PARATHYROID GLANDS. PARATHYROID GLANDS PARATHYROID GLANDS Derived from the developing pharyngeal...
44
PARATHYROID GLANDS PARATHYROID GLANDS
-
Upload
brice-simmons -
Category
Documents
-
view
233 -
download
4
Transcript of PARATHYROID GLANDS. PARATHYROID GLANDS PARATHYROID GLANDS Derived from the developing pharyngeal...

PARATHYROID GLANDSPARATHYROID GLANDS

PARATHYROID GLANDSPARATHYROID GLANDS
DeDerived from the developing pharyngeal rived from the developing pharyngeal pouches pouches
The four glands normally lie in close The four glands normally lie in close proximity to the upper and lower poles of proximity to the upper and lower poles of each thyroid lobeeach thyroid lobe
10% of individuals have only two or three 10% of individuals have only two or three glands. glands.

IIn the adult, the parathyroid is a yellow-n the adult, the parathyroid is a yellow-brown, ovoid encapsulated nodule weighing brown, ovoid encapsulated nodule weighing approximately 35 to 40 mg. approximately 35 to 40 mg.
Most of the gland is composed of Most of the gland is composed of chief cellschief cells..
TThey contain secretory granules of hey contain secretory granules of parathyroid hormone (PTH)parathyroid hormone (PTH). .
Oxyphil cellsOxyphil cells and transitional oxyphils are and transitional oxyphils are found throughout the normal parathyroid, found throughout the normal parathyroid, either singly or in small clusters. either singly or in small clusters.
TThe amount of stromal fat increases up to he amount of stromal fat increases up to age 25, reaching a maximum of age 25, reaching a maximum of approximately 30% of the glandapproximately 30% of the gland..
The activity of the parathyroid glands is The activity of the parathyroid glands is controlled by the level of free (ionized) controlled by the level of free (ionized) calcium in the bloodstream rather than by calcium in the bloodstream rather than by trophic hormones secreted by the trophic hormones secreted by the hypothalamus and pituitary. hypothalamus and pituitary.
The metabolic functions of PTH in supporting The metabolic functions of PTH in supporting serum calcium levels can be summarized as serum calcium levels can be summarized as follows:follows:
PTH activates osteoclasts, thereby mobilizing PTH activates osteoclasts, thereby mobilizing calcium from bone.calcium from bone.
It increases the renal tubular reabsorption of It increases the renal tubular reabsorption of calcium, thereby conserving free calcium.calcium, thereby conserving free calcium.
It increases the conversion of vitamin D to its It increases the conversion of vitamin D to its active dihydroxy form in the kidneys.active dihydroxy form in the kidneys.
It increases urinary phosphate excretion, It increases urinary phosphate excretion, thereby lowering serum phosphate levels.thereby lowering serum phosphate levels.
It augments gastrointestinal calcium absorption. It augments gastrointestinal calcium absorption.
Hypercalcemia of malignancy is due to Hypercalcemia of malignancy is due to increased bone resorption and subsequent increased bone resorption and subsequent release of calcium. release of calcium.
There are two major mechanisms by There are two major mechanisms by which this can occur:which this can occur:
(1) (1) osteolytic metastases and local release osteolytic metastases and local release of cytokinesof cytokines
(2) (2) release of PTH-related protein release of PTH-related protein (PTHrP)(PTHrP). .
Recently, a critical osteoclastogenic Recently, a critical osteoclastogenic pathway has been discovered that pathway has been discovered that involves the involves the osteoblast cell-surface osteoblast cell-surface receptor receptor RANKRANK (receptor activator of (receptor activator of nuclear factor κB), its ligand, nuclear factor κB), its ligand, RANKLRANKL, and , and a decoy receptor for RANKL, a decoy receptor for RANKL, osteoprotegerinosteoprotegerin.. RANKL is also known as "osteoclast RANKL is also known as "osteoclast differentiation factor," and by binding with differentiation factor," and by binding with the RANK receptor, it promotes all aspects the RANK receptor, it promotes all aspects of osteoclast function, including of osteoclast function, including proliferation, differentiation, fusion, and proliferation, differentiation, fusion, and activation. RANKL is secreted by tumor activation. RANKL is secreted by tumor cells and peritumoral stromal cells in cells and peritumoral stromal cells in metastatic foci and causes osteolysis. metastatic foci and causes osteolysis.
PTH-related protein:PTH-related protein: The most frequent The most frequent cause of hypercalcemia in nonmetastatic cause of hypercalcemia in nonmetastatic solid tumors-particularly squamous cell solid tumors-particularly squamous cell cancers cancers
PTHrP-induced hypercalcemia was known PTHrP-induced hypercalcemia was known as "humoral hypercalcemia of malignancy" as "humoral hypercalcemia of malignancy" to distinguish it from hypercalcemia arising to distinguish it from hypercalcemia arising from osteolytic metastases. from osteolytic metastases.

HyperparathyroidismHyperparathyroidism
PRIMARY HYPERPARATHYROIDISM
Primary hyperparathyroidism is one of the most common Primary hyperparathyroidism is one of the most common endocrine disorders, and it is an important cause of endocrine disorders, and it is an important cause of hypercalcemiahypercalcemia. . The frequency of the various parathyroid lesions underlying The frequency of the various parathyroid lesions underlying the hyperfunction is as follows: the hyperfunction is as follows: Adenoma: 75% to 80%Adenoma: 75% to 80%Primary hyperplasia (diffuse or nodular): 10% to 15%Primary hyperplasia (diffuse or nodular): 10% to 15%Parathyroid carcinoma: less than 5% Parathyroid carcinoma: less than 5%
Primary hyperparathyroidism is Primary hyperparathyroidism is usually a disease of adults and is usually a disease of adults and is more common in women than in men more common in women than in men by a ratio of nearly 3:1.by a ratio of nearly 3:1.
In more than 95% of cases, the In more than 95% of cases, the disorder is caused by sporadic disorder is caused by sporadic parathyroid adenomas or sporadic parathyroid adenomas or sporadic hyperplasiahyperplasia ::
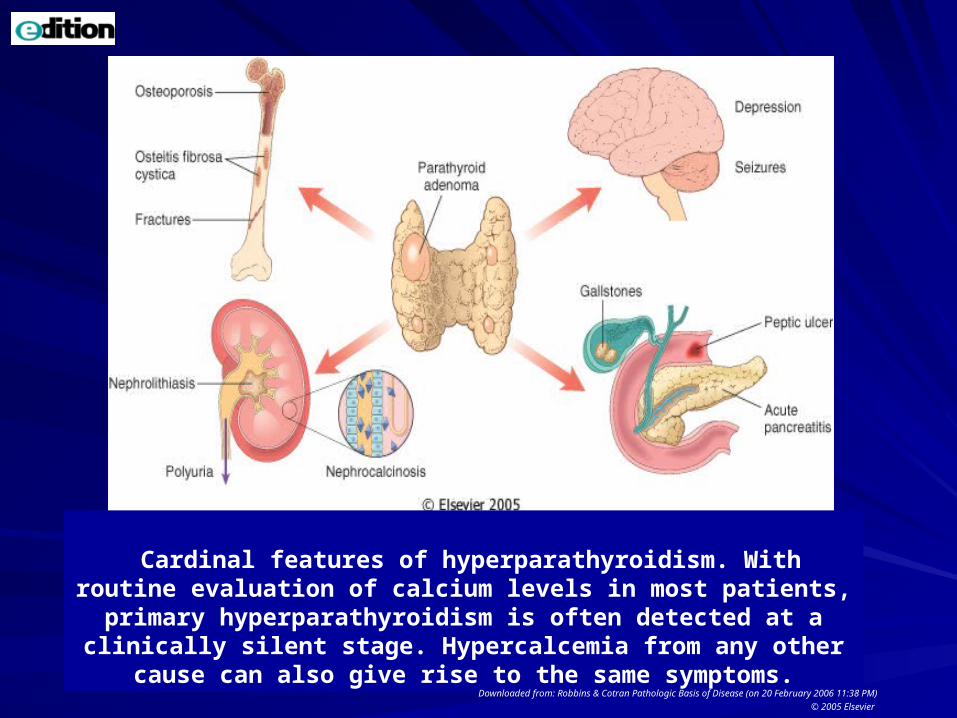
Cardinal features of hyperparathyroidism. With routine evaluation of calcium levels in most patients, primary hyperparathyroidism is often detected at a clinically silent stage. Hypercalcemia from any
other cause can also give rise to the same symptoms.Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 20 February 2006 11:38 PM)
© 2005 Elsevier
The genetic syndromes associated with The genetic syndromes associated with familial primary hyperparathyroidism familial primary hyperparathyroidism include the followinginclude the following::Multiple endocrine neoplasia-1 (MEN-1)Multiple endocrine neoplasia-1 (MEN-1)Multiple endocrine neoplasia-2 (MEN-2)Multiple endocrine neoplasia-2 (MEN-2)Familial hypocalciuric hypercalcemiaFamilial hypocalciuric hypercalcemia (FHH) is an (FHH) is an autosomal-dominant disorder characterized by autosomal-dominant disorder characterized by enhanced parathyroid function due to decreased enhanced parathyroid function due to decreased sensitivity to extracellular calcium. sensitivity to extracellular calcium. Sporadic parathyroid hyperplasia is also Sporadic parathyroid hyperplasia is also monoclonal in many instances, monoclonal in many instances,
MorphologyMorphologyParathyroid adenomasParathyroid adenomas
solitary solitary --similar to the normal parathyroid glands, similar to the normal parathyroid glands, may lie in close proximity to the thyroid gland or may lie in close proximity to the thyroid gland or in an ectopic site (e.g., the mediastinum).in an ectopic site (e.g., the mediastinum).The typical parathyroid adenoma averages 0.5 to The typical parathyroid adenoma averages 0.5 to 5.0 gm; is a well-circumscribed, soft, tan to 5.0 gm; is a well-circumscribed, soft, tan to reddish-brown nodule; and is invested by a reddish-brown nodule; and is invested by a delicate capsule delicate capsule In contrast to primary hyperplasia, the glands In contrast to primary hyperplasia, the glands outside the adenoma are outside the adenoma are usually normal in sizeusually normal in size or somewhat shrunken because of feedback or somewhat shrunken because of feedback inhibition by elevations in serum calcium. inhibition by elevations in serum calcium.
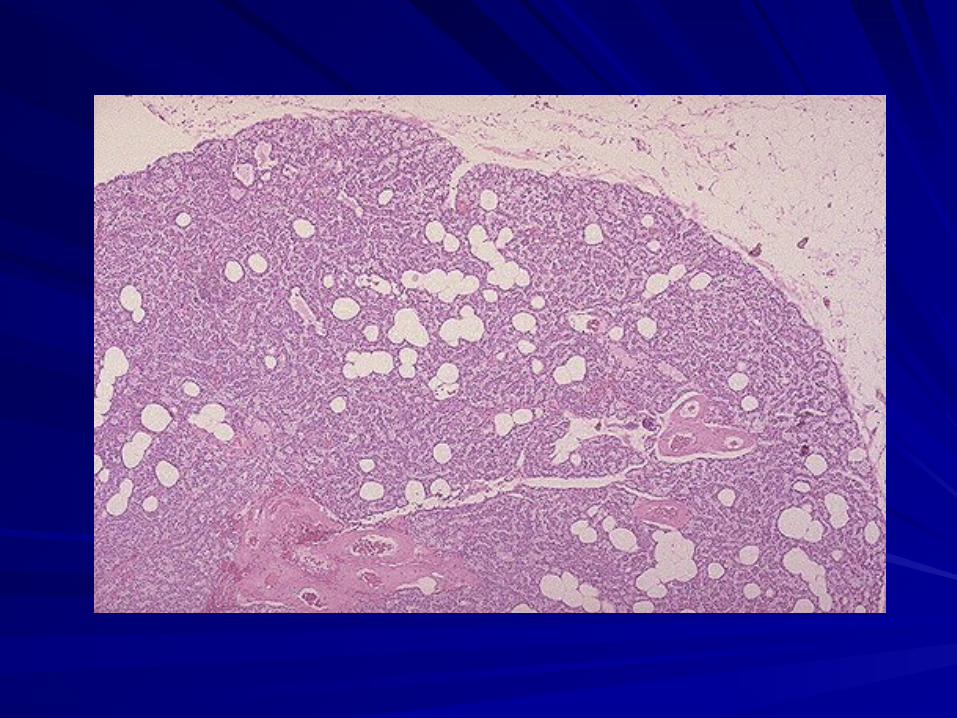
Microscopically, parathyroid adenomas Microscopically, parathyroid adenomas are often composed predominantly of fairly are often composed predominantly of fairly uniform, uniform, polygonal chief cellspolygonal chief cells with small, with small, centrally placed nuclei centrally placed nuclei
Mitotic figures are rare. A rim of Mitotic figures are rare. A rim of compressed, non-neoplastic parathyroid compressed, non-neoplastic parathyroid tissue, generally separated tissue, generally separated by a fibrous by a fibrous capsulecapsule,, is often visible at the edge of the is often visible at the edge of the adenoma. adenoma.
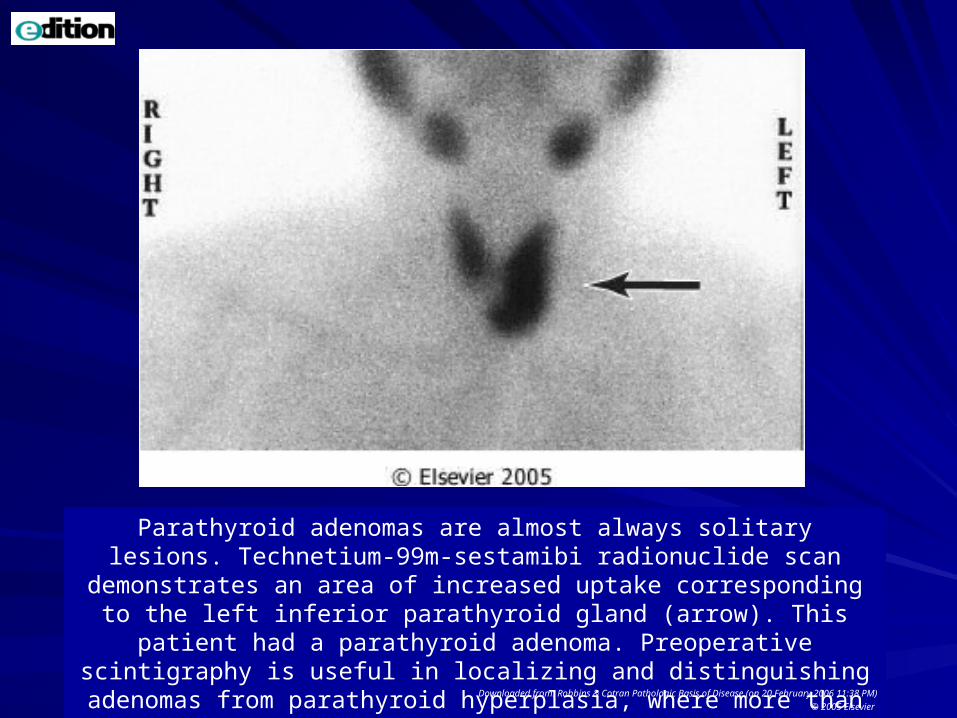
Parathyroid adenomas are almost always solitary lesions. Technetium-99m-sestamibi radionuclide scan demonstrates an area of increased uptake
corresponding to the left inferior parathyroid gland (arrow). This patient had a parathyroid adenoma. Preoperative scintigraphy is useful in localizing and
distinguishing adenomas from parathyroid hyperplasia, where more than one gland would demonstrate increased uptake.Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 20 February 2006 11:38 PM)
© 2005 Elsevier

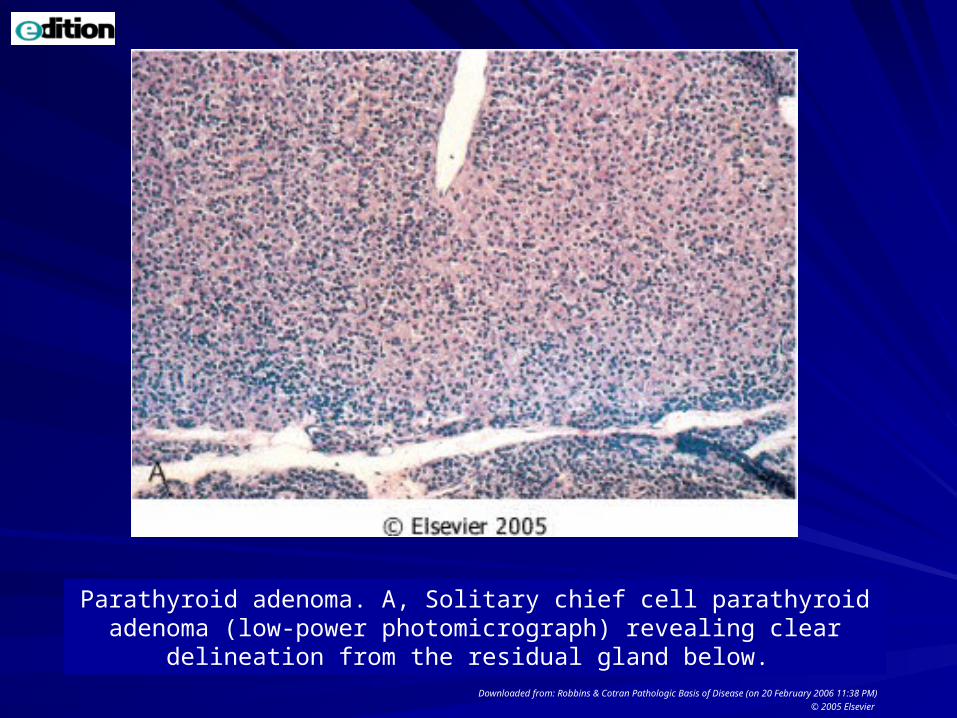
Parathyroid adenoma. A, Solitary chief cell parathyroid adenoma (low-power photomicrograph) revealing clear delineation from the residual gland
below. Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 20 February 2006 11:38 PM)
© 2005 Elsevier
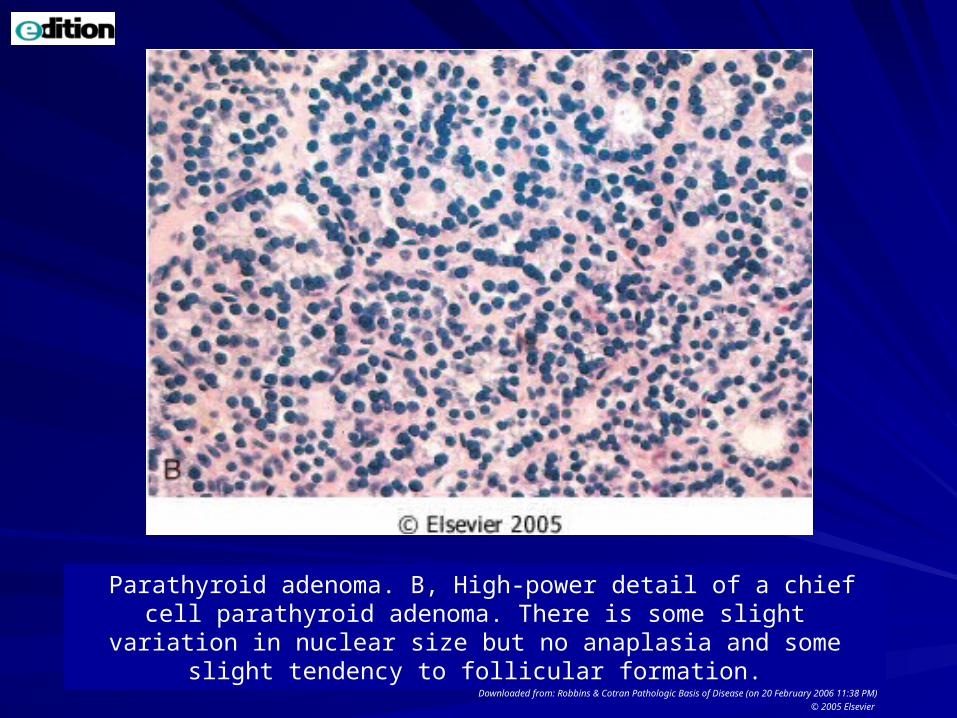
Parathyroid adenoma. B, High-power detail of a chief cell parathyroid adenoma. There is some slight variation in nuclear size but no anaplasia
and some slight tendency to follicular formation.Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 20 February 2006 11:38 PM)
© 2005 Elsevier
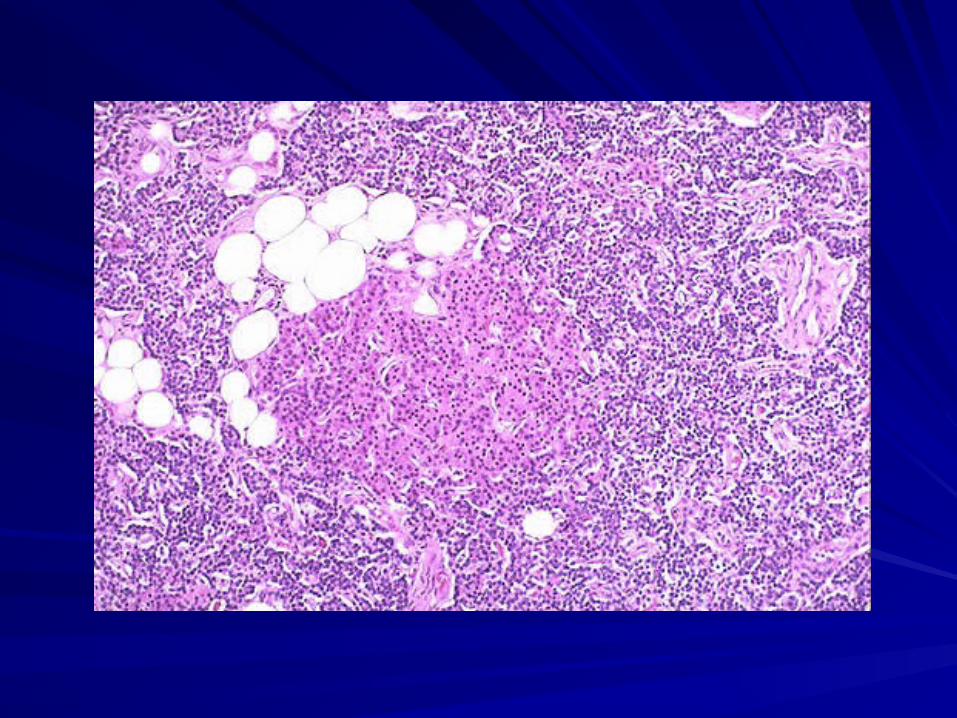
PPrimary hyperplasiarimary hyperplasiaSSporadically or as a component of MEN poradically or as a component of MEN syndrome. syndrome. CClassically all four glands are involvedlassically all four glands are involved, there is , there is frequently frequently asymmetryasymmetry with apparent sparing of with apparent sparing of one or two glands, making the distinction one or two glands, making the distinction between hyperplasia and adenoma difficult. between hyperplasia and adenoma difficult. The combined weight of all glands rarely The combined weight of all glands rarely exceeds exceeds 1.0 gm and is often less.1.0 gm and is often less. Microscopically, the most common pattern seen Microscopically, the most common pattern seen is that of is that of chief cell hyperplasia, which may chief cell hyperplasia, which may involve the glands in a diffuse or multinodular involve the glands in a diffuse or multinodular pattern. pattern.

Parathyroid carcinomasParathyroid carcinomas
CCircumscribed lesions that are difficult to ircumscribed lesions that are difficult to distinguish from adenomas, or they may distinguish from adenomas, or they may be clearly invasive neoplasms.be clearly invasive neoplasms.
These tumors enlarge one parathyroid These tumors enlarge one parathyroid gland and consist of gray-white, irregular gland and consist of gray-white, irregular masses that sometimes exceed masses that sometimes exceed 10 gm in 10 gm in weight.weight.
The cells of parathyroid carcinomas are usually The cells of parathyroid carcinomas are usually uniform and resemble normal parathyroid cells. uniform and resemble normal parathyroid cells.
They are arrayed in nodular or trabecular They are arrayed in nodular or trabecular patterns with a dense, fibrous capsule enclosing patterns with a dense, fibrous capsule enclosing the mass. the mass.
diagnosis of carcinoma based on cytologic diagnosis of carcinoma based on cytologic detail is unreliable, and invasion of detail is unreliable, and invasion of surrounding tissues and metastasis are the surrounding tissues and metastasis are the only reliable criteria of malignancy.only reliable criteria of malignancy.
Local recurrence occurs in one third of cases, Local recurrence occurs in one third of cases, and more distant dissemination occurs in and more distant dissemination occurs in another third. another third.


Skeletal changesSkeletal changes include prominence of include prominence of osteoclasts, which, in turn, erode bone matrix osteoclasts, which, in turn, erode bone matrix and mobilize calcium salts, particularly in the and mobilize calcium salts, particularly in the metaphyses of long tubular bones metaphyses of long tubular bones In more severe cases, the cortex is grossly In more severe cases, the cortex is grossly thinned, and the marrow contains increased thinned, and the marrow contains increased amounts of fibrous tissue accompanied by foci of amounts of fibrous tissue accompanied by foci of hemorrhage and cyst formation hemorrhage and cyst formation (osteitis fibrosa (osteitis fibrosa cystica)cystica). . Aggregates of osteoclasts, reactive giant cells, Aggregates of osteoclasts, reactive giant cells, and hemorrhagic debris occasionally form and hemorrhagic debris occasionally form masses that may be mistaken for neoplasms masses that may be mistaken for neoplasms ((brown tumorsbrown tumors of hyperparathyroidism). of hyperparathyroidism).
PTH-induced hypercalcemia favors PTH-induced hypercalcemia favors formation of formation of urinary tract stonesurinary tract stones (nephrolithiasis) as well as calcification of (nephrolithiasis) as well as calcification of the renal interstitium and tubules the renal interstitium and tubules (nephrocalcinosis). (nephrocalcinosis).
Metastatic calcification secondary to Metastatic calcification secondary to hypercalcemia may also be seen in other hypercalcemia may also be seen in other sites, including the stomach, lungs, sites, including the stomach, lungs, myocardium, and blood vessels. myocardium, and blood vessels.
Clinical Course.Clinical Course.
Primary hyperparathyroidism presents in Primary hyperparathyroidism presents in one of two general ways:one of two general ways:
(1) It may be asymptomatic and be (1) It may be asymptomatic and be identified after a routine chemistry profile,identified after a routine chemistry profile,
(2) (2) PPatients may have the classic clinical atients may have the classic clinical manifestations of primary manifestations of primary hhyperparathyroidism yperparathyroidism
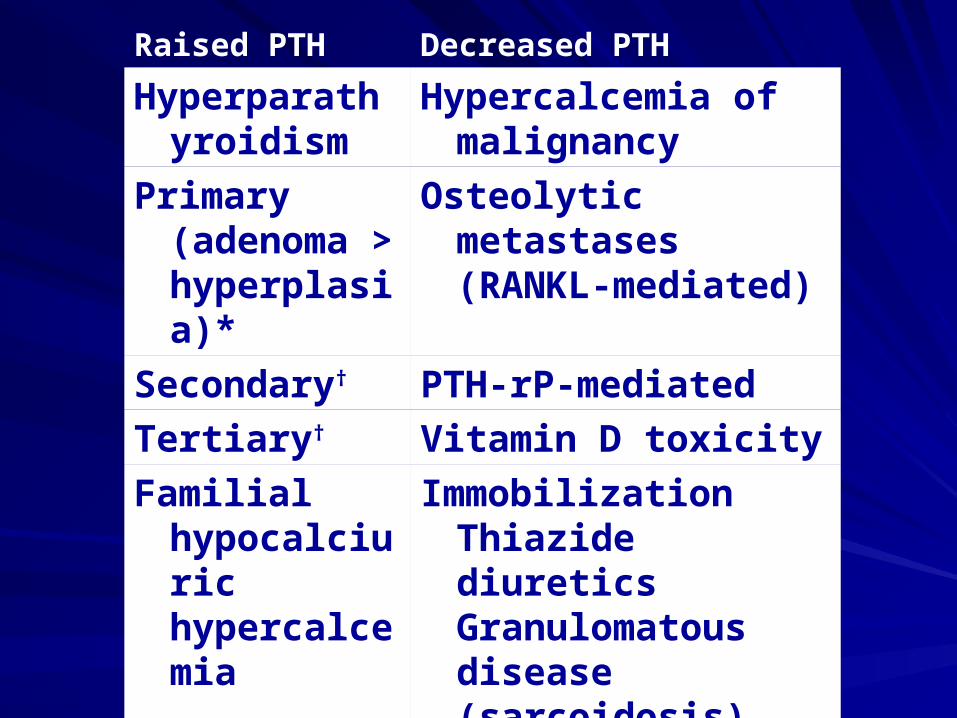
Raised PTH Decreased PTH
Hyperparathyroidism
Hypercalcemia of malignancy
Primary (adenoma > hyperplasia)*
Osteolytic metastases (RANKL-mediated)
Secondary† PTH-rP-mediated
Tertiary† Vitamin D toxicity
Familial hypocalciuric hypercalcemia
ImmobilizationThiazide diuretics Granulomatous disease (sarcoidosis)
Primary hyperparathyroidism is the most Primary hyperparathyroidism is the most common cause of hyper-calcemia overall.common cause of hyper-calcemia overall.
Malignancy is the most common cause of Malignancy is the most common cause of symptomaticsymptomatic hypercalcemia hypercalcemia. .
Primary hyperparathyroidism and Primary hyperparathyroidism and malignancy account for nearly 90% of malignancy account for nearly 90% of cases of hypercalcemia.cases of hypercalcemia.
Secondary and tertiary Secondary and tertiary hyperparathyroidism are most commonly hyperparathyroidism are most commonly associated with progressive renal failure.associated with progressive renal failure.
Asymptomatic HyperparathyroidismAsymptomatic HyperparathyroidismBecause serum calcium levels are routinely Because serum calcium levels are routinely assessed in the work-up of most patients who assessed in the work-up of most patients who need blood tests for unrelated conditions, need blood tests for unrelated conditions, clinically silent hyperparathyroidism is often clinically silent hyperparathyroidism is often detected early.detected early.
The The most common manifestation of primary most common manifestation of primary hyperparathyroidism is an increase in the level of hyperparathyroidism is an increase in the level of serum ionized calciumserum ionized calcium; in fact, ; in fact, primary primary hyperparathyroidism is the most common cause hyperparathyroidism is the most common cause of of asymptomaticasymptomatic hypercalcemia. hypercalcemia.
Symptomatic Primary HyperparathyroidismSymptomatic Primary HyperparathyroidismThe signs and symptoms of hyperparathyroidism reflect the The signs and symptoms of hyperparathyroidism reflect the combined effects of increased PTH secretion and combined effects of increased PTH secretion and hypercalcemia. hypercalcemia. TThe symptomatic presentation involves a he symptomatic presentation involves a diversity of clinical manifestations: diversity of clinical manifestations: Bone diseaseBone disease includes bone pain secondary to fractures of includes bone pain secondary to fractures of bones weakened by osteoporosis or osteitis fibrosa cystica.bones weakened by osteoporosis or osteitis fibrosa cystica.NephrolithiasisNephrolithiasis (renal stones) occurs in 20% of newly (renal stones) occurs in 20% of newly diagnosed patients, with attendant pain and obstructive diagnosed patients, with attendant pain and obstructive uropathy. Chronic renal insufficiency and a variety of uropathy. Chronic renal insufficiency and a variety of abnormalities in renal function are found, including polyuria abnormalities in renal function are found, including polyuria and secondary polydipsia.and secondary polydipsia.Gastrointestinal disturbances include constipation, nausea, Gastrointestinal disturbances include constipation, nausea, peptic ulcers, pancreatitis, and gallstones.peptic ulcers, pancreatitis, and gallstones.Central nervous system alterations include depression, Central nervous system alterations include depression, lethargy, and eventually seizures.lethargy, and eventually seizures.Neuromuscular abnormalities include complaints of Neuromuscular abnormalities include complaints of weakness and fatigue.weakness and fatigue.Cardiac manifestations include aortic or mitral valve Cardiac manifestations include aortic or mitral valve calcifications (or both). calcifications (or both).
SECONDARY SECONDARY HYPERPARATHYROIDISMHYPERPARATHYROIDISM
Secondary hyperparathyroidism is caused by any Secondary hyperparathyroidism is caused by any condition associated with a chronic depression in condition associated with a chronic depression in the serum calcium level because low serum the serum calcium level because low serum calcium leads to compensatory overactivity of the calcium leads to compensatory overactivity of the parathyroid glands.parathyroid glands.Renal failure is by far the most common cause of Renal failure is by far the most common cause of secondary hyperparathyroidismsecondary hyperparathyroidism,, although a although a number of other diseases, including inadequate number of other diseases, including inadequate dietary intake of calcium, steatorrhea, and dietary intake of calcium, steatorrhea, and vitamin D deficiency, may also cause this vitamin D deficiency, may also cause this disorder. disorder.

MorphologyMorphology:: The The parathyroid glands in secondary parathyroid glands in secondary hyperparathyroidism are hyperplastichyperparathyroidism are hyperplastic..As in the case of primary hyperplasia, the degree of As in the case of primary hyperplasia, the degree of glandular enlargement is not necessarily symmetric. glandular enlargement is not necessarily symmetric. Microscopically, the hyperplastic glands contain an Microscopically, the hyperplastic glands contain an increased number of chief cells, or cells with more increased number of chief cells, or cells with more abundant, clear cytoplasm (so-called water-clear cells) abundant, clear cytoplasm (so-called water-clear cells) in a diffuse or multinodular distribution.in a diffuse or multinodular distribution.Fat cells are decreased in number.Fat cells are decreased in number.Bone changesBone changes similar to those seen in primary similar to those seen in primary hyperparathyroidism may also be present. hyperparathyroidism may also be present. Metastatic calcificationMetastatic calcification may be seen in many may be seen in many tissues, including lungs, heart, stomach, and blood tissues, including lungs, heart, stomach, and blood vessels. vessels.
Clinical CourseClinical CourseThe clinical features of secondary The clinical features of secondary hyperparathyroidism are usually hyperparathyroidism are usually dominated by those associated with dominated by those associated with chronic renal failurechronic renal failure. .
Bone abnormalities (renal osteodystrophy) Bone abnormalities (renal osteodystrophy) and other changes associated with PTH and other changes associated with PTH excess are, in general, excess are, in general, less severeless severe than than are those seen in primary are those seen in primary hyperparathyroidism. hyperparathyroidism.
In a minority of patients, parathyroid In a minority of patients, parathyroid activity may become autonomous and activity may become autonomous and excessive, with resultant hypercalcemia, a excessive, with resultant hypercalcemia, a process that is sometimes termed process that is sometimes termed tertiary tertiary hyperparathyroidismhyperparathyroidism. Parathyroidectomy . Parathyroidectomy may be necessary to control the may be necessary to control the hyperparathyroidism in such patients. hyperparathyroidism in such patients.

HypoparathyroidismHypoparathyroidism
Hypoparathyroidism is far less common than Hypoparathyroidism is far less common than is hyperparathyroidism. There are many is hyperparathyroidism. There are many possible causes of deficient PTH secretion possible causes of deficient PTH secretion resulting in hypoparathyroidism: resulting in hypoparathyroidism: Surgically inducedSurgically induced hypoparathyroidism hypoparathyroidism occurs with inadvertent removal of all the occurs with inadvertent removal of all the parathyroid glands during parathyroid glands during thyroidectomy,thyroidectomy, excision of the parathyroid glands in the excision of the parathyroid glands in the mistakenmistaken

Congenital absenceCongenital absence of all glands of all glands, as in certain , as in certain developmental abnormalities, such as thymic developmental abnormalities, such as thymic aplasia and cardiac defects (22q11.2 syndrome) aplasia and cardiac defects (22q11.2 syndrome)
Familial hypoparathyroidismFamilial hypoparathyroidism is often associated is often associated with chronic mucocutaneous candidiasis and with chronic mucocutaneous candidiasis and primary adrenal insufficiency; this syndrome is primary adrenal insufficiency; this syndrome is known as autoimmune polyendocrine syndrome known as autoimmune polyendocrine syndrome type 1 (APS1) and is caused by mutations in the type 1 (APS1) and is caused by mutations in the autoimmune regulatorautoimmune regulator ( (AIREAIRE) gene. ) gene.
İİdiopathic hypoparathyroidismdiopathic hypoparathyroidism most likely most likely represents an autoimmune disease with isolated represents an autoimmune disease with isolated atrophy of the glands. atrophy of the glands.
The major clinical manifestations of The major clinical manifestations of hypoparathyroidism are referable to hypoparathyroidism are referable to hypocalcemia and are related to the hypocalcemia and are related to the severity and chronicity of the severity and chronicity of the hypocalcemia. hypocalcemia. The hallmark of hypocalcemiaThe hallmark of hypocalcemia is is tetanytetany, , which is characterized by which is characterized by neuromuscular irritabilityneuromuscular irritabilityMental status changesMental status changes can include can include emotional instability, anxiety and emotional instability, anxiety and depression, confusional states, depression, confusional states, hallucinations, and frank psychosis. hallucinations, and frank psychosis.
IIntracranial manifestationsntracranial manifestations include calcifications include calcifications of the basal ganglia, parkinsonian-like of the basal ganglia, parkinsonian-like movement disordersmovement disordersOcular diseaseOcular disease results results in calcification of the lens in calcification of the lens leading to cataract formation.leading to cataract formation.Cardiovascular manifestationsCardiovascular manifestations include a include a conduction defect, which produces a conduction defect, which produces a characteristic prolongation of the QT interval in characteristic prolongation of the QT interval in the electrocardiogram.the electrocardiogram.Dental abnormalitiesDental abnormalities occur when hypocalcemia occur when hypocalcemia is present during early development. These is present during early development. These findings are highly characteristic of findings are highly characteristic of hypoparathyroidism and include dental hypoparathyroidism and include dental hypoplasia, failure of eruption, defective enamel hypoplasia, failure of eruption, defective enamel and root and root
PseudohypoparathyroidismPseudohypoparathyroidism
HHypoparathyroidism occurs because of end-ypoparathyroidism occurs because of end-organ resistance to the actions of PTH.organ resistance to the actions of PTH.
SSerum PTH levels are normal or elevated. erum PTH levels are normal or elevated.
Central to the understanding of PTH resistance Central to the understanding of PTH resistance are two key concepts: (1) G-proteins, principally are two key concepts: (1) G-proteins, principally Gs, mediate the cellular actions of PTH on bone Gs, mediate the cellular actions of PTH on bone and kidney, and (2) and kidney, and (2) GNAS1GNAS1 is a selectively is a selectively imprinted gene, with tissue-specific patterns of imprinted gene, with tissue-specific patterns of imprinting imprinting
TTwo types of pseudohypoparathyroidism have wo types of pseudohypoparathyroidism have been identified depending on the parent of origin been identified depending on the parent of origin of the mutant allele: of the mutant allele:
1-1-Pseudohypoparathyroidism type 1APseudohypoparathyroidism type 1A is is associated with multihormone resistance and associated with multihormone resistance and Albright hereditary osteodystrophy (AHO), a Albright hereditary osteodystrophy (AHO), a syndrome characterized by skeletal and syndrome characterized by skeletal and developmental defects. Patients with AHO often developmental defects. Patients with AHO often have short stature, obesity, short metacarpal and have short stature, obesity, short metacarpal and metatarsal bones, and variable mental deficits. metatarsal bones, and variable mental deficits. The multihormone resistance involves three The multihormone resistance involves three hormones (PTH, TSH, and LH/FSH),hormones (PTH, TSH, and LH/FSH),
2-2-PseudopseudohypoparathyroidismPseudopseudohypoparathyroidism:: In In this disorder, this disorder, the mutation is inherited on the mutation is inherited on the paternal allele,the paternal allele, and it is characterized and it is characterized by AHO by AHO withoutwithout accompanying accompanying multihormonal resistance. As a result, multihormonal resistance. As a result, serum calcium, phosphate and PTH levels serum calcium, phosphate and PTH levels are normal. are normal.
![The prevalence and anatomy of parathyroid glands: a meta ... · glands from the third pharyngeal pouches [3]. The supe-rior glands are usually located on the upper pole of the thyroid,](https://static.fdocuments.net/doc/165x107/5fb3bb52068c194f6d6d0f1f/the-prevalence-and-anatomy-of-parathyroid-glands-a-meta-glands-from-the-third.jpg)