PERSPECTIVES IN CLINICAL GASTROENTEROLOGY AND … · Immunohistochemistry Expression of serum...
10
PERSPECTIVES IN CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Management of Hepatocellular Adenoma: Recent Advances Shefali Agrawal, * Sheela Agarwal, ‡ Thomas Arnason, § Sanjay Saini, ‡ and Jacques Belghiti k *Hepatobiliary and Pancreatic Surgery, Department of Surgical Oncology, Indraprastha Apollo Hospitals, New Delhi, India; ‡ Division of Abdominal Imaging and Intervention, Department of Radiology, and § Department of Pathology, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts; and k Department of Hepatobiliary and Transplant Surgery, Beaujon Hospital, University of Paris, Clichy, France Hepatocellular adenoma (HCA) is a rare benign liver cell neoplasm that occurs more frequently in young women with a history of prolonged use of oral contraceptives. Surgical resection is considered because of the risk of hemorrhage in 25% and of malignant transformation in 5% of patients with HCA. HCA is a heterogeneous disease comprising 3 subtypes with distinct molecular and complication profiles. The in- flammatory or telangiectatic subtype is at increased risk for hemorrhage, the b-catenin–activated subtype is at increased risk for malignant transformation, and the hepatocyte nu- clear factor-1a–inactivated or steatotic subtype is at the least risk for complications. One-third of the patients with HCA have multiple tumors on imaging with no increased risk of complications. Magnetic resonance imaging is the modality of choice for the diagnosis and subtype characterization of HCA. Systematic resection of HCA is recommended in male patients owing to the higher incidence of malignant transformation, and surgical excision in women should be reserved for tu- mors 5 cm or larger associated with an increased risk of complications. Cessation of hormonal therapy and radiologic surveillance in women with HCA tumors smaller than 5 cm shows that the vast majority of HCA remain stable or undergo spontaneous regression. Percutaneous core needle biopsy is of limited value because the therapeutic strategy is based primarily on patient sex and tumor size. Transarterial embolization is the initial treatment for HCA complicated by hemorrhage. Pregnancy should not be discouraged in the presence of HCA, however, frequent sonographic surveillance is recommended. Keywords: Hepatocellular Adenoma; Malignant Transformation; Hemorrhage; Liver Resection; Conservative Management; Pregnancy. H epatocellular adenoma (HCA) is a rare benign liver neoplasm that occurs predominantly in young women with a history of prolonged use of oral contraceptives (OCs). 1,2 Systematic resection of HCA traditionally has been recommended owing to the risks of hemorrhage and malignant transformation, however, greater knowledge of risk factors associated with these complications such as patient sex and size and subtype of the tumor have improved patient selection for less-invasive treatment. 3–14 This article reviews recent advances in etiology, radiologic diagnosis, subtype characterization, and indications for invasive treatment with the objective of identification of the optimal thera- peutic strategy based on individual considerations. Pathogenesis Although identification of genetic mutations has pro- vided novel insight into the pathogenesis of HCA, hormonal therapy remains the dominant predisposing factor in the development of HCA. 2,10,15–17 In women using OCs, there is a dose-dependent association between estrogen and the development of HCA, and the incidence of HCA has decreased with the use of modern OCs containing lower doses of estrogen. 18,19 The use of anabolic androgenic ste- roids for aplastic or Fanconi’s anemia, hereditary angioe- dema, and athletic performance enhancement is a risk factor for the development of HCA and potentially the imbalance in endogenous sex hormones in Klinefelter’s and polycystic ovarian syndromes. 20–25 Other drugs implicated in its development include barbiturates, clomiphene, and recombinant human growth hormone. 26–28 Genetic syndromes including familial adenomatous polyposis and glycogen storage diseases (GSDs) are asso- ciated with HCA tumors, which occur in 75% of patients with GSD type Ia, and more than half of the patients have multiple tumors. 22,29–31 Other underlying metabolic dis- eases include maturity-onset diabetes of the young type 3 and McCune–Albright syndrome. 15 In patients without an identifiable etiology for HCA, an association with envi- ronmental factors such as obesity and alcohol consump- tion has been reported, with multiple tumors being frequent in the presence of hepatic steatosis. 11,15,32–36 In a review of 27 patients with inflammatory HCA, 61% were overweight, of whom more than half were obese. 35 In an Abbreviations used in this paper: CT, computed tomography; FNH, focal nodular hyperplasia; GSD, glycogen storage disease; HCA, hepatocellular adenoma; HCC, hepatocellular carcinoma; HNF, hepatocyte nuclear fac- tor; MRI, magnetic resonance imaging; OC, oral contraceptive; TAE, transarterial embolization. © 2015 by the AGA Institute 1542-3565/$36.00 http://dx.doi.org/10.1016/j.cgh.2014.05.023 Clinical Gastroenterology and Hepatology 2015;13:1221–1230
Transcript of PERSPECTIVES IN CLINICAL GASTROENTEROLOGY AND … · Immunohistochemistry Expression of serum...

Clinical Gastroenterology and Hepatology 2015;13:1221–1230
PERSPECTIVES IN CLINICAL GASTROENTEROLOGY ANDHEPATOLOGY
Management of Hepatocellular Adenoma: Recent Advances
Shefali Agrawal,* Sheela Agarwal,‡ Thomas Arnason,§ Sanjay Saini,‡ and Jacques Belghitik
*Hepatobiliary and Pancreatic Surgery, Department of Surgical Oncology, Indraprastha Apollo Hospitals, New Delhi, India;‡Division of Abdominal Imaging and Intervention, Department of Radiology, and §Department of Pathology, MassachusettsGeneral Hospital and Harvard Medical School, Boston, Massachusetts; and kDepartment of Hepatobiliary and TransplantSurgery, Beaujon Hospital, University of Paris, Clichy, France
Abbreviations used in this paper: CT, computed tomography; FNH, focalnodular hyperplasia; GSD, glycogen storage disease; HCA, hepatocellularadenoma; HCC, hepatocellular carcinoma; HNF, hepatocyte nuclear fac-tor; MRI, magnetic resonance imaging; OC, oral contraceptive; TAE,transarterial embolization.
© 2015 by the AGA Institute1542-3565/$36.00
http://dx.doi.org/10.1016/j.cgh.2014.05.023
Hepatocellular adenoma (HCA) is a rare benign liver cellneoplasmthatoccursmore frequently inyoungwomenwithahistory of prolonged use of oral contraceptives. Surgicalresection is considered because of the risk of hemorrhage in25% and of malignant transformation in 5% of patients withHCA. HCA is a heterogeneous disease comprising 3 subtypeswith distinct molecular and complication profiles. The in-flammatory or telangiectatic subtype is at increased risk forhemorrhage, the b-catenin–activated subtype is at increasedrisk for malignant transformation, and the hepatocyte nu-clear factor-1a–inactivated or steatotic subtype is at the leastrisk for complications. One-third of the patients with HCAhave multiple tumors on imaging with no increased risk ofcomplications.Magnetic resonance imaging is themodality ofchoice for the diagnosis and subtype characterization ofHCA.Systematic resectionofHCA is recommended inmalepatientsowing to the higher incidence of malignant transformation,and surgical excision in women should be reserved for tu-mors 5 cm or larger associated with an increased risk ofcomplications. Cessation of hormonal therapy and radiologicsurveillance in women with HCA tumors smaller than 5 cmshows that the vastmajority ofHCA remain stable or undergospontaneous regression. Percutaneous core needle biopsy isof limited value because the therapeutic strategy is basedprimarily on patient sex and tumor size. Transarterialembolization is the initial treatment for HCA complicated byhemorrhage. Pregnancy should not be discouraged in thepresence ofHCA, however, frequent sonographic surveillanceis recommended.
Keywords: Hepatocellular Adenoma; Malignant Transformation;Hemorrhage; Liver Resection; Conservative Management;Pregnancy.
Hepatocellular adenoma (HCA) is a rare benignliver neoplasm that occurs predominantly in
young women with a history of prolonged use of oralcontraceptives (OCs).1,2 Systematic resection of HCAtraditionally has been recommended owing to the risksof hemorrhage and malignant transformation, however,greater knowledge of risk factors associated with thesecomplications such as patient sex and size and subtypeof the tumor have improved patient selection forless-invasive treatment.3–14 This article reviews recentadvances in etiology, radiologic diagnosis, subtype
characterization, and indications for invasive treatmentwith the objective of identification of the optimal thera-peutic strategy based on individual considerations.
Pathogenesis
Although identification of genetic mutations has pro-vided novel insight into the pathogenesis of HCA, hormonaltherapy remains the dominant predisposing factor in thedevelopment of HCA.2,10,15–17 In women using OCs, there isa dose-dependent association between estrogen and thedevelopment of HCA, and the incidence of HCA hasdecreased with the use of modern OCs containing lowerdoses of estrogen.18,19 The use of anabolic androgenic ste-roids for aplastic or Fanconi’s anemia, hereditary angioe-dema, and athletic performance enhancement is a riskfactor for the development of HCA and potentially theimbalance in endogenous sex hormones in Klinefelter’s andpolycystic ovarian syndromes.20–25 Other drugs implicatedin its development include barbiturates, clomiphene, andrecombinant human growth hormone.26–28
Genetic syndromes including familial adenomatouspolyposis and glycogen storage diseases (GSDs) are asso-ciated with HCA tumors, which occur in 75% of patientswith GSD type Ia, and more than half of the patients havemultiple tumors.22,29–31 Other underlying metabolic dis-eases include maturity-onset diabetes of the young type 3and McCune–Albright syndrome.15 In patients without anidentifiable etiology for HCA, an association with envi-ronmental factors such as obesity and alcohol consump-tion has been reported, with multiple tumors beingfrequent in the presence of hepatic steatosis.11,15,32–36 In areview of 27 patients with inflammatory HCA, 61% wereoverweight, of whom more than half were obese.35 In an

1222 Agrawal et al Clinical Gastroenterology and Hepatology Vol. 13, No. 7
evolving epidemiologic environment for the developmentof HCA, obesity and metabolic syndrome are emerging asimportant risk factors with a diminishing impact of OCs.Abnormalities of the hepatic vasculature including theabsence or occlusion of the portal vein and intrahepaticportosystemic venous shunt also are considered predis-posing factors in the pathogenesis of HCA.37–39
Pathology
HCAs usually are solitary, well-delineated, and, oc-casionally, pedunculated tumors with parenchyma
Table 1.Genotype–Phenotype Classification of HCA
Inflammatory HCA
Epidemiology 40%–55% of HCAsPredominantly seen in womenAssociated with a high BMI, alcohol
consumption, and systemicinflammatory syndrome
Pathology Marked polymorphous inflammatoryinfiltrates, ductular reaction,sinusoidal dilatation/peliosis,hemorrhage, and thick tortuousarteries
Immunohistochemistry Expression of serum amyloid A andC-reactive protein
MRIT1-weighted Isointense or mildly hyperintense,
without signal loss on chemicalshift sequence
Diffusely hyperintenseIntense arterial enhancement
persisting into the portal venousand delayed phases
T2-weighted Isointense or mildly hyperintense,without signal loss on chemicalshift sequence
Diffusely hyperintenseIntense arterial enhancement
persisting into the portal venousand delayed phases
Gadolinium-enhancedT1-weighted
Isointense or mildly hyperintense,without signal loss on chemicalshift sequence
Diffusely hyperintenseIntense arterial enhancement
persisting into the portal venousand delayed phases
Complications Highest risk of hemorrhage
BMI, body mass index; MODY, maturity-onset diabetes of the young.
composed of plates of hepatocytes separated by sinu-soids without portal tract elements or bile ductules, akey feature in the histologic distinction of HCA from focalnodular hyperplasia (FNH).40 Inflammatory HCA is anexception because it shows ductular structures unlikeother HCA subtypes, which previously led to its classifi-cation as telangiectatic FNH.41 HCA may be complicatedby necrosis or hemorrhage because the thin-walled si-nusoids are supplied by the high-pressure arterial sys-tem and the absence of a capsule with prominentsubcapsular vessels predisposes to tumor rupture andfree intraperitoneal hemorrhage. Distinguishing HCAfrom a well-differentiated hepatocellular carcinoma
HCA with HNF-1a mutationHCA with b-catenin
activation
35%–50% of HCAsAlmost exclusively in womenPresence of germline HNF-1a
mutation is associated withMODY type 3 and familialhepatic adenomatosis
10%–15% of HCAsMore frequent in menAssociated with use of
androgens, GSDs, andfamilial adenomatosispolyposis
Diffuse intratumoral steatosis Cytologic and nuclearabnormalities that aredifficult to distinguish fromwell-differentiated HCC
Lack of liver fatty acid–bindingprotein expression
Nuclear b-catenin staining andstrong diffuse glutaminesynthetase expression
Hyperintense or isointense withdiffuse signal loss onchemical shift sequence dueto intratumoral fat
Isointense or slightlyhyperintense
Moderate arterial enhancementnot persisting into the portalvenous phase
No specific featuresMay mimic HCC with strong
arterial enhancement andportal venous washout
Hyperintense or isointense withdiffuse signal loss onchemical shift sequence dueto intratumoral fat
Isointense or slightlyhyperintense
Moderate arterial enhancementnot persisting into the portalvenous phase
No specific featuresMay mimic HCC with strong
arterial enhancement andportal venous washout
Hyperintense or isointense withdiffuse signal loss onchemical shift sequence dueto intratumoral fat
Isointense or slightlyhyperintense
Moderate arterial enhancementnot persisting into the portalvenous phase
No specific featuresMay mimic HCC with strong
arterial enhancement andportal venous washout
Least aggressive subtype withminimal risk of complicationsin tumors <5 cm
Highest risk of malignancy

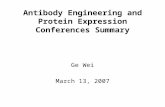
Figure 1. Pathologic sub-types of HCA. (A) HNF-1a–inactivated HCA withdiffuse steatosis (H&E). (B)Complete lack of liver fattyacid–binding protein ex-pression in HNF-1a–inactivated HCA in contrastto normal expression byhepatocytes of the non-tumoral liver (NTL). (C)Inflammatory HCA withsinusoidal dilatation,thick-walled arteries, andinflammation (H&E). (D)Diffuse overexpression ofC-reactive protein by he-patocytes (inset) of inflam-matory HCA with sharpdemarcation from the NTL.(E) Strong and diffuseexpression of glutaminesynthetase in b-catenin–activated HCA contrastingwith its normal expressionin pericentrolobular hepa-tocytes in NTL. (F) Aberrantnuclear and cytoplasmicexpression of b-catenin(arrow) in a b-catenin–activated HCA in contrastto the normal membranouspattern. Photographs cour-tesy of Professor PauletteBioulac-Sage, Departmentof Pathology, Hospital Pel-legrin, Bordeaux, France.
July 2015 Management of Hepatocellular Adenoma 1223
(HCC) may be difficult in some cases and the loss ofnormal reticulin stain in HCA may suggest a HCC.10,42
Malignant transformation of HCA is based on thedemonstration of a transition zone with dysplasticchanges within HCC or a pattern of a nodule within anodule or 2 adjacent tumors without a transitionzone.11,43
Genotype–Phenotype Classification
Identification of genetic heterogeneity in HCA tumorswas the basis of the molecular classification,44–47 withdistinct epidemiologic and clinical features of each sub-type. HCA tumors were classified into 3 subtypes,namely, inflammatory, hepatocyte nuclear factor (HNF)-1a–inactivated, and b-catenin–activated based on spe-cific genetic mutations. Approximately 10% of HCAsremain poorly characterized with no identifiable clinicalor molecular markers and are designated as unclassi-fied.3 The clinicopathologic and immunohistochemical
characteristics of each subtype are shown in Table 1 andFigure 1.48–53 The specific phenotypic and complicationprofile of each HCA subtype may have an important rolein the establishment of an individualized managementstrategy.
Needle Biopsy
In the vast majority of hepatic tumors, high-qualityimaging permits accurate characterization and diag-nosis, rendering a percutaneous core needle biopsy un-necessary.54 An image-guided percutaneous biopsy ofthe liver tumor may be useful when radiologic findingsare nondiagnostic, and specific patterns of immunostainsanalyzed by an expert pathologist may be helpful in thedistinction of HCA from FNH, well-differentiated HCC, orsteatotic nontumoral liver.55–58 In a review of 239 needlebiopsies, a diagnosis of HCA was established with routinestaining of core needle biopsy specimens in 58.6% ofpatients, which increased to 74.3% after the use of

Figure 2. Gadoxetic acid–enhanced MRI of simulta-neous HCA and FNH in a27-year-old woman. (A)Although both lesionsshow arterial enhance-ment, (B) FNH (arrow) ishyperintense comparedwith the surrounding liverparenchyma, and HCA ishypointense (asterisk) dur-ing the hepatobiliary phaseat 20 minutes.
1224 Agrawal et al Clinical Gastroenterology and Hepatology Vol. 13, No. 7
specific immunostains including identification of HCAsubtypes with a similar distribution in surgicalspecimens.57
Radiologic Diagnosis
Most HCAs are diagnosed on contrast-enhanced,multiphase computed tomography (CT) or magneticresonance imaging (MRI).59 Multiphase dynamiccontrast-enhanced MRI is considered the modality ofchoice in the diagnosis of HCA and its subtypes.4,5,60–63
HCAs typically are hypoattenuating on noncontrast CT,hypervascular and heterogeneous on the arterial phase,and isoattenuating or hypoattenuating on the portalvenous phase of contrast-enhanced CT scan.61 The ac-curate diagnosis of HCA and its differentiation from otherbenign hepatic tumors, particularly FNH, is important.Arterial enhancement is a common feature of HCA andFNH, and hepatocyte-specific contrast agents allow dif-ferentiation between the 2 lesions when standard im-aging is indeterminate, as shown in Figure 2.64,65
Laumonier et al4 and Ronot et al5 described MRI as auseful tool for the identification of the 2 major HCAsubtypes: HNF-1a–inactivated and inflammatory HCAwith specific features related to intratumoral steatosisand sinusoidal dilatation, respectively. The typical MRfindings of the HCA subtypes are summarized in Table 1.Heterogeneity of signal intensity on T2-weighted imagesowing to the presence of fat, hemorrhage, or necrosis isone the most consistent features of HCA.63 Findings ofmarked hyperintensity on T2-weighted images withdelayed persistent enhancement in inflammatory HCAand diffuse signal drop-out on chemical shift imaging as aresult of diffuse intratumoral steatosis in HNF-1a–inactivated HCA are highly sensitive and specific asshown in Figures 3 and 4.4,66 On contrast-enhanced ul-trasound, homogeneous hyperechogenicity correlatedwith fat content in HNF-1a–inactivated HCA and arterialhypervascularity with centripetal filling was predictive ofinflammatory HCA.5,67 Unclassified and b-cat-enin–activated HCA were not characterized by any spe-cific MR features and the latter subtype may mimic HCC.
Inflammation may be seen in the b-catenin–activatedtumors showing a MR pattern typical of inflammatoryHCA tumors.
Clinical Features and TreatmentOutcome
The increased use of diagnostic abdominal imaginghas led to an increase in the incidental diagnosis ofHCA.1,16 More than half of the patients are asymptomaticand abdominal pain is the most common symptom in theother patients, usually related to tumoral hemor-rhage.8,9,68,69 Abnormal liver function tests may occur inpatients with large HCA tumors including increased g-glutamyl transferase levels, alkaline phosphatase sec-ondary to cholestasis, or an increase in transaminaselevels as a result of hepatic steatosis.9 Serum biomarkersof inflammation including fibrinogen and C-reactiveprotein were increased in 90% of patients with inflam-matory HCA and returned to normal after surgicalresection of the tumor.35
Hemorrhage
Hemorrhage occurs in 21% to 40% HCAs.8–10,70–74
Bleeding is intratumoral in most cases, however, it maycause rupture of the tumor, leading to subcapsular orintraperitoneal hemorrhage. Hemorrhage occurs pre-dominantly in HCA tumors greater than 5 cm and otherrisk factors include inflammatory subtype, increasingtumor size, hormone use within the past 6 months, andpregnancy.3,8,10,68,69 Rupture of HCA may present withsevere abdominal pain and free intraperitoneal hemor-rhage, however, hemodynamic instability is uncommon,permitting conservative management in mostcases.9,71,74 Initial stabilization and selective transarterialembolization (TAE) is preferred because emergent sur-gery for ruptured HCA has a mortality rate of 5% to 10%and delayed resection is associated with lower surgicalrisk, blood loss, postoperative complications, and ashorter length of stay.9,10,69,74,75

Figure 3.Gadolinium-enhanced MRI of inflammatory HCA.(A) A T1-weighted image shows strong arterial enhancementof the HCA (arrows) in segment 6, (B) persisting into thedelayed vascular phase. (C) A T2-weighted image showsintense hyperintensity in comparison with the surroundingliver.
July 2015 Management of Hepatocellular Adenoma 1225
Malignant Transformation
The risk of malignant transformation in HCA is 5%and its predictors are patient sex, tumor size, andsubtype. A 6- to 10-fold higher incidence of malignanttransformation has been reported in men, and system-atic resection of HCA regardless of the tumor size isrecommended in men.9,11 A systematic review of the
literature showed only 3 cases of HCC in tumorsmeasuring smaller than 5 cm, with the smallestmeasuring 4 cm.9,10,76 Patients with Fanconi’s anemiaare at increased risk for developing HCC, which mayresult from the malignant transformation of HCA tu-mors developing secondary to androgen treatment.77 b-catenin mutations are associated with an increased riskof malignant transformation and up to 46% of b-cat-enin-activated HCA may show the presence of HCC(Table 1).44 Approximately 10% of inflammatory HCAshow a mutated b-catenin gene and malignant trans-formation.9,16,46 Hepatocellular dysplasia, a premalig-nant condition, may be present in HCA with malignantdegeneration, however, some investigators have ques-tioned the progression of HCA to HCC.8,43,78,79 HCCwithin HCA usually is identified on the surgical spec-imen because the preoperative serum a-fetoproteinlevel typically is normal, with no vascular involvementor satellite nodules, and the tumor is well differentiated,rendering diagnosis on biopsy difficult.9,10,77 Theprognosis after complete resection of HCA with malig-nant degeneration is favorable and recurrence isuncommon.9 These cases should be distinguished fromthe exceptional cases of multiple degenerated HCCoccurring in young severely asthenic women withsymptomatic hepatomegaly and high a-fetoproteinlevels.
Multiple Hepatocellular Adenomas
A third of patients with HCA may be diagnosedwith multiple tumors on imaging and radiographicallyundetected microadenomas have been reported onresected specimens of a single HCA.9,10,16 Conditions ofobesity, hepatic steatosis, and metabolic syndrome areassociated with multiple HCAs.15,32–36 The developmentof complications including hemorrhage or malignanttransformation is unrelated to the number of HCA tu-mors.9,10,80,81 HCA tumors in liver adenomatosis arepredominantly of the low-risk HNF-1a–inactivated sub-type.15,82 Long-term follow-up evaluation of small re-sidual HCAs after surgical resection showed that 90% oftumors remained stable, regressed, or completely dis-appeared.9 Because of several obstacles to liver trans-plantation for GSD 1a, resection of enlarging HCA tumorsmay be an effective intermediate step in the preventionof HCC.83,84 Genetic counseling is recommended for pa-tients with liver adenomatosis, particularly for the fa-milial variant, and screening of their relatives with HCAand maturity-onset diabetes of the young type 3.15,49
Pregnancy
HCA in pregnancy requires special considerationbecause of the potential for hormone-induced growthand rupture, however, the majority of HCAs remain sta-ble during pregnancy.9,85,86 Most tertiary care centers

Figure 4.Gadolinium-enhanced MRI of HNF-1a–mutated HCA. (A) A T1 in-phase image shows alesion (arrow) that is iso-intense in comparison withthe surrounding liver and(B) an out-of-phase imageshows a signal decreasewithin the lesion (arrow)compatible with intra-tumoral fat.
1226 Agrawal et al Clinical Gastroenterology and Hepatology Vol. 13, No. 7
with hepatobiliary surgeons do not discourage preg-nancy in women with HCAs smaller than 5 cm providedthe patients are accompanied and likely to be compliantwith sonographic monitoring every 3 months and in thepostpartum period.9,10,59,86–89
Therapeutic Strategy
The diagnosis of HCA, particularly in a young woman,has significant implications considering potential tumor-
Figure 5.Management of HCA. Current diagnostic accuracy ofon decision making to a restricted number of situations. These inremaining cases in which pathologic results will have an impacrequire percutaneous liver biopsy is the MRI suspicion of a stcontext, obtaining clear pathologic confirmation of the HNF-1a
related complications, impact on future pregnancies, useof OCs, and major surgical intervention.9,16 Systematicresection of newly diagnosed HCA owing to the risk oftumor-related complications is no longer acceptable andthe initial management is conservative with a selectivepolicy of intervention in tumors at increased risk ofcomplications.9–11,59 Considerations for invasive treat-ment for HCA include patient sex, tumor size, and sub-type (Figure 5). The application of percutaneous biopsyin the decision making for subtyping of HCA tumors isvariable, with some investigators advocating a
MRI for the subtyping of HCA now limits the impact of biopsyclude doubtful cases after complete imaging work-up and thet on the management of the lesions. One situation that mayeatotic lesion greater than 5 cm in a female patient. In suchsubtype is mandatory to support a nonsurgical management.

July 2015 Management of Hepatocellular Adenoma 1227
percutaneous biopsy in small HCA tumors not defini-tively subtyped by MRI and others advocating a sys-tematic biopsy in HCAs smaller than 5 cm to confirm theabsence of b-catenin activation, however, the risk ofmalignant transformation in such small tumors is negli-gible, in addition to the difficulty in the interpretation ofthe b-catenin stain, particularly in a needle biopsy.16,52
We advocate the selective use of percutaneous biopsyin HCAs restricted to tumors approaching 5 cm in sizeand not being considered for resection.
Conservative Management
In a survey of Dutch university hospitals, conserva-tive management was the initial policy in all hospitalscomprising cessation of OCs or hormonal therapy andimaging surveillance.57 After discontinuation of OCs,79% of patients showed regression of their HCAs, withsome tumors showing total regression.48,58 In a study of48 consecutive women with HCA, 23 women with tu-mors smaller than 5 cm were allocated to conservativemanagement and at a median follow-up period of 24months none of them had shown an increase in size,bleeding, or malignant degeneration, leading the in-vestigators to justify observation as the initial treatmentfor tumors smaller than 5 cm.70 Despite consensus thatOCs should be discontinued, it may not result in tumorregression, suggesting that additional factors such asobesity may play a role.8,10,32–36,90 There is no agreementon the issue of resumption of OCs even after completeresection of the tumor, however, patients tend not toresume their use.59 Radiologic surveillance is recom-mended if oral contraceptives are resumed. Conservativemanagement is recommended in women with single ormultiple HCAs smaller than 5 cm. In some tumors 5 cmor larger of the low-risk steatotic subtype, a conservativeapproach may be adopted after confirming the subtypewith a needle biopsy. The radiologic modality of choiceand interval of imaging are not well defined but weadvocate MRI for multiple HCAs and tumors not wellcharacterized on ultrasound examination. The optimalduration of follow-up evaluation is unclear and someauthors16 recommend follow-up evaluation untilmenopause.
Invasive Treatment
Surgical resection is recommended for male pa-tients regardless of tumor size and in women for tu-mors 5 cm or larger.9 Some investigators recommend alower threshold for resection at a tumor size of 4 cm orlarger.7,8,10 The surgical approach does not require awide resection margin or a regional lymphadenectomyeven in the case of suspected malignancy owing to theminimal risk of vascular invasion or lymph nodeinvolvement, and a laparoscopic approach maybe considered for a nonhemorrhagic HCA.8,91,92
Intraoperative ultrasound is useful because HCA tu-mors often are soft and nonpalpable with ill-definedmargins between the tumor and the adjacent stea-totic hepatic parenchyma. In patients with a large HCA,a 2-step surgical approach with portal vein occlusionmay be required. Resection is not indicated for multi-ple tumors smaller than 5 cm because the vast ma-jority of residual HCAs remain stable or undergospontaneous regression.9 Intrahepatic portosystemicvenous shunt is a predisposing factor in the patho-genesis of HCA and its treatment requires closure bytranscatheter embolization or surgical resec-tion.37,93,94 Failure to close the shunt may result inprogression of the residual HCAs.38 Seyama et al37
recommend simultaneous resection of the HCAs andclosure of the shunt, which resolves the disturbance inthe hepatic vascularity and may reduce the multi-centric occurrence of HCA.
TAE is recommended for HCA complicated by hem-orrhage. Patients with tumoral hemorrhage rarely pre-sent with hemodynamic instability, permitting initial TAEfollowed by delayed surgery. TAE is indicated within 2 to3 days after tumoral hemorrhage and is best performedusing a selective approach. During the first week afterthe procedure, there may be abdominal pain, fever, rightpleural effusion, and increased transaminase levels,which generally return to normal in the second week.The patient may be discharged with advice to discon-tinue hormonal therapy and undergo a CT scan after amonth and every 3 months thereafter. Liver resection isconsidered only after resorption of the peritumoral he-matoma, usually 6 months after the initial hospitaliza-tion. TAE may result in regression or complete involutionof the tumor, and the absence of residual tissue on MRImay justify a nonsurgical approach with surveillancewhereas radiographic persistence of HCA tissue remainsan indication for surgical resection.9,10,95–98 Tumorregression after TAE for hemorrhagic HCA has led toutilization of this approach for the elective reduction oftumor mass in unruptured HCA.13,69 TAE is minimallyinvasive, safely repeated, and 80% of tumors may showstability, regression, or complete involution.13,14,99
Although these results are reported in small tumors,TAE may be used in the management of large multiple orbilateral tumors or preoperative reduction in tumorsize.14,95
Radiofrequency ablation may be appropriate forpatients who are not surgical candidates, express anactive desire for pregnancy with hormone-sensitivetumors, have a centrally located tumor, underlyingliver disease, or show progression of residual tumorsafter resection.9,10,12,100–103 The size of the HCA shouldbe smaller than 4 cm for effective ablation and initialexperience suggests it is safe and well tolerated.104
Liver transplantation is no longer indicated for mul-tiple unresectable HCA tumors and a favorable long-termoutcome does not justify the use of limited grafts.9,15,82
In exceptional cases, liver transplantation may be

1228 Agrawal et al Clinical Gastroenterology and Hepatology Vol. 13, No. 7
considered for multiple unresectable HCA tumors in menor those associated with an intrahepatic portosystemicvenous shunt. Despite the tendency for HCA progressionin GSD Ia, there is no increased risk of hemorrhage ormalignant transformation. Although liver transplantationprovides definitive treatment for GSD Ia by correctingthe underlying enzymatic defect, it should be consideredonly based on the condition of the underlying liverparenchyma.
In conclusion, the inability to differentiate HCA fromother benign tumors or to identify patients at increasedrisk for tumor-related complications may result in un-necessary liver resections. With the increasing incidenceof metabolic syndrome, association of HCA with obesityand hepatic steatosis, and recognition of low-risk HCAsubtypes, a selective approach to intervention may beconsidered. Although advances in immunohistochemicaltechniques have enhanced the ability to identify high-riskHCA subtypes, tumor size and patient sex are the pri-mary criteria in the selection of patients for invasivetreatment and the choice of the optimal therapeuticmodality. Furthermore, the long-term outcome of a se-lective approach to HCA management requires system-atic evaluation and, given the rarity of the disease, it mayrequire a multicenter study.
References
1. Buell JF, Tranchart H, Cannon R, et al. Management of benignhepatic tumors. Surg Clin North Am 2010;90:719–735.
2. Rooks JB, Ory HW, Ishak KG, et al. Epidemiology of hepato-cellular adenoma. The role of oral contraceptive use. JAMA1979;242:644–648.
3. Bioulac-Sage P, Rebouissou S, Thomas C, et al. Hepatocellularadenoma subtype classification using molecular markers andimmunohistochemistry. Hepatology 2007;46:740–748.
4. Laumonier H, Bioulac-Sage P, Laurent C, et al. Hepatocellularadenomas: magnetic resonance imaging features as a functionof molecular pathological classification. Hepatology 2008;48:808–818.
5. Ronot M, Bahrami S, Calderaro J, et al. Hepatocellular ade-nomas: accuracy of magnetic resonance imaging and liver biopsyin subtype classification. Hepatology 2011;53:1182–1191.
6. Mounajjed T, Wu TT. Telangiectatic variant of hepatic adenoma:clinicopathologic features and correlation between liver needlebiopsy and resection. Am J Surg Pathol 2011;35:1356–1363.
7. Brenner DJ, Hall EJ. Computed tomography–an increasingsource of radiation exposure. N Engl J Med 2007;357:2277–2284.
8. Cho SW, Marsh JW, Steel J, et al. Surgical management ofhepatocellular adenoma: take it or leave it? Ann Surg Oncol2008;15:2795–2803.
9. Dokmak S, Paradis V, Vilgrain V, et al. A single-center surgicalexperience of 122 patients with single and multiple hepatocel-lular adenomas. Gastroenterology 2009;137:1698–1705.
10. Deneve JL, Pawlik TM, Cunningham S, et al. Liver cell adenoma:a multicenter analysis of risk factors for rupture and malignancy.Ann Surg Oncol 2009;16:640–648.
11. Farges O, Ferreira N, Dokmak S, et al. Changing trends in ma-lignant transformation of hepatocellular adenoma. Gut 2011;60:85–89.
12. van Vledder MG, van Aalten SM, Terkivatan T, et al. Safety andefficacy of radiofrequency ablation for hepatocellular adenoma.J Vasc Interv Radiol 2011;22:787–793.
13. Erdogan D, van Delden OM, Busch OR, et al. Selective trans-catheter arterial embolization for treatment of bleeding compli-cations or reduction of tumor mass of hepatocellular adenomas.Cardiovasc Intervent Radiol 2007;30:1252–1258.
14. Deodhar A, Brody LA, Covey AM, et al. Bland embolization in thetreatment of hepatic adenomas: preliminary experience. J VascInterv Radiol 2011;22:795–799.
15. Nault JC, Bioulac-Sage P, Zucman-Rossi J. Hepatocellularbenign tumors-from molecular classification to personalizedclinical care. Gastroenterology 2013;144:888–902.
16. Bioulac-Sage P, Laumonier H, Couchy G, et al. Hepatocellularadenoma management and phenotypic classification: theBordeaux experience. Hepatology 2009;50:481–489.
17. Baum JK, Bookstein JJ, Holtz F, et al. Possible associationbetween benign hepatomas and oral contraceptives. Lancet1973;2:926–929.
18. Heinemann LA, Weimann A, Gerken G, et al. Modern oral con-traceptive use and benign liver tumors: the German Benign LiverTumor Case-Control Study. Eur J Contracept Reprod HealthCare 1998;3:194–200.
19. Giannitrapani L, Soresi M, La Spada E, et al. Sex hormones andrisk of liver tumor. Ann N Y Acad Sci 2006;1089:228–236.
20. Velazquez I, Alter BP. Androgens and liver tumors: Fanconi’sanemia and non-Fanconi’s conditions. Am J Hematol 2004;77:257–267.
21. Bork K, Pitton M, Harten P, et al. Hepatocellular adenomas inpatients taking danazol for hereditary angio-oedema. Lancet1999;353:1066–1067.
22. Nakao A, Sakagami K, Nakata Y, et al. Multiple hepaticadenomas caused by long-term administration of androgenicsteroids for aplastic anemia in association with familial adeno-matous polyposis. J Gastroenterol 2000;35:557–562.
23. Socas L, Zumbado M, Pérez-Luzardo O, et al. Hepatocellularadenomas associated with anabolic androgenic steroid abuse inbodybuilders: a report of two cases and a review of the litera-ture. Br J Sports Med 2005;39:e27.
24. Beuers U, Richter WO, Ritter MM, et al. Klinefelter’s syndromeand liver adenoma. J Clin Gastroenterol 1991;13:214–216.
25. Triantafyllopoulou M, Whitington PF, Melin-Aldana H, et al.Hepatic adenoma in an adolescent with elevated androgenlevels. J Pediatr Gastroenterol Nutr 2007;44:640–642.
26. Carrasco D, Barrachina M, Prieto M, et al. Clomiphene citrateand liver-cell adenoma. N Engl J Med 1984;310:1120–1121.
27. Vázquez JJ, Marigil MA. Liver-cell adenoma in an epileptic manon barbiturates. Histol Histopathol 1989;4:301–303.
28. Espat J, Chamberlain RS, Sklar C, et al. Hepatic adenomaassociated with recombinant human growth hormone therapyin a patient with Turner’s syndrome. Dig Surg 2000;17:640–643.
29. Bioulac-Sage P, Laumonier H, Laurent C, et al. Hepatocellularadenoma: what is new in 2008. Hepatol Int 2008;2:316–321.
30. Talente GM, Coleman RA, Alter C, et al. Glycogen storage dis-ease in adults. Ann Intern Med 1994;120:218–226.
31. Choi BY, Nguyen MH. The diagnosis and management ofbenign hepatic tumors. J Clin Gastroenterol 2005;39:401–412.
32. Bunchorntavakul C, Bahirwani R, Drazek D, et al. Clinical fea-tures and natural history of hepatocellular adenomas: the impactof obesity. Aliment Pharmacol Ther 2011;34:664–674.

July 2015 Management of Hepatocellular Adenoma 1229
33. Bioulac-Sage P, Taouji S, Possenti L, et al. Hepatocellular ad-enoma subtypes: the impact of overweight and obesity. Liver Int2012;32:1217–1221.
34. Furlan A, van der Windt DJ, Nalesnik MA, et al. Multiple hepaticadenomas associated with liver steatosis at CT and MRI: acase-control study. AJR Am J Roentgenol 2008;191:1430–1435.
35. Paradis V, Champault A, Ronot M, et al. Telangiectatic ade-noma: an entity associated with increased body mass index andinflammation. Hepatology 2007;46:140–146.
36. Veteläinen R, Erdogan D, de Graaf W, et al. Liver adenomatosis:re-evaluation of aetiology and management. Liver Int 2008;28:499–508.
37. Seyama Y, Sano K, Tang W, et al. Simultaneous resection ofliver cell adenomas and an intrahepatic portosystemic venousshunt with elevation of serum PIVKA-II level. J Gastroenterol2006;41:909–912.
38. Kawakatsu M, Vilgrain V, Belghiti J, et al. Association of multipleliver cell adenomas with spontaneous intrahepatic portohepaticshunt. Abdom Imaging 1994;19:438–440.
39. Grazioli L, Federle MP, Ichikawa T, et al. Liver adenomatosis:clinical, histopathologic, and imaging findings in 15 patients.Radiology 2000;216:395–402.
40. Maillette de Buy Wenniger L, Terpstra V, Beuers U. Focalnodular hyperplasia and hepatic adenoma: epidemiology andpathology. Dig Surg 2010;27:24–31.
41. Paradis V, Benzekri A, Dargère D, et al. Telangiectatic focalnodular hyperplasia: a variant of hepatocellular adenoma.Gastroenterology 2004;126:1323–1329.
42. Singhi AD, Jain D, Kakar S, et al. Reticulin loss in benign fattyliver: an important diagnostic pitfall when considering a diagnosisof hepatocellular carcinoma. Am J Surg Pathol 2012;36:710–715.
43. Witjes CD, Ten Kate FJ, van Aalten SM, et al. Hepatocellularadenoma as a risk factor for hepatocellular carcinoma in a non-cirrhotic liver: a plea against. Gut 2012;61:1645–1646.
44. Zucman-Rossi J, Jeannot E, Nhieu JT, et al. Genotype-pheno-type correlation in hepatocellular adenoma: new classificationand relationship with HCC. Hepatology 2006;43:515–524.
45. Rebouissou S, Amessou M, Couchy G, et al. Frequent in-framesomatic deletions activate gp130 in inflammatory hepatocellulartumours. Nature 2009;457:200–204.
46. Bioulac-Sage P, Balabaud C, Zucman-Rossi J. Subtype clas-sification of hepatocellular adenoma. Dig Surg 2010;27:39–45.
47. Bluteau O, Jeannot E, Bioulac-Sage P, et al. Bi-allelic inactiva-tion of TCF1 in hepatic adenomas. Nat Genet 2002;32:312–315.
48. Foster JH, Donohue TA, Berman MM. Familial liver-cell ade-nomas and diabetes mellitus. N Engl J Med 1978;299:239–241.
49. Bacq Y, Jacquemin E, Balabaud C, et al. Familial liver adeno-matosis associated with hepatocyte nuclear factor 1alphainactivation. Gastroenterology 2003;125:1470–1475.
50. Yamagata K, Oda N, Kaisaki PJ, et al. Mutations in the hepa-tocyte nuclear factor-1alpha gene in maturity-onset diabetes ofthe young (MODY3). Nature 1996;384:455–458.
51. Rebouissou S, Imbeaud S, Balabaud C, et al. HNF1alphainactivation promotes lipogenesis in human hepatocellular ad-enoma independently of SREBP-1 and carbohydrate-responseelement-binding protein (ChREBP) activation. J Biol Chem2007;282:14437–14446.
52. van Aalten SM, Verheij J, Terkivatan T, et al. Validation of a liveradenoma classification system in a tertiary referral centre: im-plications for clinical practice. J Hepatol 2011;55:120–125.
53. Wilkens L, Bredt M, Flemming P, et al. Diagnostic impact offluorescence in situ hybridization in the differentiation of hepa-tocellular adenoma and well-differentiated hepatocellular carci-noma. J Mol Diagn 2001;3:68–73.
54. Rockey DC, Caldwell SH, Goodman ZD, et al. Liver biopsy.American Association for the Study of Liver Diseases. Hep-atology 2009;49:1017–1044.
55. Fabre A, Audet P, Vilgrain V, et al. Histologic scoring of liverbiopsy in focal nodular hyperplasia with atypical presentation.Hepatology 2002;35:414–420.
56. Ahmad I, Iyer A, Marginean CE, et al. Diagnostic use of cyto-keratins, CD34, and neuronal cell adhesion molecule staining infocal nodular hyperplasia and hepatic adenoma. Hum Pathol2009;40:726–734.
57. Bioulac-Sage P, Cubel G, Taouji S, et al. Immunohistochemicalmarkers on needle biopsies are helpful for the diagnosis of focalnodular hyperplasia and hepatocellular adenoma subtypes. AmJ Surg Pathol 2012;36:1691–1699.
58. van Aalten SM, Witjes CD, de Man RA, et al. Can a decision-making model be justified in the management of hepatocellu-lar adenoma? Liver Int 2012;32:28–37.
59. van Aalten SM, Terkivatan T, de Man RA, et al. Diagnosis andtreatment of hepatocellular adenoma in the Netherlands: simi-larities and differences. Dig Surg 2010;27:61–67.
60. Purysko AS, Remer EM, Coppa CP, et al. Characteristics anddistinguishing features of hepatocellular adenoma and focalnodular hyperplasia on gadoxetate disodium-enhanced MRI.AJR Am J Roentgenol 2012;198:115–123.
61. Brancatelli G, Federle MP, Vullierme MP, et al. CT and MR im-aging evaluation of hepatic adenoma. J Comput Assist Tomogr2006;30:745–750.
62. Ruppert-Kohlmayr AJ, Uggowitzer MM, Kugler C, et al. Focalnodular hyperplasia and hepatocellular adenoma of the liver:differentiation with multiphasic helical CT. AJR Am J Roentgenol2001;176:1493–1498.
63. Chung KY, Mayo-Smith WW, Saini S, et al. Hepatocellular ad-enoma: MR imaging features with pathologic correlation. AJRAm J Roentgenol 1995;165:303–308.
64. Bieze M, van den Esschert JW, Nio CY, et al. Diagnostic ac-curacy of MRI in differentiating hepatocellular adenoma fromfocal nodular hyperplasia: prospective study of the additionalvalue of gadoxetate disodium. AJR Am J Roentgenol 2012;199:26–34.
65. Grazioli L, Bondioni MP, Haradome H, et al. Hepatocellularadenoma and focal nodular hyperplasia: value of gadoxeticacid-enhanced MR imaging in differential diagnosis. Radiology2012;262:520–529.
66. Van Aalten SM, Thomeer MG, Terkivatan T, et al. Hepato-cellular adenomas: correlation of MR imaging findings withpathologic subtype classification. Radiology 2011;261:172–181.
67. Laumonier H, Cailliez H, Balabaud C, et al. Role of contrast-enhanced sonography in differentiation of subtypes of hepato-cellular adenoma: correlation with MRI findings. AJR Am JRoentgenol 2012;199:341–348.
68. Toso C, Majno P, Andres A, et al. Management of hepatocellularadenoma: solitary-uncomplicated, multiple and ruptured tu-mors. World J Gastroenterol 2005;11:5691–5695.
69. Leese T, Farges O, Bismuth H. Liver cell adenomas. A 12-yearsurgical experience from a specialist hepato-biliary unit. AnnSurg 1988;208:558–564.

1230 Agrawal et al Clinical Gastroenterology and Hepatology Vol. 13, No. 7
70. Van der Windt DJ, Kok NF, Hussain SM, et al. Case-orientatedapproach to the management of hepatocellular adenoma. Br JSurg 2006;93:1495–1502.
71. Van Aalten SM, de Man RA, IJzermans JN, et al. Systematicreview of haemorrhage and rupture of hepatocellular adenomas.Br J Surg 2012;99:911–916.
72. Battula N, Tsapralis D, Takhar A, et al. Aetio-pathogenesis andthe management of spontaneous liver bleeding in the West: a16-year single-centre experience. HPB (Oxford) 2012;14:382–389.
73. Maoz D, Sharon E, Chen Y, et al. Spontaneous hepatic rupture:13-year experience of a single center. Eur J GastroenterolHepatol 2010;22:997–1000.
74. Marini P, Vilgrain V, Belghiti J. Management of spontaneousrupture of liver tumours. Dig Surg 2002;19:109–113.
75. Shortell CK, Schwartz SI. Hepatic adenoma and focal nodularhyperplasia. Surg Gynecol Obstet 1991;173:426–431.
76. Stoot JH, Coelen RJ, De Jong MC, et al. Malignant trans-formation of hepatocellular adenomas into hepatocellular car-cinomas: a systematic review including more than 1600adenoma cases. HPB (Oxford) 2010;12:509–522.
77. Farges O, Dokmak S. Malignant transformation of liveradenoma: an analysis of the literature. Dig Surg 2010;27:32–38.
78. Tao LC. Oral contraceptive-associated liver cell adenomaand hepatocellular carcinoma. Cytomorphology andmechanism of malignant transformation. Cancer 1991;68:341–347.
79. Micchelli ST, Vivekanandan P, Boitnott JK, et al. Malignanttransformation of hepatic adenomas. Mod Pathol 2008;21:491–497.
80. Ribeiro A, Burgart LJ, Nagorney DM, et al. Management of liveradenomatosis: results with a conservative surgical approach.Liver Transpl Surg 1998;4:388–398.
81. Karkar AM, Tang LH, Kashikar ND, et al. Managementof hepatocellular adenoma: comparison of resection,embolization and observation. HPB (Oxford) 2013;15:235–243.
82. Greaves WO, Bhattacharya B. Hepatic adenomatosis. ArchPathol Lab Med 2008;132:1951–1955.
83. Reddy SK, Austin SL, Spencer-Manzon M, et al. Liver trans-plantation for glycogen storage disease type Ia. J Hepatol 2009;51:483–490.
84. Reddy SK, Kishnani PS, Sullivan JA, et al. Resection of hepa-tocellular adenoma in patients with glycogen storage diseasetype Ia. J Hepatol 2007;47:658–663.
85. Cobey FC, Salem RR. A review of liver masses in pregnancy anda proposed algorithm for their diagnosis and management. Am JSurg 2004;187:181–191.
86. Noels JE, van Aalten SM, van der Windt DJ, et al. Managementof hepatocellular adenoma during pregnancy. J Hepatol 2011;54:553–558.
87. Jabbour N, Brenner M, Gagandeep S, et al. Major hepatobiliarysurgery during pregnancy: safety and timing. Am Surg 2005;71:354–358.
88. Wilson CH, Manas DM, French JJ. Laparoscopic liver resectionfor hepatic adenoma in pregnancy. J Clin Gastroenterol 2011;45:828–833.
89. Stoot JH, van Roosmalen J, Terpstra OT, et al. Life-threateninghemorrhage from adenomas in the liver during pregnancy. DigSurg 2006;23:155.
90. Nagorney DM. Benign hepatic tumors: focal nodular hyperplasiaand hepatocellular adenoma. World J Surg 1995;19:13–18.
91. Buell JF, Cherqui D, Geller DA, et al. The international positionon laparoscopic liver surgery: The Louisville Statement, 2008.Ann Surg 2009;250:825–830.
92. Agrawal S, Belghiti J. Oncologic resection for malignant tumorsof the liver. Ann Surg 2011;253:656–665.
93. Jeng LB, Chen MF. Intrahepatic portohepatic venous shunt. Acase report of successful surgical resection. Arch Surg 1993;128:349–352.
94. Tanoue S, Kiyosue H, Komatsu E, et al. Symptomatic intra-hepatic portosystemic venous shunt: embolization with analternative approach. AJR Am J Roentgenol 2003;181:71–78.
95. Kobayashi S, Sakaguchi H, Takatsuka M, et al. Two cases ofhepatocellular adenomatosis treated with transcatheter arterialembolization. Hepatol Int 2009;3:416–420.
96. Erdogan D, Busch OR, van Delden OM, et al. Management ofspontaneous haemorrhage and rupture of hepatocellular ade-nomas. A single centre experience. Liver Int 2006;26:433–438.
97. Terkivatan T, de Wilt JH, de Man RA, et al. Treatment of rupturedhepatocellular adenoma. Br J Surg 2001;88:207–209.
98. Huurman VA, Schaapherder AF. Management of ruptured he-patocellular adenoma. Dig Surg 2010;27:56–60.
99. Stoot JH, van der Linden E, Terpstra OT, et al. Life-savingtherapy for haemorrhaging liver adenomas using selectivearterial embolization. Br J Surg 2007;94:1249–1253.
100. Atwell TD, Brandhagen DJ, Charboneau JW, et al. Successfultreatment of hepatocellular adenoma with percutaneous radio-frequency ablation. AJR Am J Roentgenol 2005;184:828–831.
101. Rhim H, Lim HK, Kim YS, et al. Percutaneous radiofrequencyablation of hepatocellular adenoma: initial experience in 10 pa-tients. J Gastroenterol Hepatol 2008;23:e422–e427.
102. Fujita S, Kushihata F, Herrmann GE, et al. Combined hepaticresection and radiofrequency ablation for multiple hepatic ade-nomas. J Gastroenterol Hepatol 2006;21:1351–1354.
103. Agrawal S, Daruwala C. Metabolic syndrome and hepaticresection: improving outcome. HPB (Oxford) 2011;13:846–859.
104. van der Sluis FJ, Bosch JL, Terkivatan T, et al. Hepatocellularadenoma: cost-effectiveness of different treatment strategies.Radiology 2009;252:737–746.
Reprint requestsAddress requests for reprints to: Jacques Belghiti, MD, Department of Hep-atobiliary and Transplant Surgery, Beaujon Hospital, University of Paris, 100Boulevard du General Leclerc, 92110 Clichy, France. e-mail: [email protected]; fax: +33 1 40 87 17 24.
Conflicts of interestThe authors disclose no conflicts.