Patient and Public Engagement Joint Committee
80
Title Lead Purpose B L MK 1 Welcome Housekeeping Introductions 10:00 Chair 2 Declarations of interest relating to agenda Chair Requirement 3 Chair’s update Chair Information 4 Minutes from previous meeting 18 August 2020 Chair Approval 5 Action tracker Chair Discussion 6 Consultation and Engagement pipeline - our approach 10:20 Sarah Frisby / Mark Cox Discussion / Approve 7 Communications and Engagement Strategy 2021 10:50 Michelle Summers Discussion / co- produce 8 BLMK Flu campaign 11:20 Jackie Bowry/ Christina Gleeson/ Sanhita Chakrabarti Update / Assure 9 Updates and reports • NHS 111 First • Report - BLMK One Team public engagement 11:40 Chair Information 10 Regular reports and papers relating to action log • BLMK Recovery Plan • Glossary of terms • Social media log 11:45 Chair Information 11 AOB 11:50 Chair 12 Date of next meeting: Tuesday 15 December 2020, 10:00am MS Teams Chair Information Patient and Public Engagement Joint Committee Tuesday 20 October 2020, 10:00 Virtual meeting – MS Teams
Transcript of Patient and Public Engagement Joint Committee

Title Lead Purpose B L MK 1 Welcome
Housekeeping Introductions
10:00 Chair
2 Declarations of interest relating to agenda
Chair Requirement
3 Chair’s update Chair Information
4 Minutes from previous meeting 18 August 2020
Chair Approval
5 Action tracker Chair Discussion
6 Consultation and Engagement pipeline - our approach
10:20 Sarah Frisby / Mark Cox
Discussion / Approve
7 Communications and Engagement Strategy 2021
10:50 Michelle Summers Discussion / co-produce
8 BLMK Flu campaign 11:20 Jackie Bowry/ Christina Gleeson/ Sanhita Chakrabarti
Update / Assure
9 Updates and reports • NHS 111 First• Report - BLMK One Team
public engagement
11:40 Chair Information
10 Regular reports and papers relating to action log
• BLMK Recovery Plan• Glossary of terms• Social media log
11:45 Chair Information
11 AOB 11:50 Chair
12 Date of next meeting:
Tuesday 15 December 2020, 10:00am MS Teams
Chair Information
Patient and Public Engagement Joint Committee Tuesday 20 October 2020, 10:00 Virtual meeting – MS Teams

Author: N/A
Contact Information: Anona Hoyle
Lead Executive: Jane Meggitt
Which CCGs does this agenda item apply to?
Bedfordshire
Luton Milton Keynes
Which activity does this agenda item relate to?
Draft minutes from committee meetings held on 18 August 2020.
How?
What is the Committee/ being asked to do?
Review and approve the draft Patient and Public Engagement Joint Committee Minutes from 18 August
What are the financial implications?
N/A
Set out the key risks and risk ratings
N/A
Date to which the information this paper is based on was accurate
N/A
Patient and Public Engagement Joint Committee 20 October 2020
Agenda item 4
Draft Minutes from PPEJC 18 August 2020
Information

CONFIDENTIAL Page 1 of 8
Minutes of the PPEJC Meeting Held on Tuesday 18 August 2020
Held over Microsoft teams
Patient and Organisational Representatives and Meeting Presenters Present Effie Assan Patient and public representative BLMK EA Steve Black Patient and public representative BLMK SB Diana Blackmun Healthwatch Central Bedfordshire Bedfordshire DB Cheryl Green Patient and Public Representative BLMK CGr Alan Hancock Patient and Public Representative BLMK AHa Tracy Keech Healthwatch Milton Keynes Milton Keynes TK Lucy Nicholson Healthwatch Luton Luton LN Martin Trinder Community Voluntary Services (CVS)
Bedfordshire BLMK MTr
Phil Turner Patient and public representative BLMK PT John Wright Healthwatch Bedford Borough Bedfordshire JW Lisa Wright Advocate for Children and Young People
(CYP) across BLMK BLMK LW
Members Present: Alison Borrett Chair of PPEJC / Lay Member Bedfordshire AB Dr Nessan Carson GP Member Milton Keynes NC Lloyd Denny Lay Member Luton LD Dr Christopher Longstaff
GP Member Bedfordshire CL
Nicky Poulain Director of Primary Care BLMK NP Mike Rowlands Lay Member Milton Keynes MR
CCG Staff and Presenters Present Christina Gleeson Public Health across Bedford Borough,
Central Beds and Milton Keynes Council BLMK CGl
Sarah Frisby Senior Communications and Engagement Manager
BLMK SF
Maryla Hart Governance and Committee Officer Bedfordshire MH Anona Hoyle Senior Communications and Engagement
Officer BLMK AHo
Jane Meggitt Director of Communications and Engagement
BLMK JM
Barbara Moran Head of Urgent and Emergency Care Commissioning
BLMK BM
Dr Paul Singer BLMK ICS Chief Clinical Information Officer BLMK PS Michelle Summers Head of Communications and Engagement BLMK MS Ken Thompson BLMK ICS Information Governance
Manager BLMK KT
Apologies:

Page 2 of 8 CONFIDENTIAL
Richard Alsop Director of Commissioning and Contracting BLMK RA Jackie Bowry Communications and Engagement
Manager BLMK JB
Dr Krishna Patel GP Member Milton Keynes KP Josan Race Community Action Milton Keynes BLMK JR Maxine Taffetani Healthwatch, Milton Keynes Milton Keynes MTa
1. Welcome, Housekeeping and Introductions
The Chair welcomed all members and attendees to the meeting. The Chair advised that the meeting was quorate. The Chair welcomed Alan Hancock, a Patient and Public Representative from Milton Keynes. The Chair welcomed Tracy Keech to the meeting, who will be deputising for Maxine Taffetani from Healthwatch Milton Keynes going forward.
Action
2. Apologies for absence Apologies were received and noted as above.
3. Declarations of Interest The Chair asked for any declarations of interest with regards to items on the agenda. Alan Hancock declared the following interests to be noted in the minutes for the purpose of transparency. AH holds the following posts:
• Deputy Chair, Healthwatch Milton Keynes • Public Governor, Milton Keynes University Hospital • Council Member (Expert by Experience), East of England Clinical
Senate • Member, Patient Council, Renal Association
The Chair advised that all present could stay in the meeting for all items.
4. Chair’s Update The Chair gave an introduction and verbal update.
5. Minutes of last meeting The minutes of the following meetings were approved as an accurate record:
• 16 June 2020 • 23 June 2020
6. ACTION Log The following actions were agreed as closed: 2, 4, 5, 6, 8, 9, 10, 11, 12, 13, 14, 15, 17, 18. The following updates were given:

Page 3 of 8 CONFIDENTIAL
Actions 1, 26 and 33. Update: AH to send out an update to address all of these actions. Action 2. Role and Function of the PPEJC. Update: Alan Hancock has joined the PPEJC so this action can be closed. Action 3. Role and functions of the PPEJC. Update: in progress. A meeting has been held and modelling will be carried out. Action 13. BLMK One Team Update. Update: a diagram of the BLMK Integrated Care System (ICS) has been included in the updated meeting pack as part of item 11. Closed Action 14. Glossary of Terms. This is in progress and will be shared with the committee in due course. Ongoing
7. BLMK One CCG – Engaging with Public The Committee was asked to review and provide feedback on the engagement plan in order to provide assurance to the Governing Body that the proposed engagement met statutory requirements. SF gave an update on the work done so far regarding engaging with the public advising that it was 6 week engagement piece from Monday 3 August to Sunday 13 September. An interim report of findings would be shared with the Governing Body in September and a final report published at the end of the engagement activity. SF advised that the survey was being promoted across the CCGs digital platforms and via partners and networks. There was a British Sign Language (BSL) subtitled video, and targeted Facebook advertising. 214 responses had been received as at 18 August. The team is looking to target different geographical areas and people of different ages. SF opened the floor to questions. PT asked about numbers of responses for different geographical areas ACTION: AHo to circulate response figures for different geographical areas to the PPEJC. TK and CGr asked why the CCG was conducting the survey asking residents for their feedback when there the change was nationally mandated. SF advised that engagement enabled the CCG to find out any concerns or reservations that the public had, so the CCG could address them. AHa felt reassured about the mandate and the limits but advised he found the questionnaire had a predisposition towards positive outcomes NPo advised that the Primary Care Team and local GP practices work with the Local Medical Committees (LMCs) in Buckinghamshire and Bedfordshire. NPo advised that building trust and relationships was key to the whole process. NP acknowledged that the joining of the CCGs is national policy, and that the survey was to find out any concerns that the public had. MS confirmed that conducting the survey was nationally mandated. The public can shape the way the organisation looks in the future. The CCGs have
SF/AHo

Page 4 of 8 CONFIDENTIAL
engaged with elected councillors through the Scrutiny Committees. Bedford Borough Council has made the request to have at least one Bedford Borough GP elected to the Governing Body. This has been enshrined in our governance. Any other feedback from residents can also be taken back to the governing body and may help shape how the CCG looks in the future. CGr commented that patients are worried that there may be a decline in the level of healthcare in Bedford and decisions would be taken by people who have no local knowledge. MS advised that the CCG will always continue to be clinically led and that the clinical voice will come through decision making. CL advised that he could understand CGr’s concern. He advised that there was local representation which should be strengthened in the future. The Primary Care Networks (PCNs) and the PCN Directors are becoming more influential in the system. NC commented that the CCGs would be looking at what could be done at scale and what should be done locally at place. The committee were pleased to assure the engagement plan.
8. NHS 111 First BLMK Communications Plan BM and MS presented this item. The Communications Plan which included background information regarding NHS111 First had been circulated prior to the meeting. BM and MS advised that:
• During the peak months of the coronavirus pandemic the number of people attending Emergency Departments (EDs) reduced dramatically, particularly those seeking help for minor illnesses, this was mainly due to people contacting NHS111 first
• In recent weeks the number of people visiting EDs has risen, and in some places, risen sharply.
• At the same time, due to social distancing and infection prevention and control precautions, the space in EDs has reduced by 30-50%.
• If people call NHS111 first they are less likely to attend A&E in BLMK. NHS111 can offer patients alternative care to meet their needs.
• The public should be guided in making the right healthcare choices to ensure their safety, as well as making sure they get the right treatment in the most appropriate place. Increasingly NHS111 should either book people into A&E or refer them to the most appropriate service.
• NHS 111 will make it easier and safer for patients to get the right advice or treatment when they urgently need it and increasingly, they will be able to book direct appointments/time windows into a service that is right for them.
• From 1st December 2020, NHS111 in BLMK will increasingly be able to book appointments for patients that need to attend an Emergency Department, to ensure patients are seen as safely and conveniently as possible.

Page 5 of 8 CONFIDENTIAL
The PPEJC was asked for feedback on the first draft of the communications plan before the plan is shared with the local authority scrutiny committees. SB asked whether NHS111 makes any difference to the things the NHS is aiming for. Is there any evidence that the policies actually worked? Total triage with GPs rather than bookable appointments has changed since Covid. Allowing NHS111 to book appointments is not being driven nationally as they favour total triage. There is a contradiction between national policy that works and does not. BM responded that all directly bookable slots are telephone appointments so the practices can run triage. This has been replicated across most of the direct booking offers in BLMK, as opposed to providing face-to-face appointments. CL offered a GP perspective, saying “In Leighton Buzzard we don’t have face to face appointments booked directly by anyone else except practices. This helps practices know the degree to which the patient has been screened as a Covid risk. GPs are grateful that it works in this way.” CL advised that appointments are more fluid, where a triage appointment may turn into an appointment as there is not necessarily a distinction between the triage discussion and the appointment itself. SB asked how good BLMK is at using online triage as well as telephone triage. CL advised that his practice is not using much online triage but some other practices are. It depends on the practice and their decisions which are down to patients and clinicians. AB reminded the committee that that the purpose of the committee is to review the engagement plan rather than challenge or question national policy. ACTION: JW commented the use of GP surgeries as a communication channel was missing from the plan. Communication plan to be updated to include. NC advised that different practices are using different software for engagement with patients and his practice is using Footfall. NP advised that the message is always to “ring your GP practice but if you can’t get through then ring 111”. EA commented that she had seen an NHS 111 advertisement on a screen at a GP surgery. PT suggested that some clearer communications to the public would be useful. Also Covid seems to have highlighted available services to the public. If this reduces pressures on A&E and GP surgeries then this is positive. DB asked what would happen to people who had a booked appointment at A&E if people presented themselves without an appointment. BM responded that this forms part of the operational requirements, the new approach is not about preventing people from being able to access A&E directly, but when they are unsure if the need is urgent rather than an emergency, that they be encouraged to call NHS 111.
MS/BM

Page 6 of 8 CONFIDENTIAL
The committee advised that it was very likely that patients would find it difficult to know who to contact and that the public messaging needed to be very clear. ACTION: The Communications Team to review messaging and share with the committee. BM advised that our message in BLMK has been well received /understood in the past. LD comment in the MS chat: “Phil, made a number of good points. Covid 19 may have helped with easing the pressure on A&E but is this long term? Let's carry out some form of survey, let's find out especially from the less engaged. Clearly some have got used to 111 but let's manage the demand.” CGr commented that people will continue to present at the Walk in Centre in Putnoe. NP concluded that the most important thing was keeping people safe, to try and help people help them themselves and for healthcare providers to work together as a health system. ACTION: NC asked for collateral to be available in different languages and formats
MS
MS
9. Flu Plan Christina Gleeson from the Public Health Team (BBC, CBC and MKC) and MS introduced this item. The Communications Plan which included background information regarding the BLMK Flu had been circulated prior to the meeting. CGl advised that she works for Public Health across Bedford Borough, Central Beds and Milton Keynes Councils and is working with the communications teams for BLMK CCGs and in collaboration with Luton Borough Council. CGl advised To reach the newly increased flu vaccination targets this year it will be more important than ever that all health and social care partners work together to promote flu vaccinations. We have established a BLMK Flu Communications Cell to assist with this which involves, Hospitals, providers, voluntary groups and local authorities. We are taking our lead from the Strategic Flu Group which has oversight of the vaccination programme for BLMK. We want to achieve working as one system with a consistent messages across the patch. Our communications need to be targeted and accessible. The ultimate aim is to protect the population and their health and support the national strategies around NHS staff. This is an extremely infectious disease. Just like Covid, flu can be asymptomatic or mild but can be easily passed on. MS ran through the Communications and Engagement Plan and tactics and said the new joint up working with partners was extremely beneficial. Advising

Page 7 of 8 CONFIDENTIAL
that partners will be working with different communities including faith and Black, Asian Minority Ethnic (BAME) communities in BLMK. It is clear that we need trusted people such as clinicians and cultural leaders within the community to promote the flu vaccine. MS advised that we want to launch a campaign called Trusted Voices and to create some local collateral featuring local leaders and residents in addition to the standard materials issued by NHS England (NHSE). TK recommended that the messaging be shared as soon as possible as there are already ‘discussions’ on local Facebook groups. TK advised that at PCN meetings there are lots of good ideas about how to increase uptake and patient choice, with patients eligible for a free vaccination choosing whether to have their vaccination at their GP surgery or local pharmacist. LD thanked CGl for the informative presentation and congratulated the team on the approach. He agreed that that messaging via community and faith leaders was important and myth busting crucial. ACTION: NP advised she would pick up with TK (Healthwatch Milton Keynes) regarding posts on Facebook. SB asked where we are targeting the messages. He advised that Public Health England (PHE) did some research last year about why there was low uptake. PHE findings found that the main reason was that the patients forgot and needed to be reminded to have their vaccination (by pharmacists and other health and social care professionals). CGl advised patients currently ‘shielding’ will receive letters from NHSE Intelligence Team as well as from their practice. ACTION: AB asked for flu to be kept on the agenda for the next meeting. ACTION: Any more feedback to be emailed to Anona Hoyle to send to CGl and MS.
NP
AH
All
10. My Care Record AB welcomed Dr Paul Singer and Ken Thompson. KT gave a presentation on My Care Record (MCR) which had been circulated prior to the meeting KT explained that my Care Record is an approach to improving care by joining up health and care information. It enables health and care professionals to access the information they need to look after patients, even if they work for different organisations or indifferent locations. PS advised that this isn’t a new record, it is a way of sharing existing records and respecting confidentiality and improving the standards of Health and Social Care we can provide. NC commented that it had been difficult to communicate patient data with hospitals and social care as the use different digital platforms. He hoped that MCR would resolve the issue. Action: Members of the committee to contact KT with any feedback on their approach and collateral.
All

Page 8 of 8 CONFIDENTIAL
11. Papers for information • Revised Terms of reference (v2.2)
o These were approved by Dr Nicola Smith and will go to the Governing Body in September for ratification.
• Updated engagement log • Social media reports
The PPEJC noted the papers listed above.
12. Any Other Business The Chair thanked Maryla Hart for her sterling work in pulling together the agenda packs for meetings as this was Maryla’s last meeting supporting the PPEJC.
13. Date of next meeting: Tuesday 20 October 2020,10:00am
The Meeting Closed at 12.03

Author: N/A
Contact Information: Anona Hoyle
Lead Executive: Jane Meggitt
Which CCGs does this agenda item apply to?
Bedfordshire
Luton Milton Keynes
Which activity does this agenda item relate to?
Action Tracker
How?
What is the Committee/ being asked to do?
To discuss and provide updates for the action tracker.
What are the financial implications?
N/A
Set out the key risks and risk ratings
N/A
Date to which the information this paper is based on was accurate
N/A
Patient and Public Engagement Joint Committee 20 October 2020
Agenda item 5
Action Tracker
Information

16/10/2020 PPEJC Action Log
Page 1 of 2
PPEJC
EscalatedOutstandingIn ProgressNot Yet DueCOMPLETE:
Propose closure at next meetingCLOSED
(dd/mm/yyyy)
Action No.
Meeting Date CCG Item Title Action Responsible Manager (Enter full name)
Delegated to (Enter full
name)Can hide this column when sending out
Past deadlines
(Since Revised)
Current Deadline Current Position RAG(Add date action is
agreed closed)
26 24/09/2019 Luton 4 NP to share the Primary Care options paper when available (from December) for the group to review
Nicky Poulain Jan-20 16-06-2020: This is to be addressed in action 1 below. 20-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)
33 28/01/2020 Luton 5 Npo to obtain clarity regarding hand-written prescription Nicky Poulain Anona Hoyle Mar-20 16-06-2020: This is to be addressed in action 1 below. 20-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)
1 16/06/2020 Luton Action Logs from PPEC, HSCEG and PRIAG
Anona Hoyle to send an update to the HSCEG. This will tie up the above open actions (26, 30 and 34).
Nicky Poulain Anona Hoyle 18-08-20: AH to send out an update. Update sent 3 September20-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)
3 16/06/2020 BLMK Role and functions of the PPEJC
PT asked it to be noted that Luton CCG and Luton Council’s HSCEG was a joint committee which incorporated both health and social care. The committee had been working well and that social care needs to continue to be incorporated into future work. This issue to be taken forward by the Communications Team
Michelle Summers / Anona Hoyle
Anona Hoyle Aug-20 Meeting was held with LD and PT to review situation. Further work is required, which will be undertaken once the ICS / ICP work work has been conducted10-08-20 Recommendation to leave open18-08-20: A meeting has been held and modelling will be carried out.
COMPLETE(Propose Closure 20/10/20)
14 23/06/2020 BLMK BLMK One Team Update
Produce a glossary of terms Anona Hoyle Aug-20 Shared as part of meeting pack 20-10-2020-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)
16 23/06/2020 BLMK BLMK Communication and Engagement Work Streams
Modify the plan following suggestions made at the meeting and circulate revised plan
Michelle Summers Aug-20 Shared as part of meeting pack 20-10-2020-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)
19 18/08/2020 BLMK BLMK One CCG – Engaging with Public
AHo to circulate response figures for different geographical areas to the PPEJC.
Anona Hoyle / Sarah Frisby
Aug-20 Figures circulated to PPEJC members20-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)
20 18/08/2020 BLMK NHS 111 First BLMK Communications Plan
JW commented the use of GP surgeries as a communication channel was missing from the plan. Communication plan to be updated to include.
Michelle Summers / Barbara Moran
Oct-20 Plan updated20-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)
21 18/08/2020 BLMK NHS 111 First BLMK Communications Plan
The Communications Team to review messaging and share with the committee.
Michelle Summers Oct-20 Included as agenda item 20-10-2020-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)
22 18/08/2020 BLMK NHS 111 First BLMK Communications Plan
NC asked for collateral to be available in different languages and formats
Michelle Summers Oct-20 20-10-20 Collateral being produced In progress
23 18/08/2020 BLMK Flu Plan NP advised she would pick up with Tracy Keech (Healthwatch Milton Keynes) regarding posts on Facebook.
Nicky Poulain Oct-20
24 18/08/2020 BLMK Flu Plan AB asked for flu to be kept on the agenda for the next meeting.
Anona Hoyle Oct-20 Included on agenda for October meeting20-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)
25 18/08/2020 BLMK Flu Plan Any more feedback to be emailed to Anona Hoyle to send to CG and MS.
All Oct-20 No feedback received20-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)
RAG KEY Escalated - items flagged RED for 3 subsequent meetings - BLACKOutstanding - no actions made to progress OR actions made but not on track to deliver due date - REDIn Progress. Outstanding - actions made to progress & on track to deliver due date - AMBERNot Yet DueCOMPLETE - GREEN
CLOSED

16/10/2020 PPEJC Action Log
Page 2 of 2
Action No.
Meeting Date CCG Item Title Action Responsible Manager (Enter full name)
Delegated to (Enter full
name)Can hide this column when sending out
Past deadlines
(Since Revised)
Current Deadline Current Position RAG(Add date action is
agreed closed)
26 18/08/2020 BLMK My Care Record Members of the committee to contact Ken Thompson with any feedback on their approach and collateral.
All Oct-20 Members should have contacted Ken Thompson direct20-10-20 Recommendation to close
COMPLETE(Propose Closure 20/10/20)

Author: Sarah Frisby
Contact Information: Sarah Frisby
Lead Executive: Jane Meggitt
Which CCGs does this agenda item apply to?
Bedfordshire
Luton Milton Keynes
Which activity does this agenda item relate to?
- Assure patient engagement and feedback mechanisms are in place.
- Assure the delivery of equality and health inequality duties around patient and public engagement
- Ensure patient experience is used to support service development and improvement.
How?
What is the Committee/ being asked to do?
Following the update, provide recommendations for the organisation to consider as plans are further developed.
What are the financial implications?
N/A
Set out the key risks and risk ratings
N/A
Date to which the information this paper is based on was accurate
N/A
Patient and Public Engagement Joint Committee 20 October 2020
Agenda item 6
Consultation and Engagement Pipeline – our approach
Information

Author: Michelle Summers
Contact Information: Michelle Summers
Lead Executive: Jane Meggitt
Which CCGs does this agenda item apply to?
Bedfordshire
Luton Milton Keynes
Which activity does this agenda item relate to?
- Assure patient engagement and feedback mechanisms are in place.
- Assure the delivery of equality and health inequality duties around patient and public engagement
- Ensure patient experience is used to support service development and improvement.
How?
What is the Committee/ being asked to do?
To co-produce the Communications and Engagment Strategy 2021
What are the financial implications?
N/A
Set out the key risks and risk ratings
N/A
Date to which the information this paper is based on was accurate
12/10/20
This draft document attached reflects the requirements laid out under the Health and Social Care Act 2012 and looks at strategic approaches to communications and engagement, as well as plans for future development.
The committee is asked at the meeting to help co-produce the Communications and Engagement Strategy which will be adopted by the CCGs.
Patient and Public Engagement Joint Committee 20 October 2020
Agenda item 7
Communications and Engagement Strategy 2021
Information

1
An NHS for the future NHS Bedfordshire, Luton and Milton Keynes (BLMK) Clinical Commissioning Group (CCG) DRAFT Communications and Engagement Strategy – 2021- 2023
2nd Draft v.2 DATE: 14th September 2020
Communications and Engagement Strategy – 2021 - 2023

2
Contents 1.0 Introduction 3
1.1 Mission, vision and aims 4 1.2 Target audience 5
2.0 Engagement with patients and local communities 6 2.1 Principles of engagement 2.2 Principles of engagement through Covid19 2.3 Statutory requirements 2.4 How do we deliver good engagement? 2.5 How will we engage? 2.6 Engagement and what we expect from our providers 2.7 How feedback will be collated and responded to
3.0 Communicating with patients and local communities 12 3.1 Introduction 3.2 Digital platforms 3.3 Media Relations 3.4 External communications and partnerships 3.5 Internal communications 3.6 Crisis communications
4.0 Budget and resources 4.1 Communications and engagement budget 14 4.2 Resources and our team
5.0 Review 14 6.0 Conclusion
6.1 Next steps 14

3
1.0 Introduction The NHS Clinical Commissioning Group (CCG) covering Bedfordshire, Luton and Milton Keynes is a membership organisation made up of all local General Practices (GPs) who work together to plan and buy local health care and to make sure health and care services are there for the local population when they need them. The CCG is committed to putting local patients, communities, elected members and stakeholders at the centre of this and to work in partnership to find solutions to the health and social care challenges facing the area. This strategy reflects the requirements laid out under the Health and Social Care Act 2012. Communication and engagement is vital to the success of the CCG, where local partnerships and good working relationships are important for delivering improved outcomes for patients. This document looks at strategic approaches to communications and engagement, as well as plans for future development. It looks at how the CCG can work with existing groups and forums to develop a system that is transparent, inclusive and responsive. This strategy also recognises that, although the CCG aims to reflect patient feedback as much as possible in the services it commissions, there are times when decisions will be constrained by other factors such as patient safety or availability of resources. Where this is the case the CCG will exercise its duty around consultation and engagement, and will work with patients and local people to minimise impact and to communicate our decision-making clearly. This strategy sets out our principles and priorities. In particular, we will:
• value the public voice, and develop an open culture that listens, hears, and uses these insights to inform commissioning and service transformation;
• include the voices of local clinicians to provide a rich resource to inform the design and delivery of patient care;
• listen to the views of our population through a process of continuous engagement – involving our communities in health care throughout and not just when consultation is required. This will enable us to ensure greater involvement throughout the process.
Our GP membership and clinical leadership is central to our communications and engagement strategy. We will ensure that they are involved in all aspects of co-producing our communications and engagement programme to deliver better patient outcomes. Our success will be measured on the effectiveness of our relationships with our member practices, elected members, communities and system partners and providers. We will nurture relationships to deliver our ambition to become an outstanding Clinical Commissioning Group.

4
1.1 Mission, vision and aims Mission Our mission is to improve health and wellbeing and reduce inequalities for the people of Bedfordshire, Luton and Milton Keynes, Vision Our vision is to: Work collaboratively with people who live in BLMK and our partners so that people live longer lives in good health by:
1) Taking a population-health approach to focus on the best use local resources to address locally identified health and wellbeing priorities;
2) Spreading best clinical practice and quality improvement across BLMK to reduce inequalities and unwarranted clinical variation;
3) Enabling primary care to be the catalyst that delivers transformed, personalised care.
Values We will support these goals through the following values:
• Co-producing services with residents to respond to local needs;
• Developing patient centred, local services that meet patients’ needs and expectations;
• Strengthening clinical leadership to ensure that all services and pathways are steeped in clinical decision making;
• Reducing duplication and increasing efficiencies to maximise value for tax payers money;
• Collaborating with local authorities, Healthwatch and other partners through the Health and Wellbeing Boards to ensure that all services are integrated, deliver for the local community and achieve our objective of eradicating poverty and reducing the health inequality gap.
• To observe the ‘Nolan Principles’ for the ethical standards expected of public office, which are Selflessness, Integrity, Objectivity, Accountability, Objectivity, Accountability, Openness, Honesty and Leadership.

5
1.2 Target audiences The main target audiences that we will engage with during the course of our work include:
• Patients, older people, younger people, carers, working age women, BAME and seldom heard communities;
• Internal: GP Members, staff, clinicians / clinical leads, the Governing Body, primary care;
• External: Voluntary sector, Healthwatch, third sector organisations, charities, community groups, faith groups;
• Stakeholders: NHSEI, local authorities, elected members including Councillors and MPs, opinion formers, suppliers, providers and the media.
The communications and engagement strategy is shaped by population health data and the information set out in the Joint Strategic Needs Assessment (JSNA) for the four places within BLMK, which sets out that:
• There is an older population living longer with long term health conditions;
• There is a large rural area within Central Bedfordshire that does not have the same access to healthcare as in the urban centres – meaning that more services need to be delivered closer to home;
• There are diverse communities in Luton, Bedford and Milton Keynes, which require targeted communications;
• There is a large health inequality gap within BLMK which results in many communities receiving poorer health outcomes than in more affluent areas.
These issues provide a challenging communications and engagement environment within which to operate, and require collaboration across multi agencies and engagement with community and faith groups, if the strategy is to deliver its mission and vision. 1.3 Stakeholders In delivering this strategy, it is essential that we have a comprehensive picture of our local community and stakeholders, if we are to deliver successful, inclusive engagement. Stakeholder map to be developed.

6
2.0 Engaging with local patients and communities 2.1 Principles of patient and public engagement Bedfordshire, Luton and Milton Keynes CCG will build on the six principles of engaging people and communities, as developed by ‘National Voices’ in conjunction with NHS England in 2016. The six principles require CCGs to demonstrate:
• Care and support is person-centred: personalised, coordinated, and empowering;
• Services are created in partnership with citizens and communities; • Focus is on equality and narrowing inequalities; • Carers are identified, supported and involved; • Voluntary, community and social enterprise and housing sectors are involved
as key partners and enablers; • Volunteering and social action are recognised as key enablers.
To work towards these principles, Bedfordshire, Luton and Milton Keynes CCG is committed to delivering local patient and public engagement that is:
• Inclusive – everyone will have a voice regardless of their age, gender, ability, religion, sexuality, language, or culture.
• Flexible – using different engagement methods depending on the subject and
type of insight needed, and continuing to explore new and innovative ways of engaging.
• Measured – changes to local services and other outcomes that have
happened as a result of engagement activity will be reported back by:
o contact with participants; o through our website and the local media; o through our annual report; o through our annual stakeholder event.
• Honest – about what is changing and why, and about the extent that
engagement can influence the changes.
• Transparent – by using plain English, making information readily available and producing information in different languages and formats.
• Fair – giving everyone the chance to be involved and enough time to take
part.
• Two-way - Internally and externally, encouraging feedback at all levels and showing where services and systems have changed to reflect this

7
• Meaningful – the involvement exercise itself has a clear purpose and is relevant and understandable to those involved.
• Representative – making sure the right people are involved and actively
seeking the groups and individuals less likely to come forward.
• Collaborative – using opportunities to work with other groups and partners to engage and gather insight, resulting in the building of partnerships.
• Part of the day job – all members of staff within the CCG are committed to
listening to the voice of patients and the public, and of using all opportunities to gather insight.
2.2 Principles of engagement through Covid19 The NHS has recognised the coronavirus pandemic as a level 4 incident which means that local NHS activity became subject to command and control by NHS England and Improvement with the Department of Health and Social Care. Whilst there are some changes that will be made under ‘emergency measures’ as part of the pandemic, to ensure that we can deliver services safely, we will continue to observe the ‘Nolan Principles’ for the ethical standards expected of public office, as outlined above. We will also continue to follow best practice within the context of the Covid-19 national incident in allowing local patients, public and stakeholders the maximum possible time to engage with us, and to provide a variety of innovative options to feedback during a time when meetings and the movement of local people are restricted. This will also reflect our commitment to providing our information in a range of formats such as easy read and large print where possible. All changes will be considered ‘temporary’ and will be reviewed at a later date. The timescale for the review of local service changes is likely to be set nationally. We will undertake to keep our local residents abreast of the situations as they unfold and to involve local stakeholders in the review process. Following any period of review, should there be a requirement to make any changes permanent, we will undertake a period of engagement or consultation as appropriate, involving Healthwatch organisations, and the Health Overview and Scrutiny Committees in Bedfordshire, Luton and Milton Keynes. 2.3 Legal Requirements The CCG is a legal or statutory organisation and under the Health and Social Care Act, 2012 is required to fulfil a legal duty to involve patients and members of the public in all decisions that affect them i.e. the commissioning of services for the population of Bedfordshire, Luton and Milton Keynes.
8
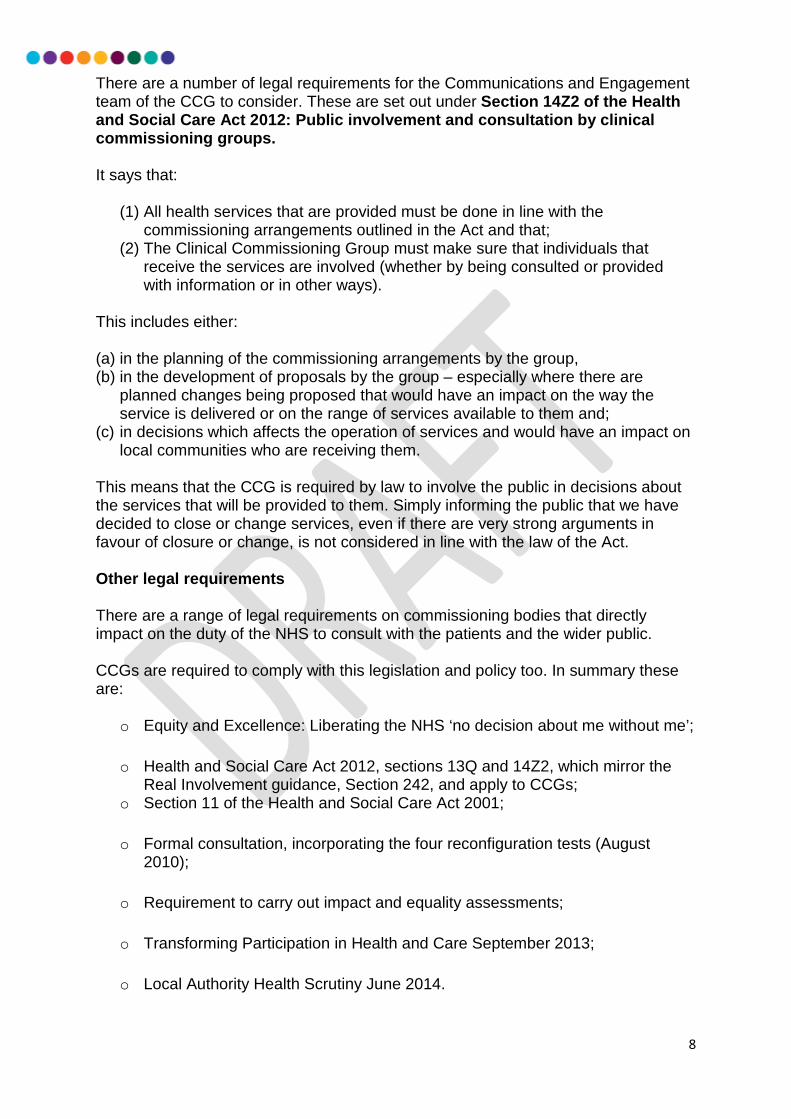
There are a number of legal requirements for the Communications and Engagement team of the CCG to consider. These are set out under Section 14Z2 of the Health and Social Care Act 2012: Public involvement and consultation by clinical commissioning groups. It says that:
(1) All health services that are provided must be done in line with the commissioning arrangements outlined in the Act and that;
(2) The Clinical Commissioning Group must make sure that individuals that receive the services are involved (whether by being consulted or provided with information or in other ways).
This includes either: (a) in the planning of the commissioning arrangements by the group, (b) in the development of proposals by the group – especially where there are
planned changes being proposed that would have an impact on the way the service is delivered or on the range of services available to them and;
(c) in decisions which affects the operation of services and would have an impact on local communities who are receiving them.
This means that the CCG is required by law to involve the public in decisions about the services that will be provided to them. Simply informing the public that we have decided to close or change services, even if there are very strong arguments in favour of closure or change, is not considered in line with the law of the Act. Other legal requirements There are a range of legal requirements on commissioning bodies that directly impact on the duty of the NHS to consult with the patients and the wider public. CCGs are required to comply with this legislation and policy too. In summary these are:
o Equity and Excellence: Liberating the NHS ‘no decision about me without me’;
o Health and Social Care Act 2012, sections 13Q and 14Z2, which mirror the Real Involvement guidance, Section 242, and apply to CCGs;
o Section 11 of the Health and Social Care Act 2001;
o Formal consultation, incorporating the four reconfiguration tests (August 2010);
o Requirement to carry out impact and equality assessments;
o Transforming Participation in Health and Care September 2013;
o Local Authority Health Scrutiny June 2014.

9
2.4 How we will deliver good engagement We will engage local people, communities and our stakeholders in setting our priorities and we will review these with them annually. Bedfordshire, Luton and Milton Keynes has established a Patient and Public Engagement Joint Committee, which is a formal sub -committee of the Governing Body, designed to provide assurance that we are delivering our statutory responsibilities. The group comprises of:
- Four public representatives from each of the four places; - Healthwatch representatives from all four BLMK places; - Local Authority representation for adult and young people’s services; - Council of Faiths; - The voluntary sector - CCG Executive Directors for Commissioning , Primary Care and
Communications and Engagement; - GP Members
All commissioning strategies are taken to the Public and Patient Engagement Joint Committee (PPEJC) for discussion at the start of commissioning programmes. Representatives are given the opportunity to provide their insights into how services should be designed and provide recommendations – either for service configuration or how local communities should be brought in to allow for richer and deeper feedback. Commissioners are then asked to respond and report back to the Committee in a “you said, we did”, so that we can provide assurance that local views are involved in shaping services. The Committee is chaired by the Lay Member for Public Involvement, who takes the lead in holding CCG Officers to account and providing assurance to the Governing Body that the CCG is delivering on its legal duty to involve. Through this committee, we aim to engage and plan how we will co-design local services, so that patients and the public are involved from the outset in shaping and designing of local services and in how they are delivered. Working in partnership with local authority colleagues, councillors, faith and community groups and public members with an identified interest in specific services, we will ensure that we provide local people with the opportunity to become involved in service redesign through and mobilisation. This involves working closely with commissioners to build public involvement into programme plans from the offset, so that patients and the public are included in discussions from the beginning of contract discussions, options appraisals and setting specifications.

10
We will follow recently issued NHS practical advice about engagement on service changes that have happened as a result of the COVID-19 outbreak and planning for the next phases (Good practice for stakeholder engagement on service change and reconfiguration during Covid-19, August 2020; Short Guide to Socially Distanced Engagement, August 2020). 2.5 How we will engage
Bedfordshire, Luton and Milton Keynes will use the NHS England ‘What matters to you’ approach to engagement, which aims to support communications between health and social care and the local community. Designed to understand what matters to residents, this approach will create more positive dialogue and help to build trust between the CCG and its local communities. As part of this approach, the CCG will look to:
• Co-produce and co-design services with residents wherever possible – bringing groups together to understand what services are required and develop patient centred, personalised and localised approaches to healthcare. This could be managed in a number of ways for example, through the Patient and Public Engagement Joint Committee where representatives are asked to form a group to shape services and strategies, or through other established forums including Maternity Voice Partnerships, interest groups, faith groups meetings or engagement with councillors and elected members.
• Collaborate with partners in health, social care and the wider system to ensure we take on board feedback in the round, maximise patient outcomes and meet the needs of local, place based populations. This would include working through the system wide communications collaborative, which comprises of communications and engagement leads from all ICS partners, and elected members to ensure patient / constituent views are included in all commissioning decisions.
• Engage community and faith groups to ensure that our engagement is truly
inclusive, reaches out to seldom heard communities through a range of methods including Council of Faiths, Council of Mosques, church groups, voluntary services and draws on the support of trusted local voices to ensure all residents are given the opportunity to be heard. Using languages most spoken in BLMK including Urdu, Bengali, Guajarati, Italian, Polish and Romanian are some of the routes to engagement that will be required to ensure meaningful communications with patients;
• Engage with seldom heard communities through voluntary services, using
easy read formats for engagement and enlisting the support of translators including BSL for all engagements to ensure all voices are included;
• Put clinicians at the heart of our engagement to build trust with local communities and ensure that all decisions are based on sound clinical evidence.

11
• Enlist the support of elected members as the democratic voice of the
public, to ensure we give all aspects of our community the opportunity to shape local healthcare decisions.
• Continuously engage with residents, elected members, voluntary groups and community groups etc. through a range of channels to promote transparency, inclusivity and build brand equity in the new single CCG.
• Retain place based identities and respect the different needs of the ‘places’. Throughout the engagement process around the proposal to create one single CCG, it was emphasised that local communities were proud of their identities and did not want this to be lost in the process of becoming one single CCG.
2.6 What we expect from our providers
The CCG has a statutory duty to ensure that providers engage with service users from the start to the end of their contract. This includes involving patients and public members in co-producing and mobilising services, through to gathering patient feedback and responding to complaints and queries. We expect that all providers will abide by their statutory duties to involve service users in service re-design and provide complete transparency, in line with the ‘Nolan Principles’ sharing information about proposed changes and attending Overview and Scrutiny Committees to provide insight and updates and respond to recommendations from elected members. Directors and Clinicians from provider organisations will be expected to join CCG Executives in attending the Patient and Public Engagement Joint Committee, a committee of the Governing Body, to enable co-production and scrutiny from Lay Members and patient representatives, to ensure inclusion, involvement and complete transparency in the management of their contract. We expect communications and engagement updates to be provided to Commissioners through commissioner / provider contract meetings and in regular dialogue with the communications and engagement team. 2.7 How feedback will be collated and responded to The CCG receives feedback through a variety of routes, including:
• Compliments, comments, concerns and complaints: The CCG formally captures all comments and complaints through a dedicated resource within the Corporate Affairs Directorate (TBC).

12
• Structured stakeholder engagement: When the CCG undertakes any and all engagement activities, it is with the expectation that we will receive various levels of detailed response from the people and stakeholders that we involve.
• Feedback from Healthwatch: The CCG works closely with Healthwatch
Bedford Borough, Healthwatch Central Bedfordshire, Healthwatch Milton Keynes and Healthwatch Luton to liaise regarding individual concerns and feedback, collaborate on joint engagement activities, and trend and stakeholder analysis.
• Annual stakeholder involvement assessment: The CCG’s engagement
processes are assessed annually as part of NHS England Improvement Assessment Framework. The CCG also monitors wider stakeholder feedback mechanisms, such as the national Patient Survey and local CQC assessments.
• Relationships with local Councillors, Members of Parliament and local
authority Health Overview and Scrutiny Committees and Joint Health Overview and Scrutiny Committee (HOSC/HASSC/JHOSC): The CCG proactively works with ward councillors and councillors involved in local Health Overview and Scrutiny Committees covering Bedford Borough, Central Bedfordshire, Luton and Milton Keynes, as well as responding to inquiries and correspondence from local elected members (Elected Mayor, councillors and MPs) on behalf of their constituents.
In addition to responding to feedback through structured mechanisms, the CCG also looks to feedback to patients and public following all engagement activity, to let them know how their involvement has influenced, changed or made a difference to the delivery of local healthcare services. Known as ‘you said, we did’, this information is published on the website, fed back through the minutes of the Public and Patient Engagement Joint Committee and referenced in the Governing Body, described through patient stories and shared with elected members. It is also published in the engagement plans and feedback documents published at the end of all engagement activity. The CCG is committed to responding to and including as many local views as possible. In some instances however, when it is not possible to incorporate feedback for examples when the CCG is implementing national policy, a rationale will be provided.

13
3.0 Communicating with local patients and communities 3.1 Introduction Good communications is crucial to our work. It helps residents to make good informed choices, take control of their health and it fosters trust between the CCG, partners and local communities. We believe in transparency with patients, GP Member practices, elected members and the public. Good communication involves:
- Establishing two way communications; - Informing and empowering stakeholders; - Being honest and transparent in our communications; - Recognising the needs of different groups and individuals; - Collaborating with partner agencies to co-ordinate communications and
strengthen local messaging. 3.2 Digital media For some time, Government Communications has encouraged a ‘digital by default’ ethos, to migrate communications over the digital platforms to ensure greater reach and value for money. The Covid19 pandemic fast tracked technological innovation and behaviour change, mobilising more residents and community groups to engage on line. This provides enormous potential for us to harness digital platforms and engage more in the digital space. The CCG has set up a new website, which has greater digital capability than the websites previously run by our legacy organisations. Social media platforms including Facebook, Twitter, Instagram and SnapChat have been established to communicate with the local population and stakeholders and to secure real time engagement, discussion and feedback across a range of issues. ‘Free to air’ channels including Twitter and Facebook profiles for our Executives and GPs have been established to increase accessibility, build the reputation of senior leaders and support engagement. You Tube is also being used as a repository for informative video content. A social media policy is being developed to set out how social media can be used to contribute to the work of the CCG, and provide guidelines for CCG who are engaging on a professional basis. 3.3 Media Relations Traditional media relations is important, as many local stations and print / digital media are considered to be credible and a good source of news. In Bedfordshire, Luton and Milton Keynes, traditional media is not as prevalent as it once was, with many regional titles folding or moving into online news forums.

14
However, given the levels of poverty and older demographic in the area, traditional media is an important vehicle to communicate key messages, as some people to not have access to digital platforms. As a result, we take steps to engage with journalists and broadcasters from Inspire FM, BBC stations, the Bedford Independent, Luton Herald and Post and MK Citizen continue, so that we can ensure we are reaching out to the non-digital demographic, as well as those who prefer social media to access their local news. The stations and publications identified have good standing locally and continues to be a credible source for many residents. 3.4 External Communications Good external communications is essential in positioning the organisation as an influential system leader. It is also important to ensure that we demonstrate complete transparency and foster a culture of openness and honesty with key stakeholders. Bedfordshire, Luton and Milton Keynes has a diverse population, which requires the CCG to employ communications that are inclusive. There are also significant health inequalities within our boundaries and areas of poverty and depravation, which means that a range of communications tools will need to be used to ensure we reach all areas of our population. A number of channels are used to ensure we engage with audiences who prefer more traditional methods of communication including:
- Street architecture i.e. lampposts, adshels/billboards, street signage, ad vans - Leaflet drops - Parish council newsletters - Newspaper advertising and wraparounds - Council vehicles i.e. recycling vehicles
In addition to the different channels, easy read versions of documents is required to engage with seldom heard communities and communications in other languages including BSL and international languages should be used to engage effectively with different audiences. 3.5 Internal communications Internal communications is essential to delivering a motivated and empowered workforce who act as advocates for the organisation. It is also an essential component of our communications and engagement strategy, as the vehicle for communicating with our GP Membership. The success of the organisation relies on having a dynamic and engaged membership and workforce that projects a strong and trusted voice. Through internal engagement, we will ensure that we:
• Share our strategic vision with colleagues, GP members and practices; • Create an honest and hardworking environment where staff and members can
be heard, listened to and valued; • Foster an organisation where decisions can be made quickly to empower
staff; • Establish systems and procedures to ensure information is easily accessible;

15
For internal communications to deliver, it is essential that HR and OD are closely aligned to ensure organisational cohesion and enable the delivery of our vision and values. 3.6 Crisis communications Planning is central to retaining the reputation of the organisation in times of crisis. Working with the CCG’s Emergency Planning and Preparedness team and engaging on a regular basis with resilience forums in Thames Valley (TVLRF) and Bedfordshire and Luton (BLRF) to prepare for crises and create joint media handling plans and protocols mitigates risk and enables greater control to ensure effective communications management. The Covid Pandemic has provided an opportunity to learn and improve our approach to crisis management. A lessons learned exercise is currently in development, which will support the approach to managing crises in the future. 4.0 Budget and resources 4.1 Resources The effective implementation of this strategy will require financial resources. This will cover the cost of hosting and maintaining the website, graphic design, hosting meetings and other associated activities. 4.2 NHS Bedfordshire, Luton and Milton Keynes staff The CCG’s Communication and Engagement directorate is led by the Director of Communications and Engagement, which is a separate function reporting into the Accountable Officer. The team will manage all associated responsibilities. 5.0 Review This strategy will be reviewed on an annual basis to ensure it is up to date. This strategy will be published in April 2021, with the review being undertaken in March/April 2022 to ensure it continues to meet the needs of the CCG and local communities. The CCG will work with patients and stakeholders to co-design and update the strategy, to ensure we are continuing to engage effectively with local audiences. 6.0 Conclusion This Communications and Engagement Strategy describes the on-going commitment of NHS Bedfordshire, Luton and Milton Keynes CCG to actively engage and involve its local patients, and communities in the design of local health and care services.

16
We will use a range of techniques to ensure that the engagement is meaningful and we will demonstrate how this has positively influenced our commissioning decisions. This information will be published on our website to aid and encourage participation and engagement. 6.1 Next steps This draft communications and engagement strategy will be shared and socialised with partners to secure their input and incorporate their feedback prior to the development of the final strategy in December 2020.
• The Patient and Public Engagement Joint Committee • Healthwatch • Overview and Scrutiny Committees

Author: Jackie Bowry, Christina Gleeson and Sanhita Chakrabarti
Contact Information: Jackie Bowry
Lead Executive: Jane Meggitt
Which CCGs does this agenda item apply to?
Bedfordshire
Luton Milton Keynes
Which activity does this agenda item relate to?
- Assure the delivery of equality and health inequality duties within engagement and consultation plans
- Co-produce and approve stakeholder engagement and consultation plans and assure the delivery of the plan.
How?
What is the Committee/ being asked to do?
To review the communications activity to date and inform further communications as the program continues to roll out
What are the financial implications?
N/A
Set out the key risks and risk ratings
N/A
Date to which the information this paper is based on was accurate
N/A
At the PPEJC meeting in August 2020, members of the PPEJC approved the communications and engagement plan to support the roll-out of the flu programme in BLMK (See PPEC papers and minutes 18.08.20)
Members of the programme will provide an update on the programme and the progress and impact of the communications to date.
No papers to attach.
Patient and Public Engagement Joint Committee 20 October 2020
Agenda item 8
BLMK Flu Campaign
Information
Summary

Author: N/A
Contact Information: Via Anona Hoyle
Lead Executive: Jane Meggitt
Which CCGs does this agenda item apply to?
Bedfordshire Luton Milton Keynes
Which activity does this agenda item relate to?
Please see summary below
How?
What is the Committee/ being asked to do?
To note the content of the reports and updated papers
What are the financial implications?
N/A
Set out the key risks and risk ratings
N/A
Date to which the information this paper is based on was accurate
12 October 2020
The committee are asked to note the following
1. NHS 111 First – (update attached)From 1st December 2020, NHS111 across BLMK will be able to book a timed arrival forpatients that need an Emergency Department appointment, to ensure patients are seen as
Patient and Public Engagement Joint Committee 20 October 2020
Agenda item 9
Updates and reports
Information
Summary

safely and conveniently as possible. Patients will still be able to ‘walk-in’ to Accident and Emergency.
The paper attached provides an update following the presentation and discussion around Communications and Engagement at the PPEJC in August 2020.
2. Report - BLMK One Team public engagement (follow links to view report)In August 2020 the PPEJC approved the proposed approach to undertake a public survey onthe proposal to become one single NHS Clinical Commissioning Group (CCG) in line with NHSEngland’s Long Term Plan (see PPEJC minutes 18.10.20)
Findings from the survey have been collated and a full report and summary report produced.Both reports were emailed to members of the PPEJC and are available to view on the BLMKCCGs website.
The findings from the survey formed part of the final submission to NHS England Improvementin October 2020 in our application to become one CCG by April 2021.

NHS 111 First
Communications and Engagement update for Patient and Public Joint Engagement Committee (PPJEC)
20 October 2020
Background
This winter ensuring patient’s access the right care in the right place is going to be more important than ever with seasonal flu and Covid-19 in co-circulation.
NHS 111 will make it easier and safer for patients to get the right advice or treatment when they urgently need it and increasingly, 111 will be able to book direct appointments/time slots into appropriate services.
From 1st December 2020, NHS111 across BLMK will be able to book a timed arrival for patients that need an Emergency Department appointment, to ensure patients are seen as safely and conveniently as possible. Patients will still be able to ‘walk-in’ to Accident and Emergency.
Update on Communications Plan
In August we shared the Communications and Engagement plan with the PPJEC, since then NHS England has confirmed that across BLMK we will be given a budget to promote NHS111. To ensure we are targeting the budget appropriately we are working with our commissioning colleagues to identify the groups that over present at A&E. Together with general awareness messages across our communities we will then be able to target our communications to these groups to ensure they are aware of the benefits of thinking NHS111 first.
We have developed an overarching schedule of advertising to illustrate where the budget could be spent across BLMK. This will be developed further as we establish the groups and areas we need to target.
NHS England are developing the creative that we will be provided with for the campaign. It is part of a wider campaign that they are developing under the ‘Help Us Help You’ banner. The wider campaign brings together messages on Flu and accessing NHS treatment. The national campaign material for 111 first will be available from 1 December 2020. We do not have artwork that we can share currently however these are some examples of the messages that will form part of the national campaign.
Draft Radio Script (Health Care Professional Voiceover)
“When something happens
And you think you need to go to A&E
Just use 111 first.
If you need it, you’ll get a time slot to be seen safely at your local Emergency Department.
Don’t just turn up.
Just use 111.
Help us help you.”

Draft Poster content
Don’t Just Turn up to A&E
Just use 111 First
So we can see people safely at your Emergency Department we’re now asking you to call ahead for a time to arrive.
If you think you need to see us, call 111 immediately and we’ll send you to the best place for you to get seen safely and quickly.
At the previous PPEJC meeting it was noted that we should consider developing materials in a variety of languages and alternative formats, we will confirm with the national team to understand what languages and formats they will be providing and then work with our local clinicians to develop messages in local community languages that are not covered by the national campaign. It was also noted at the previous meeting that the campaign plan did not include messaging through our GP practices, this has now been added to the plan.
Working with our partners we will start to engage with our local communities from November, this will be to raise awareness of NHS111 and the benefits the service offers currently. Promotion of the 111 first for an arrival time at A&E will not begin before 1 Dec 2020. The engagement in November will inform any specific local messages we develop to accompany the national campaign creative.
Next Steps
Our next steps are to identify the groups we wish to target with messages from 1 Dec 2020 and update the communications plan. Once the plan is developed further we will share it with this group as an off agenda paper.
Working with our commissioning colleagues we are reviewing activity from early adopter areas such as Cornwall and London to understand issues and learnings we can take from their approach to communications approach.

Author: N/A
Contact Information: Via Anona Hoyle
Lead Executive: Jane Meggitt
Which CCGs does this agenda item apply to?
Bedfordshire
Luton Milton Keynes
Which activity does this agenda item relate to?
Please see summary below
How?
What is the Committee/ being asked to do?
To note the content of the reports and updated papers
What are the financial implications?
N/A
Set out the key risks and risk ratings
N/A
Date to which the information this paper is based on was accurate
12 October 2020
Attached are papers and reports for the committee to note
1 BLMK Recovery Plan (refer to action log item 16 on 23/06/20). Paper has been updated to reflect contributions made at PPEJC 23/06/20
2 Glossary of terms and accronyms (refer to action log 14 on 23/06/20) 3 Social media report for period 10 August to 4 October 2020
Patient and Public Engagement Joint Committee 20 October 2020
Agenda item 10
Papers for information
Information
Summary

Aim
• Set the narrative for the NHS ‘new normal’ for BLMK;
• Build on the good will of communities to enhance the reputation of the NHS brand locally;
• Assure communities that the NHS is safe to access and can deliver Covidand non Covid services locally;
• Encourage patients and families, especially those who are living with long term conditions and chronic illnesses to use NHS services;
• Communicate changes to pathways and services;
• Engage with all aspects of our diverse communities in BLMK.
• Assure our staff that it is safe to return to work, and support them to embrace new ways of working – so we deliver our duty of care.
BLMK Recovery Plan - PPEJC 22/10/20
1

Audience Inform
Regulator – NHSE/IGoverning Body/ Boards / FT GovernorsICS Chair Councillors / MPsLeaders of CouncilsNeighbouring CCGs / Providers
Engage
GP membersLocal Authorities ProvidersOverview and Scrutiny Employees Unions Patients
Monitor
Media
Involve and inform
Healthwatch Voluntary groups / charities Patient groups Citizen’s panels Business leaders Faith groups Local communities / Public Children and young people
BLMK Recovery Plan - PPEJC 22/10/20
2
Approach
To form a health communications collaborative from the CCG, Trusts and providers – across the ICS footprint to agree a shared narrative, ensure consistency of message and pool resources around a 5 ‘e’ approach:
• To engage with key stakeholders and the local community to understandperceptions of NHS and service changes that were made underCOVID19, to create an evidence base on which to base the strategy;
• Create opportunities for two way engagement to explain the rationale forchange;
• To encourage support for the changes to services.
• Embed the changes with the local communities to create the ‘newnormal’ for the NHS in BLMK.
• Use experts (clinicians) to spearhead the campaign and position themessage appropriately.
BLMK Recovery Plan - PPEJC 22/10/20
3

Messaging (fluid at this stage)
• Covid19 will be in communities across the UK for some time – until avaccine can be brought to market. Until then, we will need to adapt to a‘new normal’, which will see us making some changes to our services, toensure we can operate effectively and ensure the safety of our staff andpatients;
• During the outbreak, we made some changes to services underemergency measures that have been well received, and which we aim toretain for the next 18 months, pending engagement with the public;
• We are committed to being open and honest with our communities andsharing the rationale for the decisions taken, as we respond in theseunprecedented times.
BLMK Recovery Plan - PPEJC 22/10/20
4

Channels Channels What?System wide perception survey
Survey with communities / patients, GPs, Board, stakeholders and staff to collate an evidence base for the campaign plan, which will allow for greater targeting and messaging for audiences and inform pathway design for commissioners
Health comms cell / warn and inform
Collaboration of health comms and warn and inform partners to synchronise messaging and cascade information
Virtual patient group / Acute and Providers Governors
To support involvement in engagement planning and provide assurance to Governing Body / etc.
Webex Councillors and MPs to explain direction of travel and explain the rationale and secure feedback.
Joint Overview and Scrutiny Committee
A single joint scrutiny committee that has been established across BLMK to ensure we continue to provide an update across the ICS patch and inform them about service changes
BLMK Recovery Plan - PPEJC 22/10/20
5

Channels Channels What?Virtual meetings Regular meeting with GPs to keep them involved
and informed as part of a wider engagement programme.
Patient stories / testimonials Testimonials from patients to demonstrate how the changes are benefitting them.
Videos To show patients what the changes mean and what the benefits are.
Multi language / accessible Given the diverse communities in BLMK and to reach out to those with disabilities, it is important that all communications are accessible and in multi language, BSL, Easy read etc.
Stakeholder newsletters Regular updates sent by email and published to our website to provide a chronology of engagement and development of narrative.
Social media and media Regular updates to keep people up to date with the latest work.
Community/ hospital Radio To ensure all communities are kept up to date
BLMK Recovery Plan - PPEJC 22/10/20
6

Channels Channels What?Website Development of a single website across all three
CCGs and the ICS to provide consistentmessaging
Intranet Development of a single intranet across all three CCGs, with a GP portal to communicate a consistent message to staff and GP Members
System-wide internal communications group
Led by Kate Jarman from MKUH, with support from the CCG to communicate messages across the system to all staff.
BLMK Recovery Plan - PPEJC 22/10/20
7

Additional support
Our approach is to set up a communications hub to provide support to health partners across the system.
To deliver this, we will require some support from NHSE/I. This includes:
• Budgetary support for dynamic video content, video recordingequipment, software editing packages, training, website design / contentwriting
• Timely campaign materials• Toolkits• Pre-approved messaging• Translated / accessible materials• Guidance on public consultation
BLMK Recovery Plan - PPEJC 22/10/20
8

Assurance
• Assurance for this campaign will be sought from:
• NHSE/I• CCG Patient and Public Engagement Forum• Healthwatch• Voluntary sector
BLMK Recovery Plan - PPEJC 22/10/20
9

Glossary of Terms for PPEJC Version 1 - 12.10.20
1 | P a g e
Glossary of NHS Terms and Acronyms BLMK – Bedfordshire, Luton and Milton Keynes
Clinical Commissioning Groups (CCGs) – CCGs are GP led organisations responsible for the planning, designing and purchasing (“commissioning”) of health services for a particular population. In our case, the CCGs are responsible for serving the nearly one million population of Bedfordshire, Luton and Milton Keynes, acting as the key link between NHS England and the point at which the patient receives care. These services include:
• Planned hospital care • Urgent and emergency care • Rehabilitation care • Community health services • Mental health and learning disability services
Governing Body – Our Governing Body is responsible for and oversees the commissioning decisions of the CCG. The group is formed from a mixture of local clinicians (GP members), CCG colleagues and lay members who ensure all commissioning decisions are transparent.
You can find out more about our Governing Body on our website: https://www.blmkccg.nhs.uk/about-us/people-and-governance/our-governing-body/
Integrated Care System (ICS) – an ICS is the alliance between NHS services, local authorities and third sector organisations to have collective responsibility for health and care services for a particular population.
Within BLMK we have one ICS that consists of partners from across the region:
• The three CCGs • Local authorities • NHS Acute trusts • NHS Ambulance trusts • NHS Community and Mental Health
services
The aim of our ICS is to provide system leadership and overall improve population health. It allows involved partners to achieve greater service integration, management of resources, delivery of services and governance arrangements – supporting the delivery of better care to patients.
Our local ICS system is made up of two Integrated Care Partnerships and 23 Primary Care Networks

2 | P a g e
Integrated Care Partnerships (ICPs) – within our ICS we have two ICPs. Similarly to our ICS, ICPs are formed through an alliance of NHS services, local authorities and third partner organisations, however, each ICP looks after a smaller population with a localised view.
In Bedfordshire and Luton, we have the Bedfordshire Care Alliance, made up of local partners including:
• Bedford Borough Council, Central Bedfordshire Council and Luton Council • NHS Bedfordshire Hospitals Foundation Trust • East London Foundation Trust (ELFT) • Cambridge Community Services (CCS) • East of England Ambulance Service
In Milton Keynes we have the Milton Keynes Integrated Care Partnership, made up of local partners including:
• Milton Keynes Council • Milton Keynes University Hospital • Central, North West London NHS Foundation Trust (CNWL) • South Central Ambulance Service (SCAS)
These two ICPs work alongside each other to determine the needs and therefore services of their individual populations and work together to feedback into the ICS and support system leadership.
Primary Care Networks (PCNs) – PCNs act as the foundations for delivering care directly into the community, closer to home with each PCN bringing together GP practices, community services, mental health services and social care to serve populations of between 30,000 and 50,000 people.
They were developed to allow GP practices to work better together, enabling greater provision of proactive, personalised, coordinated and more integrated health and social care, actively benefiting the patient.
Within BLMK we have 23 Primary Care Networks.

Weekly social media round up10.08.2020 – 04.10.2020
Reach• Total number of times the post was shown on someone’s screen
Engagement• Total number of times someone interacted with the post including likes, comments and
shares
Engagement Rate• % of people who interacted with the post from the number it reached
Media views• Number of people who started watching a video (this does not mean it was a full watch)
Terminology

Streamlined channels – updateWork stream: PositioningWhat did we do? To support the Positioning work stream and the One Team Programme we streamlined our Twitter and Facebook accounts to create one account for each platform. By doing this we aim to reflect the joint working across the patch, establish our voice as the single commissioner across BLMK and communicate important health messaging.
Channel Facebook
Likes 587
Followers 649
Total reach 19,503
Total media plays 4,037
Channel Twitter
Followers 4,825
Total reach 43,800
Number of engagements 184
Engagement rate 1.3%
@BLMK_CCGsNHS BLMK Clinical Commissioning Groups
Week commencing 10 August

Focus on asymptomatic spreadersWork stream: Covid19What did we do? From our testing we know that there are members of our community who have been spreading coronavirus without showing any symptoms. As this is very dangerous and could cause the infection rates in local areas to increase we have put more focus on messaging reminding people to social distance and wear a face covering. We have also been targeting younger people with our posts.

Top posts (non-paid for)Channel Post Overview Date Reach Shares Likes
Twitter Re-posting the ‘real-life’ text video targeting and reminding younger
people that they need to follow the rules to protect others.
10.08.20 6,073 6 3
Facebook Reminding residents that the safest way to wear a face covering is to ensure it covers both your nose
and mouth.
11.08.20 12,227 29 63
Instagram Sharing Aisha’s #WhyWeWearOursselfie showing how to safely wear a
face covering.
13.08.20 255 0 24

Reach figures
As of 17/08/20 we had a total reach of over 69,000 people.

What to expect this week?
Positioning:• We will continue to encourage our residents to have their say about the forming of the single CCG across
BLMK via our public survey.
Covid19:• Continuing with the #WhyWeWearOurs campaign with submissions from Bedfordshire Hospital Foundation
Trust.• Work is underway to further target our younger audiences with fresh, new content• Continuing work reminding people of the risk of asymptomatic spreaders and the importance of following
the guidelines
Recovery:• Supporting work done by the National Diabetes Prevention Programme with targeted tweets and
messaging.

Targeting young people – Instagram adsWork stream: Covid19What did we do? To help reduce the transmissions between asymptomatic younger people across BLMK we promoted two of our Instagram posts to remind the younger generation to play their part in slowing the spread of coronavirus. These were our first Instagram ads and were very successful as the figures show below. The ads are active until 27/08/20.
Channel Instagram
Reach 6,737
Likes 591
Shares 15
Channel Instagram
Reach 2,408
Likes 211
Shares 4Week commencing 17 August

Promoting the One Team Survey - adsWork stream: PositioningWhat did we do? We identified the demographics of those who had a low response rate across BLMK (16 – 44 year olds in Luton and Milton Keynes) and used Facebook Ads to target them and encourage them to complete our One Team Programme public survey.
Channel Reach Likes Media Plays Link Clicks
Facebook 14,246 9 8,726 103

Top posts (non-paid for)Channel Post Overview Date Reach Shares Likes
Twitter Re-posting the ‘real-life’ text video targeting and reminding younger
people that they need to follow the rules to protect others.
22.08.20 5,724 10 9
Facebook Reposting Bedfordshire Hospital Trust’s staff face covering pictures
for our #WhyWeWearOurscampaign.
18.08.20 5,126 4 4
Instagram Sharing the first Young Person Q&As “Should I be wearing my
mask when I go out with my friends if we’re social distancing?”
20.08.20 123 1 7
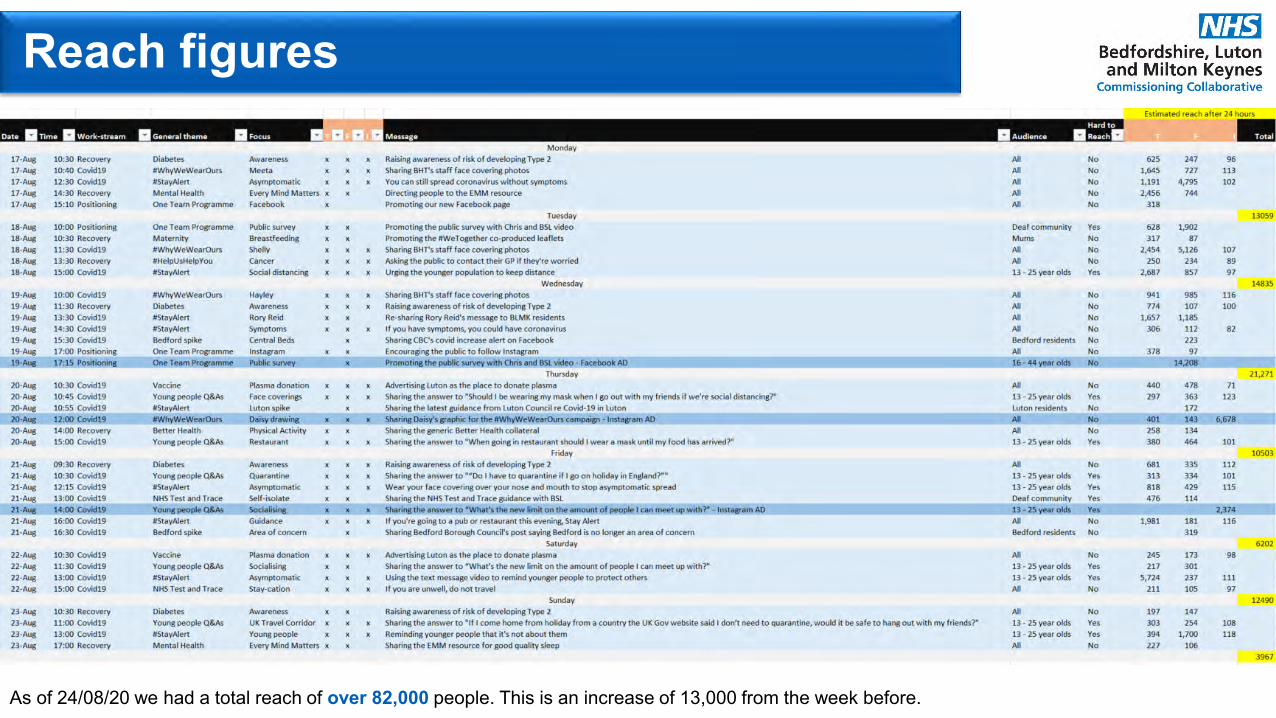
Reach figures
As of 24/08/20 we had a total reach of over 82,000 people. This is an increase of 13,000 from the week before.

What to expect this week?
Positioning:• Reviewing the responses to the public survey following the Facebook Ad to identify if gaps remain and
what we can do to close these.
Covid19:• Using Milton Keynes Rugby Club’s #WhyWeWearOurs photos to continue the face covering campaign
across BLMK.• Identifying what else we can do to target the younger population with our social media using new
concepts / ideas.• Following the lead of the local authorities and supporting any change of local guidance if cases rise or fall.
Recovery:• Focussing on mental health and promoting NHS services available the public.

Targeting young people – Instagram adsWork stream: Covid19What did we do? To help reduce the transmissions between asymptomatic younger people across BLMK we promoted two of our Instagram posts to remind the younger generation to play their part in slowing the spread of coronavirus. These were our first Instagram ads and were very successful as the figures show below.
Channel Instagram
Reach 11,452
Likes 1,185
Shares 15
Channel Instagram
Reach 4,835
Likes 478
Shares 4Week commencing 24 August

Targeting young people – #WhyWeWearOursWork stream: Covid19What did we do? To encourage younger people to wear their face covering when in public or enclosed spaces, and as part of the #WhyWeWearOurs campaign, we have been working with Milton Keynes Rugby Club to create a series of face covering selfies of their younger players.
Reach 16,919
“I wear mine because… to protect my Grandma”
“I wear mine because… to protect my Dad as he has asthma”
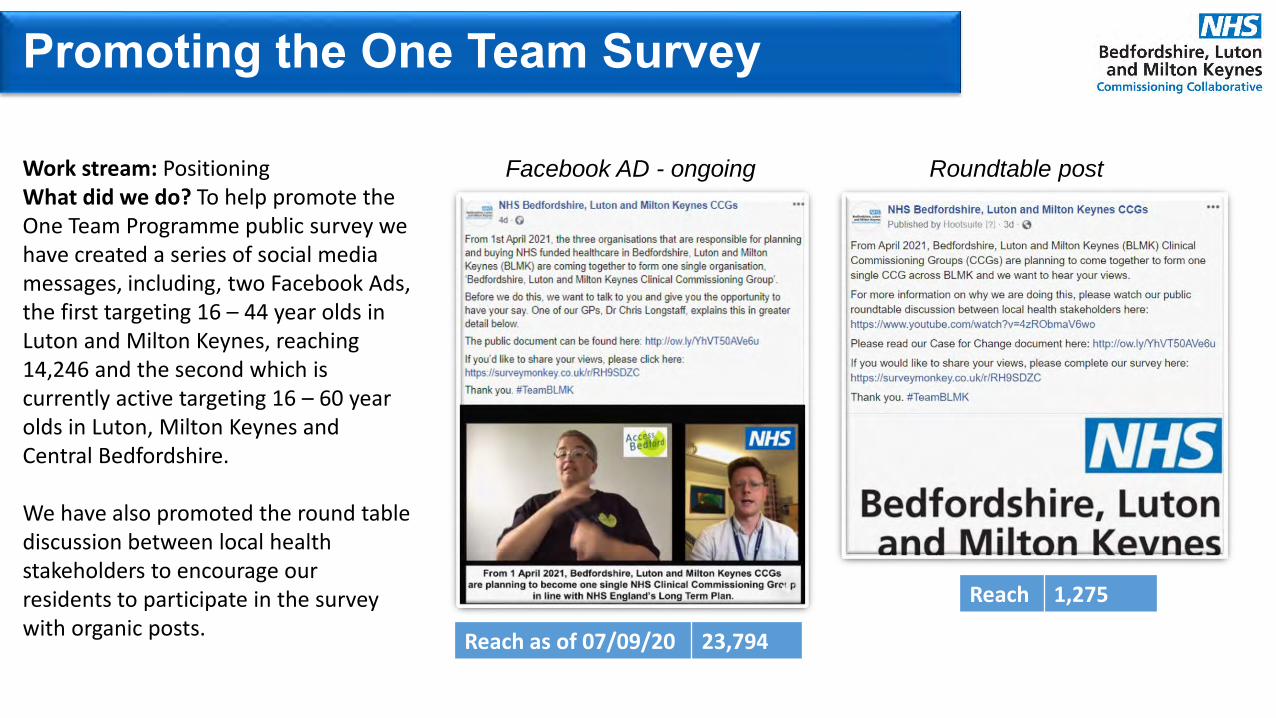
Promoting the One Team Survey
Work stream: PositioningWhat did we do? To help promote the One Team Programme public survey we have created a series of social media messages, including, two Facebook Ads, the first targeting 16 – 44 year olds in Luton and Milton Keynes, reaching 14,246 and the second which is currently active targeting 16 – 60 year olds in Luton, Milton Keynes and Central Bedfordshire.
We have also promoted the round table discussion between local health stakeholders to encourage our residents to participate in the survey with organic posts.
Reach as of 07/09/20 23,794
Facebook AD - ongoing Roundtable post
Reach 1,275
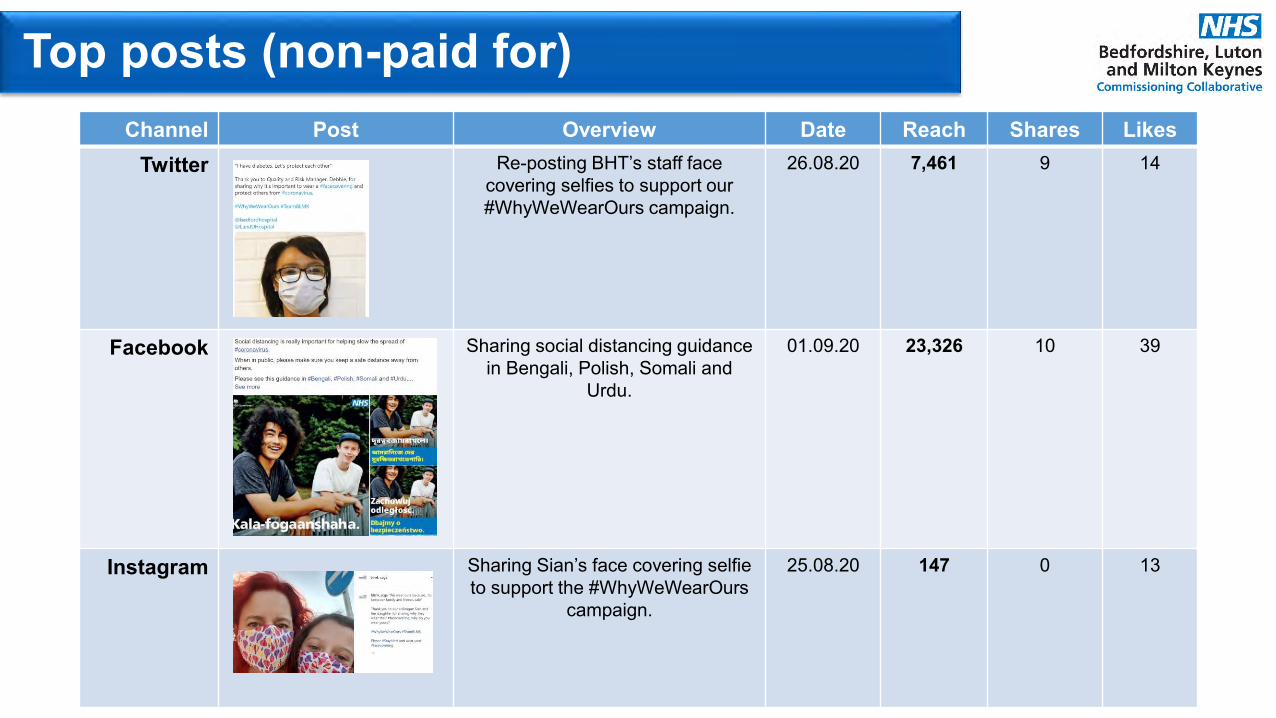
Top posts (non-paid for)Channel Post Overview Date Reach Shares Likes
Twitter Re-posting BHT’s staff face covering selfies to support our #WhyWeWearOurs campaign.
26.08.20 7,461 9 14
Facebook Sharing social distancing guidance in Bengali, Polish, Somali and
Urdu.
01.09.20 23,326 10 39
Instagram Sharing Sian’s face covering selfie to support the #WhyWeWearOurs
campaign.
25.08.20 147 0 13

Reach figures – 24.08.20 – 30.08.20
As of 07/09/20 we had a total reach of over 79,000 people. This is an decrease of 3,000 from the week before.

Reach figures – 31.08.20 – 06.08.20
As of 07/09/20 we had a total reach of over 99,000 people. This is an increase of 20,000 from the week before.

What to expect this week?
Positioning:• Continuing to review the responses to the One Team public survey to understand if gaps remain and
further targeted messaging needs to be created.• Working to create myth-busting Q&A graphics for the One Team Programme.
Covid19:• Continuing to share #StayAlert graphics and messaging with focus on asymptomatic spreading within the
younger population.
Recovery:• It’s World Suicide Prevention Day on Thursday 10 September and we will be supporting the Councils by
sharing their campaign on social media.• The Every Mind Matters resource specifically for kids will be released on Tuesday 8 September and
shared across our channels.• New collateral for #HelpUsHelpYou and how to access GP practices are now being shared across our
channels.

Promoting the One Team Survey
Reach 26,033
Work stream: PositioningWhat did we do? To help promote the One Team Programme public survey we worked with our GPs to create a series of social media video messages encouraging residents to complete the survey. We shared these as Facebook ADs.
Reach 3,745Rejected
Reach 29,476
Week commencing 7 September

Top posts (non-paid for)Channel Post Overview Date Reach Shares Likes
Twitter Posting the first of a series reminding the public not to call
NHS 111 to book a test and to use the online portal or 119 instead.
15.09.20 3,769 7 4
Facebook Urging people to not ring NHS 111 for coronavirus testing and to only use it for urgent medical advice.
01.09.20 13,419 81 1
Instagram Sharing the Every Mind Matters for kids resource.
20.08.20 241 0 0

Reach figures – 07.09.20 – 13.09.20
As of 21/09/20 we had a total reach of over 124,000 people. This is an increase of 25,000 from the week before.

Reach figures – 14.09.20 – 20.09.20
As of 07/09/20 we had a total reach of over 73,000 people. This is a decrease of 51,000 from the week before.

What to expect this week?
Positioning:• Continuing with the AGM Facebook AD inviting the public to join the first virtual AGM• Working to create myth-busting Q&A graphics for the One Team Programme
Covid19:• Sharing the updated guidance about the ‘rule of six’ and #HandsFaceSpace• Following government guidelines to ensure most up-to-date messaging is shared• Working with David from Phew to create BLMK-specific animation for ‘rule of six’• Working with Dr Anne Ingram to create a clinically-led video reminding parents what to do if their child
gets symptoms• Refocussing messaging to target younger generation and working age and remind them how to stay
safe
Recovery:• Reminding the public when the appropriate time is to access services including NHS 111 and GP services
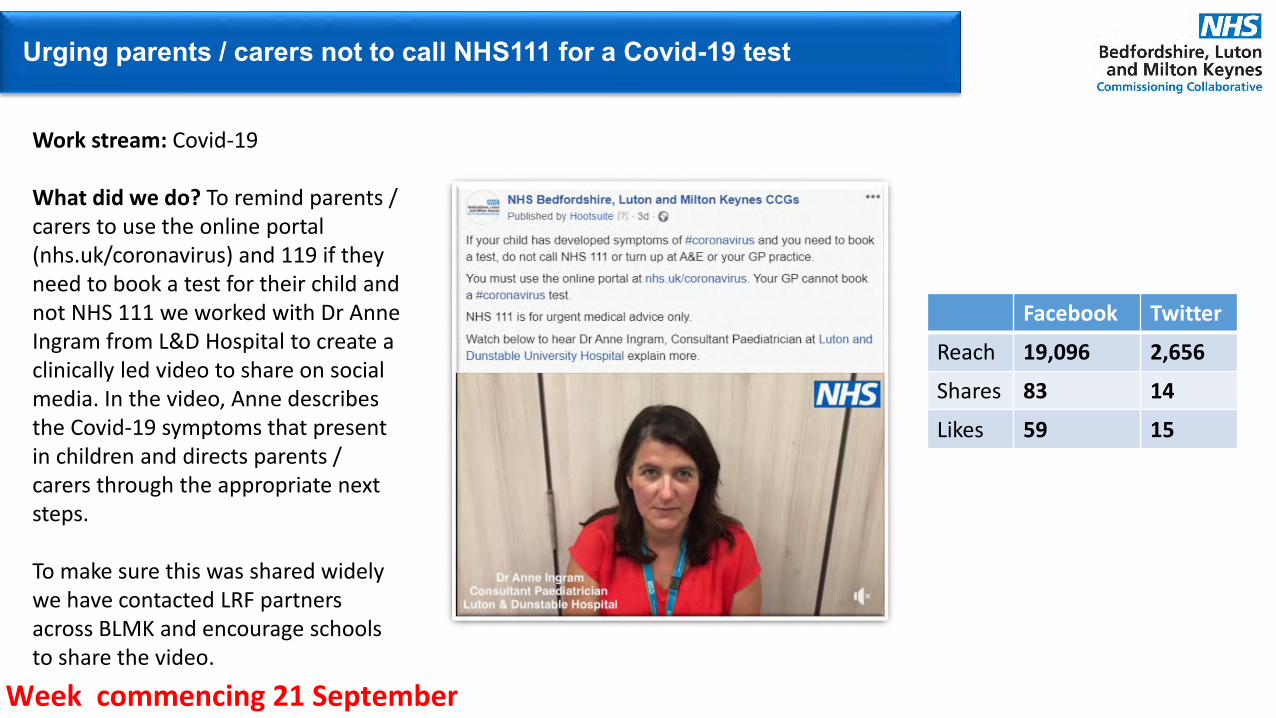
Urging parents / carers not to call NHS111 for a Covid-19 test
Work stream: Covid-19
What did we do? To remind parents / carers to use the online portal (nhs.uk/coronavirus) and 119 if they need to book a test for their child and not NHS 111 we worked with Dr Anne Ingram from L&D Hospital to create a clinically led video to share on social media. In the video, Anne describes the Covid-19 symptoms that present in children and directs parents / carers through the appropriate next steps.
To make sure this was shared widely we have contacted LRF partners across BLMK and encourage schools to share the video.
Facebook Twitter
Reach 19,096 2,656
Shares 83 14
Likes 59 15
Week commencing 21 September

Top posts (non-paid for)Channel Post Overview Date Reach Shares Likes
Twitter Reminding residents to follow the ‘Hands, Face, Space’ rule when
they’re in public.
22.09.20 4,502 7 6
Facebook Reminding residents to follow the ‘Hands, Face, Space’ rule to help
protect each other from coronavirus.
25.09.20 4,235 4 10
Instagram Sharing the first graphic from this year’s flu campaign with the
emphasis on there is no ‘just’ in Flu.
24.09.20 72 0 2

Reach figures – 07.09.20 – 13.09.20
As of 28/09/20 we had a total reach of over 57,000 people. This is a decrease of 16,000 from the week before.
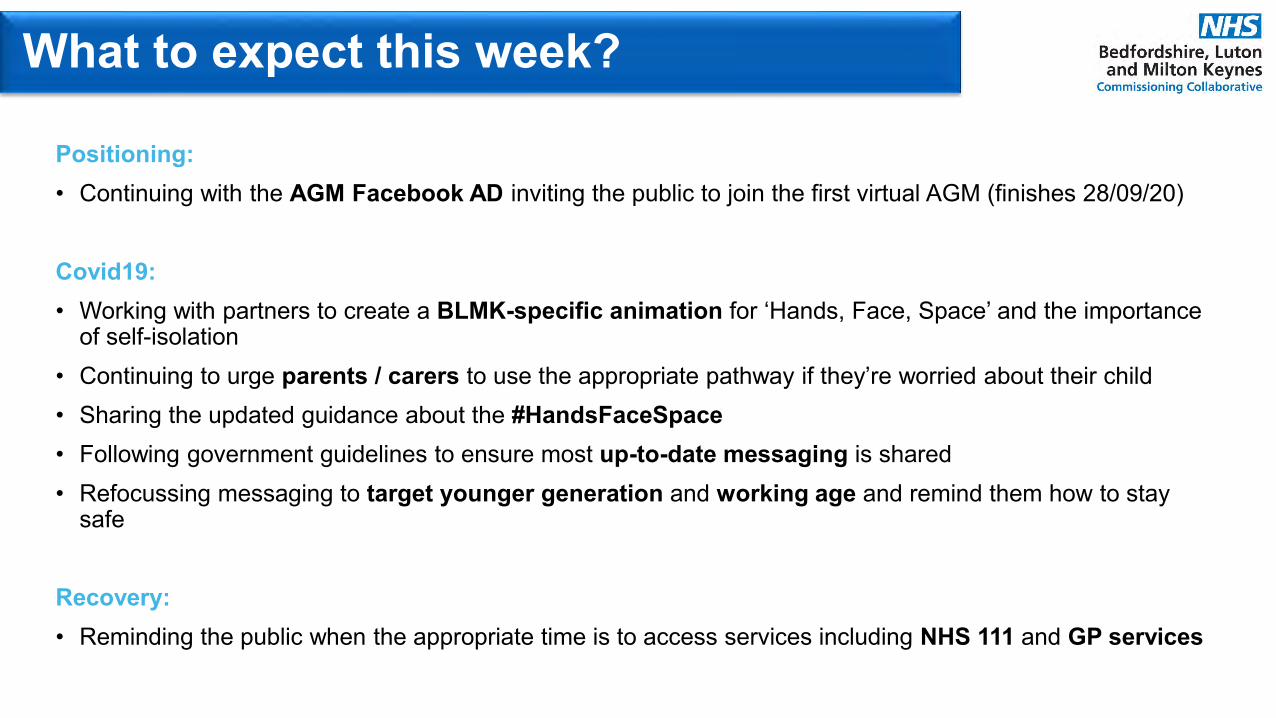
What to expect this week?
Positioning:• Continuing with the AGM Facebook AD inviting the public to join the first virtual AGM (finishes 28/09/20)
Covid19:• Working with partners to create a BLMK-specific animation for ‘Hands, Face, Space’ and the importance
of self-isolation• Continuing to urge parents / carers to use the appropriate pathway if they’re worried about their child• Sharing the updated guidance about the #HandsFaceSpace• Following government guidelines to ensure most up-to-date messaging is shared• Refocussing messaging to target younger generation and working age and remind them how to stay
safe
Recovery:• Reminding the public when the appropriate time is to access services including NHS 111 and GP services

Reminding residents to play their part and slow the spread of Covid-19
Work stream: Covid-19What did we do? We worked with Bedford Borough Council to create a series of three clinically-led videos urging residents to play their part and slow infection rate of Covid-19 in the area. As well as releasing the script in English, two of the videos were in Gujarati and Lithuanian, helping us target our seldom heard groups.
Facebook Twitter
Reach 48,735 10,935
Shares 42 21Week commencing 28 September

Top posts (non-paid for)Channel Post Overview Date Reach Shares Likes
Twitter Urging residents to self-isolate if they are alerted by NHS Test and
Trace.
28.09.20 3,877 3 4
Facebook Urging residents to use NHS 111 for urgent medical advice only and
not as a service for booking coronavirus tests.
28.09.20 4,053 3 1
Instagram Sharing the Every Mind Matters resource for children’s mental
health.
03.10.20 183 0 2
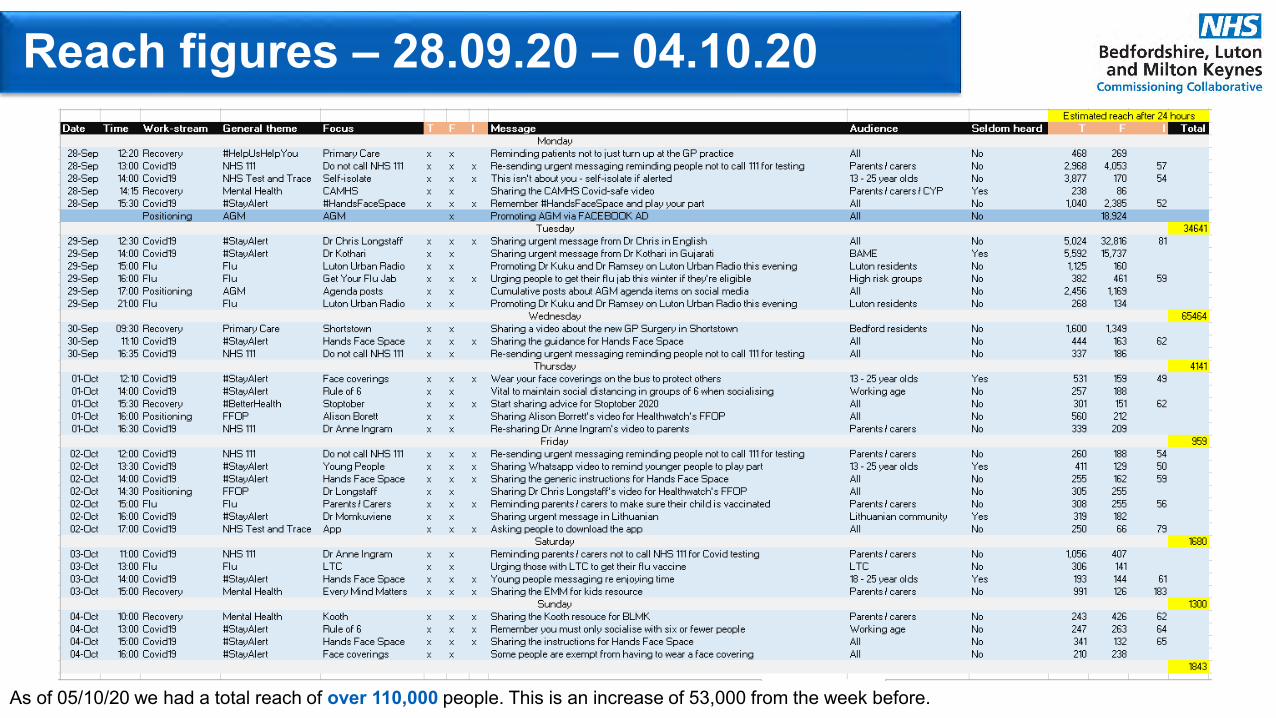
Reach figures – 28.09.20 – 04.10.20
As of 05/10/20 we had a total reach of over 110,000 people. This is an increase of 53,000 from the week before.

What to expect this week?
Positioning:• Sharing Dr Nicola Smith’s video following from the Governing Bodies in Common meeting
Covid19:• Working with partners to create a BLMK-specific animation for ‘Hands, Face, Space’ and the importance
of self-isolation• Continuing to urge parents / carers to use the appropriate pathway if they’re worried about their child• Re-sharing messaging about testing after confirmation of testing situation across BLMK
Recovery:• Focus on children’s mental health following reports from hospitals that they are seeing a spike in CYP
mental health cases• Re-iterating the message that GP services are open for face-to-face but patients must follow guidance