Personality Factors in Chronic Hemodialysis Patients
13
Personality Factors in Chronic Hemodialysis Patients Causing Noncompliance With Medical Regimen A. Kaplan De-Nour, MD and J . W. Czaczkes, PhD, MD Forty-three patients on chronic hemodialysis were observed in a prospec- tive study on the effects of a number of personality factors on noncompli- ance with a medical regimen (diet). It was found that low frustration tolerance and gains (primary and secondary) from the sick role were the most frequent causes for noncompliance, and these differentiated sig- nificantly between compilers and noncompliers, while "acting out" was frequent in both groups though more severe in the noncompliers. Other factors such as denial of sick role and suicidal behavior were also found, although more rarely. The importance of identifying the specific factors in each individual patient was stressed as it would dictate the strategy of the psychothera- peuti c intervention. Although only dialysis patients were included in this study, it was sug- gested that the personality factors described can be identified in other patients and other medical setups as well. In many areas of medicine, the patient's well- being, his health and, at times, his life greatly depend on his active participation in a treat- ment program and on his compliance with the medical recommendations—eg, taking medi- cines, adhering to a diet or undergoing surgery. Since abuse of medical recommendations often ' threatens the patient's health and life, there exists a tendency to regard noncompliance as expressing suicidal intentions (conscious or un- conscious) and to regard it as suicidal behav- ior(l). The chronic hemodialysis setup (studied also in the above-mentioned report) is ideal for From the Department of Psychiatry and the Nephrolog- ical Service, Hadassah University Hospital and Medical School, Jerusalem, Israel. Supported by Grant 06-823-2 from the US Department of Health, Education, and Welfare, Public Health Service. Received for publication July 22, 1971; final revision re- ceived Jan 5, 1972. Address for reprint requests: A. Kaplan De-Nour, MD, Department of Psychiatry, Hadassah University Hospital, PO Bo x 499, Jerusalem, Israel. studying the problems of noncompliance and abuse of medical regimen. The treatment is chronic and the contact with the patients both prolonged and intensive. They cannot switch places or simply go to another physician. The problem (common at least in our country) that a patient consults three or more physicians, gets a variety of recommendations and becomes "mixed up" and does not comply with any of them, exists only to a very small extent in dialysis patients. The medical regimen of dialysis is usually very clear-cut. Furthermore, patients' adher- ence to or abuse of many of its aspects is easily measured; if a patient drinks too much, he gains weight; if he abuses the fruit restrictions, his blood potassium goes up. Therefore, at least some aspects of compliance, often the most im- portant ones for the physical well-being of a dialysis patient, can be checked by objective methods, while for other aspects one has to ac- cept, at least to some extent, the patient's de- scription of his behavior—eg, taking the prescribed amount of some medication. Psychosomatic Medicine, Vol. 34 , No. 4 (July -Augus t 1972 ) 33 3
-
Upload
iulianadlacan -
Category
Documents
-
view
225 -
download
0
Transcript of Personality Factors in Chronic Hemodialysis Patients

8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 1/12
Personality Factors in Chronic Hemodialysis Patients
Causing Noncompliance With Medical Regimen
A. Kaplan De-Nour, MD and J . W. Czaczkes, PhD, MD
Forty-three patients on chronic hemodialysis were observed in a prospec-tive study on the effects of a number of personality factors on noncompli-
ance with a medical regimen (diet). It was found that low frustrationtolerance and gains (primary and secondary) from the sick role were themost frequent causes for noncompliance, and these differentiated sig-nificantly between compilers and noncompliers, while "acting out" wasfrequent in both groups though more severe in the noncompliers. Otherfactors such as denial of sick role and suicidal behavior were also found,although more rarely.
The importance of identifying the specific factors in each individualpatient was stressed as it would dictate the strategy of the psychothera-peutic intervention.
Although only dialysis patients were included in this study, it was sug-gested that the personality factors described can be identified in otherpatients and other medical setups as well.
In many areas of medicine, the patient's well-being, his health and, at times, his life greatly
depend on his active participation in a treat-
ment program and on his compliance with the
medical recommendations—eg, taking medi-
cines, adhering to a diet or undergoing surgery.
Since abuse of medical recommendations often '
threatens the patient's health and life, there
exists a tendency to regard noncompliance as
expressing suicidal intentions (conscious or un-
conscious) and to regard it as suicidal behav-
i o r ( l ) .
The chronic hemodialysis setup (studied also
in the above-mentioned report) is ideal for
From the Department of Psychiatry and the Nephrolog-ical Service, Hadassah University Hospital and MedicalSchool, Jerusalem, Israel.
Supported by Grant 06-823-2 from the US Departmentof Health, Education, and Welfare, Public Health Service.
Received for publication July 22, 1971; final revision re-ceived Jan 5, 1972.
Address for reprint requests: A. Kaplan De-Nour, MD,Department of Psychiatry, Hadassah University Hospital,PO Box 499, Jerusalem, Israel.
studying the problems of noncompliance andabuse of medical regimen. The treatment is
chronic and the contact with the patients both
prolonged and intensive. They cannot switch
places or simply go to another physician. The
problem (common at least in our country) that a
patient consults three or more physicians, gets a
var iety of recommendations and becomes
"mixed up" and does not comply with any of
them, exists only to a very small extent in
dialysis patients.
The medical regimen of dialysis is usually
very clear-cut. Furthermore, patients' adher-
ence to or abuse of many of its aspects is easily
measured; if a patient drinks too much, he gains
weight; if he abuses the fruit restrictions, his
blood potassium goes up. Therefore, at least
some aspects of compliance, often the most im-
portant ones for the physical well-being of a
dialysis patient, can be checked by objective
methods, while for other aspects one has to ac-
cept, at least to some extent, the patient's de-
scr ipt ion of his behavior—eg, taking the
prescribed amount of some medication.
Psychosomatic Medicine, Vol. 34 , No. 4 (July-August 1972 ) 333

8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 2/12
DE-NOUR & CZACZKES
It is not surprising, therefore, that recent re-ports concerned with the determinants of com-pliance, like the present one, deal with dialysispatients. Borkman (2) noticed that a patientmay comply with some, and at the same timeabuse other, aspects of one and the same pro-gram, and she proceeded to study compliancewith seven aspects of dialysis. In the same studyit was found that intelligence has little influence
on compliance with three aspects concernedwith keeping the diet, but that it does affectother aspects—eg, rehabilitation. Borkman alsofound a strong relationship between patients'understanding of the restrictions (as assessed byteam members) and their compliance. To quotethat report, however, "the majority' of non-compliers with any restriction has an adequateor excellent understanding of that restriction.Only one-third or less of non-compliers with adietary restriction have poor understanding ofthat restriction." We feel that her comment,"The extent to which a patient's ratings on
understanding and complying . . . are not in-dependent, cannot be ascertained" should bestressed.
Goldstein and Reznikoff (3) recently suggest-ed that one should regard abuse of the diet bydialysis patients not as suicidal behavior butrather as an attempt to adjust to the stress. "Asan attempt to cope with the continuous respon-sibility and anxiety of keeping oneself alive byfollowing a rigid treatment regimen, the he-modialysis patient adopts an external locus ofcontrol with the result that his behavior is no
longer perceived as life sustaining and athreaten ing area of responsibility is avoided."
Working with chronic hemodialysis patientsfor a number of years has brought us to theconclusion that a patient's abuse of a medicalregimen cannot be ascribed to one factor only.The medical team can affect the compliance ornoncompliance of some patients. For othermedical setups, a number of studies (4-7) in-clude reports on the effects of doctor-patientrelations on compliance. Families' attitudesinfluence the patient's behavior, and a number
of personality factors can result in abuse of themedical regimen. In the present report wewould like to concentrate mostly on the per-sonality factors which, we suggest, are the de-terminants of noncompliance with the medicalregimen of chronic hemodialysis.
METHOD AND PROCEDURE
The Patients
Forty-three patients were observed in six different dialy-
sis units in the country. Twenty-eight of these patients were
men and 15 women. The majority of the group (25) were in
the age group of 20 to 39. Five patients were under 20, and
13 patients were over 40. Fourteen were single, 28 were
married and 1 was divorced. The group as a whole were at
a low educational level; a third of the patients (14) had
either no education at all or had not completed elementary
school. Only 10 patients had high school educations and few
of them higher educations. Most of the patients were also at
a low socioeconomic level (Table 1). Patients who had
started dialysis during the last 6 months only were excluded
from this report, except for 3 patients who died on dialysis.
The duration on dialysis of the 43 patients studied is pre-sented in Table 2.
Table 1 . Socioeconomic Cond ition
of Patients Examined
No . ofOccupat ion pat ients
NoneHousewives
Unskil led workers
Skil led workersHigh school and college students
Professionals
9997
6
3
Table 2. Length of Tim e on Dialysis
for the Patients Examined
Time on dialysis No . of patients
Under 6 mo nths*7-12 months
13-24 monthsOver 2 years
317149
*These patients died after 2, 3 1/2 and 4 months
on dialysis, respectively.
33 4 Psychosomatic Medicine, Vol. 34 , No. 4 (July-August 19 72)

8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 3/12
PERSONALITY FACTORS IN HEMODIALYSIS
Psychiatric Observations
All the psychiatric observations were carried out by one
of the authors. After the initial psychiatric examination,.the
assessment of the studied personality traits was recorded.
The amount and depth of the observations varied from
patient to patient. One group (15 out of the 43 patients
examined) was on dialysis in the Hadassah University
Hospital and had all received individual psychotherapy of
varying intensity as described elsewhere (8, 9). Thes e p a-
tients had been on dialysis from 1 to 5 years. Th e other 28
patients were studied in five other centers as part of a studyon prediction of adjustment to dialysis, and they all un-
derwent a psychiatric evaluation before the beginning of
dialysis, as well as follow-up examinations at 6-month in-
tervals.
Assessment of Compliance or
Noncompliance With the Medical
Regimen
This assessment was done at 6-month intervals, begin-
ning half a year.after the start of dialytic treatment. All the
patients were assessed in a similar way by one of the au-
thors.
The patients underwent a physical checkup, and their
biochemical data was taken from the medical chart. Com-pliance to the dietary regime—ie, compliance to water, po-
tassium and salt restrictions, as well as the total caloric and
protein intake, was evaluated. As protein restriction and,
therefore, caloric intake is not so much of a problem in this
country (compared to normal dietary habits), compliance
with the diet was determined by compliance with the re-
strictions on the first three items.
Adherence to the restricted fluid intake was mainly de-
termined by the weight gain between two dialyses over the
last 3 months. Similarly, the predialysis potassium level
gave us a measurement of adherence to potassium restric-
tion. Success in keeping to sodium restriction was estimated
mainly by observing prc- and postdialysis blood pressure
measurements together with the weight gain.
The overall compliance to diet was determined accordingto a quite accurately defined five-point scale ranging from
excellent adherence to great abuse.
Except for adherence to diet, we had to rely mainly on
patients' reports on compliance with their regimen, such as
taking or not taking medicines or refusing surgical inter-
vention. Some such examples will be brought up here, but
as there are no objective quantitative methods for measur-
ing compliance in these areas, no statistical information will
be reported.
Grading of compliance with the diet was according to the
following definitions.
Excellent. Weight gain between dialyses is never
above 500 g. Predialysis serum potassium levels are never
above 6 mEq/liter and most of the time less. Predialysis
BUN levels are steady.
Good. Weight gain between dialyses is from 500 to
1000 g. Predialysis potassium levels are usually 6 mEq/
liter or less, occasionally going up to 6.5 mEq/liter.
Predialysis BUN levels are usually steady but may show
occasionaljumps.
Fair. Weight gain between dialyses is mostly 1000 to
1500 g, rarely going up to 2000 g. Predialysis potassium
levels arc from 6.0 to 6.8 mEq/liter.
Some abuse.Weight gain between dialyses is from
1500 to 2000 g, occasionally going up to 2500 or even 3000
g. Predialysis potassium levels are most of the time near 7.0
mEq/liter.
Great abuse. Weight gain between dialyses is always
above 2000 g, or most of the time above 2500 g. Predialysis
potassium levels are frequently above 7.0 mE q/lite r.
RESULTS
On the whole, adherence to the diet seemedto be rather poor; about half of the patientscould be regarded as abusers of this aspect of themedical regimen. In assessing the 43 patients'
adherence to the diet, 5 were regarded as excel-lent adherers, 10 were good, 8 were fair, 13 in-dicated some abuse, and 7 indicated greatabuse.
Because of the small number of patients, theywere divided into two subgroups for all furtheranalysis. Th e patients classified in the firstthree categories—excellent, good and fair—were referred to as good adherers, and those inthe other two categories were regarded asabusers of the diet. Of the 10 patients who died,8 w ere abusers.
The diet is a continuous source of frustrationto the patients; the fluid restriction is thehardest for them. They often report trying tokeep occupied all day long in order to avoiddrinking, and they day-dream about the "Cokein the fridge." Even the patients who do adherewell to this restriction say that it is difficult andthat they are thirsty most of the time. Some pa-tients develop ingenious methods to concealweight increase caused by overdrinking.
Patients also complain about the salt restric-tions, although those who adhere well reportthat they got used to saltless food. The neces-
Psychosomatic M edicine, Vol. 34 , No. 4 (July-August 197 2) 33 5

8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 4/12
DE-NOUR & CZACKES
sary low potassium intake is difficult for only afew patien ts.
It is suggested that the following factors,either alone or in combination with other fac-tors, lead to the abuse of diet and other medicalrecommendations: a) low frustration toleranceor little ability to delay gratification; b) actingout (usually of hostility); c) denial of sick role;d) excessive gain from sick role; e) suicidal be-
havior; f) homicidal behavior (usually by fami-ly); g) superstition, prejudices and body imageproblems.
In the present study these factors were se-lected for further observation on the basis of in-formation and impressions gathered from regu-lar psychotherapy with a few patients, as partlyreported in earlier studies (8-10).
Low Frustration Tolerance
Patients with low frustration tolerance usu-ally claim that they know and understand the
restrictions but that they simply cannot keep tothem. They swear that they try very hard butjust cannot, and their behavior on dialysis ischaracterized by brief periods of fair to goodadherence, which usually occur after a warningfrom the physician or after ill health resultingfrom their abuse of the diet. This fear, however,is not strong enough to balance their low frus-tration tolerance for an extended period of time,and they go back to abuse of the diet. These pa-tients are usually preoccupied with food anddrink and try to make dialysis hours into orgiesof drinking and eating forbidden foods. They
are also the patients who are most inclined tocheat and try to hide their abuse of the diet.
This low frustration tolerance can be seenalso in other areas of their life—they are impa-tient, they get angry when they have to wait.Their (predialysis) work history often showstroubles like coming irregularly to work orgoing off in the afternoon because they "had togo to the movies."
Except for their difficulties with the diet,many of these patients are quite happy ondialysis. Their functioning, however, is usually
poor. From the material collected so far, lowfrustration tolerance seems to be a most com-mon factor. It was found in 17 of the 20 abusersof the diet, and to a milder degree in only 8 ofthe 23 nonabusers.
Acting Out
The term "acting out" is used here to de-scribe behavior expressing an unconscious psy-chic condition—eg, emotions, memories. Thepatient does not realize and has no insight intothe fact that this behavior is caused by uncon-scious factors. Furthermore, in psychiatry oftoday, acting out is regarded as a commonmethod of reducing anxiety and/or guilt whichwould have been felt if the emotions were tobecome conscious.
In the present group of dialysis patients two"kinds" of acting out were observed, one ofwhich expressed unconscious hostility and ag-gression. In some of the patients with this kind
of acting out, it appeared only in flare -ups,while in others it was more repetitious andchronic. Less common was behavior expressingunconscious striving for independence. Thissecond type of acting out did not, on the whole,come in outbu rsts but was chronic.
Acting out of aggression, often directedagainst the team and at times against the fami-ly, can also cause abuse of the diet. One of ourbest patients has always had an "irresistibleimpulse" to take salty foods when eating withhis mother—the mother who had refused tocooperate with a home dialysis program whichthe patient badly wanted. Frequently one seespatients who, when coming for dialysis andbeing told that there has been a technical hitchand that they have to wait for a couple of hours,are later found in the cafeteria on a "drinkingspree"; or the patients who find that their"special nurse" cannot connect them to themachine on that same day and who suddenlybecome terribly thirsty; or the patients whobecome abusers of the diet when their physiciangoes on a vacation.
The characteristic pattern of the acting-out
336 Psychosomatic Medicine, Vol. 34, No . 4 (July-August 197 2)

8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 5/12
PERSONALITY FACTORS IN HEMODIALYSIS
patients is that at least some of them adhere in
general rather well to the diet, but they have
occasional periods of abuse. Most of the time
something has happened before such an attack,
to which other people would react with overt
anger and aggression. Some, however, continue
with this acting out for prolonged periods of
t ime. These are usually people with a high level
of aggression and little ability to express it ver-
bally, often with marked passive-aggressivet ra i ts .
Much less common is abuse of the diet as a
result of acting out of independence problems.
One young patient, for whom the dependency
of dialysis was very difficult, refused to report
on his weight before and after dialysis. As long
as he was pressed to give this information, he
not only abused the diet but also reported on
even greater abuse than the actual one. Once
the fight around that issue was stopped he
seemed to keep better to his diet and has been
doing extremely well on dialysis for a numberof years already. Another patient declared, "I
am not going to be ruled by this monster." As
this patient had an obsessive compulsive per-
sonality, he decided for himself on a given de-
gree of abuse of the fluid restriction, and he re-
ligiously adhered to it.
The acting-out patients may at times reach
the extreme of not coming to dialysis, as hap-
pened with 1 patient who will be described
briefly later on in this report.
Acting out seems to be a frequent phen om-
enon in dialysis patients and was found in 24
of the 43 patients studied.
Denial of Sick Role
Naturally, patients on dialysis realize that
their lives depend on this treatment. Some of
them, however, deny the severity of their con-
dition. For these patients it is hard to accept not
merely the dependency of dialysis but also the
fact that they are ill. This denial may lead to
abus e of the medical regim en and is often most
pronounced in the area of taking medicines—
eg , not taking (or taking irregularly) prescribed
antihypertensive drugs. They are also inclined
to argue that they do not need such prolonged
dialysis and ask to have it reduced.
These patients are rather easy to identify by
their history. They have usually avoided going
to physicians and tried to dissimulate and carry
on even when feeling quite ill. They have
thought that "half the dose of antibiotics is
more than enough" and often have the attitude
that physicians and medications should be
avoided altogether. On dialysis they often con-
tinue dissimulating and, when asked about how
they feel, reply "fine , fine."
As part of their denial of being ill they are
often "ideal patients." They ask for little at-
tention from the nursing staff and continue to
function in everyday life on a very high level.
Excessive Gain From Sick Role
The group of patients described here is the
exact opposite of the one described above. Some
dialysis patients get, or try to get, secondarygain from their condition—more attention, so-
cial benefits from society, etc. This tendency for
secondary gain, which is rath er common in
chronic patients, may cause or increase abuse of
the medical regimen.
There are some patients for whom dialysis
does not create problems but for whom it solves
predialysis conflicts. These patients do not
want, usually unconsciously, to "get well" and
thus have to face their problems again, and this
might lead to their abuse of the medical reg-
imen. An example of this is the patient who
has been frigid all her married life and for
whom this frigidity turned into active disgust of
sexual relations after the birth of her second
child, followed by many guilt feelings towards
her devoted and considerate husband. On
dialysis she complained of being unable to re-
sume "normal family relat ions." From the
above it is clear that every effort to convince her
to increase her caloric intake would be in vain.
Another form of primary gain is seen in pa-
tients who use their "sick condition" to solve, to
a cer tain degree, their dependency- independ-
Psychosomatic Medicine, Vol. 34, No. 4 (July-August 1972) 337

8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 6/12
DE-NOUR & CZACKES
ency problems.It can be said, therefore, that for some pa-
tients being ill has the primary gain of solvingconflicts and reducing anxiety. They thereforeensure their state by a continuous, steady abuseof the medical regimen, usually of the diet.
Suicidal Behavior
Some patients, though not many, accordingto our findings, abuse the medical regimen as aresult of suicidal tendencies. They drink toomuch, they eat forbidden foods and often saythey are "fed up." In our opinion, in order tosay that a patient's behavior is suicidal by in-tention (and not merely harmful in its results)there should be additional signs or symptomsthat the patient is "fed up"—eg, narrowing ofinterests, withdrawal from interpersonal rela-tions, decrease in future planning, depressiveaffect or its equivalent in increased physical
complaints or its projection to "others suffer somuch from me, others are fed up with me." Webelieve that abuse of diet only should not be re-garded as suicidal behavior if there is no con-comitant reduction in other areas of self-care.Among the 43 patients included in this studythere have been a number with verbalized sui-cidal thoughts. These usually took the form of,"I do not think such a life is worth living; if Xhappens (eg, inability to work, rejection bypartner, etc.) I will kill myself," or inquiry intohow many sleeping pills are necessary "to makeit foolproof." Some of these patients were
among the best in their compliance with themedical regimen. The only case of death webelieved to be suicide (slipped shunt) was thatof a woman who was perfect in her adherenceto the medical regimen. The treating physicianin that unit is of the opinion that it was an acci-dent—we are of the opinion that it was suicideas she had voiced her intentions—"One day Iwill find the courage"—and because some of theother manifestations described before werepresent.
We realize that we are describing here an
extreme contradiction: good or excellent ad-herence to a medical regimen in patients ex-pressing suicidal thoughts. Though not veryfrequent, we found it often enough to motivatethe present study, feeling that not all abuse of amedical regimen can be regarded as suicidal.
We have therefore limited the term "sui-cidal" to those patients whose behavior showsconscious or unconscious death wishes. Ex-
cluded, therefore, was the so-called demonstra-tive suicidal behavior which is manipulation ofthe surrounding. These patients were includedin the excessive (secondary) gain group.
Homicidal Behavior Against the Patient
It has been said already that when a patientattempts or commits suicide the question shouldnot only be, "Whom did the patient want topunish?" or "Whom did the patient want tokill?" but sometimes we should also ask thequestion, "Who wanted the patient dead?" We
believe this to be true in psychiatric patientsand often striking in dialysis patients, as in thefollowing examples.
An adolescent daughter of a divorced man on dialysis
came in for a consultation about her father. She described
her father's physical suffering (caused by his abuse of the
water restriction and being on and over the verge of pul-
monary edema) and his being unhappy, hopeless and de-
pressed. She continued by describing her devotion to him.
When asked what she does when her father does not feel
well she described giving him big glasses of the lemonade
that he likes, fixing him his favorite dinner of a large steak
and trying to cheer him up. We asked if she realized the
damage of such a treatment and her answer was, "He must
have some pleasure in life—maybe he would be better offdead."
A more extreme example is that of a 21-year-old patient
who was seen before start of dialysis. The prediction was
that there would be many troubles on dialysis because of the
miserable comb inat ion of extremely low frustra t ion
tolerance and very high tendencies for acting out, which
would result in extreme abuse of the medical regimen.
Transplantation was therefore preferred (also by the pa-
tient) and as there are few cadaver transplantations in our
hospital, the patient's family, a widowed mother and an
older brother, were interviewed. After some discussion each
one was ready to admit that he/she really did not want to
donate a kidney, but they objected even more strongly to the
other one's giving a kidney. The summary of the mother
33 8 Psychosomatic Me dicine, Vol. 34 , No. 4 (July-August 1 972 )
8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 7/12
Te3PoeofA
soDe
Me
sm
Cmpa
whde
Cmpawh
ohmec
remme
o
B
oo
days
Peays
b
o
F
on
Lwuao
toea
Ano
A
whs
Fog
p~o
whaa
eosa
oa
ae
Gcmpa
U
yaao
n
mpa
C
n
Vae
D
o
scoe
Fto mi
da
N
mpa
Dsmuao
osen
oehg
aey
Pmay
Scd
s
ygn
bo
Midcoc
Sea
a U
yg
Sea
Vaeoe
Wihaw
rea
pc
cmpans
de
Iea
Hoyo
Dsmuao
Vae
Vae
fuon
poemsn
opc
h
n
poems
aeo
U
yp
Vae
Vyh
De
Dn

8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 8/12
DE-NOUR & CZACZKES
was, "I am really scared of giving a kidney, but I naturally
want to save my son and of course I do not want two crip-
pled boys, so it should be my kidney." The older brother
stated the same opinion, though in a more sophisticated
way. They were therefore not accepted as potential donors.
At the end the patient was accepted for dialysis in another
unit. His abuse of the diet was extreme and his physical
condition, as a result, was very bad. He continued to exert
pressure on his family that he needed a transplantation.
The team tried very hard to convince him to adhere to the
diet and the other p atients joined in their efforts. After a
stormy argument—"You must keep the diet"—"I justcannot keep the diet, I must have a transplantation"—he
left the hospital and did not come back for his next dialysis.
The family was called in, and at first they disclaimed
knowledge of his whereabouts but later explained that they
had found a physician who could cure him without dialysis.
Some 12 days later the patient came to the emergency ward
of another hospital in severe pulmonary edema and died
before dialysis could be started.
From these, as well as from other less ex-treme and clear-cut examples, it seems that thefamilies can promote severe abuse of the medi-cal regimen out of their conscious, or more often
unconscious, hostility against the patient. This,we believe, is the main reason why some fam-ilies just cannot understand the importance ofthe diet. The family's abuse of the diet can be avery important factor in the patient's abuse ofthe medical regimen. So far, however, we havenot seen a patient whose abuse of the medicalregimen could be attribu ted only to the family.
Beliefs
Under this heading we include a variety ofillogical and emotional attitudes that may resultin abuse of the medical regimen. Often these
attitudes seem to be connected w ith problems ofbody image. Two excessively hypertensive pa-tients refused nephrectomy point-blank.Though no additional relevant information wasreceived from them, this noncompliance wasprobably caused by their inability to face lifewithout urination, as described elsewhere (10).Another, not psychotic, patient connectedejaculation difficulties with dehydration and"found out" that some overdrinking helped hispotency and ejaculation. We do not feel that weunderstand the psychodynamics of these
phenomena well but suspect that they are re-lated to body image problems and to the psy-chologic significance of urination, for men es-pecially.
Comments
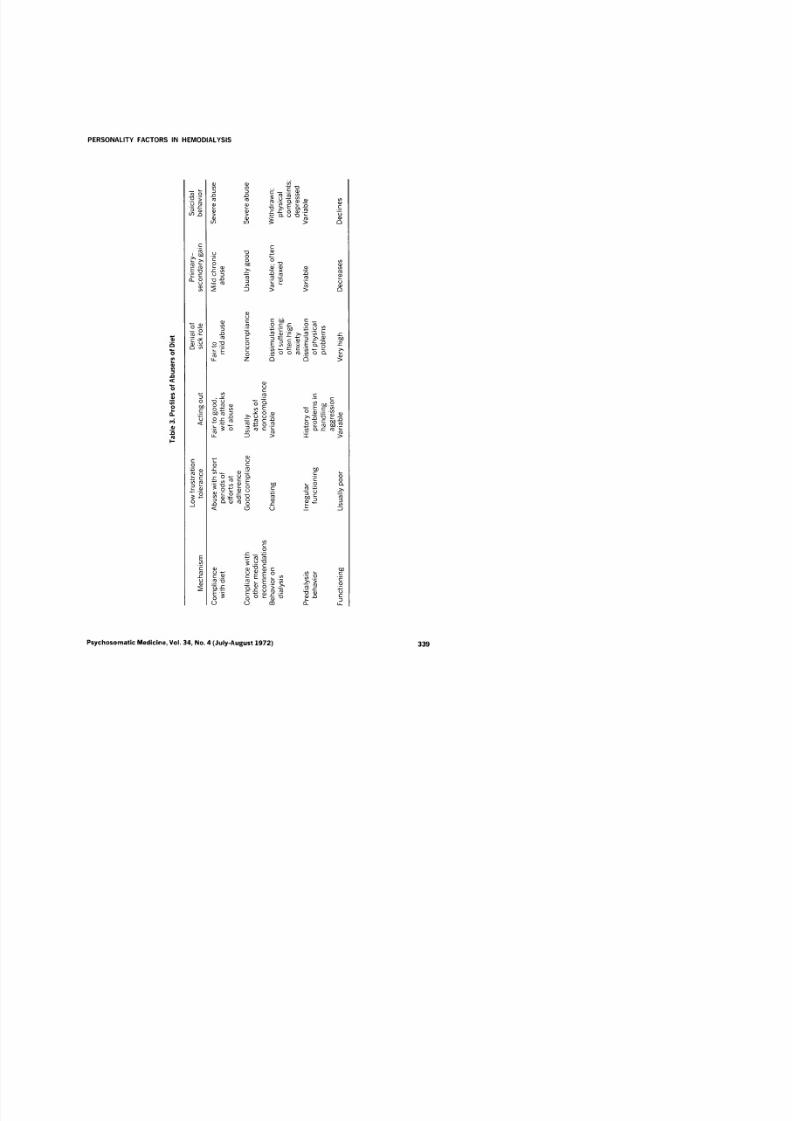
Table 3 summarizes the profiles of the pa-tients in the first five groups, which are more
homogeneous. (In some of the subgroups"variable" was put in to describe behavior,meaning that no clear pattern of behavior wasfound.)
Often, of course, a patient's noncompliancewith the medical regimen is not a result of onefactor but a combination of a number of factors.
The most common factor causing abuse of thediet seems to be low frustration tolerance. Th iswas found to some extent in 25 of the 43 pa-tients studied and seems to differentiate clearlybetween good and bad compliers (the difference
is statistically significant at the .01 level). Act-ing out is another common factor and was foundin 27 of the 43 patients. It differentiated lesswell between compliers and noncompliers, ex-cept that in the second group when acting outwas found it was severe, while in the goodcompliers we often observed mild acting out.
We would like to stress the importance of thefactor named "primary gain." Most reports ondialysis patients concentrate on the stresses ofdialysis and the emotional problems created bydialysis, which is true for many patients. Thereare, however, patients for whom dialysis is a
solution for a long-standing conflict, often in thearea of dependency-independency or activi-ty-passivity. In our group of 43 patients wefound that dialysis to some extent solved emo-tional conflicts for 21, of whom 14 were abusersof the diet. It seems, therefore, that when dialy-sis solves preexisting conflicts, the patient tendsto abuse the diet.
Denial of sick role was not a common findingin this group of patients. It was found in 10 pa-tients only, and in most of them it was notsevere enough to cause abuse of the diet.
340 Psychosomatic M edicine, Vol. 34 , No. 4 (July-August 197 2)

8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 9/12
PERSONALITY FACTORS IN HEMODIALYSIS
Suicidal thoughts were expressed by 11 pa-tients and in only 4 of them did we gain theimpression that the abuse of the diet was alsoinfluenced by suicidal behavior. As describedpreviously, some of the patients expressing sui-cidal thoughts were among the best adherers tothe diet.
No s tatistical information on the frequency ofthe effects of the family on abuse of the diet can
be presented, as we do not know enough aboutthe families of the 28 patients not on psy-chotherapy. About the other 15 patients it canbe said that in 3 of them the abuse of the dietwas to some extent influenced by their families'homicidal wishes. The families of 3 other pa-tients were also loud and clear in their wish toget rid of the patient, but those patients adheredwell to the diet. It therefore seems that a nega-tive, rejecting attitude of the family may be im-portant if and when the patient is ready to actout accordingly, while in other patients thehostility of the family will not influence adher-ence to the diet.
The three more common factors that maycause abuse of the diet are summarized in Table4.
DISCUSSION
We have described the factors that can result
in abuse of the medical regimen of chronic he-modialysis, consisting mainly of a rather strictdiet and, for some patients, of other medical rec-ommendations such as various medications. Noclinical signs of gross brain damage were foundin any of the patients. Signs of organic damagein psychologic tests were found in some of thepatients, but there was no correlation betweenabuse of the diet and signs of organicity. On the
other hand, severe and prolonged abuse of thediet seems to be caused most frequently by lowfrustration tolerance as well as by continuoussevere acting out. Patients for whom the sickrole is problem solving are also likely to abusethe diet.
Like most reports on adjustment to dialysis,those on compliance with the medical regimenof dialysis patients are often contradictory. Tomention two, Bor.kman (2) reported that 32%of patients did not adhere to one or more aspectsof the regimen, while Curtis et al (11) are of the
opinion that, on the whole, the majority of pa-tients gradually come to accept the dietary re-strictions.
In the present study about 45% of the pa-tients were rated as abusers of the diet. Studiesdealing with other patients (usually ambulatorypatients) report on one-third of noncompliers.Davis and Eichorn (4) in their summary of theliterature found the reported range of noncom-
Table 4. Three Com mon Factors That May Cause Abuse of the Diet
Low frus tration toleranceNormal frustration tolerance
Acting outNo acting out
Primary gainNo primary gain
2518
x2
P <
27
16
ns
21
22
Total
= 11.06c.01
No . of patients
Abusers
17
3
12
8
14
6
Nonabusers
815
158
7
16
= 11.34
Psychosomatic M edicine, Vol. 34, No . 4 (July-August 197 2) 341

8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 10/12
DE-NOUR & CZACZKES
pliance to extend from 15 to 93% of the pa-tients. In another study (5) Davis reported that"patients with less severe medical problemswere more likely to follow through with medi-cal advice than those with more severe illness"and that "the greater the effect of the illness onperforming daily activities the less likely wasthe patient to follow doctors' advice." Dialysispatients, therefore, can be expected to be non-
compliers.We regard the rate of abusers in the present
study as high, and this not merely because it ishigher than the accepted third of the patients.Those classified as abusers of the diet werenoncompliers in a striking way. Their non-compliance not only endangered their lives inthe long run but also made them feel physicallybad in the short run. In this aspect dialysis pa-tients are different from most patients studied sofar. Usually the physician tells the patient that"it is not good for you to ... ," but the patient
does not actually feel the harm. The dialysispatient, however, does feel it within a day ortwo. Theoretically, therefore, the immediateresults of dietary noncompliance should haveacted as repeated negative reinforcement andreduced the rate of noncompliance. This, how-ever, has not been found, and we therefore re-gard the rate of noncompliers found in thisgroup of patients as high.
We believe that this high rate of noncompli-ance can be partially attributed to a high levelof aggression. We have repeatedly expressedour opinion that in some or many patients (no
statistical information yet) the dependency ofdialysis and the loss of mastery causes an in-crease in hostility and aggression (8, 9). Few ofthem can express this hostility openly as it isqui te difficult to be aggressive to those on whomone's life depends, irrespective of basic per-sonality. Other patients repress this aggressionbut act it out, while still others introject it anddevelop depression with suicidal behavior, allcumulating in abuse of the medical regimen.
Though often more than one factor wascausing the patients' noncompliance with the
regimen, we suggest that identifying the fac-tor(s) in each individual patient is of utmostimportance, as it should dictate the psycho-therapeutic intervention with each patient,as well as the expectations from such an inter-vention.
Low Frustration Tolerance
Our experience of trying to influence thisfactor by psychotherapy has been very poor.Individual supportive psychotherapy, psy-choanalytic oriented psychotherapy and mobil-izing other patients in a sort of group psy-chotherapy, not to mention pleas and threats,have not helped. It seems that none of thesemethods is effective in either increasing the pa-tient's frustration tolerance or decreasing hisabuse of the diet. Lately we had the idea thathypnotic treatment with posthypnotic sug-gestion might be effective in these patients, butwe have not had a chance to try it out yet.
Acting Out
This factor seems more amenable to psy-chotherapy, specially in the majority of patientswho act out hostility and aggression. In psy-chodynamic psychotherapy the patient can behelped to understand the aggression underlyinghis behavior and find new methods for handlingand expressing it.
The work is somewhat more difficult withthose patients who act out their intolerance oftheir dependent situation. In these cases it
might be helpful to add work with the team tothe orthodox psychotherapy and to find waysand means to decrease the patient's actual de-pendency (12).
The main problem for this whole group is theone described previously (9) of establishing apsychotherapeutic relationship with dialysis(chronic) patients. When and where this can beachieved, there seems to be a good chance thatthe patient's abuse of the medical regimenwould decrease and gradually stop within a fewmonths.
342 Psychosomatic Medicine, Vol. 34, No. 4 (July-August 1972)
8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 11/12
PERSONALITY FACTORS IN HEMODIALYSIS
Denial of Sick Role
When this rather uncommon mechanismcauses abuse of the medical regimen, it creates aproblem because this denial has "positive" as-pects—ie, high functioning and few or no psy-chiatric symptoms. We have been afraid, there-fore, that removal of this denial would make thepatient, on the one hand, comply more but, on
the other hand, become less adjusted to theother aspects of life on dialysis.
Our policy has therefore been that as long asthe noncompliance does not endanger the pa-tient's life, nor is likely to damage his physicalcondition seriously, we should leave wellenough alone. In such cases some work with theteam should be done to enable the team to ac-cept this noncompliance as a method of ad-justment and not as symptoms of foolishness ormanipulation or plain stubborness (12, 13).
Excessive Gain From Sick Role
As described, these patients have a goodamount of primary gain as well as secondarygain from being ill. Their motivation for changeis therefore very limited. To some extent theycould be compared to psychophysiologic pa-tients who also are often resistant to psy-chotherapy. Theoretically, long-term intensivepsychotherapy should be able to help them solvethe basic problems now solved by their sickcondition, but so far ou r limited experience withpsychotherapy has not proved this to be true.
Suicidal BehaviorFrom regular psychotherapy it is well known
that work with suicidal patients, even whenthey are not psychotic, is often difficult. It ishard for the therapist to find a balanced atti-tude. If he is scared of the suicidal potential, thepatient loses all confidence in his ability to con-trol his behavior. If the therapist is notfrightened at all, the patient might be provoked"to teach him a lesson." If the therapist is very"good and supportive," it might increase thepatient's guilt feelings and promote the suicidal
behavior, and if he is not supportive the patientmight see it as rejection with the same outcome.Another problem is the time element—the psy-chotherapeutic work should progress fastenough to prevent actual suicide.
All this is even more true of dialysis patientswith suicidal behavior causing abuse of themedical regimen. The difficulties of establishing
a relationship with dialysis patients in generalhave been described elsewhere (9), and toachieve it with a withdrawn, depressed patientis even harder. Finding the correct approachwith these patients is very difficult because ofthe patient's suspicion that the psychiatrist, likethe rest of the team, will be angry at his behav-ior. Nevertheless, it can be done, and intensivefocused psychotherapy is recommended, to-gether with maximal manipulation of envi-ronment—getting the team, family and workplace to participate.
Homicidal Behavior
In these cases it is useless to work only withthe patient. It seems that working individuallywith the "homicidal family" is also often fruit-less, while family psychotherapy may producethe wished-for results. In any family therapy itmight be difficult for the therapist to remainneutral and avoid taking sides. It is even harderto achieve and retain this neutrality with dialy-sis patients and their families and to avoidblaming the family for their "inconsiderate,nonunderstanding behavior toward the
unhappy and ill patient" and to refrain fromtaking sides with the family against the "de-manding, egocentric patient." Our feeling,however, is that such family therapy can bedone and that it would be helpful to manydialysis families and not only to the few"homicidal" ones.
We would like to suggest that if a patient'snoncompliance with a m edical regimen could bediagnosed according to an outline such as theone presented here, the psychiatrist's interven-tions would be much more rational—more
Psychosomatic M edicine, Vol. 34 , No. 4 (July-August 197 2) 34 3

8/4/2019 Personality Factors in Chronic Hemodialysis Patients
http://slidepdf.com/reader/full/personality-factors-in-chronic-hemodialysis-patients 12/12