Pancreatic Neuroendocrine Neoplasm (pNEN) case
19
Pancreatic Neuroendocrine Neoplasm (pNEN) case Endocrinology Unit Pathophysiology Department Laikon General Hospital Case Presentation: Dr. Chatzellis Eleftherios MD Intern in Endocrinology
description
Pancreatic Neuroendocrine Neoplasm (pNEN) case. Case Presentation : Dr. Chatzellis Eleftherios MD Intern in Endocrinology. Endocrinology Unit Pathophysiology Department Laikon General Hospital. Case History - 2001. 58 year old male patient 2001 : abdominal pain - PowerPoint PPT Presentation
Transcript of Pancreatic Neuroendocrine Neoplasm (pNEN) case

Pancreatic Neuroendocrine Neoplasm (pNEN) case
Endocrinology UnitPathophysiology DepartmentLaikon General Hospital
Case Presentation:Dr. Chatzellis Eleftherios MD
Intern in Endocrinology

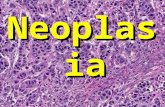
58 year old male patient 2001: abdominal pain CT scan: 5cm tumor pancreatic tail
Multiple focal lesions in the liver FNAB (liver lesion) Well Differentiated NEN
grade 2 (ki67 = 4%) CgA = 5,2 nmol/l (<4), other markers negative No secretory symptoms (non-functioning pNEN) SRS (Octreoscan): avid uptake (Krenning score = 3) in both
primary pNEN and liver metastases
Case History - 2001

Case History
Chromogranin A
ki67
H&E stain

Case History 2001-2005 Sweden (Uppsala) Suggested surgery to reduce tumor
burden and local complications Patient refused Chemotherapy (Streptozotocin + 5-FU)
+ Somatostatin analogues (SSA’s) 1 year later (2002): DISEASE PROGRESSION (PD) Addition of pegylated INF-a Chemotherapy was discontinued after 2,5 years (mild
renal impairment) 2002-2005 : STABLE DISEASE (SD) CgA = 10,5 nmol/l (<4)

Case History 2006-2008 2006: Hypercalcemia occurred for the first time
Ca = 11,8 mg/dl (8,5 - 10,1)P = 1,98 mg/dl (2,5 - 4,5)PTH = 2,54 pg/ml (10 - 65)PTHrP = 84 pmol/l (<2)CgA = 45 nmol/l (<4)
Imaging: DISEASE PROGRESSION (PD) Increased SSA’s dosage [+peg-INFa] Normalization Ca 2006-2008: STABLE DISEASE (SD) - Biochemical control
Humoral Malignancy-associated Hypercalcemia(PTHrP- related)

Case History 2008-2009 2008: peg-INFa discontinued (depression) 2008: Hypercalcemia (12,9 mg/dl)
+ DISEASE PROGRESSION (PD) 2008-2009: 177Lu-DOTATATE x5 cycles (25.6 GBq) Increased SSA’s dosage Addition of pasireotide 1200μg bid Ca = 10,7 mg/dl, CgA=115 nmol/l, PTHrP=140 pmol/l 2009: DISEASE PROGRESSION (PD)
+ biochemical relapse (Ca = 11,8 mg/dl)

Case History 2009-2010 + Temozolomide + Capecitabine (CAP-TEM) 2009-2010: STABLE DISEASE (SD) Biochemical control of Ca required additional
treatment:SOM230 and SSA’sForced DiuresisPrednisolone 40mg/dBiphosphonates (i.v. zolendronate 4mg monthly)Cinacalcet 90mg/d]
SIDE-EFFECTS: Proximal myopathy - muscle atrophy, patient immobilization (wheel chair), severe Diabetes Mellitus (~100 IU insulin/d)

Case History 2010 Tumor burden reduction (cytoreduction) necessary
Biochemical control (Ca)Reduce treatment side-effects
OPTIONS:Surgery Patient still deniedPRRT Already performed (GFR, marrow toxicity)RF Ablation Not applicable due to large liver
lesionsEmbolization (TAE/TACE)
Pre-embolization evaluation : Portal vein thrombosis
Selective approach (embolization of small branches of hepatic artery)

Case History - TAE
Pre-embolization Post-embolization

Post-embolization status TMZ + Capecitabine SSA’s Pasireotide 1200mcg/d Prednisolone 40 mg/d Zolendronate 4mg/m Insulin treatment
Ca = 10,2 mg/dlCgA = 50 nmol/l
PTHrP = 38 pmol/l
Case History - TAE
TMZ + Capecitabine SSA’s at ½ dosage X Prednisolone 8 mg/d X X

Case History 2010 6 months after TAE Ca = 13,2 mg/dl DISEASE PROGRESSION (PD) Painful lump on left thigh
T1 T2

Case History 2010
Bone scintigraphy Tc 99m

Case History 2010 BONE METASTASES vs BENIGN LESION Bone Biopsy Brown tumor (in the context of
prolonged PTHrP action on bone) New liver lesion biopsy ki67 = 4%, IHC (+) for PTHrP
PTHrP Immunohistochemistry H&E stain
Bone biopsyLiver metastases biopsy

Case History 2010-2012 Temozolomide (200mg/m2 Days 1-5 q4w) +
Bevacizumab (10 mg/kg q2w) + Everolimus (10mg/d) [+SSA’s] Ca = 8,8 mg/dl Temozolomide and Bevacizumab D/C after 6 months
due to thrombocytopenia 2010-2012: STABLE DISEASE (SD)

Case History 2012-2014 2012: DISEASE PROGRESSION (PD) Ca=9,34 mg/dl, PTHrP = 50 pmol/l Sunitinib 37,5 mg/d [+SSA’s] 6 months later: Ca = 6,5 mg/dl !!! 2012-2014: STABLE DISEASE (SD)
April 2014: Patient deceased †(hepatic encephalopathy - malnutrition)

0
20
40
60
80
100
120
140
160
20052001 2006 2006 2008 2009 2009 2009 2010 2010 2010 2012 2012 2014
SSA’s
STZ+5FU
Pegylated INFa
PRRT
Pasireotide
Everolimus Sunitinib
Embolization
PDPD PD PD
CAP-TEM
PD PD
BEV-TEM
PTHrP
Ca
CgA
†

Case synopsis WD pNEN grade 2 Stage IV (liver metastases) Change of functional status during disease course Rare PTHrP secretion (paraneoplastic syndrome) Even more rare: brown tumor due to PTHrP Employment of several treatment agents/modalities to
achieve both tumoral and biochemical control Importance of cytoreductive interventions and novel
molecular targeted therapies in controlling secretory symptoms/syndrome
Long survival despite metastatic disease at presentation (application of different therapeutic modalities)

Improving Survival of NET patients
James Yao, ENETS 2014

![Neuroendocrine Neoplasms of the Pancreas: The Pathological …€¦ · neoplasm of the pancreas, accounting for approximately 1–2% of all pancreatic neoplasms [1, 2]. The incidence](https://static.fdocuments.net/doc/165x107/5f6d4c375d58c6724b1aebea/neuroendocrine-neoplasms-of-the-pancreas-the-pathological-neoplasm-of-the-pancreas.jpg)








![Mucinous Neoplasm: A Case Report A Rare Case of Low-grade ... · cell adenocarcinoma, or neuroendocrine carcinoma [3]. Mucinous adenocarcinoma accounts for Mucinous adenocarcinoma](https://static.fdocuments.net/doc/165x107/5d66f73588c993283a8b59a1/mucinous-neoplasm-a-case-report-a-rare-case-of-low-grade-cell-adenocarcinoma.jpg)