalism”
• Genetic, epigenetic
• Environmental
NAFLD, 2015: EpidemiologyPopulation
Loomba et al, Nat Rev Gastroenterol Hepatol 2013; 10:686-690.
Reprinted with permission from TheimePublishing, Lic #3560830451577.

Usual Culprits
• Insulin Resistance • Alcohol (? How, how much and in whom)
• “ 2 doses/day”
• Men: >60g/d; Women: >10-20g/d

Usual Culprits
• Insulin Resistance • Alcohol (? How, how much & in whom)
• “ 2 doses/day”
• Men: >60g/d; Women: >10-20g/d
FLD; Cirrh; HCC
Hyperlipidemia
Truncal Obesity

Not-So-Usual Culprits
• Disordered Gut• Lipodystrophic Syndromes• Medications• Storage Disorders• Viral Hepatitis• The W’s

Not-So-Usual Culprits: Disordered (malabsorptive) GutThe Normal Gut: from the perspective of a hepatopathologist!

• Fat accumulates in the liver at both ends of the nutritional spectrum…– Over (obesity)– Under (protein/calorie)
malnutrition
Not-So-Usual Culprits: Disordered (malabsorptive) Gut
Reilly, et al. J Hepatol 2015; http://dx.doi.org/10.1016/j.jhep.2015.01.013

Not-So-Usual Culprits: Disordered (malabsorptive) Gut
Kummen, et al. Best Pract Res Clin Gastroenterol 2013;27:531-542.; reprinted with permission.

Not-So-Usual Culprits: Disordered (malabsorptive) Gut
Kummen, et al. Best Pract Res Clin Gastroenterol 2013;27:531-542; reprinted with permission.

• Inflammatory Bowel Disease: 5-10% elev TA’s– Associations in order of frequency PSC, NAFLD,
cholelithiasis, AIH, PBC
Kummen et al. Best Pract Res Clin Gastroenterol 2013;27:531-542; Vo et al. JPGN, 2014;59:288-299.
Not-So-Usual Culprits: Disordered (malabsorptive) Gut

• Inflammatory Bowel Disease: 5-10% elev TA’s– Associations in order of frequency PSC, NAFLD,
cholelithiasis, AIH, PBC…and…• AIH-PSC overlap• DILI: MTX and steroids • Granulomatous liver disease• Abscess• Budd-Chiari or portal vein thrombosis• Hepatic amyloidosis• CCa
Kummen, et al. Best Pract Res Clin Gastroenterol 2013;27:531-542 ; Vo, et al. JPGN, 2014;59:288-299.
Not-So-Usual Culprits: Disordered (malabsorptive) Gut

IBD and Steatosis/SH• UC and NAFLD: 1st described in 1873• Up to 36-50% of all IBD pts have steatosis;
hepatomegaly is unusual– Toxemia, malnutrition, prednisone, parenteral
nutrition– Related to severity of colonic involvement– May persist after colectomy
De Boer et al, Scand J Gastro 2008; 43:604-608; Kummen, et al. Best Pract Res Clin Gastroenterol 2013;27:531-542.

• Celiac Disease– Found in 1% of European and NA populations
10% of subjects with unexplained liver test elevations 3.5% of NAFLD subjects1
– “Celiac hepatitis” (after r/o AIH, PBC, PSC, GSRH)• mild steatosis, KC hyperplasia, mild mononuclear infiltrate, mild fibrosis; reversible with diet
(Maggiore, 2003)
– Possible causes of steatosis/steatohepatitis in CD• Malabsorption/chronic deficiency of lipotropic factor• Increased intestinal permeability, similar to SIBO;
increased translocation of bacterial toxin, other ags to liver– Increased risk of NAFLD in newly diagnosed Celiac2
• Highest in first year after Celiac dx, but can remain • Most commonly in children with Celiac
Not-So-Usual Culprits: Disordered (malabsorptive) Gut
1Abenavoli, et al. Minerva Gastroenterol Dietol 2013;59:89-95; 2Reilly, J Hepatol 2015; http://dx.doi.org/10.1016/j.jhep.2015.01.013

• Cystic Fibrosis: liver disease is now the most important nonpulmonary COD in CF
• While we usually think of the “focal biliary cirrhosis” in CF…
• “the most prevalent liver histopathologicfinding is … steatosis…noted in up to 60% of subjects”. – Attributed to overall malnutrition and CF related
deficiencies: EFA, carnitine, choline
Not-So-Usual Culprits: Disordered (malabsorptive) Gut
Vo et al. JPGN, 2014;59:288-299.
Not-So-Usual Culprits: Lipodystrophy
• Rare syndromes associated with IR-T2DM, dyslipidemia and NAFLD/NASH; some also assoc with premature aging
• Atrophy of body fat– Partial or generalized– Congenital or acquired
• Impairment of adipogenesis; deregulation of adipocyte droplets (perilipins)
• Leptin deficiency, PPAR dysfunction; nuclear envelope protein (lamin-B) dysfunction
• One of best known associations is ART in HIV– Partial lipodystrophy and IR
Guenantin et al. Semin Cell Dev Bio 2014;29:148-157.

Not-So-Usual Culprits: Medications
Steatosis• Corticosteroids
– Steatosis, glycogenosis– SH: exacerbation > de novo– Rarely implicated in progressive FLD
• Methotrexate– Steatosis, hepatocellular unrest,
nuclear pleomorphism– Beware: SH and/or Z3 psf may mean
concurrent Met Syn or alcohol exposure
– Fibrosis in MTX begins portal, periportal; can lead to cirrhosis
– Fibrosis most often occurs in presence of concurrent co-factors: Met Synd, DM, EtOH
Steatohepatitis• Tamoxifen
– Fatty liver: up to 1/3 of users; SH less common
– Fibrosis occurs; cirrhosis > 3-5 yrs use
– Steatosis is more common in W with elev BMI, but not related to EtOH; drug does not cause wt gain
• Amiodarone– Usually ALT, AST ( = ) elev but can
be cholestatic– Can see ballooning, MDB without
steatosis– Can lead to cirrhosis– Slow to accrue, slow to dissipate
from lipids in cell membranesLiverTox.NIH
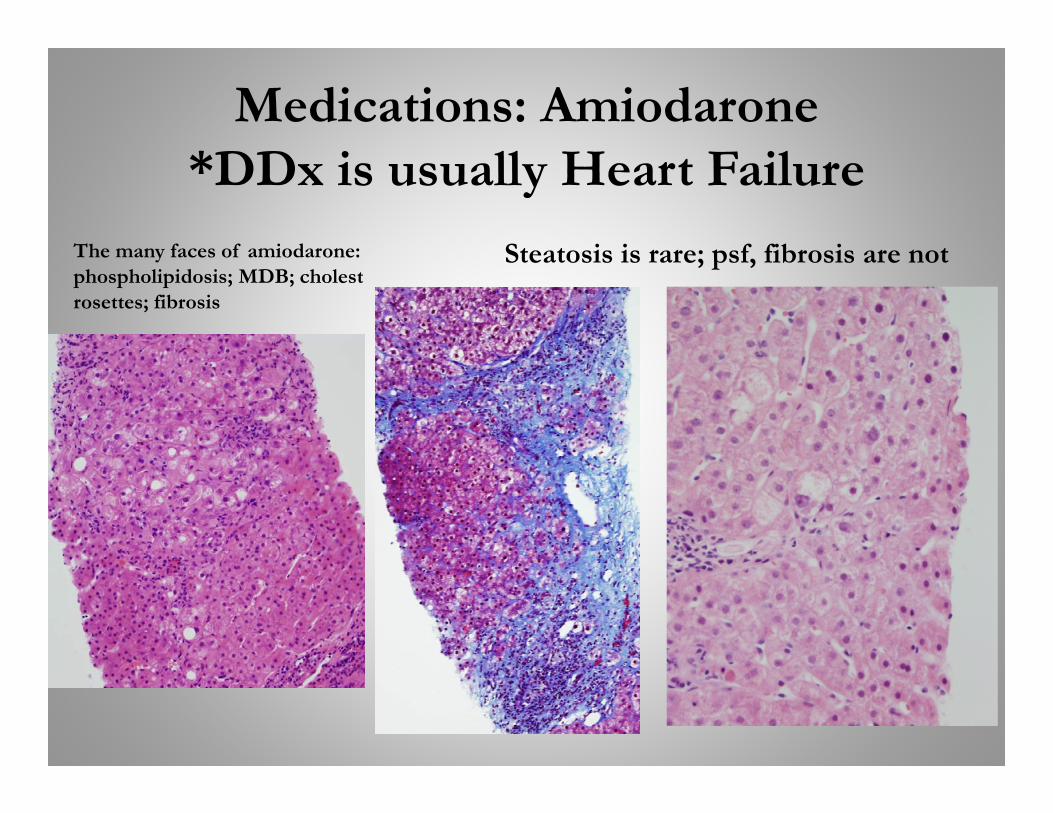
Medications: Amiodarone*DDx is usually Heart Failure
The many faces of amiodarone: phospholipidosis; MDB; cholestrosettes; fibrosis
Steatosis is rare; psf, fibrosis are not

• LAL deficiency: chol esters and TG cannot be removed from hepatocytes and Kupffer cells
Not-So-Usual Culprits: Storage Disorders
Review: 135 Cases in LiteratureJ Hepatol 2013;58:1230-1243
LAMP-1 and cathepsin D IHC for lysosome staining
Cathepsin D in -oxidation defect Steatosis, Chol in EM of CESD case
Reprinted with permission from Elsevier

• LAL deficiency: Wolman and CESD– Autosomal recessive; LIPA mutations ( > 40); trans-ethnic
• WD is RARE and fatal by 3-4 mos old– CESD is a spectrum depending on LAL activity
• Estimated to affect ~ 1/40,000; considered underestimate• Can present in infancy, childhood or up to mid-late adult• USUALLY PRESENTS AS FIBROTIC LIVER DISEASE
WITH FAT…DDX IS NAFLD/NASH• HSM, type IIb hyperlipoproteinemia (elev serum LDL chol, TG,
normal or low HDL chol)• Liver transplant or liver failure or accel ASVD early demise
Not-So-Usual Culprits: Storage Disorders
Bernstein et al. J Hepatol 2013;58:1230-1243.

Not-So-Usual Culprits: Viral HepatitisViral v Metabolic Steatosis
• HCV – Zone 1: Virus; Zone 3 steatosis +/- perisinusoidal fibrosis: Host– Gt 1, 4, other non-3: incite IR = METABOLIC STEATOSIS– Gt 3: core protein causes steatosis = VIRAL STEATOSIS– Concurrence: Met Syn +/- ALD…
• ballooning, MDB, satellitosis, sinusoidal fibrosis
– Coexistent ALD increases speed of progression
Negro, J Hepatol 2014; 61:S69-S78

Not-So-Usual Culprits: Viral HepatitisViral v Metabolic Steatosis
• HCV – Zone 1: Virus; Zone 3 steatosis +/- perisinusoidal fibrosis: Host– Gt 1, 4, other non-3: incite IR = METABOLIC STEATOSIS
– Gt 3: core protein causes steatosis = VIRAL STEATOSIS
– Concurrence: Met Syn +/- ALD…• ballooning, MDB, satellitosis, sinusoidal fibrosis
– Coexistent ALD increases speed of progression
Negro, J Hepatol 2014; 61:S69-S78

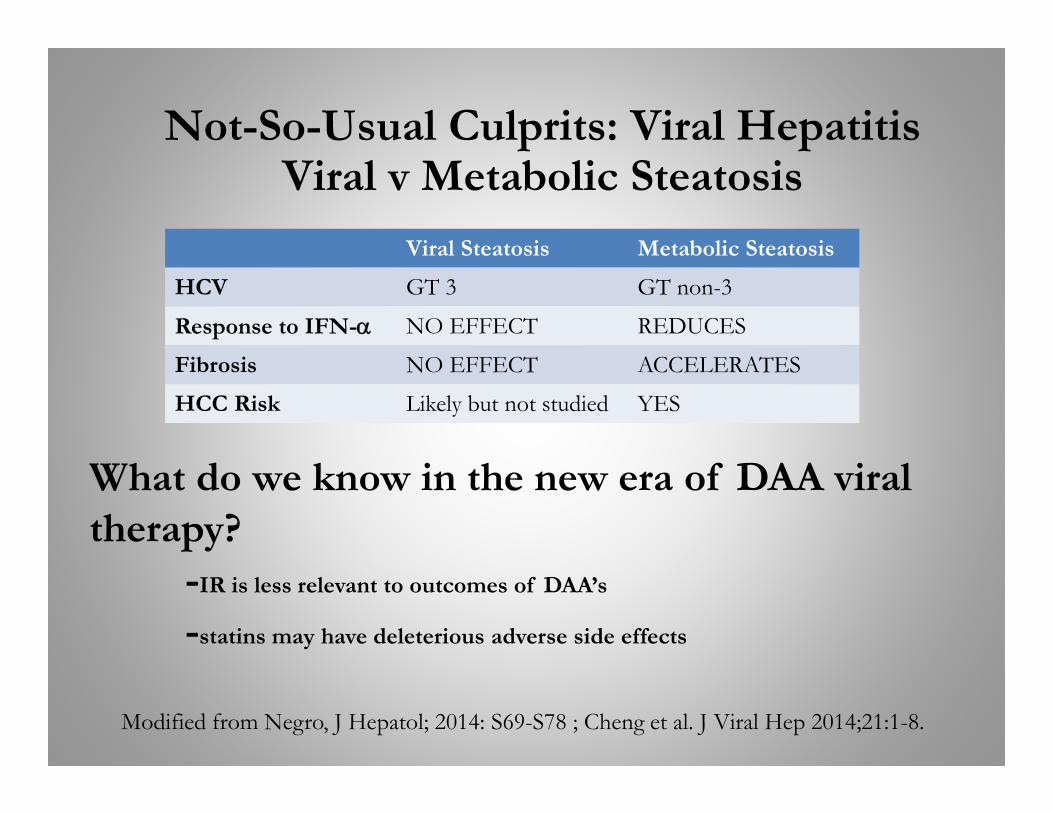
Not-So-Usual Culprits: Viral HepatitisViral v Metabolic Steatosis
Viral Steatosis Metabolic Steatosis
HCV GT 3 GT non-3
Response to IFN- NO EFFECT REDUCES
Fibrosis NO EFFECT ACCELERATES
HCC Risk Likely but not studied YES
Modified from Negro, J Hepatol; 2014: S69-S78
Not-So-Usual Culprits: Viral HepatitisViral v Metabolic Steatosis
Viral Steatosis Metabolic Steatosis
HCV GT 3 GT non-3
Response to IFN- NO EFFECT REDUCES
Fibrosis NO EFFECT ACCELERATES
HCC Risk Likely but not studied YES
Modified from Negro, J Hepatol; 2014: S69-S78 ; Cheng et al. J Viral Hep 2014;21:1-8.
What do we know in the new era of DAA viral therapy?
-IR is less relevant to outcomes of DAA’s
-statins may have deleterious adverse side effects

Not-So-Usual Culprits: Viral HepatitisViral v Metabolic Steatosis
• HCV – Zone 1: Virus; Zone 3 steatosis +/- perisinusoidal fibrosis: Host– Gt 1, 4: incite IR = METABOLIC STEATOSIS– Gt 3: core protein causes steatosis = VIRAL STEATOSIS– Concurrence: Met Syn +/- ALD…ballooning, MDB, satellitosis, sinusoidal fibrosis– Coexistent ALD increases speed of progression
• HBV– Meta-analysis of 21 studies, > 4,000 patients2
– Present in up to 1/3 of patients, but usually mild, sometimes moderate; ranged 14-70%
– Most common assoc: male, older, Met Syn features, alcohol; NO VIRAL FACTORS
– ? Protective effect of virus on steatosis– No effect on histologic progression
• Labrea Hepatitis (acute HDV)– Coinfection/superinfection with HBV; South America– Microvesicular or macrovesicular steatosis
Negro, J Hepatol 2014; 61:S69-S78; 2Machado et al. JGH 2011;21:1361-1367.
Not-So-Usual Culprits: The W’s
Weber-Christian Disease with Hepatic Involvement
• Systemic illness• Lobular panniculitis of subQ
fat, recurring febrile episodes• Unusual for liver to be
involved….but reported – Presents with transaminitis,
“fatty liver”– LOOKS LIKE SH ON BX
• Treatment is steroid therapy, other immunosuppression
Wilson Disease

Not-So-Usual Culprits: The W’s
Weber-Christian Disease with Hepatic Involvement
• Systemic illness• Lobular panniculitis of subQ
fat, recurring febrile episodes• Unusual for liver to be
involved….but reported – Presents with transaminitis,
“fatty liver”– LOOKS LIKE SH ON BX
• Treatment is steroid therapy, other immunosuppression
Wilson Disease
• The “lupus” of liver disease but can have steatosis as a major finding



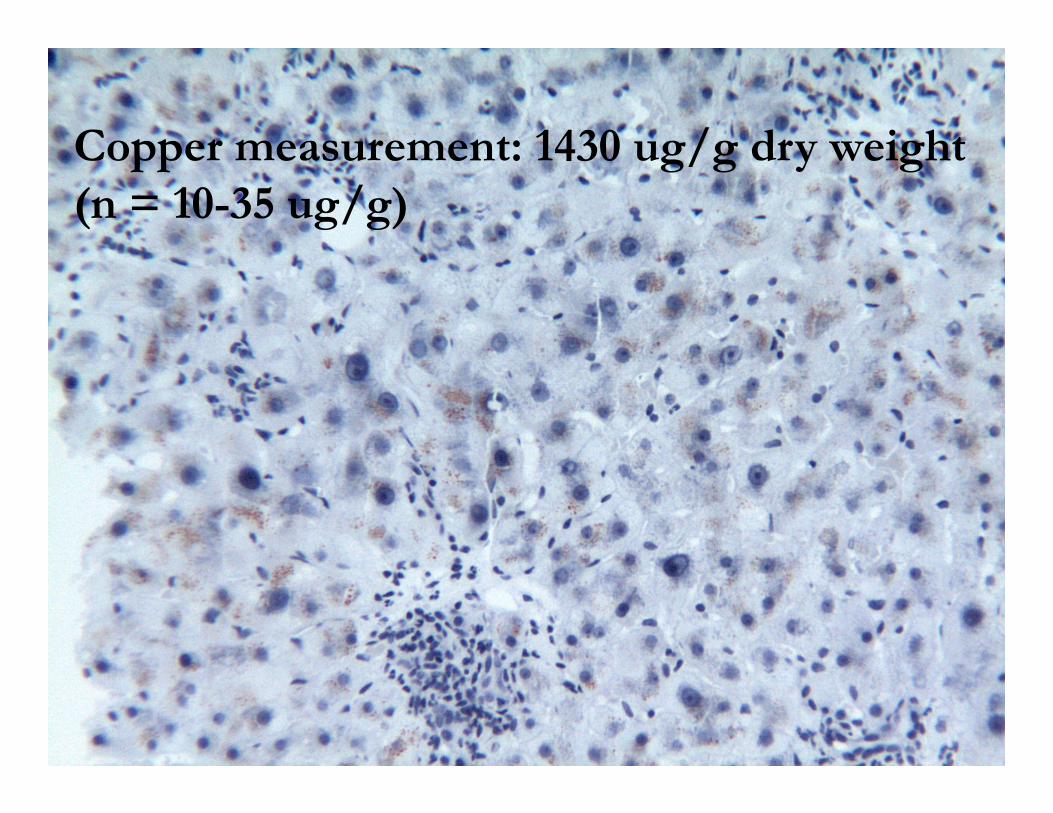
Copper measurement: 1430 ug/g dry weight (n = 10-35 ug/g)

(NA)FLD/(NA)SH: Culprits to know
Significant
• IR/Alcohol–T2DM
• Viral Hepatitis C; B+D• Malnutrition
– IBD– Celiac Sprue
• CESD• Certain medications
– Tamoxifen– Amiodarone– Methotrexate– Steroids
• Wilson Disease• Weber-Christian Disease
+/- Obesity, Metabolic Syndrome
(NA)FLD/(NA)SH: Culprits to know
Significant• IR/Alcohol
– T2DM
• Viral Hepatitis C; B+D
• Malnutrition– IBD– Celiac Sprue
• CESD
• Certain medications– Tamoxifen– Amiodarone– Methotrexate– Steroids
• Wilson Disease• Weber-Christian Disease

(NA)FLD/(NA)SH: Culprits to know
Significant
• IR/Alcohol– T2DM
• Viral Hepatitis C; B+D
• Malnutrition– IBD– Celiac Sprue
• CESD
• Certain medications– Tamoxifen– Amiodarone– Methotrexate– Steroids
• Wilson Disease• Weber-Christian Disease
Macro, large/small
True Micro
KC Steatosis
Ballo-oning, MDB
PSF may be clue
Risk of HCC, Cirrh or NON-C
Met Synd + + ++ + ++ ++
ALD + + ++ + ++ +; +/-
Viral Hep + * * ++
Malnutrit-tion
+ *
CESD small ++
Tamoxifen + + + +
Amiodar +/- ++ VOO
Methotrexate
+ ++ Zone 1
Steroids +
WD + + ++ +
WCD + MDB +* Concurrent NASH/ASH

(NA)FLD/(NA)SH: Culprits to know
Significant• IR/Alcohol
– T2DM– Psoriasis
• Viral Hepatitis C; B+D• Malnutrition
– IBD– Celiac Sprue
• CESD• Certain medications
– Tamoxifen– Amiodarone– Methotrexate– Steroids
• Wilson Disease• Weber-Christian Disease
• Metabolic disorders– Galactosemia– GSD I and III– Hereditary Fructose
Intolerance– Nieman Pick C– Tyrosinemia
• Cystic Fibrosis• Heat Stroke• Ischemic liver
Steatosis and elevated TA’s

(NA)FLD/(NA)SH: Culprits to know
Significant• IR/Alcohol
– T2DM– Psoriasis
• Viral Hepatitis C; B+D• Malnutrition
– IBD– Celiac Sprue
• CESD• Certain medications
– Tamoxifen– Amiodarone– Methotrexate– Steroids
• Wilson Disease• Weber-Christian Disease
Steatosis and elevated TA’s
• Metabolic disorders– Galactosemia– GSD I and III– Hereditary Fructose
Intolerance– Nieman Pick C– Tyrosinemia
• Cystic Fibrosis• Heat Stroke• Ischemic liver
Mitochondriopathies
• Clinical settings are very different
• Acute liver failure, SIDS
• Reye’s• Urea cycle
defects• AFLP
• Microvesicularsteatosis


Please go to the USCAP website to complete your Evaluation of
the course and claim CME and/or SAMs Credits.
Thank You!


Fatty Liver Disease
• Can a patient have more than one process that results in the same/similar microscopic features?– HCV + NAFLD/NASH or HCV + ALD/ASH
• Patients with MetSynd or ALD
• What are criteria for suggesting/diagnosing such?– In addition to portal-based features of …HCV…
• Zone 3 PSF1
• Zone 3 ballooning2
• Does harmful lipid overload always have to be in hepatocytes? – Vit A toxicity: Stellate cell loading…psf
1Brunt et al. Mod Pathol 2003;16:49-56; 2Bedossa et al. Hepatology 2007;46:380-387.

HCV (+ SH)
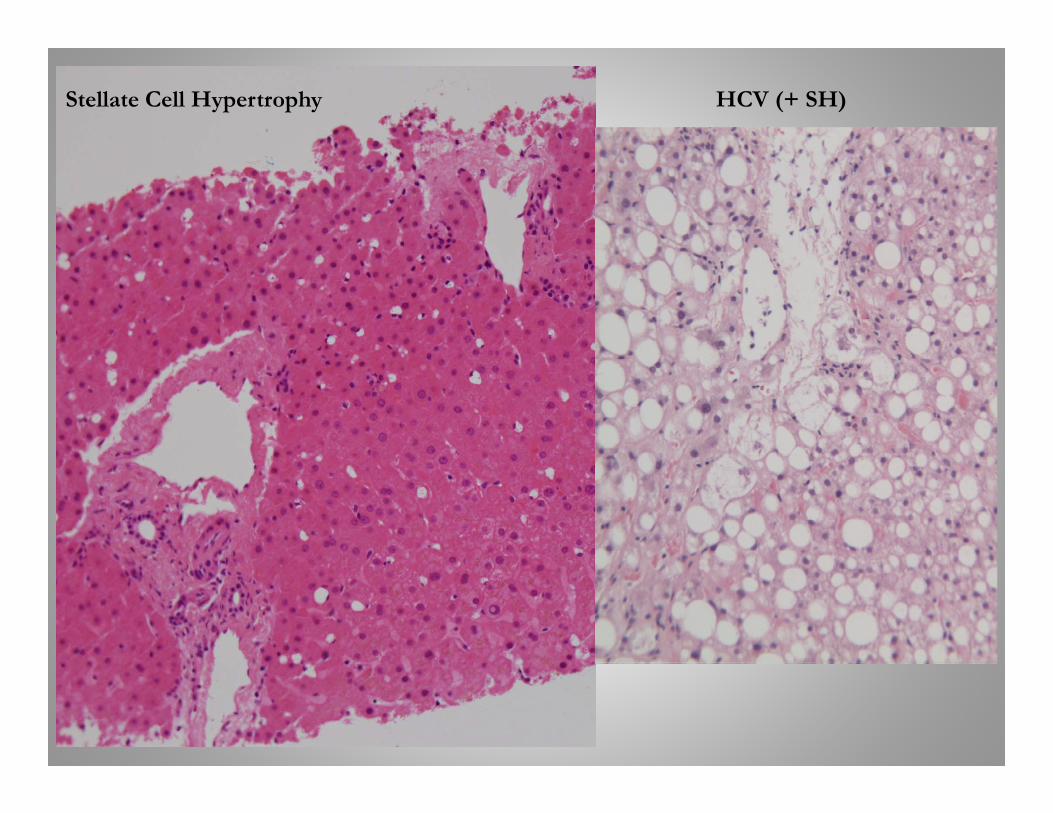
HCV (+ SH)Stellate Cell Hypertrophy

Usual Culprits of Fat in Liver
• Insulin Resistance • Obese, BMI < 40, non-DM, no
other serious complic• Metabolically Normal Obese
– < 5.6% IHTG (defn)– Protected from all metabolic
consequences of weight gain of ~ 6%
– Lipogenic pathways in fat stores
• Metabolically Abnormal Obese– > 5.6% IHTG; all parameters
worsened with similar weight gain– No adaptation by fat stores
Fabrinni, et al. JCI 2015; doi:10.1172/JCI78425.
Which statement below is true????
IR = Obesity = Fatty Liver
Obesity = IR = Fatty Liver
Fatty Liver = IR = Obesity
Fatty Liver = Obesity = IR

Usual Culprits of Fat in Liver
• Insulin Resistance • Obese, BMI < 40, non-DM, no
other serious complic• Metabolically Normal Obese
– < 5.6% IHTG (defn)– Protected from all metabolic
consequences of weight gain of ~ 6%
– Lipogenic pathways in fat stores
• Metabolically Abnormal Obese– > 5.6% IHTG; all parameters
worsened with similar weight gain– No adaptation by fat stores
Fabrinni, et al. JCI 2015; doi:10.1172/JCI78425.
Which statement below is true????
IR = Obesity = Fatty Liver
Obesity = IR = Fatty Liver
Fatty Liver = IR = Obesity
Fatty Liver = Obesity = IR
None are completely true!

Usual Culprits of Fat in Liver
• Insulin Resistance • Obese, BMI < 40, non-
DM, no other serious complic
• Metabolically Normal Obese– < 5.6% IHTG (defn)
• Metabolically Abnormal Obese– > 5.6% IHTG
• MetN – O vs MetAbn – O
– 6% wt gain, fast food diets
– Protected from all metabolic consequences of weight gain of ~ 6%
– Lipogenic pathways in fat stores
– All parameters worsened with similar weight gain
– No adaptation by fat stores
Fabrinni, et al. JCI 2015; doi:10.1172/JCI78425.