PBL Trauma - Decrease Consciousness
21
CASE II •A 48 year old man was taken to PUSKESMAS in a lost of consciousness condition. After laid on the bed and undergone some examinations, the patient was not giving any response and remained snoring with breathing frequency of 32 times per minute, weak pulse 100 bpm. According to the family who took him to the PUSKESMAS, the patient was not in any trauma preceding the condition. *keyword
-
Upload
muhammad-fawwaz -
Category
Documents
-
view
15 -
download
5
description
PBL Trauma
Transcript of PBL Trauma - Decrease Consciousness

CASE II• A 48 year old man was taken to PUSKESMAS in a lost of
consciousness condition. After laid on the bed and undergone some examinations, the patient was not giving any response and remained snoring with breathing frequency of 32 times per minute, weak pulse 100 bpm. According to the family who took him to the PUSKESMAS, the patient was not in any trauma preceding the condition.
*keyword

CLARIFICATION WORD
• Snoring-• Trauma-
The patient was unconscious? Not giving any response??
Refer to GCS!
Why snoring? tachypnea? weak pulse?
Don’t panic, do the emergency action immediately and you can find the reason for these signs!!!

ACTION IN EMERGENCY?WHAT WE HAVE TO DO???
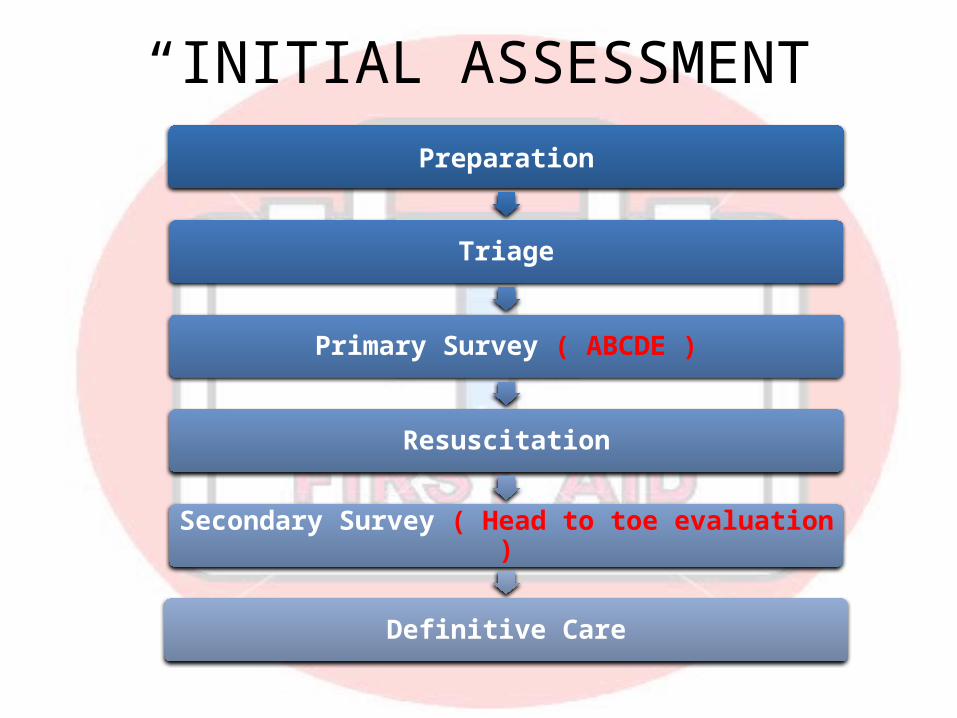
“INITIAL ASSESSMENT”Preparation
Triage
Primary Survey ( ABCDE )
Resuscitation
Secondary Survey ( Head to toe evaluation )
Definitive Care
“PRIMARY SURVEY”
A. Airway & cervical spine controlB. Breathing & ventilationC. Circulation & hemorrhage controlD. DisabilityE. Exposure/Environment
A B C D E

“PRIMARY SURVEY”A B C D E
Head tiltChin lift methodJaw thrust method
OPEN - CLEAR - MAINTAIN
• Manual stabilization of C-Spine• Noisy breathing = Obstructed breathing (But all obstructed breathing is NOT noisy)• Assume airway problems with:
• Decreased LOC• Head, face, neck, thorax trauma
Case: snoring due to base of tongue obstructs the airway ( suggesting partial airway obstruction)

“PRIMARY SURVEY”A B C D E
LOOK - LISTEN - FEEL
Give O2 immediately if: • Change in LOC• Possible shock• Possible severe hemorrhage• Chest pain• Chest Trauma• Dyspnea• Respiratory Distress
If you think about giving O2, GIVE IT!
Repiratory Rate Normal respiration 12 - 20 Bradypnea Tachypnea Apnea
Rythm• Regular• Irregular
Quality: Shallow Full Deep
Case: tachypnea, is rapid and shallow respiration commonly seen in shock

“PRIMARY SURVEY”A B C D E
Heart Rate Normal HR 60 - 90 Bradycardia Tachycardia
Quality» Weak (Thready)» Full» Bounding
Rhythm Regular irregular
Pulses present?Radial => BP > 80 systolicFemoral => BP > 70 systolicCarotid => BP > 60 systolic
Case: weak pulse with 100bpm, might be shock from loss of blood

“PRIMARY SURVEY”A B C D E
Mental status Glasgow Coma Scale Pupils Extremities
Eye opening Spontaneously 4 To Speach 3 To Pain 2 None 1
Verbal response Orientated 5 Confused 4 Inappropriate words 3 Incomprehensible sounds 2 None 1
Motor response Obeys verbal commands 6 Localising pain 5 Withdraws from pain stimuli 4 Flexing to pain 3 Extension to pain 2 No response 1
• Level of consciousness = Best indicator of brain perfusion
• Pupils-Eyes are windows of CNS• Decreased LOC:
• Head injury• Hypoxia• Hypoglycemia• Shock

“PRIMARY SURVEY”A B C D E
“PEARL”Pupils Equal And Reacting to Light
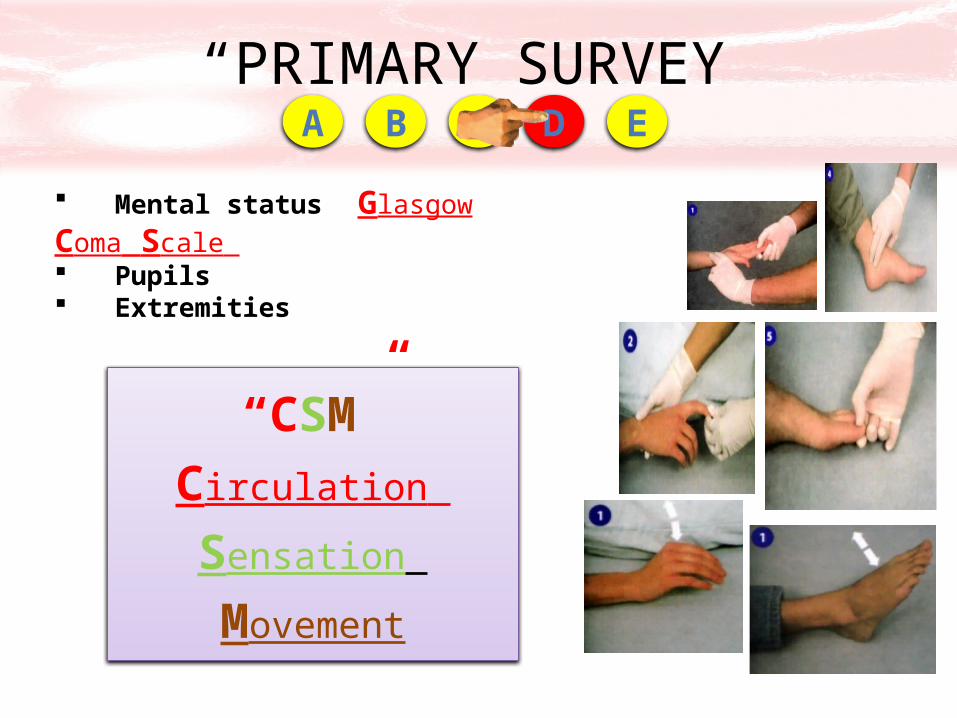
Mental status Glasgow Coma Scale Pupils Extremities
ShapeEqualityResponse to light
“PRIMARY SURVEY”A B C D E
“CSM”Circulation
Sensation
Movement
Mental status Glasgow Coma Scale Pupils Extremities
“PRIMARY SURVEY”A B C D E
Victim‘s history Physical exam
Head to toe examination
You can’t treat what you don’t findRemove clothing from critical patients ASAP!But do NOT delay resuscitation to remove clothingCover patient with blanket after exam is complete
Vitals signs are not necessary to determine whether patient is critical
“DOTS” Deformity Open wounds Tenderness Swelling
“PRIMARY SURVEY”A B C D E
Symptoms Allergies Medications Past medical history Last oral intake Events leading up to the illness or injury
“SAMPLE” history
Initial resuscitation!!• Immobilize C-spine (rigid collar)• Removal of blood or foreign bodies by suctioning with gentle techniques• Keep airway open• Administration of supplemental oxygen, 100% oxygen by highflow mask• Use of oropharyngeal or nasopharyngeal airways• Aggressively correct hypoxia, hypovolemia• Begin assisted ventilation with BVM• Apply and inflate PASG• Reassess and report in route
Minimum Time On SceneMaximum Treatment In Route

“SECONDARY SURVEY”
• To detect medical and injury-related problems that do not pose an immediate threat to survival but if left untreated, may do so!
• You WILL get here with MOST trauma patients• Perform ONLY after initial assessment is completed and life
threats corrected• Do NOT hold critical patients in field for detailed exam• Head and toe examination:
Organized, systematic Superior to Inferior Proximal to Distal Look - Listen - Feel - Smell
Extremity assessment must include: Pulse Skin color, temperature Capillary refill Motor, sensory function

Definitive care• Stable patients can receive
attention for individual injuries before transport– Bandaging– Splinting
• Reassess carefully for hidden problems
• Surgery intervention• If patient becomes unstable at any
time, refer to higher trauma center!
Reevaluation• Ventilation and perfusion status• Repeat vital signs• Continued stabilization of identified problems• Continued reassessment for unidentified problems• Go for supporting diagnosis eg. CT-scan and blood
evaluation.

References: National Safety Council; FIRST AID AND CPR.• Lecture notes of INITIAL ASSESMENT MANAGEMENT, SYAFRI K.ARIF, Dept.of
Anesthesiology,Pain Management and Intensive Care Faculty of Medicine Hasanuddin University
Chapleau, W., Pons, P. (2007) EMERGENCY MEDICAL TECHNICIAN. St. Louis: Elsevier
Caroline, N. (2007) EMERGENCY CARE IN THE STREET. 6th ed. London: Jones and Bartlett
Trauma Critical Care-volume 1 First aid, lecture notes, Charles University in Prague, 1st Faculty of Medicine,• Initial Assessment and Management of Trauma, Temple College EMS Professions

Any Question??