
Patient participation in clinical decision making in...
90
Patient participation in clinical decision making in nursing
Transcript of Patient participation in clinical decision making in...

1
Patient participation in clinical decision making in nursing

2

3
Örebro Studies in Caring Sciences 13
Jan Florin
Patient participation in clinical decision making in nursing – a collaborative effort between
patients and nurses

4
© Jan Florin, 2007
Title: Patient participation in clinical decision making in nursing – a collaborative effort between patients and nurses
Publisher: Universitetsbiblioteket 2007www.oru.se
Publications editor: Joanna [email protected]
Editor: Heinz [email protected]
Printer: DocuSys, V Frölunda 1/2007issn 1652-1153
isbn 91-7668-522-5

5
ABSTRACT
Florin, J. 2007. Patient participation in clinical decision making in nursing – a collaborative effort between patients and nurses. Örebro Studies in Caring Sciences No 13. Pp.90
The overall aim of the thesis was to study clinical decision making in nursing. This was performed by evaluation of the quality of nurses’ diagnostic statements and comparison of the concordance between nurses’ and patients’ perceptions of the patients’ nursing needs, as well as patient preferences for participation in clinical decision making. Further, predictors regarding patients’ active participation were investigated. Quasi-experimental, comparative and cross-sectional descriptive study designs were used to collect data in acute care settings from randomly selected patient records (n = 140), nurse-patient dyads (n = 80), and patients discharged from hospital care (n = 428). Data were gathered using questionnaires and review of patient records. The quality of nurses’ diagnostic statements improved by the means of education directed to nurses and implementation of new forms for recording supporting nursing care planning (I). Discrepancies were found concerning patients and nurses’ perceptions about what constitutes a problem for the patient as well as the severity and importance of acting on the problem (II). Further, nurses perceived that their patients preferred to be more active in clinical decision making compared with the patients’ own preferences for participation (III). Gender, education, living situation, and occupation were identified as predictors for preferring an active role in clinical decision making (IV).
The conclusions are that the accuracy of diagnostic statements needs to be addressed and validated further through systematic assessment of the patients’ perceptions and preferences concerning the health situation and preferences for participation in clinical decision making. Clinical implications are that nurses need to involve patients in identifying patient problems of relevance for nursing. Further, nurses also need to be aware of patients’ preferences for participation in clinical decision making in order that they can plan care in accordance with patient preferences and allow participation to the degree preferred by the patient.
Keywords: Clinical decision making, patient participation, nursing diagnosis, patient needs, nursing assessment, control preference scale.
Jan Florin, Department of Health and Social Sciences, Dalarna University, 791 88 Falun, Sweden. [email protected]

6
ORIGINAL PAPERS
This dissertation is based on the following papers, which are referred to in the text
by their Roman numerals.
I. Florin J., Ehrenberg A. & Ehnfors M. (2005) Quality of nursing diagnoses:
Evaluation of an educational intervention. International Journal of Nursing
Terminologies and Classifications 16(2), 33-43.
II. Florin J., Ehrenberg A. & Ehnfors M. (2005) Patients’ and nurses’
perceptions of nursing problems in an acute care setting. Journal of
Advanced Nursing 51(2), 140-149.
III. Florin J., Ehrenberg A. & Ehnfors M. (2006) Patient participation in
clinical decision making in nursing: a comparative study of nurses’ and
patients' perceptions. Journal of Clinical Nursing 15, 1498-1508.
IV. Florin J., Ehnfors M. & Ehrenberg A. Predictors of patients’ participation
in clinical decision making in nursing care. (Submitted)
Reprints of studies I, II, and III were made with kind permission from the
publishers.

7
CONTENTS
INTRODUCTION ...................................................................................................... 9
BACKGROUND........................................................................................................ 10 Patient’s role in health care........................................................................................ 10 Nursing care ................................................................................................................ 11 Nursing process model ............................................................................................... 12 Nursing documentation in patient records .............................................................. 13 Nursing diagnosis ....................................................................................................... 14 Needs and problems ................................................................................................... 16 Decision making.......................................................................................................... 17 Patient participation ................................................................................................... 20 Prerequisites for patient participation ...................................................................... 23 Patient participation in clinical decision making .................................................... 24 Rationale for the thesis .............................................................................................. 26
AIMS............................................................................................................................... 27
MATERIAL AND METHODS............................................................................ 28 Study I .......................................................................................................................... 29
Sample and characteristics ..................................................................................... 29 Record audit instruments....................................................................................... 30 Intervention and procedure ................................................................................... 30
Study II and III ............................................................................................................ 32 Sample and characteristics ..................................................................................... 32 Questionnaires ........................................................................................................ 34 Card sort technique ................................................................................................ 35 Procedure ................................................................................................................. 37
Study IV ....................................................................................................................... 38 Sample and characteristics ..................................................................................... 38 Questionnaire .......................................................................................................... 39 Procedure ................................................................................................................. 40
Reliability and validity ............................................................................................... 40 Ethical considerations ................................................................................................ 41 Data analyses............................................................................................................... 42
RESULTS ...................................................................................................................... 44 Quality of nursing diagnoses (Paper I) ..................................................................... 44 Congruence in perception of needs (paper II) ......................................................... 45 Participation in clinical decision making (paper III)............................................... 47 Predictors of preferences for participation (paper IV)............................................ 48
DISCUSSION .............................................................................................................. 51 Quality of nursing diagnoses ..................................................................................... 52

8
Congruence in perception of needs........................................................................... 53 Participation in clinical decision making ................................................................. 56 Congruence in perceptions of participation ............................................................ 58 Nursing process........................................................................................................... 60 Methodological considerations ................................................................................. 61
Sample selection ...................................................................................................... 62 Instruments .............................................................................................................. 63
Implications for practice ............................................................................................ 64 Future research............................................................................................................ 65
CONCLUSIONS ........................................................................................................ 67
SUMMARY IN SWEDISH .................................................................................... 68
ACKNOWLEDGEMENTS ................................................................................... 72
REFERENCES ............................................................................................................ 74
PAPERS I – IV

9
INTRODUCTION
In my previous experience as a nurse in an acute care ward and currently as a
university lecturer in nursing, I have always been a spokesperson for systematic
planning of nursing care and for the use of nursing diagnosis as basis for the
selection of specific nursing interventions to reach desired nursing outcomes. The
main idea with the nursing process model as a framework for problem solving is
the focus on the individual’s unique health situation and the possibility to tailor
interventions to suite the person’s needs. However, in order to make it work,
nurses need to ‘know’ their patients. I sometimes had the impression that the
nursing staff was not completely accurate in their descriptions of patients’ health
care needs. I read statements in the patient record and listened to verbal inter-shift
reports, sometimes revealing a lack of congruence with what I perceived when
meeting with the patient. Information and understanding of patients’ perspective
on health care needs did not always seem to be common knowledge by their
caregivers. A key issue seemed to be the interaction between the patient and the
nurse in which information was shared and communicated in both directions.
From time to time, questions were nagging my mind and just waited to be
answered: How well do nurses actually know their patients? In theory,
individualised and patient centred nursing care is a cornerstone in clinical nursing
practice, but do nurses know how the patients’ perceive their own situation and
their preferred role in clinical decision making concerning their nursing care? This
was the starting point of the research project reported in this thesis.
9

10
BACKGROUND
Registered nurses (RNs) identify patient needs and problems with the purpose of
providing individualised nursing care. The clinical judgements and decisions about
actions underpinning the care are essential for the outcome and quality of care. In
many real life events knowledge and values are inherited in the same person, the
person himself, but in health care decisions there is often an imbalance. Health
professionals have a profound knowledge base on a general level about health and
illnesses/diseases whilst the patient is the expert of his or her individual values and
preferences regarding care. A short length of stay in hospital care, combined with
demands for high quality care, increases the importance of identifying patient
needs and problems in a systematic way and to individualise care accordingly.
Therefore, RNs need to involve patients in identifying patient problems of
relevance for nursing, as well as find ways of reaching a common understanding of
the patient’s situation.
Patient’s role in health care The importance of patients’ own activity in planning and implementing care has
been stressed internationally over the years (WHO 1978, Institute of medicine
2003) and even in Sweden where patients, according to legislations, hold a strong
position in the health care system (SFS 1982). Arguments have been raised that, in
essence, patients have a “PhD” in their own uniqueness (Weed & Zimny 1989)
and ought to be considered honorary members of the health care team (Edwards
2002). Patient participation in clinical decision making is seen as an indicator of
quality in its own right (Wilde et al. 1994; Ruland 1999; IOM 2003) and inclusion
of the patient’s perspective has been noted to improve nursing care and patient
outcomes (Ruland 1999). The Institute of Medicine (IOM) in the U.S.A. identifies
patient-centred care as one of five core competencies for health professionals. A
central feature in patient-centred care is the patients’ participation, implying that
professionals share decision making and management of care with patients (IOM
10

11
2003). Further, IOM describes that the patient should be the source of control over
decisions regarding health care needs and that customisation of care should be
based on the patient’s needs and values rooted in shared knowledge and the free
flow of information (IOM 2001). The Internet is suggested to be a catalyst serving
to facilitate a balance of power among the key actors (Dickerson & Brennan
2002). To optimise care, identification and prioritisation of needs and problems
have to be decided in negotiation between health professionals and the patients in
a shared decision making encounter (Charles et al. 1997), with consideration of the
time perspective and available resources.
Nursing care The International Council of Nurses (ICN) identifies that nursing encompasses
autonomous and collaborative care of individuals of all ages, families, groups, and
communities, sick or well, and in all settings. Nursing includes the promotion of
health, prevention of illness, and the care of ill, disabled, and dying people.
Advocacy, promotion of a safe environment, research, participation in shaping
health policy and in patient and health system management, and education are also
key nursing roles (ICN). The concept of individualised nursing care has been
discussed since the late 1970s in Sweden, where a prerequisite is to ‘know the
patient’ (Radwin 1996; 1998), to have knowledge of the individual situation, and
how the patients themselves perceive the situation. RNs are guided by their
intentions to do good for the patients, described as benevolence (Lutzen & Nordin
1993) and beneficence (Woodward 1998). Communication skills are of the utmost
importance in nursing, considering that nursing always is two-folded with both
task-oriented and relational aspects (Peplau 1952; Jonsdottir et al. 2004).
However, in the case of caring for patients that cannot participate in information
exchange the burden of interpretation placed on the RN is considerable and needs
to be performed with respect and sensibility for patient integrity and autonomy.
11

12
Nursing process model The nursing process model has provided a structure for critical thinking and
reasoning in nursing since the 1950s when it was first presented by Lydia Hall. The
aim of the nursing process is to identify the needs of the individual patient and
tailor interventions to meet those needs. Values underpinning the nursing process
model identify the importance of the individual’s autonomy and free will to make
decisions regarding his/her own care. The patient and the nurse are regarded as
partners in a relationship where the nurse interacts with the patient in order to
solve the bio-psychosocial needs by maximising the individual’s positive interaction
with the environment, level of wellness, and degree of self-actualisation (Sundeen
et al.1994).
The nursing process model is a systematic general problem-solving model
originating from general system theory using the assessment of the patient’s status
as a point of departure. Initially, the process consisted of four subsequent phases:
assessment, planning, intervention, and evaluation (Yura & Walsh 1988). The
focus was mostly on nursing care needs connected to medical conditions, but the
attempts to classify nursing care problems requiring nursing attention led to the
development of nursing diagnoses. In 1973, The American Nurses Association
(ANA) published the Standards of Nursing Practice in which the nursing process
was described with five subsequent steps, adding diagnosis as the second step.
Gordon (1982) and Carnevali and colleagues (1984) extended the discussion of the
nursing process and the nurse’s management of information and making decisions.
The second generation of the nursing process model described the process with five
subsequent steps: assessment, diagnosis, planning, implementation, and evaluation.
However, the nursing process model has been criticised for focusing too heavily on
solving problems. Boychuk Duchscher (1999) points out the insufficiency of the
model as a basis for nursing practice because of the traditional product orientation
and lack of ingredients encompassing critical thinking (e.g., reflection, dialogue,
and dialectical thinking). There are suggestions of a third generation of the nursing
process model. Pesut and Herman (1999) proposed a model of reflective clinical
reasoning in which a repeated reflected comparison between present state and
12

13
outcome determines the clinical judgement and decision to end the reasoning
situation or reframing the situation, altering the decisions about the course of
action (Figure 1.)
Nursing documentation in patient records Nursing content in patient records is often categorised according to the nursing
process model. Available audit instruments for reviewing nursing documentation
initially only reflected a quantitative perspective (Nordström & Gardulf 1993), but
extended to a review of the process (Ehnfors & Smedby 1993) and explicitly
address both quantitative and qualitative dimensions (Björvell et al. 2000).
Educational interventions to improve documentation practice have positive effects
on quantity and quality of nursing documentation (Ehnfors 1993; Ehrenberg &
Ehnfors 1999a; Rosendahl Darmer et al. 2006).
REFLECTION
DECISION MAKING
TESTING
OUTCOMESTATE
PRESENTSTATE
FRAMING
JUDGMENT CUELOGICEXIT
CLIENT-IN-CONTEXT
STORY
Figure 1. The outcome-present state-test (OPT) model of reflective clinical reasoning (Pesut &
Herman 1999)
From Clinical Reasoning, The art and Science of Critical and Creative Thinking 1st edition by Pesut/Herman. 1999. Reprinted with permission of Delmar Learning, a division of Thompson Learning: www.thompsonrights.com.Fax 800 730-2215.
13

14
Altering the charting system or record forms do not seem to bring about better
content in patient records (Moen et al. 1997). However, introduction of electronic
health record systems with standardised information templates improved the
structure and content in the nursing discharge notes (Hellesö et al. 2004). An
initial positive effect of education on nurses’ ability to identify patient problems is
often not sustained over time (Heaven & Maguire 1996). Interventions combining
education and development of forms for recording seem to have positive effects on
the documentation of the nursing process (Engvall 1994; Wallentin et al. 1996;
Björvell et al. 2002). An intervention package with education in combination with
organisational change, including trained change agents and support given to chief
nurses, led to a sustained long-term increase of quantity as well as quality of
nursing documentation (Björvell et al. 2002). Even so, the improvements were
marginal and there is evidence of major deficiencies in nursing documentation in
relation to systematic structure and comprehensiveness (Ehrenberg & Ehnfors
1999b; Ehrenberg & Ehnfors 2001; Ehrenberg et al. 2004).
Nursing diagnosis A nursing diagnosis is defined by the North American Nursing Diagnosis
Association (NANDA) as a “clinical judgment about individual, family, or
community responses to actual or potential health problems/life processes. A
nursing diagnosis provides the basis for selection of nursing interventions to
achieve outcomes for which the nurse is accountable” (NANDA 2001, p. 245). A
nursing diagnosis can be regarded as both a process and a product, where the
process precedes the product and includes clinical reasoning and a judgement. The
process involves activities such as collecting, interpreting, and clustering
information about the patient and finally naming the cluster (Carnevali 1983). As
a product, it is preferably stated as a short, clear statement expressed with concise
terms that identifies the patient's problems or health status. Major approaches to
express nursing diagnoses are either to select diagnoses from taxonomies of
14

15
standardised diagnostic statements (e.g., NANDA 2001) or to express diagnoses in
free text (Carnevali 1983; 1996). When stating diagnoses, the PES format is widely
used (Gordon 1994; Carnevali 1996; NANDA 2001). Three essential components
are identified in the statement: the problem (P), its aetiologies (E), and signs and
symptoms (S). NANDA and Carnevali interpret and use the PES format slightly
different. The S-component is seen by NANDA (2001) as evidence for the presence
of the problems, whereas Carnevali (1996) often use the S-component to state
actual consequences of the problem.
Incentives for RNs to use nursing diagnoses are e.g. to be able see the patient as an
individual and as a whole, and to facilitate nursing care (Axelsson et al. 2006). A
literature review of nursing diagnoses impact on nursing practice concluded that
nursing diagnoses seemed to improve the assessment documentation, quality of
reported interventions, and outcomes attained (Muller-Staub et al. 2006).
However, there is always a risk for low accuracy nursing diagnoses, as confirmed
in several studies (Lunney 1990; 2003). The use of a framework borrowed from
evidence-based medicine incorporating clinical expertise and experience and
patient preferences and values in clinical decision making could improve the
interpretation of patient data (Levin et al. 2004)
In Sweden, varied frequencies of nursing diagnoses in patient records have been
reported, ranging from 10% in acute care settings (Ehnfors & Smedby 1993;
Nordström & Gardulf 1996) to 71% of patient records from nursing homes where
all the nurses had completed a university course in documentation of nursing care
(Fagrell et al. 1998). A study of district nurses’ documentation practice reported
that nursing diagnoses hardly existed in the records (Törnvall et al. 2004). Positive
long-term effects on quantity and quality of nursing diagnoses, although not to
very high levels, have been reported following a complex intervention with
education as one part of the package (Björvell et al. 2002).
15

16
Needs and problems Need is ‘a socially constructed concept that is closely bound up with identities,
expectation, and context’ (Cowley et al. 2000, p. 127) in relation to health. Liss
(1990) discussed varying perspectives on the concept in which one perspective was
an ill health notion, where health care needs could be understood as deficiencies in
health or social wellbeing that called for preventive, curative, or rehabilitative
actions.
In this thesis, a need is defined as “a difference between an actual state and a
goal” (Liss 1990, p. 89). According to Liss (1990, p. 117), two conditions are
needed: “1) there is a difference between two states on the health dimension –
between the actual state and the goal of need; 2) health care is necessary for the
elimination of the difference – that is, for reaching the goal of need”. To a certain
extent, the persons themselves can be the provider of personal health care activities
to eliminate the difference. However, when a person’s own resources are not
sufficient, there is a need for health care from professionals. This is in line with
Carnevali’s (1993) description of health as a balance between resources and
requirements in daily living. Health care is necessary in case of an imbalance
between resources and requirements. Further, needs can be divided into needs and
wants, where needs must be satisfied, but wants are expressions rooted in personal
psychological states and thus can be deferred (Holmes & Warelow 1997). The
concept of problem involves a perception and recognition of the discrepancy
between what is and what ought to be (Liss 1990). In this thesis, a need that the
persons can satisfy but with difficulties, or cannot satisfy by themselves, using
internal or external resources, constitutes a problem. The concepts of need and
problem are used interchangeably in the text.
Patients, as a holistic entity, can hold a variety of needs, often divided in physical,
psychological, social and spiritual, and religious needs. There is a tendency to
overemphasise the physical dimension, probably because it is easier to define and
measure, but it could be pointed out that participation in decision making in itself
16

17
could be a need, as well as integrity, continuity, and communication (Hallström &
Elander 2001a).
RNs and patients have been seen to differ in perceptions of patient health care
needs or problems though the findings are inconclusive. Nurses and patients hold
different opinions about the presence of nursing problems in somatic (Farrell 1991;
Adamsen & Tewes 2000) and psychiatric settings (Hansen et al. 2002). In general,
nurses overestimate their patients’ nursing problems, with emotional problems
being overestimated more often than physical ones (Farrell 1991; Löfmark et al.
1999). Lauri and colleagues (1997) reported a contrasting result in which nurses
underestimated almost all the patients’ nursing problems. In particular, it has been
demonstrated that nurses underestimated patients’ perceived self-care ability
(Richardson 1992), level of fatigue (Tiesinga et al. 2002), and pain intensity
(Blomqvist & Hallberg 1999; Hall-Lord et al. 1999; Hovi & Lauri 1999; Sloman
et al. 2005). Moreover, nurses overestimated patients’ anxiety and depression
(Lampic et al. 1996) and worries (Biley 1989; Harrison et al. 1996). Finally,
patients tended to report more unmet needs than health care professionals
identified (Kersten et al. 2000), predominantly in the psychosocial realm (Kent et
al. 1996; Soothill et al. 2001).
Decision making Quite a few concepts are used to describe critical thinking in health care (e.g.,
clinical reasoning, diagnostic reasoning, decision making, judgement, and problem
solving). Sometimes the concepts are used interchangeably (Hendry & Walker
2004) but they have slightly different features (Dowding & Thompson 2003).
Critical thinking is described by Ennis (1996, p.xvii) as “a process, the goal of
which is to make reasonable decisions about what to believe and what to do.”
Clinical decision making is a process that involves both diagnostic reasoning and
clinical judgement (Tanner 1987). Judgement and decision making are examples of
reasoning as both a process and a product, the outcome of the process. It is
important to realise the cyclical features of the process in which the resulting
17

18
actions are directed by reflection and reflection is in turn influenced by those
actions (Conger & Mezza 1996).
Different thinking strategies, used in clinical reasoning that are aimed at decision-
making, have been described, including the hypothetico-deductive method,
decision analysis theory, pattern recognition, and intuition (Benner 1984; Brennan
& Strombom 1998; Fonteyn 1998; Offredy 1998). Harbison (2001) argued that
RNs might have adopted Benner’s work a bit uncritically. Being reassured that
they are ‘experts’ using ‘intuition’ for high quality decision making, motivation to
examine their decisions using other perspectives might be lacking. Even so, a more
systematic ongoing process is often representing a rationale underlying the expert’s
intuitive practice (Harbison 2001). Heuristics and experiential knowledge are
important but not a sufficient basis for clinical decision making (Thompson 2003).
André (2004) reported that general practitioners’ ‘Rules of thumb’, a form of tacit
knowledge in some areas, were possible to verbalise, which makes the knowledge
explicit. A unifying framework connecting the different theories is that of
Buckingham and Adams (2000b), who interpret clinical decision making as
classification behaviour. They argued that linking cues with diagnostic categories,
usually regarded as pattern recognition, actually is the same process as connecting
evidence with hypothesis in the sense that it is a form of classification activity.
Their general model of classification could be used as a common frame of reference
for understanding clinical decision making and contributing to multidisciplinary
collaboration in which data provide cues to identify categories. However, a
prioritisation of needs has to be done as a part of the classification thinking.
Priority setting is an essential part of care planning in which patient needs are
classified as having different priority. Hendry and Walker (2004, p. 427) defined
priority setting as, “the ordering of nursing problems using notions of urgency
and/or importance, in order to establish a preferential order for nursing actions”.
The social policy statement by ANA (1980) recognises the pivotal role of
diagnostic reasoning in nursing and the ability to choose appropriate interventions
18
19
to achieve expected outcomes. In this thesis, Tanner’s definition of clinical
judgement is used:
“a series of decisions made by the nurse, in interaction with the client
regarding (a) the type of observations to be made in the client
situation, (b) the evaluation of data observed and derivation of
meaning (diagnosis), and (c) nursing actions that should be taken with
or on behalf of the client” (Tanner 1987, p. 154).
The definition reflects the phases of the nursing process, explicitly stressing the
importance of interaction with the patient. Judgement and decision making are
closely related but have distinct differences since they generate different cognitive
demands (Dowding & Thompson 2003). Judgement can be regarded as ‘an
assessment between alternatives’ integrating different aspects of information about
a person or a thing. Decision making has been described as ‘a choice between
alternatives’ in which the process is focused on choosing a particular course of
action (Dowie 1993). Dowding and Thompson (2003) stress the importance of
distinguishing between the concepts. A nurse could make an accurate judgement
(e.g., about a patient’s risk for pressure ulcer), but make a poor decision by
choosing a poor action. However, the environment of care has implications on
need identification and response. The RN needs to distinguish between ‘signal’ and
‘noise’ in order to be able to name the patients situation, combined with a stage of
framing the situation, depending on philosophy of care and organisational issues
and time (Carr 2004).
It is problematic to define judgements as good or bad since nurses operate in an
environment characterised by uncertainty (Buckingham & Adams 2000a).
Drawing on the discussion on self-assessed and others-assessed needs (Liss 1990),
the subjective dimension in clinical judgement in nursing is profound. There is
seldom a definite right or wrong and differences in opinions exist depending on
perspective, values, beliefs, and hopes related to information and knowledge in the
situation. Whose perspective is to be the prevailing one, the RN’s or the patient’s?
19

20
When uncertainty exists, there is reason to involve the patient as the primary
decision maker (Weed & Weed 1999).
Patient participation To expand the previous discussion on the patient’s role, there is growing consensus
that patients ought to be more involved in their own care. This agreement stems
from political ideas, ethical thinking, and research in health care. The patient’s
position is moving towards being a customer; evident in an increasing degree of
personal choice and personal rights, care guarantee, and a right to self-
determination (Nordgren 2004). Participation is linked to the concepts of power
and empowerment. Power is seen as extrapersonal, indicating that an increase in
one’s power must be balanced with a decrease in someone else’s power.
Prerequisites to generate power are opportunities and sufficient information.
Empowerment is an individual process in which the person is interacting with the
environment pursuing impact on his/her life (Kuokkanen & Leino-Kilpi 2000). It is
notable that a patient must be an active participant in his/her empowerment,
indicating that RNs cannot empower patients: the role is to facilitate and support
the empowerment (Laverack 2005). The major responsibility to invite patients as
active partners in decision making in nursing is inevitably the nurses’ since the
patient is in a subordinate position and cannot be expected to take the lead.
Patients experiences in relation to health issues should be valued as evidence
contributing to the decision-making process and that partnership with health care
professionals is important (Rycroft-Malone et al. 2004a). Further, there is a need
for a context receptive for change, addressing power and authority processes, and
with appropriate and transparent decision-making processes (Rycroft-Malone et al.
2004b).
Patient participation involves several dimensions, including collaboration,
partnership, and involvement, sometimes used interchangeably (Cahill 1998; Kirk
& Glendinning 1998) though Ashworth and colleagues (1992) contend that those
20

21
dimensions do not necessarily indicate genuine participation. Most commonly,
patient participation is described as a hierarchy with increasing degrees of
participation, especially in relation to decision making. Cahill (1996) described a
hierarchical relationship in which increased involvement or collaboration leads to
participation, with partnership at the top of the hierarchy. However, patient
participation in care and care giving can be seen as a process as well. Tutton
(2005) described a dynamic process, enacted through the themes of emotional
work, understanding the person, facilitation, and partnership, that takes place
within a context that could affect the process (e.g., time constraints, ward
environment, or degrees of teamwork). The concept of participation, as
understood from the patients’ perspective, was reported by Eldh and colleagues
(2004). Participation was experienced as being confident, comprehending, and
seeking and maintaining a sense of control.
A distinction needs to be made between decisional autonomy (decision making)
and executional autonomy (implementing decisions). Even though ability for
executional autonomy is decreased, the patient possibly still can perform his
decisional autonomy, but there is a risk of violation of the patient’s right to
participation in that respect (Matiasson et al. 1997). Provision of health care
involves a mutual problem-solving process between health professionals and
patients in which patients’ participation in decision making is facilitated or even
needs to be requested (Balzer-Riley 1996; ICN 2003). D’Onofrio (1980, p.274)
suggested that patient participation was “patient engagement in problem
identification and prioritisation, establishment of change objectives and the process
of making decisions about how change will be accomplished”.
Patient participation in health care decision making can be placed in an
independency-dependency continuum that could range from non-participation
through co-determination and delegation to self-determination (Sahlberg Blom
2001), sometimes expressed as passive to responsible (Latvala et al. 1999, Latvala
2002) or passive to active participation (Degner & Sloan 1992; Sainio et al. 2001;
21

22
Caress et al. 2002; Kraetschmer et al. 2004). An alternative way of describing
participation was suggested by Andershed (1998) using the metaphors
“involvement in the light”. This kind of participation is promoted by a trusting
relationship between the patient and the staff and “involvement in the dark” as
characterised by insufficient interplay and collaboration.
Charavel and colleagues (2001) described models placed on the continuum: (1)
a paternalistic model in which the health professionals make the decisions, (2) an
informative model in which health professionals provide the patients with
information to enable them to select the desired treatment, (3) an interpretative
model in which health professionals and patients interact to identify the patients
wishes and values and support them to select treatment, and (4) a deliberative
model that is very close to the interpretative model but adds a moral dimension to
the interaction that emphasises the discussion between two partners. Charles and
colleagues (1997) proposed the ‘shared model’: a two-way exchange of
information with both the patient and the professional stating their treatment
preferences and reach an agreement on the decision. The key characteristics are at
least two participants sharing information acting to build consensus and eventually
reaching an agreement.
Research findings suggest that patient preferences for participation in clinical
decision making differ because of age, gender, socio-economic status, and severity
of the medical problem (Degner & Sloan 1992, Degner et al. 1997, McKinstry
2000, Henderson & Shum 2003). These findings, however, are inconclusive. Cahill
(1998) concluded that patients generally preferred to be active but that caregivers
preferred to see the patient as a more passive recipient of care despite their
acknowledgement of the positive value of active involvement. Patient participation
was regarded by RNs as both a goal and a means in nursing care (Jewell 1994).
However, if patients and RNs have a different understanding of the concept
participation, then real patient participation might be difficult to achieve in the
clinical encounter (Sainio et al. 2001; Eldh 2006)
22

23
Prerequisites for patient participation The same factors have been identified to either facilitate or work against patient
participation in decision making. The factors include access to information and
knowledge, quality of professional-patient relationship, time, actual medical
situation, and personal characteristics of nurses and patients. Possession of
sufficient and adequate information facilitates participation, whereas lack of
knowledge functions as a hindrance for more active participation (Caress et al.
2002). Nurses’ communication skill is a pivotal prerequisite for patient
participation in decision making. Communication deficits have been identified as
one of the principal barriers to partnership building between nurses and patients
(Keatinge et al. 2002). Professionals need to be willing to listen and establish a
good provider-patient relationship (Caress et al. 2002), and they need to encourage
patients to ask questions (Timonen & Sihvonen 2000) and to probe questions
themselves (Efraimsson et al. 2004). Casey (1995) proposed a framework for
patient involvement in nursing practice. The degree of participation is indicated by
the intersection of two axes: a communication – non-communication and a person-
centred – nurse-centred continuum (Fig. 2). Nurses practicing
“communicating/nurse-centred” care are authoritative and controlling but allow
participation by giving patients permission to participate.
Communicating
Non-communicating
Person-centered
Nurse-centered
ASSUMPTIONEXCLUSION
NEGOTIATIONPERMISSION
Figure 2. Nursing approaches to involvement in care (Casey 1995)
23

24
Nurses who act according to “Non-communicating/nurse-centred” care behave in
ways in which exclusion of patients from participation is common. A “non-
communicating/person-centred” nurse makes assumptions about patients’ needs,
wishes, and abilities mostly based on her/his own subjective opinion. Nurses
applying a “communicating/person-centred” care approach share their knowledge
and expertise with patients, with negotiation of care in focus using patient
participation as an essential ingredient.
Patient participation in clinical decision making Several studies of patients’ or relatives’ participation in a Swedish nursing context
have been reported, including studies on children’s participation (Runeson 2002),
where the need for information and participation was most prominent in non-
threatening situations in comparison with threatening ones. Participation was not
allowed to the extent judged to be optimal. Sahlberg Blom (2001) showed that the
autonomy of cancer patients in the final phase of life could be categorised on a
scale from self-determination to non-participation. Andershed (1998) described the
involvement of relatives to patients in the final phase of life using the categories to
know, to be, and to do. Hedberg (2005) discussed the gap between nurses’
decision making and communication in clinical practice with the expected
performance related to work regulations and goals of conduct expressed in nursing
education. Eldh (2006) explored the concept of participation from the patients’
perspective, adding several dimensions to the concept, such as being confident,
comprehend, and seeking and maintaining a sense of control. Efraimsson (2005)
investigated women’s participation in discharge planning conferences, revealing a
professional dominance in the situation combined with feelings of being left
outside and unheard.
Studies of patient participation in medical decision making report figures of
patients preferred participatory role with quite wide ranges. To summarise,
patients in specific medical decision-making situations preferred to have a passive
24

25
role in 27-78% of the time, whereas a collaborative role was preferred in 17-64%.
Furthermore, 4-32% of the patients preferred being active in decision making
(Sätterlund-Larsson et al. 1989; Beaver et al. 1996; Butow et al. 1997; Beaver et al.
1999; Ramfelt et al. 2000; Protière et al. 2000; Gattellari et al. 2001; Sainio et al.
2001; Davison & Degner 2002; Schou et al. 2002).
Cultural differences in opinions between RNs and patients in relation to
involvement in decision making have been identified in five European countries,
where differences between the northern and southern parts might be explained by
different educational levels or the basic training systems of nurses (Scott et al.
2003a). Further, the model of autonomy, rooted in an individualistic view of
human life, may not be suitable in countries where the role of the family in
people’s lives is more pronounced. Studies reflecting the UK perspective reported
that nurses in elderly care (Scott et al. 2003b) and midwifes (Scott et al. 2003c)
reported that patients were offered opportunities to participate in decision making
to a higher extent compared with patients’ reports of being offered such an
opportunity. In contrast, surgical patients generally reported a more positive view
on frequency of involvement in decision making than what nurses reported (Scott
et al. 2003d).
Interventions aiming to increase patient participation have been reported (e.g.,
feeding forward of patient data to clinicians, which prepares for mutual
identification of patient needs and preferences, and shared decision making
(Wensing & Grol 1998; Ruland 1999; Ruland & Moore 2001), as well as
provision of information about health care providers performance, interactive
patient education, and feedback to clinicians about patients' evaluation of care
(Wensing & Grol 1998). Feeding forward of information increased clinicians’
recognition of patients’ health problems and needs for care (Wensing & Grol
1998), and the inclusion of patient preferences in decision support systems have
been seen to have great acceptance and perceived usefulness by professionals
(Ruland 2004). Patients’ daily intake of energy has been observed to increase
(Pedersen 2005). Inclusion of the patient’s perspective in health care decision
25

26
making improves nursing care and patient outcomes (e.g., care priorities in
attunement with patient preferences, greater preference achievement, and better
physical functioning) (Ruland 1999).
Rationale for the thesis Clinical decision making in nursing is a complex task often performed under a
great deal of uncertainty (e.g., rooted in subjective values and preferences). In
order to provide individualised care in accordance with patient preferences, RNs
need to be aware of the patients’ perspective and preferences for care. The review
reveals that techniques to elicit patient preferences for nursing care, and by that
increasing participation in the decision-making process, have been tested with
promising results. However, the knowledge of patients’ preferences and
experiences of participation in clinical decision making in nursing and level of
congruence with RNs’ perceptions is still rather limited. Acute somatic hospital
care is a relatively unexplored setting regarding clinical decision making in nursing.
There is a need to increase the knowledge in this context, especially because of the
necessity for clinical decision making with high accuracy to optimise nursing care
during a relatively short hospital stay. If the assessment and planning of nursing
care is not optimal, or in line with patient preferences, the care processes during
the given time frame will be negatively influenced and ultimately the quality of
nursing care could be jeopardised.
Therefore, there is a need for increased knowledge on clinical decision making,
including identification and formulation of needs of nursing care, and patient
decision-making role preferences in general, and congruence in perceptions with
RNs from a Swedish perspective.
26

27
AIMS
The overall objective of this thesis was to study clinical decision making in nursing,
with special focus on diagnostic statement quality, patient participation, and the
coherence between patients’ and nurses’ perceptions of needs and preferred
participatory role.
The specific aims of the studies were to:
1. Investigate the effect on the quality of nursing diagnoses documented in
patient records of an intervention comprising education and implementation
of new forms for recording (study I).
2. Determine the degree of consistency between RNs’ and patients’ perceptions
of presence, severity, and importance of nursing problems in an acute care
setting (study II).
3. Compare the degree of concordance between patients’ and RNs’ perceptions
of patients’ preferences in participating in clinical decision making in
nursing practice (study III).
4. Compare patients’ actual level of participation in clinical decision making in
nursing with their preferred participatory role (study III).
5. Investigate predictors of patient preferences for active participation in
nursing decision making (study IV).
27
28
MATERIAL AND METHODS
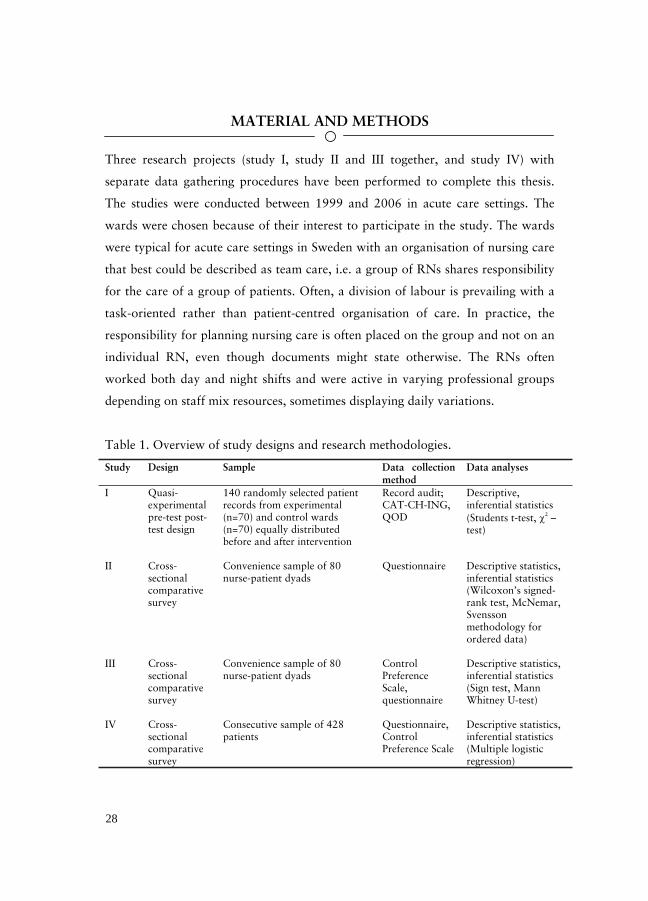
Three research projects (study I, study II and III together, and study IV) with
separate data gathering procedures have been performed to complete this thesis.
The studies were conducted between 1999 and 2006 in acute care settings. The
wards were chosen because of their interest to participate in the study. The wards
were typical for acute care settings in Sweden with an organisation of nursing care
that best could be described as team care, i.e. a group of RNs shares responsibility
for the care of a group of patients. Often, a division of labour is prevailing with a
task-oriented rather than patient-centred organisation of care. In practice, the
responsibility for planning nursing care is often placed on the group and not on an
individual RN, even though documents might state otherwise. The RNs often
worked both day and night shifts and were active in varying professional groups
depending on staff mix resources, sometimes displaying daily variations.
Table 1. Overview of study designs and research methodologies.
Study Design Sample Data collection method
Data analyses
I Quasi-experimental pre-test post-test design
140 randomly selected patient records from experimental (n=70) and control wards (n=70) equally distributed before and after intervention
Record audit; CAT-CH-ING, QOD
Descriptive, inferential statistics (Students t-test, 2 –test)
II Cross-sectional comparative survey
Convenience sample of 80 nurse-patient dyads
Questionnaire Descriptive statistics, inferential statistics (Wilcoxon’s signed-rank test, McNemar, Svensson methodology for ordered data)
III Cross-sectional comparative survey
Convenience sample of 80 nurse-patient dyads
Control Preference Scale, questionnaire
Descriptive statistics, inferential statistics (Sign test, Mann Whitney U-test)
IV Cross-sectional comparative survey
Consecutive sample of 428 patients
Questionnaire, Control Preference Scale
Descriptive statistics, inferential statistics (Multiple logistic regression)
28

29
Consequently, both patients and RNs interact with many persons, sometimes
shifting on a daily basis. An overview of study designs and research methodologies
is given in Table 1. More detailed descriptions of material and methods for each
separate research project are found below.
Study I A quasi-experimental pre-test – post-test design was used. The study was
conducted at a regional Swedish hospital at a ward for infectious diseases
(experimental group) and three medical wards (control group).
Sample and characteristics The sample comprised 140 randomly selected patient records from both the
experimental ward and control wards, which meant a retrieval of 70 patient
records from the archives for each group. Of these, 35 records reflected the
documentation practice for patients treated during a three-month time span before
and after the intervention respectively. The sample constituted approximately 10%
of the total number of records during the study period at the experimental ward
and 5% at the control wards. The records were mostly describing the care of
patients acutely admitted to hospital care (98%), displaying equal median length of
stay between groups, with a few outliers in the experimental group. The RNs in
the experimental group had a mean age of 39 years (SD 10.1), whereas RNs in the
control group were 41 years of age (SD 10.2). Apart from education in
documentation practice incorporated in basic nursing education, two RNs in the
experimental group and five RNs in the control group had a university course in
documentation practice. The staff ratio was 0.57 RNs per patient bed at the
experiment ward and 0.55 at the control wards, ranging from 0.46 to 0.72. RN’s
worked in teams with assistant nurses depending on staff mix for the shift and sick
leaves.
29

30
Record audit instruments The instrument CAT-CH-ING (Björvell et al. 2000) was used to measure the
quality of RNs diagnostic statements. CAT-CH-ING is an audit instrument that is
reported to be both valid and reliable (Björvell et al. 2000). The instrument
measures quantity and quality of documentation based on the nursing process and
Swedish regulations. In paper I, analyses of the two variables measuring quantity
and quality of nursing diagnoses, measured on a four-point ordinal scale, is
reported. The instrument comprises 26 variables in total. Further, a scale to
measure the quality of diagnostic statements was developed for this study based on
instruments developed by Ziegler (1984) and Lunney (1990). Existing instruments
were regarded relevant but not directly applicable because of differences between
Swedish and American use of nursing diagnoses. The scale Quality of Nursing
Diagnosis (QOD) (Table 2) reflects four components divided into 14 dichotomous
characteristics of a diagnostic statement, which evaluates diagnostic structure (S)
and relevance (R). The components Problem, Aetiology, and Signs/symptoms
reflect the commonly used PES format when stating nursing diagnoses, adding an
additional fourth general component to the scale. Each criterion was valued as
absent (zero points) or present (one point), yielding a maximum score of 14.
Higher scores reflect better quality in the diagnostic statement.
Intervention and procedure The intervention consisted of an educational program for RNs in the use of the
VIPS model (Ehnfors et al. 2002), acronym for the Swedish spelling of Wellbeing,
Integrity, Prevention, and Safety. The purpose was to increase the understanding
and use of the nursing process as a problem-solving method in clinical practice.
Each nurse participated in five separate 3-hour sessions, meeting approximately
every second week. During the sessions, real and fictitious patient cases were
discussed with a focus on nurses’ care planning activities (e.g., stating nursing
diagnoses, outcomes, and planned interventions). New forms for recording were
discussed during the sessions and then developed by one of the researchers (JF).
30
31
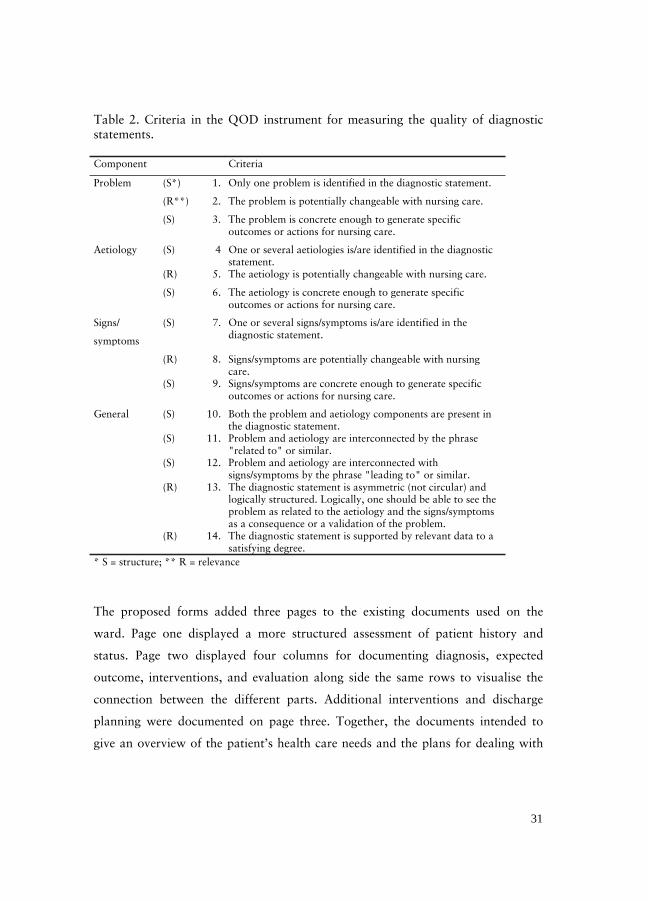
Table 2. Criteria in the QOD instrument for measuring the quality of diagnostic statements.
Component Criteria
Problem (S*) 1. Only one problem is identified in the diagnostic statement.
(R**) 2. The problem is potentially changeable with nursing care.
(S) 3. The problem is concrete enough to generate specific outcomes or actions for nursing care.
Aetiology (S) 4 One or several aetiologies is/are identified in the diagnostic statement.
(R) 5. The aetiology is potentially changeable with nursing care.
(S) 6. The aetiology is concrete enough to generate specific outcomes or actions for nursing care.
Signs/
symptoms
(S) 7. One or several signs/symptoms is/are identified in the diagnostic statement.
(R) 8. Signs/symptoms are potentially changeable with nursing care.
(S) 9. Signs/symptoms are concrete enough to generate specific outcomes or actions for nursing care.
General (S) 10. Both the problem and aetiology components are present in the diagnostic statement.
(S) 11. Problem and aetiology are interconnected by the phrase "related to" or similar.
(S) 12. Problem and aetiology are interconnected with signs/symptoms by the phrase "leading to" or similar.
(R) 13. The diagnostic statement is asymmetric (not circular) and logically structured. Logically, one should be able to see the problem as related to the aetiology and the signs/symptoms as a consequence or a validation of the problem.
(R) 14. The diagnostic statement is supported by relevant data to a satisfying degree.
* S = structure; ** R = relevance
The proposed forms added three pages to the existing documents used on the
ward. Page one displayed a more structured assessment of patient history and
status. Page two displayed four columns for documenting diagnosis, expected
outcome, interventions, and evaluation along side the same rows to visualise the
connection between the different parts. Additional interventions and discharge
planning were documented on page three. Together, the documents intended to
give an overview of the patient’s health care needs and the plans for dealing with
31

32
them, including discharge planning. The forms were subsequently presented and
implemented in the experimental ward at the end of the educational intervention.
Patient records were retrieved from the archives and documents containing
nursing notes were copied. A nursing diagnosis was defined as a statement
identifying patient problems, causes, and consequences or just problem statements
by which there was evidence in the patient record that nursing actions had been
planned or implemented to deal with the problem. When notes on a nursing
problem appeared several times, the most precise wording with most detailed
aetiology or consequences was chosen for the analysis.
Study II and III A cross-sectional comparative survey design was applied using a hospital ward for
infectious diseases as the setting for collecting data from patient-nurse dyads.
Sample and characteristics A convenience sample of 80 patients, out of an eligible group of 330 patients, and
30 RNs in charge of their care participated in the study. The study was conducted
from November 2002 to January 2003. Inclusion criteria for patients were: (1)
aged 18 years or older, (2) admitted to the ward less than 48 hours before data
collection and expected to stay for at least three days, (3) able to communicate in
Swedish, (4) participation did not jeopardise the current health condition of the
patients as judged from the interviewer’s (JF) own experience as an acute care
nurse, and (5) being cared for by a RN willing to participate in the study.
Exclusion criteria were expected length of stay less than three days, suffering from
cognitive impairments because of dementia or confusion, and too medically ill or
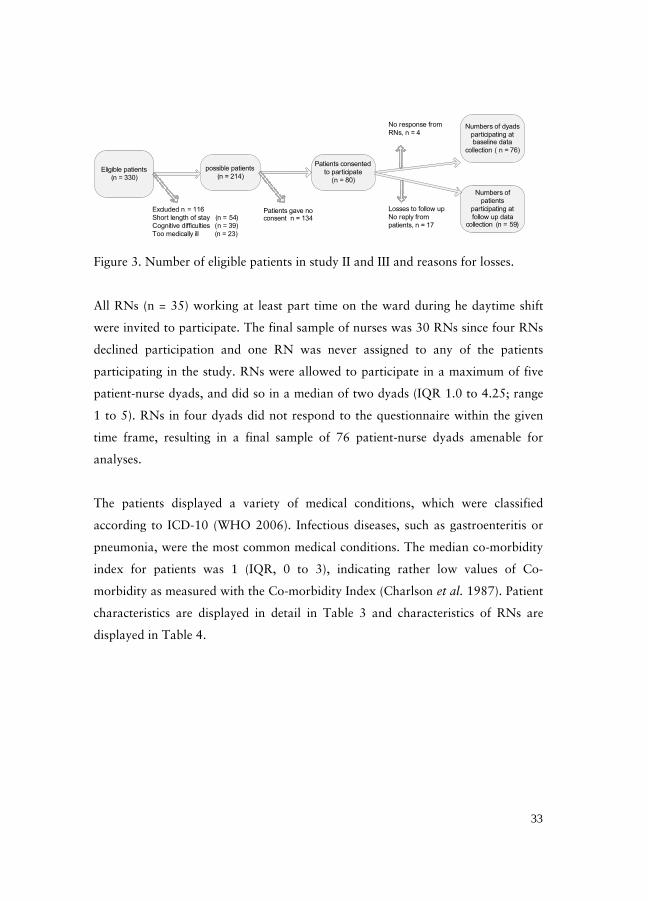
in poor health condition. Eligible participants and reasons for dropouts are
displayed in Figure 3. A final sample of 80 patients was recruited, of whom 59
patients also provided data for follow-up comparison.
32
33
Eligible patients (n = 330)
possible patients (n = 214)
Patients consented to participate
(n = 80)
Numbers of dyads participating at baseline data
collection ( n = 76)
Numbers of patients
participating at follow up data
collection (n = 59)
No response from RNs, n = 4
Losses to follow upNo reply from patients, n = 17
Excluded n = 116Short length of stay (n = 54)Cognitive difficulties (n = 39)Too medically ill (n = 23)
Patients gave no consent n = 134
Figure 3. Number of eligible patients in study II and III and reasons for losses.
All RNs (n = 35) working at least part time on the ward during he daytime shift
were invited to participate. The final sample of nurses was 30 RNs since four RNs
declined participation and one RN was never assigned to any of the patients
participating in the study. RNs were allowed to participate in a maximum of five
patient-nurse dyads, and did so in a median of two dyads (IQR 1.0 to 4.25; range
1 to 5). RNs in four dyads did not respond to the questionnaire within the given
time frame, resulting in a final sample of 76 patient-nurse dyads amenable for
analyses.
The patients displayed a variety of medical conditions, which were classified
according to ICD-10 (WHO 2006). Infectious diseases, such as gastroenteritis or
pneumonia, were the most common medical conditions. The median co-morbidity
index for patients was 1 (IQR, 0 to 3), indicating rather low values of Co-
morbidity as measured with the Co-morbidity Index (Charlson et al. 1987). Patient
characteristics are displayed in detail in Table 3 and characteristics of RNs are
displayed in Table 4.
33
34
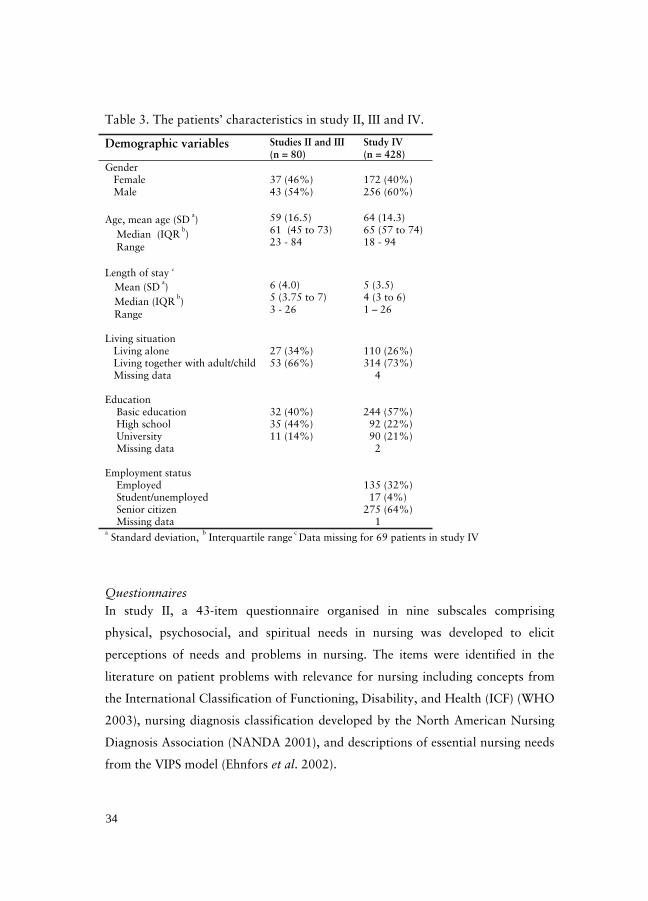
Table 3. The patients’ characteristics in study II, III and IV.
Demographic variables Studies II and III (n = 80)
Study IV (n = 428)
Gender Female 37 (46%) 172 (40%) Male 43 (54%) 256 (60%)
Age, mean age (SD a)
Median (IQR b)
Range
59 (16.5) 61 (45 to 73) 23 - 84
64 (14.3) 65 (57 to 74) 18 - 94
Length of stay c
Mean (SD a)
Median (IQR b)
Range
6 (4.0) 5 (3.75 to 7) 3 - 26
5 (3.5) 4 (3 to 6) 1 – 26
Living situation Living alone 27 (34%) 110 (26%) Living together with adult/child Missing data
53 (66%) 314 (73%) 4
Education Basic education 32 (40%) 244 (57%) High school 35 (44%) 92 (22%) University Missing data
11 (14%) 90 (21%) 2
Employment status Employed 135 (32%) Student/unemployed 17 (4%) Senior citizen Missing data
275 (64%) 1
a Standard deviation,
b Interquartile range
c Data missing for 69 patients in study IV
Questionnaires In study II, a 43-item questionnaire organised in nine subscales comprising
physical, psychosocial, and spiritual needs in nursing was developed to elicit
perceptions of needs and problems in nursing. The items were identified in the
literature on patient problems with relevance for nursing including concepts from
the International Classification of Functioning, Disability, and Health (ICF) (WHO
2003), nursing diagnosis classification developed by the North American Nursing
Diagnosis Association (NANDA 2001), and descriptions of essential nursing needs
from the VIPS model (Ehnfors et al. 2002).
34

35
Table 4. Characteristics of nurses in study II and III.
Demographic variables Study II and III
(n = 30)
Gender Female 29 (97%) Male 1 (3%)
Age Mean age (SD
a)
Median (IQR b)
Range
34 (8.7) 31 (28 to 40) 23 - 59
Time since registration as a nurse Mean years (SD
a)
Median years (IQR b)
Range
4.6 (8.1) 1.5 (1 to 4) 0.1 - 36
Employment as a nurse at the ward Mean years (SD
a)
Median years (IQR b)
Range
3.2 (6.4) 1 (1 to 3) 0.1 - 35
aStandard deviation,
bInterquartile range
Responses to each item are made in three subsequent steps: (1) to identify the
presence of a problem by indicating “yes” or “no”, (2) to describe the severity of
the problem on a four-point ordinal scale ranging from a ‘mild problem’ to a ‘very
severe problem’, and (3) rate the importance of the problem using a four-point
ordinal scale ranging from ‘not important’ to ‘very important’. If no problem was
identified in step 1, the respondent ticked the box ‘no problem’ and continued
responding to the next item. The questionnaire eliciting RNs perceptions was
identical to that of the patients but the statements reflected a professional
perspective on a specific patient.
Card sort technique The Control Preference Scale (CPS) developed by Degner and Sloan (1992) was
used in study III and IV in a slightly modified way. CPS is a card sort technique
displaying five decision-making roles in the interaction between patient and
35

36
physician. The cards should be ordered from the most preferred option to the least
preferred, which would create an ordinal scale ranging from ABCDE to EDCBA,
representing different degrees of patient control. There are 120 possible
permutations of the cards. The CPS has previously been used to elicit patients’
preferred roles in decision making in medical care (Degner & Sloan 1992; Beaver
et al. 1996, Beaver et al. 1999, Ramfelt et al. 2000). In this research project, the
wording of the cards was modified to focus on the nurse-patient relationship and
decision making in nursing; further, the scale order was reversed in order to
describe increasing degree of patient control from A to E. The cards now ranged
from a passive role (cards A and B), through a collaborative role (card C) to an
active role (cards D and E) as displayed in Figure 4.
In study III, patients used the CPS to state their preferred clinical decision-
making role in the following dimensions: (1) needs of nursing care in general, (2)
physiological needs and (3) psychological/spiritual needs. The cards were presented
I prefer to make the final selection about which treatment I will receive
I prefer to make the final selection of my treatment after
seriously considering my nurses’ opinion
I prefer that my nurses and I share responsibility in
deciding which treatment is best for me
I prefer that my nurses make the final decision about which
treatment will be used, but seriously considers my opinion
I prefer to leave all decisions regarding the treatment to my
nurses.
Active role
Collaborative role
Passive role
A
B
C
D
E
Figure 4. The card options in the modified Control Preference Scale
36

37
in the fixed order A, B, C, D, and E before each response. The wording of the
cards was also used as categorical descriptions described in questionnaires in both
study III and IV. In study III, RNs stated how they perceived their patients’
preferences for participation in clinical decision making by ordering the role
descriptions A, B, C, D, and E. The wording of the descriptions was rephrased to
reflect an outside perspective: ‘The patient prefers to…’ instead of ‘ I prefer to…’.
A follow-up self-reporting questionnaire to elicit patients experienced participation
in clinical decision making was based on the same categorical descriptions. The
questionnaire covered both physical and psychological/spiritual needs, divided into
nine broad areas labelled according to some of the key words for current health
status in the VIPS model (Ehnfors et al. 2002). The nine categories were
communication, breathing and circulation, nutrition, elimination, skin care,
activity, sleep, pain, and psychosocial needs and problems. Patients stated their
preferences by selecting one card for each of the nine areas, if applicable, that best
described their decision-making role during the recent hospitalisation.
ProcedureThe patients responded to the questionnaire (paper II) through structured
interviews, taking approximately 15 minutes. The interviews were conducted in
each patient’s room. Patients’ median time on the ward before completing the
questionnaire was 26 hours (IQR 20 to 39 hours). The patients then continued
responding by ordering the options in the CPS (paper III). The RN assigned to the
patients’ care received a corresponding questionnaire and was asked to complete it
during the current work shift. This questionnaire, however, included the additional
questions abut patient preferences for participation. All questionnaires were coded
so that the answers from the patient-nurse dyads could be identified. Patients
received the follow-up questionnaire before leaving the hospital and could either
respond directly by handing in the questionnaire in a sealed envelope or take it
home and return it by mail in a pre-stamped envelope. Agreements were made with
37

38
five patients having severely impaired vision to respond to the follow-up
questionnaire by a telephone interview conducted within a week from discharge.
Study IV A cross-sectional comparative survey design was applied collecting data from
patients recently being cared for in acute somatic hospital care. In all, 15 wards
participated, which included internal medical wards, orthopaedic, surgical, and
cardiology wards at a university hospital and a regional hospital in Sweden.
Sample and characteristics Respondents were recruited from the group of approximately 2000 patients who
had been discharged in April to June 2006 at the participating wards. Further,
participants should be 18 years or older for inclusion. Exclusion criteria were lack
of ability to communicate in Swedish and cognitive deficits hampering the ability
to participate, as judged by the RNs before discharge. Totally, 876 persons gave
informed consent to the wards to communicate personal contact information
about them to the research team and thus were eligible for inclusion in the study.
Totally, 487 responses from patients were received, making up 56% of the eligible
population. However, 59 respondents did not answer the key question about
participation preferences and were therefore excluded, which leaves a final sample
of 428 responses (49%) amenable for analyses.
The patients displayed a broad disease spectrum, reflecting the specialities of
participating wards. Totally, 127 patients were treated for circulatory system
disorders (e.g., myocardial infarction, angina pectoris, and arrhythmias), 64 for
various surgical diseases (e.g., diseases from the abdomen and urinary tract), 40 for
various cancer diseases, 37 for disorders in the skeletal system (e.g., fractures,
arthritis, and lumbago), 20 for respiratory diseases (e.g., acute breathing problems,
chronic obstructive lung diseases, and pneumonia), and 62 were categorised as
others, classified with the International Classification of Diseases (WHO 2006),
hereby including a variety of disorders not being placed in the before mentioned
38

39
categories. A total of 78 values were missing because of lack of 69 patients’
consent to extract the information from the record and because 9 patient records
were not found at the time. Median co-morbidity index was 1 (IQR, 0 to 2),
indicating rather low values of co-morbidity as measured with the Co-morbidity
Index (Charlson et al. 1987)
Questionnaire The categorical descriptions derived from the CPS were used, with respondents
selecting the one description that best described: (1) their preferences for
participation, and if applicable, (2) experienced degree of participation during their
recent hospitalisation. The questionnaire consisted of a global question about
participation in the area of nursing needs in general. Further, questions were posed
on a more detailed level for physical and psychological/spiritual needs. The
category labels, derived from the key words for current health status in the VIPS
model (Ehnfors et al. 2002), were communication, breathing and circulation,
nutrition, elimination, skin care, activity, sleep, pain, psychosocial, and
spiritual/cultural needs and problems. However, only the global question
concerning nursing needs in general is reported in paper IV. The questionnaire also
elicited patient characteristics such as age, gender, education, living conditions, and
employment status. Moreover, a measurement of personal disposition was used
based on the following three questions proposed by Lundberg & Nyström Peck
(1995): [1] Do you usually see solutions to problems and difficulties that other
people find hopeless? [2] Do you usually feel that your daily life is a source for
personal satisfaction? [3] Do you usually feel that things happening to you in your
daily life are hard to understand? Responses were given on a 3-point ordinal scale
with the categories: ‘no’, ‘yes, sometimes’, and ‘yes, always’. Additionally, nine
questions related to clinical decision making were identified and elicited from the
Empowerment scale (Faulkner 2001). The response set for these items was a 3-
point scale with the categories: ‘no’, ‘yes, sometimes’, and ‘yes, often’, with a
possibility to state ‘not applicable’.
39

40
Patients weighted sum of co-morbidity conditions was described using Charlson’s
Co-morbidity Index, where the patients’ medical diagnoses received a weight
ranging from 0 to 4 points depending on the seriousness of the condition (Charlson
et al. 1987).
ProcedureAfter permission obtained by written informed consent, names and addresses of
discharged patients were communicated once a week from the wards to the
research team. Information about the study and invitation to participate was sent
by mail to all persons on the lists within eight days from discharge, including a
form for informed consent to participate and a questionnaire. The informed
consent also included permission to abstract some information from the patient’s
record. A pre-paid return envelope was included for the responses and non-
respondents received a reminder letter within three weeks.
Reliability and validity Face validity of the QOD scale (study I) was judged to be good through minor
pilot testing of the understandability and usage of the scale. Content validity was
established by identifying characteristics in existing instruments and the ongoing
professional discussions in the literature on requirements for nursing diagnoses
statements. The facet of the construct is restricted to the structural quality of the
diagnostic statement to a high extent and is not intended to reflect the accuracy of
the diagnosis in the clinical arena. Estimates of internal consistency for the QOD
scale showed a Cronbach’s alpha coefficient value of 0.863. Concurrent validity of
the QOD scale was estimated by the use of items in CAT-CH-ING (Björvell et al.
2002), showing a correlation of 0.31 between measures, which was judged as
reasonably good considering that the two measures do not reflect exactly the same
dimensions in the concept nursing diagnosis. Interrater reliability was calculated
for 10% of the sample, showing a Kappa value of 0.93 for the whole QOD scale.
A kappa value > 0.75 was interpreted as excellent agreement (Fleiss 1981).
40

41
Cronbach’s alpha for the 43-item questionnaire developed in study II was
0.875, which was obtained after removal of the item dental hygiene from the scale
because of zero variance. Alpha values exceeded the suggested minimal value of
0.75 for a scale to be considered reliable (Nunally 1978).
The reconstruction and rephrasing of the items in the CPS scale (study II and
III) was tested on a small group of patients and nurse specialists, indicating that it
measured the same concept and showed good face validity. The use of the scale as
response categories in a questionnaire is a modification that has previously been
used (e.g. Ford et al. 2003; Doherty & Doherty 2005).
A pilot test in study IV of the questionnaire’s comprehensibility and
understandability was conducted to test face validity. This test led to minor
revisions of the wording and layout of the questionnaire.
Ethical considerations Patients and RNs in study I-IV were invited to participate in the studies after
receiving written and/or verbal information. Participants were informed about the
voluntary nature of participation, the right to withdraw at any time, and
confidential handling of the data. In particular, patients were informed that their
decision to participate or not in the study was a separate issue without any
connection to their care or relation with the staff. Informed consent to participate
was elicited verbally from patients and RNs in study II and III and in writing by
the respondents in study IV. The researcher and not the staff performed data
gathering in study II and III. The patients in study IV were approached after
discharge, thereby reducing a possible ‘white coat’-effect. Written permission to
conduct the studies was obtained from chief executives at the clinics. No ethics
review was performed in study I since it did not directly involve patients or
intervene with the care given and was regarded as ethically correct according to
prevailing national research ethics praxis. Data were collected through a
retrospective review of patient records stripped from personal identification to
41

42
preserve anonymity. The research ethics committee at Uppsala University gave
approval to study II and III (No. 275/02) and study IV (No. 355/2005).
Data analyses For descriptive purposes in study I – IV, raw numbers, percentage proportions,
means, standard deviation, median, interquartile range, and range were used
depending on the properties of the data (Altman 1991). SPSS version 11.0, 13.0
and 14.0 were used for analyses. The level of statistical significance was set to
0.05.
In study I, data were treated as interval data and a subsequent paired student’s t-
test was used in analyses of differences between pre- and post-test performance.
After categorisation of the diagnoses, the Chi-square test was used to make
analysis of differences between groups.
In study II, data were derived from paired observations in which the patients’
perceptions were seen as the gold standard. Wilcoxon’s signed-rank test analysed
differences between groups for continuous variables. Sensitivity, specificity, and
predictive values on the RNs’ perceptions in relation to patient perceptions were
calculated. McNemar’s test was employed to analyse agreement/disagreement
between groups for categorical data. Finally, the pattern of
agreement/disagreement between the pairs of ordered categorical values was also
analysed using the methodology developed by Svensson (Svensson 1998; Svensson
& Starmark 2002).
In study III, the Sign test was used for analysing differences between patients
and RNs’ perception of the patients’ most preferred role in clinical decision
making. Differences between subgroups, identified by gender, social situation, and
age, were analysed using the Mann-Whitney U test. A discrepancy score was also
calculated by subtracting the preferred role score from the experienced role score.
In study IV, univariate logistic regression analyses were performed to examine
relationships between independent and dependent variables. The five categories of
42

43
the variable preferred decision-making role (dependent variable) was dichotomised
into ‘passive’ versus ‘active’ for purposes of multiple regression analyses, where the
mid alternative (I prefer that my nurses and I share responsibility for deciding
which treatment is best for me) on the scale was referred to as passive. Multiple
logistic regression analyses were employed with variables showing a significant
relationship with the dependent variable as explanatory variables. The variable
occupation was also included in the analysis since the p-value was in the realm of
significance. Odds ratios and probability values for adopting an active role in
clinical decision making were calculated. Cohen’s kappa and percentage agreement
were used for analyses of interrater reliability. Spearman’s rho and Cronbach’s
alpha coefficient were used as validity measures.
43

44
RESULTS
Quality of nursing diagnoses (Paper I) The quality of RNs formulation of nursing diagnoses improved at the experimental
ward after education and implementation of new forms for recording, whereas no
improvement was found at the control wards. However, control wards could not
act as true controls because of significant differences between wards on the
outcome variable at pre-test. Thus, the control wards could serve merely as a
comparison in general terms (Figure 5). The frequency of specific diagnoses stated
at the experimental ward after the intervention was doubled, whereas mere
problem statements decreased with 50%. The average diagnostic quality score at
the experimental ward increased from 6.5 to 8.8 points. No quality improvement
of the diagnostic statements was observed for the problem component in which
average scores were high at both measurement times. However, the quality values
improved concerning the etiologic component, the sign/symptom component, and
the general component as well. Five diagnoses obtained the maximum score of 14
points and 10 points or more were identified at post-test in 49% of the diagnoses
(n = 28) as compared with 29% (n = 16) at pre-test.
No quality improvement of the diagnostic statements was observed at the control
wards over time for any of the four components. The average diagnostic quality
scores obtained before and after the intervention period were 4.3 and 4.4,
respectively. In general, serious flaws in the use of the aetiology component were
found. The etiologic component was not identified in 37% of the diagnoses, and
when present, the descriptions lacked precision and were largely not potentially
changeable with nursing care. Notably, the patients’ needs or problems often
focused on medical conditions and were not documented at all in 33% of the
patient records in the control wards and 13% in the experimental ward.
44

45
05
10152025303540
experimentpretest n=56
experimentpost test
n=57 *
controlpretest n=36
control posttest n=42
frequ
ency
problem statement general diagnoses specific diagnoses
* improvement in the experimental ward at post-test, X2 (2) = 12.69; p< .01
Figure 5. Diagnostic levels at pre- and post-test for experimental and control wards.
Congruence in perception of needs (paper II) A rather large discrepancy in identification was revealed between patients and
RNs’ perceptions of patient needs. RNs, in general, identified more needs than the
patients did, while 38% of the RNs identified fewer needs. However, the needs
perceived by patients were identified by the RNs with a sensitivity of 0.53 and a
predictive value of 0.50 (Table 5).
Lowest mean sensitivity values were found for needs related to the areas Nutrition
(0.22) and Emotions/spirituality (0.24). Furthermore, low positive predictive
values for the subscales indicate that RNs and patients often identified different
problems.
45

46
Table 5. RNs’ sensitivity, specificity, and predictive values of problems perceived by patients (n= 614), displayed for subscales.
Subscale Number of problems
n
Sensitivity
m (SD)
Specificity
m (SD)
Positive predictive value in %
Communication 16 0.31 (0.27) 0.94 (0.05) 31
Breathing/circulation 59 0.57 (0.09) 0.84 (0.11) 59
Nutrition 104 0.22 (0.26) 0.90 (0.11) 25
Elimination 47 0.42 (0.35) 0.91 (0.06) 38
Skin 35 0.49 (0.54) 0.89 (0.13) 60
Activity 51 0.80 (0.22) 0.82 (0.03) 35
Sleep/tiredness 124 0.55 (0.14) 0.60 (0.19) 51
Pain/sensory perception 86 0.34 (0.29) 0.78 (0.12) 44
Emotions/spirituality 92 0.24 (0.21) 0.81 (0.15) 20
Total 614 0.53 (0.29) 0.85 (0.11) 50
Patients identified 309 needs that were not identified by their RNs, including
several severe needs (33%), particularly in the areas of Nutrition, Sleep, Pain, and
Emotions/spirituality (Figure 6). RNs underestimated the severity in 47% of the
305 mutually identified problems. The RNs perceived the same degree of severity
as reported by the patients in 27% of the needs, whereas a higher degree of
severity was perceived in 27%. Estimated values for Relative Position (RP)
indicated systematic disagreement in position on the scale, whereas values for
Relative Concentration (RC) indicated minor overall systematic disagreement in
concentration. A rather large individual variation in pairs of responses,
unexplained by the systematic disagreement, was revealed by relative Rank-
Variance (RV) estimates. An overall agreement of the importance of patient
problems was found in 44% of the needs.
46

47
Figure 6. Frequency of problems identified by either patients or nurses.
The RNs underestimated the importance of 273 of the 305 mutually identified
needs. The RNs underestimated the importance of 32% of the needs and
overestimated the importance in 24%. Low values on RP and RC indicated minor
systematic differences, whereas the RV value indicated a moderate individual
variance between nurse and patient perceptions.
Participation in clinical decision making (paper III) Patients most frequent choice of preference order for nursing needs in general was
ABCDE, going from passive to active, (20%, n = 16) and for RNs it was CDEBA
(14%, n = 11). Patients never chose the option E as their first choice of preference,
whereas the RNs did so in 12 of the 76 dyads. Patients preferred to be more active
in clinical decision making concerning psychosocial needs and physical problems as
compared with needs for nursing in general. In comparison with RNs perceptions,
patients preferred a more passive role in clinical decision making for nursing needs
in general. More specifically, 61% of the patients preferred a passive role, whereas
the RNs perceived that only 24% of the patients preferred such a role. An active
role was preferred by 9% of the patients, whereas the RNs perceived that 45% of
the patients preferred to be active participants (Table 6).
nurses
0 20 40 60 80 100
Psychosocial
Pain
Sleep
Activity
Skin care
Elimination
Nutrition
Breathing
Communication
Number of problems
patients
0 20 40 60 80 100Number of problems
mild
moderate
severe
extremelysevere
47

48
Table 6. Distribution of patients’ (n = 76) and RNs’ (n = 76) first choice concerning patients’ role of participation in clinical decision making for general, physical, and psychosocial nursing needs.
Participatory role TypeOf needs
Passive role (cards A and B)
Shared role (card C )
Active role (cards D and E)
Missing data
Total
% n % n % n n % n Patients 61 46 30 23 9 7 0 100 76
Needs in general RNs 24 18 32 24 45 34 0 100 76
Patients 41 31 24 18 34 26 1 100 76Physical needs
RNs 7 5 12 9 82 62 0 100 76
Patients 37 28 37 28 25 19 1 100 76Psychosocial needs
RNs 4 3 24 18 72 54 1 100 76
The RNs in 64% (n = 49) of the dyads perceived that their patients preferred a
more active participatory role than the patients’ own perceptions. The RNs
perceived that their patients preferred a more passive role in 20% (n = 15) of the
dyads, whereas there was agreement about the preferred role in 16% (n = 12). In
general, 29% of the patients (n = 80) perceived that the actual decision-making
role cohered with the preferred role, whereas 37% had been more passive and
34% more active than they had preferred to be. The patients made 228 judgements
about the experienced participatory role across the nine specific categories of
needs. The patients had been more active than preferred in 88 (39%) of those
judgements and more passive in 94 (41%). An actual role matching the preferred
role was found in 46 (20%) of the judgements (Figure 7).
Predictors of preferences for participation (paper IV) Respondents in general preferred adopting a passive role in clinical decision
making in nursing, most commonly preferring option B, indicating that “my nurses
make the final decision about which treatment will be used, but seriously considers
my opinion”. No significant relationships were found between the dependent
variable and the age of the patients, length of stay, medical speciality, occupational
48

49
Figure 7. Relative distribution of discrepancy scores for patients’ preferred and actual role in clinical decision making in nursing care (n = 228).
status, previous working experience in the health care system, or experience from
hospital care as such or from the actual ward. Nor was any relationships identified
in relation to the measured internal disposition factors: perceived ability to find
solutions on problems/difficulties that others find hopeless, perspective on daily life
as a source of personal satisfaction, and perceived difficulties understanding things
happening in daily life. However, multiple regression analyses showed that gender,
education, living conditions, and occupational status were related to active role
preferences (Table 7). Females were 1.8 times more likely to prefer an active
decision making role as compared with male respondents, whereas respondents
living alone were 1.8 times more likely to prefer an active role compared with
respondents living together with someone else, be it another adult or a child.
Higher educated respondents more likely preferred an active role (odds ration 2.2)
compared with those with lower level education. At the same time, senior citizens
were more likely to prefer an active participation (odds ratio 2.0) compared with
respondents who were working, unemployed, or students.
49

50
Table 7. Odds ratio for patient (n = 428) preference for active participation
Variable Univariate analyses Multivariate analyses
ORa CI b p-value ORa CI b p-value Gender 1.922 1.213 – 3.045 .005 1.762 1.089 – 2.853 .021
Living conditions
2.147 1.316 – 3.504 .002 1.818 1.086 – 3.043 .023
Education 1.384 1.054 – 1.818 .019 2.210 1.329 – 3.677 .002
Occupation 1.623 .0982 – 2.683 .059 1.982 1.133 – 3.466 .017 a OR, odds ratio b CI, confidence interval
A probability value of 53% was estimated that female senior citizens with high
education and living alone would prefer an active role in decision making. A
probability value for men in the same situation was estimated to 39%. At the same
time, working females with low education living together with someone had a
probability value of 13% for preferring active participation in decision making.
The corresponding figure for working men living with someone was 8% (Table 8).
Table 8. Probability values for active participation preferences depending on patient (n = 428) characteristics. Men
%Women
%Gender 18 29 living alone 26 38 living together 15 24 living alone, low education 22 33 living alone, high education 33 46 living together, low education 12 19 living together, high education 20 30 living alone, low education, working 13 21 living alone, high education, working 25 37 living together, low education, working 8 13 living together, high education, working 15 24 living alone, low education, senior citizen 23 34 living alone, high education, senior citizen 39 53 living together, low education, senior citizen 14 22 living together, high education, senior citizen 26 39
50

51
DISCUSSION
The overarching questions of this thesis concern clinical decision making in nursing
care planning and patient participation in this process. To fulfil the intentions and
utilise the potential of patient-centred or individualised nursing care there needs to
be a mutual understanding between RN’s and patients - an understanding of what
constitutes the patient’s need for nursing care, and what are the relevant actions to
reach the goal of care, as well as the roles in the interaction between patients and
RNs. However, the present findings indicate that the diagnostic statements of RNs
need to improve and can be improved in a short time frame through education.
Furthermore, there was a discrepancy between the RN and the patient in the
perception of the patient’s needs, which might hamper the quality of the decision
making as a foundation for care decisions. At the same time, patients preferred
adopting a passive role in clinical decision making, where gender, education, living
conditions and occupational status were identified as predictors of active
participation.
The identified discrepancies between patients and RNs’ perceptions of needs
and role preferences form the basis for a model of clinical decision making (Fig. 8),
modified from Brunswik’s lens model (Brunswik 1956) as reported in Dowding
and Thompson (2003). Both the patients and the RNs’ subjective perspectives need
to be considered in clinical decision making, as this would allow participation in
accordance with the patients’ preferences. The aim of the process is a common
understanding through a shared decision-making process with mutual information
exchange. Extensions could be made to involve the family as a third actor, which
would create a decisional triad (Dalton 2003; Ishikawa & Yamazaki 2005). In this
thesis, a modification of Brunswik’s lens model is proposed involving both the
patient and the RN in the decision-making process. The modified model also
depicts that patients and RNs possibly utilise different cues with different
weighting of the cues resulting in their respective subjective judgements of the
situation at hand, where ultimately these are united and form a common
understanding.
51

52
Y e
Y nurse
X 2
X 4
X 1
X 5
CUES
CUE UTILIZATION
VALIDITY
CRITERION
JUDGEMENT
ACHIEVEMENT
Y patient
Y nurse
Y patient
COMMON UNDERSTANDING
X 3
Study I
Study IV Study II and III
Figure 8. Model of clinical decision making to reach a common understanding (modified from Brunswik 1956)
The findings of differences in perceptions of needs and patients’ preferred
participatory role is useful in discussions about patient-centred care, and the need
for personal interaction between two subjects- the patient and the RN. The
findings are discussed in further details in the following section.
Quality of nursing diagnoses A combination of education and new forms for recording (study I) seemed to be a
way to improve the RNs’ documentation skills (e.g., the quality of nursing
diagnoses). However, because of pre-test differences between groups, the initial
study design could not be utilised and the degree of improvement was not possible
to determine. The improvement of documentation practice in a short time frame in
the experimental ward supports previous findings (Fagrell et al. 1998; Björvell et
al. 2002), although the sustainability over longer time remains unanswered in this
study. No similar improvement was identified in the control wards, implying that
52
53
change of professional practice requires external triggering and facilitation
(Rycroft-Malone et al. 2004b). This finding is in contrast to reports that improved
documentation practice occurs over time in the control group as well (Björvell et
al. 2002). A longer time span for follow-up and threats to internal validity (such as
effects of history and maturation) could explain such improvements.
Identification of the aetiology component in the diagnosis seemed to be the
most crucial step, with remaining difficulties to achieve focus and precision in the
statement. This flaw in diagnostic statements is in line with previous findings
(Minton & Creason 1991, Dobrszyn 1995).
Congruence in perception of needs Despite how well RNs manage to express their perceptions of the patients’ health
care needs in diagnostic statements, the diagnoses can be questioned if the RNs
have made inaccurate assessments of the patients’ needs. However, it must be
pointed out that accuracy is not absolute; it is depending on one’s perspective and
purpose (Fiske 1993). Further, there is not an absolute demand that the patients
should agree: RNs sometimes need to state diagnoses and plan care without having
a mutual understanding with the patient about the situation, i.e. lack of knowledge
in handling daily life as a diabetic. Furthermore, the patients cannot always
participate and give their perspective (e.g., because of cognitive deficits) in which
case an RN or a significant other needs to function as a proxy. Here, the
interpreter burden is extremely high and RNs advocacy task needs to be done with
high sensitivity and respect for the person’s values and integrity.
RNs had considerable difficulties in identifying the needs perceived by their
patients, at least during the initial phase of the hospital period (II). The RNs
inability to identify needs on an individual basis in this study is consistent with
previous findings (Farrell 1991; Lauri et al. 1997; Löfmark et al. 1999; Adamsen
& Tewes 2000). Several needs were perceived by either the patient or the RN, but
not by both at the same time. The RNs identified about half of the patients’
perceived needs, of which one out of four was described with the same degree of
53

54
severity as the patients described them. A mutual perception of the importance of
attending to the needs was reached in less than half of the cases. Other studies have
reported RNs’ recognition of patient-perceived needs with 70% agreement or
better (Adamsen & Tewes 2000; Hansen et al 2002). However, comparisons
between studies are difficult because of different study designs and varying
populations and settings. The present study used nurse-patient dyads as the basis
for comparison, whereas other studies have used a group of RNs’ perceptions of
the patients’ situation, elicited from focus group interviews (Adamsen & Tewes
2000), perceptions of a general patient population and not in relation to specific
patients (Hallström & Elander 2001b), and from dyads in which the RNs chose an
appropriate patient whom they thought they knew well (Löfmark et al. 1999). The
lower levels of agreement in our study might reflect the different samples and time
frames used. It is noteworthy that many of the needs perceived by either the patient
or the RN were found within the same areas: nutrition, pain, sleep/tiredness, and
emotions/spirituality. Standardised tools are available for assessment of nutrition
(e.g., Vellas et al. 1999) and pain (e.g., Gaston-Johansson 1996), but are not
widely used in clinical practice, whereas tools for assessing psychosocial features
are not available to the same extent. The use of more structured assessment
methods is anticipated to support high quality decision making. In a study by
Abayomi and Hackett (2004) RNs subjective risk assessment overlooked one third
of patients identified with standardised risk score assessment. The correct
categorisation of patients was 57%, just above a random categorisation, which
supports the findings in this study with low sensitivity values based on subjective
assessment. The RNs omitted many patient-perceived problems of pain and
underestimated the severity of about one third of the mutually identified problems,
which supports findings that RNs underestimated the patients pain (Blomqvist &
Hallberg 1999; Hall-Lord et al. 1999; Hovi & Lauri 1999; Sloman et al. 2005),
indicating a risk for undetected and untreated pain. The patients in study II
expressed several needs in the psychosocial realm (e.g., anxiety, loneliness) that the
RNs were not aware of, which supports findings showing that 23% of patients
54

55
with cancer reported unmet psychological needs (Kent et al. 1996; Soothill et al.
2001).
In Sweden, it is customary that the assigned RN assesses the patient at admission
and then makes a clinical judgement of the patient’s care needs, but it is not
common to use standardised assessment tools. After a thorough assessment, the
RN should “know” the patient’s perspective and be able to combine that with
knowledge that is of a more professional nature when planning care. The use of
standardised assessment tools could increase the accuracy in patient assessment,
especially if the patient contributes with data as well. Promising results have been
reported, i.e. decision support aids for patient preference based care planning
(Ruland 1998; 1999; Ruland & Moore 2001), and challenges for nursing
informatics to meet patients needs and facilitate information exchange have been
depicted (Gassert 1998). There is however, a backside with the use of standardised
tools, namely the risk that the RNs critical reflective thinking will be hampered.
The format chosen and the pre-formulated statements available might narrow the
thinking about the patient and the situation at hand.
The patients and RNs’ merging perspectives of the health situation are vital
parts in creating individualised nursing care. An essential subjective component
needs to be taken into account when identifying needs of nursing care, goals, and
actions, i.e. the patient’s preferences. Low-level agreements on what constitutes the
patient’s health care needs will hamper the possibility to plan individualised care in
accordance with the preferences and values of the patient. The identified lack of
congruence in perceptions imply the existence of a “non-communicating/nurse-
centred” care (Casey 1995) by which the nurse makes assumptions about patients’
needs, wishes, and abilities based on her/his subjective opinion. RNs ‘naming’ and
‘framing’ of patients’ needs in the encounter - negotiation of need and role
perceptions - do not seem to have taken place as outlined by Carr (2004). It can be
assumed that over time the RNs would have identified more of the needs perceived
by the patients, but considering the limited length of stay in hospital care there is
not much time to correct an initial lack of congruence in perceptions.
55

56
Participation in clinical decision making The present findings indicate that RNs failed to assess the patients’ preferences
accurately, and possibly articulated perceptions rooted in a general view of a
standardised patient population instead. The patients preferred a rather passive
role in clinical decision making in nursing care, whereas RNs perceived the patients
to prefer to be more active (study III and IV). Preferences for adopting a passive
role, in this analysis including a shared role, have previously been reported such as
in samples of cancer patients (Beaver et al. 1996, Beaver et al. 1999, Ramfelt et al
2000). The fact that the decision-making task in this study was quite vague,
focusing on nursing needs in general might have affected the patients’ preferences
for a passive role. The finding that patients in study III preferred to be more active
in decision making concerning physical or psychosocial needs compared with needs
in general supports this interpretation. There is a tendency in Western societies to
draw the conclusion that active participation is the preferred behaviour of patients.
However, several studies have shown that not all patients want to be active in
decisions about their care (Waterworth & Luker 1990; Biley 1992; Cahill 1998).
Furthermore, the patient’s choice of a passive role in clinical decision making can
be a deliberate action, which indicates a not totally passive role but more of an
active decision to adopt a passive role.
Personal characteristics, such as gender, education, living conditions, and
occupational status, were all associated with patients’ preferences for adopting an
active role in clinical decision making (IV). Female senior citizens with high
education and living alone were more likely to prefer an active role, whereas male
respondents with low education, working, and living together with someone
displayed the lowest probabilities for adopting an active role. High education as a
predictor of active participation has previously been identified (Beaver et al. 1996;
O’Connor et al. 2003; Sanders & Skevington 2003) though the findings that active
participation was preferred by senior citizens (study IV) and persons living alone
(study III and IV) are in contrast with several reports (Hämäläinen et al. 2003;
Lemonidou et al. 2003; Sainio & Lauri 2003). In study IV, women preferred
adopting an active role, which supports some findings (Kristensson-Hallström
56

57
1999; Sainio & Lauri 2003), but are in contrast to other findings of low
preferences for active participation among women (Hämäläinen et al. 2003) or no
differences related to gender (Butow et al.1997, Caress et al. 2002). The focus in
this study on needs of nursing, instead of medical decision making, might explain
why persons living alone preferred to be more active participants than persons co-
habiting, contrasting reports where persons living together adopted a more active
role in medical decision making (Sainio & Lauri 2003). Single people may have to
take on the responsibility for their daily life, whereas persons who are co-habiting
can rely on their next of kin being interested in their wellbeing as well. Women’s
preferences for more active participatory roles might be explained by social role
expectations, historically and culturally fostered and expected to be interested in
taking care of themselves, as well as attending to others. Taking responsibility for
care is more intertwined in the female social role than in the male role. A diffusion
of roles in this aspect has happened over time, but a diversion is still thought to be
common in older age groups. However, it should be noted that a majority of the
respondents preferred adopting a passive role.
In this study age was not a predictor for participation, which is in contrast with
an extensive amount of previous findings (mostly in medical decision making) in
which younger patients tended to prefer more active roles (Beaver et al. 1996;
Frosch & Kaplan 1999; Runesson 2002; Henderson & Shum 2003; Hämäläinen et
al. 2003; Sainio & Lauri 2003; Kidd et al. 2004). However, age is implicitly
related to being retired or working, so age must be taken into account when
interpreting the findings. Explanations to why older persons are more reluctant to
participate in decisions about their care are suggested to be found in the social
exchange theory of ageing (Kenny 1990), or that passive dependent behaviour
might be related to learned helplessness and not so much to a desire not to be in
control (Barder et al. 1994). The learned helplessness concept could be understood
in the idea of being a patient, but still, senior citizens were represented more often
in the small group of patients preferring to adopt an active role in this study. Older
patients’ higher preferences for privacy, as compared with younger patients (Bauer
1994), could possibly be a factor explaining senior citizens’ higher preferences for
57

58
participation in clinical decision making found in study IV. Older patients also
regarded control and choice as characteristics of dignity (Walsh & Kowanko
2002), which might be a factor that should be taken under consideration.
Congruence in perceptions of participation In comparison with RNs’ perceptions, patients preferred a more passive role in
clinical decision making about nursing needs in general (study III). One out of ten
patients preferred an active role whereas the RNs perceived that almost half of the
patients preferred to be active. An agreement about role preferences was found in
16% of the dyads, whereas almost two thirds of the RNs overestimated their
patients’ willingness to adopt an active role. An interpretation of these findings is
that the RNs held a generalised position based on social desirability, emphasising
the value of active patient participation based on ethical and legal points of view as
well as therapeutic values (Guadagnoli & Ward 1998, Hickey & Kipping 1998).
Thus, the RNs failed to grasp the individual’s perspective.
About one third of the patients in study III perceived that their experienced
participatory role in decision making equalled their preferences: approximately one
third perceived being more active and one third being more passive than preferred.
RNs seemed to adopt the rhetoric of patient participation but were not successful
in involving patients in decision making according to their own stated perceptions
of the patients’ preferences, not even to the level preferred by the patients
themselves, which was even more moderate. Agreement between patients’ preferred
and experienced participation in decision making, irrespective of preferred degree
of participation, is assumed to increase patients’ satisfaction with care (Lam et al.
2003) and will perhaps affect compliance with prescribed care as well.
The findings in this thesis describe a rather large discrepancy between patients and
RNs’ perspectives on role preferences as well as identification of needs for nursing.
Several factors need to be considered when interpreting the findings, of which,
some aspects are outlined below. There needs to be more transparency in clinical
58

59
decision making on various levels, both from an individual standpoint as well as
on an organisational level. The use of heuristics or disease schemata, which are
knowledge structures formed from previous experience, might be underpinning
wrongly stated initial hypotheses, leading to errors in selection of diagnosis and
treatment. Initially stated hypotheses have been seen to be maintained by
professionals even if subsequent data contradicts the hypotheses (Patel & Currie
2005).
Clinical decision making is also a question of power and who is supposed to
hold and exercise that power. There is a risk that patients’ inability to be
independent in the performance of activities in daily life is equalled with an equal
lack of ability to execute decisional autonomy. True participation might be
difficult to achieve as long as the concept of ‘patient’ is used, implying a
subordinate role relative to health professionals. At the same time, professionals
seem unable to feel comfortable and succeed in sharing power and knowledge with
the patients in practice, even though they acknowledge the idea in theory (Poulton
1999; Thorne et al. 2000; Henderson 2003). Further, health professionals’
blocking behaviours, lack of facilitating behaviours, retaining information, and
reduction of time for the encounter (Paterson 2001; Sainio et al. 2001; Runesson
2002; Martin et al. 2003; Millard et al. 2006) could all hinder active participation
of patients. Institutional constraints and the environment where nursing care takes
place need to be considered as well. Exchange of information between a patient
and a RN is a matter of mutual trust, and the organisation of care and actual ward
environment need to support an open and honest relation. Exchange of
information of a more private nature in a shared patient room at the ward might
be hampered because of lack of privacy and confidentiality. The RNs might adopt
a ‘careful conversation’ style, which would leave out more sensitive subjects and
questions (Torjuul & Sorlie 2006). The significance of time, continuity, and the
RN being present in a close relationship with the patient has been reported as
prerequisites for reaching a shared understanding in community nursing (Öhman
& Söderberg 2004). There is reason to believe that it is relevant for nursing in an
acute care environment as well. An authentic encounter characterised by an “I-
59

60
Thou” relation between patient and RN (Snellman 2001) is thought to be
beneficial for the congruence in perceptions and the quality of nursing care. These
aspects of the patient–nurse interaction have not been explicitly investigated in this
thesis. However, the conditions for the encounter and formats for eliciting patient
needs and preferences is of vital importance for the equality in the encounter as
well as the quality of the information gathered, and as a consequence to that, of
the RNs’ understanding of the patient’s perspective.
Nursing process There are several advocates for the benefits of using a structured approach for
assessment and planning of nursing care (Clark & Lang 1992; Hansebo et al.
1999; Lockwood & Marshall 1999), but standardised assessment needs to be
utilised with the aim of identifying the patient’s unique health situation as an
existential human being. The use of systematic data collection/assessment tools that
is, e.g., based on the nursing process model or the VIPS model (Ehnfors et al.
2002), always holds a risk for professional use of a check-list approach instead of a
patient-led approach, and by that a risk of overlooking the patient’s perspective.
The nursing process in itself is focused on the individual patient’s unique situation
and needs but the use of the model does not assure that the individual’s perspective
is identified. In a way, it is problematic and possibly contradictory to use a model
derived from system theory to describe and grasp health situations that, perhaps
more correctly, could be described in an existentialistic perspective. The explicit
use of a nursing philosophy or nursing theory underpinning care could be useful in
this respect. However, despite the long tradition of using the nursing process model
as a framework for problem solving, the revealed discrepancies in perceptions
between the patient and the RN indicate that patient assessment might not be
systematic and comprehensive enough to elicit the patient’s perspective. This
finding indicates that the idea, or the focus, of the nursing process model has not
been fully understood or reached. The RNs did not know their patients well
enough to grasp the patients’ perspective of their health care needs. Reasons for the
60

61
lack of agreement might be found in the still prevailing common perception of the
professionals as the expert and the patient as the help-seeker and task-oriented
organisation of nursing care. What possibilities do RNs in the Swedish health care
systems of today have to get to know the patient? RNs are often assigned to ward
duty schemes that comprise both day and night shifts, with an input on the
resource planning allowing for more personal solutions of ward duty schemes.
Furthermore, wards in Sweden are often organised according to a group allocation
system in which RNs might shift groups depending on staff mix needs. Because of
this relocation, both patients and RNs interact with several persons, sometimes
shifting on a daily basis. The organisation has thus in a way declined from the
responsibility to assure continuity in patient-nurse interaction, placing the
responsibility for continuity on the individual RN. At the same time, a division in
labour is often prevailing, with a task-oriented rather than patient-centred
organisation of care. RNs take on the responsibility for medical and administrative
activities while nurse assistants perform the nursing activities. In Sweden,
discussions about primary nursing as an ideology and way to organise nursing care
is largely absent, even though some debate has recently taken place dealing with
the concept of patient-focused care (Myers 1998) (“patientnärmre vård” in
Swedish, Inde 2006). It is also necessary to consider the environment as an
important part of caring and use the environment’s therapeutic potential in nursing
care (Edvardsson et al. 2006). RNs need to regain access to nursing tasks in acute
care settings in order to be able to identify the needs and wants of their patients.
The RNs need to be more active at bedside in all aspects of nursing care. If RNs
should provide care according to their own perceptions of patient needs, it is likely
that in some respects they would offer care that is not wanted and therefore fail to
attend to needs that are important to the patient.
Methodological considerations Considering relatively small sample sizes, non-randomised sampling procedures,
and data collection methods in need of further validation, generalisation of the
61

62
findings in study I-IV must be done with caution. Further, a general objection that
could be raised is my own involvement at the ward for infectious diseases. I was
previously employed at the ward and was involved as leader for the educational
intervention in study I. To evaluate ones own practice is not optimal, but was in
this study the only feasible way to perform data collection. Here, the evaluation of
diagnostic statements was performed in randomly selected patient records where I,
as a nurse, had participated with documented problem statements for two patients
at pre-test and post-test, which was considered to have minor effects on the
outcome. The choice to use the patient’s perception as the gold standard can be
discussed since the comparison was performed based on two subjective
perceptions.
Sample selection A common way to evaluate effects of educational interventions on documentation
practice is to compare the content in patient records before and after an
intervention (e.g., Björvell et al. 2002). This was also done in study I. Confounding
factors could be that RNs were given time to sit down and talk about
documentation practice, the researchers role as facilitator, or that the RNs were
already in a development process of their documentation practice. Staff ratios were
similar but cultural differences on the wards could play a role, primarily explaining
the initial differences in diagnostic quality between experimental and control
wards. However, the selection of patient records as the unit of analysis is
somewhat troublesome since the intervention was supposed to lead to a
hypothesised improvement in the RNs’ thinking, knowledge, and ability to
document clinical judgements. This ability is of course reflected in the recorded
content, but there is a risk that comparisons will be performed on content derived
from two partly different groups of RNs. Staff exchange happens over time so the
groups of participating RNs might vary. Further, the result could be biased if
individual RNs provide more content that is documented to the analyses than
others do, which lets individual characteristics influence the findings to a higher
62

63
extent. An alternative design would have been to compare the performance of
identified RNs before and after the intervention.
Possible threats to external validity in study II, III and IV are the sample
selection and personal characteristics of both patients and RNs, implying that
generalisation of the findings needs to be done with caution. Here, an intended
consecutive approach could not be fully accomplished and convenience samples of
patients were included in the studies (II, III, and IV). Reasons for the flaws in
sampling were difficulties on the wards with providing names of all patients that
matched the inclusion criteria because of time constraints or because of problems
in the continuity in eliciting informed consent before discharge. No systematic bias
is anticipated though generalisation of the findings should be done with great care
considering the response rate in study IV. It must be pointed out that the patients
participating in the studies were those that could talk and interact verbally with the
RNs. The group of patients thought to be most vulnerable has not been included in
the studies, and their perceptions of nursing needs and preferences of participation
could not be inferred from the reported findings. Randomised sampling procedures
would have been preferable but were not seen as feasible in the clinical settings.
Instruments The QOD scale for measuring the quality of diagnostic statements (study I) was
regarded as easy to use and showed satisfactory reliability and validity, but further
psychometric testing is warranted. The relatively narrow range of the scale might
hamper discriminative ability. However, a variety of responses were identified,
even if there was a tendency that summed scores were positioned at certain points
because of internal correlations between variables. For example, the existence of an
aetiology component was positively associated with the aetiology being specific
enough, and possible to affect. A positive association was established with the item
existence of both problem and aetiology, which is more or less implicit, leading to
a lower discriminative ability of the scale.
Needs of nursing care may vary depending on the patients’ medical condition.
There is, however, no reason to believe that the findings in study II would have
63

64
been different with patients displaying other nursing care needs since the level of
agreement in the dyads on each subscale was moderate. The 43 separate variables
in study II were identified in the literature and were not intended to lead to a
summed severity score for nursing needs. Further refinement of the questions can
be done using factor analysis, but calculation of Cronbach’s alpha measurements
was not considered necessary. The robustness and reliability of the response
alternatives over time need further testing.
The focus of the questions in study III and IV were deliberately broad: e.g., the
respondents were asked to state their preferences for participation in clinical
decision making about their nursing care as such, and not for a narrowly defined
decision. Arguments have been posed that it is illogical to ask about patients’
preferred role without assuring that they have adequate information to make
decisions (Elwyn et al. 1999). The research question posed here was intended to
describe an attitude about participation in clinical decision making, well aware
that respondents presumably used slightly different foundations for their responses.
The CPS scale was rephrased and a reversed order of response categories was used,
still thought to measure the concept of patient preferences for participation in
clinical decision making. However, the alteration made, which is a departure from
the recommended use of CPS, might have influenced the result of the analyses (e.g.,
the choice to present the alternatives in a fixed order from A to E and not pair-wise
and the transfer of the response categories into a questionnaire format). Further, it
is recommended to use Coombs unfolding theory in the analyses. According to the
theory, only 11 response alternatives fall on the main hypothesised dimension and
only these should be analysed (Coombs 1964; Degner & Sloan 2002). However, in
this thesis all combinations of the response alternatives were included in the
analyses.
Implications for practice RNs need to identify their interaction and communication with the patients as
important prerequisites for care as well as an important part of the nursing care.
64

65
RNs need to reflect on their communication skills in the assessment of patients.
There is a need for thorough and structured methods and tools for eliciting patient
preferences with regards to needs of nursing and participation in decision making
in the clinical setting. The specific methods and tools might vary depending on the
clinical area, but the need for comprehensible and structured methods is common.
Nursing informatics can provide interesting possibilities with decision support
systems to enhance such an endeavour. Further, RNs need to address the issue of
shared decision making, not just in theory but also in their clinical practice, and
realise the professionals’ initial responsibility to invite to a dialogue with the
patient. More deliberate facilitation of patient participation in clinical decision
making needs to be applied in clinical practice. It is important to point out that
patient typologies of participation preferences, as described in this thesis, cannot
function as a justification of a paternalistic decision-making approach over time
for patients preferring a passive role. Autonomy is still a valid principle fostering
self-determination and patients ought to be in a position to determine how they
want to exercise their autonomy, even if that is by deliberately adopting a passive
role. The RNs have a professional responsibility to act in such a way that patients
can participate and make decisions according to their own values from an
informed position.
Future research It would be of further interest to study the variability of practice of individual RNs
in relation to agreement with their patients’ perception of needs and preferences
for participation in nursing care. Does the individual RN maintain the same degree
of agreement regardless of type of care needs or over time? What factors seem to
influence the RNs’ accuracy in identifying patient needs?
Further studies are needed of the effects on care processes of feeding
information forward to RNs about the patients’ perspective regarding their health
care needs and participation preferences in clinical decision making. Patients’ self-
reporting using information technology applications as an information vehicle
65

66
(e.g., CHOICE) (Ruland 1999) could be applied and tested in new patient groups
covering new areas of information interchange, i.e. various chronic disease groups
and senior citizens in community dwellings where the encounters take place over
longer periods of time. Studies of patient self-reporting of information in the
patient record could be conducted from aspects such as effects on care processes,
care activities attuned to patient perceived needs, goal attainment, and satisfaction
with care. The demands on information technology applications used to support
clinical decision-making processes need further validation. There is also a need to
develop standardised terms for the concepts of participation and autonomy to be
integrated with, information about diagnosis, interventions, and outcomes in a
patient-centred multi-professional electronic health care record. Some work has
been reported of the use of semantic structures to represent preference elicitations
(Ruland & Bakken 2001) and some research has started in the area (Caldwell et al.
2003) but more research is needed.
66

67
CONCLUSIONS
The major conclusions drawn from the studies in this thesis are:
The quality of RNs’ stated nursing diagnoses could be improved by
education and development of forms for recording
The aetiology component in the diagnosis was a weak link in nurses’
diagnostic statements
Patients and RNs in acute care settings did not agree to a rather large extent
on the patients’ needs for nursing care
The RNs often underestimated the severity and importance of patients’
perceived needs.
Patients on admission to hospital care mostly preferred adopting a passive
role in clinical decision making concerning their nursing care
Patients’ gender, education, social living conditions, and occupational status
were predictors of active participation in clinical decision making regarding
nursing care
There was considerable disagreement in patients’ and RNs’ perceptions
concerning the patients’ preferences for participation in clinical decision
making in nursing in acute care settings
The coherence between patients’ preferences for participation and their
experienced participation in clinical decision making in nursing varied
considerably. Many patients were more active or more passive than
preferred.
To summarize, the best way to know patients’ preferences is through assessment of
the individual patient by thorough identification of needs for nursing care and
preferred participatory role in clinical decision making. The establishment of a
trusting relationship between the patient and the RN is the key in getting to know
the patient, and as a consequence, being able to give individualised nursing care.
67

68
SUMMARY IN SWEDISH
Patientens delaktighet i kliniskt beslutsfattande i omvårdnad – ett gemensamt ansvar för patienter och sjuksköterskor
Bakgrund
Patienten har, med bas i lagstiftning och förordningar, en stark ställning inom
svensk hälso- och sjukvård. Det grundas delvis på en samhällelig uppfattning om
betydelsen av patientens delaktighet i såväl planering som genomförande av sin
egen vård. I ett etiskt perspektiv har delaktigheten ett värde i sig själv, som en
förutsättning för individens autonomi och integritet. Sjuksköterskan identifierar
patientens behov och problem i syfte att kunna ge en individuellt anpassad
omvårdnad. Sjuksköterskan har ofta djupgående professionell kunskap om
patientens omvårdnadsproblem, medan patienten har preferenser och värderingar
beträffande vårdens genomförande. Om planeringen av omvårdnaden inte utgår
från patientens preferenser så finns det stor risk att patientens perspektiv inte
kommer med som bedömningsgrund. En samsyn mellan patient och sjuksköterska
om patientens behov av omvårdnad och roll i beslutsfattandet kan öka möjligheten
att optimera omvårdnadsinsatserna och främja en hög kvalitet på omvårdnaden.
Kunskapen om kliniskt beslutsfattande inom omvårdnad är bristfällig, framförallt
med fokus på patientens delaktighet och graden av samsyn mellan patienternas och
sjuksköterskornas subjektiva perspektiv.
Syfte
Avhandlingens övergripande syfte var att undersöka kliniskt beslutsfattande inom
omvårdnad med speciellt fokus på omvårdnadsdiagnosers kvalitet, patientens
delaktighet i beslutsprocessen och överensstämmelsen mellan patienters och
sjuksköterskors uppfattningar om behov och problem inom omvårdnad.
Specifika syften för respektive delarbeten var att I) undersöka effekten av
utbildning i omvårdnadsdiagnostik riktad till sjuksköterskor och utveckling av
68

69
journaldokument på omvårdnadsdiagnosers kvalitet, II) beskriva överensstämmelse
i patienters och sjuksköterskors bedömningar av förekomst, svårighetsgrad och
betydelse av problem inom omvårdnaden, III) beskriva samstämmighet mellan
patienters och sjuksköterskors uppfattning om patientens preferenser för
delaktighet i kliniskt beslutsfattande i omvårdnaden, jämte samstämmighet mellan
patienters preferenser och faktiska erfarenhet av delaktighet samt IV) identifiera
prediktorer för patienters preferenser att delta i kliniskt beslutsfattande om den
egna omvårdnaden.
Material och metod
Studier har genomförts med beskrivande, jämförande och kvasi-experimentell
design på avdelningar inom somatisk sjukhusvård. Urvalet består av 140
patientjournaler (studie I), 80 patient-sjuksköterskepar (studie II och III) samt 428
patienter som nyligen blivit utskrivna från somatisk sjukhusvård (studie IV). Data
har insamlats genom granskning av innehåll i patientjournaler samt genom enkäter
till patienter och sjuksköterskor. Instrumenten CAT-CH-ING och Control
Preference Scale har använts tillsammans med frågeformulär som utvecklats
specifikt för studien.
Resultat
Delarbete I
Kvaliteten på omvårdnadsdiagnoserna förbättrades signifikant efter att
sjuksköterskorna på experimentavdelningen genomgått en utbildning och nya
journaldokument hade introducerats. Störst kvarvarande svårigheter var
förknippade med hur etiologin i omvårdnadsdiagnosen formulerades.
Omvårdnadsdiagnosernas kvalitet förbättrades inte på motsvarande sätt på
kontrollavdelningarna.
Delarbete II
Sjuksköterskorna identifierade de omvårdnadsbehov och problem som patienterna
uppfattade sig ha med en sensitivitet på 0.53 och ett prediktivt värde på 0.50. Det
69
70
innebär att patienterna delvis identifierade andra problem än sjuksköterskorna;
framför allt var det vanligt inom områdena nutrition, sömn, smärta och
känslor/andlighet. Sjuksköterskorna underskattade problemens svårighetsgrad för
47 % av de behov och problem som hade identifierats gemensamt av patienter och
sjuksköterskor. En gemensam uppfattning om betydelsen av att få stöd och hjälp
med att lösa omvårdnadsproblemet fanns i knappt hälften av fallen.
Delarbete III
En majoritet av sjuksköterskorna uppfattade att patienterna föredrog att vara mer
aktiva i det kliniska beslutsfattandet om omvårdnad än vad patienterna själva
uppgav. Sammanlagt 61 % av patienterna föredrog en passiv roll i
beslutsfattandet, medan sjuksköterskorna angav att 24 % ville vara passiva.
Preferenser om en aktiv roll i beslutsfattande angavs av 9 % av patienterna, medan
sjuksköterskorna hade uppfattat att 45 % av patienterna föredrog en aktiv roll.
Totalt 71 % av patienterna upplevde att de inte hade varit delaktiga i den
utsträckning de själva hade föredragit; 37 % hade varit mer passiva och 34 % mer
aktiva. Patienterna uppgav att de intagit en mer passiv roll än vad de hade önskat i
samband med behov och problem inom områdena kommunikation, andning och
smärta, medan en mer aktiv roll än önskat förekom i samband med behov och
problem inom områdena aktivitet och känslor/roller.
Delarbete IV
En majoritet av patienterna i sluten somatisk vård föredrog att inledningsvis under
vårdperioden inta en passiv roll i kliniskt beslutsfattande om omvårdnad.
Sammanlagt 22 % av patienterna föredrog en aktiv roll. Faktorer som predicerade
preferenser för att inta en aktiv roll var kön (Odds ratio [OR] = 1.8), utbildning
(OR = 2.2), levnadsförhållanden (OR = 1.8) och sysselsättning, d.v.s. om personen
var yrkesarbetande eller pensionär (OR = 2.0). Sannolikheten var 53 % att en
pensionerad högutbildad kvinna som levde ensam föredrog att vara aktiv i
beslutsfattandet om sin egen omvårdnad. Sannolikheten för att en yrkesarbetande
70

71
lågutbildad man som levde tillsammans med någon annan föredrog att vara aktiv
var 8 %.
Slutsatser
Kvaliteten på de omvårdnadsdiagnoser som sjuksköterskan ställer kan förbättras
genom utbildning, men orsakerna till omvårdnadsproblemen behöver identifieras
på ett tydligare sätt. Det fanns en skillnad i hur patienter och sjuksköterskor
uppfattade vad som utgjorde ett omvårdnadsbehov eller problem samt problemets
svårighetsgrad och betydelse. Sjuksköterskan identifierade 53 % av de
omvårdnadsproblem som patienten själv identifierade, samtidigt som
sjuksköterskan identifierade andra omvårdnadsproblem som inte patienten
uppfattade. Uppfattningarna skiljde sig också åt om vilken roll patienten föredrog
att ha i det kliniska beslutsfattande om omvårdnad. Faktorer som kunde predicera
patientens preferenser att ha en aktiv roll i kliniskt beslutsfattande var kön,
utbildningsnivå, boendesituation och om personen yrkesarbetade eller var
pensionär.
En slutsats av den påvisade diskrepansen i uppfattningar är att sjuksköterskor i
högre grad behöver involvera patienterna i en diskussion om hälsotillståndet,
behovet av omvårdnad och patientens önskan att delta i beslut om sin omvårdnad.
Det är nödvändigt för att så långt det är möjligt kunna uppnå en samsyn som
grund för planering och genomförande av omvårdnaden. Om sjuksköterskan
validerar sina egna bedömningar om behovet av omvårdnad med patienten kan
kvaliteten på bedömningarna förbättras. Patientens perspektiv blir en explicit del
av beslutsunderlaget vid planering av omvårdnad, vilket sannolikt också påverkar
omvårdnadens innehåll och därmed även omvårdnadens kvalitet. Det bästa sättet
att identifiera det individuella perspektivet är genom en systematisk bedömning i
dialog mellan sjuksköterskan och den enskilde patienten. Mötet och dialogen
mellan patienten och sjuksköterskan är en förutsättning för en god omvårdnad
men är också en central del av själva omvårdnaden.
71
72
ACKNOWLEDGEMENTS
I have met several persons during this endeavour. People who have positively
contributed to the project by letting me take part of their skills and knowledge,
sharing experiences, and good friendship. In particular, I would like to express my
sincere gratitude to my supervisors:
associate professor Anna Ehrenberg, my primary supervisor, for your
constructive criticism combined with excellent guidance and support on the
knobbled path, spiced with a great dose of friendship and memories from our
travels around the world of research.
professor Margareta Ehnfors, my co-supervisor, for your excellent guidance
and positive encouragement and constructive criticism, as well as for your
friendship and our shared experiences and memories from around the globe.
I would like to give special thanks to:
All the patients and nurses who have participated in the studies.
The department of Health and Social Sciences at Dalarna University, and
especially director Eva Bäck for providing generous working conditions and
support for the completion of this thesis.
The department of Health Sciences at Örebro University, and director Eva
Sahlberg Blom, for providing me with a working environment, including
financial support that made this work possible.
The whole group of doctoral students at the department of Health Sciences,
Örebro University, for many intriguing and interesting discussions at our
seminars.
All my colleagues at the institution of Health and Social Sciences at Högskolan
Dalarna for your interest in my work and providing an inspiring
counterbalance by sharing every day concerns, in education as well as in life.
Leslie Shaps for your skilled and rapidly performed language revisions.
72

73
Birgitte Kolsung, research administrator at the Department of Health Sciences
at Örebro University, for your help with organising, facilitating my life as a
doctoral student, and getting things together at the end of the project.
Ingrid Hellegren Fix, head nurse during my previous employment as a nurse,
for believing in me and supporting me over the years.
Last but not least. I would like to thank:
Marie, Martin and Alice, my three beloved children, for just being the ones you
are, and for the things we do that enrich life far beyond any thesis project.
The studies have been financially supported by The Dalarna Research Council
(Dalarnas Forskningsråd) and Högskolan Dalarna.
73

74
REFERENCES
Abayomi J. & Hackett A. (2004) Assessment of malnutrition in mental health clients: nurses’ judgement vs. a nutrition risk tool. Journal of Advanced Nursing 45(4), 430-437.
Adamsen L. & Tewes M. (2000) Discrepancy between patients' perspectives, staff's documentation and reflections on basic nursing care. Scandinavian Journal of Caring Sciences 14, 120-129.
Altman D.G. (1991) Practical Statistics for Medical Research. Chapman & Hall, Great Britain.
American Nurses Association (1973) Standards of Nursing Practice. American Nurses Association. MO, Kansas City.
American Nurses Association (1980) Nursing: A social Policy Statement. American Nurses’ Association. MO, Kansas City.
Andershed B. (1998) Att vara nära anhörig i livets slut. Delaktighet i ljuset – delaktighet i mörkret. (Being a close relative in the final phase of life. Involvement in the light – involvement in the dark) Uppsala Dissertations from the Faculty of Medicine 774. Uppsala University, Uppsala. (In Swedish)
André M. (2004) Rules of thumb and management of common infections in general practice. Linköping University Medical dissertations 840. Department of Health and Society, Linköpings University, Linköping.
Ashworth P.D., Longmate M.A. & Morrison P. (1992) Patient participation: its meaning and significance in the context of caring. Journal of Advanced Nursing17, 1430-1439.
Axelsson L., Björvell C., Mattiasson A-C. & Randers I. (2006) Swedish registered nurses’ incentives to use nursing diagnoses in clinical practice. Journal of Clinical nursing 15, 936-945.
Balzer-Riley J.W. (1996) Communication in nursing. 3rd ed. Mosby-Year Book Inc., St.Louis.
Barder L., Slummer L. & LeSage J. (1994) Depression and issues of control among elderly people in health care settings. Journal of Advanced Nursing 20, 597-604.
Bauer I. (1994) Patients' privacy: exploratory study of patients' perceptions of their privacy in a German Acute Care Hospital. Avebury Ashgate, Aldershot.
74
75
Benner P. (1984) From novice to expert: Excellence and power in clinical nursing practice, Addison-Wesley, California.
Beaver K., Luker K.A, Owens R.G., Leinster S.J. & Degner L.F. (1996) Treatment decision making in women newly diagnosed with breast cancer. Cancer Nursing19, 8-19.
Beaver K., Bogg J. & Luker K.A. (1999) Decision-making role preferences and information needs: a comparison of colorectal and breast cancer. Health Expectations 2, 266-276.
Biley F.C. (1989) Nurses' perception of stress in preoperative surgical patients. Journal of Advanced Nursing 14, 575-581.
Biley F.C. (1992) Some determinants that effect patient participation in decision-making about nursing care. Journal of Advanced Nursing 17, 414-421.
Björvell C., Thorell-Ekstrand I. & Wredling R. (2000) Development of an audit instrument for nursing care plans in the patient record. Quality in Health Care 9,6-13.
Björvell C., Wredling R., & Thorell-Ekstrand I. (2002) Long-term increase in quality of nursing documentation: effects of a comprehensive intervention. Scandinavian Journal of Caring Sciences 16, 34-42.
Blomqvist K. & Hallberg I.R. (1999) Pain in older adults living in sheltered accommodation - agreement between assessments by older adults and staff. Journalof Clinical Nursing 8, 159-169.
Boychuk Duchscher J.E. (1999) Catching the wave: understanding the concept of critical thinking. Journal of Advanced Nursing 29(3), 577-583.
Brennan P.F. & Strombom I. (1998) Improving health care by understanding patient preferences: The role of computer technology. Journal of the American Medical Informatics Association 5(3), 257-262.
Brunswik E. (1956) Perception and the representative design of psychological experiments. University of California Press, Berkeley, California.
Buckingham C.D. & Adams A. (2000a) Classifying clinical decision making: a unifying approach. Journal of Advanced Nursing 32(4), 981-989.
75

76
Buckingham C.D. & Adams A. (2000b) Classifying clinical decision making: a unifying approach interpreting nursing intuition, heuristics and medical diagnosis. Journal of Advanced Nursing 32(4), 990-998.
Butow P.N., Maclean M., Dunn S.M., Tattersall M.H.N. & Boyer M.J. (1997) The dynamics of change: Cancer patients' preferences for information, involvement and support. Annals of Oncology 8, 857-863.
Cahill J. (1996) Patient participation: a concept analysis. Journal of Advanced Nursing 24, 561-571.
Cahill, J. (1998) Patient participation - a review of the literature. Journal of Clinical Nursing 7, 119-128.
Caldwell, C.L., Wasson D., Brighton V., Dixon L. & Anderson M.A. (2003) Personal autonomy: development of a nursing outcomes classification label. Journal of the American Psychiatric Nurses Association 9(5), 167-172.
Caress A-L., Luker K., Woodcock A. & Beaver K. (2002) A qualitative exploration of treatment decision-making role preference in adult asthma patients. Health Expectations 5, 223-235
Carnevali D. (1983) Nursing Care Planning: Diagnosis and Management, 3rd ed. JB Lippincott Company, Philadelphia.
Carnevali D. (1993) Health care for the elderly: nursing’s area of accountability. In Nursing Management for the elderly. 3rd ed. Eds. Carnevali D. & Patrick M. J.B. Lippincott Company, Philadelphia.
Carnevali D. (1996) Handbok i omvårdnadsdiagnostik. (Handbook of Nursing Diagnosis). Liber AB, Falköping (in Swedish)
Carnevali D., Mitchell P., Woods N. & Tanner C. (1984) Diagnostic reasoning in nursing. J.B. Lippincott, Philadelphia.
Carr S.M. (2004) A framework for understanding clinical reasoning in community nursing. Journal of Clinical Nursing 13, 850-857.
Casey A. (1995) Partnership nursing: influences on involvement of informal carers. Journal of Advanced Nursing 22, 1058-1062.
Charavel M., Bremond A., Moumjid-Ferdjaoui N., Mignotte H. & Carrere M.O. (2001) Shared decision-making in question. Psycho-Oncology 10, 93-102.
76

77
Charles C., Gafni A. & Whelan T. (1997) Shared decision-making in the medical encounter: What does it mean? (Or, it takes two to tango). Social Science & Medicine 44, 681-692.
Charlson M.E., Pompei P., Ales K.L. & McKenzie C.R. (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. Journal of Chronic Disability 40, 373- 383.
Clark J. & Lang N.M. (1992) Nursing next advance: An international classification for nursing practice. International Nursing Review 39, 109-112.
Conger M.M. & Mezza I. (1996) Fostering critical thinking in nursing students in the clinical setting. Nurse Educator 21, 11-15.
Coombs C.A. (1964) Theory of data. John Wiley & Sons, New York.
Cowley S., Bergen A., Young K. & Kavanagh A. (2000) A taxonomy of needs assessment elicited from a multiple case study of community nursing education and practice. Journal of Advanced Nursing 31, 126-134.
Dalton J.M. (2003) Development and testing of theory of collaborative decision-making in nursing practice for triads. Journal of Advanced Nursing 41, 22-33.
Davison B.J. & Degner L.F. (2002) Feasibility of using a computer-assisted intervention to enhance the way women with breast cancer communicate with their physicians. Cancer Nursing 25 (6), 417-424.
Degner L. F. & Sloan J.A. (1992) Decision making during serious illness: What role do patients really want to play? Journal of Clinical Epidemiology 45(9): 941-950.
Degner L.F., Sloan J.A. & Venkatesh P. (1997) The control preferences scale. Canadian Journal of Nursing Research 29, 21-43.
Dickerson S.S. & Brennan P.F. (2002) The Internet as a catalyst for shifting power in provider-patient relationship. Nursing Outlook 50, 195-203.
Dobrzyn J. (1995). Components of Written Nursing Diagnostic Statements. Nursing Diagnosis, 6 (1), 29-36.
Doherty C. & Doherty W. (2005) Patients’ preferences for involvement in clinical decision-making within secondary care and the factors that influence their preferences. Journal of Nursing Management 13, 119-127.
77
78
D’Onofrio C. (1980) Patient compliance and patient education. In Patient education: An enquiry into the state of the art (Squyres W., ed.) Springer, New York.
Dowding D. & Thompson C. (2003) Measuring the quality of judgement and decision-making in nursing. Journal of Advanced Nursing 44(1), 49-57.
Dowie J. (1993) Clinical decision analysis: background and introduction: In Analysing how we reach clinical decision. (Llewelyn H. & Hopkins A., eds.) Royal College of Physicians, London.
Edvardsson D., Sandman P.O. & Rasmussen B. (2006) Caring or uncaring – meanings of being in an oncology environment. Journal of Advanced Nursing 55(2), 188-197.
Edwards C. (2002) A proposal that patients be considered honorary members of the health care team. Journal of Clinical Nursing 11, 340-348.
Efraimsson E., Sandman P., Hydén L-C. & Rasmussen B.H. (2004) Discharge planning: 'fooling ourselves?' - patient participation in conferences. Journal of Clinical Nursing 13, 562-570.
Efraimsson E. (2005) Vårdplaneringsmötet. En studie av det institutionella samtalet mellan äldre kvinnor, närstående och vårdare. (Discharge planning conference. A study of the institutionalized conversation between elderly women, next of kin and staff). Umeå University Medical Dissertations 967. The Department of Nursing, Umeå University, Umeå. (In Swedish)
Ehnfors M. (1993) Effects of introducing a nursing documentation model on content and comprehensiveness of nursing records. In: Ehnfors M. Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 415. Uppsala University, Uppsala.
Ehnfors M. & Smedby B. (1993) Nursing Care as Documented in Patient Records. Scandinavian Journal of Caring Sciences 7, 209-222.
Ehnfors M., Ehrenberg A. & Thorell-Ekstrand I. (2002). The development and use of the VIPS-model in the Nordic countries. In: Oud N. (ed). ACENDIO 2002.Proceedings of the special conference of the Association of Common European Nursing Diagnoses, Interventions and Outcomes in Vienna. Verlag Hans Huber, Bern. pp.139-168.
Ehrenberg A. & Ehnfors M. (1999a) Patient Records in Nursing Homes. Effects of Training on Content and Comprehensiveness. Scandinavian Journal of Caring Sciences 13, 72-82.
78

79
Ehrenberg A. & Ehnfors M. (1999 b) Patient problems, needs, and nursing diagnoses in Swedish nursing home records. Nursing Diagnosis 10 (2), 65-76.
Ehrenberg A. & Ehnfors M. (2001) The accuracy of patient records in Swedish nursing homes: congruence of record content and nurses’ and patients’ descriptions. Scandinavian Journal of Caring Sciences 15, 303-310.
Ehrenberg A. Ehnfors M. & Ekman I. (2004) Older patients with chronic heart failure within Swedish community health care: a record review of nursing assessments and interventions. Journal of Clinical Nursing 13, 90-96.
Eldh A.C., Ehnfors M. & Ekman I. (2004) The phenomena of participation and non-participation in health care- experiences of patients attending a nurse-led clinic for chronic heart failure. European Journal of Cardiovascular Nursing 3, 239-246.
Eldh A-K.(2006) Patient participation – what it is and what it is not. Örebro Studies in Caring Sciences 11, Örebro University, Örebro.
Elwyn G., Edwards A. & Kinnersley P. (1999) Shared decision-making in primary care: The neglected second half of the consultation. British Journal of General Practice 49, 477-482.
Engvall G. (1994) Utvärdering av en omvårdnadsdokumentationsmodell. (Evaluation of a model for nursing documentation). Vård i Norden 14, 19-23. (in Swedish)
Ennis R. (1996) Critical thinking. Prentice Hall, Upper Saddle River, NJ.
Fagrell B., Funcke L. & Nyberg K. (1998) Omvårdnadsdokumentation enligt VIPS modellen på sjukhem. En studie av sjuksköterskors vårddokumentation vid svenska sjukhem. (Nursing documentation using the VIPS model in nursing homes. A study of nurses’ documentation practice in Swedish nursing homes). Vård i Norden 18, 40-5 (in Swedish).
Farrell G. (1991) How accurately do nurses perceive patients' needs? A comparison of general and psychiatric settings. Journal of Advanced Nursing16(9), 1062-1070.
Faulkner M. (2001) A measure of patient empowerment in hospital environments catering for older people. Journal of Advanced Nursing 34(5), 676-686.
Fiske S.T. (1993) Social cognition and social perception. Annual Review of Psychology 44, 155-194.
79

80
Fleiss, J.L. (1981) Statistical methods for rates and proportions (2nd ed.). John Wiley, New York
Fonteyn M.E. (1998) Thinking strategies for nursing practice. Lippincott-Ravens Publishers, Philadelphia.
Ford S. & Schofield T. & Hope T. (2003) Are patients decision-making preferences being met? Health Expectations 6, 72-80.
Frosch D.L. & Kaplan R.M. (1999) Shared decision making in clinical medicine: past research and future directions. American Journal of Preventive Medicine17(4), 285-294.
Gaston-Johansson F. (1996) Measurement of pain: The psychometric properties of the pain-o-meter, a simple, inexpensive pain assessment tool that could change health care practice. Journal of Pain and Symptom Management 12(3), 172-181.
Gassert C. (1998) The challenge of meeting patients’ needs with a national informatics agenda. Journal of American Medical Informatics Association 5, 263-268.
Gatellari M., Butow P.N. & Tattersall M.H. (2001) Sharing decisions in cancer care. Social Science & Medicine 52, 1865-1878.
Gordon M. (1982) Nursing Diagnosis. McGraw Hill, New York.
Gordon M. (1994) Nursing Diagnosis: Process and Application (3rd ed). Mosby, St. Louis.
Guadagnoli E. & Ward P (1998) Patient participation in decision-making. Social Science & Medicine 47, 329-339.
Hall-Lord M.L., Larsson G. & Steen B. (1999) Chronic pain and distress among elderly in the community: comparison of patients' experiences with enrolled nurses' assessments. Journal of Nursing Management 7, 45-54.
Hallström I. & Elander G. (2001a) Needs during hospitalization: definitions and descriptions made by patients. Nursing Ethics 8(5), 409-418.
Hallström I. & Elander G. (2001b) A comparison of patient needs as ranked by patients and nurses. Scandinavian Journal of Caring Sciences 15, 228-234.
Hansebo G., Kihlgren M. & Ljunggren G. (1999) Review of nursing documentation in nursing home wards – changes after intervention for individualized care. Journal of advanced nursing 29(6), 1462-1473.
80
81
Hansen T., Hatling T., Lidal E. & Ruud T. (2002) Discrepancies between patients and professionals in the assessment of patient needs: a quantitative study of Norwegian mental health care. Journal of Advanced Nursing 39(6), 554-562.
Harbison J. (2001) Clinical decision making in nursing: theoretical perspectives and their relevance to practice. Journal of Advanced Nursing 35(1), 126-133.
Harrison A., Busabir A.A., Al-Kaabi A.O. & Al-Awadi H.K. (1996) Does sharing a mother-tongue affect how closely patients and nurses agree when rating the patients' pain, worry and knowledge? Journal of Advanced Nursing 24, 229-235.
Heaven C.M. & Maguire P. (1996) Training hospice nurses to elicit patient concerns. Journal of Advanced Nursing 23, 280-6.
Hedberg B. (2005) Decision making and communication in nursing practice – aspects of nursing competence. Göteborg studies in educational sciences 235. Göteborgs University, Göteborg
Hellesö R., Lorensen M. & Sorensen L. (2004) Challenging the information gap – the patients transfer from hospital to home health care. International Journal of Medical Informatics 73, 569-580.
Henderson S. (2003) Power imbalance between nurses and patients: a potential inhibitor of partnership in care. Journal of Clinical Nursing 12, 501-508.
Henderson A. & Shum D. (2003) Decision-making preferences towards surgical intervention in a Hong Kong Chinese population. International Nursing Review50, 95-100.
Hendry C. & Walker A. (2004) Priority setting in clinical nursing practice: literature review. Journal of Advanced Nursing 47(4), 427-436.
Hickey G. & Kipping C. (1998) Exploring the concept of user involvement in mental health through a participation continuum. Journal of Clinical Nursing 7,83-88.
Holmes H.A. & Warelow P.J. (1997) Culture, needs and nursing: a critical theory approach. Journal of Advanced Nursing 25, 463-470.
Hovi S.L. & Lauri S. (1999) Patients' and nurses' assessment of cancer pain. European Journal of Cancer Care 8, 213-219.
81

82
Hämäläinen P.M., Perälä M-L., Poussa T. & Pelkonen M. (2003) Patient participation in decision-making on the introduction of home respiratory care: who does not participate? Health Expectations 6, 118-127.
ICN Definition of nursing. Internet access 2006-11-08. http://www.icn.ch/definition.htm
ICN (2003) Patient Talk! The ICN Informed Patient Project (2003) Internet access 2006-11-08. http://www.patienttalk.info/psinfopatients03.htm
Inde M. (2006) Patientnärmre vård. Hur gör man? (Patient-focused care. How is it performed?) Utvecklingsstaben Landstinget Värmland.
Institute of Medicine (2001) Crossing the Quality Chasm: A New Health System for the 21st Century. National Academy Press, Washington D.C.
Institute of Medicine (2003) Health Professions Education. A bridge to quality.Eds. Greiner A.C. & Knebel E. National Academy Press, Washington D.C.
Ishikawa H. & Yamazaki Y. (2005) How applicable are western models of patient-physician relationship in Asia? Changing patient-physician relationship in contemporary Japan. International Journal of Japanese Sociology 14, 84-93.
Jewell, S. E. (1994). Patient participation: what does it mean to nurses? Journal of Advanced Nursing 19, 433-438.
Jonsdottir H., Litchfield M. & Pharris M.D. (2004) The relational core of nursing practice as partnership. Journal of Advanced Nursing 47(3), 241-250.
Keatinge D., Bellchambers H., Bujack E., Cholowski K., Conway J. & Neal P. (2002) Communication: Principal barrier to nurse-consumer partnerships. International Journal of Nursing Practice 8, 16-22.
Kenny T. (1990) Erosion of individuality in care of elderly people in hospital: an alternative approach. Journal of Advanced Nursing 15(5), 571-576.
Kent G., Wills G., Faulkner A., Parry G., Whipp M. & Coleman R. (1996) Patient reactions to met and unmet psychological need: A critical incident analysis. Patient Education and Counseling 28 (2), 187-190.
Kersten P., George S., McLellan L., Smith J.A.E. & Mullee M.A. (2000) Disabled people and professionals differ in their perceptions of rehabilitation needs. Journal of Public Health Medicine 22(3), 393-399.
82

83
Kidd J., Marteau T.M., Robinson S., Ukoumunne O.C. & Tydeman C. (2004) Promoting patient participation in consultations: a randomised controlled trial to evaluate the effectiveness of three patient-focused interventions. Patient Education and Counseling 52, 107-112.
Kirk S. & Glendinning C. (1998) Trends in community care and patient participation: implications for the roles of informal carers and community nurses in the United Kingdom. Journal of Advanced Nursing 28(2), 370-381.
Kraetchmer N., Sharpe N., Urowitz S. & Deber R.B. (2004) How does trust affect patient preferences for participation in decision-making? Health Expectations 7,317-326.
Kristensson-Hallström I. (1999) Strategies for feeling secure influence parents' participation in care. Journal of Clinical Nursing 8, 586-592.
Kuokkanen L. & Leino-Kilpi H. (2000) Power and empowerment in nursing: three theoretical approaches. Journal of Advanced Nursing 31(1), 235-241.
Lam W., Fielding R., Chan M., Chow L. & Ho E. (2003) Participation and satisfaction with surgical treatment decision-making in breast cancer among Chinese women. Breast Cancer Research and Treatment 80, 171-80
Lampic C.L., von Essen L., Widmark Pettersson V., Larsson G. & Sjödén P.O. (1996) Anxiety and depression in hospitalized patients with cancer: agreement in patient-staff dyads. Cancer Nursing 19 (6), 419-428.
Latvala E., Janhonen S. & Wahlberg K-E. (1999) Patient initiatives during assessment and planning of psychiatric nursing in a hospital environment. Journalof Advanced Nursing 29(1), 64-71.
Latvala E. (2002) Developing and testing methods for improving patient-oriented mental health care. Journal of Psychiatric and Mental Health Nursing 9, 41-47.
Lauri S., Lepistö M. & Käppeli S. (1997) Patients' needs in hospital: nurses' and patients' views. Journal of Advanced Nursing 25(2), 339-346.
Laverack G. (2005) Public health: power, empowerment, and professional practice. Palgrave Macmillan, New York.
Lemonidou C., Merkouris A., Leino-Kilpi H., Välimäki M., Dassen T., Gasull M., Scott P.A., Tafas C., 6 Arndt M. (2003) A comparison of surgical patients' and nurses' perceptions of patients' autonomy, privacy, and informed consent in nursing interventions. Clinical Effectiveness in Nursing 7, 73-83.
83

84
Levin R. F., Lunney M. & Krainovich-Miller B. (2004) Improving diagnostic accuracy using an evidence-based nursing model. International Journal of Nursing Terminologies and Classifications 15(4), 114-122.
Liss P-E. (1990) Health care need. Meaning and measurement. Linköping University, Linköping (thesis).
Lockwood A. & Marshall M. (1999) Can a standardized needs assessment be used to improve the care of people with severe mental disorders? A pilot study of 'needs feedback'. Journal of advanced nursing 30(6), 1408-1415.
Lundberg O. & Nyström Peck M (1995) A simplified way of measuring sense of coherence. Experiences from a population survey in Sweden. European Journal of Public Health 5(1), 56-59.
Lunney M. (1990) Accuracy of Nursing Diagnosis: Concept Development. Nursing Diagnosis, 1, 12-17.
Lunney M. (2003) Critical thinking and accuracy of nurses’ diagnoses. International Journal of Nursing terminologies and classifications 14(3), 96-107.
Lutzen K. & Nordin C. (1993) Benevolence, a central moral concept derived from a grounded theory study of nursing decision making in psychiatric settings. Journal of Advanced Nursing 18, 1106-1111.
Löfmark A., Hannersjö S. & Wikblad K. (1999) A summative evaluation of clinical competence: students' and nurses' perceptions of inpatients' individual physical and emotional needs. Journal of Advanced Nursing 29 (4), 942-949.
Martin L.R., Jahng K.H., Golin C.E. & DiMatteo M.R. (2003) Physician facilitation of patient involvement in care: correspondence between patient and observer reports. Behavioral Medicine 28, 159-164.
Matiasson A-C., Andersson L., Mullins L.C. & Moody L. (1997) A comparative empirical study of autonomy in nursing homes in Sweden and Florida, USA. Journal of Cross-cultural Gerontology 12, 299-316.
McKinstry B. (2000) Do patients wish to be involved in decision making in the consultation? A cross sectional survey with video vignettes. British Medical Journal321, 867-871.
Millard L., Hallett C., & Luker K. (2006) Nurse-patient interaction and decision-making in care: patient involvement in community nursing. Journal of Advanced Nursing 55(2), 142-150.
84

85
Minton J.A. & Creason N.S. (1991). Evaluation of Admission Nursing Diagnoses. Nursing Diagnosis, 2, 119-125.
Moen A., Hellesö R. & Olsen M.F. (1997) Nursing Documentation – beyond the question of structure. Vård i Norden 4, 26-9.
Muller-Staub M., Lavin M. A:, Needham I. & van Achterberg T. (2006) Nursing diagnoses, interventions and outcomes – application and impact on nursing practice: systematic review. Journal of Advanced Nursing 56(5), 514-531.
Myers H. & Nikoletti S. (2003) Fall risk assessment: A prospective investigation of nurses’ clinical judgement and risk assessment tools in predicting patient falls. International Journal of Nursing Practice 9, 158-165.
Myers S.M. (1998) Patient-focused care: What managers should know. NursingEconomics 16(4), 180-188.
NANDA (2001) Nursing Diagnoses: Definitions & Classification 2001-2002. NANDA, USA.
Nordgren L. (2004) Från patient till kund. Intåget av marknadstänkande i sjukvården och förskjutningen av patientens position. (From patient to consumer. The entrance of a market approach in health care and the displacement of power of the patient) Lund Studies in Economics and Management 77, Institute of Economic Research, Lund University. Lund (In Swedish)
Nordström G. & Gardulf A. (1993) Kvalitetsindikatorer för omvårdnad och mätinstrument. NoGa – en möjlighet att mäta och beskriva omvårdnadens kvalitet. (Quality indicators for nursing care and the instrument NoGa© – a possibility to measure and describe the quality of nursing care) Vårdadministratören 4. 12-17. (in Swedish)
Nordström G. & Gardulf A. (1996) Nursing Documentation in Patient Records. Scandinavian Journal of Caring Sciences 10, 27-33.
Nunally J.C. (1978) Psychometric theory. McGraw Hill, New York.
O'Connor A.M., Drake E.R., Wells G.A., Tugwell P., Laupacis A. & Elmslie T. (2003) A survey of the decision-making needs of Canadians faced with complex health decisions. Health Expectations 6, 97-109.
Offredy M. (1998) The application of decision making concepts by nurse practitioners in general practice. Journal of Advanced Nursing 28(5), 988-1000.
85
86
Patel V.L. & Currie L.M. (2005) Clinical cognition and bio-medical informatics: issues of patient safety. International Journal of Medical Informatics 74, 869-885.
Paterson B. (2001) Myth of empowerment in chronic illness. Journal of Advanced Nursing 34(5), 574-581.
Pedersen P.U. (2005) Nutritional care: the effectiveness of actively involving older patients. Journal of Clinical Nursing 14, 247-255.
Peplau H.E. (1952) Interpersonal relations in nursing. Putnam’s, New York.
Pesut D.J. & Herman J. (1999) Clinical reasoning. The art & science of critical & creative thinking. Delmar Publishers, USA.
Poulton B. (1999) User involvement in identifying health needs and shaping and evaluating services: is it being realised? Journal of Advanced Nursing 30(6), 1289-1296.
Protière C., Viens P., Genre D., Cowen D., Camerlo J., Gravis G. et al. (2000)Patient participation in medical decision-making: A French study in adjuvant radio-chemotherapy for early breast cancer. Annals of Oncology 11, 39-45.
Radwin L.E. (1996) ‘Knowing the patient’: a review of research on an emerging concept. Journal of Advanced Nursing 23, 1142-1146.
Radwin L.E. (1998) Empirically generated attributes of experience in nursing. Journal of Advanced Nursing 27, 590-595.
Ramfelt E., Langius A., Björvell H. & Nordström G. (2000) Treatment decision-making and its relation to the sense of coherence and the meaning of the disease in a group of patients with colorectal cancer. European Journal of Cancer Care 9,158-165.
Richardson A. (1992) Studies exploring self-care for the person coping with cancer treatment: a review. International Journal of Nursing Studies 29 (2), 191-204.
Rosendahl Darmer M., Ankersen L., Geissler Nielsen B., Landberger G., Lippert E. & Egerod I. (2006) Nursing documentation audit – the effect of a VIPS implementation programme in Denmark. Journal of Clinical Nursing 15, 525-534.
Ruland C. (1998) Improving patient outcomes by including patient preferences in nursing care. Journal of American Medical Informatics Association, 448-452.
86

87
Ruland C. (1999) Decision support for patient preference-based care planning. Effects on nursing care and patient outcomes. Journal of the American Medical Informatics Association 6, 304-312.
Ruland C.M. & Bakken S. (2001) Representing patient preference-related concepts for inclusion in electronic health rcords. Journal of Bimedical Informatics 34, 415-422.
Ruland C.M. & Moore S.M. (2001) Eliciting exercise preferences in cardiac rehabilitation: initial evaluation of a new strategy. Patient education and counseling 44, 283-291.
Ruland C.M. (2004) A survey about the usefulness of computerized systems to support illness management in clinical practice. International Journal of Medical Informatics 73, 797-805.
Runeson I. (2002) Children’s participation in decision-making in health care.Department of Medical Ethics, Faculty of Medicine, Lund University, Lund.
Rycroft-Malone J., Seers K., Titchen A., Harvey G., Kitson A. & McCormack B. (2004a) What counts as evidence in evidence-based practice? Journal of Advanced Nursing 47(1), 81-90.
Rycroft-Malone J., Harvey G., Seers K., Kitson A., McCormack B. & Titchen A. (2004b) An exploration of the factors that influence the implementation of evidence into practice. Journal of Clinical Nursing 13, 913-924.
Sahlberg Blom E. (2001) Autonomi, beroende, livskvalitet. Livets sista månad för 56 cancerpatienter. (Autonomy, dependence, and quality of life. The last month in the lives of 56 patients with cancer.) Uppsala Dissertations from the Faculty of Medicine 997, Uppsala University, Uppsala. (In Swedish)
Sainio C., Lauri S. & Eriksson E. (2001) Cancer patients ́views and experiences of participation in care and decision making. Nursing Ethics 8, 97-115.
Sainio C. & Lauri S. (2003) Cancer patients' decision-making regarding treatment and nursing care. Journal of Advanced Nursing 41(3), 250-260.
Sanders T. & Skevington S. (2003) Do bowel cancer patients participate in treatment decision-making? Findings from a qualitative study. European Journal of Cancer Care 12, 166-175.
Schou I., Ekeberg O, Ruland C.M. & Kåresen R. (2002) Do women newly diagnosed with breast cancer and consulting surgeon assess decision-making equally? The Breast 11, 434-441.
87

88
Scott P.A., Välimäki M., Leino-Kilpi H., Dassen T., Gasull M., Lemonidou C., Arndt M., Schopp A., Suhonen R. & Kaljonen A. (2003a) Perceptions of autonomy in the care of elderly people in five European countries. Nursing Ethics10(1), 28-38.
Scott P.A., Välimäki M., Leino-Kilpi H., Dassen T., Gasull M., Lemonidou C. & Arndt M. (2003b) Autonomy, privacy and informed consent 3: elderly care perspective. British Journal of Nursing 12 (3), 158-168.
Scott P.A., Taylor A., Välimäki M., Leino-Kilpi H., Dassen T., Gasull M., Lemonidou C. & Arndt M. (2003c) Autonomy, privacy and informed consent 2: postnatal perspective. British Journal of Nursing 12 (2), 117-127.
Scott P.A., Taylor A., Välimäki M., Leino-Kilpi H., Dassen T., Gasull M., Lemonidou C. & Arndt M. (2003d) Autonomy, privacy and informed consent 4: surgical perspective. British Journal of Nursing 12(5), 311-320.
SFS (1982) Hälso- och sjukvårdslagen (The Health Care Law). Svensk författningssamling 1982:763. Liber, Allmänna förlaget, Stockholm. (In Swedish)
Sloman R., Rosen G., Rom M. & Shir Y. (2005) Nurses’ assessment of pain in surgical patients. Journal of Advanced Nursing 52(2), 125-132.
Snellman I. (2001) Den mänskliga professionaliteten. En filosofisk undersökning av det autentiska mötets betydelse för patientens välbefinnande. (Human professionalism: A philosophical investigation of the significance of the authentic encounter for the well-being of the patient). Uppsala dissertations from the Department of Theology, Uppsala University, Uppsala (In Swedish).
Soothill K., Morris S.M., Harman J., Francis B., Thomas C. & McIllmurray M.B. (2001) The significant unmet needs of cancer patients: probing psychological concerns. Supportive Care in Cancer 9(8), 597-605.
Sundeen S.J., Stuart G.W., Rankin E.A.D. & Cohen S.A. (1994) Nurse-client interaction. Implementing the nursing process. 5th ed. Mosby-Year Book, USA.
Svensson E. (1998) Ordinal invariant measures for individual and group changes in ordered categorical data. Statistics in Medicine 17, 2923-2936.
Svensson E. & Starmark J-E. (2002) Evaluation of individual and group changes in social outcome after aneurysmal subarachnoid haemorrhage: a long-term follow-up study. Journal of Rehabilitation Medicine 34, 251-259.
88

89
Sätterlund Larsson U., Svärdsudd K., Wedel H. & Säljö R. (1989) Patient involvement in decision making in surgical and orthopaedic practice: The project perioperative risk. Social Science and Medicine 28 (8), 829-835.
Tanner C.A. (1987) Teaching clinical judgment. In: Fitzpatrick J.J. & Taunton R.L. (Eds) Annual Review of Nursing Research , 153-173. Springer, New York.
Thompson C. (2003) Clinical experience as evidence in evidence-based practice. Journal of Advanced Nursing 43(3), 230-237.
Thorne S., Ternulf Nyhlin K. & Paterson B. (2000) Attitudes toward patient expertise in chronic illness. International Journal of Nursing Studies 37, 303-311.
Tiesinga L.J., Dijkstra A., Dassen T.W.N., Halfens R.J.G. & van den Heuvel W.J.A. (2002) Are nurses able to assess fatigue, exertion fatigue and types of fatigue in residential home patients? Scandinavian Journal of Caring Sciences 16,129-136.
Timonen L. & Sihvonen M. (2000) Patient participation in bedside reporting in surgical wards. Journal of Clinical Nursing 9, 542-548.
Torjuul K. & Sorlie V. (2006) Nursing is different than medicine: ethical difficulties in the process of care in surgical units. Journal of Advanced Nursing56(4), 404-413.
Tutton E.M.M. (2005) Patient participation on a ward for frail older people. Journal of Advanced Nursing 50(2), 143-152.
Törnvall E., Wilhelmsson S. & Wahren L.K. (2004) Electronic nursing documentation in primary health care. Scandinavian Journal of Caring Sciences 18,310-317.
Vellas B., Guigoz Y., Garry P.J., Nourhashemi F., Bennahum D., Lauque S. & Albarede J.L. (1999) The mini nutritional assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 15, 116-122.
Wallentin L., Palm C.-A. & Gardulf A. (1996) Revision av omvårdnadsdokumentation, skriftliga läkemedelsordinationer och iordningställande av läkemedel på sjukhem. (Revision of nursing documentation, written medical orders and preparation of medicines in nursing homes). Vårdadministratören, 2, 7-14 (in Swedish).
Walsh K. & Kowankok I. (2002) Nurses’ and patients’ perceptions of dignity. International Journal of Nursing Practice 8, 143-151.
89

90
Waterworth S. & Luker K.A. (1990) Reluctant collaborators: do patients want to be involved in decision about care. Journal of Advanced Nursing 15, 971-976.
Weed L.L. & Zimny N.J (1989) The problem-oriented system, problem-knowledge coupling, and clinical decision making. Physical Therapy 69(7):565-568..
Weed L.L. & Weed L. (1999) Opening the black box of clinical judgment – an overview. British Medical Journal 319, 1-4.
Wensing M. & Grol R. (1998) What can patients do to improve health care?Health Expectations 1(1), 37-49.
Wilde B., Larsson G., Larsson M. & Starrin B. (1994) Quality of care: development of a patient-centered questionnaire based on a grounded theory model. Scandinavian Journal of Caring Sciences 8, 39-48.
WHO (1978) Declaration of Alma Ata. World Health Organization (Internet access 2006-10-31: http://www.who.dk/AboutWHO/Policy/20010827_1)
WHO (2003) International Classification of Functioning, Disability and Health.Online version. World Health Organization (Internet access 2006-10-02: http://www3.who.int/icf/onlinebrowser/icf.cfm
WHO (2006) ICD-10. International Statistical Classification of Diseases and Related Health Problems (10th rev.) Online version for 2006. World Health Organization (Internet access 2006-10-31: http://www.who.int/classifications/apps/icd/icd10online/)
Woodward V.M. (1998) Caring, patient autonomy, and the stigma of paternalism. Journal of Advanced Nursing 28(5), 1046-1052.
Yura H. & Walsh M.B. (1988) The nursing process. Assessing, planning, implementing, evaluation. 5th ed., Appleton & Lange, Norwalk, CT.
Ziegler S.M. (1984) Nursing Diagnosis - the state of the art as reflected in graduate student’s work. In M.J. Kim, G.K. McFarland, & A.M. McLane (Eds.), Classification of nursing diagnoses: Proceedings of the fifth national conference(pp. 199-208). The CV Mosby Company. St. Louis.
Öhman M. & Söderberg S. (2004) District nursing – sharing an understanding by being present. Experiences of encounters with people with serious illness and their close relatives in their homes. Journal of Clinical Nursing 13, 858-866.
90


















