
PathogenesisofPulmonaryTuberculosis
55
Pathogenesis of Pathogenesis of Pulmonary Pulmonary Tuberculosis Tuberculosis Original Speaker : Dr M S Original Speaker : Dr M S Thakkar Thakkar Dr J B Lengkong, Sp.A Dr J B Lengkong, Sp.A
-
Upload
muhamad-fathi -
Category
Documents
-
view
38 -
download
0
description
tbc
Transcript of PathogenesisofPulmonaryTuberculosis

Pathogenesis of Pathogenesis of Pulmonary Pulmonary
TuberculosisTuberculosis
Original Speaker : Dr M S Original Speaker : Dr M S ThakkarThakkar
Dr J B Lengkong, Sp.ADr J B Lengkong, Sp.A

Latar Belakang Sudah sekitar 125 tahun lalu Robert Koch menemukan
basil TB namun dunia masih tetap harus berjuang keras untuk mengendalikan penyakit, yang dengan mudah dapat disembuhkan, namun dapat mematikan.
Di India diperkirakan dua dari setiap lima orang terinfeksi dengan basil TB, diduga kuat 10% diantaranya akan mengalami TB sepanjang hidupnya.
Dari 1,8 juta kasus TB baru yg terjadi setiap tahunnya, sekitar 0,8 juta memiliki TB paru sputum positif.
Dahak seorang pasien BTA-positif dapat menulari 10 – 15 orang per tahun jika tidak diobati. Pasien yang tidak berobat tuntas dapat mengalami resistensi-obat dan besar kemungkinann mengahasilkan bentuk2 TB yang tidak dapat diobati.
(WHO Report 2007: Global Tuberculosis Control Surveillance, Planning and Financing)

Distribusi Tuberkulosis di Dunia

U.S. Distribution of Tuberculosis

Latar Belakang
Paru-paru adalah lokasi predominan utama infeksi tuberkulosis postnatal.
Mycobacterium tuberculosis (MTb) adalah patogen yang paling sering
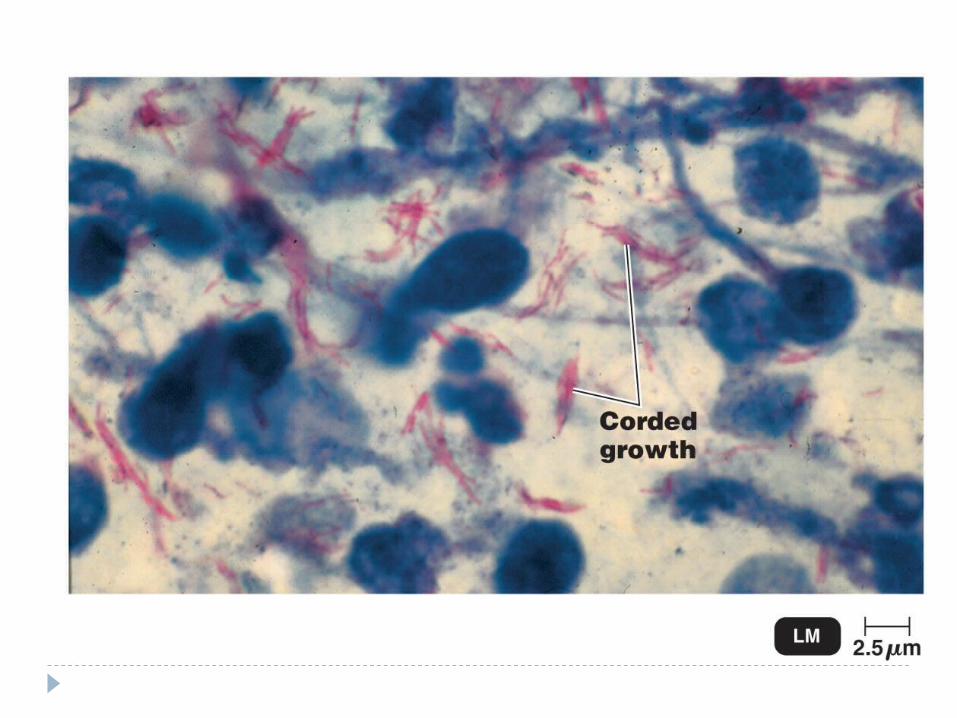
MTb adalah bakteri batang tahan asam, aerobik, penghasil katalase, non-motil dan perlu media khusus untuk biakan.

Penularan MTb ditularkan dari orang ke orang lewat
udara (airbone-route). Infeksi terjadi setelah seseorang yang
mulanya tidak infeksius menghirup droplet yang mengandung MTb, yang biasanya dibatukkan oleh seseorang penderita TB-paru.
Seperti air menguap, partikel2 residu, yang dikenal sebagai droplet-nuklei tetap melayang di udara.

Penularan Ketika terhirup, partikel-partikel yang
karena kecilnya (berukuran 1-5μm ) dapat melewati pertahanan pernapasan atas dan menetap di alveoli paru-paru, menyebabkan infeksi pada orang yang rentan.
Prosedur medis dengan aerosol sekresi pernafasan seperti induksi dahak dan bronkoskopi, irigasi luka dan pemeriksaan otopsi, mengandung risiko yang signifikan dalam transmisi MTb, jika tidak diambil tindakan pencegahan

Imunopatologi TB Paru primer
Robert Koch (1845-1910) orang pertama yg mengemukakan bahwa sistem kekebalan berperan penting dalam TB.
Reaksi imunologis tubuh terhadap infeksi TB berupa :i. Cell mediated immunity (Imunitas yg
diperantarai sel)ii. Delayed type hypersensitivity
(Hipersensitivitas tipe lambat) Penyakit TB adalah hasil dari interaksi antara basil
TB dan gen tubuh yang mengatur respon imun.

Immune Response and Pathogenesis
Percobaan TB pada kelinci, yg diprakarsai oleh Max B Lurie and Dannenberg, memberikan banyak informasi tentang perubahan immunopatologik yang terjadi setelah infeksi aerosol dengan MTb.
Secara skematis percobaan itu menunjukkan 4 fase.

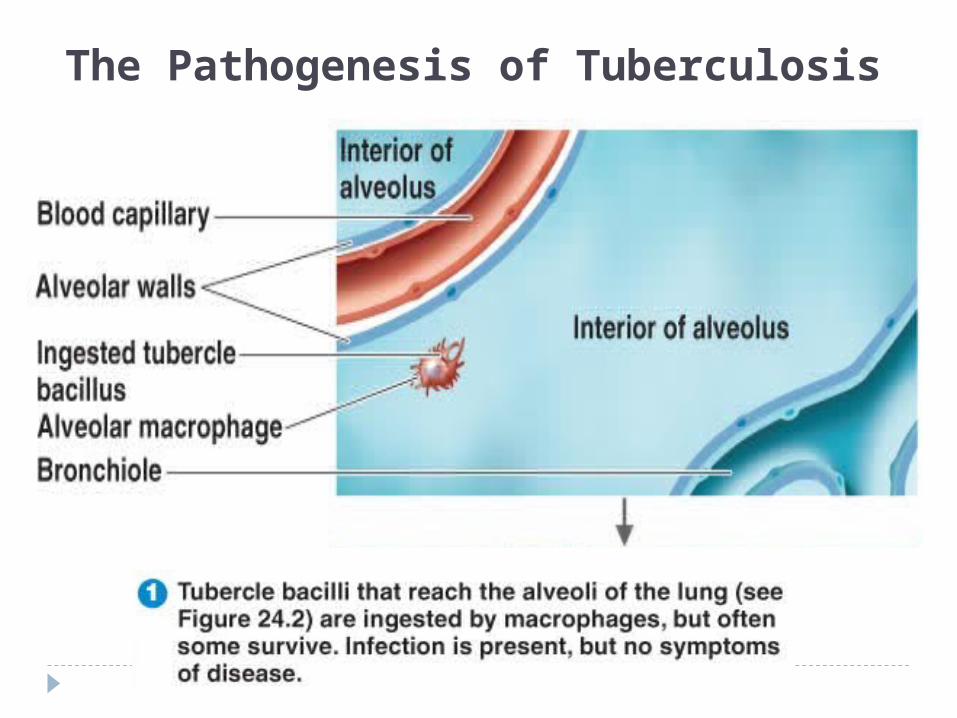
Immunopathogenesis – Phase I Ketika basil TB sampai di alveolus : basil ini ditelan oleh
makrofag alveolar Makrofag alveolar terus-menerus menelan partikel yang
terinhalasi dan hasilnya biasanya ada yg masih dalam keadaan aktif sebagian, tergantung pada sifat alamiah dari partikel dan bagaimana mekanisme material itu ditelan.
Makrofag alveolar menelan MTb melalui reseptor2 tertentu seperti Multipel Complement (CR1, CR3, and CR4), mannose receptor, CD14, immunoglobulin G Fcγ receptor, and scavenger receptors.
Apakah basil yang ditelan makrofag akan hancur atau tetap survive dan bermultiplikasi, tergantung pada virulensi basil dan kemampuan makrofag alveolar itu sendiri.
The Pathogenesis of Tuberculosis

The Pathogenesis of Tuberculosis

The Pathogenesis of Tuberculosis

The Pathogenesis of Tuberculosis

Immunopathogenesis – Phase II Makrofag alveoler gagal menghancurkan atau
menghambat multiplikasi basil yang ditelan dan basil tersebut bermultiplikasi dalam makrofag dan akhirnya makrofag pecah maka muncullah faktor kemotaktik seperti complement c5a dan sitokin seperti monocyte chemotactic factor(mcf-1).
Monosit2 ini bermigrasi ke alveoli dan menelan basil-basil tersebut (monosit ini tidak aktip dan juga tidak memiliki resisten genetik terhadap basil tuberkel).
Basil2 and monosit2 kemudian berkembang secara simbiotik.
Fase ini berlangsung 7 sampai 21 hari.

Phagocytosis
10) Peptide-loaded MHC II expressed on cells surface
1) Adherence
2) Ingestion of the microbe
3) Formation of a phagosome
4) Fusion of the phagosome with the early endosome
5) Fusion of the phagosome with the late endosome 6) Formation of
phagolysosome
7) Digestion of microbe
8) Formation of residual body
9) MHC II molecules enter and loaded with microbial peptide
ER

Phagosome Maturation
• Rabs (GTP binding proteins) control conversion of early to late endosome
• Rab5 on early endosome • Rab7 on late endosome• Rab5 on Mtb phagosomes• Rab7 absent from Mtb
phagosomes• Mtb blocks at the level of Rab
conversion
4) Fusion of the phagosome with the early endosome
5) Fusion of the phagosome with the late endosome
6) Formation of phagolysosome
X

Phagosome Maturation
• Rab5 and Ca+ generate Phosphatidylinositol 3 phosphate (PI3P ) on endosomal membranes
• PI3P is critical for the fusion of early and late endosome
• Two Mtb products interact with PI3P to inhibit maturation
Early endosome
Late endosome
P
Ca+
Ca+
Ca+
Ca+
Ca+
PP
PP
P

Mtb Products: Cause block
• Liparabinomannan (LAM) prevents generation of PI3P– Inhibits Ca+ flux– Prevents
phosphorylation of PI into PI3P
• SapM (PI3P phoshatase) removes PI3P
• Protein kinase G unknown mechanism
Early endosome
Late endosome
P PP
PP
LAM SapM
X

Immunopathogenesis – Phase III Persons who enter phase III develop sufficient
immunity to control TB for lifetime. This phase is characterised by development of
cell-mediated immunity (CMI) and delayed-type hypersensitivity (DTH) which inhibit multiplication of bacilli.
It begins around 2-3 weeks following inhalation.

Granuloma formation Following ingestion of MTb by the alveolar
macrophages and the initial replication within this cell, the resulting bacilli are taken up by the newly arriving macrophages derived from blood monocytes.
By 2 weeks post-infection, infected macrophages at the center of the lesion have acquired an epithelioid morphology.
Sebagai sel-sel mati, merupakan bahan baku untuk proses caseation nekrosis.

Granuloma formation The periphery of the lesion consists largely of
activated macrophages and neutrophils. At 4 weeks post-infection, the number of mature
macrophages seen at the periphery of the caseous lesion has increased.
Multinucleated giant cells (Langhans cells) are often seen by this time, formed by the fusion of activated macrophages.
In addition, MTb-specific lymphocytes have appeared and surrounded the lesion, along with plasma cells and fibroblasts. These fibroblasts encase the granuloma, forming so called “hard granuloma” or “hard tubercle”

Granuloma formation Within 2-3 weeks the center of the hard tubercle
undergoes caseation necrosis due to hypersensitivity to the tubercle bacilli and its tuberculin like products and other factors such as cytokines TNF-α, immune complexes, complement and toxic products from bacilli.
Thus hard tubercle is converted to soft tubercle (this phenomenon is coincident with positive skin reaction).
The bacilli can survive in this caseous material for years but their multiplication is inhibited due to low pH(6.5), anoxia and inhibiting fatty acids.

A Positive Tuberculin Skin Test

Granuloma formation Bacterial entry T Lymphocytes. Macrophages. Epitheloid cells. Proliferation. Central Necrosis. Giant cell
formation. Fibrosis.

CMI vs. DTH CMI (cell-mediated immunity) is described as an
immunologic mechanism in which macrophages are activated by antigen-specific T-cells, thereby acquiring an enhanced ability to destroy bacilli they have ingested.
DTH (delayed-type hypersensitivity) , on the other hand, is a separate phenomenon whereby bacille-laden macrophages are themselves destroyed, along with some surrounding tissue, resulting in caseous necrosis.
Both CMI and DTH occur within the environment of the granuloma after the onset of adaptive immunity.

Tuberculous Granulomas
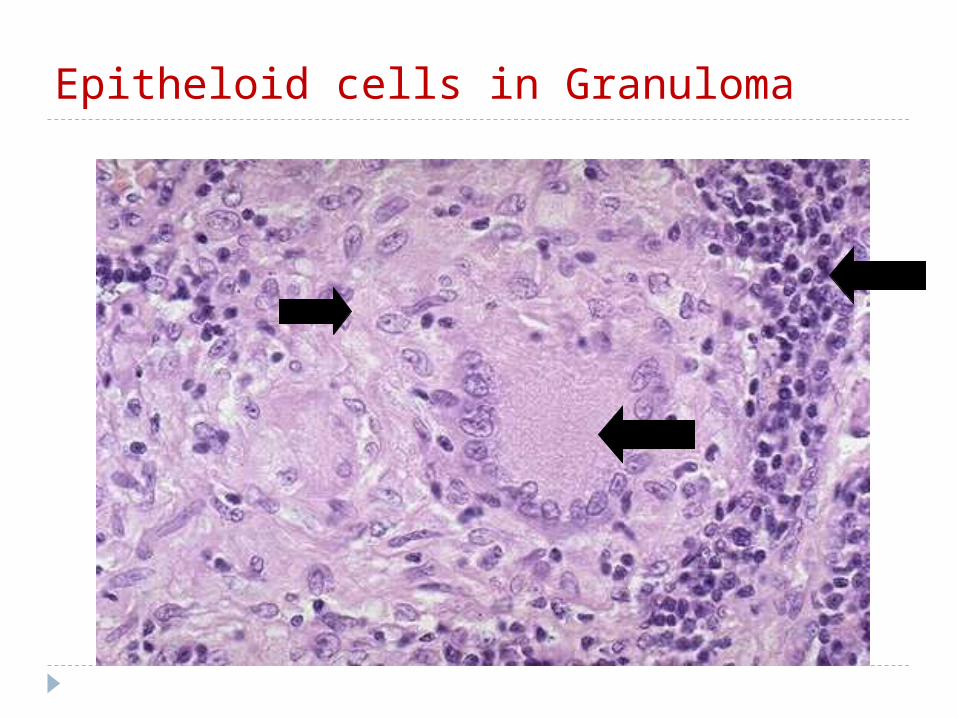
Epitheloid cells in Granuloma

Immunopathogenesis – Phase IV Generally soft granulomas heal by fibrosis or
calcification, but in some cases liquefaction of central caseous material occur and adjacent granulomas coalesce to form cavities.
Caseous material may disseminate through bronchi or lymphatics to other parts of same lung or to the opposite lung causing multiple patchy areas of cheesy consolidation (that may cavitate). This is called progressive primary tuberculosis or disseminated tuberculosis. This particularly common in immunocompromised host.

Immunopathogenesis – Phase IV Sometimes bacilli lying dormant in healed
caseous material are reactivated when host defences are compromised thus giving rise to reactivation or secondary tuberculosis.
Bacilli may erode blood vessel and enter the circulation causing miliary TB.
Rupture of granuloma into bronchus may lead to endobronchial tuberculosis,and rupture into pleural space may cause tuberculous pleurisy.

Mechanism of cavity formation In some immunocompetent hosts, due to the
hydrolytic enzymes and DTH, liquefaction of solid caseous material occurs.
In biochemical terms it means increased tissue acidity whereby inhibitors of certain enzymes systems concerned in tissue autolysis cease to function.
Bacilli multiply but macrophages do not survive in this environment. Free oxygen supply favours the multiplication of the bacilli which are not eliminated.
A cavity may heal by calcification, or by formation of a radiating scar or by the process of open healing.

Fibrosis All sorts of connective tissue may be
formed in tuberculous tissue- procollagen reticulum fibres, collagen fibres, and elastic fibres.
Proliferation of reticulum fibres is typical of tubercles and tuberculous granulation tissue.
Tubercules, especially those that are not caseous, may entirely converted into collagen and more particularly hyaline scars.

Calcification A tuberculous lesion does not calcify unless it is
caseous. Usually the caseous mass that occupies the
alveolar spaces calcifies first and the alveolar septae follow, so that eventually the whole focus calcifies.
The calcium deposits form concentric circles comparable to Liesegang’s rings.
Lesions that become arrested soon after caseation have an especial tendency to calcify.
Foci with thicker capsules have a less tendency to calcify.

Primary Tuberculosis The infection of an individual who has not been
previously infected or immunized is called primary tuberculosis.
When the bacilli enter the lung a small patch of caseous bronchopneumonia develops and later encapsulates. This is called the primary focus.(Ghon’s focus)
Before the primary focus is fully developed a similar lesion appears in one of the regional lymph nodes and so a primary complex is formed.(primary complex of Ranke)
Primary focus in lung is commonly located sub-pleurally in middle portion (upper region of the lower lobe or the lower portion of the middle lobe when on the right side.)

Primary Tuberculosis Pathogenesis – inhalation of bacilli from
droplet nuclei – tissue reaction leading to formation of granuloma. The draining the lymphatics and hilar lymphnodes are involved.
Vasculitis (with edema, transmural infiltration with lymphocytes and plasma cells) is frequently seen. Vascular involvement may lead to bacillaemia at this stage.
Hematogenous spread from primary focus to apex of the affected lung may give rise to focus at the apex.(Simon’s focus)

Primary Tuberculosis The route by which the bacilli are transmitted
from the primary focus to the regional lymph node may be recognized by a chain of small nodules developing in lymphatic adventitial sheath. When these foci heal slight fibrosis of the alveolar septa is found.
Bronchial erosion may arise from pressure by calcified lymph nodes and followed by tracheo-bronchial perforation, traction diverticula of esophagus, bronchiectasis (the middle lobe syndrome) and even superior vena cava obstruction.

Epituberculosis Non caseating and therefore resorbing tuberculous
infiltrations are known as epituberculosis.(found most commonly in connection with primary focus)
Pathology- A perifocal infiltration may be seen when a small
bacillary focus is surrounded by a large area of toxic edema or gelatinous infiltration, attributable to a hypersensitivity response to tuberculo-protein.
Tuberculous pneumonia may occur without tendency to caseation and so may resorb.
Innumerable tuberculoid granulomata with Langhans giant cells but without tubercle bacilli and caseation may be found.

Primary focus- fate Healing – by fibrosis, calcification, or
ossification. Bronchial dissemination. Vascular dissemination. Bacilli may remain dormant in healed caseous
lesions and may reactivate the disease when host defences are compromised.
Tuberculous pleurisy. Enlarged lymph node may compress and
obstruct the bronchi which may lead to collapse.

Post primary Tuberculosis The infection of an individual who has been
previously infected or sensitized is called post primary (secondary) tuberculosis.
It is either generalized (disseminated, hematogenus) i.e. more than one organ is involved or it is limited to lungs (bronchogenic).
The post primary TB may result from:1. Direct progression of primary lesion called as progressive
primary TB2. Reactivation of dormant primary complex3. Exogenous re-infection4. Superinfection 5. Pulmonary lesions of hematogenous or lymphogenous
spread

Hematogenous pulmonary tuberculosis1. Acute hematogenous dissemination
1. Acute miliary tuberculosis2. Meningeal TB3. Septic and non reactive forms
2. Chronic hematogenous dissemination1. Chronic miliary TB of the lungs2. Chronic disseminated focal TB3. Polyserositis4. Abortive apical foci
3. Localised pulmonary diseasei. Local infiltrationsii. Round foci

Hematogenous pulmonary tuberculosis Acute miliary dissemination may be caused by:i. Recrudescence (of a primary lesion) is
accompanied by liquefaction which may lead to erosion of vessels and transmission bacilli in blood stream.
ii. Vascular tuberculous lesion (Weigert’s focus-a caseous focus in the intima, rich in bacilli)
Proliferation of cells seen in typical miliary tubercle requires more time, so miliary foci of short duration(2-4 weeks) have areas of leucocytic pneumonia with necrosis, whereas the typical epitheloid and giant cell tubercles occur only if duration of the disease is more protracted.

Hematogenous pulmonary tuberculosis The origin of bacilli which enter the circulation in
the more chronic forms of dissemination may be the lymph node component of the primary complex, infection being carried by the lymphatic duct and falling upon the pulmonary circulation first.
Bacilli may pass the capillary bed of the lungs to enter the general circulation.
Since the bronchial and pulmonary arteries are end arteries and do not anastamose and since they terminate a few mm below the pleural surface, small doses of bacilli may be held in this area and give a corticopleural distribution of the foci.

Hematogenous pulmonary tuberculosis The round foci in post primary TB are multiple. These foci do not invade the bronchi till late,
hence local symptoms and physical signs are lacking, general toxemia is prominent.
Hematogenous pulmonary tuberculosis has tendency to heal by calcification.
Such calcified or latent foci may contain living bacteria and from these a local relapse is possible.
In long standing foci chronic thick walled cavities develop and canalicular spread in the lungs result.

Bronchogenic pulmonary tuberculosis It has a tendency to restriction to the lungs where
spreads by the natural channels of bronchi as well as directly by continuity.
Pathologically the lesions coalesce together to form larger areas of pneumonia. This area undergoes massive caseation necrosis. The disease in the lungs have a tendency to heal by encapsulation and fibrosis, and calcification is less prominent than in hematogenous forms.
Cavities tend to persist since adhesions to the chest wall become firmer and increase of fibrous tissue in their walls renders them more rigid. Active multiplication of bacilli continues in the caseous lining.
Aspiration of bacilli in other segmental bronchi may cause TB endobronchitis.

Bronchogenic pulmonary tuberculosis The lesion typically involves apical and posterior
segments of the upper lobe. If the lower lobe is involved, the superior segment is the most common site of disease.
(The predilection for the upper lobes is thought to be due to decreased lymph flow in the upper regions of the lung. Historically, an alternative explanation is the presence of higher oxygen tension in that region.)
This may be accompanied by a spread to the midzone of the other lung.(which includes apical branch of the lower lobe and also posterior branch of the upper lobe). They may be due to aspiration during sleep or anesthesia.

Lower lung field tuberculosis The lower lung field is defined as that area on
postero-anterior chest radiograph which extends below an imaginary line traced across the hila and includes the parahilar regions.
The most common pathogenetic mechanism is ulceration of a bronchus by a lymph node affected by tuberculosis with spillage of tuberculous material into the bronchus.
Pathogenetic mechanisms proposed – restricted ventilation and retrograde lymphatic flow from involved hilar lymph nodes.

Endobronchial tuberculosis Endobronchial tuberculosis is defined as
tuberculous infection of the tracheobronchial tree. Pathogenesis- 5 mechanisms are being considered:i. Direct extension from an adjacent parenchymal
infection (cavitary lesion),ii. Implantation of organisms from infected sputum,iii.Hematogenous spread,iv.Erosion of a lymph node into the tracheobronchial
tree, and,v. Spread of infection from parenchyma to
peribronchial region via lymphatics.

Influence of HIV Infection on the Pathogenesis of Tuberculosis HIV is the strongest risk factor known for the
development of TB. In the vast majority of immunocompetent individuals
infected with M. tuberculosis, the bacilli are contained in pulmonary granulomas, leading to LTBI.
Successful containment of TB infection is dependent on the induction of a type 1 adaptive immune response characterized by the production of interferon-gamma (IFN-γ) by CD4 T-cells for activation of macrophages and subsequent destruction of intracellular bacilli.
TB develops either by progression of recently acquired infection or reactivation of latent TB.
The risk of disease following infection with MTb increases dramatically in patients with HIV coinfection.

Primary Complex Primary
tuberculosis is the pattern seen with initial infection with tuberculosis in children.
Reactivation, or secondary tuberculosis, is more typically seen in adults.

Primary Complex

Cavitary Tuberculosis

Cavitary Secondary Tuberculosis

References Tuberculosis – Pagel, Simmonds, Tuberculosis – Pagel, Simmonds,
NassauNassau
Reichman and Hershfield’s Reichman and Hershfield’s Tuberculosis: A Comprehensive, Tuberculosis: A Comprehensive, International Approach - Mario International Approach - Mario RaviglioneRaviglione
Tuberculosis – SK Sharma, A MohanTuberculosis – SK Sharma, A Mohan
Internet (various resources)Internet (various resources)

Thank YouThank You
“I have no business to live this life if I cannot eradicate this horrible scourge from the mankind,”
Robert Koch, delivering a lecture at Berlin University on his discovery of tuberculosis bacilli, 1882.


















