Periodontitis as a risk factor for systemic diseases
75
-
Upload
dr-kritika-jangid -
Category
Health & Medicine
-
view
58 -
download
2
Transcript of Periodontitis as a risk factor for systemic diseases


IMPACT OF PERIODONTAL INFECTION
ON SYSTEMIC HEALTH
DR. KRITIKA JANGID(MDS- PERIO)

CONTENTS
PATHOBIOLOGY OF PERIODONTITIS
FOCAL INFECTION THEORY REVISITED
SUBGINGIVAL ENVIRONMENT AS A RESERVOIR OF BACTERIA
PERIODONTAL DISEASE AND SYSTEMIC DISEASES

INTRODUCTION Pathogenesis of Periodontitis


Can the inflammatory response to bacterial infection of the periodontium have an effect remote from the oral cavity???
Is periodontal infection a risk factor for systemic diseases or conditions that affect the human health???

FOCAL INFECTION THORY
William Hunter (1909)- A British physician : Oral micro-organisms were responsible for a wide range of systemic diseases which were not easily recognised as infectious in nature.
Extract rather than restore.
Widely accepted and widespread extraction of teeth.
Frank Billings- Father of theory of focal infection; Coined the term ‘Focal Sepsis’

In 1940s and 1950s
Widespread extraction often of the entire dentition failed to reduce or eliminate the systemic conditions to which the supposedly infected dentition had been linked.
No scientific evidence

FOCAL INFECTION THORY REVISITED
Mechanism of Focal Infection. J Am Dent Assoc, Vol 42, June 1951
Article states clearly that ‘The concept of focal infection in relation to systemic diseases is firmly established.’

Def. By ADA
Focus of Infection: ‘A circumscribed area infected with micro-organisms which may or may not give rise to clinical manifestations.’
Focal infection: ‘Sepsis arising from a focus of infection that initiates a secondary infection in a nearby or distant tissue or organs’.

Mechanism of Focal Infection. J Am Dent Assoc, Vol 42, June 1951
2 major mechanisms of focal infection:
a) An actual metastasis of organisms from the focus
b) The spread of toxins or toxic products from a remote focus to other tissues by the blood stream


Mechanism of Focal Infection. J Am Dent Assoc, Vol 42, June 1951
Once the infection passes about the tooth:
a) They may multiply in the blood setting up an acute or chronic septicaemia.
b) They may be carried live to a suitable nidus where they infect the surrounding tissues.
c) They may produce a slow but progressive atrophy with replacement fibrosis in various organs of the body.

Organ Systems or Conditions possibly influenced by Periodontal Infection
CVS› Atherosclerosis› CHD› Angina› MI
Cerebrovascular system› Stroke
Endocrine System› DM
Reproductive System› Pre-term LBW infants› Preeclampsia
Respiratory System› COPD› Acute Bacterial Pneumonia

CVS


Pathophysiology of CHDEndothelial injury
Surface adhesion molecules (Endothelial cells)
Monocyte adhesion by MCP-1
Macrophage in intima layer of vessel wall
Secrete GF, Cytokines
Smooth muscle proliferation in vessel wallStimulate endothelial cells
Accumulate LDL
Progressive oxidation
Lipid peroxidases
FOAM CELLS, FATTY STREAK

Fatty Streak
Complex fibrous plaque with lipid core (Along
with extra cellular proteins)
Attached to vessel wall


MI
Fibrotic Plaque (thin)
Ruptures
Activation of clotting system
Thrombus formation
MI

CHD
Periodontitis as a risk factor for CVS diseases


Animal model
Inbred mice when challenged orally or IV with invasive strains of P.g, increased aortic athrosclerosis. Li et al (2002), Lalla et al (2003), Chi et al
(2004), Gibson et al (2004)



Biological Rationale

Role of Sub-gingival plaque


4 Pathways
1. Direct bacterial effects on platelets2. Auto-immune responses3. Invasion and/or uptake of bacteria in
endothelial cells and macrophages4. Endocrine like effects of pro-
inflammatory mediators

Direct bacterial effects on platelets
2 oral bacteria P.g. and S. Sanguis express virulence factors called ‘Collagen- like platelet aggregation associated proteins” (PAAP) that induce platelet aggregation in vitro and in vivo.(Hertzberg 1996 & Meyer 1998)

Auto-immune responses
Antibodies that cross react with periodontal bacteria and human heat shock proteins have been identified. (Hinode et al 1998 and Sims et al 2002)
Invasion and/or uptake of bacteria in endothelial cells and macrophages
Deshpande et al (1998) have demonstrated that P.g. can invade aortic and heart endothelial cells via fimbriae.
Chui et al (1999) and Haraszthy et al (2000) have idntified specific oral pathogens in atheromatous tissues.
Giacona et al (2004) demonstrated that macrophages incubated in vivo with P.g. and LDL uptake the bacteria intracellularly and transform into foam cells.

Endocrine like effects of pro-inflammatory mediators
Systemic pro-inflammatory mediators are up-regulated for effects in vascular tissues
Elevation in CRP and fibrinogen consistently seen among periodontally diseased subjects.(Slade et al 2000, Wu et al 2000)


Role of Obesity

Stroke/ Ischaemic Cerebral Infarction


Periodontitis as a risk factor for Stroke






Biological Rationale


Direct bacterial challenge
Persistent bacterial challenge to the arterial
endothelium
Monocyte macrophage driven inflammatory process
Atheromatosis
Narrowing of vessel lumen

Indirect Systemic effects
Elevated production of fibrinogen and CRP
Atheroma formation

Platelet aggregation
Platelets selectively bind with some strains of S. Sanguis and P.g.
Aggregation of platelets is induced by Platelet aggregation associated protein (PAAP) expressed on some strains of these bacteria
Thrombus formation Thromboembolism Stroke

Diabetes
Retinopathy Nephropathy Neuropathy Macrovascula
r disease Altered
wound healing
Periodontal disease

Periodontitis as a risk factor for Diabetes



Conclusion
Biological Rationale

Gram negative periodontal
infection
Increased insulin
resistance
Worsened glycaemic
control
Periodontal treatment
Decreased inflammation
Improved insulin sensitivity
Improved glycaemic control

ADVERSE PREGNANCY OUTCOMES

LBW babies
<2500g at birth Vaginal colonisation with group B
streptococci or Bacteroides species increases the risk of premature rupture of membrane, preterm delivery and LBW infants.
Prostaglandins, proinflammatory cytokines (IL-1, IL-6, TNF-α) have been found in the amniotic fluid of women with pre-term labor.

Detection of Oral microbes
Culture positive amniotic fluid, isolated F. nucleatum in preterm labor
Hill GB (1993) found F. Nucleatum to be closely matched to those found in subgingival plaque than in the lower genital tract.
Occasional isolation of Capnocytophaga in amniotic fluid in preterm labor

2 Possible route of spread
Haematogenous spread
Oral-genital contact

Pre-eclampsia

Periodontitis as a risk factor for Adverse Pregnancy Outcomes



Biological Rationale

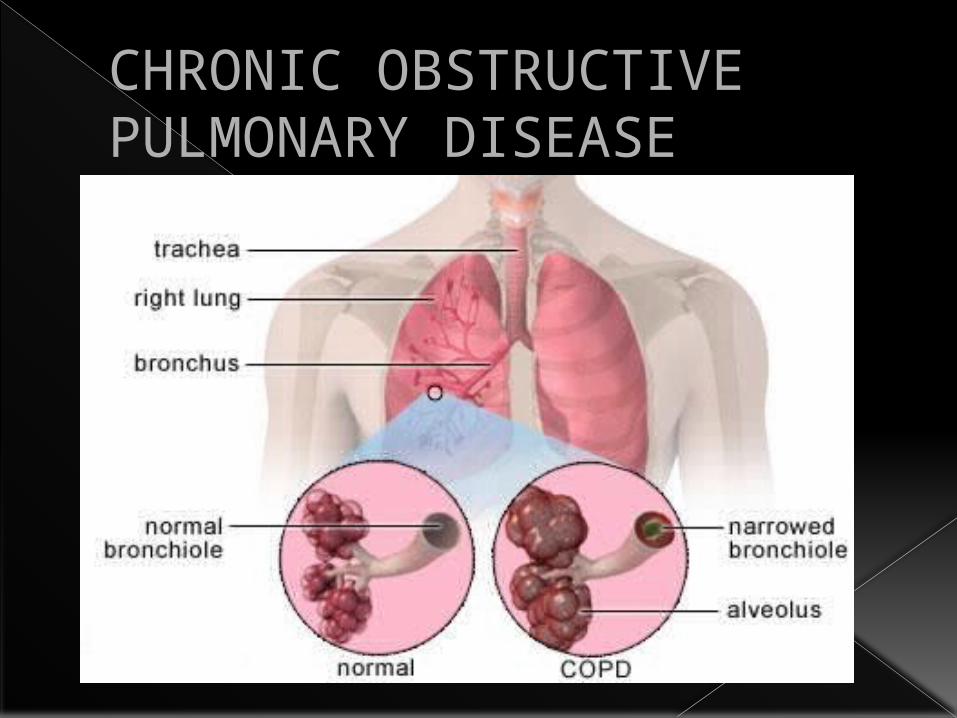
CHRONIC OBSTRUCTIVE PULMONARY DISEASE


Periodontitis as a risk factor for COPD


Biological Rationale