
PhD thesis
54
Clinical aspects of ghrelin: Pharmacokinetics and metabolic effects PhD dissertation Esben Thyssen Vestergaard, MD Faculty of Health Sciences University of Aarhus 2008
-
Upload
esben-vestergaard -
Category
Documents
-
view
73 -
download
3
Transcript of PhD thesis

Clinical aspects of ghrelin: Pharmacokinetics and
metabolic effects
PhD dissertation
Esben Thyssen Vestergaard, MD
Faculty of Health Sciences University of Aarhus 2008

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Clinical aspects of ghrelin: Pharmacokinetics and
metabolic effects
PhD dissertation
Esben Thyssen Vestergaard, MD
Faculty of Health Sciences University of Aarhus Medical Department M and Medical Research Laboratories Aarhus University Hospital DK-8000 Aarhus C Denmark
1

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Publications This dissertation is based on the following articles
i. ET Vestergaard, TK Hansen, LC Gormsen, P Jakobsen, N Møller, JS Christiansen,
JOL Jørgensen. Constant intravenous ghrelin infusion in healthy young men: Clini-
cal pharmacokinetics and metabolic effects. 2007. American Journal of Physiology
– Endocrinology and Metabolism 292(6): E1829-1836.
ii. ET Vestergaard, CB Djurhuus, J Gjedsted, S Nielsen, N Møller, JJ Holst, JOL Jør-
gensen, O Schmitz. Acute effects of ghrelin administration on glucose and lipid
metabolism. 2007. Journal of Clinical Endocrinology & Metabolism. Epub.
iii. ET Vestergaard, LC Gormsen, N Jessen, S Lund, TK Hansen, N Møller, JOL Jør-
gensen. Ghrelin infusion in humans induces acute insulin resistance and lipolysis
independent of GH-signaling. Article submitted for publication.
2

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Contents Publications ............................................................................................................... 2 Contents .................................................................................................................... 3 List of abbreviations ................................................................................................... 6 Preface ...................................................................................................................... 8 Background...............................................................................................................10 Methods ...................................................................................................................12
Subjects ................................................................................................................12
Pharmacokinetic study ........................................................................................12
Somatostatin study .............................................................................................13
Hypopituitary study.............................................................................................13
Study design..........................................................................................................14
Pharmacokinetic study ........................................................................................14
Somatostatin study .............................................................................................15
Hypopituitary study.............................................................................................16
Pharmacokinetic modeling ......................................................................................17
Tracers..................................................................................................................19
Indirect calorimetry................................................................................................20
Microdialysis ..........................................................................................................21
Western blotting and PI3K assay.............................................................................21
Analyses................................................................................................................22
Statistics................................................................................................................23
Summary of results ...................................................................................................24 Pharmacokinetic study............................................................................................24
Ghrelin pharmacokinetics ....................................................................................24
Correlations........................................................................................................24
Hormones and metabolites..................................................................................24
Appetite .............................................................................................................25
Somatostatin study ................................................................................................26
Hormones and metabolites..................................................................................26
Indirect calorimetry ............................................................................................26
Glucose and palmitate metabolism.......................................................................27
Correlations........................................................................................................28
Interstitial glycerol concentrations .......................................................................28
Hypopituitary study................................................................................................29
3

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Hormones and metabolites..................................................................................29
Resting energy expenditure.................................................................................30
Glucose metabolism and substrate oxidation ........................................................30
Lipid metabolism ................................................................................................30
Regional substrate metabolism (microdialysis)......................................................31
GH and insulin signaling......................................................................................31
Discussion.................................................................................................................31 Methodological considerations ................................................................................31
Pharmacokinetic study ........................................................................................31
Somatostatin study .............................................................................................32
Hypopituitary study.............................................................................................33
Considerations of possible mechanisms and explana- ...............................................33
tions - implications and review of literature..............................................................33
Endogenous ghrelin excursions and previous pharmacokinetic studies ...................33
Pharmacokinetics in a clinical context...................................................................33
Predictors of ghrelin levels ..................................................................................34
Effects on appetite..............................................................................................35
Hormonal and metabolite effects .........................................................................35
Effects on substrate metabolism ..........................................................................36
Effects on resting energy expenditure ..................................................................38
Methodological limitations and pitfalls .....................................................................38
Pharmacokinetic study ........................................................................................38
Somatostatin study .............................................................................................39
Hypopituitary study.............................................................................................40
Conclusions & Perspectives.....................................................................................40
Conclusions ........................................................................................................40
Perspectives .......................................................................................................41
Summary ..................................................................................................................43 Summary in Danish ...................................................................................................44 Acknowledgements....................................................................................................45 References................................................................................................................46
Appendix 1
Original manuscript “Constant intravenous ghrelin infusion in healthy young men: Clinical
pharmacokinetics and metabolic effects”
Appendix 2
4

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Original manuscript “Acute effects of ghrelin administration on glucose and lipid metabolism”
Appendix 3
Original manuscript “Ghrelin infusion in humans induces acute insulin resistance and lipolysis
independent of GH-signaling”
Appendix 4
Author declarations
5

Esben Thyssen Vestergaard Clinical aspects of ghrelin
List of abbreviations A Coefficient with unit of concentration ACC Acetyl-CoA carboxylase ACTH Adrenocorticotropic hormone AMPK adenosine 5′ monophosphate-activated protein kinase ANOVA Analysis of variance AS160 Akt substrate AUC and AUC∞ Area under concentration-time curve AUMC Area under the first moment curve B Coefficient with unit of concentration BMI Body mass index C Concentration Cl Clearance Cmax Maximal serum or plasma concentration Co Corticotropin Css Steady state concentration dpm Disintegrations per minute e Mathematical constant, base e EE Energy expenditure ELISA Enzyme-Linked ImmunoSorbent Assay EGP Endogenous glucose production ERK Extracellular signal-regulated kinase F Tracer infusion rate f1 Fraction eliminated associated with initial exponential term f2 Fraction eliminated associated with terminal exponential term FFA Free fatty acids GCP Good Clinical practice GH Growth hormone GHD Growth hormone deficiency GHRH Growth hormone releasing hormone GHS Growth hormone secretagogue GHS-R Growth hormone secretagogue receptor GIR Glucose infusion rate GOX Oxidative glucose disposal rate Gn Gonadotropin HDL High-density lipoprotein HPLC High-performance liquid chromatography IGF-I Insulin-like growth factor I IMP Investigational medicinal product IRS Insulin receptor substrate ITT Insulin tolerance test JAK Janus kinase K01 Elimination rate constant λ1 Slope of the initial elimination concentration-time curve λ2 Slope of the initial terminal concentration-time curve MRT Mean residence time M value Glucose metabolized NOGD Non-oxidative glucose disposal NS Non-significant
6

Esben Thyssen Vestergaard Clinical aspects of ghrelin
p Denotes phosphorylation of an enzyme p- Plasma levels of a specific compound PI3K Phosphatidylinositol 3-kinase PKB Protein kinase B Q Pool size QUICKI Quantitative insulin sensitivity check index R0 Rate of infusion Rd Rate of disappearance RIA Radio immuno assay RQ Respiratory quotient s- Serum levels of a specific compound SA Specific activity s.c. Subcutaneous SE Standard error of the mean STAT Signal transducer of activation and transcription T Infusion period Th Thyrotropin t Time t
½ Half-life V Vasopressin VAS Visual analogue scale Vc Volume of distribution, central compartment VD Volume of distributionV (λ2) Volume of distribution, terminal phase Vs. Versus Vss Volume of distribution, at steady state concentrations
7
Esben Thyssen Vestergaard Clinical aspects of ghrelin
Preface Ghrelin is a pleiotropic gut-derived peptide-hormone and more than 2,500 papers on
ghrelin have already been published since the first and famous Nature paper appeared on
December 9 1999. For more than three years I have with much joy and thrill had the chance
to participate in the ever evolving field of ghrelin research. This PhD dissertation is based on
clinical trials performed at Medical Department M and the Medical Research Laboratories at
Aarhus University Hospital, which have offered unique scientific surroundings.
Many skilled and dedicated people contributed to these studies. First of all, I would like to
mention and express my extensive acknowledgments to my principal supervisor Professor
Jens Otto Lunde Jørgensen for inviting and introducing me to metabolic research and for
always keeping focus, being optimistic ye realistic and for scientific guiding as well as for
introducing me to correct scientific writing. I am grateful to Professor Jens Sandahl
Christiansen for providing a stimulating scientific environment with many PhD-students as
colleagues and for providing funding. I wish to thank my supervisors Professor Niels Møller
and Dr. Troels Krarup Hansen for scientific tuition and guidance as well as stimulating scien-
tific discussions. I have enjoyed collaborating with Professor Ole Schmitz and would like to
acknowledge his assistance and continuous interest in my research projects and thank for
the scientific discussions we have had. I am indebted to Preben Jakobsen for pharmacoki-
netic tuition and discussions.
t
rt
I have enjoyed working with and appreciate all the experienced and highly skilled tech-
nicians at the Medical Research Laboratories and I am especially indebted to Susanne Søren-
sen, Elsebeth Hornemann, Merete Møller, Joan Hansen, and Anette Mengel for excellent
technical assistance and for sharing their invaluable experience on clinical research with me.
I would also like to thank Bente Mo ensen and Elin Carstensen for excellent technical assis-
tance.
I have enjoyed working with Dr. Sten Lund, Dr. Jan Frystyk, Dr. Søren Nielsen, Dr. Claus
Gravholt, Dr. Keld Sørensen, Dr. Erik Sloth, Dr. Rolf Dall, and Professor Lars Melholt Rasmus-
sen, and they are all thanked for their continuous help and supervision. I appreciate the col-
laboration with Dr. Kai Lange, Professor Michael Kjær, Dr. Steen Nielsen, and Professor Jens
Juul Holst.
I have had the great joy of working together with a number of enthusiastic present and
former PhD-students who have all contributed to a unique scientific environment by contin-
ued guidance, taking part in fruitful discussions and providing support in all imaginable ways.
8

Esben Thyssen Vestergaard Clinical aspects of ghrelin
I am especially indebted to Dr. Lars Christian Gormsen, Dr. Niels Jessen, Dr. Niels Holmark
Andersen, Dr. Christian Born Djurhuus, Dr. Jakob Gjedsted, Dr. Mads Buhl, Dr. Ande s Boje-
sen, Dr. Signe Gjedde, Dr. Britta Hjerrild, Dr. Charlot e Nielsen, Dr. Tina Parkner and Dr.
Jian-Wen Chen.
r
t
Finally, I avail myself of expressing my sincere gratitude to my family for their extraordi-
nary support and patience.
9

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Background The history of ghrelin is already fascinating. It began and evolved years before the identi-
fication of ghrelin by reverse pharmacology and before the ghrelin receptor was discovered.
Bowers and colleagues demonstrated that met enkephalins were weakly active growth hor-
mone (GH) releasing factors and
they designed more potent ana-
logues in a series of experiments
(1). These molecules are now
denoted GH secretagogues
(GHS). In 1996, Howard and
colleagues characterized and
cloned the GHS receptor (GHS-R
or ghrelin receptor) (2). After
more than a year of systematic
search for an endogenous ligand for the GHS-R, ghrelin was successfully discovered in 1999
by Masayasu Kojima and colleagues (3). Unexpectedly, ghrelin was primarily produced by
gastric cells and the structure turned out to be a unique n-octanoyl acylated peptide (4),
Figure 1.
Figure 1
Administration of ghrelin was shown to potently induce GH secretion (5). Traditionally,
the pulsatile secretion of GH from the pituitary gland is considered to be under both positive
and negative regulation by hypothalamic factors. GH releasing hormone (GHRH) stimulates
GH release, whereas somatostatin exerts an inhibitory influence (6). Circulating ghrelin is
mainly derived from the gut (7;8), and although the ghrelin receptor is abundantly present in
the pituitary gland (9;10), it remains to be convincingly demonstrated that stomach-derived
ghrelin is a physiological regulator of GH secretion. Conditions characterized by high GH lev-
els such as exercise (11), fasting (12), and insulin-induced hypoglycemia (13), are not pre-
ceded by consistent elevations in serum ghrelin levels.
The GHS-R is present not only in the hypothalamus and the pituitary gland but also in
many peripheral organs and tissues (9;10) for which reason pleiotropic effects of the en-
dogenous ligand could be expected. Subsequently, ghrelin research has included a variety of
different research fields such as endocrinology, metabolism, gastroenterology, cardiology,
reproduction, bone growth, and immunology. Additional effects of exogenous ghrelin espe-
cially of interest in relation to this PhD project include stimulation of adrenocorticotropic
10

Esben Thyssen Vestergaard Clinical aspects of ghrelin
hormone (ACTH) and prolactin secretion (5;14). Moreover, there is accumulating evidence to
support that ghrelin plays an important role in the regulation of food intake (15-19), energy
metabolism (20-22), and gastric motility (23;24). Administration of ghrelin stimulates appe-
tite and food intake in rodents as well as in humans (16-19), and circulating ghrelin levels
increase prior to food intake and are suppressed postprandially, which has led to the hy-
pothesis that gastric ghrelin acts as a meal-initiator (15). In addition, ghrelin accelerates
gastric emptying (23;24) and increases gastric acid secretion (25;26). In rodents, admini-
stration of ghrelin induces adiposity (20).
There does not seem to be a simple causal link between ghrelin secretion and conditions
such as simple obesity and anorexia nervosa. By contrast, ghrelin levels are suppressed in
obesity and elevated in anorexia nervosa (27;28), which is more compatible with a compen-
satory response to increased and reduced fat stores, respectively. The endocrine response to
ghrelin (i.e. GH-release) is, however, attenuated in obesity (17). It remains to be studied
whether this decrease in ghrelin levels in obesity is caused by increased ghrelin degradation
or decreased secretion and whether any biochemical or anthropometrical variables predict
ghrelin turnover. These issues point to the study object of the first paper, namely the phar-
macokinetics of ghrelin. Until now, only two articles have reported pharmacokinetic data
(29;30) and both describe first-order elimination in a one-compartment model with a half-life
between 9-31 minutes. Several trials involving ghrelin, ghrelin agonists as well as antagonists
are presently ongoing. Optimal administration calls for knowledge about distribution and
elimination as well as the kinetics of these processes.
In clinical trials, administration of ghrelin increases plasma glucose and free fatty acids
(FFA) (31;32) and reduces glucose disposal rates (33) compatible with an impairment of
insulin sensitivity, but it has been difficult to dissect direct peripheral effects from indirect
GH- and cortisol-mediated effects. Several lines of evidence suggest that ghrelin exerts direct
metabolic effects: (i) in rodent pancreatic islets both ghrelin and GHS-R are present, and
ghrelin inhibits glucose-induced insulin secretion via a paracrine mechanism (34). In a clinical
setting ghrelin also inhibits insulin secretion (22). (ii) a GHS-R antagonist enhanced glucose-
induced insulin secretion from perfused rodent pancreas, whereas exogenous ghrelin sup-
pressed insulin secretion (35). (iii) ghrelin knockout mice display enhanced glucose-induced
insulin release from isolated islets (35;36) and exhibit increased peripheral insulin sensitivity
(36). Ghrelin/GHS-R double knockout mice show lower glucose levels after a glucose toler-
ance test and a more rapid drop in plasma glucose levels after an insulin tolerance test (37).
11

Esben Thyssen Vestergaard Clinical aspects of ghrelin
The objective of the second study was therefore to determine the GH- and cortisol-
independent effects of ghrelin on glucose and lipid metabolism in a clinical setting. Ghrelin
has previously been shown to cause GH-release despite concomitant somatostatin infusion
(38). In order to suppress GH secretion, the somatostatin dose therefore was doubled as
compared to the previous study by De Vito et al. (38) and a constant infusion of ghrelin was
used instead of bolus administration.
The second study revealed that somatostatin does not fully suppress ghrelin-induced GH
and cortisol secretion. Hypopituitary patients replaced with GH and hydrocortisone constitute
an in vivo model for studying putative GH- and ACTH-independent effects of ghrelin. Hypopi-
tuitary patients have participated in one study reporting the effect of ghrelin on metabolites
only (31). In the third study, the objective was to further determine potential direct effects
of ghrelin on whole body and regional substrate metabolism.
Methods Subjects The studies were conducted in accordance to the Helsinki Declaration and all subjects
gave their oral and written informed consent to participate in the respective trials. Study
protocols were approved by the local Ethics Committee of Aarhus County. According to the
International Committee of Medical Journal Editors the protocols were registered in a public
database (www.clinicaltrials.gov). All subjects fasted for at least 9 hrs before study com-
mencement and remained fasting throughout the study day.
Pharmacokinetic study
Seventeen healthy men participated in this study. The quite large number of participants
for a cross-over pharmacokinetic study was chosen to obtain sufficient statistical power (39)
for a cardiovascular study performed in parallel in the same subjects (40). The baseline
characteristics are provided in Table 1.
12

Esben Thyssen Vestergaard Clinical aspects of ghrelin
All participants
had a normal
physical examina-
tion, normal he-
matological indi-
ces, and normal
renal and liver
function tests. All
were non-smokers
and none were abusing alcohol or taking any medication. Subjects were recruited among
university students.
Ta
F
ble 1. Baseline characteristics of the subjects in the pharmacokinetic studyMean ± SE Range(n = 17)
Age (years) 23.1 ± 0.4 21 - 26Height (m) 1.84 ± 0.01 1.70 - 1.96Weight (kg) 77.6 ± 1.5 68.8 - 88.8BMI (kg/m2) 23.0 ± 0.3 20.7 - 25.6Fasting plasma glucose (mmol/l) 4.9 ± 0.1 4.2 - 6.0asting serum ghrelin (µg/l) 0.74 ± 0.06 0.41 - 1.23
Total cholesterol (mmol/l) 3.98 ± 0.16 2.90 - 5.70HDL cholesterol (mmol/l) 1.58 ± 0.09 1.1 - 2.7Plasma albumin (µmol/l) 676.0 ± 5.6 624 - 713
The study protocol was approved by the Danish Medicines Agency and the Good Clinical
Practice (GCP) Unit of Aarhus University Hospital.
Somatostatin study
Eight healthy men aged 27.2 ± 0.9 years with a body mass index (BMI) of 23.4 ± 0.5
kg/m2 volunteered in this study. All had a normal physical examination.
Hypopituitary study
Eight hypopituitary men on stable replacement therapy with GH and hydrocortisone (for
> 3 months) participated. None of the patients had diabetes or any other concomitant
chronic disease. Their baseline characteristics are provided in Table 2.
Table 2. Characterization of the hypopituitary subjectsPatient Age BMI Diagnosis IGF-I Insufficient pituitary axes
yr kg/m2 µg/l1 60 28.8 Pituitary apoplexy 143 GH, Th, Co, Gn2 51 27.5 Prolactinoma 188 GH, Th, Co, Gn3 56 36.0 Cushing disease 193 GH, Th, Co4 60 33.8 Pituitary apoplexy 245 GH, Th, Co, Gn5 62 31.7 Pituitary apoplexy 196 GH, Th, Co, Gn6 46 29.9 Clinically nonfunctioning pituitary adenoma 199 GH, Th, Co, Gn7 31 30.6 Craniopharyngeoma 222 GH, Th, Co, Gn, V8 60 34.4 Cushing disease 270 GH, Th, Co, Gn
BMI, body mass index; IGF-I levels at baseline during GH substitionGH, growth hormone; Th, thyrotropin; Co, corticotropin; Gn, gonadotropin; V, vasopressin
13

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Study design
Pharmacokinetic study
This study was initiated after May 1 2004 and accordingly assigned to EMEAs guidelines
for clinical trials of Investigational Medicinal Products (IMPs). Thus, the IMP (ghrelin) was
required to fulfill both the legislation for Good Manufacturing Practice and Good Distribution
Practice and the clinical trial itself should follow the GCP directive. After completing a com-
prehensive application process we obtained the first national permission from the Danish
Medicines Agency to conduct clinical trials using ghrelin as a trial medication.
Synthetic human acylated ghrelin (NeoMPS, Strasbourg, France) was dissolved in isotonic
saline and sterilized by double passage through a 0.8 and a 0.2 µm pore size filter (Super
Acrodisc, Gelman Sciences, Ann Arbor, MI, USA) by the local University Hospital Pharmacy
Service.
Two volunteers participated in a pilot study, whereafter tolerability, safety, and serum
ghrelin levels were evaluated. The pilot study revealed no safety concerns and subsequently
15 additional subjects were screened, enrolled, randomized, and investigated.
The University Hospital Pharmacy generated a randomization scheme using the Web
hosted generator at http://www.randomization.com. The study design was a randomized,
placebo-controlled double-blind cross-over study.
Two intravenous cannulaes were placed in cubital veins for blood sampling and infusion,
respectively. At t = 0 min, a constant 3-h infusion of ghrelin (5 pmol/kg body weight per
min) or an isovolumetric saline infusion commenced. Blood samples were drawn every 20
min for the 3-h infusion period whereafter blood was drawn at 5-min intervals for a 1-h pe-
riod and subsequently blood was drawn at 10-min intervals for the last two hours.
A muscle biopsy was obtained at t = 90 min from the lateral vastus muscle with a
Bergström biopsy needle under local anesthesia (1% lidocaine). A total amount of ~ 200 mg
muscle was aspirated; biopsies were cleaned for blood within 15 sec and snap-frozen in liq-
uid nitrogen. Muscle biopsies were stored at -80°C until analyzed.
To determine the effects of ghrelin infusion on appetite related scores, a visual analogue
scale (VAS) was used. The subjects reported VAS ratings of (VAS1) hunger, (VAS2) satiety,
(VAS3) desire to eat, and (VAS4) prospective food consumption. Subjects were instructed to
make a single vertical mark on a horizontal line (possible scores 0 to 100 mm) to indicate
their current feelings, Figure 2:
14

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Ghrelins farmakokinetik hos raske kontroller Appetitregulation
Appetitvurdering ved infusionsstart og -slut
Initialer: __ __ __ Projekt id: __ __ __ Dato: __/ __ - __
Sult
Hvor sulten er du?
Slet ikke sulten _______________________________________________ Maximalt sulten
Mæthed
Hvor mæt er du?
Slet ikke mæt _______________________________________________ Helt mæt
Hvor stor er din trang til at spise?
Slet ikke trang til at spise Størst mulig trang til at spise
_______________________________________________
Hvor meget kan du spise?
Ingenting _______________________________________________ Så meget som muligt
Figure 2
Hunger was defined as "the subjective driving force for the search for, choice of, and in-
gestion of food.” Satiety was defined as "the sensation after eating so that a person does not
feel the need to eat for some time afterwards.” The desire to eat was defined as "the per-
son's subjective feeling of the need to consume a meal.” The prospec ive food consumption
was defined "the quantity of food the subject imagined himself able to eat at the given
time.” Baseline evaluations were collected prior to the infusion period (t = 0) and at termina-
tion of the infusion period (t = 180 min). A blinded observer measured the scores.
t
Somatostatin study
All participants were examined on two occasions separated by a minimum of five weeks.
The subjects were studied at 07.00 am in a quiet, thermo neutral in-door environment.
One intra-venous cannula was inserted in the antecubital region for infusion, and one in-
tra-venous cannula was inserted in a dorsal hand vein for blood sampling. The latter was
placed in a heated box at 65°C allowing for arterialized blood samples to be drawn. Plasma
glucose levels were determined every 10 min and blood samples were drawn every 30 min
and analyzed for ghrelin, GH, cortisol, glucagon, insulin, C-peptide, and FFA.
The study design is illustrated in Figure 3. In a randomized, single-blind, placebo-
controlled cross-over design a constant infusion of human acylated ghrelin lasting 300 min-
utes at 5 pmol/kg body weight per min or saline (as placebo) was used. The period from t =
15

Esben Thyssen Vestergaard Clinical aspects of ghrelin
0 to t = 180 min is referred to as the basal period and the period from t = 180 to t = 300
min as the clamp period.
At t = 0 min infusion of somatostatin (Ferring Pharmaceuticals, Copenhagen, Denmark)
330 µg/h, insulin (Actrapid, Novo Nordisk, Bagsværd, Denmark) 0.1 mU/kg/min, GH
(Norditropin, Novo Nordisk)
2 ng/kg/min was com-
menced. Infusion of gluca-
gon (Glucagen, Novo Nord-
isk) 0.5 ng/kg/min was
added at t = 30 min. Eu-
glycemia was intended and
if necessary isotonic glu-
cose was infused to main-
tain a plasma glucose level
of ~ 5.0 mmol/l in order to
prevent somatostatin-
induced hypoglycemia.
From t = 180 min and on-
wards a hyperinsulinemic
euglycemic clamp (insulin
0.6 mU/kg/min) was per-
formed. Plasma glucose was clamped at 5.0 mmol/l by adjusting the rate of infusion of 20%
glucose according to plasma glucose measurements every 10 min. Insulin sensitivity was
estimated by the level of glucose infusion rate (GIR) during the hyperinsulinemic euglycemic
clamp.
Figure 3
Hypopituitary study
All patients were studied on two occasions (ghrelin 5 pmol/kg body weight per min and
saline for 300 min) in a randomized, double-blind, placebo-controlled cross-over design. In-
tra-venous cannulaes were inserted as in the Somatostatin study.
16

Esben Thyssen Vestergaard Clinical aspects of ghrelin
The study design is il-
lustrated in Figure 4. At t
= 0 saline or a primed-
continuous ghrelin infu-
sion was commenced.
The bolus dose was esti-
mated from the elimina-
tion rate constant of
ghrelin k01 calculated in
the pharmacokinetic
study and infused over a
20-min interval to avoid
an overshoot of steady
state levels. Subse-
quently, ghrelin was infused at a rate of 5 pmol/kg body weight per min.
Figure 4
Muscle and fat biopsies were obtained at t = 120 min. A hyperinsulinemic euglycemic
clamp was performed from t = 120 to 300 min. Blood samples were obtained as indicated in
Figure 4. Indirect calorimetry was performed for the terminal 30 min of both the basal and
the clamp period.
Pharmacokinetic modeling
A review of PubMed indexed journals1 showed that ghrelin has been administered more
than 500 times in patients and healthy volunteers. Ghrelin has mostly been administered as
intravenous bolus injections, but also intravenous infusions as well as subcutaneous (s.c.)
administrations have been tested. Surprisingly, the pharmacokinetics of ghrelin is reported
by two papers only (29;30). Both reported first-order elimination in a one-compartment
model with a half-life between 9-31 minutes but the pharmacokinetic approach was not de-
scribed in detail. We decided to extend the current pharmacokinetic knowledge and used a
constant intravenous ghrelin infusion to investigate (i) if steady state levels were obtained
after ~ 6 times the reported half-life i.e. ~ 180 min as expected, (ii) if systemic ghrelin levels
could be predicted based on experimentally derived pharmacokinetic variables and (iii) the
1Review of papers retrieved by search term “ghrelin” on the Web-hosted database
http://www.ncbi.nlm.nih.gov/sites/entrez?db=pubmed by end of September 2007. The sum of ghrelin administrations does not take non-identifiable double publications into account.
17

Esben Thyssen Vestergaard Clinical aspects of ghrelin
mean residence time (MRT) of ghrelin in the human body. MRT is a summary pharmacoki-
netic term, which refers to the average time (in min) a molecule spends in the human body.
The postinfusion concentration-time curve was analyzed from each of the 17 subjects us-
ing a nonlinear least-squares regression analysis based on both a mono- and a biexponential
decay model. By visual inspection of the concentration-time curve on a linear and a log-
transformed scale the more complicated biexponential model:
tt eBeAC ⋅−⋅− ⋅+⋅= 21 '' λλ
provided the best fit and, subsequently by statistical testing, had significantly lower sum-of-
squares, 0.92 vs. 0.04. The statistical extra sum-of-squares F-test was applied to compare
the two nes ed models and favored the 2-phase model, P < 0.0001. λt 1 and λ2 denote the
initial and terminal slopes. Pharmacokinetic analyzes were performed by using the computer
software GraphPad Prism v4.00 for Windows (GraphPad Software, San Diego, USA). To cor-
rect the serum ghrelin levels for endogenous ghrelin secretion, serum ghrelin levels on the
placebo day were subtracted from the levels measured during active treatment. Because
pharmacokinetic parameters were estimated based on a post-infusion curve, intercepts
should be corrected according to Loo and Riegelman (41):
,1
',
1
'21
21TT e
TBB
eTA
A⋅−⋅− −
⋅⋅=
−
⋅⋅=
λλ
λλ
where T is the infusion period.
The distribution half-life t½(λ1) and the elimination (terminal) half-life t½(λ2) were calculated
as
11½
)2ln()(
λλ =t and
22½
)2ln()(
λλ =t ,
respectively. The area under the serum concentration-time curve AUC∞ was calculated as
21 λλBAAUC +=∞ .
The so-called area under the first moment curve AUMC – a prerequisite to estimate MRT –
was calculated as
22
21 λλ
BAAUMC += .
Total clearance Cl was calculated as follows:
18

Esben Thyssen Vestergaard Clinical aspects of ghrelin
∞
=AUCDoseCl ,
MRT was calculated as
∞
=AUCAUMCMRT .
Simulation of the serum concentration during the infusion was done according to the follow-
ing equation (42)
CleRf
CleRf
Ctt )1()1( 21
0201⋅−⋅− −⋅⋅
+−⋅⋅
=λλ
,
where R0 is the rate of infusion and f1 and f2 denominate the fraction of elimination associ-
ated with the first and last exponential term, respectively:
∞
=AUC
Af 1
1λ
and∞
=AUC
Bf 2
2λ
.
Serum concentration at steady state CSS was calculated as
ClR
C ss0= .
An elaborate list of pharmacokinetics including the volume of distribution of the central com-
partment Vc, the volume of distribution during the terminal phase V (λ2) and the volume of
distribution at steady state Vss is reported in the first paper.
Tracers
A primed-continuous infusion of [3-3H]-glucose was used (Somatostatin study: 17 µCi bo-
lus followed by 0.17 µCi/min; Hypopituitary study: 12 µCi bolus followed by 0.17 µCi/min,
NEN Life Science Products, Boston, MA, USA). Glucose flux rates were calculated at 10-min
intervals during the last 30-min intervals of the basal and clamp periods, respectively, using
Steele’s nonsteady-state equations (43) and, based on empirical observations, a pool fraction
of 0.65 and a volume of distribution of 200 ml/kg body weight are used (43;44):
.SA
dtdSACVQF
RglcD
a
×××−=
19

Esben Thyssen Vestergaard Clinical aspects of ghrelin
During the clamp period, endogenous glucose production (EGP) was calculated by sub-
tracting the rate of exogenous glucose infusion from the rate of appearance of [3-3H]-
glucose:
.GIRREGP a −=
In the Hypopituitary study, oxidative glucose disposal rate (GOX) was calculated from
energy expenditure (EE) and respiratory quotient (RQ) after correction for protein oxidation
rates, which was estimated from the urinary excretion of urea
.29.0
71.0 EEnonproteinRQnonproteinGOX ×−
=
Nonoxidative glucose disposal (NOGD) was calculated as whole body glucose disposal Rd
minus the rate of GOX adjusted for body weight and calculated per minute (45)
,GOXRNOGD d −= where
.dt
dCVQRR glc
Dad ××−=
[9,10-3H]-palmitate (Danish Medicines Agency, Copenhagen, Denmark and Department
of Nuclear Medicine, Aarhus University Hospital, Denmark) was infused continuously at 0.3
µCi/min. Blood samples were drawn for analysis of palmitate concentration and specific ac-
tivity (SA). Steady state of SA was verified (last 30-min interval of a palmitate-infusion pe-
riod). Plasma palmitate concentration and SA were determined by HPLC using [2H31]-
palmitate as internal standard. Systemic palmitate flux (Ra, µmol/min) was calculated using
the [9,10-3H]-palmitate infusion rate (dpm/min) divided by the steady state palmitate SA
(dpm/µmol)
.SAFRa =
Indirect calorimetry
RQ and EE were assessed by indirect calorimetry (45) (Deltatrac; Datex Instruments, Hel-
sinki, Finland), which was performed for the terminal 30 min of the basal and clamp periods
in the Somatostatin and the Hypopituitary studies as indicated in Figures 3 and 4. An addi-
tional calorimetry period was included at baseline in the Somatostatin study before infusion
of saline and ghrelin. In the Hypopituitary study, lipid oxidation was calculated from EE and
RQ after correction for protein oxidation rates,
20

Esben Thyssen Vestergaard Clinical aspects of ghrelin
.29.0
1 RQnonproteinEEnonproteintionLipidoxida −×=
Microdialysis
Muscle microdialysis catheters (CMA-60, CMA, Stockholm, Sweden) were inserted after
applying local analgesic of 1 ml 1% lidocaine superficial to the fascia. Correct placement of
the microdialysis catheters was confirmed by the presence of muscle twitches during inser-
tion. In the Somatostatin study, two catheters were used in order to ensure viability of at
least one (gastrocnemius and the lateral vastus muscle approximately 10 cm below and 14
cm above the patella, respectively). In the Hypopituitary study, only one muscle microdialy-
sis catheter was used because no membranes were disrupted in the earlier study. Subse-
quently, two additional microdialysis catheters were positioned in the s.c. adipose tissue ap-
proximately 5 cm lateral of the umbilicus and in the femoral s.c. adipose tissue after 0.25 ml
of lidocaine s.c. pre-administration.
The microdialysis catheters have a molecular cut-off of 20 kDa and a membrane length
of 30 mm. Prior to insertion the catheters were manually flushed with perfusion fluid (Ringer
Chloride, T1, CMA, Na+ 147 mmol/l; K+ 1.4 mmol/l; Ca2+ 2.3 mmol/l; Cl- 156 mmol/l, pH 6;
osmolality 290 mosmol/kg) to allow for clearance of air bubbles from the microdialysis mem-
branes. The microdialysis systems were perfused at a flow rate of 1 µl/min using CMA-107
perfusion pumps (CMA).
The relative recovery of interstitial glycerol was assessed by the internal reference
method using 3H-glycerol (46). 3H-glycerol was added to the perfusate in order to obtain
approximately 1000 cpm/µl. Perfusate and dialysate were counted using a Wallac 1450 liquid
scintillation counter applying the Optiphase supermix scintillation fluid (Wallac, Turku,
Finland) for muscle and Ultima Gold scintillation fluid (Packard Biosciences, Meriden, CT,
USA) for adipose tissue. Changes in interstitial glycerol concentration correspond to regional
lipolysis (47).
60 min of equilibration was allowed in order to minimize the influence of local edema and
hemorrhage. The sampling was performed every 30 min and continued until t = 300 min.
Western blotting and PI3K assay
Muscle biopsies were homogenized as previously described (48). Aliquots of protein were
resolved by SDS-PAGE, and proteins were electro-blotted onto nitrocellulose membranes.
Immunoblotting was performed using primary antibodies as follows: pSTAT5a and -b,
21

Esben Thyssen Vestergaard Clinical aspects of ghrelin
STAT5, pSTAT3, STAT3, pERK1 and -2, ERK1 and -2, pAMPKα, AMPKα-pan, pACC, pAkt, Akt,
PAS, and AS160. Membranes were incubated with HRP-coupled secondary antibodies, visu-
alized by BioWest enhanced chemiluminescence (UVP LabWorks, Upland, CA, USA) and
quantified by UVP BioImaging System. Densitometric measurements were adjusted to an
internal control.
PI3K activity was assessed as previously described (48).
Analyses
Biochemical methods were similar in all three studies unless indicated and specified. Se-
rum total ghrelin levels were measured in duplicate by an in-house assay as described previ-
ously (12). The assay measures immunoreactive levels of ghrelin using 125I-labelled bioactive
ghrelin tracer and rabbit polyclonal antibodies raised against octanoylated human ghrelin.
The assay recognizes the COOH-terminal of ghrelin and as such determines acylated as well
as des-acylated ghrelin. The intraassay coefficient of variation is usually low in this assay
(2.8% in a random sample). Samples from each individual were analyzed in the same assay
run. A double commercial monoclonal immunofluorometric assay (DELFIA, Perkin Elmer, Wal-
lac, Turku, Finland) was used to measure serum levels of GH, cortisol and insulin. Plasma
glucose levels were measured in duplicate on a glucose analyzer (Beckman Instruments,
Palo Alto, CA, USA). Serum FFA was determined using a commercial kit (Wako Chemicals,
Neuss, Germany). Plasma ACTH was determined using a commercial method (Immulite Di-
agnostic Product Corporation Scandinavia). Plasma albumin, total cholesterol and high-
density lipoprotein (HDL) cholesterol levels were determined by commercial methods (Cobas
Integra 800) using an immunoturbidimetric measurement, an enzymatic colorimetric and a
homogeneous enzymatic colorimetric method, respectively. In the Somatostatin study, corti-
sol was measured with a solid-phase, time-resolved fluoroimmunoassay (Delfia), insulin and
C-peptide were measured with an immunoassay (DAKO, Denmark), and plasma glucagon
was measured by an in-house radioimmuno assay modified from (49).
Glucose, glycerol, lactate, and urea in the microdialysis dialysate were measured in dupli-
cate by an automated spectrophotometric kinetic enzymatic analyzer (CMA 600; CMA).
22

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Statistics
Results are expressed as mean ± SE.
Systemic levels of ghrelin, GH, ACTH, prolactin, cortisol, glucagon, insulin, C-peptide,
epinephrine, norepinephrine, glucose (and skeletal muscle interstitial glucose), FFA, GIR, and
the time series of revised QUICKI estimates were analyzed by two-way analysis of variance
(ANOVA). The interaction between time and treatment ("time x treatment") was considered
the term of interest. The Bonferroni correction was used to account for multiple comparisons
when appropriate.
Comparisons of baseline values were carried out by Student’s two-tailed paired t test.
Glucose kinetics, M value, palmitate fluxes, RQ, EE, lipid oxidation, time averaged intersti-
tial concentrations, changes in VAS, densitometric quantitative measures of Western blots,
and PI3K activity were examined by Student’s two-tailed paired t test when appropriate.
In the Pharmacokinetic study, backward regressions analyses were performed including
BMI, total and HDL cholesterol levels as independent variables, and the following variables
for ghrelin: MRT, AUC, half-lives, k01, or Cl were included as dependent variables.
In the Somatostatin study, effects of GH, cortisol, glucagon, insulin levels, and GIR (in-
cluded as independent variables) on lipolysis (palmitate flux and FFA increase) (included as
dependent variables) were analyzed by comparing the changes in rates (GIR and palmitate
flux) and areas under concentration-time curves (∆AUC, GH, cortisol, glucagon, insulin, and
NEFA) by backward regression analyses.
A P value less than 0.05 was considered significant. Statistical analysis was performed us-
ing SPSS versions 13.0 and 14.0 for Windows.
23

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Summary of results Pharmacokinetic study
Ghrelin pharmacokinetics
Mean levels of circulating ghrelin (total ghrelin) vs. time are shown in Figure 5. Serum
ghrelin increased to 4.41 ± 0.29 µg/l above placebo levels after 180 min infusion. This level
was comparable to predicted Cmax (4.35 ± 0.28 µg/l, P = 0.45), whereas it was significantly
smaller than predicted CSS (5.00 ± 0.35 µg/l, P = 0.03).
CSS
Cmax
3.32e-0.033t
1.35e-0.007t
Figure 5. Levels of total serum ghrelin above baseline vs. time and key pharmacokinetic
parameters.
The initial and terminal ghrelin half-lives, t½(λ1) and t½(λ2) were 24.2 ± 2.5 and 146.0 ±
35.6 min, respectively and MRT was 92.7 ± 16.3 min.
Correlations
MRT was included as a dependent parameter in a backward stepwise multiple regression
analysis. Both BMI (r = 0.51, P < 0.001) and HDL cholesterol (r = 0.75, P < 0.001) were
positively associated with MRT.
Hormones and metabolites
The hormonal and metabolite responses to ghrelin and saline infusions are shown in Fig-
ure 6. Ghrelin caused an increase in systemic levels of GH, prolactin, ACTH, cortisol, FFA,
and glucose, whereas insulin remained constant until termination of the infusion period. Ele-
vations in levels of both FFA and glucose concomitantly with constant and elevated insulin
levels suggested a significant decrease in insulin sensitivity. Insulin sensitivity was not meas-
24

Esben Thyssen Vestergaard Clinical aspects of ghrelin
ured directly, as a hyperinsulinemic euglycemic clamp would have hampered or interfered
with the measurements of
appetite and cardiovascular
indexes. However, to obtain
a measure for insulin sensi-
tivity revised QUICKI (50)
for the time series was used
although this model is vali-
dated on fasting subjects
only. Revised QUICKI indi-
cated that insulin sensitivity
decreased after 40 min of
ghrelin infusion and did not
reach pre-infusion levels
throughout the study day.
Appetite
scores were
sim
0
All VAS
ilar at baseline on both
study days (placebo vs.
ghrelin, in cm: VAS1: 4.2 ±
.5 vs. 3.9 ± 0.5, P = 0.52;
VAS2: 3.6 ± 0.5 vs. 4.1 ±
0.5, P = 0.32; VAS3: 4.2 ±
0.5 vs. 4.7 ± 0.5, P = 0.43; and VAS4: 5.6 ± 0.4 vs. 5.3 ± 0.5, P = 0.40, respectively) and
after 180 min of infusion (placebo vs. ghrelin, in cm: VAS1: 5.9 ± 0.5 vs. 5.4 ± 0.6, P =
0.45; VAS2: 2.9 ± 0.4 vs. 2.5 ± 0.4, P = 0.38; VAS3: 6.3 ± 0.3 vs. 6.2 ± 0.4, P = 0.83; and
VAS4: 6.4 ± 0.4 vs. 6.8 ± 0.3, P = 0.28, respectively). Comparing the changes in VAS scores
during the 3-h infusion period revealed that ghrelin affected the delta score of “satiety” only,
P = 0.03. However, it was obvious that some of the subjects experienced a transient in-
crease of hunger after 40 - 90 min of ghrelin infusion, but these observations were not for-
mally recorded.
Time (minutes)
0 100 200 300
Rev
ised
QU
ICK
I
0.0
0.2
0.4
0.6
*
G
**
* ** * *
Seru
m in
sulin
(pm
ol/l)
0
10
20
30
40
50
*
E
* *
*
*
Pla
sma
gluc
ose
(mm
ol/l)
0.0
4.8
5.0
5.2
5.4
5.6
**C
Ser
um F
FA (m
mol
/l)0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6GhrelinPlacebo
A
*
* *
*
* *
Time (minutes)
0 100 200 300
Ser
um c
ortis
ol (n
mol
/l)
0
100
200
300
400
500
*
H
*
* *
*
Seru
m A
CTH
(ng/
ml)
0
5
10
15
20
25
30 *F
Ser
um p
rola
ctin
(µg/
l)
0
2
4
6
8
10
12
14
*
D
** *
Seru
m G
H (n
g/m
l)
0
10
20
30
40
50
*
B
*
*
*
** * * *
Infusion period Infusion period
Figure 6
25

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Somatostatin study
Hormones and metabolites
Serum ghrelin levels were similar at baseline on both study days, P = 0.30. Infusion of
ghrelin resulted in a 4.5–fold increase in circulating ghrelin levels during both the basal and
the clamp period. In the saline study serum ghrelin levels decreased moderately and gradu-
ally with time, ANOVA P =
0.001. The hormonal and
metabolite responses are
shown in Figure 7.
Serum GH increased
moderately in response to
ghrelin infusion, ANOVA P
< 0.001, and reached a
maximum of 4.6 ± 1.3
ng/ml (i.e. somatostatin
infusion blunted the GH
response by a factor 10 as
compared with the phar-
macokinetic study) after
60 min of infusion where-
after a gradual decline
towards placebo levels
was observed. Serum cor-
tisol increased approxi-
mately 1.9–fold after 90
min of ghrelin exposure as
compared to placebo fol-
lowed by a decline to-
wards placebo levels after
270 minutes.
Indirect calorimetry
The rates of EE and RQ were
1552 ± 39 kcal/24-h, P = 0.30
Figure 7
Time (minutes)
-100 0 100 200 300
Plas
ma
gluc
agon
(pg/
ml)
0
20
40
60
80
100
120
Ser
um g
hrel
in (µ
g/l)
0
1
2
3
4
5
6
7
GhrelinSaline
P < 0.001
Ser
um g
row
th h
orm
one
(ng/
ml)
0
2
4
6
8
10
*
***
*
P < 0.001
Seru
m c
ortis
ol (n
mol
/l)
0
200
400
600
800
*
P < 0.001
****
**
P < 0.01
Ser
um in
sulin
(pm
ol/l)
0
50
100
150
200
250
300
P = 0.41
P = 0.61
Seru
m C
-pep
tide
(pm
ol/l)
0
200
400
600P = 0.93
Plas
ma
gluc
ose
(mm
ol/l)
0
4
6
8
P = 0.63 P = 0.28
Time (minutes)
-100 0 100 200 300
Ser
um F
FA (µ
mol
/l)
0
200
400
600
800
1000
P = 0.10 P < 0.001
**
Basal Clamp
A
B
C
D
E
F
G
H
*
*
Pancreatic clampBasal ClampPancreatic clamp
comparable in the basal period [EE: 1521 ± 43 (ghrelin) vs.
and RQ: 0.89 ± 0.01 (ghrelin) vs. 0.88 ± 0.01, P = 0.53, re-
26

Esben Thyssen Vestergaard Clinical aspects of ghrelin
spectively], whereas insulin-stimulated EE was significantly lower during ghrelin infusion as
compared with placebo [EE: 1539 ± 28 (ghrelin) vs. 1608 ± 32 kcal/24-h, P = 0.048]. RQ
was similar during the clamp period [0.92 ± 0.03 (ghrelin) vs. 0.93 ± 0.01, P = 0.65].
Glucose and palmitate metabolism
Glucose metabolism is depicted in Figure 8. The rate of isotopically determined total glu-
cose turnover (Rd) during the basal [1.9 ± 0.1 (ghrelin) vs. 2.3 ± 0.1 mg/kg/min, P = 0.03]
as well as the clamp period [3.9 ± 0.6 (ghrelin) vs. 6.1 ± 0.5 mg/kg/min, P = 0.02] was sig-
nificantly lower during ghrelin administration as compared with placebo infusion. By contrast,
endogenous glucose production was similar during ghrelin and placebo administration in the
basal period and was suppressed to a similar degree during the hyperinsulinemic clamp (P
NS). Significantly lower GIR during the ghrelin study resulted in similar plasma glucose lev-
els.
Rate of glucose disappearance
Saline Ghrelin Saline Ghrelin
Rd
(mg/
kg/m
in)
0
1
2
3
4
5
6
7
8
Glucose infusion rate
Time (minutes)-100 0 100 200 300
GIR
(mg/
kg/m
in)
0
2
4
6
8
GhrelinSaline
P < 0.001
* **
*
*
**** *
**
A
C
M-value
Saline Ghrelin
M-v
alue
(mg/
kg/m
in)
0
2
4
6
8
10
P = 0.007
Basal Clamp
P = 0.02
P = 0.03
Endogenous glucose production
Saline Ghrelin Saline Ghrelin
EGP
(mg/
kg/m
in)
0
1
2
3
4
P = 0.48
P = 0.44
Basal Clamp
Figure 8
27
Esben Thyssen Vestergaard Clinical aspects of ghrelin
Insulin sensitivity, as assessed by GIR, was reduced during ghrelin infusion as compared
with placebo infusion [4.0 ± 0.7 (ghrelin) vs. 6.9 ± 0.9 mg/kg/min, P = 0.007].
Basal systemic palmitate flux was significantly increased during ghrelin administration
(131 ± 26 (ghrelin) vs. 69 ± 5 µmol/min, P = 0.048).
Correlations
Backward regressions analyses excluded ∆AUC of glucagon, insulin, and GIR and re-
vealed that ∆AUC of GH, P = 0.005, and cortisol, P = 0.002 were both significant predictors
of ∆AUC of FFA. However, similar analyses where ∆AUC of FFA was replaced by palmitate
flux (as a marker for lipolysis) as the dependent variable excluded all independent variables
of the model as predictors of lipolysis.
Interstitial glycerol concentrations
In general, the hyperinsulinemic clamp suppressed interstitial glycerol levels in muscle
and adipose tissue during both ghrelin and placebo treatment. Glycerol levels were elevated
in femoral s.c. fat during ghrelin and clamp conditions, P = 0.01, and overall, the regional
glycerol release was elevated during ghrelin infusion, although it failed to reach statistical
significance. Interstitial glycerol levels decreased, as expected, during the hyperinsulinemic
clamp period, but the suppression of interstitial glycerol levels was attenuated on the ghrelin
day as compared to the saline day. In abdominal s.c. fat tissue hyperinsulinemia caused a
reduction of 56.3 ± 10.5 µmol/l during ghrelin infusion as compared to a reduction of 131.6
± 19.4 µmol/l during saline infusion, P = 0.002.
28
Esben Thyssen Vestergaard Clinical aspects of ghrelin
Hypopituitary study
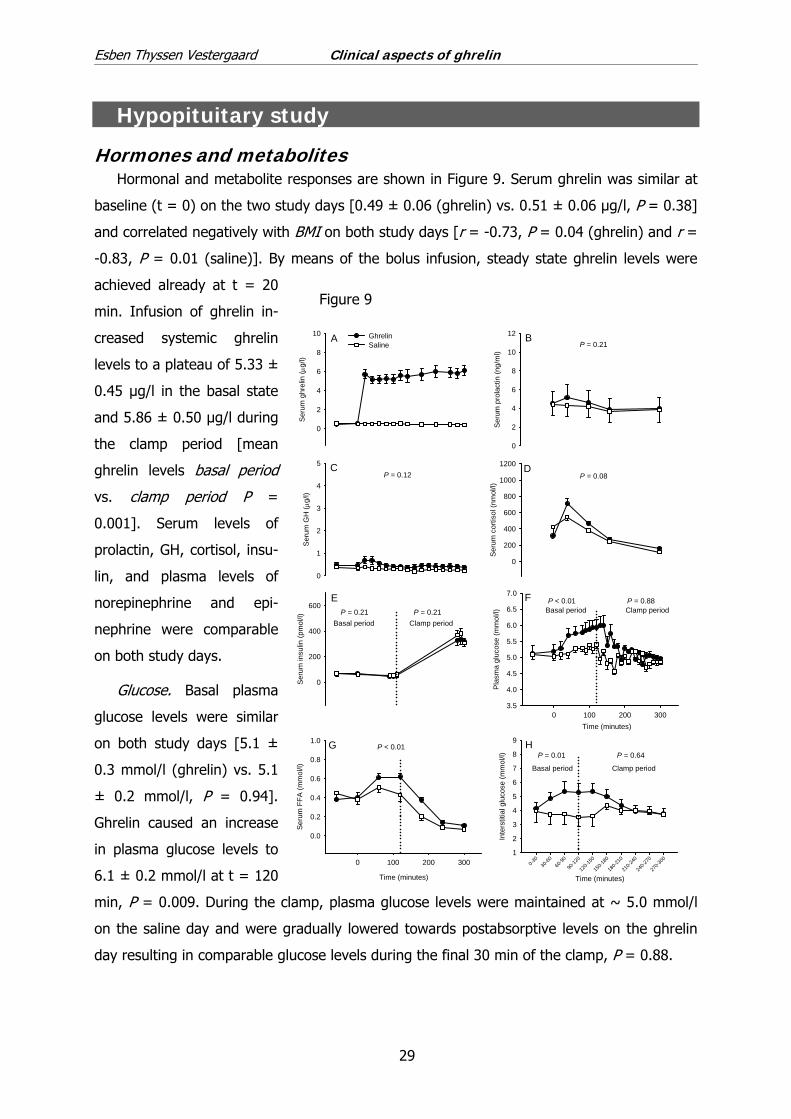
Hormones and metabolites Hormonal and metabolite responses are shown in Figure 9. Serum ghrelin was similar at
baseline (t = 0) on the two study days [0.49 ± 0.06 (ghrelin) vs. 0.51 ± 0.06 µg/l, P = 0.38]
and correlated negatively with BMI on both study days [r = -0.73, P = 0.04 (ghrelin) and r =
-0.83, P = 0.01 (saline)]. By means of the bolus infusion, steady state ghrelin levels were
achieved already at t = 20
min. Infusion of ghrelin in-
creased systemic ghrelin
levels to a plateau of 5.33 ±
0.45 µg/l in the basal state
and 5.86 ± 0.50 µg/l during
the clamp period [mean
ghrelin levels basal period
s. clamp period P =
0.001]. Serum levels of
prolactin, GH, cortisol, insu-
lin, and plasma levels of
norepinephrine and epi-
nephrine were comparable
on both study days.
v
Glucose. Basal plasma
glucose levels were similar
on both study days [5.1 ±
0.3 mmol/l (ghrelin) vs. 5.1
± 0.2 mmol/l, P = 0.94].
Ghrelin caused an increase
in plasma glucose levels to
6.1 ± 0.2 mmol/l at t = 120
min, P = 0.009. During the clamp, plasma glucose levels were maintained at ~ 5.0 mmol/l
on the saline day and were gradually lowered towards postabsorptive levels on the ghrelin
day resulting in comparable glucose levels during the final 30 min of the clamp, P = 0.88.
Ser
um g
hrel
in ( µ
g/l)
0
2
4
6
8
10
Ser
um G
H ( µ
g/l)
0
1
2
3
4
5
GhrelinSaline
CP = 0.12
Ser
um p
rola
ctin
(ng/
ml)
0
2
4
6
8
10
12P = 0.21
B
Ser
um c
ortis
ol (n
mol
/l)
0
200
400
600
800
1000
1200 DP = 0.08
A
Time (minutes)0 100 200 300
Pla
sma
gluc
ose
(mm
ol/l)
3.5
4.0
4.5
5.0
5.5
6.0
6.5
7.0
Basal period Clamp periodP < 0.01 P = 0.88
Time (minutes)
0-30
30-60
60-90
90-12
0
120-1
50
150-1
80
180-2
10
210-2
40
240-2
70
270-3
00
Inte
rstit
ial g
luco
se (m
mol
/l)
1
2
3
4
5
6
7
8
9
Basal period Clamp period
P = 0.01 P = 0.64
F
H
Time (minutes)
0 100 200 300
Seru
m F
FA (m
mol
/l)
0.0
0.2
0.4
0.6
0.8
1.0 G P < 0.01
Ser
um in
sulin
(pm
ol/l)
0
200
400
600
Basal period Clamp periodP = 0.21 P = 0.21
E
Figure 9
29

Esben Thyssen Vestergaard Clinical aspects of ghrelin
FFA. The basal levels were comparable [0.38 ± 0.05 (ghrelin) vs. 0.45 ± 0.08 mmol/l, P
= 0.47]. Ghrelin infusion induced an 80% increase in FFA to 0.62 ± 0.03 mmol/l at t = 120
min, P < 0.05, followed by a decline and a return to placebo levels during the clamp period.
Resting energy expenditure
Resting energy expenditure (EE) was not significantly affected by ghrelin neither in the
basal nor in the clamp period.
Glucose metabolism and substrate oxidation
Glucose metabolism is
shown in Figure 10. GIR
was significantly decreased
during ghrelin administra-
tion (P < 0.01, Figure 10A)
and the M value was re-
duced by ~ 60% (P =
0.0001, Figure 10A insert).
Ghrelin reduced the
rates of oxidative, non-
oxidative and total glucose
disposal during the clamp
period (P = 0.009, P =
0.033, and P = 0.012, re-
spectively; Figure 10B),
whereas ghrelin did not
significantly have an impact
on glucose metabolism in
the basal state.
Lipid metabolism
Ghrelin did not signifi-
cantly affect RQ in the basal
state, but showed a trend
towards increased lipid oxidation during the clamp period. Overall, ghrelin caused metabolic
inflexibility, in the sense that RQ increased 0.07 ± 0.01 in the saline study (RQclamp – RQbasal)
Time (minutes)
50 100 150 200 250 300
Glu
cose
infu
sion
rate
(mg
x kg
-1 x
min
-1)
0
1
2
3
4
5
GhrelinSaline
P < 0.01
Saline Ghrelin
Glu
cose
infu
sion
rate
(mg
x kg
-1 x
min
-1)
0
1
2
3
4
5P < 0.001
Basal period Clamp periodSaline Ghrelin Saline Ghrelin
Glu
cose
Rd
(mg
x kg
-1 x
min
-1)
0
1
2
3
4
5
6
NOGD
GOX
*
*
P = 0.012
GOX clamp P = 0.009NOGD clamp P = 0.033
A
B
Figure 10
30
Esben Thyssen Vestergaard Clinical aspects of ghrelin
as compared to 0.03 ± 0.01 in the ghrelin study (P = 0.03). Infusion of ghrelin had no sig-
nificant effects on neither basal nor insulin-stimulated rates of lipid oxidation (P = 0.37 and P
= 0.19) although ghrelin caused a trend towards metabolic inflexibility (percentage decrease
in lipid oxidation rates: saline 55 ± 5% vs. ghrelin 22 ± 17%, P = 0.11) implicating that
ghrelin caused a tendency to increase rate of lipidoxidation.
Regional substrate metabolism (microdialysis)
Interstitial skeletal muscle glucose levels mirrored the fluctuations in the plasma levels of
glucose during ghrelin infusion (Figure 9H). By contrast, interstitial levels of glucose in ab-
dominal and femoral fat remained at placebo levels. Ghrelin did not significantly influence
the levels of interstitial glycerol, lactate, or urea in neither skeletal muscle nor s.c. tissues.
GH and insulin signaling
AMP-activated protein kinase (AMPK) and acetyl-CoA carboxylase (ACC) phosphorylation
were similar during saline and ghrelin administration, P = 0.57 and P = 0.87, respectively.
Moreover, ghrelin did not evoke Janus kinase/signal transducer of activation and transcrip-
tion (JAK/STAT) signaling as assessed by STAT5, P = 0.20, or STAT3 phosphorylation, P =
0.51, MAPK-stimulation as assessed by extracellular signal-regulated kinase (ERK) 1, P =
0.15, and ERK2 activation, P = 0.94, or suppression of insulin signaling pathways as as-
sessed by protein kinase B (PKB/Akt), P = 0.58, and Akt substrate (AS160) phosphorylation,
P = 0.43. IRS-associated phosphatidylinositol 3-kinase (PI3K) activity was not modified by
ghrelin infusion either [IRS-1 (arbitrary units): 84.7 ± 11.4 (ghrelin) vs. 115.3 ± 19.3, P =
0.36; IRS-2 (arbitrary units): 77.6 ± 22.1 (ghrelin) vs. 122.4 ± 29.6, P = 0.29].
Discussion Methodological considerations
Pharmacokinetic study
Serum ghrelin was measured by our in-house ghrelin assay in all three studies. Methods
for measurement of ghrelin are much debated and no gold standard exists. Several commer-
cially available assays based on RIA and ELISA techniques recognize different epitopes of the
ghrelin amino acid sequence with or without the acyl side chain, which implies that results
obtained by different assays are not comparable. For example, Hotta et al. applied several
different ghrelin assays on the same plasma samples and depending on the assay, acylated
31

Esben Thyssen Vestergaard Clinical aspects of ghrelin
ghrelin levels were either reported to be increased, similar and decreased in women with
anorexia nervosa as compared with age-matched healthy controls (51). This fundamental
problem is even more complicated because the two most popular kits (from Phoenix Phar-
maceuticals and Linco Research) yield a 10-fold difference in measured ghrelin levels (52)!
This variation may be reduced by time-consuming RIA-HPLC methods or a new liquid chro-
matography tandem mass spectrometry technique (53). The latter method has also revealed
that ghrelin degrades rapidly in serum (53), but only recently systematic in vitro studies has
resulted in detailed sample preparation protocols that describe optimal acidification and es-
terase-inhibition procedures.2
When the pharmacokinetic study was designed, the pharmacokinetics (half-life) of ghrelin
was reported by one other study only (30). We aimed to estimate the pharmacokinetics in
detail and to investigate if the previously reported half-life could predict time to steady state.
Therefore a constant intravenous ghrelin infusion was applied.
To investigate if 180-min of ghrelin infusion induced hunger in the post-absorptive pe-
riod, similar visual analogue scales as previously used during ghrelin infusion and ad libitum
meals (19) and in patients with anorexia nervosa (54) were applied.
Muscle biopsies were included to study ghrelins direct putative effects of on JAK/STAT,
insulin, ghrelin and AMPK signaling.
Somatostatin study
From the pharmacokinetic study it was clear that ghrelin infusion caused metabolic
changes, but it was not elucidated if elevations in plasma glucose and serum FFA were
caused by ghrelin itself or by the concomitant release of GH and cortisol. A rough measure of
insulin sensitivity (revised QUICKI) revealed that ghrelin infusion caused insulin resistance
from t = 40 min and during the rest of the study day. The pharmacokinetic study also dem-
onstrated that GH and cortisol peaked after 60 and 120 min, respectively, whereafter a
gradual decline towards baseline levels was observed. In a previous study, concomitant
somatostatin infusion clearly impaired the ghrelin-induced GH release. Therefore, we used a
higher somatostatin infusion rate together with a constant ghrelin infusion and applied gold
standard technique for measurement of insulin sensitivity (hyperinsulinemic euglycemic
2 Bruce D Gaylinn et al. 2007 Long Term Fasting Inhibits Ghrelin Acylation but Not Ghrelin Secre-
tion in Normal Young Men; Evidence from New Assays for Full Length Acyl- and Des-Acyl Ghrelin. Proc 89th Ann Meeting Endocrine Soc P1-62 Abstract
32
Esben Thyssen Vestergaard Clinical aspects of ghrelin
clamp) in addition to tracer methodology and microdialysis to determine peripheral, hepatic,
and regional s.c. effects of ghrelin.
Hypopituitary study
The Somatostatin study revealed a moderate but detectable GH and cortisol break-
through. Although the GH and cortisol elevations were minute and comparable to – or lower
than – levels measured in the postabsorptive state (GH) (55) and during nighttime (cortisol)
(56) both GH and cortisol elevations reached statistical significance and may in part have
had metabolic effects. Therefore, a similar study comprising hypopituitary patients (GH re-
sponse to a dynamic GH stimulation test 0.3 ± 0.1 µg/l) on stable replacement therapy with
GH and hydrocortisone was undertaken. In addition to the methods applied to the Soma-
tostatin study, muscle and fat biopsies were performed and the Hypopituitary study included
more regional s.c. measurements to elaborate regional effects of ghrelin. Muscle biopsies
also enabled comparisons with biopsies from the pharmacokinetic study thereby delineating
JAK/STAT signaling by endogenous GH.
Considerations of possible mechanisms and explana-
tions - implications and review of literature
Endogenous ghrelin excursions and previous pharmacokinetic
studies
Endogenous ghrelin exhibits approximately 22 surges per 24 hours (57). Nagaya et al.
reported that total ghrelin levels disappeared from plasma with a half-life of 10 minutes after
a bolus injection (30). Subsequently, Akamizu et al. reported half-lives of both total (t½ 27 to
31 minutes) and acylated plasma ghrelin (t½ 9 to 13 minutes) in a one-compartment model
calculated from ghrelin concentrations in blood samples taken every 15 minutes (29). These
previously reported half-lives of total ghrelin are in line with the initial half-life (t½ 24.2 min-
utes) in our pharmacokinetic study.
Pharmacokinetics in a clinical context
Our study revealed that a bi-exponential equation gave the best fit as compared to a
mono-exponential approach. One explanation can be attributed to the frequency of blood
sampling since the concentration-time curve appears monophasic when the fraction of a
substance eliminated by the last exponential term (f2) is relatively large (in this study 33%)
33
Esben Thyssen Vestergaard Clinical aspects of ghrelin
and blood is drawn less frequently. To circumvent this problem, blood samples were col-
lected every five minutes for the first hour after termination of the ghrelin infusion in order
to detect the two distinct slopes of the decay curve. Another plausible explanation is attrib-
utable to our assay that recognizes ghrelin as well as desacyl ghrelin. Recently, ghrelin has
been demonstrated to degrade to desacyl ghrelin (53) and because desacyl ghrelin has a
larger half-life than ghrelin (29), ghrelin elimination appears to follow a bi-exponential decay
curve. Of note, Gauna et al. detected higher total serum ghrelin levels after administration of
acylated ghrelin than after an equal dose of desacyl ghrelin (31). Systematic in vitro experi-
ments demonstrated that this surprising observation was not caused by an assay problem.
Rather, they suggested that the apparent increase in desacyl ghrelin following administration
of acylated ghrelin stemmed from endogenous release of desacyl ghrelin or was caused by
an acute change in the capacity to degrade ghrelin (31).
However, pharmacokinetic parameters from our bi-exponential approach predicted the
experimentally obtained ghrelin levels during the infusion period. A small tendency to overes-
timate the experimental ghrelin levels by the two-compartment analysis indicates that simpli-
fying distribution kinetics of ghrelin to a one-compartment model is inadequate.
The peak ghrelin concentration observed was very similar to the mathematically pre-
dicted level, but a steady state level was not reached again in accordance with a two-
compartment model. Our observations contrast previous ghrelin infusion studies reporting
steady state within 60 to 90 minutes (18;19;33;58). However, none of the previous reports
provides the pharmacokinetic approach, making it difficult to draw direct comparisons to our
results. The clinical implications of the two-compartment characteristics of ghrelin are that
longer infusion periods are required to obtain steady state levels of ghrelin in clinical ghrelin
infusion studies.
Predictors of ghrelin levels
Systemic ghrelin levels change dynamically to feeding state (59;60). The present studies
revealed a positive correlation between BMI and MRT of ghrelin. Thus, the counter-
regulatory decline in ghrelin levels that presumably serves to compensate for a positive en-
ergy expenditure in obese individuals (61-63) is not attributable to increased clear-
ance/decreased MRT of ghrelin. Therefore, decreased ghrelin levels in obesity appear to be
caused by decreased secretion rates. Our observation (MRT of ghrelin correlates positively
with BMI) is substantiated by a previous report, where a constant ghrelin infusion increased
circulating ghrelin levels more in obese than in lean subjects (17), and it is compatible with
34
Esben Thyssen Vestergaard Clinical aspects of ghrelin
previous studies reporting that obese individuals have a reduced postprandial decrease in
ghrelin levels as compared to lean subjects (61-63).
A positive correlation between MRT and HDL cholesterol levels was also revealed. Al-
though correlation does not imply causality, it has previously been shown that the majority
of circulating acylated ghrelin is bound to larger molecules (64), and the high-density lipo-
protein-fraction has been demonstrated to bind acylated ghrelin in vi (65). HDL choles-
terol levels could thus be an independent biological determinant of ghrelin bioavailability in
humans and may account for the 2
tro
nd compartment.
Effects on appetite
The appetite related results were moderate and mostly non-significant as compared to
previous publications (17-19;66). Temporal and concentration differences between the ear-
lier reports and the present results may have caused these discrepancies. Wren et al. (19)
studied orexigenic and appetite effects of more physiological increments (approximately 2-
fold elevations from baseline), significantly less than the 6.5-fold increase we obtained. High
ghrelin levels may entail compensatory mechanisms such as internalization of the GHS-R
from the cell surface in order to desensitize the cell responsiveness (67) and the effect of
ghrelin on food intake in rodents is indeed bell-shaped (68). The studies by Druce et al. (17),
Schmid et al. (66), and Neary et al. (18) reported the orexigenic effects of ghrelin after 45,
60, and 90 minutes respectively.
Hormonal and metabolite effects
In the pharmacokinetic study, significant elevations were observed in circulating levels of
GH, ACTH, cortisol, prolactin, glucose and FFAs in accordance with most previous reports
(4;5;14;17-19;29-33;66;69;70). A small but significant increase in plasma glucose levels was
also observed, but in contrast to one former study (22), this was associated with an increase
rather than a decrease in insulin levels. From this study it is not possible to determine any
direct metabolic effect of ghrelin, but our results appear to corroborate earlier observations
reporting that ghrelin induces insulin resistance in humans (31)
At first glance, the increase in cortisol levels contrasts the previous established inverse
correlation between ghrelin and cortisol observed during fasting (12). However, the ACTH
concentration-time curve reveals a transient increase in ACTH levels after 60 minutes of
ghrelin infusion only, whereafter ACTH levels return to baseline levels. The present ghrelin
infusion period is not sufficient to disclose any effect of ghrelin on cortisol levels after nor-
35

Esben Thyssen Vestergaard Clinical aspects of ghrelin
malization of ACTH levels, but the decrease in cortisol levels at t = 360 minutes indicates
that ghrelin may actually inhibit cortisol levels on the long term.
Pancreatic clamp technique and adjustable glucose infusion in the Somatostatin study
ensured comparable levels of glucose, FFA, insulin, C-peptide, and glucagon. Somatostatin
attenuated the ghrelin-induced GH response to levels comparable to physiological GH bursts
in the postabsorptive state (55), but cortisol excursions recorded during ghrelin infusion
were comparable to the levels reported in the pharmacokinetic study.
In the Hypopituitary study, similar hormonal levels during ghrelin and saline infusion
were successfully achieved. The increases in glucose and FFA levels therefore seemed di-
rectly attributable to ghrelin exposure.
Effects on substrate metabolism
In the Somatostatin study, ghrelin infusion combined with a pancreatic clamp caused a
significant reduction in glucose disposal rates and GIR, and lipolysis in terms of increased
palmitate rate of appearance and FFA levels. Although the GH response was clearly attenu-
ated as compared with previous ghrelin infusion studies (22;32;33;71;72), small and physio-
logical GH excursions may affect substrate metabolism, although its significance is disputable
(73-76). In the present study cortisol levels during ghrelin infusion surpassed placebo levels
from time 60 to 240 min and reached ~ 2-fold the corresponding placebo level after 90 min.
The metabolic impact of such increments in cortisol levels on glucose and lipid metabolism is
also uncertain (77-80). In our study, a correlation between GH, cortisol and FFA indicate that
GH and cortisol actually caused lipolysis, which, in turn can induce insulin resistance. How-
ever, neither GH nor cortisol was predictor, when palmitate turn-over rate was included as
the dependent variable.
In the Hypopituitary study, we accomplished to factor out GH and cortisol increments.
Ghrelin infusion did indeed cause a decrease in glucose disposal rates, GIR, and lipolysis. We
recorded significantly increased interstitial glucose levels in skeletal muscle substantiating
that insulin sensitivity was significantly attenuated in this tissue. The molecular mechanisms
by which, ghrelin influences glucose and lipid metabolism remain however to be determined,
because no detectable aberrations in AMPK, PI3K, PKB/Akt, or AS160 were retrieved in
skeletal muscle. In particular, it is still not evident whether ghrelin causes insulin resistance
directly and, as a secondary phenomenon, lipolysis or vice versa. It is possible to suppress
lipolysis pharmacologically and the role of the concomitant ghrelin-induced FFA increase
could be explored by using an inhibitor of lipolysis (e.g. acipimox). It is, however, important
36

Esben Thyssen Vestergaard Clinical aspects of ghrelin
to note that biopsies were only obtained in the basal state, and it remains to be demon-
strated whether ghrelin may influence the same signaling pathways during concomitant insu-
lin stimulation.
Although our results demonstrate an insulin antagonistic effect rather than a stimulation
of insulin signaling, which is evident in in vitro experiments (81-85), our results are in line
with the in vivo evidence that ghrelin induces insulin resistance (31;36).
FFA levels increased in response to ghrelin administration, but this increase did not trans-
late into an increase in whole body lipid oxidation or energy expenditure contrasting obser-
vations in rodent models (20;86-88). The mechanism by which lipid oxidation remained unaf-
fected in the present study is undetermined. However in rodents, it has been demonstrated
that ghrelin induces a hepatic lipogenic gene expression together with a reduction in AMPK
levels, which is a stimulator of FFA oxidation (89). It remains to be elucidated if ghrelin also
affects expressions of genes involved in lipid oxidation in humans as indicated by our clinical
observations.
It remains speculative what the exact physiological role of ghrelin is in humans. The role
of ghrelin in appetite regulation and food intake has been studied extensively. Numerous
rodent models comprising ghrelin knockouts, ghrelin receptor knockouts, measurements of
neuropeptide Y and agouti-related peptide expressions following ghrelin administration,
blocking antibodies, ghrelin antagonists, and blocking RNA Spiegelmers indicate that ghrelin
stimulates food intake. In humans, ghrelin increases before food intake and decreases
shortly after feeding even without time and food-related cues and ghrelin has therefore been
suggested to initiate food intake (90). This study reported total levels of ghrelin only, so the
relationship between appetite and acylated ghrelin (i.e. the orexigenic subtype) is still not
clarified and one study by Avram et al. found no effects of either fasting or feeding on acy-
lated ghrelin levels (91).
The role of ghrelin in regulation of GH secretion has been addressed in a number of stud-
ies. The preprandial and nocturnal increments of ghrelin may hypothetically cause subse-
quent GH secretion, but analyses of the ghrelin-GH interrelationship have reported inconsis-
tent results: 1) positive association between ghrelin and GH pulsatility (92), 2) no relation
between GH and ghrelin pulses (91), and 3) a correlation depending on certain conditions
(93). Moreover, physiological conditions characterized by a GH increase are not preceded by
elevated peripheral ghrelin levels (11-13). Thus, it remains to be convincingly demonstrated
that gut-derived ghrelin is a significant GH releasing factor.
37

Esben Thyssen Vestergaard Clinical aspects of ghrelin
The role of ghrelin in substrate metabolism is currently a matter of debate. Numerous ro-
dent models demonstrate that ghrelin administration increases adiposity, whereas data from
ghrelin and ghrelin receptor knockout models have not convincingly supported the adipo-
genic properties of ghrelin (86;88;94;95). There seems to be more evidence that ghrelin
affects glucose homeostasis and decreases insulin sensitivity (22;34-37). All of our three
studies in this dissertation support that ghrelin acutely causes insulin resistance directly as
well as indirectly by elevation of GH and cortisol levels. It therefore seems possible that a
natural metabolic domain for ghrelin action is in conditions characterized by short term en-
ergy shortage, where ghrelin gradually increases during the time interval until the next meal,
whereafter food intake causes the next ghrelin decrease (15;96). Ghrelin could be specu-
lated to counteract fasting-induced hypoglycemia and thereby secure fuel supply for glucose
dependent tissues such as the central nervous system (97). Ghrelin does not increase consis-
tently after prolonged fasting (12), and it therefore remains uncertain whether ghrelin in this
condition regulates GH secretion or substrate metabolism.
Effects on resting energy expenditure
Resting energy expenditure decreased in response to ghrelin and the pancreatic clamp
during hyperinsulinemia, whereas no change was evident in the Hypopituitary study. In GHD
rodents, 24-h EE was not affected, but transient and small negative deflections in EE were
recorded immediately following ghrelin injections (20) indicating that ghrelin exerted some
effects on EE. Numerous rodent studies report either increased or decreased spontaneous
activity following ghrelin administration, whereas the effect of ghrelin on resting EE in hu-
mans, to our knowledge, has not been reported previously. Our present studies suggest that
ghrelin is not a major determinant of EE, but more powerful studies need to be undertaken
to further investigate this matter.
Methodological limitations and pitfalls
Pharmacokinetic study
Only total levels of serum ghrelin were measured. Total ghrelin comprises of the acylated
as well as the desacyl 28 amino-acid peptide, probably along with other shorter fragments
and elongated ghrelin forms. Of note, the endocrine effects of ghrelin are mainly attributed
to the octanoylation on serine number 3 (4;98). By the time the pharmacokinetic study was
designed, this was not an obvious limitation, because we planned to infuse the genuine acy-
lated human ghrelin form and the assay would therefore presumably mainly measure acy-
38

Esben Thyssen Vestergaard Clinical aspects of ghrelin
lated ghrelin levels. Recently, it became evident that ghrelin is indeed degraded by cleaving
off of the acyl side chain, because a sensitive, quantitative mass spectrometry method
documented that serum levels of ghrelin decreased, whereas desacyl ghrelins levels in-
creased in a stoichiometric ratio (53). Thus, the assay used in this study is a limitation, and
this should be kept in mind when interpreting the results and conclusions with regards to the
pharmacokinetics. However, the equation used to predict steady state concentrations ap-
pears to be a useful tool, since it was successfully used in the Hypopituitary study, where a
primed continuous ghrelin infusion accurately predicted steady state concentrations (5.12 ±
0.45 µg/l vs. predicted 5.00 ± 0.35 µg/l).
The hunger data are conflicting and therefore difficult to interpret. The lack of compelling
appetite effects in this study may in part be attributed to the infrequent measurements on
the visual analogue scale. Instead, study participants could have been offered an ad libitum
buffet to measure energy intake rather than relying on a hypothetical response.
Somatostatin study
The somatostatin clamp did not abolish ghrelin-induced GH release. A small but signifi-
cant GH peak occurred and at least part of the effects on glucose and lipids are presumably
explained by GH. The study question: whether ghrelin per se has direct effects on glucose
and lipid metabolism can therefore not be fully answered by the study.
The fact that glucose levels fell during the basal period of the saline/ghrelin period indi-
cates that the low-dose insulin infusion had an effect, and at the end of the basal period the
glucose levels rose and the glucose infusion rate dropped. This indicates that lipolysis was
ongoing and glucose uptake reduced, most likely due to the small dose of GH infusion and
on the ghrelin day also due to the GH peak induced. In, addition, regression analysis re-
vealed that ∆AUC of GH, P = 0.005, and cortisol, P = 0.002, were both significant predictors
of ∆AUC of FFA, but the correlation was not supported when palmitate flux was included
instead of ∆AUC of FFA as dependent variable. The discrepancy between the effects of ghre-
lin on ∆AUC of FFA and palmitate flux may be attributable to a smaller method sensitivity of
the tracer technique as compared to the measurements of FFA concentrations. However, the
exact cause of the discrepancy has not been elucidated.
Plasma glucagon was stable during initial 30-min, whereafter an increasing trend was
evident. The reason for this increase is not clear and contrasts similar somatostatin gluca-
gon-replacement studies, where plasma glucagon remains at steady state. However, plasma
39

Esben Thyssen Vestergaard Clinical aspects of ghrelin
glucagon levels were similar during both saline and ghrelin administration. Therefore, it
seems unlikely that glucagon caused the effects on GIR and substrate metabolism.
Hypopituitary study
Due to the extensive and complex study design the number of biopsies was limited. Per-
forming a biopsy in the basal period favored the study of GH signaling, whereas a biopsy
during hyperinsulinemia would have been optimal for studying insulin signaling. The basal
period was chosen in order to make it comparable to the biopsy timing of the pharmacoki-
netic study. In the basal state, insulin signaling activity is low a priori, and it would have
been relevant and informative also to have biopsies during the hyperinsulinemic clamp pe-
riod.
In the basal period plasma glucose increased in response to ghrelin, although glucose
disposal rate, endogenous glucose production and glucose infusion were constant. This
seems to be attributable to methodological insensitivity unless, unlikely so, changes in vol-
ume of distribution for glucose could explain the apparent discrepancy.
Conclusions & Perspectives
Conclusions
In conclusion, the kinetics of infused ghrelin follows a two-compartment model and the
mean residence time of infused ghrelin correlates positively with both HDL cholesterol and
BMI. The pharmacokinetic study provides useful data when tailoring ghrelin infusion rates in
clinical experiments. Ghrelin infusion induces a robust release of both GH and cortisol ac-
companied by an increase in systemic glucose and FFA levels.
Concomitant somatostatin infusion blunts the ghrelin-induced GH release, but the effects
on systemic glucose and FFA levels prevail in addition to a reduction of insulin sensitivity.
Hypopituitary patients with GH and ACTH deficiency constitute an attractive in vivo model
for studying putative GH- and cortisol-independent effects of ghrelin. In the Hypopituitary
study, we demonstrate that ghrelin infusion per se causes insulin resistance and increments
of systemic glucose and FFA levels. These effects were not attributed to direct detectable
effects on AMPK, insulin or JAK/STAT signaling.
40

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Perspectives
Potential therapeutic applications of ghrelin in conditions characterized by
impaired ghrelin secretion
Conditions characterized by low GH levels such as obesity (99) and aging (100) and con-
ditions characterized by “ghrelin resistance”, e.g. cachexia (101) and anorexia nervosa (102),
may benefit from prolonged treatment with ghrelin or GHS. These conditions have been the
objective of a few controlled trials, but the potential therapeutic role of ghrelin and GHS still
needs to be elucidated in detail. Ghrelin administration has, indeed, proved successful in
short term treatment of cardiac and pulmonary cachexia; three weeks of ghrelin administra-
tion to 10 patients suffering from chronic heart failure improved lean body mass, muscle
strength, peak workload and oxygen consumption during exercise (103). A similar trial com-
prising a three week period and equal ghrelin doses improved body composition, muscle
wasting, and functional capacity in patients suffering from cachexia due to chronic pulmo-
nary obstructive disease (104).
Certain subgroups of patients with classic GHD such as patients suffering from pituitary
stalk lesions (105) may benefit from chronic treatment with GHS or ghrelin. In a randomized,
placebo-controlled, double-blind study 11% (n = 83) of adult GHD patients responded with a
peak GH response ≥ 5 µg/L after the first or the last dose of the oral GHS NN703 (106). Ad-
ministration of another oral GHS, MK-0677, during a 7 – 8 day period in 18 prepubertal chil-
dren with idiopathic GHD also induced an increase in GH in the subjects receiving the highest
dose (n = 12) (107). Patients with baseline serum IGF-I levels greater than 50 µg/L showed
a more pronounced GH response to MK-0677 in comparison with patients whose baseline
serum IGF-I levels were below 50 µg/L (107). A third randomized, double-blind, cross-over
study confirmed that the effect of GHS correlates inversely with the degree of GHD (108).
A potential advantage of GHS or ghrelin treatment in the subgroups above includes pres-
ervation of the negative IGF-I feedback on GH secretion and for GHS treatment the possibil-
ity of oral administration is appealing. Future studies may reveal whether GHS or ghrelin
actually have therapeutic potential in the above-mentioned conditions.
Limitations for ghrelin treatment in a clinical setting
Ghrelin is one of the most potent GHS and in comparison to hexarelin, a synthetic GHS
for intravenous administration, ghrelin has a stronger GH-releasing effect (14). The major
limitation of ghrelin treatment in a clinical setting is attributable to a very short half-life when
injected intravenously and oral bioavailability is probably negligible although it has never
41

Esben Thyssen Vestergaard Clinical aspects of ghrelin
been tested. S.c. ghrelin administration elicits a bell-shaped GH response after 30 minutes,
but the response only lasts between 60 and 90 minutes (69).
Diagnostic potential of ghrelin
Ghrelin levels are not altered in patients with GHD (11;109;110), and ghrelin measure-
ments therefore do not seem helpful for the diagnosis and follow-up of these patients. The
diagnosis of GHD is established by provocative tests and the test of choice is the insulin tol-
erance test (ITT) (111). Certain contraindications apply to this test, e.g. patient history of
ischemic heart disease or seizure disorder, in the event of which the GHRH plus arginine test
is considered as a second choice. GHS binds to hypothalamic and pituitary cells (112) and
augments the effect of GHRH on GH-release (113). The GHS GHRP-6 in combination with
GHRH has also proved useful as a diagnostic tool in adult GHD (114;115). If appropriate cut-
off levels are taken into account, these tests may prove an alternative to the ITT.
It is a potential concern that patients with GHD secondary to pituitary stalk lesions may
be misdiagnosed by exhibiting a normal response to exogenous ghrelin or a GHS. Whether
this is a clinically significant problem is, however, uncertain; at least it has been reported
that GHRH in combination with pyridostigmine correctly diagnoses patients with severe GHD,
irrespective of etiology, provided that an appropriate cut-off is available (116).
Other aspects of ghrelin administration to hypopituitary patients
The vast majority of clinical and many animal studies reporting effects of exogenous
ghrelin are hampered by the concomitant increase of GH secretion in addition to cortisol in-
crements. Many scientific articles should be interpreted with care, because they report the
combined effects of ghrelin, GH, IGF-I and cortisol rather than effects of ghrelin per se.
Therefore, hypopituitary patients constitute an interesting model for studying GH- and ACTH-
independent effects of ghrelin and future studies comprising this group of patients may re-
sult in more valid conclusions regarding direct effects of ghrelin.
Potential therapeutic applications of ghrelin antagonists
Obesity, the metabolic syndrome, type 2 diabetes, and the associated complications are
major and growing problems in the health care services and the lay public. It is evident that
preventing or treating obesity, hyperlipidemia, and diabetes by life style interventions and
medical therapy improves quality of life and health. Among numerous factors leading to a
positive energy balance, ghrelin has attracted attention because it induces appetite
(17;19;66), increases food intake (17-19), decreases insulin secretion (22;34;68;117-119),
and causes insulin resistance (33). In turn, antagonists of ghrelin and animal ghre-
42

Esben Thyssen Vestergaard Clinical aspects of ghrelin
lin(receptor) knockout models have demonstrated beneficial effects on appetite and food
intake (86;88;119), insulin secretion (35;36;119) and insulin sensitivity (36;37;94). Future
clinical trials will reveal whether results from rodent studies apply to human physiology; i.e. if
antagonism of ghrelin enhances insulin secretion to match increased insulin requirements in
diet-induced obesity and improves glycemic control, and if ghrelin antagonists thereby have
therapeutic potential in the treatment of the metabolic syndrome and type 2 diabetes in ad-
dition to body weight control.
Summary Ghrelin is a gastrointestinal peptide hormone originally discovered as the endogenous
ligand for the GHS-R. The GHS-R is widely distributed and ongoing research suggests plei-
otropic effects of ghrelin. In view of the potential therapeutic applications of ghrelin the
overall aim of this PhD study was to investigate clinical pharmacokinetics and acute meta-
bolic effects of ghrelin in detail.
The PhD dissertation consists of three original papers based on three randomized, pla-
cebo-controlled cross-over clinical protocols comprising both healthy subjects and hypopitui-
tary patients: 1) Pharmacokinetic study, 2) Somatostatin study, and 3) Hypopituitary study.
Two articles have been published in international peer-reviewed journals and a third manu-
script has been submitted for review.
In the first protocol, acylated ghrelin was infused into 17 healthy subjects. By measure-
ments of ghrelin levels and pharmacokinetic modeling an extensive list of pharmacokinetic
parameters was calculated and correlated with central parameters of individual characteris-
tics. In addition, muscle biopsies were sampled to study pertinent ghrelin signaling path-
ways.
In the second protocol comprising eight healthy subjects receiving ghrelin and placebo
infusion on two different occasions, the aim was to suppress the ghrelin-induced GH- and
cortisol-secretion by concomitant somatostatin infusion in order to measure the direct effects
of ghrelin on glucose and lipid metabolism. Insulin sensitivity was measured by a hyperinsu-
linemic euglycemic clamp and substrate metabolism was measured by tracer and microdialy-
sis technique. The Somatostatin study revealed a moderate but detectable GH and cortisol
breakthrough.
To circumvent the effects of endogenous GH and cortisol on glucose and lipid metabo-
lism, a third study comprising eight hypopituitary adults on stable replacement therapy with
43

Esben Thyssen Vestergaard Clinical aspects of ghrelin
GH and hydrocortisone was performed. In this protocol, we also used the pharmacokinetic
parameters to calculate a ghrelin bolus dose to rapidly achieve steady state concentrations.
The pharmacokinetic results showed that ghrelin infusion followed a two-compartment
model. The MRT of exogenous ghrelin correlated positively with both HDL cholesterol levels
and BMI. The pharmacokinetic parameters are useful for designing future clinical ghrelin
infusion studies. Concomitant somatostatin infusion attenuated ghrelin induced GH secretion,
but GH levels were significantly increased as compared to GH levels during placebo admini-
stration. In the Hypopituitary study, it was demonstrated that ghrelin infusion per se caused
insulin resistance and increments in levels of systemic glucose and FFA levels. These effects
were not attributed to direct detectable effects on AMPK, insulin or JAK/STAT signaling. No
aberrations in putative ghrelin signaling pathways were detected. In addition, our studies
demonstrated that ghrelin-induced endogenous GH release translated into GH receptor sig-
naling in skeletal muscle.
Summary in Danish Ghrelin er et gastrointestinalt peptid-hormon bestående af 28 aminosyrer med en unik
acyl-sidekæde. Ghrelin blev opdaget i 1999 af en forskergruppe, som ledte efter en endogen
ligand for den såkaldte GHS receptor. GHS receptoren var forinden karakteriseret og klonet i
1996. GHS receptoren forefindes i størstedelen af kroppens væv. Man kunne derfor forvente,
at dette relativt nyopdagede peptid-hormon ville frembyde en række forskelligartede effek-
ter. Talrige kliniske, dyreeksperimentelle og laboratoriebaserede forsøg indenfor dette områ-
de har efterfølgende vist, at ghrelin i overensstemmelse med receptorens lokalisation, har
adskillige effekter. Heriblandt er det muligt, at ghrelin kan have et terapeutisk potentiale og
dette PhD-studium havde til formål at undersøge og tilvejebringe ny viden om ghrelins klini-
ske farmakokinetiske og akutte metaboliske effekter.
PhD-afhandlingen består af tre originalartikler, som er baseret på tre kliniske, randomise-
rede, placebo-kontrollerede overkrydsningsstudier, hvor både raske og hypofyseinsufficiente
patienter blev undersøgt. Studierne er 1) Farmakokinetikstudiet, 2) Somatostatinstudiet og
3) Hypofyseinsufficiensstudiet. Artiklerne fra det første og andet studium er allerede publice-
ret i internationale peer-reviewed tidsskrifter, mens artiklen vedr. det sidste studium er ind-
sendt til bedømmelse ligeledes ved et internationalt tidsskrift.
I det første studium deltog 17 raske, unge mænd. Vi infunderede henholdsvis ghrelin og
saltvand på to forskellige undersøgelsesdage og målte efterfølgende ghrelinniveauerne i se-
rum. Ved hjælp af farmakokinetisk modellering og beregninger estimerede vi en række væ-
44

Esben Thyssen Vestergaard Clinical aspects of ghrelin
sentlige farmakokinetiske variabler og udførte korrelationsstudier, hvor centrale individaf-
hængige karakteristika indgik. Målinger af GH, kortisol, glukose og frie fedtsyrer viste, at
ghrelin medførte sekretion af begge hormoner og øgede de systemiske niveauer af begge
substrater.
I det andet studium deltog 8 raske, unge mænd. Vi infunderede henholdsvis ghrelin og
saltvand på to forskellige undersøgelsesdage samtidig med somatostatin for at undertrykke
GH og kortisol sekretionen og for dermed at undersøge ghrelins direkte effekter på glukose-
og lipidmetabolisme. Insulinfølsomhed blev målt med hyperinsulinæmisk euglykæmisk
clampteknik og substratmetabolisme blev målt med både tracerteknik og mikrodialyse. I det-
te studium var der på trods af somatostatininfusionen en moderat GH og kortisol sekretion.
For at undgå den endogene GH og kortisolsekretion og disses effekter på glukose- og li-
pidmetabolisme, udførte vi et tredje studium med hypofyseinsufficiente voksne patienter
behandlet med GH- og hydrokortisonsubstitution. I dette forsøg anvendte vi også den far-
makokinetiske viden fra det første forsøg til at beregne en ghrelin bolus-dosis, således at
ghrelin ligevægtsniveauet blev opnået hurtigere end ved en konstant ghrelininfusion.
Det farmakokinetiske studium viste, at infunderet ghrelin følger to-kompartment-
karakteristik. Det farmakokinetiske begreb mean residence ime (et udtryk for den gennem-
snitlige tid et givent molekyle opholder sig i kroppen) udviste positiv korrelation med både
højdensitet kolesterol niveauer og body mass index. De beregnede farmakokinetiske para-
metre kan med fordel benyttes i designet af fremtidige ghrelininfusionsstudier og har allere-
de fundet anvendelse i Hypofyse-insufficiensstudiet. Somatostatinstudiet viste, at somatosta-
tin nedsatte den endogene GH sekretion betydeligt, men GH niveauerne var signifikant høje-
re end de tilsvarende niveauer under placebo- og somatostatinindgift. Hypofyseinsufficiens-
studiet viste, at ghrelininfusion uafhængigt af GH og kortisol medførte insulinresistens og
øgede plasmaniveauerne af glukose og serumniveauerne af frie fedtsyrer. Effekterne kunne
ikke tilskrives målbare ændringer af AMPK, insulin eller JAK/STAT signalvejs-molekyler og vi
fandt ingen ændring af formodede ghrelinsignalvejs enzymer. Derudover viste vores studier,
at ghrelininduceret GH sekretion medførte aktivering af GH signalvejen i skeletmuskulatur.
t
Acknowledgements I am indebted to Aarhus University for providing a research fellowship and to Novo Nord-
isk for an unrestricted educational grant. I wish to thank the following foundations for pro-
viding me financial support: The World Anti-Doping Agency (WADA), The Research Initiative
of Aarhus University Hospital, The John and Birthe Meyer Foundation, The FOOD Study
45

Esben Thyssen Vestergaard Clinical aspects of ghrelin
Group/Ministry of Food, Agriculture and Fisheries & Ministry of Family and Consumer Affairs,
The Maersk McKinney Møller and wife Chastine McKinney Møller Foundation, The Danish
Diabetes Association, and Roche Diagnostics for kindly providing microdialysis catheters.
References 1. Momany FA, Bowers CY, Reynolds GA, Chang D, Hong A, Newlander K 1981 Design, synthesis,
and biological activity of peptides which release growth hormone in vitro. Endocrinology 108:31-39
2. Howard AD, Feighner SD, Cully DF, Arena JP, Liberator PA, Rosenblum CI, Hamelin M, Hreniuk DL, Palyha OC, Anderson J, Paress PS, Diaz C, Chou M, Liu KK, McKee KK, Pong SS, Chaung LY, Elbrecht A, Dashkevicz M, Heavens R, Rigby M, Sirinathsinghji DJ, Dean DC, Melillo DG, Van der Ploeg LH, . 1996 A receptor in pituitary and hypothalamus that functions in growth hormone release. Science 273:974-977
3. Kojima M 2007 The discovery of ghrelin - A personal memory. Regul Pept
4. Kojima M, Hosoda H, Date Y, Nakazato M, Matsuo H, Kangawa K 1999 Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature 402:656-660
5. Takaya K, Ariyasu H, Kanamoto N, Iwakura H, Yoshimoto A, Harada M, Mori K, Komatsu Y, Usui T, Shimatsu A, Ogawa Y, Hosoda K, Akamizu T, Kojima M, Kangawa K, Nakao K 2000 Ghrelin strongly stimulates growth hormone release in humans. J Clin Endocrinol Metab 85:4908-4911
6. Tannenbaum GS, Ling N 1984 The interrelationship of growth hormone (GH)-releasing factor and somatostatin in generation of the ultradian rhythm of GH secretion. Endocrinology 115:1952-1957
7. Moller N, Nygren J, Hansen TK, Orskov H, Frystyk J, Nair KS 2003 Splanchnic release of ghrelin in humans. J Clin Endocrinol Metab 88:850-852
8. Jeon TY, Lee S, Kim HH, Kim YJ, Son HC, Kim DH, Sim MS 2004 Changes in plasma ghrelin con-centration immediately after gastrectomy in patients with early gastric cancer. J Clin Endocrinol Metab 89:5392-5396
9. Gnanapavan S, Kola B, Bustin SA, Morris DG, McGee P, Fairclough P, Bhattacharya S, Car-penter R, Grossman AB, Korbonits M 2002 The tissue distribution of the mRNA of ghrelin and sub-types of its receptor, GHS-R, in humans. J Clin Endocrinol Metab 87:2988
10. Papotti M, Ghe C, Cassoni P, Catapano F, Deghenghi R, Ghigo E, Muccioli G 2000 Growth hor-mone secretagogue binding sites in peripheral human tissues. J Clin Endocrinol Metab 85:3803-3807
11. Dall R, Kanaley J, Hansen TK, Moller N, Christiansen JS, Hosoda H, Kangawa K, Jorgensen JO 2002 Plasma ghrelin levels during exercise in healthy subjects and in growth hormone-deficient pa-tients. Eur J Endocrinol 147:65-70
12. Espelund U, Hansen TK, Hojlund K, Beck-Nielsen H, Clausen JT, Hansen BS, Orskov H, Jorgensen JO, Frystyk J 2005 Fasting unmasks a strong inverse association between ghrelin and cor-tisol in serum: studies in obese and normal-weight subjects. J Clin Endocrinol Metab 90:741-746
13. Lucidi P, Murdolo G, Di Loreto C, De Cicco A, Parlanti N, Fanelli C, Santeusanio F, Bolli GB, De Feo P 2002 Ghrelin is not necessary for adequate hormonal counterregulation of insulin-induced hy-poglycemia. Diabetes 51:2911-2914
14. Arvat E, Maccario M, Di Vito L, Broglio F, Benso A, Gottero C, Papotti M, Muccioli G, Dieguez C, Casanueva FF, Deghenghi R, Camanni F, Ghigo E 2001 Endocrine activities of ghrelin, a natural growth hormone secretagogue (GHS), in humans: comparison and interactions with hexarelin, a non-natural peptidyl GHS, and GH-releasing hormone. J Clin Endocrinol Metab 86:1169-1174
46
Esben Thyssen Vestergaard Clinical aspects of ghrelin
15. Cummings DE, Purnell JQ, Frayo RS, Schmidova K, Wisse BE, Weigle DS 2001 A preprandial rise in plasma ghrelin levels suggests a role in meal initiation in humans. Diabetes 50:1714-1719
16. Nakazato M, Murakami N, Date Y, Kojima M, Matsuo H, Kangawa K, Matsukura S 2001 A role for ghrelin in the central regulation of feeding. Nature 409:194-198
17. Druce MR, Wren AM, Park AJ, Milton JE, Patterson M, Frost G, Ghatei MA, Small C, Bloom SR 2005 Ghrelin increases food intake in obese as well as lean subjects. Int J Obes Relat Metab Disord
18. Neary NM, Small CJ, Wren AM, Lee JL, Druce MR, Palmieri C, Frost GS, Ghatei MA, Coombes RC, Bloom SR 2004 Ghrelin increases energy intake in cancer patients with impaired appetite: acute, randomized, placebo-controlled trial. J Clin Endocrinol Metab 89:2832-2836
19. Wren AM, Seal LJ, Cohen MA, Brynes AE, Frost GS, Murphy KG, Dhillo WS, Ghatei MA, Bloom SR 2001 Ghrelin enhances appetite and increases food intake in humans. J Clin Endocrinol Metab 86:5992-5995
20. Tschop M, Smiley DL, Heiman ML 2000 Ghrelin induces adiposity in rodents. Nature 407:908-913
21. Arosio M, Ronchi CL, Gebbia C, Cappiello V, Beck-Peccoz P, Peracchi M 2003 Stimulatory effects of ghrelin on circulating somatostatin and pancreatic polypeptide levels. J Clin Endocrinol Metab 88:701-704
22. Broglio F, Arvat E, Benso A, Gottero C, Muccioli G, Papotti M, Van der Lely AJ, Deghenghi R, Ghigo E 2001 Ghrelin, a natural GH secretagogue produced by the stomach, induces hyperglycemia and reduces insulin secretion in humans. J Clin Endocrinol Metab 86:5083-5086
23. Tack J, Depoortere I, Bisschops R, Verbeke K, Janssens J, Peeters T 2005 Influence of ghrelin on gastric emptying and meal-related symptoms in idiopathic gastroparesis. Aliment Pharmacol Ther 22:847-853
24. Dornonville dlC, Lindstrom E, Norlen P, Hakanson R 2004 Ghrelin stimulates gastric emptying but is without effect on acid secretion and gastric endocrine cells. Regul Pept 120:23-32
25. Date Y, Nakazato M, Murakami N, Kojima M, Kangawa K, Matsukura S 2001 Ghrelin acts in the central nervous system to stimulate gastric acid secretion. Biochem Biophys Res Commun 280:904-907
26. Masuda Y, Tanaka T, Inomata N, Ohnuma N, Tanaka S, Itoh Z, Hosoda H, Kojima M, Kan-gawa K 2000 Ghrelin stimulates gastric acid secretion and motility in rats. Biochem Biophys Res Com-mun 276:905-908
27. Tschop M, Weyer C, Tataranni PA, Devanarayan V, Ravussin E, Heiman ML 2001 Circulating ghrelin levels are decreased in human obesity. Diabetes 50:707-709
28. Otto B, Cuntz U, Fruehauf E, Wawarta R, Folwaczny C, Riepl RL, Heiman ML, Lehnert P, Fich-ter M, Tschop M 2001 Weight gain decreases elevated plasma ghrelin concentrations of patients with anorexia nervosa. Eur J Endocrinol 145:669-673
29. Akamizu T, Takaya K, Irako T, Hosoda H, Teramukai S, Matsuyama A, Tada H, Miura K, Shi-mizu A, Fukushima M, Yokode M, Tanaka K, Kangawa K 2004 Pharmacokinetics, safety, and en-docrine and appetite effects of ghrelin administration in young healthy subjects. Eur J Endocrinol 150:447-455
30. Nagaya N, Kojima M, Uematsu M, Yamagishi M, Hosoda H, Oya H, Hayashi Y, Kangawa K 2001 Hemodynamic and hormonal effects of human ghrelin in healthy volunteers. Am J Physiol Regul In-tegr Comp Physiol 280:R1483-R1487
31. Gauna C, Meyler FM, Janssen JA, Delhanty PJ, Abribat T, Van Koetsveld P, Hofland LJ, Bro-glio F, Ghigo E, Van der Lely AJ 2004 Administration of acylated ghrelin reduces insulin sensitivity, whereas the combination of acylated plus unacylated ghrelin strongly improves insulin sensitivity. J Clin Endocrinol Metab 89:5035-5042
47

Esben Thyssen Vestergaard Clinical aspects of ghrelin
32. Lucidi P, Murdolo G, Di Loreto C, Parlanti N, De Cicco A, Fatone C, Taglioni C, Fanelli C, Bro-glio F, Ghigo E, Bolli GB, Santeusanio F, De Feo P 2005 Metabolic and endocrine effects of physio-logical increments in plasma ghrelin concentrations. Nutr Metab Cardiovasc Dis 15:410-417
33. Damjanovic SS, Lalic NM, Pesko PM, Petakov MS, Jotic A, Miljic D, Lalic KS, Lukic L, Djurovic M, Djukic VB 2006 Acute Effects of Ghrelin on Insulin Secretion and Glucose Disposal Rate in Gastrec-tomized Patients. J Clin Endocrinol Metab 91:2574-2581
34. Kageyama H, Funahashi H, Hirayama M, Takenoya F, Kita T, Kato S, Sakurai J, Lee EY, Inoue S, Date Y, Nakazato M, Kangawa K, Shioda S 2005 Morphological analysis of ghrelin and its recep-tor distribution in the rat pancreas. Regul Pept 126:67-71
35. Dezaki K, Sone H, Koizumi M, Nakata M, Kakei M, Nagai H, Hosoda H, Kangawa K, Yada T 2006 Blockade of pancreatic islet-derived ghrelin enhances insulin secretion to prevent high-fat diet-induced glucose intolerance. Diabetes 55:3486-3493
36. Sun Y, Asnicar M, Saha PK, Chan L, Smith RG 2006 Ablation of ghrelin improves the diabetic but not obese phenotype of ob/ob mice. Cell Metab 3:379-386
37. Pfluger PT, Kirchner H, Gunnel S, Schrott B, Perez-Tilve D, Fu S, Benoit SC, Horvath T, Joost HG, Wortley KE, Sleeman MW, Tschop MH 2007 Simultaneous deletion of ghrelin and its receptor increases motor activity and energy expenditure. Am J Physiol Gastrointest Liver Physiol
38. Di Vito L, Broglio F, Benso A, Gottero C, Prodam F, Papotti M, Muccioli G, Dieguez C, Casa-nueva FF, Deghenghi R, Ghigo E, Arvat E 2002 The GH-releasing effect of ghrelin, a natural GH se-cretagogue, is only blunted by the infusion of exogenous somatostatin in humans. Clin Endocrinol (Oxf) 56:643-648
39. Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau F, Creager MA, Dean-field J, Drexler H, Gerhard-Herman M, Herrington D, Vallance P, Vita J, Vogel R 2002 Guide-lines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. J Am Coll Cardiol 39:257-265
40. Vestergaard ET, Andersen NH, Hansen TK, Rasmussen LM, Moller N, Sorensen KE, Sloth E, Jorgensen JO 2007 Cardiovascular effects of intravenous ghrelin infusion in healthy young men. Am J Physiol Heart Circ Physiol00496
41. Loo JC, Riegelman S 1970 Assessment of pharmacokinetic constants from postinfusion blood curves obtained after I.V. infusion. J Pharm Sci 59:53-55
42. Rowland M & Tozer TN 1995 Clinical Pharmacokinetics: Concepts and Applications. Third Edition ed.; 313-335
43. STEELE R 1959 Influences of glucose loading and of injected insulin on hepatic glucose output. Ann N Y Acad Sci 82:420-430
44. DEBODO RC, STEELE R, ALTSZULER N, DUNN A, BISHOP JS 1963 ON THE HORMONAL REGULA-TION OF CARBOHYDRATE METABOLISM; STUDIES WITH C14 GLUCOSE. Recent Prog Horm Res 19:445-488
45. Ferrannini E 1988 The theoretical bases of indirect calorimetry: a review. Metabolism 37:287-301
46. Scheller D, Kolb J 1991 The internal reference technique in microdialysis: a practical approach to monitoring dialysis efficiency and to calculating tissue concentration from dialysate samples. J Neurosci Methods 40:31-38
47. Hagstrom-Toft E, Enoksson S, Moberg E, Bolinder J, Arner P 1997 Absolute concentrations of glycerol and lactate in human skeletal muscle, adipose tissue, and blood. Am J Physiol 273:E584-E592
48. Wojtaszewski JF, Hansen BF, Urso B, Richter EA 1996 Wortmannin inhibits both insulin- and con-traction-stimulated glucose uptake and transport in rat skeletal muscle. J Appl Physiol 81:1501-1509
48

Esben Thyssen Vestergaard Clinical aspects of ghrelin
49. Orskov H, Thomsen HG, Yde H 1968 Wick chromatography for rapid and reliable immunoassay of insulin, glucagon and growth hormone. Nature 219:193-195
50. Perseghin G, Caumo A, Caloni M, Testolin G, Luzi L 2001 Incorporation of the fasting plasma FFA concentration into QUICKI improves its association with insulin sensitivity in nonobese individuals. J Clin Endocrinol Metab 86:4776-4781
51. Hotta M, Ohwada R, Katakami H, Shibasaki T, Hizuka N, Takano K 2004 Plasma levels of intact and degraded ghrelin and their responses to glucose infusion in anorexia nervosa. J Clin Endocrinol Me-tab 89:5707-5712
52. Groschl M, Uhr M, Kraus T 2004 Evaluation of the comparability of commercial ghrelin assays. Clin Chem 50:457-458
53. Rauh M, Groschl M, Rascher W 2007 Simultaneous Quantification of Ghrelin and Desacyl-Ghrelin by Liquid Chromatography-Tandem Mass Spectrometry in Plasma, Serum, and Cell Supernatants. Clin Chem
54. Miljic D, Pekic S, Djurovic M, Doknic M, Milic N, Casanueva F, Ghatei M, Popovic V 2006 Ghre-lin has partial or no effect on appetite, growth hormone (GH), prolactin and cortisol release in patients with anorexia nervosa. J Clin Endocrinol Metab
55. Jorgensen JO, Jessen N, Pedersen SB, Vestergaard E, Gormsen L, Lund SA, Billestrup N 2006 Growth Hormone Receptor Signaling in Skeletal Muscle and Adipose Tissue in Human Subjects Following Exposure to an Intravenous GH Bolus. Am J Physiol Endocrinol Metab 291:E899-E905
56. Van Cauter E, Blackman JD, Roland D, Spire JP, Refetoff S, Polonsky KS 1991 Modulation of glucose regulation and insulin secretion by circadian rhythmicity and sleep. J Clin Invest 88:934-942
57. Yildiz BO, Suchard MA, Wong ML, McCann SM, Licinio J 2004 Alterations in the dynamics of circu-lating ghrelin, adiponectin, and leptin in human obesity. Proc Natl Acad Sci U S A
58. Murray CD, Martin NM, Patterson M, Taylor S, Ghatei MA, Kamm MA, Johnston C, Bloom SR, Emmanuel AV 2005 Ghrelin enhances gastric emptying in diabetic gastroparesis: a double-blind, pla-cebo-controlled, cross- over study. Gut
59. Hansen TK, Dall R, Hosoda H, Kojima M, Kangawa K, Christiansen JS, Jorgensen JO 2002 Weight loss increases circulating levels of ghrelin in human obesity. Clin Endocrinol (Oxf) 56:203-206
60. Cummings DE, Weigle DS, Frayo RS, Breen PA, Ma MK, Dellinger EP, Purnell JQ 2002 Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery. N Engl J Med 346:1623-1630
61. English PJ, Ghatei MA, Malik IA, Bloom SR, Wilding JP 2002 Food fails to suppress ghrelin levels in obese humans. J Clin Endocrinol Metab 87:2984
62. Marzullo P, Caumo A, Savia G, Verti B, Walker GE, Maestrini S, Tagliaferri A, Di Blasio AM, Liuzzi A 2006 Predictors of postabsorptive ghrelin secretion after intake of different macronutrients. J Clin Endocrinol Metab
63. le Roux C, Patterson M, Vincent R, Hunt C, Ghatei M, Bloom S 2004 Postprandial plasma ghrelin is suppressed proportional to meal calorie content in normal weight but not obese subjects. J Clin Endo-crinol Metab
64. Patterson M, Murphy KG, le Roux CW, Ghatei MA, Bloom SR 2005 CHARACTERISATION OF GHRELIN-LIKE IMMUNOREACTIVITY IN HUMAN PLASMA. J Clin Endocrinol Metab
65. Beaumont NJ, Skinner VO, Tan TM, Ramesh BS, Byrne DJ, MacColl GS, Keen JN, Bouloux PM, Mikhailidis DP, Bruckdorfer KR, Vanderpump MP, Srai KS 2003 Ghrelin can bind to a species of high density lipoprotein associated with paraoxonase. J Biol Chem 278:8877-8880
66. Schmid DA, Held K, Ising M, Uhr M, Weikel JC, Steiger A 2005 Ghrelin Stimulates Appetite, Imagination of Food, GH, ACTH, and Cortisol, but does not Affect Leptin in Normal Controls. Neuropsy-chopharmacology
49

Esben Thyssen Vestergaard Clinical aspects of ghrelin
67. Camina JP 2006 Cell biology of the ghrelin receptor. J Neuroendocrinol 18:65-76
68. De Smet B, Depoortere I, Moechars D, Swennen Q, Moreaux B, Cryns K, Tack J, Buyse J, Coulie B, Peeters TL 2006 Energy homeostasis and gastric emptying in ghrelin knockout mice. J Pharmacol Exp Ther 316:431-439
69. Enomoto M, Nagaya N, Uematsu M, Okumura H, Nakagawa E, Ono F, Hosoda H, Oya H, Ko-jima M, Kanmatsuse K, Kangawa K 2003 Cardiovascular and hormonal effects of subcutaneous ad-ministration of ghrelin, a novel growth hormone-releasing peptide, in healthy humans. Clin Sci (Lond) 105:431-435
70. Nagaya N, Miyatake K, Uematsu M, Oya H, Shimizu W, Hosoda H, Kojima M, Nakanishi N, Mori H, Kangawa K 2001 Hemodynamic, renal, and hormonal effects of ghrelin infusion in patients with chronic heart failure. J Clin Endocrinol Metab 86:5854-5859
71. Vestergaard ET, Hansen TK, Gormsen LC, Jakobsen P, Moller N, Christiansen JS, Jorgensen JO 2007 Constant intravenous ghrelin infusion in healthy young men: Clinical pharmacokinetics and metabolic effects. Am J Physiol Endocrinol Metab 292:E1829-E1836
72. Broglio F, Gottero C, Prodam F, Gauna C, Muccioli G, Papotti M, Abribat T, Van der Lely AJ, Ghigo E 2004 Non-acylated ghrelin counteracts the metabolic but not the neuroendocrine response to acylated ghrelin in humans. J Clin Endocrinol Metab 89:3062-3065
73. MacGorman LR, Rizza RA, Gerich JE 1981 Physiological concentrations of growth hormone exert insulin-like and insulin antagonistic effects on both hepatic and extrahepatic tissues in man. J Clin Endo-crinol Metab 53:556-559
74. Bratusch-Marrain PR, Smith D, DeFronzo RA 1982 The effect of growth hormone on glucose me-tabolism and insulin secretion in man. J Clin Endocrinol Metab 55:973-982
75. Fowelin J, Attvall S, von Schenck H, Smith U, Lager I 1991 Characterization of the insulin-antagonistic effect of growth hormone in man. Diabetologia 34:500-506
76. Hansen TK, Gravholt CH, Orskov H, Rasmussen MH, Christiansen JS, Jorgensen JO 2002 Dose dependency of the pharmacokinetics and acute lipolytic actions of growth hormone. J Clin Endocrinol Metab 87:4691-4698
77. Djurhuus CB, Gravholt CH, Nielsen S, Mengel A, Christiansen JS, Schmitz OE, Moller N 2002 Effects of cortisol on lipolysis and regional interstitial glycerol levels in humans. Am J Physiol Endocrinol Metab 283:E172-E177
78. Divertie GD, Jensen MD, Miles JM 1991 Stimulation of lipolysis in humans by physiological hypercor-tisolemia. Diabetes 40:1228-1232
79. Rooney DP, Neely RD, Cullen C, Ennis CN, Sheridan B, Atkinson AB, Trimble ER, Bell PM 1993 The effect of cortisol on glucose/glucose-6-phosphate cycle activity and insulin action. J Clin Endocrinol Metab 77:1180-1183
80. Nielsen MF, Caumo A, Chandramouli V, Schumann WC, Cobelli C, Landau BR, Vilstrup H, Rizza RA, Schmitz O 2004 Impaired basal glucose effectiveness but unaltered fasting glucose release and gluconeogenesis during short-term hypercortisolemia in healthy subjects. Am J Physiol Endocrinol Metab 286:E102-E110
81. Murata M, Okimura Y, Iida K, Matsumoto M, Sowa H, Kaji H, Kojima M, Kangawa K, Chihara K 2002 Ghrelin modulates the downstream molecules of insulin signaling in hepatoma cells. J Biol Chem 277:5667-5674
82. Kim MS, Yoon CY, Jang PG, Park YJ, Shin CS, Park HS, Ryu JW, Pak YK, Park JY, Lee KU, Kim SY, Lee HK, Kim YB, Park KS 2004 The mitogenic and antiapoptotic actions of ghrelin in 3T3-L1 adi-pocytes. Mol Endocrinol 18:2291-2301
50

Esben Thyssen Vestergaard Clinical aspects of ghrelin
83. Iantorno M, Chen H, Kim JA, Tesauro M, Lauro D, Cardillo C, Quon MJ 2006 Ghrelin has Novel Vascular Actions that Mimic Only PI 3-kinase-dependent Insulin-stimulated Production of Nitric Oxide (NO) but Not MAP-kinase-dependent Insulin-stimulated Secretion of ET-1 From Endothelial Cells. Am J Physiol Endocrinol Metab
84. Baldanzi G, Filigheddu N, Cutrupi S, Catapano F, Bonissoni S, Fubini A, Malan D, Baj G, Granata R, Broglio F, Papotti M, Surico N, Bussolino F, Isgaard J, Deghenghi R, Sinigaglia F, Prat M, Muccioli G, Ghigo E, Graziani A 2002 Ghrelin and des-acyl ghrelin inhibit cell death in car-diomyocytes and endothelial cells through ERK1/2 and PI 3-kinase/AKT. J Cell Biol 159:1029-1037
85. Granata R, Settanni F, Biancone L, Trovato L, Nano R, Bertuzzi F, Destefanis S, Annunziata M, Martinetti M, Catapano F, Ghe C, Isgaard J, Papotti M, Ghigo E, Muccioli G 2006 Acylated and unacylated ghrelin promote proliferation and inhibit apoptosis of pancreatic {beta} cells and human islets. Involvement of cAMP/PKA, ERK1/2 and PI3K/AKT signaling. Endocrinology 148:512-529
86. Zigman JM, Nakano Y, Coppari R, Balthasar N, Marcus JN, Lee CE, Jones JE, Deysher AE, Waxman AR, White RD, Williams TD, Lachey JL, Seeley RJ, Lowell BB, Elmquist JK 2005 Mice lacking ghrelin receptors resist the development of diet-induced obesity. J Clin Invest 115:3564-3572
87. Theander-Carrillo C, Wiedmer P, Cettour-Rose P, Nogueiras R, Perez-Tilve D, Pfluger P, Cas-taneda TR, Muzzin P, Schurmann A, Szanto I, Tschop MH, Rohner-Jeanrenaud F 2006 Ghrelin action in the brain controls adipocyte metabolism. J Clin Invest 116:1983-1993
88. Wortley KE, Del Rincon JP, Murray JD, Garcia K, Iida K, Thorner MO, Sleeman MW 2005 Ab-sence of ghrelin protects against early-onset obesity. J Clin Invest 115:3573-3578
89. Barazzoni R, Bosutti A, Stebel M, Cattin MR, Roder E, Visintin L, Cattin L, Biolo G, Zanetti M, Guarnieri G 2005 Ghrelin regulates mitochondrial-lipid metabolism gene expression and tissue fat dis-tribution in liver and skeletal muscle. Am J Physiol Endocrinol Metab 288:E228-E235
90. Cummings DE, Frayo RS, Marmonier C, Aubert R, Chapelot D 2004 Plasma ghrelin levels and hunger scores in humans initiating meals voluntarily without time- and food-related cues. Am J Physiol Endocrinol Metab 287:E297-E304
91. Avram AM, Jaffe CA, Symons KV, Barkan AL 2005 Endogenous circulating ghrelin does not mediate GH rhythmicity or response to fasting. J Clin Endocrinol Metab
92. Koutkia P, Canavan B, Breu J, Johnson ML, Grinspoon SK 2004 Nocturnal ghrelin pulsatility and response to growth hormone secretagogues in healthy men. Am J Physiol Endocrinol Metab 287:E506-E512
93. Muller AF, Lamberts SW, Janssen JA, Hofland LJ, Koetsveld PV, Bidlingmaier M, Strasburger CJ, Ghigo E, Van der Lely AJ 2002 Ghrelin drives GH secretion during fasting in man. Eur J Endocrinol 146:203-207
94. Sun Y, Butte NF, Garcia JM, Smith RG 2007 Characterization of adult ghrelin and ghrelin receptor knockout mice under positive and negative energy balance. Endocrinology
95. Wortley KE, Anderson KD, Garcia K, Murray JD, Malinova L, Liu R, Moncrieffe M, Thabet K, Cox HJ, Yancopoulos GD, Wiegand SJ, Sleeman MW 2004 Genetic deletion of ghrelin does not de-crease food intake but influences metabolic fuel preference. Proc Natl Acad Sci U S A 101:8227-8232
96. Natalucci G, Riedl S, Gleiss A, Zidek T, Frisch H 2005 Spontaneous 24-h ghrelin secretion pattern in fasting subjects: maintenance of a meal-related pattern. Eur J Endocrinol 152:845-850
97. Owen OE, Morgan AP, Kemp HG, Sullivan JM, Herrera MG, Cahill GF, Jr. 1967 Brain metabolism during fasting. J Clin Invest 46:1589-1595
98. Muccioli G, Tschop M, Papotti M, Deghenghi R, Heiman M, Ghigo E 2002 Neuroendocrine and peripheral activities of ghrelin: implications in metabolism and obesity. Eur J Pharmacol 440:235-254
51

Esben Thyssen Vestergaard Clinical aspects of ghrelin
99. Lindeman JH, Pijl H, Van Dielen FM, Lentjes EG, Van Leuven C, Kooistra T 2002 Ghrelin and the hyposomatotropism of obesity. Obes Res 10:1161-1166
100. Zadik Z, Chalew SA, McCarter RJ, Jr., Meistas M, Kowarski AA 1985 The influence of age on the 24-hour integrated concentration of growth hormone in normal individuals. J Clin Endocrinol Metab 60:513-516
101. Nagaya N, Uematsu M, Kojima M, Date Y, Nakazato M, Okumura H, Hosoda H, Shimizu W, Yamagishi M, Oya H, Koh H, Yutani C, Kangawa K 2001 Elevated circulating level of ghrelin in cachexia associated with chronic heart failure: relationships between ghrelin and anabolic/catabolic fac-tors. Circulation 104:2034-2038
102. Shiiya T, Nakazato M, Mizuta M, Date Y, Mondal MS, Tanaka M, Nozoe S, Hosoda H, Kan-gawa K, Matsukura S 2002 Plasma ghrelin levels in lean and obese humans and the effect of glucose on ghrelin secretion. J Clin Endocrinol Metab 87:240-244
103. Nagaya N, Moriya J, Yasumura Y, Uematsu M, Ono F, Shimizu W, Ueno K, Kitakaze M, Mi-yatake K, Kangawa K 2004 Effects of Ghrelin Administration on Left Ventricular Function, Exercise Capacity, and Muscle Wasting in Patients With Chronic Heart Failure. Circulation
104. Nagaya N, Itoh T, Murakami S, Oya H, Uematsu M, Miyatake K, Kangawa K 2005 Treatment of Cachexia With Ghrelin in Patients With COPD. Chest 128:1187-1193
105. Maghnie M, Pennati MC, Civardi E, Di Iorgi N, Aimaretti G, Foschini ML, Corneli G, Tinelli C, Ghigo E, Lorini R, Loche S 2007 GH response to ghrelin in subjects with congenital GH deficiency: evidence that ghrelin action requires hypothalamic-pituitary connections. Eur J Endocrinol 156:449-454
106. Svensson J, Monson JP, Vetter T, Hansen TK, Savine R, Kann P, Bex M, Reincke M, Hagen C, Beckers A, Ilondo MM, Zdravkovic M, Bengtsson BA, Korbonits M 2003 Oral administration of the growth hormone secretagogue NN703 in adult patients with growth hormone deficiency. Clin Endo-crinol (Oxf) 58:572-580
107. Codner E, Cassorla F, Tiulpakov AN, Mericq MV, Avila A, Pescovitz OH, Svensson J, Cerchio K, Krupa D, Gertz BJ, Murphy G 2001 Effects of oral administration of ibutamoren mesylate, a nonpep-tide growth hormone secretagogue, on the growth hormone-insulin-like growth factor I axis in growth hormone-deficient children. Clin Pharmacol Ther 70:91-98
108. Chapman IM, Pescovitz OH, Murphy G, Treep T, Cerchio KA, Krupa D, Gertz B, Polvino WJ, Skiles EH, Pezzoli SS, Thorner MO 1997 Oral administration of growth hormone (GH) releasing pep-tide-mimetic MK-677 stimulates the GH/insulin-like growth factor-I axis in selected GH-deficient adults. J Clin Endocrinol Metab 82:3455-3463
109. Janssen JA, van der Toorn FM, Hofland LJ, Van Koetsveld P, Broglio F, Ghigo E, Lamberts SW, Jan vdL 2001 Systemic ghrelin levels in subjects with growth hormone deficiency are not modified by one year of growth hormone replacement therapy. Eur J Endocrinol 145:711-716
110. Malik IA, English PJ, Ghatei MA, Bloom SR, MacFarlane IA, Wilding JP 2004 The relationship of ghrelin to biochemical and anthropometric markers of adult growth hormone deficiency. Clin Endocrinol (Oxf) 60:137-141
111. Consensus guidelines for the diagnosis and treatment of adults with growth hormone deficiency: sum-mary statement of the Growth Hormone Research Society Workshop on Adult Growth Hormone Defi-ciency 1998 J Clin Endocrinol Metab 83:379-381
112. Muccioli G, Ghe C, Ghigo MC, Papotti M, Arvat E, Boghen MF, Nilsson MH, Deghenghi R, Ong H, Ghigo E 1998 Specific receptors for synthetic GH secretagogues in the human brain and pituitary gland. J Endocrinol 157:99-106
113. Cheng K, Chan WW, Barreto A, Jr., Convey EM, Smith RG 1989 The synergistic effects of His-D-Trp-Ala-Trp-D-Phe-Lys-NH2 on growth hormone (GH)-releasing factor-stimulated GH release and intra-cellular adenosine 3',5'-monophosphate accumulation in rat primary pituitary cell culture. Endocrinology 124:2791-2798
52

Esben Thyssen Vestergaard Clinical aspects of ghrelin
114. Popovic V, Pekic S, Micic D, Damjanovic S, Marikovic J, Simic M, Dieguez C, Casanueva FF 2004 Evaluation of the reproducibility of the GHRH plus GHRP-6 test of growth hormone reserve in adults. Clin Endocrinol (Oxf) 60:185-191
115. Popovic V, Leal A, Micic D, Koppeschaar HP, Torres E, Paramo C, Obradovic S, Dieguez C, Casanueva FF 2000 GH-releasing hormone and GH-releasing peptide-6 for diagnostic testing in GH-deficient adults. Lancet 356:1137-1142
116. Andersen M, Hansen TB, Stoving RK, Bertelsen J, Hangaard J, Hyltoft Petersen P, Hagen C 1996 The pyridostigmine-growth-hormone-releasing-hormone test in adults. The reference interval and a comparison with the insulin tolerance test. ENDOCRINOL METAB 3:197-206
117. Dezaki K, Hosoda H, Kakei M, Hashiguchi S, Watanabe M, Kangawa K, Yada T 2004 Endoge-nous Ghrelin in Pancreatic Islets Restricts Insulin Release by Attenuating Ca2+ Signaling in {beta}-Cells: Implication in the Glycemic Control in Rodents. Diabetes 53:3142-3151
118. Egido EM, Rodriguez-Gallardo J, Silvestre RA, Marco J 2002 Inhibitory effect of ghrelin on insulin and pancreatic somatostatin secretion. Eur J Endocrinol 146:241-244
119. Esler WP, Rudolph J, Claus TH, Tang W, Barucci N, Brown SE, Bullock W, Daly M, Decarr L, Li Y, Milardo L, Molstad D, Zhu J, Gardell SJ, Livingston JN, Sweet LJ 2007 Small-molecule ghrelin receptor antagonists improve glucose tolerance, suppress appetite, and promote weight loss. Endocri-nology
53
