Patient Safety & Clinical Quality: Information Technology at THR Internal Medicine Update...
31
Patient Safety & Clinical Quality: Information Technology at THR Internal Medicine Update Presbyterian Hospital of Dallas October 29, 2003
-
Upload
marian-may -
Category
Documents
-
view
215 -
download
0
Transcript of Patient Safety & Clinical Quality: Information Technology at THR Internal Medicine Update...

Patient Safety& Clinical Quality:
Information Technology at THR
Internal Medicine UpdatePresbyterian Hospital of Dallas
October 29, 2003

10/29/2003 Internal Medicine Update 2
Overview
Case study (Cleary 2003) Quality (IOM 2001) Safety (Bates 2003) Projects NOVA (IOM 2003) Key Success Factors (Berwick 2003)

10/29/2003 Internal Medicine Update 3
Case Study
Cleary (2003;138:33-39) A Patient’s Perspective on Quality

10/29/2003 Internal Medicine Update 4
Case Study
Cleary (2003;138:33-39) Admission experience Postoperative experience Teamwork failures Pain management Discharge services

10/29/2003 Internal Medicine Update 5
Crossing the Quality Chasm
IOM (2001) “Information technology has
enormous potential to improve thequality of health care”

10/29/2003 Internal Medicine Update 6
Crossing the Quality Chasm
IOM (2001) Safety Effectiveness Patient-centered Timeliness Efficiency Equity

10/29/2003 Internal Medicine Update 7
Efficiency and Timeliness
Case study: PACS and voice recognition technology
Ted Wen MD, RadiologyPresbyterian Hospital of Plano

10/29/2003 Internal Medicine Update 8
IT and Patient Safety
Bates and Gawande (2003; 348:2526-2534) Prevention of errors and adverse events Facilitating a more rapid response to adverse
events Tracking and providing feedback about adverse
events

10/29/2003 Internal Medicine Update 9
IT and Patient Safety
Bates and Gawande (2003; 348:2526-2534)) Improve communication Access to knowledge Require key information Assist with monitoring Provide decision support

10/29/2003 Internal Medicine Update 10
Communication
Case study: electronic messaging
Ed Goodman MD, Infectious DiseasePresbyterian Hospital of Dallas

10/29/2003 Internal Medicine Update 11
Communication

10/29/2003 Internal Medicine Update 12
Access to Knowledge
Case study: medical references and clinical data
Robert Lilli MD, Family PracticeHarris Methodist Fort Worth Hospital

10/29/2003 Internal Medicine Update 13
Access to Knowledge

10/29/2003 Internal Medicine Update 14
Assist with monitoring
ICU monitoring Fetal monitoring

10/29/2003 Internal Medicine Update 15
Decision Support

10/29/2003 Internal Medicine Update 16
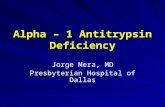
Decision Support
Case study: Weight based dosing for intravenous unfractionated heparin Rashke et al (1993;119:874-881)

NEW YORK-PRESBYTERIAN HOSPITAL DRAFT #12B (10/11/00)Columbia Presbyterian CenterNew York Weill Cornell Center
Bar code
ORDER FORM FOR INTRAVENOUS UNFRACTIONATEDHEPARIN BOLUS AND INITIAL INFUSIONIN ADULT INPATIENTS (page 1 of 2) If no plate, state patient name and medical record number
ALLERGIES:Patient’s weight: kilograms
DIAGNOSIS:
V: Start IV- ______________________ (specify IV solution) @ KVO rate of 10 ml/hrNOTE: An IV site (or port of a central venous catheter) should be dedicated to heparin.LABTESTS
Initial: Obtain emergent PT, aPTT and CBC with platelet count prior to administration of heparin. Document stool guaiac result (check one) negative po sitive no t performed
line, NO DRAWS THROUGH HEPARINIZED LINES OR FOLLOWING HEPARINIZED SYRINGES OR TUBES)Follow-up: Obtain an emergent aPTT in 6 hours after heparin bolus is given (and after any change in heparin dose)
Notify MD/NP/PA for an elevated baseline aPTT that is >5 seconds above the upper limit of normal for a patient not currently anticoagulated AND for any aPTT value less than 48 or greater than 146.Assess and monitor for signs and symptoms of bleeding.Notify MD/NP/PA for any signs and/or symptoms of bleeding.NITIATION OF HEPARIN BOLUS: Heparin bolus (Dose based on weight as per Table 1) __________ units (do not bolus stroke patients) Give IV push OR IVSS diluted in 50 ml of € D 5W OR € 0 .9% NaCl infused over 10 minutes INFUSION: Heparin infusion 25,000 units in o 250 ml D5W OR o 250 ml 0.45% NaCl at __________ units/ hour (based on weight as noted per Table 1) INFUSION INSTRUCTIONS: Use infusion pump
Weight Range Heparin Bolus Initial Heparin Infusion Initial Heparin Infusion
kilograms Dose (units) Rate (units/hour) Rate (ml/ hour)
36-40 3000 700 7 ml/hr
41-45 3500 800 8 ml/hr
46-50 3500 900 9 ml/hr
51-54 4000 900 9 ml/hr
55-58 4500 1000 10 ml/hr
59-63 5000 1100 11 ml/hr
64-67 5000 1200 12 ml/hr
68-72 5500 1300 13 ml/hr
73-76 6000 1300 13 ml/hr
77-81 6500 1400 14 ml/hr
82-85 6500 1500 15 ml/hr
86-90 7000 1600 16 ml/hr
91-95 7500 1700 17 ml/hr
96-99 8000 1800 18 ml/hr
100-104 8000 1800 18 ml/hr
105-108 8500 1900 19 ml/hr
109-113 9000 2000 20 ml/hr
114-117 9000 2100 21 ml/hr
118-122 9500 2200 22 ml/hr
123-126 10,000 2200 22 ml/hr
127-131 10,000 2300 23 ml/hr
132-135 10,000 2400 24 ml/hr
>136 10,000 2500 25 ml/hr
Prescriber signature and ID #
Date/Time Order checked


10/29/2003 Internal Medicine Update 19
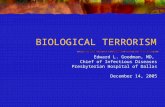
Impact of Decision Support
Compliance with weight-based dosing for Heparin pre-CPOE: 15% post-CPOE: 85%
0102030405060708090
100
Paper forms CPOE

10/29/2003 Internal Medicine Update 20
Projects NOVA
Infrastructure Mainframe Network Common desktop Interface engine
Applications Surgical management and scheduling Laboratory information system Physician portal (CareGate)

10/29/2003 Internal Medicine Update 21
Projects NOVA Applications
Clinical documentation Orders management Medication management

10/29/2003 Internal Medicine Update 22
Selection Methodology
NOVA Advisory Board IOM Report: Key Capabilities of an
Electronic Health Record System (2003) THR functional requirements Vendor evaluations

10/29/2003 Internal Medicine Update 23
Information Services
National recognition

10/29/2003 Internal Medicine Update 24
Challenges
Cultural Administrative Technical

10/29/2003 Internal Medicine Update 25
Change Leadership
Berwick (2003; 289:1969-1975) Find sound innovations Find and support innovators Invest in early adopters Make early adopter activity observable

10/29/2003 Internal Medicine Update 26
Change Leadership
Berwick (2003) Trust and enable reinvention Create slack for change Lead by example

10/29/2003 Internal Medicine Update 27
Discussion
Roles of allied health professionals Achieving consistency of clinical practice
(e.g., formulary, order sets) Using decision support to influence clinical
practice Medical staff by-laws



10/29/2003 Internal Medicine Update 30
Bibliography
Cleary PD: Ann Intern Med. 2003;138:33-39 Institute of Medicine. Crossing the Quality Chasm: A
New Health System for the 21st Century. Washington, DC: National Academy Press; 2001:1
Bates DW and Gawande AA: N Engl J Med 2003; 348:2526-2534
Institute of Medicine. Key Capabilities of an Electronic Health Record System. Washington, DC: National Academy Press; 2003:1
Berwick DM: JAMA 2003; 289:1969-1975

10/29/2003 Internal Medicine Update 31
Presenter Contact Information
Ferdinand Velasco, MD Chief Medical Information Officer
Texas Health Resources 601 Ryan Plaza Dr., Suite 301 Arlington, TX 76011 (817) 462-6723 E-mail: [email protected]