
KULIT Induksi Nekrosis Sel Lemak Dalam Jaringan Lemak Manusia Setelah
Upload
nguyenkhanhCategory
view
228download
0
Pharmacotherapy
PSORIASIS
Yani Mulyani, M.Si, apt
Yani Mulyani - STFB

Komponen
Definisi
Pathofisiology
Clinical Presentation
Diagnosis
Desired outcome
Treatment
Evaluation of theurapeutic outcomes
Yani Mulyani - STFB

Definisi
• Jenis penyakit gangguan imun, yang mempengaruhi tampilan pada kulit
• Penyakit tidak menular ini ditandai oleh lesi peradangan yang ditutupi dengan keropeng putih perak dari kulit mati.
• Psoriasis disebabkan sel-sel kulit menua dalam waktu kurang dari seminggu.
• Karena tubuh tidak dapat melepaskan kulit tua secepat sel-sel baru meningkat ke permukaan, pengelupasan kulit mati menimbulkan keropeng yang berkembang di lengan, punggung, dada, siku, kaki, kuku, lipatan antara pantat, dan kulit kepala.
Yani Mulyani - STFB
Tingkatan Psoriasis
• Mild/Ringan, jika mempengaruhi kurang dari 5% dari permukaan tubuh,
• Sedang/moderat, jika 5-30% dari kulit yang terlibat, dan
• Parah/severe , jika penyakit memengaruhi lebih dari 30% dari permukaan tubuh.
Yani Mulyani - STFB

What is the genetic risk of psoriasis?
• 41% if both parents have psoriasis 14% if one parent 4% if no genetic link
Yani Mulyani - STFB
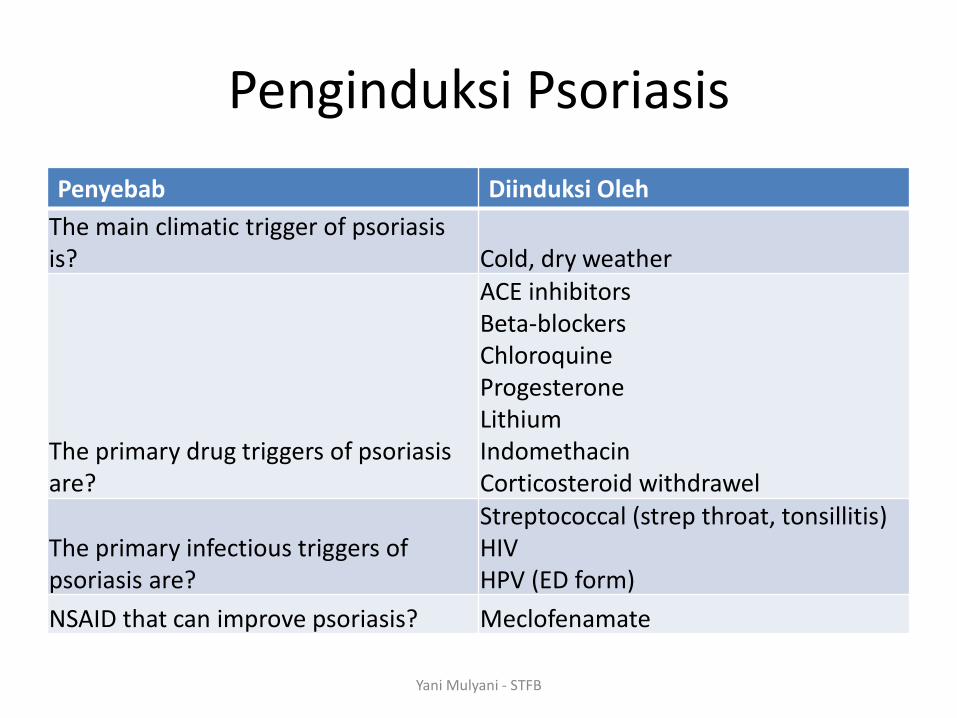
Penginduksi Psoriasis
Penyebab Diinduksi Oleh
The main climatic trigger of psoriasis is? Cold, dry weather
The primary drug triggers of psoriasis are?
ACE inhibitors Beta-blockers Chloroquine Progesterone Lithium Indomethacin Corticosteroid withdrawel
The primary infectious triggers of psoriasis are?
Streptococcal (strep throat, tonsillitis) HIV HPV (ED form)
NSAID that can improve psoriasis? Meclofenamate
Yani Mulyani - STFB

ICAM, Intracellurar ce;; adhesion molecules APCs, Antigen Presenting Cell
LFA, Leucocyte function associated type 3 Yani Mulyani - STFB

Phatofisiology
T Cell, diproduksi banyak
T cell diikat kuat oleh ICAM pada sel endhotel
Merangsang Pelepasan Antigen APC, Aktivated T CELL
Kehadiran LFA-3-CD2, Meningkat Proliferation T Cell . Saat Aktivasi T Cell, Meningkat Interleukin, Cytokines, dll,..yang menginisiasi Inflamasi di KULIT
PSORIASIS
Yani Mulyani - STFB
In which layer of the skin does psoriasis begin?
In the basal layer of the epidermis where keratinocytes form.
Yani Mulyani - STFB
Clinical Presentation
Yani Mulyani - STFB

Yani Mulyani - STFB

Yani Mulyani - STFB
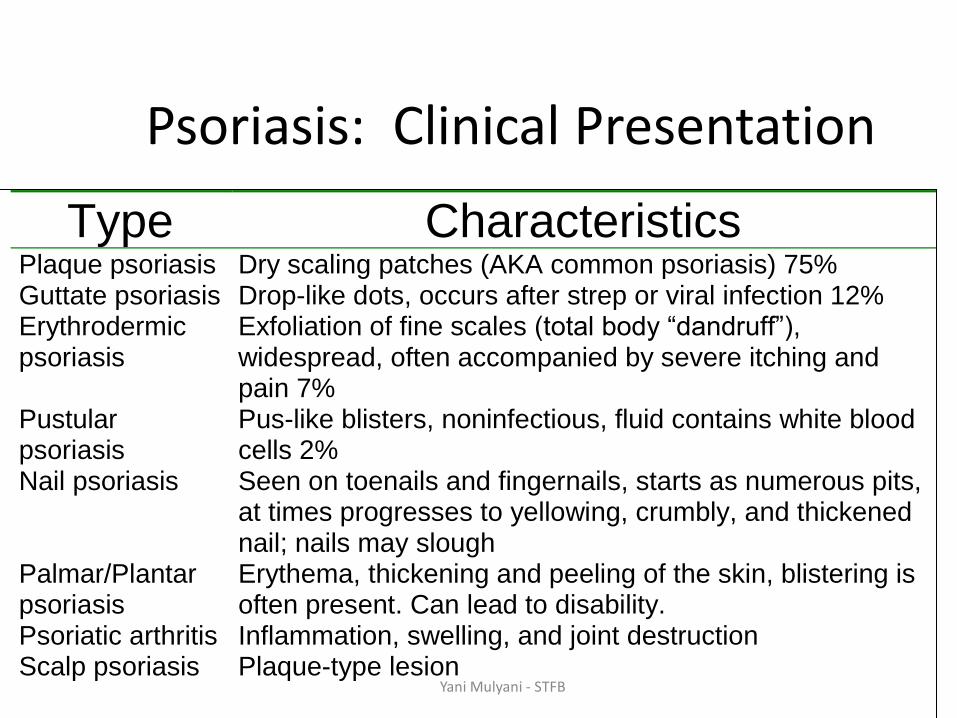
Psoriasis: Clinical Presentation
Type Characteristics Plaque psoriasis Guttate psoriasis Erythrodermic psoriasis Pustular psoriasis Nail psoriasis Palmar/Plantar psoriasis Psoriatic arthritis Scalp psoriasis
Dry scaling patches (AKA common psoriasis) 75% Drop-like dots, occurs after strep or viral infection 12% Exfoliation of fine scales (total body “dandruff”), widespread, often accompanied by severe itching and pain 7% Pus-like blisters, noninfectious, fluid contains white blood cells 2% Seen on toenails and fingernails, starts as numerous pits, at times progresses to yellowing, crumbly, and thickened nail; nails may slough Erythema, thickening and peeling of the skin, blistering is often present. Can lead to disability. Inflammation, swelling, and joint destruction Plaque-type lesion
Yani Mulyani - STFB

Psoriatic Plaque
Yani Mulyani - STFB

Chronic Plaque Psoriasis
Yani Mulyani - STFB

Erythrodermic Psoriasis
Yani Mulyani - STFB

Nail changes
Yani Mulyani - STFB

Guttate Psoriasis
Yani Mulyani - STFB

Nail Changes
• In 78% of psoriatic patients
• Fingernails>Toenails
• Four changes
1. Onycholysis (= separation from nail bed)
2. Pitting*
3. Subungual debris accumulation
4. Color alterations
*Pitting rules out a fungal infection Yani Mulyani - STFB

DIAGNOSIS
Physical examination
BSA (body surface Area)
Psoriasis Area and Severity Index
Yani Mulyani - STFB

OLA Photonumeric Guidelines (overall lesion assessment)
0 = none
5 = very severe 4 = severe 3 = moderate
1 = minimal 2 = mild
Yani Mulyani - STFB

Desired Outcome
Caranya???
• Mencegah Aktivasi T Cell
• Menghambat Kerja dari Inflammatory agent
• Menurunkan Imun
• Mengurangi pembentukan Keratin
• Membuang Keratin yangg terbentuk
Outcome
Yani Mulyani - STFB
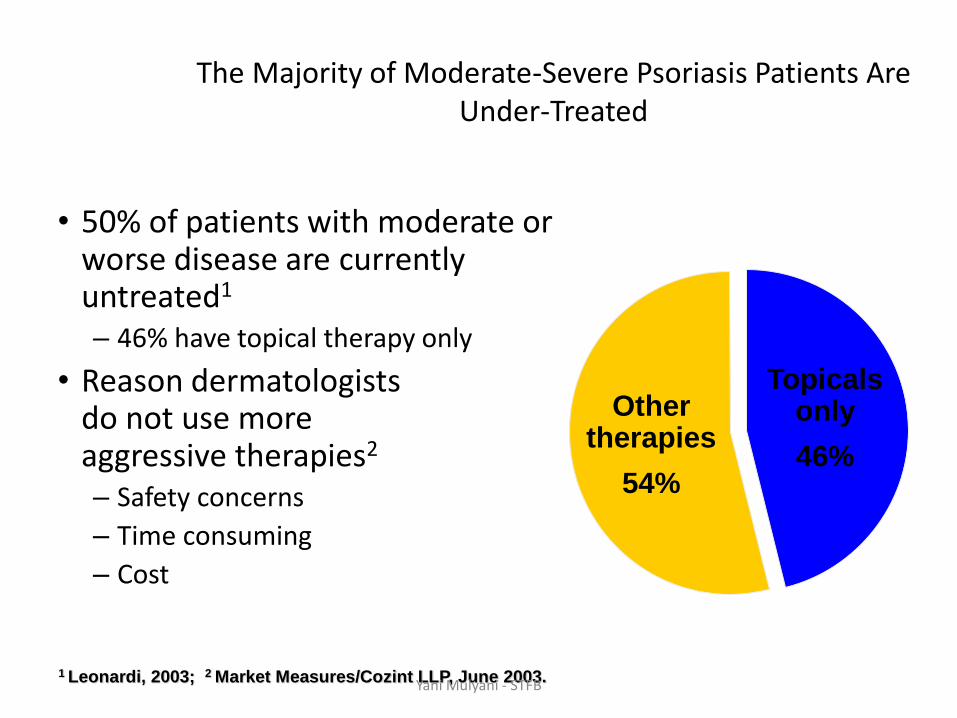
1 Leonardi, 2003; 2 Market Measures/Cozint LLP, June 2003.
Other therapies
54%
Topicals only
46%
The Majority of Moderate-Severe Psoriasis Patients Are Under-Treated
• 50% of patients with moderate or worse disease are currently untreated1
– 46% have topical therapy only
• Reason dermatologists do not use more aggressive therapies2
– Safety concerns
– Time consuming
– Cost
Yani Mulyani - STFB

Psoriasis: Treatment
• Lubrication
• Removal of scales
• Slow down lesion proliferation
• Pruritus management
• Prevent complications
• Lessen patient stress
• Season and climate
Yani Mulyani - STFB

Treatment
Non Pharmacology
Pharmacology Treatment
Yani Mulyani - STFB

Non Pharmacology
• Mengurangi stress
• Memberikan Pelembab
• Menggunakan Jenis sabun khusus
• Sunscreen
Yani Mulyani - STFB

Pharmacology Treatment
Korticosteroid
Keratolytic
Keratonycte proliferation inhibitor
Phototherapy (UV a dan UV B)
Photochemotherapy (Broadband UV B)
Systemic Therapies
BRM (biologic response modifiers)
Yani Mulyani - STFB

Algorithm Treatment Of Psoriasis Mild to Moderate
Yani Mulyani - STFB
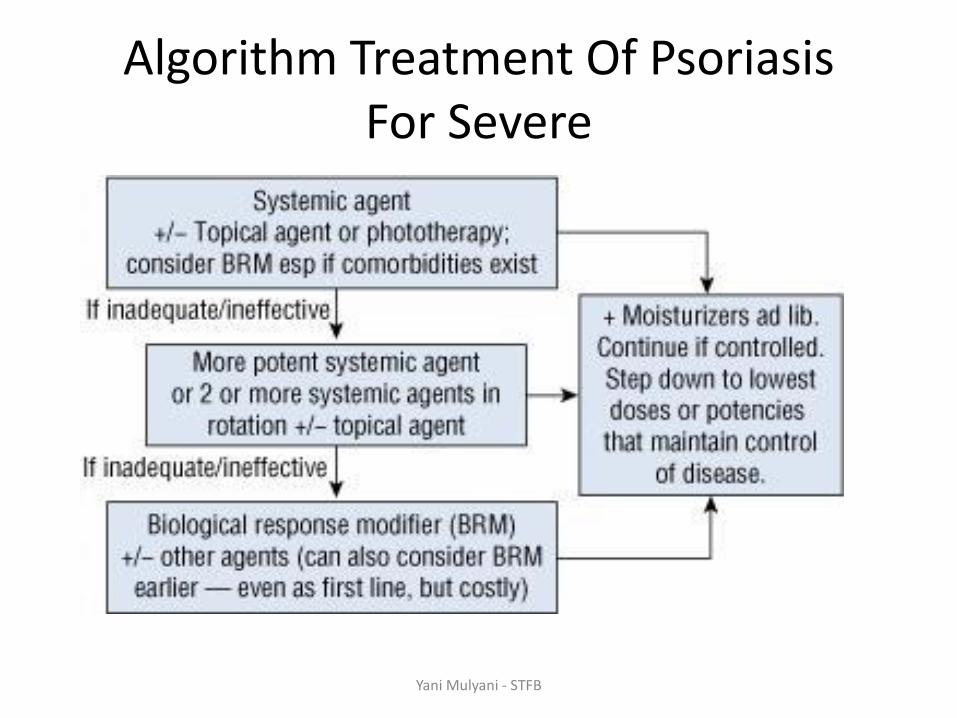
Algorithm Treatment Of Psoriasis For Severe
Yani Mulyani - STFB

Step 1
Anthralin Calcipotriene
Coal Tar
Tazarotene Intralesional Steroid
Topical Steroid
Climatotherapy Moisturizers Keratolytics
Step 2
PUVA PUVA +Step 1 agent
Acitretin
Step 3
Methotrexate Cyclosporine
Rotational:12-24 months
of eachstep 3 agent
Supplementary
Tx
Step 4
Enbrel/Remicade/Amevive/Raptiva
Yani Mulyani - STFB

Corticosteroid
Betamethasone
Amcinonide
Triamcinolone
Fluticasone,
Dll
Yani Mulyani - STFB

Corticosteroids
Level of Potency Corticosteroid Commercial Products
Ultra-high Halobetasol propionate
Clobetasol propionate
Betamethasone dipropionate
Diflorasone diacetate
Ultravate crm/oint
Temovate crm/oint
Diprolene oint
Psorcon oint
High Halcinonide
Amcinonide
Betamethasone dipropionate
Mometasone furoate
Diflorasone diacetate
Fluocinonide
Desoximetasone
Halog crm
Cylocort oint
Diprolene AF crm
Elocon oint
Florone oint
Lidex crm,gel,oint
Topicort crm,oint,gel
Mild to high Halcinonide
Triamcinolone acetonide
Betamethasone dipropionate
Fluocinonide
Halog oint,crm,soln
Aristocort A oint
Diprosone crm
Lidex-E crm Yani Mulyani - STFB

Corticosteroids
Level of Potency Corticosteroid Commercial Products
Mild Hydrocortisone valerate
Triamcinolone acetonide
Flurandrenolide
Mometasone furoate
Fluocinolone acetonide
Westcort
Kenalog crm and oint
Cordran oint
Elocon crm
Synalar oint
Low to mild Hydrocortisone valerate
Triamcinolone acetonide
Flurandrenolide
Betamethasone dipropionate
Hydrocortisone butyrate
Flucolone acetonide
Westcort crm
Kenalog crm and oint
Cordran crm
Diprosone lotion
Locoid crm
Synalar crm
Low Alclometasone dipropionate
Betamethasone valerate
Fluocinolone acetonide
Hydrocortisone, dexamethasone,
prednisolone, methylprednisolone
Aclovate crm and oint
Valisone lotion
Synalar soln and crm
Yani Mulyani - STFB

Inhibitor keratinocyte
Calcipotriene
Tazarotene
Anthralin
Coal tar
Asam salisilat
Yani Mulyani - STFB

Phototherapy
Yani Mulyani - STFB

BRM
Adalimumab
Etanercept
Infliximab
Alefacept
Ustekinumab
Yani Mulyani - STFB

(soluble TNF receptor) Yani Mulyani - STFB


















