
Neuro -ventilatory Coupling Neurally Adjusted … to improving lung compliance during Respiratory...
8
10/10/2012 1 NAVA Neurally Adjusted Ventilatory Assist In Neonates Toledo Children’s Hospital Toledo, Ohio Howard Stein, M.D. Neonatologist Disclaimers Dr Stein: Is discussing products made by Maquet Has no commercial interest in NAVA or Maquet Has received no financial support or incentives from Maquet to use NAVA or collect this data Toledo Children’s Hospital 151 bed hospital Level 3 NICU 60 beds Inborn – 70% Outborn – 30% 2011: > 800 admissions/year Average daily census 40 – 45 patients C entral nervous system Phrenic nerve Diaphragm excitation Diaphragm contraction C hest wall and lung expansion ∆ Airway pressure, flow and volume Neuro-ventilatory Coupling Adapted from S inderby, Nature Med 1999 Central nervous system Phrenic nerve Diaphragm excitation Nasogastric tube Ventilator Unit Diaphragm contraction Assisted Breath Chest wall and lung expansion Airway pressure, flow and volume Adapted from Sinderby, Nature Med 1999 How NAVA works Conventional Ventilation Patient Controls using Flow Trigger: Initiation of Breath Rate (in some modes) Ventilator Controls: Peak Pressure or Tidal Volume Inspiratory Time Termination of Breath PEEP Minimum Rate FiO2 Synchrony: Only for Initiation of Breath NAVA Ventilation Patient Controls using Neural Trigger: Initiation of Breath Inspiratory Time Rate Peak Pressure Termination of Breath Ventilator Controls: FiO2 PEEP NAVA Level Apnea time (minimum rate) Peak Inspiratory pressure alarm Synchrony: Initiation of Breath Size of Breath Termination of Breath
Transcript of Neuro -ventilatory Coupling Neurally Adjusted … to improving lung compliance during Respiratory...

10/10/2012
1
NAVA
Neurally Adjusted Ventilatory Assist
In Neonates
Toledo Children’s Hospital Toledo, Ohio
Howard Stein, M.D. Neonatologist
Disclaimers
Dr Stein:
Is discussing products made by Maquet
Has no commercial interest in NAVA or Maquet
Has received no financial support or incentives from Maquet to use NAVA or collect this data
Toledo Children’s Hospital 151 bed hospital
Level 3 NICU 60 beds
Inborn – 70% Outborn – 30% 2011: > 800 admissions/year Average daily census 40 – 45 patients
C entral nervous s ys tem
P hrenic nerve
Neural Trigger
Diaphragm excitation Ventilator Unit
Diaphragm contractionFlow Trigger
C hes t wall and lung expans ion
Assisted
∆ Airway pres sure, flow and volume Breath
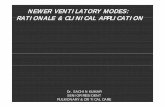
Neuro-ventilatory Coupling
Adapted from S inderby,Nature Med 1999
Central nervous system Phrenic nerve Diaphragm excitation Nasogastric tube Ventilator Unit Diaphragm contraction Assisted Breath Chest wall and lung expansion Airway pressure, flow and volume
Adapted from Sinderby, Nature Med 1999
How NAVA works Conventional Ventilation
Patient Controls using Flow Trigger: Initiation of Breath Rate (in some modes)
Ventilator Controls: Peak Pressure or Tidal Volume Inspiratory Time Termination of Breath PEEP Minimum Rate FiO2
Synchrony: Only for Initiation of Breath
NAVA Ventilation
Patient Controls using Neural Trigger: Initiation of Breath Inspiratory Time Rate Peak Pressure Termination of Breath
Ventilator Controls: FiO2 PEEP NAVA Level Apnea time (minimum rate) Peak Inspiratory pressure alarm
Synchrony: Initiation of Breath Size of Breath Termination of Breath

10/10/2012
2
1. Beck J, Tucci M, Emeriaud G, Lacroix J, Sinderby C. Prolonged neural expiratory time induced by mechanical ventilation in infants. Pediatr Res 2004, 55: 747-754.
2. Emeriaud G, Beck J, Tucci M, Lacroix J, Sinderby C. Diaphragm electrical activity during expiration in mechanically ventilated infants. Pediatric Research 2006;59:705-10.
2008 – FDA Approval
3. Beck J, Reilly M, Grasselli G, Mirabella L, Slutsky AS, Dunn MS, et al. Patient-ventilator interaction during neurally adjusted ventilatory assist in low birth weight infants. Pediatr Res 2009, 65: 663-668.
4. Zhu L, Shi Z, Ji G, et al. [Application of neurally adjusted ventilatory assist in infants who underwent cardiac surgery for congenital heart disease]. Zhongguo Dang Dai Er Ke Za Zhi 2009;11:433-6.
5. O'Reilly R, Freir N, Healy M, O'Hare BP. A case series: Nava and congenital diaphragmatic hernia. Am J Respir Crit Care Med 2009;179:A5820.
2004
Published Neonatal and Pediatric Studies
2006
2009
6. Breatnach C, Conlon NP, Stack M, Healy M, O'Hare BP. A prospective crossover comparison of neurally adjusted ventilatory assist and pressure-support ventilation in a pediatric and neonatal intensive care unit population. Pediatr Crit Care Med 2010, 11: 7-11.
7. Stein HM. NAVA ventilation allows for patient determination of peak pressures facilitating weaning in response to improving lung compliance during Respiratory Distress Syndrome: A case report. Neonatology Today 2010, 5: 1-4.
8. Bengtsson JA, Edberg KE. Neurally adjusted ventilatory assist in children: An observational study. Pediatr Crit Care Med 2010, 11: 253-257.
9. Durrani N, Chedid F, Rahmani A. Neurally Adjusted Ventilatory Asist Mode Unsed in Congential Diaphragmatic Hernia. Journal of the College of Physicians and Surgeons Pakistan. 2010, Vol. 21 (10); 637-639.
10. Wolf G, Walsh B, Green M, Arnold J. Electrical activity of the diaphragm during extubation readiness testing in critically ill children. Pediatr Crit Care Med 2010;12:e220-4.
11. Vitale V, Ricci Z, Morelli S, et al. Neurally adjusted ventilatory assist and lung transplant in a child: A case report. Pediatr Crit Care Med 2010;11:e48-e54.
12. Alander M, Peltoniemi O, Pokka T, Kontiokari T. Comparison of Pressure-, Flow-, and NAVA-Triggering in
Pediatric and Neonatal Ventilatory Care. Pediatric Pulmonology 2011: 1 -8. 13. Beck J, Reilly M, Grasselli G, Qui H, Slutsky AS, Dunn MS, et al. Charaterization of neural breathing
pattern in spontaneously breathing preterm infants. Pediatr Res 2011, 70: 607-613. 14. Liet J, Dejode J, Joram N, Gaillard-LeRouz B, Roze J. Respiratory support by neurally adjusted ventilatory
assist (NAVA) in severe RSV-related bronchiolitis: a case series report. BMC Pediatrics 2011;11.
15. Clement K, Thurman T, Holt S, Heulitt M. Neurally triggered breaths reduce trigger delay and improve ventilator response times in ventilated infants with bronchiolitis. Intensive Care Med 2011 September 23.
Published Neonatal and Pediatric Studies
2010
2011
17. Stein HM, Howard D. Neurally Adjusted Ventilatory Assist (NAVA) in Neonates less than 1500 grams: A Retrospective Analysis. J Pediatr 2012 160: 786-789.
18. Stein HM, Burton J, Wilmoth J. Electrical Activity of the Diaphragm Values in a Small Cohort of Term Neonates. Resp Care 2012 ; 57(9) 1483-7
19. Bordessoule A, Emeriaud G, Morneau S, Jouvet P, Beck, J. NAVA improves patient-ventilator interaction in infants compared to conventional ventilation. i Pediatr Res. 2012 May 11. [Epub ahead of print]
20. Lee J, Kim H, Sohn J, Choi C, Kim E, Kim B, et al. Randomized crossover study of Neurally Adjusted Ventilatory Assist in preterm infants. J Pediatr 2012, in press,
21. Stein H, Alosh H, Ethington P, White D: Prospective Crossover Comparison Between NAVA and Pressure Control Ventilation in Premature Neonates Less Than 1500 Grams - J Perinatol, in press
22. Stein H, Davis K, Hall R, White D: Electrical Activity of the Diaphragm (Edi) Values and NAVA Nasogastric Catheter Placement in Non-Ventilated Preterm Neonates - J Perinatol in revision
Published Neonatal and Pediatric Studies
2012 Samples sizes : 1 (case reports) – 52 patients
(retrospective review)
Time on NAVA: 5 min – 24 hours
Age: 26 weeks – teenagers
Weight: ~ 550 grams – ~ 55 kg
Published Neonatal and Pediatric Studies
NAVA ventilation has been reported in patients with :
– Congenital heart disease
– Respiratory Distress Syndrome
– Chronic Lung Disease
– Congenital Diaphragmatic Hernia
– Respiratory Syncytial Virus
Published Neonatal and Pediatric Studies
Published Neonatal and Pediatric Studies
NAVA improved patient-ventilator interaction and synchrony in neonates even in the presence of large air leaks.
Peak inspiratory pressures decreased when changing from conventional ventilation to NAVA.
Respiratory rate increased on NAVA in some studies and decreased or remained the same in others.
Blood gases improved on NAVA in some studies and remained the same in others.
No change in mean airway pressure.
No adverse events were noted while on NAVA.

10/10/2012
3
Toledo Children’s Hospital
NAVA - May 2008 NIV NAVA – July 2010
Over 500 neonates on NAVA/NIV NAVA
Over 25 pediatric patients on NAVA
Used NAVA/NIV NAVA in patients with:
– RDS CLD
– PPHN (NO) CHD
– Pneumothorax Pleural Effusion
– Gastroschisis Oomphalocele
– HIE with cooling
Is SIMV (pressure control) in premature infants really
‘synchronized’?
SIMV (pressure control) in a 3 week old ex 26 week infant with CLD shows evidence of flow triggering (purple lines).
SIMV (pressure control) with EDI superimposed shows the lack of synchrony on the flow triggered breaths
SIMV (Pressure Control) in an ‘Apneic’ neonate
‘Apnea’ - Failure to trigger

10/10/2012
4
Is the Neural Trigger
Synchronous?
Data from Toledo Children’s Hospital’s NICU
Normative Edi data
– Term neonates
– Premature neonates
Retrospective review of neonates < 1500 grams on NAVA
Prospective controlled study in VLBW neonates between NAVA and PC
Term Neonates with no active respiratory problems and feeding normally
0
5
10
15
20
Edi Peak Edi Min
Overall
Awake
Asleep
Pre parandial
Feeding
Post parandial
* *
* P < 0.05
Stein ,Wilmoth and Burton J Resp Care 2012, 57(9): 1483-7
Normative Edi Data
Premature neonates off mechanical ventilation
– HFNC (3 - 6 lpm)
– NC (0.5 - 2 lpm)
– RA
0
5
10
15
20
26 27 28 29 30 31 32 33 34 35 36
Gestational age (weeks)
Ed
i (m
cV
)
Edi peak
Edi min
Normative Edi Peak and Min at various gestational ages in non-ventilated
premature neonates
0
2
4
6
8
10
12
14
16
18
20
26 27 28 29 30 31 32 33 34 35 36
high Flow Nasal Cannula Nasal Cannula Room Air
Gestational age (weeks)
Edi
(mcV
)
Edi Peak Edi Min
Respiratory support and Edi Peak and Min over gestational age
Stein, Davis and Hall 2011

10/10/2012
5
52 Neonates
–31 RDS
–21 CLD
Gestational age: 26.3+2.6 weeks
Birth weight: 837+271 grams
Age at study: 15+15 days (range 0-50 days)
Weight at study: 958+294 grams
NAVA in Neonates < 1501 grams
Stein HM, Howard D. Neurally Adjusted Ventilatory Assist (NAVA) in Neonates less than 1500 grams: A Retrospective Analysis. J Pediatr 2012 160: 786-789.
NAVA in Neonates < 1501 grams Results
17.1
13.6 13.4 13.3 12.6
32
27
25 26
28
5
10
15
20
25
30
35
SIMV/PC 1 hour 4 hours 12 hours 24 hours
PIP
FiO2
. p < 0.05 for all values compared to SIMV/PC
NAVA in Neonates < 1501 grams Results
. p < 0.03 for all values compared to SIMV/PC
7.29
7.32
7.34
7.27
7.29
7.31
7.33
7.35
7.37
SIMV/PC 1 hour 24 hours
pH < 7.35 (33/49)
54
50
47
40
45
50
55
SIMV/PC 1 hour 24 hours
pCO2 > 45 (33/49)
NAVA Versus Pressure Control
First prolonged prospective study in VLBW neonates
NAVA ventilation for 4 hours
Pressure Control ventilation for 4 hours
Cycle repeated for 24 hours
4 hours NAVA
4 hours PC
4 hours NAVA
4 hours NAVA
4 hours PC
4 hours PC
Results
5 neonates with CLD were studied
– 15 changes from NAVA to PC
– 10 changes from PC to NAVA
Gestational age: 26.2 + 0.8 weeks
Birth weight: 810 + 245 grams
Age at study: 24 + 10 days
Stein. Alosh , Ethington and White 2012 J Perinatol – in press
54.4
56.3 55.7
60.6
58 57.9
50
52
54
56
58
60
62
interval 1 interval 2 interval 3
Tc pCO2 (mmHg)
15.6
14.6 14.6
16.8 16.7 16.4
14
14.5
15
15.5
16
16.5
17
interval 1 interval 2 interval 3
PIP (cm H2O)
0.33
0.4 0.39
0.21 0.26
0.33
0.1
0.2
0.3
0.4
0.5
interval 1 interval 2 interval 3
Compliance (ml/cmH2O)
NAVA Pressure Control p < 0.05
2.7
3.2 3
2.4 2.5 2.2
1
2
3
4
interval 1 interval 2 interval 3
TV (ml/kg)

10/10/2012
6
38.7
35.3
38.8
39.8 38.3
42.7
32
34
36
38
40
42
44
interval 1 interval 2 interval 3
FiO2 (%)
52.9 52.2
53.1
55.7
57.4 57.1
50
52
54
56
58
60
interval 1 interval 2 interval 3
Respiratory Rate (bpm)
3.5
3.2
2.9 3.2
2.5 2.7
2
2.5
3
3.5
4
interval 1 interval 2 interval 3
Edi min (mcV)
NAVA Pressure Control p < 0.05
10.3 9.2 8.9
13.8
10.8 11.3
5
10
15
interval 1 interval 2 interval 3
Edi Peak (mcV)
NAVA Conclusions In neonates:
Intact neuro-ventilatory coupling with functional feedback pathways.
Ventilate on NAVA with lower PIP, better TV and lower FiO2 then on conventional ventilation.
Improved blood gases on NAVA despite ventilating with lower pressures.
Improved compliance on NAVA.
No adverse events noted while on NAVA.
Non-Invasive NAVA Ventilation
Available since July 2010
About 90 patients treated with NIV NAVA
Uses:
– Prevent intubation
– Facilitate earlier extubation
23 weeks gestation, 650 grams
Intubated in DR and treated with surfactant
NAVA invasively by 2 hours
Extubated at 36 hours to NIV NAVA
Weaned to CPAP on day 8 for 1 day and then to high flow nasal cannula 5 lpm
Case Presentation 1
26 weeks 655 grams
Intubated in the DR and treated with surfactant
Extubated on day 1 to NIV NAVA
On NIV NAVA for 6 days and then weaned to HFNC 5 lpm
Case Presentation 2 Clinical Guidelines
Ventilator settings in NAVA:
– Apnea time
– Peak Inspiratory pressure alarm
– How to set the NAVA level

10/10/2012
7
Apnea Time
Time the neonate is apneic before getting a backup breath
Apnea time can now be lowered to minimum of 2 seconds
– After 2 seconds the neonate gets a pressure control breath
– This allows the user to deliver a minimum
guaranteed back-up rate of 30 breaths/min
Apnea alarm Minimum rate
15 sec 4 breaths/min
10 sec 6 breaths/min
5 sec 12 breaths/min
4 sec 15 breaths/min
3 sec 20 breaths/min
2 sec 30 breaths/min This is different from the backup rate: RR when the
neonate is apneic and getting pressure control
Apnea Time
•Apnea for 5 sec – ventilator gives a backup breath •The backup breath stretches the diaphragm and causes an Edi signal - Heads paradoxical reflex •Signal is not converted into a breath but the apnea timer is restarted •After 5 seconds of apnea the ventilator goes into backup again
Peak Inspiratory pressure alarm
Case presentation:
22 year old G1 at 32 weeks gestation
Primary C-section for maternal PIH
1.8 kg Apgars 7/8
8 minutes developed grunting and retractions – placed on CPAP 5
CXR showed mild to moderate RDS
0
20
40
60
80
100
3:18 4:18 5:18 6:18 7:18 8:18 9:18 10:18 11:18
Edi peak µV
3 - NIV NAVA 2
PEEP 5
PIP Limit 20
4 - NIV NAVA 2
PEEP 5
PIP Limit 40
2 4
2 - NIV PC 14/5, 40
PEEP 5
3
pH 7.05 pCO2 98 BE -8
pH 7.14 pCO2 80 BE -5
pH 7.25 pCO2 56 BE -4
pH 7.30 pCO2 50 BE -3
1
1 - CPAP 5
Respiratory Rate
Peak Pressure
How to set the NAVA level
NAVA level is the proportionality factor that converts the Edi signal into a pressure The higher the NAVA level the more work of breathing the ventilator does The lower the NAVA level the more work of breathing the patient does Goal – to unload the work of breathing from the patient to the ventilator without over assisting the patient The ventilator continues to respond to the patient’s respiratory drive but supports the patient’s respiratory effort

10/10/2012
8
0.5 1
1.5 2
2.5 3
3.5 4
3 6 9 12 15 18 21 24
NAVA Level
Time (minutes)
HR, RR and Sats recorded every 30 sec
BP recorded every 3 minutes
Edi Titration Study – to determine the optimal NAVA level
Edi Titration Study – to determine the optimal NAVA level
0
5
10
15
20
25
30
35
40
45
09:0
3:47
09:0
6:33
09:0
9:57
09:1
3:28
09:1
6:50
09:2
0:20
09:2
3:59
09:2
7:59
Ppeak [cmH₂O] Edi peak [µV]
How to set the NAVA level
0
2
4
6
8
10
12
14
16
Peak Pressure (cmH2)O
Edi Peak (mcV)
NAVA Level (cmH2O/mcV)
Break point
NAVA Ventilation in Neonates:
Clinical Guidelines and Management Strategies
Howard Stein M.D. and Kimberly Firestone BS, RRT
Neonatology Today April 2012
NeonatologyToday.net 5 videos:
Placing the Edi Catheter
Setting the NAVA level
Setting the Apnea Time
Setting the Edi trigger
Setting the Peak Pressure Limit
% CLD in neonates < 1500 grams VON Data
0
5
10
15
20
25
30
35
2004 2005 2006 2007 2008 2009 2010 2011 2012
TCH VON 50% VON 75%
%
NAVA NIV NAVA
Large multi-center trials are needed to answer questions if:
– NAVA prevents intubation or decreases time on ventilators?
– NAVA decreases the incidence of chronic lung disease?
– NAVA improves outcomes?
But does it make a difference?
NAVA WORKS IN NEONATES!














![Effects of Neurally Adjusted Ventilatory Assist (NAVA ... · Non-invasive ventilation (NIV) is widely used in cases of acute respiratory failure [1] and for patients who are considered](https://static.fdocuments.net/doc/165x107/60429fc39aac7877ad39cec0/effects-of-neurally-adjusted-ventilatory-assist-nava-non-invasive-ventilation.jpg)

