Anatomy of thyroid and parathyroid glands
48
Anatomy of thyroid and parathyroid glands BY- DR DHAVAL TRIVEDI
-
Upload
dhaval-trivedi -
Category
Health & Medicine
-
view
4.165 -
download
2
Transcript of Anatomy of thyroid and parathyroid glands
Anatomy of thyroid and parathyroid glands
BY- DR DHAVAL TRIVEDI
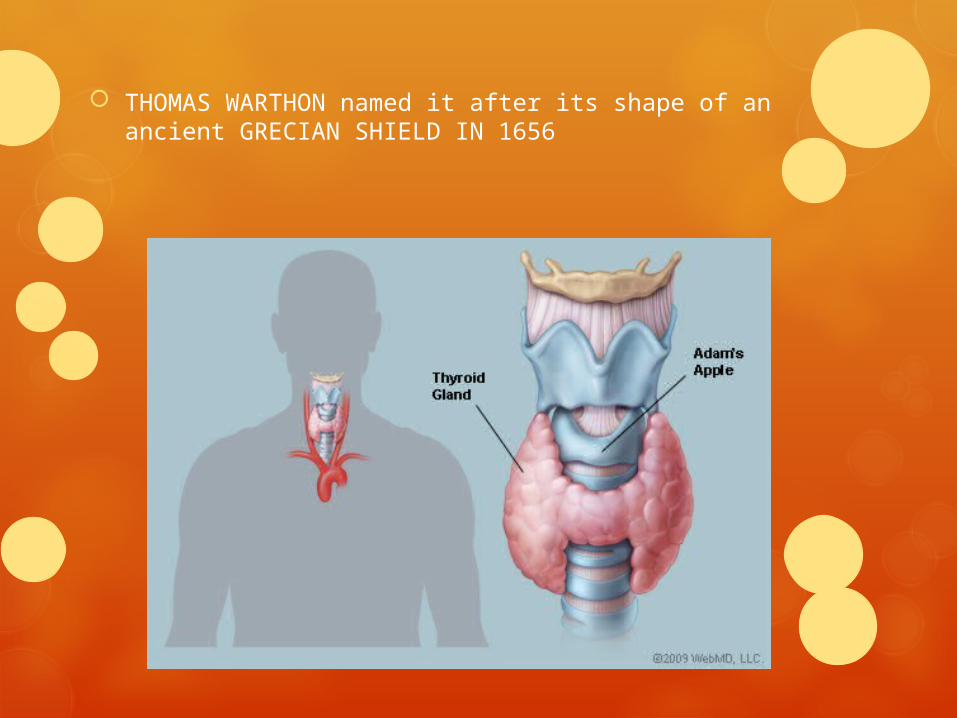
THOMAS WARTHON named it after its shape of an ancient GRECIAN SHIELD IN 1656
developement
The thyroid gland develops from an endodermal extension in the floor of
the pharynx known as the thyroglossal duct. The thyroglossal duct
descends through the tongue and usually degenerates when the thyroid
develops.
The vestigial marking of the thyroglossal duct is the foramen cecum of
the tongue.
Remnants of thyroglossal duct anywhere else in its track can develop
into a thyroglossal cyst. These present as neck lumps that rise when
the tongue is protruded.
In 50% of people a remnant of this duct forms a small pyramidal lobe extending superiorly from the isthmus.
The parafollicular (C) cells are derived from the neural rest.
The thyroid gland, brownish-red and highly vascular, is placed anteriorly in the lower neck, level with the fifth cervical to the first thoracic vertebrae
It is ensheathed by the pretracheal layer of deep cervical fascia and consists of right and left lobes connected by a narrow, median isthmus. Its weight is usually c.25g, but this varies.
The gland is slightly heavier in females, and enlarges during menstruation and pregnancy.
Estimation of the size of the thyroid gland is clinically important in the evaluation and management of thyroid disorders
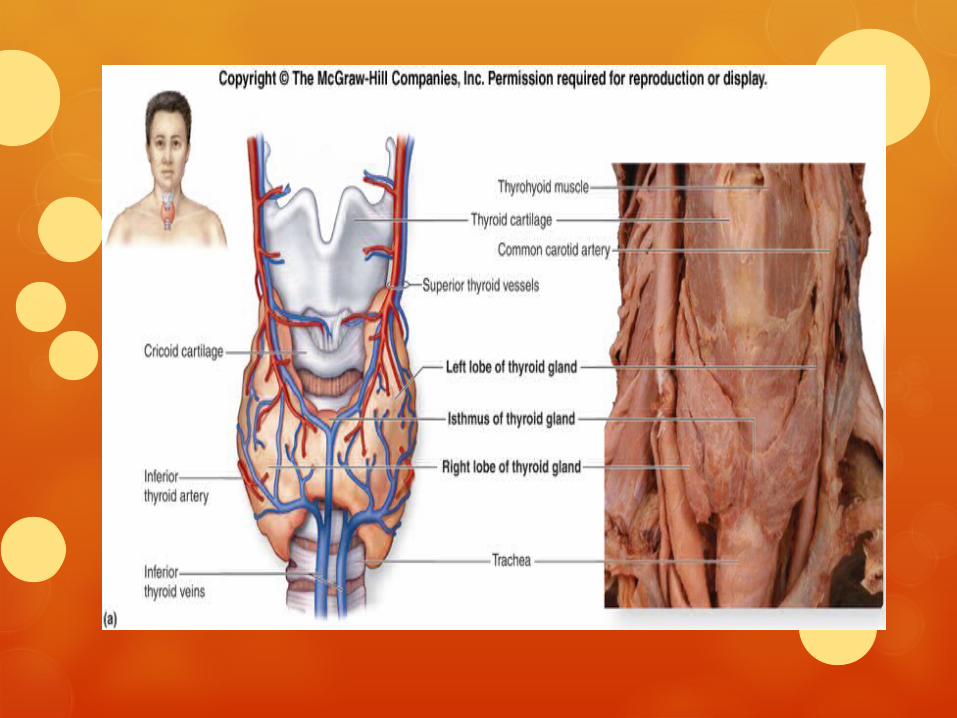
It is located in the neck, inferior to the larynx and cricoid cartilage.
The lobes of the thyroid gland are approximately conical.
Their ascending apices diverge laterally to the level of the oblique lines on the laminae of the thyroid cartilage, and their bases are level with the fourth or fifth tracheal cartilages.
Each lobe is c.5 cm long, its greatest transverse and anteroposterior extents being c.3 cm and 2 cm respectively.
The posteromedial aspects of the lobes are attached to the side of the cricoid cartilage by a lateral thyroid ligament
The isthmus connects the lower parts of the two lobes, although occasionally it may be absent
It measures c.1.25 cm transversely and vertically, and is usually anterior to the second and third tracheal cartilages, though often higher or sometimes lower because its site and size vary greatly.
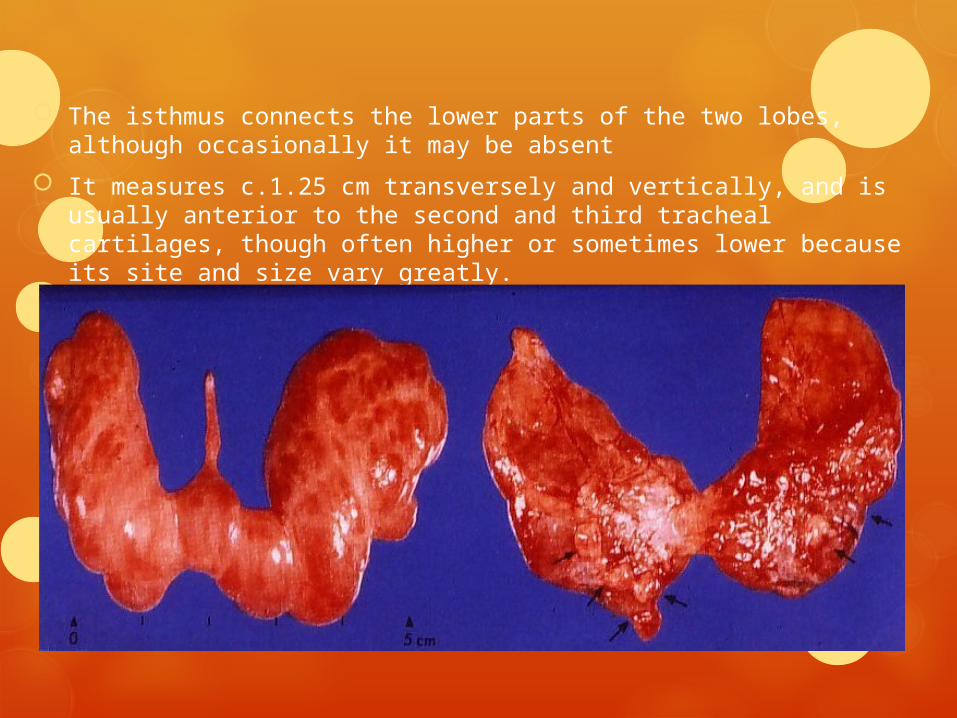
A conical pyramidal lobe often ascends towards the hyoid bone from the isthmus or the adjacent part of either lobe (more often the left).
The thyroid gland is surrounded by a fibrous capsule derived from the pretracheal layer of the deep cervical fascia.
Extensions of this capsule into the body of the thyroid create septae, which divide the gland into lobules.
This connective tissue firmly connects the thyroid to the larynx and explains why the thyroid moves on swallowing.
SURFACES AND RELATIONS
The convex lateral (superficial) surface is covered by sternothyroid, whose attachment to the oblique thyroid line prevents the upper pole of the gland from extending on to thyrohyoid
More anteriorly lie sternohyoid and the superior belly of omohyoid, overlapped inferiorly by the anterior border of sternocleidomastoid
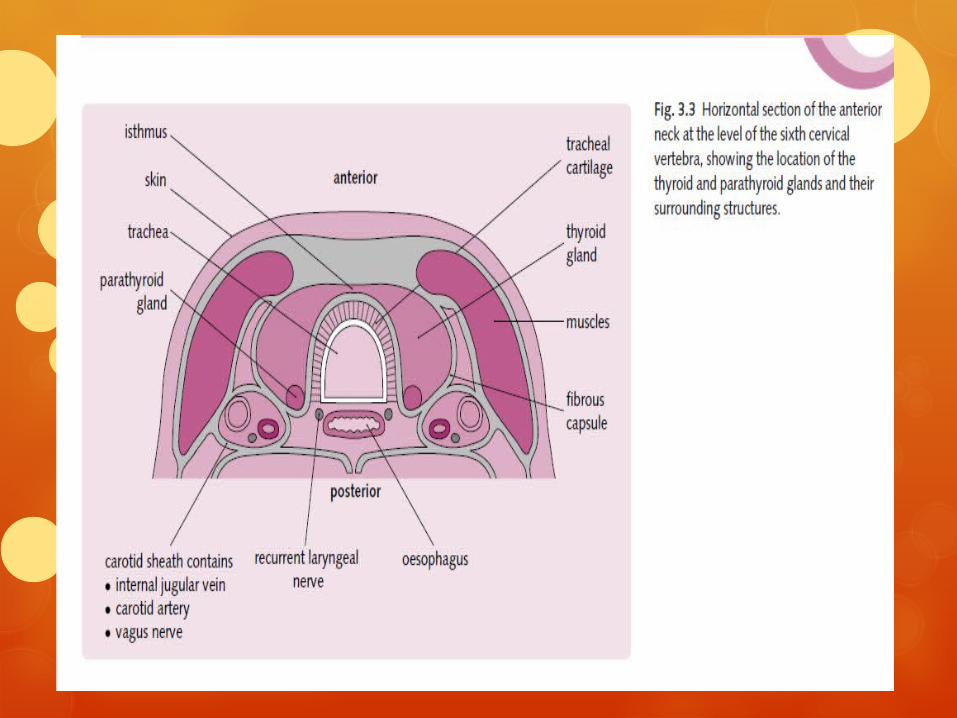
The medial surface of the gland is adapted to the larynx and trachea, contacting at its superior pole the inferior pharyngeal constrictor and the posterior part of cricothyroid, which separate it from the posterior part of the thyroid lamina and the side of the cricoid cartilage
The external laryngeal nerve is medial to this part of the gland as it passes to supply cricothyroid. Inferiorly, the trachea and, more posteriorly, the recurrent laryngeal nerve and oesophagus (which is closer on the left) are medial relations.
The posterolateral surface of the thyroid gland is close to the carotid sheath, and overlaps the common carotid artery
The thin anterior border of the gland, near the anterior branch of the superior thyroid artery, slants down medially.
The rounded posterior border is related below to the inferior thyroid artery and its anastomosis with the posterior branch of the superior thyroid artery
The lower end of the posterior border on the left side lies near the thoracic duct
The isthmus is covered by sternothyoid, from which it is separated by pretracheal fascia. More superficially it is covered by sternohyoid, the anterior jugular veins, fascia and skin.
The superior thyroid arteries anastomose along its upper border and the inferior thyroid veins leave the gland at its lower border
Blood supply, nerves
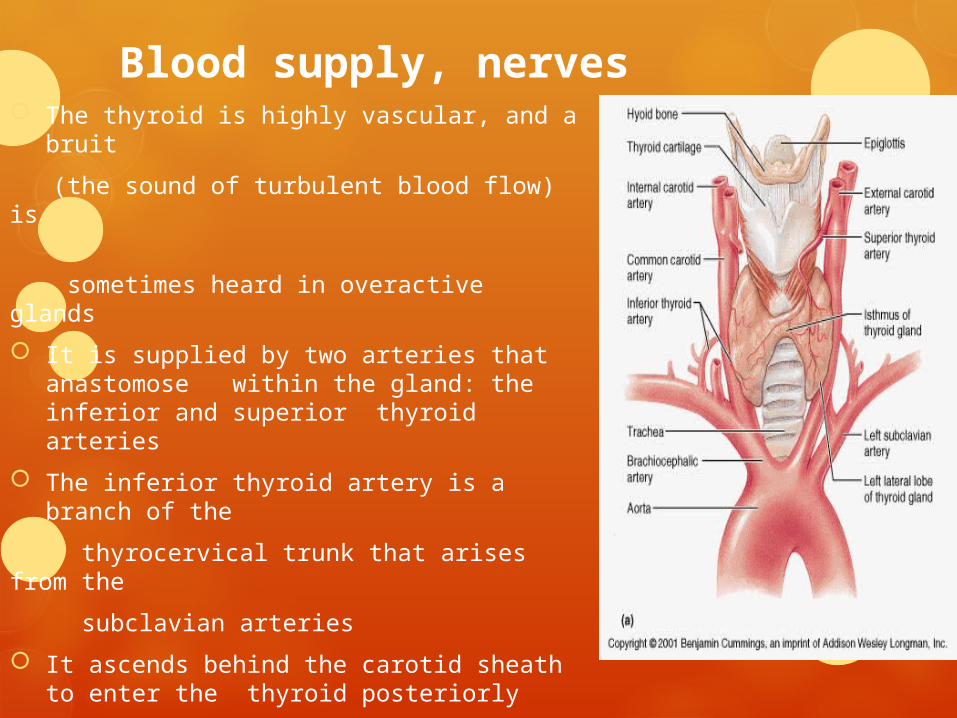
The thyroid is highly vascular, and a bruit
(the sound of turbulent blood flow) is
sometimes heard in overactive glands
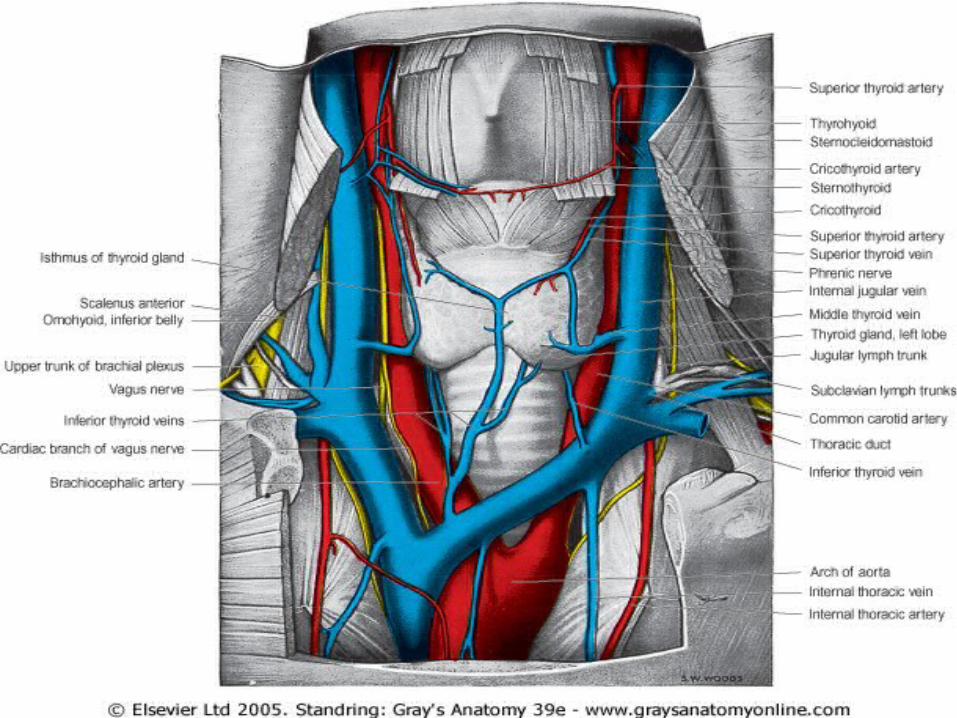
It is supplied by two arteries that anastomose within the gland: the inferior and superior thyroid arteries
The inferior thyroid artery is a branch of the
thyrocervical trunk that arises from the
subclavian arteries
It ascends behind the carotid sheath to enter the thyroid posteriorly
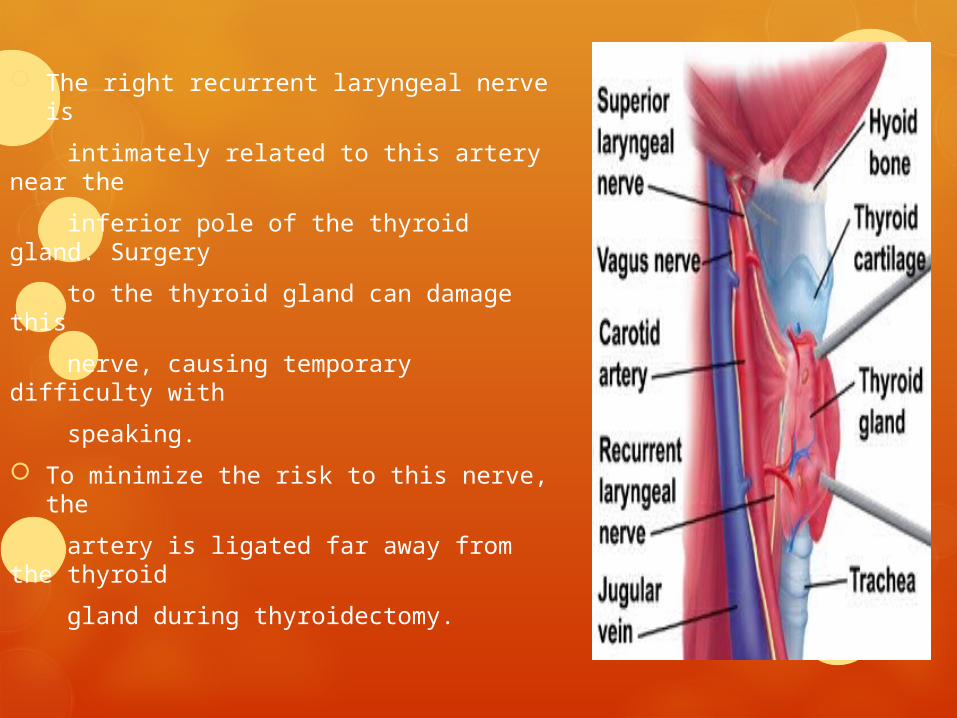
The right recurrent laryngeal nerve is
intimately related to this artery near the
inferior pole of the thyroid gland. Surgery
to the thyroid gland can damage this
nerve, causing temporary difficulty with
speaking.
To minimize the risk to this nerve, the
artery is ligated far away from the thyroid
gland during thyroidectomy.
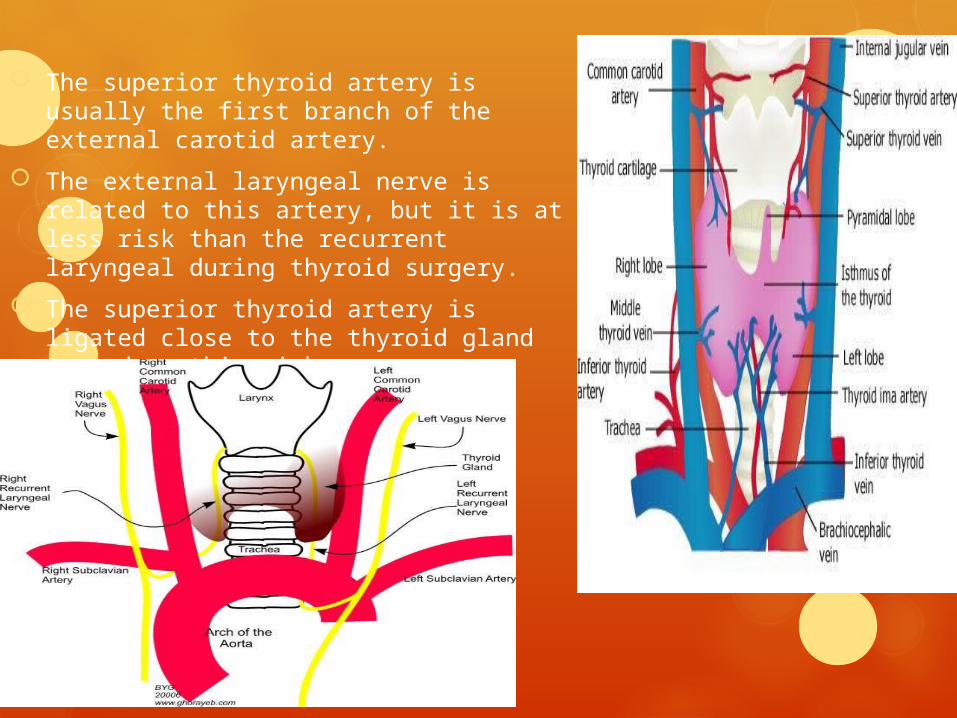
The superior thyroid artery is usually the first branch of the external carotid artery.
The external laryngeal nerve is related to this artery, but it is at less risk than the recurrent laryngeal during thyroid surgery.
The superior thyroid artery is ligated close to the thyroid gland to reduce this risk
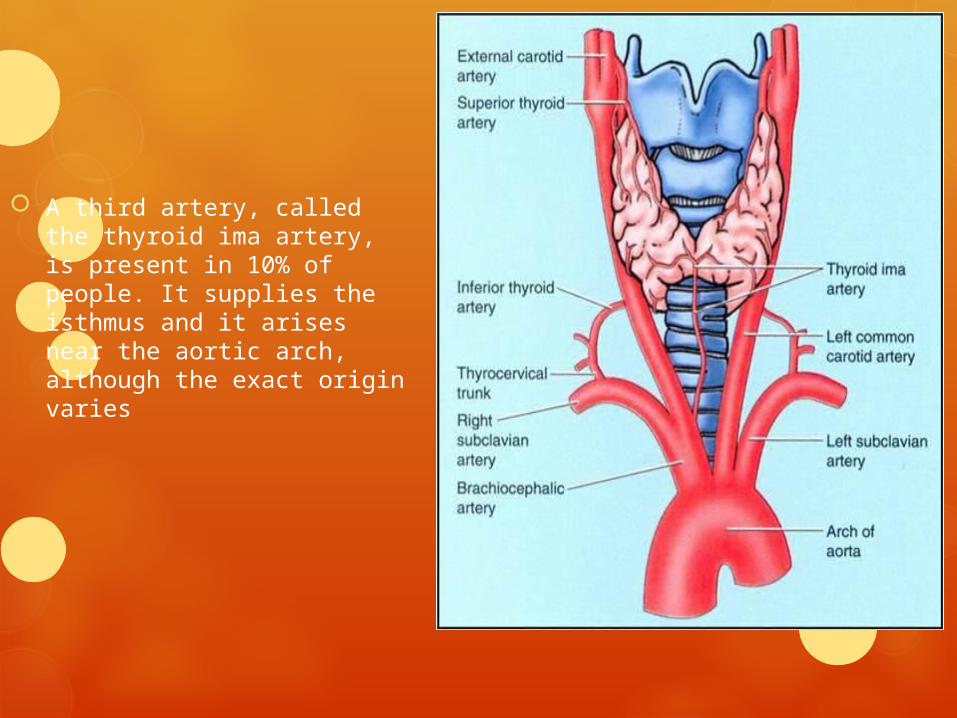
A third artery, called the thyroid ima artery, is present in 10% of people. It supplies the isthmus and it arises near the aortic arch, although the exact origin varies
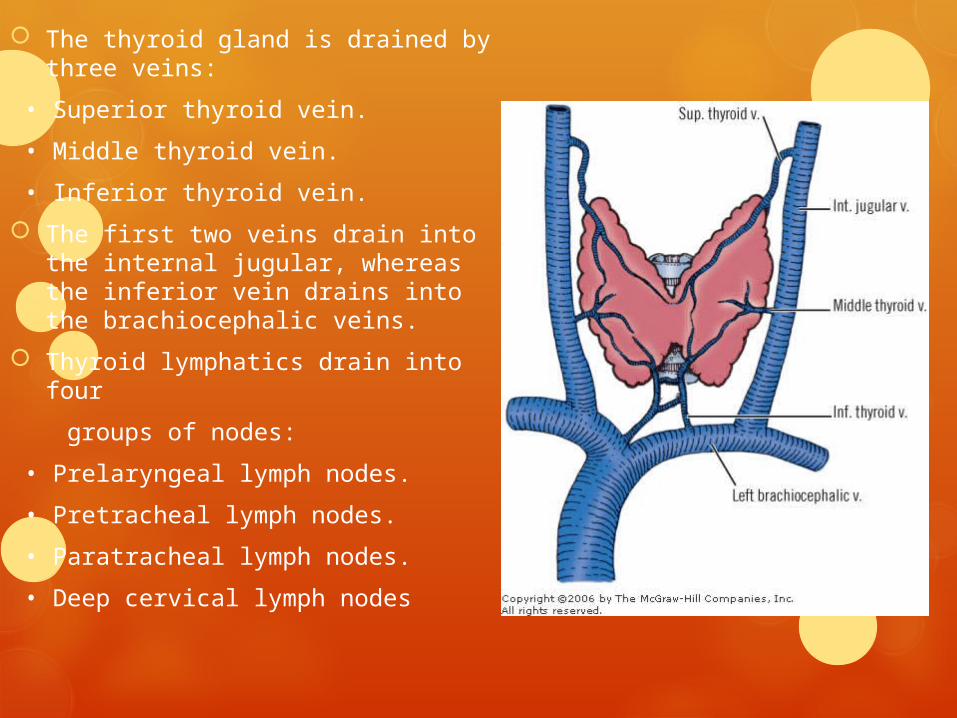
The thyroid gland is drained by three veins:
• Superior thyroid vein.
• Middle thyroid vein.
• Inferior thyroid vein.
The first two veins drain into the internal jugular, whereas the inferior vein drains into the brachiocephalic veins.
Thyroid lymphatics drain into four
groups of nodes:
• Prelaryngeal lymph nodes.
• Pretracheal lymph nodes.
• Paratracheal lymph nodes.
• Deep cervical lymph nodes

HORMONES
The thyroid gland synthesizes and secretes three hormones:
• Thyroxine (T4).
• Tri-iodothyronine (T3).
• Calcitonin
Regulation
Hypothalamic thyrotrophin-releasing hormone (TRH)
stimulates the release of thyroid-stimulating hormone
(TSH) from thyrotrophs in the anterior pituitary gland
and also causes upregulation of TSH gene transcription.
Thyroxine (T4) andTri-iodothyronine (T3).
Both of these hormones profoundly increase the metabolic rate of the body.
Complete lack of thyroid secretion usually causes the basal metabolic rate to fall 40 to 50 per cent below normal, and extreme excesses of thyroid secretion can increase the basal metabolic rate to 60 to 100 per cent above normal.
Thyroid secretion is controlled primarily by thyroid-stimulating hormone (TSH) secreted by the anterior pituitary gland.
About 93 per cent of the metabolically active hormones secreted by the thyroid gland is thyroxine, and 7 per cent triiodothyronine.
However, almost all the thyroxine is eventually converted to triiodothyronine in the tissues, so that both are functionally important.
The functions of these two hormones are qualitatively the same, but they differ in rapidity and intensity of action.
Triiodothyronine is about four times as potent as thyroxine, but it is present in the blood in much smaller quantities and persists for a much shorter time than does thyroxine
The thyroid gland is composed of large numbers of closed follicles (100 to 300 micrometers in diameter) filled with a secretory substance called colloid and lined with cuboidal epithelial cells that secrete into the interior of the follicles.
The major constituent of colloid is the large glycoprotein thyroglobulin, which contains the thyroid hormones within its molecule.
Once the secretion has entered the follicles, it must be absorbed back through the follicular epithelium into the blood before it can function in the body.
The thyroid gland has a blood flow about five times the weight of the gland each minute, which is a blood supply as great as that of any other area of the body
To form normal quantities of thyroxine, about 50 milligrams of ingested iodine in the form of iodides are required each year, or about 1 mg/week.
Calcitonin Calcitonin (also known as thyrocalcitonin) is a 32-amino acid linear
polypeptide hormone
Calcitonin was purified in 1962 by Copp and Cheney.
While it was initially considered a secretion of the parathyroid glands it
was later identified as the secretion of the C-cells of the thyroid gland
It acts to reduce blood calcium , opposing the effects of PTH
- Inhibits Ca2+ absorption by the intestines
- Inhibits osteoclast activity in bones
- Inhibits renal tubular cell reabsorption of Ca2+ allowing it to be excreted
in the urine
There is a relationship between the subcutaneous dose of calcitonin and
peak plasma concentrations. Following parenteral administration of 100 IU
calcitonin, peak plasma concentration lies between about 200 and 400
pg/ml. Higher blood levels may be associated with increased incidence of
nausea, vomiting, and secretory diarrhea.
Physiologic Functions of theThyroid Hormones
Increase the Transcription of Large Numbers of Genes
Increase Cellular Metabolic Activity
Thyroid hormone has both general and specific effects on growth
Stimulation of Carbohydrate Metabolism
Stimulation of Fat Metabolism
Effect on Plasma and Liver Fats.
- increased thyroid hormone decreases the concentrations of
cholesterol, phospholipids, and triglycerides in the plasma, even though it
increases the free fatty acids.
-Conversely, decreased thyroid secretion greatly increases the plasma
concentrations of cholesterol, phospholipids, and triglycerides and
almost always causes excessive deposition of fat in the liver as well
Increased Requirement for Vitamins.
- Therefore, a relative vitamin deficiency can occur when excess thyroid
hormone is secreted, unless at the same time increased quantities of
vitamins are made available.
Increased Basal Metabolic Rate
-Decreased Body Weight
- Increased Blood Flow and Cardiac Output
- Increased Heart Rate
- Increased Respiration
- Increased Gastrointestinal Motility
Slight increase in thyroid hormone usually makes the muscles react with
vigor, but when the quantity of hormone becomes excessive, the muscles
become weakened because of excess protein catabolism
Muscle Tremor
Effect on sleep - extreme somnolence is characteristic of hypothyroidism, with sleep sometimes lasting 12 to 14 hours a day.
Regulation of ThyroidHormone Secretion
TSH, also known as thyrotropin, is an anterior pituitary hormone, a
glycoprotein with a molecular weight of about 28,000.
It s effect on thyroid is
Increased proteolysis of the thyroglobulin
Increased activity of the iodide pump
Increased iodination of tyrosine to form the thyroid hormones
Increased size and increased secretory activity of the thyroid cells
Increased number of thyroid cells
The most important early effect after administration of TSH is to initiate
proteolysis of the thyroglobulin, which causes release of thyroxine and
triiodothyronine into the blood within 30 minutes. The other effects
require hours or even days and weeks to develop fully.
Feedback Effect of Thyroid Hormone to Decrease Anterior Pituitary Secretion of TSH
Increased thyroid hormone in the body fluids decreases secretion of TSH
by the anterior pituitary.
When the rate of thyroid hormone secretion rises to about 1.75 times
normal, the rate of TSH secretion Falls essentially to zero
Drugs that suppress thyroid secretion are called antithyroid
substances.The best known of these substances are thiocyanate,
propylthiouracil, and high concentrations of inorganic iodides.
Iodides in high concentrations decrease all phases of thyroid activity,
they slightly decrease the size of the thyroid gland and especially
decrease its blood supply, in contradistinction to the opposite effects
caused by most of the other antithyroid agents.
For this reason, iodides are frequently administered to patients for 2 to 3
weeks before surgical removal of the thyroid gland to decrease the
necessary amount of surgery, especially to decrease the amount of
bleeding.
DISEASES OF THYROID
HYPERTHYROIDISM -excess of thyroid hormone production.
When this becomes symptomatic it is called thyrotoxicosis.
Thyrotoxicosis can occur in the absence of true hyperthyroidism.
It is a common disorder affecting 1/50 females and 1/250 males
Presentation is usually slow with a history lasting over 6 months.
SIGNS AND SYMPTOMS
Hair - loss
Eyes – exophthalmos,lid retraction,lid lag ,predisposes to keratitis
Brain - emotional lability,fatigue,anxiety,restlessness
Heart - palpitations,tachycardia ,atrial fibrillation
Neck – goitre
Muscles - proximal myopathy
Bowel - diarrhoea,increased appetite
Uterus - menorrhagia,infertility,reduced libido
Hands - tremor,warmth,sweating
Reflexes – increased
bones – osteoporosis
skin and adipose tissue - increased sweating,heat intolerance ,weight
loss

The main causes of hyperthyroidism are:
Diffuse toxic goitre: Graves’ disease—an autoimmune disease involving autoantibody stimulation of TSH receptors.
Toxic multinodular goitre—nodular enlargement of the thyroid in the elderly.
Toxic nodule—autonomously functioning thyroid nodule; most are adenomas (benign thyroid hormone producing tumours).
Lymphocytic thyroiditis—inflammation causes release of stored hormones
Subacute thyroiditis—thyroiditis associated with a painful goitre.
Diagnosis
Thyroid function tests
Serum TSH, free T3, and free T4 are measured by radioimmunoassay
- Raised T3 and T4 indicate that hyperthyroidism is present. Raised TSH
suggests the fault lies in or above the pituitary gland, whereas low TSH
points to a thyroid organ lesion
Autoantibody detection, e.g. Graves’ disease.
Radioisotope scanning to show the size of the thyroid gland and any
abnormal ‘hot’ areas such as a toxic adenoma.
ECG for sinus tachycardia or atrial fibrillation
Treatment
Carbimazole—this drug inhibits the peroxidase reactions of T3 and T4
synthesis. It takes 3–4 weeks to have an effect
Radioactive iodine therapy—131I is only taken up by thyroid tissue; it kills
the cells leading to reduced T3 and T4 synthesis. The response is slow and
carbimazole may be required
Partial thyroidectomy—the thyroid gland is surgically removed leaving
some tissue and the parathyroid glands. Used in patients with relapsing
disease or allergy to medical treatment. Carries risk of recurrent laryngeal
nerve palsy and hypocalcaemia due to the removal of parathyroid glands.
Hypothyroidism
Hypothyroidism is defined as an underactive thyroid gland leading to
deficient thyroid hormones .
When this becomes symptomatic, it is called myxoedema. It is slightly
less common than hyperthyroidism, affecting 1/100 females and 1/500
males
Presentation is even more gradual than in hyperthyroidism, with many
symptoms frequently being ignored

Signs and symptoms
Hair - coarse and thin hair,loss of outer third of eyebrows
Brain- mental slowing,apathy,tiredness,psychosis
Face -pale puffy face, coarse features,deafness
Heart – bradycardia
Neck – goitre
Muscles - slowing of activity,muscle weakness in upper arms and legs
Bowel – constipation
Hands - cold hands,carpal tunnel syndrome
Uterus – amenorrhoea
Reflexes - slow relaxing
skin and adipose tissue - weight gain/obesity,intolerance to cold
decreased sweating ,chronic oedema ,cold dry skin
Diagnosis
Hypothyroidism is not investigated as thoroughly as
hyperthyroidism, since treatment does not vary.
Free T3 and T4 levels are low, whereas TSH levels are
usually raised.
If TSH is low then a lesion of the hypothalamus or
pituitary is likely.
Autoantibodies can be detected in Hashimoto’s
thyroiditis
Treatment
All hypothyroidism is treated with thyroxine (T4) administered as an oral
tablet in varying doses.
The dose is increased over several months, with regular monitoring of
TSH levels until they are within the normal boundaries.
This process is slow, since it takes 4 weeks for TSH levels to reflect an
increased dose due to the long half-life of thyroxine.
Thyroxine therapy is usually maintained for life
Hashimoto’s thyroiditis When the thyroid gland is inflamed, the disease is
called thyroiditis. This can be caused by autoimmune
or viral processes.
Hashimoto’s thyroiditis is a destructive autoimmune
disease that is especially common in middle-aged women.
It is mediated by autoantibodies against rough endoplasmic
reticulum (microsomal antibodies) or thyroglobulin. The
presence ofthese antibodies can be tested to confirm the
diagnosis.
The thyroid gland is infiltrated by lymphocytes that cause
the gland to enlarge, forming a goitre.
The initial destruction of the thyroid gland can release the
thyroglobulin colloid causing temporary hyperthyroidism.
The patients usually progress to a euthyroid (normal) state
and finally develop progressive hypothyroidism.
Goitres
A goitre is a swelling in the neck caused by an enlarged thyroid
gland. It is a common finding, and it is usually asymptomatic;
however, large goitres can compress the oesophagus and trachea.
If a goitre is associated with hyperthyroidism it is described as
‘toxic’. Non-toxic goitres secrete normal or reduced levels of thyroid
hormones.
Non-toxic goitres are usually the result of excessive TSH stimulation
in the presence of hypothyroidism.
Goitres are treated by correcting the underlying pathology or by
surgical removal for cosmetic reasons or to prevent compression of
surrounding structures
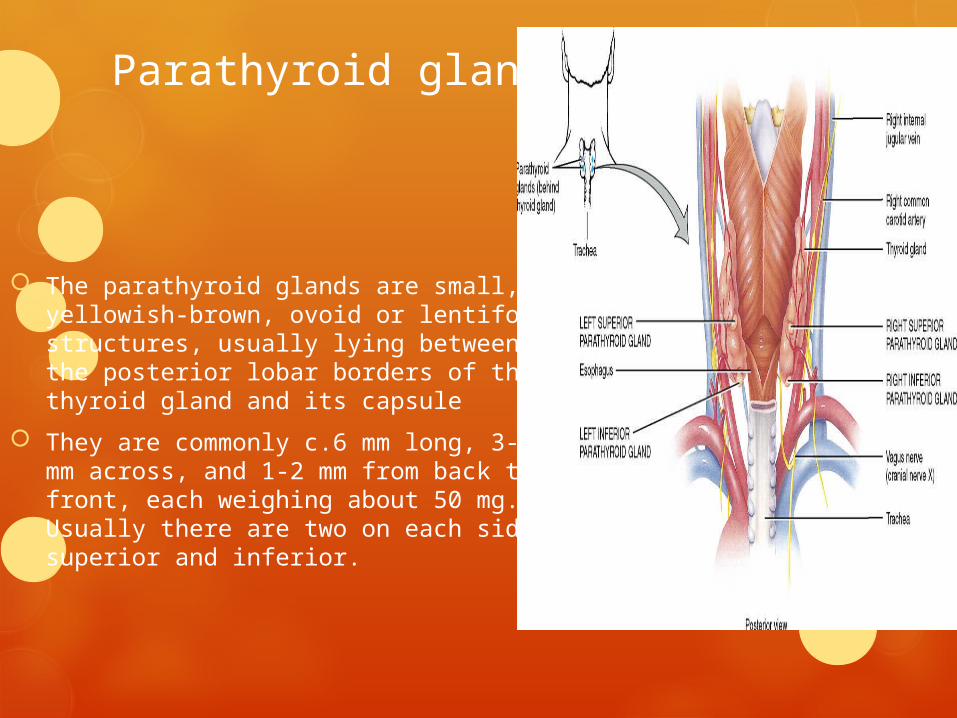
Parathyroid glands
The parathyroid glands are small, yellowish-brown, ovoid or lentiform structures, usually lying between the posterior lobar borders of the thyroid gland and its capsule
They are commonly c.6 mm long, 3-4 mm across, and 1-2 mm from back to front, each weighing about 50 mg. Usually there are two on each side, superior and inferior.
The superior parathyroid glands are more constant in location than the inferior and are usually to be found midway along the posterior borders of the thyroid gland, although they may be higher.
The inferior pair are more variably situated and may be within the fascial thyroid sheath, below the inferior thyroid arteries and near the inferior lobar poles; or outside the sheath, immediately above an inferior thyroid artery; or in the thyroid gland near its inferior pole.
The superior parathyroids are usually dorsal, the inferior parathyroids ventral, to the recurrent laryngeal nerves.
The parathyroid glands are very flattened in cross-section and are not normally visible by current imaging methods, including scintigraphy
VASCULAR SUPPLY AND LYMPHATIC DRAINAGE
The parathyroid glands have a rich blood supply from the inferior thyroid arteries or from anastomoses between the superior and inferior vessels.
Approximately one-third of human parathyroid glands have two or more parathyroid arteries.
Lymph vessels are numerous and associated with those of the thyroid and thymus glands.
INNERVATION
The nerve supply is sympathetic, either direct from the superior or middle cervical ganglia or via a plexus in the fascia on the posterior lobar aspects.
Parathyroid activity is controlled by variations in blood calcium level: it is inhibited by a rise and stimulated by a fall.
The nerves are believed to be vasomotor but not secretomotor
Parathyroid hormones
Parathyroid hormone (PTH), parathormone or parathyrin, is
secreted by the chief cells of the parathyroid glands
It acts to increase the concentration of calcium (Ca2+) in the blood,
PTH half-life is approximately 4 minutes
PTH can be measured in the blood in several different forms: intact PTH;
N-terminal PTH; mid-molecule PTH, and C-terminal PTH, and different
tests are used in different clinical situations.
The average PTH level is 10-60 pg/ml.
Functions
Parathyroid hormone raises blood Ca by acting on 3 organs:
- Bone: main effect- stimulates osteoclasts -> bone breaks down -> Ca
released
- Intestines: increases uptake of Ca from intestine
- Kidney: stimulates reabsorption of Ca from the Ca in kidney tubules
PTH reduces the reabsorption of phosphate from the proximal tubule of
the kidney which means more phosphate is excreted through the urine
PTH increases the activity of 1-α-hydroxylase enzyme, which converts 25-
hydroxycholecalciferol to 1,25-dihydroxycholecalciferol, the active form of
vitamin D.
Stimulators
- Decreased serum Ca2+
- Mild decreases in serum Mg2+
- An increase in serum phosphate
Inhibitors
- Increased serum Ca2+
- Severe decreases in serum Mg2+, which also produces symptoms
of hypoparathyroidism[
Clinical significance
Hyperparathyroidism, the presence in the blood of excessive amounts of
parathyroid hormone, occurs in two very distinct sets of circumstances.
Primary hyperparathyroidism is due to autonomous, abnormal
hypersecretion of PTH in the parathyroid gland while secondary
hyperparathyroidism is an appropriately high PTH level seen as a
physiological response to hypocalcaemia
A low level of PTH in the blood is known as hypoparathyroidism and is
most commonly due to damage to or removal of parathyroid glands during
thyroid surgery
THANK YOU